Submitted:
24 November 2023
Posted:
27 November 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The COVID-19 pandemic has significantly impacted global health and economies, necessitating the development of effective vaccines against the novel virus. Understanding the structure and function of SARS-CoV-2 is crucial for rational vaccine design. The virus consists of several key proteins, including the spike protein, envelope protein, membrane protein, and nucleocapsid protein. The spike protein plays a crucial role in host cell entry by binding to the angiotensin-converting enzyme 2 (ACE2) receptor on human cells. The replication of the virus within host cells is facilitated by various viral proteins, such as the RNA-dependent RNA polymerase (RdRp) and the main protease (Mpro). Rational vaccine design strategies for SARS-CoV-2 primarily focus on targeting the spike protein due to its role in host cell entry. However, developing vaccines against this protein is challenging due to its highly mutable nature and potential conformational changes. Alternative strategies involve using other viral proteins, such as the nucleocapsid protein, which is conserved and essential for viral replication. Considering T-cell responses in vaccine design is also vital as they play a vital role in controlling viral infections. Vaccines that elicit both antibody and T-cell responses are more likely to provide robust and durable immunity against SARS-CoV-2. Advancements in rational vaccine design for SARS-CoV-2 include mRNA-based vaccines, viral vector-based vaccines, and protein subunit vaccines. However, challenges remain in developing a universally effective vaccine, including the emergence of new SARS-CoV-2 variants and mutations that may affect the efficacy of existing vaccines. In conclusion, rational vaccine design for SARS-CoV-2 requires a comprehensive understanding of the virus's structure and function, targeting key viral proteins, and considering T-cell responses.
Keywords:
COVID-19
; SARS-COV2
; rational vaccine design
; coronavirus
; epitope prediction
; antibodies
; RNA vaccines
1. Introduction
1.1. Overview
Viruses are nanoparticles filled with genetic nanomaterials, with reproductive capabilities assisted by host enzymes and ribosomes [1,2,3]. SARS-CoV-2, a severe acute respiratory syndrome coronavirus, was found in clinical samples and can be found on various surfaces in contaminated environments [4]. The virus is highly stable at 4°C, but heat-sensitive, and inactivation period reduces when incubation temperature is raised to 70°C [4].
SARS is a severe acute respiratory disease caused by the SARS-associated coronavirus, which can be transmitted through airborne droplets of saliva. Incubation typically lasts 2-7 days, with some patients experiencing moderate respiratory symptoms at the start. The lower respiratory stage begins after 3-7 days, with dry, unproductive cough or dyspnea, and hypoxemia. In 10-20% of cases [5], intubation and mechanical ventilation are required. Chest radiographs are usually standard in all patients, and white blood cell counts often drop prematurely during the disease. Most people have low platelet counts at the peak of the disease [5].
Middle East coronavirus respiratory syndrome (MERS-CoV) is a human-borne infectious disease transmitted to infected camels [6]. It is a zoonotic virus shared between animals and humans, acquired through direct or indirect contact with infected animals [6]. Since 2012, 27 countries have reported cases, leading to 858 deaths due to infection and associated complications [6]. The origin of the virus is unknown, but it is thought to have started with bats and spread to camels. Person-to-person transfers are possible, but they are found within relationships residing within the same building.
MERS-CoV infection in healthcare is primarily person-to-person, causing a range of symptoms from asymptomatic to severe disease and death [6]. Common signs include fever, coughing, and breathing problems. Severe disease can lead to respiratory failure, necessitating mechanical respiration and medical care unit support [6]. The virus can cause severe illnesses like renal disease, cancer, chronic obstructive pulmonary disease, diabetes, compromised immune systems, and chronic diseases [6]. Approximately 35% of MERS-CoV patients have died, possibly due to overdoses. Patients with diabetes, insufficiency, chronic obstructive pulmonary disease, and autoimmune diseases are at higher risk of severe infection complications [6].
The coronavirus SARS-CoV-2 is responsible for the COVID-19 pandemic, a respiratory disease. The virus was declared an international public health emergency by the WHO on March 11, 2020 [7]. SARS-CoV-2, the most frequent respiratory-related coronavirus, could also be infected by SARSr-CoV. The person-to-person transmission of SARS-CoV-2 was confirmed during the COVID-19 epidemic on January 20, 2020 [7]. Transmission was initially thought to occur predominantly with respiratory drops, but some studies suggest that the virus may also be present in the air through aerosols. An average of 1000 infectious virions of SARS-CoV-2 are believed to initiate a new infection during human transmission [7]. Preliminary studies show that the virus can survive in plastic and stainless steel for a few days, but not on cardboard or copper. The virus does not operate with soap, making its lipid structure unstable. In infected individuals, viral RNA is also present in wild and sperm samples [7]. The extent of the virus's infection is uncertain, but studies show that the pharynx reaches a high level of the virus in the blood approximately four days after infection or the first week of symptoms [7]. Figure 1 shows different ways of transmission for SARS-COV2.
1.2. Global Scenario
Thus, in line with WHO, these viruses' potential to grow to become a plague worldwide represents a significant public health risk [8]. The pandemic feature of COVID-19 may be a hallmark of the disease and, therefore, the indisputable fact that the virus is not well-known, of substantial concern for humanity the sole radical measure that may prevent the host's infection and block the virus's spread, is a vaccine. Figure 2a,b indicate the amount of COVID-19 cases and deaths reported till now and weekly by WHO Region (global region) [9,10].
1.3. Mutation
In recent months, several additional varieties of the original virus have been found, and they appear to induce major changes in the pathogen's behavior, including contagiousness. These viral variants have developed in fast succession in several countries, including the United Kingdom, South Africa, and Brazil, and have outcompeted existing varieties in certain cases. Although better surveillance and sequencing efforts may explain why these variants are suddenly showing up, a certain pattern repeating shows that the changes are not random (Figure 3) [11]. Based on evidence that it contains several alterations that could impact the mode of its function, WHO has recognized the most recent COVID-19 variation Omicron (B.1.1.529) as a variant of concern. There is consistent evidence that Omicron spreads far faster than Delta in settings where community transmission is established, with a doubling period of 2-3 days. The overall risk associated with this new variant remains very high.
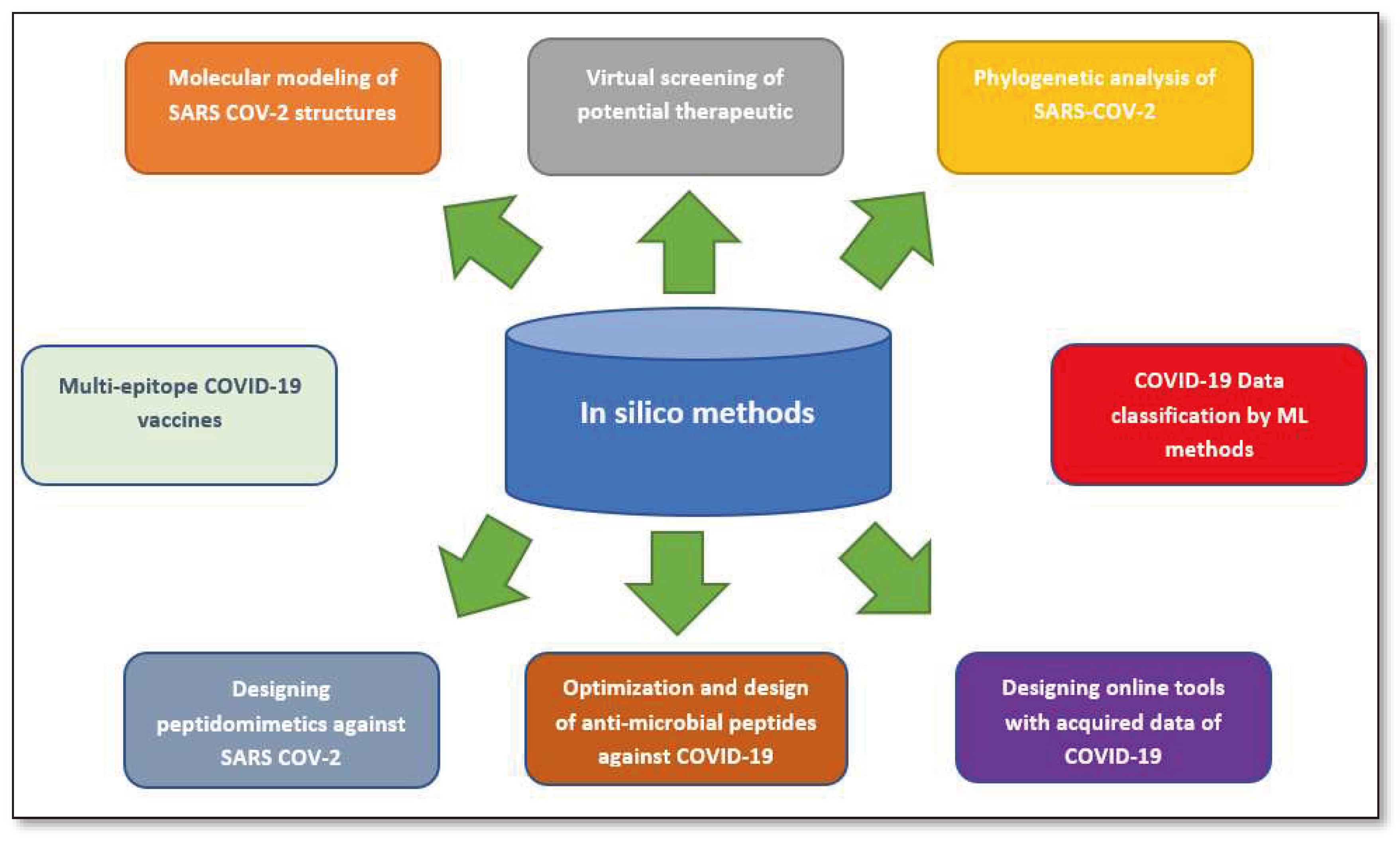
This paper reviews the research on rational vaccinology models, including reverse vaccinology, RNA vaccinology, and machine learning approaches, in response to SARS-CoV-2 infection. The review aims to provide readers with an overview of how in silico methods have been effective in handling COVID-19 components and their potential for future use in crisis situations. The authors highlight the limitations of existing research, such as only discussing scientific applications, not reviewing comparisons with benchmark models, and not yet maturing big data analysis. The paper illustrates how in silico techniques helped life science professionals during the COVID-19 pandemic to improve their research quality.
Figure 4.
The crucial part in silico assays play in the global fight against COVID-19 and some of its applications in biology and medicine [12].
Figure 4.
The crucial part in silico assays play in the global fight against COVID-19 and some of its applications in biology and medicine [12].
2. This publication provides a concise review of the existing literature on in silico strategies for combating COVID-19, focusing on SARS-CoV-2 structure predictions, phylogenetic analysis, drug virtual screening, natural compound production, vaccine development, and machine learning and AI. It also discusses potential challenges in using machine learning for future pandemics.Vaccine Development Strategies: Historical Outline
Vaccine development strategies have evolved significantly over time, from empirical methods like smallpox to modern rational design approaches. Traditional methods include inactivated and live attenuated vaccines, which have been instrumental in controlling and eradicating infectious diseases in the past [13]. Newer approaches like recombinant protein subunit vaccines and nucleic acid-based vaccines have emerged, allowing for more precision in vaccine creation and faster development and manufacturing [13]. The recent development of mRNA vaccines and viral vector vaccines has been particularly promising in the fight against COVID-19 [13,14]. However, safety and efficacy remain crucial, and clinical trials are necessary to ensure the vaccine's effectiveness and safety in both short-term and long-term [13,15]. Collaborative efforts between researchers and pharmaceutical companies have expedited the development of a COVID-19 vaccine, with previous research on similar viruses informing the process [13,14]. To ensure safety, purity must be checked, and sterile production lines provided [15,16]. Knowledge gaps remain regarding the correlates of protection, how to best induce immunity in vulnerable populations, and the longevity of immunity induced by vaccination or natural infection [14]. A chronology of vaccine developments and achievements are shown in Figure 5.
Modern vaccinology focuses on improving subunit immunizations to increase viability and limit risks in healthy, compromised individuals. Advancements and information contribute to a comprehensive plan that not only enhances execution but also reduces time and costs associated with preclinical and clinical events. Promising methodologies/empowering variables and road obstructions are featured in green and pink, separately in Figure 6.
3. Molecular Architecture of SARS CoV-2
Other coronaviruses, such as HKU1, NL63, OC43, and 229E, are more frequently found infecting people and producing serious infections, but SARS-CoV and MERS-CoV are more commonly seen infecting humans and causing serious infections [19]. Virion particles attach to the Angiotensin-converting enzyme 2 (ACE2) cell surface receptor to join the center cell [20]. The 3C-like protease (3CLpro) and the papain-like protease (PLpro) [21,22]- induced proteolysis breaks down large polyproteins into smaller molecules for coagulation and packaging of new virions, allowing infection to spread more easily. SARS-main CoV-2 enzyme, which controls viral replication and transcription, is also a prominent protease, making it a popular therapeutic target [23]. Toxicity is necessary for viral replication by RNA-dependent RNA polymerase (RdRp), another interesting enzyme [24].
These major enzymes, 3CLpro, PLpro, and RdRp, are responsible for the proteolysis, replication, and synthesis of new virions [26]. Because these enzymes are required for virus survival, reproduction, and transmission, they could be used as drug targets in therapeutic strategies. There are successive similarities between these proteins and their viruses, which are closely related to SARS-CoV (2002) and MERS-CoV (2004), during the vision period for developing medications and vaccines (2013). As a result, because SARS-CoV-2 has high sequence ownership of its RdRp and 3CLpro proteins in SARS-CoV and MERS-CoV, medical molecules assumed to be used to classify SARS-CoV, and MERS-CoV might be also helpful in treating COVID-19 with similar success like SARS-CoV and MERS-CoV. The SARS-CoV-2 spike receptor-binding domain (RBD), on the other hand, differs significantly from the SARS-CoV domain, particularly in the two ACE2 receptor-interacting regions. Because of these structural differences, previously used SARS-CoV spike RBD antibodies and treatment peptides are less effective against SARS-CoV-2, necessitating new formulations and treatment modalities [27]. Figure 7 explains the above structure in pictorial form.
