
Submitted:
22 November 2023
Posted:
23 November 2023
You are already at the latest version
Abstract
Background and Objectives: The risk of developing cardiovascular diseases (CVD) in patients suffering from rheumatoid arthritis (RA) is two times higher compared to the general population. The objective of this retrospective study was to determine the type of cardiovascular complications that can appear in men vs. women with rheumatoid arth-ritis. Early diagnosis and initiation of therapeutic measures to reduce the progression rate of rheumatoid arthritis, while also maintaining an active lifestyle, are the most important problems in young patients. Materials and Methods: We included a number of 200 pa-tients, divided in 2 groups according to gender (124 women and 76 men) with rheumatoid arthritis, presenting various stages of disease concomitant with cardiovascular complications. We assessed traditional and non-traditional risk factors, electrocardio-graphic and echocardiographic findings in both groups. Results: All patients presented an atherogenic coefficient over two, indicating a significant risk of atherogenesis. Men had elevated levels of total cholesterol compared with women (≥ 200 mg/dL; 77.6% - men vs. 25.8% - women, p<0.001). The participants presented cardiac arrhythmias, especially in the active stage of RA. Women had an increased risk of atrial fibrillation by 2.308 times compared with men (p=0.020). One of the most important complications in young women was pulmonary arterial hypertension (p=0.007). Conclusion: However, in daily clinical practice, the screening for RA is poorly done. Thus, patients are often undiagnosed, while the risk factors are not assessed and RA patients continue to present an increased risk of developing CVD.
Keywords:
rheumatoid arthritis
; cardiovascular complications
; atherogenesis
; cardiac arrhythmias
; inflammation
; disease
; traditional factors
; “non-traditional” factors
1. Introduction
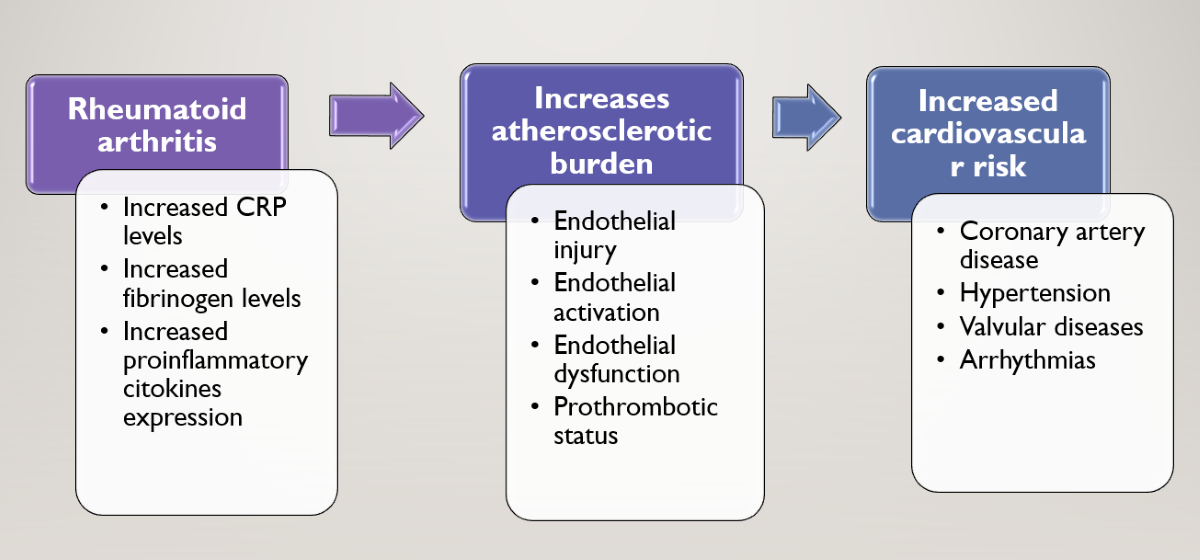
Rheumatoid arthritis (RA) is a systemic autoimmune disease defined by chronic inflammatory joint disease and extra-articular complications with a prevalence of 460 per 100,000 people [1]. It is known that cardiovascular diseases (CVD) are common complications in rheumatoid arthritis patients, resulting in a more severe disease burden [2]. Patients with RA have an increased risk of developing coronary artery disease compared with the general population. RA patients are over three times predispose to have a prior myocardial infarction and also have twice risk of developing heart failure than individuals without RA. Some studies showed an increased risk of cerebrovascular disease, the risk of stroke is increased in RA patients, especially in younger patients. In a Danish study the incidence of atrial fibrillation (AF) in patients with RA was approximately 40% higher than in the general population. Women had higher risk of developing AF compared to men and it was markedly increased in the youngest age groups. Compared with men, RA is more aggressive in women and the prognosis is worse. Sex hormones (especially estrogen) seem to play an important role in the regulation of the immune response.
The etiology of RA is based on interaction between patients’ genotypes and environmental factors. The risk of developing rheumatoid arthritis has been associated with HLA-DRB1 alleles. Several meta-analyses have indicated an increased risk of cardiovascular death by 50–60% [3,4]. This could be explained by the contribution of systemic inflammation in the development of atherogenesis, while the “traditional” cardiovascular risk factors are also attributed to nearly 50% of the total cardiovascular disease (CVD) risk [5].
Patients with active RA have significantly lower high- and low-density lipoprotein cholesterol (HDL-c/LDL-c) levels compared to the healthy population [6]. Treatment with statin at patients with RA tends to reduce the levels of lipids in the blood and inflammatory factors. Smoking is also significantly associated with a higher disease activity score, leading to worse clinical outcomes [7].
In the pathophysiology of RA, the risk of atherogenesis is increased by the inflammatory mechanisms involved in the disease. A useful marker of disease activity, elevated levels of C-reactive protein hold a significant prognostic value [8]. The T-cell mediated cytotoxicity, characterizing the disease, as well as the circulating cytokines such as TNF- α, activates the endothelial cells, directly leading to endothelial injury and up-regulation of the adhesion molecules [9,10]. Even in the absence of identifiable CV risk factors, endothelial dysfunction is frequently present in RA patients, and improves with anti-TNF-α therapy [11,12].
Numerous cardiac structures are involved in the pathological processes of RA, leading to atherosclerosis, arterial stiffness, coronary arteritis, congestive heart failure, valvular disease and fibrinous pericarditis, thus increasing the risk of cardiovascular mortality [13]. Prognostic markers of diseases like hypertension and dyslipidemia could be potentially included [14].
Speckle tracking assessment is useful at RA patients with unexplained dyspnea and a preserved ejection fraction. Impaired global longitudinal strains values in combination with echocardiography findings of elevated filling pressures in the absence of valvular disease of pulmonary abnormalities are consistent with heart failure with preserved ejection fraction. Also, speckle tracking is helpful for the assessment of the effects of anti-inflammatory treatment in RA.
The aim of this study was to determine the cardiovascular complications that can appear in men vs. women with rheumatoid arthritis, while also preventing their appearance through better control strategies of the “traditional” and “non-traditional” CV risk factors.
2. Materials and methods
2.1. Study design and study approval
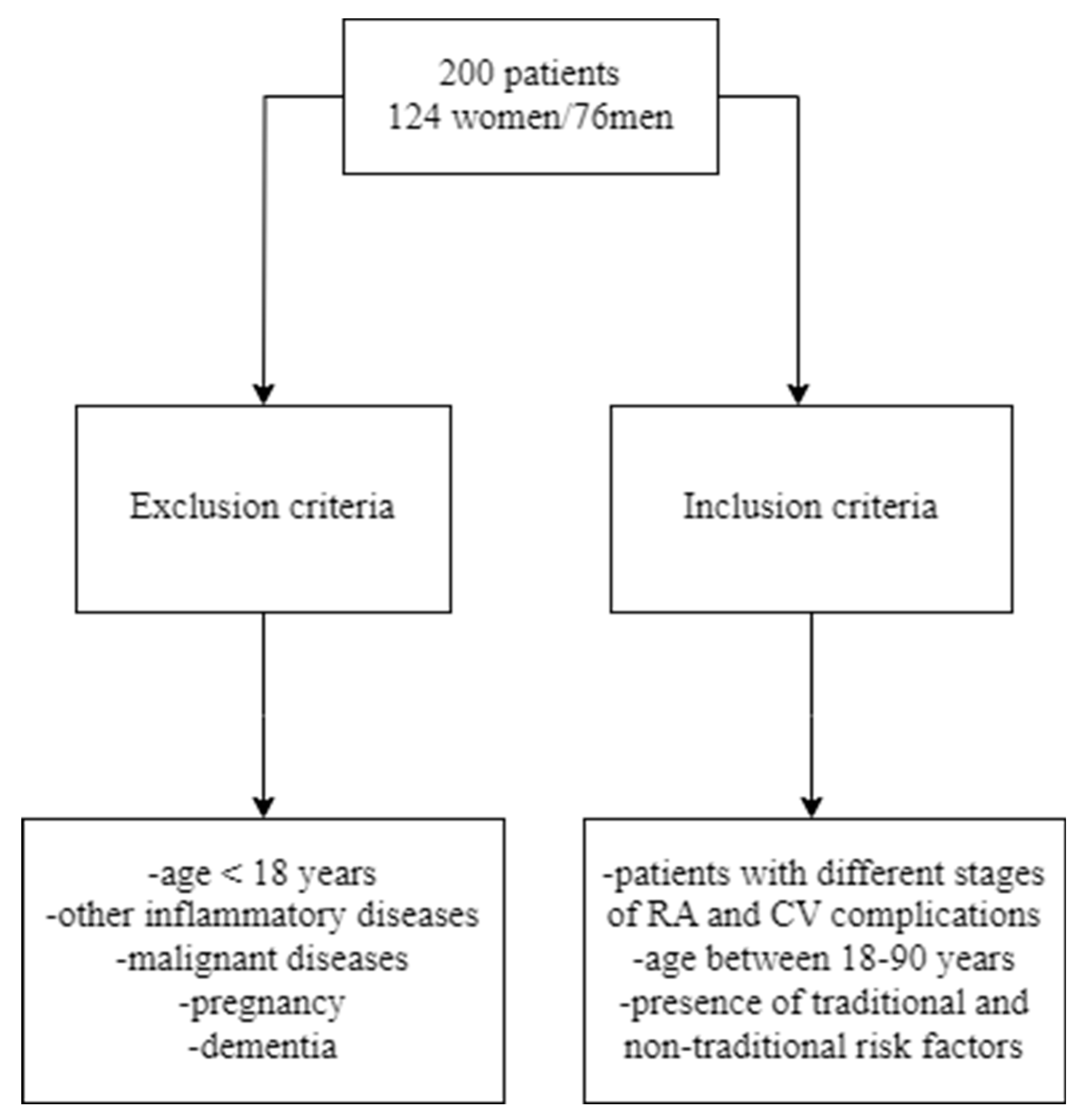
In this retrospective study were included 200 patients (124 women and 76 men) diagnosed with different stages of rheumatoid arthritis and treated in Cardiology Department, of the Bihor County Clinical and Emergency Hospital, between March 2020 and March 2023. The study protocol was approved by the ethics committee of Bihor County Clinical and Emergency Hospital Decision No. 34/26.09.2019.
