
Submitted:
19 November 2023
Posted:
20 November 2023
You are already at the latest version
Abstract
This study determined the temporal variation of PM2.5 in ambient air in Thohoyandou and further assessed the associated health risks. The levels of PM2.5 were quantified for a period of 1 year (April 2017-April 2018) using the gravimetric method. There was no significant difference (P-value = 0.18) in concentrations of both PM2.5 samples collected during weekdays (11.29 µg.m-3) and weekends (9.86 µg.m-3). However, higher concentrations of PM2.5 were measured in spring and the lowest was measured in summer. The cancer risk obtained for PM2.5 (2.21 × 10−5, 3 × 10-4, and 5 × 10-4 for infants, children, and adults respectively) in the outdoor air of Thohoyandou has exceeded the limit values by the USEPA and WHO, implying a significant risk for the whole population. For non-carcinogenic risks, the HQ values were 2.60, 4.81, and 2.60 for infants, children, and adults respectively. The HQ value >1 indicates a non-carcinogenic risk to the residents in Thohoyandou and a higher risk to children. Moreover, PM2.5 in Thohoyandou is responsible for 0.15% and 0.13% of deaths resulting from cardiovascular disease and lung cancer respectively for adults above 30 years. PM2.5 is causing adverse health effects in Thohoyandou as deduced from the health risk assessment. Therefore, it is recommended that further epidemiological studies be conducted in Thohoyandou to estimate the burden of disease due to exposure to particulate matter and suitable controlling policies be arranged to reduce particulate matter.
Keywords:
Ambient air
; PM2.5
; Gravimetric method
; WHO guideline
; Health risk assessment
1. Introduction
Exposure to higher concentrations of fine particulate matter (PM2.5) is a major public health concern across the world. This is mainly because of their small size, PM2.5 can penetrate deep into the lungs, heart, and bloodstream causing detrimental health effects (Chen et al., 2022). The health effects of PM2.5 range from respiratory diseases, cardiovascular diseases, and cancer to mortality in worst cases(Wang et al., 2021) (Ahani et al., 2020). The World Health Organization (WHO) estimated that ambient air pollution was responsible for 4.2 million deaths in 2019 due to stroke, heart disease, lung cancer, and acute and chronic respiratory diseases (WHO, 2022). In trying to reduce the health effects of PM2.5, the WHO has set the limit for daily exposure at 25 µg.m-3 (WHO, 2021). However, it is estimated 9 out of 10 people worldwide reside in areas where air pollution levels exceed the WHO guideline (WHO, 2021). This means that the majority of people are at risk of air pollution-related illnesses.
To reduce air pollution and for countries to set management policies to control air pollution, there is a need for routine monitoring of various air pollutants particularly PM2.5 which is more toxic. In South Africa, several studies have been conducted to monitor the concentrations of PM2.5 (Petkova et al., 2013; (Gumede and Savage, 2017; Langerman and Pauw, 2018 ). However, these studies only concentrated on PM2.5 in “hotspot” areas and urban areas with little emphasis on rural areas (Morakinyo et al., 2020). Moreover, in most of these studies, the main focus was on the quantification of PM2.5 and its chemical composition without estimating the health risks associated with PM2.5 and its components. Amongst the epidemiological studies that assessed the health risks associated with air pollutants in South Africa, Naidoo et al., (2013) examined the association between ambient air pollutants and respiratory outcomes amongst school children in Durban and reported that 32.1% of school children who were in grade 3-6 at a time were showing symptoms of asthma. The prevalence was found to have been higher in the southern part where the concentration of air pollutants was high (Naidoo et al., 2013). A study by (Norman et al., 2007) aimed at estimating the burden of diseases attributable to urban outdoor air pollution in South Africa in 2000. Their results showed that 3.7% of the national mortality from cardiopulmonary diseases and 5.1% of mortality from cancer of the trachea, bronchus, and lungs particularly in adults aged above 30 were attributable to outdoor pollution in urban areas. Based on this, much is desired in the understanding of the temporal variations of air pollutants in rural areas and further estimate of their health-associated risks.
