
Submitted:
16 November 2023
Posted:
17 November 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Data from the WHO and UNICEF Estimates of National Immunization Coverage (WUENIC) 2022 revision were analyzed to assess the status of routine immunization in the WHO African Region, disrupted by the COVID-19 pandemic. In 2022, the coverage with the first and third dose of diphtheria-tetanus-pertussis containing vaccine (DTP1 and DTP3 respectively) and with the first dose of measles-containing vaccine (MCV1), in the region, was estimated at 80%, 72% and 69%, respectively (all below the 2019 level). Only 13 of the 47 countries (28%) achieved the global target coverage of 90% or above with DTP3 in 2022. From 2019 to 2022, 28.7 million zero-dose were recorded (19.0% of target population). Ten countries of the region accounted for 80.3% of all zero-dose children including the four most populous countries (Nigeria, Ethiopia, Democratic Republic of the Congo, United Republic of Tanzania). Reported administrative coverage greater than WUENIC was found in 19 countries, highlighting routine immunization data quality issues. The WHO African region has not yet recovered from COVID-19 disruptions to routine immunization. It is critical for Governments to ensure that processes are in place to prioritize investments for restoring immunization services, catching-up on vaccination of zero-dose and un-der-vaccinated children and improving data quality.
Keywords:
Routine immunization
; vaccination coverage
; zero-dose
; WUENIC
; COVID-19
; Catch-up
; African region
1. Introduction
The COVID-19 pandemic has substantially disrupted routine immunization services in the World Health Organization (WHO) African Region, leading to precipitous decline in childhood vaccination rates compared to pre-pandemic levels [1,2,3,4]. The African region is one of the six regions of the WHO and is made up of 47 out the 54 countries of the African continent [5]. The first laboratory confirmed case of COVID-19 in the African region was reported on 25 February 2020, in Algeria [6]. COVID-19 then quickly spread to all African region’s countries [6]. In addition to setting up surveillance and case-management systems, governments in the region implemented non-pharmaceutical interventions to minimize social contacts, including but not limited to travel restrictions, curfews, school closures and partial or full lockdowns [6,7]. The COVID-19 lockdowns have had adverse consequences on health services provision and utilization. Childhood routine immunization is among the public health services disrupted by the COVID-19 pandemic and its response measures, leading to parents avoiding routine immunization sessions due to fear of getting infected by COVID-19 [8], postponement of mass vaccination campaigns and diversion of resources due to COVID-19 pandemic response in an already underfunded health system [9,10]. Accordingly, the COVID-19 pandemic significantly contributed to the decline in routine immunization coverage, resulting in a greater number of zero-dose and under-immunized children [10]. Zero-dose children refers to children who have not received any routine vaccination and more specifically are lacking the first dose of diphtheria-tetanus-pertussis containing vaccine (DTP), while under-immunized children are those missing the third dose of DTP vaccine [11].
To speed up the recovery of immunization services, the Immunization Agenda 2030 (IA2030) partners, including WHO, UNICEF and Ministries of Health, joined forces on April 2023 to call for “The Big Catch-Up”, a targeted global effort to boost vaccination among children following COVID-19-related declines, with a particular focus on countries that recorded the highest number of zero-dose [12]. This Big Catch-Up takes a three-pillar strategic approach, including (i) catching-up on vaccination of children missed since 2019, (ii) restoring the immunization services to close the gap between the current and the 2019 pre-pandemic status in terms of immunization coverage, and (iii) strengthening immunization and primary health care (PHC) systems to ensure that countries get back on track towards the IA2030 targets [13].
Given the lifting of the public health emergency of international concern (PHEIC) status for the COVID-19 pandemic by the WHO [13], it is critical to assess the status of routine immunization in the African region. This paper summarizes the trend and geographical distribution of immunization coverage as well as number of un- and under-immunized children in the WHO African region from 2019, representing the pre-pandemic period, to 2022 as the end point of the emergency phase of the COVID-19 pandemic.
2. Materials and Methods
A retrospective descriptive analysis of secondary data pertaining to routine immunization coverage in the WHO African Region as of the end of 2022 compared to the pre-COVID-19 pandemic level (2019) was conducted.
Inclusion and Exclusion Criteria
Countries in the WHO African Region that reported data on routine immunization coverage to the WHO and UNICEF in 2022 through the Joint Reporting Forms (JRF) [14] were included. All 47 countries of the WHO African Region met this criterion and were included. The seven African countries that are part of the WHO Eastern Mediterranean Region were excluded.
Data Sources and Measurement
The WHO and UNICEF Estimates of National Immunization Coverage (WUENIC) 2022 revision and administrative data reported to WHO and UNICEF through JRF [14] were used for this analysis. These estimates [15,16] are country-specific and limited to the national level. The primary indicator (variable) of interest was national-level coverage of each antigen or combination of antigens. Coverage was measured as the number of children immunized with each antigen/combination of antigen divided by the target population.
Fourteen antigens or combination of antigens were tracked in the 2022 revision of WUENIC (released in July 2023). All the 14 antigens or combination of antigens were considered in this study: Bacille Calmette-Guérin (BCG), the first and second dose of measles-containing vaccine (MCV1 and MCV2), the first and third dose of the diphtheria-tetanus-pertussis containing vaccine (DTP1 and DPT3), the third dose of the oral poliovirus vaccine (POL3), the first dose of the inactivated poliovirus vaccine (IPV1), the first dose of the rubella-containing vaccine (RCV1), the hepatitis B vaccine at birth (HEPBB) and the third dose (HEPB3), the third dose of the Haemophilus influenzae type b vaccine (HIB3), the yellow fever vaccine (YFV), the last dose of the rotavirus vaccine (ROTAC), and the third dose of the pneumococcal conjugate vaccine (PCV3). HEPBB dose estimates were considered only for countries with ability to record data within 48 hours of vaccination. Some countries provided birth dose but were unable to record timely vaccination and therefore coverage estimates were not made.
Data Analysis
Data from WUENIC from 2015 to 2022 were analyzed.
In addition to the immunization coverage for each antigen or combination of antigens (provided by the WUENIC 2022 revision), the following parameters were calculated:
- Percentage of difference in immunization coverage compared to pre-pandemic coverage: coverage of the year under review divided by the 2019 coverage, minus one and multiplied by 100. To calculate a percentage difference in the few countries where coverage was null in 2019 but non-zero in 2022, coverage in 2019 was set to 1.
- Number of zero-dose (ZD) children: number of surviving infants (aged 0-11 months) for a given year (from the United Nations (UN) Population Estimates 2022 revision) [17] minus the number of children vaccinated with DTP1 during the same year.
- Number of un-immunized children for vaccines other than DTP: number of target population for a given year and antigen (from UN Population Estimates 2022 revision), minus the number of children vaccinated with the related vaccine during the same year.
- Number of under-immunized children: number of children vaccinated with the last dose of a given vaccine minus the number of children vaccinated with the first dose of the said vaccine.
- Percentage of ZD children: Number of zero-dose children divided by surviving infants for the same period, multiplied by 100.
Countries’ administrative coverages in 2022 for DTP3 were compared to the WHO and UNICEF estimates. Administrative coverage was computed from administrative target population and number of doses administered from health facilities as reported by national authorities to WHO and UNICEF on a yearly basis, through JRF.
All data analyses and visualizations were performed using the R software version 4.1.2 [18].
3. Results
Overview of Data Reported
Data on immunization coverage in 2022 were available for 47 countries for BCG, DTP1, DTP3, HEPB3, HIB3, MCV1 and POL3. The number of countries with data available was 41 for MCV2, 40 for PCV3, 38 for ROTAC, 32 for RCV1, 24 for YFV and 11 for HEPBB.
Immunization Coverage Trends
In 2022, 30.8 million children aged 0-11 months were immunized with the first dose of DTP compared to 30.4 million in 2021, resulting in immunization of about 350 000 additional children. The percentage of children having received the first and third doses of DTP in the WHO African Region in 2022 was estimated at 80% and 72%, respectively. DTP1 coverage declined from 83% in 2019 to 81% in 2020, before plateauing at 80% in 2021 and 2022, while DTP3 coverage declined from 77% in 2019 to 74% in 2020 before plateauing at 72% in 2021 and 2022.
