
Submitted:
14 November 2023
Posted:
15 November 2023
You are already at the latest version
Abstract
Bone morphogenetic protein (BMP) and platelet-derived growth factor (PDGF) are known to regulate and stimulate osteogenesis, both proteins playing an important role in bone homeostasis, constituting good candidates for osteoporosis´ treatment. Herein we aim to evaluate the effects of recombinant human BMP-7 (rhBMP7) and PDGF-BB (rhPDGF-BB) in oophorectomy-induced osteoporosis in rats. To this end, 40 Sprague-Dawley rats were submitted to oophorectomy surgery and treatments were started at the 100th day after the surgery, when all animals showed signs of osteoporosis. These peptide growth factors were applied intravenously once or twice a week and animals were followed for a total of five weeks. Two weeks after the end of the treatments, the animals were euthanized, the tissues were collected and Alkaline Phosphatase, X-ray, micro-CT and histology were assessed. The results indicate that the most promising treatments are: 20 µg/kg PDGF-BB + 30 µg/kg BMP-7 2x/week and 30 µg/kg BMP-7 2x/week, presenting an increase of 15% (p<0.05) and 13% (p<0.05) in bone volume fraction and 21% (p<0.05) and 23% (p<0.05) in trabecular number, respectively. In conclusion, rhPDGF-BB and rhBMP-7 are capable of inducing an increase in bone volume and density in this osteoporotic animal model, constituting interesting candidates for osteoporosis treatment.
Keywords:
Osteoporosis
; BMP-7
; PDGF-BB
; peptide growth factors
; bone repair.
1. Introduction
Osteoporosis is a degenerative disease, whose main characteristic is the loss of bone mass and degeneration of the tissue microarchitecture, generating an increased risk of fractures, being considered as a serious public health problem [1]. Osteoporosis occurs in about 200 million people in the World, affecting mainly post-menopausal women and elderly men [2], being the cause of more than 8.9 million fractures annually worldwide. In Europe, the disease causes more debilitation than tumors, with the exception of lung cancer [3]. Osteoporotic patients have greater morbidity and mortality as a result of fractures and due to compromised bone tissue regeneration [4]. Moreover, fractures of the hip and vertebrae are related to increased risk of death, with about 20% of the people who suffer a hip fracture dying within six months of the injury [5].
Bones are among the few organs capable of regenerating, being a tissue that continually remodels itself throughout life [6]. The main cells that participate in this process, which are associated to maintenance of tissue homeostasis are: osteoclasts, which are responsible for bone resorption, osteoblasts that secrete bone matrix and osteocytes, which maintain tissue homeostasis [7]. When an imbalance between bone formation and resorption occurs as a result of the activity of osteoblasts and osteoclasts, respectively, loss of bone tissue mass and degeneration of the trabecular bone microarchitecture ensue [8,9]. Thus, when filling of the bone pores caused by resorption is incomplete, a progressive decrease in bone density occurs, leading to the development of osteoporosis [7]. Since antiresorptive drugs have no effect in bone tissue regeneration, development of anabolic drugs to recover bone mass is needed [6]. Therefore, new treatments are being developed, with the class of molecules displaying the potential to stimulate an increase in bone density being peptide growth factors, which affect bone regeneration and osteogenesis [10].
BMPs are proteins which belong to the TGF-β superfamily, participating in regulation of bone and cartilage repair and formation, embryonic development maintenance, bone tissue homeostasis [11], organogenesis, apoptosis, cell proliferation and differentiation, chemotaxis, as well as repair of various types of tissues [12] and in stem cell biology. They are the most powerful osteoinductive growth factors, their role in regulating the formation of new bones being widely studied [6]. BMP-7 induces the differentiation of mesenchymal stem cells into the osteoblastic lineage, thereby inducing endochondral/intramembranous ossification and chondrogenesis [13]. In addition, there is evidence of the efficacy of this protein in accelerating bone tissue regeneration and injury recovery in vitro, in vivo and in preclinical studies [6,7,11].
PDGF is a chemoattractant protein, displaying mitogenic activity for tissues of mesodermal origin and acting as a vascular anchorage agent, playing an important role in bone and soft tissue wound healing [14]. It also promotes the development of the central nervous system, acting together with embryonic and developmental factors to promote organogenesis [15]. PDGF-BB is expressed during the fracture repair process by promoting infiltration of mesenchymal and angiogenic progenitor cells and regulating the chondrogenic and osteogenic responses. PDGF-BB is also related to regulation of osteoblast chemotaxis and cell proliferation and differentiation, resulting in rapid bone formation [14,16]. In addition, PDGF-BB is an angiogenic factor related to angiogenesis and osteogenesis, affecting bone shaping in the periosteum region and in trabecular bone. Furthermore, its downregulation generates loss of trabecular and cortical bone mass [17].
Pountos et al. (2010) demonstrated that BMP-7 and PDGF-BB were able to increase mesenchymal stem cells´ proliferation and enable osteogenic differentiation, when applied separately, promoting bone regeneration in an in vitro model [18]. Therefore, we reasoned that co-treatment of osteoporotic animals with these two proteins could promote the recovery of affected tissue in an in vivo model of osteoporosis and possibly result in disease regression or attenuation.
Considering the large number of osteoporosis cases in Brazil and worldwide, the impact of this disease in patient morbidity and mortality, the difficulty in repairing and regenerating osteoporotic fractures and the high costs for the public health system, it is important to pursue a treatment capable of strengthening the patients' bones, thus preventing fractures and promoting bone tissue repair more rapidly and effectively. PDGF-BB and BMP-7 peptide growth factors play an important role in regulating bone formation and tissue regeneration. Therefore, these proteins are potential candidates for osteoporosis´ treatment, since they are able to stimulate bone formation and promote increased tissue density, rendering this tissue more robust and less prone to fractures. Therefore, the main aim of the present study was to evaluate the effects of rhBMP7 and rhPDGF-BB in oophorectomy-induced osteoporosis in rats. Our results indicate that the osteoporosis animal model was successfully established one hundred days after the surgery, and, also, that the systemic treatment with both recombinant proteins for five weeks (two weekly applications of 30µg/kg of BMP-7 and 20µg/kg of PDGF -BB) was effective to increase bone volume and density in this osteoporotic animal model, constituting interesting candidates for osteoporosis treatment.
2. Materials and Methods
2.1. Growth Factors
The growth factors used in this work, namely: recombinant human platelet-derived growth factor (rhPDGF-BB) and recombinant human bone morphogenetic protein (rhBMP-7) were previously produced in our laboratory in mammalian cells (293T), according to previously established protocols, presenting high biological activity [19].
2.2. Animals and Treatment
For this study, 44 female Sprague-Dawley rats aged 12 weeks, weighing around 270g, were used. The animals were acclimatized for one week and maintained under constant conditions of temperature (22 ± 1°C) and light (12h- light/dark cycle) with ad libitum access to food and water. The oophorectomy surgery was performed based on the literature [20,21,22]. The study protocol was approved by the Ethics Committee on Animal Use (CEUA) of the School of Veterinary Medicine and Animal Science of the University of São Paulo) (FMVZ-USP), protocol number 8033260918. The animals were divided into eleven groups as described in Table 1.
The surgery was carried out in the Experimental Animal Facility using a horizontal laminar flow hood. The surgery area was disinfected with 70% ethanol and Povidone iodine. The animals were anesthetized by inhalation with 2% isoflurane. The transverse abdominal muscle was accessed after the skin incision and, after the muscle was dissected, the peritoneal space was exposed. After accessing the peritoneal cavity, the uterus and ovaries were exposed and excess organ adipose tissue was removed. The uterus was ligated and both ovaries were removed. After reinserting the uterus into the peritoneal cavity, the surgical wound was closed, and the internal planes were sutured. The rats were weighed weekly and blood was collected at days 0, 100, 115, 130 and 150.
After 100 days of surgery, the animals in the oophorectomy group were euthanized using an overdose of xylazine and ketamine by intraperitoneal injection, to confirm establishment of the disease (oophorectomy). Treatments of the other groups were also started on the 100th day after surgery by injection of 30 µg/kg of rhBMP7, 20 µg/kg of rhPDGF-BB or a combination of both, as described in Table 1.
The treatments were administered intravenously once or twice a week, according to the established experimental groups (Table 1), in a total volume of 150 µl through the animals' retro-orbital plexus. The solution used as the vehicle for all injections was PBSA (saline-phosphate solution without calcium or magnesium) and treatment was maintained for five weeks.
Two weeks after the end of treatments, the animals were euthanized using an overdose of xylazine and ketamine by intraperitoneal injection, thus totaling 150 days after the osteoporosis induction surgery. Femurs were collected and kept in 10% formaldehyde for histological (and micro-CT) analysis.
2.3. Blood and serum collection
On days 0 and 100 after oophorectomy surgery, the animals' blood was gingivally collected in tubes containing separating gel in a total volume of 500 µl. About half an hour after collection, the blood was centrifuged at 1,250xg for 10 minutes at 4ºC (Eppendorf centrifuge-5810R). Serum was isolated and about 250 µl was collected and stored at -80 ºC.
2.4. Quantification of Alkaline Phosphatase (ALP)
ALP is an enzyme associated with bone metabolism and may therefore be used as a marker for osteoporosis. ALP quantification was performed using the LabTest kit (Brazil) following the manufacturer's recommendations and adapting the protocol to the volume of solutions in 96-well plates. The results were assessed using a spectrophotometer (SpectraMax Paradigm) at 590 nm wavelength.
2.5. X-ray
On the 100th day after the oophorectomy surgery, the animals were scanned using the In-Vivo Imaging System FX PRO (Carestream Molecular Imaging) device. X-ray images were generated and then analyzed by selecting the region of interest, named ROI. The selected region was the left femur neck, the same region commonly used to perform bone densitometry in humans. The bone volume content variables (g/cm3) were analyzed to quantify the animals' BMD (Bone Mineral Density).
2.6. Micro CT
The left femurs were analyzed in a microtomography equipment (SkyScan 1176 In Vivo Microtomograph, Bruker) and the data obtained were analyzed in the CT Analyzer software (Bruker). The region of the femur selected was the proximal portion of the femoral epiphysis and 10 sections were analyzed, totaling an area of about 10 µm thick and the ROI was used to select for the region of the cancellous bone and then cortical bone. Bone Mineral Density (BMD), Bone Volume Fraction (BV/TV; bone volume/total volume), trabecular thickness, and trabecular separation were quantified.
2.7. Histology
48h after collection, the tissues collected from the animals were washed in running water to remove the fixative and then stored in 70% ethanol. The right femurs were sent for decalcification, processing, paraffinization, cutting and staining with HE and Masson's Trichrome at the Histotech company (São Paulo, SP, Brazil).
The microscopic analysis and morphological diagnosis of the slides were carried out blindly. The microscopic findings were classified into a score, as defined in Table 2. In addition, the findings of each slide resulted in the suggestion of a clinical condition, which was also classified according to a score, described in Table 3 [23,24,25].
3. Results
3.1. Oophorectomy causes body mass gain
3.2. Oophorectomized animals show increased serum ALP concentration
Upon comparing the ALP concentration in animals´ serum at the oophorectomy day (D0) and 100 days after this procedure (D100), a significant increase (p<0.05) of 3U/l is observed, which represents 7% (Figure 3). This increase is expected, being an indication that the animals are displaying alteration in their bone metabolism.
3.3. In vivo X-Ray Analysis
The data obtained from the in vivo X-ray analysis showed that at 100 days after the oophorectomy surgery the animals significantly lose bone density, when compared to the animals from the Sham group (Figure 4). Therefore, the animals were considered to be osteoporotic after the 100th day of surgery.
3.4. Micro-CT Analysis
The results obtained with Micro-CT reinforce the data from the X-ray analysis and confirm that after 100 days of surgery the animals are osteoporotic. The oophorectomized animals have a significantly lower fraction of bone volume in the trabecular region, when compared to animals in the Sham group, with a decrease of 33% in the analyzed region (Figure 5). These values represent a 35% reduction in bone fraction, respectively, relative to the Sham group.
