
Submitted:
21 November 2023
Posted:
22 November 2023
You are already at the latest version
Abstract
Musculoskeletal infections (MIs) are among the most difficult-to-treat staphylococcal diseases. The limited availability of effective antibiotics has encouraged the development of innovative strategies such as combinatory therapy to combat MI. The aim of this study was to investigate the in vitro antistaphylococcal activity of anti-inflammatory and the antimicrobial combinatory effect of celecoxib with oxacillin. The minimum inhibitory concentrations (MICs) of 17 anti-inflammatory drugs were determined for standard strains and clinical isolates of S. aureus strains, counting methicillin-resistant strains (MRSA), by the broth microdilution method. The fractional inhibitory concentration indices (FICIs) were evaluated by the checkerboard assays. Celecoxib produced the most potent antistaphylococcal effect against all the tested strains (MIC ranging from 32 to 64 mg/mL), followed by diacerein against MRSA3 and MRSA ATCC 33592 (MIC 64 mg/mL). Several synergistic effects were observed for tested S. aureus strains, including MRSA (FICI ranging from 0.087 to 0.471). The strongest synergistic interaction (FICI 0.087) was obtained against MRSA ATCC 33592 at a celecoxib concentration of 2 mg/mL with a 19-fold oxacillin MIC reduction (from 512 to 26.888 mg/mL). This is the first report on the antistaphylococcal combinatory effect of celecoxib with oxacillin. Our findings suggest celecoxib and its combination with oxacillin as perspective agents for research focused on the development of novel therapies for MI caused by S. aureus. Thus, this study presents novel findings that celecoxib could, in some cases, resensitise MRSA strains to become susceptible to certain β-lactams (e.g., oxacillin) not previously tested.
Keywords:
antibacterial activity
; antistaphylococcal synergistic effect
; methicillin resistant S. aureus
; musculoskeletal infections
; non-steroidal anti-inflammatory drugs
1. Introduction
Staphylococcus aureus is part of the normal human flora, and about 30% of healthy individuals colonised permanently by this bacterium are asymptomatic [1,2]. On the other hand, S. aureus has become a dangerous human pathogen, causing various infections ranging from common boils to severe septicemia [3]. Staphylococcal infections are commonly treated with antibiotics; however, many strains are nowadays resistant to them. A previous study showed that more than 150,000 patients are infected with methicillin-resistant S. aureus (MRSA) yearly in the EU, causing additional costs of € 380 million to the EU healthcare system [4]. Musculoskeletal infections (MIs) belong to the most difficult-to-treat staphylococcal diseases, which are affecting the bone and surrounding tissues [5,6]. Although several other microorganisms, including fungi (e.g., Exophiala dermatitidis) and certain viruses (e.g., Varicella zoster), have been identified for causing MI [7,8]. S. aureus is the principal bacterial agent responsible for the most severe forms of MI, such as osteomyelitis and septic arthritis [9]. Osteomyelitis may cause progressive destruction and loss of bone in infected patients through the uncoupling of the activities of osteoblasts and osteoclasts, which may foster inflammation and osteoclastogenesis [3,10]. Similarly, septic arthritis is an infection of the joints induced by the colonisation of the joint cavity by bacteria leading to irreversible destruction of the joints despite antibiotics intervention [11,12]. Both these conditions are associated with patient morbidity and mortality [13,14]. Epidemiological data from Germany showed an osteomyelitis incidence rate of 17 cases per 100,000 inhabitants [15]. At the same time, four to ten issues per 100,000 patients per year were reported in septic arthritis, with a high mortality rate of 10-15 % [16,17]. Therefore, new therapeutic options and innovative treatments are needed for patients with MI caused by S. aureus.
Antibiotic therapy and surgical debridement are the main treatment options for osteomyelitis and septic arthritis [18,19]. Surgical debridement, a procedure removing the necrotic bone and irrigating abscessed tissue, is used to reduce the bacterial burden and enhance antibiotic delivery [20,21,22]. However, this surgical procedure may cause pain and inflammation [23]. On the other hand, antibiotics such as glycopeptides (vancomycin) and lincosamides (clindamycin) are commonly used in treating MI, such as osteomyelitis caused by MRSA. Nonetheless, the efficacy of vancomycin is inferior to β-lactams (e.g., oxacillin) in treating methicillin-sensitive S. aureus (MSSA) osteomyelitis and its administration is associated with adverse reactions such as nephrotoxicity, ototoxicity, and thrombocytopenia [24,25]. The main problem associated with the use of clindamycin for the treatment of S. aureus infection is a high resistance rate of >20% [21]. In contrast, antistaphylococcal penicillins (e.g., oxacillin) have a good patient tolerance profile with a superior bone penetration (ranging from 15 to 17%) compared to other β-lactams (e.g., cephalosporins) with a bone penetration profile of 6 to 7% [26]. For this reason, oxacillin is among the preferred drugs for treating MI (e.g., infectious osteomyelitis) caused by MSSA [24]. A clinical study with patients with MI caused by MSSA infection treated with oxacillin resulted in a 92% rate of clinical success [27]. Furthermore, this drug is used primarily as an antistaphylococcal agent in treating suspected hematogenous osteomyelitis in children with mild to moderate illness, especially in regions with low rates of community-acquired MRSA osteomyelitis [28]. Despite the benefits of using oxacillin in the treatment of MI, the oxacillin-resistant S. aureus (ORSA) and MRSA, which causes chronic MI (e.g., septic arthritis), remains a serious clinical challenge [29,30]. The combination of antimicrobial agents may be one of the options for the treatment of MI caused by ORSA and MRSA strains. In general, the combination therapy brings many benefits, especially the reduction of concentrations for each drug used in the combination (with reduced side effects) and delay of developing drug resistance because of the multiple targeting mechanisms of the drug combination [31]. Clavulanic acid can be mentioned as an example of an agent which is in clinical use, often combined with penicillins such as amoxicillin or ticarcillin to fight antibiotic resistance as it enhances the therapeutic potential of the antibiotics [32]. Due to the serious challenge encountered in treating ORSA and MRSA-induced MI with antibiotics, combination therapy involving oxacillin and other agents with different mechanisms of action (e.g., anti-inflammatory drugs) seems to be a promising treatment option to combat these difficult-to-treat infections.
