
Submitted:
16 November 2023
Posted:
17 November 2023
You are already at the latest version
Abstract
Coronary microvascular dysfunction (CMD) is a clinical entity linked with various risk factors that significantly affect cardiac morbidity and mortality. Hypertension, one of the most important, causes both functional and structural alterations in the microvasculature, promoting the occurrence and progression of microvascular angina. Endothelial dysfunction and capillary rarefaction play the most significant role in the development of CMD among patients with hypertension. CMD is also related to several hypertension-related morphological and functional changes in the myocardium in the subclinical and early clinical stages, including left ventricular hypertrophy, interstitial myocardial fibrosis, and diastolic dysfunction. This indicates the fact that CMD, especially if associated with hypertension, is a subclinical marker of end-organ damage and heart failure, particularly the one with preserved ejection fraction. This is why it is important to search for microvascular angina in every patient with hypertension and chest pain not associated with obstructive coronary artery disease. Several highly sensitive and specific non-invasive and invasive diagnostic modalities have been developed to evaluate the presence and severity of CMD, but also to investigate additional complications that can affect further prognosis, especially among those with hypertensive heart disease. Although various pharmacological and interventional treatments demonstrated certain clinical effects, integrated diagnostic and therapeutic algorithms are necessary to reduce the burden of this emerging condition.
Keywords:
coronary microvascular dysfunction
; hypertension
; hypertensive heart disease
; myocardial fibrosis
; heart failure
1. Introduction
Hypertension is a well-established risk factor for the development of coronary microvascular dysfunction (CMD) [1]. The constant high pressure within the larger arteries can lead to damage and remodeling of the smallest arteries and arterioles in the microcirculation, capillaries, and venules, affecting their ability to regulate blood flow [2]. This leads to structural and functional remodeling of the coronary microcirculation in which endothelial dysfunction is one of the most important pathogenetic mechanisms [3]. The endothelium plays a crucial role in regulating blood vessel tone and controlling blood flow. In hypertensive individuals, endothelial dysfunction significantly contributes to the development of CMD, which progressively leads to increased resistance in coronary microcirculation and limited blood flow, causing a reduced oxygen supply to the myocardium [4]. This is why the finding of myocardial ischemia as a result of coronary microvascular dysfunction is relatively common in patients with hypertension, especially in patients with hypertensive heart disease. Many additional risk factors also contribute to the development of CMD in hypertensive patients including metabolic syndrome, diabetes mellitus, hyperlipidemia, smoking, and others [5, 6, 7]. As the development of hypertensive heart disease progresses, left ventricular hypertrophy is more pronounced, consequently leading to more severe impairment of coronary microcirculation. These changes, accompanied by myocardial fibrosis, are leading to an increased risk of heart failure with both preserved (HFpEF) and reduced ejection fraction (HFrEF) [8, 9]. This is why coronary microvascular dysfunction significantly affects morbidity and mortality of the patients, demanding more purposeful diagnostic and therapeutic algorithms.
The purpose of this narrative review is to describe the relationship between coronary microvascular dysfunction and systemic hypertension, its pathogenetic mechanisms, characteristics, and potential role in the development of adverse cardiovascular events, especially heart failure with preserved ejection fraction (HFpEF).
2. Pathogenetic Mechanisms of Coronary Microvascular Dysfunction
Coronary microcirculation consists of prearterioles, arterioles, and capillaries. The mechanisms involved in CMD can be structural, functional, or a combination of both [10]. The main pathogenetic mechanisms of coronary microvascular dysfunction in patients with hypertension are still insufficiently researched. Until now, it has been postulated that the pathogenetic basis for the development of CMD is a variety of mechanisms, including microvascular spasm, endothelial dysfunction, sympathetic over-activity, influence of female hormones, certain psychological disorders, and others [11, 12]. These mechanisms are more prone to cause CMD in susceptible patients with hypertension, hyperlipidemia, obesity, or diabetes mellitus [13]. In patients with hypertension, the development of left ventricular hypertrophy and subsequent development of myocardial fibrosis and diastolic dysfunction, are important mechanisms of CMD due to several functional and anatomical changes in the microcirculation [14]. Maladaptive mechanisms in hypertension, perivascular fibrosis, thickening of small vessel walls, and their rarefaction, are responsible for increased microvascular resistance and inappropriate blood flow distribution [15]. Also, several functional mechanisms are described as a cause of CMD in patients with hypertension including reduced nitric oxide availability as the most important one [16, 17]. It is shown that chronic RAS overactivity, nicotinamide adenine dinucleotide phosphate oxidase, cyclooxygenase, xanthine oxidase, and uncoupled endothelial NO synthase as sources of reactive oxygen species are the main causes of NO deficiency [18]. Also, adrenergic activation and prolonged vasoconstriction can also lead to microvascular remodeling and rarefaction, causing ischemia and clinically manifested angina [19, 20]. It is also important to note that certain studies registered these microvascular changes even in patients without elevated blood pressure, suggesting that microvascular dysfunction and remodeling can precede the onset and development of hypertension [21, 22]. However, this cause-effect relationship needs further investigation.
2.1. Microvascular Angina and Endothelial Dysfunction
Endothelial dysfunction is bi-directionally related to systemic hypertension. It is shown that endothelium controls vascular smooth muscle tone in response to various agents, as well as participating in the pathogenesis of hypertension by producing different mediators with systemic effects [23]. In patients with hypertension, endothelial dysfunction is mainly characterized by impaired nitric oxide synthesis and availability, as well as prostacyclin (PGI2), and endothelium-derived hyperpolarizing factors (EDHF) deficiency [24]. On the other side, as a response to reactive oxygen species, increased production of endothelium-derived vasoconstrictors (mainly endothelin-1 and angiotensin-converting enzyme) was observed [25]. This is subsequently associated with the development of vascular inflammation, vascular remodeling, and atherosclerosis. As a result, vasoconstrictive, pro-inflammatory, and pro-thrombotic mediators are causing increased vasoconstrictive microvascular reactivity [26]. This process is leading to both functional and structural changes in the microvasculature and the development of microvascular dysfunction. It is important to emphasize that coronary microvascular dysfunction in patients with hypertension is not a result of hypertension solely, but a multifactorial disease with a significant impact on cardiovascular morbidity and mortality.
3. Additional Risk Factors
3.1. Sex-Related Differences in Patients with Coronary Microvascular Dysfunction and Hypertension
Coronary microvascular dysfunction is more prevalent in women than in men [27]. Early works on estimating the sex-related differences in coronary microcirculation revealed lower CFR values in women, predominantly due to differences in resting coronary flow [28]. This is also in relation to different mechanisms involved with autonomic regulation and response to oxidative stress, adenosine, endothelin-1, and angiotensin II [29]. It is also notable that women have smaller vessel size than men which can contribute to lower CFR values [30]. Studies on cardiac magnetic resonance revealed notable differences whereas women in comparison with men had less or no associations in the development of CMD with traditional risk factors, including hyperlipidemia, diabetes, smoking, and obesity [31]. This can mainly be the effect of ovarian hormone deficiency, as microvascular angina and estrogen deficiency in hypertensive women have demonstrated an association [32]. In the subgroup of both premenopausal and postmenopausal women with hypertension, ovarian dysfunction, and consequent estrogen deficiency played a role in the pathogenesis of CMD [33].
3.2. Metabolic Syndrome
Metabolic syndrome includes a cluster of conditions such as central obesity, dyslipidemia, high blood pressure, and impaired fasting glucose, all related to an increased cardiovascular risk [34]. Several studies demonstrated a correlation of different variables with the presence of microvascular dysfunction in these patients, including age, sex, pulse pressure, fasting glucose, hemoglobin A1c (HbA1c), total cholesterol, low-density lipoprotein (LDL)-cholesterol, eGFR, and albuminuria [35]. In patients with hypertension, it is shown that those patients with metabolic syndrome had a more severe form of coronary microvascular dysfunction than those without metabolic syndrome. Sucato et al. demonstrated that these patients had worse coronary perfusion than patients with diabetes mellitus [36].
