
Submitted:
13 November 2023
Posted:
13 November 2023
You are already at the latest version
Abstract
Several chronic diseases derive from metabolic, genetic, or inflammatory causes and often these causes are interconnected. Pharmacological treatments, although effective, often lead to unpleasant side effects. In this context, preventive approaches are of growing interest. The literature data of recent years support that the dietary intake of bioactive compounds can positively influence the biological functions of an organism.
Among the bioactive compounds in the diet, polyphenols are widely recognized for their beneficial effects on health, as useful compounds for preventing/combating a series of pathologies related to lifestyle, metabolism, and aging. The artichoke (Cynara scolymus L.), a member of the Asteraceae family, is widely used in the food and herbal medicine fields for its beneficial properties. Artichokes are rich in polyphenols (including cynarin), flavonoids and their derivatives, and, for this reason, they have aroused interest in their pharmacological properties. The best-known activity of polyphenols is antioxidant activity. Through it, they help to neutralize free radicals, preventing cellular damage and the subsequent risk of conditions such as cancer, diabetes, and heart disease. Related to the antioxidant action we find the anti-inflammatory activity. This is an important benefit since chronic inflammation is a cause or contributory cause of many chronic diseases.
Although many scientific results are of great interest and potential, there are still gaps to be filled.
In this review, we report and discuss new insights providing documented evidence regarding the benefits of the artichoke compounds and their possible use to support the pharmacological treatment of pathologies associated with inflammation.
Keywords:
artichoke
; inflammation
; physicochemical properties
; functional food
; polyphenols.
1. Introduction
Polyphenols are a broad class of organic substances with important human health benefits. Every day, the diet provides varying amounts of polyphenols, which are concentrated in plant-based products such as fruits, vegetables, spices, nuts, cocoa, tea, and extra virgin olive oil. Some plant sources are particularly rich in polyphenols, which are extracted, concentrated, and marketed for their health benefits [1]. Examples of polyphenol-rich plant extracts include those from artichoke.
Artichoke (Cynara cardunculus var. scolymus), a member of the Asteraceae family, is native to the Mediterranean area (North Africa and southern Europe) and widely used as food and in medicine. Italy holds the world record in the production of this vegetable (approximately 30%): the areas of greatest production are Sicilia, Sardinia, and Apulia [2]. Artichokes leaf extracts contain abundant polyphenols (especially chlorogenic acid and cynarin), flavonoids, and their derivatives known for their health effects [3].
The consumption of artichoke, especially the leaves and the extract, has proven to be effective in reducing the levels of bad cholesterol in the blood, helping to prevent cardiovascular diseases, thanks to the presence of inulin, a fiber, and various acids. Furthermore, artichoke is able to reduce the level of triglycerides. It is also rich in antioxidants useful in counteracting the action of free radicals. Artichokes contain chlorogenic acid (CLA), a strong antioxidant useful in the prevention of cardiovascular and atherosclerotic diseases. In this regard, some Italian scientists, in the middle of the last century, isolated a compound from artichoke leaves, cynarin, the major dicaffeoylquinic acid derivative of artichoke, that seemed to duplicate many of the effects of the whole artichoke [4]. Most studies concerning beneficial effects of artichoke extracts are linked to the antioxidant potential of phenolic contents, such as CLA, caffeic acid, cynarin and flavonoids. Mono- and di-caffeoylquinic acid derivatives are major polyphenols of artichoke [5].
These components have widely attracted scientific interest for their multiple pharmacological properties, such as antioxidant, anti-inflammatory, anti-microbial, lipid-lowering, and anticancer effects [6,7]. It has been reported that artichoke leaf extract (ALE) attenuates oxidative stress and lipoprotein dyshomeostasis in rats fed on high cholesterol diet [8], as well as in streptozotocin-induced diabetic rats [9]. Similarly, the ethanol extract of artichoke exhibited significant protective effects against acute alcohol-induced liver injury, probably through anti-inflammatory and antioxidant effects [10].
Scientific observations have also shown that artichoke exhibits anti-inflammatory effects on tissue plasminogen activator-induced inflammation and antitumor activity in an in vivo carcinogenesis assay [11]. Furthermore, it has been widely reported that artichoke extract is very well tolerated by the human body, as no obvious side effects have been observed even after prolonged administration for several months [12]. For these reasons, artichoke might deserve broad prospects for application in the treatment of chronic inflammation-based diseases due to its antioxidant and anti-inflammatory effects.
Intestinal anti-inflammatory effects of artichoke pectin and modified pectin fractions in the dextran sulfate sodium model of mice colitis have been recently reported, highlighting the significant improvement due to the administration of artichoke pectin of inflammatory bowel disease in the animal model of colitis [13].
In case of intestinal diseases, the vascular barrier, essential for maintaining homeostasis, may be damaged and becomes more permeable. This malfunction of the intestine-vascular unit causes the leakage of inflammatory and bacterial mediators. Once the molecules pass through the bloodstream they can migrate to any organ in the body, including the brain [14].
In this review, we provide a comprehensive summary and present advances in understanding the mechanisms by which artichoke extracts modulate inflammatory biomarkers by exerting a protective role against inflammation and oxidative stress. We also provide perspectives on the use of artichoke extracts in the control of inflammation and suggest further studies that will help evaluate the efficacy of artichoke extracts in the therapy of human inflammatory diseases.
2. Phenolic compounds isolated from ALE (Cynara scolymus L.)
The bioactive richness of ALE is well-documented for the low-fat content and elevated levels of minerals (K, Na, and P), vitamin C, insoluble fibers, and inulin [15] with a notable presence of various phenolic compounds and derivatives that can be categorized into three main classes: flavonoids, phenolic acids, and polyphenolic amides [16]. The class of flavonoids includes cynarins, luteolin, quercetin, and apigenin while the class of phenolic acids in artichoke is mainly represented by chlorogenic, caffeic, and ferulic acids. Further contributing to the overall artichoke polyphenolic content, luteolin-7-O-glucoside and cynaroside belong to the class of polyphenolic amides. Among all these compounds, cynarin stands out as a key player, renowned for its potential hepatoprotective effects [4] and, consequently, studies have delved into its role in promoting liver health, making it a focal point in the exploration of artichoke consumption benefits. Chlorogenic acid (CLA), another prominent constituent of ALE, is widely distributed across plants and fruits. Its widespread acclaim stems from its antioxidant properties contributing to the overall health benefits associated with artichokes significantly [5]. CLA, by mitigating oxidative stress, becomes a valuable component in the pursuit of well-being. Luteolin, quercetin, and apigenin are pivotal elements found in ALE with anti-inflammatory properties and scavenging activities adding a layer of complexity to the spectrum of benefits linked to artichoke consumption. In fact, the range of positive effects spans from cardiovascular support to potential anticancer properties [17]. Still, it should be mentioned that these flavonoids, working in harmony, create a synergy that enhances the overall impact, fostering antioxidant defenses, mitigating inflammation, and contributing to liver protection. The nuanced interplay of these compounds underscores the holistic approach of ALE in conferring health benefits. Whether it be through antioxidant fortification, anti-inflammatory prowess, or liver support, the amalgamation of these bioactive entities paints a comprehensive picture of the potential advantages associated with the consumption of ALE. Noteworthy, the composition of phenolic compounds in ALE can exhibit variability since factors such as the artichoke variety, growing conditions, and the methods employed in the extraction process play a role in shaping the final profile of bioactive components.
Focusing to differences caused by artichoke variety, the study conducted by Negro et al. [18], accounting for a qualitative and quantitative assessment of the phenolic profile of six varieties cultivated in the Mediterranean area. The analysis included three bract orders and various plant parts, including flower heads and leaves, at different developmental stages. Using a HPLC-MS based approach, 14 compounds, belonging to hydroxycinnamate and flavone groups, were identified. The total phenolic content varied significantly between genotypes (P < 0.05) and plant parts (P < 0.01), with ALE generally having higher levels than those extracted from heads. One variety, the "Violet de Provence", displayed the highest phenolic content in both capitula and leaves (66,658.20 and 82,625.63 mg/kg fresh matter, respectively) confirming data provided by previous studies on the same variety [19,20]. In the study carried out by Negro et al. [18] hydroxycinnamic acids, particularly CLA and cynarin, were identified as major compounds, contributing to the choleretic and antioxidant properties of artichoke. Authors also observed a decrease in hydroxycinnamic acids from immature to mature flower heads. Still, luteolin derivatives – especially luteolin-7-O-rutinoside and luteolin-7-O-glucoside – were abundant in flower heads and leaves, with variations across developmental stages. The study found no significant influence of the year on polyphenol content, suggesting that genotype and plant part are primary factors affecting polyphenol levels in artichoke. A different study [7] profiled three different artichoke varieties, including “Violet”, and based on methanolic extracts, the Folin-Ciocalteu colorimetric method used to quantify total phenols in ALE allowed to assess the “Violet” exhibit the lowest phenol amount compared to others, i.e., “Green Globe” and “Imperial Star”.
Besides the instrument (e.g., LC-MS, GC-MS, or NMR) used for the ALE profiling and compound identification, the polyphenol content also fluctuates based on the extraction method employed [21]. On average, CLA (5-O-caffeoylquinic acid) is the most abundant single substance (~39%), followed by other caffeic acid derivatives, such as 1,5-O-dicaffeoylquinic acid (~21%) and 3,4-O-dicaffeoylquinic acid (~11%) [15]. Among phenolic acids, CLA is recognized as the primary substance and, consequently, serves as the marker for quality control in the trade of artichoke herbs. Regarding a specific analytical method for assessing the quality of dry artichoke leaves, The European Pharmacopoeia (Ph. Eur.) stipulates that artichoke leaves used as herbal drugs should contain a minimum of 0.7% chlorogenic acid. However, the defined method, involving heat reflux with two cycles of heating the sample in methanol up to 70 °C for 1 h each, is time-consuming and requires a substantial quantity of organic solvents. Consequently, subsequent various studies have delved into this area of research. Stumpf et al. [22] investigated the suitability of ultrasound-assisted extraction (UAE) as a potential replacement for the standard Ph. Eur. procedure in extracting phenolic compounds from artichoke leaves. This study considered concentrations of specific phenolic compounds and their antioxidant properties, examining additional factors such as the choice of solvent. While organic solvents are commonly used for laboratory analysis, the industry frequently relies on hot water for extracting phenolic compounds from herbal drugs. Stumpf et al. compared the phenolic compound yield from methanol extraction (ME) to that from hot water extraction (HWE). They observed a wide variation in the concentration of CLA, ranging from 0.80% to 3.38% dry matter in ME. The maximum concentration was approximately four times higher than the minimum. Comparisons between ME and UAE extracts showed similar concentrations of CLA and antioxidant capacity whereas UAE extracts exhibited significantly lower levels of total phenolic content, cynaroside (-16%), total flavonoids (-11%), and total phenol content (-2.5%). On average, concentrations of caffeoylquinic acids were 4.5 and 5.1 times higher than flavonoid concentrations for ME and UAE extracts, respectively. Conversely, all parameters measured in HWE extracts were significantly lower than ME, with reductions in CLA (-9.45%), total caffeoylquinic acids (-25.0%), cynaroside (-33.6%), total flavonoids (-22.2%), and total phenol content (-9.7%). Notably, chromatograms of HWE revealed two additional peaks of caffeoylquinic acid derivatives compared to methanolic extracts [22] (Stumpf et al.). Similarly, Garcia-Castello et al. [23] optimized the extraction of these compounds from artichoke wastes using hot-water (89 °C) or hot water–ethanol mixtures (81 °C) as extracting agents. While hot-water proved optimal for simultaneous inulin and polyphenol extraction, water–ethanol (EtOH = 22.4%) extractions yielded the best results in terms of total phenol content (90%) and scavenging activity (38%) despite decreased content of inulin extracted. Using GC-MS profiling, Abd El-Ghany [24] specifically concentrated on peaks of volatile compounds from ALE that varied as the consequence of ethanolic vs. methanolic sample processing, identifying 21 and 22 different VOCs, respectively. A significant disparity was observed for identified VOCs, as well as their relative quantification. In fact, only Luteolin and Homobutein were found in both ALEs, while all other identified compounds (i.e., 19 and 20 for ethanolic vs. methanolic ALEs, respectively) were individually detectable based on the extraction protocol adopted.
3. Biological activities of sesquiterpene lactones derived from artichoke.
Between significant bioactive phytochemical, artichoke also contains considerable amounts of sesquiterpene lactones, such as cynaropicrin, that possess several biological activities. In this regard, cynaropicrin exhibits anti-inflammatory, anti-tumor, antioxidative, antiparasitic, antiphotoaging agent, anti-hyperlipidemic activities and anti-inflammatory properties [25,26].
The bioavailability of both polyphenols and sesquiterpene lactones from artichoke was evaluated using Caco-2 cells monolayers as a model of absorption in the large intestine confirming that artichoke is a nutritionally relevant source of both phenolic compounds and sesquiterpene lactones [27].