CoVs affect cells that are responsible for their cytocidal activity in addition to the immune response [28]. Numerous studies show that CoV infection results in cytopathic effects such as apoptosis, membrane damage, and cell lysis. The virus causes cell adhesions, which result in syncytial formation [29]. The above-mentioned processes are observed within the cell because of vesicle fusion, complicating viral replication and disrupting Golgi structures [30]. In comparison to other CoVs, such as SARS-CoV and MERS-CoV, cytopathic effects within renal cells and the development of syncytia in lung tissue have been demonstrated [25].
The replication of the mutation mechanism is required for SARS-CoV-2 pathogenesis [31]. T cells and secondary messengers such as cytokines play a significant role in disease progression during infection. Molecules associated with a disease or secreted from damaged cells have been discovered to be involved in measuring the body's response to congenital and mutational SARS-CoV-2 disorders (PRRs). In addition to T cells, humoral antibodies are important in CoV-induced infections [32].
4. The COVID-19 Vaccine Landscape
Around 51 vaccinated clinicians and 16 vaccines are currently in the pre-treatment phase or under study [33]. Most viral vaccinations work by activating antibodies that neutralize the virus envelope or spike glycoproteins (NAbs) (Table 1). In the case of respiratory pathogens like SARS-CoV-2, the vaccine may be required to supplement systemic nAbs and prevent low-grade infections. Designing safe and effective mucosal vaccines remains a top objective to protect against infectious illnesses like tuberculosis, HIV, diarrheas, or influenza. The vaccine will contribute to the production of an effective nAb vaccine by addressing the vaccine's versatility in producing nAbs, the nAbs required for immunity, the strength of the nAb response, the concentration of memory cells for viral expression, nAb dependence on drug-inducing Abs, and the need for an immunosuppressive medicine [33].
5. Different Coronavirus Vaccines in Development
Pfizer, a US company, has led in developing a coronavirus vaccine, claiming that patients who received both vaccinations were less likely to acquire COVID-19. This is contrary to common perception, as all vaccinations rely on the development of antibodies produced by a non-harmful viral component. Pfizer's proposal is an mRNA vaccine, which has already been tested and successfully protected people from COVID-19. Moderna is another mRNA vaccine that produces antibodies using a fragment of the coronavirus genome. Protein-based vaccines, like Novavax and a partnership between Sanofi and GlaxoSmithKline, require injecting directly into the coronavirus surface in the circulation. The modified virus used in COVID-19 viral vector vaccines is safe, providing crucial instructions to cells on how to identify and combat the virus. According to a presentation given at a Senate hearing on September 9, 2020, by the National Institutes of Health, three types of coronavirus vaccines are currently developed (Figure 8).
5.1. mRNA Vaccine: A New Possibility
RNA vaccines are the first coronavirus vaccines to enter the market, using a tiny portion of the coronavirus messenger RNA (mRNA) genome to create a spike protein. This spike protein helps the virus attach to and enter cells, and antibodies to neutralize it develop in infected individuals. RNA vaccinations generate the spike protein when mRNA enters cells encased in a lipid molecule and transmits a coded message. Advantages of RNA vaccines include activating killer T-cells, inhibiting coronavirus replication, and being produced in test tubes or tanks. However, they are also inconvenient to carry and store, as they require a deep freezer or dry ice vaccine at -94 degrees Fahrenheit at vaccination sites. Early clinical data on RNA vaccines are just beginning to emerge before the pandemic.
5.2. Protein-based Vaccine: The Slower, Traditional Method
Scientists are developing synthetic spike protein vaccines for the coronavirus, similar to the hepatitis B vaccine developed in the 1980s. Novax and Sanofi-GSK produce these vaccines, grown in insect cells using a baculovirus vector. The protein is filtered before injection into the bloodstream, but is longer than competitors. Phase three tests for these protein-based vaccines have not yet started in the US. Sanofi-GSK will start its trial in December, while Sanofi-Genzyme plans to start its Warp-backed study in November. The vaccines require a chemical agent to stimulate immune response, causing pain or swelling at the injection site. However, they can be stored at room temperature, making them more affordable than competitors.
5.3. Viral Vector Vaccine: The Powerful Immune Response
Vector vaccines use an adenovirus, a virus that causes the common cold, as a middleman instead of injecting the spike protein directly into the body. The adenovirus is connected to the spike protein gene, which distributes the gene throughout the body. The spike protein is released, prompting the immune system to produce antibodies to neutralize it. This technique was first used in the 1980s, but only Sanofi's Dengue vaccine has been approved for human use. Vector vaccines induce a robust immune response without an adjuvant, but designers must balance eliciting an immune response and preventing aggressive inflammation. However, this method cannot be natural, as people exposed to the adenovirus already need to fight it before the spike protein gene can be made. AstraZeneca and Johnson & Johnson, two leading developers of coronavirus vector vaccines, have delayed their studies in the United States until this autumn to investigate participant diseases. AstraZeneca's vaccine requires two doses, while Johnson & Johnson is only looking into a single injection.
6. The Rational Approach to develop a SARS-CoV-2 Vaccine
Rational vaccine design techniques could be employed to direct the immune response towards protective epitopes on the S protein if current methods are insufficient. This approach could lead to longer-lasting vaccination protection and reduce the generation of non- or weakly-neutralizing antibodies. One strategy could be to immunize only with the receptor binding domain (RBD), as most anti-CoV nAbs target the RBD. This method has been initially successful in inducing nAbs in an animal model, as demonstrated by Quinlan et al. (2020) [41].
Reverse vaccinology 2.0 involves developing vaccine antigens by investigating the interactions between powerful non-immune antibodies (nAbs) and their target epitopes [42]. However, producing powerful nAbs from naturally infected donors has historically been a challenge. Researchers have used screening many donors to find those with the strongest neutralizing serum responses and high-throughput single B cell technologies to deep mine memory B cell repertoires specific to antigens [43]. These methods have produced highly effective and occasionally widely cross-reactive nAbs against a wide range of viral infections over the last 10 years [44]. Preliminary data suggests that the isolation of powerful neutralizing antibodies against SARS-CoV-2 may not be as challenging as it has been for other viruses.
Structural studies of panels of potent nAbs in complex with full-length or sub-domains of S are necessary to create immunogens that present neutralizing epitopes to the immune system. Antigen engineering techniques, such as germline targeting, epitope-based protein scaffolds, and structure-guided stabilization of full-length envelope proteins, have been used to concentrate the antibody response on protective epitopes. The stabilized MERS S protein was initially applied to the RSV F protein, producing higher titers of neutralizing antibodies than wild-type S [45]. Immunogenicity studies will reveal the effectiveness of this molecule in inducing nAbs to SARS-CoV-2 [46]. Studies of how nAbs and non-neutralizing Abs (nnAbs) bind to the immunogen can reveal potential design flaws if nAbs are not elevated in most vaccine recipients. To decrease the immunogenicity of undesirable epitopes, various immunogen design techniques can be used. For example, a stabilized E-dimer-based subunit vaccine against the Zika virus was developed to prevent the induction of antibodies against the immunodominant fusion loop and precursor membrane protein [47]. Mice immunized with this stabilized Zika E antigen developed protective antibodies that did not cause an ADE from a DENV infection or cross-react with DENV. The possibility of ADE occurring in the SARS-CoV-2 vaccine is debated, but it is suggested that precise immunogen design is appropriate. Glycan masking has also been successful in reducing antibody responses to undesirable epitopes.
Conventional SARS-CoV-2 vaccinations may cause short-lived nAb responses, which is concerning as many people exposed to SARS and MERS do not produce long-lasting nAb responses [48,49]. New information suggests that SARS-CoV-2 may not exhibit short-lived nAb responses, as seen in MERS [48,49]. To improve the immunogenicity of HIV, methods such as "slow delivery" immunization, which increases the antigen dose gradually over days to weeks, have been investigated. This mode of immunogen delivery results in longer antigen retention in lymph nodes and higher germinal center B cells [50]. Slow delivery immunization also improves nAb development in non-neutralizing epitopes in HIV immunization by modifying the immunodominance of non-neutralizing epitopes [51]. Site-specific immobilization of HIV trimer antigens on alum prolongs immunogen bioavailability, resulting in enhanced germinal center and nAb responses [52]. The creation of strong adjuvants like GSK's AS01B can significantly improve antibody responses to glycoproteins.
Rational Vaccine Design (RVD), combined with Machine Learning (ML) and non-random extensive data samples, can provide a guide for vaccine design in wet labs. This method saves time and helps choose the best candidates for CoV-2 infection prevention. Combining RVD with computational approaches can be a useful tool for designing CoV-2 infection and spreading prevention, accelerating vaccine production, and promoting better outcomes (Figure 9).
7. A Rational Approach to Pan-coronavirus Vaccines
The future of coronaviruses is likely to follow the pattern of SARS and MERS, with other pathogens like West Nile, Zika, and flaviviruses also expected to emerge. Ebola Bundibungyo emerged after Ebola Zaire and Ebola Sudan, while Hantaviruses like Puumala and Seoul were well-known in Eurasia. The mutation of pathogens further suggests that many of the COVID-19 countermeasures currently being considered as band-aid solutions may be a potential solution to the chronic issue.
Pan-pathogen vaccines are a promising approach to protect against both current and future pathogens [53]. The discovery of broadly neutralizing antibodies (bnAbs) has shown that even against significant variation, antibodies can recognize relatively conserved epitopes. This is due to the ability of antibodies to detect every nook and cranny of a pathogen surface, even in a minority of people. Early data supports the development of a potent mAb that cross-neutralizes SARS-CoV-2 and SARS-CoV-1, with the receptor binding domain (RBD) of the two viruses being bound by the cross-reactive nAb [54]. Pan-betacoronavirus vaccine development is likely to be more challenging due to the high conserved and accessible fusion peptide of MERS-CoV and SARS-CoV-2, which is highly conserved and accessible. Overall, pan-pathogen vaccines offer a promising solution for future vaccine development [55].
A pan-coronavirus vaccine that produces cross-reactive antibodies may be more potent against variations of the same virus than strain-specific antibodies. These antibodies target a restricted set of critical conserved residues, exhibiting less propensity for mutation. Antibodies targeting a more compact conserved footprint within the functional binding site may achieve this feature. However, there is concern that a new virus affecting millions of people worldwide will produce variants that require a vaccine that induces antibodies with a certain degree of flexibility in their specific recognition properties.
Antibodies, also known as "super-antibodies," due to their potency and cross-reactivity, are promising agents for viral infection prevention and treatment. Their high potency reduces the high cost of antibodies, requiring less for efficacy. Additionally, antibody half-lives and production and delivery developments can lower costs. Antibodies also have a quicker FDA approval route than vaccines and small-molecule medications, making them a potential first line of defense against infectious disease outbreaks in the future.
8. Machine Learning Approaches
8.1. Introduction
The COVID-19 pandemic has become the world's leading cause of death, and predictions of time series have gained significant attention in the literature [54]. Contemporary methods, such as the Autoregressive Integrated Average (ARIMA) hybrid model and deep belief networks (DBN), have been used for local time forecasting issues [55]. CNN and LSTM are used for traffic flow forecasting [56].
Machine learning techniques, particularly in time series issues, have been employed in prediction systems. The Auto-Regressive Integrated Moving Average (ARIMA) method is widely used for forecasting consecutive temporal issues [57], containing self-expression, a moving component, and a different term. Advanced learning algorithms (DL) have been recently used for time-series predictions [58]. Long short-term memory (LSTM) [59] is a repetitive neural network that generates three gates parallel between successive inputs to control the relationship between previous input, current input, and output.
CNN variants [60] are commonly used in image and video classification, but CNN filters that collect neighboring records via an optional window have gained attention in local time-series predictors. The ANN model [61] is a simple DL algorithm approach that extracts non-linear data relationships using activation functions between all two layers. Although ANN does not use sets of nearby records or prior values like CNN or LSTM, it delivers reasonable results.
8.2. Machine Learning Algorithms to Combat COVID-19
Effective SARS-CoV-2 screening can reduce healthcare system impact by enabling prompt and accurate identification of COVID-19. Prediction models have been developed to aid healthcare professionals in prioritizing patients, especially in scarce healthcare resources, thereby reducing infection risk. Here, we summarized (Table 2) various machine learning (ML) techniques already used by researchers to predict COVID-19.
8.3. Machine Learning Approaches for COVID-19 Forecast
Researchers from MIT's CSAIL have developed two machine learning tools, OptiVax and EvalVax, to predict the number of people who will benefit from vaccines in the future, as effective vaccinations may not produce immunity for large populations due to individual responses [95].
OptiVax uses 11 pre-existing programs to test peptide and surface cell receptor combinations, identifying the best peptides for the surface cell receptor trench. The program classifies appropriate peptides from 155,000 samples and uses a beam scan tool, a common feature in natural language programs (NLP), to select the best set of peptides.
EvalVax is a technology that uses population data from thousands of people to identify individuals with specific allele patterns and genetic variants of the surface cell receptor that function with specific peptide clusters. It predicts vaccine coverage and allows others to evaluate different vaccine formulations. OptiVax focuses on finding all possible peptide fragments from viral or tumor proteins that could be used as vaccine candidates. However, obtaining accurate data on genetic composition was a challenge.
MIT and other companies are utilizing artificial intelligence and machine learning to identify and screen existing vaccines and medicines for COVID-19 treatment (Table 3) [96].
