
Submitted:
21 November 2023
Posted:
21 November 2023
You are already at the latest version
Abstract
The study aimed to determine, through a systematic review, the relationship between Reactive Attachment Disorder (RAD) and the presence of psychopathology in children and adolescents and to determine the existence of differences about the presence of internalising and externalising psychological problems between the RAD group and groups with other disorders or with typical development. Following the PRISMA methodology, a search was carried out in the Web of Science, PubMed and Scopus databases. The search yielded 770 results, of which only 25 met the inclusion criteria. The results, indicate a relationship between the presence of RAD and/or Disinhibited social engagement disorder (DSED) with the presence of internalising and externalising problems. These difficulties are more present in children with RAD compared to children without personal difficulties, or children with DSED, children with autism, children with intellectual disabilities or children with hyperactivity. It can be concluded that the presence of RAD has negative consequences on the mental health of children and adolescents, with these being greater in the inhibited group than in the disinhibited group, and with respect to children with autism or hyperactivity.
Keywords:
reactive attachment disorder
; children
; adolescents
; internalising problems
; externalising problems
; systematic review
1. Introduction
The quality of the interactions established in the first years of human life is crucial and plays a significant role in the way human beings bond affectively and adapt personally and socially during adolescence and adulthood [1].
Attachment is the emotional connection between the baby and its caregiver, also called attachment figure [2]. According to [3], the first attachments are usually established at seven months of age and are often conditioned by the primary caregiver's responses to the child's needs, establishing an internal model of representation of the child's self, the caregiver and the relationship between the two [4].
Reactive Attachment Disorder (RAD hereafter) is characterised by difficulties in forming emotional attachments to others, a reduced ability to experience well-being and a fluctuation in mood that is apparently unexplained [5]. These alterations should appear after the age of 9 months and before the age of 5 years, having as their origin the experience of neglectful and unstable care [6,7,8,9].
In earlier versions of the DSM [10], RAD is divided into two types: inhibited (RAD-I, hereafter), characterised by emotionally withdrawn behaviours, fear of other people and selectivity in the choice of attachment figure; and disinhibited (DSED, hereafter), characterised by excessive sociability and an indiscriminate response in showing attachment to other people, even those unknown to the child [11,12].
However, the subtypes are now understood to be distinct diagnostic entities, with RAD corresponding to the inhibited form in DSM-IV and DSED to the disinhibited form [6,13]. For [13] RAD is related to a greater extent to poorer care in the first five years of life compared to DSED, where this relationship is not as evident.
The presence of RAD or DSED has been associated with being male, with other comorbid disorders, with parental mental health problems [14]. Having been exposed to a greater number of traumatic events or adverse childhood experiences [8]. Having had an early separation experience as a consequence of taking protective measures [15] mainly about DSED symptomatology when the change of caregivers occurs for the first time between 7 and 24 months regardless of the severity of maltreatment, the age of adoption and the number of family changes [16]. Having experienced poor caregiving in infancy, primarily in the development of RAD-I symptomatology, and with insecure or disorganised attachments in the case of inhibited and disinhibited symptomatology [13].
Focusing on RAD, according to the DSM-5-TR [6], comorbidity is common with some developmental difficulties, especially cognitive and language difficulties, stereotypies, internalising and externalising problems such as attention deficit hyperactivity disorder, conditions that have been associated with neglect and abuse experiences [17,18], institutional care or frequent changes of caregivers [3,18,19,20,21].
To date, the true prevalence of RAD has not been established and there is a need to know in greater depth which entities are comorbid to this difficulty, as well as the factors associated with it. There is a large gap in the literature on the difficulties associated with RAD. For this reason, the present study aims to determine, through a systematic review, the relationship between RAD and the presence of psychopathology in children and adolescents, as well as to determine the existence of differences to the presence of internalising and externalising psychological problems between the group with RAD and groups with other disorders or typical development.
The hypotheses put forward in this review are:
Hypothesis 1: There would be a relationship between the presence of RAD and greater psychopathology. It is expected to find a relationship between RAD and internalising and externalising problems, and greater comorbidity with other disorders. Furthermore, this relationship is expected to be stronger in the case of the group with an inhibited RAD-I attachment disorder versus the disinhibited DSED.
Hypothesis 2: There will be a greater presence of psychological problems and comorbid disorders in children with RAD compared to children and adolescents with ASD, ADHD, social risk and typical development.
2. Materials and Methods
2.1. Search Strategy
A systematic review of the scientific literature related to RAD was conducted according to the guidelines established by the PRISMA statement [22]. The search was carried out in October 2022 in the Web of Science, PubMed and Scopus databases. Based on the PICO strategy [23], an attempt was made to answer the following question: Is there a greater affectation in children and adolescents diagnosed with RAD compared to children without protective measures or with other types of disorders?
The final search combined the proposed key elements. The following Boolean (using MeSH terms) expression was therefore used in Web of Science, PubMed and Scopus: reactive attachment disorder (Topic) AND behavior* OR psychological health OR psychological well-being (Topic) in WoS; in PubMED ((reactive attachment disorder) AND (behavior* OR psychological health OR psychological wellbeing)) and in Scopus (reactive AND attachment AND disorder) AND (behavior* OR psychological AND health OR psychological AND well-being).
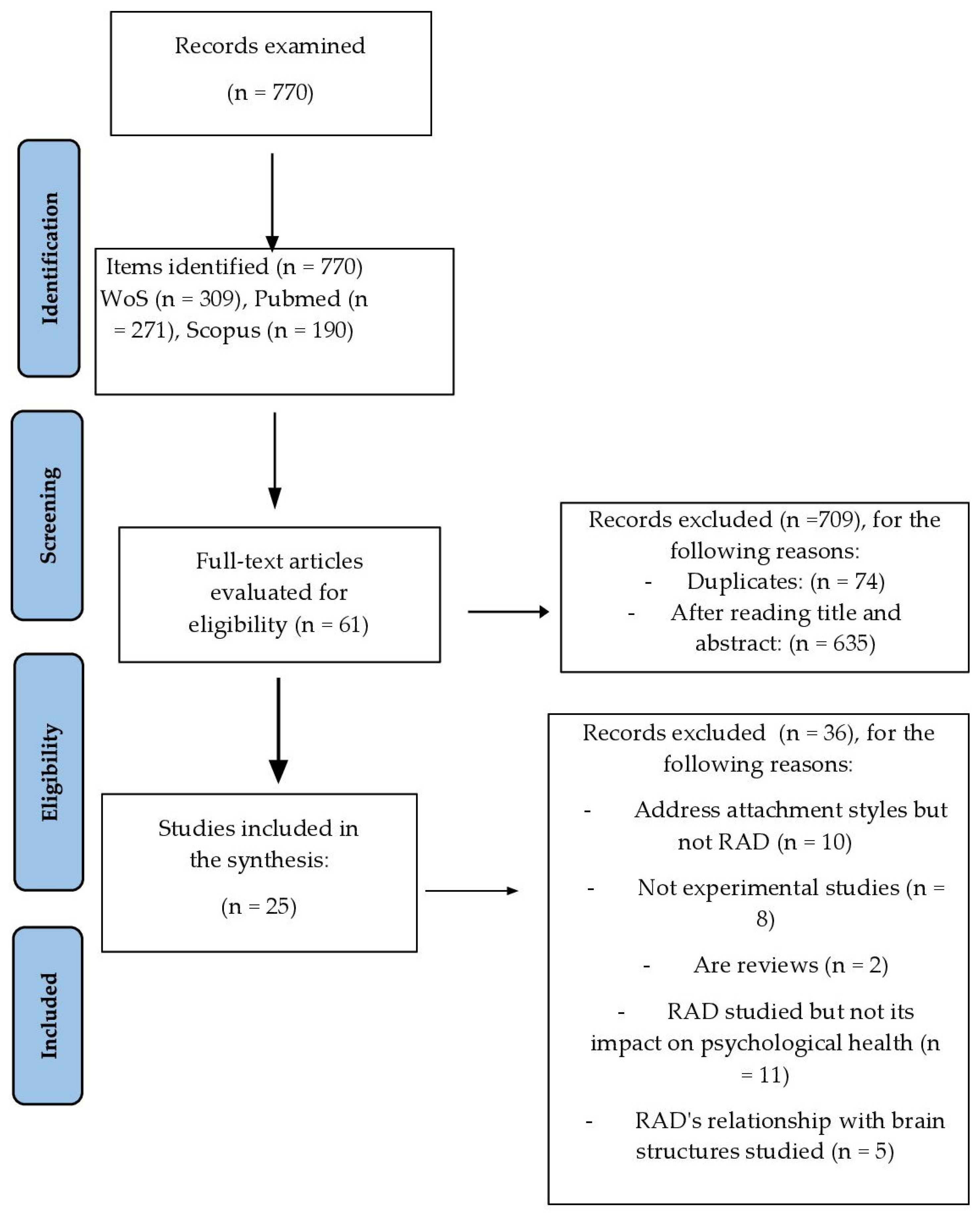
This resulted in 770 articles of which 309 were extracted from the Web of Science, 271 from PubMed and 190 from Scopus. All records were downloaded in an Excel sheet including authors' names, titles, journals and abstracts.