About 26.5 million children were immunized with the first dose of MCV (MCV1) in 2022 compared to 26 million in 2021, that is about 484 000 additional children immunized. The percentage of children having received MCV1 in 2022 in the WHO African region was estimated at 69%. This coverage declined from 71% in 2019 to 70% in 2020, before fluctuating between 68% in 2021 and 69% in 2022. The same trends were observed with BCG, HEPB3, HIB3, POL3 and PCV3. With regards to newly introduced vaccines (MCV2, HEPBB, IPV1, RCV1, ROTAC and YFV), the coverage increased or plateaued from 2019 to 2022 (Figure 1).
Figure 2 presents the immunization coverage in 2022 by countries grouped by sub-region, for DTP1, DTP3 and MCV1. The median coverages for DTP1, DTP3 and MCV1 were 89% [range: 53%;99%], 82% [range: 42%; 99%] and 79% [range: 37%; 98%], respectively. Thirteen countries out of 47 (28%) in the WHO African Region achieved the global target coverage of 90% or above for DTP3 in 2022.
Figure 3 presents a country-specific comparison of immunization coverage in 2022 and in the pre-pandemic period (2019) for the 14 antigens or combinations considered in this study. The immunization coverage in 2022 compared to 2019 decreased by more than 10% in 4 countries (8%) for DTP1, in 7 countries (15%) for DTP3 and in 14 countries (25%) for MCV1. The number of countries that recorded an increase by at least 10% in immunization coverage in 2022 compared to 2019 was 3 countries (6%) for DTP1, 4 countries (8%) for DTP3 and 6 countries (13%) for MCV1. The highest proportion of countries whose immunization coverage increased by at least 10% in 2022 compared to 2019 was recorded for vaccines recently introduced in the immunization schedules, mainly HEPBB (5 countries out of 7 that reported to WHO and UNICEF, 71%), MCV2 (17 countries out of 41 reporting, 41%), ROTAC (6 countries out of 38 reporting, 16%).
Un- and Under-Immunized Children
In 2022, the number of surviving children who have never received a single dose of vaccine, known as zero-dose children, was estimated at 7.7 million (20% of surviving children), compared to 7.6 million (20% of surviving children) in 2021, 7.1 million (19% of surviving children) in 2020, and 6.2 million (17% of surviving children) in 2019. Cumulatively, the number of zero-dose children from 2019 to 2022 in the WHO African Region was estimated at 28.7 million, accounting for 19.0% of the four cohorts of surviving children (Table 1).
Figure 4 presents the geographical distribution of zero-dose children in the WHO African Region.
The 10 countries with the highest number of cumulative zero-dose children from 2019 to 2022 (Nigeria, Ethiopia, Democratic Republic of the Congo, Angola, United Republic of Tanzania, Madagascar, Mozambique, Mali, Chad, and Cameroon) accounted for 80.3% of the total zero-dose children in the region. The four most populous countries (Nigeria, Ethiopia, Democratic Republic of the Congo and United Republic of Tanzania) accounted for 57.7% of these zero-dose children. The number of surviving children who had never received a single dose of MCV was estimated at 12.1 million (31% of surviving children) in 2022, compared to 10.8 million (29% of surviving children) in 2019. Figure 5 presents the distribution of the number of children un-immunized with DTP (zero-dose children) and MCV in the 10 countries with the highest burden of zero-dose children.
Figure 6 presents the percentage of children un-immunized with DTP and MCV in 2019 and 2022. The percentage of zero-dose and un-immunized children with MCV increased in 2022 compared to 2019 in 24 countries (51%) and 27 countries (57%), respectively. Mozambique (+24%), Angola (+14%), Gabon (+12%) and Madagascar (+11%) experienced the most dramatic increase in zero-dose children (Figure 6A), while Sao Tome and Principe (+18%), Madagascar (+16%), Angola (+14%), Niger (+14%), The Gambia (+11%), Gabon (+10%) and Malawi (+10%) recorded the largest increase in children un-immunized with MCV (Figure 6B). The percentage of MCV un-immunized children in 2022 compared to 2019 dropped considerably in three countries: Chad (-15%), Liberia (-11%) and Namibia (-11%; Figure 6B).
WUENIC and Administrative Coverage Data Comparison
The comparison of the administrative and WUENIC coverage estimates in 2022 using DTP3 vaccine as a tracer showed 16 countries (47%) with a percentage of difference between -10% and 10%, 19 countries (40%) with over 10% difference (administrative coverage greater than WUENIC coverage) and six countries (13%) with below -10% difference (WUENIC coverage greater than administrative coverage; Figure 7). Botswana, Comoros, Eritrea, Mauritius, Sao Tome and Principe, and Senegal were the six countries with WUENIC estimates greater than administrative coverage.
4. Discussion
Routine immunization services have been severely disrupted by the COVID-19 pandemic in the WHO African Region, leading to a decline in immunization coverage for lifesaving vaccines, and increasing vulnerability to vaccine preventable diseases for millions of children [12,19,20]. This study, using the latest WUENIC data at the time of publication, has shown that immunization coverages for most routine vaccines in the WHO African Region, in 2022, have not yet reached pre-pandemic levels. Overall coverage with the first and third dose of DTP plateaued at 80% and 72% in 2021 and 2022, respectively, after a sharp decline in 2020. Only 13 countries out of 47 (28%) achieved the global target coverage of 90% or above with DTP3 in 2022. Worldwide, DTP1 coverage increased from 86% in 2021 to 89% in 2022 but remained below the 90% coverage achieved in 2019 [21,22]. Similarly, DTP3 coverage, increased globally from 81% in 2021 to 84% in 2022 but remained below the 2019 level (86%). Unlike the WHO African Region, DTP3 coverage has recovered to pre-pandemic levels in the South-East Asia, the Eastern Mediterranean and the Americas WHO regions [21,23]. Conflicting public health priorities, armed conflicts, fragile health systems, suboptimal community engagement, and political and economic instability, are considered as the main reasons for the slow recovery of routine immunization in the WHO African Region [24,25]. The reemergence of vaccine preventable disease outbreaks reported in several countries in the region, and particularly the ongoing diphtheria outbreak in West Africa, serve as a reminder of the increasing threat of infectious diseases due to low vaccination rates [26].
The dramatic increase in the number of zero-dose children is one of the consequences of routine vaccination disruptions that led to low vaccination coverage. In this study, the cumulative number of zero-dose children in the WHO African region from 2019 to 2022 was estimated at over 28 million, accounting for 19% of the four cohorts of surviving infants. It is well known that a high proportion of zero-dose children leads to gaps in population immunity and heightens the risk of child deaths and disease outbreaks [11,27]. One of the challenges of programmes aiming at reducing the burden of zero-dose children is to identify missed communities for targeted and tailored interventions. Many zero-dose and under-vaccinated children live in challenging settings including remote rural areas, built-up and resource-poor urban settlements and areas experiencing conflicts and crises [28]. Hogan et al. [27] stated that reaching zero-dose children is key to achieving sustainable development goals (SDG). These children face multiple deprivations related to education, water and sanitation, nutrition, and access to other health services, and account for one-third of all child deaths in low- and middle-income countries [27]. To this end, the “Big Catch-up” initiative [29], an essential immunization recovery plan for 2023 and beyond, represents a unique opportunity for catching-up children who have missed immunization, restoring immunization services to the pre-pandemic levels, and strengthening these services to achieve the targets of Immunization Agenda 2030. However, reaching zero-dose children requires context-specific interventions to overcome barriers to vaccination that are multifaceted and nuanced to each setting [30]. In addition, mechanisms need to be in place to reduce drop-out in an equitable manner so that children are not only reached once, but get all vaccines they need [31]. The quest to ensure that no child is left behind requires a tailored approach that addresses multiple and intersecting economic vulnerabilities, sociocultural barriers, and health system challenges to deliver immunization services through the primary healthcare system [32]. From 2019 to 2022, there are four cohorts of zero-dose and under-immunized children who, in 2023, are aged 12 to 59 months. Catching-up vaccination for all these zero-dose cohorts may require adjusting immunization policies and schedules with the national immunization technical advisory groups’ guidance [32] to remove restrictive target age groups or upper age limits for Expanded Programmes on Immunization. As part of such a process, local disease epidemiology, current immunization coverage levels and programme performance, health system capacity, implications on budget and logistics should be taken into consideration, as recommended by the WHO [33]. The implementation of Big Catch-up plans will result in increasing financing challenges to immunization programmes due to constrained or shrinking health budgets [34]. It is critical for governments in the African Region to ensure that processes are in place for prioritizing immunization programme investments including for catch-up activities [34]. In February 2023, African Union Heads of states committed, through the declaration “Building Momentum for Routine Immunization Recovery in Africa”, to prioritizing universal access to immunization, increasing and sustaining domestic investments in vaccines, as well as addressing bottlenecks in vaccine delivery and improving disease surveillance, with the shared goal of stopping and reversing the decline in immunization for zero-dose children [35]. In addition, on April 2023, Médecins Sans Frontières (MSF) called on Gavi, the Vaccine Alliance, and other donors to expand vaccine supply to ensure that all children up to age five are given the opportunity to catch up on their vaccination.