3.3. Diabetes Mellitus
The key mechanisms of coronary microvascular dysfunction in patients with diabetes are impaired coronary arteriole vasomotion, including impaired endothelial-mediated vasodilation, hypoxia-induced vasodilation, and myogenic response [37]. It is shown that hyperglycemia and insulin resistance play central roles in the development of CMD by leading to oxidative stress, inflammatory activation, and endothelial dysfunction [38]. In the later stage of diabetes, structural changes occur. Thickening of the capillary basement membrane and of the arteriole wall results in luminal narrowing, but also in perivascular fibrosis with focal constriction, and capillary rarefaction. These mechanisms lead to increased coronary microvascular resistance and reduced coronary flow reserve and can cause myocardial ischemia [39]. Coronary microvascular dysfunction is common in patients with diabetes and can be present with or without the finding of significant epicardial coronary artery disease. It is shown, by certain studies, that more than 70% of patients with type 2 diabetes mellitus have CMD, which can seriously affect future cardiovascular events and prognosis, especially in those with acute myocardial infarction and heart failure [40].
3.4. Hypercholesterolemia
Numerous studies have shown that hypercholesterolemia leads to an inflammatory response within the microvasculature, decreased availability of nitric oxide, and increased production of reactive oxygen species (ROS) [41, 42]. Endothelial dysfunction and capillary rarefaction are the two most important mechanisms, leading to severe microvascular impairment in different organs, provoking glomerulopathy-induced kidney dysfunction and hypertension, reduction in coronary flow reserve leading to coronary microvascular dysfunction, and hepatic dysfunction as non-alcoholic fatty liver disease [43].
3.5. Obstructive Sleep Apnea
Obstructive sleep apnea is a condition linked to an increased cardiovascular morbidity and mortality [44]. Repetitive episodes of hypoxemia are leading to the excessive production of reactive oxygen species, development of low-grade inflammation and endothelial dysfunction. It is shown that patients with moderate to severe obstructive sleep apnea have lower values of CFR [45]. However, the exact influence of OSA on the development and progression of coronary microvascular dysfunction is hard to observe, as these patients usually have several other risk factors related to CMD, including hypertension, diabetes mellitus, obesity, hyperlipidemia.
3.6. Smoking
Cigarette smoke is known as an exertion factor with the most detrimental effects on endothelium, especially coronary endothelial system [46]. Various toxic components can cause severe endothelial damage, reduce hyperaemic coronary blood flow velocity, and provoke the development of microvascular dysfunction. Regarding the presence of CMD, Gullu et al. demonstrated that smokers without obstructive epicardial coronary disease had significantly lower values of coronary flow velocity reserve (CFVR) in comparison to the control group [47]. On the other hand, even in patients with epicardial coronary artery disease, smoking was associated with impaired invasively-derived indices of coronary microvascular dysfunction, which can additionally contribute to a worse prognosis [48].
4. Diagnostics of Coronary Microvascular Dysfunction in Patients with Hypertension
The diagnostic algorithm in patients with suspected CMD starts with the exclusion of significant epicardial coronary artery disease. Although CMD can be present in patients with obstructive CAD, the presence of CMD in the absence of obstructive CAD is extremely important to diagnose, especially in patients with additional risk factors for the development of adverse cardiovascular events, primarily heart failure [49]. In patients with microvascular angina, non-invasive diagnostic imaging modalities, primarily echocardiography, and CMR, are important in the evaluation of alternative causes of chest pain, including structural and inflammatory conditions [50]. Patients with a negative coronary angiogram, a positive stress test on myocardial ischemia, and additional risk factors for the development of CMD (especially those with hypertensive heart disease), should be considered for non-invasive and invasive investigation of coronary microvascular dysfunction.
4.1. Non-Invasive Diagnostics
4.1.1. Echocardiography
Conventional echocardiographic stress tests have limited utility in the diagnosis of CMD, as significant inter-observer variability is present in cases with low to moderate ischemia burden, resulting in hypokinesia [51]. The use of echocardiography in detecting coronary microvascular dysfunction mainly relies on myocardial contrast echocardography and the estimation of myocardial blood flow or coronary flow velocity reserve (CFVR), using pulsed-wave Doppler sampling of the proximal left anterior descending coronary artery [52]. Nowadays, CFVR has higher diagnostic accuracy and better correlation with intracoronary Doppler wire-based techniques, especially in patients with HFpEF, as demonstrated in the PROMIS-HFpEF trial [53]. Numerous studies investigated the prognostic significance of CFVR in patients with hypertension, demonstrating an impairment in microvascular vasodilatation capacity even in the early stages of the disease [54, 55]. The study by Volz et al. showed that CFVR was significantly lower in patients with resistant hypertension as compared to individuals with non-resistant hypertension, indicating a more severe impairment of coronary microvascular function that could account for the increased risk of adverse outcomes [54]. The main disadvantages of MBF assessment of CFVR are the presence of artifacts and high inter-observer variability, especially in obese patients and patients with lung disease. However, these methods can be helpful as inexpensive methods in the initial assessment of patients with CMD.
4.1.2. Computerized Tomographic Angiography (CTA)
Although the role of CT coronary angiography is to primarily exclude the existence of significant epicardial coronary artery disease, recent technical and software advancements provided the possibility to follow the first pass of contrast through the myocardium at frequent intervals and estimate the absolute myocardial flow. The estimation of myocardial perfusion can be compared in different layers of the myocardium, providing evidence of reduced subendocardial perfusion in patients with CMD [56]. Novel techniques of combining CTA-derived FFR and estimation of myocardial perfusion can provide an accurate anatomical and functional assessment of both the myocardium and the coronary circulation within one examination, which can be significant especially in patients with hypertensive heart disease [57]. Studies that investigated myocardial perfusion and coronary volume to left ventricular mass ratio showed promising results in diagnosing patients with CMD [58]. However, the results in patients with hypertension are controversial. The study by van Rosendal and colleagues demonstrated that patients with hypertension and increased LV mass did not have reduced coronary vascular volume that can be associated with the presence of abnormal perfusion reserve [59]. This can also be a result of predominantly functional impairment of coronary microcirculation, as well as the lack of the estimation of coronary vasodilator reserve.
4.1.3. Single-Photon Emission Computed Tomography (SPECT)
With recent advancements in high-sensitivity cardiac cameras and radiotracers, dynamic SPECT found its place in the quantification of myocardial blood flow and the assessment of CMD [60]. As the accuracy, diagnostic, and prognostic significance of SPECT is still under PET and CMR, it can allow clinically useful measurements in the absence of previously mentioned modalities.
4.1.4. Positron Emission Tomography (PET)
The main advantages of PET in the estimation of CMD are global and regional measurements of perfusion, quantitative MBF, and function, both at stress and rest. By estimating myocardial perfusion during rest and stress, it can accurately estimate myocardial perfusion reserve (MPR), a value that has an excellent correlation with invasive modalities and also with adverse outcomes [61]. As it can estimate both epicardial and microvascular coronary distribution, PET can improve risk stratification for patients being investigated for ischemia. Studies on patients with hypertension revealed that the “endogen” type of CMD, predominantly related to alterations in resting myocardial blood flow, is more prevalent in these patients [62]. High radiation exposure and cost are the main disadvantages of this method. In comparison to cardiac magnetic resonance, PET lacks the possibility to additionally provide a sophisticated myocardial tissue characterization.
4.1.5. Cardiac Magnetic Resonance (CMR)
Cardiac magnetic resonance has an important place in cardiac diagnostics, considering that it is a non-invasive method during which, with high specificity and sensitivity, the existence of both significant epicardial obstructive coronary disease and coronary microvascular dysfunction can be confirmed or excluded. Diagnostics of coronary microvascular dysfunction via CMR can be established by analyzing myocardial perfusion during the stress test in comparison with myocardial perfusion at rest, which actually evaluates the vasodilatory flow reserve [63]. Methods within cardiac magnetic resonance to evaluate the existence of coronary microvascular dysfunction can be qualitative and quantitative. A qualitative method of assessment includes visual evaluation of the perfusion during stress, whereby a characteristic diffuse subendocardial perfusion defect is observed. The drawback of the qualitative evaluation of the stress perfusion study is the extremely low sensitivity of only 41%, but also the inability to clearly differentiate between patients who have a pronounced degree of coronary microvascular dysfunction and patients who have multi-vessel CAD, which can also cause a diffuse subendocardial defect in perfusion [64]. If coronary angiography was not done before the stress perfusion test, in the differentiation of coronary microvascular dysfunction and obstructive coronary disease, LGE sequences can be helpful, on which the zones of the LGE phenomenon are not registered in patients with microvascular dysfunction. Novel CMR diagnostic modalities, myocardial tissue mapping, and ECV are important in estimating the presence and degree of interstitial fibrosis, which can be significant in risk stratification, especially in patients with hypertension who have left ventricular hypertrophy, diastolic dysfunction, and consequently an increased risk of HFpEF [65].
