
Submitted:
21 November 2023
Posted:
24 November 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Cross-sectional survey was conducted to capture the true extent of COVID-19 exposure among students and staff of Polytechnic High School (PHS). Random cluster sampling was carried out between May 19 and August 18, 2022, after the fourth wave of COVID-19 transmission. IgM and IgG SARS-CoV-2 antibodies were screened using WANTAI SARS-CoV-2 ELISA assays. Seroprevalence and descriptive statistics were calculated. Moreo-ver, the association between seropositivity and different factors (age, gender, preventive measures comorbidity, and symptoms, etc.) was determined using Logistic Regression. The overall IgG and IgM seroprevalence were 92% and 6.91% respectively. We found a higher IgM seroprevalence in men than women (9.4% vs. 5.6%) and a lower IgM seroprevalence in (18-25) age group compared to (55-65) years. Low compliance with preventive measures was found with a significant IgM seroprevalence depending on non-respect of social distancing (p = 0.008). A total of 70% of participants presented symptoms linked to COVID-19 at the moment of the survey. Results revealed a significant difference according to IgG seroprevalence among participants who declared fa-tigue symptoms 92.06% compared to those who did not 80.39% (p = 0.0027). IgM seropositivity was associated with Body Mass Indice (BMI) categorized (O.R. 0.238, p = 0.043), ethnic group (O.R. 0.723, p = 0.046) and marital status (O.R. 2.399, p = 0.021). Moreover, IgG seropositivity was associated with Chronic sinusitis comorbidity (O.R. 0.238, p = 0.043) and vaccination status (O.R. 4.741, p < 0.001). The majority of students and staff have al-ready been exposed to SARS-CoV-2 and confirm the circulation of SARS-CoV-2 in PHS at the time of the survey. Our results underline the importance of sero-epidemiological surveys to estimate the real impact of the COVID-19 pandemic in a community and to monitor disparities in antibody response in the population.
Keywords:
COVID-19
; SARS-CoV-2 antibodies
; sero-epidemiological survey
; Polytechnic High School
; Senegal
1. Introduction
The Coronavirus 2019 (COVID-19), newly identified in December 2019 in Wuhan, China, is an infectious disease caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) [1,2]. On January 30 2020, the World Health Organization (WHO) declared COVID-19 a public health emergency of global concern, and on March 11, 2020, it announced the COVID-19 epidemic as a pandemic [3]. By November 12, 2023, more than 697 million of people had been infected worldwide, with over 6.9 million deaths [4].
The COVID-19 outbreak had substantial economic, social, and health repercussions and damaging educational consequences [5,6,7]. In April 2020, the World Bank estimated that higher education institutions had been closed in 175 countries and that studies had been interrupted or significantly disrupted due to COVID-19, affecting more than 220 million students [8]. The pandemic forced academic communities to adopt online platforms for the continuity of teaching and learning activities, negatively impacting learning outcomes, particularly in developing countries where the lack of network infrastructures, computers, and internet access is challenging distance learning in developing countries [9,10,11].
In Senegal, a West Africa Country, the first case of SARS-CoV-2 was identified on March 2, 2020. Since then, the number of cases has risen considerably, and the country currently has more than 89,022 confirmed cases of COVID-19 and 1,971 deaths [12]. The onset of the pandemic led the government authorities to close higher education establishments from March 16 to August 31 2020. The reopening of the establishments took place with the introduction of sanitary protocols that emphasized the reinforcement of barrier measures (wearing masks, hand washing with soapy water or hydroalcoholic gel, respect for social distancing and systematic taking of body temperature at campus access points) [13]. However, these measures have often been insufficient to stem the spread of the virus. Clusters quickly appeared in some establishments, including the Cheikh Anta Diop (CAD) University, located in Dakar, the capital of Senegal.
The failure of strategies to combat the spread of the virus could be linked to multiple factors, including (i) CAD University ecosystem, with its over 80,000 students from diverse origins. The consequence is overcrowding in student residences that caused the spread of the virus; (ii) the university environment is mainly populated by young people, who do not seem to be fully aware of the risks associated with the COVID-19 health crisis. [14]; (iii) the promiscuity in the Halls of residence, making it difficult to comply with social distanciation measures; (iv) Lastly, lack of vaccine deployment, also reluctance was noted among young people, which also contributes to low vaccination coverage in universities [15].
Faced with all these difficulties, it was essential to adopt cyclical measures to manage the COVID-19 pandemic, characterised by the virus spreading in waves [16,17]. These measures could involve introducing survey studies based on diagnostic testing and mass screening protocols to diagnose and follow up with people exposed to or infected with SARS-CoV-2. In practice, detecting viral RNA by RT-PCR is the reference method for confirming the diagnosis of SARS-CoV-2 infection [18,19]. However, access to diagnostic tests still needs to be improved in poor countries [20]. The other way to estimate the true extent of the epidemic is to conduct Seroprevalence surveys [21,22]. Sero-epidemiological studies to detect the presence of anti-SARS-CoV-2 antibodies are a valuable tool for assessing the timing of the epidemic. It can help to confirm the presence of a recent infection when PCR is limited. Some antibodies, such as IgG, can even be detected years after exposure [23]. Their detection can be used to identify previous or recent exposure to SARS-CoV-2. By carrying out this analysis on a representative population, it is possible to estimate what proportion of the population has already been exposed to the new coronavirus [24]. This information is helpful in identifying the epidemic phases and can help the authorities to make decisions and even to anticipate appropriate on measures to contain the pandemic's spread [25]. Sero-epidemiological studies have been conducted in academic institutions such as universities in many countries [26,27,28,29]. However, more studies are highly relevant because university communities (faculty, staff and students) could be among the most exposed to SARS-CoV-2. In Senegal, no seroprevalence studies have been conducted in cohorts of educational institutions.
Therefore, we conducted an on-site screening project at Polytechnic High School (PHS), a public institution with an inter-African vocation at Cheikh Anta Diop University from May to August 2022 after the fourth wave of Coronavirus disease in Senegal. We aimed to assess the seropositivity of SARS-CoV-2 IgM and IgG antibodies to estimate the fraction of the PHS population already infected by the virus, including recent or current and anterior or vaccination exposition, and to investigate the factors associated with seropositivity against SARS-CoV-2 antibodies.
2. Materials and Methods
2.1. Study Design and Population
The SARSESP (“Etude de Seroprevalence du SARS-CoV-2 au sein de l’École Supérieure Polytechnique”, in the Cheikh anta DIOP University (CAD University)) project is an on-site university population-based cross-sectional study. The sampling occurred at the PHS, an establishment of CAD university. Sixty thousand and one hundred thirty-three Students, Professors, and Technicians, Administrative and Service (TAS) officers at SPS were invited by e-mail to enrol in the study. The participants were volunteers and have been registered online from May 19 to August 18 2022. A questionnaire was administered to each participant after consent, blood samples were taken for SARS-CoV-2 antibody detection.
2.2. Sample Size Calculation
We used stratified random sampling: the first stratum concerned professors, the second TAS officers and the third students. Systematic random sampling was used within each stratum to determine the required number of subjects. Using the lists provided by the student affairs and human resources departments, we calculated the sample size based on the hypothesis of an expected seroprevalence of 45%, with a precision of 5%, a design effect of 1.96, and a nonresponse rate of 65%. We determined that >450 participants needed to be recruited. To increase the accuracy of the results, this size was multiplied by 2, giving a sample size of 898, and rounded up to 1000 to account for any lost records. The survey step for selecting statistical units was 6133/1000, i.e. a step = 6. In this study, an allocation proportional to the size of each stratum was used. Thus, we considered a proportion of 83.54% for students, 9.97% for professors and 6.47% for TAS officers. Then, we obtained 65 TAS officers, 100 professors and 835 students. The inclusion criteria were age over eighteen (18) years, informed consent signed, and questionnaire completion. Then, the non-inclusion criteria were under 18 years of age, non-consent and contraindications to venous blood sampling (anaemia, Infection or hematoma at a prospective venipuncture site, etc.).
2.3. Questionnaire
We shared an interviewer-administered questionnaire with participants on an electronic tablet (https://enquete.ucad.sn/index.php/598685?lang=fr). The questionnaire covered points regarding different factors to assess for relationships between IgM and IgG seropositivity and these factors. Questions relating to sociodemographic characteristics were collected, such as age, sex, occupation, education level, nationality, ethnic group and accommodation type. We also collected comorbidities and alcohol and tobacco intake, SARS-CoV-2 vaccination status, preventive measures related to SARS–CoV–2 practices, and exposures to SARS-CoV-2. Exposures to SARS-CoV-2 comprised a previous SARS-CoV-2 infection, auto-diagnostic or laboratory-confirmed SARS-CoV-2 infection during 2 weeks before the survey were also collected (Supplementary Materials 1). We provided all recruitment participants with face masks and hand sanitisers and encouraged them to practice physical and social distancing. The questionnaire on COVID-19 was posted online by the IT and Information Systems Department of Cheikh Anta Diop University.
2.4. Blood Collection and SARS-CoV-2 Antibodies Detection
After each participant signed the consent form (Supplementary Materials 2), 10 mL whole blood sample was collected into a dry vacutainer tube by standard venipuncture technique. Blood samples were centrifuged at 2,500 rpm for 10 minutes. Then, the plasma was collected and stored in cryotubes at -80 °C at the GRBA-BE laboratory biobank in Polytechnic High School until the tests were carried out. Seropositivity to anti-SARS-CoV-2 antibodies was used as a biomarker of exposure to the SARS-CoV-2 virus. IgM class immunoglobulins were used as a marker of recent or current infection (usually from days 5-7 after symptoms appear, but sometimes later and decrease at days 15-22), and IgG class immunoglobulins were used as a biomarker of older infection (detectable from day 11 post symptom, reaching a maximum 3-4 weeks after and persist days 90 after) [30,31].
Serological tests were performed by qualitative ELISA for IgM and quantitative ELISA for IgG following the instructions for the WANTAI SARS-CoV-2 IgM ELISA (Beijing Wantai Biological Pharmacy Enterprise, Beijing, China; Ref. WS-1196 and WS-1396) recommended by the WHO for sero-epidemiological studies, which detects total antibodies (including IgM and IgG) binding the SARS-CoV-2 spike protein receptor-binding domain (S1/RBD) [32]. The main characteristics of each immunoassay are depicted in Supplementary Materials 2&3. Serum samples were analysed in duplicate according to the supplier’s recommendations.
2.5. Statistical Analyses
Statistical analyses were performed using Rstudio (version R 4.2.1) and GraphPad Prism (version 10.1.1 (316)) softwares. Continuous variables were described as mean (standard deviation) or median (interquartile range). Normally distributed variables were compared with a t-test, and nonparametric data were compared with the Mann-Whitney test. Categorical variables were presented as percent, and Fisher exact tests or chi-squared tests were used for proportional assessments. For all statistical tests, we accepted a two-sided level of significance was set at p ≤ 0.05.
SARS-CoV-2 seroprevalence was defined as the ratio of the number of people who developed anti-SARS-CoV-2 antibodies to the general population. Confidence intervals (95% CI) for seroprevalence were estimated using the Clopper-Pearson method. Using logistic regressions, we sought to understand how the IgM and IgG seropositivity are influenced by various variables such as age, gender, occupation, education level, nationality, type of accommodation, etc. Then we assess how these factors are associated with an individual's immune response to a disease such as COVID-19 or a specific pathogen. The analyses were carried out after carefully handling the database and processing missing data.
2.6. Ethics Statement
This research complies with ethical recommendations. The project protocol has been validated by the National Health Research Ethics Committee (CNERS) of the Ministry of Health and Social Action. The research protocol was drawn up in accordance with Senegalese laws and regulations governing the confidentiality of personal data. The study was approved by the Senegalese National Ethics Committee for Research in Health (Reference number N°000043/MSAS/CNERS/SP, 28 February 2022).