Our Previous study characterized the chemical composition of fine particulate matter in Thohoyandou (Novela et al., 2020), a rural town located in the Limpopo Province of South Africa. From the study, a mean PM2.5 concentration of 10.9 µg/m3 over the sampling period of April 2017 to April 2018 was recorded. Moreover, the daily concentrations were found to exceed the WHO guideline for daily exposure (25µg.m-3) on nine occasions. The study also showed that air mass passing through Thohoyandou contains Pd, Sn, Sb, Mg, Al, and Si as dominant elements. Based on these findings there is a need to estimate the health risks that could be posed by the PM2.5 within the area. This study therefore presents the temporal variations of PM2.5 over the same period of April 2017 to April 2018. Lastly, the study estimates the health risks associated with PM2.5 in Thohoyandou.
2. Materials and Methods
2.1. Study Area
The details of the study area are presented in our earlier publication (Novela et al., 2020). The sampling was carried out at a height of 9 m on the rooftop of the Department of Geography and Environmental Sciences building at the University of Venda. Thohoyandou normally receives seasonal rainfall, with most rainfall occurring mainly during midsummer to the beginning of autumn, with an average of 372 mm/annum (Osidele, 2016).
2.2. PM2.5 Sampling Procedure
This study is a part of the project which was piloted simultaneously in other two cities, Pretoria (Adeyemi et al., 2021) and Cape Town (Williams et al., 2021). Consequently, the same sampling methodology as these studies was employed (Adeyemi et al., 2021). A total of 147 samples were collected in 24 hours from 18 April 2017 to 16 April 2018. Samples were collected on a 3-day interval period with a duplicate sample collected after every 15th day. Before sampling, filter membranes were weighed using ultra-micro balance (mettle-Toledo XP6) batches of 20 at the University of Pretoria. The weighed filters were then hand-delivered to the University of Venda where they were stored in the refrigerator before sampling. After sampling, the filters were hand-delivered to the University of Pretoria, conditioned for 24 hours, and then weighed again. Equations 1, 2, and 3 were used to determine the mass of particulate matter, the volume of the sampled air, and the concentration of PM2.5, respectively.
where (µg) is the mass of the particulate matter, (µg) is the mass of the filter before sampling, (µg) is the mass of the filter after sampling, (µg) is the mass of the control filter, (m3) is the sampled air volume, (l.min-1) is the average flow rate and t (min) time elapsed.
2.3. Human Health Risk Assessment
The human health risk assessment was conducted following USEPA guidelines involving hazard identification (HI), dose-response assessment (DRA), exposure assessment (EA), and risk assessment (RA) as displayed in Figure 1 (USEPA, 2022). The first stage of hazard identification was to account for carcinogenic and non-carcinogenic effects of PM2.5 and the subsequent steps were carried out to calculate those two effects.
Excess lifetime cancer risk (ELCR) for carcinogenic risk and hazard quotient for non-carcinogenic risk in this study were estimated using the equations presented on the Integrated Risk Information System (IRIS) (IRIS, 2022). ELCR involves the estimation of the magnitude of lifetime exposure to PM2.5. The ELCR is given by (Eq. 4):
The SF for ELCR was estimated by Eq. (5):
where, UR = unit risk, IR = inhalation rate (m3.day-1), and BW = body weight (kg). USEPA recommended ELCR values of <1 × 10-6 (USEPA 2007; Heydari et al., 2019).
Lifetime Average daily dose is given by (Eq.6):
where C is the average yearly concentration measured in Thohoyandou.
The non-carcinogenic risks induced by the inhalation of PM2.5 were evaluated by calculating the hazard quotient (HQ):
The HQ value of </= 1 indicates no significant non-carcinogenic effect of PM2.5, whereas the HQ value of >1 indicates a significant non-carcinogenic effect on the exposed population.
where C is the annual WHO guidelines (5 μg.m-3). All these parameters are depicted in Table 1.