In 2022, the DTP1 administrative coverage was greater than estimates from WHO and UNICEF in 19 countries out of 47 (40%). This means that the WUENIC process downgraded the administrative coverage, highlighting data quality issues experienced by several countries in the WHO African Region [36,37]. Mihigo et al. [38] identified over-reporting and underestimation of target population as the main reasons for over-estimation of immunization coverages in Nigeria. In most countries, target populations are estimated based on projections using old and inaccurate population census data, without applying WHO recommendations on methods for assessing target population accuracy, such as comparing estimates with alternative sources, plotting, and analyzing target populations over time, and monitoring target population growth rates [39]. Assessing immunization data quality of routine reports in Ho municipality of Volta region in Ghana, Ziema et al. [40] found 20% overreporting of data on children vaccinated with BCG, DTP3 and MCV2. Reasons attributable to overreporting could be arithmetic errors during monthly data compilation or deliberate overreporting to achieve high coverage to avoid queries by higher staff levels [40]. Data quality issues leading to over- or under-estimation of immunization coverage highlights the need to revamping the whole immunization information systems including expanding the deployment and utilization of electronic immunization registries, leveraging from COVID-19 vaccination data management. Use of electronic immunization registries may enhance immunization programmes by improving the data collection process, easing immunization programmes’ ability to track individual children and by supporting more specific monitoring of programme inefficiencies and coverage [41]. Tools such as the “COVID-19 to Routine Immunization Information System Transferability Assessment” (CRIISTA) under development by the MOMENTUM Routine Immunization Transformation and Equity project [42] will help countries to optimize COVID-19 vaccination data investments for the future, by applying lessons learned from COVID-19 vaccination to strengthen routine immunization information systems.
Limitations
The WUENIC estimates are only made at the national level and cannot be used to guide operational decisions at sub-national levels. Estimation of un- and under-immunized children are derived using WUENIC coverage and the latest available data on population estimates from the United Nations. This may lead to over or under-estimation of the number of zero-dose and other under-immunized children [43]. The WUENIC estimates are made on a yearly basis. This does not allow for timely decisions to improve the performance of immunization services. By the time the WUENIC estimates are published, the situation for some countries may have already improved or even deteriorated. The factors associated with success or failure in achieving set global targets were not analyzed, as the WUENIC estimates do not include any qualitative information about countries’ vaccination programmes.
The interpretation of the results of this report should take these limitations into account.
5. Conclusions
The results of this study have shown that the WHO African Region has not yet recovered from the disruptions on routine immunization caused by the COVID-19 pandemic. In many countries of the region, the immunization coverage with most lifesaving vaccines is still below the 2019 levels, contributing to an increasing risk of vaccine preventable disease outbreaks. As a result of low vaccination coverage during the emergency phase of the COVID-19 pandemic, millions of children partially or fully missed routine vaccines and have seen their vulnerability to vaccine preventable diseases and risk of death heightened. It is critical for governments in the African Region to restore immunization services and catch-up with vaccination for un- and under-immunized children as a priority, in line with commitments made by African Union Heads of States in February 2023 towards building momentum for routine immunization recovery in Africa, but above all to strengthening the vaccination system for greater resilience. All technical and financial partners are called on to intensify their support to country efforts to mitigate the impact of COVID-19 on health systems in general, and on immunization services, as well as reducing the burden of zero-dose children, in particular. The discrepancies between WHO and UNICEF estimates and administrative data on immunization coverages highlight the need to invest more in data quality for routine immunization and to extend the use of electronic immunization registries.
Author Contributions
Conceptualization, F.M., C.S.W. and B.I.; methodology, F.M. and S.K.; formal analysis, F.M. and S.K.; data curation, S.K.; writing—original draft preparation, F.M. and S.K.; writing—review and editing, B.F., B.I., M.C.D.-Hs., M.G.D., J.C.S., A.B., A.A., Y.V.M., R.N. and C.S.W.; visualization, S.K. and R.N.; supervision, B.I. and C.S.W.; project administration, F.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available from the corresponding author upon request.
Acknowledgments
The authors would like to express their gratitude to Ministries of Health in the WHO African Region for submitting their reports on immunization coverage to WHO and UNICEF through Joint Reporting Forms, and to all colleagues working within the Vaccine Preventable Disease Programme at the WHO Regional Office for Africa and WHO Country Offices.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Gaythorpe, K.A.; Abbas, K.; Huber, J.; Karachaliou, A.; Thakkar, N.; Woodruff, K.; Li, X.; Echeverria-Londono, S.; Ferrari, M. Impact of COVID-19-related disruptions to measles, meningococcal A, and yellow fever vaccination in 10 countries. Elife 2021, 10, e67023. [Google Scholar] [CrossRef] [PubMed]
- Masresha, B.G.; Luce Jr, R.; Shibeshi, M.E.; Ntsama, B.; N’Diaye, A.; Chakauya, J.; Poy, A.; Mihigo, R. The performance of routine immunization in selected African countries during the first six months of the COVID-19 pandemic. The Pan African Medical Journal 2020, 37. [Google Scholar] [CrossRef]
- Saidu, Y.; Di Mattei, P.; Nchinjoh, S.C.; Edwige, N.N.; Nsah, B.; Muteh, N.J.; Ndoula, S.T.; Abdullahi, R.; Zamir, C.S.; Njoh, A.A.; et al. The Hidden Impact of the COVID-19 Pandemic on Routine Childhood Immunization Coverage in Cameroon. Vaccines 2023, 11. [Google Scholar] [CrossRef]
- Babatunde, O.A.; Olatunji, M.B.; Omotajo, O.R.; Ikwunne, O.I.; Babatunde, A.M.; Nihinlola, E.T.; Patrick, G.F.; Dairo, D.M. Impact of COVID-19 on routine immunization in Oyo State, Nigeria: trend analysis of immunization data in the pre-and post-index case period; 2019-2020. Pan African Medical Journal 2022, 41. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. About WHO: Regional Office for Africa. Available online: https://www.afro.who.int/countries (accessed on 1 February 2023).
- Impouma, B.; Mboussou, F.; Farham, B.; Wolfe, C.M.; Johnson, K.; Clary, C.; Mihigo, R.; Nsenga, N.; Talisuna, A.; Yoti, Z. The COVID-19 pandemic in the WHO African region: the first year (February 2020 to February 2021). Epidemiology & Infection 2021, 149, e263. [Google Scholar]
- Mbow, M.; Lell, B.; Jochems, S.P.; Cisse, B.; Mboup, S.; Dewals, B.G.; Jaye, A.; Dieye, A.; Yazdanbakhsh, M. COVID-19 in Africa: Dampening the storm? Science 2020, 369, 624–626. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Singh, S.K.; Sharma, L.; Dwiwedi, M.K.; Agarwal, D.; Gupta, G.K.; Dhiman, R. Magnitude and causes of routine immunization disruptions during COVID-19 pandemic in developing countries. Journal of Family Medicine and Primary Care 2021, 10, 3991. [Google Scholar] [CrossRef] [PubMed]
- Ho, L.L.; Gurung, S.; Mirza, I.; Nicolas, H.D.; Steulet, C.; Burman, A.L.; Danovaro-Holliday, M.C.; Sodha, S.V.; Kretsinger, K. Impact of the SARS-CoV-2 pandemic on vaccine-preventable disease campaigns. International Journal of Infectious Diseases 2022, 119, 201–209. [Google Scholar] [CrossRef]
- Shet, A.; Carr, K.; Danovaro-Holliday, M.C.; Sodha, S.V.; Prosperi, C.; Wunderlich, J.; Wonodi, C.; Reynolds, H.W.; Mirza, I.; Gacic-Dobo, M. Impact of the SARS-CoV-2 pandemic on routine immunisation services: evidence of disruption and recovery from 170 countries and territories. The Lancet Global Health 2022, 10, e186–e194. [Google Scholar] [CrossRef]
- Gavi, the Vaccine Alliance. Reaching zero-dose children. Available online: https://www.gavi.org/our-alliance/strategy/phase-5-2021-2025/equity-goal/zero-dose-children-missed-communities (accessed on 7 November 2023).