3. Results
3.1. Baseline characteristics of participants
From the 6,133 students, professors and, TAS officers of PHS who were invited to participate in the study between 19 May 2020 and 18 August 2022, 637 (10,38%) participants were finally included (Figure 1). The most represented group was students ( 88.38%), followed by TAS officers (8.16%), and professors (3.45%). The mean age was 23.20 years, ranging from 18 to 63 years. The population's median age was 21 years, with most participants aged 18 to 25 years, representing 85.7% of the population (Table I). 62.0% of the participants were female, and 36.89% were male with male-to-female ratio = 0.59. Most participants were Senegalese (94.66%) and lived in family homes (54.6%). In addition, most ethnic groups in the PHS population were Wolof (31.24%), Fula (24.33%) and Serer (21.98%). The prevalences of active smoking and taking alcohol were relatively low in the PHS community at the moment of the survey (1.9%) and (3.62%), respectively. Demographic data are shown in Table I. Calculation of body mass index also revealed the highest prevalence of normal weight (37.68%), followed by underweight (10.8%) and overweight/obesity, 8.32%). The most common blood group is 0+ (47.08%). At the time of data collection, unvaccinated vs. vaccinated participants were 57.46% and 35.01 %)respectively. Regarding the clinical characteristics of the population, several comorbidities have been reported. In decreasing order of frequency, we found asthma (14.1%), allergy (4.6%), rheumatism (3.6%), sickle cell disease (2.8%), hypertension (1.9%) and sinusitis (1.6%) (Supplementary Data S1).
3.2. Seroprevalence of IgM et IgG SARS-CoV-2 antibodies
For overall participants, 6.91%, (95% CI: 4.93 – 8.87) were seropositive for SARS-CoV-2 IgM antibody, and 92%, (95% CI: 89.90 – 94.11)were seropositive for SARS-CoV-2 IgG. Then, we analysed IgM and IgG seroprevalence according to the different characteristics of the study population shown in Table I.
Regarding IgM seroprevalence, the results showed significant age-dependent (p < 0.001) with higher seroprevalence in the (25-35) age group with 23.69% (95% CI: 20.39 – 27) compared to (18-25) age group with 5.5% (95% CI: 3.73 – 7.27). According to gender, IgM seroprevalence was higher in men, 9.4% (95% CI: 7.13 – 11.67) than in women, 5.6% (95% CI: 3.51 – 7.38), but no significant differences were found by sex (p = 0.83). There were no significant differences according to the other sociodemographic parameters regarding IgM antibodies seropositivity, such as occupation, level of education, ethnic group, accommodation type and size, but with some differences between sub-groups. For example, depending on the type of residence, we found a higher IgM seroprevalence among those living in halls of residence, 7.97% (95% CI: 5.87 – 10.07) compared to those living in family homes, 6.68% (95% CI: 4.74 – 8.62)], p = 0.73.
Concerning IgG seroprevalence, we found a significant difference between people who drank alcohol [95.24% (95% CI: 93.58 – 96.89)] and those who didn’t [90.80%, (95% CI: 88.55, 93.04)], with p = 0.038. Then, a very significant difference was found according to vaccination status, with a high seropositivity rate in vaccinated people [96.83% (95% CI: 95.47 – 98.19)] compared to unvaccinated [86.58% (95% CI: 83.93 – 89.22)], p < 0.0001. No significant difference was found between IgG seroprevalence according to age groups, while IgG seroprevalence was lower in men [89.9% (95% CI: 87.60 – 92.24)] than in women [90.6% (95% CI: 88.33 – 92.87)], p = 0.98. Then, no significant differences were found by sex (p = 0.83). IgM and IgG seroprevalences were higher in Professors and TAS officers than in students, yet this difference was not statistically significant (p = 0.71). We then analysed the IgM and IgG antibodies' seroprevalence according to different comorbidities reported in the study and didn’t find significant differences (Appendix A).
3.3. Compliance with preventive measures and antibodies’ seroprevalence
Most respondents reported a low level of compliance with the following preventive measures recommended by the health authorities: 31.39% among participants declared that they had wearing mask always or often, and 18.21% observed a physical distance (minimum 2 m) over the last 15 days. However, most participants reported high-level of compliance with hand washing: 75.35% had washed their hands always or often (Figure 2A). For social distancing, the majority of participants, 71.58%, reported 0-2 frequencies of Participation in social events during the 15 days before the survey; 70.8% declared that they used public transport at least 2 times a day; and finally, 62.16% had visited someone 15 days before the survey (Figure 2B). Concerning antibodies’ seroprevalence, we found a significant difference in IgM seroprevalence according to the ‘number of visits made to someone’ during the 15 days before the survey (p = 0.008) (Appendix B). However, we found no significant difference in IgG seroprevalence and compliance with barrier measures.
3.4. Diagnosis and Clinical symptoms related to COVID-19 and antibodies’ seroprevalence
During the survey, a low rate of participants, 8.95% declared to be tested positive by RT-PCR for COVID-19 infection since the start of the pandemic, 82.89% declared tested negative, while 8.16% did not state this question (Figure 3A). 8.16% participants reported having been diagnosed as COVID-19 positive by a practitioner, and 29.98% reported having been self-diagnosed as COVID-19 positive. A large proportion of participants 69.70%, declared to have had a history of symptoms compatible with COVID-19 during the 15 days before the survey with at least one COVID-related clinical symptom, including most common: cough (25.43%), fatigue/weakness (39.56%), fever (12.87%), sore throat (14.91%) and headache (50.08%). Finally, 21.98% participants were asymptomatic (Figure 3B).
Concerning COVID-19 diagnosis and clinical symptoms, we found a significant difference between IgM seroprevalence and self-COVID-19-diagnosis with higher seroprevalence among those who didn’t declare self-diagnosis of the disease 10.57% (95% CI: 7.88 – 12.59) than who did 5.24% (95% CI: 3.51 – 6.97), p = 0.049 (Table II). According clinical symptoms, no significant differences in terms of IgM seroprevalence were found; however, a higher IgG seroprevalence was found in participants who declared fatigue symptoms, 92.06% (95% CI: 89.96 – 94.16) compared to those who did not 80.39% (95% CI: 77.31 – 83.47) with a significant p = 0.0027.
3.5. Risk factors associated with SARS-CoV-2 IgM and IgG seropositivity among PHS community
Multiple Logistic regression analysis didn’t show an association between IgG seropositivity and the factors studied. Interestingly, an association between IgM seropositivity and participants’ ethnic group [O.R. 0.723 95% CI: 0.49 – 0.96, (p = 0.046)] was reported (Table III). Using a univariate analysis, we found a significant association between IgM seropositivity and marital status [O.R. 2.399 95% CI: 1.08 – 4.87 (p = 0.021)], and Body Mass Indice (BMI) categorised [O.R. 2.015 95% CI: 1.12 – 3.56, (p = 0.016)]. In addition, on one hand, we found a significant association between vaccination and IgG seropositivity [O.R. 4.741 95% CI: 2.25 – 11.65, (p < 0.001)]; on the other hand, no associations were observed between SARS-CoV-2 seropositivity and sex and age groups. Concerning comorbidities, our result showed a significant association between sinusitis and IgG seropositivity [O.R. 0.238 95% CI: 0.064 – 1.13, (p = 0.043)]. No association was found between antibodies seropositivity and other comorbidities and preventive measures (Appendix C & D). About COVID-19 symptoms, we found a significant association between fatigue symptoms and IgG seropositivity [O.R. 2.829, 95% CI: 1.44 – 5.55 (p = 0.0023)] (Appendix D).
4. Discussion
This is the first sero-epidemiological survey of COVID-19 carried out in an educational establishment in Senegal. The study aimed to determine the seroprevalence of IgM and IgG SARS-CoV-2 antibodies and associated risk factors in order to assess the extent of virus exposure within the Polytechnic High School in Cheikh Anta Diop University. The survey was carried out on samples collected from personnel and students from May 2022 to August 2022, after the fourth wave of COVID-19 in Senegal.
A total of 637 participants were included in the study, 62% of whom were women and 37% men. The median age was 21, which is justified by the fact that the study was conducted in a university environment. Consequently, the study population predominantly comprises students representing around 86% of the participants.
We showed high IgG and IgM SARS-CoV-2 antibodies seroprevalences of 92% (95% CI: 89.90 – 94.11) and 6.91% (95% CI: 4.93 – 8.87), respectively. The IgM seroprevalence indicates that the virus was circulating within PHS at the time of the survey, with people who were currently or recently infected. Indeed, in seroprevalence surveys, it is recommended to use IgM and IgG detection to diagnose recent and previous infections [33]. IgM antibody levels rise around a week after the initial infection, indicating a recent infection [23]. IgG antibodies appear later than IgM antibodies (generally within 14 days of infection). They can persist for up to a year [34,35], meaning that IgG antibodies serve as an indicator of an old infection [36].
The very IgG high seroprevalence could be due to increased exposure to the SARS-CoV-2 virus and the anti-COVID vaccination policy implemented by the authorities. Data from the Ministry of Health showed that our study occurred after the fourth wave of COVID-19 in Senegal in January 2022 and the deployment of the COVID-19 vaccine began on February 2021 [12], which could explain our result. The first seroprevalence surveys carried out in Senegal were conducted in 2020 after the first wave and showed a lower seroprevalence of around 20%. Between June and September 2020, Seck et al. found a SARS-CoV-2 seroprevalence rate of 21.1% (95% CI = 16.7–26.1%) [37]. During the same period, Ahouidi et al. conducting a study between June and October 2020. They found that the overall positivity rate was 20.4% and significant geographical differences in seropositivity with a higher seroprevalence in Dakar, around 40% [38]. Then, Talla et al. found an adjusted national prevalence of anti-SARS-CoV-2 IgG/IgM in Senegal estimated to be 28.4% between October 24 and November 26, 2020 [39]. A high SARS-CoV-2 seroprevalences and its variability between localities were also reported in the second national population based cross-sectional survey (72,2%) conducted in November 2021 [40] [and among pregnant women attending the antenatal consultation (69,4%) during the second and third waves of COVID-19 in Senegal [41].
Results showed a sharp increase in seroprevalence since 2020 in Senegal, and data corroborating the finding that several variants have circulated in the country, including the delta variant, which has been the most deadly and caused a peak in the number of confirmed cases in July 2021 [42]. Study carried out in Africa at the same time as our survey showed similarly high seroprevalence, with 74% between July and August 2022 in Bangui, Central African Republic [43]. In Nigeria, in early 2021, there was a high SARS-CoV-2 seroprevalence of 72.4% [44]. Given this situation, it seems very important to carry out cyclical epidemiological survey studies to measure the extent of the spread of the SARS-CoV-2.
Interestingly, we found a higher IgM seroprevalence in men than women (9.4% vs. 5.6%). Then, our result would suggest that men are more sensitive to infection and/or reinfection with SARS-CoV-2 than women. A study conducted at the start of the pandemic by Takahashi et al. showed that men were more susceptible to severe forms of COVID-19 than women [45]. Gender differences in immune responses were also reported, with higher levels of pro-inflammatory cytokines (IL-8 and IL-18) and a more robust induction of non-classical monocytes in men [46]. This is consistent with studies that analysed the sex difference in antibody responses [47]. In further studies, it will be interesting compare immune responses according to gender and serological status in order to discover the mechanisms underlying sex differences.
Our results also showed a different distribution by age group, with lower IgM seroprevalence in younger individuals, particularly those aged 18-25 years, compared to those aged 55-65 years (5.5% and 33.34%, respectively) with a p < 0,001. The 18-25 age group appears less affected by recent infections. This reinforces the data showing that young people are less affected by SARS-CoV-2 infection [48]. Furthermore, they often experience an asymptomatic or mild SARS-CoV-2 infection associated with lower serum titers [49]. In Senegal, during the first wave, it was reported that seroprevalence of SARS-CoV-2 was higher in patients older than 65 years [37].
We investigated whether there was a link between the type of residence and IgM seroprevalence to determine the proportion of new infections accordingly. Surprisingly, we didn’t find a significant difference in terms of IgM seroprevalence among those living in halls of residence [7.97% (95% CI: 5.87 – 10.07)] compared to those living in family homes [6.68% (95% CI: 4.74 – 8.62)], p =0.73. This invalidates our hypothesis that the particular ecosystem of CAD University, with its over 80,000 students from diverse origins, would constitute a niche for spreading the virus, which is not proven in our study. It also appears that, even though the PHS community is mainly be composed by young people, they do not seem to facilitate new infection, contrary to what has been reported in other studies [48,50]. Our study also established that the prevention and control measures taken by the university authorities, such as hand washing throughout the social campus, are mainly responsible for preventing the increase in positive cases within the social campus.