2.2. Eligibility Criteria
Inclusion criteria were established as documentary typology Articles published between 2010 and 2022 in Spanish or English, in which an empirical study was carried out that included at least one group with RAD and that studied the relationship between RAD and psychological problems, as well as the existence of differences between groups with and without RAD or with other disorders in children or adolescents.
Exclusion criteria included other types of documents such as conference proceedings, books, book chapters or grey literature, articles published in languages other than those established in the inclusion criteria, papers that did not include a group with ADR in the study, descriptive articles, narrative reviews, systematic reviews or case studies, and studies that included adults in their samples.
2.3. Procedure
All records were imported into Covidence [24], a screening and extraction tool for systematic reviews. Duplicate articles were removed and then screened in a blinded fashion by two authors. When there was disagreement, a third reviewer interceded.
The number of articles analysed was 770, of which 74 were eliminated as duplicates and 635 were eliminated after reading the title and abstract. After analysis of the full body of the remaining 61 articles, a total of 36 articles were removed for different reasons: Focusing on attachment styles but not on RAD (10 articles), being systematic reviews (2 articles), not being experimental but descriptive studies (8 articles), not addressing the consequences of RAD on psychological health (11 articles) and analysing the relationship between RAD with brain structures (5 articles). Following this process, a total of 25 articles were included in the final study (see Figure 1).
This systematic review was registered in PROSPERO with code CRD42022359220.
2.4. Methodological Quality of the Selected Articles
The quality assessment of the selected articles was carried out by two independent and blinded reviewers. For this purpose, the QUIRE Guidelines 2.0 quality scale [25] was used, selecting 11 of the 18 indicators included in the scale - title, abstract, problem description, available knowledge, specific aims, measures, analysis, results, discussion: interpretation, limitations and conclusions -. After application, two researchers classified the papers into three categories: good quality - when 9 or more of the indicators were met, medium quality - when between 8 and 6 indicators were met, and low quality - when 5 or fewer indicators were met. All papers included in the present review were classified by both researchers in the good quality category. The inter-judge agreement following Cohen's Kappa [26] was 1, a very satisfactory value according to [27].
3. Results
Table 1 summarises the articles included in this review, including authors, year of publication, diagnostic instruments and criteria, main results and limitations of the studies.
3.1. RAD Diagnostic and Assessment Tests Used in the Articles Included in the Systematic Review
Research has used nine instruments to assess and diagnose RAD and some adaptations of these. The most commonly used was the Disturbance Attachment Interview - DAI [28], others that have been used are: The Child and Adolescent Psychiatric Assessment – CAPA [29], Relationship Problems Questionnaire - RPQ [30], Reactive Attachment Disorder and Disinhibited Social Engagement Disorder Assessment – RADA [31], Development and Wellbeing Assessment–RAD/DSED Section (DAWBA-RAD/DSED) [30], Relationship Patterns Questionnaire (RPQ) [32], The Rating of Inhibited Attachment Behavior Scale - RInAB [33] and FinAdo-RAD [34].
Also, some research, [35,36,37,38] do not use assessment instruments as the persons included in the study samples had been previously diagnosed based on the DSM-IV-TR, DSM-5, World Health Organisation ICD-10 criteria, for the most part. A more detailed analysis of this information can be found in Table 1.

Table 1.
Studies linking the presence of RAD to psychological problems and group differences.
| Article | Country of sample and life history or protection measures | Sample | Instrument used to assess RAD or DSED or diagnostic criteria used | Main results | Study limitations |
|---|---|---|---|---|---|
| Bosmans et al. (2019) [39] |
Belgium. Children in special education schools. 48% suspected of mistreatment, abuse or neglect. |
Children with RAD: n = 21. Children without RAD: n = 46. Mage: 8.70 years, SD= 0.99 27.2 % were diagnosed or suspected with RAD. |
Disturbance Attachment Interview – DAI [28]. | RAD correlates negatively with trust in teachers and emotional security compared to the group without RAD. | They only focus on children's emotional safety in relation to teachers, rather than on their general context. |
| Bruce et al. (2019) [40] |
Scotland. Children in foster care. | Moment 1: N = 100 Moment 2: N = 76 Age: 12-61 months |
The Rating of Inhibited Attachment Behavior Scale - RInAB [33]. | There is a relationship between RAD symptomatology and the presence of internalising and externalising problems, as well as lower verbal and total IQ. | Small sample size and small number of children with RAD. Change in protective measure between moment 1 and moment 2. The procedure used to activate the attachment mechanism in children may not be sufficiently stressful. Change of caregivers at moment 1 in some children. |
| Coughlan et al. (2021) [35] |
England. There is no information on its previous history. |
Group RAD (n =39), Group ADHD (n=1.430) Group ASD (n= 1.193) Age 17 years< |
World Health Organisation ICD-10 [56] | There are significant differences between groups (p < 0.001) in all factors of the SDQ questionnaire. The ASD group had more emotional problems, difficulties with peers and fewer prosocial strengths than the ADHD or RAD group. ADHD and RAD group more hyperactivity and behavioural problems. | Additional information from the children's context is not available for a better understanding of the results. |
| Davidson et al. (2015) [41] |
Scotland RAD Group, history of abuse and fostering. |
Children 5-11 years. Group RAD: n = 67 Group ASD: n = 58 |
Disturbance Attachment Interview - DAI [28]. | Higher prevalence of comorbidity with other mental health problems, as well as more disinhibition and indiscriminate friendliness in the RAD group. | Failure to discriminate between different types of RAD. The discrepancy between RAD diagnostic criteria (DSM-IV) and RAD assessment instrument that follows DSM-5 criteria. |
| Elovainio et al. (2015) [34] |
Finland. Adopted children. |
N= 853. Age: 6-15 years. No RAD n = 348; DSED n = 153; RAD n = 137, comorbid (DSED+TAR) n = 214. |
Disturbance Attachment Interview - DAI [28]. | Relationship between RAD and DSED with the presence of emotional, hyperactive and behavioural symptoms. The comorbid group had greater internalising, externalising and total problems than the other groups. | Does not allow for causal relationships between attachment disorders and psychological problems. Heteroinformed assessment (adoptive parents). |
| Giltaij et al. (2016) [36] |
The Netherlands. No data on life history. RAD group has higher indicators of neglectful care. |
N = 55. Age: 5-11 years. Mild intellectual disability. RAD (n= 3); DSED (n= 1); RAD+DSED (n=6). Control group (n= 45). |
Diagnosis is based on the criteria of the DSM-5 [6]. | RAD+DSED group has greater difficulties in adaptive behaviour in the area of socialisation and motor skills. RAD and/or DSED group had more disruptive and antisocial behaviour than the control group. DSED had greater emotional problems compared to the non-DSED group. |
Hetero- information (teachers). |
| Gleason et al. (2011) [13] |
Romania Children spent an average of 86% of their lives in institutional care. |
N= 136 initially (6-30 months). These were followed up at 30, 42 and 54 months of age. n= 68 assigned to care as usual. n=68 foster care. |
Disturbance Attachment Interview - DAI [28]. | DSED criteria met: Study start 41/129 (31.8 %), 30 months 22/122 (17.9 %), 42 months 22/122 (18.0 %) and 54 months of age 22/125 (17.6 %). RAD-I criteria met: Study entry 6/130 (4.6 %), 30 months 4/123 (3.3 %), 42 months 2/125 (1.6 %) and 54 months of age 5/122 (4.1 %). |