Upon observing the cortical bone, we found that oophorectomized animals presented a decrease in the bone volume fraction with a 12% reduction, representing a 14% bone loss, when compared to the sham group (p<0.01) (Figure 6).
Upon analyzing the effects of the different treatments, we found that the fraction of bone volume in the groups treated with BMP-7 2x/week and PDGF-BB + BMP-7 2x/week showed a significant increase, corresponding to 13% and 15%, respectively (Figure 7-A). Treatment with BMP-7 2x/week and PDGF-BB + BMP-7 2x/week also caused a significant increase (p<0.05) in the number of trabeculae (Figure 7-C), equivalent to 21% and 23%, respectively. Upon observing the BMD of treated animals relative to the Vehicle group, it can be noted that the treatments with and PDGF-BB + BMP-7 2x/week and Zoledronic Acid show a tendency to increase the animals' BMD, although no statistical significance was found (Figure 7-E).
3.5. Histology
Histological slides were prepared from the animals' right femur and stained with HE, pink/reddish indicating the cytoplasmic region and collagen fibers and in purple are the cell nuclei and the extracellular matrix of the cartilage. Masson's Trichrome stain indicates collagen in blue, cytoplasm in red, and cell nuclei in purple. For this analysis, the animals in the Control group were used as a reference for the other groups.
To determine whether at the 100th day after the oophorectomy, the animals are, in fact, osteoporotic, the animals in the Oophorectomy and Sham groups were compared, relative to the Control (Figure 8-A to F). We observed that the Sham group has normal trabecular thickness (Figure 8-G) and the number of trabeculae and medullary cellularity are within the expected range for the animals’ age, indicating that the bone tissue is within the expected parameters and its clinical condition is normal. Animals in the Oophorectomy group show a pronounced to moderate reduction in trabecular thickness, compared to the Control group (Figure 8-G), in addition to a reduction in the number of trabeculae, reduction in medullary cellularity and considerable increase in the amount of intramedullary adipocytes, in some cases even showing a reduction in cortical thickness. These microscopic findings indicate an osteoporotic condition, which varies from mild to severe (Figure 8-H), confirming that 100 days after the oophorectomy surgery, the animals indeed present the development of osteoporosis.
In addition, in the histological analysis, all groups of oophorectomy surgery showed an increase in the number of intramedullary adipocytes and a reduction in medullary cellularity, which is more pronounced in animals with greater reduction in trabecular bone thickness and more severe osteoporosis (Figure 9 A-G, Figure 10 A-G).
The animals from the Vehicle group showed mild to moderate reduction of the articular cartilage (Figure 11), and some animals also displayed erosion (Figure 9-A). Based on the microscopic findings, the animals clinical condition indicates moderate osteoporosis and one case of severe osteoporosis (Figure 12). The group treated with Zoledronic acid, the positive control in this study, presented one animal with pronounced reduction in trabecular thickness, one animal with a discrete reduction and two with normal trabecular thickness (Figure 11). The clinical condition follows the pattern of thickness reduction, with one animal with severe osteoporosis, one with mild osteoporosis and two animals with normal clinical condition (Figure 12).
A pronounced reduction in trabecular bone thickness was found in two animals of the group that received PDGF-BB 2x/week, one with moderate reduction and one with normal thickness of the trabeculae (Figure 11). Analysis of the clinical condition of these animals indicated that both of them displayed severe osteoporosis, one had a moderate condition of the disease and the other one as was considered normal (Figure 12). There were signs of trabecular fractures, cartilage erosion and a considerable increase in the number of adipocytes throughout the animals of this group. The group that received PDGF-BB 1x/week showed a moderate reduction in the thickness of the bone trabeculae in two animals and the other two presented a discrete reduction in trabecular tissue (Figure 11). Regarding their clinical condition, two of these animals displayed moderate osteoporosis, another one displayed mild osteoporosis and one animal had a normal clinical condition (Figure 12). The histological slides showed occasional cementation lines, which are the boundaries between the old and new bone matrix, neoformation of bone tissue, apparently intact cortical bone and a focus of clustered regenerative chondrocytes, in addition to a considerable increase in intramedullary adipocytes (Figure 9-D).
Treatment with BMP-7 2x/week resulted in a very distinct reduction in trabecular thickness, with each animal presenting a different score (Figure 11). Areas of neoformed trabecular bone tissue and cementing lines were observed. Regarding the clinical condition, two animals were considered normal, one had moderate osteoporosis and the other one displayed severe osteoporosis (Figure 12). When treated with BMP-7 1x/week, the animals showed a moderate reduction in trabecular thickness and one animal had a discrete reduction (Figure 11). This group also presented regions of newly formed bone with young osteocytes and an increase in osteoblasts and osteoclasts, even in animals with moderate reduction. However, one of the animals presented fragmentation of the bone trabeculae. Upon observing the results (Figure 12), it may be noted that one of the animals in this group had severe osteoporosis, two animals displayed moderate osteoporosis and one had a clinical condition of mild osteoporosis (Figure 12).
By associating the two recombinant proteins, namely, PDGF-BB and BMP-7 2x/week, in the treatment of the animals, one of the animals displayed a pronounced reduction in trabecular thickness, another one a moderate reduction and the last two had only a discrete reduction (Figure 11). Histological analysis showed that the group that received PDGF-BB and BMP-7 1x/week was the one showing the best performance among those treated with recombinant proteins, with three animals being classified as mild reduction in trabecular thickness and one as a moderate reduction (Figure 11). The presence of cementation lines and areas of bone neoformation, increased amount of adipocytes and erosion in the articular cartilage were also observed.
4. Discussion
Osteoporosis is a disease characterized by loss of bone mass and tissue microarchitecture, rendering it more fragile and prone to fractures, being difficult to repair due to changes in bone metabolism. The disease affects mainly menopaused women and men over 70 years of age. It is caused by the imbalance between bone formation and resorption, which causes pores formation in the tissue, being responsible for its lower resistance [26].
Among the available therapies, bisphosphonates are anti-resorptive drugs that act on osteoclasts inhibiting their activity, being more widely used. However, these drugs only stabilize the loss of bone tissue, being uncapable of treating the disease and inducing the replacement of the bone mass lost [27]. In search for new therapies which are able to increase tissue volume and density, there are treatments with growth factors, including BMP-7 and PDGF-BB whose functions involve proliferation and differentiation of osteoblasts that participate in tissue formation through the secretion of bone matrix. Therefore, we set out to investigate the role of recombinant human proteins PDGF-BB and BMP-7 in the progression of osteoporosis in oophorectomized animals.
After performing the oophorectomy surgery, the animals showed a marked and significant increase in weight, especially 30 days after the procedure (Figure 1). This characteristic of oophorectomized rats is described in the literature, indicating the success of the surgery and establishment of the disease [28]. After 90 days of the surgery, the animals weight reached a plateau, with minimal variation thereafter, both for the oophorectomized animals and for the surgical control animals (Sham).
At the 100th day after surgery, the animals' serum ALP levels showed a significant increase, as expected after the onset of the disease, being an indication of bone metabolism disorder [29,30,31]. The predominant inorganic component in the bone matrix is hydroxyapatite, whose synthesis is inhibited by the presence of pyrophosphate. ALP is synthesized by osteoblasts, acting by hydrolyzing pyrophosphate and releasing inorganic phosphate, which participates in the synthesis of hydroxyapatite [32]. In osteoporosis, when an imbalance between tissue formation and resorption ensues, an attempt to increase osteoblast-mediated bone formation is expected and the concentration of ALP reflects the activity of these cells [29]. Moreover, it is possible to use the total quantification of the enzyme activity as a complement test to diagnose osteoporosis.
In addition to changes in ALP levels, a reduction in bone volume and density was also observed through in vivo X-Ray (Figure 4) and ex vivo Micro-CT (Figure 5 and Figure 6) analysis of the left femur. These data are indicative that the animals became osteoporotic and that the model was successfully established at the given time point.
This animal model mimics post-menopausal osteoporosis and, as it occurs in women, the animals undergo a drastic reduction in estrogen concentration. This hormone has great importance in bone metabolism, being associated with increased expression of RANKL by B lymphocytes. This transcription factor acts in the differentiation of osteoclasts, which leads to greater bone resorption. Indeed, low estrogen levels are also related to a reduction in the expression of osteoprotegerin (OPG), one of the main RANKL inhibitors [33], further increasing the imbalance between bone resorption and formation.
Among the molecules with potential to treat the disease are the PDGF-BB and BMP-7 peptide growth factors. PDGF-BB is a chemotactic and mitogenic growth factor, capable of promoting cell proliferation and migration of mesenchymal cells, such as fibroblasts and MSC (mesenchymal stem cells) [15]. During their differentiation process, pre-osteoclasts secrete PDGF-BB [34], which acts by inducing MSC migration and differentiation into osteoblasts, stimulating cortical bone formation during tissue damage and formation of type H vessels, which are important during bone remodeling [17]. Furthermore, studies indicate that the use of PDGF-BB induces an increase in osteoclast differentiation, both in vitro and in vivo. PDGF-BB is an osteoclast precursor chemotactic agent [35], increasing osteoclast resorption activity through the PDGF receptor beta (PDGFR-β) in vitro [36]. Therefore, this molecule has an important and complex role in bone remodeling.
Application of PDGF-BB, 20µg/kg 1x/week, led to a more significant improvement of the trabecular tissue, when compared to the 2x/week treatment in all regions. Taking into account the functions performed by this factor, its application once a week can stimulate bone remodeling and activate osteoclasts proliferation. However, when treated twice/week, PDGF-BB may be a greater stimulus for the differentiation of osteoclasts, which act more rapidly on bone tissue than osteoblasts, thus leading to an imbalance in bone metabolism, which it is characteristic of osteoporosis.
BMPs are crucial for bone metabolism and repair [37], playing a mitogenic, chemotactic, proliferative activity and being able to induce MSC differentiation into osteoblasts. Among the growth factors of this family is BMP-7, which has been shown to have repairing activity in bone fractures [38,39,40] and great capacity to induce osteoblasts differentiation, even greater than that of the PTH hormone [18], which is a widely used therapeutic alternative for osteoporosis treatment.
Considering the role of BMP-7 in osteoblasts, it was expected that treatment with this protein would bring benefits and result in an improvement in the osteoporotic condition of animals. Among the BMP-7 tested treatments employed in this work, the one that showed the best response was application of BMP-7 (30 µg/kg) twice a week, which led to a 15% increase in bone volume fraction in the 2nd region. Therefore, only a weekly application of the recombinant protein was not sufficient to improve the quality of the bone tissue.
As for treatment with PDGF-BB (20 µg/kg) and BMP-7 (30 µg/kg) proteins concomitantly, it was expected that it would present an increase in bone volume and density, since it is known that, separately, PDGF-BB has mitogenic capacity and BMP-7 acts in the differentiation of MSCs into osteoblasts. The results indicate that, in two weekly doses, this treatment showed positive results in the 1st region analyzed by micro-CT. When only one dose per week is applied, the results are significant in all of the regions, indicating that the regimen of treatment applications is a determining factor to induce an increase in bone volume and, consequently, positive clinical results.
Therefore, these results also indicate that with administration of the two proteins simultaneously, an antagonistic interaction between the proteins can occur, preventing them from performing the functions they execute when used individually. Chan et al. (2010) demonstrated that PDGF-BB may have a role as an antagonist of BMPs and the TGF-β family by reducing the expression of Trb3 (Tribbles-like protein-3), a modulator of Smad protein expression, which causes a decrease in the expression of these proteins and thus reduces the activity of BMPs [41].
The work by Bayer et al. (2016) demonstrated that, for in vitro angiogenic repair, the order in which the administration of PDGF-BB and BMP-2, which belongs to the same family as BMP-7, is of great importance, and must occur following a specific regimen to ensure good results. In addition, they also observed an antagonistic effect between the signaling of these two proteins, when they were administered simultaneously [42].