Concerning compliance with preventive measures, we found a low level of compliance with preventive measures recommended by the health authorities, particularly for wearing masks (31.40%) and keeping a physical distance (minimum 2 m) (17.42%). However, most participants reported high-level compliance with hand washing (75.35%). Social distancing and staying at home were also registered although to a lower degree. Our results were in contradiction with those of Kearney et al. who observed high compliance with recommended COVID-19 prevention behaviors among their sample of Senegal respondents, particularly for masking and personal hygiene practices [51]. This difference could be explained by the fact that our study population is younger and less inclined to comply with preventive measures [52,53].
Our findings revealed that IgM seropositivity depends on the ‘number of visits made to someone’, meaning non-respect of social distancing (p = 0.008), which shows the importance of WHO measures concerning the adoption of extensive social distancing as a non-pharmaceutical intervention to reduce the infection's spread and the associated mortalities [54]. However, studies have shown that the impact of social distancing measures depends upon a host of demographic, environmental, and economic dimensions [55].
Regarding vaccination, around 35% of participants had been partially or totally vaccinated, which is higher than the national vaccination rate of 16.9% at the moment of the survey [56]. This could be explained by our population's education level and knowledge of vaccination's stakes. Efforts were also made by the CAD University authorities, who set up a vaccination campaign at various sites during October 2021. However, the vaccination rate remains low compared to the national level, where more than 70% of the population vaccinated since the pandemic started [57].
Furthermore, we found no significant differences in IgM seroprevalences between vaccinated and unvaccinated individuals. It would, therefore, appear that vaccination does not protect against the new variants and reinfections, as has already been demonstrated in numerous studies [58,59,60] indeed, WHO recommendations suggest that seasonal vaccination is necessary to protect against new variants [61].
During the survey, a low rate of participants (8.95%) declared to have tested positive by RT-PCR for COVID-19 infection since the start of the pandemic. Those have been diagnosed as COVID-19 positive were 8.16%, and 29.98% reported having been self-diagnosed as COVID-19 positive. This result contrasts with the high seroprevalence of IgG, which was over 90% for the study population. It shows the limited access to rapid RT-PCR diagnostic tests in Senegal. In October 2021, WHO stated that only one in seven COVID-19 infections in Africa are being detected, highlighting the need to expand testing capabilities [62]. In Senegal, a West African country of 17 million people, about 1,5 million tests have been carried out since the beginning of the pandemic till the mid-2021. By contrast, the USA has administered more than 880 million tests for a population of around 335 million [63].
Around 70% of participants presented symptoms linked to COVID-19 at the moment of the survey, with the more common cough, fatigue/weakness, fever, sore throat and headache. According to China CDC data, people with COVID-19 have had a wide range of symptoms reported – ranging from mild symptoms to severe illness. Symptoms may appear 2-14 days after exposure to the virus. However, these symptoms can be confused with those of the flu caused by influenza [64]. This could explain the difference between the percentage of symptomatic people and IgM seroprevalence. In Senegal, Influenza shows year-round circulation and has 2 distinct epidemic peaks: during January–March and during the rainy season in August–October [65]. During 2021 – 2022 period, the expected January–March influenza peak completely disappeared, corresponding to periods of active SARS-CoV-2 circulation. Lampros et al. noted an unexpected influenza epidemic peak from May to July 2022. The observed co-circulation of SARS-CoV-2 and influenza suggests that factors such as viral interference might be at play and should be further investigated in tropical settings.
Our findings revealed a significant difference according to IgG seroprevalence among participants who declared fatigue symptoms [92.06% (95% CI: 89.96 – 94.16)] compared to those who did not [80.39% (95% CI: 77.31 – 83.47)] with a significant p = 0.0027. Fatigue/easy fatigability, myalgia, and weight loss were the most frequent persistent symptoms (overall 29.3%), followed by respiratory symptoms (25.4%) in COVID-19 infection. Data showed that the main sequela is persistent fatigue. Post-viral fatigue is common and affects patients with mild, asymptomatic COVID-19. Herein, it pointed out the instruments that can be used to assess fatigue in long-term COVID-19: fatigue in a subjective manner or fatigability in an objective manner [66].
We investigated the association of sociodemographic, clinical and lifestyle factors, such as comorbidities, BMI, blood type, smoking and alcohol consumption, with seropositivity. Previous research has shown an association between various pathologies and SARS-CoV-2 infection [67]. High blood pressure was found to be the most common comorbidity, followed by obesity, diabetes and coronary heart disease [68]. In other study, obesity and adiposity-related diseases were shown to be clearly related to worse disease evolution [69].
Using logistics, we found an association between Chronic sinusitis and IgG seropositivity (O.R. 0.238, p = 0.043). Previous studies showed that chronic sinusitis might have a negative impact on COVID-19 outcomes. However, our current results are conflicting, and further studies are needed. On the other hand, COVID-19 can also cause olfactory dysfunction, which is usually temporary [70]. Then, no association was found between diabetes and IgM and IgG seropositivity.
Moreover, a significant association was found between BMI categorised and IgM seropositivity (O.R. 0.238, p = 0.043). Previous studies have shown that obese individuals (BMI > 30 kg/m2) were significantly more likely to be seropositive. It is uncertain whether the raised seroprevalence in these groups represents a greater risk of SARS-CoV-2 infection. However, obese individuals are known to experience more severe COVID-19 symptoms [71,72].
Interestingly, a significant association between IgM seropositivity and ethnic group was found (O.R. 0.723, p = 0.046), suggesting a difference in susceptibility to SARS-CoV2- depending on race and ethnicity. According to previous findings, it seems there are disparities in the effects of COVID-19 infection among different racial/ethnic groups [73,74]. Then, understanding the mechanisms for the disparity will help to evaluate the risk for COVID-19 according to ethnicity.
Our findings showed that IgM seropositivity was associated with marital status (unmarried/married) (O.R. 2.39, p = 0.021); another study reveals that transmission of SARS-CoV-2 is variable among different people within the home. For instance, the risk for infection was higher between spouses, at 43%, which could be a reflection of transmission through intimacy or longer or more direct exposure [75].
Regarding vaccination status, we found a relationship between vaccination and IgG seroprevalence (O.R. 4.741, p < 0.001), showing that people who had received vaccine doses were four times more likely to produce anti-SARS-CoV-2 antibodies than those who had not. It will be interesting to determine the IgG-neutralizing antibodies and to determine antibody levels according to vaccination status and type. Indeed, it has been shown that vaccines from different manufacturers might induce different antibody responses [76].
Limitations and Strengths
Some limitations of our study must be considered. By design, we carried out an on-site university population-based cross-sectional study. Thus, the results cannot be extrapolated directly to the general CAD University population. Participants were subjected to recall bias when completing the questionnaires, particularly preventive measures and symptoms at the time of contact. We also noted a very low level of participation from professors and TAS officers. This constitutes a bias in the statistical calculations. Missing data for certain criteria and non-prefer responders were a limitation for statistics. To date, our study is the only SARS-CoV-2 sero-epidemiological survey conducted in a university community in Senegal. Data on the Serological testing performed by measuring IgM and IgG immunoglobulins against the SARS-CoV-2 targeting peak S1 protein separately is a strength of our study. This allowed us to differentiate recent from late infection. Finally, with our questionnaire we were able to collect a lot of data, which was useful in calculating associations with risk factors.
5. Conclusions
In summary, our analysis of more than 630 subjects from Polytechnic High School community members estimated the extent of exposure to SARS-CoV-2. Our study revealed a high seroprevalence from May–August 2022 following the fourth wave of COVID-19 in Senegal. Our results show that the majority of students and staff have already been exposed to SARS-CoV-2 and confirm the circulation of the virus (SARS-CoV-2) at the time of the survey as shown by the high IgM and IgG seroprevalence. The data show a link between seropositivity and various factors such as age, non-compliance with prevention measures, co-morbidities and post-COVID-19 symptoms such as fatigue. These results underline the importance of sero-epidemiological surveys to estimate the real impact of the COVID-19 pandemic and the disparities between populations in order to establish a profile of the transmission dynamics of the virus and to better manage populations with comorbidities associated with seropositivity. In addition, these results may be essential for the CAD university in the event of the emergence of future waves in order to make appropriate decisions and put in place means of monitoring the evolution of the pandemic after the relaxation of social distancing measures and the implementation of a vaccination schedule at CAD University, which will serve as a basis for other universities in Senegal.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Questionnaire for collecting socio-demographic and clinical data; File S1: Consent form; File S2: Brochure of QUANTITATIVE ELISA for IgG Antibody to COVID-19; File S3: Brochure of WANTAI SARS-CoV-2 IgM ELISA.
Author Contributions
Conceptualization, F.T. and A.A.M.D, C.M.N, M.D.; methodology, F.T., A.A.M.D., C.S.C.A.N., S.S., S.D.T, S.C., A.S., D.D., and M.N.M; software, F.T., C.S.C.A.N., I.D., D.D., K.K., I.D.; A.L.D, M.D..; validation, F.T., A.A.M.D., C.M.N., S.M.S.; formal analysis, F.T., K.K, C.S.C.A.N., I.D., D.D.; A.L.D., M.D.; investigation, sample collection and biobank management, F.T., A.A.M.D., M.N.M, C.S.C.A.N, D.D., S.C., S.S., S.D.T., A.S.; resources, F.T., A.A.M.D., S.M.S, M.D.; data curation, F.T., S.S., C.S.C.A.N., D.D.; writing—original draft preparation, F.T.; writing—review and editing, F.T., A.A.M.D., MNM, MD, CMN, KK, ID, SMS; visualization, F.T, A.A.M.D.; supervision, F.T.,A.A.M.D., S.M.S.,M.D.,C.M.N; project administration, F.T.; funding acquisition, F.T., A.A.M.D., and C.M.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Ecole Supérieure Polytechnique's competitive research impulse fund.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved approved by the Senegalese National Ethics Committee for Research in Health (Reference number N°000043/MSAS/CNERS/SP, 28 February 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank the top management of the “Ecole Supérieure Polytechnique de Dakar” for financial support and all students, Technicians, Administrative, Service officer and professors’ members who voluntarily participated to the study.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results”.
Appendix A

Table A1.
Distribution of SARS-CoV-2 Ig M and G seropositive and seronegative among individuals suffering from different co-morbidities.
Table A1.