- World Health Organization. The big catch-up: an essential immunization recovery plan for 2023 and beyond. Available online: https://www.who.int/publications/i/item/9789240075511 (accessed on 10 October 2023).
- World Health Organization Statement on the Fifteenth Meeting of the IHR (2005) Emergency Committee on the COVID-19 Pandemic. Available online: https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations- (accessed on 7 September 2023).
- World Health Organization. WHO/UNICEF Joint Reporting Process. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/who-unicef-joint-reporting-process (accessed on 22 October 2023).
- Burton, A.; Monasch, R.; Lautenbach, B.; Gacic-Dobo, M.; Neill, M.; Karimov, R.; Wolfson, L.; Jones, G.; Birmingham, M. WHO and UNICEF estimates of national infant immunization coverage: methods and processes. Bulletin of the World Health Organization 2009, 87, 535–541. [Google Scholar] [CrossRef]
- Burton, A.; Kowalski, R.; Gacic-Dobo, M.; Karimov, R.; Brown, D. A Formal Representation of the WHO and UNICEF Estimates of National Immunization Coverage: A Computational Logic Approach. PLOS ONE 2012, 7, e47806. [Google Scholar] [CrossRef] [PubMed]
- United Nations. World Population Prospects 2022. Available online: https://population.un.org/wpp/ (accessed on 3 October 2023).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Dalton, M.; Sanderson, B.; Robinson, L.J.; Homer, C.S.E.; Pomat, W.; Danchin, M.; Vaccher, S. Impact of COVID-19 on routine childhood immunisations in low- and middle-income countries: A scoping review. PLOS Global Public Health 2023, 3, e0002268. [Google Scholar] [CrossRef] [PubMed]
- Ota, M.O.C.; Badur, S.; Romano-Mazzotti, L.; Friedland, L.R. Impact of COVID-19 pandemic on routine immunization. Annals of Medicine 2021, 53, 2286–2297. [Google Scholar] [CrossRef] [PubMed]
- Kaur, G. Routine Vaccination Coverage—Worldwide, 2022. MMWR. Morbidity and Mortality Weekly Report 2023, 72. [Google Scholar] [CrossRef]
- World Health Organization. Immunization coverage. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 6 November 2023).
- World Health Organization. WHO South-East Asia Region lauds countries for routine immunization coverage scale-up, says accelerated efforts must continue. Available online: https://www.who.int/southeastasia/news/detail/18-07-2023-who-south-east-asia-region-lauds-countries-for-routine-immunization-coverage-scale-up--says-accelerated-efforts-must-continue. (accessed on 6 November 2023).
- Borba, R.C.; Vidal, V.M.; Moreira, L.O. The re-emergency and persistence of vaccine preventable diseases. Anais da Academia Brasileira de Ciências 2015, 87, 1311–1322. [Google Scholar] [CrossRef] [PubMed]
- IntraAction. Global rise in vaccine-preventable diseases highlights urgent actions needed to save lives and alleviate future suffering. Available online: https://www.interaction.org/blog/global-rise-in-vaccine-preventable-diseases-highlights-urgent-actions-needed-to-save-lives-and-alleviate-future-suffering/ (accessed on 6 November 2023).
- Adegboye, O.A.; Alele, F.O.; Pak, A.; Castellanos, M.E.; Abdullahi, M.A.S.; Okeke, M.I.; Emeto, T.I.; McBryde, E.S. A resurgence and re-emergence of diphtheria in Nigeria, 2023. Therapeutic Advances in Infection 2023, 10, 20499361231161936. [Google Scholar] [CrossRef] [PubMed]
- Hogan, D.; Gupta, A. Why Reaching Zero-Dose Children Holds the Key to Achieving the Sustainable Development Goals. Vaccines 2023, 11. [Google Scholar] [CrossRef]
- Gavi, the Vaccine Alliance. The Zero-Dose Child: Explained. Available online: https://www.gavi.org/vaccineswork/zero-dose-child-explained (accessed on 7 November 2023).
- O’Brien, K.L.; Lemango, E. The big catch-up in immunisation coverage after the COVID-19 pandemic: progress and challenges to achieving equitable recovery. The Lancet 2023, 402, 510–512. [Google Scholar] [CrossRef]
- Ingle, E.A.; Shrestha, P.; Seth, A.; Lalika, M.S.; Azie, J.I.; Patel, R.C. Interventions to Vaccinate Zero-Dose Children: A Narrative Review and Synthesis. Viruses 2023, 15. [Google Scholar] [CrossRef]
- Kirkby, K.; Bergen, N.; Schlotheuber, A.; Sodha, S.V.; Danovaro-Holliday, M.C.; Hosseinpoor, A.R. Subnational Inequalities in Diphtheria–Tetanus–Pertussis Immunization in 24 Countries in the African Region. Bulletin of the World Health Organization 2021, 99, 627. [Google Scholar] [CrossRef]
- IQVIA Middle-East and Africa. Removing the immunization barriers for zero-dose children: How to make it work. Available online: https://www.iqvia.com/locations/middle-east-and-africa/blogs/2023/02/removing-immunization-barriers-for-zero-dose-children-how-to-make-it-work. (accessed on 7 November 2023).
- World Health Organization Leave no one behind: guidance for planning and implementing catch-up vaccination. Available online: https://www.who.int/publications/i/item/9789240016514 (accessed on 10 October 2023).
- World Bank blogs. How to finance “The Big Catch-Up,” allowing more children and communities to be protected from vaccine-preventable diseases. Available online: https://blogs.worldbank.org/health/how-finance-big-catch-allowing-more-children-and-communities-be-protected-vaccine (accessed on 8 November 2023).
- World Health Organization. Regional Office for Africa. African leaders call for urgent action to revitalize routine immunization. Available online: https://www.afro.who.int/news/african-leaders-call-urgent-action-revitalize-routine-immunization (accessed on 8 November 2023).
- Rau, C.; Lüdecke, D.; Dumolard, L.B.; Grevendonk, J.; Wiernik, B.M.; Kobbe, R.; Gacic-Dobo, M.; Danovaro-Holliday, M.C. Data quality of reported child immunization coverage in 194 countries between 2000 and 2019. PLOS Global Public Health 2022, 2, e0000140. [Google Scholar] [CrossRef] [PubMed]
- Harrison, K.; Rahimi, N.; Danovaro-Holliday, M.C. Factors Limiting Data Quality in the Expanded Programme on Immunization in Low and Middle-Income Countries: A Scoping Review. Vaccine 2020, 38, 4652–4663. [Google Scholar] [CrossRef] [PubMed]
- Mihigo, R.; Okeibunor, J.; Anya, B.; Mkanda, P.; Zawaira, F. Challenges of immunization in the African Region. The Pan African Medical Journal 2017, 27. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Assessing and improving the accuracy of target population estimates for immunization coverage. Available online: https://www.who.int/publications/m/item/assessing-and-improving-the-accuracy-of-target-population-estimates-for-immunization-coverage (accessed on 2 November 2023).
- Ziema, S.A.; Asem, L. Assessment of immunization data quality of routine reports in Ho municipality of Volta region, Ghana. BMC Health Services Research 2020, 20, 1013. [Google Scholar] [CrossRef]
- VillageReach. Lessons Learned from a Landscape Analysis of EIR Implementations in Low- and Middle-Income Coun-tries. Available online: https://www.villagereach.org/wp-content/uploads/2020/06/2020-EIR-Landscape-Analysis.pdf (accessed on 15 November 2023).
- Momentum. Optimizing COVID-19 Vaccination Data Investments for the Future: The COVID-19 to Routine Immunization Information System Transferability Assessment. Available online: https://usaidmomentum.org/webinar-optimizing-covid-19-vaccination-data-investments-for-the-future/ (accessed on 14 September 2023).
- Danovaro-Holliday, M.C.; Gacic-Dobo, M.; Diallo, M.S.; Murphy, P.; Brown, D.W. Compliance of WHO and UNICEF Estimates of National Immunization Coverage (WUENIC) with Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) Criteria. Gates Open Research 2021, 5. [Google Scholar] [CrossRef]
Figure 1.