Environmental Burden Disease (EBD) due to air pollution was carried out following similar studies (Chalvatzaki et al., 2019). The number of deaths caused by cardiopulmonary and lung cancer diseases due to long-term exposure to PM2.5 is determined using log-linear models (Amoatey et al., 2018). The EBD was calculated using relative risk (RR) which is an estimate of the likelihood of cardiopulmonary and lung cancer mortality in people exposed to PM2.5 higher than the theoretical counterfactual concentration and attributable fractions (AF) which estimates the percentage of deaths from cardiopulmonary and lung cancer disease which could be prevented if PM2.5 levels were lowered to the theoretical counterfactual concentration (Odekanle et al., 2020). RR was calculated using equation 9:
The attributable fractions are given by (Eq. 10):
= mean concentration of the pollutants; = baseline concentration: 5 μg.m-3; β = coefficient of risk function for long-term exposure which is 0.15515 (95% CI; 0.0562–0.2541) and 0.23218 (95% CI: 0.08563–0.37873) for cardiopulmonary and lung cancer mortality respectively.
2.4. Statistical Analysis
RStudio V1.3.1093 software for Windows (Affero General Public License v) was used to analyze the data. The distribution of the data was checked by the Shapiro-Wilk normality test (S-W test). Wilcoxon rank-sum test was used to test the significance of the difference of the PM2.5 concentration measured during weekdays and weekends, whereas Kruskal Wallis was used to test if there is a significant difference between samples measured in different seasons.
3. Results
3.1. Temporal Variation of PM2.5
The descriptive statistics data in terms of weekends, weekdays, seasonally, and annually for PM2.5 is depicted in Table 2. The highest concentrations of PM2.5 were measured during weekdays as compared to weekends (Table 2). However, there is no significant difference in the PM2.5 (p > 0.05) levels between weekdays and weekends. The highest mean PM2.5 level was observed in spring, followed by autumn (Table 2). Statistically, the mean of PM2.5 (p = 0.06) did not differ significantly across the four seasons.
3.2. Health Risk Assessment
Table 3 presents the cancer and non-cancer risks associated with PM2.5 in Thohoyandou. The cancer risk posed by PM2.5 in the ambient air passing through Thohoyandou was found to be 2 × 10−5, 3 × 10−4, and 5 × 10−4 for infants, children, and adults respectively (Table 3). The HQ value for non-carcinogenic risks associated with PM2.5 was found to be 1.91, 3.15, and 1.55 for infants, children, and adults respectively when using WHO guideline (HQa) and 0.61, 1.20, and 0.64 55 for infants, children, and adults respectively when using South African national ambient air quality standards (SANAAQS) (HQb). The ER and AF were calculated for lung cancer mortality and cardiopulmonary mortality for adults aged 30 and above. The ER and AF values for lung cancer mortality are slightly higher (0.17 and 0.15, respectively) (Table 3) compared to the ER and AF values for cardiopulmonary mortality (0.11 and 0.10 respectively).
4. Discussion
Thohoyandou has recorded a low number of exceedances when compared to other cities. A study by Adeyemi et al., (2021) observed three times the number of exceedances in Pretoria, South Africa. This could be because Thohoyandou is the smallest city compared to the other 2 cities. Higher exceedances in spring than in winter were also observed by (Williams, et al., 2021) in Cape Town, South Africa, wherein there were 9 exceedances in spring and 5 exceedances in winter. Higher exceedances in spring are attributable to biomass burning and agricultural activities resulting in increased particulate matter in Thohoyandou (Novela, et al., 2020).
There is no significant difference in air quality in Thohoyandou between weekdays and weekends. The study by Adeyemi et al., (2021) also reported an insignificant difference (P value was greater than 0.05) for the mean level of weekdays and weekends PM2.5 concentrations. Although the study expected higher concentrations during weekdays due to high traffic, they attributed this insignificant difference to other sources of PM2.5 during weekends such as the South African tradition of barbequing (Adeyemi, et al., 2021). In addition, there is also no seasonal change in overall air quality in Thohoyandou. This insignificant difference in air quality seasonally can be attributed to the sources contributing to PM2.5 and PM2.5 components in Thohoyandou not varying seasonally. However, in Pretoria, there was a significant difference (p-value less than 0.001) for the mean level of PM2.5 concentration measured in winter (35.5 µg.m-3), autumn (23.4 µg.m-3), spring (14.3 µg.m-3), and summer (10.7 µg.m-3). Overall the highest concentrations were measured in Pretoria recording the annual mean of 21.1 µg.m-3 (Adeyemi et al., 2021), followed by Cape Town recording an annual mean of 13.3 µg.m-3, and Thohoyandou recording the lowest mean.