Anti-inflammatory drugs are among the most prescribed medications worldwide [33]. They are generally classified into corticosteroids and non-steroidal anti-inflammatory drugs (NSAIDs). Corticosteroids are essential for the treatment of inflammatory conditions as well as for repressing unpleasant immune reactions. Although their short-term administration is beneficial, their use in chronic situations, even at a low dose, causes significant adverse effects such as hypertension, pancreatitis, osteoporosis, and aseptic joint necrosis, among others [34]. Thus, it is not a preferred treatment option for chronic conditions [35]. Despite certain corticosteroids (e.g., corticosterone) having demonstrated some antimicrobial properties, only a few of them show an effect which is inferior to the currently used antimicrobial agents [36]. In contrast, the antimicrobial potency of NSAIDs (e.g., celecoxib and diclofenac) against certain bacteria, such as S. aureus and S. epidermidis, has previously been demonstrated in several studies [37,38,39]. Although NSAIDs (e.g., celecoxib) are generally considered efficient and well-tolerated drugs in treating chronic inflammatory conditions, non-selective COX inhibitors, such as naproxen, may cause gastrointestinal damage in some patients [40,41]. Contrastingly, selective COX-2 inhibitors have a lesser propensity to cause severe side effects [42]. Celecoxib is a selective COX-2 inhibitor approved for treating rheumatoid arthritis, which is one of the most common risk factors associated with MI [43,44,45]. The synergistic effects of celecoxib with conventional antibiotics, such as vancomycin and clindamycin, against S. aureus have been previously demonstrated [38]. Despite the above-mentioned studies, research on the antistaphylococcal effects of NSAIDs and their combinatory effects with other antibiotics have not been sufficiently explored yet. Thus, this study investigates in vitro growth-inhibitory effect of 17 anti-inflammatory drugs (16 NSAIDs and one corticosteroid) against standard strains and clinical isolates of S. aureus and the antistaphylococcal combinatory effect of celecoxib with oxacillin.
2. Materials and Methods
2.1. Chemicals
The anti-inflammatory agents (acetylsalicylic acid, acemetacin, ampyrone, celecoxib, cortisone, diacerein, diclofenac sodium, diflunisal, ethenzamide, felbinac, ibuprofen, mefenamic acid, nabumetone, propyphenazone, sulindac sulfide, sulindac, and tolfenamic acid) and oxacillin were obtained from Sigma-Aldrich (Prague, CZ). The stock solutions of the anti-inflammatory agents were prepared using dimethyl sulfoxide (DMSO, Penta, Prague, CZ) and deionized water for oxacillin.
2.2. Staphylococcal Strains and Growth Media
In this study, ten S. aureus strains, including antibiotic-resistant and sensitive forms, were tested. American Type Culture Collection (ATCC) standard strains 25923, 29213, 33591, 33592, 43300, and BAA 976 were purchased from Oxoid (Basingstoke, UK) on ready-to-use bacteriological Culti-Loops, and clinical isolates (MRSA1, MRSA2, MRSA3 and MRSA4) were obtained from the Motol University Hospital (Prague, CZ). The identification of clinical isolates was performed by matrix-assisted laser desorption/ionisation time-of-flight mass spectrometry, as previously described [46]. Mueller-Hinton broth (MHB, Oxoid, Basingstoke, UK) was used as the cultivation and assay medium. The pH of the broth was equilibrated to a final value of pH 7.6 using Trizma base (Sigma-Aldrich, Prague, CZ).
2.3. Minimum inhibitory Concentrations (MICs) Determination
The in vitro growth inhibitory activities of the tested compounds against S. aureus strains were evaluated by the broth microdilution method using the 96-well microtiter plates according to the Clinical and Laboratory Standards Institute (CLSI) protocols [47]. Before testing, the bacteria strains were subcultured in MHB media at 37°C for 24 h. The subcultured bacterial density of 1.5 × 108 colony forming unit (CFU mg/mL) was adjusted by 0.5 McFarland standard using a Densi-La-Meter II instrument (Lachema, Brno, CZ) to inoculate the 96-well plates (5 μg/well). Assay microplate preparation and serial dilution of tested compounds were performed through the automated pipetting platform Freedom EVO 100 equipped with a four-channel liquid handling (Tecan, Mannedorf, Switzerland). The initial concentration of oxacillin was optimised based on the susceptibility of the bacteria strains tested (4 and 512 mg/mL for sensitive and resistant strains, respectively), whereas that of all other agents tested in this study was 512 mg/mL. The microplates were then inoculated with bacterial cultures and incubated at 37°C for 24 h. Subsequently, the bacterial growth was measured spectrophotometrically using a Multimode Reader Cytation 3 (BioTek Instruments, Winooski, VT) at 405 nm [48]. The MICs were expressed as the lowest concentrations that inhibited bacteria growth by ≥80% compared with the agent-free growth control [49]. Assay was performed as three independent experiments, each carried out in triplicate. According to the widely accepted norm in MIC testing, the mode and median were used for the final value calculation when the triplicate endpoints were within the two- and three-dilution range, respectively [50]. The highest concentration of DMSO present in the microtiter plates (1%) did not inhibit the bacterial growth of any of the tested strains. S. aureus ATCC 29213 was used as a control strain for antibiotic susceptibility testing. Oxacillin was used as a marker of methicillin resistance (MIC ≥ 4 mg/mL) [47].
2.4. Evaluation of the combined Antistaphylococcal Effect
The combinatory effect of oxacillin with celecoxib against S. aureus was evaluated by the checkerboard assays according to the fractional inhibitory concentration indices (FICIs) [51]. In combination, eight two-fold serial dilutions of the oxacillin prepared in horizontal rows of the microtiter plate were cross-diluted vertically by eight two-fold serial dilutions of celecoxib. Assay microplate preparation and serial dilution for the bacteria’s growth were performed as described in the MICs determination section above. The combinatory effects of oxacillin (A) with celecoxib (B) were determined based on the sum of the fractional inhibitory concentration index (∑FICI) values, which was calculated according to the following parameters: ∑FIC = FICA + FICB, where FICA = MICA (in the presence of B)/MICA (alone), and FICB = MICB (in the presence of A)/MICB (alone). The results were interpreted as follows: a synergistic effect if ΣFICI ≤ 0.5, no interaction if ΣFICI > 0.5 - 4, and antagonistic if ΣFICI > 4 [52]. The MIC values used for FICs calculations are the average of MICs obtained from three independent experiments performed in triplicate.
3. Results
Among the seventeen anti-inflammatory agents tested in this study, six compounds (celecoxib, diacerein, diflunisal, mefenamic acid, sulindac sulfide, and tolfenamic acid) demonstrated in vitro growth-inhibitory effects against various S. aureus strains. Celecoxib showed the most potent antistaphylococcal effect against all the tested strains, including clinical MRSA isolates, with MICs ranging from 32 to 64 mg/mL, followed by diacerein, which inhibited MRSA3 and ATCC 33592 with MIC 64 mg/mL and produced moderate activity against all the other strains (MIC=128 mg/mL). In addition, sulindac sulfide and tolfenamic acid displayed moderate to weak effects, with MICs ranging from 128 to 512 mg/mL against all strains tested. Similarly, mefenamic acid and diflunisal showed weak to no antistaphylococcal activity (MIC ≥ 512 mg/mL). Other compounds tested, namely acetylsalicylic acid, acemetacin, ampyrone, cortisone, diclofenac sodium, ethenzamide, felbinac, ibuprofen, nabumetone, propyphenazone, and sulindac produced no effect on the growth of S. aureus (MIC > 512 mg/mL). The clinical isolate (MRSA1) was the most susceptible strain to celecoxib treatment with MIC 32 mg/mL. The complete data on the growth inhibitory effect of the tested anti-inflammatory drugs against S. aureus are summarised in Table 1.