Coverage with BCG, DTP1, DTP3, HEPB, HEPBB, HIB3, IPV1, POL3, MCV1, MCV2, PCV3, RCV1, ROTAC and YFV over time in the African region. Abbreviations: BCG: Bacille Calmette-Guérin vaccine; DTP1: first dose of diphtheria-tetanus-pertussis containing vaccine; DTP3: third dose of diphtheria-tetanus-pertussis containing vaccine; HEPBB: hepatitis B vaccine birth dose; HEPB3: third dose of hepatitis B vaccine; POL3: third dose of oral poliovirus vaccine; IPV1: first dose of inactivated poliovirus containing vaccine; MCV1: first dose of measles-containing vaccine; MCV2: second dose of measles-containing vaccine; HIB3: third dose of Haemophilus influenzae type b vaccine; PCV3: third dose of pneumococcal conjugate vaccine; RCV1: First dose of rubella containing vaccine; ROTAC: final dose of rotavirus vaccine; YFV: yellow fever vaccine.
Figure 1.
Coverage with BCG, DTP1, DTP3, HEPB, HEPBB, HIB3, IPV1, POL3, MCV1, MCV2, PCV3, RCV1, ROTAC and YFV over time in the African region. Abbreviations: BCG: Bacille Calmette-Guérin vaccine; DTP1: first dose of diphtheria-tetanus-pertussis containing vaccine; DTP3: third dose of diphtheria-tetanus-pertussis containing vaccine; HEPBB: hepatitis B vaccine birth dose; HEPB3: third dose of hepatitis B vaccine; POL3: third dose of oral poliovirus vaccine; IPV1: first dose of inactivated poliovirus containing vaccine; MCV1: first dose of measles-containing vaccine; MCV2: second dose of measles-containing vaccine; HIB3: third dose of Haemophilus influenzae type b vaccine; PCV3: third dose of pneumococcal conjugate vaccine; RCV1: First dose of rubella containing vaccine; ROTAC: final dose of rotavirus vaccine; YFV: yellow fever vaccine.
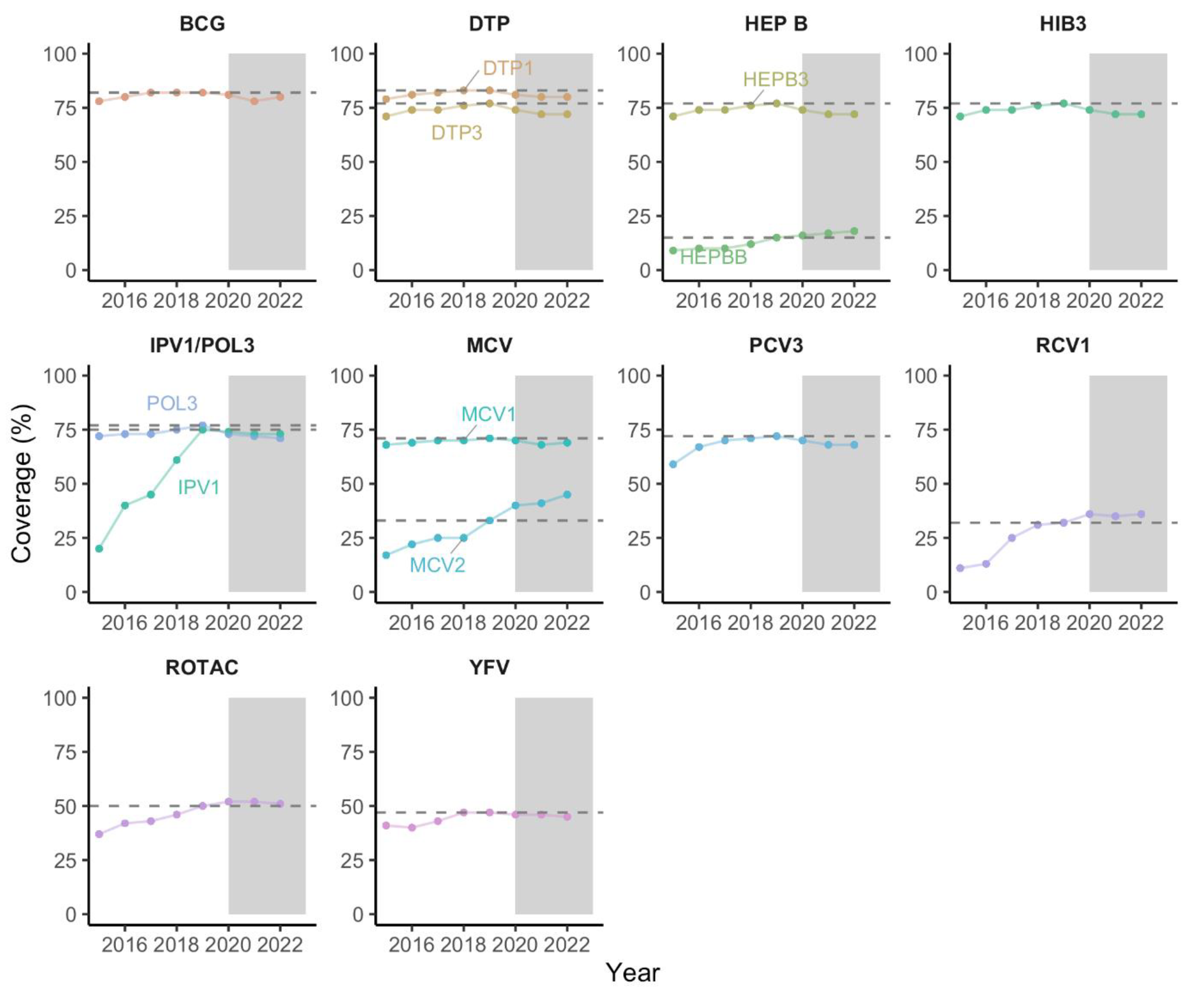
Figure 2.
DTP1, DTP3 and MCV1 coverage by country in 2022 in the WHO African region. Abbreviations: DTP1: first dose of diphtheria-tetanus-pertussis containing vaccine; DTP3: third dose of diphtheria-tetanus-pertussis containing vaccine. MCV1: first dose of measles-containing vaccine; CAR: Central African Republic; DRC: Democratic Republic of Congo; STP: Sao Tome and Principe; Eq. Guinea: Equatorial Guinea.
Figure 2.
DTP1, DTP3 and MCV1 coverage by country in 2022 in the WHO African region. Abbreviations: DTP1: first dose of diphtheria-tetanus-pertussis containing vaccine; DTP3: third dose of diphtheria-tetanus-pertussis containing vaccine. MCV1: first dose of measles-containing vaccine; CAR: Central African Republic; DRC: Democratic Republic of Congo; STP: Sao Tome and Principe; Eq. Guinea: Equatorial Guinea.
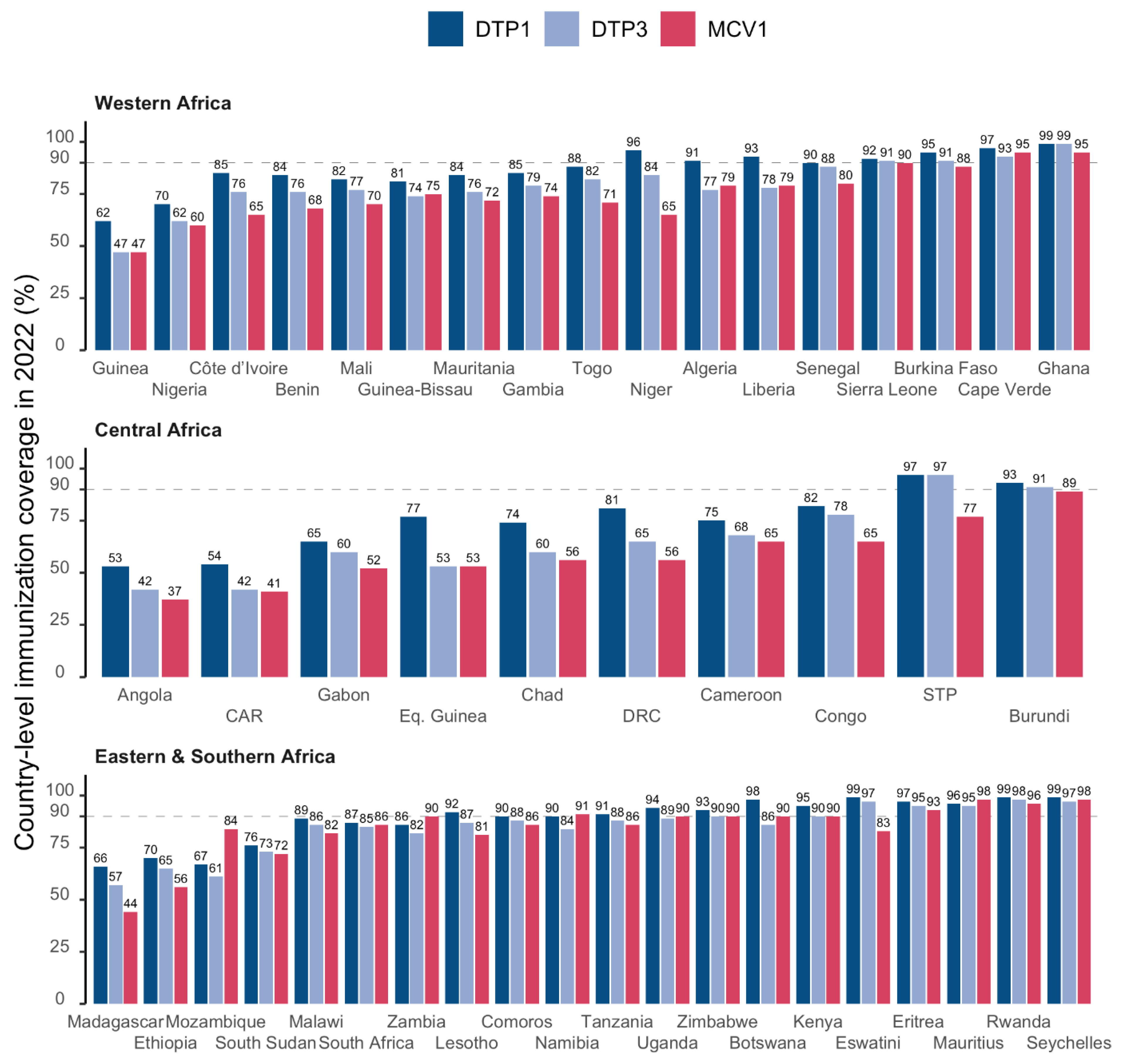
Figure 3.