Semiquantitative and, especially, quantitative methods of evaluation of the stress perfusion study are used for definitive assessment. Quantitative methods of assessing coronary microvascular dysfunction can, in addition to establishing a diagnosis, evaluate the severity of the disease, as well as monitor the effect of different therapeutic modalities. New sophisticated and fully automated CMR methods in the analysis of myocardial perfusion enable high diagnostic accuracy, strong prognostic significance, as well as complete independence from the level of staff training [66]. The basic parameter for the analysis is the value of the blood flow through the myocardium (myocardial blood flow - MBF), which is analyzed both at rest (rest perfusion) and under stress (stress perfusion). Patients with global stress MBF below 2.25 mL/g/min without visual defects in perfusion are likely to have coronary microvascular dysfunction [67]. The difference in myocardial blood flow at rest and under stress represents the myocardial perfusion reserve (MPR), whose indexed value (MPRI) is the most sensitive parameter in the diagnosis of coronary microvascular dysfunction [68]. The accuracy of this method can be significantly increased by analyzing the myocardial perfusion reserve in the subendocardial layer (MPRendo), bearing in mind that the subendocardial layer of the myocardium is the most sensitive to the existence of ischemia [69]. The values of these parameters can be fully evaluated and quantified using pixelated perfusion maps at the level of individual segments according to the 16-segment model of the left ventricle. This kind of analysis makes it possible to establish a diagnosis with high sensitivity and specificity but also to differentiate the existence of obstructive coronary disease from coronary microvascular dysfunction. Clinically relevant values of the above-mentioned parameters for the diagnosis of coronary microvascular dysfunction can be registered even in the absence of qualitative changes in perfusion. In studies that used a fully quantitative assessment of the stress perfusion study to diagnose CMD, an excellent correlation was shown with the values of invasively measured coronary flow parameters (dominantly with the value of the coronary flow reserve - CFR), but also with the value of the index of microvascular resistance (IMR) [70, 71]. In terms of clinical outcomes, stress MBF and MPR/MPRI have been shown to be associated with serious adverse cardiovascular events and mortality [72].
Figure 1.
A combination of qualitative, semiquantitative and quantitative methods for the evaluation of CMR stress perfusion study in a patient with coronary microvascular dysfunction (a) LGE PSIR sequence, short axis view; showing the absence of LGE phenomenon; b) Qualitative analysis of stress perfusion study; a global subendocardial perfusion defect is observed; c) Perfusion map during stress perfusion study, short axis section, medial level; a global subendocardial perfusion defect is observed; d) Semiquantitative analysis (flow/time curve), short axis section, medial level; the perfusion curves indicate a global perfusion defect in the subendocardial layers of the myocardium (green and blue curves) in comparison to the subepicardial layers (red and orange curves); e) Quantitative analysis of stress perfusion study; diffusely reduced normalized values of myocardial perfusion reserve (MPRI) are observed).
Figure 1.
A combination of qualitative, semiquantitative and quantitative methods for the evaluation of CMR stress perfusion study in a patient with coronary microvascular dysfunction (a) LGE PSIR sequence, short axis view; showing the absence of LGE phenomenon; b) Qualitative analysis of stress perfusion study; a global subendocardial perfusion defect is observed; c) Perfusion map during stress perfusion study, short axis section, medial level; a global subendocardial perfusion defect is observed; d) Semiquantitative analysis (flow/time curve), short axis section, medial level; the perfusion curves indicate a global perfusion defect in the subendocardial layers of the myocardium (green and blue curves) in comparison to the subepicardial layers (red and orange curves); e) Quantitative analysis of stress perfusion study; diffusely reduced normalized values of myocardial perfusion reserve (MPRI) are observed).

Non-contrast-based CMR techniques for perfusion estimation are the future of CMD diagnostics as they are more sensitive and have even higher diagnostic accuracy compared to today’s widely available techniques. They are based on the principle of estimating the myocardial tissue oxygenation by specific protocols or comparing the changes of myocardial native T1 time during the rest and stress perfusion study [73]. These techniques can overlook different limitations of conventional techniques, including imaging artifacts, long scan time, interobserver variability, problems with the absolute quantitation of myocardial blood flow, and restricted use in patients with chronic kidney disease.

Table 1.
Characteristics of non-invasive imaging modalities in the evaluation of CMD.
| Diagnostic modality | Parameter | Advantages | Disadvantages |
|---|---|---|---|
| Echocardiography | CFRV |
|
|
| CT coronary angiography and cardiac perfusion | MPR |
|
|
| PET | MPR, MBF |
|
|
| CMR | MBF, MPR, MPRI |
|
|
CAD – coronary artery disease; CRFV – coronary flow velocity reserve; CMR – cardiac magnetic resonance; CT – computerized tomography; LAD – left anterior descending artery; MBF – myocardial blood flow; MPR - myocardial perfusion reserve; MPRI – myocardial perfusion reserve index; PET – positron emission tomography.
4.2. Invasive Diagnostics
The invasive modalities in the diagnostics of CMD are mainly based on the estimation of coronary blood flow. Coronary blood flow can be estimated by Doppler (measuring coronary flow velocity) or thermodilution (measuring cold bolus transit time), each by a different sensor-tipped intracoronary guidewire [74]. In regard to the endothelium function, coronary blood flow can be estimated in response to adenosine (nonendothelium-dependent function) or in response to acetylcholine (endothelium-dependent function). CFR value (the ratio of the maximal or hyperemic flow to the resting flow) of less than 2.0-2.5 (thermodilution) or 2.5 (Doppler) in the absence of epicardial obstructive coronary artery disease reffers to the presence of coronary microvascular dysfunction [75]. The ratio between myocardial perfusion reserve and flow can be used to calculate coronary microvascular resistance (CMR). In the thermodilution-based method, the index of microvascular resistance (IMR), which a cut-off value of >25 is significant for confirming the presence of CMD, while in the Doppler-based technique the resulting index is called hyperaemic microvascular resistance (hMR) with the cut-off value of ≤2.5 mmHg/cm/s [76, 77]. Regarding endothelium-dependent microvascular dysfunction, the diagnosis can be set if there is an increase of less than 50% in coronary blood flow, accompanied by ischaemic ECG changes and angina symptoms, and in the absence of epicardial vasoconstriction. It is important to have in mind that patients with CMD may have both endothelium-dependent and independent types of microvascular dysfunction. Studies evaluating the invasive indices of CMD in patients with HFpEF revealed abnormalities of coronary flow and resistance [78]. The study by Dryer et al. revealed that HFpEF patients had lower CFR and higher IMR values compared to the control group. These patients were also older, had higher values of NT-proBNP, and higher left ventricular end-diastolic pressure, while 93% of them had hypertension as one of the comorbidities [79].
5. Coronary Microvascular Dysfunction, Hypertension, and HFpEF
Recent studies that researched the pathophysiology of HFpEF and the role of CMD revealed that, across various studies, 40-86% of patients with HFpEF have coronary microvascular dysfunction, proven by both non-invasive and invasive diagnostic modalities [80, 81]. It is still uncertain whether CMD is a cause or a consequence of HFpEF. Since myocardial interstitial and focal fibrosis are one of the main mechanisms in HFpEF responsible for increased myocardial stiffness, it is believed that CMD and its consequences are at the core of HFpEF pathophysiology, mostly due to chronic microvascular inflammation [82]. The emerging role of inflammation in the development of HFpEF has been the subject of numerous studies in recent years. In patients with hypertension, inflammation is driven mainly by oxidative stress, inducing hypertension-related vascular aging through various mediators [83]. This process is shown to be one of the main mechanisms in the development and progression of HFpEF. Kanagala et al. demonstrated that CMD is an independent predictor of all-cause mortality and heart failure hospitalizations in patients with HFpEF [84]. It is important to note that a variety of other parameters were found to correlate between CMD and HFpEF, including age, heart rate, diastolic blood pressure, hemoglobine, urea, creatinine, eGFR, BNP, usage of loop diuretics, and increased LV filling pressures). Hypertension is one of the most important factors for the development of endothelial dysfunction, promotion of pro-hypertrophic, and pro-fibrotic signaling, thus directly increasing the risk for the development of CMD, diffuse and focal fibrosis, and HFpEF [85]. It is shown that a significant number of patients with HFpEF have hypertension as a comorbidity (up to 90%) [86]. The presence of CMD and hypertension, or more precisely, hypertensive heart disease, have prognostic significance in patients with HFpEF. Extracellular volume fraction, a marker of interstitial fibrosis accessed by cardiac magnetic resonance, is one of the most important parameters to discriminate between hypertensive heart disease and HFpEF. The amount of interstitial fibrosis that clinically correlates with significant LV stiffness, the development of HFpEF, and the transition from hypertensive heart disease to HFpEF is the value of ECV of 31.2%. This value can discriminate between HFpEF and HHD with 100% sensitivity and 75% specificity [87]. One more parameter derived from non-invasive diagnostic modalities that can differentiate between HHD and HFpEF is the global longitudinal strain (GLS). In hypertensive heart disease, but also in HFpEF, fibrosis involves the myocardial mid-wall, where circumferential shortening fibers are located, which is why GCS is affected before longitudinal shortening. It is found that GLS is significantly more depressed in patients with HFpEF than in patients with HHD, marking it as a more powerful prognostic marker in HFpEF [88]. One of the possible explanations could be the more pronounced focal, and especially interstitial fibrosis in HFpEF patients, as a consequence of advanced stages of CMD and LV hypertrophy. However, the exact relationship between all these clinical entities is yet to be determined.