Since celecoxib produced the most potent antibacterial action against all tested S. aureus strains, including the clinical isolates, we investigated its antistaphylococcal effect when combined with oxacillin. In this combination, several synergistic effects were observed for all the standard S. aureus strains and two of the clinical isolates (MRSA1 and MRSA4) tested, with FICI ranging from 0.087 to 0.471. The strongest synergistic interactions (FICI 0.087) were obtained against MRSA ATCC 33592 at a celecoxib concentration of 2 mg/mL with a 19-fold oxacillin MIC reduction (from 512 to 26.888 mg/mL). Besides, there was a consistently strong synergistic effect (FICI 0.087, 0.095 and 0.097) against this strain at a celecoxib concentration ranging from 4 to 0.5 mg/mL with 12-fold and 40-fold oxacillin MIC reduction from 512 to 40.888 mg/mL (highest reduction) and from 512 to 12.777 mg/mL, respectively. Moreover, the MIC of oxacillin against MRSA ATCC 33591, ATCC 33592 and ATCC 43300 was decreased from resistant (MICs ranging from 227.56 to 512 mg/mL) to a sensitive level (MICs ranging from 2 to 3.555 mg/mL) at celecoxib concentration of 16 mg/mL. Regarding the susceptible strains, celecoxib also showed a relatively strong synergistic effect (FICI 0.369) at the drug concentration of 0.5 mg/mL with a 3-fold antibiotic MIC reduction ranging from 0.25 to 0.090 mg/mL and from 0.5 to 0.180 mg/mL against ATCC 25923 and ATCC 29213, respectively. On the other hand, there was no interaction (FICI ranging from 0.507 to 1.006) between oxacillin and celecoxib against MRSA2, MRSA3, and ATCC BAA 976. No antagonistic effect was observed when celecoxib and oxacillin were combined against all the tested strains. The complete results on the combinatory effects of oxacillin with celecoxib against S. aureus strains are summarised in Table 2.
The combination profiles of the most sensitive S. aureus strains are shown graphically in the form of isobologram curves in Figure 1, representing the FICI values, whereas the axes of each isobologram are the dose-axes of the individual drugs. The resulting graphs confirmed a synergistic effect of oxacillin in combination with celecoxib against S. aureus strains, where the most robust synergy was observed for six ratios in the isobolograms of MRSA ATCC 33591 and ATCC 33592.
4. Discussion
In several previous studies, celecoxib produced in vitro growth-inhibitory effects against standard strains of S. aureus. For example, the suppressive effect of this anti-inflammatory drug against S. aureus ATCC 29213 and ATCC 33592 with MIC 32 mg/mL has previously been reported [37]. Furthermore, another study showed the antimicrobial action of celecoxib against MRSA ATCC 4330 with a MIC of 32 mg/mL. In addition, the susceptibility assessment of clinical isolates to celecoxib showed MIC ranging from 16 to 128 mg/mL [38]. Since the endpoint values determined in our study lie within the two-dilution range of previously published MICs, our results correspond well with the data previously published in the literature. Diacerein is a semisynthetic anthraquinone class of anti-inflammatory drugs used in treating osteoarthritis [53,54]. According to a previous study, this drug displayed an antistaphylococcal activity against S. aureus (sensitive and resistant strains) with MIC ranging from 16 to 64 mg/mL [55]. Additionally, it has been previously demonstrated that diacerein exerted in vitro antimicrobial action against S. aureus clinical isolates with MIC ranging from 4 to 32 mg/mL [56]. In our investigation, this drug also produced an antibacterial effect against all the S. aureus strains tested, including the clinical isolates and MRSA, with an endpoint value within the two dilutions range of previously obtained MICs. Tolfenamic acid is an NSAID belonging to anthranilic acid drugs, usually administered with antibiotics in treating inflammation and other symptoms associated with bacterial infections [57]. A previous experiment showed the antibacterial effects of tolfenamic acid against S. aureus NCTC8325 with a MIC of 163 mg/mL [58], which is similar to the results obtained in our study. It is well described in the literature that sulindac, a sulfinylindene derivative prodrug, must be converted in vivo to its pharmacologically active metabolite sulindac sulfide to act as a non-selective COX inhibitor [59]. Although this agent produced no antimicrobial action in our study, its metabolite showed a moderate growth-inhibitory effect against all tested S. aureus strains. Our finding agrees with the previous study that demonstrated the anti-bacterial effect of sulindac sulfide against S. aureus strains (including ATCC 29213) with a MIC of 175 mg/mL [60]. In accordance with the breakpoint values indicated in standards for antibacterial susceptibility testing, the MIC range of oxacillin obtained in this study for S. aureus ATCC 29213 standard strain indicates their susceptibility to positive antibiotic control [47]. The synergistic effect of celecoxib with various classes of antibiotics has previously been reported in several studies [38,61]. As far as the antistaphylococcal activity of celecoxib with β-lactam antibiotics is considered, its combination with ampicillin significantly reduced numbers of CFU of clinical isolates and mouse macrophage-phagocytosed standard strain of S aureus in agar dilution method and intracellular bacterial viability assay, respectively [61,62]. Nevertheless, this is the first report on the antistaphylococcal combinatory effect of celecoxib with oxacillin demonstrating that celecoxib could resensitize MRSA strains to become susceptible to β-lactams.
Drug efflux is a first-line mechanism of defence against antibiotics in S. aureus [63,64]. A study showed that celecoxib increased the sensitivity of S. aureus to ampicillin by blocking the multi-drug resistance efflux pump [65]. This finding suggests that the combinatory antistaphylococcal effect observed in our study can be due to the inhibition of the efflux pump by celecoxib, which reduces the ability of S. aureus to remove oxacillin from the bacterial cells. Moreover, S. aureus can acquire antibiotic resistance through the hydrolysis of β-lactams [66]. Besides its main action towards COX-2, celecoxib has been observed to inhibit several other enzymes, such as Cytochrome P450 2D6 and carbonic anhydrases [67]. Thus, the inhibition of enzymes or proteins responsible for imparting resistance to the bacteria (e.g., β-lactamases and efflux pumps) by celecoxib can be suggested as a possible mechanism of its synergistic antibacterial action with oxacillin in S. aureus. Nevertheless, further laboratory experiments will be necessary for clarification of the possible mechanism of the synergistic antistaphylococcal action of celecoxib with oxacillin.