The content of sesquiterpene lactones in artichoke leaves is variable and strongly influenced by the cultivar. Apart from cynaropicrin, dehydrocynaropicrin, and grosheimin, the other two sesquiterpene lactones cynaratriol, and 8-deoxy-11,13-dihydroxygrosheimin can be present in a comparable amount in artichoke leaves [28].
The protective and therapeutic potential of cynaropicrin seems to correlate to the increased the expression of several antioxidant genes, such as glutamate–cysteine ligase and heme oxygenase-1, by promoting the activation of the transcription factor nuclear factor E2-related factor 2 (Nrf-2) [29]. Nrf2 is considered the master regulator of natural antioxidant defense; this molecule is able to protect brain cells from ischemic lesions, since, after ischemic damage, the impairment of Nrf2 amplifies the degree of cerebral infarction, aggravating the neurological damage [30]. This natural product has been reported to be involved in the inhibition of NF-κB: Jin et al. reported that cynaropicrin has an anti-inflammatory property associated with the suppression of the NF-κB pathway [31]. In particular, cynaropicrin counteracts in a dose-dependent manner both the oxidative stress and neuroinflammation in an animal model of ischemic/reperfusion injury by inhibiting the NF-κB transcriptional activation pathway. NF-κB activation is known to occur as an immediate reaction to stroke onset and plays a key role in BBB disruption, inflammation, and cell apoptosis, thus suggesting that cynaropicrin can serve as an effective therapeutic agent for cerebral ischemia-reperfusion injury [31]. In addition, cynaropicrin causes potent inhibition of hematopoietic tumor cells in vitro and in vivo by inhibiting c-Myc, STAT3, AKT, and ERK1/2, and by suppressing the tubulin network as reported by Boulos et al. [32].
Matsumoto et al., in addition, demonstrated that the methanolic extract of the leaves of artichoke Cynara scolymus L. was found to inhibit NO production in LPS-stimulated RAW264.7 cells. It was demonstrated, in fact, that six different sesquiterpene lactones, including cynaropicrin, from artichoke leaves were able to inhibit not only NO production but also iNOS induction in LPS-stimulated RAW264.7 cells [33].
Moreover, the anti-inflammatory effects of the artichoke extract and cynaropicrin was also evaluated on Porphyromonas gingivalis (P. gingivalis) LPS-induced expression of inflammatory cytokines in human gingival fibroblasts, which provide a tissue framework for tooth anchorage and function as inflammation regulators being the major cells in periodontal connective tissues. In this work was found that cynaropicrin inhibited IL-8 and IL-6 mRNA and protein synthesis in LPS-stimulated human gingival fibrblasts in a dose-dependent manner and that inhibition of P. gingivalis LPS-induced IL-8 and IL-6 expression by cynaropicrin may be due to the inhibition of the NF-κB pathway. In the same work was also investigated the potential of cynaropicrin to inhibit differentiation of RAW264.7 into osteoclast-like cells, showing that cynaropicrin can reduce drastically RANKL-induced osteoclast differentiation. Cynaropicrin, therefore, seems that may be useful for preventing periodontal diseases and could be a valuable molecule in the development of more efficiently preventative approaches for periodontal diseases [34].
4. Antimicrobial activity of ALE (Cynara scolymus L.)
The surge in antimicrobial resistance has spurred intensive research into alternative therapeutic agents, and plant-derived compounds have emerged as promising candidates [35]. While artichoke extract has a history of medicinal use, its potential as an antimicrobial agent has not been extensively explored although some studies suggest a broad inhibitory activity against various microorganisms until to indicate a potential application in the food industry [36]. Understanding the synergy and interactions between these constituents is crucial for unraveling the mechanisms of artichoke's antimicrobial effects. Research suggests that artichoke extracts exhibit antimicrobial effects through multiple mechanisms. Caffeoylquinic acids, for instance, have been shown to disrupt bacterial cell walls [36,37], while flavonoids may interfere with microbial enzyme activity [38]. These compounds collectively demonstrate a broad spectrum of antimicrobial activity against bacteria, fungi, and even some viruses [24,39,40]. The specific molecular targets of artichoke extracts vary, providing a versatile profile for combating diverse pathogens. Numerous studies have investigated the antibacterial potential of artichoke extracts against both Gram-positive and Gram-negative bacteria. Extracts have shown inhibitory effects on the growth of common pathogens such as Staphylococcus aureus, Escherichia coli, and Salmonella spp. [24,39,40]. The ability of artichoke extracts to modulate bacterial virulence factors further emphasizes their potential role in preventing and treating bacterial infections. Artichoke extracts also exhibit antifungal properties, making them potential candidates for addressing fungal infections. Research has demonstrated inhibitory effects against various fungi, including Candida species [39]. The interference with fungal cell membrane integrity and the modulation of key enzymes contribute to the antifungal efficacy of artichoke extracts. While the antiviral effects of artichoke extracts are less explored compared to antibacterial and antifungal effects, preliminary studies suggest potential inhibitory activity against certain viruses. This includes inhibition of viral replication and interference with viral attachment to host cells [41,42]. However, further investigations are needed to elucidate the specific mechanisms and potential applications in antiviral therapies or concerning the combination between artichoke extracts and antibiotics or antifungals to enhance their efficacy and to reduce the required doses and minimizing the risk of resistance development.
5. Pharmacological Studies of ALE and Health Benefits
Deng et al reported a study regarding the ability of water extract from artichoke (WEA) to ameliorate high-fat diet (HFD)-induced non-alcoholic fatty liver disease in rats [43]. The authors revealed that in this in vivo model, WEA administration to animals determined a marked reduction of both hepatic protein and mRNA levels of pro-inflammatory cytokines (TNF-α, IL-1β, and IL-6) [43]. Interestingly, the histopathological analysis revealed that the livers of rats treated with WEA showed a significant reduction in steatosis, and lobular inflammation. It is known that HFD-induced obesity is associated with insulin resistance and hyperglycemia, however findings of this study showed that treatment with WEA induced a significant decrease in serum glucose and insulin levels, suggesting that serum glucose reduction was not possibly be related to the reduced serum insulin levels. Mechanistically, may be a possible involvement of the insulin signaling pathway. In fact, the PI3K-Akt plays a potential role in the insulin signaling pathway, being a key regulator of gluconeogenesis and glycogen synthesis, thus the observed increase of Akt phosphorylation at Ser473, in in vivo model, suggested a mechanism through which the WEA administration reduces liver insulin resistance [43]. Since inflammation promotes insulin resistance in tissues as the liver, it is possible that inhibiting insulin signal transduction may reduce the inflammatory state observed in WEA-treated rats with non-alcoholic fatty liver disease. Interestingly, previous observations report that artichokes reduced postprandial glycemic and insulinemic responses in normal subjects [4], thus evidencing that improved insulin signaling in the liver might partly be attributable to the reduced inflammation observed in WEA-treated rats [43].
Cynarin, the main derivative of dicaffeoylquinic acid present in artichokes, is a biologically active functional food component. It has various pharmacological properties, including antioxidant activity [5]. Furthermore, cynarin has been shown to exert an inhibitory effect on the expression of the inducible form of NOS (iNOS) induced by a pool of cytokines containing interferon (IFN)-γ, IL-1β and TNF-α in arterial smooth muscle cells human coronary artery [44]. To investigate the mechanisms by which cynarin exerts anti-inflammatory activity, the study conducted by Kim et al showed that cynarin suppressed the lipopolysaccharide (LPS)-induced increase of vascular cell adhesion molecule-1 expression levels and of proinflammatory mediators such as monocyte chemoattractant protein-1 (MCP-1), TNF-α, and IL-1β in human endothelial cells [45]. Furthermore, cynarin inhibited the activation of p38 and NF-κB pathways by inducing the negative regulator of mitogen-activated protein kinase phosphatase 3 (MKP-3) in LPS-stimulated endothelial cells. These observations show that cynarin alleviates inflammation by upregulating MKP-3, a negative regulator of p38 and NF-κB, suggesting that this compound may represent a therapeutic option for the treatment of diseases related to endothelial inflammation [45].
In the following paragraphs we analyze the anti-inflammatory actions of artichoke extracts during gastrointestinal, cardiovascular, and neurodegenerative disorders.
6. Beneficial Health Effects of Artichoke on Inflammatory and Gastrointestinal Diseases
As discussed in various studies bioactive compounds play an important role in modulating inflammation, managing, and preventing many inflammatory diseases, including the inflammatory bowel diseases (IBD) targeting gut microbiota [46,47]. As it was already mentioned, artichoke is a widely consumed vegetable known for its potential health benefits. Its function in relation to inflammatory and gastrointestinal (GI) illnesses is the focus of this section. Although artichoke has a rich culinary history, recent scientific research has revealed its therapeutic properties, indicating its potential to ameliorate various GI disorders and to exert antioxidant and anti-inflammatory effects (Figure 1). This section explores the latest research about the beneficial health effects of artichoke in modulating inflammatory responses, improving GI health, and preventing the GI diseases.
Recent study investigating the health benefits of human serum enriched with ALE on a cellular model and its potential effects on various chronic inflammatory diseases showed protective effect on human hepatocytes against lipotoxic stress. Additionally, ALE was able to prevent the excessive hypertrophy and differentiation of adipocytes and exhibited chondroprotective properties in an inflammatory context. This suggests that plant-derived micronutrients, particularly polyphenols found in artichokes, known with their powerful antioxidant potential could offer a promising alternative aimed at addressing chronic diseases associated with inflammation and metabolic dysregulation [48]. Furthermore, the artichoke extracts, derived from artichoke stems, are rich in phenolic compounds, characterized by low dietary fiber and high carbohydrate content, making them a potential fat-free ingredient with significant antioxidant properties. Of particular interest, is the abundance of chlorogenic acid, a type of caffeoylquinic acid known also by its antioxidant activity. Remarkably, these artichoke extracts exhibited both antioxidant and anti-inflammatory properties when tested on LPS-stimulated human THP-1 macrophages. Considering the critical role of intestinal macrophages in maintaining GI tract homeostasis, recent research has highlighted the significance of these immune cells. Disruptions in macrophage abundance and function have been associated with the disturbances in gut homeostasis, leading to chronic inflammation associated with various GI diseases [49,50]. Based on these findings, it is suggested that Artichoke extract may indirectly contribute to GI homeostasis by influencing intestinal macrophages, implying a potential avenue for further investigation.
Another study by Speciale et al., it was investigated the molecular mechanisms underlying the protective effects of a polyphenol-rich extract obtained from Cynara cardunculus L. leaves (CCLE), widely grown in Mediterranean basin, against acute intestinal inflammation induced by TNF-α in differentiated Caco-2 cells [51]. It is well documented, in fact, that the IBDs are characterized by overactive mucosal immune cells and dysregulated cytokine production, leading to chronic inflammation [52].
CCLE exhibited a protective effect against the activation of the NF-κB pathway induced by TNF-α. Moreover, CCLE was able to modulate the expression of the proinflammatory cytokine IL-8, triggered by NF-κB pathway activation. Additionally, COX-2 expression induced by TNF-α was inhibited by CCLE. Furthermore, CCLE has also demonstrated the ability to enhance cellular antioxidant defense against an altered intracellular redox status induced by TNF-α. This effect involving potentially Nrf2 pathway activation. Despite being considered a waste, CCLE can be used to produce extracts rich in bioactive polyphenols that may be useful in the prevention and treatment of IBDs [51].
In the same context, another study on experimental colitis mouse model found that CCLE treatment attenuated several IBD-related symptoms, including diarrhea and anal edema. While it didn’t promote significant weight recovery. Moreover, CCLE was shown to increase colon length, reduced fecal hemoglobin in a dose-dependent manner, and reduced alkaline phosphatase (ALP) levels in colitic mice. It has also reduced significantly the pro-inflammatory cytokine TNF-α, suggesting an anti-inflammatory effect. Furthermore, CCLE seemed to protect renal function, as evidenced by the decreased urea and creatinine levels. However, it did not reverse hepatic alterations induced by colitis. This study highlights the anti-inflammatory potential of CCLE and suggests its role as a complementary therapeutic approach for IBD management, with potential applications in chronic cases and through oral administration [53].
Additionally, as it was previously demonstrated ALE have also shown choleretic, hepatoprotective, bile-enhancing, anti-microbial, hypocholesterolemic, hypoglycemic and anti-cancer effects in both in vitro and in vivo research [4,54,55,56,57,58,59].
Artichoke by-products are typically discarded even though they contain a high concentration of dietary fibers, phenolic acids, and other micronutrients. Furthermore, artichoke by-products extracted from the stems, leaves and bracts, can be used as a good source of pectin [60].
Given the importance of pectin in ameliorating the manifestations of IBDs, recent emerging research suggests that artichoke pectin exhibited anti-inflammatory effects in mouse model of dextran sodium sulfate (DSS)-induced colitis [61,62].