The results obtained in the histological analysis indicate that in all groups of oophorectomized animals we observed an expressive increase in intramedullary adipocytes and a reduction in cellularity in the bone marrow. The MSCs located in the bone marrow have the ability to differentiate, mainly into osteoblasts, adipocytes and chondrocytes [43]. The differentiation of MSCs is finely regulated, being mediated by several factors and signaling pathways. Transcription factors play a fundamental role in the cell differentiation process and among the main and essential factors are: Runx2, which induces the differentiation of MSCs into osteoblasts and inhibits adipogenesis [44], and PPARγ, which promotes the inverse process, inducing differentiation into adipocytes and inhibiting osteoblastogenesis [45]. In addition to transcription factors, the signaling pathways of BMPs and Wnt/β-catenin play an important role in this process, since they can induce MSC differentiation into both cell types. It has been observed that increased concentration of BMP-2 induces osteoblastogenesis, while low concentrations of this protein promotes adipogenesis [46], both through the canonical pathway, namely, the Smad 1/5/8 proteins and, also, through the MAPK signaling. BMPs promote adipogenesis through activation of PPARγ [47]. The Wnt pathway, on the other hand, induces the expression of Runx2 and inhibits the expression of PPAR, leading to osteoblast differentiation. However, when suppressed, this pathway inhibits osteoblastogenesis and promotes the differentiation of MSCs into adipocytes. Among the other factors that regulate cell differentiation are miRNAs, a high-fat diet and mechanical stimulation [48]. Studies have observed that MSCs derived from patients with osteoporosis present an increased potential to differentiate into adipocytes at the expense of osteoblasts [49]. Furthermore, there are studies showing that these adipocytes are distinct from others found in the body and, more importantly, these cells express RANKL, an important factor for osteoclast differentiation and activity and bone resorption [50].
The study by Hu and colleagues made important discoveries about how RANKL expressed by intramedullary adipocytes acts on bone remodeling. Using a model of oophorectomized female mice with RANKL deletion in adipocytes, they verified that the animals did not show reduction in trabecular and cortical bone density, which is observed in oophorectomized control animals. They concluded that the RANKL produced by adipocytes has an essential role in bone resorption and increased differentiation of osteoclasts in bone tissue, thus having great importance in the development of osteoporosis [51]. Also, using a genetically mutated animal model, Yu and colleagues observed that, in addition to reducing bone resorption and osteoclastogenesis, deletion of RANKL synthesis in these cells results in no change in MSCs differentiation into adipocytes or osteoblasts [52]. Therefore, the increase in intramedullary adipogenesis observed in osteoporotic animals is expected, and this fact may be related to the imbalance in bone remodeling and the development of osteoporosis.
Furthermore, the histological data obtained also indicate that the best treatments for osteoporosis were administration of zoledronic acid and PDGF-BB and BMP-7 1x/week. As in the results of micro-CT, it can be observed that the group treated with the commercial drug showed good results, even improving the quality of the animals' femurs. Similar results were obtained by Black et al. (2007), who observed an increase in BMD in patients using zoledronic acid annually for three years, these effects being observed in several places, such as the femur and hip [53].
Therefore, induction of osteoporosis through oophorectomy was successful, being evidenced by the increase in the animals' weight and ALP´s concentration in the blood, reduction in BMD and bone volume fraction and by histological analysis, which showed a reduction of trabecular thickness, increased intramedullary adipocytes and a clinical condition compatible with that of osteoporosis. Regarding the investigated treatments, it was observed that they did not cause changes in the weight of the animals and the micro-CT data showed that BMP-7 2x/week and PDGF-BB + BMP-7 2x/week led to an increase in the fraction of the bone volume and the number of trabeculae. Finally, histomorphology indicated that the best treatments also include zoledronic acid and PDGF-BB + BMP-7 1x/week.
5. Conclusions
An animal model for osteoporosis was successfully established, since at the 100th day after the oophorectomy surgery, the animals displayed a reduction in bone density and volume, in addition to an increase in the concentration of ALP, the presence of a high number of intramedullary adipocytes and a significant reduction in trabeculae, indicating an osteoporotic state. Systemic treatment with recombinant proteins for five weeks (two weekly applications of 30µg/kg of BMP-7 and 20µg/kg of PDGF -BB) was effective to revert osteoporosis. We hope that this work will contribute to a new and effective treatment regimen and to improve the life quality of individuals affected by osteoporosis.
Author Contributions
Conceptualization: T.G.R, M.C.S and A.C.O.C; methodology: T.G.R and A.C.O.C; validation: T.G.R and A.C.O.C; formal analysis: T.G.R; investigation: T.G.R, A.M.S.D.C, L.A.S.S and B.A.A.K; Resources: M.C.S; Writing: original draft preparation T.G.R; review and editing: M.C.S and A.C.O.C; Visualization: T.G.R; Supervision: A.C.O.C; project management: A.C.O.C; Funding acquisition: M.C.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Council for Scientific and Technological Development (CNPq), grant number 134625/2018-8; the São Paulo Research Foundation (FAPESP), Thematic grant number 2016/05311-2; the Coordination for the Improvement of Higher Education Personnel (CAPES) grant numbers 88881.068070/2014-01 and 88882.315613/2019-01; and the National Institute of Science and Technology in Regenerative Medicine (INCT-Regenera) grant number.
Institutional Review Board Statement
The animal study protocol was approved by the Ethic Committee on Animal Use of the School of Veterinary Medicine and Animal Science (University of São Paulo) (CEUA/FMVZ), (protocol number CEUA 8033260918, data of approval 12/12/2018).
Data Availability Statement
Data are available upon request from the corresponding author.
Acknowledgments
The authors acknowledge Zizi Mendonça, Alan Pereira dos Santos and Amanda Cordeiro, for technical support and help with the animals maintenance and experiments.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Vestergaard, P.; Rejnmark, L.; Mosekilde, L. Increased Mortality in Patients with a Hip Fracture-Effect of Pre-Morbid Conditions and Post-Fracture Complications. Osteoporosis International 2007, 18, 1583–1593. [Google Scholar] [CrossRef] [PubMed]
- Qaseem, A.; Forciea, M.A.; McLean, R.M.; Denberg, T.D. Treatment of Low Bone Density or Osteoporosis to Prevent Fractures in Men and Women: A Clinical Practice Guideline Update from the American College of Physicians. Ann Intern Med 2017, 166, 818–839. [Google Scholar] [CrossRef] [PubMed]
- Johnell, O.; Kanis, J.A. An Estimate of the Worldwide Prevalence and Disability Associated with Osteoporotic Fractures. Osteoporos Int 2006, 17, 1726–1733. [Google Scholar] [CrossRef] [PubMed]
- Zofkova, I.; Blahos, J. New Molecules Modulating Bone Metabolism – New Perspectives in the Treatment of Osteoporosis. Physiol. Res 2017, 66, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Åkesson, K.; Mitchell, P. Capture a Fratura 2012, 1–28.
- Kim, H.K.; Lee, J.S.; Kim, J.H.; Seon, J.K.; Park, K.S.; Jeong, M.H.; Yoon, T.R. Bone-Forming Peptide-2 Derived from BMP-7 Enhances Osteoblast Differentiation from Multipotent Bone Marrow Stromal Cells and Bone Formation. Exp Mol Med 2017, 49, e328-7. [Google Scholar] [CrossRef] [PubMed]
- Segredo-Morales, E.; García-García, P.; Évora, C.; Delgado, A. BMP Delivery Systems for Bone Regeneration: Healthy vs Osteoporotic Population. Review. J Drug Deliv Sci Technol 2017, 42, 107–118. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, S.; Chen, X.; Hu, Y.; Wu, J.; Chen, S.; Chang, J.; Wang, G.; Gao, Y. Emodin Promotes the Osteogenesis of MC3T3-E1 Cells via BMP-9/Smad Pathway and Exerts a Preventive Effect in Ovariectomized Rats. Acta Biochim Biophys Sin (Shanghai) 2017, 49, 867–878. [Google Scholar] [CrossRef]
- Bartelt, A.; Behler-Janbeck, F.; Beil, F.T.; Koehne, T.; Müller, B.; Schmidt, T.; Heine, M.; Ochs, L.; Yilmaz, T.; Dietrich, M.; et al. Lrp1 in Osteoblasts Controls Osteoclast Activity and Protects against Osteoporosis by Limiting PDGF-RANKL Signaling. Bone Res 2018, 6, 1–10. [Google Scholar] [CrossRef]
- Lee, Z.H.; Kim, H.-J.; Ryoo, H.M. A Novel Osteogenic Activity of Suberoylanilide Hydroxamic Acid Is Synergized by BMP-2. J Bone Metab 2015, 22, 51–56. [Google Scholar] [CrossRef]
- Carreira, A.C.; Alves, G.G.; Zambuzzi, W.F.; Sogayar, M.C.; Granjeiro, J.M. Bone Morphogenetic Proteins: Structure, Biological Function and Therapeutic Applications. Arch Biochem Biophys 2014, 561, 64–73. [Google Scholar] [CrossRef]
- Ducy, P.; Karsenty, G. The Family of Bone Morphogenetic Proteins. Kidney Int 2000, 57, 2207–2214. [Google Scholar] [CrossRef] [PubMed]
- Leboy, P.; Grasso-Knight, G.; D’Angelo, M.; Volk, S.W.; Lian, J. v; Drissi, H.; Stein, G.S.; Adams, S.L. Smad-Runx Interactions during Chondrocyte Maturation. J Bone Joint Surg Am 2001, 83-A Suppl, S15-22. [CrossRef]
- Caplan, A.I.; Correa, D. PDGF in Bone Formation and Regeneration: New Insights into a Novel Mechanism Involving MSCs. Journal of Orthopaedic Research 2011, 29, 1795–1803. [Google Scholar] [CrossRef] [PubMed]
- Andrae, J.; Gallini, R.; Betsholtz, C. Role of Platelet-Derived Growth Factors in Physiology and Medicine. Genes Dev 2008, 22, 1276–1312. [Google Scholar] [CrossRef] [PubMed]
- Hollinger, J.O.; Onikepe, A.O.; MacKrell, J.; Einhorn, T.; Bradica, G.; Lynch, S.; Hart, C.E. Accelerated Fracture Healing in the Geriatric, Osteoporotic Rat with Recombinant Human Platelet-Derived Growth Factor-BB and an Injectable Beta-Tricalcium Phosphate/Collagen Matrix. J Orthop Res 2008, 26, 83–90. [Google Scholar] [CrossRef]
- Xie, H.; Cui, Z.; Wang, L.; Xia, Z.; Hu, Y.; Xian, L.; Li, C.; Xie, L.; Crane, J.; Wan, M.; et al. PDGF-BB Secreted by Preosteoclasts Induces Angiogenesis during Coupling with Osteogenesis. Nat Med 2014, 20, 1–12. [Google Scholar] [CrossRef]
- Pountos, I.; Georgouli, T.; Henshaw, K.; Bird, H.; Jones, E.; Giannoudis, P. v. The Effect of Bone Morphogenetic Protein-2, Bone Morphogenetic Protein-7, Parathyroid Hormone, and Platelet-Derived Growth Factor on the Proliferation and Osteogenic Differentiation of Mesenchymal Stem Cells Derived from Osteoporotic Bone. J Orthop Trauma 2010, 24, 552–556. [Google Scholar] [CrossRef] [PubMed]
- Bustos-Valenzuela, J.C.; Halcsik, E.; Bassi, E.J.; Demasi, M.A.; Granjeiro, J.M.; Sogayar, M.C. Expression, Purification, Bioactivity, and Partial Characterization of a Recombinant Human Bone Morphogenetic Protein-7 Produced in Human 293T Cells. Mol Biotechnol 2010, 46, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Lasota, A.; Danowska-Klonowska, D. Experimental Osteoporosis--Different Methods of Ovariectomy in Female White Rats. Rocz Akad Med Bialymst 2004, 49 Suppl 1, 129–131. [Google Scholar]
- Khajuria, D.K.; Razdan, R.; Mahapatra, D.R. Description of a New Method of Ovariectomy in Female Rats. Rev Bras Reumatol 2012, 52, 462–470. [Google Scholar]
- Azzi, C.M.G.; Nishiyama, A.C.O.C. Desenvolvimento de Um Modelo Animal Para Osteoporose Induzido Por Ooforectomia Em Rato Fêmea Nude (Rowett). São Paulo University (USP), 2017.
