
Submitted:
11 November 2023
Posted:
13 November 2023
You are already at the latest version
Abstract
The management of blunt abdominopelvic trauma with combined hemoperitoneum and pelvic fractures is challenging for trauma surgeons. Although angioembolization can achieve hemostasis in most visceral organ injuries and pelvic fractures after blunt abdominal trauma, it cannot effectively control hemorrhage in patients with blunt bowel mesenteric injury (BBMI). This study aimed to determine the risk factors associated with hemodynamically unstable patients with BBMI and to test the hypothesis that pelvic fracture is an independent risk factor for patients with unstable BBMI and concomitant pelvic fracture to guide the therapeutic sequence for difficult-to-manage patients. This retrospective study reviewed the data of hospitalized patients with trauma between 2009 and 2021 and included 158 adult patients with surgically proven BBMI. The patients were divided on the basis of the presence of a shock episode before emergency laparotomy. The shock group included 44.3% of all patients in the study (n = 70). Clinical injury severity and prognosis for patients in the shock group were poorer than those for patients in the non-shock group, and more invasive treatments and transfusions were performed for patients in the shock group than for those in the non-shock group. Pelvic fractures were more frequently associated in the shock group than in the non-shock group (21.4% vs. 5.7%; p = 0.003). In multivariate analysis, the presence of intracerebral hemorrhage (odds ratio [OR] = 10.87, 95% confidence intervals [CIs]: 1.70–69.75) and rib fracture (OR = 5.94, 95% CIs = 1.06–33.45) were identified as independent predictors of shock, whereas the effect of pelvic fracture did not achieve statistical significance (OR = 2.94, 95% CIs = 0.66–13.13) after adjusting for confounding factors. For patients with BBMI, outcomes need to be improved during early diagnosis and treatments should be expeditiously performed on the basis of the rapid identification of unstable hemodynamic status. In unstable patients with concomitant pelvic fractures, we support the current management algorithm that recommends performing laparotomy first.
Keywords:
blunt abdominal trauma
; blunt bowel mesenteric injuries
; pelvic fracture
; emergency department
; laparotomy
1. Introduction
Despite advances in trauma surgery and care, blunt abdominopelvic injuries remain challenging for trauma surgeons, particularly in the face of hemodynamic instability (HI). In addition to intraperitoneal bleeding from blunt abdominal trauma (BAT), retroperitoneal bleeding should be considered in unstable patients with concomitant pelvic fracture (PF). Similarly, patients with any PF may experience a concomitant intra-abdominal injury from 16% to 42%, which have increased from 62% to77 % in patients with concomitant retroperitoneal hemorrhage and 70% in unstable patients, respectively [1,2,3,4,5]. PF also results in approximately 7% to13% retroperitoneal hemorrhages requiring emergency interventions and 7.6% to 55% HI [3,4,6,7,8,9], contributing to a mortality rate of 4.3% to 19%, and even up to 31% to 46% in unstable patients [4,5,6,8,10,11]. Accordingly, it is difficult to rapidly determine the bleeding source and make decisions in a short period under stressful situations involving HI. It is a good thing that in the ear of non-operative management (NOM), transcatheter arterial embolization (TAE) can achieve hemostasis in most solid organ injuries following BAT and PF [3,8,9,12]. However, it is noteworthy that intra-abdominal injury is easily overlooked in unstable BAT patients with concomitant PF who had received TAE first for hemostasis before computed tomography (CT) examination, in whom blunt bowel mesenteric injuries (BBMIs) accounted for 86% of missed injuries [7]. Given the enthusiasm for NOM, potential shock, regardless of mesentery tear or sepsis as a result of bowel injuries, has been proved to be not only the most common indication for laparotomy but also a reason for NOM failure in BAT patients [7,12]. Although the widespread use of CT enhances the success rate of NOM, the high false-negative rate of CT and the nonspecific clinical presentation in BBMI often lead to delayed management, which increases morbidity and mortality [13,14,15,16,17,18]. However, the CT findings of combined hemopneumoperitoneum and PF in patients with unstable BAT clinically aggravate the management dilemma.
Although numerous publications have established protocol-based algorithm implantation with cavity hemorrhage management in life-threatening patients with PF [8], the therapeutic strategy and sequence of pre-peritoneal packing or TAE for PF still vary in different trauma centers because of the resources available in clinical practice [1,11,19,20]. Clinical studies [19] have reported that hemodynamically unstable BAT patients with concomitant intraperitoneal and retroperitoneal hemorrhage can be treated with post-laparotomy TAE; PF is a useful predictor for this clinical practice. Thorson et al. supported this proposal and suggested that laparotomy should take priority over TAE in patients with hemodynamically unstable PF [11]. By contrast, Eastridge et al. considered that in patients in shock with unstable type PF TAE should be arranged before laparotomy even in the presence of hemoperitoneum [1]. Other studies [20] supported these treatment strategies and reported that difficult-to-manage patients with PF and hemoperitoneum had the same mortality rate regardless of hemodynamic status or initial treatment sequence (laparotomy first or TAE first). Nevertheless, the above-mentioned populations estimated in these studies usually included overall organ injuries within the abdomen (either solid organs or hollow organs) after BAT; the discussion on the context between BBMI necessitating laparotomy and PF is limited.
Although BBMI is the third vulnerable organ after BAT, followed by the liver and spleen, its incidence only accounts for approximately 0.3% to 0.6% of total trauma admissions and 4% to 4.7% of BAT admissions in Taiwan trauma centers [16,21]. Given the high dependence on CT use, rarity of BBMI, and preference for NOM, the challenge for trauma surgeons in the face of surgical BBMI patients continues to evolve. These challenges are further exacerbated by unstable patients with BBMI and concurrent PF. To the best of our knowledge, no study has documented the association between surgical BBMI and HI after considering associated injuries. There is a need to assist with decision-making for an optimal strategy early such that appropriate treatment may be expeditiously administered to unstable patients with BBMI and PF. The objectives of this study were as follows: (1) to investigate the clinical presentation, associated injuries, and outcomes that might correlate with unstable patients with surgical BBMI and (2) to analyze the effect of concurrent PF in the determinants of patients sustaining HI following surgical BBMI to guide the therapeutic sequence.
2. Materials and Methods
2.1. Ethics statement
This study was approved by the Institutional Review Board (IRB) of Chang Gung Memorial Hospital (approval number: 201902275B0). The need for informed consent was waived according to IRB regulations.
2.2. Study population
This retrospective study reviewed all data added to the Trauma Registry System from January 1, 2009, to December 31, 2021, in a 2686-bed facility and Level I regional trauma center that provides care to trauma patients in southern Taiwan. All data were prospectively collected from the medical records of hospitalized patients with trauma and retrospectively analyzed. The patients enrolled in this study were adult trauma patients (>16 years of age) who underwent emergency therapeutic laparotomy for suspected BBMI. During the 13-year investigation period, only patients with BBMI and surgically proven gastrointestinal tract or mesenteric injury were recruited. Patients with isolated stomach, duodenal, or rectal injuries were included. Therapeutic laparotomy was defined as the use of procedures to repair or resect the bowel or control active bleeding. Finally, the included patients were categorized into two groups on the basis of the presence of shock episodes during the period between arrival at the initial emergency department (ED) and emergency laparotomy. Shock was defined as systolic blood pressure (SBP) less than 90 mmHg. Patients with a history of shock before laparotomy were compared with patients without a history of shock episodes, and associated injuries were assessed for their ability to predict the presence of shock.