TCS Innovation Lab scientists in India have identified 31 molecular components from 1450 molecules that could be potential COVID-19 vaccines [97]. Benevolent AI developed a COVID-19 drug using AI-based discovery [98]. UK-based Exscientia and Diamond Light Source collaborated to identify compounds against COVID-19 using their 15000 clinically ready molecules [99]. Hong Kong-based Insilco Medicine published 97 candidate epitopes for antigen production (Table 3) [100].

Table 3.
Machine Learning Approaches for COVID-19 Forecast.
| Organization | Principals | Advantages | Disadvantages |
|---|---|---|---|
| MIT | OptiVax works by looking for all possible peptide fragments from a set of viral or tumor proteins that could be used as vaccine candidates. | This method improves the presentation likelihood of a diverse group of vaccine peptides based on the HLA haplotype distribution of a target human population and predicted epitope drift. | Getting excellent data on how people differ in their genetic composition, particularly in important genes that affect the response to a vaccine or viral infection, was one of the hurdles. |
| EvalVax is a complimentary technology they created that predicts vaccine coverage and allows others to evaluate different vaccine formulations. | |||
| TCS | For the de novo design of small compounds capable of blocking the 3CL protease, they used deep neural network-based generative and predictive models. The small compounds that were created were filtered and screened against the binding site of SARS-3CL CoV-2's protease structure. | They identified 31 possible compounds as good candidates for further production and testing against SARS-CoV-2 based on the screening results and additional research. | This was done to make the challenge resemble the class of natural language processing (NLP) problems for which sophisticated AI models and architectures have been built throughout time. |
| Benevolent AI | Rather than focusing primarily on medications that could directly affect the virus, they investigated strategies to stop the virus from infecting human cells through biological processes. | Find approved medications that could potentially stop COVID-19 from progressing, suppress the "cytokine storm," and minimize the inflammatory damage caused by the disease. | Takes 1.5 hours to process. |
| UK-based company Exscientia and Diamond Light Source and Calibr, a division of Scripps Research, US | Applied improved biosensor platforms to screen the collection of 15,000 clinically ready molecules. | The first objective is to find any current medications that can be repurposed to protect humans. | Discovering potential prospects among the currently available medications is difficult and time-consuming. |
| Insilco Medicine, a Hong Kong-based pharmaceutical research company | The seven promising compounds against COVID-19 were discovered, and two of them have already been synthesized for testing. | Used Virtual Reality to Fine-Tune New AI-Generated COVID-19 Drugs | Synthesis and validation could take a long time and cost a lot of money. |
9. Reverse Vaccinology Approach
Reverse vaccinology is a bioinformatic method that screens entire pathogen genomes to identify genes associated with good epitopes, which are peptides in antigens that antibodies form bindings with [101]. This technique is time and cost-efficient, reducing the number of proteins studied and allowing research of risky microorganisms [102]. After obtaining the genome sequence from multiple databases, it is crucial to identify all possible proteins using software packages [103,104]. This helps determine physicochemical properties to identify suitable antigens or vaccine candidates, leading to vaccine design. A detailed diagram will make the internal process of reverse vaccinology clear below (Figure 10).
Currently, several research groups are working on a potential COVID-19 vaccine using the reverse vaccinology technique. The following table describes the summarized overview of each research (Table 4).
Reverse Vaccinology with Machine Learning Approach
Researchers have used machine learning and artificial intelligence to design the COVID-19 vaccine, demonstrating the potential of reverse vaccination for faster and more accurate antigen prediction [115].
Table 5.
Overview of the recent reverse vaccinology approach combined with the Machine Learning approach to get the COVID-19 vaccine.
Table 5.
Overview of the recent reverse vaccinology approach combined with the Machine Learning approach to get the COVID-19 vaccine.
| Research Group | Database | Target Proteins | B-cell and T-cell Epitope Prediction |
Antigenicity and Allergenicity test | Molecular Docking | Immunogenicity Evaluation |
Energy Minimization and Binding Affinity Prediction | In Silico Cloning and Codon Optimization | ML Approach |
|---|---|---|---|---|---|---|---|---|---|
| Ong et al.[116] | NCBI | S, E, M, N proteins | ✔ | ✔ | ● | ✔ | ● | ● | Vaxign-ML protegenicity (protective antigenicity) score calculation |
The analysis of SARS-CoV-2's proteome revealed six adhesins, including the S protein and five non-structural proteins (nsp3, 3CL-pro, np8-10), crucial for viral adhesion and host invasion, and predicted by Vaxign-ML to induce high protective antigenicity.
10. RNA Vaccine Design
mRNA vaccines are a new type of vaccine platform that uses messenger RNA to instruct cells to produce a protein that triggers an immune response [117]. These vaccines work by delivering mRNA molecules into cells for the expression of a gene of interest, which in turn produces the antigen [117]. Three types of host cells can be transfected after administration: non-immune cells, immune cells found in tissues at the injection site, and immune cells in peripheral lymphoid organs [118].
MRNA vaccines are encapsulated in lipid nanoparticles (LNPs) to enter the target cell, as they are negatively charged and unstable [118]. The vaccine provides cells with a blueprint to construct the protein of the pathogen being studied [119], unlike traditional vaccines that contain a weakened or inactive pathogen to trigger an immune response. mRNA vaccines do not require actual exposure to the pathogen to mount an immune response, and the immune response elicits the production of antibodies that allow the body to develop immunity against the specific pathogen [119].
mRNA vaccines contain the coding region of S protein flanked by optimized 5'- and 3'-UTRs and polyA tail [117]. The mRNA molecules are modified with cap1 structure, pseudouridine substitution, preferred human codon usage, optimized UTR and polyA tail sequence to increase RNA stability and translation efficiency [117].
mRNA vaccines are synthesized via IVT and encapsulated with LNP for intramuscular injection (IM injection) [117]. They are delivered into muscle cells or antigen-presenting cells via endocytosis [117], with translation taking place in the cytoplasm rather than the nucleus. mRNA is a safer vector than DNA because it carries a short sequence to be translated, is a transient molecule, and does not interact with the host genome [117].
11.1. Effectiveness of mRNA vaccines in preventing COVID-19
mRNA vaccines have been found to be highly effective in preventing COVID-19 [117], with clinical trials confirming their high efficacy [117]. These vaccines are crucial for achieving herd immunity and decreasing future surges of COVID-19 infections [119]. Early data suggests a reduction in the number of infected individuals, and the safety data of mRNA vaccines against COVID-19 are reassuring [120]. Encapsulated mRNA in lipid nanoparticles facilitate mRNA uptake and endocellular penetration, protecting against degradation. mRNA vaccines can induce antibody and cell-mediated immune responses and have demonstrated efficacy in preventing COVID-19 [120].
The ongoing COVID-19 pandemic highlights the urgent need for safe and effective vaccines [121], and mRNA vaccine technology has the most promising application prospects for COVID-19 [118,122]. mRNA vaccines, including Pfizer-BioNTech and Moderna, were the fastest vaccine development in medical history. Pfizer-BioNTech was the first COVID-19 vaccine approved for commercialization by the FDA and for use in children aged 5-11 [118].
Previous vaccination with a 2-dose mRNA vaccine has been associated with hospitalization for COVID-19, suggesting that mRNA vaccines may be effective in preventing severe COVID-19 that requires hospitalization. Two mRNA vaccines against COVID-19 have completed late-stage clinical assessment at an unprecedented speed and reported positive results [122].
11.2. Reported Side Effects of mRNA Vaccines
The mRNA vaccines have been reported to have mild to moderate side effects, usually localized to the injection site and resolving quickly. Symptoms usually arise within 24 hours of vaccination and resolve quickly [119]. Common side effects include chills, headache, injection site pain, fatigue, and myalgias, especially among those over 55 years old. A higher incidence of local and systemic reactions was reported following the second vaccine dose [119]. Only two systemic adverse events were classified as severe. Of the 71 adverse events reported, 17 were associated with the vaccine [119]. However, no serious side effects have been identified in the ongoing phase 3 clinical trials for both the Moderna and Pfzier/BioNTech mRNA vaccines [119]. Other systemic side effects, such as fatigue, fever, headache, myalgias, and arthralgias, occur more frequently with the vaccine than with the placebo, with most occurring within 1 to 2 days following vaccination [119]. Hypersensitivity adverse side effects were equivalent in both the placebo and vaccine groups. Mild local side effects, such as heat, pain, redness, and swelling, are more common with the vaccines than with the placebo [119].
11. Conclusions and Future Directions
The development of a rational vaccine for SARS-CoV-2 is a complex task due to various factors. The need for different vaccine types for different populations, such as infants, children, pregnant women, and immunocompromised individuals [123], and the need for post-marketing surveillance to record adverse events. Most vaccines target the healthy population, 18-55 years old adults, making a safe regulatory pathway necessary. DNA-based vaccines generate high titer of neutralizing antibodies when given with an inactivated vaccine but can cause adverse events (ADE) when used alone. DNA-based vaccines are unproven in practice, while RNA vaccines have the potential to induce ADE [123]. Limited information on antibodies targeting the S2 subunit of the spike protein poses challenges in developing a rational vaccine for SARS-CoV-2. Antibody-dependent enhancement (ADE) can worsen disease after the second infection with other serotypes due to pre-existing vaccine-elicited antibodies with low or no cross-neutralizing activity. Optimizing animal models and further investigating ADE risk about SARS-CoV-2 are necessary. The conformational shift induced by the D614G mutation could influence the effectivity of some NAbs, making it challenging to develop a rational vaccine [123].
12.1. Potential Drawbacks of Rational Vaccines for SARS-CoV-2
The development of rational vaccines for SARS-CoV-2 is promising, but there are potential drawbacks [123]. The effectiveness of vaccines varies across age groups, with older individuals showing lower efficacy compared to younger adults. Low-dose vaccines may be necessary for children due to increased reactogenicity. Fast-tracking vaccine development can lead to incomplete or limited data, resulting in ineffective vaccines or adverse events [123]. Building trust in public health systems through transparency and accurate reporting is crucial. The risk of vaccine-associated enhanced respiratory disease (VAERD) and ADE must also be considered. High viral loads may lead to VAERD, while inactivated vaccine candidates pose a risk of ADE [123]. ADE has been reported in other coronaviruses and could be a risk for CVCs. State-sponsored vaccine candidates in Russia and China may also have limited data. Therefore, careful consideration of these potential drawbacks is necessary when developing rational vaccines for SARS-CoV-2 [123].
12.2. The ways to address challenges and drawbacks in the development and distribution of a rational vaccine for SARS-CoV-2
The development and distribution of a rational vaccine for SARS-CoV-2 is crucial in the fight against COVID-19. However, there are several challenges and drawbacks associated with vaccine design. One major challenge is the potential development of resistance to RBD-targeting NAbs due to naturally occurring mutations of SARS-CoV-2 [124]. Cocktail antibodies targeting two independent epitopes of RBD can neutralize mutated variants and reduce the emergence of resistance strains compared to single mAb treatment [124]. Combination treatment of two or more NAbs targeting distinct epitopes is an effective means to suppress escape variants [124].
Another challenge is the long-term clinical trials and uncertainty of vaccine efficacy in humans [124]. Information collected about the immune responses in COVID-19 patients can aid in the development of a rational vaccine. Developing SARS-CoV-2 NAbs that target the trimeric spike (S) glycoproteins and have the capacity to elicit high levels of neutralizing antibodies is a part of the strategy for the treatment of COVID-19 [124].
Currently, there are no approved vaccines or specific therapeutics against COVID-19, but monoclonal antibodies and polyclonal antibodies have been reported under different states of clinical trials. Cocktail antibodies are considered a superior therapy against SARS-CoV-2 in preclinical studies [124]. The progress of clinical trials for specific antibodies, such as LY-CoV555 and NAb CB6, provides hope for the development of an effective treatment for COVID-19 [124].
Author Contributions
Aritra Ghosh collected the data and wrote the manuscript. Dr. Mirjana Pavlovic helped with some key references and information. All authors read and approved the final manuscript..
Funding
Not applicable.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is available upon request.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare that they have no competing interests.
References
- J. Boonyaratanakornkit and J. J. Taylor, “Techniques to Study Antigen-Specific B Cell Responses,” Frontiers in immunology. 2019. [CrossRef]
- J. L. Sanchez-Trincado, M. Gomez-Perosanz, and P. A. Reche, “Fundamentals and Methods for T- and B-Cell Epitope Prediction,” Journal of Immunology Research. 2017. [CrossRef]
- P. Forterre, “Defining Life: The Virus Viewpoint,” Orig. Life Evol. Biosph., 2010. [CrossRef]
- A. W. H. Chin et al., “Stability of SARS-CoV-2 in different environmental conditions,” The Lancet Microbe, 2020. [CrossRef]
- C. Arnold, “How computational immunology changed the face of COVID-19 vaccine development,” Nat. Med., Jul. 2020. [CrossRef]
- R. R. María, C. J. Arturo, J. A. Alicia, M. G. Paulina, and A. O. Gerardo, “The Impact of Bioinformatics on Vaccine Design and Development,” in Vaccines, 2017.
- V. C. C. Cheng, S. K. P. Lau, P. C. Y. Woo, and Y. Y. Kwok, “Severe acute respiratory syndrome coronavirus as an agent of emerging and reemerging infection,” Clinical Microbiology Reviews. 2007. [CrossRef]
- J. Cui, F. Li, and Z. L. Shi, “Origin and evolution of pathogenic coronaviruses,” Nature Reviews Microbiology. 2019. [CrossRef]
- M. A. Shereen, S. Khan, A. Kazmi, N. Bashir, and R. Siddique, “COVID-19 infection: Origin, transmission, and characteristics of human coronaviruses,” Journal of Advanced Research. 2020. [CrossRef]
- M. Cascella, M. Rajnik, A. Cuomo, S. C. Dulebohn, and R. Di Napoli, Features, Evaluation and Treatment Coronavirus (COVID-19). 2020.