Although celecoxib produced the strongest in vitro antistaphylococcal activity compared with other anti-inflammatory drugs tested in this study, its MICs were higher than those of commonly used antibiotics. For example, teicoplanin, a glycopeptide used for the treatment of MRSA infections, was significantly associated with a favourable outcome at MIC < 1.5 mg/mL when used as a maintenance therapy against MRSA [68]. Nevertheless, celecoxib significantly lowered the bacterial burden in the mouse model of MRSA skin infection, which suggests its better in vivo efficacy [38]. Moreover, the antibacterial effect of the drug against other bacteria causing MI, such as Listeria monocytogenes, responsible for L. monocytogenes osteomyelitis, has been previously reported [69]. Data from previous experiments, therefore, suggest celecoxib and its derivatives, which demonstrated a high antibacterial effect (MIC= ≤ 2 mg/mL) against S. aureus and S. epidermidis as perspective candidates for developing agents with dual anti-inflammatory and antibacterial actions for the treatment of MI [37]. In this study, celecoxib also produced a strong synergistic effect with oxacillin, which proposes both agents for combinatory therapeutical use. Since the oral administration of celecoxib demonstrated an effect minimising post-operative inflammation and pain associated with arthroplasty [70], coadministration of celecoxib with antibiotics could increase the efficacy of the preoperative antibiotic prophylaxis. Nevertheless, it is necessary to mention that a much higher concentration of celecoxib than those typically achieved in patients during the use of this agent as an anti-inflammatory drug should be required. For example, a previous clinical report showed that the peak plasma concentrations of celecoxib in humans were between 0.6 to 0.9 mg/mL following a single dose of 200 mg [71]. However, another options for the administration of anti-MI drugs, such as implantable drug-delivery systems, are also commonly used in medical practice [22,72]. These implants allow the drugs to diffuse slowly in a more targeted approach, leading to a controlled and sustained drug release from the implants to the site of infection in the body [22]. Since in commercially available bone cements (e.g., PALACOS R+G, Heraeus Medical, Wehrheim, Germany), the active ingredients (e.g., antibiotics) are present in percentage amounts; the celecoxib can theoretically be incorporated in this therapeutical form in higher concentrations [73]. Therefore, the implantable drug-delivery systems may be an alternative for the coadministration of celecoxib and antibiotics. In the future, the results of this study must be confirmed in animal studies and clinical trials prior to the use of a combination of these drugs in clinical praxis.
5. Conclusions
In conclusion, six of 17 anti-inflammatory drugs tested in this study, namely celecoxib, diacerein, diflunisal, mefenamic acid, sulindac sulfide, and tolfenamic acid, produced in vitro growth-inhibitory effects against S. aureus. Celecoxib showed the most potent antistaphylococcal effect against all the tested strains, including clinical MRSA isolates. In combination with oxacillin, this drug also exhibited synergistic effects against both standard strains and clinical isolates of S. aureus, including MRSA. According to our best knowledge, this is the first report on the antistaphylococcal combinatory effect of celecoxib with oxacillin. Our findings suggest celecoxib and its combination with oxacillin as perspective agents for research focused on the development of novel therapies for MI caused by S. aureus.
Author Contributions
Conceptualization: L.K.: Formal analysis: O.E.O.: Investigation: O.E.O, H.O., J.R. and T.K.: Data curation: O.E.O.: Writing—original draft preparation: O.E.O.: Writing—review and editing: O.E.O., L.K., T.K., H.O. and J.R.: Supervision: L.K. All authors have read and agreed to the published version of the manuscript.
Funding
This work was financially supported by the Internal Grant Agency of the Faculty of Tropical AgriSciences (grant no IGA 20233109).
Institutional Review Board Statement
This study does not need an ethical statement.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data underlying this article is available in the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sakr, A.; Bregeon, F.; Mege, J.L.; Rolain, J.M.; Blin, O. Staphylococcus aureus nasal colonisation: an update on mechanisms, epidemiology, risk factors, and subsequent infections. Front. Microbiol. 2018, 9, 2419. [Google Scholar] [CrossRef] [PubMed]
- Brouillette, E.; Goetz, C.; Droppa-Almeida, D.; Chamberland, S.; Jacques, M.; Malouin, F. Secondary Staphylococcus aureus intramammary colonisation is reduced by non-aureus staphylococci exoproducts. Microbes Infect. 2022, 24, 104879. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, N.; Ryan, J.E.; Widaa, A.; Sexton, G.; Fennell, J.; O’Rourke, S.; Cahill, K.C.; Kearney, C.J.; O’Brien, F.J.; Kerrigan, S.W. Staphylococcal osteomyelitis: disease progression, treatment challenges, and future directions. Clin. Microbiol. Rev. 2018, 31, e00084–17. [Google Scholar] [CrossRef] [PubMed]
- Kock, R.; Becker, K.; Cookson, B.; van Gemert-Pijnen, J.E.; Harbarth, S.; Kluytmans, J.; Mielke, M.; Peters, G.; Skov, R.L.; Struelens, M.J.; et al. Methicillin-resistant Staphylococcus aureus (MRSA): burden of disease and control challenges in Europe. Euro surveill. 2010, 15, pii–19688. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.S. Management of bone and joint infections due to Staphylococcus aureus. Intern. Med. J. 2005, 35, S79–S96. [Google Scholar] [CrossRef] [PubMed]