2.3. Study parameters
The following variables were extracted for each patient: demographic data such as age and sex; clinical and trauma data such as injury severity score (ISS), new ISS (NISS), trauma resuscitation ISS (TRISS), revised trauma score (RTS), and abbreviated injury score (AIS) over the head, face, chest, abdomen, and extremities; vital signs at the ED including SBP, heart rate, respiratory rate, and Glasgow Coma Scale score; injury mechanisms; clinical presentation such as hemoglobin level upon arrival at the ED, incidence of intubation, and tube thoracostomy at the ED; status of blood transfusion (BT) including the incidence of BT at the ED and massive transfusion; amount of packed red blood cells and fresh frozen plasma transfused at the ED within 24 hours and at the operating room and ward; operative findings including the incidence of isolated small bowel injury (defined as gastric, duodenum or small bowel injury including ischemia, rupture, serosa injury, or hematoma), isolated colon injury (defined as colon or rectum injury including ischemia, rupture, serosa injury, or hematoma), isolated mesentery injury (defined as mesentery injury including ischemia, rupture, serosa injury, or hematoma), combined injury (defined as either small bowel or colon injury concomitant with mesenteric injury including ischemia, rupture, serosa injury, or hematoma), and operative blood loss and delayed operation (defined as patients whose emergency laparotomy was performed during the admission to the intensive care unit (ICU) or ward under a miss diagnosis rather than initially at the ED). Outcome data: Morbidity and mortality were classified by cause as either caused by the bowel injury or bleeding injury, 24-hour mortality, and length of stay in the hospital and ICU. Morbidities were identified during chart reviews on the basis of standard definitions. Overall morbidities included sepsis, pneumonia, septic shock, unplanned intubation, intra-abdominal abscess, leakage, coagulopathy, acute kidney injury, acidosis, urinary tract infection, stroke, pulmonary embolism, acute respiratory distress syndrome, pleural effusion, enterocutaneous fistula, wound infection, wound dehiscence, abdominal compartment, tracheostomy, extracorporeal membrane oxygenation (ECMO), return to the operating room, and hemodialysis.
2.4. Statistical analysis
The collected data were compared using IBM SPSS Statistics for Windows (version 20.0; IBM Corp., Armonk, NY). Continuous data were reported as medians and interquartile ranges, whereas categorical data were reported as frequencies and percentages. Two-sided Fisher’s exact test or Pearson’s chi-square test was used to compare the categorical variables. Unpaired Student’s t-test was used to analyze normally distributed continuous variables, whereas the Mann–Whitney U test was used to compare non-normally distributed data. Statistical significance was set at p < 0.05. Factors including age, sex, associated injuries, and BBMI injury pattern according to intra-operative findings that were statistically significant in the univariate analysis were entered into a multivariate regression model to identify independent predictors of shock episodes. Kaplan–Meier analysis was used to identify whether the shock group had a higher risk of morbidity and mortality than the non-shock group. The log-rank test was used to assess the differences in the morbidity and mortality curves between the patient groups.
3. Results
3.1. Patient characteristics, clinical presentation, and outcome
After a detailed chart review, 7 patients were excluded, including those aged <16 years (n = 2) and those who underwent non-therapeutic laparotomy (n = 5). One hundred fifty-eight patents meeting the study criteria for surgically proven BBMI were initially treated in the ED and subsequently admitted to the ward or ICU. Among the 158 patients, gastric injury (n = 1) and duodenal injury (n = 4) were classified as bowel injury types, whereas rectal injury (n = 2) was classified as a colon injury type. Among these, 88 and 70 were respectively assigned to the non-shock group and shock group without differences in age and sex. The most common cause of injury was motorcycle accidents (n = 80, 50.6%). When comparing the non-shock group with shock group, the shock group had more severe anatomic injuries due to ISS (9 versus 21.5, p < 0.001) and NISS (13 versus 27, p < 0.001); physiological injuries due to RTS (7.84 versus 7.108, p < 0.001); probability of survival due to TRISS (0.99 versus 0.97, p < 0.001); worse ED vital signs; a more critical ED clinical presentation; and a greater percentage of transfusion at ED or massive transfusion and transfusion requirements at ED, operative room, and ward or within 24 hours than the non-shock group. Regarding intra-operative findings, the non-shock group had a significantly higher incidence of isolated bowel injury (p < 0.001) and isolated colon injury (p = 0.012) than the shock group, whereas the shock group had a significantly higher incidence of isolated mesenteric injury (p < 0.001) or combined injury (p = 0.004) and a significantly greater amount of operative blood loss (p < 0.001) than the non-shock group. Note that the non-shock group had a significantly higher frequency of delayed operations as compared with the shock group (17% vs. 4.3%, p = 0.012). Additionally, overall morbidity and mortality were greater in the shock group than in the non-shock group (90% vs. 48.9% [p < 0.001] and 27.1% vs. 2.3% [p < 0.001], respectively) (Table 1). On the basis of the results of the Kaplan–Meier analysis, patients in shock had a higher and earlier mortality rate than those who were not in shock. (p < 0.001) (Figure 1).
3.2. Injury severity and injury pattern
The distribution of AIS injuries in each body region in the two groups is shown in Table 2. The shock group had significantly higher injury severity over AIS of the head (p < 0.001), chest (p = 0.05), abdomen (p < 0.001), and extremities (p = 0.014) than the non-shock group. Furthermore, the shock group had more frequency in AIS head ≥ 2 (p < 0.001), AIS head ≥ 3 (p < 0.001), AIS chest ≥ 3 (p = 0.034), and AIS extremities ≥ 2 (p = 0.006) compared with the shock (-) group.
The most commonly associated injured organs were the liver (18.4%), low limb fractures (17.7%), rib fractures (17.1%), and hemopneumothorax (17.1%). PFs were significantly more frequent in the shock group than in the non-shock group (21.4% vs. 12.7%, p = 0.003). A comparison of the incidence of each specific injury between the two groups is presented in Table 3.
3.3. Predicting factors of shock episode
Univariate and subsequent multivariate analyses identified the injury-related risk factors associated with shock episodes (Table 4). Univariate analyses revealed that vessel injury (p = 0.011), intracerebral hemorrhage (ICH) (p = 0.001), rib fracture (p < 0.001), PF (p = 0.006), and lower limb fracture (p = 0.022) were associated with an increased risk of shock. Multivariate analyses revealed that only ICH (OR = 10.87, 95% confidence interval [CI] = 1.70–69.75) and rib fracture (OR = 5.94, 95% CI = 1.06–33.45) were independently associated with the presence of shock. The effect of PF (OR = 2.94, 95% CI 0.66–13.13) during a shock episode was not statistically significant after adjusting confounders. Furthermore, it is expected that isolated mesentery injury (OR = 23.5, 95% CI = 4.61–119.88) and combined injury (OR = 25.43, 95% CI = 4.89–132.28) are strongly independent predictors of shock.
3.4. Overall morbidities
Morbidity rates are shown in Table 5. There were no significant differences in the overall morbidity rates between the groups, except for unplanned ventilation (p < 0.001), coagulopathy (p < 0.001), acute renal failure (p < 0.001), acidosis (p < 0.001), stroke (p = 0.023), abdominal compartment syndrome (p = 0.045), and ECMO intervention (p = 0.037), which were significantly more common in the shock group than in the non-shock group. Additionally, according to the results of the Kaplan–Meier analysis, patients in the shock-positive group had a significantly higher and earlier rate of complications compared with those in the shock-negative patients (p < 0.001) (Figure 2).