- Marcu, F.; Bogdan, F.; Muţiu, G.; Lazăr, L. The Histopathological Study of Osteoporosis. Rom J Morphol Embryol 2011, 52, 321–325. [Google Scholar]
- Carlsson, C.; Weisbrod, S. Ossos, Articulações, Tendões e Ligamentos. In Bases da Patologia em Veterinária; Zachary, J.F., McGavin, M.D., Eds.; Elsevier Ltd: Rio de Janeiro, 2013; pp. 923–974. [Google Scholar]
- Xu, H.; Liu, T.; Hu, L.; Li, J.; Gan, C.; Xu, J.; Chen, F.; Xiang, Z.; Wang, X.; Sheng, J. Effect of Caffeine on Ovariectomy-Induced Osteoporosis in Rats. Biomed Pharmacother 2019, 112, 108650. [Google Scholar] [CrossRef] [PubMed]
- Compston, J.E.; McClung, M.R.; Leslie, W.D. Osteoporosis. The Lancet 2019, 393, 364–376. [Google Scholar] [CrossRef] [PubMed]
- Vidal, M.; Thibodaux, R.J.; Neira, L.F.V.; Messina, O.D. Osteoporosis: A Clinical and Pharmacological Update. Clin Rheumatol 2019, 38, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Heiman, M.L. Increased Weight Gain after Ovariectomy Is Not a Consequence of Leptin Resistance. Am J Physiol Endocrinol Metab 2001, 280, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.Y.; Hong, Y.S.; Park, S.-H.; Ju, J.H. Increased Serum Alkaline Phosphatase Levels Correlate with High Disease Activity and Low Bone Mineral Density in Patients with Axial Spondyloarthritis. Semin Arthritis Rheum 2015, 45, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Mukaiyama, K.; Kamimura, M.; Uchiyama, S.; Ikegami, S.; Nakamura, Y.; Kato, H. Elevation of Serum Alkaline Phosphatase (ALP) Level in Postmenopausal Women Is Caused by High Bone Turnover. Aging Clin Exp Res 2015, 27, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Grigoryan, A. V.; Dimitrova, A.A.; Kostov, K.G.; Russeva, A.L.; Atanasova, M.A.; Blagev, A.B.; Betova, T.M.; Trifonov, R.G. Changes of Serum Concentrations of Alkaline Phosphatase and Metalloproteinase-9 in an Ovariectomized Wistar Rat Model of Osteoporosis. Journal of Biomedical and Clinical Research 2017, 10, 32–36. [Google Scholar] [CrossRef]
- Lang, J.; Zhao, Q.; He, Y.; Yu, X. Bone Turnover Markers and Novel Biomarkers in Lung Cancer Bone Metastases. Biomarkers 2018, 23, 518–526. [Google Scholar] [CrossRef]
- Salamanna, F.; Borsari, V.; Contartese, D.; Nicoli Aldini, N.; Fini, M. Link between Estrogen Deficiency Osteoporosis and Susceptibility to Bone Metastases: A Way towards Precision Medicine in Cancer Patients. Breast 2018, 41, 42–50. [Google Scholar] [CrossRef]
- Rahman, M.M.; Matsuoka, K.; Takeshita, S.; Ikeda, K. Secretion of PDGF Isoforms during Osteoclastogenesis and Its Modulation by Anti-Osteoclast Drugs. Biochem Biophys Res Commun 2015, 462, 159–164. [Google Scholar] [CrossRef]
- Li, D.; Wan, Q.; Pathak, J.L.; Li, Z. Platelet-Derived Growth Factor BB Enhances Osteoclast Formation and Osteoclast Precursor Cell Chemotaxis. J Bone Miner Metab 2017, 35, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Chen, J.; Jin, D. Platelet-Derived Growth Factor (PDGF)-BB Stimulates Osteoclastic Bone Resorption Directly: The Role of Receptor Beta. Biochem Biophys Res Commun 1998, 251, 190–194. [Google Scholar] [CrossRef]
- Salazar, V.S.; Gamer, L.W.; Rosen, V. BMP Signalling in Skeletal Development, Disease and Repair. Nat Rev Endocrinol 2016, 12, 203–221. [Google Scholar] [CrossRef] [PubMed]
- Desmyter, S.; Goubau, Y.; Benahmed, N.; de Wever, A.; Verdonk, R. The Role of Bone Morphogenetic Protein-7 (Osteogenic Protein-1) in the Treatment of Tibial Fracture Non-Unions. An Overview of the Use in Belgium. Acta Orthop Belg 2008, 74, 534–537. [Google Scholar] [PubMed]
- Cecchi, S.; Bennet, S.J.; Arora, M. Bone Morphogenetic Protein-7: Review of Signalling and Efficacy in Fracture Healing. J Orthop Translat 2016, 4, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Helbig, L.; Omlor, G.W.; Ivanova, A.; Guehring, T.; Sonntag, R.; Kretzer, J.P.; Minkwitz, S.; Wildemann, B.; Schmidmaier, G. Bone Morphogenetic Proteins - 7 and - 2 in the Treatment of Delayed Osseous Union Secondary to Bacterial Osteitis in a Rat Model. BMC Musculoskelet Disord 2018, 19, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.C.; Hilyard, A.C.; Wu, C.; Davis, B.N.; Hill, N.S.; Lal, A.; Lieberman, J.; Lagna, G.; Hata, A.; Rahman, M.M.; et al. Molecular Basis for Antagonism between PDGF and the TGFΒ Family of Signalling Pathways by Control of MiR-24 Expression. EMBO Journal 2010, 29, 559–573. [Google Scholar] [CrossRef] [PubMed]
- Bayer, E.A.; Fedorchak, M. v.; Little, S.R. The Influence of Platelet-Derived Growth Factor and Bone Morphogenetic Protein Presentation on Tubule Organization by Human Umbilical Vascular Endothelial Cells and Human Mesenchymal Stem Cells in Coculture. Tissue Eng Part A 2016, 22, 1296–1304. [Google Scholar] [CrossRef] [PubMed]
- Pittenger, M.F.; Mackay, A.M.; Beck, S.C.; Jaiswal, R.K.; Douglas, R.; Mosca, J.D.; Moorman, M.A.; Simonetti, D.W.; Craig, S.; Marshak, D.R. Multilineage Potential of Adult Human Mesenchymal Stem Cells. Science 1999, 284, 143–147. [Google Scholar] [CrossRef]
- Komori, T. Regulation of Osteoblast Differentiation by Transcription Factors. J Cell Biochem 2006, 99, 1233–1239. [Google Scholar] [CrossRef]
- Zhuang, H.; Zhang, X.; Zhu, C.; Tang, X.; Yu, F.; Shang, G.W.; Cai, X. Molecular Mechanisms of PPAR-γ Governing MSC Osteogenic and Adipogenic Differentiation. Curr Stem Cell Res Ther 2016, 11, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.A.; Israel, D.I.; Kelly, S.; Luxenberg, D.P. Bone Morphogenetic Protein-2 Causes Commitment and Differentiation in C3H10T1/2 and 3T3 Cells. Growth Factors 1993, 9, 57–71. [Google Scholar] [CrossRef] [PubMed]
- Hata, K.; Nishimura, R.; Ikeda, F.; Yamashita, K.; Matsubara, T.; Nokubi, T.; Yoneda, T. Differential Roles of Smad1 and P38 Kinase in Regulation of Peroxisome Proliferator-Activating Receptor Gamma during Bone Morphogenetic Protein 2-Induced Adipogenesis. Mol Biol Cell 2003, 14, 545–555. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Yin, C.; Zhao, F.; Ali, A.; Ma, J.; Qian, A. Mesenchymal Stem Cells: Cell Fate Decision to Osteoblast or Adipocyte and Application in Osteoporosis Treatment. Int J Mol Sci 2018, 19. [Google Scholar] [CrossRef] [PubMed]
- Astudillo, P.; Ríos, S.; Pastenes, L.; Pino, A.M.; Rodríguez, J.P. Increased Adipogenesis of Osteoporotic Human-Mesenchymal Stem Cells (MSCs) Characterizes by Impaired Leptin Action. J Cell Biochem 2008, 103, 1054–1065. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, M.C.; Berry, R.; Holtrup, B.; Sebo, Z.; Nelson, T.; Fretz, J.A.; Lindskog, D.; Kaplan, J.L.; Ables, G.; Rodeheffer, M.S.; et al. Bone Marrow Adipocytes. Adipocyte 2017, 6, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Li, X.; Zhi, X.; Cong, W.; Huang, B.; Chen, H.; Wang, Y.; Li, Y.; Wang, L.; Fang, C.; et al. RANKL from Bone Marrow Adipose Lineage Cells Promotes Osteoclast Formation and Bone Loss. EMBO Rep 2021, e52481. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Zhong, L.; Yao, L.; Wei, Y.; Gui, T.; Li, Z.; Kim, H.; Holdreith, N.; Jiang, X.; Tong, W.; et al. Bone Marrow Adipogenic Lineage Precursors Promote Osteoclastogenesis in Bone Remodeling and Pathologic Bone Loss. Journal of Clinical Investigation 2021, 131. [Google Scholar] [CrossRef]
- Black, D.M.; Delmas, P.D.; Eastell, R.; Reid, I.R.; Boonen, S.; Cauley, J.A.; Cosman, F.; Lakatos, P.; Leung, P.C.; Man, Z.; et al. Once-Yearly Zoledronic Acid for Treatment of Postmenopausal Osteoporosis. N Engl J Med 2007, 356, 1809–1822. [Google Scholar] [CrossRef]
Figure 1.
Comparison of weight gain on day 0 between oophorectomized animals, the control groups and the Sham group. Two-way ANOVA test, p<0.001. N. Control: 4; N. Sham: 4; N. Oophorectomy: 36.
Figure 1.
Comparison of weight gain on day 0 between oophorectomized animals, the control groups and the Sham group. Two-way ANOVA test, p<0.001. N. Control: 4; N. Sham: 4; N. Oophorectomy: 36.
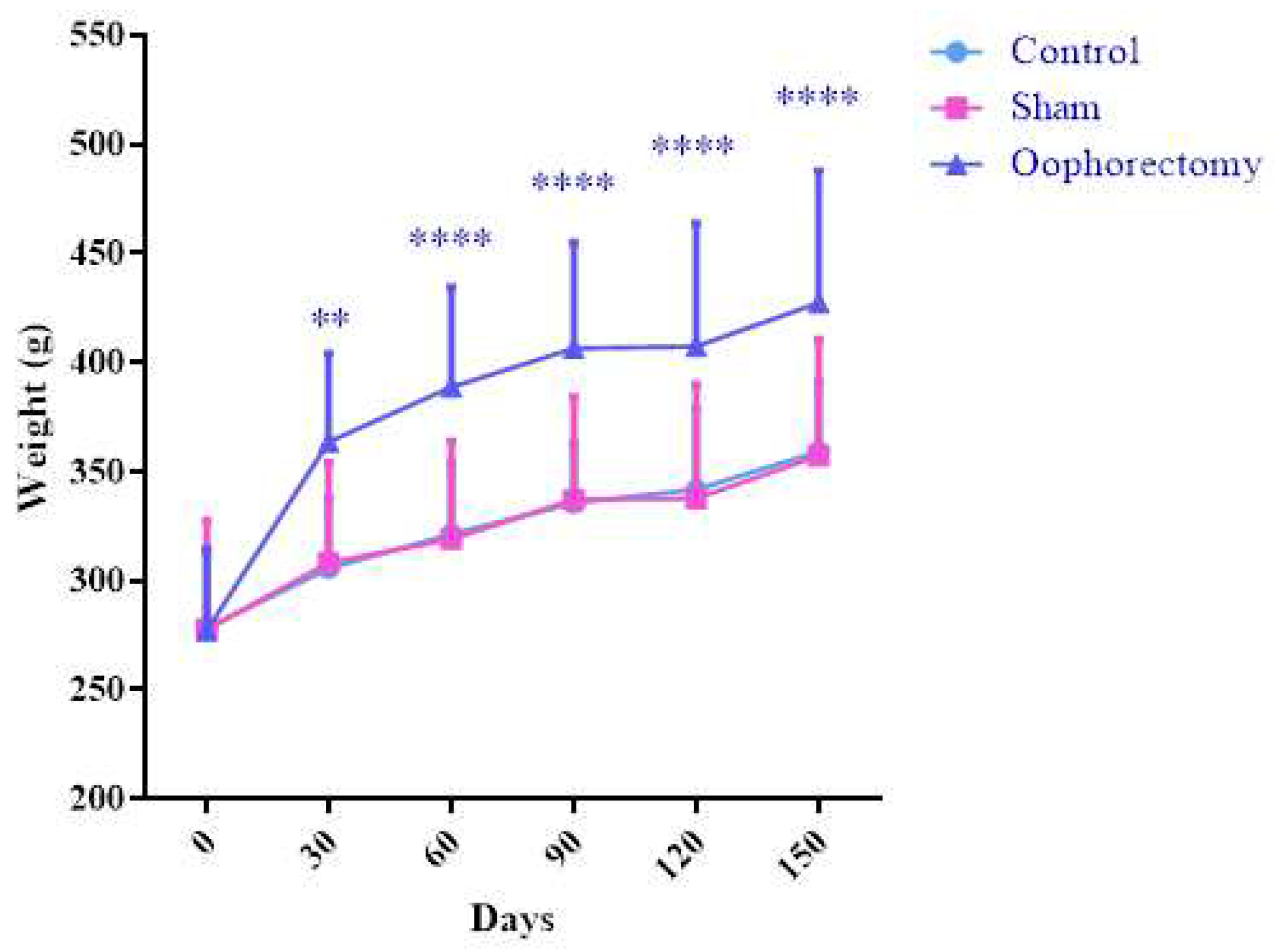
Figure 2.
