
Submitted:
19 November 2023
Posted:
20 November 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background
There is a considerable overlap between clinical presentation of post-COVID-19 condition (PCC) and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) . Many of their common symptoms can be linked to dysregulation of the autonomic nervous system (dysautonomia). This study aimed to objectively assess autonomic function in patients with PCC and in patients with ME/CFS whose disease was not related to COVID-19.
Methods
Synchronous recordings of an electrocardiogram, continuous dynamics of blood pressure in the digital artery using the Penaz method and ultrasound pneumotachography with the spirography function were obtained with spiroarteriocardiorhythmography method in 34 patients diagnosed with ME/CFS, in whom the onset of the disease was not associated with COVID-19, 29 patients meeting PCC definition and 32 healthy controls. Heart rate variability (HRV), systolic and diastolic blood pressure variability (RV), respiration variability were assessed at rest and in tests with fixed respiratory rates. At rest, indicators of baroreflex regulation were additionally determined (baroreflex effectiveness index and baroreflex sensitivity).
Results
The total power, power of very low frequency, low-frequency and high-frequency of RR interval variability at rest as well as baroreflex effectiveness index in up-ramps of arterial blood pressure and baroreflex sensitivity were significantly lower both in PCC and ME/CFS patients compared to HC. Several diagnostic prediction models for ME/CFS were developed based on HRV parameters. During slow breathing HRV parameters return to normal in PCC, but not in ME/CFS. Correlation analysis revealed a close relationship of HRV, RV parameters and baroreflex sensitivity with fatigue, but not with HADS depressive/anxiety symptoms in ME/CFS and PCC.
Conclusion
A similar pattern of HRV and baroreflex failure with signs of a pathological acceleration of age-dependant dysautonomia was identified in ME/CFS and PCC. The clinical, diagnostic and therapeutic implications of these findings are discussed, in light of previously described relationship between inflammation, vascular pathology, atherosclerotic cardiovascular disease and autonomic dysfunction.
Keywords:
chronic fatigue syndrome
; COVID-19
; Post-COVID
; heart rate variability
; autonomic dysfunction
1. Introduction
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a debilitating disease that is characterized by persistent fatigue and exertional intolerance with disproportionate worsening after physical or cognitive exertion[1]. This marked and prolonged exacerbation of symptoms of ME/CFS is termed post-exertional malaise and may last several days. Other key symptoms include unrefreshing sleep, cognitive impairment, orthostatic intolerance, and pain, including muscle and joint pain and headaches. The symptoms are persistent or recurrent over long periods of time and lead to a significant reduction in previous levels of functioning. Diagnosis is clinical, owing to the absence of biomarkers, and based on detailed clinical history and physical examination by a competent clinician[2]. Up to 75% of people with ME/CFS cannot work full-time and 25% have severe ME/CFS, which often means they are bed-bound, have extreme sensitivity to sensory input and are dependent on others for care. ME/CFS is classified as a chronic neurologic disease and there is a vast collection of biomedical findings regarding this condition, although these are not well known to researchers and clinicians in other fields[3]. The disease in 49–93% of cases is preceded by infection[4]There has been increased interest in ME/CFS recently because of its significant overlap with the post-COVID-19 condition (PCC, also known as long COVID/post-COVID syndrome), with several studies estimating that 58% of patients with PCC fulfill ME/CFS criteria[5]. PCC was officially recognised by WHO in October 2021, and a clinical case definition was developed in a Delphi process. According to this definition, “post-COVID-19 condition occurs in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually 3 months from the onset, with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis. Common symptoms include, but are not limited to, fatigue, shortness of breath, and cognitive dysfunction, and generally have an impact on everyday functioning. Symptoms might be new onset following initial recovery from an acute COVID-19 episode or persist from the initial illness. Symptoms might also fluctuate or relapse over time”[6]. There is evidence for a close relationships between ME/CFS and PCC regarding the key mechanisms (neuroinflammation, dysautonomia and vascular pathology). In particular, as summarized by Komaroff and Lipkin[7] autonomic dysfunction have been well documented in both ME/CFS and PCC. Significant platelet hyperactivity and endothelial dysfunction as well as circulatory disorders were documented both in PCC and ME/CFS, although in PCC possible pro-atherogenic evidences were registered [8], while in ME/CFS (also related to viral etiology) the circulatory disorders look like non-atherosclerotic cardiological disease and “it seems that neurological (autonomic) dysfunction underlies these abnormalities”[9]. Abnormalities of both the sympathetic and parasympathetic arms of the autonomic nervous system have been reported, with the imbalance favoring expression of the sympathetic system. However, to the best of our knowledge there is no studies which compare ME/CFS and PCC in terms of the objective parameters of autonomic dysfunction.
2. Materials and Methods
2.1. Participants
In this study three group of subjects were involved (34 patients with ME/CFS, that was not related to COVID-19; 29 patients with PCC; 32 healthy controls (HC)). Patients with ME/CFS were included in the study if they met all three of the most commonly used sets of ME/CFS diagnostic criteria (Fukuda et al. (1994) CFS criteria[10], the Canadian Consensus criteria of ME/CFS (2003) [1], and US Institute of Medicine, now called the National Academy of Medicine (IOM/NAM) criteria (2015) [11]). The details of the diagnostic processes can be found in the literature [2]. The diagnosis of PCC was defined based on the WHO criteria [6]. Age- and sex-matched HC who denied chronic fatigue were recruited through word-of-mouth from the local community. The common exclusion criteria for all groups were as follows: age of <18 or >60 years; cardiac arrhythmias; structural heart diseases; current usage of beta-blockers; any acute illness during the last month before the study. The study was approved by the biomedical Ethics Committee of I.P. Pavlov First Saint Petersburg State Medical University. All participants gave informed consent.
2.2. Measures
2.2.1. Symptom Assessment Tools
The Multidimensional Fatigue Inventory (MFI) and Hospital Anxiety and Depression Scale (HADS) were used to assess symptoms in all participants. The MFI comprises a 20-item self-reported questionnaire focused on general, physical and mental fatigue, reduced activity, and reduced motivation[12]. HADS is a reliable scale for identifying and assessing the symptom severity in anxiety disorders and depression, both in patients with somatic diseases and in patients with mental disorders[13]. The score 0–7 for each subscale (depression and anxiety symptoms) indicated “normal results”; 8–10—“borderline results, or doubtful case of anxiety/depression”; 11 or more—“probable case of anxiety/depression”.
2.2.2. Assessment of Autonomic Nervous System Function
The integrated method of studying the cardiorespiratory system – spiroarteriocardiorhythmography (SACR) ("Intox", Russia) - was applied to analyse heart rate variablitiy (HRV), arterial blood pressure variability (BPV) and respiratory pattern. This device was recommended for use in medical practice by the Ministry of Health of Russia (registration certificate No 29/03020703/5869-04) and combines three physiological methods into an integrated hardware complex. R-R interval data was recorded using a three-lead electrocardiogram (Lead I configuration). HRV was analyzed applying a simple Fourier transform, obtaining a spectrum distribution curve of the frequency changes in heart rate. The total power of HRV was calculated (TP), as well as three standard components of the spectrum: very low-frequency oscillations (HRV_VLF, 0-0,04 Hz), low-frequency oscillations (HRV_LF, 0,04-0,15 Hz) and high-frequency oscillations (HRV_HF, 0,15-0,4 Hz). Beat-to-beat blood pressure was collected using the Penaz’s method with the finger cuff placed around the left middle finger. Similarly to HRV, the total power of the spectrum of systolic (SBPV_TP, mmHg2 ) and diastolic (DBPV_TP, mmHg2) blood pressure and their frequency components were calculated.The ultrasonic sensor of the SACR device allows to measure flows of air on inspiration and expiration and to define the average parameters of a respiration pattern and calculate the parameters of respiration variability (RV): total power of respiration (RV_TP, (L×min–1)2), respiration power in the very low-frequency range (RV_VLF (L×min–1)2), respiration power in the low-frequency range (RV_LF (L×min–1)2) and respiration power in the high frequency range (RV_HF (L×min–1)2)[14]
Subjects were tested in a quiet room in the sitting position. Recordings were made during: a) spontaneous breathing (5 min); b)controlled breathing at 0.2 Hz (i.e., 12 breaths/min for 2 min); c)controlled breathing at 0.1 Hz (i.e., 6 breaths/min for 2 min). All recordings were manually analyzed for the presence of artefacts.
Baroreflex sensitivity (BRS) was determined using the sequence method using artefact-free heart rate and blood pressure recordings at spontaneous breathing. The sequence method involves manual detection of up sequences, which are sequences of increases in SBP corresponding to lengthening of the R–R interval over three or more consecutive heart beats and down sequences or decreases in SBP corresponding to shortening of the R–R interval. BRS was determined by the change in R–R interval (ms) over the change in SBP (mmHg). The baroreflex effectiveness index (BEI) was calculated as the ratio between the number of SBP ramps associated with corresponding changes in R–R interval within two heart beats to the total number of SBP ramps. The mean BRS and BEI for up ramps and down ramps are presented separately, as well as cumulatively as total ramps[15].