4. Discussion
In our series, we analyzed a cohort of patients with surgically proven BBMI and compared the clinical presence of shock episodes in patients with BBMI to determine the risk factors associated with sustaining an unstable hemodynamic status and to assess whether PF was an independent factor in guiding the therapeutic sequence. Particularly remarkable was the fact that near half (44%) of the patients who have hypotension episode in the ED or ICU before surgery had a median ISS of 21.5 and accounted for 65% (55/85) of ISS ≥ 16 and 78% (32/41) of ISS ≥ 25, respectively, thus underscoring the severity of injury in unstable patients with surgical BBMI. Our results showed that patients with shock had worse clinical presentation and increased morbidity and mortality. This finding is also supported by studies [22] that reported that a stable hemodynamic status was related to significantly fewer complications and better outcomes; however, this is not in agreement with the study of Al-Hassani [15]. In addition, some authors believe that given the advances in resuscitation and ICU care, the effect of hemodynamics on the outcomes in patients with BBMI has decreased, and it is not a significant predictor for surgical intervention. Instead, they considered the time to surgery to be a key component for better prognosis and adaptable determinants [23,24]. Malinoski et al. [14] retrospectively studied 195 patients with blunt bowel injuries and concluded that patients who had a delay of more than 5 h between ED arrival and laparotomy had 3.2 times odds of mortality. Meanwhile, in another multicenter study, Fakhry et al. [13] retrospectively studied 198 patients with blunt intestinal injuries and recommended that even a short delay of less than 8 hours in the diagnosis of this injury would increase morbidity and mortality. They reported that, regarding isolated bowel injuries, patients who had a delayed diagnosis had 19.3 the odds of mortality than those who had a prompt diagnosis. Interestingly, a unique finding of our study is that although previous studies have reported poor prognosis in delayed operation, our results showed a significant decrease in the incidence of delayed operation in patients with shock, thus implying that the patient’s unstable hemodynamic status could attract us to acquire more attention and early intervention. Our observation is consistent with that reported by Okishio et al. [24], in which BBMI patients with HI had a significantly shorter time interval between ED admission and surgical intervention than stable patients (109 min vs. 191 min, p = 0.0009). Similarly, this finding is supported by the study by Al-Hassani et al. [15], in which patients with hypotension were significantly more frequently in the group surgically treated within 8 h than in the group treated after 8 h. Conversely, this finding is inconsistent with the study of Hong et al. [25] in evaluating outcomes of delay in surgical intervention for blunt small bowel injuries. They found that patients did not have significantly different percentage of shock in comparison into either three groups (≤8, 8–24, and >24 h) or two groups (≤24 and >24 h). Our results also indicated that BBMI is more easily underestimated in patients with stable hemodynamics after BAT. Although our study did not directly explore the causality between delayed operation and HI, further investigations into the association between shock and the time from admission to surgery are needed.
With regard to associated injuries, BBMI can be a part of patients with polytrauma, which accounts for over half of the cases in a cohort of BBMI and plays a role in determining clinical exhibitions [13,15]. According to our results, there are frequently more hemodynamically unstable patients than stable patients, thus implying that PF is frequently associated with life-threatening BAT. In other words, one of the chief reasons that abdominopelvic trauma is so complicated is the failure to find the concomitant intra-abdominal injuries in a timely manner, with BBMI accounting for only 4.4% of the population with PF [5]. A previous study using Japan Trauma Data Bank (JTDB), including blunt trauma patients with concomitant PF and hemoperitoneum who received laparotomy or TAE as the initial therapeutic intervention, showed that over half of 317 patients (52%) exhibited HI, whereas only 18% of 317 patients involved BBMI-related injuries [20]. Fu et al. [7] retrospectively studied unstable PF patients who received TAE for hemostasis initially without CT survey and concluded that 36% of 41 patients required post-TAE laparotomy because of clinical deterioration after post-TAE imaging, and 86% of whom were associated with surgical BBMI. They also underlined the easy neglect in such patients and importance of early CT imaging after hemodynamic stability. A previous study [15] evaluating the predictors of surgical BBMI reported that PF can aid in the early detection of surgical BBMI without being related to mortality; however, this finding was not supported by Loftus et al. [26], who concluded that any type of PF was not an independent predictor of surgical BBMI after multivariate analysis. The present study indicates that although PF is significantly more likely to occur in unstable BBMI patients than in stable patients, it is no longer significant after controlling for relevant confounders, thus suggesting that it is less likely to be the main cause of HI in unstable BBMI patients with concomitant PF, whose contributing factors to shock can be attributed to rib fracture–related chest trauma or ICH-related head injury. Accordingly, there is a need to investigate the association of contributors to the hemodynamic status between PF and surgical BBMI. Nevertheless, the lower incidence of PF in patients with surgical BBMI (24%) with smaller sample sizes in previous studies makes it more difficult to draw a powerful correlation [15]. In our retrospective analysis, the incidence of PF was 12.7%. Therefore, future large samples prospective studies are still warranted.
Previous evidence has documented that delays of more than five to eight hours for treating surgical BBMI would lead to increased morbidity or mortality [13,14,15], whereas every one hour delay in TAE for PF-related bleeding would have an odds of 1.79 times risk of in-hospital mortality [3]. Given the different resuscitation locations (operative room or angiosuite), it is difficult to prioritize the management of unstable blunt abdominopelvic trauma patients with the possibility of both retroperitoneal bleeding from PF and intraperitoneal bleeding from BAT, which has troubled trauma surgeons; similar publications have been discussed extensively [1,6,7,11,19,20]. Trauma surgeons must weigh the risks of time-consuming negative pelvic angiography versus the risk of active bleeding in mesenteric tears when planning treatment for patients with BBMI with concomitant PF. Even in the absence of pneumoperitoneum, concomitant mild hemoperitoneum and stable-type simple PF pose difficulty to trauma surgeons because these difficult-to-manage patients usually present a life-threatening condition with 52%–87% unstable hemodynamic and 23%–32% mortality rates [6,20]. CT presentation of free fluid without solid organ injuries was a strong independent predictor of BBMI on multivariate analysis in a study by Loftus et al. [26], whereas the size of hemoperitoneum did not indicate a significant peritoneal bleeding requiring therapeutic intervention in patients with PF, even large hemoperitoneum may pose a 30% pseudo-positive possibility in unstable patients with PF without any active intra-abdominal bleeding [6]. In addition, previous studies have mentioned that the outcomes of PF are dependent on the severity of associated injuries and hemodynamics on admission due to the context of multiple traumas rather than the unstable pattern of PF [4]. Even though a simple pelvic ramus fracture might lead to a severe pelvic hemorrhage or an enhancement CT of the PF without the presence of contrast extravasation cannot entirely exclude arterial bleeding, both of which have been described in previous literatures [2,9,27,28]. As mentioned above, rapid decision-making for unstable patients with blunt abdominopelvic trauma despite mild hemoperitoneum and simple PF is challenging for trauma surgeons.