Distribution of SARS-CoV-2 Ig M and G seropositive and seronegative among individuals suffering from different co-morbidities.
| Variable | Total, N (%) | IgM | IgG | ||||
|---|---|---|---|---|---|---|---|
| Seronegative N ( %) | Seropositive N (%) |
p-value | Seronegative N (%) |
Seropositive N (%) |
p-value | ||
| Chronic Condition | |||||||
| Asthma | 0.30 | 0.78 | |||||
| Yes | 90 (14.13) | 81 (90) | 9 (10) | 10 (11.11) | 80 (88.89) | ||
| No | 547 (85.87) | 512 (93.6) | 35 (6.40) | 51 (9.32) | 496 (90.38) | ||
| Cardiac disease | 1 | 1 | |||||
| Yes | 5 (0.78) | 5 (100) | 0 (0) | 0 (0) | 5 (100) | ||
| No | 632 (99.22) | 588 (93.04) | 44 (6.96) | 61 (9.65) | 571 (90.35) | ||
| Rheumatism | 0.94 | 0.61 | |||||
| Yes | 23 (3.61) | 22 (95.65) | 1 (4.35) | 1 (4.35) | 22 (95.65) | ||
| No | 614 (96.39) | 571 (93) | 43 (7) | 60 (9.77) | 554 (90.23) | ||
| Hypertension | 1 | 1 | |||||
| Yes | 12 (1.89) | 11 (91.67) | 1 (8.33) | 1 (8.33) | 11 (91.67) | ||
| No | 625 (98.11) | 582 (93.12) | 43 (6.88) | 60 (9.6) | 565 (90.4) | ||
| Diabetes | 1 | 1 | |||||
| Yes | 5 (0.78) | 5 (100) | 0 (0) | 0 (0) | 5 (100) | ||
| No | 632 (99.22) | 588 (93.04) | 44 (6.96) | 61 (9.65) | 571 (90.35) | ||
| HIV | 1 | 1 | |||||
| Yes | 4 (0.63) | 4 (100) | 0 (0) | 0 (0) | 4 (100) | ||
| No | 633 (99.37) | 589 (93.05) | 44 (6.95) | 61 (9.64) | 572 (90.36) | ||
| Sickle cell disease | 1 | 0.37 | |||||
| Yes | 16 (2.51) | 15 (93.75) | 1 (6.25) | 0 (0) | 16 (100) | ||
| No | 621 (97.49) | 578 (93.08) | 43 (6.92) | 61 (9.82) | 560 (90.18) | ||
| Allergy | 1 | 1 | |||||
| Yes | 39 (6.12) | 36 (92.31) | 3 (7.69) | 4 (10.26) | 35 (89.74) | ||
| No | 598 (93.88) | 557 (93.15) | 41 (6.85) | 57 (8.53) | 541 (90.47) | ||
| Spasmophilia | 1 | 1 | |||||
| Yes | 7 (1.1) | 7 (100) | 0 (0) | 1 (14.29) | 6 (85.71) | ||
| No | 630 (98.90) | 586 (93.02) | 44 (6.98) | 60 (9.52) | 570 (90.48) | ||
| Sinusitis | 0.81 | 0.094 | |||||
| Yes | 10 (1.57) | 10 (100) | 0 (0) | 3 (30) | 7 (70) | ||
| No | 627 (98.43) | 583 (92.98) | 44 (7.02) | 58 (9.25) | 569 (90.75) | ||
| Hepatitis B | 0.44 | 0.52 | |||||
| Yes | 12 (1.89) | 10 (83.33) | 2 (16.67) | 0 (0) | 12 (100) | ||
| No | 625 (98.11) | 583 (93.28) | 42 (6.72) | 61 (9.76) | 564 (90.24) | ||
Appendix B
Table A2.
Distribution of SARS-CoV-2 Ig M and G seropositive and seronegative according to preventive measures.
Table A2.
Distribution of SARS-CoV-2 Ig M and G seropositive and seronegative according to preventive measures.
| Total, N (%) | IgM | IgG | |||||
|---|---|---|---|---|---|---|---|
| Seronegative n ( %) |
Seropositive n ( %) |
p- value | Seronegative n ( %) |
Seropositive n ( %) |
p- value | ||
| Wearing masks | 0.17 | 0.73 | |||||
| Always/Often | 201 (31.39) | 183 (91.04) | 18 (8.96) | 19 (9.45) | 182 (90.55) | ||
| Sometimes/Rarely | 380 (59.81) | 355 (93.42) | 25 (6.58) | 38 (10) | 342 (90) | ||
| Never | 30 (4.71) | 30 (100) | 0 (0) | 4 (13.33) | 26 (86.67) | ||
| Kept a physical distance of 2 m | 0.35 | 0.33 | |||||
| Always/Often | 116 (18.21) | 110 (94.83) | 6 (5.17) | 8 (6.90) | 108 (93.10) | ||
| Sometimes/Rarely | 303 (47.56) | 277 (91.42) | 26 (8.58) | 31 (10.23) | 272 (89.77) | ||
| Never | 171 (26.84) | 161 (94.15) | 10 (5.85) | 21 (12.28) | 150 (87.72) | ||
|
Wash hands with hydroalcoholic or with soap and water |
0.105 | 0.599 | |||||
| Always/Often | 480 (75.35) | 451 (93.96) | 29 (6.04) | 51 (10.62) | 429 (89.38) | ||
| Sometimes/Rarely | 122 (19.15) | 108 (88.52) | 14 (11.48) | 10 (8.20) | 112 (91.80) | ||
| Never | 4 (0.63) | 4 (100) | 0 (0) | 0 (0) | 4 (100) | ||
| Number of visits received in the last 15 days | 0.583 | 0.971 | |||||
| 0-2 | 219 (34.38) | 205 (93.61) | 14 (6.39) | 23 (10.50) | 196 (89.50) | ||
| 3-8 | 204 (32.02) | 188 (92.16) | 16 (7.84) | 21 (10.29) | 183 (89.71) | ||
| ≥9 | 154 (24.17) | 146 (94.80) | 8 (5.20) | 15 (9.74) | 139 (90.26) | ||
| Number of visits made in the last 15 days | 0.008* | 0.946 | |||||
| 0-2 | 396 (62.17) | 373 (94.20) | 23 (5.81) | 41 (10.35) | 355 (89.65) | ||
| 3-8 | 125 (19.62) | 109 (87.20) | 16 (12.80) | 12 (9.60) | 113 (90.40) | ||
| ≥9 | 75 (11.78) | 73 (97.33) | 2 (2.67) | 7 (9.33) | 68 (90.67) | ||
| Public transport use per day over the last 15 days | 0.878 | 0.668 | |||||
| 0-2 | 451 (70.8) | 419 (92.9) | 32 (7.1) | 44 (9.75) | 407 (90.25) | ||
| 3-5 | 113 (17.74) | 105 (92.92) | 8 (7.1) | 14 (12.39) | 99 (87.61) | ||
| ≥9 | 36 (5.65) | 33 (91.67) | 3 (8.33) | 3 (8.33) | 33 (91.67) | ||
| Participation in a social event in the last 15 days | 0.589 | 0.289 | |||||
| 0-2 | 456 (71.58) | 423 (92.76) | 33 (7.24) | 51 (11.18) | 405 (88.82) | ||
| 3-8 | 87 (13.66) | 79 (90.80) | 8 (9.20) | 5 (5.75) | 82 (94.25) | ||
| ≥9 | 46 (7.22) | 44 (95.65) | 2 (4.35) | 4 (8.70) | 42 (91.30) | ||
Appendix C
Table A3.
Univariable analysis of comorbidities associated with anti-SARS-CoV-2 antibodies.
| IgM | IgG | |||
|---|---|---|---|---|
| Variable | Univariate OR (95% CI) |
p- value | Univariate OR (95% CI) |
p- value |
| Allergy | 1.132 [0.26 – 3.32] | 0.842 | 0.922 [0,35 - 3,16] | 0.881 |
| Asthma | 1.625 [0.71 – 3.37] | 0.216 | 0.822 [0.42 – 1.78] | 0.594 |
| Cardiac disease | ||||
| Rheumatism | 0.603 [0.03 – 2.98] | 0.625 | 2.383 [0.49 -43.02] | 0.399 |
| Hypertension | 1.230 [0.06 – 6.55] | 0.844 | 1.169 [0,22 - 21,53] | 0.882 |
| Sickle cell disease | 0.896 [0.05 – 4.6] | 0,916 | ||
| Sinusitis | - | - | 0.238 [0,064 - 1,13] | 0.041 * |
| Diabetes | - | - | ||
| HIV | - | - | ||
| Spasmophilia | - | - | 0.632 [0.10 – 12.03] | 0.673 |
Appendix D
Table A4.
Univariable analysis of symptoms associated with anti-SARS-CoV-2 antibodies.
| IgM | IgG | |||
|---|---|---|---|---|
| Variable | Univariate OR (95% CI) |
p- value | Univariate OR (95% CI) |
p- value |
| Wearing masks | 0.796 [0,5893 - 1,073] | 0.134 | 0.966 [0.74 – 1.25] | 0.793 |
| Failure to respect the 2m distance | 0.980 [0,7380 - 1,278] | 0.886 | 1.229 [0.96 – 1.59] | 0.108 |
| Number of visits received in the last 14 days | 0.901 [0.701 – 1.15] | 0.404 | 1.002 [0.82 – 1.23] | 0.984 |
| Number of visits made in the last 14 days | ||||
| Wash hands with hydroalcoholic | 0.854 [0.62 – 1.17] | 0.327 | 0.891 [0.68 – 1.17] | 0.405 |
| Public transport use per day over the last 15 days | 1.043 [0.75 – 1.40] | 0.793 | 1.072 [0.82 – 1.441] | 0.630 |
| Participation in a social event in the last 15 days | 0.952 [0.71 – 1.24] | 0.734 | 1.094 [0.86 – 1.420] | 0.473 |
| Positive COVID-19 test since the start of the pandemic | 1.657 [0.60 – 3.87] | 0.278 | 0.909 [0.398 – 2.45] | 0.834 |
| COVID-19 diagosis by a doctor | 0.264 [0.014 – 1.28] | 0.95 | 0.576 [0.263 – 1.40] | 0.191 |
| COVID-19 self-diagosis | 0.467 [0.21 – 0.97] | 0.051 | 0.742 [0.39 - 1.41] | 0.360 |
| Treatment | 1.269 [0.36 - 8.072] | 0.742 | ||
| COVID-19 symptoms 2 weeks before survey | 0.880 [0.44 – 1.88] | 0.727 | 0.885 [0.45 - 1.65] | 0.713 |
| Fever | 0.889 [0.28 – 2.45] | 0.829 | 1.908 [0.80 - 5.306] | 0.174 |
| Cough | 1.222 [0.52 – 2.89] | 0.643 | 1.321 [0.68 – 2.59] | 0.409 |
| Fatigue | 0.608 [0.26 – 1.50] | 0.262 | 2.829 [1.44 – 5.55] | 0.0023 * |
| Headaches | 0.765 [0.33 – 2] | 0.556 | 0.838 [0.35 - 1.79] | 0.669 |
| Sore throat | 1.299 [ 0.51 – 3.06] | 0.5 | 0.999 [0.488 – 2.18] | 0.998 |
| Runny nose | 0.889 [0.38 – 2.11] | 0.807 | 1.323 [0.697 – 2.54] | 0.394 |
| Breathing difficulties | 0.654 [0.186 – 1.79] | 0.451 | 1.850 [0.80 – 5.046] | 0.183 |
| Abdominal pain | 0.831 [0.13 – 3.03] | 0.809 | 2.327 [0.66 – 14.74] | 0.261 |
| Diarrhea | 0.357 [0.056 – 1.27] | 0.172 | 1.382 [0.62 – 3.52] | 0.460 |
| Anosmia/ageusia | 0.899 [0.14 – 3.28] | 0.890 | 2.209 [0.63 – 14.00] | 0.291 |
References
- Asselah, T.; Durantel, D.; Pasmant, E.; Lau, G.; Schinazi, R.F. COVID-19: Discovery, diagnostics and drug development. J. Hepatol. 2021, 74, 168–184. [Google Scholar] [CrossRef] [PubMed]
- Yesudhas, D.; Srivastava, A.; Gromiha, M.M. COVID-19 outbreak: history, mechanism, transmission, structural studies and therapeutics. Infection 2021, 49, 199–213. [Google Scholar] [CrossRef] [PubMed]
- WHO Director-General’s opening remarks at the media briefing on COVID19 -March 2020.
- https://www.worldometers.info/coronavirus/. (accessed on 12 November 2023).
- Mofijur, M.; Fattah, I.M.R.; Alam, M.A.; Ong, H.C.; Rahman, S.M.A.; Najafi, G.; Ahmed, S.F.; Uddin, M.A.; Mahlia, T.M.I. Impact of COVID-19 on the social, economic, environmental and energy domains: Lessons learnt from a global pandemic. Sustain. Prod. Consum. 2021, 26, 343–359. [Google Scholar] [CrossRef] [PubMed]
- Hosseinzadeh, P.; Zareipour, M.; Baljani, E.; Moradali, M.R. Social Consequences of the COVID-19 Pandemic. A Systematic Review. Invest. Educ. Enferm. 2022, 40. [Google Scholar] [CrossRef] [PubMed]
- Shang, Y.; Li, H.; Zhang, R. Effects of Pandemic Outbreak on Economies: Evidence From Business History Context. Front. Public. Health 2021, 9, 632043. [Google Scholar] [CrossRef] [PubMed]
- World Bank Open Data. Data. 2021. Available online: https://data.worldbank.org/.