2.3. Statistical Analysis
Statistical processing was performed with the Statistica 10.0 software package. Results are shown as median (percentile 25–percentile 75). Differences in the distribution of qualitative variables were determined with the Chi-square test, while the differences in quantitative variables were determined with the use of the nonparametric Mann–Whitney test. The strength and significance of the correlation between selected variables were calculated using the nonparametric Spearman’s test. The multiple regression models and one-factor regression models, based on HRV and RV parameters, were used in order to determine significant predictors for the diagnosis of ME/CFS. The ROC curve analysis was used to determine the appropriate cut-off values of HRV and RV parameters. The level of significance for all tests was set at p < 0.05.
3. Results
3.1. Demographic and Clinical Characteristics of Participants
Table 1 shows descriptive statistics for patients with ME/CFS, patients with PCC and participants in the control group. There were no differences between the groups in terms of age, gender and body mass index (BMI).
ME/CFS and PCС patients experienced significant fatigue on all subscales of MFI-20, with the obvious difference from HC. The patients had also higher scores of anxiety and depression (HADS) and lower level of physical activity (total IPAQ score) compared with HC (Table 1).
3.2. Baseline Variability Indices
The frequency-domain analysis of RR intervals revealed significantly lower values for all analysed HRV parameters (except for LF/HF index) in PCC patients compared to the HC (Table 2). Similar results were obtained for the group of ME/CFS patients, and the differences in HRV parameters between ME/CFS and HC were even more pronounced. Additionally, ME/CFS patients had higher values of LF/HF than the controls.
The spectral analysis of beat-to-beat arterial blood pressure revealed no differences between that ME/CFS or PCC patients and healthy controls in any of the frequency-domain parameters. Regarding RV parameters, patients with ME/CFS showed significantly higher TP and HF power than HC.
3.3. Variability Indices during Breathing at 12 Breaths Per Minute
Compared spontaneous breathing, traditional spectral analysis showed decreased LF power, and increased HF power of HRV at 12 breaths/minute in all three groups (P < .05, see Figure 1a, b, c). TP of HRV decreased only in healthy controls. This decline in HC was mostly due to decreased VLF power, which could not be analysed in short-term HRV recordings. TP and HF power of RV increased in all groups (P < .05, see Figure 1 d, e, f)
It should be noticed that patients with ME/CFS still had significantly lower TP, LF and HF components of HRV compared to HC. A similar trend was observed for PCC patients, who still differed from healthy controls in terms of LF and HF HRV components but showed comparable TP values. Regarding RV parameters, no significant difference existed at 12 breaths/minute between groups. At the same time some differences in SBPV and DBPV between ME/CFS and HC, and to the lesser extent between PCC and HC have appeared (Table 3).
3.4. Variability Indices during Breathing at 6 Breaths per Minute
Compared spontaneous breathing, traditional spectral analysis showed increased TP and LF power of HRV at 6 breaths/minute in all three groups (P < .05, see Figure 1a, b, c). HF power of HRV increased only in ME/CFS and PCC groups. TP and LF power of RV increased, and HF power of RV decreased in all groups (P < .05, see Figure 1 d, e, f)
At this respiration rate patients with ME/CFS still had significantly lower TP and LF components of HRV compared to HC, but HF was comparable. PCC patients showed all HRV values comparable with healthy controls. Regarding RV parameters, ME/CFS and PCC patients had higher TP and LF power, and PCC patients had also higher HF power at 6 breaths/minute than healthy controls. Only HF power os SBPV in ME/CFS group differed from HC (Table 3).
3.5. Multifactorial Logistic Regression Analysis in ME/CFS Group
A logistic regression was performed to ascertain HRV and RV parameters with p value <0.05 on the likelihood that participants have ME/CFS. Two multifactorial models were created, based on two different methods of variable selection. Model 1, which was based on forward stepwise logistic regression, included TP of HRV and TP of RV at spontaneous breathing. Model 2, which was based on backward Wald selection, retained LF of HRV, TP of RV at spontaneous breathing, and HF of HRV at 12 breaths/minute (Table 4).
There was no collinearity between the parameters included in these models as variance inflation factor (VIF) scores were well below 10. One-factor regression models, based on each significant (p value <0.05) HRV and RV parameter were also created. Two of these one-factor models had AUCROC>0.8 and were included in the comparison with multifactorial models (Table 5, Figure 2).
3.6. Correlations of Heart Rate, Arterial Blood Pressure and Respiration Variability Parameters with Clinical Characteristics in Patient Groups
Spearman correlation test was performed separately in ME/CFS, PSC and HC groups to detect correlations between variability parameters and clinical characteristics (five domains of fatigue according to MFI-20; depression and anxiety according to HADS; age; BMI; physical activity according to IPAQ). The analysis showed considerably different patterns between three groups (Table 6). Heart, arterial blood pressure and respiration variability parameters had a number of correlations with general fatigue and physical fatigue in ME/CFS and PCC groups, but not in healthy controls. In general, HRV had negative and SBPV, DBPV had positive correlations with fatigue. Notably, that fatigue showed much more correlations with variability parameters than with depression. Patients with higher BMI (but not healthy participants) were characterized with higher RV. At the same time, RV had opposite correlations with anxiety in ME/CFS and in PCC. Physical activity level did not show any correlation with HRV or clinical characteristics in ME/CFS or HC but correlates negatively with general fatigue and physical fatigue in patients with PCC.
3.7. Baroreflex Sensitivity and Baroreflex Effectiveness Index
BRS was significantly lower in patients with ME/CFS and PCC compared to HC both for up and down SBP ramps (Table 7). Interestingly, that BEI was reduced only in up SBP ramps in both groups of patients.
Spearman correlation test was performed separately in ME/CFS, PSC and HC groups to detect correlations between BRS, BEI_up and clinical characteristics (five domains of fatigue according to MFI-20; depression and anxiety according to HADS; age; BMI; physical activity according to IPAQ). In HC BRSup correlated negatively with age (-0.406) and BEI_up - with activity domain of fatigue according to MFI-20 (-0.416), but not with the level of physical activity according to IPAQ. In ME/CFS only fatigue domains showed significant correlation with BRSup, BRSdown, BRSmean (-0.559, -0.394 and -0.546 respectively with general fatigue domain of MFI-20) and BEI_up (- 0.404 - with motivation domain of fatigue in MFI-20). In PCC no significant relationships were found.
4. Discussion
This study assessed autonomic function at rest, during breathing at 12 breaths per minute and during breathing at 6 breaths per minute in patients with PCC and in patients with ME/CFS whose disease was not related to COVID-19. Correlation analysis of HRV indices with clinical features of the patients was performed to better understand determinants of autonomic dysfunction or its contribution to the clinical presentation. The obtained HRV indices was used to develop a multifactorial model for predicting likelihood of ME/CFS diagnosis. Assessment of baroreflex function enable deeper insights into the pathogenesis of orthostatic intolerance in both PCC and ME/CFS.
First of all, it should me noted that study groups were matched by age, gender and BMI to eliminate the influence of these factors on HRV and baroreflex function. All patients and controls were under 60 years old which enable us not to make allowances on aging of the autonomic nervous system. Patients with PCC and ME/CFS were significantly more anxious and depressed than HC according to HADS, however median level of both anxiety and depression in patients’ groups corresponded to the subclinical level (i.e. did not warrant treatment but may nevertheless interfere with an individual's ability to function effectively). At the same time, MFI-20 subscales scores in both patients group were similar and corresponded to the severe fatigue. Patients were less physically active than HC according to the IPAQ. In our study patients with PCC were comparable with ME/CFS patients and more physically active than patients with PCC in the study of Twomey et al (the authors reported 503 (99-1361) MET-min/week total IPAQ score in patients with long COVID).
Although LF/HF ratio was higher in ME/CFS (but not in PCC) than in HC, absolute values of LF, HF and VLF in ME/CFS and PCC were lower than in healthy subjects. This observation could indicate reduced sympathetic and parasympathetic activity in ME/CFS and PCC at rest, with the shift to the sympathetic predominance in ME/CFS, while in PCC sympatho/vagal balance is maintained. However, there are serious doubts about the assessment of cardiac autonomic nervous functions through the analysis of HRV frequency components (LF and HF)[15]. Particularly, the framework to associate LF and HF with the divisions of the autonomic nervous system (sympathetic and parasympathetic) is already too simplistic. To date, it is known that two major components in short-term HRV are respiratory sinus arrhythmia (RSA) and a fluctuation at ~ 0.1 Hz (which corresponds to LF band) called Mayer wave sinus arrhythmia. The mechanism mediating the heart rate fluctuation at ~ 0.1 Hz is believed to be the baroreceptor reflex cardiovascular regulation system, by which the fluctuation of arterial blood pressure at ~ 0.1 Hz that are known as Mayer waves is reflected in the fluctuation of heart rate[15]. As LF is related to baroreflex function, a decreased LF HRV, which is is constantly reported in ME/CFS, could reflect baroreflex failure and encouraged us to perform beat-to-beat measures of HR and BP in order to confirm this hypothesis.