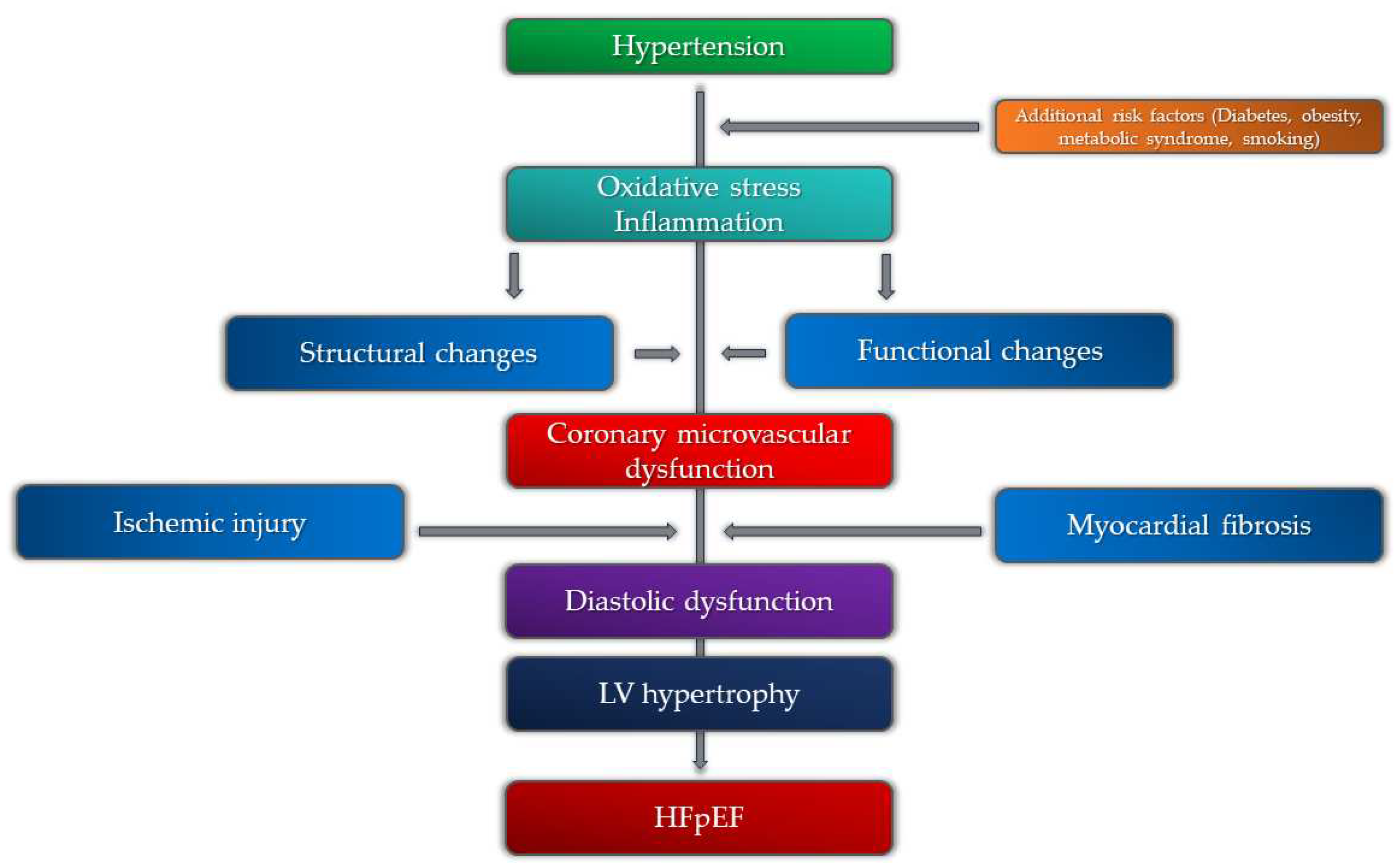
Figure 2.
Pathophysiological mechanisms of heart failure with preserved ejection fraction (HFpEF) in relation to coronary microvascular dysfunction and hypertension.
Figure 2.
Pathophysiological mechanisms of heart failure with preserved ejection fraction (HFpEF) in relation to coronary microvascular dysfunction and hypertension.
6. Coronary Microvascular Dysfunction, Hypertension, and Atrial Fibrilation
As previously mentioned, myocardial fibrosis is one of the main consequences of both hypertensive heart disease and coronary microvascular dysfunction, but also an important pathophysiological mechanism of HFpEF. Cardiac magnetic resonance studies demonstrated the presence of myocardial fibrosis not only in the LV myocardium but also in the left atrium, subsequently increasing the risk of atrial fibrillation occurrence [89]. It is notable that, aside from being the most prevalent sustained arrhythmia in clinical practice, atrial fibrillation is particularly common in patients with HFpEF [90]. Although there is a lack of evidence on the exact relationship between CMD and AF, it is proposed that impaired myocardial perfusion in patients with CMD is causing atrial remodeling and electrical instability, thus facilitating the occurrence of AF in patients with CMD. Recent studies evaluating the presence and impact of AF in patients with HFpEF revealed that AF is present in 79% of patients with HFpEF [91]. Among patients with AF and HFpEF, more than 90% of patients had impaired invasively derived values of CFR, indicating the presence of CMD. It is important to underline that in these patients hypertension was significantly more prevalent, contributing to the development of CMD, AF, and HFpEF. Based on the above, it is important to search for CMD in patients with hypertension and atrial fibrillation, as these patients have an increased risk of developing HFpEF.
7. Management of Coronary Microvascular Dysfunction in Patients with Hypertension
Having in mind the variety of pathophysiological mechanisms and different clinical phenotypes, the management of coronary microvascular dysfunction is a challenging task. It is mainly a combination of pharmacological treatment and lifestyle modification, although, in the last few years, several interventional techniques have appeared as potential therapeutic solutions. Lifestyle interventions, including smoking cessation, weight loss, regular exercise, and improved nutrition have demonstrated positive effects on microvascular function [92, 93]. It is shown that the optimization of underlying diabetes mellitus and hyperlipidemia, and also the treatment of hypertension, as one of the most important risk factors, is beneficial in patients with CMD [94]. Early and continuous regulation of hypertension in patients with CMD is significant as it can slow down the occurrence and progression of several subclinical and clinical entities such as left ventricular hypertrophy, interstitial myocardial fibrosis, and diastolic dysfunction. This can reduce the ischemic burden, improve symptoms, and reduce the risk of adverse events, especially HFpEF. AEC inhibitors, angiotensin receptor blockers (ARB), calcium channel blockers, and beta blockers with vasodilatory properties, have substantial effects in improving microvascular perfusion [95, 96, 97]. Regarding the effects of ACE inhibitors, it is shown that certain medications, can also slow down and even reverse reactive interstitial fibrosis, which is important in patients with hypertension [98]. The ongoing trial regarding the interventional treatment of hypertension (renal denervation) tends to prove the positive effects of this procedure in patients with hypertension-related microvascular dysfunction, although the results of previous studies were controversial [99]. Considering the already proven positive effects of renal denervation on cardiac morphology and function, the additional effects on the improvement of microvascular function can be helpful in preventing both HFpEF and HFrEF. Interventional procedures for the treatment of microvascular angina have been under development in recent years with promising results. The implantation of a coronary sinus reducer, which leads to a significant reduction in vascular resistance in the subendocardium, showed positive effects on angina symptom relief in patients with CMD [100]. Future studies should demonstrate the overall clinical benefit of this procedure in everyday practice.