The HQ values greater than 1 indicates that the population in Thohoyandou is exposed to higher PM2.5 concentration and is at a higher risk of non-carcinogenic diseases such as neurological, cardiovascular, respiratory, and immune system damage. The HQ values followed a similar trend with the highest HQ values reported in Pretoria (16. 38, 15.03, and 5.04 for infants, children, and adults respectively) (Howlett-Downing et al., 2023), followed by Cape Town (8.73, 8.02 and 2.72 for infants, children and adults respectively) (Alfeus et al., 2022). However both Cape Town and Pretoria studies obtained higher HQ for infants, this is because they calculated the same SAAD across all ages using body weight and inhalation rate values for adults as reference. A study by (Morakinyo et al., 2020) has also reported HQ greater than 1 only for children as well as slightly different HQ for children and infants when SA NAAQS was used. Other studies (Alfeus et al., 2022; Howlett-Downing et al., 2023) also confirms that using SA NAAQS underestimate the effect of PM2.5 on non-carcinogenic risk and recommends that the standards be the same as WHO guideline (Alfeus et al., 2022) or even lowered to 3 µg.m-3 (Edlund et al., 2021), to protect human beings. Children are more susceptible because they have low body weight and higher inhalation rate resulting in higher LAAD and subsequently higher HQ values. Adults have been reported to have low non-carcinogenic risk (Morakinyo et al., 2020; Edlund et al., 2021; Alfeus et al., 2022; Howlett-Downing et al., 2023) this can be attributed to their lower inhalation rate to body weight ratio when compared to that of children and infants, furthermore, adults spends most of their time working indoors. It will be beneficial if the standards can be lowered because children spend a lot of time playing outdoors where they are exposed to higher doses of PM2.5.
The ELCR for all ages in Thohoyandou exceeded the threshold limit value by the USEPA (<1 × 10-6) and WHO (1 × 10-5 - 1 × 10-6). Moreover, the risk of having cancer due to exposure to PM2.5 was opposite the risk of non-carcinogenic diseases, with adults having a higher risk compared to children and infants. It is even higher than the ELCR (3 × 10-5 obtained in Nigeria by Odekanle, et al., (2020), further showing a significant risk for cancer to the general population living in Thohoyandou and surrounding areas. The results indicate that individuals at Thohoyandou will have a higher risk of cancer such as cancer risk than persons who are exposed to a theoretical counterfactual concentration of 5 μg.m-3.
The ER could imply that for an individual in Thohoyandou, there is at least a 0.11% likelihood of having cardiopulmonary disease, and at least 0.17% of having lung cancer higher than an individual who is exposed to the theoretical counterfactual concentration. The AF implies that 0.10% of deaths from cardiopulmonary, and 0.15% from lung cancer could be circumvented if PM2.5 is reduced to the theoretical counterfactual concentration. Although both the ER and AF for lung cancer and cardiopulmonary mortality were lower than what was obtained by Odekanle, et al., (2020) in Nigeria. The community in Thohoyandou is still at higher risk of mortalities due to lung cancer than cardiopulmonary diseases. The study conducted in Ghana by Amoatey et al., (2018) has also shown that individuals in Ghana have a higher risk of lung cancer than cardiopulmonary disease.
5. Conclusion
This study assessed the temporal variation of PM2.5 in Thohoyandou and further assessed the health risk. The study has shown that the residents in Thohoyandou have an excess lifetime cancer risk above the recommended limit by WHO and USEPA. For non-carcinogenic risks, the HQ value for PM2.5 in Thohoyandou is > 1. Moreover, PM2.5 in Thohoyandou could be responsible for 0.11% and 0.17% of deaths resulting from cardiovascular disease and lung cancer respectively. It is recommended that further studies be conducted to estimate the total mortality resulting from cardiopulmonary or lung cancer attributable to exposure to PM2.5 in Thohoyandou.
Author Contributions
This manuscript was part of the MSc. project of Rirhandzu Novela (R.N). Supervision, Prof Wilson Gitari (W.G) and Janine Wichmann (J.W); Sampling, data curation, and analysis R.N; Writing – Original Draft Preparation, R.N.; Writing – Review & Editing, Rabelani Mudzielwana (R.M); Funding Acquisition, J.W and W.G.