Regarding the second mechanism of short-term HRV, respiration modulates the heart rate creating excess power in the HRV at a frequency equal to the respiratory rate, a phenomenon known as RSA, which has been associated with the efficiency of pulmonary gas exchange[15]. RSA is generated by the oscillation of firing in cardiac vagal motor neurons, which are inhibited during inspiration and excited post inspiration[16]. Natural breathing rates between 10 and 24 cycles per minute (0,16-0,4 Hz) allows to estimate parasympathetic activity by HF HRV power, since RSA at this breathing rate corresponds to HRV HF band and does not overlap with LF HRV band.
Our results for the comparison of HRV indices between spontaneous breathing rate and during breathing at 12 breaths per minute (i.e.the increase in HF power and decrease in LF power in all three groups) are in line with the statement of the separation of two major sources of HRV (RSA and Mayer wave sinus arrhythmia) by frequency bands at this respiratory rate. Therefore, decreased LF and HF HRV in ME/CFS and PCC compared to HC at 12 breaths per minute confirmed reduced parasympathetic activity and give additional evidence for baroreflex failure in both patients group.
It is very important to take into consideration individuals’ breathing rate when HF and LF components of HRV are interpreted as indicators of parasympathetic and sympathetic nervous system activity. Thus, for athletes, who breathe more slowly (for example at 6 cycles per minute, which corresponds to a frequency of 0.1 Hz), vagal-related power would shift from HF into LF[17], resulting in overestimation of the SNS contribution and underestimation of the PNS contribution in traditional HRV framework. But the exact mechanism of the LF increase in this case is not the increase of sympathetic activity, but the synchronization of RSA with the baroreflex frequency[17].
Maximization of HRV at around 6 breaths per min due to LF power has been confirmed by numerous studies[18]. This indicates cardiorespiratory system resonance, and slow breathing (∼6 breaths per min) is hence referred to as a “resonance breathing”, though this resonant frequency does vary between individuals (4-7.5 breaths per min)[18]. Slow breathing has been shown to benefit health and performance within clinical and non-clinical populations. EEG studies show an increase in alpha and a decrease in theta power. FMRI study highlights increased activity in cortical (e.g., prefrontal, motor, and parietal cortices) and subcortical (e.g., pons, thalamus, sub-parabrachial nucleus, periaqueductal gray, and hypothalamus) structures. Psychological/behavioral outputs related to the abovementioned changes are increased comfort, relaxation, pleasantness, vigor and alertness, and reduced symptoms of arousal, anxiety, depression, anger, and confusion[19].
In our study the effect of slow breathing (6 breaths/minutes) on HRV in patients and HC was consistent with earlier studies[18], which implies the integrity of positive effects of slow breathing (and in particular resonance frequency breathing) in ME/CFS and PCC. Moreover, our results suggest that slow breathing has a therapeutic potential regarding PCC since HRV parameters in this group at 6 bresths/min increased to the level of HC. Autonomic dysfunction in ME/CFS is presumably more profound than in PCC, since in ME/CFS it has not resolved during breathing at 6 breaths/min.
In view of the observed great difference in HRV parameters between ME/CFS and HC as well as the absence of clinically available diagnostic test for ME/CFS, we used multifactorial logistic regression analysis to created two multifactorial models for the prediction of ME/CFS based on HRV parameters. However, two single-factor models based on TP of HRV and HF of HRV at spontaneous breathing showed AUC, sensitivity and specificity comparable with multifactorial models. The most optimal model, in our view, is based on HF HRV at spontaneous breathing and shows 81.3% sensitivity and 79.4% specificity for the differentiation of ME/CFS from HC (with the cut-off 286.95 ms2).
Correlation analysis allowed to reveal some important differences between patients and HC. First of all, depression and anxiety were associated with fatigue only in HC, but not in ME/CFS or PCC. The association of fatigue with depressive is well-known and a differential diagnosis of MEC/CFS or CC with depression is often difficult due to the overlapping psychological and somatic symptoms in both disorders, including fatigability, a lowering of concentration, and sleep disturbance. Our study showed that fatigue is not related to depression/anxiety in ME/CFS and PCC.
Depression was not associated with HRV parameters in any study groups, while anxiety was inversely correlated with HRV-HF at spontaneous breathing in HC. Since as have been mentioned above, low HRV-HF was characteristic of ME/CFS an PCC, one may presume that low HRV-HF in HC with subclinical anxiety represents a risk factor for post-infectious fatigue syndromes. Correlations of “general fatigue” and “physical fatigue” domains of MFI20 are the most indicative for the hypothesis that fatigue in ME/CFS and PCC is related to the autonomic dysfunction in contrast to HC, where depression/anxiety are the most common causes of fatigue. In general, lower HRV and higher SBPV/DBPV in patients were associated with more pronounced fatigue. These results are in line with previous studies which have been scarce, but reported similar relationships[20,21,22]
Interestingly, that in our study some HRV and SBPV parameters (which were associated with greater fatigue only in patients’ groups), both in patients and HC were correlated with age, while the age itself was not correlated with any domain of fatigue. These findings could be interpreted as evidence for the existence of age-related autonomic dysfunction, which is accelerated in ME/CFS and PCC. A similar pattern was observed for another measure of autonomic cardiovascular control - baroreceptor reflex. BRS reflects the complex interaction between the cardiac, vascular and autonomic function to manage the blood pressure fluctuations of daily life within normal levels. The afferents arising from the arterial baroreceptors terminate in the nucleus tractus solitarii of the brain stem, which activates vagal motor neurons and inhibits spinal sympathetic neurons. When the BP rises, the baroreflex stimulates vagal cardiac activity (increase of HRV), inhibits β1-adrenergic efferents to the myocardium (reduction of contractility), and reduces α-adrenergic outflow to the vasculature (vasodilation). Conversely, when the BP decreases, the opposite change occurs, such that the reflex buffers short-term BP fluctuations.
A close relationship between orthostatic intolerance, fatigue, cognitive impairment, chronic pain and baroreflex failure has been recently reported[23,24].
Our results are in line with these observations, since baroreflex failure was detected both in ME/CFS and PCC patients. However, in patients with PCC baroreflex failure was not correlated with fatigue, in contrast to ME/CFS. It should be noticed that there are conflicting data on the presence of baroreflex failure in PCC in the literature[25]. The negative correlation of BRSup with age in HC (but not in ME/CFS where it was correlated only with the severity of fatigue) gives another evidence for the hypothesis of the accelerated ageing of autonomic nervous system in ME/CFS. .
The decreased BEI in ME/CFS and PCC only in up SBP ramps could represent a new mechanism for the higher risk of POTS and inappropriate sinus tachycardia in these group of patients.
Several potential mechanisms connecting abnormal baroreflex to fatigue and cognitive impairment has been suggested, including reduced or dysregulated cerebral perfusion, the effects of decreased vagal afferent input to the nucleus tractus solitarii on higher cortical networks[24], and deactivation of physiological baroreflex-induced reduction of systemic inflammation and neuroinflammation[26,27]
The last mechanism let us to discuss in more detail a close relationship between neuroinflammation, cardiac autonomic dysfunction and vascular pathology,
Inflammation is defined as a typical pathological process involving the immune system in response to [vascularized] tissue injury or invasion by pathogens, resulting in tissue repair and/or pathogen elimination[28]
Inflammatory responses that are centralized within the brain and spinal cord are generally referred to as “neuroinflammation”. Neuroinflammation is the innate and adaptive immune responses that are initiated toward a variety of harmful insults (such as infection, ischemia, stress, and trauma) through the release of inflammatory mediators (such as cytokines, chemokines, and reactive oxygen species) by various immune cells (like microglia, astrocytes, peripherally derived immune cells, and endothelial cells). Neuroinflammation in the initial stage is mainly beneficial and protective; however, evidence from both clinical and experimental studies indicates that prolonged or excessive inflammation is a pivotal pathological driver of several neurological disorders, such as cerebrovascular diseases, traumatic brain and spinal cord injuries, neurodegenerative diseases, epilepsy, multiple sclerosis, psychological disorders, and chronic pain. Therefore, neuroinflammation is the common mechanism that connects ischemic, degenerative, traumatic, demyelinating, epileptic, and psychiatric pathologies[29]. It has been also reported in ME/CFS[30] and PCC[31].