Comparison of weight gain during treatment, between the different treatments studied. Two-way ANOVA test. N.: 4. Zol. Ac.: Zoledronic Acid.
Figure 2.
Comparison of weight gain during treatment, between the different treatments studied. Two-way ANOVA test. N.: 4. Zol. Ac.: Zoledronic Acid.
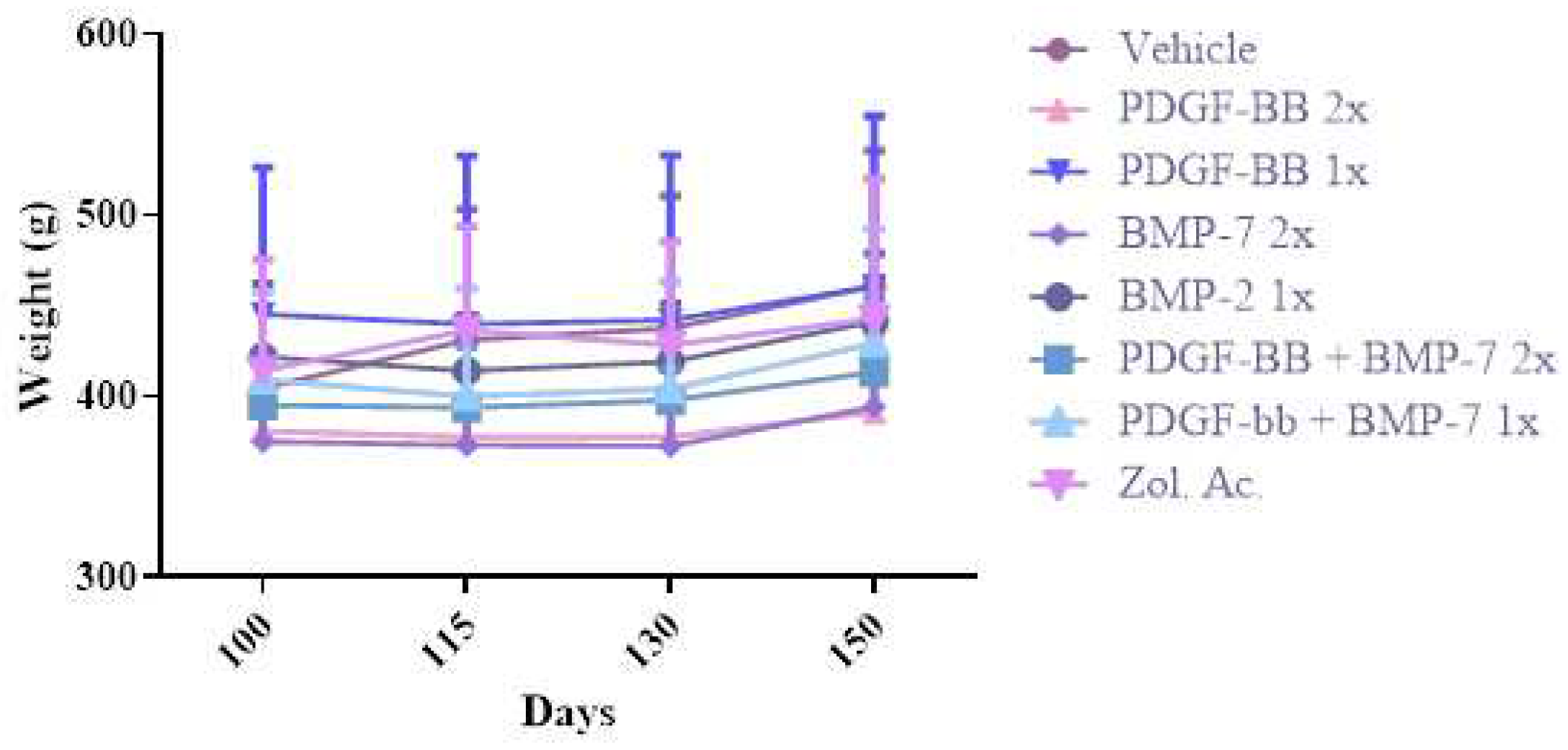
Figure 3.
Alkaline phosphatase (ALP) concentration in animal serum on days 0 (D0) and 100 (D100) after oophorectomy surgery. U/L= Units per liter. Paired T-test, *: p<0.05. N.: 32.
Figure 3.
Alkaline phosphatase (ALP) concentration in animal serum on days 0 (D0) and 100 (D100) after oophorectomy surgery. U/L= Units per liter. Paired T-test, *: p<0.05. N.: 32.
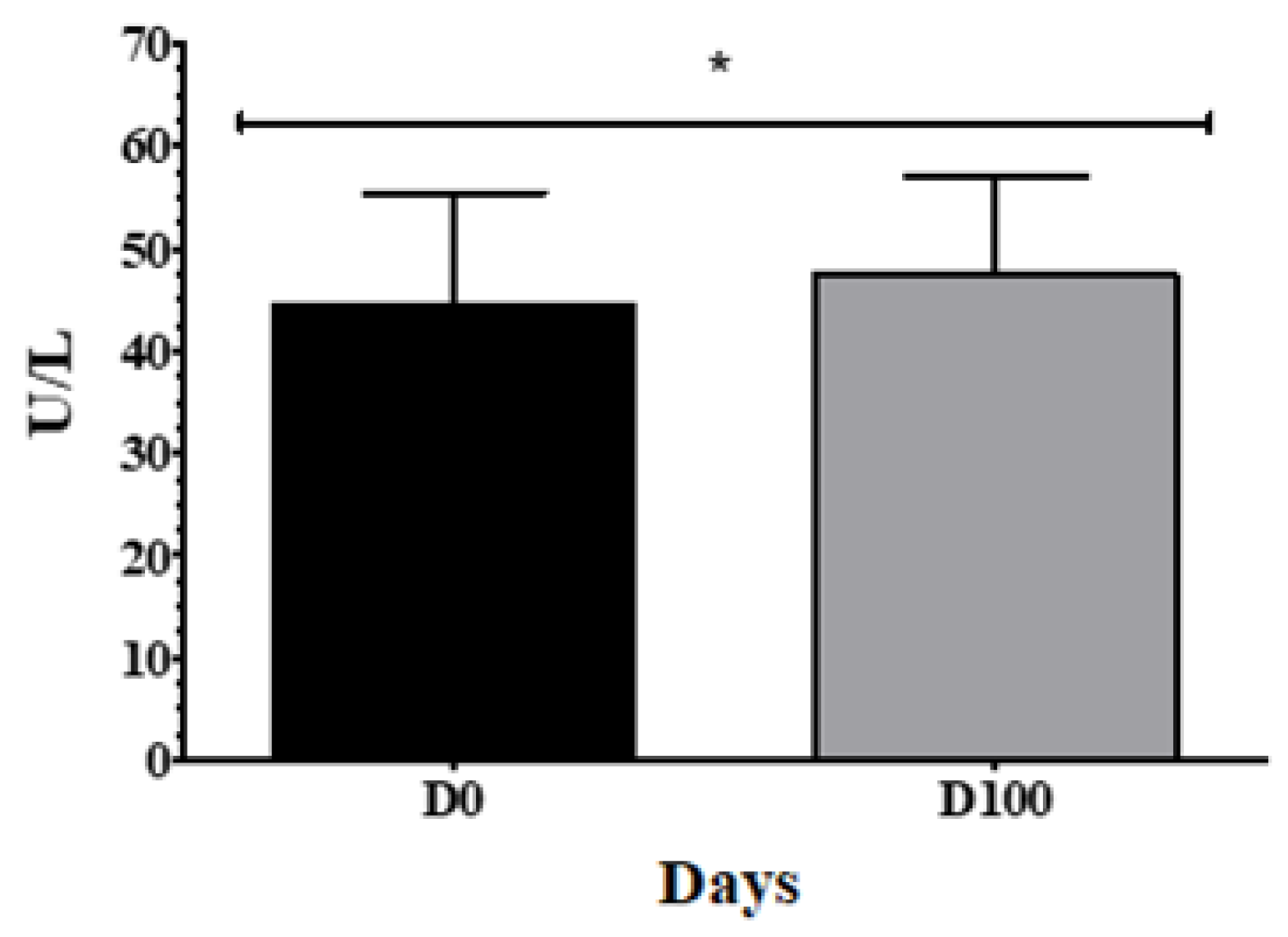
Figure 4.
X-Ray Analysis. On the 100th day after surgery (D100) the Bone Mineral Density of the femoral neck of the oophorectomized animals showed a significant reduction compared to the Sham group. Unpaired t-test, *: p<0.05. N. Oophorectomy: 32, N. Sham: 4.
Figure 4.
X-Ray Analysis. On the 100th day after surgery (D100) the Bone Mineral Density of the femoral neck of the oophorectomized animals showed a significant reduction compared to the Sham group. Unpaired t-test, *: p<0.05. N. Oophorectomy: 32, N. Sham: 4.