According to the concept and algorithm of Advanced Trauma Life Support, emergency laparotomy appears to be the recommended choice for patients with unstable BAT and PF [29]. The necessity of cavity exploration due to BBMI might impede pre-peritoneal packing, whereas intraperitoneal packing via laparotomy might decrease the abdominal pressure and reduce the tamponade effect for retroperitoneal hemorrhage, as documented in an experimental study [30]. Previous retrospective study evaluating shock patients with unstable pattern PF by Eastridge et al. [1] reported that there was a 25% mortality rate for patients who underwent angiography before laparotomy and a 60% mortality rate for those who underwent laparotomy before angiography. They recommended that TAE should be considered before laparotomy for unstable patients with concomitant hemoperitoneum and unstable type PF because the hemorrhagic origin is predominantly retroperitoneum. Another study from the JTDB concluded that there was no significant difference in the mortality rate in patients with concomitant PF and hemoperitoneum whether they received TAE first or laparotomy first regardless of hemodynamic status [20]. This evidence seems to contradict the current guidelines, which suggest that laparotomy should be performed early in patients with ongoing shock after BAT with concomitant PF [29]. In our experience, we support the current ATLS management algorithm because PF failed to be an independent risk factor for HI in surgical BBMI patients, thus suggesting that clinically significant hypotension is less likely in unstable BBMI patients with PF. Another study [11] by Thorson et al. also supported the same concept. They reported that for unstable patients with PF, those who underwent immediate laparotomy followed by TAE had better mortality rates than those who received TAE first with subsequent laparotomy (20% vs. 67%). Additionally, a study evaluating unstable BAT patients from Wu et al. [19] suggested that post-laparotomy TAE should be considered in unstable BAT patients with concomitant PF, particularly in patients with ISS ≥ 16. Nevertheless, a trauma hybrid operating room should be the optimal option for these difficult-to-manage patients. Given the unusual practice of a hybrid operative room in Taiwan, in our opinion, while facing unstable patients with combined surgical BBMI and PF, the rapid identification of the bleeding source is difficult, and taking priority over laparotomy along with simultaneous preparation of possible subsequent angiography in cases of ongoing HI should diminish the risk of morbidity and mortality.
Limitations
One major weakness, in addition to its retrospective nature and small sample size, was that the main focus of our series was surgically proven BBMI. Therefore, there are limitations to this study regarding associated PFs. Thus, a selection bias may have limited our conclusions. Furthermore, a detailed direct comparison or discussion in patients with concomitant PF was not evaluated, such as TAE first or laparotomy first, quantity of free intraperitoneal fluid, shock duration, resuscitation responders or non-responders, with or without a retroperitoneal contrast brush, or fracture patterns of the pelvis. Rather, we believe that our observations will be helpful in assisting timely decision-making for difficult-to-manage patients in clinical practice. For a robust investigation of the effect of different PFs on the quality of management of surgical BBMI, a larger prospective registry study is necessary to validate our results.
5. Conclusions
In our study, nearly half of patients (44%) experienced shock episodes before surgical intervention and had significantly severe injury severity, critical clinical presentation, and increased morbidity and mortality, reflecting the crucial status clinically in the face of this issue. Although BBMI patients in whom a PF occurs present a significantly higher incidence of HI, BBMI patients with other associated injuries, including rib fracture–related chest trauma or intracerebral hemorrhage, are of greater concern because of the higher probability of HI. Accordingly, especially in patients with unstable BBMI with concomitant PFs, we support the current protocol recommendations suggesting laparotomy first with a damage-control procedure followed by TAE if needed as the management sequence.
Author Contributions
T.-M.H. conceived and wrote the manuscript and performed the analyses. P.-C.C., C.-T.L. and B.-Y.W. contributed to data collection and measurements. F.-J.C. and C.-H.W. were mainly involved in data analysis and quality management. F.-J.C. and C.-H.W. supervised the study, edited the manuscript, and submitted it for publication. F.-J.C. and C.-H.W. contributed equally and are considered co-corresponding authors. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Institutional Review Board (IRB) of Chang Gung Memorial Hospital (approval number: 201902275B0). The need for informed consent was waived according to IRB regulations.
Informed Consent Statement
The need for informed consent was waived owing to the retrospective nature of the study.
Data Availability Statement
Data were obtained from Chang Gung Research Database and are available by corresponding with the author and obtaining permission.
Acknowledgments
We appreciate the statistical support provided by the Biostatistics Center of Kaohsiung Chang Gung Memorial Hospital.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Eastridge, B.J.; Starr, A.; Minei, J.P.; O’Keefe, G.E.; Scalea, T.M. The importance of fracture pattern in guiding therapeutic decision-making in patients with hemorrhagic shock and pelvic ring disruptions. J Trauma. 2002, 53, 446–450; discussion 450–451. [CrossRef]
- Ciriano Hernández, P.; Moreno Hidalgo, A.; Grao Torrente, I.; Ruiz Moreno, C.; Seisdedos Rodrigez, L.; Kayser Mata, S.; Echenagusia Boyra, M.J.; González Leyte, M.; Pérez Díaz, M.D.; Turégano Fuentes, F. Pelvic fractures with associated retroperitoneal hematoma: time until angioembolization and results. Cir Esp (Engl). 2019, 97, 261–267. Fracturas de pelvis con hematoma retroperitoneal asociado: tiempo hasta la angioembolización y resultados. [CrossRef]
- Matsushima, K.; Piccinini, A.; Schellenberg, M.; Cheng, V.; Heindel, P.; Strumwasser, A.; Benjamin, E.; Inaba, K.; Demetriades, D. Effect of door-to-angioembolization time on mortality in pelvic fracture: every hour of delay counts. J Trauma Acute Care Surg. 2018, 84, 685–692. [Google Scholar] [CrossRef]
- Gustavo Parreira, J.; Coimbra, R.; Rasslan, S.; Oliveira, A.; Fregoneze, M.; Mercadante, M. The role of associated injuries on outcome of blunt trauma patients sustaining pelvic fractures. Injury. 2000, 31, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Demetriades, D.; Karaiskakis, M.; Velmahos, G.C.; Alo, K.; Murray, J.; Chan, L. Pelvic fractures in pediatric and adult trauma patients: are they different injuries? J Trauma. 2003, 54, 1146–1151; discussion 1151. [CrossRef]