Neglectful care conditions other than institutionalisation were not assessed. The life history and background of caregivers (maltreatment or mental health status) are not considered. (maltreatment or mental health status). Low rates of emotionally withdrawn/inhibited RAD. |
| Guyon-Harris et al. (2019) [42] |
Romania. Foster care |
Experimental group (n = 55). Control group (n = 50). Mage = 12.80, (SD=0.71) years. | Version DAI-EA [20] adapted Disturbance Attachment Interview - DAI [28]. | A greater presence of RAD signs predicts worse overall social functioning and lower social competence. A greater presence of DSED signs predicts worse social functioning, more relationship victimisation and lower social competence. |
Adolescent self-reports are not included. Signs of RAD are examined, but not the diagnosis. Focuses on social functioning and does not explore other domains. |
| Hong et al. (2018) [37] |
Corea del Sur General population |
Children <10 years. N = 14,029,571 RAD = 736 |
Diagnosis is based on the criteria of the [57]. | Higher prevalence of comorbid disorders in children with RAD than in typically developing children. This type of disorder varies according to age group. | Patients who underwent treatment outside the hospital are not included. The precise incidence of RAD is not reflected. |
| Jonkman et al. (2014) [43] |
Netherlands The children had experienced at least one foster care disruption. |
N=126 in Foster care families. Age: 24-72 months with the foster family). Control group n = 84; RAD-I: n =11; DSED: n = 19; RAD-I+DSED n = 12. |
Disturbance Attachment Interview - DAI [28]. | RAD and DSED groups presented greater internalising, externalising and total problems. | Small sample size. Observational measures. Hetero-informed assessment (family members and teachers). |
| Kay y Green (2013) [15] |
England Residential care and children at risk of social exclusion. |
Group RAD foster care: N= 153. Group RAD social risk: n = 42. Age: 10-15 years. |
Development and Wellbeing Assessment–RAD/DSED Section (DAWBA-RAD/DSED; [30] 24-item version. | Greater presence of RAD symptomatology in the group in foster care compared to the social risk group. Relationship between RAD symptomatology and greater behavioural and emotional problems and a lower adaptive capacity. |
Hetero- information (social workers). Incomplete data on participants' life history. |
| Kay et al. (2016) [16] |
England Adopción. Sin antecedes de institucionalización previa. |
Adoption group: n = 60. Group with externalising disorder: n = 26. Group at social risk: n = 55 Age: 6-11 month. |
CAPA-RAD [16,41] adaption of CAPA [29] based on the DSM-5 criteria [6]. | In the adoption group, there is a significant relationship between the presence of DSED and ADHD according to the teachers. According to parents, this relationship is found with ADHD, emotional and behavioural problems. | Small sample size. Biases in sample selection. No clinical diagnosis of DSED. Lack of pre-adoption information on children's life history. Hetero-informed assessment (family members and teachers). |
| Kocovska et al. (2012) [44] |
United Kingdom. Adopted children who have suffered abuse, neglect, abandonment and abuse. | N = 66. Age: 5-12 years. Adopted group (n = 33) of which 20 had RAD. Control group (n = 32). |
Relationship Patterns Questionnaire (RPQ) [32]. | The group of adopted children presented greater behavioural problems than the group of non-adopted children. High prevalence of children with RAD in the adopted group. | Possible bias in the sample of adopted families as those with higher motivation and better family functioning participated. The attachment assessment measure used has shown adequate psychometric properties in children under 8 years of age and the sample is somewhat larger. |
| Lehmann et al. (2016) [14] |
Norway Foster care. |
N = 122 Age: 6-10 years. | Reactive Attachment Disorder and Disinhibited Social Engagement Disorder Assessment – RADA [31]. | The positive association between RAD symptoms and DSED. RAD is associated with more comorbid personal difficulties than DSED. | Small sample size. Hetero-informed (caregiver) assessment. Broad, general categories of experiences of maltreatment. |
| Mayes et al. (2017) [45] |
United States. Children who have suffered severe abuse or neglect (N= 16) and children adopted from Russian or Chinese orphanages (N= 4). |
RAD+DSED n = 15; DSED n = 5; ASD n = 933; ADHD-C n = 631; ADHD-I n = 264. | The Rating of Inhibited Attachment Behavior Scale - RInAB [33]. | RAD group: All of them had callous-unemotional traits and 73 % had behavioural problems. RAD-I+DSED group: More behavioural problems and emotional insensitivity than DSED group. RAD group had more behavioural and emotional problems than the group with ASD, with ADHD-C and ADHD-I. |
Unrepresentative sample of children with RAD because of their size and because they initially presented other personal difficulties that required referral. |
| Moran et al. (2017) [46] |
Young people in the Youth Justice Service. 86% had experienced abuse. |
N = 29. Age: 12-17 years. Mage = 16.2; SD = 1.3. Carers: n = 29. Teachers: n = 20. | The Child and Adolescent Psychiatric Assessment – CAPA [29] | Relationship between RAD symptoms and other mental health problems. More mental health problems in the RAD group than in the non-ADR group. | Does not allow causal relationships to be established. Heteroassessment (parents and teachers). It is not known whether the children had any other psychological or neuropsychological problems. |
| Pritchett et al. (2013) [52] |
England. The general population with socio-cultural deprivation. RAD group have histories of abuse. |
N = 1.600. Age: 6-12 years. RAD group (n = 22). Of these 13 with a diagnosis of RAD and 9 with suspected | The Child and Adolescent Psychiatric Assessment – CAPA [29] | RAD group has a high comorbidity with other disorders and with the presence of behavioural problems. | Small sample size. |
| Raaska et al. (2012) [47] |
Finland. Children adopted between 1985 and 2007 from different countries. | N= 365. Age: 9-15 years. (47,8 % man). | FinAdo-RAD [34]. | There is a significant relationship between the severity of RAD symptomatology and participation in bullying situations, both victimisation and peer bullying. | Relatively low response rate. Children completed the questionnaires at home (possible parental influence). There is no information on whether RAD also relates to those children who engage in bullying in normative samples. |
| Sadiq et al. (2012) [38] |
Muestra con TAR: 1/3 vivía con la familia biológica y 2/3 eran adoptados. | N = 126. Age: 5-8 years. RAD group: n = 35. ASD group: n = 52. TD: n = 13 grupo. |
Diagnosis is based on the criteria of World Health Organisation ICD-10 [58] | RAD group had difficulties in the use of context, rapport and social relations than ASD group. | Clinical sample and not general population. |
| Seim et al. (2021) [48] |
Norway Residential care. 71% exposure to abuse. |
N = 306. Age: 12.2-20.2 years. Of these, with RAD (n = 28), with DSED (n = 26). Control group: n = 10480. Age: 12-20 years. |
The Preschool Age Psychiatric Assessment - PAPA [55] adaptation of CAPA [29] for children between 2 and 8 years. | RAD group lower self-esteem in school competence and higher self-esteem for close friendships than the control group. DSED group lower self-esteem in social acceptance, sports competence, romantic attractiveness and close friendship than control group. |
Hetero- information (caregivers). Inability to determine whether symptoms were present before the age of 5 years. |
| Seim et al. (2022) [49] |
Norway. Foster care. Exposure to neglect. 71% exposed to abuse. |
N = 381. Age:12.2-20.2 years. RAD (n = 33). DSED (n = 31). RAD+DSED (n = 2) | The Preschool Age Psychiatric Assessment - PAPA [55] adaptation of CAPA [29] for children between 2-8 years | High prevalence of mental disorders in children with RAD and DSED. Children with RAD and/or DSED high prevalence of emotional and behavioural problems. |
Heteroassessment (caregivers). Difficulty in demonstrating the presence of RAD before the age of 5 years. |
| Shimada et al. (2015) [50] |
Japan. Residential Foster care. RAD Group has suffered abuse and neglect |