8. Prognosis
Recent studies that investigated the prognostic significance of invasively derived indices of CMD revealed that depressed CFR was associated with an increased risk of cardiovascular death and heart failure admission, while elevated IMR alone still has a limited prognostic value [101]. It is still unclear why IMR has uncertain prognostic significance in patients with preserved CFR. However, one of the possible explanations can be that impaired IMR value can be an earlier indicator of CMD in the subclinical phase of the disease, with dominant functional alterations of the microcirculation. On the other hand, depressed CFR is more significant in the clinical phase of the disease, reflecting both functional and structural alterations, and is more associated with clinical outcomes in these patients. Non-invasive estimation of myocardial perfusion seems to have an additional prognostic significance. The biggest number of studies are referred to CMR and PET as the two most important non-invasive modalities. In PET studies, there was a positive correlation with clinical outcomes in the group of patients with both epicardial and microvascular coronary artery disease, as well as with CMD solely [102]. The reduction of myocardial flow reserve was associated with MACE in both of these groups. The study by Murthy et al. demonstrated that there was a 3-year cardiac mortality rate of 8% in patients with impaired MFR among which over 80% had hypertension as a comorbidity [103].
Quantitative CMR methods of estimating myocardial perfusion demonstrated a significant correlation with major adverse cardiovascular events. The value of MPRI (myocardial perfusion reserve index) below the optimal predictive threshold value of 1.47 was related to a three-fold increased risk of having MACE in the 5-year follow-up. It is important to underline that hypertension, alongside MPRI value, was also a significant predictor of poor prognosis in these patients, indicating an important mutual relationship between microvascular angina and hypertension [104].
9. Future Perspectives
A more integrated algorithm of CMD diagnostics, especially in symptomatic patients and patients with increased risk of HFpEF is mandatory. This is important not only to control symptoms but also to minimize the possibility of future adverse cardiovascular events. Investigating the relationship between different clinical entities, especially CMD, myocardial fibrosis, hypertensive heart disease, and HFpEF, will be helpful in the proper identification of patients at risk and also to guide further development of different therapeutic modalities.
10. Conclusions
Coronary microvascular dysfunction is a clinical entity linked with various risk factors that significantly affect cardiac morbidity and mortality. Hypertension, one of the most important, causes both functional and structural alterations in the microvasculature, promoting the occurrence and progression of microvascular dysfunction. CMD is also related to several hypertension-related morphological and functional changes in the myocardium in the subclinical and early clinical stages, including left ventricular hypertrophy, interstitial myocardial fibrosis, and diastolic dysfunction. This indicates the fact that CMD, especially if associated with hypertension, is a subclinical marker of end-organ damage and heart failure, particularly the one with preserved ejection fraction. Although various pharmacological and interventional modalities demonstrated certain clinical effects, integrated diagnostic and therapeutic algorithms are necessary to reduce the burden of this emerging condition.
Author Contributions
Conceptualization, M.Z. and Z.V.; investigation, D.L.; writing— original draft preparation, V.P., A.K., and T.I.; writing—review and editing, R.L. and S.K.; supervision, G.K. and D.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable, the paper does not have information or images that can identify any patient.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chen C, Wei J, AlBadri A, Zarrini P, Bairey Merz CN. Coronary Microvascular Dysfunction - Epidemiology, Pathogenesis, Prognosis, Diagnosis, Risk Factors and Therapy. Circ J. 2016, 81, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Bradley C, Berry C. Definition and epidemiology of coronary microvascular disease. J Nucl Cardiol. 2022, 29, 1763–1775. [Google Scholar] [CrossRef]
- Vancheri F, Longo G, Vancheri S, Henein M. Coronary Microvascular Dysfunction. J Clin Med. 2020, 9, 2880. [Google Scholar] [CrossRef] [PubMed]
- Godo S, Takahashi J, Yasuda S, Shimokawa H. Endothelium in Coronary Macrovascular and Microvascular Diseases. J Cardiovasc Pharmacol. 2021, 78 Suppl 6, S19–S29. [Google Scholar] [CrossRef] [PubMed]
- Labazi H, Trask AJ. Coronary microvascular disease as an early culprit in the pathophysiology of diabetes and metabolic syndrome. Pharmacol Res. 2017, 123, 114–21. [Google Scholar] [CrossRef] [PubMed]
- Emanuelsson F, Nordestgaard BG, Tybjærg-Hansen A, Benn M. Impact of LDL Cholesterol on Microvascular Versus Macrovascular Disease: A Mendelian Randomization Study. J Am Coll Cardiol. 2019, 74, 1465–1476. [Google Scholar] [CrossRef] [PubMed]
- Kibel A, Selthofer-Relatic K, Drenjancevic I, Bacun T, Bosnjak I, Kibel D, et al. Coronary microvascular dysfunction in diabetes mellitus. J Int Med Res. 2017, 45, 1901–29. [Google Scholar] [CrossRef] [PubMed]
- Lee MP, Glynn RJ, Schneeweiss S, Lin KJ, Patorno E, Barberio J, et al. Risk Factors for Heart Failure with Preserved or Reduced Ejection Fraction Among Medicare Beneficiaries: Application of Competing Risks Analysis and Gradient Boosted Model. Clin Epidemiol. 2020, 12, 607–16. [Google Scholar] [CrossRef] [PubMed]
- Paulus WJ, Tschöpe C. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol. 2013, 62, 263–71. [Google Scholar] [CrossRef]
- Crea F, Montone RA, Rinaldi R. Pathophysiology of Coronary Microvascular Dysfunction. Circ J. 2022, 86, 1319–28. [Google Scholar] [CrossRef]
- Masi S, Rizzoni D, Taddei S, Widmer RJ, Montezano AC, Lüscher TF, et al. Assessment and pathophysiology of microvascular disease: recent progress and clinical implications. Eur Heart J. 2021, 42, 2590–2604. [Google Scholar] [CrossRef] [PubMed]
- Suda A, Takahashi J, Hao K, Kikuchi Y, Shindo T, Ikeda S, et al. Coronary Functional Abnormalities in Patients With Angina and Nonobstructive Coronary Artery Disease. J Am Coll Cardiol. 2019, 74, 2350–60. [Google Scholar] [CrossRef] [PubMed]
- Sorop O, Heinonen I, van Kranenburg M, van de Wouw J, de Beer VJ, Nguyen ITN, et al. Multiple common comorbidities produce left ventricular diastolic dysfunction associated with coronary microvascular dysfunction, oxidative stress, and myocardial stiffening. Cardiovasc Res. 2018, 114, 954–64. [Google Scholar] [CrossRef] [PubMed]
- Kwiecinski J, Lennen RJ, Gray GA, Borthwick G, Boswell L, Baker AH, et al. Progression and regression of left ventricular hypertrophy and myocardial fibrosis in a mouse model of hypertension and concomitant cardiomyopathy. J Cardiovasc Magn Reson. 2020, 22, 57. [Google Scholar] [CrossRef] [PubMed]