- Mok, K.H. Impact of COVID-19 on Higher Education: Critical Reflections. High. Educ. Policy 2022, 35, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Selvaraj, A.; Radhin, V.; Ka, N.; Benson, N.; Mathew, A.J. Effect of pandemic based online education on teaching and learning system. Int. J. Educ. Dev. 2021, 85, 102444. [Google Scholar] [CrossRef] [PubMed]
- Diouara, A.A.M.; Lo, S.; Nguer, C.M.; Senghor, A.; Diop Ndiaye, H.; Manga, N.M.; Danfakha, F.; Diallo, S.; Faye Dieme, M.E.; Thiam, O.; et al. Hepatitis E Virus Seroprevalence and Associated Risk Factors in Pregnant Women Attending Antenatal Consultations in Senegal. Viruses 2022, 14, 1742. [Google Scholar] [CrossRef] [PubMed]
- https://www.worldometers.info/coronavirus/country/senegal/. (accessed on 12 November 2023).
- Diallo, A.I.; Faye, A.; Tine, J.A.D.; Ba, M.F.; Gaye, I.; Bonnet, E.; Traore, Z.; Ridde, V. Factors associated with the acceptability of government measures to address COVID-19 in Senegal. Rev. Epidemiol. Sante Publique 2022, 70, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Ba, M.F.; Ridde, V.; Diallo, A.I.; Tine, J.A.D.; Kane, B.; Gaye, I.; Traore, Z.; Bonnet, E.; Faye, A. Acceptability of contact management and care of simple cases of COVID-19 at home: a cross-sectional study in Senegal. Trans. R. Soc. Trop. Med. Hyg. 2022, 116, 1214–1222. [Google Scholar] [CrossRef] [PubMed]
- https://www.worldbank.org/en/results/2021/08/31/world-bank-financing-helps-to-support-senegal-in-the-fight-against-covid-191. (accessed on 13 May 2023).
- Zhou, Y.; Rahman, M.M.; Khanam, R. The impact of the government response on pandemic control in the long run-A dynamic empirical analysis based on COVID-19. PLoS One 2022, 17, e0267232. [Google Scholar] [CrossRef] [PubMed]
- Bedford, J.; Enria, D.; Giesecke, J.; Heymann, D.L.; Ihekweazu, C.; Kobinger, G.; Lane, H.C.; Memish, Z.A.; Oh, M.D.; Sall, A.A.; et al. Living with the COVID-19 pandemic: act now with the tools we have. Lancet 2020, 396, 1314–1316. [Google Scholar] [CrossRef] [PubMed]
- Torretta, S.; Zuccotti, G.; Cristofaro, V.; Ettori, J.; Solimeno, L.; Battilocchi, L.; D'Onghia, A.; Bonsembiante, A.; Pignataro, L.; et al. Diagnosis of SARS-CoV-2 by RT-PCR Using Different Sample Sources: Review of the Literature. Ear Nose Throat J. 2021, 100, 131S–138S. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.S.; Lee, N.J.; Woo, S.H.; Kim, J.M.; Kim, H.M.; Jo, H.J.; Park, Y.E.; Han, M.G. Validation of real-time RT-PCR for detection of SARS-CoV-2 in the early stages of the COVID-19 outbreak in the Republic of Korea. Sci. Rep. 2021, 11, 14817. [Google Scholar] [CrossRef] [PubMed]
- Maniruzzaman, M.; Islam, M.M.; Ali, M.H.; Mukerjee, N.; Maitra, S.; Kamal, M.A.; Ghosh, A.; Castrosanto, M.A.; Alexiou, A.; Ashraf, G.M.; et al. COVID-19 diagnostic methods in developing countries. Environ. Sci. Pollut. Res. Int. 2022, 29, 51384–51397. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; Wang, J.H.; Hsueh, P.R. Population-based seroprevalence surveys of anti-SARS-CoV-2 antibody: An up-to-date review. Int. J. Infect. Dis. 2020, 101, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Rostami, A.; Sepidarkish, M.; Leeflang, M.M.G.; Riahi, S.M. , Nourollahpour Shiadeh, M.; Esfandyari, S.; Mokdad, A.H., Hotez, P.J., Gasser, R.B. SARS-CoV-2 seroprevalence worldwide: a systematic review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 331–340. [Google Scholar] [CrossRef]
- Hou, H.; Wang, T.; Zhang, B.; Luo, Y.; Mao, L.; Wang, F.; Wu, S.; Sun, Z. Detection of IgM and IgG antibodies in patients with coronavirus disease 2019. Clin Transl Immunology 2020, 9, e01136. [Google Scholar] [CrossRef] [PubMed]
- Feikin, D.R.; Widdowson, M.A.; Mulholland, K. Estimating the Percentage of a Population Infected with SARS-CoV-2 Using the Number of Reported Deaths: A Policy Planning Tool. Pathogens 2020, 9, 838. [Google Scholar] [CrossRef] [PubMed]
- Cascini, F.; Failla, G.; Gobbi, C.; Pallini, E.; Hui, J.; Luxi, W.; Villani, L.; Quentin, W.; Boccia, S.; Ricciardi, W. A cross-country comparison of Covid-19 containment measures and their effects on the epidemic curves. BMC Public. Health 2022, 22, 1765. [Google Scholar] [CrossRef] [PubMed]
- Vusirikala, A.; Whitaker, H.; Jones, S.; Tessier, E.; Borrow, R.; Linley, E.; Hoschler, K.; Baawuah, F.; Ahmad, S.; et al. Seroprevalence of SARS-CoV-2 antibodies in university students: Cross-sectional study, December 2020, England. J Infect 2021, 83, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Tsitsilonis, O.E.; Paraskevis, D.; Lianidou, E.; Pierros, V.; Akalestos, A.; Kastritis, E.; Moutsatsou, P.; Scorilas, A.; Sphicopoulos, T.; Terpos, E.; et al. Seroprevalence of Antibodies against SARS-CoV-2 among the Personnel and Students of the National and Kapodistrian University of Athens, Greece: A Preliminary Report. Life 2020, 10, 214. [Google Scholar] [CrossRef] [PubMed]
- Arnold, C.R.K.; Srinivasan, S.; Rodriguez, S.; Rydzak, N.; Herzog, C.M.; Gontu, A.; Bharti, N.; Small, M.; Rogers, C.J.; Schade, M.M. et al; et al. SARS-CoV-2 Seroprevalence in a University Community: A Longitudinal Study of the Impact of Student Return to Campus on Infection Risk Among Community Members. medRxiv.
- Migliara, G.; Renzi, E.; Baccolini, V.; Cerri, A.; Donia, P.; Massimi, A.; Marzuillo, C.; De Vito, C.; Casini, L.; et al. Predictors of SARS-CoV-2 Infection in University Students: A Case-Control Study. Int. J. Environ. Res. Public. Health 2022, 19, 14376. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Kilcoyne, A.; Ucer, C. Non-infectious status indicated by detectable IgG antibody to SARS-CoV-2. Br. Dent. J. 2020, 229, 521–524. [Google Scholar] [CrossRef] [PubMed]
- Assaid, N.; Arich, S.; Charoute, H.; Akarid, K.; Anouar Sadat, M.; Maaroufi, A.; Ezzikouri, S.; Sarih, M. Kinetics of SARS-CoV-2 IgM and IgG Antibodies 3 Months after COVID-19 Onset in Moroccan Patients. Am. J. Trop. Med. Hyg. 2023, 108, 145–154. [Google Scholar] [CrossRef]
- GeurtsvanKessel, C.H.; Okba, N.M.A.; Igloi, Z.; Bogers, S.; Embregts, C.W.E.; Laksono, B.M.; Leijten, L.; Rokx, C.; Rijnders, B.; Rahamat-Langendoen, J.; et al. An evaluation of COVID-19 serological assays informs future diagnostics and exposure assessment. Nat. Commun. 2020, 11, 3436. [Google Scholar] [CrossRef] [PubMed]
- Wajnberg, A.; Mansour, M.; Leven, E.; Bouvier, N.M.; Patel, G.; Firpo-Betancourt, A.; Mendu, R.; Jhang, J.; Arinsburg, S.; Gitman, M.; et al. Humoral response and PCR positivity in patients with COVID-19 in the New York City region, USA: an observational study. Lancet Microbe 2020, 1, e283–e289. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, A.; Haq, M.; Rehman, A.; Haq, N.U. Anti-nucleocapsid IgG antibodies in SARS-CoV-2 recovered health care workers. One year follow-up study. Int. J. Immunopathol. Pharmacol. 2023, 37, 3946320231187744. [Google Scholar] [CrossRef] [PubMed]
- Haveri, A.; Ekstrom, N.; Solastie, A.; Virta, C.; Osterlund, P.; Isosaari, E.; Nohynek, H.; Palmu, A.A.; Melin, M. Persistence of neutralizing antibodies a year after SARS-CoV-2 infection in humans. Eur. J. Immunol. 2021, 51, 3202–3213. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.; Feng, Y.; Mo, X.; Zheng, P.; Wang, Q.; Li, P.; Peng, P.; Liu, X.; Chen, Z.; et al. Kinetics of SARS-CoV-2 specific IgM and IgG responses in COVID-19 patients. Emerg. Microbes Infect. 2020, 9, 940–948. [Google Scholar] [CrossRef]
- Seck, S.M.; Mbow, M.; Kane, Y.; Cisse, M.M.; Faye, G.; Kama, A.; Sarr, M.; Nitcheu, P.; Dahaba, M.; Diallo, I.M. et al.; et al. Prevalence of SARS-CoV-2 antibodies in hemodialysis patients in Senegal: a multicenter cross-sectional study. BMC Nephrol. 2021, 22, 384. [Google Scholar] [CrossRef] [PubMed]
- Ahouidi, A.D.; Anderson, M.; Diedhiou, C.K.; Dia, A.; Mbow, M.; Dia, Y.; Mboup, A.; Gaye, A.G.; Manga, N.M.; Cloherty, G.; et al. Seroprevalence of SARS-CoV-2 IgG antibodies in a healthcare setting during the first pandemic wave in Senegal. IJID Reg. 2022, 2, 96–98. [Google Scholar] [CrossRef] [PubMed]
- Talla, C.; Loucoubar, C.; Roka, J.L.; Barry, M.A.; Ndiaye, S.; Diarra, M.; Thiam, M.S.; Faye, O.; Dia, M.; Diop, M.; et al. Seroprevalence of anti-SARS-CoV-2 antibodies in Senegal: a national population-based cross-sectional survey, between October and November 2020. IJID Reg 2022, 3, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Senegalese Ministry of Health and Social Action., [Final report of the 2nd seroprevalence survey of Covid-19 in Senegal, 2023.
- Diouara, A.A.M.; Thiam, F.; Coundoul, S.; Manga, N.M.; Ndiaye, H.D.; Senghor, A.; Tene, S.D.; Sané, S.; Kane, B.; Sarr, H.; et al. High Exposure to SARS-CoV-2 among Pregnant Women after the First and Second Waves of COVID-19 in Senegal. Preprints. [CrossRef]
- Ndiaye, A.J.S.; Beye, M.; Lo, G.; Kacel, I.; Sow, A.; Leye, N.; Padane, A.; Mboup, A.; Diop-Ndiaye, H.; et al. Genomic Epidemiology of SARS-CoV-2 in Urban Settings in Senegal. Viruses 2023, 15, 1233. [Google Scholar] [CrossRef]
- Manirakiza, A.; Malaka, C.; Longo, J.D.; Yambiyo, B.M.; Diemer, S.H.; Namsenei, J.; Coti-Reckoundji, C.S.G.; Bouhouda, M.; Belizaire, M.R.D.; Roungou, J.B.; et al. Sero-prevalence of anti-SARS-CoV-2 antibodies among communities between July and August 2022 in Bangui, Central African Republic. J Public Health Afr 2023, 14, 2315. [Google Scholar] [CrossRef] [PubMed]
- Akanmu, S.; Herrera, B.B.; Chaplin, B.; Ogunsola, S.; Osibogun, A.; Onawoga, F.; John-Olabode, S.; Akase, I.E.; Nwosu, A.; Hamel, D.J. et al.; et al. High SARS-CoV-2 seroprevalence in Lagos, Nigeria with robust antibody and cellular immune responses. J. Clin. Virol. Plus 2023, 3, 100156. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Wong, P.; Ellingson, M.K.; Lucas, C.; Klein, J.; Israelow, B.; Silva, J.; Oh, J.E.; Mao, T.; Tokuyama, M.; et al. Sex differences in immune responses to SARS-CoV-2 that underlie disease outcomes. medRxiv.