Funding
This study was funded by the National Research Foundation grant (CPT160424162937,) and supported by South African Department of Higher Education and Training Research incentive funds (W.M Gitari) and NRF scholarship (R.J Novela).
Data Availability Statement
Data are available upon request.
Disclosure statement: The authors declare no conflict of interest.
References
- Adeyemi, A., Molnar, P., Boman, J., Wichmann, J. Source apportionment of fine atmospheric particles using positive matrix factorization in Pretoria, South Africa. Environ. Monit. Assess. 2021, 193, 716. [CrossRef] [PubMed]
- Ahani, I.K., Salari, M., Shadman, A. An ensemble multi-step-ahead forecasting system for fine particulate matter in urban areas. J. Clean. Prod. 2020, 263, 120983. [CrossRef]
- Alfeus, A, Molnar, P., Boman, J., Shirinde, J., Wichmann, J. Inhalation health risk assessment of ambient PM 2.5 and associated trace elements in Cape Town, South Africa. Hum. Ecol. Risk Assess. Int. J. 2022, 28, 917–929. [CrossRef]
- Amoatey, P., Omidvarborna, H., Baawain, M. The modeling and health risk assessment of PM 2.5 from Tema Oil Refinery. Hum. Ecol. Risk Assess. Int. J. 2018, 24, 1181–1196. [CrossRef]
- Chalvatzaki, E., Chatoutsidou, S., Lehtomäki, H., Almeida, S., Eleftheriadis, K., Hänninen, O., Lazaridis, M. Characterization of Human Health Risks from Particulate Air Pollution in Selected European Cities. Atmosphere 2019, 10, 96. [CrossRef]
- Chen, M., Zhu, H., Chen, Y., Wang, Y. A Novel Missing Data Imputation Approach for Time Series Air Quality Data Based on Logistic Regression. Atmosphere 2022, 13, 1044. [CrossRef]
- Edlund, K.K., Killman, F., Molnár, P., Boman, J., Stockfelt, L., Wichmann, J. Health Risk Assessment of PM2.5 and PM2.5-Bound Trace Elements in Thohoyandou, South Africa. Int. J. Environ. Res. Public Health 2021, 18, 1359. [CrossRef]
- Gumede, P.R., Savage, M.J. Respiratory health effects associated with indoor particulate matter (PM2.5) in children residing near a landfill site in Durban, South Africa. Air Qual. Atmos. Health 2017, 10, 853–860. [CrossRef]
- Heydari, G., Taghizdeh, F., Fazlzadeh, M., Jafari, A.J., Asadgol, Z., Mehrizi, E.A., Moradi, M., Arfaeinia, H. Levels and health risk assessments of particulate matters (PM2.5 and PM10) in indoor/outdoor air of waterpipe cafés in Tehran, Iran. Environ. Sci. Pollut. Res. 2019, 26, 7205–7215. [CrossRef]
- Howlett-Downing, C., Boman, J., Molnár, P., Shirinde, J., Wichmann, J. Health risk assessment of PM 2.5 and PM 2.5-bound trace elements in Pretoria, South Africa. J. Environ. Sci. Health Part A 2023, 58, 342–358. [CrossRef]
- IRIS. The risk assessment information system. 2022.
- Kim, H., Kang, K., Kim, T. Measurement of Particulate Matter (PM2.5) and Health Risk Assessment of Cooking-Generated Particles in the Kitchen and Living Rooms of Apartment Houses. Sustainability 2018, 10, 843. [CrossRef]
- Langerman, K., Pauw, C. A critical review of health risk assessments of exposure to emissions from coal-fired power stations in South Africa. Clean Air J. 2018, 28. [CrossRef]
- Morakinyo, O.M., Mukhola, M.S., Mokgobu, M.I. Ambient Gaseous Pollutants in an Urban Area in South Africa: Levels and Potential Human Health Risk. Atmosphere 2020, 11, 751. [CrossRef]
- Mzezewa, J., Misi, T., Van Rensburg, L. Characterization of rainfall at a semi-arid ecotope in the Limpopo Province (South Africa) and its implications for sustainable crop production. Water SA 2010, 36. [CrossRef]
- Naidoo, R.N., Robins, T.G., Batterman, S., Mentz, G., Jack, C. Ambient pollution and respiratory outcomes among schoolchildren in Durban, South Africa. S. Afr. J. Child Health 2013, 7, 127. [CrossRef] [PubMed]
- Norman, R., Cairncross, E., Witi, J., Bradshaw, D. Estimating the burden of disease attributable to urban outdoor air pollution in South Africa in 2000. S. Afr. Med. J. 2007, 97, 782–790.