The change in autonomic nervous system activity against the background of neuroinflammation may be a potential intermediate link between microglia and cardiovascular diseases[32]. The ANS innervates vascular walls and regulates contractility and tension. Therefore, autonomic dysfunction may exert detrimental effects on endothelial and vascular tissues, favoring atherogenesis. The relation between dysautonomia and atherosclerotic cardiovascular disease mortality has been documented [33]. Subclinical atherosclerosis risk factors and markers were associated with signs of dysautonomia in general populations of various ethnic origin [34,35]. Sympathetic hyper-activation leads to vasoconstriction, loss of vascular elasticity, accumulation of modified lipoproteins in the vascular wall. It also increases peripheral vascular resistance, induces endothelial dysfunction, stimulates oxidative stress, and vascular remodelling, and favors micro- and macro-calcification in both the vascular intima and media[36,37]. Sympathetic hyper-activation also favors pro-inflammatory and prothrombotic effects[36] driven by cytokines, chemokines, and other biologically active mediators, while parasympathetic branch of autonomic nervous system plays an anti-inflammatory effects mediated by the so called cholinergic anti-inflammatory pathway, This pathway is characterized by signals communicated via the vagus nerve (with the possible involvement of the splenic nerves) through acetylcholine release to down-regulate the inflammatory actions of macrophages, key players of inflammaging[38]. Hypothalamic–pituitary–adrenal axis is another pathway related to ANS, which promotes some anti-inflammatory response mainly through increased cortisol levels (notably, that this mechanism is also impaired in ME/CFS [39]). In line with these pathophysiological mechanisms, reduced HRV predicted the severity, extent and progression of human coronary atherosclerosis , even in asymptomatic subjects[40,41].
In conclusion, we obtained evidence for the similar pattern of HRV, blood pressure variability and baroreflex failure in ME/CFS and PCC, which can be interpreted as a pathological acceleration of age-dependant dysautonomia and applied for the diagnosis of ME/CFS. Correlation analysis revealed a close relationship between fatigue and parameters which objectively prove dysautonomia in ME/CFS and PCC, but not with mental problems. Since neuroinflammation has been addressed as one of the most important mechanism of ME/CFS and PCC pathogenesis, we discussed dysautonomia in a broad context of neuroinflammation and drew attention to the potential negative vascular consequences of this conditions.
Author Contributions
Conceptualization, V.A.R., V.N.M., V.I.T., L.P.C.; methodology, V.A.R., A.V.R.; formal analysis, V.A.R.; investigation, V.A.R., A.V.R.; resources, V.N.M., V.I.T., L.P.C.; writing—original draft preparation, V.A.R.; writing—review and editing, L.P.C.; visualization, V.A.R.; supervision, L.P.C.; project administration, V.I.T., L.P.C.; funding acquisition, L.P.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the grant of the Russian Scientific Foundation of the Russian Academy of Sciences No. 075-15-2022-1110 dated 30.06.2022.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of I.P. Pavlov First Saint Petersburg State Medical University (protocol code 261, date of approval 25.04.2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
We authors would like to express our deepest gratitude to the patients who suffered from ME/CFS and post-COVID-19 condition and found the strength to take part in the study (especially in the very beginning, when few specialists recognize the importance of the studied conditions), and provided new ideas for research in the area.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Carruthers BM, Jain AK, De Meirleir KL, Peterson DL, Klimas NG, Lerner AM, et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J Chronic Fatigue Syndr 2003, 11, 7–115. [CrossRef]
- Nacul L, Jérôme Authier F, Scheibenbogen C, Lorusso L, Bergliot Helland I, Alegre Martin J, et al. European Network on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (EUROMENE): Expert Consensus on the Diagnosis, Service Provision, and Care of People with ME/CFS in Europe. Medicina (B Aires) 2021, 57, 510. [CrossRef] [PubMed]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol 2023, 21, 133–46. [Google Scholar] [CrossRef]
- Chu, L.; Valencia, I.J.; Garvert, D.W.; Montoya, J.G. Onset patterns and course of myalgic encephalomyelitis/chronic fatigue syndrome. Front Pediatr 2019, 7, 427132. [Google Scholar] [CrossRef]
- Jason LA, Dorri JA. ME/CFS and Post-Exertional Malaise among Patients with Long COVID. Neurol Int 2023 2022, 15, 1–11. [CrossRef] [PubMed]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis 2022, 22, e102–7. [Google Scholar] [CrossRef] [PubMed]
- Komaroff AL, Lipkin WI. ME/CFS and Long COVID share similar symptoms and biological abnormalities: road map to the literature. Front Med 2023, 10, 1187163. [CrossRef] [PubMed]
- Macarova JA, Malakhova SA, Novitskaya TA, Shapkina VA, Churilov LP. COVID-19 and Vasa vasorum: New Atherogenic Factor? A Case Report and Autopsy Findings. Diagnostics (Basel). 2023, 13, 1097. [CrossRef] [PubMed]
- Nunes JM, Kell DB, Pretorius E. Cardiovascular and haematological pathology in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): A role for viruses. Blood Rev. 2023, 60, 101075. [CrossRef]
- Fukuda K, Straus SE, Hickie I, Sharpe MC, Dobbins JG, Komaroff A. The Chronic Fatigue Syndrome: A Comprehensive Approach to Its Definition and Study. Ann Intern Med 1994, 121, 953. [CrossRef]
- IOM (Institute of Medicine). Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. Washington, DC, USA: National Academies Press; 2015. [CrossRef]
- Smets, E.M.A.; Garssen, B.; Bonke, B.; De Haes, J.C.J.M. The multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom Res 1995, 39, 315–25. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale: An updated literature review. J Psychosom Res 2002, 52, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Romanchuk, A.; Guzii, O. Variability and Pattern of Spontaneous Respiration in Different Types of Cardiac Rhythm Regulation of Highly Trained Athletes. Int J Hum Mov Sport Sci 2020, 8, 483–93. [Google Scholar] [CrossRef]
- Di Rienzo, M.; Parati, G.; Castiglioni, P.; Tordi, R.; Mancia, G.; Pedotti, A. Baroreflex effectiveness index: an additional measure of baroreflex control of heart rate in daily life. Am J Physiol Regul Integr Comp Physiol 2001, 280. [Google Scholar] [CrossRef] [PubMed]
- Skytioti, M.; Elstad, M. Respiratory Sinus Arrhythmia is Mainly Driven by Central Feedforward Mechanisms in Healthy Humans. Front Physiol 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Saboul, D.; Pialoux, V.; Hautier, C. The breathing effect of the LF/HF ratio in the heart rate variability measurements of athletes. Eur J Sport Sci 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Russo, M.A.; Santarelli, D.M.; O’Rourke, D. The physiological effects of slow breathing in the healthy human. Breathe (Sheffield, England) 2017, 13, 298–309. [Google Scholar] [CrossRef] [PubMed]