- Charbit, J.; Millet, I.; Martinez, O.; Roustan, J.P.; Merigeaud, S.; Taourel, P.; Capdevila, X. Does the size of the hemoperitoneum help to discriminate the bleeding source and guide therapeutic decisions in blunt trauma patients with pelvic ring fracture? J Trauma Acute Care Surg. 2012, 73, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Fu, C.Y.; Liao, C.A.; Liao, C.H.; Kang, S.C.; Wang, S.Y.; Hsu, Y.P.; Lin, B.C.; Yuan, K.C.; Kuo, I.M.; Ouyang, C.H. Intra-abdominal injury is easily overlooked in the patients with concomitant unstable hemodynamics and pelvic fractures. Am J Emerg Med. 2014, 32, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Fu, C.Y.; Chan, S.Y.; Wang, S.Y.; Hsieh, C.H.; Liao, C.H.; Huang, J.F.; Hsu, Y.P.; Kang, S.C. The effect of angioembolization for life-threatening retroperitoneal hemorrhage in patients with pelvic fracture. Am J Emerg Med. 2019, 37, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Tesoriero, R.B.; Bruns, B.R.; Narayan, M.; Dubose, J.; Guliani, S.S.; Brenner, M.L.; Boswell, S.; Stein, D.M.; Scalea, T.M. Angiographic embolization for hemorrhage following pelvic fracture: is it “time” for a paradigm shift? J Trauma Acute Care Surg. 2017, 82, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Kido, A.; Inoue, F.; Takakura, Y.; Hoshida, T. Statistical analysis of fatal bleeding pelvic fracture patients with severe associated injuries. J Orthop Sci. 2008, 13, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Thorson, C.M.; Ryan, M.L.; Otero, C.A.; Vu, T.; Borja, M.J.; Jose, J.; Schulman, C.I.; Livingstone, A.S.; Proctor, K.G. Operating room or angiography suite for hemodynamically unstable pelvic fractures? J Trauma Acute Care Surg. 2012, 72, 364–370; discussion 371–372. [CrossRef]
- Hsieh, T.M.; Cheng Tsai, T.; Liang, J.L.; Che Lin, C. Non-operative management attempted for selective high grade blunt hepatosplenic trauma is a feasible strategy. World J Emerg Surg. 2014, 9, 51. [Google Scholar] [CrossRef] [PubMed]
- Fakhry, S.M.; Brownstein, M.; Watts, D.D.; Baker, C.C.; Oller, D. Relatively short diagnostic delays (<8 hours) produce morbidity and mortality in blunt small bowel injury: an analysis of time to operative intervention in 198 patients from a multicenter experience. J Trauma. 2000, 48, 408–414; discussion 414–415. [CrossRef]
- Malinoski, D.J.; Patel, M.S.; Yakar, D.O.; Green, D.; Qureshi, F.; Inaba, K.; Brown, C.V.; Salim, A. A diagnostic delay of 5 hours increases the risk of death after blunt hollow viscus injury. J Trauma. 2010, 69, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Al-Hassani, A.; Tuma, M.; Mahmood, I.; Afifi, I.; Almadani, A.; El-Menyar, A.; Zarour, A.; Mollazehi, M.; Latifi, R.; Al-Thani, H. Dilemma of blunt bowel injury: what are the factors affecting early diagnosis and outcomes. Am Surg. 2013, 79, 922–927. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.H.; Hsieh, F.J.; Chen, C.C.; Cheng, C.T.; Ooyang, C.H.; Hsieh, C.H.; Yang, S.J.; Fu, C.Y. The prognosis of blunt bowel and mesenteric injury-the pitfall in the contemporary image survey. J Clin Med. 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Fakhry, S.M.; Allawi, A.; Ferguson, P.L.; Michetti, C.P.; Newcomb, A.B.; Liu, C.; Brownstein, M.R. ; EAST small bowel perforation (SBP) Multi-Center Study Group. Blunt small bowel perforation (SBP): an Eastern Association for the Surgery of Trauma multicenter update 15 years later. J Trauma Acute Care Surg. 2019, 86, 642–650. [Google Scholar] [CrossRef] [PubMed]
- Bonomi, A.M.; Granieri, S.; Gupta, S.; Altomare, M.; Cioffi, S.P.B.; Sammartano, F.; Cimbanassi, S.; Chiara, O. Traumatic hollow viscus and mesenteric injury: role of CT and potential diagnostic-therapeutic algorithm. Update Surg. 2021, 73, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.Y.; Yang, S.J.; Fu, C.Y.; Liao, C.H.; Kang, S.C.; Hsu, Y.P.; Lin, B.C.; Yuan, K.C.; Wang, S.Y. The risk factors of concomitant intraperitoneal and retroperitoneal hemorrhage in the patients with blunt abdominal trauma. World J Emerg Surg. 2015, 10, 4. [Google Scholar] [CrossRef] [PubMed]
- Katsura, M.; Yamazaki, S.; Fukuma, S.; Matsushima, K.; Yamashiro, T.; Fukuhara, S. Comparison between laparotomy first versus angiographic embolization first in patients with pelvic fracture and hemoperitoneum: a nationwide observational study from the Japan Trauma Data Bank. Scand J Trauma Resusc Emerg Med. 2013, 21, 82. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, T.M.; Chuang, P.C.; Liu, C.T.; Wu, B.Y.; Liu, Y.W.; Hsieh, C.H. Protective role of obesity on trauma impact: A retrospective analysis of patients with surgical blunt bowel mesenteric injury due to road traffic accidents. Risk Manag Healthc Policy. 2022, 15, 1533–1543. [Google Scholar] [CrossRef] [PubMed]
- Salinas-Aragón, L.E.; Guevara-Torres, L.; Vaca-Pérez, E.; Belmares-Taboada, J.A.; Ortiz-Castillo, G.; Sánchez-Aguilar, M. Primary closure in colon trauma. Cir Cir. 2009, 77, 359–364. [Google Scholar] [PubMed]
- Faria, G.R.; Almeida, A.B.; Moreira, H.; Barbosa, E.; Correia-da-Silva, P.; Costa-Maia, J. Prognostic factors for traumatic bowel injuries: killing time. World J Surg. 2012, 36, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Okishio, Y.; Ueda, K.; Nasu, T.; Kawashima, S.; Kunitatsu, K.; Kato, S. Surgical intervention for blunt bowel and mesenteric injury: indications and time intervals. Eur J Trauma Emerg Surg. 2021, 47, 1739–1744. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.Y.; Kim, S.H.; Kim, K.H. Blunt isolated small bowel perforation intervention: does a delay in management matter? Emerg Med Int. 2020, 2020, 7478485. [Google Scholar] [CrossRef]
- Loftus, T.J.; Morrow, M.L.; Lottenberg, L.; Rosenthal, M.D.; Croft, C.A.; Smith, R.S.; Moore, F.A.; Brakenridge, S.C.; Borrego, R.; Efron, P.A.; et al. The impact of prior laparotomy and intra-abdominal adhesions on bowel and mesenteric injury following blunt abdominal trauma. World J Surg. 2019, 43, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Juern, J.S.; Milia, D.; Codner, P.; Beckman, M.; Somberg, L.; Webb, T.; Weigelt, J.A. Clinical significance of computed tomography contrast extravasation in blunt trauma patients with a pelvic fracture. J Trauma Acute Care Surg. 2017, 82, 138–140. [Google Scholar] [CrossRef] [PubMed]
- Krappinger, D.; Zegg, M.; Jeske, C.; El Attal, R.; Blauth, M.; Rieger, M. Hemorrhage after low-energy pelvic trauma. J Trauma Acute Care Surg. 2012, 72, 437–442. [Google Scholar] [CrossRef] [PubMed]
- ATLS Subcommittee; American College of Surgeons’ Committee on Trauma; International ATLS working group. Advanced trauma life support (ATLS®): the ninth edition. J Trauma Acute Care Surg: ninth edition. 2013, 74, 1363–1366. [CrossRef]
- Grimm, M.R.; Vrahas, M.S.; Thomas, K.A. Pressure-volume characteristics of the intact and disrupted pelvic retroperitoneum. J Trauma. 1998, 44, 454–459. [Google Scholar] [CrossRef]
Figure 1.
In-hospital survival rate. Kaplan–Meier curves displaying in-hospital survival for patients who experienced surgical BBMI in shock and non-shock groups.
Figure 1.
In-hospital survival rate. Kaplan–Meier curves displaying in-hospital survival for patients who experienced surgical BBMI in shock and non-shock groups.