- Zhang, H.; Tang, Y.; Tao, J. Sex-Related Overactivation of NLRP3 Inflammasome Increases Lethality of the Male COVID-19 Patients. Front. Mol. Biosci. 2021, 8, 671363. [Google Scholar] [CrossRef] [PubMed]
- Zeng, F.; Dai, C.; Cai, P.; Wang, J.; Xu, L.; Li, J.; Hu, G.; Wang, Z.; Zheng, F.; Wang, L. A comparison study of SARS-CoV-2 IgG antibody between male and female COVID-19 patients: A possible reason underlying different outcome between sex. J. Med. Virol. 2020, 92, 2050–2054. [Google Scholar] [CrossRef] [PubMed]
- Felsenstein, S.; Hedrich, C.M. SARS-CoV-2 infections in children and young people. Clin. Immunol. 2020, 220, 108588. [Google Scholar] [CrossRef]
- Backhaus, I.; Hermsen, D.; Timm, J.; Boege, F.; Lubke, N.; Degode, T.; Gobels, K.; Dragano, N. SARS-CoV-2 seroprevalence and determinants of infection in young adults: a population-based seroepidemiological study. Public. Health 2022, 207, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Zhang, L.; Du, H.; Zhang, J.; Li, Y.Y.; Qu, J.; Zhang, W.; Wang, Y.; Bao, S.; Li, Y.; et al. SARS-CoV-2 Infection in Children. N. Engl. J. Med. 2020, 382, 1663–1665. [Google Scholar] [CrossRef] [PubMed]
- Kearney, M.; Bornstein, M.; Fall, M.; Nianogo, R.; Glik, D.; Massey, P. Cross-sectional study of COVID-19 knowledge, beliefs and prevention behaviours among adults in Senegal. BMJ Open 2022, 12, e057914. [Google Scholar] [CrossRef] [PubMed]
- Jaureguizar, J.; Redondo, I.; Galende, N.; Ozamiz, N. Factors related to compliance with the COVID-19 health regulations among young people. World J. Psychiatry 2021, 11, 1247–1258. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.K.; Crimmins, E.M. How does age affect personal and social reactions to COVID-19: Results from the national Understanding America Study. PLoS One 2020, 15, e0241950. [Google Scholar] [CrossRef] [PubMed]
- https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-27-october-2022. (accessed on 12 November 2023).
- Prakash, N.; Srivastava, B.; Singh, S.; Sharma, S.; Jain, S. Effectiveness of social distancing interventions in containing COVID-19 incidence: International evidence using Kalman filter. Econ. Hum. Biol. 2022, 44, 101091. [Google Scholar] [CrossRef]
- https://tradingeconomics.com/senegal/coronavirus-vaccination-rate. (accessed on 12 November 2023).
- https://ourworldindata.org/covid-vaccinations. (accessed on 12 November 2023).
- Van Egeren, D.; Stoddard, M.; White, L.F.; Hochberg, N.S.; Rogers, M.S.; Zetter, B.; Joseph-McCarthy, D.; Chakravarty, A. Vaccines Alone Cannot Slow the Evolution of SARS-CoV-2. Vaccines 2023, 11, 853. [Google Scholar] [CrossRef]
- Malik, J.A.; Ahmed, S.; Mir, A.; Shinde, M.; Bender, O.; Alshammari, F.; Ansari, M.; Anwar, S. The SARS-CoV-2 mutations versus vaccine effectiveness: New opportunities to new challenges. J. Infect. Public. Health 2022, 15, 228–240. [Google Scholar] [CrossRef] [PubMed]
- Lopez Bernal, J.; Gower, C.; Andrews, N.; Public Health England Delta Variant Vaccine Effectiveness Study, G. Effectiveness of Covid-19 Vaccines against the B.1.617.2 (Delta) Variant. Reply. N. Engl. J. Med. 2021, 385, e92. [Google Scholar] [CrossRef]
- Cohen, J.I.; Burbelo, P.D. Reinfection With SARS-CoV-2: Implications for Vaccines. Clin. Infect. Dis. 2021, 73, e4223–e4228. [Google Scholar] [CrossRef]
- Adepoju, P. Closing Africa's wide COVID-19 testing and vaccination gaps. Lancet Microbe 2021, 2, e573. [Google Scholar] [CrossRef] [PubMed]
- https://covid.cdc.gov/covid-data-tracker/#vaccinations_vacc-people-booster-percent-pop5. (accessed on 12 November 2023).
- https://www.cdc.gov/flu/symptoms/flu-vs-covid19.htm. (accessed on 12 November 2023).
- Lampros, A.; Talla, C.; Diarra, M.; Tall, B.; Sagne, S.; Diallo, M.K.; Diop, B.; Oumar, I.; Dia, N.; Sall, A.A. et al.; et al. Shifting Patterns of Influenza Circulation during the COVID-19 Pandemic, Senegal. Emerg. Infect. Dis. 2023, 29, 1808–1817. [Google Scholar] [CrossRef] [PubMed]
- Campos, M.C.; Nery, T.; Starke, A.C.; de Bem Alves, A.C.; Speck, A.E.; A, S.A. Post-viral fatigue in COVID-19: A review of symptom assessment methods, mental, cognitive, and physical impairment. Neurosci. Biobehav. Rev. 2022, 142, 104902. [Google Scholar] [CrossRef] [PubMed]
- Silaghi-Dumitrescu, R.; Patrascu, I.; Lehene, M.; Bercea, I. Comorbidities of COVID-19 Patients. Medicina 2023, 59, 1393. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Chi, J.; Lv, W.; Wang, Y. Obesity and diabetes as high-risk factors for severe coronavirus disease 2019 (Covid-19). Diabetes Metab Res Rev 2021, 37, e3377. [Google Scholar] [CrossRef] [PubMed]
- Cornejo-Pareja, I.M.; Gomez-Perez, A.M.; Fernandez-Garcia, J.C.; Barahona San Millan, R.; Aguilera Luque, A.; de Hollanda, A.; Jimenez, A.; Jimenez-Murcia, S.; Munguia, L.; Ortega, E.; et al. Coronavirus disease 2019 (COVID-19) and obesity. Impact of obesity and its main comorbidities in the evolution of the disease. Eur Eat Disord Rev 2020, 28, 799–815. [Google Scholar] [CrossRef] [PubMed]
- A NA-R, A.D.A.; Alshalan, A.; Muteb Alshalan, K.; Muharib, R.A.K.; Hamdan, R.A.A.; Talal Alruwaili, A.; Abdulhamid Alanazi, A.; Khalid Alshalan, M.; Fahid, A.A. Epidemiological Characteristics, Pathogenesis and Clinical Implications of Sinusitis in the Era of COVID-19: A Narrative Review. J. Asthma Allergy 2023, 16, 201–211. [Google Scholar]
- Wolff, D.; Nee, S.; Hickey, N.S.; Marschollek, M. Risk factors for Covid-19 severity and fatality: a structured literature review. Infection 2021, 49, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Aburto, S.; Cisterna, M.; Acuna, J.; Ruiz, C.; Viscardi, S.; Marquez, J.L.; Villano, I.; Letelier, P.; Guzman, N. Obesity as a Risk Factor for Severe COVID-19 in Hospitalized Patients: Epidemiology and Potential Mechanisms. Healthcare 2022, 10, 1838. [Google Scholar] [CrossRef] [PubMed]
- Mackey, K.; Ayers, C.K.; Kondo, K.K.; Saha, S.; Advani, S.M.; Young, S.; Spencer, H.; Rusek, M.; Anderson, J.; Veazie, S.; et al. Racial and Ethnic Disparities in COVID-19-Related Infections, Hospitalizations, and Deaths : A Systematic Review. Ann. Intern. Med. 2021, 174, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Carethers, J.M. Insights into disparities observed with COVID-19. J. Intern. Med. 2021, 289, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Fogh, K.; Eriksen, A.R.R.; Hasselbalch, R.B.; Kristensen, E.S.; Bundgaard, H.; Nielsen, S.D.; Jorgensen, C.S.; Scharff, B.; Erikstrup, C.; Saekmose, S.G.; et al. Seroprevalence of SARS-CoV-2 antibodies in social housing areas in Denmark. BMC Infect. Dis. 2022, 22, 143. [Google Scholar] [CrossRef] [PubMed]
- Megasari, N.L.A.; Yamani, L.N.; Juniastuti, J.; Lusida, M.I.; Mori, Y. Seroprevalence of SARS-CoV-2 anti-spike IgG antibody among COVID-19 vaccinated individuals residing in Surabaya, East Java, Indonesia. PeerJ 2023, 11, e16142. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of participants' enrolment for the anti-SARS-CoV-2 antibody seroprevalence study in Superior Polytechnic School.
Figure 1.
Flowchart of participants' enrolment for the anti-SARS-CoV-2 antibody seroprevalence study in Superior Polytechnic School.
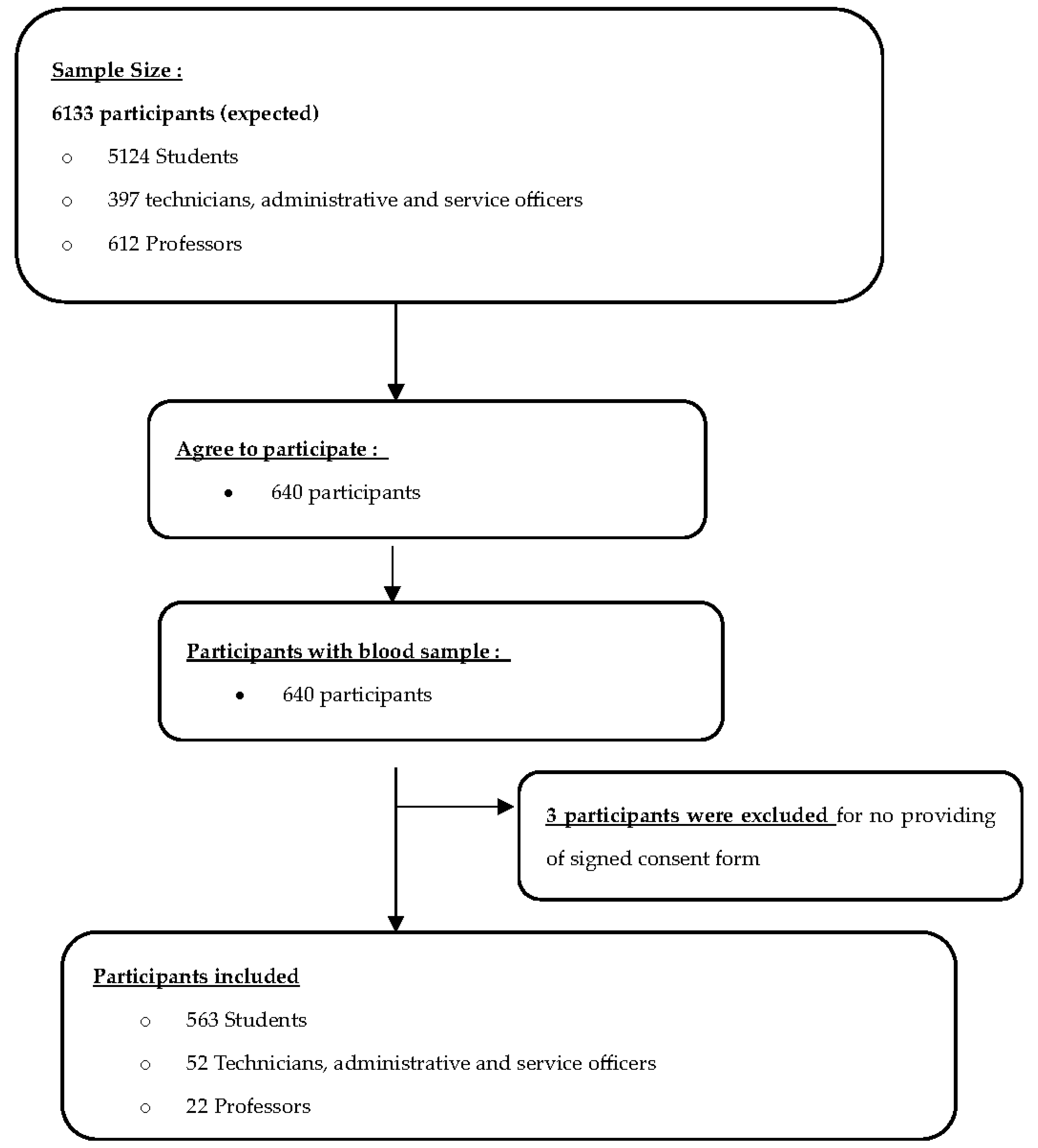
Figure 2.