The mice receiving artichoke pectin have shown reduced inflammatory markers such as: TNF-α, ICAM-I, IL-1β and IL-6 expression. This has resulted in decreased expression of iNOS and TLR4 in favour of reducing inflammation. Interestingly, artichoke pectin increased the intestinal barrier genes expression, MUC-1 and Occludin. These findings suggest that artichoke pectin has the potential to ameliorate IBD through anti-inflammatory actions and promoting the expression of genes associated with intestinal barrier function [13].
Although the etiology of IBD is uncertain, gut microbiota dysbiosis is thought to be a pivotal factor implicated in the pathogenesis of IBD. Indeed, altering the gut microbiota is a pivotal factor in the pathogenesis of many inflammatory bowel diseases [63,64,65]. A recent study conducted by Sasaki et al. has shown that the consumption of artichoke has altered gut microbiota, reduced cecal pH in mice on a high fat diet, raised levels of Short-chain fatty acids, which play an important role in the maintenance of gut and metabolic health. When compared to inulin, they were found to have a different effect on gut microbiota, but a similar effect on SCFA levels and cecal pH. Other bioactive components have been shown to affect the microbiota. The organic extract of this variant of artichoke was predominantly responsible for changing microbiota populations, and that the organic and water-soluble extracts jointly increased SCFA synthesis and decreased cecal pH [66]. Figure 2 reports ALE positive effects both in in vitro and in in vivo model of IBD.
Celiac disease (CD), a common heritable chronic inflammatory condition affecting the small intestine caused by a persistent intolerance to gluten/gliadin (prolamin), is characterized by a complex interplay between genetic and environmental factors [67,68,69]. Moreover, Vacca and colleagues have shown that the gluten-free bread enriched with the leaf extract of artichoke has not only an antioxidant effects but also was found to modulate the expression of pro-inflammatory cytokines in Caco-2 cells including decreasing the cellular expression of TNF-α and IL1-β.
This suggests the possible application of the artichoke extract in developing novel gluten-free products showing improved biological properties that prevent the occurrence of those problems associated with CD [70] (see Figure 2).
Taken together, artichoke, with its anti-inflammatory compounds and beneficial effects on GI tract physiological functions and homeostasis, presents a promising avenue to improve the health and well-being of patients diagnosed with IBDs. The growing evidence highlights the potential of artichoke and its by-products as a valuable bioactive component in the management and prevention of GI disorders associated with chronic inflammation. However, further clinical research is needed to elucidate the underlying mechanisms of action, optimal dosages, and long-term effects of artichoke-based interventions.
7. Anti-inflammatory effects in the cardiovascular system
Cardiovascular diseases (CVDs) represent the main cause of death all over the world. It was estimated that CVDs killed 17.9 million people in 2019, representing 32% of global deaths. Out of these deaths, 85% were due to heart attack and stroke [71].
CVDs refers to broad spectrum of diseases that various criteria can categorized them into different categories. Coronary artery disease, heart failure, myocardial infarction, cardiomyopathies, peripheral vascular diseases, hypertension, and peripheral vascular diseases represent the most known CVDs. The etiology of CVDs is complicated, the risk factors which contribute to CVDs could be unmodifiable (e.g., family history, race, and age) or modifiable (e.g., hypertension, high cholesterol, obesity, type 2 diabetes) [72].
Moreover, these risk factors can trigger oxidative damage, inflammation, fibrosis, and apoptosis, which eventually aggravate the progression of CVDs. These mechanisms, in fact, may induce cardiac hypertrophy, cardiac fibrosis, endothelial dysfunction, vascular stiffness, myocardial ischemia, and, ultimately, CVDs. Therefore, targeting oxidative stress, inflammation, fibrosis, and apoptosis in hypertension, dyslipidemia, and hyperglycemia that eventually contribute to CVDs remains a primary strategy in controlling and managing the development of CVDs.
As also above reported, artichoke is well known for its nutritional values and therapeutic properties, particularly it is a source of antioxidants, and can serve as an alternative treatment for various diseases, and accumulated evidence has proven that artichoke, contains many phytochemical compounds that are considered to be influential in providing various health benefits, especially as having anti-hyperlipidemic, anti-hyperglycemic, anti-hypertensive, antioxidative, anti-inflammatory, and anti-fibrosis effects (Figure 3) [73,74,75].
Artichoke can also be considered a rich source of vitamin C, K and Ca, Fe and Zn [75], as well as polyphenols [76,77,78].
All these components have an important scavenging activity against reactive oxygen species (ROS) and free radicals and perform as a protective shield against oxidative damage to biological molecules, such as proteins, lipids, and DNA [79].
Hyperlipidemia is characterized as an abnormally high concentration of lipids in the blood, such as triglycerides (TG), total cholesterol (TC), and low-density lipoprotein cholesterol (LDL-c) and a reduction in high-density lipoprotein cholesterol (HDL-c) values [80]. This unbalanced lipidic profile is one of the most relevant risk factors for cardiovascular diseases [81]. The most common causes of hyperlipidemia are lifestyle habits (smoking, obesity, and sedentarism), type 2 diabetes, alcohol, lipoprotein lipase mutations, hypothyroidism, and environmental and genetic factors [82].
Different studies have demonstrated that artichoke extracts influence lipid metabolism by decreasing the production of cholesterol and endogenous triglycerides by acting on their excretion or redistribution in the organism. They also enhance bile production by increasing the amount of biliary acids and cholesterol elimination with bile. Salem and coworkers have studied the effect of ALE on the lipidic profile, cardiac markers, and antioxidant levels in obese rats. They have found that the addition of ALE (200 mg/kg and 400 mg/kg) induce in rats an improvement of the lipidic profile due to the decrease in TC, TG, and LDL-c levels and increase in HDL-c levels. Moreover, ALE addition also decreased the cardiac markers and increased the antioxidant enzyme SOD, GPx, and GSH activities [83].
Heidarian and colleagues have studied the response of liver phosphatide phosphohydrolase and lipid profile in hyperlipidemic rats after artichoke extracts addition. The addition of a mix of 10% artichoke in rat pellets for 60 days induces a decrease in the lipids in the serum and the phosphatide phosphohydrolase activity, this led to a decrease in the levels of TG [84].
Subjects with primary mild hypercholesterolemia were treated for 8 weeks with ALE (2 daily doses of 250 mg) and TC, LDL-c/HDL-c and TC/HDL-c ratio levels was significantly reduces instead HDL-c, which plays an important role in the prevention of cardiovascular diseases, resulted increased [85].
To study the modulation of the lipidic profile operated by luteolin, Kwon and coworkers have evaluated the effect of luteolin-enriched artichoke versus artichoke leaf finding that artichoke leaf had a higher effect on the lipidic profile than the luteolin-enriched [86].
Also, CLA induces AMP-activated protein kinase and consequently inhibits sterol regulatory element-binding protein, which results in a reduction in cholesterol synthesis. Moreover, CLA can also induces β-oxidation and inhibit malonyl-CoA, due to carnitine palmitoyl transferase stimulation, this decreases triglycerides levels [87].
Lastly, inulin, results capable of modulating the lipid profile by increasing the conversion of cholesterol in bile salts, subsequently reducing very-low-density lipoprotein and LDL-c serum levels [88].
Since 1930s scientists discovered that artichoke extract had a positive effect on atherosclerotic plaques in the arteries. Artichoke extract prevented a rise in serum cholesterol levels and atherosclerotic plaque manifestations in rats fed with HFD. The effects of artichoke on cholesterol metabolism could be explain in different ways in fact, it increases the breakdown of cholesterol to bile salts, it enhances their elimination by stimulating bile production and flow; it also increases the internal production of cholesterol in the liver. Gebhardt in rat hepatocyte has demonstrated the inhibiting effect of ALE on cholesterol synthesis founding a highly significant concentration dependent inhibition of cholesterol synthesis. The reduction of cholesterol synthesis operated by ALE persisted for some hours following the period of exposure [89].
HMGCoA-reductase is a key enzyme in cholesterol synthesis, and HMG CoA-reductase inhibitors generally reduce total cholesterol, LDL -cholesterol and triglyceride. Artichoke extract acts by inducing an indirect inhibition of the enzyme HMG CoA-reductase, reducing the effects caused by direct inhibitors of HMG CoA-reductase during long-term treatment. In fac, the ALE effectively blocked insulin-dependent stimulation of HMG CoA-reductase without affecting insulin in general. [75,90].
Cardioprotective effect of ALE is also provided by the activity of ALE on the regulation of the endothelial nitric oxide synthase (eNOS) gene. A study has investigated the effects of ALE on cultured human umbilical vein endothelial cells and has demonstrated that treatment with ALE increased activity and expression of the e NOS gene and increased nitric oxide production [91]. The results are confirmed by a randomized placebo-controlled trial conducted on 107 mildly hypertensive or healthy male subjects, which demonstrated a drop in systolic and diastolic blood pressure after 12 weeks oral administration of concentrate artichoke leaf juice [92].
ALE is also known to have antioxidant potential. Many in vitro studies have demonstrated that the antioxidant potential of ALE is due to radical scavenging and metal ion chelating effect of its constituents such as cynarin, CLA and flavonoids [93,94].
The compounds of ALE are also involved in the prevention of development of atherosclerotic plaques. The anti-atherosclerosis action could be the product of two mechanisms: an antioxidant effect that reduced lipoprotein low density (LDL) oxidation and the inhibition of cholesterol synthesis [95].
8. Anti-inflammatory effects in the brain and protective effects in neurodegenerative diseases
The term “neuroinflammation” refers to the inflammatory response of the system central nervous system (CNS) to a neuronal insult, mediated by astrocytes and brain cells microglia, the main cellular mediators of the inflammatory response of the CNS. The cells of microglia constitute the population of resident macrophages of the CNS, where they represent approximately 10% of the total cell population; as well as playing a role fundamental in neurogenesis, plasticity and neuronal regeneration, microglia it is also the first line of defense against any kind of brain damage, having the ability to phagocytose toxins, release cytotoxic factors and perform the function of presenting cells the antigen. In the absence of external stimuli, microglia are in an "inactive" state in which, thanks to its branched cellular morphology, it implements constant monitoring of the neuronal microenvironment without interfering with the activity of surrounding neurons [96]. However, once activated, the microglia undergo a morphological modification that leads to take on a mobile amoeboid shape to be able to reach the site of the insult. The microglial cells can remain active for a long time, releasing cytokines and neurotoxic factors which may in turn contribute to increasing neuronal damage. The activation pattern of these cells has allowed their classification into two phenotypes: the M1 phenotype, or from classical activation, and the M2 phenotype, or from alternative activation. The M1 phenotype responds to stimulation with lipopolysaccharide and produces a massive response inflammatory with the release of IL-1, IL-12, TNF, while the M2 phenotype generally presents an anti-inflammatory profile [97]. The switching from one phenotype to another is a dynamic process in which peripheral inflammation plays a decisive role. Apart microglia, also astrocytes are able to release pro-inflammatory molecules in response to a stimulus. Several evidence indicates that neurodegenerative diseases are accompanied by neuroinflammation chronic, which in turn contributes to the progression of neuronal damage [98,99].
Growing evidence suggests the neuroprotective role of polyphenols: underlying a possible protective effect of polyphenols at the cerebrovascular level can be evoked two main actions. The first concerns the cardiovascular system: many polyphenols have anticoagulant and antiplatelet activity, preventing the possible formation of thrombi, the main cause of cerebral ischemia [100]. In addition, some of these molecules have the ability to reduce hypertension, an important risk factor for cerebral hemorrhage. The second action exerted by polyphenols is neuroprotection, which is not only through a direct action on neurons, but also through an effect on cells that modulate inflammation in the brain, such as microglia [101]. Many polyphenols are able to regulate gene expression without changing the Dna sequence. These molecules can modulate the action of histone deacetylase and histone acetyltransferase, enzymes that control the interaction between Dna and histones, the proteins responsible for compacting and organizing Dna within the cell nucleus. Through controlling gene expression regulatory proteins, such as histone proteins and the transcriptional factor NF-kappaB, polyphenols can thus reduce inflammation and increase the resistance of the heart and brain to harmful stimuli [102]. For example, resveratrol (RSV), a well-known natural compound present in plant species belonging to the flavonoid polyphenol family [103], has been reported to display anti-inflammatory and neuroprotective properties. In this regard, RSV has been reported as a promising candidate and therapeutic agent for Intracerebral Hemorrhage (IHC) since its administration after IHC alleviates neuroinflammation and pro-inflammatory effects of microglia by enhancing Sirt3 expression, thus indicating Sirt3 as a potential target for RSV to inhibit inflammation [104]. Recently a protective effect by micronutrient against ischemic stroke, Alzheimer’s disease (AD), postoperative cognitive dysfunction, and other CNS disorders it was reported [105,106,107].
An impressive body of scientific work has investigated the effect of polyphenols in pre-clinical models of stroke brain [108]. Dozens of compounds have been shown to be effective in both cellular and animal models of stroke. An interesting aspect of this research is that many of the molecules tested promoted a beneficial effect not only when administered before the onset of stroke, but also when brain damage had already been induced. This suggests a potential use of polyphenols not only in a preventive setting, but also in a post-stroke rehabilitation phase [101].