RAD group: n = 21. Mage = 12.76 years. Group control: n = 22. Mage = 12.95 years. |
Diagnosis based on the criteria of DSM-5 criteria [6] | RAD group: smaller volume of grey matter. This is related to greater internalising and externalising problems according to the SDQ. | Small sample size. Cross-sectional design. Differences in IQ between RAD group and control group. |
| Vervoort et al. (2013) [53] |
Belgium. School-aged children with emotional and behavioural problems. 25% diagnosed or suspected RAD. 48% maltreatment, abuse or neglect. | Children DAI n = 77. Children RPQ n = 152. Mage 7.92 years. |
Disturbance Attachment Interview - DAI [28]. Relationship Problems Questionnaire - RPQ [30] |
More frequent and stronger associations between RAD and emotional and behavioural difficulties than DSED. | Small sample size. Need to use other measures to confirm the diagnosis of RAD. |
| Vervoort et al. (2014) [54] |
Belgium. Special education children with emotional and behavioural problems (suspected DSED). | DSED group: N = 33 special education. Control group: N = 33 general education. Mage 8.52 years |
Relationship Problems Questionnaire - RPQ [30] | DSED group showed more indiscriminate kindness and more behavioural problems than the control group. DSED group showed more positive overall self-concept and greater confidence in relationships compared to general education children. | The study focuses on one DSED indicator (indiscriminate kindness). Cross-sectional study. |
| Zimmerman & Iwanski (2019) [51] |
Germany. Children at risk of RAD-I had experienced severe neglect or abuse. |
N= 64 children in institutions and the general population. Age: 5-10 years. Of these, 32 suffered from RAD (foster homes or families). | Relationship Patterns Questionnaire - RPQ [32] | RAD risk group has a poorer self-concept, a greater number of negative signals from others through Internal Working Models and greater mental health problems. Positive association RAD with personal difficulties and negative association with prosocial behaviour. | Not specified |
3.2. Conditions and Previous History of the Sample According to the Articles Included in the Review
The majority of studies (84 %; n = 21) use children whose life history is characterised by protective measures, such as residential care, foster care or adoption, either because they have experienced or there are well-founded suspicions of maltreatment, neglect or abuse [13–16,31,34,35,38–51].
One study uses a clinical sample with externalising problems and general population [16], another sample with sociocultural deprivation with suspected malingering [52], two studies use children in special schools with emotional or behavioural problems [53,54], one study uses people with intellectual disabilities [36] and one study uses children with a diagnosis of RAD but no information on their life history [37].
3.3. Association between RAD Diagnosis and Other Personal, Social and Mental Health Difficulties
The 18 articles included in this review mainly address the presence of internalising, externalising and social difficulties in children with RAD (Table 1). More specifically, the presence of RAD in children aged 12-62 months in foster care is related to more internalising and externalising difficulties (rho = .33, p = 0.02) [40]. Also, in general, RAD-I (r = .33) and DSED (r = .28) are related to more emotional, behavioural and social problems. In this sense, children with RAD-I or DSED showed more symptoms than children who had neither of these difficulties. Those with both RAD and DSED also showed more symptoms [34], with the RAD-I group having higher mean scores than the DSED group for internalising, externalising and total problems.
In the same line, [51] report a significant association between RAD and emotional, social, behavioural and hyperactive difficulties with coefficients between r = .57 (p < 0.001) and r = .30 (p < 0.05). This conclusion is also reached by [54], who relate DSED to difficulties in these areas (r = .76, p < 0.001). Furthermore, he concludes that there are also more conflictual relationships with teachers (r = .25, p < 0.05) and dependency (r = .40, p < 0.01) and more trust towards significant others (r = .35, p < 0.01) and a better global self-concept (r = .22, p < 0.05).
In another study by [53], when the informants are caregivers, RAD-I is positively related to emotional (r = .41, p < 0.01), behavioural (r = .52, p < 0.01; r = .32, p < 0.01) and with peers (r = .24, p < 0.01; r = .28, p < 0.05) and negatively with prosocial behaviour (r = -.50; r = -.24, p < 0.05). The DSED was associated with conduct problems (r = .18, p < 0.05), hyperactivity (r = 0.21, p < 0.05) and peer problems (r = .24, p < 0.01). When the assessments are made by teachers, there are positive and significant relationships between the RAD-I group and the SDQ factors, with coefficients between .48 and .33 (p < 0.01) and a negative relationship with prosocial behaviour (r = .37, p < 0.01). In contrast, for the DSED type, there were no significant relationships.
On the other hand, although RAD-I and DSED were not associated with aggressive behaviour. However, an association with lower behavioural inhibition (r = -.28, p < 0.05) and higher ADHD symptomatology (r = .45; p < 0.001), oppositional defiant disorder, dissocial behaviour disorder (r = .30, p < 0.01) and depressive disorder over time, at 30 months (r = .35, p < 0.001), at 42 months (r = .72, p < 0.001) and at 54 months (r = .62, p < 0.05). However, in the RAD-I group there was greater functional impairment in different contexts and lower socioemotional competence than in the DSED group [13]. Along the same lines, in a study comparing children who have been adopted with children who have not been adopted, it was observed that 60 % of adopted children had RAD, while among non-adopted children there were no cases of RAD. Furthermore, 85 % showed comorbid ADHD, 85 % conduct disorder, 75 % had oppositional defiant disorder, 70 % had ASD and 55 % had PTSD, with these data being significantly higher in children who had been adopted compared to those who had not (p < 0.001) [44].
Meanwhile, in the work of [52] it was noted that 75 % of children in the RAD group had a clinical range of problems compared to 15 % of the general school population according to the SDQ. Similarly, 52 % of children with RAD also had ADHD, 29 % had oppositional defiant disorder, 29 % had a possible conduct disorder, 14% had ASD and 19 % had PTSD.
The study by [15] obtained similar findings, associating RAD and DSED with internalising (β = 0.832, p ≤. .001; β = 0.909, p ≤ .001) and externalising problems (β = 1.96, p ≤ 0.001; β = 1.18, p ≤ 0.001). Similarly, superficial social relationships were also related to more internalising and externalising problems (β =1.17, p ≤ 0.001) and (β = 2.33, p ≤ 0.001) respectively. The same was true for the feeling of Unpredictability, which was associated with internalising problems (β =1.52, p ≤ 0.001) and externalising problems (β = 2.70, p ≤ 0.001).
However, when different informants are used in the studies, disparate results are obtained, for example, in a sample of adopted children (65 % with mental health problems), children with externalising problems and low-risk children (19 % with mental health problems) when DSED was reported by teachers it was associated with conduct disorder (OR = 1.630, p < 0.01). In the case of researcher assessment, it was associated with ADHA (OR = 1.95, p < 0.01) and in the case of parents with emotional problems (OR = 1.644, p < 0.01), with ADHD (OR = 1.792, p < 0.01) and Oppositional Defiance Disorder/Conduct Disorder (OR = 1.711, p < 0.01) [16]. Similarly, taking caregiver assessments, in the case of RAD, this was related to behavioural and emotional problems (rs = .60, p < 0.001), but this association was not significant on the DSED (rs = .30, p = 0.118). In the case of teachers as informants there is a significant relationship between RAD and Conduct Problems (rs = .54) and Hyperactivity (rs = .46). The same conclusions were reached in the work of [14], where RAD was associated with conduct problems (r = .79), hyperactivity (r = .77), emotional problems (r = .50) and problems with peers (r = .62), which was not the case in the DSED.