Percent change in immunization compared to 2019 in the 47 countries o of the WHO African region. Abbreviations: CAR: Central African Republic; DRC: Democratic Republic of Congo; STP: Sao Tome and Principe; Eq. Guinea: Equatorial Guinea; NA: Data not available. BCG: Bacille Calmette-Guérin vaccine; DTP1: first dose of diphtheria-tetanus-pertussis containing vaccine; DTP3: third dose of diphtheria-tetanus-pertussis containing vaccine; HEPBB: hepatitis B vaccine birth dose; HEPB3: third dose of hepatitis B vaccine; POL3: third dose of oral poliovirus vaccine; IPV1: first dose of inactivated poliovirus containing vaccine; MCV1: first dose of measles-containing vaccine; MCV2: second dose of measles-containing vaccine; HIB3: third dose of Haemophilus influenzae type b vaccine; PCV3: third dose of pneumococcal conjugate vaccine; RCV1: First dose of rubella containing vaccine; ROTAC: final dose of rotavirus vaccine; YFV: yellow fever vaccine.
Figure 3.
Percent change in immunization compared to 2019 in the 47 countries o of the WHO African region. Abbreviations: CAR: Central African Republic; DRC: Democratic Republic of Congo; STP: Sao Tome and Principe; Eq. Guinea: Equatorial Guinea; NA: Data not available. BCG: Bacille Calmette-Guérin vaccine; DTP1: first dose of diphtheria-tetanus-pertussis containing vaccine; DTP3: third dose of diphtheria-tetanus-pertussis containing vaccine; HEPBB: hepatitis B vaccine birth dose; HEPB3: third dose of hepatitis B vaccine; POL3: third dose of oral poliovirus vaccine; IPV1: first dose of inactivated poliovirus containing vaccine; MCV1: first dose of measles-containing vaccine; MCV2: second dose of measles-containing vaccine; HIB3: third dose of Haemophilus influenzae type b vaccine; PCV3: third dose of pneumococcal conjugate vaccine; RCV1: First dose of rubella containing vaccine; ROTAC: final dose of rotavirus vaccine; YFV: yellow fever vaccine.
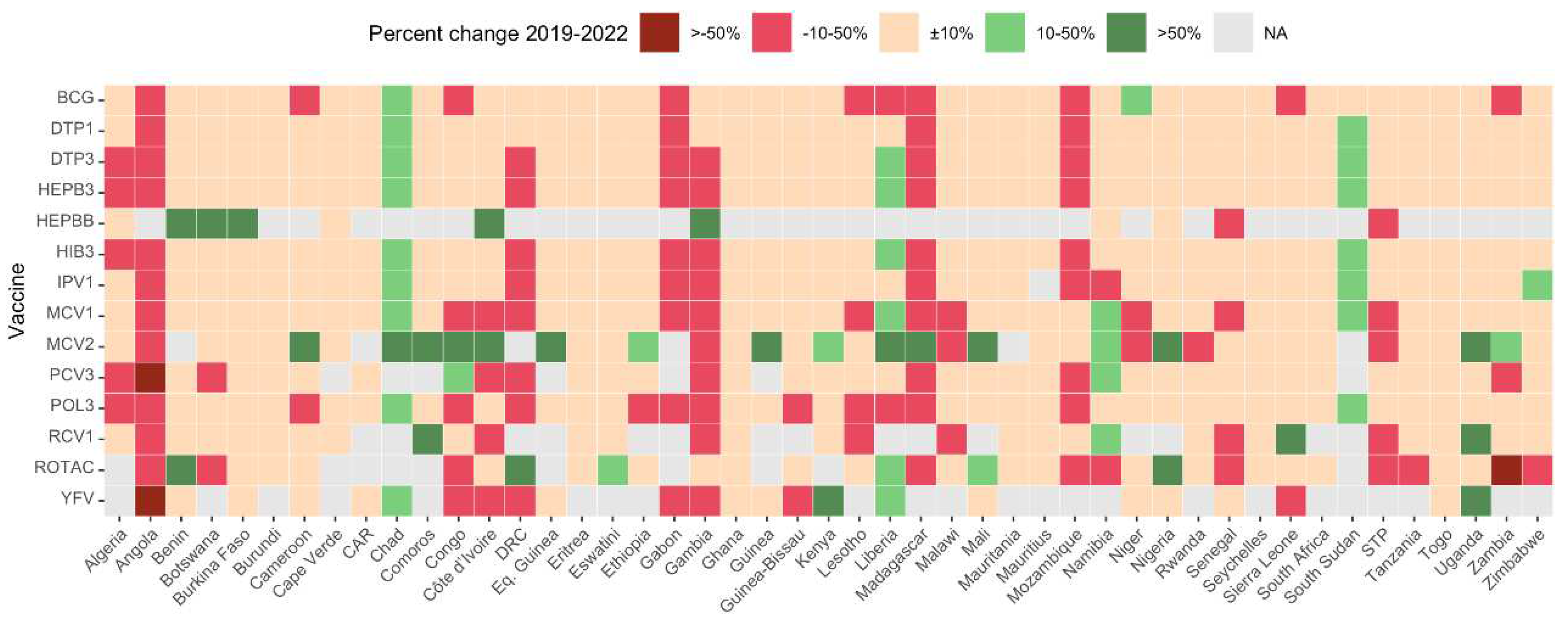
Figure 4.
Geographical distribution of cumulative number of zero-dose children in the WHO African Region during the pandemic period.
Figure 4.
Geographical distribution of cumulative number of zero-dose children in the WHO African Region during the pandemic period.