It is widely demonstrated that oxidative stress is related to neuronal functional alterations associated with neurodegenerative diseases, including Parkinson's disease (PD) and AD. DNA damage, oxidative stress, lipid peroxidation and, finally, cell death can be induced by compounds ascribable to nitrosamines. Albeit to a limited extent, there are observations in the literature that report how exposure to diethylnitrosamine (DEN), present in processed or preserved foods, can cause biochemical abnormalities in the brain. Some authors have demonstrated that the methanolic extract of exogenous artichoke leaves (Cynara scolymus) is able to determine an improvement in the deleterious effects induced by DEN in the brain of BALB/c mice [109]. In fact, in this animal model it was observed that the motor alterations and elevated markers of oxidative stress induced by DEN intoxication were markedly restored by treatment with high doses of artichoke extracts. From a mechanistic point of view, the artichoke significantly increased the levels of Klotho and PPARγ, factors with neuroprotective action, in the brain tissue of mice exposed to DEN. A significant reduction in caspase-3 and Bax levels was also observed, while an increase in Bcl-2 was observed following treatment with artichoke. These results led to the conclusion that artichoke exerted neuroprotective effects against DEN-induced brain toxicity through antioxidant and antiapoptotic action [109].
In recent years, there is growing evidence that polyphenols derived from plants have beneficial effects, and therefore they can be exploited for food purposes for their biological properties, using them as unique nutraceuticals for the supplementary treatment of metabolic and/or inflammatory disorders [110]. In particular, the artichoke (Cynara cardunculus) has several beneficial properties for health. Some research has highlighted both anti-inflammatory, antioxidant and anti-bacterial effects, as well as the inhibition of cholesterol biosynthesis, oxidation of low-density lipoproteins [111]. These effects have been attributed to the presence of polyphenolic compounds contained in the artichoke.
In this regard, it was recently found in a mouse model of induced obesity that the ethanolic extract of Cynara cardunculus leaves has beneficial effects on neuroinflammatory parameters.
It is well known that obesity can cause neuroinflammation and increased oxidative stress in the brain [112]. In this regard, in a study conducted by Piccinini et al. in mice subjected to a high-fat diet the effect of the leaf ethanol extract of Cynara cardunculus on inflammatory and oxidative stress in different brain areas, including hypothalamus, prefrontal cortex, hippocampus, striatum, and cerebral cortex, was evaluated [111]. From this study it emerges that the ethanolic extract of C. cardunculus leaves brought benefits to the brain of obese mice by attenuating the production of inflammatory cytokines. These results corroborate those of studies indicating that the leaf ethanolic extract of C. cardunculus may be useful for the treatment of obesity as well as for its anti-inflammatory and antioxidant properties [111].
Santos et al reported that the polyphenolic content and phytosterols present in the artichoke may have a protective effect due to their ability to contain oxidative and inhibit inflammatory and antioxidant inflammatory pathways. In this regard, Guo et al. have demonstrated in in vitro model of encephalitis that CLA it is able to significantly increase cell survival, and reduce the levels of TLR2, TLR9 and Myd88 as well as suppressing the activation of NF-κB, thus interfering with the signaling pathways responsible for inflammatory responses [113].
Polyphenols increase serotonin levels in the brain, brain derived neurotrophic factor (BDNF) production, and reduce inflammation, and this may partly explain their positive effect on mood [114]. Oxidative stress other that induces apoptosis, leading to neuronal damage, is also a crucial factor in neuroinflammation, anxiety, and depression [115,116,117].
Isochlorogenic acid B (ICAB, 3,4-Dicaffeoylquinic acid), a dietary flavonoid found in several plants including artichoke, exhibits multiple pharmacological effects, such as anti-oxidative, anti-inflammatory, and hepatoprotective effect [118,119,120]. Very recently, it was reported a study conducted in a murine model showing that isochlorogenic acid B is able to alleviate lead-induced anxiety, as well as depression and neuroinflammation by the BDNF pathway. Interestingly, ICAB is able to inhibit inflammatory response in brain, decreasing the release of pro-inflammatory cytokines, such as TNF-α and IL-6. and NF-κBp65 phosphorylation, thus suggesting its excellent anti-inflammatory capacity. In addition, ICAB increases the expression levels BDNF, a factor capable of providing neuroprotection against anxiety, depression, and memory impairment by increasing phosphorylation of the transcription factor CREB, implicated in the regulation of genes involved in the expression of numerous proteins related to neurogenesis [121,122].
Chronic oxidative stress may represent a cause for the development of neurodegenerative diseases and free radicals may act as secondary messengers capable to modify inflammatory responses by microglia, altering kinase cascades and activating transcription factors, such as NF-kB [123,124].
Various studies have demonstrated that modulation of an excessive inflammatory response by activated microglial cells may attenuate the severity of neurodegenerative diseases [125,126]. It has been reported in a mouse model of AD that artichoke extracts show neuroprotective efficacy. The neuroprotective efficacy of ALE was recently studied in a murine model of sporadic AD induced by streptozotocin, in a preparation made of solid lipid nanoparticles. In this study, in fact, was shown a significant improvement in cognitive functions and recovery of spatial memory, as well as a marked reduction of the inflammatory biomarker TNF-α. Furthermore, reduced levels of both β-amyloid and tau protein were observed. These results suggest the strong potential of artichoke bracts as an herbal medicine, opening up the use of agro-industrial waste to future medicinal prospects [127].
A study by Mekkey investigated the anti-inflammatory, antioxidant, and anti-apoptotic effects of whole artichoke dry extract in a mouse model of PD. In particular, this study revealed beneficial effects against PD experimentally induced by rotenone, highlighting anti-inflammatory and anti-apoptotic properties in addition to its ability to reduce the expression of alpha synuclein, a pathological hallmark of PD [128].
From what has been illustrated, it emerges that ALE leaf extracts can represent a valid promising botanical therapeutic approach for the treatment of neuroinflammation and pathologies associated with inflammation, including neurodegenerative pathologies (Figure 4). Phytochemical analysis of artichoke bract extract reveals a high concentration of caffeoylquinic acid, apigenin, luteolin, and quercetin, highlighting the richness of the total content of phenols and flavonoids. greater effectiveness of the preparations in order to overcome the problems of bioavailability and/or degradation of the living organism could derive from the use of nanoformulations, such as solid lipid nanoparticles, as reported in a previously mentioned study [127]. In any case, the effectiveness of these compounds is confirmed through evidence of a significant improvement in memory, cognitive functions, motor skills and a significant reduction in inflammatory levels, histopathological and functional signs that distinguish various neurodegenerative pathologies such as AD and PD. Further studies are essential to propose a botanical treatment for neurodegenerative diseases or chronic inflammatory pathologies to be suggested future medicinal perspectives in the therapeutic use of agro-industrial waste such as artichoke bracts.
9. Conclusions
The current review provided the nutritional and phytochemical composition of artichoke and its therapeutic applications as anti-inflammatory functional foods. Artichoke is a plant widely used in the Mediterranean diet and traditional medicine, composed of several bioactive compounds. Different studies have demonstrated that artichoke has the capacity to act as an anti-inflammatory, lipid-lowering, antimicrobial, and neuroprotective agent due to its phytochemical composition (Figure 5).
Thanks to their therapeutic effects, phytopharmaceuticals are gaining increasing importance both as traditional medicine and as modern medicine. New antioxidants can be considered a safe and effective way to strengthen the body's defense system against potentially harmful molecules, such as free radicals and inflammatory mediators. From the analysis of the observations reported in this review it emerges that the compounds extracted from the artichoke can facilitate protection against various inflammatory diseases including neurodegenerative diseases such as AD, PD and others. In conclusion, the compounds extracted from the artichoke can constitute a valid pharmacological support, highlighting medicinal plants as therapeutics in the pathogenesis of various inflammatory diseases.
Further studies are needed to fully comprehend the mechanism of action of artichoke metabolites underlying the biological activities as well as clinical trials to clarify the dose and duration of its therapeutic properties.
Author Contributions
Conceptualization, M.A.P.; writing—original draft preparation, C.P. and T.B.; writing—review and editing, A.C., M.V.; M.C., M.D. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Project funded under the National Recovery and Resilience Plan (NRRP), Mission 4 Component 2 Investment 1.3 - Call for proposals No. 341 of 15 March 2022 of Italian Ministry of University and Research funded by the European Union – NextGenerationEU; Award Number: Project code PE00000003, Concession Decree No. 1550 of 11 October 2022 adopted by the Italian Ministry of University and Research, CUP D93C22000890001, Project title “ON Foods - Research and innovation network on food and nutrition Sustainability, Safety and Security – Working ON Foods”.
Conflicts of Interest
The authors declare that they have no competing financial interest.