- I. Alam et al., “CovMT: an interactive SARS-CoV-2 mutation tracker, with a focus on critical variants,” The Lancet Infectious Diseases. 2021. [CrossRef]
- M. Moradi, R. Golmohammadi, A. Najafi, M. Moosazadeh Moghaddam, M. Fasihi-Ramandi, and R. Mirnejad, “A contemporary review on the important role of in silico approaches for managing different aspects of COVID-19 crisis,” Informatics in Medicine Unlocked. 2022. [CrossRef]
- Mani, S. Viruses, Vaccines and the Race for a Covid-19 Vaccine: A Tutorial. (n.d.) Retrieved October 24, 2023, from www.preprints.org/manuscript/202009.0153.
- Koch, T., Fathi, A., Addo, M. The COVID-19 Vaccine Landscape. (n.d.) Retrieved October 24, 2023, from link.springer.com/chapter/10.1007/978-3-030-63761-3_31. [CrossRef]
- Smitha, T., Thomas, A. A brief outlook on the current emerging trends of COVID 19 vaccines. (n.d.) Retrieved October 24, 2023, from www.ncbi.nlm.nih.gov/pmc/articles/PMC7802844/.
- Few, M. Epidemics, indigenous communities, and public health in the COVID-19 era: views from smallpox inoculation campaigns in colonial Guatemala. (n.d.) Retrieved October 24, 2023, from www.cambridge.org.
- Saleh A, Qamar S, Tekin A, et al. (July 26, 2021) Vaccine Development Throughout History. Cureus 13(7): e16635. [CrossRef]
- C. Rueckert and C. A. Guzmán, “Vaccines: From Empirical Development to Rational Design,” PLoS Pathogens, vol. 8, no. 11, p. e1003001, Nov. 2012. [CrossRef]
- K. G. Andersen, A. Rambaut, W. I. Lipkin, E. C. Holmes, and R. F. Garry, “The proximal origin of SARS-CoV-2,” Nature Medicine. 2020. [CrossRef]
- S. Belouzard, J. K. Millet, B. N. Licitra, and G. R. Whittaker, “Mechanisms of coronavirus cell entry mediated by the viral spike protein.,” Viruses. 2012. [CrossRef]
- A. T. Ton, F. Gentile, M. Hsing, F. Ban, and A. Cherkasov, “Rapid Identification of Potential Inhibitors of SARS-CoV-2 Main Protease by Deep Docking of 1.3 Billion Compounds,” Mol. Inform., 2020. [CrossRef]
- L. Zhang et al., “Crystal structure of SARS-CoV-2 main protease provides a basis for design of improved a-ketoamide inhibitors,” Science (80-. )., 2020. [CrossRef]
- A. Shamsi et al., “Glecaprevir and Maraviroc are high-affinity inhibitors of SARS-CoV-2 main protease: Possible implication in COVID-19 therapy,” Biosci. Rep., 2020. [CrossRef]
- R. L. Graham, J. S. Sparks, L. D. Eckerle, A. C. Sims, and M. R. Denison, “SARS coronavirus replicase proteins in pathogenesis,” Virus Res., 2008. [CrossRef]
- A. A. T. Naqvi et al., “Insights into SARS-CoV-2 genome, structure, evolution, pathogenesis and therapies: Structural genomics approach,” Biochimica et Biophysica Acta - Molecular Basis of Disease. 2020. [CrossRef]
- J. Shang et al., “Structural basis of receptor recognition by SARS-CoV-2,” Nature, 2020. [CrossRef]
- D. Wrapp et al., “Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation,” Science (80-. )., 2020. [CrossRef]
- T. Suzuki, Y. Otake, S. Uchimoto, A. Hasebe, and Y. Goto, “Genomic characterization and phylogenetic classification of bovine coronaviruses through whole genome sequence analysis,” Viruses, 2020. [CrossRef]
- H. Higuchi, S. F. Bronk, A. Bateman, K. Harrington, R. G. Vile, and G. J. Gores, “Viral fusogenic membrane glycoprotein expression causes syncytia formation with bioenergetic cell death: Implications for gene therapy,” Cancer Res., 2000.
- B. Alberts, A. Johnson, J. Lewis, K. Raff, Martin Roberts, and P. Walter, “Transport from the ER through the Golgi Apparatus,” Mol. Biol. Cell, 2002.
- J. S. Morse, T. Lalonde, S. Xu, and W. R. Liu, “Learning from the Past: Possible Urgent Prevention and Treatment Options for Severe Acute Respiratory Infections Caused by 2019-nCoV,” ChemBioChem, 2020. [CrossRef]
- H. Iqbal, “The importance of cell-mediated immunity in COVID-19 – An opinion,” Medical Hypotheses. 2020. [CrossRef]
- N. C. Kyriakidis, A. López-Cortés, E. V. González, A. B. Grimaldos, and E. O. Prado, “SARS-CoV-2 vaccines strategies: a comprehensive review of phase 3 candidates,” npj Vaccines. 2021. [CrossRef]
- D. R. Burton and L. M. Walker, “Rational Vaccine Design in the Time of COVID-19,” Cell Host Microbe, 2020. [CrossRef]
- F. X. Heinz and K. Stiasny, “Distinguishing features of current COVID-19 vaccines: knowns and unknowns of antigen presentation and modes of action,” npj Vaccines. 2021. [CrossRef]
- T. Thanh Le et al., “The COVID-19 vaccine development landscape,” Nature reviews. Drug discovery. 2020. [CrossRef]
- T. T. Le, J. P. Cramer, R. Chen, and S. Mayhew, “Evolution of the COVID-19 vaccine development landscape,” Nature reviews. Drug discovery. 2020. [CrossRef]
- World Health Organization (WHO)., “COVID-19 - Landscape of novel coronavirus candidate vaccine development worldwide,” Who, 2020.
- World Health Organization, “COVID-19 vaccine tracker and landscape,” Who. 2021.
- [41] Quinlan et al., 2020 B.D. Quinlan, H. Mou, L. Zhang, Y. Guo, W. He, A. Ojha, M.S. Parcells, G. Luo, W. Li, G. Zhong, et al. The SARS-CoV-2 receptor-binding domain elicits a potent neutralizing response without antibody-dependent enhancement bioRxiv (2020). [CrossRef]
- D.R. Burton What Are the Most Powerful Immunogen Design Vaccine Strategies? Reverse Vaccinology 2.0 Shows Great Promise Cold Spring Harb. Perspect. Biol., 9 (2017), p. 030262.
- L.M. Walker, D.R. Burton Passive immunotherapy of viral infections: ‘super-antibodies’ enter the fray Nat. Rev. Immunol., 18 (2018), pp. 297-308. [CrossRef]
- D. Corti, A. Lanzavecchia Broadly neutralizing antiviral antibodies Annu. Rev. Immunol., 31 (2013), pp. 705-742. [CrossRef]
- J. Pallesen, N. Wang, K.S. Corbett, D. Wrapp, R.N. Kirchdoerfer, H.L. Turner, C.A. Cottrell, M.M. Becker, L. Wang, W. Shi, et al. Immunogenicity and structures of a rationally designed prefusion MERS-CoV spike antigen Proc. Natl. Acad. Sci. USA, 114 (2017), pp. E7348-E7357. [CrossRef]
- D. Wrapp, N. Wang, K.S. Corbett, J.A. Goldsmith, C.L. Hsieh, O. Abiona, B.S. Graham, J.S. McLellan Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation Science, 367 (2020), pp. 1260-1263. [CrossRef]
- J.L. Slon-Campos, W. Dejnirattisai, B.W. Jagger, C. López-Camacho, W. Wongwiwat, L.A. Durnell, E.S. Winkler, R.E. Chen, A. Reyes Sandoval, F.A. Rey, et al. A protective Zika virus E-dimer-based subunit vaccine engineered to abrogate antibody-dependent enhancement of dengue infection Nat. Immunol., 20 (2019), pp. 1291-1298. [CrossRef]
- P.G. Choe, R.A.P.M. Perera, W.B. Park, K.H. Song, J.H. Bang, E.S. Kim, H.B. Kim, L.W.R. Ko, S.W. Park, N.J. Kim, et al. MERS-CoV Antibody Responses 1 Year after Symptom Onset, South Korea, 2015 Emerg. Infect. Dis., 23 (2017), pp. 1079-1084. [CrossRef]
- L.P. Wu, N.C. Wang, Y.H. Chang, X.Y. Tian, D.Y. Na, L.Y. Zhang, L. Zheng, T. Lan, L.F. Wang, G.D. Liang Duration of antibody responses after severe acute respiratory syndrome Emerg. Infect. Dis., 13 (2007), pp. 1562-1564. [CrossRef]
- H.H. Tam, M.B. Melo, M. Kang, J.M. Pelet, V.M. Ruda, M.H. Foley, J.K. Hu, S. Kumari, J. Crampton, A.D. Baldeon, et al. Sustained antigen availability during germinal center initiation enhances antibody responses to vaccination Proc. Natl. Acad. Sci. U S A, 113 (2016), pp. E6639-E6648. [CrossRef]
- K.M. Cirelli, D.G. Carnathan, B. Nogal, J.T. Martin, O.L. Rodriguez, A.A. Upadhyay, C.A. Enemuo, E.H. Gebru, Y. Choe, F. Viviano, et al. Slow delivery immunization enhances HIV neutralizing antibody and germinal center responses via modulation of immunodominance Cell, 177 (2019), pp. 1153-1171.e1128. [CrossRef]
- T.J. Moyer, Y. Kato, W. Abraham, J.Y.H. Chang, D.W. Kulp, N. Watson, H.L. Turner, S. Menis, R.K. Abbott, J.N. Bhiman, et al. Engineered immunogen binding to alum adjuvant enhances humoral immunity Nat. Med., 26 (2020), pp. 430-440. [CrossRef]
- L.M. Walker, D.R. Burton Passive immunotherapy of viral infections: ‘super-antibodies’ enter the fray Nat. Rev. Immunol., 18 (2018), pp. 297-308. [CrossRef]
- D. Pinto, Y.J. Park, M. Beltramello, A.C. Walls, M.A. Tortorici, S. Bianchi, S. Jaconi, K. Culap, F. Zatta, A. De Marco, et al. Structural and functional analysis of a potent sarbecovirus neutralizing antibody bioRxiv (2020). [CrossRef]
- A.C. Walls, M.A. Tortorici, B.J. Bosch, B. Frenz, P.J.M. Rottier, F. DiMaio, F.A. Rey, D. Veesler Cryo-electron microscopy structure of a coronavirus spike glycoprotein trimer Nature, 531 (2016), pp. 114-117. [CrossRef]
- G. Mahalakshmi, S. Sridevi, and S. Rajaram, “A survey on forecasting of time series data,” 2016. [CrossRef]
- M. Qin, Z. Li, and Z. Du, “Red tide time series forecasting by combining ARIMA and deep belief network,” Knowledge-Based Syst., 2017. [CrossRef]
- Z. Zhao, W. Chen, X. Wu, P. C. V. Chen, and J. Liu, “LSTM network: A deep learning approach for short-term traffic forecast,” IET Image Process., 2017. [CrossRef]
- E. M. de Oliveira and F. L. Cyrino Oliveira, “Forecasting mid-long term electric energy consumption through bagging ARIMA and exponential smoothing methods,” Energy, 2018. [CrossRef]
- M. Längkvist, L. Karlsson, and A. Loutfi, “A review of unsupervised feature learning and deep learning for time-series modeling,” Pattern Recognit. Lett., 2014. [CrossRef]
- F. A. Gers, J. Schmidhuber, and F. Cummins, “Learning to forget: Continual prediction with LSTM,” Neural Comput., 2000. [CrossRef]
- K. Fukushima, “Neocognitron: A self-organizing neural network model for a mechanism of pattern recognition unaffected by shift in position,” Biol. Cybern., 1980. [CrossRef]
- X. Yao, “Evolving artificial neural networks,” Proc. IEEE, 1999. [CrossRef]
- N. L. W. S. R. Ginantra, I. G. A. D. Indradewi, and E. Hartono, “Machine learning approach for Acute Respiratory Infections (ISPA) prediction: Case study Indonesia,” 2020. [CrossRef]
- R. Yin, V. H. Tran, X. Zhou, J. Zheng, and C. K. Kwoh, “Predicting antigenic variants of H1N1 influenza virus based on epidemics and pandemics using a stacking model,” PLoS One, 2018. [CrossRef]
- S. B. Cho, “Exploiting machine learning techniques for location recognition and prediction with smartphone logs,” Neurocomputing, 2016. [CrossRef]
- K. Mori, T. Wada, and K. Ohtsuki, “A New Disaster Recognition Algorithm Based on SVM for ERESS: Buffering and Bagging-SVM,” 2016. [CrossRef]
- D. N. Le, V. S. Parvathy, D. Gupta, A. Khanna, J. J. P. C. Rodrigues, and K. Shankar, “IoT enabled depthwise separable convolution neural network with deep support vector machine for COVID-19 diagnosis and classification,” Int. J. Mach. Learn. Cybern., 2021. [CrossRef]