2.2. Inclusion and exclusion criteria
Figure 1.
Inclusion and exclusion criteria of the patients.
2.3. Data collection
At admission, data regarding the main symptoms which have led to admission in the hospital, complete medical history, history of family diseases, harmful behaviors, details regarding home medication were collected. Each patient underwent the general clinical examination. Moreover, we determined the blood pressure of all patients and conducted concurrent electrocardiograms in conjunction with echocardiographic examinations and laboratory tests.
The patients were divided into two groups:
- group I consisted of 124 women diagnosed with rheumatoid arthritis with different stages of illness, cardiovascular complications, traditional and “non-traditional” risk factors, inflammatory markers, the pattern of joints involved, DAS28 score, CDAI score, ECG and echocardiographic findings and the medication used to treat rheumatoid arthritis.
- group II consisted of 76 men diagnosed with rheumatoid arthritis with different stages of illness, cardiovascular complications, traditional and “non-traditional” risk factors, inflammatory markers, the pattern of joints involved, DAS28 score, CDAI score, ECG and echocardiographic findings and the medication used to treat rheumatoid arthritis.
The score Disease Activity Score 28 (DAS28) helps physicians assess the disease activity, based on the number of swollen and painful joints (the total of joints being 28) and acute-phase reactants: most commonly ESR, but CRP can be used instead. The DAS 28 is calculated on an application because it is not a simple sum and it has a scale of disease activity of 0-10.
DAS28 = 0.56 * √ (TJC) + 0.28 * √ (SJC) + 0.36 * ln (CRP + 1) + 0.014 * PGA + 0.
TJC= Tender Joint Count; SJC= Swollen Joint Count; CRP=C-reactive protein; PGA=Patient Global Assessment of Disease Activity.
According to the DAS28, the disease is classified as:
-very active disease if DAS28>5.1
-active if the DAS is between 5.1 and 3.2
-low disease activity if DAS is 2.6-3.2
-remission if DAS28< 2.6 [45].
Clinical disease activity index (CDAI) is a simplification from the SDAI (Simplified Disease Activity Index). CDAI does not count for the value of acute phase reactants, using the same clinical assessments as the SDAI.
CDAI is calculated as follows: SJC+ TJC+PGA+EGA.
SJC= Swollen Joint Count; TJC= Tender Joint Count; PGA= Patient Global Assessment of Disease Activity; EGA= Evaluator Global Assessment of Disease Activity.
1.The SJC-28 joints are assessed, including: shoulders, elbows, knees, hands: first through fifth metacarpophalangeal joint, the interphalangeal joint of the thumb and the second through fifth proximal interphalangeal joint.
2.The TJC-28 joints are assessed, including: shoulders, elbows, knees, hands: first through fifth metacarpophalangeal joint, the interphalangeal joint of the thumb, and the second through fifth proximal interphalangeal joint.
3.The PGA or Patient Global disease Activity estimate represents the patient’s self-assessment of disease activity on a 0-10 scale where 10 means maximal activity.
4.The EGA or Evaluator Global disease Activity estimate represents the evaluator’s assessment of disease activity on a 0-10 scale where 10 means maximal activity [46].

Table 1.
CDAI score interpretation.
| Clinical Disease Activity Index(CDAI) | |
|---|---|
| 0.0-2.8 | Remission |
| 2.9-10.0 | Low activity |
| 10.1-22.0 | Moderate activity |
| 22.1-76.0 | High activity |
The diagnostic of rheumatoid arthritis was established based on:
- medical history of joint symptoms (pain, tenderness, stiffness, swelling);
- joint symptoms have lasted more than six weeks;
- elevated levels of CRP or ESR;
- positive biomarker test like rheumatoid factor (RF);
- radiographic changes of bones and joints.
The four stages of rheumatoid arthritis are:
-Stage I: In early stage of rheumatoid arthritis, the tissue around the joint(s) is inflamed. Pain and stiffness are common. The destructive changes of bones are not visible on X-rays.
-Stage II: Moderate Stage RA-The inflammation has begun to damage the joint cartilage. Stiffness and a decreased range of motion can appear.
-Stage III: Severe Stage RA- The severe inflammation causes bone damage. Higher pain, stiffness and an even more decreased range of motions compared to stage 2 appear, as well as physical changes.
-Stage IV: End-stage RA- In this stage, the inflammation stops but the joints damage exacerbates. In this stage, severe pain, swelling, stiffness, and loss of joint mobility are the most common [15].
During the hospitalization period, the number of swollen and tender joints, the presence of cardiovascular and non-traditional risk factors, inflammatory markers, ECG and echocardiographic findings were assessed. Some patients performed coronary angiography. The indication for this procedure was the presence of acute coronary syndrome. Before the intervention, the patients had been informed about the risks and the benefits of the procedure. The patients signed the informed consent of the procedure. The coronary angiography revealed monovascular, bivascular and trivascular coronary artery disease. The patients with rheumatoid arthritis presented the following cardiovascular risk factors: smoking, consumption of alcohol, hypertension, hypercholesterolemia and diabetes mellitus.
All patients received DMARDs, with 40 (20%) of them also taking NSAIDs. Remissive treatment was administered as follows: triple therapy (methotrexate, hydroxychloroquine, and sulfasalazine) to 50 patients (25%), DMARDs in monotherapy to 93 patients (46.5%), and DMARDs in dual therapy to 57 patients (28.5%). Corticosteroids were included in the remissive treatment of 86 patients (43%). (Table 2)
2.4. Statistical Analyses
All the data from the study was analyzed using IBM SPSS Statistics 25 and illustrated using Microsoft Office Excel/Word 2021. Quantitative variables were tested for normal distribution using the Shapiro-Wilk Test and were written as averages with standard deviations or medians with interquartile ranges. Quantitative independent variables with non-parametric distribution were tested between groups using Mann-Whitney U tests.
Quantitative paired variables with non-parametric distribution were tested between groups using the Related-Sample Wilcoxon’s Signed Rank Test. Qualitative variables were written as counts or percentages and differences between groups were tested using Fisher’s Exact test/ Pearson Chi-Square Test. Z-tests with Bonferroni corrections were used to further detail the results obtained in the contingency tables.
Logistic regression univariable and multivariable models were used to predict the odds of cardiac complications and arterial fibrillation. The measure of prediction was quantified as odds ratios with 95% confidence intervals. The validity and significance of models were tested along with the goodness-of-fit tests and validation of linearity assumption. In the case of atrial fibrillation, a multivariable model was constructed using the forward stepwise selection based on the Wald criterium.
3. Results
3.1. Patient characteristics and outcomes
The highest prevalence of the disease was observed in patients aged between 50 to 69 years old.
The majority of patients were diagnosed with stage III of the disease; 13% of patients were diagnosed during stage I, 19% of patients were diagnosed with stage II, 42.5 % in stage III and quite a high percentage of 25.5% were diagnosed in stage IV (Table 3).
According to the data presented in Table 3, men were significantly more associated with the dyslipidemia criteria, having more frequently elevated levels of total cholesterol (≥ 200 mg/dL) (77.6% - men vs. 25.8% - women, Fisher’s Exact Test – p<0.001), LDL-cholesterol (≥ 140 mg/dL) (72.4% - men vs. 22.6% - women, Fisher’s Exact Test – p<0.001), triglycerides (≥ 150 mg/dL) (81.6% - men vs. 25.8% - women, Fisher’s Exact Test – p<0.001) and lower concentrations of HDL-cholesterol (< 40 mg/dL) (25% - men vs. 8.1% - women, Fisher’s Exact Test – p=0.002).