References
- Zagoskina, N.V.; Zubova, M.Y.; Nechaeva, T.L.; Kazantseva, V.V.; Goncharuk, E.A.; Katanskaya, V.M.; Baranova, E.N.; Aksenova, M.A. Polyphenols in Plants: Structure, Biosynthesis, Abiotic Stress Regulation, and Practical Applications. Int. J. Mol. Sci. 2023, 24, 13874. [Google Scholar] [CrossRef]
- Gatto, A.; De Paola, D.; Bagnoli, F.; Vendramin, G.G.; Sonnante, G. Population structure of Cynara cardunculus complex and the origin of the conspecific crops artichoke and cardoon. Ann. Bot. 2013, 112, 855–865. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.R.; Jacinto, T.A.; Coutinho, P. Bioactive Compounds from Cardoon as Health Promoters in Metabolic Disorders. Foods. 2022, 11, 336. [Google Scholar] [CrossRef]
- Salem, M.B.; Affes, H.; Ksouda, K.; Dhouibi, R.; Sahnoun, Z.; Hammami, S.; Zeghal, K.M. Pharmacological Studies of Artichoke Leaf Extract and Their Health Benefits. Plant Foods Hum. Nutr. 2015, 70, 441–453. [Google Scholar] [CrossRef]
- Jiménez-Moreno, N.; Cimminelli, M.J.; Volpe, F.; Ansó, R.; Esparza, I.; Mármol, I.; Rodríguez-Yoldi, M.J.; Ancín-Azpilicueta, C. Phenolic Composition of Artichoke Waste and its Antioxidant Capacity on Differentiated Caco-2 Cells. Nutrients. 2019, 11, 1723. [Google Scholar] [CrossRef]
- Turkiewicz, I.P.; Wojdyło, A.; Tkacz, K.; Nowicka, P.; Hernández, F. Antidiabetic, Anticholinesterase and Antioxidant Activity vs. Terpenoids and Phenolic Compounds in Selected New Cultivars and Hybrids of Artichoke Cynara scolymus L. Molecules. 2019, 24, 1222. [Google Scholar] [CrossRef]
- Wang, M.; Simon, J.E.; Aviles, I.F.; He, K.; Zheng, Q.-Y.; Tadmor, Y. Analysis of antioxidative phenolic compounds in artichoke (Cynara scolymus L.). J. Agric. Food Chem. 2003, 51, 601–608. [Google Scholar] [CrossRef]
- Küskü-Kiraz, Z.; Mehmetçik, G.; Dogru-Abbasoglu, S.; Uysal, M. Artichoke leaf extract reduces oxidative stress and lipoprotein dyshomeostasis in rats fed on high cholesterol diet. Phytother. Res. 2010, 24, 565–570. [Google Scholar] [CrossRef]
- Magielse, J.; Verlaet, A.; Breynaert, A.; Keenoy, B.M.; Apers, S.; Pieters, L.; Hermans, N. Investigation of the in vivo antioxidative activity of Cynara scolymus (artichoke) leaf extract in the streptozotocin-induced diabetic rat. Mol. Nutr. Food Res. 2014, 58, 211–215. [Google Scholar] [CrossRef]
- Tang, X.; Wei, R.; Deng, A.; Lei, T. Protective Effects of Ethanolic Extracts from Artichoke, an Edible Herbal Medicine, against Acute Alcohol-Induced Liver Injury in Mice. Nutrients. 2017, 9, 1000. [Google Scholar] [CrossRef]
- Yasukawa, K.; Matsubara, H.; Sano, Y. Inhibitory effect of the flowers of artichoke (Cynara cardunculus) on TPA-induced inflammation and tumor promotion in two-stage carcinogenesis in mouse skin. J. Nat. Med. 2010, 64, 388–391. [Google Scholar] [CrossRef] [PubMed]
- Gebhardt, R. Inhibition of cholesterol biosynthesis in HepG2 cells by artichoke extracts is reinforced by glucosidase pretreatment. Phytother. Res. 2002, 16, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Sabater, C.; Molina-Tijeras, J.A.; Vezza, T.; Corzo, N.; Montilla, A.; Utrilla, P. Intestinal anti-inflammatory effects of artichoke pectin and modified pectin fractions in the dextran sulfate sodium model of mice colitis. Artificial neural network modelling of inflammatory markers. Food Funct. 2019, 10, 7793–7805. [Google Scholar] [CrossRef] [PubMed]
- Carloni, S.; Rescigno, M. Unveiling the gut-brain axis: Structural and functional analogies between the gut and the choroid plexus vascular and immune barriers. Semin. Immunopathol. 2022, 44, 869–882. [Google Scholar] [CrossRef] [PubMed]
- Lattanzio, V.; Kroon, P.A.; Linsalata, V.; Cardinali, A. Globe artichoke: A functional food and source of nutraceutical ingredients. J. Functional Foods. J. Funct. Foods. 2009, 1, 131–144. [Google Scholar] [CrossRef]
- Robards, K. Strategies for the determination of bioactive phenols in plants, fruit and vegetables. J. Chromatogr. A. 2003, 1000, 657–691. [Google Scholar] [CrossRef] [PubMed]
- Crascì, L.; Cardile, V.; Longhitano, G.; Nanfitò, F.; Panico, A. Anti-degenerative effect of Apigenin, Luteolin and Quercetin on human keratinocyte and chondrocyte cultures: SAR evaluation. Drug Res. (Stuttg). 2018, 68, 132–138. [Google Scholar] [CrossRef]
- Negro, D.; Montesano, V.; Grieco, S.; Crupi, P.; Sarli, G.; De Lisi, A.; Sonnante, G. Polyphenol compounds in artichoke plant tissues and varieties. J. Food Sci. 2012, 77, C244–C252. [Google Scholar] [CrossRef] [PubMed]
- Bonasia, A.; Conversa, G.; Lazzizera, C.; Gambacorta, G.; Elia, A. Morphological and qualitative characterization of globe artichoke head from new seed-propagated cultivars. J. Sci. Food Agric. 2010, 90, 2689–2693. [Google Scholar] [CrossRef]
- Lombardo, S.; Pandino, G.; Mauromicale, G.; Knödler, M.; Carle, R.; Schieber, A. Influence of genotype, harvest time and plant part on polyphenolic composition of globe artichoke [Cynara cardunculus L. var. scolymus (L.) Fiori]. Food Chem. 2010, 119, 1175–1181. [Google Scholar] [CrossRef]
- Llorach, R.; Espín, J.C.; Tomás-Barberán, F.A.; Ferreres, F. Artichoke (Cynara scolymus L.) byproducts as a potential source of health-promoting antioxidant phenolics. J. Agric Food Chem. 2002, 50, 3458–3464. [Google Scholar] [CrossRef] [PubMed]
- Stumpf, B.; Künne, M.; Ma, L.; Xu, M.; Yan, F.; Piepho, H.P.; Honermeier, B. Optimization of the extraction procedure for the determination of phenolic acids and flavonoids in the leaves of globe artichoke (Cynara cardunculus var. scolymus L.). J. Pharm. Biomed. Anal. 2020, 177, 112879. [Google Scholar] [CrossRef]
- Garcia-Castello, E.M.; Mayor, L.; Calvo-Ramirez, A.; Ruiz-Melero, R.; Rodriguez-Lopez, A.D. Response Surface Optimization of Inulin and Polyphenol Extraction from Artichoke (Cynara scolymus (L.) Solid Wastes. Appl. Sci. 2022, 12, 7957. [Google Scholar] [CrossRef]
- Abd El-Ghany, Z. Evaluation of Antibacterial Activity, Gas Chromatography Analysis and Antioxidant Efficacy of Artichoke (Cynara scolymus L.). J. Agric. Chem. Biotech. 2017, 8, 265–280. [Google Scholar] [CrossRef]
- Elsebai, M.F.; Mocan, A.; Atanasov, A.G. Cynaropicrin: A Comprehensive Research Review and Therapeutic Potential As an Anti-Hepatitis C Virus Agent. Front. Pharmacol. 2016, 7, 472. [Google Scholar] [CrossRef] [PubMed]
- Possart, K.; Herrmann, F.C.; Jose, J.; Costi, M.P.; Schmidt, T.J. Sesquiterpene Lactones with Dual Inhibitory Activity against the Trypanosoma brucei Pteridine Reductase 1 and Dihydrofolate Reductase. Molecules. 2021, 27, 149. [Google Scholar] [CrossRef]
- Rocchetti, G.; Giuberti, G.; Lucchini, F.; Lucini, L. Polyphenols and Sesquiterpene Lactones from Artichoke Heads: Modulation of Starch Digestion, Gut Bioaccessibility, and Bioavailability following In Vitro Digestion and Large Intestine Fermentation. Antioxidants (Basel). 2020, 9, 306. [Google Scholar] [CrossRef]
- Ingallina, C.; Di Matteo, G.; Spano, M.; Acciaro, E.; Campiglia, E.; Mannina, L.; Sobolev, A.P. Byproducts of Globe Artichoke and Cauliflower Production as a New Source of Bioactive Compounds in the Green Economy Perspective: An NMR Study. Molecules. 2023, 28, 1363. [Google Scholar] [CrossRef]
- De Cicco, P.; Busà, R.; Ercolano, G.; Formisano, C.; Allegra, M.; Taglialatela-Scafati, O.; Ianaro, A. Inhibitory effects of cynaropicrin on human melanoma progression by targeting MAPK, NF-κB, and Nrf-2 signaling pathways in vitro. Phytother. Res. 2021, 35, 1432–1442. [Google Scholar] [CrossRef]
- Zhang, R.; Xu, M.; Wang, Y.; Xie, F.; Zhang, G.; Qin, X. Nrf2-a Promising Therapeutic Target for Defensing Against Oxidative Stress in Stroke. Mol. Neurobiol. 2017, 54, 6006–6017. [Google Scholar] [CrossRef]
- Jin, T.; Leng, B. Cynaropicrin Averts the Oxidative Stress and Neuroinflammation in Ischemic/Reperfusion Injury Through the Modulation of NF-kB. Appl. Biochem. Biotechnol. 2023, 195, 5424–5438. [Google Scholar] [CrossRef]
- Boulos, J.C.; Omer, E.A.; Rigano, D.; Formisano, C.; Chatterjee, M.; Leich, E.; Klauck, S.M.; Shan, L.T.; Efferth, T. Cynaropicrin disrupts tubulin and c-Myc-related signaling and induces parthanatos-type cell death in multiple myeloma. Acta Pharmacol. Sin. 2023, 44, 2265–2281. [Google Scholar] [CrossRef]
- Matsumoto, T.; Nakashima, S.; Nakamura, S.; Hattori, Y.; Ando, T.; Matsuda, H. Inhibitory effects of cynaropicrin and related sesquiterpene lactones from leaves of artichoke (Cynara scolymus L.) on induction of iNOS in RAW264.7 cells and its high-affinity proteins. J. Nat. Med. 2021, 75, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Hayata, M.; Watanabe, N.; Kamio, N.; Tamura, M.; Nodomi, K.; Tanaka, K.; Iddamalgoda, A.; Tsuda, H.; Ogata, Y.; Sato, S.; Ueda, K.; Imai, K. Cynaropicrin from Cynara scolymus L. suppresses Porphyromonas gingivalis LPS-induced production of inflammatory cytokines in human gingival fibroblasts and RANKL-induced osteoclast differentiation in RAW264.7 cells. J. Nat. Med. 2019, 73, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Vaou, N.; Stavropoulou, E.; Voidarou, C.; Tsigalou, C.; Bezirtzoglou, E. Towards Advances in Medicinal Plant Antimicrobial Activity: A Review Study on Challenges and Future Perspectives. Microorganisms. 2021, 9, 2041. [Google Scholar] [CrossRef]
- Wang, L.; Pan, X.; Jiang, L.; Chu, Y.; Gao, S.; Jiang, X.; Zhang, Y.; Chen, Y.; Luo, S.; Peng, C. The Biological Activity Mechanism of Chlorogenic Acid and Its Applications in Food Industry: A Review. Front. Nutr. 2022, 9, 94391–1. [Google Scholar] [CrossRef] [PubMed]
- Makarewicz, M.; Drożdż, I.; Tarko, T.; Duda-Chodak, A. The Interactions between Polyphenols and Microorganisms, Especially Gut Microbiota. Antioxidants (Basel). 2021, 10, 188. [Google Scholar] [CrossRef]
- Donadio, G.; Mensitieri, F.; Santoro, V.; Parisi, V.; Bellone, M.L.; De Tommasi, N.; Izzo, V.; Dal Piaz, F. Interactions with Microbial Proteins Driving the Antibacterial Activity of Flavonoids. Pharmaceutics. 2021, 13, 660. [Google Scholar] [CrossRef]
- Zhu, X.; Zhang, H.; Zhang, H.; Lo, R.; Lu, Y. Antimicrobial Activities of Cynara scolymus L. Leaf, Head, and Stem Extracts. J. Food. Sci. 2006, 70, M149–M152. [Google Scholar] [CrossRef]
- Yildirim, A.B.; Basay, S.; Turker, A.U. A comparison of organically and conventionally grown artichokes: Phenolic constituents, antioxidant and antibacterial activities. Acta Alimentaria. 2020, 49, 69–75. [Google Scholar] [CrossRef]