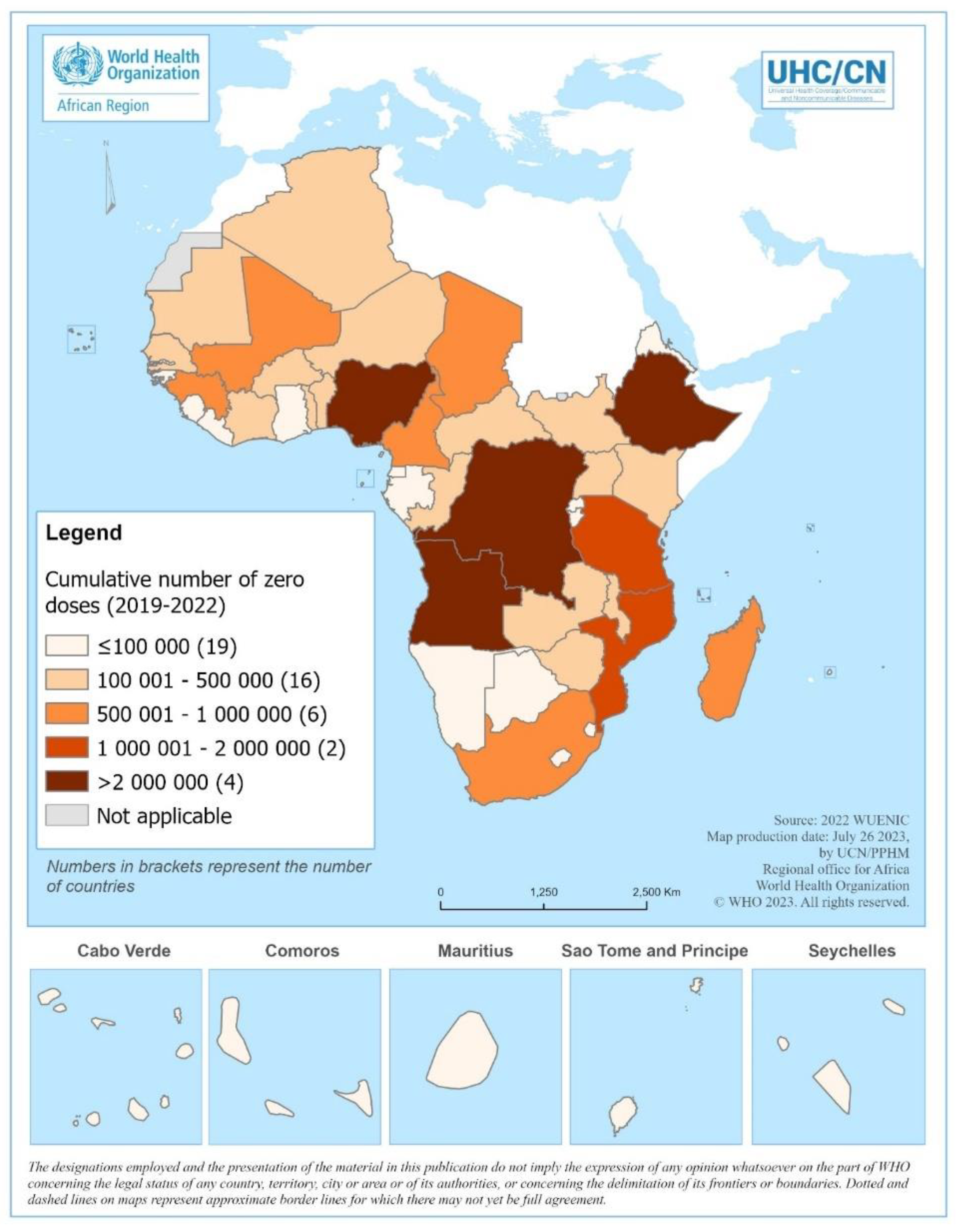
Figure 5.
Cumulative number of unvaccinated children from 2019 to 2022 for the diphtheria-tetanus-pertussis (DTP) containing vaccine and measles-containing vaccine (MCV) in the 10 countries of the WHO African Region with the highest burden of zero-dose children.
Figure 5.
Cumulative number of unvaccinated children from 2019 to 2022 for the diphtheria-tetanus-pertussis (DTP) containing vaccine and measles-containing vaccine (MCV) in the 10 countries of the WHO African Region with the highest burden of zero-dose children.
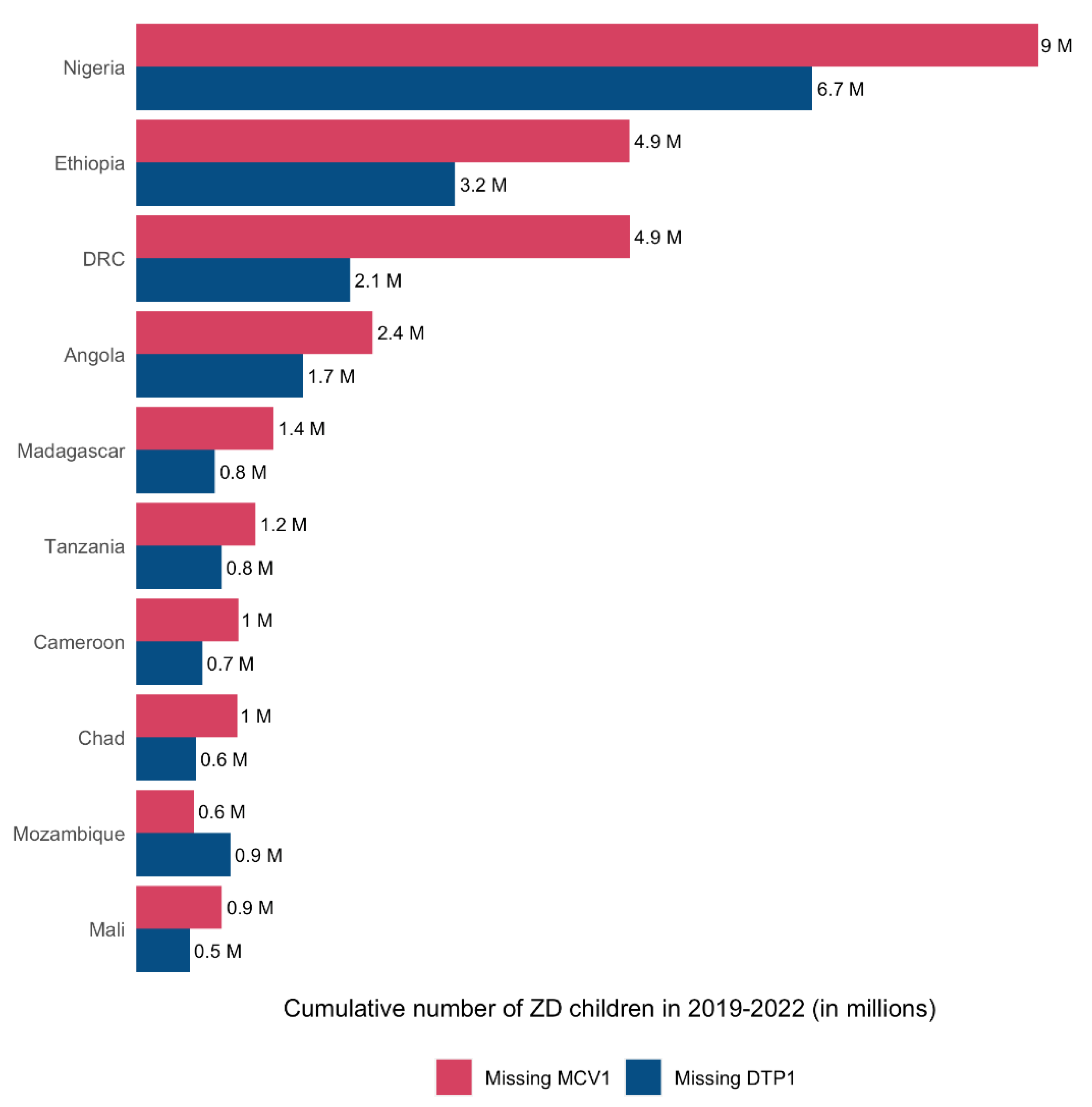
Figure 6.
(a) Percentage of un-immunized children the measles-containing vaccine (MCV) in 2019 and 2022 by country and (b) percentage of zero-dose children (i.e., children not immunized with any DTP vaccine) in 2019 and 2022 by country in the WHO African region. Abbreviations: CAR: Central African Republic; DRC: Democratic Republic of Congo; STP: Sao Tome and Principe; Eq. Guinea: Equatorial Guinea.
Figure 6.
(a) Percentage of un-immunized children the measles-containing vaccine (MCV) in 2019 and 2022 by country and (b) percentage of zero-dose children (i.e., children not immunized with any DTP vaccine) in 2019 and 2022 by country in the WHO African region. Abbreviations: CAR: Central African Republic; DRC: Democratic Republic of Congo; STP: Sao Tome and Principe; Eq. Guinea: Equatorial Guinea.