Similarly, it is observed that in those children with comorbid DSED and RAD, the majority have behavioural problems (73 %) and emotional insensitivity (100 %) compared to the DSED group (χ2 = 8.1, p = 0.008). There were no differences between the RAD+DSED group and the DSED group about challenging behaviour, ASD, ADHD-C, ADHD-I, anxiety and depression [45]. On the other hand, a higher incidence of social problems was observed in children with RAD. Thus, children with RAD vs. children without RAD typically trust primary attachment figures such as teachers less (r = -.28, p < 0.05), irrespective of age, presence of autism or ADHD [39].
Similarly, RAD predicts low social functioning (β = -0.36, p < 0.01, 95%, [CI] [-.33, -.09]) and low social competence (β= -0.38, p < 0.01, 95%CI[-.05, -.01]) regardless of the length of time institutionalised and the number of changes of protective measure. On the other hand, DSED indicators (β = -0.38, p < 0.001, 95 % CI[-.49, -.16]) together with the number of measure changes (β = -0.22, p < 0.05, 95 % CI[-.29, -.01]) predicted worse social functioning. Furthermore, DSED predicted relational victimization (β = 0.29, p < 0.05, 95 % CI[.02, .14]) and lower social competence (β = -0.29, p < 0.01, 95 % CI[-.06, -.01]) [42]. It has been observed that children with RAD are more likely to be victims of bullying (RR 2.68, 95 % CI 1.50-4.77; p < 0.001), in particular, these children reported three times more bullying experiences than children without RAD. Similarly, the variable being bullied (RR 2.08, 95 % CI 1.17-3.69, p = 0.01) showed 2.8 times higher rates than children without RAD [47].
TAR-I symptomatology was significantly associated with lower social acceptance (B = - 0.051, p =0 .013), athletic competence (B = - 0.048, p = 0.028), romantic appeal (B = - 0.053, p = 0.007), and close friendship (B = - 0.052, p = 0.005), while higher DSED symptomatology with lower scores on scholastic competence (B = - 0.125, p = 0.038) [48].
3.4. Differences between the RAD Group with Other Children with Neurodevelopmental or Typical Developmental Problems
Fourteen articles included comparisons of children with RAD with other children, with neurodevelopmental difficulties, typically developing children or children at risk of social exclusion.
Firstly, when comparing children with RAD with children without RAD, it was observed that the former had a more negative internal model of themselves and others [51]. In general, children in protective measures versus children who were socially at risk showed more symptoms of RAD (p < 0.001) [15]. Ref. [50] find that the RAD group presented lower intellectual ability (F(1, 39) = 8.78, p < 0.01), more hyperactive (F(1, 38) = 10.86, p < 0.01), more depressive (F(1, 38) = 9.86, p < 0.01), anxious (F(1, 39) = 6.14, p < 0.05), depressive (F(1, 39) = 8.80, p < 0.01), anger (F(1, 39) = 8.93, p < 0.01), post-traumatic stress (F(1, 39) = 10.53, p < 0.01), dissociation (F(1, 39) = 11.34, p < 0.01) and autism-related symptoms (F(1, 37) = 7.28, p < 0.05), than the non-RAD group.
When comparing children with DSED with children without attachment disorders, the former showed higher scores in indiscriminate friendliness (t(35.78) = 9.47, p < 0.001), in reliability trust (t(64) = 2.58, p = 0.02), in general problem behaviour (t(64) = 8.09, p < 0.001), higher dependence on the teacher figure (t(58.26) = 3.76, p < 0.001), better overall self-concept (t(64) = 2.47, p = 0.02) and higher conflictual relationships with teachers (t(57.95) = 2.90, p = 0.005) [54]. Likewise, when adolescents in residential care with and without DSED were compared, the latter had lower mean scores on social acceptance (p = 0.012) and self-worth (p = 0.037). In the case of adolescents with RAD-I, they presented lower school self-concept (p = 0.020) and higher social self-concept (p = 0.021) than the control group. On the other hand, the DSED group presented lower mean scores in school self-esteem (p = 0.005), social acceptance (p = 0.015), athletic competence (p = 0.038), physical appearance (p = 0.048), and self-worth (p = 0.013) than the control group [48].
On the other hand, it is observed that children with RAD-I/DSED or ADHD have more behavioural problems and hyperactive symptoms than children with ASD, differences that were found to be statistically significant (p < 0.001). When comparing the RAD-I/DSED group with children with ASD, the RAD-I/DSED group showed fewer peer problems (p < 0.001), more behavioural problems (p = 0.008) and more prosocial behaviour (p = 0.006). However, children with ADHD showed more hyperactive symptoms than children with RAD-I/DSED (p < 0.001) [35].
In contrast to these results, the study by [45] showed that children with RAD and/or DSED showed higher percentages of more oppositional behaviour, conduct problems, impulsivity, hyperactivity and depression than the group of children with ADHD-I, as well as a higher percentage of conduct problems than the group of children with ADHD-C and the group of children with ASD. These differences in the percentages of problems between groups were statistically significant (χ2 = 6.8 - 128.8, p = 0.009 - p < 0.001). Also, children with RAD and/or DSED showed more lying, steal, unresponsive and overeating than children with ADHD-I, ADHD- or ASD. Likewise, children with RAD vs. children with ASD and typically developing children report more social difficulties in the use of context (t(81) = 2.886, p = 0.005), rapport (t(83) = 4.173, p < 0.001) and social relationships (t(82) = 2.849, p = 0.006). It is observed that up to 60% of these children meet the diagnostic criteria for autism [38].
In addition, children with RAD showed more socially disinhibited behaviour, hypervigilance and greater comfort with strangers than children with ASD (p < 0.05). In addition, children with RAD were more likely than children with ASD to report anxiety disorders (73 % vs. 18 %), ADHD (49 % vs. 29 %) and conduct problems (27 % vs. 2 %) [41]. However, children with RAD were also found to be more likely to have developmental speech and language disorders, ASD, ADHD, intellectual disability, anxiety disorders, conduct disorder, stress-related disorders, tic disorder and affective disorders than children with neurotypical development [37].
The comorbidity of RAD with DSED significantly increased the likelihood of showing more internalising problems, externalising problems and difficulties in general (p < 0.001) compared to children without personal difficulties or children with RAD or DSED only [34].When assessed in a sample of children with intellectual disabilities with and without attachment difficulties, it was observed that those with RAD showed more difficulties in daily living skills (p = 0.017) and communication (p = 0.037) than children without RAD. Similarly, children with DSED showed more problems in emotional (p = 0.023), socialisation (p = 0.044) and motor skills (p = 0.016). In both cases, children with RAD (p = 0.023) and children with DSED (p = 0.003) showed more egocentric behaviour than children without attachment problems and more antisocial behaviour problems (p = 0.047) [36].
Along the same lines, [43] focused their study on children in foster care. They differentiated into four groups: DSED, RAD-I, DSED+RAD-I (comorbid group) and no attachment disorder. The results indicate the existence of differences between groups concerning the presence of psychopathology (F(18, 267) = 2.15, p = 0.005). In particular, parents report that the DSED group had more clinical problems than the group without symptoms (F(1, 101)= 3.97 - 8.80, p = 0.049 - 0.004). Related to the above, when children present DSED and RAD (comorbid), they show more difficulties in general (F(12, 178) = 3.00, p = 0.001) but also more internalising (X = 76.84; SD = 17.04, p < 0.001) and externalising (X = 73.24; SD = 12.45, p < 0.001) problems than children without difficulties. On the other hand, children with DSED show more internalising (X = 57.48; SD = 13.66, p < 0.05), externalising (X = 61.14; SD = 13.75, p < 0.01) and general difficulties (X = 60.35; SD = 13.68, p < 0.01) than children without difficulties. The same conclusions were reached by the teachers when they assessed the group of children with RAD and DSED. They found more internalising problems (X = 61.05; SD = 16.97, p < 0.01), externalising problems (X = 66.83; SD = 12.91, p < 0.05) and total problems (X = 60.60; SD = 10.53, p < 0.05) than the group without attachment-related difficulties. These results are similar to those found by [46], who found that the group of children with RAD had higher percentages of emotional problems (60% vs. 36%), conduct problems (100 % vs. 71 %), hyperactivity (67 % vs. 21 %) and problems with peers (87 % vs. 71 %) than children without attachment problems.