- Chojnacka, K.; Skrzypczak, D.; Izydorczyk, G.; Mikula, K.; Szopa, D.; Witek-Krowiak, A. Antiviral Properties of Polyphenols from Plants. Foods. 2021, 10, 2277. [Google Scholar] [CrossRef] [PubMed]
- Zakaryan, H.; Arabyan, E.; Oo, A.; Zandi, K. Flavonoids: Promising natural compounds against viral infections. Arch Virol. 2017, 162, 2539–2551. [Google Scholar] [CrossRef]
- Deng, A.; Liu, F.; Tang, X.; Wang, Y.; Xie, P.; Yang, Q.; Xiao, B. Water extract from artichoke ameliorates high-fat diet-induced non-alcoholic fatty liver disease in rats. 2022. BMC Complement Med. Ther. 2022, 22, 308. [Google Scholar] [CrossRef]
- Xia, N.; Pautz, A.; Wollscheid, U.; Reifenberg, G.; Förstermann, U.; Li, H. Artichoke, cynarin and cyanidin downregulate the expression of inducible nitric oxide synthase in human coronary smooth muscle cells. Molecules. 2014, 19, 3654–3668. [Google Scholar] [CrossRef]
- Kim, D.B.; Unenkhuu, B.; Kim, G.J.; Kim, S.W.; Kim, H.S. Cynarin attenuates LPS-induced endothelial inflammation via upregulation of the negative regulator MKP-3. Anim. Cells Syst. (Seoul). 2022, 26, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Benameur, T.; Porro, C.; Twfieg, M.-E.; Benameur, N.; Panaro, M.A.; Filannino, F.M.; Hasan, A. Emerging Paradigms in Inflammatory Disease Management: Exploring Bioactive Compounds and the Gut Microbiota. Brain Sci. 2023, 13, 1226. [Google Scholar] [CrossRef] [PubMed]
- Valdes, A.M.; Walter, J.; Segal, E.; Spector, T.D. Role of the Gut Microbiota in Nutrition and Health. BMJ. 2018, 361, k2179. [Google Scholar] [CrossRef]
- Wauquier, F.; Boutin-Wittrant, L.; Viret, A.; Guilhaudis, L.; Oulyadi, H.; Bourafai-Aziez, A.; Charpentier, G.; Rousselot, G.; Cassin, E.; Descamps, S.; et al. Metabolic and Anti-Inflammatory Protective Properties of Human Enriched Serum Following Artichoke Leaf Extract Absorption: Results from an Innovative Ex Vivo Clinical Trial. Nutrients. 2021, 13, 2653. [Google Scholar] [CrossRef]
- Yip, J.L.K.; Balasuriya, G.K.; Spencer, S.J.; Hill-Yardin, E.L. The Role of Intestinal Macrophages in Gastrointestinal Homeostasis: Heterogeneity and Implications in Disease. Cell. Mol. Gastroenterol. Hepatol. 2021, 12, 1701–1718. [Google Scholar] [CrossRef]
- Carpentieri, S.; Augimeri, G.; Ceramella, J.; Vivacqua, A.; Sinicropi, M.S.; Pataro, G.; Bonofiglio, D.; Ferrari, G. Antioxidant and Anti-Inflammatory Effects of Extracts from Pulsed Electric Field-Treated Artichoke By-Products in Lipopolysaccharide-Stimulated Human THP-1 Macrophages. Foods (Basel, Switzerland). 2022, 11, 2250. [Google Scholar] [CrossRef]
- Speciale, A.; Muscarà, C.; Molonia, M.S.; Toscano, G.; Cimino, F.; Saija, A. In Vitro Protective Effects of a Standardized Extract From Cynara Cardunculus L. Leaves against TNF-α-Induced Intestinal Inflammation. Front. Pharmacol. 2022, 13, 809938. [Google Scholar] [CrossRef] [PubMed]
- Ahluwalia, B.; Moraes, L.; Magnusson, M.K.; Öhman, L. Immunopathogenesis of inflammatory bowel disease and mechanisms of biological therapies. Scand. J. Gastroenterol. 2018, 53, 379–389. [Google Scholar] [CrossRef]
- Mateus, V.; Estarreja, J.; Silva, I.; Barracosa, P.; Teixeira-Lemos, E.; Pinto, R. Effect of Cynara cardunculus L. var. altilis (DC) in Inflammatory Bowel Disease. Appl. Sci. 2021, 11, 1629. [Google Scholar] [CrossRef]
- Ebrahimi-Mameghani, M.; Asghari-Jafarabadi, M. Rezazadeh KTCF7L2-rs7903146 polymorphism modulates the effect of artichoke leaf extract supplementation on insulin resistance in metabolic syndrome: A randomized double-blind placebo-controlled trial. J. Integr. Med. 2018, 16, 329–334. [Google Scholar] [CrossRef]
- Al-Ahdab, M.J. Protective effect of artichoke (Cynara scolymus L.) leaves and pulp extracts against carbon tetrachloride-induced acute hepatotoxicity in rats. World Appl. Sci. J. 2014, 32, 1004–1014. [Google Scholar]
- El Sohaimy, S.A. Chemical composition, antioxidant and antimicrobial potential of artichoke. Open Nutraceuticals J. 2014, 7, 15–20. [Google Scholar] [CrossRef]
- Rezazadeh, K.; Rahmati-Yamchi, M.; Mohammadnejad, L.; Ebrahimi-Mameghani, M.; Delazar, A. Effects of artichoke leaf extract supplementation on metabolic parameters in women with metabolic syndrome: Influence of TCF7L2-rs7903146 and FTO-rs9939609 polymorphisms. Phytother Res. 2018, 32, 84–93. [Google Scholar] [CrossRef]
- Rondanelli, M.; Opizzi, A.; Faliva, M.; Sala, P.; Perna, S.; Riva, A.; Morazzoni, P.; Bombardelli, E.; Giacosa, A. Metabolic management in overweight suIs withIe impaired fasting glycaemia by means of a highly standardized extract from Cynara scolymus: A double-blind, placebo-controlled, randomized clinical trial. Phytother. Res. 2014, 28, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Amini, M.R.; Sheikhhossein, F.; Talebyan, A.; Bazshahi, E.; Djafari, F.; Hekmatdoost, A. Effects of Artichoke Supplementation on Liver Enzymes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin. Nutr. Res. 2022, 11, 228–239. [Google Scholar] [CrossRef]
- Sabater, C.; Corzo, N.; Olano, A.; Montilla, A. Enzymatic extraction of pectin from artichoke (Cynara scolymus L.) by-products using Celluclast®1.5L. Carbohydr. Polym. 2018, 190, 43–49. [Google Scholar] [CrossRef]
- Jin, M.; Wang, Y.; Yang, X.; Yin, H.; Nie, S.; Wu, X. Structure characterization of a polysaccharide extracted from noni (Morinda citrifolia L.) and its protective effect against DSS-induced bowel disease in mice. Food Hydrocolloids. 2019, 90, 189–197. [Google Scholar] [CrossRef]
- Pacheco, M.T.; Vezza, T.; Diez-Echave, P.; Utrilla, P.; Villamiel, M.; Moreno, F.J. Anti-inflammatory bowel effect of industrial orange by-products in DSS-treated mice. Food Funct. 2018, 9, 4888–4896. [Google Scholar] [CrossRef]
- Khan, I.; Ullah, N.; Zha, L.; Bai, Y.; Khan, A.; Zhao, T.; Che, T.; Zhang, C. Alteration of Gut Microbiota in Inflammatory Bowel Disease (IBD): Cause or Consequence? IBD Treatment Targeting the Gut Microbiome. Pathogens. 2019, 8, 126. [Google Scholar] [CrossRef]
- Nishida, A.; Inoue, R.; Inatomi, O.; Bamba, S.; Naito, Y.; Andoh, A. Gut microbiota in the pathogenesis of inflammatory bowel disease. Clin. J. Gastroenterol. 2018, 11, 1–10. [Google Scholar] [CrossRef]
- Hold, G.L.; Smith, M.; Grange, C.; Watt, E.R.; El-Omar, E.M.; Mukhopadhya, I. Role of the gut microbiota in inflammatory bowel disease pathogenesis: What have we learnt in the past 10 years? World J. Gastroenterol. 2014, 20, 1192–1210. [Google Scholar] [CrossRef]
- Sasaki, H.; Lyu, Y.; Nakayama, Y.; Nakamura, F.; Watanabe, A.; Miyakawa, H.; Nakao, Y.; Shibata, S. Combinatorial Effects of Soluble, Insoluble, and Organic Extracts from Jerusalem Artichokes on Gut Microbiota in Mice. Microorganisms. 2020, 8, 954. [Google Scholar] [CrossRef]
- Ferretti, G.; Bacchetti, T.; Masciangelo, S.; Saturni, L. Celiac disease, inflammation and oxidative damage: A nutrigenetic approach. Nutrients. 2012, 4, 243–257. [Google Scholar] [CrossRef]
- Sollid, L.M.; Jabri, B. Triggers and drivers of autoimmunity: Lessons from coeliac disease. Nat. Rev. Immunol. 2013, 13, 294–30. [Google Scholar] [CrossRef]
- Barone, M.V.; Auricchio, R.; Nanayakkara, M.; Greco, L.; Troncone, R.; Auricchio, S. Pivotal Role of Inflammation in Celiac Disease. Int. J. Mol. Sci. 2022, 23, 7177. [Google Scholar] [CrossRef]
- Vacca, M.; Pinto, D.; Annunziato, A.; Ressa, A.; Calasso, M.; Pontonio, E.; Celano, G.; De Angelis, M. Gluten-Free Bread Enriched with Artichoke Leaf Extract In Vitro Exerted Antioxidant and Anti-Inflammatory Properties. Antioxidants. 2023, 12, 845. [Google Scholar] [CrossRef]
- Kim, H.C. Epidemiology of cardiovascular disease and its risk factors in Korea. Glob. Health Med. 2021, 3, 134–141. [Google Scholar] [CrossRef]
- Frąk, W.; Wojtasińska, A.; Lisińska, W.; Młynarska, E.; Franczyk, B.; Rysz, J. Pathophysiology of Cardiovascular Diseases: New Insights into Molecular Mechanisms of Atherosclerosis, Arterial Hypertension, and Coronary Artery Disease. Biomedicines. 2022, 10, 1938. [Google Scholar] [CrossRef]
- Ożarowski, M.; Karpiński, T.M.; Szulc, M.; Wielgus, K.; Kujawski, R.; Wolski, H.; Seremak-Mrozikiewicz, A. Plant Phenolics and Extracts in Animal Models of Preeclampsia and Clinical Trials-Review of Perspectives for Novel Therapies. Pharmaceuticals. 2021, 14, 269. [Google Scholar] [CrossRef] [PubMed]
- Newman, D.J.; Cragg, G.M. Natural Products Sources of New Drugs over the Nearly Four Decades from 01/1981 to 09/2019. J. Nat. Prod. 2020 83, 770–803. [CrossRef]
- D’Antuono, I.; Carola, A.; Sena, L.M.; Linsalata, V.; Cardinali, A.; Logrieco, A.F.; Colucci, M.G.; Apone, F. Artichoke Polyphenols Produce Skin Anti-Age Effects by Improving Endothelial Cell Integrity and Functionality. Molecules. 2018, 23, 2729. [Google Scholar] [CrossRef]
- Mandim, F.; Petropoulos, S.A.; Fernandes, Â.; Santos-Buelga, C.; Ferreira, I.C.F.R.; Barros, L. Chemical Composition of Cynara Cardunculus L. var. altilis Heads: The Impact of Harvesting Time. Agronomy. 2020, 10, 1088. [Google Scholar] [CrossRef]
- Zayed, A.; Serag, A.; Farag, M.A. Cynara cardunculus L.: Outgoing and potential trends of phytochemical, industrial, nutritive and medicinal merits. J. Funct. Foods. 2020, 69, 103937. [Google Scholar] [CrossRef]
- Gouveia, S.C.; Castilho, P.C. Phenolic composition and antioxidant capacity of cultivated artichoke, Madeira cardoon and artichoke-based dietary supplements. Food Res. Int. 2012, 48, 712–724. [Google Scholar] [CrossRef]
- Ceccarelli, N.; Curadi, M.; Picciarelli, P.; Martelloni, L.; Sbrana, C.; Giovannetti, M. Globe artichoke as functional food. Mediterr. J. Nutr. Metab. 2010, 3, 197–201. [Google Scholar] [CrossRef]
- Liu, J.; Rajendram, R.; Zhang, L. Effects of Oleanolic Acid and Maslinic Acid on Glucose and Lipid Metabolism: Implications for the Beneficial Effects of Olive Oil on Health. In Olives and Olive Oil in Health and Disease Prevention; Elsevier: Amsterdam, The Netherlands, 2010; pp. 1423–1429. [Google Scholar] [CrossRef]
- Avci, E.; Dolapoglu, A.; Akgun, D. Role of Cholesterol as a Risk Factor in Cardiovascular Diseases. In Cholesterol—Good, Bad and the Heart; IntechOpen: London, UK, 2018. [Google Scholar] [CrossRef]
- Nirosha, K.; Divya, M.; Vamsi, S.; Sadiq, M. A review on hyperlipidemia. Int. J. Novel Trends Pharm. Sci. 2014, 4, 81–92. Available online: https://scienztech.org/index.php/ijntps/article/view/112.