There was a higher incidence in men regarding traditional and non-traditional CV risk factors. CRP, ESR, fibrinogen, rheumatoid factor values were increased in men compared with women. (Table 3)
As displayed in the table above, men presented a higher incidence of coronary disease compared to women (Fisher’s Exact Test with Bonferroni corrected Z-tests – p<0.001). 42.1% of men presented monovascular coronary artery disease, 19.7% bivascular coronary artery disease, and 11.8% trivascular coronary artery disease. Women exhibited monovascular coronary artery disease in 24.1% of cases, bivascular coronary artery disease in 9.6% of cases, and trivascular coronary artery disease in 4% of cases. (Table 3)
Electrocardiogram examinations were recorded for every patient enrolled in the study. Left ventricular hypertrophy was significantly more frequent in men (51.3%) than women (27.4%), p=0.001. Secondary ST-T appeared in 39.5% of men and 26.6% of women (showing a tendency towards statistical significance in the direction of higher frequencies in men than women, p=0.062), while atrial fibrillation was more frequently in women (32.3%) than men (17.1%) (p=0.021). Thus, a higher incidence of ECG abnormalities could be observed in men. The examination of the ECGs highlighted the presence of arrhythmias and conduction disorders (supraventricular extrasystoles, left anterior fascicular block, left bundle branch block, premature ventricular contractions, atrial fibrillation). (Table 3)
The echocardiography confirmed the presence of ventricular hypertrophy, previously reported on the ECGs. Moreover, pericarditis, pulmonary arterial hypertension, and mitral valve prolapse appeared to have a higher incidence in women compared to men, although significant differences between genders were not observed (Fisher’s Exact Tests – pericarditis (p=0.174), mitral Valve Prolapse (p=0.083), mitral Regurgitation (p=0.771), pulmonary arterial hypertension (p=0.199), tricuspid regurgitation (p=0.874), pulmonary regurgitation (p=0.880)), while wall motion abnormalities (hypokinesia and akinesia) were present in 31 patients (17 men and 14 women), possibly due to past myocardial infarctions. Young participants, particularly women, had a high incidence of pulmonary arterial hypertension. (Table 3)
The main cause of heart failure was arterial hypertension (44.5%), while coronary artery disease was responsible for 17.5%, valvular heart disease for 14% of cases, and arrhythmias and conduction disorders for 7.5% of cases. (Table3)
Data from Table 4 show the comparison of lipid profile parameters in evolution before and after atorvastatin treatment. Distribution of all variables was non-parametric for all measurements according to the Shapiro-Wilk test (p<0.001). The differences between pre- and post-atorvastatin treatment for all lipid profile parameters were statistically significant according to the Wilcoxon tests, showing the following:
- -
- A decrease of total cholesterol (pre: median = 172.5, IQR = 155-229 vs. post: median = 150, IQR = 145-200) (p<0.001) the observed difference being significant (23.78 ± 18.9, median = 20 (IQR = 10-30.75));
- -
- A decrease of triglycerides (pre: median = 120, IQR = 95-160 vs. post: median = 100, IQR = 90-150) (p<0.001) the observed difference being significant (14.32 ± 22.95, median = 10 (IQR = 5-25));
- -
- A decrease of LDL-cholesterol (pre: median = 110, IQR = 92.25-153 vs. post: median = 90.5, IQR = 82.25-129 (p<0.001) the observed difference being significant (22.34 ± 17, median = 18 (IQR = 11-30.75));
- -
- An increase of HDL cholesterol (pre: median = 40, IQR = 40-44 vs. post: median = 42, IQR = 41-45) (p<0.001) the observed difference being significant (1.13 ± 2.5, median = 1 (IQR = 0-2)).
As we can see in Table 5, women had a higher incidence regarding the damage of joints in RA compared with men.
Data from Table 6 presents DAS28 and CDAI score at both groups. As can be seen, women had a higher incidence of DAS score at 5.1-3.2 (active disease) compared with men who had a higher incidence of DAS score at 3.2-2.6 (low disease activity). Regarding CDAI score, women had a higher incidence of moderate activity disease index (10.1-22.0) compared with men who had a higher incidence of low activity disease index (2.9-10.0).
Data from Table 7 and Figure 2 show the correlation between CDAI and DAS28. Distribution of both variables was non-parametric according to the Shapiro-Wilk test (p<0.001). The correlation observed was statistically significant (p=0.022, R= -0.162), being a weak negative correlation, which shows that patients with high values of the CDAI score were significantly more associated with lower values of DAS28 scores and vice versa.
As displayed in Table 8, 70% of patients (140 individuals) presented an ESR exceeding the upper limits, while the remaining cases presented values within the normal range. Additionally, C-reactive protein levels were within the normal range for 34.5% of patients (69 cases), while 65.5% (132 patients) displayed elevated C-reactive protein values.
Based on collected data, we determined the atherogenic coefficient, men scoring an average value of 4,52 +/- 0,27 (median = 4.60, IQR = 4-5) and women scoring 3,13 +/- 0,20 (median = 2.75, IQR = 2.37-4.10), the Mann-Whitney U Test showing higher values in men versus women (p<0.001). In conclusion, both groups scored an atherogenic coefficient over 2, indicating a higher risk of atherogenesis, more frequently in men (100%) than women (93.5%) (Fisher’s Exact Test – p=0.025). (Figure 3)
3.2. Correlation of patients‘ parameters
The comparison of the analyzed parameters between patients according to the existence of cardiac complications showed that in patients with pericarditis, only HDL-cholesterol and atrial fibrillation were significantly different between groups. Patients with pericarditis had significantly higher values of HDL-cholesterol (median = 42, IQR = 40-45) comparing to patients without pericarditis (median = 40, IQR = 40-43) (p=0.039). Also, atrial fibrillation was significantly more frequently associated with pericarditis (41.2% vs. 23.5%, (p=0.033).
Data from Table 9 show the logistic regression models used for the prediction of cardiac complications In patients with mitral valve prolapse, only frequency of LVH was significantly different between groups, patients with LVH were significantly less associated with mitral valve prolapse (40.9% vs. 21.7%) than patients without LVH (78.3% vs. 59.1%) (p=0.023). CRP, tryglicerides, HDL-cholesterol and secondary ST-T changes were significantly different between groups in patients with mitral regurgitation. This patients had a higher CRP values (median = 121, IQR = 4-150 vs. median = 105, IQR = 2-132.5, p=0.012), lower values of HDL-cholesterol (median = 40, IQR = 40-42 vs. median = 42, IQR = 40-44, p=0.018), higher frequencies of triglycerides dyslipidemia (55.2% vs. 40.7%, p=0.047) and lower frequencies of secondary ST-T changes (38.1% vs. 23%, p=0.031) than patients without mitral regurgitation.
In case of pulmonary arterial hypertension, only rheumatoid factor and HDL-cholesterol were significantly different between groups, patients with pulmonary arterial hypertension had significantly higher values of rheumatoid factor (median = 206, IQR = 137-216 vs. median = 202, IQR = 123-211, p=0.036) and higher values of HDL-cholesterol (median = 42, IQR = 40-45 vs. median = 40, IQR = 40-43, p=0.045) in comparison to patients without pulmonary arterial hypertension. In case of tricuspid regurgitation, none of the parameters were significantly different between groups (p>0.05).
Left ventricular hypertrophy was a significant predictor for mitral valve prolapse (p=0.020). Patients without left ventricular hypertrophy have increased odds of having mitral valve prolapse by 2.493 times (95% C.I.: 1.153-5.376); In case of mitral regurgitation, in univariate models, HDL-cholesterol was not a significant predictor (p=0.055), while CRP (p=0.019), triglycerides dyslipidemia (p=0.043) and secondary ST-T changes (p=0.024) were significant predictors. Each increase of 1 unit of CRP was associated with increased odds of having mitral regurgitation by 1.005 times (95% C.I.:1.001-1.009); Patients with dyslipidemia had increased odds of having mitral regurgitation by 1.793 times (95% C.I.:1.019-3.154). Patients without secondary ST-T changes had increased odds of having mitral regurgitation by 2.057 times (95% C.I.:1.098-3.861);
In case of pulmonary arterial hypertension, none of the variables were significant predictors (p>0.05). For pulmonary regurgitation, left bundle branch block was a significant predictor (p=0.009), patients with this condition had increased odds of having pulmonary regurgitation by 7.264 times (95% C.I.: 1.656-31.869).
Data from Table 10 show the comparison of analyzed parameters between patients according to the existence of atrial fibrillation. Men were significantly less associated with atrial fibrillation (42.9% vs. 24.5%) than women (75.5% vs. 57.1%) (p=0.021) Patients with arterial hypertension were significantly less associated with atrial fibrillation (57.8% vs. 39.6%) than patients without arterial hypertension (60.4% vs. 42.2%) (p=0.025). Fibrinogen levels were significantly lower in patients with atrial fibrillation (median = 4.6, IQR = 4.5-4.85) than in patients without atrial fibrillation (median = 4.7, IQR = 4.5-5.1) (p=0.022). Rheumatoid factor levels were significantly higher in patients with atrial fibrillation (median = 206, IQR = 168.5-213.5) than in patients without atrial fibrillation (median = 201, IQR = 121-213) (p=0.047);
Patients without coronary artery disease were significantly more associated with atrial fibrillation (62.3% vs. 43.5%) (p=0.030);
Data from Table 11 show the logistic regression models used for the prediction of atrial fibrillation. In univariate models, each of the analyzed parameters were significant predictors (p<0.05). Female patients had increased odds of atrial fibrillation by 2.308 times (95% C.I.:1.139-4.674) (p=0.020), Non-smokers had increased odds of atrial fibrillation by 2.557 times (95% C.I.:1.219-5.376) (p=0.013) and non-hypertensive patients had increased odds of atrial fibrillation by 2.087 times (95% C.I.:1.101-3.968) (p=0.024). Each decrease of 1 unit of fibrinogen had increased odds of atrial fibrillation by 3.322 times (95% C.I.:1.183-9.345) (p=0.023), each increase of 1 unit of rheumatoid factor had increased odds of atrial fibrillation by 1.009 times (95% C.I.: 1.001-1.017) (p=0.020). Also, patients without coronary artery disease had increased odds of atrial fibrillation by 1.972 times (95% C.I.:1.008-3.861) (p=0.047); Each decrease of 1 unit of atherogenic coefficient had increased odds of atrial fibrillation by 1.388 times (95% C.I.:1.055-1.828) (p=0.019) and each decrease of 1 unit of total cholesterol had increased odds of atrial fibrillation by 1.010 times (95% C.I.:1.002-1.018) (p=0.011);
The multivariable model was selected using the forward step-wise selection, such as only total cholesterol, coronary artery disease and pericarditis were the selected variables in the prediction, all of them being independent significant predictors.
4. Discussions
This study aimed to identify cardiovascular complications in men vs. women with rheumatoid arthritis (RA), with the purpose of reducing the cardiovascular risk through comprehensive management of traditional and non-traditional risk factors. In this retrospective study we enrolled 200 patients; the majority of them were women, with the highest prevalence of the disease observed in patients aged between 50 to 69 years old. A meta-analysis of 14 controlled observational studies involving 41.490 patients reported that the risk of CVD increases by over 48% in RA patients compared to the general population [16].
Rheumatoid arthritis is two- to three-fold more frequent in women than in men and a strong association with sex hormones has been demonstrated. There is strong evidence that autoimmunity is under genetic control, and genes in sexual chromosomes can play a role in supporting the female prevalence. On the other hand, it is widely accepted that sex hormones- estrogens in particular- may regulate the immune response by promoting the survival of forbidden autoreactive clones and ultimately the prevalence of autoimmunity in women. Accordingly, estrogens have been suggested to be associated with the development of RA [17]. As you can see, our study and other studies shows that women are at higher risk to develop RA compared to men and the reason is because sex hormones (estrogen) play an important role in autoimmunity.