Along the same lines, [43] focused their study on children in foster care. They differentiated into four groups: DSED, RAD-I, DSED+RAD-I (comorbid group) and no attachment disorder. The results indicate the existence of differences between groups concerning the presence of psychopathology (F(18, 267) = 2.15, p = 0.005). In particular, parents report that the DSED group had more clinical problems than the group without symptoms (F(1, 101)= 3.97 - 8.80, p = 0.049 - 0.004). Related to the above, when children present DSED and RAD (comorbid), they show more difficulties in general (F(12, 178) = 3.00, p = 0.001) but also more internalising (X = 76.84; SD = 17.04, p < 0.001) and externalising (X = 73.24; SD = 12.45, p < 0.001) problems than children without difficulties. On the other hand, children with DSED show more internalising (X = 57.48; SD = 13.66, p < 0.05), externalising (X = 61.14; SD = 13.75, p < 0.01) and general difficulties (X = 60.35; SD = 13.68, p < 0.01) than children without difficulties. The same conclusions were reached by the teachers when they assessed the group of children with RAD and DSED. They found more internalising problems (X = 61.05; SD = 16.97, p < 0.01), externalising problems (X = 66.83; SD = 12.91, p < 0.05) and total problems (X = 60.60; SD = 10.53, p < 0.05) than the group without attachment-related difficulties. These results are similar to those found by [46], who found that the group of children with RAD had higher percentages of emotional problems (60% vs. 36%), conduct problems (100 % vs. 71 %), hyperactivity (67 % vs. 21 %) and problems with peers (87 % vs. 71 %) than children without attachment problems.
4. Discussion
The results obtained in the present review point to a relationship between the presence of RAD inhibited, disinhibited or mixed, with other mental health and developmental problems, such as emotional symptoms (anxiety and depression), dissociative symptoms, stress-related difficulties (PTSD), behavioural problems (oppositional defiant disorder, dissocial disorder), relationship with peers, hyperactivity, autism or intellectual disability, among others. In addition to the above, children with RAD-I or DSED also present other difficulties in self-concept, social skills, bullying (victims and aggressors) or prosocial behaviour [13–16,34,39,40,42,44–48,51–54].
Research indicates that these problems are mainly related to the presence of a TAR-I and a lesser extent to the presence of a DSED [14,34,42,46,53], with the presence of personal and psychological difficulties being greater when RAD and DSED coexist [45]. All these data would confirm the first hypothesis of the study. Other qualitative studies, such as the one by [59] support these results by finding that children with RAD have more tantrums, which last longer, with the severity of the tantrums increasing with age. Attacks of rage are mainly directed towards the primary caregiver, suggesting that the child may use the caregiver, with whom they feel secure, as a way to release accumulated tensions due to their inability to cope with the tasks and demands of the context. The authors point to the relationship that may exist between implicit memory and anger attacks, addressing cognitive aspects related to the behaviour of children with RAD [60], an aspect that seems to be related to the neglect they suffered in the first years of life, affecting their capacity for self-regulation [61].
These problems in turn have repercussions at the social level. Ref. [47] point out that schoolchildren with symptoms of RAD are more likely to engage in victimisation or bullying towards their peers. This could be explained by the difficulty in early bonding with their attachment figures, misinterpreting the behaviours of other children, leading to victimisation or bullying during the school years, and perceiving the behaviours of others as possible threats, even in safe care settings.
Several authors highlight disinhibition/indiscriminate friendliness as one of the factors most present in children with RAD [15,41,54]. The hyper-sociable behaviours and positive appraisals they make of themselves and others could be related to a possible disconnection from their negative parenting experiences and challenging behaviours, playing a defensive or protective role for themselves. Importantly, overreliance on others can lead to the construction of unhealthy future relationships [54].
To the second hypothesis, which posed a greater presence of problems and comorbid disorders in the group with attachment disorders compared to other groups, the results indicate more problems in the RAD and/or DSED group compared to children who do not have disorders. Ref. [39] report lower trust in teachers and lower emotional security in the RAD group. Ref. [34] have more internalising and externalising problems, more hyperactivity and more behavioural problems. Ref. [43] more internalising and externalising problems as rated by parents or caregivers, while in the case of teacher ratings only when compared to the mixed group and not to the DSED. Ref. [37] a higher comorbidity with psychiatric disorders. Ref. [46] a higher presence of emotional, behavioural, hyperactivity and peer problems. Ref. [48] report lower self-concept in different areas, as do [51]. Ref. [50] report greater problems related to traumatic experiences such as anxiety, depression, anger and dissociation among others, as well as more internalising and externalising problems according to parents. [54] found in the DSED group a worse self-concept, more conflictual relationships, greater indiscriminate friendliness, reliability trust and general problems behaviour.
Ref. [36] found no differences in the presence of comorbid disorders between the RAD group and the group with ASD and ADHD. On the other hand, according to parents' assessments, the RAD-I and DSED groups show a greater presence of disruptive and antisocial behaviour in their children. Teachers reported more emotional problems in the DSED group and communication disorders in the RAD-I group.
When comparing the RAD group with the ASD group, [35] report greater behavioural problems and hyperactivity in the RAD group, as well as fewer problems with peers and greater prosociality. Ref. [41] report a higher presence of comorbid disorders such as anxiety disorders, ADHD and conduct problems. Ref. [37] an increased presence of conduct and emotional disorders. Ref. [38] greater difficulties in the use of pragmatics in language and a high relationship with ASD symptomatology.
About the ADHD and RAD groups, [46] report a greater presence of conduct problems, oppositional behaviour and depression, while [37] report a greater presence of anxiety disorders, adjustment disorders, and tics, among others, depending on the age of the children. On the other hand, [35] report greater hyperactivity in the ADHD group than in the RAD group.
All these results allow us to accept the second hypothesis of the study, which is that the group with RAD presents greater problematicity at different levels than children and adolescents without attachment disorders, with ADHD or with ASD.
The main limitations of this study are the number of databases consulted and the number of articles studied. Future studies should mainly address the study of the predictor variables of RAD, controlling for aspects such as the type of protection measure, changes in the measure, the quality of care or the typology that leads to a situation of neglect. All of this takes into account their relationship with the age variable. Furthermore, it may be important, both from an empirical and practical point of view, to study specific interventions aimed at reducing the emotional, psychological and social problems presented by children with RAD. To this end, it could be considered whether interventions aimed at addressing problems associated with insecure attachments or specific programmes associated with traumatic situations may have a beneficial effect in the case of RAD, or whether specific interventions focused on attachment disorders could be developed.
Given the scientific evidence pointing to the consequences on the psychological health of children with RAD, it is worth considering a diagnostic assessment in this sense, confirming or not the presence of the disorder, which can help to understand the behaviours and ways of relating to these children, giving guidance to caregivers, professionals and teachers, which can help, in the specific case of foster care, to favour child-family adaptation and prevent ruptures that lead to the failure of the placement, and therefore produce a new change of caregiver, This can help, in the specific case of foster care, to favour child-family adaptation and prevent ruptures that lead to the failure of foster care, and therefore produce a new change of caregivers, a variable related to the presence of RAD, but also to its maintenance.
Moreover, these results must be taken into account in the design of protection policies, avoiding as much as possible the transit of the child from one measure to another and from one caregiver to another, encouraging the most stable measures possible from the moment the child leaves his or her biological family.