- S. Sadhukhan, S. Banerjee, P. Das, and A. K. Sangaiah, “Producing better disaster management plan in post-disaster situation using social media mining,” in Computational Intelligence for Multimedia Big Data on the Cloud with Engineering Applications, 2018. [CrossRef]
- N. Assery, Y. Xiaohong, S. Almalki, R. Kaushik, and Q. Xiuli, “Comparing learning-based methods for identifying disaster-related tweets,” 2019. [CrossRef]
- F. Mohammadi et al., “Artificial neural network and logistic regression modelling to characterize COVID-19 infected patients in local areas of Iran,” Biomed. J., 2021. [CrossRef]
- Bhandari et al., “Logistic regression analysis to predict mortality risk in COVID-19 patients from routine hematologic parameters,” Ibnosina J. Med. Biomed. Sci., 2020. [CrossRef]
- A. M. Almeshal, A. I. Almazrouee, M. R. Alenizi, and S. N. Alhajeri, “Forecasting the spread of COVID-19 in kuwait using compartmental and logistic regression models,” Appl. Sci., 2020. [CrossRef]
- M. Elhoseny, “Multi-object Detection and Tracking (MODT) Machine Learning Model for Real-Time Video Surveillance Systems,” Circuits, Syst. Signal Process., 2020. [CrossRef]
- Y. Chen and Y. Liu, “Which risk factors matter more for psychological distress during the covid-19 pandemic? An application approach of gradient boosting decision trees,” Int. J. Environ. Res. Public Health, 2021. [CrossRef]
- M. Loey, G. Manogaran, M. H. N. Taha, and N. E. M. Khalifa, “A hybrid deep transfer learning model with machine learning methods for face mask detection in the era of the COVID-19 pandemic,” Meas. J. Int. Meas. Confed., 2021. [CrossRef]
- C. Iwendi et al., “COVID-19 patient health prediction using boosted random forest algorithm,” Front. Public Heal., 2020. [CrossRef]
- C. M. YEŞİLKANAT, “Spatio-temporal estimation of the daily cases of COVID-19 in worldwide using random forest machine learning algorithm,” Chaos, Solitons and Fractals, 2020. [CrossRef]
- L. Luoh, “ZigBee-based intelligent indoor positioning system soft computing,” Soft Comput., 2014. [CrossRef]
- M. Polese, R. Jana, V. Kounev, K. Zhang, S. Deb, and M. Zorzi, “Machine Learning at the Edge: A Data-Driven Architecture with Applications to 5G Cellular Networks,” IEEE Trans. Mob. Comput., 2021. [CrossRef]
- P. Chhikara, R. Tekchandani, N. Kumar, V. Chamola, and M. Guizani, “DCNN-GA: A Deep Neural Net Architecture for Navigation of UAV in Indoor Environment,” IEEE Internet Things J., 2021. [CrossRef]
- S. More et al., “Security Assured CNN-Based Model for Reconstruction of Medical Images on the Internet of Healthcare Things,” IEEE Access, 2020. [CrossRef]
- S. Rath, A. Tripathy, and A. R. Tripathy, “Prediction of new active cases of coronavirus disease (COVID-19) pandemic using multiple linear regression model,” Diabetes Metab. Syndr. Clin. Res. Rev., 2020. [CrossRef]
- R. O. Ogundokun, A. F. Lukman, G. B. M. Kibria, J. B. Awotunde, and B. B. Aladeitan, “Predictive modelling of COVID-19 confirmed cases in Nigeria,” Infect. Dis. Model., 2020. [CrossRef]
- R. Gupta, G. Pandey, P. Chaudhary, and S. K. Pal, “Machine Learning Models for Government to Predict COVID-19 Outbreak,” Digit. Gov. Res. Pract., 2020. [CrossRef]
- E. Matthew and O. Adeyinka, “Application of Hierarchical Polynomial Regression Models to Predict Transmission of COVID-19 at Global Level,” Int. J. Clin. Biostat. Biometrics, 2020. [CrossRef]
- M. H. D. M. Ribeiro, R. G. da Silva, V. C. Mariani, and L. dos S. Coelho, “Short-term forecasting COVID-19 cumulative confirmed cases: Perspectives for Brazil,” Chaos, Solitons and Fractals, 2020. [CrossRef]
- M. Saqib, “Forecasting COVID-19 outbreak progression using hybrid polynomial-Bayesian ridge regression model,” Appl. Intell., 2021. [CrossRef]
- S. R. Vadyala, S. N. Betgeri, E. A. Sherer, and A. Amritphale, “Prediction of the number of COVID-19 confirmed cases based on K-means-LSTM,” Array, 2021. [CrossRef]
- T. Zhang and G. Lin, “Generalized k-means in GLMs with applications to the outbreak of COVID-19 in the United States,” Comput. Stat. Data Anal., 2021. [CrossRef]
- Z. R. S. Elsi et al., “Utilization of Data Mining Techniques in National Food Security during the Covid-19 Pandemic in Indonesia,” 2020. [CrossRef]
- A. M. Anter, D. Oliva, A. Thakare, and Z. Zhang, “AFCM-LSMA: New intelligent model based on Lévy slime mould algorithm and adaptive fuzzy C-means for identification of COVID-19 infection from chest X-ray images,” Adv. Eng. Informatics, 2021. [CrossRef]
- K. Chadaga, S. Prabhu, B. K. Vivekananda, S. Niranjana, and S. Umakanth, “Battling COVID-19 using machine learning: A review,” Cogent Engineering. 2021. [CrossRef]
- B. Sahu, P. K. Das, M. R. Kabat, and R. Kumar, “Prevention of Covid-19 affected patient using multi robot cooperation and Q-learning approach: a solution,” Qual. Quant., 2022. [CrossRef]
- L. Miralles-Pechuán, F. Jiménez, H. Ponce, and L. Martínez-Villaseñor, “A Methodology Based on Deep Q-Learning/Genetic Algorithms for Optimizing COVID-19 Pandemic Government Actions,” 2020. [CrossRef]
- W. Zhang et al., “Analysis of COVID-19 epidemic and clinical risk factors of patients under epidemiological Markov model,” Results Phys., 2021. [CrossRef]
- Liu et al., “Computationally Optimized SARS-CoV-2 MHC Class I and II Vaccine Formulations Predicted to Target Human Haplotype Distributions,” Cell Syst., 2020. [CrossRef]
- A. Chandra Kaushik and U. Raj, “AI-driven drug discovery: A boon against COVID-19?,” AI Open, 2020. [CrossRef]
- “COVID-19: Role of Artificial Intelligent in Drug Discovery.” https://www.tcs.com/company-overview/tcs-artificial-intelligence-cure-covid-19 (accessed Nov. 02, 2020).
- “Potential new treatment for COVID-19 uncovered by BenevolentAI enters trials | TechCrunch.” https://techcrunch.com/2020/04/14/potential-new-treatment-for-covid-19-uncovered-by-benevolentai-enters-trials/?guccounter=1 (accessed Nov. 02, 2020).
- “AI technology to screen existing drugs for use against COVID-19.” https://www.drugtargetreview.com/news/59188/ai-technology-to-screen-existing-drugs-for-use-against-covid-19/ (accessed Nov. 02, 2020).
- “AI Speeds Drug Discovery to fight COVID-19 | by Arijit Roy | Towards Data Science.” https://towardsdatascience.com/ai-speeds-drug-discovery-to-fight-covid-19-b853a3f93e82 (accessed Nov. 02, 2020).
- A. Nandy and S. C. Basak, “Bioinformatics in design of antiviral vaccines,” in Encyclopedia of Biomedical Engineering, 2018. [CrossRef]
- R. Rappuoli, “Reverse vaccinology,” Current Opinion in Microbiology. 2000. [CrossRef]
- G. P. Monterrubio-López, J. A. González-Y-Merchand, and R. M. Ribas-Aparicio, “Identification of novel potential vaccine candidates against tuberculosis based on reverse vaccinology,” Biomed Res. Int., 2015. [CrossRef]
- S. Vivona, F. Bernante, and F. Filippini, “NERVE: New Enhanced Reverse Vaccinology Environment,” BMC Biotechnol., 2006. [CrossRef]
- Y. Hisham and Y. Ashhab, “Identification of cross-protective potential antigens against pathogenic brucella spp. through combining pan-genome analysis with reverse vaccinology,” J. Immunol. Res., 2018. [CrossRef]
- M. Tahir Ul Qamar et al., “Reverse vaccinology assisted designing of multiepitope-based subunit vaccine against SARS-CoV-2,” Infect. Dis. Poverty, 2020. [CrossRef]
- H. Z. Chen, L. L. Tang, X. L. Yu, J. Zhou, Y. F. Chang, and X. Wu, “Bioinformatics analysis of epitope-based vaccine design against the novel SARS-CoV-2,” Infect. Dis. Poverty, 2020. [CrossRef]
- M. Bhattacharya et al., “Development of epitope-based peptide vaccine against novel coronavirus 2019 (SARS-COV-2): Immunoinformatics approach,” J. Med. Virol., 2020. [CrossRef]
- A. Rakib et al., “Immunoinformatics-guided design of an epitope-based vaccine against severe acute respiratory syndrome coronavirus 2 spike glycoprotein,” Comput. Biol. Med., 2020. [CrossRef]
- A. Naz, F. Shahid, T. T. Butt, F. M. Awan, A. Ali, and A. Malik, “Designing Multi-Epitope Vaccines to Combat Emerging Coronavirus Disease 2019 (COVID-19) by Employing Immuno-Informatics Approach,” Front. Immunol., 2020. [CrossRef]
- T. Kar et al., “A candidate multi-epitope vaccine against SARS-CoV-2,” Sci. Rep., 2020. [CrossRef]
- B. Robson, “COVID-19 Coronavirus spike protein analysis for synthetic vaccines, a peptidomimetic antagonist, and therapeutic drugs, and analysis of a proposed achilles’ heel conserved region to minimize probability of escape mutations and drug resistance,” Comput. Biol. Med., 2020. [CrossRef]
- M. Enayatkhani et al., “Reverse vaccinology approach to design a novel multi-epitope vaccine candidate against COVID-19: an in silico study,” J. Biomol. Struct. Dyn., 2020. [CrossRef]
- B. Sarkar, M. A. Ullah, F. T. Johora, M. A. Taniya, and Y. Araf, “Immunoinformatics-guided designing of epitope-based subunit vaccines against the SARS Coronavirus-2 (SARS-CoV-2),” Immunobiology, 2020. [CrossRef]
- Park, J., Lagniton, P., Liu, Y. mRNA vaccines for COVID-19: what, why and how. (n.d.) Retrieved October 26, 2023, from www.ncbi.nlm.nih.gov/pmc/articles/PMC8071766/.
- Fang, E., Liu, X., Li, M., Zhang, Z., Song, L., Zhu, B. Advances in COVID-19 mRNA vaccine development. (n.d.) Retrieved October 26, 2023, from www.nature.com/articles/s41392-022-00950-y.
- Anand, P., Stahel, V. The safety of Covid-19 mRNA vaccines: a review. (n.d.) Retrieved October 26, 2023, from pssjournal.biomedcentral.com.
- Vitiello, A., Ferrara, F. Brief review of the mRNA vaccines COVID-19. (n.d.) Retrieved October 26, 2023, from link.springer.com/article/10.1007/s10787-021-00811-0. [CrossRef]
- Tenforde, M., Self, W., Adams, K., Gaglani, M., Ginde, A. Association Between mRNA Vaccination and COVID-19 Hospitalization and Disease Severity. (n.d.) Retrieved October 26, 2023, from jamanetwork.com/journals/jama/article-abstract/2786039.
- Huang, Q., Zeng, J., Yan, J. Review COVID-19 mRNA vaccines. (n.d.) Retrieved October 26, 2023, from www.sciencedirect.com/science/article/pii/S167385272100045X.
- Kashte, S., Gulbake, A., El-Amin III, S., Gupta, A. COVID-19 vaccines: rapid development, implications, challenges and future prospects. (n.d.) Retrieved October 26, 2023, from link.springer.com/article/10.1007/s13577-021-00512-4. [CrossRef]
- Huang, Y., Sun, H., Yu, H., Li, S., Zheng, Q. Neutralizing antibodies against SARS-CoV-2: current understanding, challenge and perspective | Antibody Therapeutics | Oxford Academic. (n.d.) Retrieved October 26, 2023, from academic.oup.com/abt/article-abstract/3/4/285/6053820.
Figure 1.
SARS-COV2 Transmission.