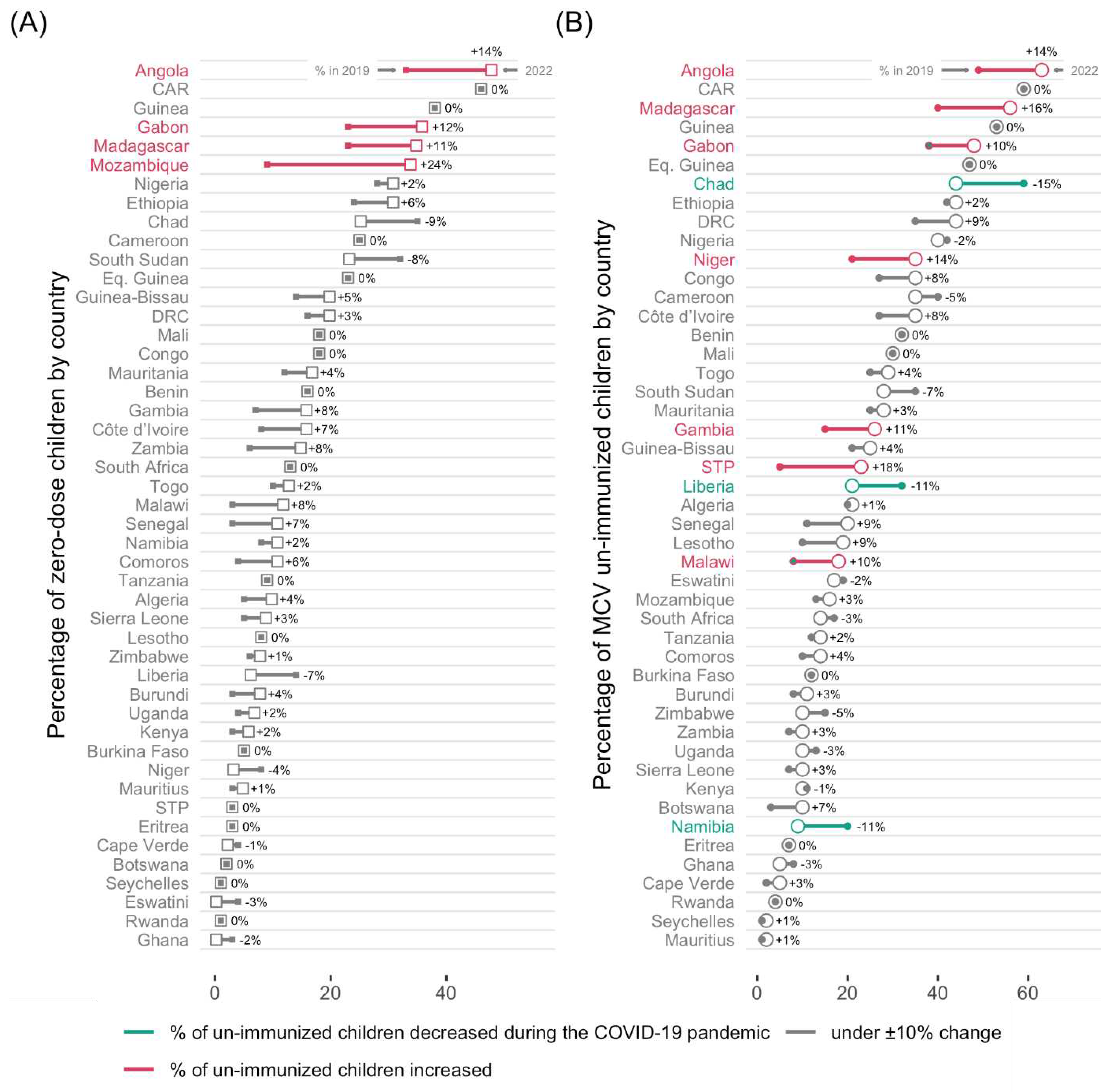
Figure 7.
Percentage of change in the third dose diphtheria-tetanus-pertussis containing vaccine (DTP3) coverage between WUENIC and administrative reports in 2022 in 47 countries of the WHO African region. Abbreviations: CAR: Central African Republic; DRC: Democratic Republic of Congo; STP: Sao Tome and Principe; Eq. Guinea: Equatorial Guinea; MZ: Mozambique.
Figure 7.
Percentage of change in the third dose diphtheria-tetanus-pertussis containing vaccine (DTP3) coverage between WUENIC and administrative reports in 2022 in 47 countries of the WHO African region. Abbreviations: CAR: Central African Republic; DRC: Democratic Republic of Congo; STP: Sao Tome and Principe; Eq. Guinea: Equatorial Guinea; MZ: Mozambique.
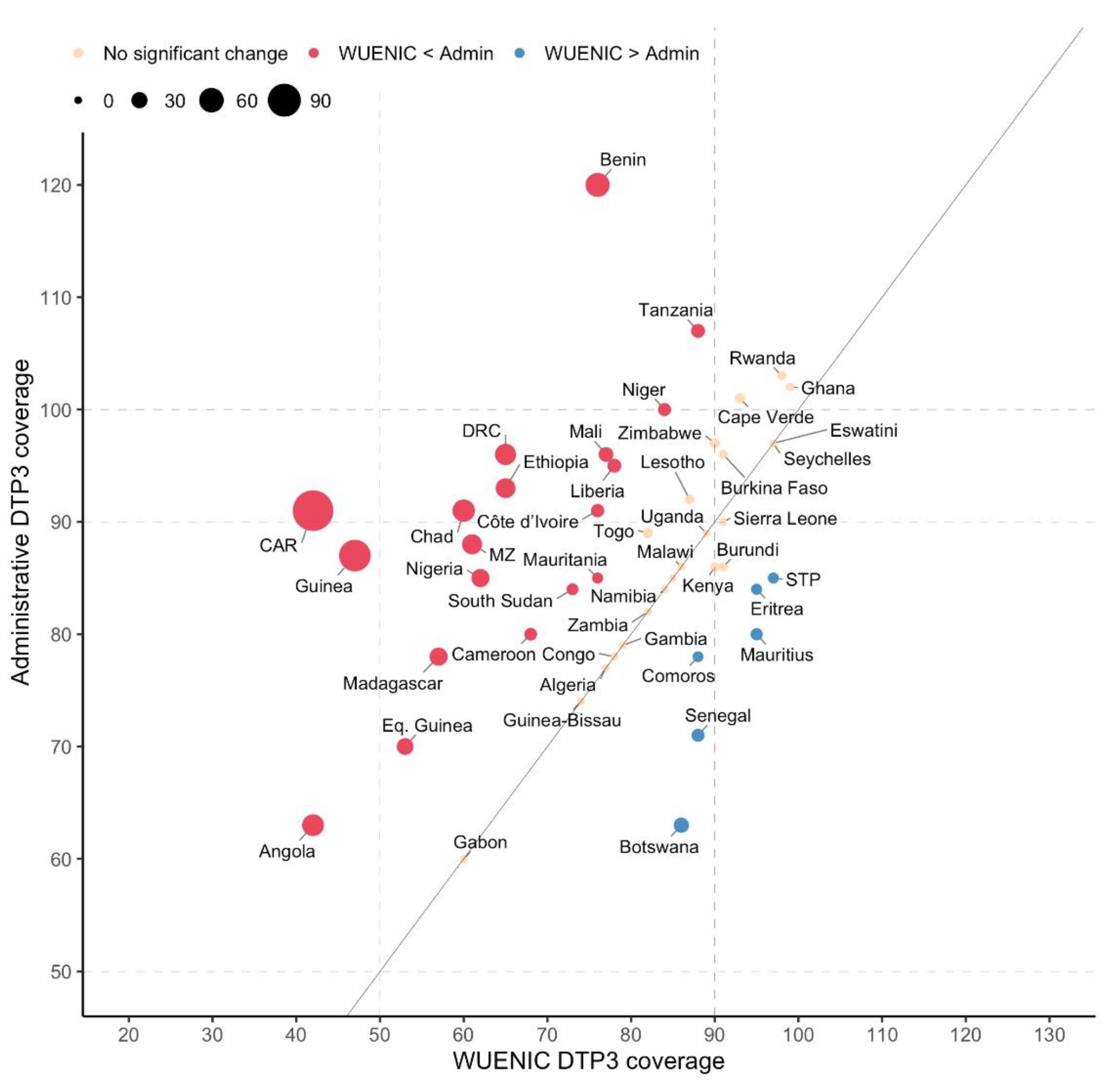

Table 1.
Estimated number of zero-dose children in the WHO African Region from 2019 to 2022.
| Year | # Surviving Children | Estimated Number of Vaccinated with DTP1 | Estimated Number of Zero-Dose Children | % Zero-Dose Children |
|---|---|---|---|---|
| 2019 | 36 995 277 | 30 763 363 | 6 231 914 | 16.8 |
| 2020 | 37 521 132 | 30 463 727 | 7 057 405 | 18.8 |
| 2021 | 38 080 516 | 30 439 539 | 7 640 977 | 20.1 |
| 2022 | 38 567 250 | 30 791 574 | 7 775 676 | 20.2 |
| Cumulative 2019-2022 | 151 164 175 | 122 458 203 | 28 705 972 | 19.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