- Masters, E.A.; Ricciardi, B.F.; Bentley, K.L.D.M.; Moriarty, T.F.; Schwarz, E.M.; Muthukrishnan, G. Skeletal infections: microbial pathogenesis, immunity, and clinical management. Nat. Rev. Microbial. 2022, 20, 385–400. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.; Minion, J.; Skinner, S.; Wong, A. Disseminated Exophiala dermatitidis causing septic arthritis and osteomyelitis. BMC Infect. Dis. 2018, 18, 255. [Google Scholar] [CrossRef] [PubMed]
- Sommer, T.; Karsy, M.; Driscoll, M.J.; Jensen, R.L. Varicella-zoster virus infection and osteomyelitis of the skull. World Neurosurg. 2018, 115, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Tong, S.Y.C.; Davis, J.S.; Eichenberger, E.; Holland, T.L.; Fowler, V.G. Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clin. Microbial. Rev. 2015, 28, 603–661. [Google Scholar] [CrossRef] [PubMed]
- Marriott, I. Apoptosis-associated uncoupling of bone formation and resorption in osteomyelitis. Front. Cell. Infect. Microbiol. 2013, 3, 67718. [Google Scholar] [CrossRef] [PubMed]
- Josefsson, E.; Tarkowski, A. Staphylococcus aureus-induced inflammation and bone destruction in experimental models of septic arthritis. J. Periodontal. Res. 1999, 34, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, L. Novel therapeutic interventions towards improved management of septic arthritis. BMC. Musculoskelet. Disord. 2021, 22, 530. [Google Scholar] [CrossRef] [PubMed]
- Ferrand, J.; El Samad, Y.; Brunschweiler, B.; Grados, F.; Dehamchia-Rehailia, N.; Sejourne, A.; Schmit, J.L.; Gabrion, A.; Fardellone, P.; Paccou, J. Morbimortality in adult patients with septic arthritis: a three- year hospital-based study. BMC. Infect. Dis. 2016, 16, 239. [Google Scholar] [CrossRef]
- Huang, J.F.; Wu, Q.N.; Zheng, X.Q.; Sun, X.L.; Wu, C.Y.; Wang, X.B.; Wu, C.W.; Wang, B.; Wang, X.Y.; Bergman, M.; et al. The characteristics and mortality of osteoporosis, osteomyelitis, or rheumatoid arthritis in the diabetes population: a retrospective study. Int J Endocrinol. 2020, 2020, 8821978. [Google Scholar] [CrossRef] [PubMed]
- Walter, N.; Baertl, S.; Alt, V.; Rupp, M. What is the burden of osteomyelitis in Germany? an analysis of inpatient data from 2008 through 2018. BMC Infect. Dis. 2021, 21, 550. [Google Scholar] [CrossRef] [PubMed]
- Minguez, S.; Molinos, S.; Mateo, L.; Gimenez, M.; Mateu, L.; Cabello, J.; Olive, A. Septic arthritis due to methicillin-resistant Staphylococcus aureus in adults. Reumatol Clin. 2015, 11, 381–386. [Google Scholar] [CrossRef]
- Abram, S.G.F.; Alvand, A.; Judge, A.; Beard, D.J.; Price, A.J. Mortality and adverse joint outcomes following septic arthritis of the native knee: a longitudinal cohort study of patients receiving arthroscopic washout. Lancet Infect. Dis. 2020, 20, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Lew, D.P.; Waldvogel, F.A. Osteomyelitis. Lancet. 2004, 364, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Stake, S.; Scully, R.; Swenson, S.; Lee, D.; Lee, R.; Sparks, A.; Pandarinath, R. Repeat irrigation and debridement for patients with acute septic knee arthritis: incidence and risk factors. J Clin Orthop Trauma. 2020, 11, S177–S183. [Google Scholar] [CrossRef] [PubMed]
- Vowden, K.R.; Vowden, P. Wound debridement part 2: sharp techniques. J.Wound Care. 1999, 8, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Urish, K.L.; Cassat, J.E. Staphylococcus aureus osteomyelitis: bone, bugs, and surgery. Infect. Immun. 2020, 88, e00932–19. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.; Roberts, M.; Al-Kassas, R. Implantable drug delivery systems for the treatment of osteomyelitis. Drug Dev Ind Pharm. 2022, 48, 511–527. [Google Scholar] [CrossRef] [PubMed]
- Lima, A.L.L.; Oliveira, P.R.; Carvalho, V. C.; Cimerman, S.; Savio, E. Recommendations for the treatment of osteomyelitis. Braz J Infect Dis. 2014, 18, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Dombrowski, J.C.; Winston, L.G. Clinical failures of appropriately treated methicillin-resistant Staphylococcus aureus infections. J. Infect. 2008, 57, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Marinho, D.S.; Huff, G.; Ferreira, B.L.; Castro, H.; Rodrigues, C.R.; de Sousa, V.P.; Cabral, L.M. The study of vancomycin use and its adverse reactions associated to patients of a Brazilian university hospital. BMC Res. Notes. 2011, 4, 236. [Google Scholar] [CrossRef] [PubMed]
- Congedi, S.; Minotti, C.; Giaquinto, C.; Da Dalt, L.; Dona, D. Acute infectious osteomyelitis in children: new treatment strategies for an old enemy. World J Pediatr. 2020, 16, 446–455. [Google Scholar] [CrossRef] [PubMed]
- Wieland, B.W.; Marcantoni, J.R.; Bommarito, K.M.; Warren, D.K.; Marschall, J. A retrospective comparison of ceftriaxone versus oxacillin for osteoarticular infections due to methicillin-susceptible Staphylococcus aureus. Clin. Infect. Dis. 2012, 54, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Woods, C.R.; Bradley, J.S.; Chatterjee, A.; Copley, L.A.; Robinson, J.; Kronman, M.P.; Arrieta, A.; Fowler, S.L.; Harrison, C.; Carrillo-Marquez, M.A.; et al. Clinical practice guideline by the pediatric infectious diseases society and the infectious diseases society of America: 2021 guideline on diagnosis and management of acute hematogenous osteomyelitis in pediatrics. J. Pediatric. Infect. Dis. Soc. 2021, 10, 801–844. [Google Scholar] [CrossRef] [PubMed]
- Bell, J.M.; Turnidge, J.D.; Sentry, A. High prevalence of oxacillin-resistant Staphylococcus aureus isolates from hospitalized patients in Asia-Pacific and South Africa: results from sentry antimicrobial surveillance programme, 1998-1999. Antimicrob. Agents Chemother. 2002, 46, 879–881. [Google Scholar] [CrossRef] [PubMed]