Compliance with preventive measures recommended by authorities.
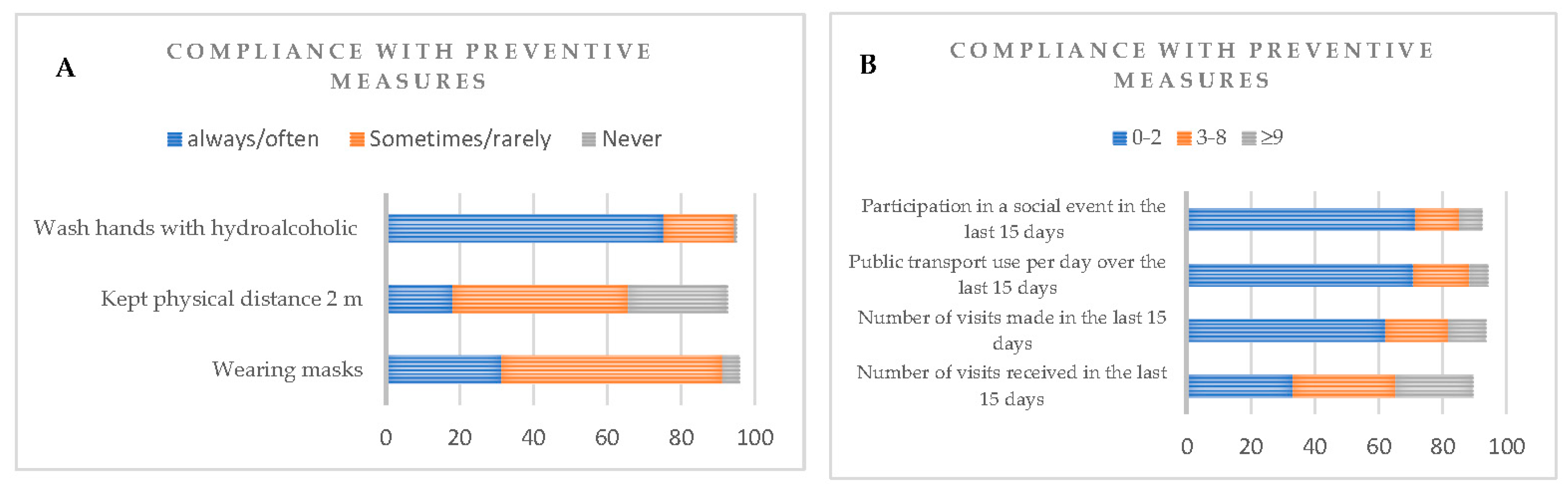
Figure 3.
Diagnosis and clinical related symptoms to COVID-19.
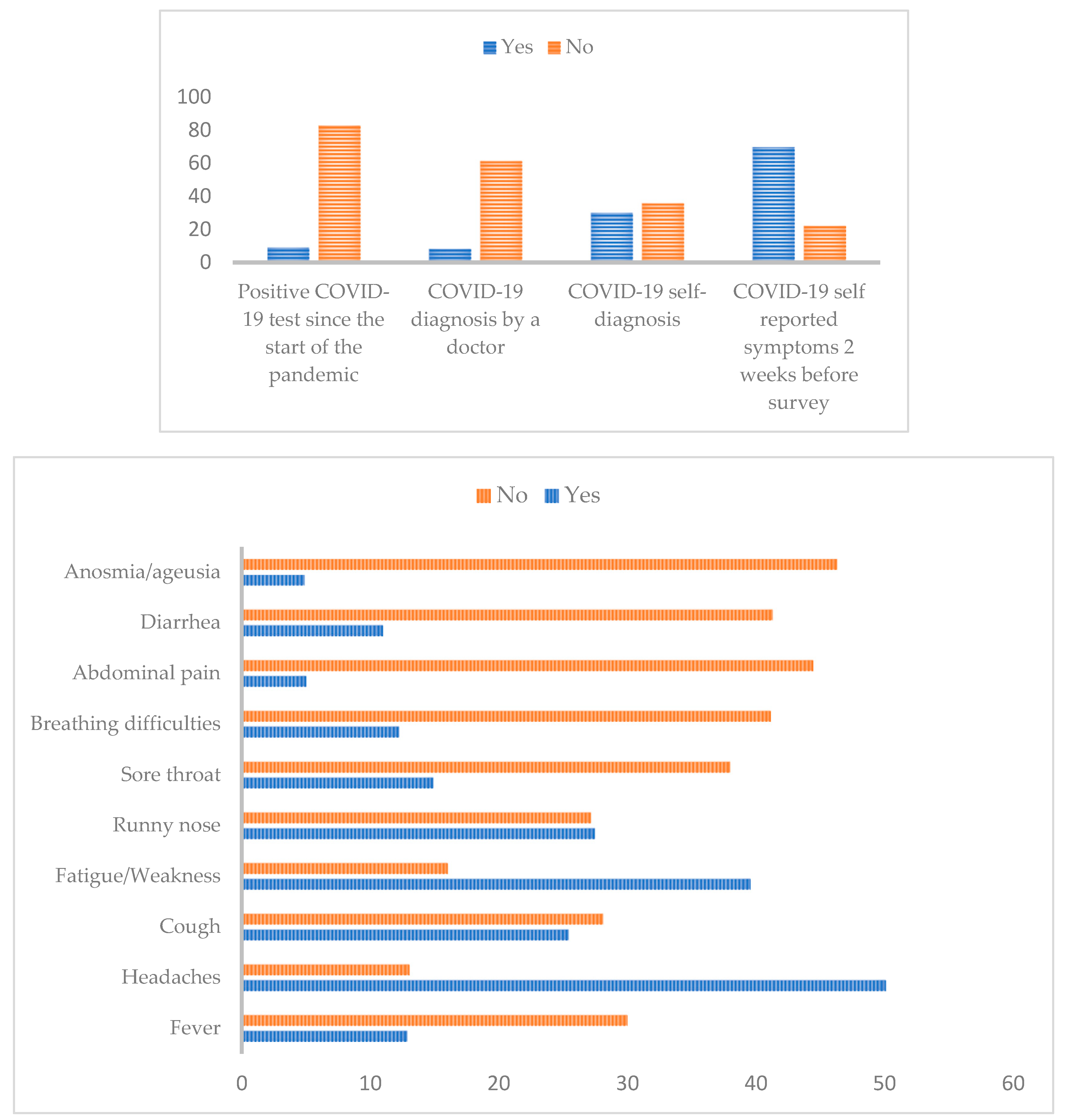
Table I.
Ig M and G seropositive and seronegative individuals among the 637 participants enrolled.
| Variable | Total, N (%) | IgM | IgG | ||||
|---|---|---|---|---|---|---|---|
| Seronegative N (%) |
Seropositive N (%) |
p-value | Seronegative N (%) |
Seropositive N (%) |
p-value | ||
| Overall | 637 (100) | 593 (93.09) | 44 (6.91) | 51 (8) | 576 (92) | ||
| Age (years) | |||||||
| Mean | 23.20 | 23.06 | 25.16 | 22.4 | 23.28 | ||
| Median | 21 | 21 | 21 | 21 | 21 | ||
| Range | 18 - 63 | 18 - 63 | 18 - 59 | 18 - 47 | 18 - 63 | ||
| Age group | <0,001* | 0,98 | |||||
| [18-25] | 546 (85.71) | 516 (94.50) | 30 (5.5) | 53 (9.7) | 493 (92.3) | ||
| (25-35] | 38 (5.96) | 29 (76.31) | 9 (23.69) | 4 (10.53) | 34 (89.47) | ||
| (35-45] | 26 (4.08) | 24 (92.31) | 2 (7.69) | 2 (7.69) | 24 (92.31) | ||
| (45-55] | 12 (1.88) | 12 (100) | 0 (0) | 1 (8.33) | 11 (91.67) | ||
| (55-65] | 6 (0.94) | 4 (66.67) | 2 (33.34) | 0 (0) | 6 (100) | ||
| Gender | 0.16 | 0.89 | |||||
| Women | 395 (62) | 373 (94.43) | 22 (5.57) | 37 (9.36) | 358 (90.63) | ||
| Men | 235 (36.89) | 213 (90.64) | 22 (9.36) | 24 (10.21) | 211 (89.79) | ||
| Occupation | 0.15 | 0.71 | |||||
| Students | 563 (88.38) | 528 (93.78) | 35 (6.22) | 55 (9.77) | 508 (90.23) | ||
| Professors | 22 (3.45) | 19 (86.36) | 3 (13.64) | 1 (9.61) | 21 (90.38) | ||
| TAS Officers | 52 (8.16) | 46 (88.46) | 6 (11.54) | 5 (4.54) | 47 (95.45) | ||
| Level of education | 0.18 | 0.45 | |||||
| Bachelor degree | 450 (70.64) | 423 (94) | 27 (6) | 46 (10.22) | 404 (89.78) | ||
| Master degree | 117 (18.36) | 105 (84.74) | 12 (10.26) | 12 (10.25) | 105 (89.75) | ||
| PhD | 20 (3.14) | 17 (85) | 3 (15) | 1 (5) | 19 (95) | ||
| others | 18 (2.82) | 16 (88.89) | 2 (11.11) | 0 (0) | 18 (100) | ||
| Nationality | 0.29 | 0.30 | |||||
| Senegalese | 605 (94.66) | 565 (93.39) | 40 (6.61) | 56 (9.26) | 549 (90.74) | ||
| Others † | 30 (5.03) | 26 (86.67) | 4 (13.33) | 5 (16.67) | 25 (83.33) | ||
| Ethnic groups | 0.25 | 0.17 | |||||
| Wolof | 153 (24.02) | 145 (94.77) | 8 (5.23) | 14 (9.15) | 139 (90.85) | ||
| Fula | 139 (21.82) | 128 (92.09) | 11 (7.91) | 11 (7.91) | 128 (92.09) | ||
| Serer | 79 (12.40) | 72 (91.14) | 7 (8.86) | 8 (10.13) | 71 (89.87) | ||
| Jola | 16 (2.50) | 14 (87.50) | 2 (12.50) | 0 (0) | 16 (100) | ||
| Malinke | 17 (2.67) | 16 (94.12) | 1 (5.88) | 3 (17.65) | 14 (82.35) | ||
| Soninke | 9 (1.41) | 9 (100) | 0 (0) | 3 (33.33) | 6 (66.67) | ||
| Mauri | 7 (1.1) | 7 (100) | 0 (0) | 0 (0) | 7 (100) | ||
| Others † | 18 (2.82) | 14 (77.78) | 4 (22.22) | 2 (11.12) | 16 (88.88) | ||
| Accommodation type | 0.73 | 0.76 | |||||
| Halls of residence | 138 (21.67) | 127 (92.03) | 11 (7.97) | 12 (8.69) | 126 (91.31) | ||
| Family home | 479 (75.19) | 447 (93.32) | 32 (6.68) | 48 (10.02) | 431 (89.98) | ||
| Family members | 0.54 | 0.32 | |||||
| 1-2 | 37 (5.81) | 36 (97.30) | 1 (2.70) | 2 (5.40) | 35 (94.60) | ||
| 3-5 | 247 (38.77) | 227 (91.90) | 20 (8.10) | 29 (11.75) | 218 (88.25) | ||
| 6-8 | 188 (29.51) | 176 (93.62) | 12 (6.38) | 20 (10.64) | 168 (89.36) | ||
| 9 or plus | 74 (11.61) | 78 (90.70) | 8 (9.30) | 5 (5.81) | 81 (94.19) | ||
| Matrimonial status | 0.062 | 0.53 | |||||
| Single | 558 (87.60) | 524 (93.9) | 34 (6.1) | 54 (9.68) | 504 (90.32) | ||
| Married | 60 (9.42) | 51 (85) | 9 (15) | 7 (11.67) | 53 (88.33) | ||
| Divorced | 2 (0.31) | 2 (100) | 0 (0) | 0 (0) | 2 (100) | ||
| Smoker | 0.08 | 0.16 | |||||
| Yes | 10 (1.88) | 10 (100) | 0 (0) | 0 (0) | 14 (100) | ||
| No | 538 (84.30) | 503 (93.49) | 35 (6.51) | 57 (9.69) | 531 (90.31) | ||
| Stopped > 1 year | 10 (1.41) | 8 (80) | 2 (20) | 0 (0) | 10 (100) | ||
| Alcohol consumer | 0.12 | 0.038 | |||||
| Yes | 21 (3.62) | 19 (90.48) | 2 (9.52) | 1 (4.76) | 20 (95.24) | ||
| No | 554 (86.81) | 516 (93.14) | 38 (6.86) | 51 (9.20) | 503 (90.80) | ||
| Stopped > 1 year | 3 (0.31) | 3 (100) | 0 (0) | 1 (33.34) | 2 (66.66) | ||
| BMI Categorized | 0.089 | 0.55 | |||||
| Underweight | 69 (10.83) | 67 (97.10) | 2 (2.90) | 6 (8.70) | 63 (91.30) | ||
| Normal weight | 240 (37.68) | 224 (93.33) | 16 (6.67) | 28 (11.67) | 212 (88.33) | ||
| Overweight /Obesity | 53 (8.32) | 46 (86.79) | 7 (11.36) | 8 (15.09) | 45 (84.91) | ||
| Blood Group | 0.95 | 0.094 | |||||
| A- | 9 (1.41) | 8 (88.89) | 1 (11.11) | 1 (11.11) | 8 (88.89) | ||
| A+ | 140 (21.98) | 131 (93.57) | 9 (6.43) | 14 (10) | 126 (90) | ||
| AB- | 1 (0.15) | 1 (100) | 0 (0) | 1 (100) | 0 (0) | ||
| AB+ | 25 (3.92) | 24 (96) | 1 (4) | 3 (12) | 22 (88) | ||
| B- | 5 (0.78) | 4 (80) | 1 (20) | 0 (0) | 5 (100) | ||
| B+ | 102 (16.01) | 94 (92.16) | 8 (7.84) | 7 (6.86) | 95 (93.14) | ||
| O- | 24 (3.77) | 22 (91.67) | 2 (8.33) | 1 (4.17) | 23 (95.83) | ||
| O+ | 300 (47.08) | 279 (93) | 21 (7) | 29 (9.67) | 271 (90.33) | ||
| COVID-19 Vaccination | 0.624 | <0.0001 | |||||
| Yes | 221 (35.01) | 203 (91.85) | 18 (8.15) | 7 (3.17) | 214 (96.83) | ||
| No | 365 (57.46) | 340 (95.15) | 25 (6.85) | 49 (13.42) | 316 (86.58) | ||
| Prefer not to say | 51 (7.54) | 50 (98.04) | 1 (1.96) | 5 (9.8) | 46 (90.2) | ||
BMI: Body Mass Indice; *Statistics were calculated without missing values. TASO: technicians, administrative and service officers; † For nationality and ethnic group, others correspond to others of African nationality or ethnic group with tiny numbers (maximum 5).