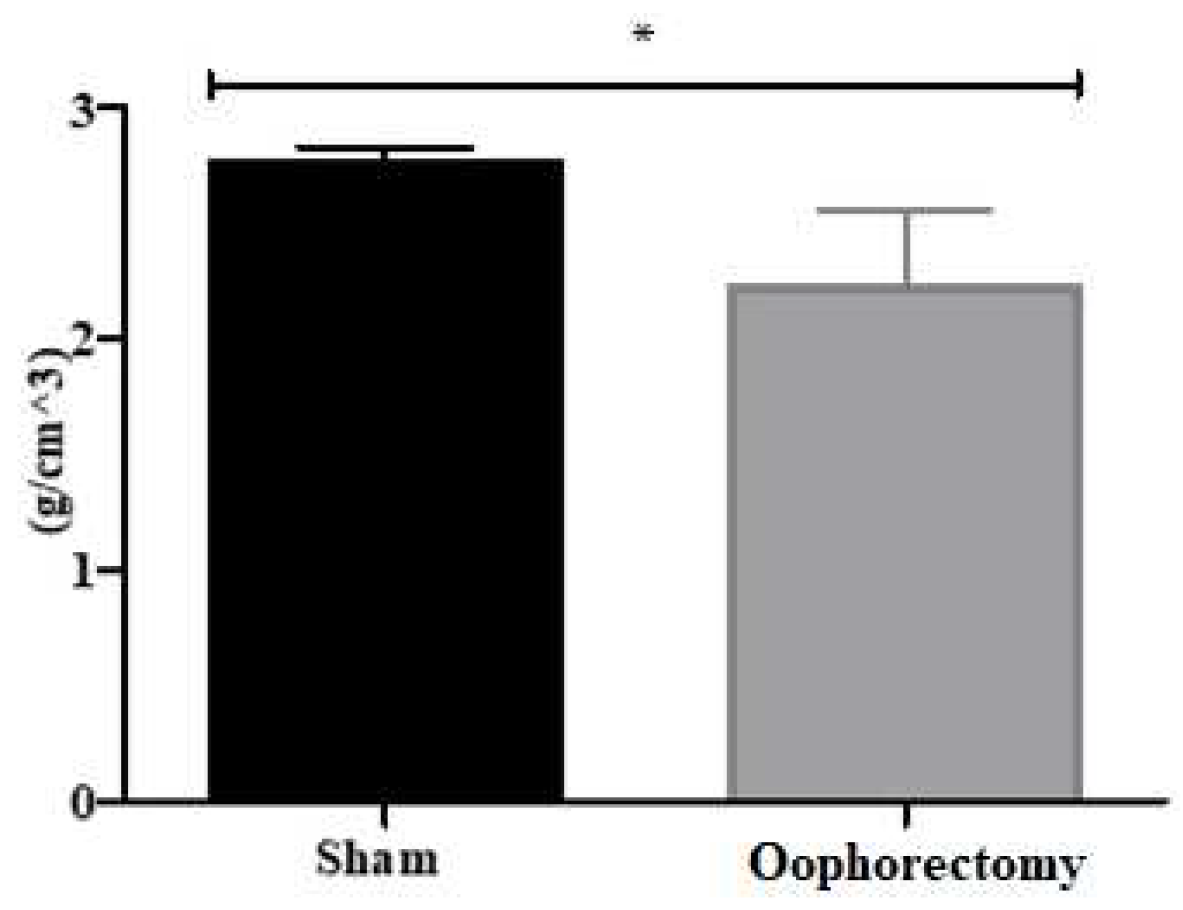
Figure 5.
Comparison of the bone volume fraction (BV/TV) of the trabecular region between animals in the Sham and Oophorectomy group, expressed in percentage. Unpaired t-test, **: p<0.01. N=4.
Figure 5.
Comparison of the bone volume fraction (BV/TV) of the trabecular region between animals in the Sham and Oophorectomy group, expressed in percentage. Unpaired t-test, **: p<0.01. N=4.
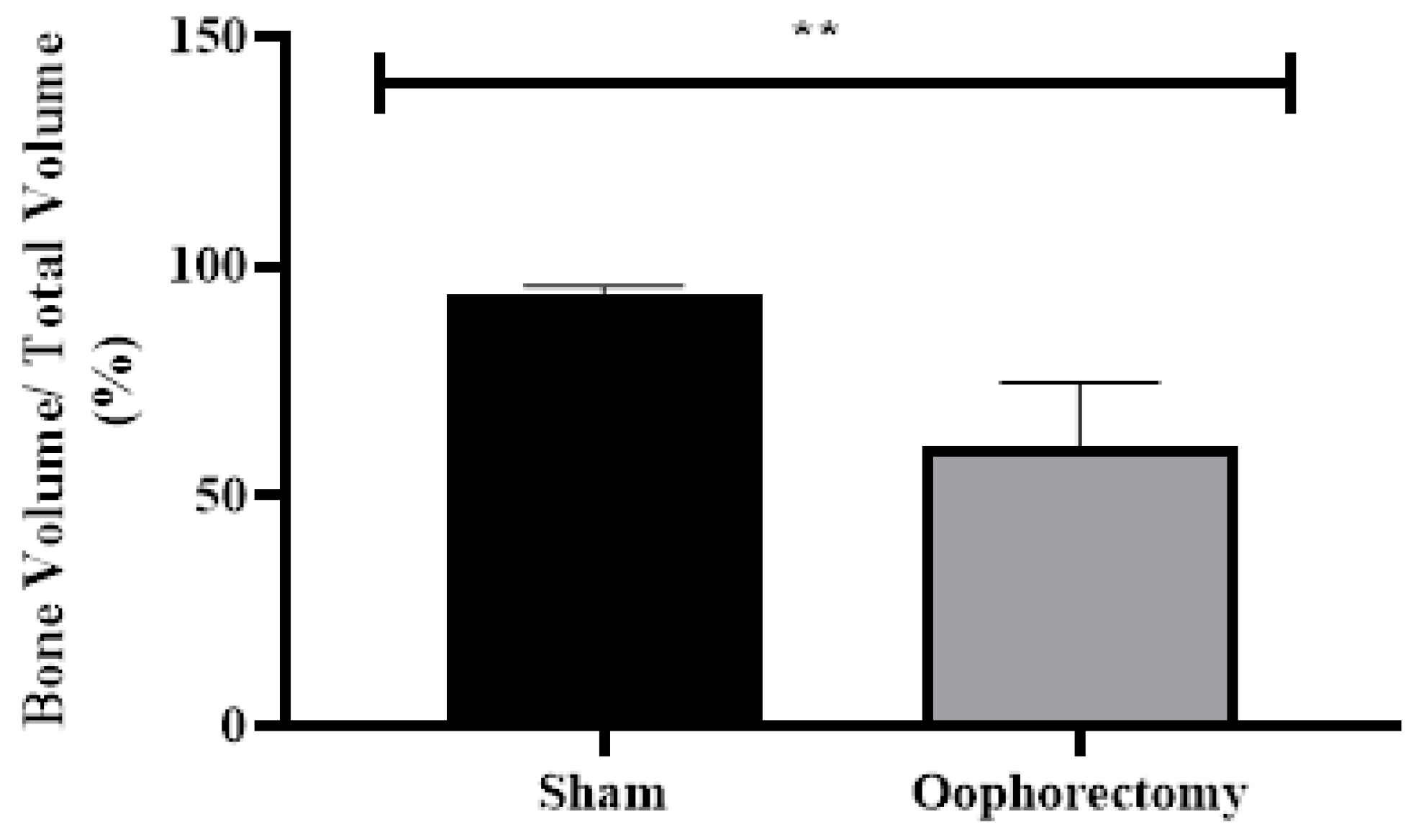
Figure 6.
Comparison of the bone volume fraction of the cortical region between the animals in the Sham and Oophorectomy groups, expressed in percentage. Unpaired t-test, *: p<0.05. N=4.
Figure 6.
Comparison of the bone volume fraction of the cortical region between the animals in the Sham and Oophorectomy groups, expressed in percentage. Unpaired t-test, *: p<0.05. N=4.
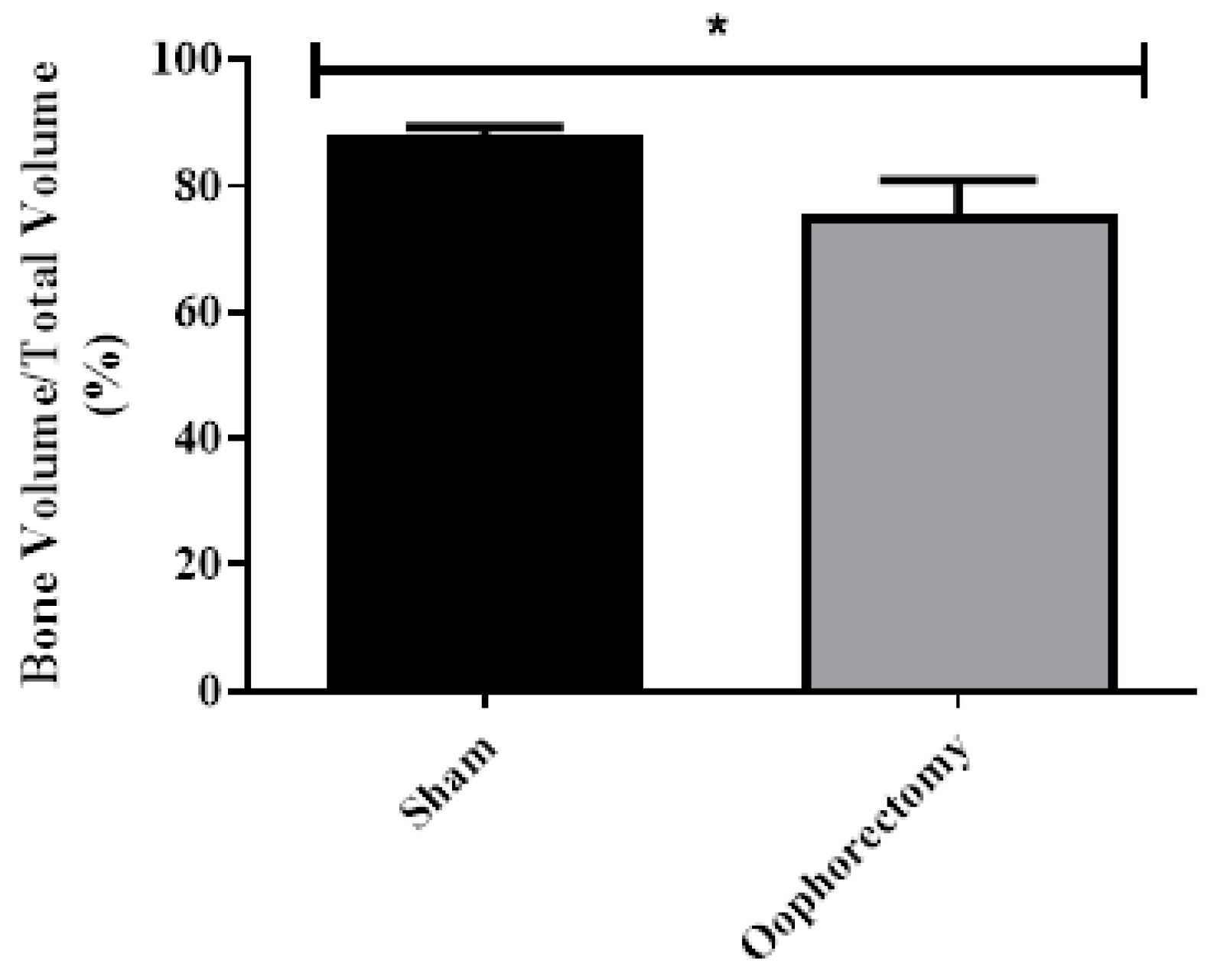
Figure 7.
Micro-CT analysis of the proximal portion of the femoral epiphysis (1st Region). [A]: Bone volume fraction; [B]: Thickness of trabeculae; [C]: Number of trabeculae; [D]: Separation of trabeculae; [E]: Bone mineral density (BMD). One way ANOVA Test and Dunnett's Test against Vehicle, *: p<0.05, **: p<0.01. N=4. Zol. Acid: Zoledronic Acid.
Figure 7.
Micro-CT analysis of the proximal portion of the femoral epiphysis (1st Region). [A]: Bone volume fraction; [B]: Thickness of trabeculae; [C]: Number of trabeculae; [D]: Separation of trabeculae; [E]: Bone mineral density (BMD). One way ANOVA Test and Dunnett's Test against Vehicle, *: p<0.05, **: p<0.01. N=4. Zol. Acid: Zoledronic Acid.