- Helito, C.P.; Zanon, B.B.; Miyahara, H.D.E.S.; Pecora, J.R.; Lima, A.L.; Oliveira, P.R.; Vicente, J.R.; Demange, M.K.; Camanho, G.L. Clinical and epidemiological differences between septic arthritis of the knee and hip caused by oxacillin-sensitive and-resistant Staphylococcus aureus. Clinics (Sao Paulo). 2015, 70, 30–33. [Google Scholar] [CrossRef]
- Sun, W.; Sanderson, P.E.; Zheng, W. Drug combination therapy increases successful drug repositioning. Drug Discov. Today. 2016, 21, 1189–1195. [Google Scholar] [CrossRef] [PubMed]
- Huttner, A.; Bielicki, J.; Clements, M.N.; Frimodt-Moller, N.; Muller, A.E.; Paccaud, J.P.; Mouton, J.W. Oral amoxicillin, and amoxicillin–clavulanic acid: properties, indications, and usage. Clin. Microbiol. Infect. 2020, 26, 871–879. [Google Scholar] [CrossRef] [PubMed]
- Domingos, O.D.S.; Alcantara, B.G.V.; Santos, M.F.C.; Maiolini, T.C.S.; Dias, D.F.; Baldim, J.L.; Lago, J.H.G.; Soares, M.G.; Chagas-Paula, D.A. Anti-inflammatory derivatives with dual mechanism of action from the metabolomic screening of Poincianella pluviosa. Molecules. 2019, 24, 4375. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.L. Side effects of corticosteroid therapy. J. Clin. Gastroenterol. 2001, 33, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.M. Clinical pharmacology of corticosteroids. Respir Care. 2018, 63, 655–670. [Google Scholar] [CrossRef] [PubMed]
- Dogan, A.; Otlu, S.; Celebi, O.; Aksu, P.; Saglam, A.G.; Dogan, A.N.C.; Mutlu, N. An investigation of antibacterial effects of steroids. Turkish J. Vet. Anim. Sci. 2017, 41, 22. [Google Scholar] [CrossRef]
- Chiu, H.C.; Lee, S.L.; Kapuriya, N.; Wang, D.; Chen, Y.R.; Yu, S.L.; Kulp, S.K.; Teng, L.J.; Chen, C.S. Development of novel antibacterial agents against methicillin-resistant Staphylococcus aureus. Bioorg Med. Chem. 2012, 20, 4653–4660. [Google Scholar] [CrossRef]
- Thangamani, S.; Younis, W.; Seleem, M.N. Repurposing celecoxib as a topical antimicrobial agent. Front. Microbiol. 2015, 6, 750. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Qu, X.; Tang, H.; Wang, Y.; Yang, H.; Yuan, W.; Yue, B. Diclofenac resensitises methicillin-resistant Staphylococcus aureus to β-lactams and prevents implant infections. Adv. Sci. 2021, 8, 2100681. [Google Scholar] [CrossRef] [PubMed]
- Kivitz, A.J.; Espinoza, L.R.; Sherrer, Y.R.; Liu-Dumaw, M.; West, C.R.A. Comparison of the efficacy and safety of celecoxib 200 mg and celecoxib 400 mg once daily in treating the signs and symptoms of psoriatic arthritis. Semin. Arthritis Rheum. 2007, 37, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Tai, F.W.D.; McAlindon, M.E. Non-steroidal anti-inflammatory drugs and the gastrointestinal tract. Clin Med (Lond). 2021, 21, 131–134. [Google Scholar] [CrossRef] [PubMed]
- FitzGerald, G.A. COX-2 and beyond: approaches to prostaglandin inhibition in human disease. Nat. Rev. Drug Discov. 2003, 2, 879–890. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, F.E.; Faich, G.; Goldstein, J.L.; Simon, L.S.; Pincus, T.; Whelton, A.; Makuch, R.; Eisen, G.; Agrawal, N.M.; Stenson, W.F.; et al. Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: the class study: a randomised controlled trial. celecoxib long-term arthritis safety study. JAMA. 2000, 284, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Krasselt, M.; Baerwald, C.; Petros, S.; Seifert, O. Mortality of sepsis in patients with rheumatoid arthritis: a single-center retrospective analysis and comparison with a control group. J. Intensive Care Med. 2021, 36, 766–774. [Google Scholar] [CrossRef] [PubMed]
- Dinescu, S.C.; Barbulescu, A.L.; Firulescu, S.C.; Chisalau, A.B.; Parvanescu, C.D.; Ciurea, P.L.; Sandu, R.E.; Turcu-Stiolica, A.; Boldeanu, M.V.; Vintila, E.M.; et al. Staphylococcus aureus-induced septic arthritis of the ankle related to malum perforans in a diabetes patient. Rom J Morphol Embryol. 2021, 62, 615–619. [Google Scholar] [CrossRef] [PubMed]
- Rondevaldova, J.; Hummelova, J.; Tauchen, J.; Kokoska, L. In vitro antistaphylococcal synergistic effect of isoflavone metabolite demethyltexasin with amoxicillin and oxacillin. Microb. Drug Resist. 2018, 24, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Clinical and Laboratory Standards Institute. Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically-8th edition: Approved Standard M7-A8. CLSI, Wayne, PA, USA. 2009. [Google Scholar]
- Cos, P.; Vlietinck, A.J.; Berghe, D.V.; Maes, L. Anti-infective potential of natural products: how to develop a stronger in vitro proof-of-concept. J Ethnopharmacol. 2006, 106, 290–302. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, J.H.; Turnidge, J.D.; Washington, J.A. Antimicrobial agents and susceptibility testing: dilution and disc diffusion testing methods. In Murray PR, Baron EJ, Pfaller MA et al ed. Manual of clinical microbiology, 7th ed. Washington DC: ASM Press. 1999; 1531–1533. [Google Scholar]
- Frankova, A.; Vistejnova, L.; Merinas-Amo, T.; Leheckova, Z.; Doskocil, I.; Wong Soon, J.; Kudera, T.; Laupua, F.; Alonso-Moraga, A.; Kokoska, L. In vitro antibacterial activity of extracts from Samoan medicinal plants and their effect on proliferation and migration of human fibroblasts. J Ethnopharmacol. 2021, 264, 113220. [Google Scholar] [CrossRef] [PubMed]
- White, R.L.; Burgess, D.S.; Manduru, M.; Bosso, J. Comparison of three different in vitro methods of detecting synergy: time-kill, checkerboard, and E-test. Antimicrob. Agents Chemother. 1996, 40, 1914–1918. [Google Scholar] [CrossRef] [PubMed]
- Odds, F.C. Synergy, antagonism, and what the chequerboard puts between them. J. Antimicrob. Chemother. 2003, 52, 1. [Google Scholar] [CrossRef] [PubMed]
- Fidelix, T.S.; Macedo, C.R.; Maxwell, L.J.; Fernandes Moca Trevisani, V. Diacerein for osteoarthritis. Cochrane Database Syst. Rev. 2014, 10, CD005117. [Google Scholar] [CrossRef] [PubMed]