- Salem, M.B.; Affes, H.; Dhouibi, R.; Charfi, S.; Turki, M.; Hammami, S.; Ayedi, F.; Sahnoun, Z.; Zeghal, K.M.; Ksouda, K. Effect of Artichoke ynaraa scolymus) on cardiac markers, lipid profile and antioxidants levels in tissue of HFD-induced obesity. Arch. Physiol. Biochem. 2022, 128, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Heidarian, E.; Rafieian-Kopaei, M. Protective effect of artichoke (Cynara scolymus) leaf extract against lead toxicity in rat. Pharm. Biol. 2013, 51, 1104–1109. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Giacosa, A.; Opizzi, A.; Faliva, M.A.; Sala, P.; Perna, S.; Riva, A.; Morazzoni, P.; Bombardelli, E. Beneficial effects of artichoke leaf extract supplementation on increasing HDL-cholesterol in subjects with primary mild hypercholesterolaemia: A double-blind, randomized, placebo-controlled trial. Int. J. Food Sci. Nutr. 2013, 64, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Kwon, E.Y.; Kim, S.Y.; Choi, M.S. Luteolin-Enriched Artichoke Leaf Extract Alleviates the Metabolic Syndrome in Mice with High-Fat Diet-Induced Obesity. Nutrients. 2018, 10, 979. [Google Scholar] [CrossRef]
- Santos, H.O.; Bueno, A.A.; Mota, J.F. The effect of artichoke on lipid profile: A review of possible mechanisms of action. Pharmacol. Res. 2018, 137, 170–178. [Google Scholar] [CrossRef]
- Davidson, M.H.; Maki, K.C. Effects of Dietary Inulin on Serum Lipids. J. Nutr. 1999, 129, 1474S–1477S. [Google Scholar] [CrossRef] [PubMed]
- Gebhardt, R.; Fausel, M. Antioxidant and hepatoprotective effects of artichoke extracts and constituents in cultured rat hepatocytes. Toxicol In Vitro. 1997, 11, 669–672. [Google Scholar] [CrossRef] [PubMed]
- Ernst, E.; De Smet, P.A.; Shaw, D.; Muraay, V. Traditional remedies and the test of time. Eur. J. Clin. Pharmacol. 1998, 54, 99–100. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Xia, N.; Brausch, I.; Yao, Y.; Förstermann, U. Flavonoids from artichoke (Cynara scolymus L.) up-regulate endothelial-type nitric-oxide synthase gene expression in human endothelial cells. J. Pharmacol. Exp. Ther. 2004, 310, 926–932. [Google Scholar] [CrossRef]
- Roghani-Dehkordi, F.; Kamkhah, A.F. Artichoke leaf juice contains antihypertensive effect in patients with mild hypertension. J. Diet Suppl. 2009, 6, 328–341. [Google Scholar] [CrossRef]
- Perez-Garcia, F.; Adzet, T.; Caniqueral, S. Activity of artichoke leaf extract on reactive oxygen species in human leukocytes. Free Radic. Res. 2000 33, 661–665. [CrossRef]
- Valerio, F.; De Bellis, P.; Lonigro, S.L.; Morelli, L.; Visconti, A.; Lavermicocca, P. In vitro and in vivo survival and transit tolerance of potentially probiotic strains carried by artichokes in the gastrointestinal tract. Appl. Environ. Microbiol. 2006, 72, 3042–3045. [Google Scholar] [CrossRef] [PubMed]
- Mocelin, R.; Marcon, M.; Santo, G.D.; et al. Hypolipidemic and antiatherogenic effects of Cynara scolymus in cholesterol-fed rats. Rev. Bras. Farmacogn. 2016, 26, 233–239. [Google Scholar] [CrossRef]
- Vidal-Itriago, A.; Radford, R.A.W.; Aramideh, J.A.; Maurel, C.; Scherer, N.M.; Don, E.K.; Lee, A.; Chung, R.S.; Graeber, M.B.; Morsch, M. Microglia morphophysiological diversity and its implications for the CNS. Front. Immunol. 2022, 13, 997786. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Wang, H.; Yin, Y. Microglia Polarization From M1 to M2 in Neurodegenerative Diseases. Front. Aging Neurosci. 2022, 14, 815347. [Google Scholar] [CrossRef] [PubMed]
- Cianciulli, A.; Porro, C.; Calvello, R.; Trotta, T.; Lofrumento, D.D.; Panaro, M.A. Microglia Mediated Neuroinflammation: Focus on PI3K Modulation. Biomolecules. 2020, 10, 137. [Google Scholar] [CrossRef] [PubMed]
- Biswas, K. Microglia mediated neuroinflammation in neurodegenerative diseases: A review on the cell signaling pathways involved in microglial activation. J. Neuroimmunol. 2023, 383, 578180. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zhang, S.; Fan, X. Role of Polyphenols as Antioxidant Supplementation in Ischemic Stroke. Oxid. Med. Cell. Longev. 2021, 2021, 5471347. [Google Scholar] [CrossRef] [PubMed]
- Parrella, E.; Gussago, C.; Porrini, V.; Benarese, M.; Pizzi, M. From Preclinical Stroke Models to Humans: Polyphenols in the Prevention and Treatment of Stroke. Nutrients. 2020, 13, 85. [Google Scholar] [CrossRef]
- Číž, M.; Dvořáková, A.; Skočková, V.; Kubala, L. The Role of Dietary Phenolic Compounds in Epigenetic Modulation Involved in Inflammatory Processes. Antioxidants (Basel). 2020, 9, 691. [Google Scholar] [CrossRef]
- Kong, L.; An, X.; Hu, L.; Zhang, S.; Liu, L.; Zhao, S.; Wang, R.; Nan, Y. Resveratrol ameliorates nutritional steatohepatitis through the mmu-miR-599/PXR pathway. Int. J. Mol. Med. 2022, 49, 47. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Pu, C.; Yang, E.; Zhang, H.; Feng, Y.; Luo, P.; Yang, Y.; Zhang, L.; Li, X.; Jiang, X.; Dai, S. Macrophage/Microglia Sirt3 Contributes to the Anti-inflammatory Effects of Resveratrol Against Experimental Intracerebral Hemorrhage in Mice. Cell. Mol. Neurobiol. 2023, 43, 2871–2882. [Google Scholar] [CrossRef] [PubMed]
- Koronowski, K.B.; Khoury, N.; Saul, I.; Loris, Z.B.; Cohan, C.H.; Stradecki-Cohan, H.M.; Dave, K.R.; Young, J.I.; Perez-Pinzon, M.A. Neuronal SIRT1 (Silent Information Regulator 2 Homologue 1) Regulates Glycolysis and Mediates Resveratrol-Induced Ischemic Tolerance. Stroke. 2017, 48, 3117–3125. [Google Scholar] [CrossRef]
- Yan, X.; Liu, K.; Sun, X.; Qin, S.; Wu, M.; Qin, L.; Wang, Y.; Li, Z.; Zhong, X.; Wei, X. A cross-sectional study of blood selenium concentration and cognitive function in elderly Americans: National Health and Nutrition Examination Survey 2011-2014. Ann. Hum. Biol. 2020, 47, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Lei, T.; Zhang, J.; Yan, Y.; Wang, N.; Song, C.; Li, C.; Sun, M.; Li, J.; Guo, Y.; Yang, J.; Kang, T. Longan (Dimocarpus longan Lour.) Aril ameliorates cognitive impairment in AD mice induced by combination of D-gal/AlCl3 and an irregular diet via RAS/MEK/ERK signaling pathway. J. Ethnopharmacol. 2021, 267, 113612. [Google Scholar] [CrossRef] [PubMed]
- Tressera-Rimbau, A.; Arranz, S.; Eder, M.; Vallverdú-Queralt, A. Dietary Polyphenols in the Prevention of Stroke. Oxid. Med. Cell. Longev. 2017, 2017, 7467962. [Google Scholar] [CrossRef] [PubMed]
- Cicek, B.; Genc, S.; Yeni, Y.; Kuzucu, M.; Cetin, A.; Yildirim, S.; Bolat, I.; Kantarci, M.; Hacimuftuoglu, A.; Lazopoulos, G.; Tsatsakis, A.; Tsarouhas, K.; Taghizadehghalehjoughi, A. Artichoke (Cynara Scolymus) Methanolic Leaf Extract Alleviates Diethylnitrosamine-Induced Toxicity in BALB/c Mouse Brain: Involvement of Oxidative Stress and Apoptotically Related Klotho/PPARγ Signaling. J. Pers. Med. 2022, 12, 2012. [Google Scholar] [CrossRef] [PubMed]
- Cory, H.; Passarelli, S.; Szeto, J.; Tamez, M.; Mattei, J. The Role of Polyphenols in Human Health and Food Systems: A Mini-Review. Front. Nutr. 2018, 5, 87. [Google Scholar] [CrossRef]
- Piccinini, A.; Oliveira, M.P.; Silva, M.R.; Bett, G.S.; Becker, I.B.; Mendes, T.F.; Salla, D.H.; Silva, L.E.; Vilela, T.C.; et al. Effects of Ethanolic Extract of Cynara cardunculus (Artichoke) Leaves on Neuroinflammatory and Neurochemical Parameters in a Diet-Induced Mice Obesity Model. Neurochem. Res. 2022, 47, 1888–1903. [Google Scholar] [CrossRef]
- Klöting, N.; Blüher, M. Adipocyte dysfunction, inflammation and metabolic syndrome. Rev. Endocr. Metab. Disord. 2014, 15, 277–287. [Google Scholar] [CrossRef]
- Guo, Y.J.; Luo, T.; Wu, F.; Mei, Y.W.; Peng, J.; Liu, H.; Li, H.R.; Zhang, S.L.; Dong, J.H.; Fang, Y.; Zhao, L. Involvement of TLR2 and TLR9 in the anti-inflammatory effects of chlorogenic acid in HSV-1-infected microglia. Life Sci. 2015, 127, 12–18. [Google Scholar] [CrossRef]
- Gomez-Pinilla, F.; Tyagi, E. Diet and cognition: Interplay between cell metabolism and neuronal plasticity. Curr. Opin. Clin. Nutr. Metab. Care. 2013, 16, 726–733. [Google Scholar] [CrossRef]
- Olufunmilayo, E.O.; Gerke-Duncan, M.B.; Holsinger, R.M.D. Oxidative Stress and Antioxidants in Neurodegenerative Disorders. Antioxidants (Basel). 2023, 12, 517. [Google Scholar] [CrossRef] [PubMed]
- Porter, G.A.; O'Connor, J.C. Brain-derived neurotrophic factor and inflammation in depression: Pathogenic partners in crime? World J. Psychiatry. 2022, 12, 77–97. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Sun-Waterhouse, D.; Ouyang, F.; Tan, X.; Li, D.; Xu, L.; Li, B.; Wang, Y.; Li, F. Apple phenolic extracts ameliorate lead-induced cognitive impairment and depression- and anxiety-like behavior in mice by abating oxidative stress, inflammation and apoptosis via the miR-22-3p/SIRT1 axis. Food Funct. 2022, 13, 2647–2661. [Google Scholar] [CrossRef]
- Liu, X.; Huang, K.; Niu, Z.; Mei, D.; Zhang, B. Protective effect of isochlorogenic acid B on liver fibrosis in non-alcoholic steatohepatitis of mice. Basic Clin. Pharmacol. Toxicol. 2019, 124, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Qi, H.; Shi, Y.; Wu, H.; Niu, C.; Sun, X.; Wang, K. Inhibition of temperature-sensitive TRPV3 channel by two natural isochlorogenic acid isomers for alleviation of dermatitis and chronic pruritus. Acta Pharm. Sin. B. 2022, 12, 723–734. [Google Scholar] [CrossRef] [PubMed]
- Sroka, Z.; Cisowski, W. Hydrogen peroxide scavenging, antioxidant and anti-radical activity of some phenolic acids. Food Chem. Toxicol. 2003, 41, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Azman, K.F.; Zakaria, R. Recent Advances on the Role of Brain-Derived Neurotrophic Factor (BDNF) in Neurodegenerative Diseases. Int. J. Mol. Sci. 2022, 23, 6827. [Google Scholar] [CrossRef]
- Wang, X.L.; Gardner, W.; Yu, S.Y.; Serchov, T. A Pattern to Link Adenosine Signaling, Circadian System, and Potential Final Common Pathway in the Pathogenesis of Major Depressive Disorder. Mol. Neurobiol. 2022, 59, 6713–6723. [Google Scholar] [CrossRef]
- Simpson, D.S.A.; Oliver, P.L. ROS Generation in Microglia: Understanding Oxidative Stress and Inflammation in Neurodegenerative Disease. Antioxidants (Basel). 2020, 9, 743. [Google Scholar] [CrossRef]
- Cianciulli, A.; Salvatore, R.; Porro, C.; Trotta, T.; Panaro, M.A. Folic Acid Is Able to Polarize the Inflammatory Response in LPS Activated Microglia by Regulating Multiple Signaling Pathways. Mediators Inflamm. 2016, 2016, 5240127. [Google Scholar] [CrossRef]
- Hirsch, E.C.; Jenner, P.; Przedborski, S. Pathogenesis of Parkinson's disease. Mov. Disord. 2013, 28, 24–30. [Google Scholar] [CrossRef]
- Maccioni, R.B.; Rojo, L.E.; Fernández, J.A.; Kuljis, R.O. The role of neuroimmunomodulation in Alzheimer's disease. Ann. N. Y. Acad. Sci. 2009, 1153, 240–246. [Google Scholar] [CrossRef]
- El-Nashar, H.A.S.; Abbas, H.; Zewail, M.; Noureldin, M.H.; Ali, M.M.; Shamaa, M.M.; Khattab, M.A.; Ibrahim, N. Neuroprotective Effect of Artichoke-Based Nanoformulation in Sporadic Alzheimer's Disease Mouse Model: Focus on Antioxidant, Anti-Inflammatory, and Amyloidogenic Pathways. Pharmaceuticals (Basel). 2022, 15, 1202. [Google Scholar] [CrossRef] [PubMed]
- Mekkey, S.M.; Raghif, A.R.A.; Alkafaj, H.A.R.; Hadi, N.R. The Anti-Parkinson Effects of Cyanara Scoluymus (Artichoke) Extract in Rat Model of Rotenone Induced Parkinsonism. Annals of the Romanian Society for Cell Biology. 2021, 25, 2318–2329. Available online: https://www.annalsofrscb.ro/index.php/journal/article/view/5845/4508.
Figure 1.
Anti-inflammatory action of ALE in IBD.
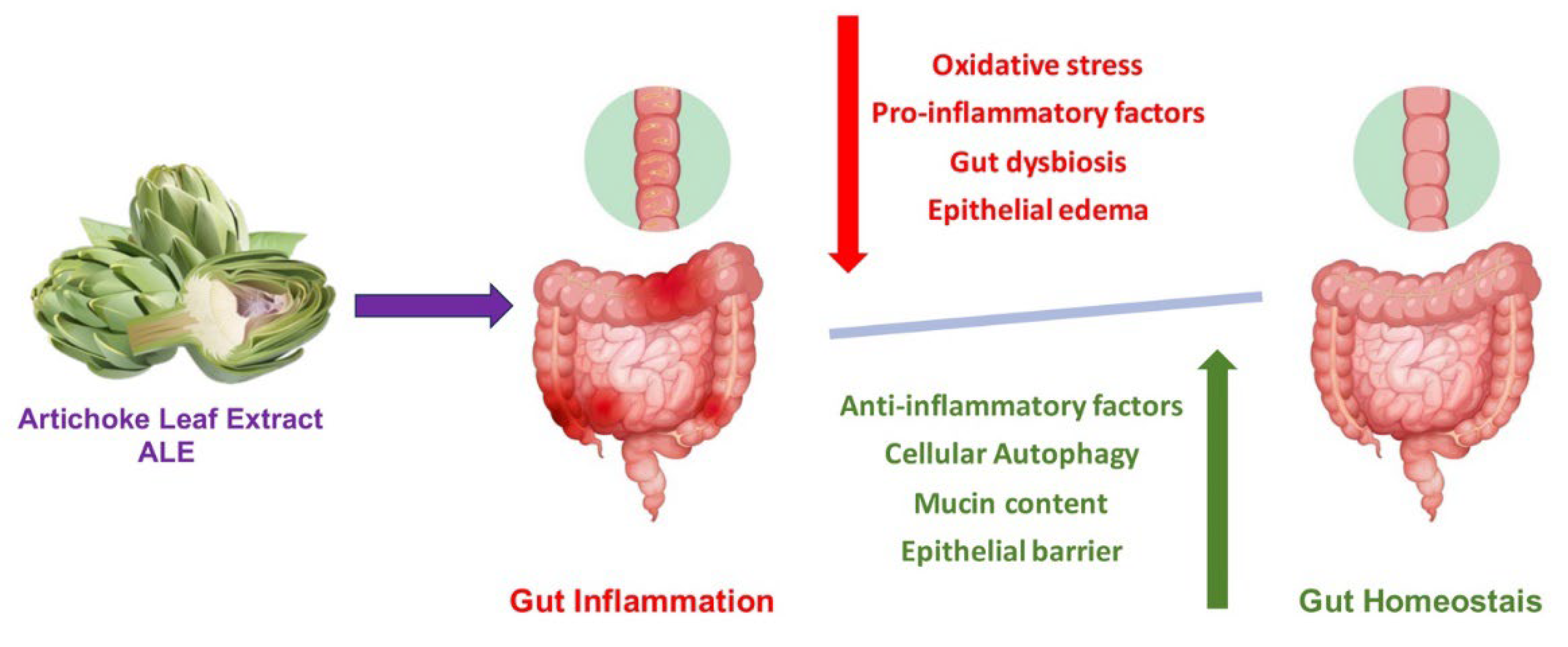
Figure 2.