- Novela, R.J., Gitari, W.M., Chikoore, H., Molnar, P., Mudzielwana, R., Wichmann, J. Chemical characterization of fine particulate matter, source apportionment, and long-range transport clusters in Thohoyandou, South Africa. Clean Air J. 2020, 30. [CrossRef]
- Odekanle, E.L., Sonibare, O.O., Odejobi, O.J., Fakinle, B.S., Akeredolu, F.A. Air emissions and health risk assessment around abattoir facility. Heliyon 2020, 6, e04365. [CrossRef] [PubMed]
- Osidele, O. An analysis of patterns and trends of road traffic injuries and fatalities in Vhembe District, Limpopo Province, South Africa. University of Venda. 2016.
- Petkova, E.P., Jack, D.W., Volavka-Close, N.H., Kinney, P.L. Particulate matter pollution in African cities. Air Qual. Atmos. Health 2013, 6, 603–614. [CrossRef]
- USEPA. Conducting a human health risk assessment. 2022.
- Wang, B., Yuan, Q., Yang, Q., Zhu, L., Li, T., Zhang, L. Estimate hourly PM2.5 concentrations from Himawari-8 TOA reflectance directly using a geo-intelligent long short-term memory network. Environ. Pollut. 2021, 271, 116327. [CrossRef]
- WHO. Ambient (outdoor) air pollution. 2022.
- WHO. WHO global air quality guidelines. 2021. 2021.
- Williams, J., Petrik, L., Wichmann, J. PM2.5 chemical composition and geographical origin of air masses in Cape Town, South Africa. Air Qual. Atmos. Health 2021, 14, 431–442. [CrossRef] [PubMed]
Figure 1.
The framework for human health risk assessment framework.
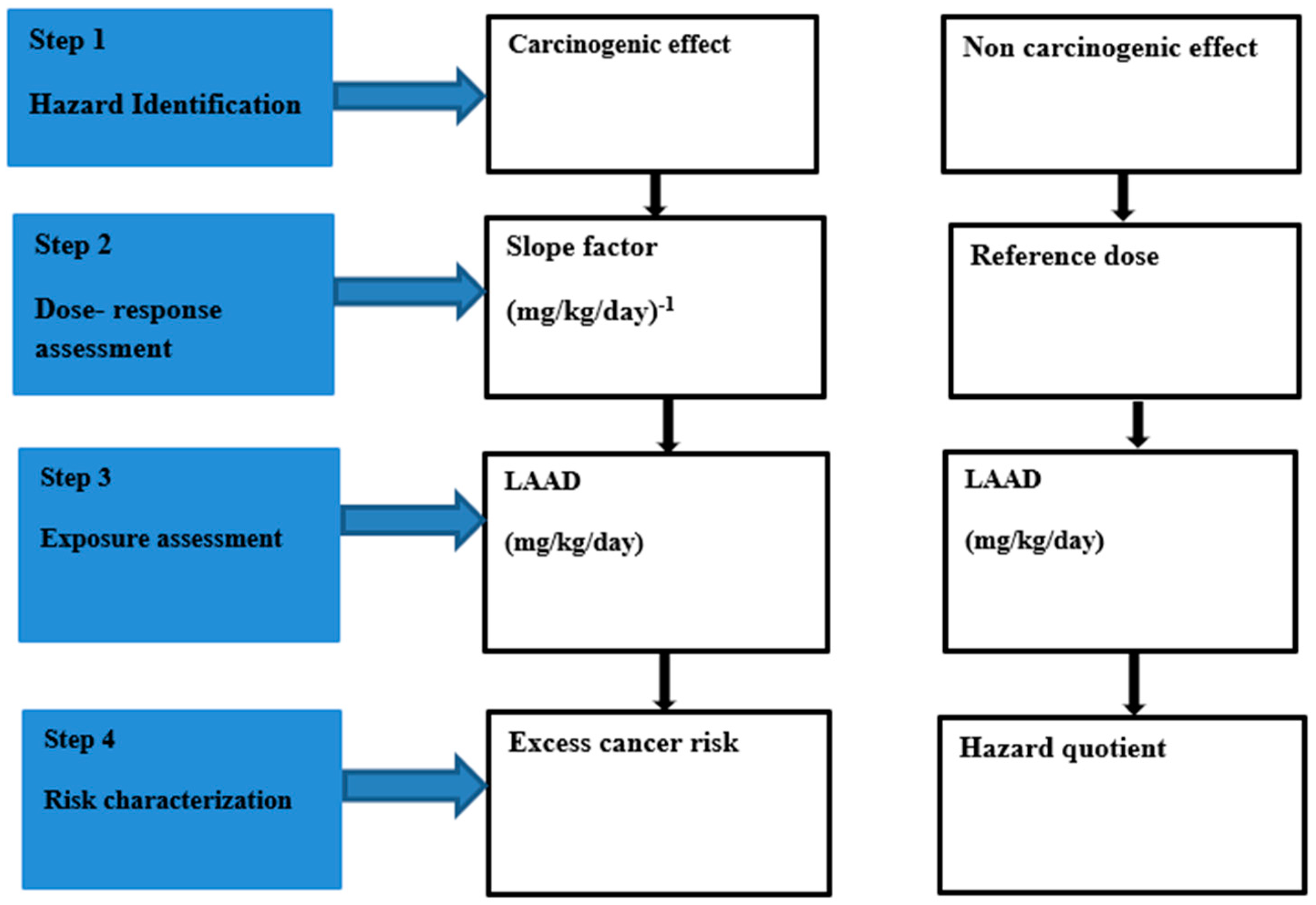

Table 1.
Health risk assessment input data for both carcinogenic and non-carcinogenic effects.
| Parameters | Reference | ||