- Zaccaro A, Piarulli A, Laurino M, Garbella E, Menicucci D, Neri B, et al. How Breath-Control Can Change Your Life: A Systematic Review on Psycho-Physiological Correlates of Slow Breathing. Front Hum Neurosci 2018, 12. [CrossRef] [PubMed]
- Frith J, Zalewski P, Klawe JJ, Pairman J, Bitner A, Tafil-Klawe M, et al. Impaired blood pressure variability in chronic fatigue syndrome—a potential biomarker. QJM An Int J Med 2012, 105, 831–8. [CrossRef]
- Escorihuela RM, Capdevila L, Castro JR, Zaragozà MC, Maurel S, Alegre J, et al. Reduced heart rate variability predicts fatigue severity in individuals with chronic fatigue syndrome/myalgic encephalomyelitis. J Transl Med 2020, 18, 1–12. [CrossRef]
- Boissoneault, J.; Letzen, J.; Robinson, M.; Staud, R. Cerebral blood flow and heart rate variability predict fatigue severity in patients with chronic fatigue syndrome. Brain Imaging Behav 2019, 13, 789–97. [Google Scholar] [CrossRef] [PubMed]
- Reyes del Paso, G.A.; Contreras-Merino, A.M.; de la Coba, P.; Duschek, S. The cardiac, vasomotor, and myocardial branches of the baroreflex in fibromyalgia: Associations with pain, affective impairments, sleep problems, and fatigue. Psychophysiology 2021, 58, e13800. [Google Scholar] [CrossRef] [PubMed]
- Mueller, B.R.; Ray, C.; Benitez, A.; Robinson-Papp, J. Reduced cardiovagal baroreflex sensitivity is associated with postural orthostatic tachycardia syndrome (POTS) and pain chronification in patients with headache. Front Hum Neurosci 2023, 17. [Google Scholar] [CrossRef] [PubMed]
- Skow RJ, Garza NA, Nandadeva D, Stephens BY, Wright AN, Grotle AK, et al. Impact of COVID-19 on cardiac autonomic function in healthy young adults: potential role of symptomatology and time since diagnosis. Am J Physiol Hear Circ Physiol 2022, 323, H1206–H1211. [CrossRef] [PubMed]
- Brognara, F.; Castania, J.A.; Kanashiro, A.; Dias, D.P.M.; Salgado, H.C. Physiological Sympathetic Activation Reduces Systemic Inflammation: Role of Baroreflex and Chemoreflex. Front Immunol 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Amorim MR, de Deus JL, Pereira CA, da Silva LEV, Borges GS, Ferreira NS, et al. Baroreceptor denervation reduces inflammatory status but worsens cardiovascular collapse during systemic inflammation. Sci Reports 2020 101 2020, 10, 1–13. [CrossRef] [PubMed]
- Okin, D.; Medzhitov, R. Review Evolution of Inflammatory Diseases. Curr Biol 2012, 22, R733–R740. [Google Scholar] [CrossRef]
- Gorji, A. Neuroinflammation: The Pathogenic Mechanism of Neurological Disorders. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef] [PubMed]
- Tate, W.P.; Walker, M.O.M.; Peppercorn, K.; Blair, A.L.H.; Edgar, C.D. Towards a Better Understanding of the Complexities of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Long COVID. Int J Mol Sci 2023, 24, 5124. [Google Scholar] [CrossRef]
- Braga J, Lepra M, Kish SJ, Rusjan PM, Nasser Z, Verhoeff N, et al. Neuroinflammation After COVID-19 With Persistent Depressive and Cognitive Symptoms. JAMA Psychiatry 2023, 80, 787–95. [CrossRef]
- Wang, M.; Pan, W.; Xu, Y.; Zhang, J.; Wan, J.; Jiang, H. Microglia-Mediated Neuroinflammation: A Potential Target for the Treatment of Cardiovascular Diseases. J Inflamm Res 2022, 15, 3083–94. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, M.G. Atherosclerosis and Blood Pressure Variability. Hypertension. 2018, 71, 403–405. [Google Scholar] [CrossRef] [PubMed]
- Zambach C, Fedorowski A, Gerward S, Johansson M, Engström G, Hamrefors V. Subclinical atherosclerosis and risk factors in relation to autonomic indices in the general population. J Hypertens. 2023, 41, 759–767. [CrossRef] [PubMed]
- akahashi M, Miyai N, Nagano S, Utsumi M, Oka M, Yamamoto M, Shiba M, Uematsu Y, Nishimura Y, Takeshita T, Arita M. Orthostatic Blood Pressure Changes and Subclinical Markers of Atherosclerosis. Am J Hypertens. 2015, 28, 1134–40. [CrossRef] [PubMed]
- Sheng, Y.; Zhu, L. The crosstalk between autonomic nervous system and blood vessels. Int J Physiol Pathophysiol Pharmacol 2018, 10, 17. [Google Scholar] [PubMed]
- Chistiakov, D.A.; Ashwell, K.W.; Orekhov, A.N.; Bobryshev, Y.V. Innervation of the arterial wall and its modification in atherosclerosis. Auton Neurosci 2015, 193, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Giunta, S.; Xia, S.; Pelliccioni, G.; Olivieri, F. Autonomic nervous system imbalance during aging contributes to impair endogenous anti-inflammaging strategies. GeroScience 2023. [CrossRef] [PubMed]
- Rivera, M.C.; Mastronardi, C.; Silva-Aldana, C.T.; Arcos-Burgos, M.; Lidbury, B.A. Myalgic encephalomyelitis/chronic fatigue syndrome: A comprehensive review. Diagnostics 2019, 9, 91. [Google Scholar] [CrossRef] [PubMed]
- Simula S, Vanninen E, Lehto S, Hedman A, Pajunen P, Syvänne M, et al. Heart rate variability associates with asymptomatic coronary atherosclerosis. Clin Auton Res 2014, 24, 31–7. [CrossRef]
- Huikuri H, V. , Jokinen V, Syvänne M, Nieminen MS, Airaksinen KEJ, Ikäheimo MJ, et al. Heart Rate Variability and Progression of Coronary Atherosclerosis. Arterioscler Thromb Vasc Biol 1999, 19, 1979–85. [Google Scholar] [CrossRef]
Figure 1.
Heart rate variability (HRV) and respiration variability (RV) in three study groups (healthy controls (HC), myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and post-COVID-19 syndrome (PCS)) at spontaneous breathing (SR), at 12 breaths/minute (12br) and at 6 breaths/minute (6br). Significant differences of variability indices in ME/CFS and PCS from HC and significant changes of these indices at 12 breaths/minute and at 6 breaths/minute within patient groups are marked with asterisk brackets at the top and at the bottom of the plots respectively. We regarded * p < 0.05 as statistically significant differences between the two groups. (a) Total power (TP) of HRV; (b) Low frequency (LF) of HRV; (c) High frequency (HF) of HRV; (d) TP of RV; (e) LF of RV; (f) HF of RV.
Figure 1.
Heart rate variability (HRV) and respiration variability (RV) in three study groups (healthy controls (HC), myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and post-COVID-19 syndrome (PCS)) at spontaneous breathing (SR), at 12 breaths/minute (12br) and at 6 breaths/minute (6br). Significant differences of variability indices in ME/CFS and PCS from HC and significant changes of these indices at 12 breaths/minute and at 6 breaths/minute within patient groups are marked with asterisk brackets at the top and at the bottom of the plots respectively. We regarded * p < 0.05 as statistically significant differences between the two groups. (a) Total power (TP) of HRV; (b) Low frequency (LF) of HRV; (c) High frequency (HF) of HRV; (d) TP of RV; (e) LF of RV; (f) HF of RV.
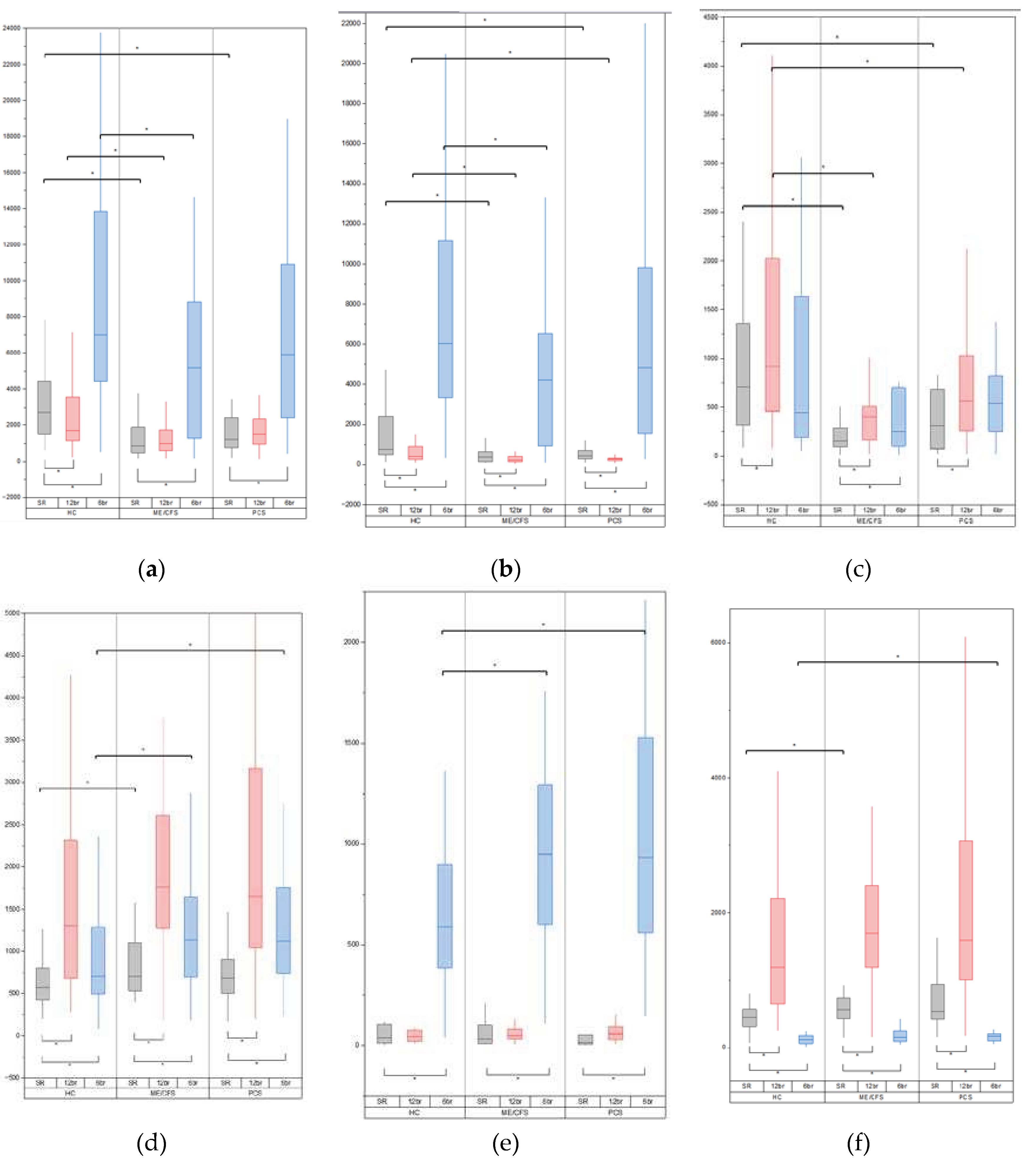
Figure 2.