Table II.
Seroprevalence according to diagnosis and clinical related symptoms.
| Total, N (%) | IgM | IgG | |||||
|---|---|---|---|---|---|---|---|
| Seronegative N, (%) |
Seropositive N, (%) |
p-value | Seronegative N, (%) |
Seropositive N, (%) |
p-value | ||
| Positive COVID-19 test since the start of the pandemic | 0.411 | 0.814 | |||||
| Yes | 57 (8.95) | 51 (89.47) | 6 (10.53) | 6 (10.53) | 51 (89.47) | ||
| No | 528 (82.89) | 493 (93.37) | 35 (6.63) | 51 (9.66) | 477 (90.34) | ||
| COVID-19 diagnosis by a doctor | 0.276 | 0.281 | |||||
| Yes | 52 (8.16) | 51 (98.08) | 1 (1.92) | 8 (15.38) | 44 (84.62) | ||
| No | 390 (61.22) | 363 (93.08) | 27 (6.92) | 37 (9.49) | 353 (90.51) | ||
| COVID-19 self-diagnosis | 0.049 * | 0.45 | |||||
| Yes | 191 (29.98) | 181 (94.76) | 10 (5.24) | 22 (11.52) | 169 (88.48) | ||
| No | 227 (35.64) | 203 (89.43) | 24 (10.57) | 20 (8.81) | 207 (91.19) | ||
| COVID-19 symptoms 2 weeks before survey | 0.871 | 0.835 | |||||
| Yes | 444 (69.70) | 413 (93.02) | 31 (6.98) | 46 (10.36) | 398 (89.64) | ||
| No | 140 (21.98) | 129 (92.14) | 11 (7.86) | 13 (9.29) | 127 (90.71) | ||
| Fever | 1 | 0.242 | |||||
| Yes | 82 (12.87) | 77 (93.90) | 5 (6.10) | 6 (7.32) | 76 (92.68) | ||
| No | 191 (29.98) | 178 (93.19) | 13 (6.81) | 25 (13.09) | 166 (86.91) | ||
| Headaches | 0.727 | 0.817 | |||||
| Yes | 319 (50.08) | 298 (93.42) | 21 (6.58) | 36 (11.28) | 283 (88.72) | ||
| No | 83 (13.03) | 76 (91.57) | 7 (8.43) | 8 (9.64) | 75 (90.36) | ||
| Cough | 0.804 | 0.509 | |||||
| Yes | 162 (25.43) | 150 (92.59) | 12 (7.41) | 17 (10.49) | 145 (89.51) | ||
| No | 179 (28.10) | 168 (93.86) | 11 (6.14) | 24 (13.41) | 155 (86.59) | ||
| Fatigue | 0.372 | 0.0027 * | |||||
| Yes | 252 (39.56) | 238 (94.44) | 14 (5.56) | 20 (7.94) | 232 (92.06) | ||
| No | 102 (16.01) | 93 (91.18) | 9 (8.82) | 20 (19.61) | 82 (80.39) | ||
| Runny nose | 0.977 | 0.489 | |||||
| Yes | 175 (27.47) | 164 (93.71) | 11 (6.29) | 19 (10.86) | 156 (89.14) | ||
| No | 173 (27.16) | 161 (93.06) | 12 (6.94) | 24 (13.87) | 149 (86.13) | ||
| Sore throat | 0.729 | 1 | |||||
| Yes | 95 (14.91) | 87 (91.58) | 8 (8.42) | 11 (11.58) | 84 (88.42) | ||
| No | 242 (37.99) | 226 (93.39) | 16 (6.61) | 28 (11.57) | 214 (88.43) | ||
| Missing | 300 (47.10) | 280 (93.33) | 20 (6.67) | 22 (7.33) | 278 (92.67) | ||
| Breathing difficulties | 0.61 | 0.23 | |||||
| Yes | 78 (12.24) | 74 (94.87) | 4 (5.13) | 6 (7.69) | 72 (92.31) | ||
| No | 262 (41.13) | 242 (92.37) | 20 (7.63) | 35 (13.36) | 227 (86.64) | ||
| Abdominal pain | 0.92 | 0.39 | |||||
| Yes | 32 (5.02) | 30 (93.75) | 2 (6.25) | 2 (6.25) | 30 (93.75) | ||
| No | 283 (44.43) | 262 (93.58) | 21 (7.42) | 38 (13.43) | 245 (86.57) | ||
| Diarrhea | 0.25 | 0.59 | |||||
| Yes | 70 (10.99) | 68 (97.14) | 2 (2.86) | 7 (10) | 63 (90) | ||
| No | 263 (41.29) | 243 (92.39) | 20 (7.61) | 35 (13.31) | 228 (86.69) | ||
| Anosmia/ageusia | 1 | 0.397 | |||||
| Yes | 31 (4.87) | 29 (93.55) | 2 (6.45) | 2 (6.45) | 29 (93.55) | ||
| No | 295 (46.31) | 274 (92.88) | 21 (7.12) | 39 (13.22) | 256 (86.78) | ||
Table III.
Multiple logistic regression of risk factors affecting seropositivity.
| IgM | IgG | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Univariate OR (95% CI) |
p- value | Multivariate OR (95% CI) |
p-value | Univariate OR (95% CI) |
p- value | Multivariate OR (95% CI) |
p-value |
| Age | 1.034 [0.99 -1.06] | 0.055 | 0.971 [0,74 -1,21] | 0,808 | 1.023 [0.98 – 1.081] | 0.345 | 0.974 [0.89 – 1.071] | 0.573 |
| Gender | 1.75 [0.943 -3.25] | 0.073 | 0.776 [0,10 – 4.6] | 0.791 | 0.906 [0.53 -1.578] | 0.728 | 0.913 [0.52 -1.62 | 0.757 |
| Occupation | 1.652 [0.92 – 2.72] | 0.065 | 1.345[0,06 – 22.03] | 0.834 | 1.26 [0.69 – 2.75] | 0.508 | 2.545 [0.60 – 15.33] | 0.250 |
| Level of education | 1.526 [0.91 – 2.47] | 0.095 | 1.709 [0.31 – 9.47] | 0.532 | 0.973 [0.61 – 1.61] | 0.911 | 0.917 [0.48 – 1.73] | 0.790 |
| Nationality | 0.074 [0.003 – 2.21] | 0.083 | 1.96 [0.64 – 4.93] | 0.186 | 2.286 [0.49 – 7.82] | 0.225 | ||
| Ethnic groups | 0.985 [0.86 – 1.13] | 0.826 | 0.723 [0.49 – 0.96] | 0.046 * | 0.95 [0.84 - 1.07] | 0.426 | 0.967 [0.85 – 1.095] | 0.6 |
| Place of residence | 0.995 [0.72 – 1.23] | 0.740 | 0.562 [0.17 – 1.24] | 0.23 | 0.998 [0.80 – 1.27] | 0.992 | 0.981 [0.74 – 1.32] | 0.894 |
| Accommodation type | 1.21 [0.57 – 2.40] | 0.60 | 4.209 [0.91 – 21.62) | 0.067 | 1.17 [0.62 – 2.37] | 0.643 | 0.924 [0.41 – 2.23] | 0.854 |
| Family members | 1.133 [0.77 – 1.66] | 0.522 | 1.849 [0.78 – 4.78] | 0.175 | 1.138 [0.81 – 1.6] | 0.452 | 1.234 [0.83 – 1.85] | 0.296 |
| Marital status | 2.399 [1.08 – 4.87] | 0.021 * | 4.44 [0.28 – 54.32] | 0.235 | 1.02 [0.47 – 2.68] | 0.956 | 1.135 [0.43 – 3.95] | 0.818 |
| Smoker | 1.004 [0.21 – 2.48] | 0.995 | 2.897 [0.087 – 36.8] | 0.457 | ||||
| Alcohol | 1.064 [0.18 -3.17] | 0.926 | 2.06 [0.066 – 30.84} | 0.622 | 0.835 [0.32 – 3.25] | 0.747 | ||
| BMI Categorized | 2.015 [1.12 – 3.56] | 0.016 * | 1.215 [0.39 – 3.73] | 0.729 | 0.785 [0.49 – 1.29] | 0.329 | 0.718 [0.43 – 1.21] | 0.206 |
| Blood Group | 1.011 [0.89 – 1.152] | 0.861 | 1.049 [0.786 – 1.47] | 0.235 | 1.023 [0.91 – 1.14] | 0.679 | 0.988 [0.86 – 1.24] | 0.842 |
| Vaccination Status | 1.206 [0.63 – 2.25] | 0.560 | 0.428 [0.08 – 1.89] | 0.285 | 4.741 [2.25 – 11.65] | <0.001 * | 2.714 [0.59 – 48.48] | 0.325 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