|---|---|---|---|
| Body weight, BW | Adults | 71.9 kg | (US AID, 2016; Alfeus et al., 2022) |
| Children | 13.8 kg | ||
| Infants | 7.6 kg | ||
| Reference | (Morakinyo et al., 2017) | ||
| Inhalation rate, IR | Adults | 14.9 m3.day-1 | (US EPA, 2011; Alfeus et al., 2022) |
| Children | 9.0 m3.day-1 | ||
| Infants | 5.4 m3.day-1 | ||
| Reference | (Morakinyo et al., 2017) | ||
| coefficient of risk function, β | Cardiopulmonary mortality | 0.15515 | (Ostro, 2004; Norman et al., 2007) |
| lung cancer mortality | 0.23218 | ||
| Unit risk, UR | 0.008 µg.m-3 | (Kim, et al., 2018) |
Table 2.
Descriptive statistics of PM2.5 measured in Thohoyandou, South Africa from 18 April 2017 to 16 April 2018.
Table 2.
Descriptive statistics of PM2.5 measured in Thohoyandou, South Africa from 18 April 2017 to 16 April 2018.
| Mean ±SD | Min-Max | WHO daily guideline Exceedance | P-Value | |
|---|---|---|---|---|
| Weekend | 9.86±8.75 | 1.06-33.57 | 0.18 | |
| Weekday | 11.29±8.519 | 1.35-37.53 | ||
| Autumn | 10.41±7.17 | 1.35-33.57 | 2 | 0.06 |
| Winter | 9.83±8.10 | 1.18-37.53 | 1 | |
| Spring | 14.69±9.53 | 1.06-31.33 | 4 | |
| Summer | 8.64±7.22 | 1.83-34.28 | 2 | |
| Annual | 10.89±8.29 | 1.06-37.53 | 9 |
Table 3.
The health risk posed by PM2.5 in Thohoyandou.
| HQa | HQb | ELCR | ER | AF | |
|---|---|---|---|---|---|
| Adults | 2.59 | 0.64 | 5 × 10-4 | ||
| Children | 4.81 | 1.20 | 3 × 10-4 | ||
| Infants | 2.46 | 0.61 | 2 × 10-5 | ||
| Cardiopulmonary mortality | 0.11 | 0.10 | |||
| lung cancer mortality | 0.17 | 0.15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