- Pavelka, K.; Bruyere, O.; Cooper, C. Diacerein: benefits, risks, and place in the management of osteoarthritis. an opinion-based report from the ESCEO. Drugs Aging. 2016; 33, 75–85. [Google Scholar] [CrossRef]
- Nguon, S.; Novy, P.; Kokoska, L. Potentiation of the in vitro antistaphylococcal effect of oxacillin and tetracycline by the anti-inflammatory drug diacetyl rhein. Chemotherapy. 2013, 59, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Liu, S.; Yue, J.; Sun, S.; Lv, Q.; Jian, S.; Xie, Y.; Han, L.; Zhang, F.; Dai, Y.; et al. In vitro antimicrobial activity of diacerein on 76 isolates of gram-positive cocci from bacterial keratitis patients and in vivo study of diacerein eye drops on Staphylococcus aureus keratitis in mice. Antimicrob. Agents Chemother. 2019, 63, e01874–18. [Google Scholar] [CrossRef] [PubMed]
- Seong, Y.J.; Alhashimi, M.; Mayhoub, A.; Mohammad, H.; Seleem, M.N. Repurposing fenamic acid drugs to combat multidrug resistant Neisseria gonorrhoeae. Antimicrob. Agents Chemother. 2020, 64, e02206–19. [Google Scholar] [CrossRef] [PubMed]
- Yin, Z.; Wang, Y.; Whittell, L.R.; Jergic, S.; Liu, M.; Harry, E.; Dixon, N.E.; Kelso, M.J.; Beck, J.L.; Oakley, A.J. DNA replication is the target for the antibacterial effects of nonsteroidal anti-inflammatory drugs. Chem. Biol. 2014, 21, 481–487. [Google Scholar] [CrossRef]
- Etienne, F.; Resnick, L.; Sagher, D.; Brot, N.; Weissbach, H. Reduction of sulindac to its active metabolite, sulindac sulfide: assay and role of the methionine sulfoxide reductase system. Biochem. Biophys. Res. Commun. 2003, 312, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Shirin, H.; Moss, S.F.; Kancherla., S.; Kancherla, K.; Holt, P.R.; Weinstein, I.B.; Sordillo, E.M. Nonsteroidal anti-inflammatory drugs have bacteriostatic and bactericidal activity against Helicobacter pylori. J. Gastroenterol. Hepatol. 2006, 21, 1388–1393. [Google Scholar] [CrossRef] [PubMed]
- Annamanedi, M.; Kalle, A.M. Celecoxib sensitises Staphylococcus aureus to antibiotics in macrophages by modulating SIRT1. PLoS one. 2014, 9, e99285. [Google Scholar] [CrossRef] [PubMed]
- Annamanedi, M.; Varma, G.Y.N.; Anuradha, K.; Kalle, A.M. Celecoxib enhances the efficacy of low-dose antibiotic treatment against polymicrobial sepsis in mice and clinical Isolates of ESKAPE pathogens. Front. Microbiol. 2017, 8, 805. [Google Scholar] [CrossRef]
- DeMarco, C.E.; Cushing, LA.; Frempong-Manso, E.; Seo, S.M.; Jaravaza, T.A.; Kaatz, G.W. Efflux-related resistance to norfloxacin, dyes, and biocides in bloodstream isolates of Staphylococcus aureus. Antimicrob. Agents Chemother. 2007, 51, 3235–3239. [Google Scholar] [CrossRef] [PubMed]
- Costa, S.S.; Viveiros, M.; Amaral, L.; Couto, I. Multidrug efflux pumps in Staphylococcus aureus: an update. Open Microbiol. J. 2013, 7, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Kalle, A.M.; Rizvi, A. Inhibition of bacterial multidrug resistance by celecoxib, a cyclooxygenase-2 inhibitor. Antimicrob. Agents Chemother. 2011, 50, 439–442. [Google Scholar] [CrossRef]
- Worthington, R.L.; Melander, C. Combination approaches to combat multi-drug resistant bacteria. Trends Biotechnol. 2013, 31, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Gonga, L.; Thorn, C.F.; Bertagnolli, M.M.; Grosser, T.; Altman, R.B.; Klein, T.E. Celecoxib pathways: pharmacokinetics and pharmacodynamics. Pharmacognet. Genomics. 2012, 22, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.Y.; Lee, C.H.; Chien, C.C.; Chen, I.L. Impact of teicoplanin maintenance dose and MIC values on the clinical outcomes of patients treated for methicillin-resistant Staphylococcus aureus bacteremia. Infect. Drug Resist. 2018, 11, 1205–1217. [Google Scholar] [CrossRef] [PubMed]
- Kubota, T.; Mori, Y.; Yamada, G.; Cammack, I.; Shinohara, T.; Matsuzaka, S.; Hoshi, T. Listeria monocytogenes ankle osteomyelitis in a patient with rheumatoid arthritis on adalimumab: a report and literature review of Listeria monocytogenes osteomyelitis. Intern. Med. 2021, 60, 3171–3176. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Li, H.; Zheng, C.; Zheng, C.; Wang, B.; Shen, P.; Xie, Z.; Qu, Y. Efficacy of pre-emptive use of cyclooxygenase-2 inhibitors for total knee arthroplasty: a mini-review. Arthroplasty. 2019, 1, 13. [Google Scholar] [CrossRef] [PubMed]
- FDA. Centre for drug evaluation and research: application number NDA 20-998. Published 1998. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/98/20998AP_clinphrmr_P1.pdf (accessed on 3 August 2023).
- Sidney, L.E.; Heathman, T.R.; Britchford, E.R.; Abed, A.; Rahman, C.V.; Buttery, L.D. Investigation of localized delivery of diclofenac sodium from poly (D, L-lactic acid-co-glycolic acid)/poly (ethylene glycol) scaffolds using an in vitro osteoblast inflammation model. Tissue Eng. Part A. 2015, 21, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Heraeus Medical. Palacos R+G: high-viscosity, radiopaque bone cement containing gentamicin. Published 2020. Available online: https://www.heraeus.com/media/media/hme/doc_hme/products_us/PALACOS_RG_IFU_US.pdf (accessed on 15 August 2023).
Figure 1.
Isobolograms of the most potent synergistic interactions for oxacillin with celecoxib against ATCC 33591(A) and ATCC 33592 (B). An upward concave curve (dark red solid lines) confirms the antibacterial synergy observed against the S. aureus strains, while dotted purple lines represent the synergy border (FICI=0.5).
Figure 1.
Isobolograms of the most potent synergistic interactions for oxacillin with celecoxib against ATCC 33591(A) and ATCC 33592 (B). An upward concave curve (dark red solid lines) confirms the antibacterial synergy observed against the S. aureus strains, while dotted purple lines represent the synergy border (FICI=0.5).
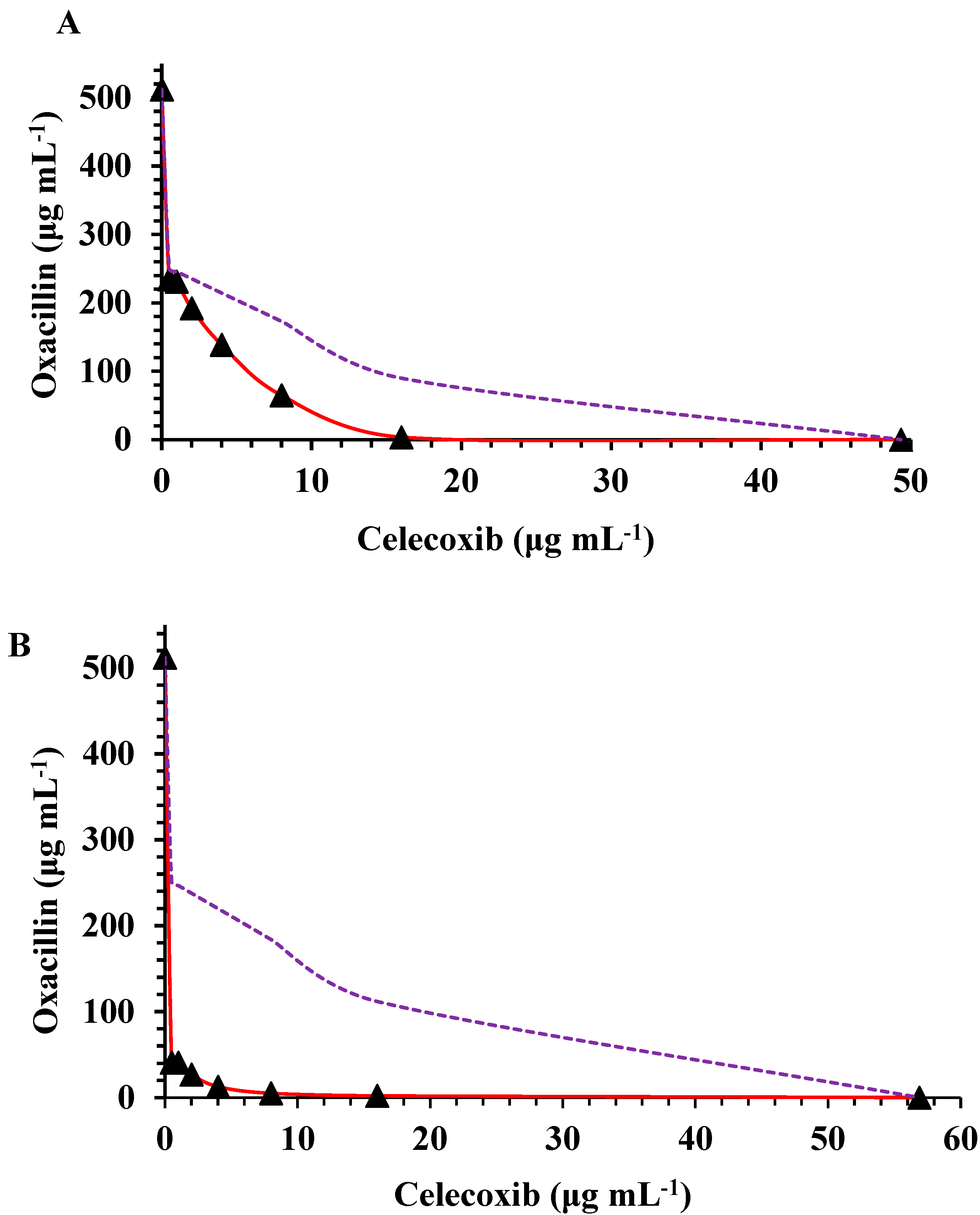

Table 1.