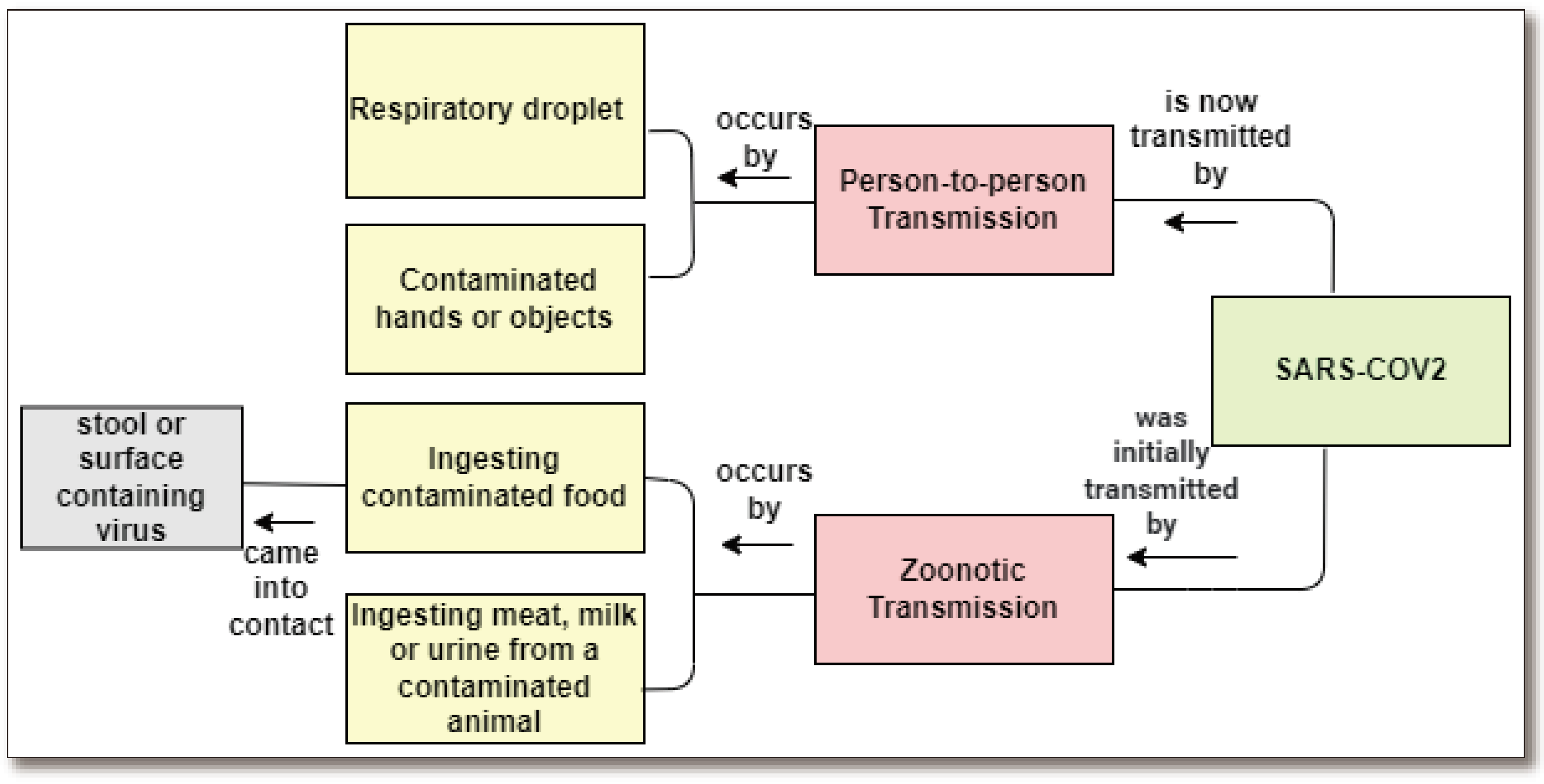
Figure 2.
a. Globally, as of 12 August 2022, there have been 585,950,085 confirmed cases of COVID-19, including 6,425,422 deaths, reported to WHO. [https://covid19.who.int/ ---12-August-2022]. Figure 2b. Total number of cases and deaths from coronavirus (COVID-19) in the WHO region as of August 12, 2022, weekly [https://covid19.who.int/---12-August-2022].
Figure 2.
a. Globally, as of 12 August 2022, there have been 585,950,085 confirmed cases of COVID-19, including 6,425,422 deaths, reported to WHO. [https://covid19.who.int/ ---12-August-2022]. Figure 2b. Total number of cases and deaths from coronavirus (COVID-19) in the WHO region as of August 12, 2022, weekly [https://covid19.who.int/---12-August-2022].
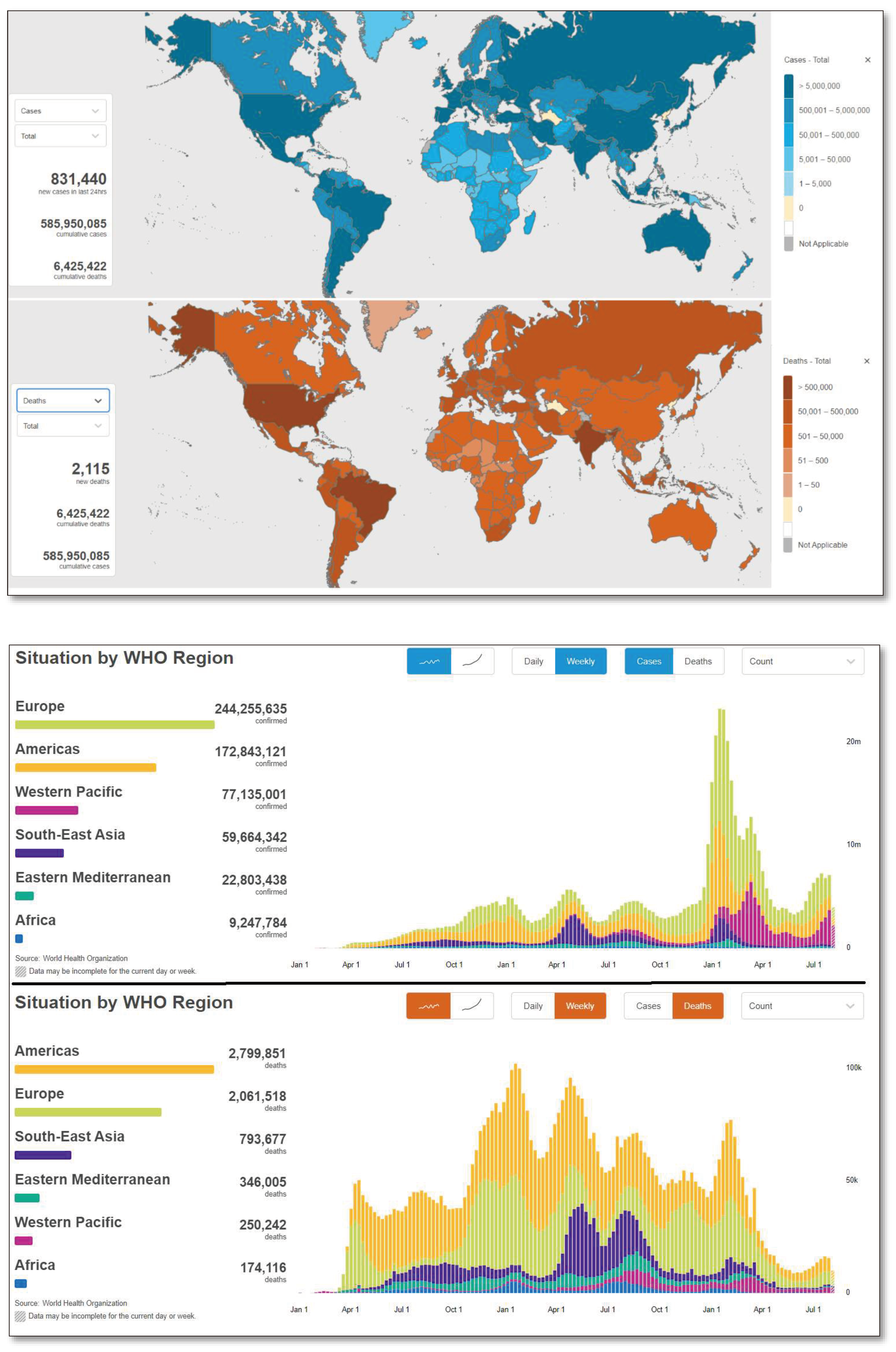
Figure 3.
COVID Mutation worldwide1.4 Problem Statement/The State of the Art.
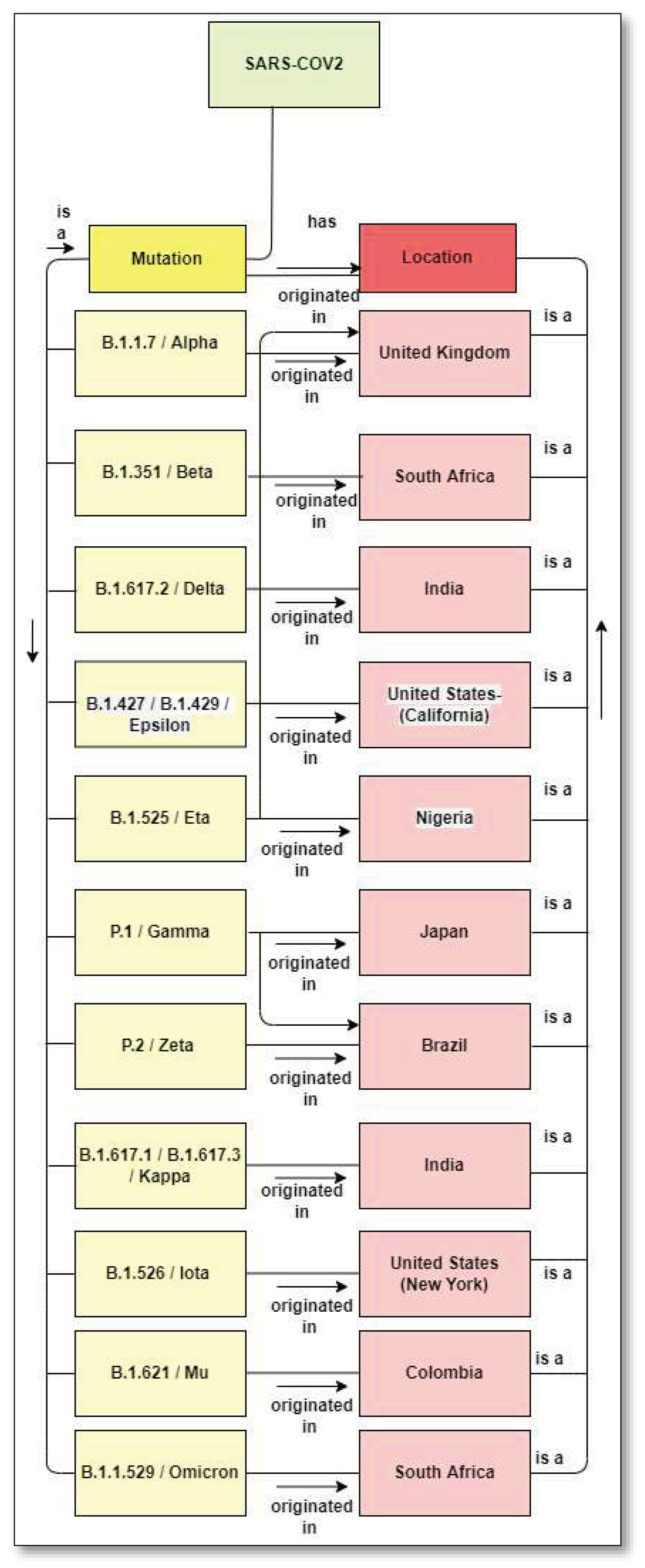
Figure 5.
Vaccine Development History [17].
Figure 5.
Vaccine Development History [17].
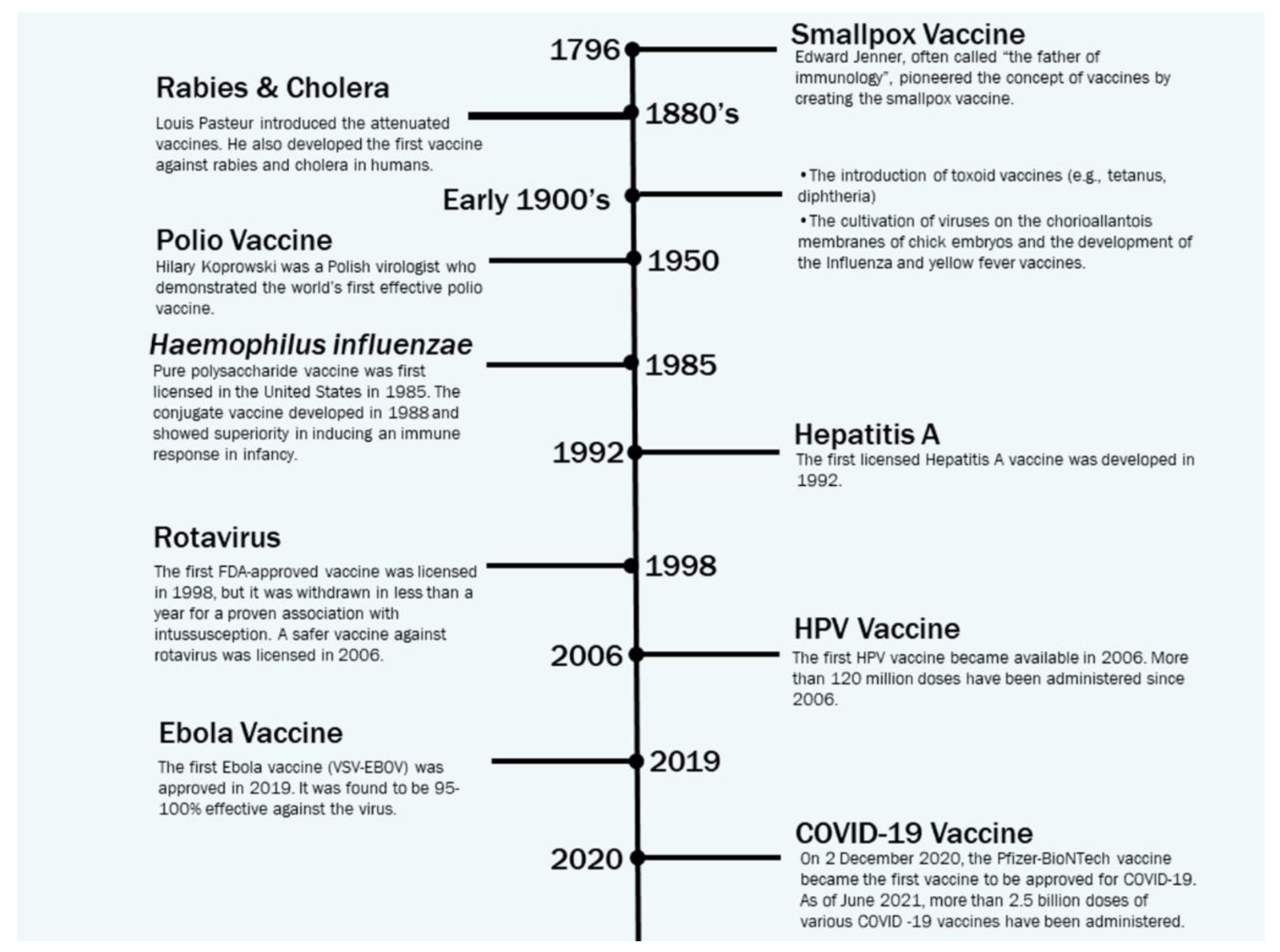
Figure 6.