- de Moraes R, Tibirica E. Early Functional and Structural Microvascular Changes in Hypertension Related to Aging. Curr Hypertens Rev. 2017, 13, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Hermann M, Flammer A, Lüscher TF. Nitric oxide in hypertension. J Clin Hypertens (Greenwich) 2006, 8 12 Suppl 4, 17–29. [Google Scholar] [CrossRef]
- da Silva GM, da Silva MC, Nascimento DVG, Lima Silva EM, Gouvêa FFF, de França Lopes LG, et al. Nitric Oxide as a Central Molecule in Hypertension: Focus on the Vasorelaxant Activity of New Nitric Oxide Donors. Biology (Basel). 2021, 10, 1041. [Google Scholar] [CrossRef]
- Montezano AC, Touyz RM. Reactive oxygen species, vascular Noxs, and hypertension: focus on translational and clinical research. Antioxid Redox Signal. 2014, 20, 164–82. [Google Scholar] [CrossRef] [PubMed]
- Brandt MM, Cheng C, Merkus D, Duncker DJ, Sorop O. Mechanobiology of Microvascular Function and Structure in Health and Disease: Focus on the Coronary Circulation. Front Physiol 2021, 12, 771960. [Google Scholar] [CrossRef]
- Pries AR, Badimon L, Bugiardini R, Camici PG, Dorobantu M, Duncker DJ, et al. Coronary vascular regulation, remodelling, and collateralization: mechanisms and clinical implications on behalf of the working group on coronary pathophysiology and microcirculation. Eur Heart J. 2015, 36, 3134–46. [Google Scholar] [CrossRef]
- Konst RE, Guzik TJ, Kaski JC, Maas AHEM, Elias-Smale SE. The pathogenic role of coronary microvascular dysfunction in the setting of other cardiac or systemic conditions. Cardiovasc Res. 2020, 116, 817–28. [Google Scholar] [CrossRef] [PubMed]
- Ding J, Wai KL, McGeechan K, Ikram MK, Kawasaki R, Xie J, et al. Retinal vascular caliber and the development of hypertension: a meta-analysis of individual participant data. J Hypertens. 2014, 32, 207–15. [Google Scholar] [CrossRef] [PubMed]
- Dharmashankar K, Widlansky ME. Vascular endothelial function and hypertension: insights and directions. Curr Hypertens Rep. 2010, 12, 448–55. [Google Scholar] [CrossRef] [PubMed]
- Goto K, Ohtsubo T, Kitazono T. Endothelium-Dependent Hyperpolarization (EDH) in Hypertension: The Role of Endothelial Ion Channels. Int J Mol Sci. 2018, 19, 315. [Google Scholar] [CrossRef] [PubMed]
- Kostov, K. The Causal Relationship between Endothelin-1 and Hypertension: Focusing on Endothelial Dysfunction, Arterial Stiffness, Vascular Remodeling, and Blood Pressure Regulation. Life (Basel). 2021, 11, 986. [Google Scholar] [CrossRef] [PubMed]
- Hamilos M, Petousis S, Parthenakis F. Interaction between platelets and endothelium: from pathophysiology to new therapeutic options. Cardiovasc Diagn Ther. 2018, 8, 568–80. [Google Scholar] [CrossRef] [PubMed]
- Aribas E, Roeters van Lennep JE, Elias-Smale SE, Piek JJ, Roos M, Ahmadizar F, et al. Prevalence of microvascular angina among patients with stable symptoms in the absence of obstructive coronary artery disease: a systematic review. Cardiovasc Res. 2022, 118, 763–71. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi Y, Fearon WF, Honda Y, Tanaka S, Pargaonkar V, Fitzgerald PJ, et al. Effect of Sex Differences on Invasive Measures of Coronary Microvascular Dysfunction in Patients With Angina in the Absence of Obstructive Coronary Artery Disease. JACC Cardiovasc Interv. 2015, 8, 1433–41. [Google Scholar] [CrossRef] [PubMed]
- Loperena R, Harrison DG. Oxidative Stress and Hypertensive Diseases. Med Clin North Am. 2017, 101, 169–93. [Google Scholar] [CrossRef]
- Reynolds HR, Bairey Merz CN, Berry C, Samuel R, Saw J, Smilowitz NR, et al. Coronary Arterial Function and Disease in Women With No Obstructive Coronary Arteries. Circ Res. 2022, 130, 529–51. [Google Scholar] [CrossRef]
- Agarwal M, Shufelt C, Mehta PK, Gill E, Berman DS, Li D, et al. Cardiac risk factors and myocardial perfusion reserve in women with microvascular coronary dysfunction. Cardiovasc Diagn Ther. 2013, 3, 146–52. [Google Scholar] [CrossRef] [PubMed]
- Barnabas O, Wang H, Gao XM. Role of estrogen in angiogenesis in cardiovascular diseases. J Geriatr Cardiol. 2013, 10, 377–82. [Google Scholar] [CrossRef] [PubMed]
- Tunc E, Eve AA, Madak-Erdogan Z. Coronary Microvascular Dysfunction and Estrogen Receptor Signaling. Trends Endocrinol Metab. 2020, 31, 228–38. [Google Scholar] [CrossRef] [PubMed]
- Mottillo S, Filion KB, Genest J, Joseph L, Pilote L, Poirier P, et al. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J Am Coll Cardiol. 2010, 56, 1113–32. [Google Scholar] [CrossRef]
- Chilian W, Nystoriak MA, Sisakian H, Ohanyan V. Coronary microvascular disease during metabolic syndrome: What is known and unknown: Pathological consequences of redox imbalance for endothelial K+ channels. Int J Cardiol 2020, 321, 18–19. [Google Scholar] [CrossRef] [PubMed]
- Sucato V, Madaudo C, Di Fazio L, Manno G, Vadalà G, Novo S, et al. Impact of Metabolic Syndrome on Coronary Microvascular Dysfunction: A Single Center Experience. Cardiology and Cardiovascular Medicine 2023, 145–50. [Google Scholar] [CrossRef]
- Salvatore T, Galiero R, Caturano A, Vetrano E, Loffredo G, Rinaldi L, et al. Coronary Microvascular Dysfunction in Diabetes Mellitus: Pathogenetic Mechanisms and Potential Therapeutic Options. Biomedicines. 2022, 10, 2274. [Google Scholar] [CrossRef] [PubMed]
- Ormazabal V, Nair S, Elfeky O, Aguayo C, Salomon C, Zuñiga FA. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef] [PubMed]
- Russo I, Frangogiannis NG. Diabetes-associated cardiac fibrosis: Cellular effectors, molecular mechanisms and therapeutic opportunities. J Mol Cell Cardiol 2016, 90, 84–93. [Google Scholar] [CrossRef]
- Zhang W, Singh S, Liu L, Mohammed AQ, Yin G, Xu S, et al. Prognostic value of coronary microvascular dysfunction assessed by coronary angiography-derived index of microcirculatory resistance in diabetic patients with chronic coronary syndrome. Cardiovasc Diabetol. 2022, 21, 222. [Google Scholar] [CrossRef]
- Stapleton PA, Goodwill AG, James ME, Brock RW, Frisbee JC. Hypercholesterolemia and microvascular dysfunction: interventional strategies. J Inflamm (Lond) 2010, 7, 54. [Google Scholar] [CrossRef] [PubMed]
- Padró T, Vilahur G, Badimon L. Dyslipidemias and Microcirculation. Curr Pharm Des. 2018, 24, 2921–26. [Google Scholar] [CrossRef] [PubMed]
- Avtaar Singh SS, Nappi F. Pathophysiology and Outcomes of Endothelium Function in Coronary Microvascular Diseases: A Systematic Review of Randomized Controlled Trials and Multicenter Study. Biomedicines. 2022, 10, 3010. [Google Scholar] [CrossRef] [PubMed]
- Zdravkovic M, Popadic V, Klasnja S, Milic N, Rajovic N, Divac A, et al. Obstructive Sleep Apnea and Cardiovascular Risk: The Role of Dyslipidemia, Inflammation, and Obesity. Front Pharmacol 2022, 13, 898072. [Google Scholar] [CrossRef] [PubMed]
- Bozbas SS, Eroglu S, Ozyurek BA, Eyuboglu FO. Coronary flow reserve is impaired in patients with obstructive sleep apnea. Ann Thorac Med. 2017, 12, 272–77. [Google Scholar] [CrossRef] [PubMed]
- Michael Pittilo, R. Cigarette smoking, endothelial injury and cardiovascular disease. Int J Exp Pathol. 2000, 81, 219–30. [Google Scholar] [CrossRef] [PubMed]