It was interesting to observe that there were several cases of young RA patients, particularly women, who had cardiac complications like pulmonary arterial hypertension, which suggests a potential connection between early onset of RA and premature cardiovascular comorbidities. One reason why pulmonary arterial hypertension is associated in patients with RA is because they have chronic systemic inflammation, especially in the respiratory system which leads to endothelial cell injury, inflammation, coagulation vasoconstriction and fibrosis. A particularly grim prognosis with faster progression of disease and poor response to therapy is found in patients with pulmonary arterial hypertension (PAH) associated with RA [18]. Additionally, a case-control study assessed potential cardiac abnormalities in 47 RA patients without manifested cardiovascular symptoms using Doppler echocardiography technique, emphasizing a high incidence of pulmonary hypertension and left ventricular diastolic dysfunction [18].
Both groups showed elevated atherogenic coefficients, indicating an increased atherogenesis risk. Men also had elevated levels of LDL-cholesterol and an increased prevalence of smoking than women. Atherosclerotic plaques, the main CVD mechanism in RA, result from vascular, metabolic, and inflammatory factors. Dyslipidemia, hypertension, smoking, and inflammation contribute to arterial endothelial damage, causing atherosclerosis. Plaques may grow gradually or become unstable, leading to acute cardiovascular events [19]. The JAK/STAT signaling pathway, regulated by cytokines like interleukin-6, plays a role in RA pathogenesis, increasing systemic inflammation and extra-articular comorbidities such as atherosclerosis [20,21,22]. This and another studies show that chronic inflammation in combination with dyslipidemia and smoking plays an important role in development of atherosclerotic plaque.
The European Society of Cardiology (ESC) recognizes the heightened risk of RA but provides fewer specific recommendations. It suggests a thorough evaluation of total CVD risk in adult patients with a lower threshold and considers multiplying the calculated risk by 1.5 based on disease activity [23]. Additionally, the ESC recommends similar interventions for managing CVD risk as applied to the general high-risk population.
The differences between pre- and post-atorvastatin treatment for both groups were statistically significant (p<0.001). Among statin-treated patients, it was observed an improved lipid profile and reduced inflammatory markers (ESR, CRP), especially in men. A meta-analysis on the use of statins in patients with RA indicated that they may have an anti-inflammatory effect as well as a lipid-lowering property [24,25] with atorvastatin reducing the disease activity score more than simvastatin, although there are conflicting reports where statins are associated with increased risk of developing RA in the first year of use [26].
ECG findings included left ventricular hypertrophy, secondary ST-T changes, left bundle branch block, atrial fibrillation, premature ventricular contraction, sinus tachycardia, and supraventricular extrasystole, particularly during active disease periods. Atrial fibrillation incidence was higher in women. Regarding atrial fibrillation (AF), the systemic inflammatory state in chronic inflammatory conditions like RA may increase the risk. Studies suggest a significantly increased incidence of AF in RA compared to the general population [27]. A Danish nationwide cohort study by Lindhardsen et al. reported an overall 40% higher incidence of AF in RA patients [28]. Using data from a large US commercial insurance plan, Kim et al. found that hospitalization for AF in RA patients was 1.4 times higher than in non-RA patients [29].
Comparable to our results, Shenavar-Masooleh et al. [30] focused on a study on 100 RA patients and found that 32% had abnormal ECG findings. The most abnormal findings were ST-segment and T-wave changes which were similar to those reported in our patients; however, they occurred as 46.9% of abnormalities. Moreover, sinus tachycardia and low voltage were observed in 3.1% each, premature ventricular tachycardia in 6.2%, axis deviation and poor R progression in 9.3% each, branch block in 12.5%, and pulmonary P in 15.6% of abnormalities.
The echocardiography assessment revealed pericarditis, pulmonary arterial hypertension, mitral valve prolapse, mitral and tricuspid regurgitation, and pulmonary regurgitation. We observed no significant differences between genders regarding cardiac valvulopathies. Mac Donald et al. [31] achieved clinical, electrocardiographic (ECG) and echocardiography examinations in 51 American outpatients with RA. Thirty-one percentage of patients had echocardiographic evidence of pericardial effusion and in two patients pericardial thickening was demonstrated. The authors concluded that in unselected outpatients with RA pericardial abnormalities detected by echocardiograph are common although usually clinically unapparent. Pericardial effusion is one of the echocardiographic findings in RA patients. In our study only 20% of women and 12% of men had minimum pericarditis as a reaction of inflammation. Toumanidis et al. [32] observed mitral and aortic cusps change in about 24% of their patients. Our patients had minor mitral valve prolapse and minor mitral regurgitation, especially in women.
Common causes of congestive heart failure included coronary artery disease and arterial hypertension. The patients with RA have approximately a double risk of atherosclerotic CVD, stroke, heart failure, and atrial fibrillation (AF) compared to the general population [33,34,35]. Furthermore, the patients with active RA, differently from the general population, have increased CV events and mortality.
The exact etiology of RA remains incompletely understood; however, both genetic and environmental factors contribute to its development. Several genetic and epigenetic components have been linked to RA, in addition to various environmental factors like cigarette smoke, dust exposure, and the microbiome. Disease progression often begins years before symptom onset, with the development of specific autoantibodies, including rheumatoid factor (RF) and anti-citrullinated protein antibodies (ACPA). ACPA-positive RA patients typically experience more severe disease activity and an elevated risk of cardiovascular mortality. The presence of these antibodies may also contribute to the atherosclerotic process. Interestingly, ACPA has been identified in non-RA patients with cardiovascular disease, correlating with worse cardiovascular outcomes [36].
According to numerous studies, physical activity significantly reduces inflammation, relieves arthritis pain, and improves mobility, making it a recommended treatment by the American College of Rheumatology [37]. The pattern of the disease is fluctuant, with episodic exacerbations and remission periods. Without optimal treatment, symptoms worsen over time, with the joints gradually becoming irreversibly damaged [38]. The life expectancy is reduced by several years, due to RA complications and comorbidities [38].The treatment target is to reduce the side effects and obtain remission [39]. Pharmacological agents that help maintain joint function can be classified as conventional synthetic disease-modifying antirheumatic drugs (DMARDs), biologic DMARDs and targeted synthetic DMARDs, which are included in a new class of nonbiologic DMARDs by the American College of Rheumatology (ACR) [40]. Nonsteroidal anti-inflammatory drugs (NSAIDs) and glucocorticoids (GCs) are often used as adjunctive therapy in reducing inflammation, when patients present inadequate symptom control [41].
Glucocorticoids, like prednisolone, may elevate cardiovascular risk among RA patients in a dose- and duration-dependent manner. In an extensive retrospective registry study by Ocon et al., RA patients who used below five mg daily or had a cumulative dose of <750 mg in total did not experience an increased CV risk [41].However, patients with higher daily doses, greater cumulative doses, or longer treatment durations did face an elevated CV risk. In the recent GLORIA trial, where patients received low-dose glucocorticoids (5 mg prednisolone) for 24 months, there was a 35% increase in the incidence of CV events (2.4 cases per 100 patient years in the prednisolone group vs. 1.7 in the placebo group) [42].Selective COX-2 inhibitors are known to increase the CV risk in the general population by approximately 35–40% [43]. This increase is comparable to that of traditional NSAIDs such as ibuprofen or diclofenac [44].
The strengths of this retrospective study were the facile means of accessing the patient database, no costs for doing the study and age diversity of patients (inclusion criteria was 18-90 years).
The study limitations were as following:
-the study sample is relatively small (200 participants). A larger and more diverse sample could provide more accurate representation of cardiovascular complications of these patients;
-some data are not reported by participants;
-the duration of the study (3 years) might not capture all cardiovascular complications in young patients with rheumatoid arthritis;
- possible selection bias.
We are conscious that our research may have limitations. For example, the number of RA patients is relatively small. However, many studies had a similar number of patients. Further, we did not have clinical endpoints and longitudinal follow up, and therefore, we were not able to assess the clinical impact of our findings.
5. Conclusions
The results of this study suggest that patients with rheumatoid arthritis present an increased risk of cardiovascular complications. Men presented a higher incidence of traditional cardiovascular and non-traditional risk factors compared to women. Regular cardiovascular risk assessment is important in patients with rheumatoid arthritis. Traditional risk factors are often underdiagnosed, particularly in young patients, leading to increased cardiovascular morbidity and mortality.
One of the most important complications in young patients with RA, included in our study was pulmonary arterial hypertension. If untreated, this disease can lead to right-sided heart failure and increased mortality. Also, the examination of the ECGs highlighted a higher incidence of arrhythmias and conduction disorders in men, except for atrial fibrillation which was frequent in women.
Prevention strategies and comprehensive therapeutic schemes require a close collaboration between the rheumatologist, cardiologist, and primary care physician of each RA patient, considering the severity of the disease, the cardiovascular risk factors, as well as the age of each affected individual. Patients with RA should be advice about possible cardiovascular complications and how to recognize early signs of such complications.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, M.R.; methodology, A.I.A, software, M.I.G. validation, F.L.C.A, formal analysis, S.C. and P.M.; investigation, M.R. and A.I.A.; resources, C.J.P.; data curation, A.S.O. and A.G.O.; visualization, V.H. and O.L.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee Bihor County Clinical and Emergency Hospital. (No. 34/26.09.2019).
Informed Consent Statement
Informed consent regarding data processing was obtained from all the participants involved in the study during the hospital admission. All the patients agreed to have their data processed by the hospital for scientific and educational purposes.