Susceptibility of S. aureus to anti-inflammatory agents in vitro.
| Compound | Minimum inhibitory concentration (mg/mL) | |||||||||
| Standard ATCCa strains | Clinical isolates | |||||||||
| 25923 | 29213 | 33591b | 33592b | 43300b | BAA 976b | MRSA1b | MRSA2b | MRSA3b | MRSA4b | |
| Acetylsalicylic acid | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a |
| Acemetacin | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a |
| Ampyrone | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a |
| Celecoxib | 64 | 64 | 64 | 64 | 64 | 64 | 32 | 64 | 64 | 64 |
| Cortisone | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a |
| Diacerein | 128 | 128 | 128 | 64 | 128 | 128 | 128 | 128 | 64 | 128 |
| Diclofenac sodium | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a |
| Diflunisal | 512 | 512 | 512 | 512 | 512 | n.a | 512 | 512 | n.a | n.a |
| Ethenzamide | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a |
| Felbinac | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a |
| Ibuprofen | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a |
| Mefenamic acid | 512 | 512 | 512 | 512 | 512 | n.a | n.a | 512 | 512 | n.a |
| Nabumetone | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a |
| Propyphenazone | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a |
| Sulindac sulfide | 128 | 128 | 128 | 128 | 128 | 128 | 128 | 128 | 128 | 128 |
| Sulindac | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a |
| Tolfenamic acid | 256 | 256 | 256 | 256 | 256 | 256 | 256 | 512 | 256 | 128 |
| Oxacillinc | 0.25 | 0.5 | 512 | 512 | 256 | 64 | 512 | 256 | 256 | 256 |
The minimum inhibitory concentrations are expressed as mode and median values for triplicate endpoints within the two-and three-dilution range, respectively. aAmerican Type Culture Collection. bMethicillin-resistant S. aureus. cPositive antibiotic control. n.a - not active.
Table 2.
In vitro growth-inhibitory activity of oxacillin and celecoxib combination against S. aureus.
Table 2.
In vitro growth-inhibitory activity of oxacillin and celecoxib combination against S. aureus.
| S. aureus | MICsa alone | CX concentrations (indicated in bold) in combination with OX at the concentration indicated in the MIC column (mg/mL) and related to FICIb | ||||||||||||
| OXc | CXd | 16 | 8 | 4 | 2 | 1 | 0.5 | |||||||
| MIC | FICI | MIC | FICI | MIC | FICI | MIC | FICI | MIC | FICI | MIC | FICI | |||
| ATCCe 29213 | 0.5 | 60.444 | 0.225 | 0.716 | 0.189 | 0.510 | 0.166 | 0.399 | 0.194 | 0.421 | 0.180 | 0.377 | 0.180 | 0.369 |
| ATCC 25923 | 0.25 | 56.888 | 0.230 | 1.204 | 0.263 | 1.196 | 0.166 | 0.736 | 0.152 | 0.646 | 0.125 | 0.517 | 0.090 | 0.369 |
| ATCC 33591 | 512 | 49.332 | 3.555 | 0.331 | 64.888 | 0.288 | 138.890 | 0.352 | 192.000 | 0.415 | 231.110 | 0.471 | 234.670 | 0.468 |
| ATCC 33592 | 512 | 56.888 | 2.222 | 0.285 | 5.110 | 0.150 | 12.777 | 0.095 | 26.888 | 0.087 | 40.888 | 0.097 | 40.888 | 0.088 |
| ATCC 43300 | 227.56 | 53.333 | 2.000 | 0.308 | 44.222 | 0.344 | 88.000 | 0.461 | 156.444 | 0.725 | 156.444 | 0.706 | - | - |
| BAA 976 | 64 | 64 | 55.999 | 1.124 | 39.999 | 0.749 | 42.666 | 0.729 | 32.000 | 0.531 | 32.000 | 0.515 | 32.000 | 0.507 |
| MRSA1f | 512 | 53.333 | 199.560 | 0.689 | 216.111 | 0.572 | 231.111 | 0.526 | 202.666 | 0.433 | 181.333 | 0.372 | 181.333 | 0.363 |
| MRSA2 | 256 | 64 | 114.000 | 0.695 | 213.333 | 0.958 | 241.777 | 1.006 | 241.777 | 0.975 | 241.777 | 0.960 | 241.777 | 0.952 |
| MRSA3 | 256 | 64 | 88.666 | 0.596 | 135.111 | 0.652 | 142.222 | 0.618 | 156.444 | 0.642 | 156.444 | 0.626 | 156.444 | 0.618 |
| MRSA4 | 256 | 64 | 55.555 | 0.467 | 117.333 | 0.583 | 142.222 | 0.618 | 156.444 | 0.642 | 156.444 | 0.626 | 156.444 | 0.618 |
The values are expressed as an average of three independent experiments conducted in triplicate, with a synergistic effect if FICI≤0.5, no interaction if FICI>0.5-4, and antagonistic if FICI>4. aMinimum inhibitory concentration. bFractional inhibitory concentration index. cOxacillin. dCelecoxib. eAmerican Type Culture Collection. fMethicillin-resistant S. aureus. - = not evaluated.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