Receiver operating characteristic (ROC) curves for the analysed models. TP1: total power of heart rate variability at spontaneous breathing; HF1: high frequency of heart rate variability at spontaneous breathing.
Figure 2.
Receiver operating characteristic (ROC) curves for the analysed models. TP1: total power of heart rate variability at spontaneous breathing; HF1: high frequency of heart rate variability at spontaneous breathing.
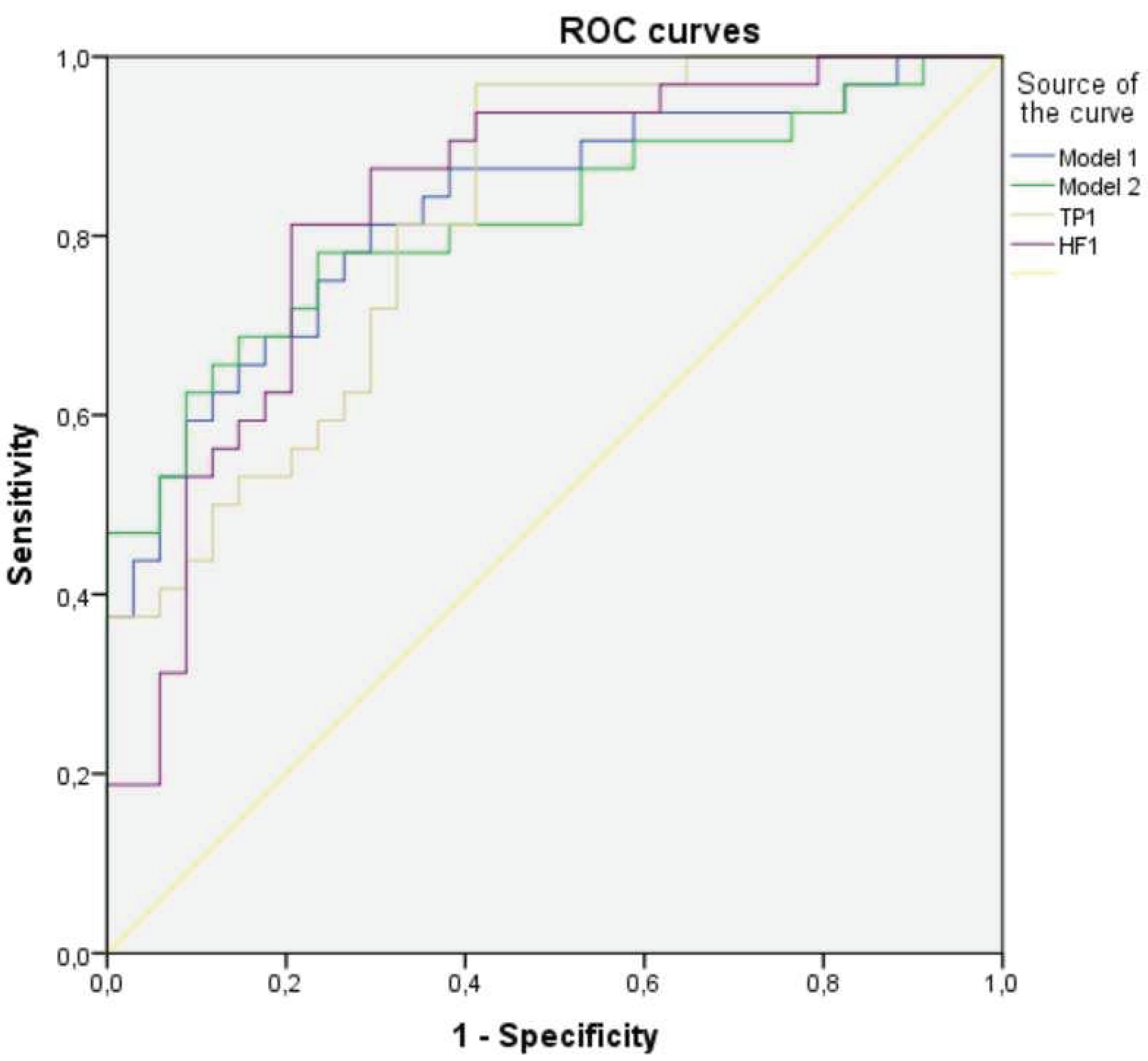

Table 1.
Baseline demographic and clinical parameters among participants.
| Variable | ME/CFS | PCС | HC | p-Value ME/CFS vs HC |
p-Value PCС vs HC |
|---|---|---|---|---|---|
| Age (years) | 35.00 (30.0-41.25) | 35.00 (29.50-41.50) | 34.50 (21.25-43.75) | 0.190 | 0.174 |
| BMI (kg/m2) | 23.41 (19.45-28.70) | 23.51 (20.54-27.86) | 22.07 (20.14-25.41) | 0.530 | 0.323 |
| Gender | |||||
| Male | 8 (23.53%) | 6 (20.69%) | 10 (31.25%) | 0.482 | 0.395 |
| Female | 26 (76.47%) | 23 (79.31%) | 22 (68.75%) | ||
| HADS | |||||
| Anxiety | 10.00 (5.75-12.00) | 10.00 (6.00-12.00) | 6.00 (2.00-8.00) | 0.001 | 0.001 |
| Depression | 10.00 (7.75-11.25) | 9.00 (6.00-10.00) | 3.00 (1.25-4.00) | 0.000 | 0.000 |
| MFI-20 | |||||
| General fatigue | 19.00 (17.75-20.00) | 18.00 (14.50-20.00) | 8.00 (5.25-9.75) | 0.000 | 0.000 |
| Physical fatigue | 17.50 (15.00-19.00) | 16.00 (14.00-18.00) | 7.00 (5.00-9.75) | 0.000 | 0.000 |
| Reduced activity | 18.00 (16.00-19.00) | 16.00 (12.5-19.00) | 7.50 (4.25-11.00) | 0.000 | 0.000 |
| Reduced motivation | 13.50 (11.00-16.00) | 12.00 (9.50-15.00) | 8.00 (6.00-9.00) | 0.000 | 0.000 |
| Mental fatigue | 16.50 (15.00-18.00) | 13.00 (11.00-16.00) | 6.00 (4.00-9.00) | 0.000 | 0.000 |
| IPAQ | |||||
| Total score IPAQ (MET-min/Week) | 1857.00 (590.25-2841.00) | 1506.00 (1039.50-2814.00) | 3027.00 (1606.50-5399.00) | 0.004 | 0.011 |
Medians [IQR: interquartile ranges] and percentages (%) are shown. BMI: body mass index; HADS: Hospital Anxiety and Depression Scale; HC: healthy controls; IPAQ: International Physical Activity Questionnaires; ME/CFS: myalgic encephalomyelitis/chronic fatigue syndrome; MFI: Multidimensional Fatigue Inventory; PCС: post-COVID-19 condition. We regarded * p < 0.05 as statistically significant differences between the two groups.
Table 2.
Baseline parameters of heart rate, arterial blood pressure and respiration variability among participants.
Table 2.