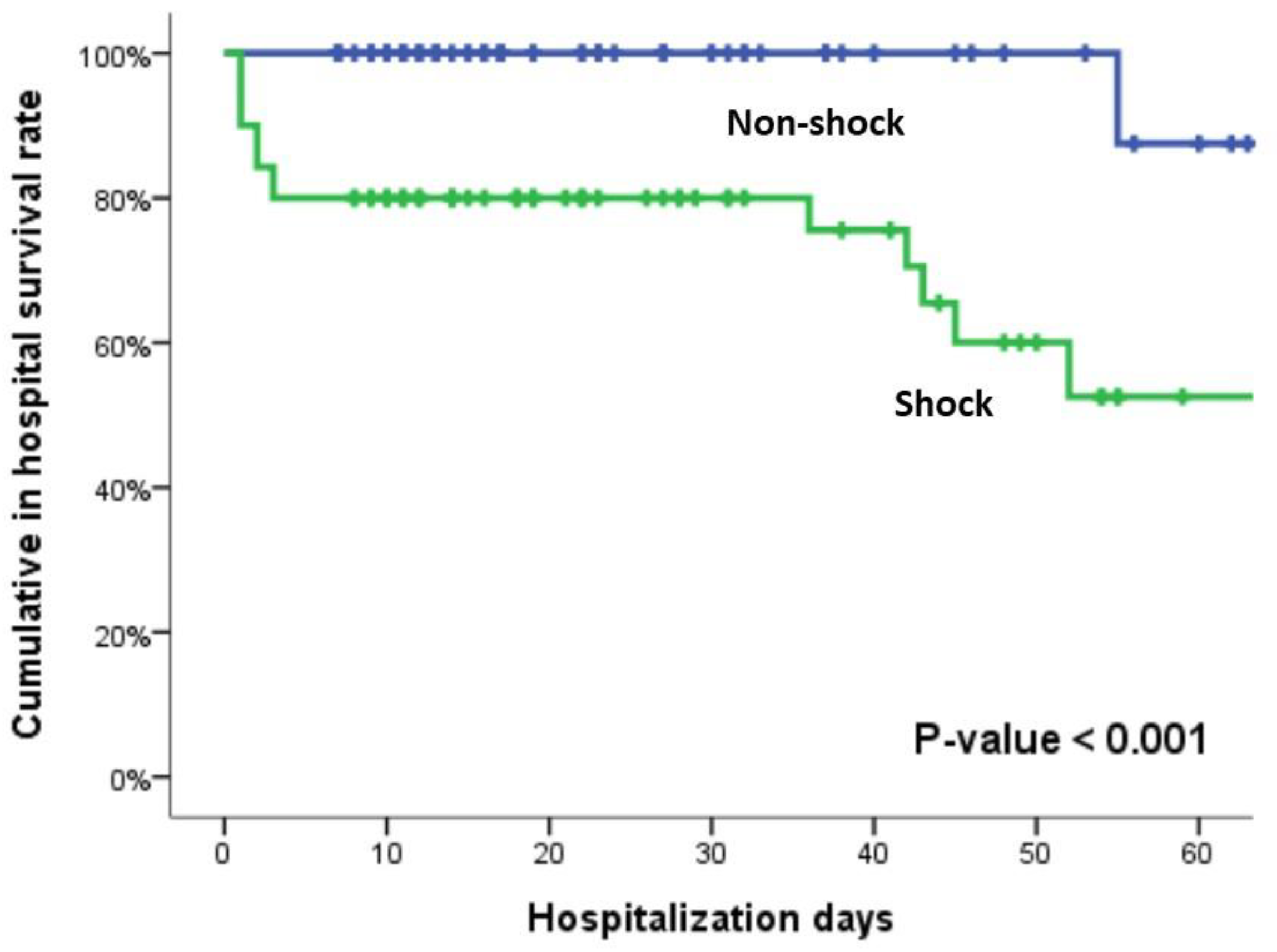
Figure 2.
Kaplan–Meier curves displaying in-hospital morbidity for patients who experienced surgical BBMI in shock-positive and shock-negative groups.
Figure 2.
Kaplan–Meier curves displaying in-hospital morbidity for patients who experienced surgical BBMI in shock-positive and shock-negative groups.
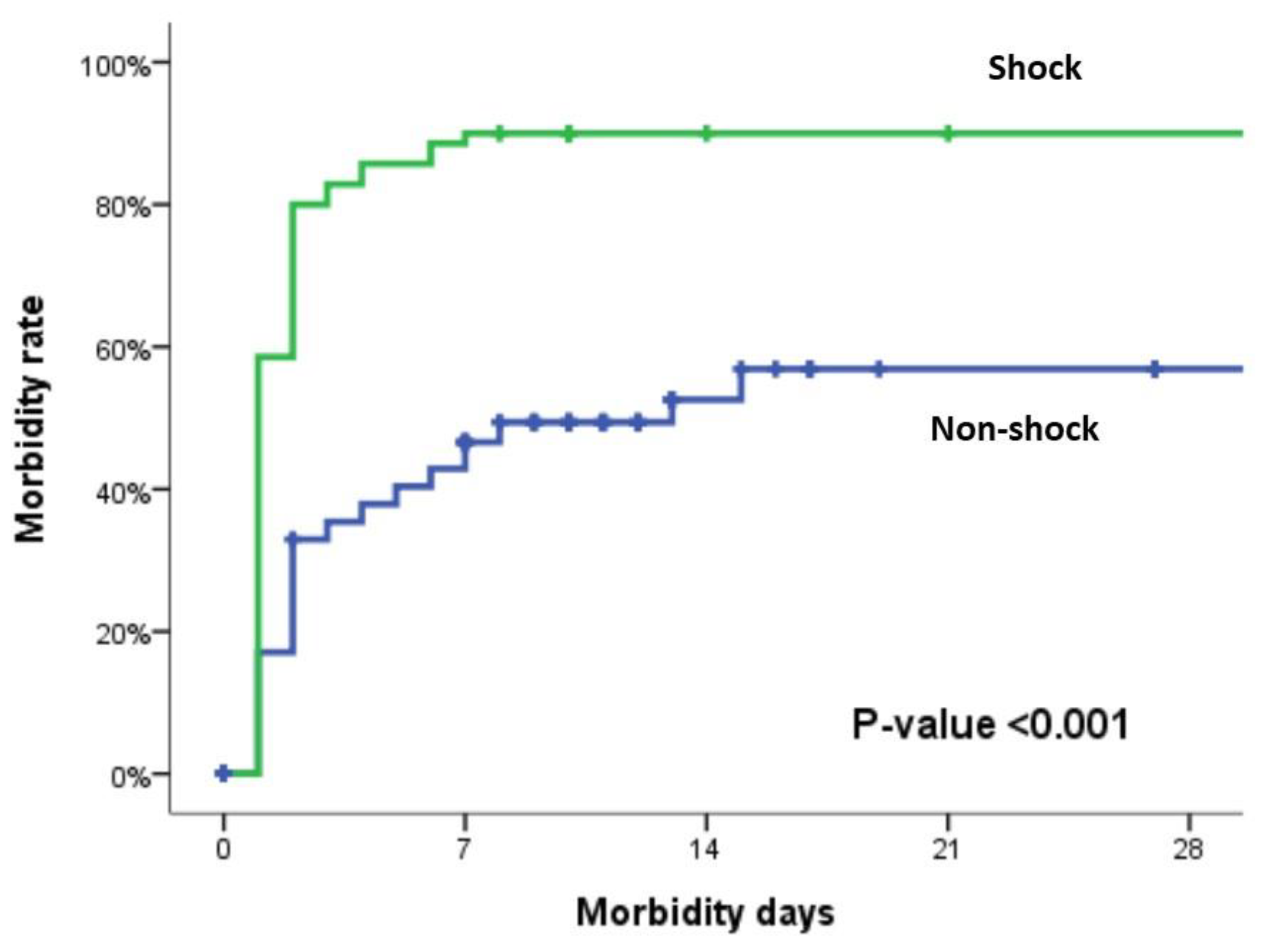

Table 1.