It can be concluded that the presence of RAD has negative consequences on the mental health of children and adolescents. These consequences are greater in the case of RAD-I compared to DSED, being more important in this group of children compared to children with other disorders, such as ADHD or ASD.
Author Contributions
Conceptualization, F.T-K. and F.G-S..; methodology, F.T-K. and F.G-S; software, F. -K. and F.G-S; investigation, F.T-K., F.G-S, L.L-T. P.S-G; writing—original draft preparation, F.T-K. and F.G-S; writing—review and editing, F.G-S, L.L-T., P.S-G., supervision, F.G-S, L.L-T., P.S-G.; project administration, F.G-S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to thank Sofía Díaz Crespo, whose Master's thesis was directed by Dr. Francisco González-Sala, for his involvement in the study of reactive attachment disorder.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bowlby, J. The Diagnosis and Treatment of Psychological Disorders in Childhood. Health Education Journal 1954, 12, 59–68. [Google Scholar] [CrossRef]
- Zeanah, C.H.; Gleason, M.M. Annual Research Review: Attachment disorders in early childhood - clinical presentation, causes, correlates, and treatment. J. Child. Psychol. Psychiatry 2015, 56, 207–222. [Google Scholar] [CrossRef] [PubMed]
- Main, M. Introduction to the special section on attachment and psychopathology: 2. Overview of the field of attachment. J. Consult. Clin. Psychol. 1996, 64, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Fresno, A.; Spencer, R.; Retamal, T. Maltrato infantil y representaciones de apego: defensas, memoria y estrategias, una revisión. Univ. Psychol. 2012, 11, 829–838. [Google Scholar]
- Ellis, E.E.; Yilanli, M.; Saadabadi, A. Reactive Attachment Disorder. In StatPearls. StatPearls Publishing, 2023.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Washington, DC: American Psychiatric Association, 2013.
- Granqvist, P.; Sroufe, L.A.; Dozier, M.; Hesse, E.; Steele, M.; Van Ijzendoorn, M.; et al. Disorganized attachment in infancy: a review of the phenomenon and its implications for clinicians and policy-makers. Attach. Hum. Dev. 2017, 19, 534–558. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, S.; Breivik, K.; Monette, S.; Minnis, H. Potentially traumatic events in foster youth, and association with DSM-5 trauma- and stressor related symptoms. Child. Abuse Negl. 2020, 101, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.; Beckwith, H.; Duschinsky, R.; Forslund, T.; Foster, S.L.; Coughlan, B.; Pal, S.; Schuengel, C. Attachment difficulties and disorders. InnovAiT 2019, 12, 173–179. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (4th ed.). American Psychiatric Publishing, 1994.
- Zeanah, C.H. Beyond insecurity. J. Consult. Clin. Psychol. 1996, 64, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Zilberstein, K. Clarifying core characteristics of attachment disorders. Am. J. Orthopsychiatry 2006, 76, 55–64. [Google Scholar] [CrossRef]
- Gleason, MM.; Fox, NA.; Drury, S.; Smyke, A.; Egger, HL.; Nelson, CA.; Gregas, MC.; Zeanah, CH. Validity of evidence-derived criteria for Reactive Attachment Disorder: Indiscriminately Social/Disinhibited and Emotionally Withdrawn/Inhibited types. J. Am. Aca Child. Adol Psychiatry 2011, 50, 216–231. [Google Scholar] [CrossRef]
- Lehmann, S. , Breivik, K.; Heiervang, ER.; Havik, T.; Havik, OE. Reactive Attachment Disorder and Disinhibited Social Engagement Disorder in school-aged foster children - a confirmatory approach to dimensional measures. J. Abnorm. Child. Psychol. 2016, 44, 445–457. [Google Scholar] [CrossRef] [PubMed]
- Kay, C.; Green, J. Reactive Attachment Disorder following early maltreatment: Systematic evidence beyond the institution. J. Abnorm. Child. Psychol. 2013, 41, 571–581. [Google Scholar] [CrossRef] [PubMed]
- Kay, C.; Green, J.; Sharma, K. Disinhibited Attachment Disorder in UK adopted children during middle childhood: Prevalence, validity and possible developmental rigin. J. Abnorm. Child. Psychol. 2016, 44, 1375–1386. [Google Scholar] [CrossRef] [PubMed]
- Haugaard, JJ.; Hazan, C. ; Recognizing and treating uncommon behavioral and emotional disorders in children and adolescents who have been severely maltreated: Reactive Attachment Disorder. Child. Maltreat 2004, 9, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, S.; Havik, OE.; Havik, T.; Heiervang, ER. Mental disorders in foster children: a study of prevalence, comorbidity and risk factors. Child. Adolesc. Psychiatry Ment. Health 2013, 7, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Black, C.; Zeanah, CH. Reactive Attachment Disorder and Disinhibited Social Engagement Disorder. The Encyclopedia Clin. Psychol. 2015, 1–3. [Google Scholar]
- Humphreys, KL.; Nelson, CA.; Fox, NA.; Zeanah, CH. Signs of reactive attachment disorder and disinhibited social engagement disorder at age 12 years: Effects of institutional care history and high-quality foster care. Dev. Psychopathol. 2017, 29, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Román, M.; Palacios, J.; Minnis, H. Changes in Attachment Disorder symptoms in children internationally adopted and in residential care. Child. Abuse Negl. 2022, 130, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372. [Google Scholar] [CrossRef]
- Santos, CM.; Pimenta, CA.; Nobre, MR. The PICO strategy for the research question construction and evidence search. Rev. Latino-am Enfermagem 2007, 15, 508–511. [Google Scholar] [CrossRef]
- Covidence systematic review software. Veritas Health Innovation, Melbourne, Australia. https://www.covidence.org. Accessed 22 Feb 2023.
- Ogrinc, G.; Davies, L.; Goodman, D.; Batalden, P.; Davidoff, F.; Stevens, D. SQUIRE 2.0 (Standards for QUality Improvement Reporting Excellence): Revised Publication Guidelines from a Detailed Consensus Process. J. Nurs. Care Qual. 2016, 31, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Orwin, R.G. Evaluating coding decisions. In The handbook of research synthesis; Russell Sage Foundation, EEUU, 2018. pp. 95–107.
- Hernández-Nieto, RA. Contributions to Statistical Analysis: The Coefficients of Proportional Variance, Content Validity and Kappa. CreateSpace Independent Publishing Platform, 2002.
- Smyke AT, Zeanah CH. Disturbances of attachment interview. New Orleans: Tulane University; 1999 (Unpublished Manual).
- Angold, A.; Prendergast, M.; Cox, A.; Harrington, R.; Simonoff, E.; Rutter, M. The child and adolescent psychiatric assessment (CAPA). Psychol. Med. 1995, 25, 739–753. [Google Scholar] [CrossRef] [PubMed]
- Minnis, H.; Green, J.; O’Connor, T.; Liew, A.; Glaser, D.; Taylor, E.; Follan, M.; Young, D.; Barnes, J.; Gillberg, C.; et al. An exploratory study of the association between reactive attachment disorder and attachment narratives in early school-age children. J. Child. Psychol. Psychiatry 2009, 50, 931–942. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, S.; Monette, S.; Egger, H.; Breivik, K.; Young, D.; Davidson, C.; Minnis, H. Development and examination of the reactive attachment disorder and disinhibited social engagement disorder assessment interview. Assessment 2020, 27, 749–765. [Google Scholar] [CrossRef] [PubMed]
- Kurth, R.A.; Körner, A.; Geyer, M.; Pokorny, D. Relationship Patterns Questionnaire (RPQ): Psychometric properties and clinical applications. Psychother. Res. 2004, 14, 418–434. [Google Scholar] [CrossRef]
- Corval, R.; Baptista, J.; Fachada, I.; Soares, I. Rating of inhibited attachment disordered behavior. Unpublished manuscript, Universidade do Minho, 2016.