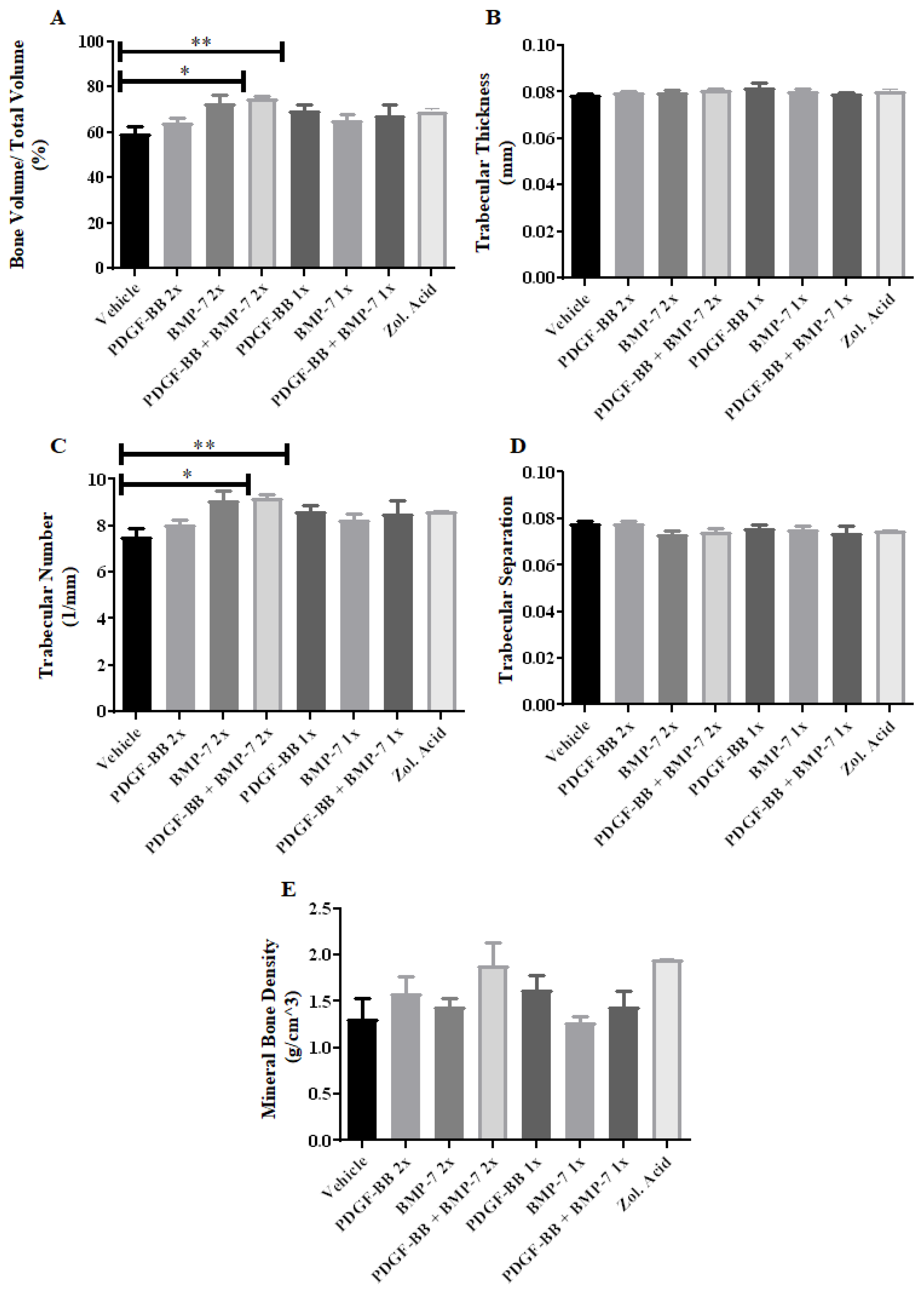
Figure 8.
Histological data indicating the development of osteoporosis in oophorectomized animals. [A]: Control stained with HE; [B]: Sham stained with HE stained; [C]: Oophorectomy stained with HE stained; [D]: Control stained with Masson's Trichrome; [E]: Sham stained with Masson's Trichrome; [F]: Masson's Trichrome stained oophorectomy; [G]: Score of the clinical status of controls referring to histopathological analysis; [H]: Controls trabecular reduction score for histopathological analysis. N.: 4. Scale bar: 200µm. Ad: Adipocytes; BM: Bone Marrow; Tr: Trabeculae; EL: Epiphyseal Line.
Figure 8.
Histological data indicating the development of osteoporosis in oophorectomized animals. [A]: Control stained with HE; [B]: Sham stained with HE stained; [C]: Oophorectomy stained with HE stained; [D]: Control stained with Masson's Trichrome; [E]: Sham stained with Masson's Trichrome; [F]: Masson's Trichrome stained oophorectomy; [G]: Score of the clinical status of controls referring to histopathological analysis; [H]: Controls trabecular reduction score for histopathological analysis. N.: 4. Scale bar: 200µm. Ad: Adipocytes; BM: Bone Marrow; Tr: Trabeculae; EL: Epiphyseal Line.
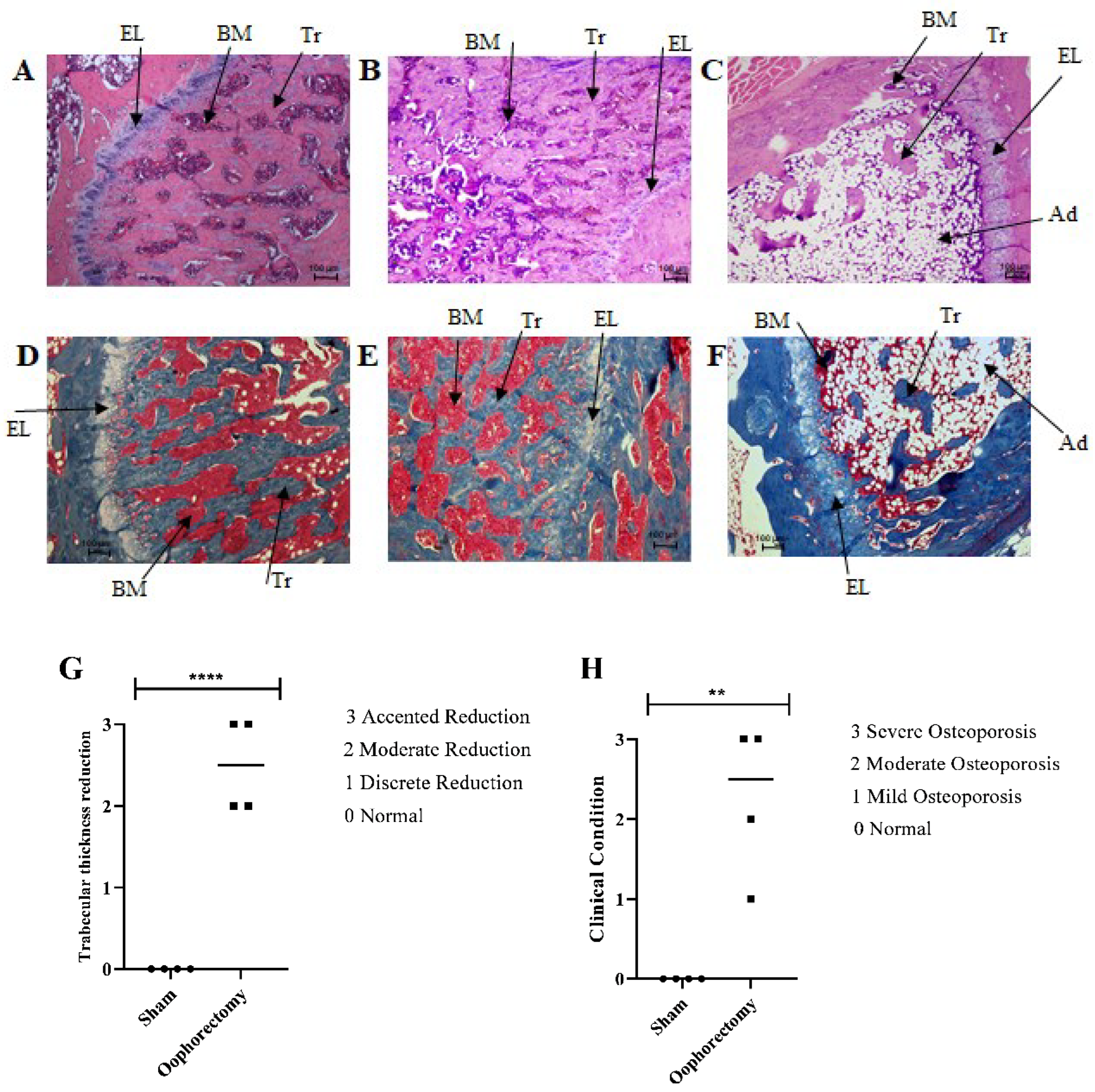
Figure 9.
Masson's Trichrome stained histological slides comparing the different treatments. [A]: Vehicle; [B]: Zoledronic acid; [C]: PDGF-BB 2x/week; [D]: PDGF-BB 1x/week; [E]: BMP-7 2x/week [F]: BMP-7 1/week; [G]: PDGF-BB + BMP-7 2x/week [H]: PDGF-BB + BMP-7 1x/week. Scale bar: 200µm. In blue are collagen fibers, cytoplasm in red and cell nuclei in purple. Ad: Adipocytes; BM: Bone Marrow; Tr: Trabeculae; EL: Epiphyseal Line.
Figure 9.
Masson's Trichrome stained histological slides comparing the different treatments. [A]: Vehicle; [B]: Zoledronic acid; [C]: PDGF-BB 2x/week; [D]: PDGF-BB 1x/week; [E]: BMP-7 2x/week [F]: BMP-7 1/week; [G]: PDGF-BB + BMP-7 2x/week [H]: PDGF-BB + BMP-7 1x/week. Scale bar: 200µm. In blue are collagen fibers, cytoplasm in red and cell nuclei in purple. Ad: Adipocytes; BM: Bone Marrow; Tr: Trabeculae; EL: Epiphyseal Line.

Figure 10.
HE stained histological slides comparing the different treatments. [A]: Vehicle; [B]: Zoledronic acid; [C]: PDGF-BB 2x/week; [D]: PDGF-BB 1x/week; [E]: BMP-7 2x/week [F]: BMP-7 1/week; [G]: PDGF-BB + BMP-7 2x/week [H]: PDGF-BB + BMP-7 1x/week. Scale bar: 100µm. In pink/reddish are the cytoplasms and collagen fibers, in purple were stained the cell nuclei. Ad: Adipocytes; BM: Bone Marrow; Tr: Trabeculae; EL: Epiphyseal Line.
Figure 10.
HE stained histological slides comparing the different treatments. [A]: Vehicle; [B]: Zoledronic acid; [C]: PDGF-BB 2x/week; [D]: PDGF-BB 1x/week; [E]: BMP-7 2x/week [F]: BMP-7 1/week; [G]: PDGF-BB + BMP-7 2x/week [H]: PDGF-BB + BMP-7 1x/week. Scale bar: 100µm. In pink/reddish are the cytoplasms and collagen fibers, in purple were stained the cell nuclei. Ad: Adipocytes; BM: Bone Marrow; Tr: Trabeculae; EL: Epiphyseal Line.