Clinical and injury characteristics of patients with BBMI according to the shock group.
|
Overall (N=158) |
Non-shock (n=88) |
Shock (n=70) |
P value | |
| Age | 46.5 (30-59) | 48.5 (28-60) | 44.5 (33-58) | 0.805 |
| Male sex | 128 (81%) | 75 (85.2%) | 53 (75.7%) | 0.130 |
| ISS | 16 (9-25) | 9 (9-18) | 21.5 (16-29) | <0.001 |
| ISS≥16 | 85 (53.8%) | 30 (34.1%) | 55 (78.6%) | <0.001 |
| ISS≥25 | 41 (25.9%) | 9 (10.2%) | 32 (45.7%) | <0.001 |
| NISS | 18 (9-27) | 13 (9-22) | 27 (17-34) | <0.001 |
| TRISS | 0.99 (0.938-0.735) | 0.99 (0.968-0.994) | 0.97 (0.994-0.938) | <0.001 |
| RTS | 7.84 (7.108-7.84) | 7.84 (7.84-7.84) | 7.108 (6.17-7.84) | <0.001 |
| ED vital sign | ||||
| SBP (mm/Hg) | 116(91-134) | 124(112-140) | 86 (73-123) | <0.001 |
| HR (/min) | 96 (80-117) | 91 (79-104) | 104 (83-126) | 0.020 |
| RR (/min) | 20 (18-20) | 20 (18-20) | 20 (17-22) | 0.671 |
| GCS | 15 (15-15) | 15 (15-15) | 15 (6-15) | <0.001 |
| Mechanism | ||||
| Motorcycle (%) | 80 (50.6%) | 41 (46.6%) | 39 (55.7%) | 0.515 |
| Car (%) | 42 (26.6%) | 22 (25%) | 20 (28.6%) | |
| Fall (%) | 3 (1.9%) | 3 (3.4%) | 0 (0%) | |
| High fall (%) | 6 (3.8%) | 4 (4.5%) | 2 (2.9%) | |
| Pedestrian (%) | 8 (5.1%) | 4 (4.5%) | 4 (5.7%) | |
| Assault (%) | 5 (3.2%) | 4 (4.5%) | 1 (1.4%) | |
| Bicycle (%) | 7 (4.4%) | 5 (5.7%) | 2 (2.9%) | |
| Impact (%) | 7 (4.4%) | 5 (5.7%) | 2 (2.9%) | |
| Clinical presentation | ||||
| ED hemoglobin g/dL | 12.6 (10.7-14.2) | 13.4 (12-14.8) | 11.5 (9-12.7) | <0.001 |
| ED Intubation (%) | 34 (21.5%) | 4 (4.5%) | 30 (42.9%) | <0.001 |
| Chest tube (%) | 31 (19.6%) | 11 (12.5%) | 20 (28.6%) | 0.012 |
| Blood transfusion | ||||
| Blood transfusion at ED (%) | 85 (53.8%) | 22 (25%) | 63 (90%) | <0.001 |
| ED Pack RBC (U) | 2 (0-4) | 0 (0-1) | 4 (2-7) | <0.001 |
| ED FFP (U) | 0 (0-2) | 0 (0-0) | 2 (0-4) | <0.001 |
| 24 HR Pack RBC (U) | 4 (0-12) | 0 (0-4) | 12 (8-21) | <0.001 |
| 24 HR FFP (U) | 2 (0-8) | 0 (0-2) | 9 (4-16) | <0.001 |
| Massive transfusion (%) | 49 (31%) | 3 (3.4%) | 46 (65.7%) | <0.001 |
| OR Pack RBC (U) | 2 (0-6) | 0 (0-2) | 7 (4-12) | <0.001 |
| OR FFP (U) | 0 (0-4) | 0 (0-0) | 4 (2-8) | <0.001 |
| Ward pack RBC (U) | 0 (0-4) | 0 (0-0) | 2 (0-6) | <0.001 |
| Ward FFP (U) | 0 (0-4) | 0 (0-0) | 2 (0-10) | <0.001 |
| Operative finding: | ||||
| Isolated bowel injury (%) | 41 (25.9%) | 38 (43.2%) | 3 (4.3%) | <0.001 |
| Isolated colon injury (%) | 18 (11.4%) | 15 (17%) | 3 (4.3%) | 0.012 |
| Isolated mesentery injury (%) | 48 (30.4%) | 15 (17%) | 33 (47.1%) | <0.001 |
| Combined injury (%) | 51 (32.3%) | 20 (22.7%) | 31 (44.3%) | 0.004 |
| OP blood loss (ml) | 500 (100-2000) | 100 (50-400) | 2000 (1000-3500) | <0.001 |
| Delayed OP | 18 (11.4%) | 15 (17%) | 3 (4.3%) | 0.012 |
| Outcome | ||||
| Morbidity (%) | 106 (67.1%) | 43 (48.9%) | 63 (90%) | <0.001 |
| Mortality (%) | 21 (13.3%) | 2 (2.3%) | 19 (27.1%) | <0.001 |
| 24 hours mortality (%) | 7 (4.4%) | 1 (1.1%) | 6 (8.6%) | 0.045 |
| Bowel related mortality (%) | 5 (3.2%) | 2 (2.3%) | 3 (4.3%) | 0.656 |
| Exsanguination mortality (%) | 11 (7%) | 0 (0%) | 11 (15.7%) | <0.001 |
| ICU length of stay (day) | 3 (2-7) | 2 (0-5) | 4 (2-14) | <0.001 |
| Hospitalization LOS (day) | 17 (11-31) | 16.5 (11-30) | 18 (9-36) | 0.704 |
BBMI, blunt bowel mesentery injury; ISS, injury severity score; NISS, new injury severity score; TRISS, trauma resuscitation injury severity score; RTS, reverse trauma score; ED, emergency department; SBP, systolic blood pressure; HR, heart rate; RR, respiratory rate; GCS, Glasgow Coma Scale; RBC, red blood cell; FFP, fresh frozen plasma; OR, operative room; OP, operation; ICU, intensive care unit; LOS, length of stay; Data were presented as a number (percentage) and median IQR (25–75%).
Table 2.
Severity of injury in body regions of patients with BBMI according to the shock group.
|
Overall (N=158) |
Shock (-) (n=88) |
Shock (+) (n=70) |
P value | |
| AIS head | 0 (0-0) | 0 (0-0) | 0 (0-2) | <0.001 |
| AIS face | 0 (0-0) | 0 (0-0) | 0 (0-0) | 0.413 |
| AIS chest | 0 (0-1) | 0 (0-0) | 0 (0-3) | 0.05 |
| AIS abdomen | 3 (3-4) | 3 (3-3) | 3 (3-4) | <0.001 |
| AIS extremities | 0 (0-2) | 0 (0-2) | 0 (0-2) | 0.014 |
| AIS head ≥2 | 21 (13.3%) | 1 (1.1%) | 20 (28.6%) | <0.001 |
| AIS head ≥3 | 15 (9.5%) | 1 (1.1%) | 14 (20%) | <0.001 |
| AIS face ≥2 | 10 (6.3%) | 4 (4.5%) | 6 (8.6%) | 0.340 |
| AIS face ≥3 | 0 (0%) | 0 (0%) | 0 (0%) | ─ |
| AIS chest≥2 | 38 (24.1%) | 17 (19.3%) | 21 (30%) | 0.119 |
| AIS chest≥3 | 35 (22.2%) | 14 (15.9%) | 21 (30%) | 0.034 |
| AIS abdomen ≥2 | 158 (100%) | 88 (100%) | 70 (100%) | ─ |
| AIS abdomen ≥3 | 144 (91.1%) | 79 (89.8%) | 65 (92.9%) | 0.498 |
| AIS extremities ≥2 | 58 (36.7%) | 24 (27.3%) | 34 (48.6%) | 0.006 |
| AIS extremities ≥3 | 28 (17.7%) | 12 (13.6%) | 16 (22.9%) | 0.132 |
Data were presented as a number (percentage) and median IQR (25–75%). AIS, abbreviated injury score; BBMI, blunt bowel mesentery injury.