Baseline parameters of heart rate, arterial blood pressure and respiration variability among participants.
| Variable | ME/CFS | PCC | HC | p-Value ME/CFS vs HC |
p-Value PCC vs HC |
|
|---|---|---|---|---|---|---|
| Heart rate variability | ||||||
| TP (ms2) | 852.45 (469.03-1912.88) | 1358.10 (834.15-2687.15) | 2709.05 (1483.38-4454.36) | 0.000 | 0.008 | |
| LF (ms2) | 367.10 (137.45-635.13) | 429.20 (279.65-867.70) | 759.30 (477.33-2480.68) | 0.000 | 0.038 | |
| HF (ms2) | 152.90 (91.93-284.78) | 335.00 (102.45-717.10) | 703.70 (311.00-1394.80) | 0.000 | 0.012 | |
| VLF (ms2) | 256.15 (192.03-619.38) | 469.20 (237.10-814.60) | 727.50 (431.85-1014.80) | 0.000 | 0.017 | |
| LF/HF | 2.14 (1.20-4.13) | 1.46 (1.02-4.01) | 1.25 (0.71-2.31) | 0.029 | 0.155 | |
| Beat-to-beat systolic arterial blood pressure variability | ||||||
| TP (ms2) | 50.15 (23.38-66.78) | 42.20 (26.85-65.80) | 41.35 (22.15-63.15) | 0.434 | 0.598 | |
| LF (ms2) | 13.95 (6.45-21.85) | 13.50 (8.80-23.30) | 9.50 (6.30-19.68) | 0.438 | 0.157 | |
| HF (ms2) | 7.80 (4.38-16.73) | 8.40 (3.60-11.45) | 8.50 (4.48-14.28) | 0.944 | 0.718 | |
| VLF (ms2) | 20.30 (10.08-31.83) | 17.50 (7.80-29.60) | 12.90 (5.63-33.60) | 0.178 | 0.470 | |
| LF/HF | 1.63 (0.77-2.43) | 1.79 (1.20-2.92) | 1.11 (0.65-2.85) | 0.369 | 0.053 | |
| Beat-to-beat diastolic arterial blood pressure variability | ||||||
| TP (ms2) | 12.95 (7.38-25.28) | 12.80 (8.05-25.35) | 11.75 (7.60-20.53) | 0.559 | 0.488 | |
| LF (ms2) | 5.15 (2.93-7.98) | 5.30 (3.15-8.70) | 4.45 (2.25-7.90) | 0.585 | 0.593 | |
| HF (ms2) | 1.50 (0.90-2.15) | 1.10 (0.70-2.50) | 1.45 (0.70-2.68) | 0.832 | 0.772 | |
| VLF (ms2) | 5.75 (3.03-12.15) | 6.20 (2.80-13.15) | 4.45 (2.83-13.48) | 0.847 | 0.868 | |
| LF/HF | 3.39 (1.84-5.53) | 3.91 (2.35-6.83) | 3.02 (2.17-5.74) | 0.807 | 0.573 | |
| Respiration variability | ||||||
| TP (ms2) | 703.00 (523.63-1122.15) | 722.90 (480.45-993.45) | 576.10 (418.93-809.75) | 0.022 | 0.153 | |
| LF (ms2) | 32.65 (11.20-101.05) | 20.60 (7.20-182.80) | 39.45 (13.33-105.73) | 0.748 | 0.263 | |
| HF (ms2) | 560.85 (421.90-769.85) | 481.80 (350.90-951.95) | 449.85 (309.00-569.55) | 0.024 | 0.137 | |
| VLF (ms2) | 3.05 (2.05-4.88) | 3.40 (2.15-5.45) | 3.15 (2.25-6.20) | 0.572 | 0.960 | |
| LF/HF | 0.06 (0.02-0.13) | 0.03 (0.02-0.26) | 0.08 (0.03-0.29) | 0.403 | 0.132 | |
Medians [IQR: interquartile ranges] are shown. HC: healthy controls; HF: high frequency; ME/CFS: myalgic encephalomyelitis/chronic fatigue syndrome; LF: low frequency; PCC: post-COVID-19 syndrome; TP: total power; VLF: very low frequency. We regarded * p < 0.05 as statistically significant differences between the two groups.
Table 3.
Heart rate, arterial blood pressure and respiration variability among participants at 12 breaths/minute and at 6 breaths/minute respiration rate.
Table 3.
Heart rate, arterial blood pressure and respiration variability among participants at 12 breaths/minute and at 6 breaths/minute respiration rate.
| Variable | ME/CFS | PCC | HC | p-Value ME/CFS vs HC |
p-Value PCC vs HC |
|
|---|---|---|---|---|---|---|
| Heart rate variability at 12 breaths/minute | ||||||
| TP (ms2) | 998.90 (573.93-1729.15) | 1506.80 (948.90-2410.35) | 1682.35 (1120.95-3607.90) | 0.001 | 0.088 | |
| LF (ms2) | 226.55 (140.28-399.68) | 272.60 (198.90-329.50) | 402.7 (237.35-908.75) | 0.002 | 0.018 | |
| HF (ms2) | 399.15 (162.38-529.75) | 564.50 (253.85-1095.35) | 920.45 (439.75-2023.70) | 0.000 | 0.038 | |
| Beat-to-beat systolic arterial blood pressure variability at 12 breaths/minute | ||||||
| TP (ms2) | 49.30 (24.85-65.45) | 42.40 (26.00-97.60) | 33.00 (18.85-49.18) | 0.101 | 0.231 | |
| LF (ms2) | 11.90 (5.93-21.33) | 9.60 (4.75-23.10) | 5.75 (3.70-10.85) | 0.007 | 0.029 | |
| HF (ms2) | 14.74 (6.08-32.05) | 12.80 (6.40-35.80) | 13.80 (8.38-22.50) | 0.773 | 0.960 | |
| Beat-to-beat dyastolic arterial blood pressure variability at 12 breaths/minute | ||||||
| TP (ms2) | 12.35 (7.48-22.78) | 13.90 (7.15-20.60) | 9.35 (4.63-14.55) | 0.034 | 0.067 | |
| LF (ms2) | 4.10 (2.13-6.90) | 4.10 (1.85-8.15) | 2.70 (1.73-4.70) | 0.061 | 0.161 | |
| HF (ms2) | 3.35 (1.45-5.83) | 2.60 (1.00-6.40) | 1.45 (0.93-3.15) | 0.010 | 0.126 | |
| Respiration variability at 12 breaths/minute | ||||||
| TP (ms2) | 1763.45 (1247.75-2613.40) | 1647.10 (1020.70-3323.25) | 1303.65 (683.95-2337.68) | 0.124 | 0.126 | |
| LF (ms2) | 51.10 (34.28-81.90) | 57.50 (27.90-112.10) | 45.20 (22.50-75.28) | 0.216 | 0.166 | |
| HF (ms2) | 1692.00 (1154.40-2413.70) | 1591.30 (988.10-3197.25) | 1189.25 (645.40-2238.68) | 0.118 | 0.126 | |
| Heart rate variability at 6 breaths/minute | ||||||
| TP (ms2) | 5179.75 (1260.90-8857.20) | 5891.10 (2363.10-11520.45) | 7007.30 (4443.65-14608.75) | 0.022 | 0.220 | |
| LF (ms2) | 4220.15 (921.70-6590.25) | 4824.30 (1528.40-9957.70) | 6022.40 (3333.65-11796.05) | 0.013 | 0.112 | |
| HF (ms2) | 249.90 (98.28-698.98) | 536.10 (231.55-1099.25) | 442.90 (183.50-1643.08) | 0.057 | 0.931 | |
| Beat-to-beat systolic arterial blood pressure variability at 6 breaths/minute | ||||||
| TP (ms2) | 77.20 (43.58-136.63) | 84.40 (48.90-157.35) | 62.90 (39.38-96.05) | 0.184 | 0.137 | |
| LF (ms2) | 53.60 (22.05-106.18) | 57.70 (27.30-122.60) | 39.25 (22.23-69.70) | 0.225 | 0.054 | |
| HF (ms2) | 5.35 (2.80-10.85) | 5.20 (2.65-8.95) | 3.15 (1.93-6.23) | 0.026 | 0.086 | |
| Beat-to-beat dyastolic arterial blood pressure variability at 6 breaths/minute | ||||||
| TP (ms2) | 21.15 (11.45-39.48) | 17.90 (12.70-35.20) | 15.30 (10.45-27.23) | 0.359 | 0.295 | |
| LF (ms2) | 14.25 (5.23-26.93) | 12.60 (6.35-27.00) | 9.40 (5.05-20.80) | 0.333 | 0.245 | |
| HF (ms2) | 1.70 (1.10-2.53) | 2.10 (1.40-3.80) | 1.10 (0.70-3.38) | 0.386 | 0.079 | |
| Respiration variability at 6 breaths/minute | ||||||
| TP (ms2) | 1133.80 (688.13-1664.75) | 1122.20 (724.45-1865.40) | 701.45 (492.33-1332.78) | 0.030 | 0.022 | |
| LF (ms2) | 947.55 (591.03-1304.13) | 933.80 (537.65-1612.40) | 588.45 (370.00-937.15) | 0.013 | 0.015 | |
| HF (ms2) | 157.40 (91.43-249.58) | 165.50 (97.20-214.10) | 116.55 (61.58-183.60) | 0.072 | 0.033 | |
Medians [IQR: interquartile ranges] are shown. HC: healthy controls; HF: high frequency; ME/CFS: myalgic encephalomyelitis/chronic fatigue syndrome; LF: low frequency; PCC: post-COVID-19 condition; TP: total power; VLF: very low frequency. We regarded * p < 0.05 as statistically significant differences between the two groups.
Table 4.