- Gullu H, Caliskan M, Ciftci O, Erdogan D, Topcu S, Yildirim E, et al. Light cigarette smoking impairs coronary microvascular functions as severely as smoking regular cigarettes. Heart. 2007, 93, 1274–7. [Google Scholar] [CrossRef] [PubMed]
- Haig C, Carrick D, Carberry J, Mangion K, Maznyczka A, Wetherall K, et al. Current Smoking and Prognosis After Acute ST-Segment Elevation Myocardial Infarction: New Pathophysiological Insights. JACC Cardiovasc Imaging. 2019, 12, 993–1003. [Google Scholar] [CrossRef] [PubMed]
- Toya T, Nagatomo Y, Ikegami Y, Masaki N, Adachi T. Coronary microvascular dysfunction in heart failure patients. Front Cardiovasc Med 2023, 10, 1153994. [Google Scholar] [CrossRef]
- Fordyce CB, Newby DE, Douglas PS. Diagnostic Strategies for the Evaluation of Chest Pain: Clinical Implications From SCOT-HEART and PROMISE. J Am Coll Cardiol. 2016, 67, 843–52. [Google Scholar] [CrossRef]
- Carbone A, D'Andrea A, Sperlongano S, Tagliamonte E, Mandoli GE, Santoro C, et al. Echocardiographic assessment of coronary microvascular dysfunction: Basic concepts, technical aspects, and clinical settings. Echocardiography. 2021, 38, 993–1001. [Google Scholar] [CrossRef] [PubMed]
- Schroder J, Prescott E. Doppler Echocardiography Assessment of Coronary Microvascular Function in Patients With Angina and No Obstructive Coronary Artery Disease. Front Cardiovasc Med 2021, 8, 723542. [Google Scholar] [CrossRef] [PubMed]
- Shah SJ, Lam CSP, Svedlund S, Saraste A, Hage C, Tan RS, et al. Prevalence and correlates of coronary microvascular dysfunction in heart failure with preserved ejection fraction: PROMIS-HFpEF. Eur Heart J. 2018, 39, 3439–50. [Google Scholar] [CrossRef] [PubMed]
- Völz S, Svedlund S, Andersson B, Li-Ming G, Rundqvist B. Coronary flow reserve in patients with resistant hypertension. Clin Res Cardiol. 2017, 106, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Clemmensen TS, Christensen M, Løgstrup BB, Kronborg CJS, Knudsen UB. Reduced coronary flow velocity reserve in women with previous pre-eclampsia: link to increased cardiovascular disease risk. Ultrasound Obstet Gynecol. 2020, 55, 786–792. [Google Scholar] [CrossRef]
- Nieman K, Balla S. Dynamic CT myocardial perfusion imaging. J Cardiovasc Comput Tomogr. 2020, 14, 303–06. [Google Scholar] [CrossRef] [PubMed]
- Seitun S, Clemente A, De Lorenzi C, Benenati S, Chiappino D, Mantini C, et al. Cardiac CT perfusion and FFRCTA: pathophysiological features in ischemic heart disease. Cardiovasc Diagn Ther. 2020, 10, 1954–78. [Google Scholar] [CrossRef]
- Ihdayhid AR, Fairbairn TA, Gulsin GS, Tzimas G, Danehy E, Updegrove A, et al. Cardiac computed tomography-derived coronary artery volume to myocardial mass. J Cardiovasc Comput Tomogr. 2022, 16, 198–206. [Google Scholar] [CrossRef] [PubMed]
- van Rosendael SE, van Rosendael AR, Kuneman JH, Patel MR, Nørgaard BL, Fairbairn TA, et al. Coronary Volume to Left Ventricular Mass Ratio in Patients With Hypertension. Am J Cardiol 2023, 199, 100–9. [Google Scholar] [CrossRef]
- Djaïleb L, Riou L, Piliero N, Carabelli A, Vautrin E, Broisat A, et al. SPECT myocardial ischemia in the absence of obstructive CAD: Contribution of the invasive assessment of microvascular dysfunction. J Nucl Cardiol. 2018, 25, 1017–22. [Google Scholar] [CrossRef]
- Mathew RC, Bourque JM, Salerno M, Kramer CM. Cardiovascular Imaging Techniques to Assess Microvascular Dysfunction. JACC Cardiovasc Imaging. 2020, 13, 1577–1590. [Google Scholar] [CrossRef] [PubMed]
- Zhou W, Brown JM, Bajaj NS, Chandra A, Divakaran S, Weber B, et al. Hypertensive coronary microvascular dysfunction: a subclinical marker of end organ damage and heart failure. Eur Heart J. 2020, 41, 2366–75. [Google Scholar] [CrossRef] [PubMed]
- Patel AR, Salerno M, Kwong RY, Singh A, Heydari B, Kramer CM. Stress Cardiac Magnetic Resonance Myocardial Perfusion Imaging: JACC Review Topic of the Week. J Am Coll Cardiol. 2021, 78, 1655–68. [Google Scholar] [CrossRef] [PubMed]
- Zdravkovic M, Klasnja S, Popovic M, Djuran P, Mrda D, Ivankovic T, et al. Cardiac Magnetic Resonance in Hypertensive Heart Disease: Time for a New Chapter. Diagnostics (Basel). 2022, 13, 137. [Google Scholar] [CrossRef] [PubMed]
- Liang L, Wang X, Yu Y, Zhang Y, Liu J, Chen M, et al. T1 Mapping and Extracellular Volume in Cardiomyopathy Showing Left Ventricular Hypertrophy: Differentiation Between Hypertrophic Cardiomyopathy and Hypertensive Heart Disease. Int J Gen Med 2022, 15, 4163–4173. [Google Scholar] [CrossRef] [PubMed]
- Engblom H, Xue H, Akil S, Carlsson M, Hindorf C, Oddstig J, et al. Fully quantitative cardiovascular magnetic resonance myocardial perfusion ready for clinical use: a comparison between cardiovascular magnetic resonance imaging and positron emission tomography. J Cardiovasc Magn Reson. 2017, 19, 78. [Google Scholar] [CrossRef] [PubMed]
- Zorach B, Shaw PW, Bourque J, Kuruvilla S, Balfour PC Jr, Yang Y, et al. Quantitative cardiovascular magnetic resonance perfusion imaging identifies reduced flow reserve in microvascular coronary artery disease. J Cardiovasc Magn Reson. 2018, 20, 14. [Google Scholar] [CrossRef] [PubMed]
- Thomson LE, Wei J, Agarwal M, Haft-Baradaran A, Shufelt C, Mehta PK, et al. Cardiac magnetic resonance myocardial perfusion reserve index is reduced in women with coronary microvascular dysfunction. A National Heart, Lung, and Blood Institute-sponsored study from the Women's Ischemia Syndrome Evaluation. Circ Cardiovasc Imaging. 2015, 8, 101161/CIRCIMAGING114002481 e002481. [Google Scholar] [CrossRef]
- Rahman H, Scannell CM, Demir OM, Ryan M, McConkey H, Ellis H, et al. High-Resolution Cardiac Magnetic Resonance Imaging Techniques for the Identification of Coronary Microvascular Dysfunction. JACC Cardiovasc Imaging. 2021, 14, 978–986. [Google Scholar] [CrossRef]
- Chang A, Kang N, Chung J, Gupta AR, Parwani P. Evaluation of Ischemia with No Obstructive Coronary Arteries (INOCA) and Contemporary Applications of Cardiac Magnetic Resonance (CMR). Medicina (Kaunas). 2023, 59, 1570. [Google Scholar] [CrossRef]
- Scarsini R, Shanmuganathan M, De Maria GL, Borlotti A, Kotronias RA, Burrage MK, et al. Coronary Microvascular Dysfunction Assessed by Pressure Wire and CMR After STEMI Predicts Long-Term Outcomes. JACC Cardiovasc Imaging. 2021, 14, 1948–59. [Google Scholar] [CrossRef]
- Knott KD, Seraphim A, Augusto JB, Xue H, Chacko L, Aung N, et al. The Prognostic Significance of Quantitative Myocardial Perfusion: An Artificial Intelligence-Based Approach Using Perfusion Mapping. Circulation. 2020, 141, 1282–91. [Google Scholar] [CrossRef] [PubMed]
- Levelt E, Piechnik SK, Liu A, Wijesurendra RS, Mahmod M, Ariga R, et al. Adenosine stress CMR T1-mapping detects early microvascular dysfunction in patients with type 2 diabetes mellitus without obstructive coronary artery disease. J Cardiovasc Magn Reson. 2017, 19, 81. [Google Scholar] [CrossRef]
- Travieso A, Jeronimo-Baza A, Faria D, Shabbir A, Mejia-Rentería H, Escaned J. Invasive evaluation of coronary microvascular dysfunction. J Nucl Cardiol. 2022, 29, 2474–86. [Google Scholar] [CrossRef] [PubMed]