Data Availability Statement
The data presented in this study are available on request from the corresponding authors.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Almutairi, K.; Nossent, J.; Preen, D.; Keen, H.; Inderjeeth, C. The global prevalence of rheumatoid arthritis: A meta-analysis based on a systematic review. Rheumatology International 2020, 41, 863–877. [Google Scholar] [CrossRef]
- Logstrup, B.B.; Ellingsen, T.; Pedersen, A.B.; Darvalics, B.; Olesen, K.K.W.; Botker, H.E.; Maeng, M. Cardiovascular risk and mortality in rheumatoid arthritis compared with diabetes mellitus and the general population. Rheumatology 2021, 60, 1400–1409. [Google Scholar] [CrossRef] [PubMed]
- Avina-Zubieta, J.A.; Choi, H.K.; Sadatsafavi, M.; Etminan, M.; Esdaile, J.M.; Lacaille, D. Risk of cardiovascular mortality in patients with rheumatoid arthritis: A meta-analysis of observational studies. Arthr. Rheum. 2008, 59, 1690–1697. [Google Scholar] [CrossRef] [PubMed]
- Meune, C.; Touze, E.; Trinquart, L.; Allanore, Y. Trends in cardiovascular mortality in patients with rheumatoid arthritis over 50 years:A systematic review and meta-analysis of cohort studies. Rheumatology 2009, 48, 1309–1313. [Google Scholar] [CrossRef] [PubMed]
- Crowson, C.S.; Rollefstad, S.; Ikdahl, E.; Kitas, G.D.; van Riel, P.; Gabriel, S.E.; Matteson, E.L.; Kvien, T.K.; Douglas, K.; Sandoo, A.; et al. Impact of risk factors associated with cardiovascular outcomes in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2018, 77, 48–54. [Google Scholar] [CrossRef]
- Boyer, J.-F.; Gourraud, P.-A.; Cantagrel, A.; Davignon, J.-L.; Constantin, A. Traditional cardiovascular risk factors in rheumatoid arthritis: A meta-analysis. Jt. Bone Spine 2011, 78, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Gianfrancesco, M.A.; Trupin, L.; Shiboski, S.; van der Laan, M.; Graf, J.; Imboden, J.; Yazdany, J.; Schmajuk, G. Smoking Is Associated with Higher Disease Activity in Rheumatoid Arthritis: A Longitudinal Study Controlling for Time-varying Covariates. J. Rheumatol. 2019, 46, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Abbot, S.E.; Whish, W.J.; Jennison, C.; Blake, D.R.; Stevens, C.R. Tumour necrosis factor alpha stimulated rheumatoid synovial microvascular endothelial cells exhibit increased shear rate dependent leucocyte adhesion in vitro. Ann Rheum Dis. 1999; 58, 573–581. [Google Scholar]
- Vaudo G, Marchesi S, Gerli R, Allegrucci R, Giordano A, Siepi D, Pirro M, Shoenfeld Y, Schillaci G, Mannarino E. Endothelial dysfunction in young patients with rheumatoid arthritis and low disease activity. Ann Rheum Dis. 2004, 63, 31–35.
- Hurlimann, D.; Forster, A.; Noll, G.; Enseleit, F.; Chenevard, R.; Distler, O.; Bechir, M.; Spieker, L.E.; Neidhart, M.; Michel, B.A.; et al. Anti-tumor necrosis factor-alpha treatment improves endothelial function in patients with rheumatoid arthritis. Circulation. 2002, 106, 2184–2187. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, M.A.; van der Heijde, D.M.F.M.; van Rijswijk, M.H.; et al. Interrelationship of outcome measures and process variables in early rheumatoid arthritis: a comparison of radiologic damage, physical disability, joint counts, and acute phase reactants. J Rheumatol 1994, 21, 425–429. [Google Scholar] [PubMed]
- Naranjo, A.; Sokka, T.; Descalzo, M.A.; Calvo-Alén, J.; Hørslev-Petersen, K.; Luukkainen, R.K.; Combe, B.; Burmester, G.R.; Devlin, J.; Ferraccioli, G.; Morelli, A.; Hoekstra, M.; Majdan, M.; Sadkiewicz, S.; Belmonte, M.; et al. Cardiovascular disease in patients with rheumatoid arthritis: Results from the quest-ra study. Arthritis Research; Therapy. 2008; 10. [Google Scholar]
- Roman, M.J.; Salmon, J.E. Cardiovascular manifestations of rheumatologic diseases. Circulation 2007, 116, 2346–2355. [Google Scholar] [CrossRef] [PubMed]
- Baghdadi, L.R.; Woodman, R.J.; Shanahan, E.M.; Mangoni, A.A. The impact of traditional cardiovascular risk factors on cardiovascular outcomes in patients with rheumatoid arthritis: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0117952. [Google Scholar] [CrossRef] [PubMed]
- Abdulqader, Y.; Al-Ani, M.; Parperis, K. Rheumatoid vasculitis: early presentation of rheumatoid arthritis. BMJ Case Rep. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Avina-Zubieta, J.A.; Thomas, J.; Sadatsafavi, M.; Lehman, A.J.; Lacaille, D. Risk of incident cardiovascular events in patients with rheumatoid arthritis: A meta-analysis of observational studies. Ann. Rheum. Dis. 2012, 71, 1524–1529. [Google Scholar] [CrossRef] [PubMed]
- Gerosa, M.; De Angelis, V.; Riboldi, P.; Meroni, P.L. Rheumatoid arthritis: a female challenge. Womens Health 2008, 4, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Juanatey, C.; Testa, A.; Garcia-Castelo, A.; Garcia-Porrua, C.; Llorca, J.; Ollier, W.E.R.; Gonzalez-Gay, M.A. Echocardiographic and Doppler findings in long-term treated rheumatoid arthritis patients without clinically evident cardiovascular disease. Semin. Arthritis Rheum. 2004, 33, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Lassere, M.N.; Rappo, J.; Portek, I.J.; Sturgess, A.; Edmonds, J.P. How many life years are lost in patients with rheumatoid arthritis? Secular cause-specific and all-cause mortality in rheumatoid arthritis, and their predictors in a long-term Australian cohort study. Intern. Med. J. 2013, 43, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, D.; Nishimura, K.; Tamaki, K.; Tsuji, G.; Nakazawa, T.; Morinobu, A.; Kumagai, S. Impact of smoking as a risk factor for developing rheumatoid arthritis: A meta-analysis of observational studies. Ann. Rheum. Dis. 2010, 69, 70–81. [Google Scholar] [CrossRef]
- Gianfrancesco, M.A.; Trupin, L.; Shiboski, S.; van der Laan, M.; Graf, J.; Imboden, J.; Yazdany, J.; Schmajuk, G. Smoking Is Associated with Higher Disease Activity in Rheumatoid Arthritis: A Longitudinal Study Controlling for Time-varying Covariates. J. Rheumatol. 2019, 46, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Boyer, J.-F.; Gourraud, P.-A.; Cantagrel, A.; Davignon, J.-L.; Constantin, A. Traditional cardiovascular risk factors in rheumatoid arthritis: A meta-analysis. Jt. Bone Spine. 2011, 78, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Hallajzadeh, J.; Safiri, S.; Mansournia, M.A.; Khoramdad, M.; Izadi, N.; Almasi-Hashiani, A.; Pakzad, R.; Ayubi, E.; Sullman, M.J.; Karamzad, N. Metabolic syndrome and its components among rheumatoid arthritis patients: A comprehensive updated systematic review and meta-analysis. PLoS ONE. 2017, 12, e0170361. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Zhao, J.; Li, B.; et al. The anti-inflammatory effects of statins on patients with rheumatoid arthritis: A systemic review and meta-analysis of 15 randomized controlled trials. Autoimmun Rev. 2018, 17, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Soulaidopoulos, S.; Nikiphorou, E.; Dimitroulas, T.; Kitas, G.D. The Role of Statins in Disease Modification and Cardiovascular Risk in Rheumatoid Arthritis. Front Med 2018, 5, 24. [Google Scholar] [CrossRef] [PubMed]