- Elovainio, M.; Raaska, H.; Sinkkonen, J.; Makipaa, S.; Lapinleimu, H. Associations between attachment-related symptoms and later psychological problems among international adoptees: results from the FinAdo study. Scand. J. Psychol. 2015, 56, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Coughlan, B.; Woolgar, M.; Van Ijzendoorn, MH.; Duschinsky, R. Socioemotional profiles of autism spectrum disorders, attention deficit hyperactivity disorder, and disinhibited and reactive attachment disorders: a symptom comparison and network approach. Dev. Psychopathol. 2021, 35, 1026–1035. [Google Scholar] [CrossRef] [PubMed]
- Giltaij, HP.; Sterkenburg, PS.; Schuengel, C. Psychiatric diagnostic screening of social maladaptive behaviour in children with mild intellectual disability: differentiating disordered attachment and pervasive developmental disorder behaviour. J. Intellec Disabil. Res. 2015, 59, 138–149. [Google Scholar] [CrossRef] [PubMed]
- Hong, M.; Moon, D.S.; Chang, H.; Lee, S.Y.; Cho, S.W.; Lee, K.; Bahn, G.H. Incidence and comorbidity of Reactive Attachment Disorder: Based on national health insurance claims data, 2010–2012 in Korea. Psychiatry Investig 2018, 15, 118–123. [Google Scholar] [CrossRef]
- Sadiq, FA.; Slator, L.; Skuse, D.; Law, J.; Gillberg, C.; Minnis, H. Social use of language in children with reactive attachment disorder and autism spectrum disorders. Eur. Child. Adolesc. Psychiatry 2012, 21, 267–276. [Google Scholar] [CrossRef]
- Bosmans, G.; Spilt, J.; Vervoort, E.; Verschueren, K. Inhibited symptoms of Reactive Attachment Disorder: links with working models of significant others and the self. Attach. Hum. Dev. 2019, 21, 190–204. [Google Scholar] [CrossRef]
- Bruce, M.; Young, D.; Turnbull, S.; Rooksby, M.; Chadwick, G.; Oates, C.; et al. Reactive Attachment Disorder in maltreated young children in foster care. Attach. Hum. Dev. 2019, 21, 152–169. [Google Scholar] [CrossRef]
- Davidson, C.; O’Hare, A.; Mactaggart, F.; Green, J.; Young, D.; Gillberg, C.; et al. Social relationship difficulties in autism and reactive attachment disorder: Improving diagnostic validity through structured assessment. Res. Dev. Disabil. 2015, 40, 63–72. [Google Scholar] [CrossRef]
- Guyon-Harris, K.L.; Humphreys, K.L.; Fox, N.A.; Nelson, C.A.; Zeanah, C.H. Signs of attachment disorders and social functioning among early adolescents with a history of institutional care. Child. Abuse Negl. 2019, 88, 96–106. [Google Scholar] [CrossRef]
- Jonkman, C.S.; Oosterman, M.; Schuengel, C.; Bolle, E.A.; Boer, F.; Lindauer, R.J. Disturbances in attachment: inhibited and disinhibited symptoms in foster children. Child. Adolesc. Psychiatry Ment. Health 2014, 15, 1–7. [Google Scholar] [CrossRef]
- Kocovska, E.; Puckering, C.; Follan, M.; Smillie, M.; Gorski, C.; Lidstone, E.; Pritchett, R.; Hockaday, H.; Minnis, H. Neurodevelopmental problems in maltreated children referred with indiscriminate friendliness. Res. Dev. Disabil. 2012, 33, 1560–1565. [Google Scholar] [CrossRef] [PubMed]
- Mayes, S.D.; Calhoun, S.L.; Waschbusch, D.A.; Breaux, R.P.; Baweja, R. Reactive attachment/disinhibited social engagement disorders: Callous-unemotional traits and comorbid disorders. Res. Dev. Disabil. 2017, 63, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Moran, K.; McDonald, J.; Jackson, A.; Turnbull, S.; Minnis, H. A study of Attachment Disorders of young offenders attending specialist services. Child. Abuse Negl. 2017, 65, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Raaska, H.; Lapinleimu, H.; Sinkkonen, J.; Salmivalli, C.; Matomäki, J.; Mäkipää, S.; et al. Experiences of School Bullying Among Internationally Adopted Children: Results from the Finnish Adoption (FINADO) Study. Child. Psychiatry Hum. Dev. 2012, 43, 592–611. [Google Scholar] [CrossRef]
- Seim, A.R.; Jozefiak, T.; Wichstrøm, L.; Lydersen, S.; Kayed, N.S. Self-esteem in adolescents with reactive attachment disorder or disinhibited social engagement disorder. Child. Abuse Negl. 2021, 118, 1–13. [Google Scholar] [CrossRef]
- Seim, A.R.; Jozefiak, T.; Wichstrøm, L.; Lydersen, S.; Kayed, N.S. Reactive attachment disorder and disinhibited social engagement disorder in adolescence: co-occurring psychopathology and psychosocial problems. Eur. Child. Adolesc. Psychiatry 2022, 31, 85–98. [Google Scholar] [CrossRef]
- Shimada, K.; Takiguchi, S.; Mizushima, S.; Fujisawa, T.X.; Saito, D.N.; Kosaka, H.; et al. Reduced visual cortex grey matter volume in children and adolescents with reactive attachment disorder. NeuroImage Clinical 2015, 9, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, P.; Iwanski, A. Attachment Disorder behavior in early and middle childhood: associations with children's self-concept and observed signs of negative internal working models. Attach. Hum. Dev. 2019, 21, 170–189. [Google Scholar] [CrossRef] [PubMed]
- Pritchett, R.; Pritchett, J.; Marshall, E.; Davidson, C.; Minnis, H. Reactive Attachment Disorder in the general population: A hidden ESSENCE disorder. Sci. World J. 2013, 2013, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Vervoort, T.; Trost, Z.; Van Ryckeghem, D.M.L. Children’s selective attention to pain and avoidance behaviour: The role of child and parental catastrophizing about pain. Pain. 2013, 154, 1979–1988. [Google Scholar] [CrossRef]
- Vervoort, E.; Bosmans, G.; Doumen, S.; Minnis, H.; Verschueren, K. Perceptions of self, significant others, and teacher–child relationships in indiscriminately friendly children. Res. Dev. Disabil. 2014, 35, 2802–2811. [Google Scholar] [CrossRef] [PubMed]
- Egger, H.L.; Erkanli, A.; Keeler, G.; Potts, E.; Walter, B.K.; Angold, A. Test-Retest Reliability of the Preschool Age Psychiatric Assessment (PAPA). J. Am. Acad. Child. Adolesc. Psychiatry 2006, 45, 538–549. [Google Scholar] [CrossRef]
- World Health Organization. The ICD-10: Version 2010. Classification of Mental and Behavioral Disorders: Diagnostic Criteria for Research. Geneva. 2010.
- World Health Organization. The ICD-10 Classification of Mental and Behavioral Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva, Switzerland: World Health Organization, 1992.
- World Health Organisation. The ICD-10 classification of mental and behavioural disorders: diagnostic criteria for research. World Health Organisation, Geneva. 1993.
- Vasquez, M.; Miller, N. Aggression in Children with Reactive Attachment Disorder: A sign of deficits in emotional regulatory processes? J. Aggress, Maltreat Trauma. 2018, 27, 347–366. [Google Scholar] [CrossRef]
- Corbin, J. Reactive Attachment Disorder: A biopsychosocial Disturbance of Attachment. Child. Adolesc. Soc. Work. J. 2007, 24, 539–552. [Google Scholar] [CrossRef]
- Schore, J.R.; Schore, A.N. Modern attachment theory: The central role of affect regulation in development and treatment. Clin. Soc. Work. J. 2008, 36, 9–20. [Google Scholar] [CrossRef]
Figure 1.
Flow of information through the different phases of a systematic review.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