ALE beneficial on inflammatory and GI diseases.
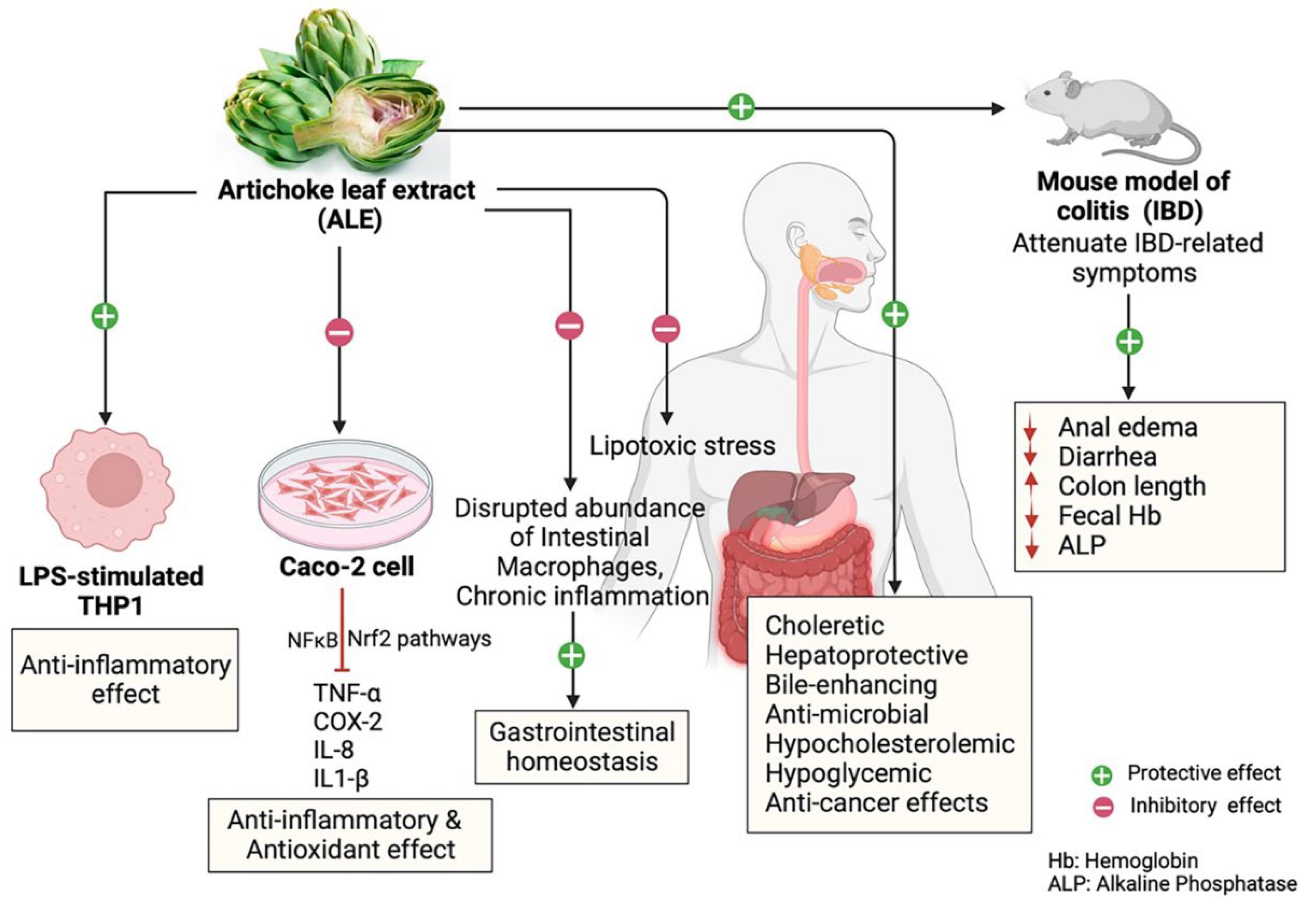
Figure 3.
Mechanisms of artichoke in cardiovascular protection.
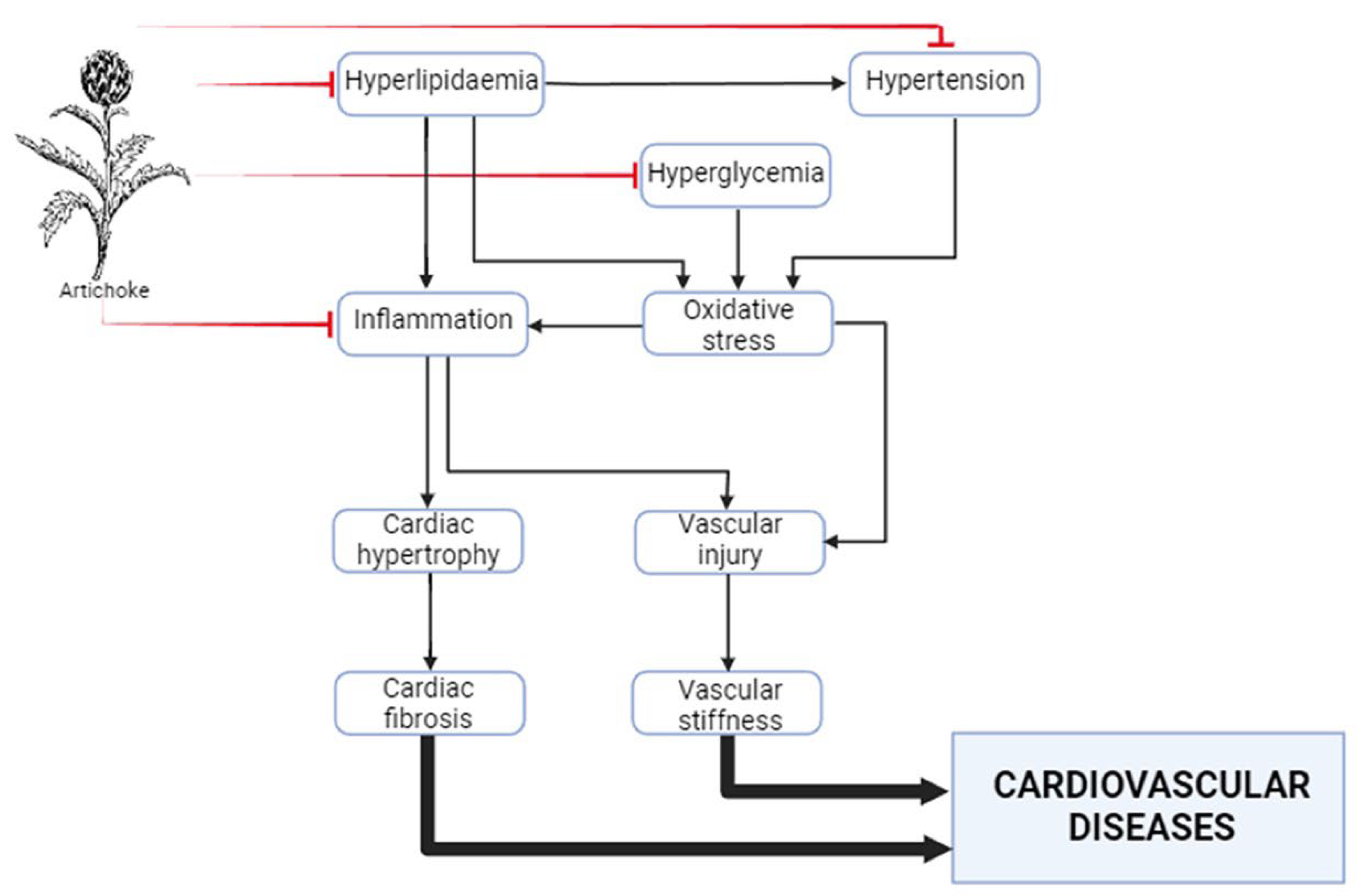
Figure 4.
Positive effects of ALE in neurodegenerative diseases.
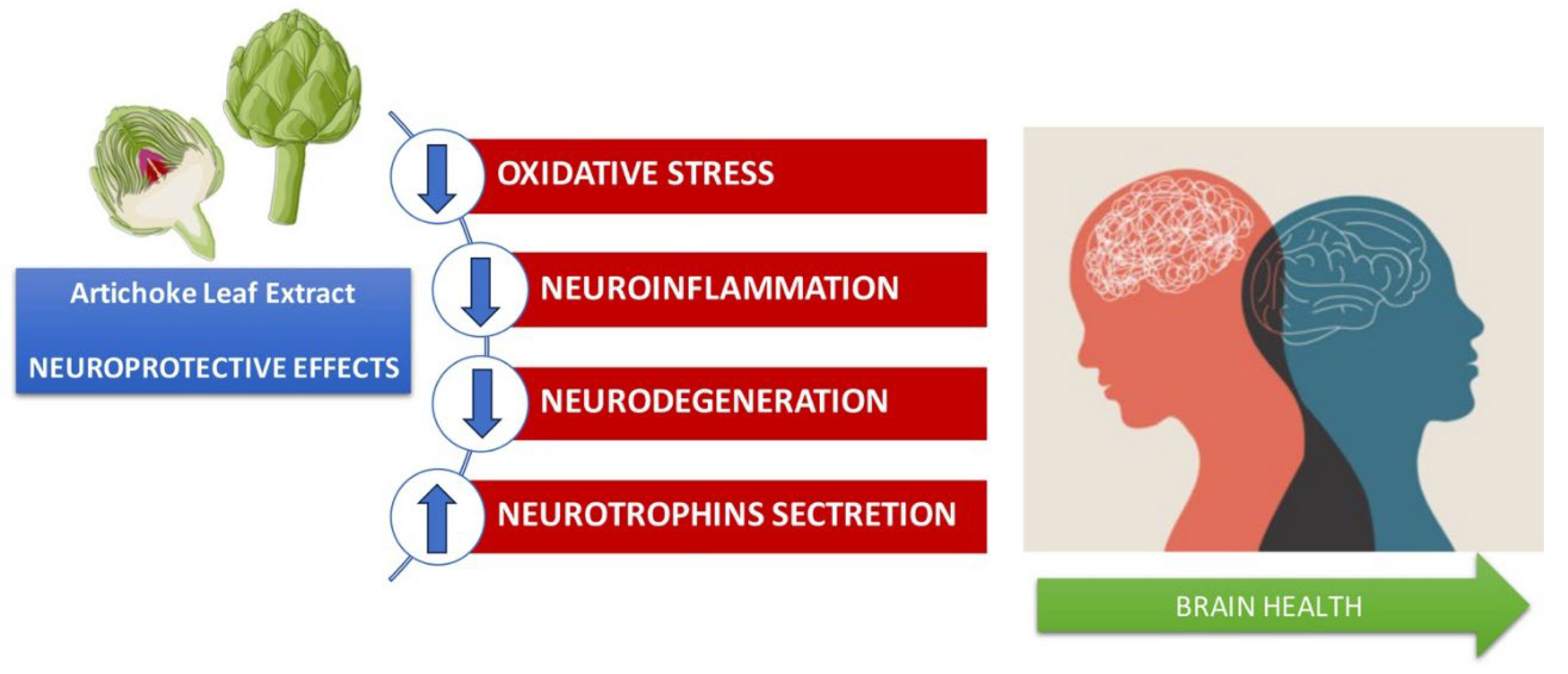
Figure 5.
Artichoke benefits on human health.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