- de Jong, H.J.I.; Cohen Tervaert, J.W.; Lalmohamed, A.; et al. Pattern of risks of rheumatoid arthritis among patients using statins: A cohort study with the clinical practice research datalink. PLoS ONE 2018, 13, e0193297. [Google Scholar] [CrossRef] [PubMed]
- Naranjo, A.; Sokka, T.; Descalzo, M.A.; Calvo-Alén, J.; Hørslev-Petersen, K.; Luukkainen, R.K.; Combe, B.; Burmester, G.R.; Devlin, J.; Ferraccioli, G.; Morelli, A.; Hoekstra, M.; Majdan, M.; Sadkiewicz, S.; Belmonte, M.; et al. Cardiovascular disease in patients with rheumatoid arthritis: Results from the quest-ra study. Arthritis Research; Therapy. 2008, 10. [Google Scholar] [CrossRef] [PubMed]
- Mihaylova, B.; Emberson, J.; Blackwell, L.; Keech, A.; Simes, J.; Barnes, E.H.; et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet 2012, 380, 581–590. [Google Scholar] [PubMed]
- Minder, C.M.; Blumenthal, R.S.; Blaha, M.J. Statins for primary prevention of cardiovascular disease. CurrOpinCardiol 2013, 28, 554–60. [Google Scholar] [CrossRef] [PubMed]
- Shenavar-Masooleh, I.; Zayeni, H.; Haji-Abbasi, A.; Azarpira, M.; Hadian, A.; Hassankhani, A.; et al. Cardiac involvement in rheumatoid arthritis: a crosssectional study in Iran. Indian Heart J 2016, 68, 332–335. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, W.J., Jr.; Crawford, M.H.; Klippel, J.H.; Zvaifler, N.J.; O’Rourke, R.A. Echocardiographic assessment of cardiac structure and function in patients with rheumatoid arthritis. Am J Med. 1977, 63, 890–896. [Google Scholar] [CrossRef] [PubMed]
- Toumanidis, S.T.; Papamichael, C.M.; Antoniades, L.G.; Pantelia, M.I.; Saridakis, N.S.; Mavrikakis, M.E.; Sideris, D.A.; Moulopoulos, S.D. Cardiac involvement in collagen diseases. Eur Heart 1995, 16, 257262. [Google Scholar]
- Semb, A.G.; Ikdahl, E.; Wibetoe, G.; Crowson, C.; Rollefstad, S. Atherosclerotic cardiovascular disease prevention in rheumatoid arthritis. Nat Rev Rheumatol. 2020, 6, 361–379. [Google Scholar] [CrossRef]
- Castañeda, S.; Nurmohamed, M.T.; González-Gay, MA. Cardiovascular disease in inflammatory rheumatic diseases. Best Pract Res Clin Rheumatol. 2016, 30, 851–869. [Google Scholar] [CrossRef] [PubMed]
- Jagpal, A.; Navarro-Millán, I. Cardiovascular co-morbidity in patients with rheumatoid arthritis: a narrative review of risk factors, cardiovascular risk assessment and treatment. BMC Rheumatol. 2018, 2, 10. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, D.; Discacciati, A.; Orsini, N.; Wolk, A. Cigarette smoking and risk of rheumatoid arthritis: A dose-response meta-analysis. Arthritis Res. 2014, 16, R61. [Google Scholar] [CrossRef] [PubMed]
- Otterness, I.G. The value of C-reactive protein measurement in rheumatoid arthritis. Semin Arthritis Rheum. 1994, 24, 91–104. [Google Scholar] [CrossRef]
- Chaurasia, N.; Singh, A.; Singh, I.L.; Singh, T.; Tiwari, T. Cognitive dysfunction in patients of rheumatoid arthritis. J. Fam. Med. Prim. Care 2020, 9, 2219–2225. [Google Scholar] [CrossRef] [PubMed]
- Guo, Q.; Wang, Y.; Xu, D.; Nossent, J.; Pavlos, N.J.; Xu, J. Rheumatoid arthritis: Pathological mechanisms and modern pharmacologic therapies. Bone Res. 2018, 6, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Saag, K.G.; Bridges, S.L.; Akl, E.A.; Bannuru, R.R.; Sullivan, M.C.; Vaysbrot, E.; McNaughton, C.; Osani, M.; Shmerling, R.H.; et al. 2015 American college of rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2016, 68, 1–26. [Google Scholar] [CrossRef]
- Moura, M.D.G.; Lopes, L.C.; Silva, M.T.; Barberato-Filho, S.; Motta, R.H.L.; Bergamaschi, C.C. Use of steroid and nonsteroidal anti-inflammatories in the treatment of rheumatoid arthritis: Systematic review protocol. Medicine 2018, 97, e12658. [Google Scholar] [CrossRef] [PubMed]
- Abbot, S.E.; Whish, W.J.; Jennison, C.; Blake, D.R.; Stevens, C.R. Tumour necrosis factor alpha stimulated rheumatoid synovial microvascular endothelial cells exhibit increased shear rate dependent leucocyte adhesion in vitro. Ann Rheum Dis. 1999, 58, 573–581. [Google Scholar] [CrossRef]
- Hurlimann, D.; Forster, A.; Noll, G.; Enseleit, F.; Chenevard, R.; Distler, O.; Bechir, M.; Spieker, L.E.; Neidhart, M.; Michel, B.A.; et al. Anti-tumor necrosis factor-alpha treatment improves endothelial function in patients with rheumatoid arthritis. Circulation. 2002, 106, 2184–2187. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, M.A.; van der Heijde, D.M.F.M.; van Rijswijk, M.H.; et al. Interrelationship of outcome measures and process variables in early rheumatoid arthritis: a comparison of radiologic damage, physical disability, joint counts, and acute phase reactants. J Rheumatol 1994, 21, 425–429. [Google Scholar] [PubMed]
- Jensen, I.M.H.; Asmussen Andreasen, R.; van Bui Hansen, M.N.; Emamifar, A. The reliability of disease activity score in 28 joints-C-reactive protein might be overestimated in a subgroup of rheumatoid arthritis patients, when the score is solely based on subjective parameters: A cross-sectional, exploratory study. Journal of clinical rheumatology: practical reports on rheumatic & musculoskeletal diseases, U.S. National Library of Medicine. 2017. [Google Scholar]
- Dissanayake, K.; Jayasinghe, C.; Wanigasekara, P.; Dissanayake, J.; Sominanda, A. Validity of clinical disease activity index (CDAI) to evaluate the disease activity of rheumatoid arthritis patients in Sri Lanka: A prospective follow up study based on newly diagnosed patients. PLoS ONE 2022, 17. [Google Scholar] [CrossRef] [PubMed]
Figure 2.
Correlation between CDAI and DAS28.
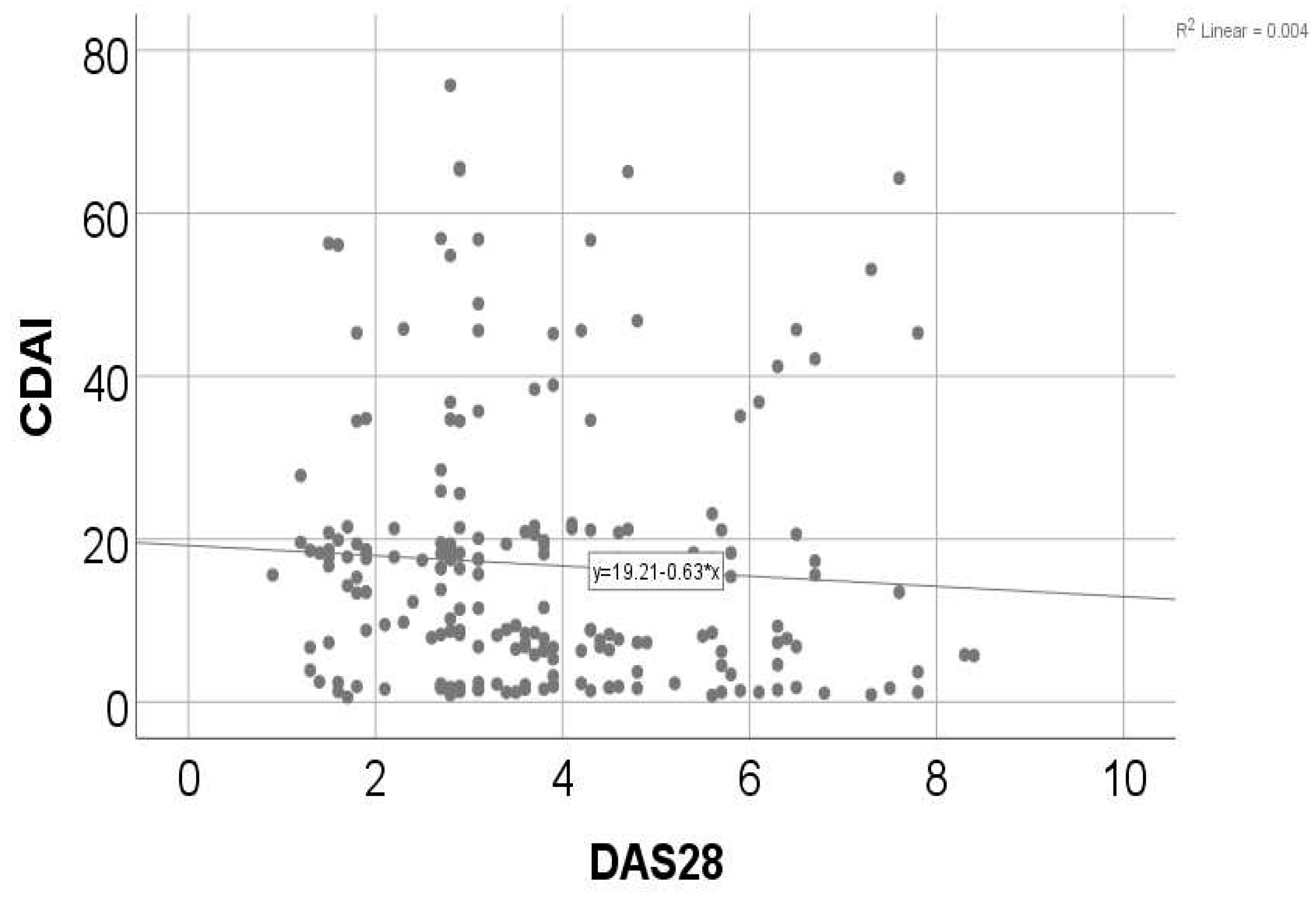
Figure 3.
Comparison of atherogenic coefficient according to gender.
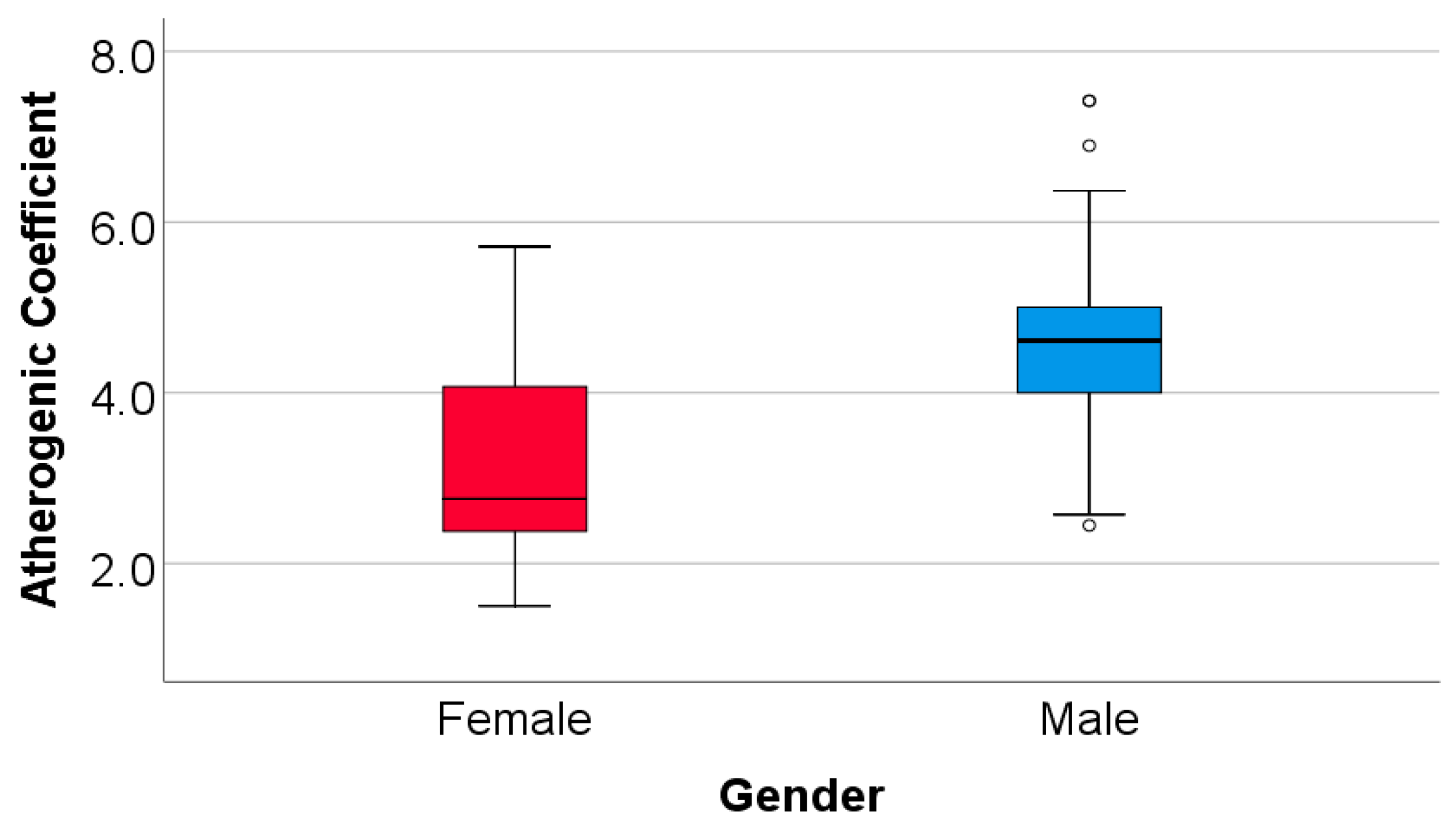
Table 2.