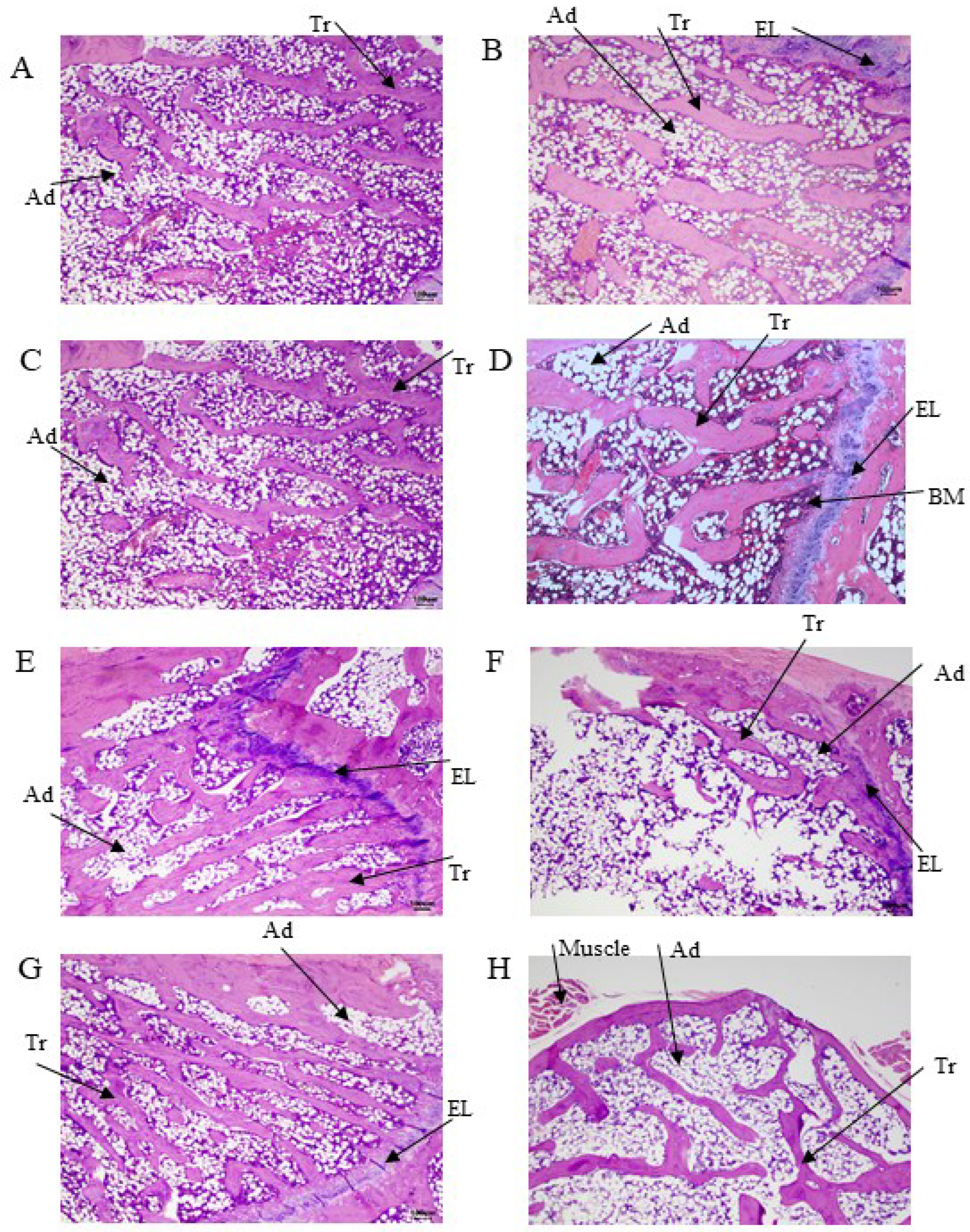
Figure 11.
Trabecular thickness scores of different treatment groups referring to histomorphological analysis.
Figure 11.
Trabecular thickness scores of different treatment groups referring to histomorphological analysis.
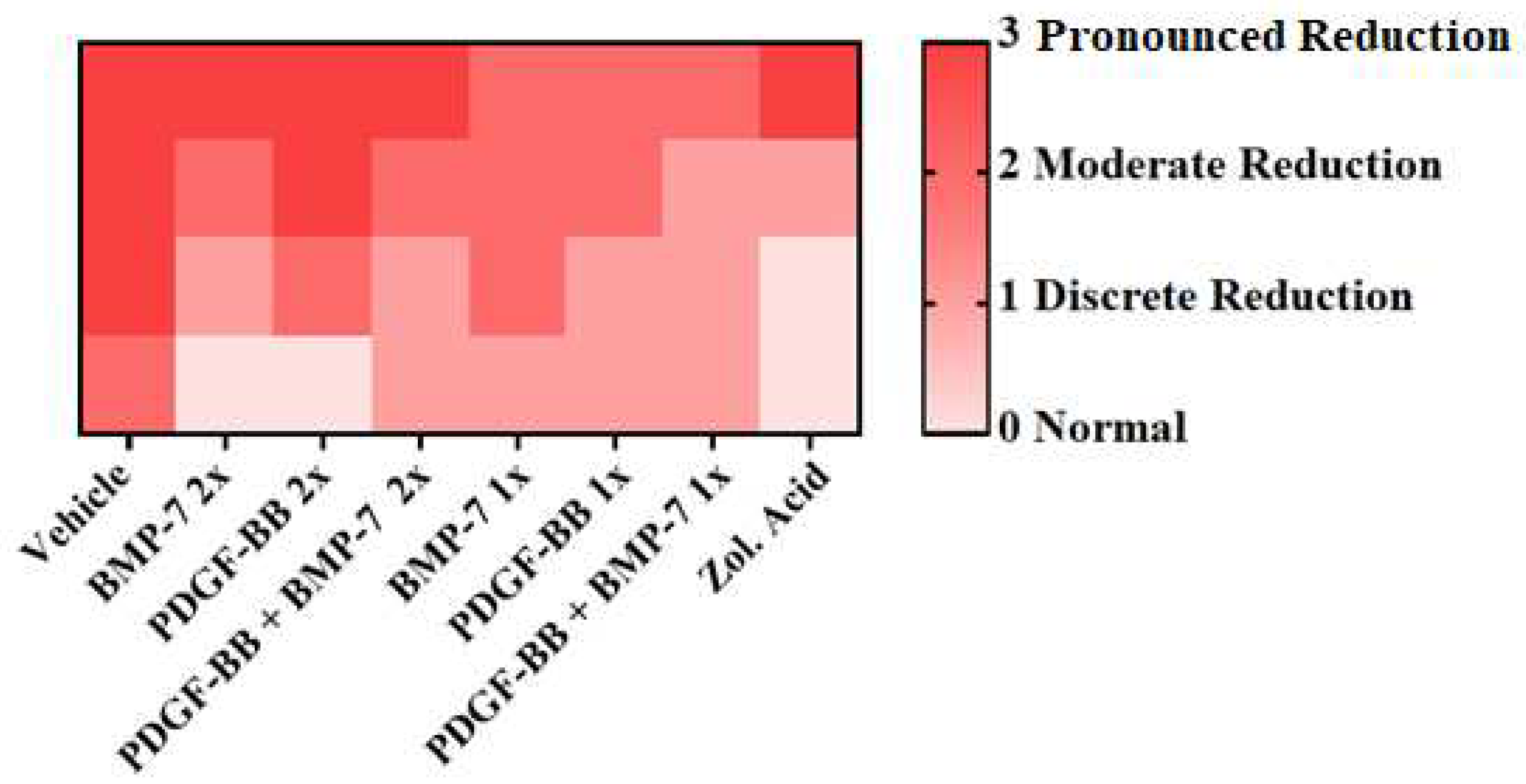
Figure 12.
Scores of the clinical picture of the different treatment groups regarding the histopathological analysis.
Figure 12.
Scores of the clinical picture of the different treatment groups regarding the histopathological analysis.
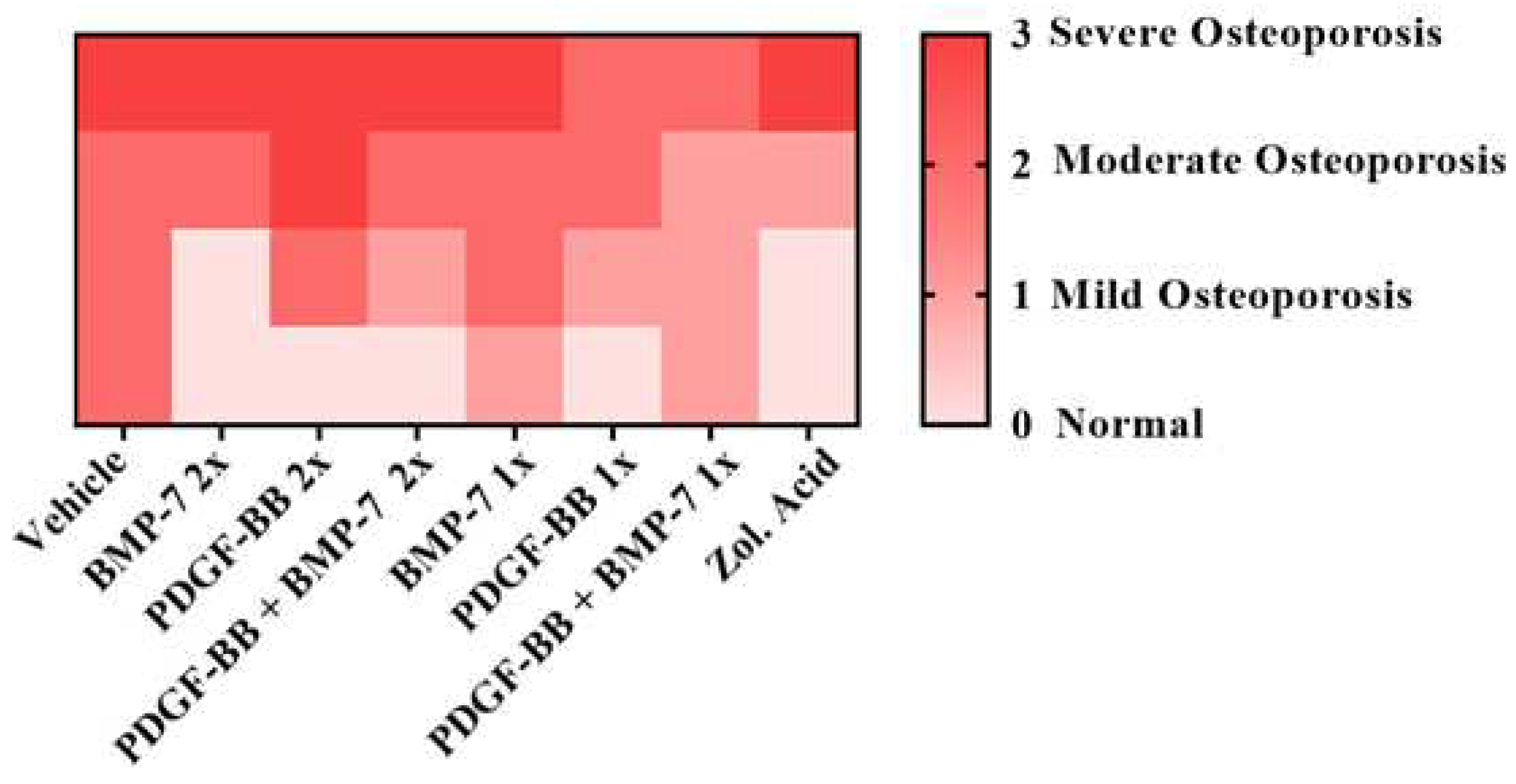

Table 1.
Group treatment´s division.
| Group | Surgery | Treatment | Number of injections | Dose/Injection | Euthanasia |
|---|---|---|---|---|---|
| Control | Not performed | None | Not applicable | Not applicable | 150 days |
| Sham | Surgery without ovaries remotion | None | Not applicable | Not applicable | 150 days |
|
Zoledronic Acid |
Oophorectomy | Zoledronic acid | Two injections with 22 days interval | 100 µg/kg | 150 days |
| Vehicle | Oophorectomy | None | 2x/week | 20mM Tris-HCl pH 7.2 + 300 mM NaCl | 150 days |
| PDGF-BB 2x | Oophorectomy | PDGF-BB | 2x/week | 20 µg/kg | 150 days |
| BMP-7 2x | Oophorectomy | BMP-7 | 2x/week | 30 µg/kg | 150 days |
| PDGF-BB + BMP-7 2x | Oophorectomy | PDGF-BB + BMP-7 | 2x/week | 20 µg/kg of PDGF-BB + 30 µg/kg of BMP-7 | 150 days |
| PDGF-BB 1x | Oophorectomy | PDGF-BB | 1x/week | 20 µg/kg | 150 days |
| BMP-7 2x | Oophorectomy | BMP-7 | 1x/week | 30 µg/kg | 150 days |
| PDGF-BB + BMP-7 1x | Oophorectomy | PDGF-BB + BMP-7 | 1x/week | 20 µg/kg of PDGF-BB + 30 µg/kg of BMP-7 | 150 days |
| Oophorectomy | Oophorectomy | None | Not applicable | Not applicable | 100 days |
Table 2.
Trabecular thickness observed in the histomorphological analysis and respective score.
| Score | Trabecular Thickness |
|---|---|
| 0 | Normal |
| 1 | Discrete reduction |
| 2 | Moderate reduction |
| 3 | Pronounced reduction |
Table 3.
Clinical characteristics resulting from the microscopic findings e their respective score.
| Score | Clinical condition |
|---|---|
| 0 | Normal |
| 1 | Mild osteoporosis |
| 2 | Moderate osteoporosis |
| 3 | Severe osteoporosis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