Optimizing the Design for Efficient Vaccines [18].
Figure 6.
Optimizing the Design for Efficient Vaccines [18].
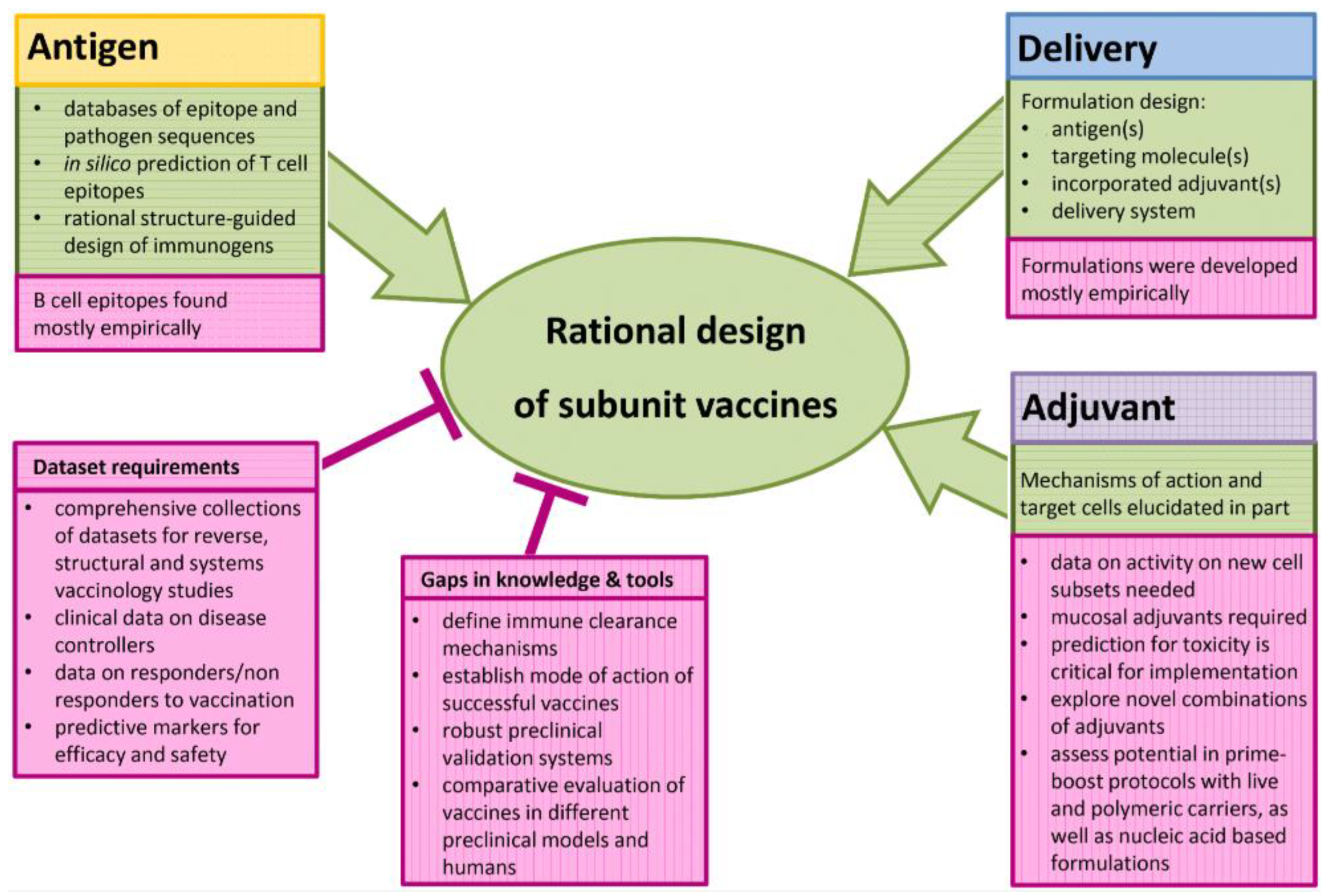
Figure 7.
Insights into SARS-CoV-2 genome, structure [25].
Figure 7.
Insights into SARS-CoV-2 genome, structure [25].
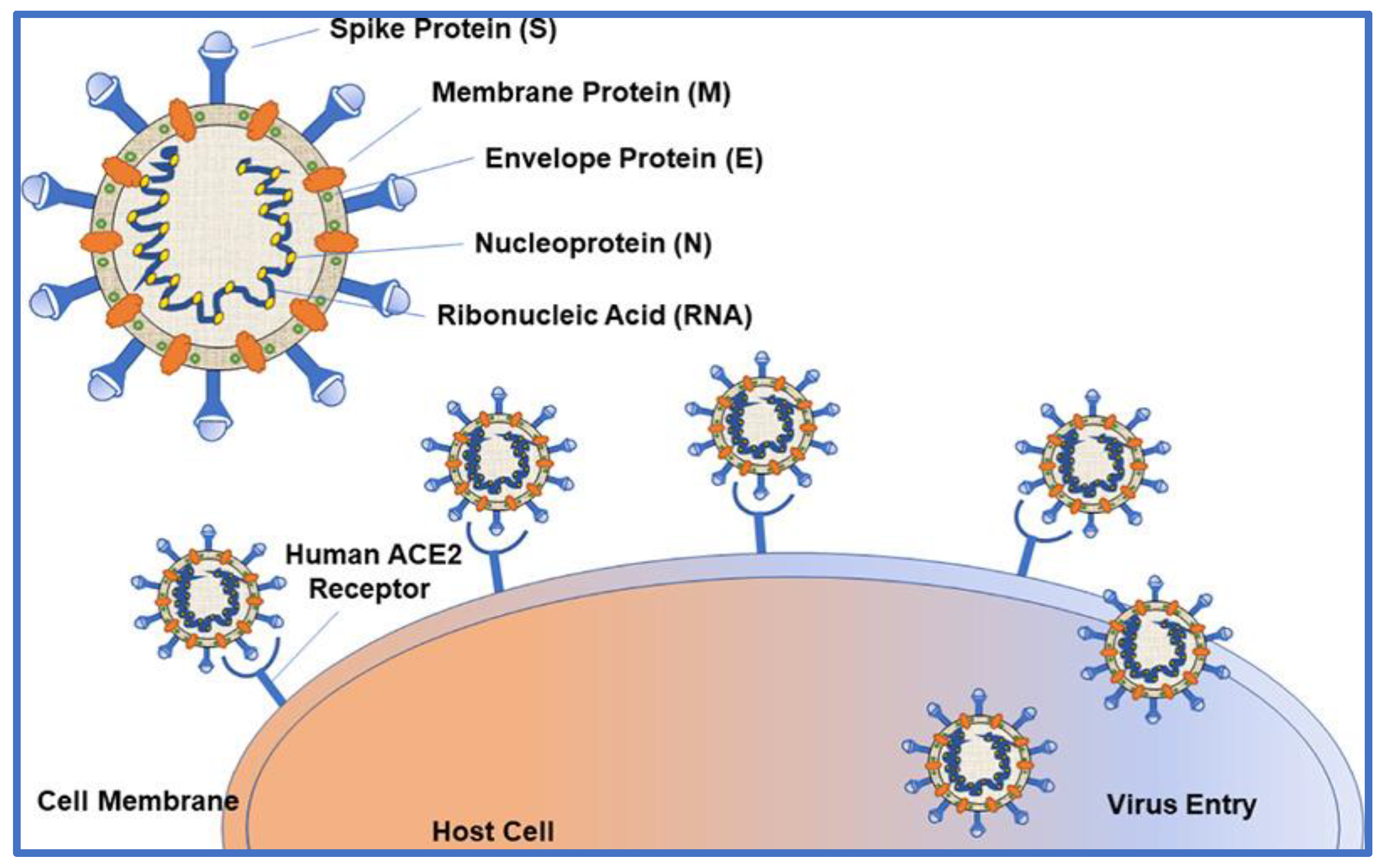
Figure 8.
Three types of coronavirus vaccines are currently being developed. (From a presentation given at a Senate hearing on September 9, 2020, by the National Institutes of Health).
Figure 8.
Three types of coronavirus vaccines are currently being developed. (From a presentation given at a Senate hearing on September 9, 2020, by the National Institutes of Health).
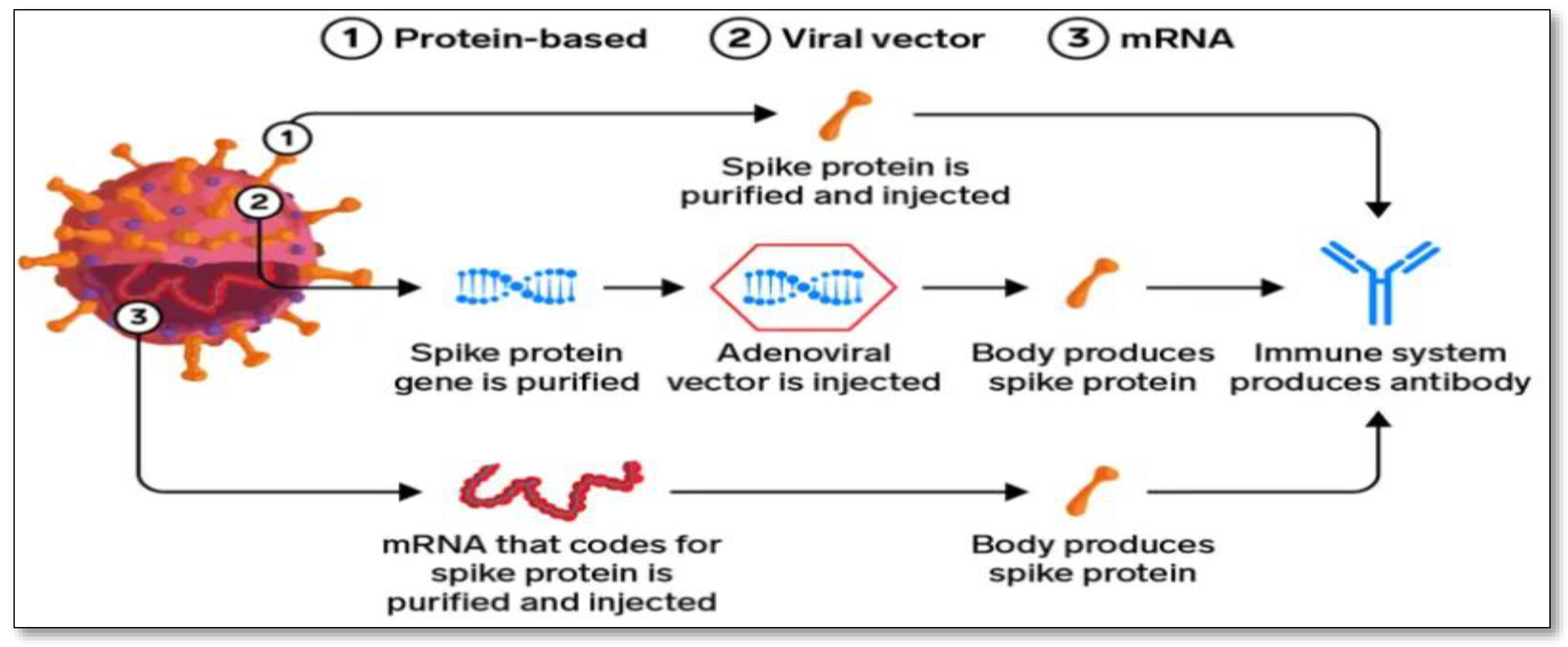
Figure 9.
Vaccine development approaches.
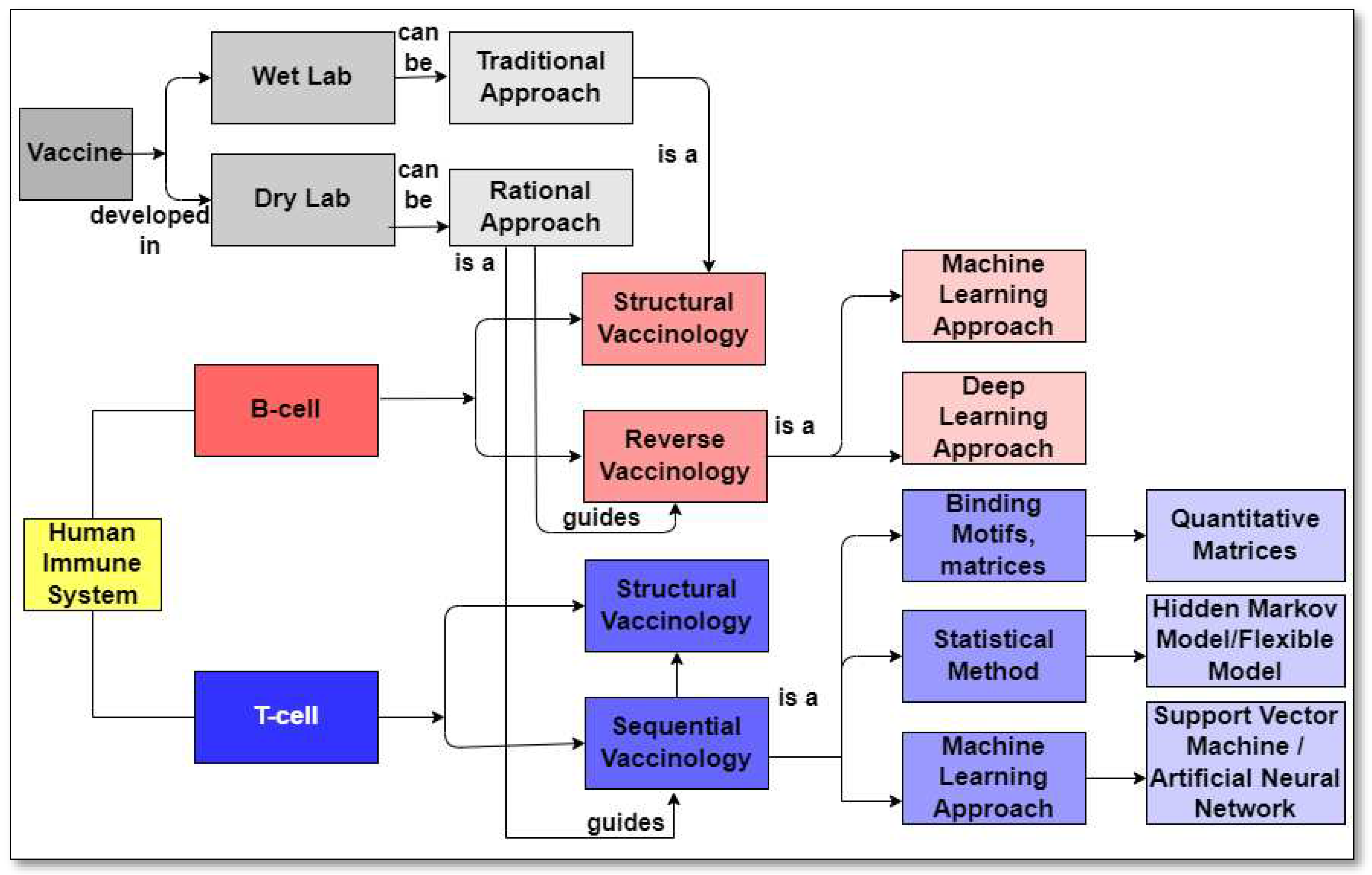
Figure 10.