Distribution of patients according to treatment.
| Therapy | Number of cases | Percentage(%) |
|---|---|---|
| DMARDs | 200 | 100 |
| DMARDs +NSAIDs | 40 | 20 |
| DMARDs in monotherapy | 93 | 46.5 |
| DMARDs in dual therapy | 57 | 28.5 |
| MTX+HCQ+SSZ | 50 | 25 |
| Corticosteroids | 86 | 43 |
DMARDs= disease- modifying antirheumatic drugs; NSAIDs= nonsteroidal anti-inflammatory drugs; MTX=methotrexate; HCQ=hydroxychloroquine; SSZ= sulfasalazine.
Table 3.
Analyzed characteristics in the entire study group and according to gender.
| Parameter | Total | Men (N=76) | Women (N=124) | p |
|---|---|---|---|---|
| Age group (Nr., %) | ||||
| 40-49 years | 25 (12.5%) | 11 (14.5%) | 14 (11.3%) | 0.291* |
| 50-69 years | 112 (56%) | 46 (60.5%) | 66 (53.2%) | |
| ≥ 70 years | 63 (31.5%) | 19 (25%) | 44 (35.5%) | |
| Stage of RA (Nr., %) | ||||
| Stage I | 26 (13%) | 13 (17.1%) | 13 (10.5%) | 0.004* |
| Stage II | 38 (19%) | 17 (22.4%) | 21 (16.9%) | |
| Stage III | 85 (42.5%) | 37 (48.7%) | 48 (38.7%) | |
| Stage IV† | 51 (25.5%) | 9 (11.8%) | 42 (33.9%) | |
| Smoking (Nr., %) | 70 (35%) | 50 (65.8%) | 20 (16.1%) | <0.001* |
| Consumption of alcohol (Nr., %) | 47 (23.5%) | 32 (42.1%) | 15 (12.1%) | <0.001* |
| Hypertension (Nr., %) | 106 (53%) | 68 (89.5%) | 38 (30.6%) | <0.001* |
| Hypercholesterolemia (Nr., %) | 91 (45.5%) | 59 (77.6%) | 32 (25.8%) | <0.001* |
| Diabetes mellitus (Nr., %) | 28 (14%) | 15 (19.7%) | 13 (10.5%) | 0.054* |
| CRP (mg/L) (Mean ± SD, Median (IQR)) | 89.04 ± 67.6, 110 (3-142) |
94.68 ± 73.7, 123 (2-153.75) |
79.83 ± 55.5, 105.5 (3-116.5) |
0.006** |
| Fibrinogen (g/L) (Mean ± SD, Median (IQR)) | 4.77 ± 0.32, 4.7 (4.5-5.1) |
5.14 ± 0.15, 5.2 (5.1-5.2) |
4.54 ± 0.14, 4.6 (4.5-4.6) |
<0.001** |
| Rheumatoid factor (UI) (Mean ± SD, Median (IQR)) | 177.52 ± 45.86, 203.5 (125-213) |
212.22 ± 10.6, 210 (205-216.75) |
120.91 ± 12.61, 119 (111-132) |
<0.001** |
| Atherogenic coefficient (Mean ± SD, Median (IQR)) | 3.655 ± 1.251, 3.25 (2.571-4.731) |
4.518 ± 1.08, 4.61 (4-5) |
3.127 ± 1.04 2.75 (2.37-4.1) |
<0.001** |
| ESR (mm/h) (Mean ± SD, Median (IQR)) | 76.98 ± 44.94, 98 (15-106.75) |
75.21 ± 43.46, 97.5 (15-105) |
78.06 ± 45.97, 98.5 (15-107) |
0.552** |
| Dyslipidemia – Total cholesterol (Nr., %) | 91 (45.5%) | 59 (77.6%) | 32 (25.8%) | <0.001* |
| Dyslipidemia – Tryglicerides (Nr., %) | 94 (47%) | 62 (81.6%) | 32 (25.8%) | <0.001* |
| Dyslipidemia – HDL-cholesterol (Nr., %) | 29 (14.5%) | 19 (25%) | 10 (8.1%) | 0.002* |
| Dyslipidemia – LDL-cholesterol (Nr., %) | 83 (41.5%) | 55 (72.4%) | 28 (22.6%) | <0.001* |
| Coronary artery disease (Nr., %) | ||||
| Absent | 97 (48.5%) | 20 (26.3%) | 77 (62.1%) | <0.001* |
| Monovascular coronary a. disease | 62 (31%) | 32 (42.1%) | 30 (24.2%) | |
| Bivascular coronary a. disease | 27 (13.5%) | 15 (19.7%) | 12 (9.7%) | |
| Trivascular coronary a. disease | 14 (7%) | 9 (11.8%) | 5 (4%) | |
| Sinus tachycardia (Nr., %) | 40 (20%) | 15 (19.7%) | 25 (20.2%) | 1.000* |
| Left ventricular hypertrophy (Nr., %) | 73 (36.5%) | 39 (51.3%) | 34 (27.4%) | 0.001* |
| Secondary ST-T changes (Nr., %) | 63 (31.5%) | 30 (39.5%) | 33 (26.6%) | 0.062* |
| Atrial fibrillation (Nr., %) | 53 (26.5%) | 13 (17.1%) | 40 (32.3%) | 0.021* |
| Supraventricular extrasystole (Nr., %) | 42 (21%) | 20 (26.3%) | 22 (17.7%) | 0.210* |
| Left anterior fascicular block (Nr., %) | 32 (16%) | 14 (18.4%) | 18 (14.5%) | 0.552* |
| Premature ventricular contraction (Nr., %) | 26 (13%) | 12 (15.8%) | 14 (11.3%) | 0.391* |
| Left bundle branch block (Nr., %) | 24 (12%) | 10 (13.2%) | 14 (11.3%) | 0.823* |
| Pericarditis (Nr., %) | 34 (17%) | 9 (11.8%) | 25 (20.2%) | 0.174* |
| Mitral valve prolapse grade I-II (Nr., %) | 46 (23%) | 12 (15.8%) | 34 (27.4%) | 0.083* |
| Mitral regurgitation grade I-II (Nr., %) | 87 (43.5%) | 32 (44.1%) | 55 (44.4%) | 0.771* |
| Pulmonary arterial hypertension (Nr., %) | 39 (19.5%) | 11 (14.5%) | 28 (22.6%) | 0.199* |
| Tricuspid regurgitation grade I-II (Nr., %) | 139 (69.5%) | 52 (68.4%) | 87 (70.2%) | 0.874* |
| Pulmonary regurgitation grade I-II (Nr., %) | 128 (64%) | 48 (63.2%) | 80 (64.5%) | 0.880* |
| Etiology – CHF – High blood pressure (Nr., %) | 89 (44.5%) | 38 (50%) | 51 (41.1%) | 0.243* |
| Etiology – CHF – Coronary artery disease (Nr., %) | 35 (17.5%) | 15 (19.7%) | 20 (16.1%) | 0.567* |
| Etiology – CHF – Valvular heart disease (Nr., %) | 28 (14%) | 12 (15.8%) | 16 (12.9%) | 0.675* |
|
Etiology – CHF – Arrhythmias and conduction disorders (Nr., %) |
15 (7.5%) | 5 (6.6%) | 10 (8.1%) | 0.788* |
*Fisher’s Exact Test, **Mann-Whitney U Test, †Stage IV of RA disease significantly more frequent in women than men (according to Bonferroni corrected Z-tests), CHF = Congestive heart failure, IQR = interquartile range, SD = standard deviation, RA = Rheumatoid arthritis.
Table 4.
Comparison of lipid profile parameters in evolution before and after atorvastatin treatment *Related-Samples Wilcoxon Signed Rank Test.
Table 4.
Comparison of lipid profile parameters in evolution before and after atorvastatin treatment *Related-Samples Wilcoxon Signed Rank Test.
| Parameter/Measurement | Pre-Atorvastatin | Post-Atorvastatin | p* | |
|---|---|---|---|---|
| Total cholesterol | Average ± SD | 191 ± 43.33 | 167.22 ± 32.83 | <0.001 |
| Median (IQR) | 172.5 (155-229) | 150 (145-200) | ||
| Triglycerides | Average ± SD | 128.68 ± 39.02 | 114.35 ± 31.45 | <0.001 |
| Median (IQR) | 120 (95-160) | 100 (90-150) | ||
| HDL-cholesterol | Average ± SD | 41.54 ± 2.61 | 42.67 ± 2.81 | <0.001 |
| Median (IQR) | 40 (40-44) | 42 (41-45) | ||
| LDL-cholesterol | Average ± SD | 123.71 ± 38.2 | 101.37 ± 28.61 | <0.001 |
| Median (IQR) | 110 (92.25-153) | 90.5 (82.25-129) | ||
Table 5.