- Mangiacapra F, Viscusi MM, Verolino G, Paolucci L, Nusca A, Melfi R, et al. Invasive Assessment of Coronary Microvascular Function. J Clin Med. 2021, 11, 228. [Google Scholar] [CrossRef]
- Geng Y, Wu X, Liu H, Zheng D, Xia L. Index of microcirculatory resistance: state-of-the-art and potential applications in computational simulation of coronary artery disease. J Zhejiang Univ Sci B. 2022, 23, 123–40 English. [Google Scholar] [CrossRef]
- Fearon WF, Kobayashi Y. Invasive Assessment of the Coronary Microvasculature: The Index of Microcirculatory Resistance. Circ Cardiovasc Interv. 2017, 10, e005361. [Google Scholar] [CrossRef] [PubMed]
- Toya T, Nagatomo Y, Ikegami Y, Masaki N, Adachi T. Coronary microvascular dysfunction in heart failure patients. Front Cardiovasc Med 2023, 10, 1153994. [Google Scholar] [CrossRef]
- Dryer K, Gajjar M, Narang N, Lee M, Paul J, Shah AP, et al. Coronary microvascular dysfunction in patients with heart failure with preserved ejection fraction. Am J Physiol Heart Circ Physiol. 2018, 314, H1033–H1042. [Google Scholar] [CrossRef]
- Lin X, Wu G, Wang S, Huang J. The prevalence of coronary microvascular dysfunction (CMD) in heart failure with preserved ejection fraction (HFpEF): a systematic review and meta-analysis. Heart Fail Rev 2023. [Google Scholar] [CrossRef]
- D'Amario D, Migliaro S, Borovac JA, Restivo A, Vergallo R, Galli M, et al. Microvascular Dysfunction in Heart Failure With Preserved Ejection Fraction. Front Physiol 2019, 10, 1347. [Google Scholar] [CrossRef] [PubMed]
- Paulus WJ, Zile MR. From Systemic Inflammation to Myocardial Fibrosis: The Heart Failure With Preserved Ejection Fraction Paradigm Revisited. Circ Res. 2021, 128, 1451–67. [Google Scholar] [CrossRef] [PubMed]
- Sagris M, Theofilis P, Antonopoulos AS, Oikonomou E, Paschaliori C, Galiatsatos N, et al. Inflammation in Coronary Microvascular Dysfunction. Int J Mol Sci. 2021, 22, 13471. [Google Scholar] [CrossRef] [PubMed]
- Kanagala P, Arnold JR, Singh A, Chan DCS, Cheng ASH, Khan JN, et al. Characterizing heart failure with preserved and reduced ejection fraction: An imaging and plasma biomarker approach. PLoS One. 2020, 15, e0232280. [Google Scholar] [CrossRef] [PubMed]
- Cornuault L, Rouault P, Duplàa C, Couffinhal T, Renault MA. Endothelial Dysfunction in Heart Failure With Preserved Ejection Fraction: What are the Experimental Proofs? Front Physiol 2022, 13, 906272. [Google Scholar] [CrossRef] [PubMed]
- Tam MC, Lee R, Cascino TM, Konerman MC, Hummel SL. Current Perspectives on Systemic Hypertension in Heart Failure with Preserved Ejection Fraction. Curr Hypertens Rep. 2017, 19, 12. [Google Scholar] [CrossRef] [PubMed]
- Su MY, Lin LY, Tseng YH, Chang CC, Wu CK, Lin JL, et al. CMR-verified diffuse myocardial fibrosis is associated with diastolic dysfunction in HFpEF. JACC Cardiovasc Imaging. 2014, 7, 991–7. [Google Scholar] [CrossRef] [PubMed]
- Brann A, Miller J, Eshraghian E, Park JJ, Greenberg B. Global longitudinal strain predicts clinical outcomes in patients with heart failure with preserved ejection fraction. Global longitudinal strain predicts clinical outcomes in patients with heart failure with preserved ejection fraction. Eur J Heart Fail. 2023. [CrossRef] [PubMed]
- Ma J, Chen Q, Ma S. Left atrial fibrosis in atrial fibrillation: Mechanisms, clinical evaluation and management. J Cell Mol Med. 2021, 25, 2764–75. [Google Scholar] [CrossRef]
- Fauchier L, Bisson A, Bodin A. Heart failure with preserved ejection fraction and atrial fibrillation: recent advances and open questions. BMC Med. 2023, 21, 54. [Google Scholar] [CrossRef]
- Gorter TM, van Veldhuisen DJ, Mulder BA, Artola Arita VA, van Empel VPM, Manintveld OC, et al. Prevalence and Incidence of Atrial Fibrillation in Heart Failure with Mildly Reduced or Preserved Ejection Fraction: (Additive) Value of Implantable Loop Recorders. J Clin Med. 2023, 12, 3682. [Google Scholar] [CrossRef] [PubMed]
- Millan-Orge M, Torres-Peña JD, Arenas-Larriva A, Quintana-Navarro GM, Peña-Orihuela P, Alcala-Diaz JF, et al. Influence of dietary intervention on microvascular endothelial function in coronary patients and atherothrombotic risk of recurrence. Sci Rep. 2021, 11, 20301. [Google Scholar] [CrossRef] [PubMed]
- Torres-Peña JD, Rangel-Zuñiga OA, Alcala-Diaz JF, Lopez-Miranda J, Delgado-Lista J. Mediterranean Diet and Endothelial Function: A Review of its Effects at Different Vascular Bed Levels. Nutrients 2020, 12, 2212. [Google Scholar] [CrossRef]
- Schindler TH, Valenta I. Coronary microvascular dysfunction and prognostication in diabetes mellitus. Eur Heart J Cardiovasc Imaging. 2023, 24, 572–573. [Google Scholar] [CrossRef] [PubMed]
- Ong P, Athanasiadis A, Sechtem U. Pharmacotherapy for coronary microvascular dysfunction. Eur Heart J Cardiovasc Pharmacother. 2015, 1, 65–71. [Google Scholar] [CrossRef]
- Michelsen MM, Rask AB, Suhrs E, Raft KF, Høst N, Prescott E. Effect of ACE-inhibition on coronary microvascular function and symptoms in normotensive women with microvascular angina: A randomized placebo-controlled trial. PLoS One. 2018, 13, e0196962. [Google Scholar] [CrossRef]
- Soleymani M, Masoudkabir F, Shabani M, Vasheghani-Farahani A, Behnoush AH, Khalaji A. Updates on Pharmacologic Management of Microvascular Angina. Cardiovasc Ther 2022, 2022, 6080258. [Google Scholar] [CrossRef]
- Weber KT, Sun Y, Gerling IC, Guntaka RV. Regression of Established Cardiac Fibrosis in Hypertensive Heart Disease. Am J Hypertens. 2017, 30, 1049–1052. [Google Scholar] [CrossRef]
- Engholm M, Bertelsen JB, Mathiassen ON, Bøtker HE, Vase H, Peters CD, et al. Effects of renal denervation on coronary flow reserve and forearm dilation capacity in patients with treatment-resistant hypertension. A randomized, double-blinded, sham-controlled clinical trial. Int J Cardiol. 2018, 250, 29–34. [Google Scholar] [CrossRef]
- Ullrich H, Hammer P, Olschewski M, Münzel T, Escaned J, Gori T. Coronary Venous Pressure and Microvascular Hemodynamics in Patients With Microvascular Angina: A Randomized Clinical Trial. JAMA Cardiol. 2023, 8, 979–83. [Google Scholar] [CrossRef]
- Kelshiker MA, Seligman H, Howard JP, Rahman H, Foley M, Nowbar AN, et al. Coronary flow reserve and cardiovascular outcomes: a systematic review and meta-analysis. Eur Heart J. 2022, 43, 1582–93. [Google Scholar] [CrossRef] [PubMed]
- Dorbala S, Di Carli MF. Cardiac PET perfusion: prognosis, risk stratification, and clinical management. Semin Nucl Med. 2014, 44, 344–57. [Google Scholar] [CrossRef] [PubMed]
- Murthy VL, Naya M, Foster CR, Hainer J, Gaber M, Di Carli G, et al. Improved cardiac risk assessment with noninvasive measures of coronary flow reserve. Circulation. 2011, 124, 2215–24. [Google Scholar] [CrossRef]
- Zhou W, Lee JCY, Leung ST, Lai A, Lee TF, Chiang JB, et al. Long-Term Prognosis of Patients With Coronary Microvascular Disease Using Stress Perfusion Cardiac Magnetic Resonance. JACC Cardiovasc Imaging. 2021, 14, 602–11. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