Multivariate logistic regression analysis for predicting the presence of ME/CFS.
| Variable | Adj. B | Adj. OR (95% CI) | P value |
|---|---|---|---|
| Model 1 | |||
| TP of HRV at spontaneous breathing | -0.001 | 0.999 (0.999-1.002) | 0.001 |
| TP of RV at spontaneous breathing | 0.002 | 1.002 (1.000-1.004) | 0.044 |
| Hosmer Lemeshow test, p-value=0.952; constant = 0.504 | |||
| Model 2 | |||
| LF of HRV at spontaneous breathing | -0.001 | 0.999 (0.998-1.000) | 0.012 |
| HF of HRV at 12 breaths/minute | -0.001 | 0.999 (0.998-1.000) | 0.047 |
| TP of RV at spontaneous breathing | 0.002 | 1.002 (1.000-1.003) | 0.088 |
| Hosmer Lemeshow test, p-value=0.730; constant = 0.562 | |||
RV: respiration variability; HF: high frequency; HRV: heart rate variability; LF: low frequency; TP: total power; VLF: very low frequency. We regarded * p < 0.05 as statistically significant differences between the two groups.
Table 5.
Comparison of predictive performance in receiver operating characteristic analysis.
| Variable | TP of HRV at SR | HF of HRV at SR | Model 1 | Model 2 |
|---|---|---|---|---|
| AUC (95% CI) | 0.819 (0.720-0.918) | 0.834 (0.735-0.933) | 0.830 (0.730-0.929) | 0.817 (0.712-0.922) |
| Сut-off (Maximum Youden’s index) | 1047.95 | 286.95 | 0.580 | 0.496 |
| Sensitivity %, (95% CI) | 96.9% | 81.3% | 73.5% | 85.3% |
| Specificity %, (95% CI) | 58.8% | 79.4% | 75% | 68.8% |
| Cut-off (Se=Sp) | 1587.55 | 296.95 | 0.603 | 0.612 |
| Sensitivity %, (95% CI) | 71.9% | 78.1% | 70.6% | 76.5% |
| Specificity %, (95% CI) | 70.6% | 79.4% | 81.3% | 75.% |
AUC: area under the curve, CI: confidence interval; HF: high frequency; HRV: heart rate variability; SR: spontaneous breathing (rest); TP: total power.
Table 6.
Significant (p<0.05) Spearman correlations of heart rate, arterial blood pressure and respiration variability parameters with clinical characteristics in patient groups. Positive correlations marked with red colour, and negative correlations - with blue one.
Table 6.
Significant (p<0.05) Spearman correlations of heart rate, arterial blood pressure and respiration variability parameters with clinical characteristics in patient groups. Positive correlations marked with red colour, and negative correlations - with blue one.
| Variable | ME/CFS | PCC | HC | |||
|---|---|---|---|---|---|---|
| (+) | (-) | (+) | (-) | (+) | (-) | |
| HADS_D | BMI DBPV_HF_6br/min |
RM HADS_A DBPV_TP_12br/min |
GF, PF, RA, RM, MF | |||
| HADS_A | RV_TP_6br/min RV_LF_6br/min RV_HF_6br/min |
HRV_TP_12br/min |
SBPV_TP_SR SBPV_VLF_SR RV_TP_6br/min RV_LF_6br/min |
GF, PF, RM RV_HF_6br/min |
HRV_HF_SR | |
| General fatigue | PF, RA SBPV_HF_SR DBPV_LF_12br/min SBPV_LF_6br/min DBPV_LF_6br/min |
HRV_TP_SR HRV_HF_SR HRV_VLF_SR HRV_TP_12br/min HRV_LF_12br/min HRV_HF_12br/min |
PF, RA | PF, RA, RM, MF HADS_D |
||
| Physical fatigue | GF, RA SBPV_TP_6br/min SBPV_LF_6br/min DBPV_TP_6br/min DBPV_LF_6br/min |
GF, RA SBPV_TP_12br/min SBPV_LF_12br/min DBPV_LF_12br/min SBPV_TP_6br/min SBPV_LF_6br/min DBPV_TP_6br/min DBPV_LF_6br/min |
GF, RA, RM, MF HADS_D, HADS_A DBPV_VLF_SR |
Age | ||
| Reduced activity | GF, PF |
HRV_HF_SR |
GF, PF, RM, MF DBPV_TP_12br/min |
GF, PF, RM, MF HADS_D SBPV_VLF_SR |
||
| Reduced motivation | SBPV_TP_SR SBPV_LF_SR |
RA, MF HADS_D |
GF, PF, RA, MF HADS_D, HADS_A |
|||
| Mental fatigue | RA, RM DBPV_HF_6br/min |
GF, PF, RA, RM HADS_D SBPV_TP_SR DBPV_TP_SR DBPV_HF_SR |
||||
| Age | SBPV_TP_6br/min SBPV_LF_6br/min SBPV_HF_6br/min |
RV_TP_SR RV_HF_SR RV_TP_6br/min RV_LF_6br/min |
HRV_LF_SR SBPV_LF_SR DBPV_LF_SR DBPV_HF_SR SBPV_TP_12br/min SBPV_HF_12br/min DBPV_HF_12br/min HRV_TP_6br/min HRV_LF_6br/min HRV_HF_6br/min |
SBPV_TP_6br/min SBPV_LF_6br/min |
PF DBPV_HF_SR HRV_TP_12br/min HRV_LF_12br/min HRV_TP_6br/min HRV_LF_6br/min HRV_HF_6br/min |
|
| BMI | RV_TP_12br/min RV_LF_12br/min RV_HF_12br/min RV_TP_6br/min RV_LF_6br/min RV_HF_6br/min |
HADS_D HRV_TP_SR HRV_HF_SR HRV_LF_SR DBPV_HF_6br/min |
RV_TP_12br/min RV_HF_12br/min SBPV_HF_6br/min RV_HF_6br/min |
HRV_HF_12br/min SBPV_HF_12br/min HRV_TP_6br/min HRV_LF_6br/min HRV_HF_6br/min |
SBPV_HF_12br/min |
|
| IPAQ | GF, PF; DBPV_TP_12br/min RV_LF_6br/min |
DBPV_TP_12br/min | ||||
BMI: body mass index; RV: respiration variability; DBPV: diastolic blood pressure variablility; GF: general fatigue MFI-20 domain; HADS_A: Hospital Anxiety and Depression Scale - Anxiety subscale; HADS_D: Hospital Anxiety and Depression Scale - Depression subscale; HC: healthy controls; HF: high frequency; HRV: heart rate variability; IPAQ: International Physical Activity Questionnaires; LF: low frequency; ME/CFS: myalgic encephalomyelitis/chronic fatigue syndrome; MF: mental fatigue MFI-20 domain; PCC: post-COVID-19 syndrome; PF: physical fatigue MFI-20 domain; RA: reduced anxiety MFI-20 domain; RM: reduced motivation MFI-20 domain; SBPV: syslolic blood pressure variability; SR: spontaneous breathing; TP: total power; VLF: very low frequency.
Table 7.
Baroreflex sensitivity and baroreflex effectiveness index among participants.
| Variable | ME/CFS | PCC | HC | p-Value ME/CFS vs HC |
p-Value PCC vs HC |
|---|---|---|---|---|---|
| BRSup | 4.42 (2.88-6.28) | 5.91 (3.54-7.92) | 7.40 (4.90-14.03) | 0.000 | 0.041 |
| BRSdown | 4.85 (2.93-7.42) | 5.24 (3.97-8.48) | 9.15 (6.42-12.01) | 0.000 | 0.002 |
| BRSmean | 4.60 (3.12-6.40) | 5.99 (3.88-8.48) | 8.45 (5.25-13.40) | 0.000 | 0.016 |
| BEI_up | 0.57 (0.43-0.80) | 0.64 (0.44-0.78) | 0.70 (0.56-0.88) | 0.024 | 0.049 |
| BEI_down | 0.45 (0.37-0.62) | 0.44 (0.29-0.77) | 0.49 (0.36-0.82) | 0.434 | 0.470 |
| BR_up | 16.00 (7.50-25.00) | 18.00 (10.00-27.50) | 18.50 (9.25-29.00) | 0.362 | 0.942 |
| BR_down | 19.00 (9.00-25.75) | 12.00 (6.00-24.00) | 19.5 (7.00 - 32.75) | 0.529 | 0.191 |
| BRX_up | 10.5 (4.75-18.00) | 9.00 (5.50-14.00) | 5.50 (2.00-9.00) | 0.009 | 0.018 |
| BRX_down | 18.5 (9.00-25.00) | 14.00 (5.00-23.00) | 16.00 (5.00-21.50) | 0.218 | 0.931 |
BMI body mass index; BEI baroreflex effectiveness index; BR number of effective baroreflex events; BRX number of ineffective baroreflex events; BRS baroreflex sensitivity; HC: healthy controls; ME/CFS: myalgic encephalomyelitis/chronic fatigue syndrome; PCC: post-COVID-19 condition.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