Distribution of the patients depending on the joint involvement in RA.
| Joint involvement in RA | Women | Men |
|---|---|---|
| Wrists | 64(51.6%) | 33(43.4%) |
| MCP | 67(54%) | 32(42.1%) |
| PIP | 54(43.5%) | 15(19.7%) |
| Spares DIP | 44(35.4%) | 22(28.9%) |
| First CMC | 30(24.1%) | 12(15.7%) |
MCP, metacarpophalangeal joints; PIP, proximal interphalangeal joints; DIP, distal interphalangeal joints; CMC, carpometacarpal joints.
Table 6.
DAS28 and CDAI score according to gender; DAS28=Disease Activity Score and 28 refers to the 28 joints that are assessed; CDAI=Clinical Disease Activity Index.
Table 6.
DAS28 and CDAI score according to gender; DAS28=Disease Activity Score and 28 refers to the 28 joints that are assessed; CDAI=Clinical Disease Activity Index.
| DAS28 | >5.1 | 5.1-3.2 | 3.2-2.6 | <2.6 |
|---|---|---|---|---|
| Men | 15(19.73%) | 20(26.31%) | 24(31.57%) | 17(22.36%) |
| Women | 28(22.58%) | 44(35.48%) | 27(21.77%) | 25(20.16%) |
| CDAI score | 0.0-2.8 | 2.9-10.0 | 10.1-22.0 | 22.1-76.0 |
| Men | 17(22.36%) | 23(30.26%) | 21(27.63%) | 15(19.73%) |
| Women | 26(20.96%) | 28(22.58%) | 46(37.09%) | 24(19.35%) |
Table 7.
Correlation between CDAI and DAS28 *Spearman’s rho Correlation Coefficient, **Shapiro-Wilk Test.
Table 7.
Correlation between CDAI and DAS28 *Spearman’s rho Correlation Coefficient, **Shapiro-Wilk Test.
| Correlation | p* |
|---|---|
| CDAI (p<0.001**)x DAS28 (p<0.001**) | 0.022, R= -0.162 |
Table 8.
Biomarkers of inflammation in patients with rheumatoid arthritis.
| Inflammation biomarkers | Number of cases | Percentage(%) |
|---|---|---|
| ESR | 140 | 70 |
| CRP | 131 | 65.5 |
Table 9.
Logistic regression models used for the prediction of cardiac complications.
| Pericarditis | ||||
|---|---|---|---|---|
| Parameter | Univariable | Multivariable | ||
| OR (95% C.I.) | p* | OR (95% C.I.) | p* | |
| HDL-cholesterol | 1.138 (0.996-1.301) | 0.057 | - | - |
| Atrial fibrillation | 2.279 (1.054-4.931) | 0.036 | - | - |
| Mitral valve prolapse | ||||
| LVH | 0.401 (0.186-0.867) | 0.020 | - | - |
| Mitral regurgitation | ||||
| CRP | 1.005 (1.001-1.009) | 0.019 | 1.005 (1.001-1.009) | 0.025 |
| Dyslipidemia – Triglycerides | 1.793 (1.019-3.154) | 0.043 | 1.760 (0.985-3.145) | 0.056 |
| HDL-cholesterol | 0.895 (0.800-1.002) | 0.055 | - | - |
| Secondary ST-T changes | 0.486 (0.259-0.910) | 0.024 | 0.522 (0.275-0.989) | 0.046 |
| Pulmonary arterial hypertension | ||||
| Rheumatoid factor | 1.008 (1.000-1.016) | 0.063 | - | - |
| HDL-cholesterol | 1.113 (0.979-1.264) | 0.102 | - | - |
| Pulmonary regurgitation | ||||
| Left bundle branch block | 7.264 (1.656-31.869) | 0.009 | - | - |
Table 10.
Comparison of analyzed parameters between patients according to the existence of atrial fibrillation (*Fisher’s Exact Test, **Mann-Whitney U Test, ***Pearson Chi-Square Test, ****Fisher’s Exact Test with Bonferroni corrected Z-tests).
Table 10.
Comparison of analyzed parameters between patients according to the existence of atrial fibrillation (*Fisher’s Exact Test, **Mann-Whitney U Test, ***Pearson Chi-Square Test, ****Fisher’s Exact Test with Bonferroni corrected Z-tests).
| Parameter / Group | Atrial fibrillation | p | |
|---|---|---|---|
| Absent (N=147) | Present (N=53) | ||
| Gender (Male) (Nr., %) | 63 (42.9%) | 13 (24.5%) | 0.021* |
| Age (Median (IQR)) | 63 (55-73) | 61 (55-70.5) | 0.642** |
| Stages of RA disease (Nr., %) | 0.890* | ||
| Stage I | 20 (13.6%) | 6 (11.3%) | |
| Stage II | 28 (19%) | 10 (18.9%) | |
| Stage III | 60 (40.8%) | 25 (47.2%) | |
| Stage IV | 39 (26.5%) | 12 (22.6%) | |
| Smoking (Nr., %) | 59 (40.1%) | 11 (20.8%) | 0.012* |
| Alcohol consumption (Nr., %) | 37 (25.2%) | 10 (18.9%) | 0.450* |
| Hypertension (Nr., %) | 85 (57.8%) | 21 (39.6%) | 0.025* |
| Hypercholesterolemia (Nr., %) | 72 (49%) | 19 (35.8%) | 0.110* |
| Diabetes mellitus (Nr., %) | 24 (16.3%) | 4 (7.5%) | 0.165* |
| CRP (Median (IQR)) | 110 (2-135) | 114 (3-147) | 0.505** |
| Fibrinogen (Median (IQR)) | 4.7 (4.5-5.1) | 4.6 (4.5-4.85) | 0.022** |
| ESR (Median (IQR)) | 98 (14-106) | 98 (15.5-110.5) | 0.535** |
| Rheumatoid factor (Median (IQR)) | 201 (121-213) | 206 (168.5-213.5) | 0.047** |
| Atherogenic coefficient (Median (IQR)) | 3.375 (2.75-4.75) | 2.90 (2.29-4.67) | 0.016** |
| Total cholesterol (Median (IQR)) | 180 (157-230) | 160 (145-222.5) | 0.003** |
| Dyslipidemia – Total cholesterol (Nr., %) | 72 (49%) | 19 (35.8%) | 0.110* |
| Triglycerides (Median (IQR)) | 150 (100-170) | 110 (85-157.5) | 0.028** |
| Dyslipidemia – Triglycerides (Nr., %) | 74 (50.3%) | 20 (37.7%) | 0.148* |
| HDL-cholesterol (Median (IQR)) | 40 (40-44) | 40 (40-44.5) | 0.460** |
| Dyslipidemia – HDL-cholesterol (Nr., %) | 24 (16.3%) | 5 (9.4%) | 0.262* |
| LDL-cholesterol (Median (IQR)) | 116 (95-154) | 100 (83.5-149) | 0.008** |
| Dyslipidemia – LDL-cholesterol (Nr., %) | 65 (44.2%) | 18 (34%) | 0.255* |
| Coronary artery disease (Nr., %) | 0.030**** | ||
| Absent | 64 (43.5%) | 33 (62.3%) | |
| Monovascular artery disease | 46 (31.3%) | 16 (30.2%) | |
| Bivascular artery disease | 24 (16.3%) | 3 (5.7%) | |
| Trivascular artery disease | 13 (8.8%) | 1 (1.9%) | |
| Pericarditis (Nr., %) | 20 (13.6%) | 14 (26.4%) | 0.033*** |
| Mitral valve prolapse (Nr., %) | 33 (22.4%) | 13 (24.5%) | 0.849* |
| Mitral regurgitation (Nr., %) | 63 (42.9%) | 24 (45.3%) | 0.872* |
| Pulmonary arterial hypertension (Nr., %) | 24 (16.3%) | 15 (28.3%) | 0.070* |
| Tricuspid regurgitation (Nr., %) | 102 (69.4%) | 37 (69.8%) | 1.000* |
| Pulmonary regurgitation (Nr., %) | 90 (61.2%) | 38 (71.7%) | 0.186* |
| CHF etiology | |||
| Hypertension (Nr., %) | 69 (46.9%) | 20 (37.7%) | 0.264* |
| Coronary artery disease (Nr., %) | 30 (20.4%) | 5 (9.4%) | 0.091* |
| Valvular heart disease (Nr., %) | 18 (12.2%) | 10 (18.9%) | 0.252* |
| Arrhythmias (Nr., %) | 1 (0.7%) | 14 (26.4%) | <0.001* |
Table 11.
Logistic regression models used for the prediction of atrial fibrillation (*Multivariable model selected based on the Forward stepwise selection).
Table 11.
Logistic regression models used for the prediction of atrial fibrillation (*Multivariable model selected based on the Forward stepwise selection).
| Parameter | Univariable | Multivariable* | ||
|---|---|---|---|---|
| OR (95% C.I.) | p* | OR (95% C.I.) | p* | |
| Gender (Female) | 2.308 (1.139-4.674) | 0.020 | - | - |
| Smoking | 0.391 (0.186-0.820) | 0.013 | - | - |
| Hypertension | 0.479 (0.252-0.908) | 0.024 | - | - |
| Fibrinogen | 0.301 (0.107-0.845) | 0.023 | - | - |
| Rheumatoid factor | 1.009 (1.001-1.017) | 0.020 | - | - |
| Atherogenic coefficient | 0.720 (0.547-0.947) | 0.019 | - | - |
| Total cholesterol | 0.990 (0.982-0.998) | 0.011 | 0.991 (0.983-0.999) | 0.034 |
| Triglycerides | 0.991 (0.983-0.999) | 0.029 | - | - |
| LDL-cholesterol | 0.988 (0.979-0.997) | 0.012 | - | - |
| Coronary artery disease | 0.467 (0.245-0.890) | 0.021 | 0.507 (0.259-0.992) | 0.047 |
| Pericarditis | 2.279 (1.054-4.931) | 0.036 | 2.401 (1.078-5.350) | 0.032 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