Table 3.
Associated injuries of the patients with BBMI according to the shock group.
|
Overall (N=158) |
Shock (-) (n=88) |
Shock (+) (n=70) |
P value | |
| Spleen | 13 (8.2%) | 6 (6.8%) | 7 (10%) | 0.470 |
| Liver | 29 (18.4%) | 13 (14.8%) | 16 (22.9%) | 0.192 |
| Pancreas | 9 (5.7%) | 4 (4.5%) | 5 (7.1%) | 0.511 |
| Urinary bladder | 2 (1.3%) | 2 (2.3%) | 0 (0%) | 0.503 |
| Kidney | 10 (6.3%) | 3 (3.4%) | 7 (10%) | 0.109 |
| Diaphragm | 6 (3.8%) | 3 (3.4%) | 3 (4.3%) | 1.000 |
| Vessel | 23 (14.6%) | 7 (8%) | 16 (22.9%) | 0.008 |
| Intracerebral hemorrhage | 18 (11.4%) | 2 (2.3%) | 16 (22.9%) | <0.001 |
| Skull fracture | 4 (2.5%) | 0 (0%) | 4 (5.7%) | 0.037 |
| Facial bone fracture | 15 (9.5%) | 6 (6.8%) | 9 (12.9%) | 0.275 |
| C-spine | 4 (2.5%) | 2 (2.3%) | 2 (2.9%) | 1.000 |
| Lung contusion | 18 (11.4%) | 7 (8%) | 11 (15.7%) | 0.127 |
| Rib fracture | 27 (17.1%) | 6 (6.8%) | 21 (30%) | <0.001 |
| Clavicle fracture | 10 (6.3%) | 2 (2.3%) | 8 (11.4%) | 0.023 |
| Scapula | 3 (1.9%) | 2 (2.3%) | 1 (1.4%) | 1.000 |
| Hemopneumothorax | 27 (17.1%) | 12 (13.6%) | 15 (21.4%) | 0.196 |
| Thoracic spine fracture | 3 (1.9%) | 2 (2.3%) | 1 (1.4%) | 1.000 |
| Lumbar spine fracture | 8 (5.1%) | 5 (5.7%) | 3 (4.3%) | 1.000 |
| Pelvis fracture | 20 (12.7%) | 5 (5.7%) | 15 (21.4%) | 0.003 |
| Upper limb fracture | 25 (15.8%) | 14 (15.9%) | 11 (15.7%) | 1.000 |
| Lower limb fracture | 28 (17.7%) | 10 (11.4%) | 18 (25.7%) | 0.019 |
Data were presented as a number (percentage). BBMI, blunt bowel mesenteric injury.
Table 4.
Predictors of shock.
| Univariate analysis | Multivariate analysis | |||
| OR (95% CI) | P value | AOR (95% CI) | P value | |
| Age | 1.00 (0.96-1.02) | 0.786 | ─ | ─ |
| Male sex | 0.54 (0.24-1.21) | 0.133 | ─ | ─ |
| Liver | 1.71 (0.76-3.85) | 0.195 | ─ | ─ |
| Kidney | 3.15 (0.78-12.66) | 0.106 | ─ | ─ |
| Vessel | 3.43 (1.32-8.89) | 0.011 | 1.10 (0.32-3.72) | 0.882 |
| ICH | 12.74 (2.82-57.61) | 0.001 | 10.87 (1.70-69.75) | 0.012 |
| Lung contusion | 2.16 (0.79-5.90) | 0.134 | ─ | ─ |
| Rib fracture | 5.86 (2.21-15.51) | <0.001 | 5.94 (1.06-33.45) | 0.043 |
| Hemopneumothorax | 1.73 (0.75-3.98) | 0.199 | ─ | ─ |
| Pelvic fracture | 4.53 (1.56-13.17) | 0.006 | 2.94 (0.66-13.13) | 0.157 |
| Low limb fracture | 2.70 (1.16-6.31) | 0.022 | 1.66 (0.51.41) | 0.405 |
| Operation finding (compare to Isolated bowel injury) | ||||
| Isolated colon injury | 2.53 (0.46-13.98) | 0.286 | ─ | ─ |
| Isolated mesentery injury | 27.86 (7.41-104.78) | <0.001 | 23.50 (4.61-119.88) | <0.001 |
| Combined injury | 19.63 (5.34-72.25) | <0.001 | 25.43 (4.89-132.28) | <0.001 |
OR, odds ratio; AOR, adjusted odds ratio.
Table 5.
Incidence rates of complications among patients with BBMI according to the shock group.
|
Overall (N=158) |
Non-shock (n=88) |
Shock (n=70) |
P value | |
| Sepsis | 25 (15.8%) | 12 (13.6%) | 13 (18.6%) | 0.398 |
| Pumonia | 24 (15.2%) | 9 (10.2%) | 15 (21.4%) | 0.051 |
| Septic shock | 10 (6.3%) | 3 (3.4%) | 7 (10%) | 0.091 |
| Unplanned ventilator | 33 (20.9%) | 8 (9.1%) | 25 (35.7%) | <0.001 |
| Intraabdominal abscess | 17 (10.8%) | 8 (9.1%) | 9 (12.9%) | 0.448 |
| Leakage | 9 (5.7%) | 5 (5.7%) | 4 (5.7%) | 0.993 |
| Coagulopathy | 63 (39.9%) | 14 (15.9%) | 49 (70%) | <0.001 |
| Acute renal failure | 57 (36.1%) | 21 (23.9%) | 36 (51.4%) | <0.001 |
| Acidosis | 46 (29.1%) | 11 (12.5%) | 35 (50%) | <0.001 |
| Urinary tract infection | 26 (16.5%) | 11 (12.5%) | 15 (21.4%) | 0.133 |
| Stroke | 4 (2.5%) | 0 (0%) | 4 (5.7%) | 0.023 |
| Pulmonary embolism | 2 (1.3%) | 1 (1.1%) | 1 (1.4%) | 1.000 |
| ARDS | 5 (3.2%) | 1 (1.1%) | 4 (5.7%) | 0.171 |
| Pleural effusion | 25 (15.8%) | 12 (13.6%) | 13 (18.6%) | 0.398 |
| Enterocutaneous fistula | 2 (1.3%) | 2 (2.3%) | 0 (0%) | 0.503 |
| Wound infection | 33 (20.9%) | 18 (20.5%) | 15 (21.4%) | 0.881 |
| Wound dehiscence | 8 (5.1%) | 2 (2.3%) | 6 (8.6%) | 0.140 |
| Abdomen compartment | 7 (4.4%) | 1 (1.1%) | 6 (8.6%) | 0.045 |
| tracheostomy | 3 (1.9%) | 1 (1.1%) | 2 (2.9%) | 0.585 |
| ECMO | 4 (2.5%) | 0 (0%) | 4 (5.7%) | 0.037 |
| Return to OR | 24 (15.2%) | 9 (10.2%) | 15 (21.4%) | 0.051 |
| Hemodialysis | 3 (1.9%) | 1 (1.1%) | 2 (2.9%) | 0.585 |
Data were presented as a number (percentage). ARDS, acute respiratory distress syndrome; ECMO, Extracorporeal Membrane Oxygenation; OR, operation room.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