Internal process of reverse vaccinology [105].
Figure 10.
Internal process of reverse vaccinology [105].
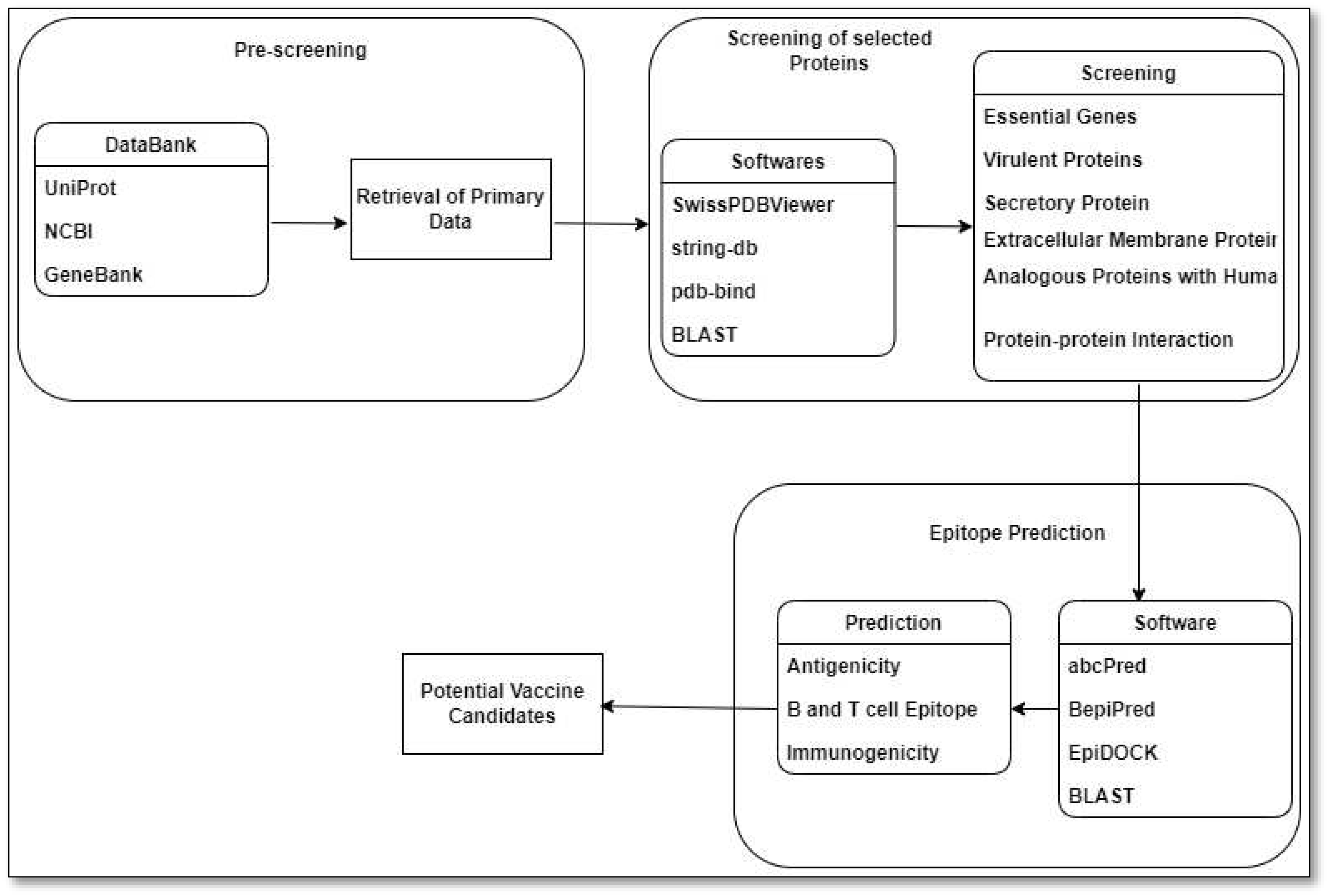
Table 1.
Pipeline of COVID-19 vaccine candidates by the technology platform. There are currently 261 vaccine candidates being tracked by the London School of Hygiene and Tropical Medicine [34,35,36,37,38,39,40].
| Country | Stabilizing Mutations | Carrier | Type | Mechanism |
|---|---|---|---|---|
| Germany,USA/BioNTech/Pfizer | Yes | Simian Monkey A Virus | mRNA | Following injection, the vaccine particles collide with cells and fuse with them, releasing mRNA. Molecules in the cell read the sequence and construct spike proteins. The cell eventually destroys the vaccine's mRNA, leaving no permanent trace. |
| USA/Moderna | Yes | Human AA Virus | mRNA | The vaccine's nucleoside-modified mRNA is formulated in lipid particles, allowing delivery of the nucleoside-modified mRNA into host cells and expression of the SARS CoV 2 Spike antigen. |
| UK, Sweden/Oxford/AstraZeneca | No | Monkey AA Virus | Adenovector | The adenoviruses collide with cells and latch onto proteins on their surfaces after being injected into a person's arm. The virus is engulfed in a bubble by the cell, which pulls it inside. Once inside, the adenovirus escapes the bubble and travels to the nucleus, which houses the cell's DNA. |
| China/Cansino | No | Adenovector | The new coronavirus is carried into the human body using a modified common cold virus. | |
| Russia/Sputnik V | No | Human AA Virus | Adenovector | A weakened virus is used to deliver small amounts of a pathogen and to stimulate an immune response. |
| China/Sinopharm | Not applicable | Inactivated | It works by exposing the body's immune system to the virus via killing viral particles without risking a serious disease response. | |
| India/BharatCovaxin | Not applicable | Inactivated | It is made from a weakened version of a common cold virus (called an adenovirus) derived from chimps. It has been altered to resemble a coronavirus. | |
| China/Sinovac CoronaVac | Not applicable | Inactivated | It works by exposing the body's immune system to the virus via killing viral particles without risking a serious disease response. | |
| Russia/Vector Institute EpiVacCorona | Yes | Subunit | The vaccine is based on chemically synthesized SARS-CoV-2 protein-peptide antigens conjugated to a carrier protein and adsorbed on an aluminum-containing adjuvant (aluminum hydroxide). | |
| Germany/CureVac | Yes | mRNA | Following vaccination, the body recognizes the protein as potentially harmful and activates the immune system, producing antibodies and T cells to combat it. In this way, we mimic natural viral infection and activate the immune system. | |
| USA/Johnson & Johnson | Yes | Adenovector | An adenovirus serves as a vehicle for the transmission of coronavirus genetic material (DNA). The adenovirus delivers the small piece of DNA to the cell, which then produces the spike protein. |
Table 2.
Machine Learning Algorithms for COVID-19 Forecast.
| Algorithms | Subcategory | Methods | Recent Publications |
|---|---|---|---|
| Supervised Learning | Classification | K-nearest Neighbours (KNN) | KNN was used to identify respiratory diseases by Ginantra et al. [62] KNN was utilized by Yin et al. [63] to identify severe influenza. In (Cho, 2016) [64], KNN was used to track the infected users' locations. |
| Support Vector Machine (SVM) | SVM was employed by Mori et al. [65] to forecast the onset of a disaster in a particular area. For the diagnosis of COVID-19, SVM was used with IoT (Internet of Things) and CNN (Convolutional Neural Networks) by Le et al. [66]. | ||
| Naïve Bayes | Naive Bayes classifier has been used by Sadhukhan et al. [67] and Assery et al. [68] to group tweets. During the pandemic, it assisted in managing social networking issues. | ||
| Logistic Regression | To categorize COVID-19 patients in Iran, Mohammadi et al. [69] employed ANN and LR. Various blood and clinical indicators were employed by Bhandari et al. [70] to use Logistic Regression to predict the death rate. COVID-19 in Kuwait was predicted using LR by Almeshal et al. [71] | ||
| Decision Trees | During pandemics, decision trees have been used to determine the location of the users by Elhoseny [72]. Decision trees were used to discuss the prediction of several aspects that contributed to psychological suffering during the pandemic by Chen & Liu [73]. Using decision trees, a hybrid face mask detection application was created by Loey et al.[74]. | ||
| Random Forest | RF method was used to predict COVID-19 health by Iwendi et al. [75] The spatial-temporal distribution of COVID-19 daily cases worldwide was estimated using the random forest machine learning approach by Yeşilkanat [76]. | ||
| Artificial Neural Network (ANN) | IoT and ANN were combined to determine the user's position by Luoh [77]. Although there was little data available, the accuracy was great. ANN was employed by Polese et al. [78] to identify the precise group of persons who were present in a location. | ||
| Deep Neural Network (DNN) | DNN was employed by Chhikara et al. [79] to evacuate a crowd in a crisis. Transferring healthy individuals to areas free of infectious diseases is crucial. | ||
| Convolution Neural Network (CNN) | People with COVID-19 were diagnosed using an IoHT (Internet of Health Things) and CNN-based model by More et al. [80] | ||
| Regression | Linear | To anticipate new COVID-19 coronavirus illness cases that are currently active, a multivariate linear regression model was applied by Rath et al. [81] A linear regression model was used to predict COVID-19 positive samples in Nigeria by Ogundokun et al.[82] | |
| Polynomial | Based on the polynomial regression model, estimates of the COVID-19 epidemic in India were examined by Pandey et al.[83]. To predict the global spread of COVID-19, hierarchical polynomial regression models were used by Ekum & Ogunsanya [84]. | ||
| Support Vector | It was applied in Brazil to anticipate COVID-19 confirmed cases in the short term by Ribeiro et al.[85] | ||
| Ridge | It was explored in utilizing a hybrid polynomial-Bayesian ridge regression model to predict the progression of the COVID-19 pandemic by Saqib [86]. | ||
| Unsupervised Learning | K-Means | The use of k-means to project the number of COVID-19 cases reported was covered by Vadyala et al. [87] In the United States of America, the K-Means method was used to forecast COVID-19 instances by Zhang & Lin [88]. | |
| K-Medoids | Indonesia's National Food Security during the COVID-19 epidemic utilized data mining techniques, including the k-medoids algorithm, as was discussed in by Elsi et al.[89] | ||
| Fuzzy C-Means | For detecting COVID-19 infection in chest X-rays, an intelligent model based on the Lévy slime mould algorithm and adaptive fuzzy C-means has been constructed by Anter et al. [90] Using Fast Fuzzy C means clustering, ROI extraction in COVID-19 CT lung images was mentioned by Chadaga et al. [91] The radiologists and other medical specialists benefited from this. | ||
| Reinforcement Learning | Q-Learning | Using multi-robot cooperation and the Q-learning approach, a strategy for the prevention of COVID-19 affected patients was provided by Sahu et al. [92] Miralles-Pechuán et al. [93] presented a novel methodology based on Deep Q-learning/Genetic Algorithms for optimizing Covid-19 pandemic government activities. | |
| Markov’s Decision Process | Clinical risk factors of patients and the COVID-19 pandemic were analyzed using the epidemiological Markov model by W. Zhang et al. [94] |
Table 4.
Overview of recent reverse vaccinology approaches of getting COVID-19 vaccine.
| Research Group | Database | Target Proteins | B-cell and T-cell Epitope Prediction |
Antigenicity and Allergenicity Test | Molecular Docking | Immunogenicity Evaluation |
Energy Minimization and Binding Affinity Prediction | In Silico Cloning and Codon Optimization |
|---|---|---|---|---|---|---|---|---|
| Qamar et al.[106] | GenBank | S, E, M proteins | ✔ | ✔ | ✔ | ✔ | ● | ✔ |
| Chen et al.[107] | NCBI | S, N proteins | ✔ | ✔ | ● | ● | ● | ● |
| Bhattacharya et al.[108] | NCBI | S protein | ✔ | ✔ | ✔ | ● | ● | ● |
| Ahmed et al.[109] | UniProt | S protein | ✔ | ✔ | ✔ | ● | ● | ● |
| Naz et al.[110] | NCBI | S protein | ✔ | ✔ | ✔ | ● | ✔ | ● |
| Kar et al.[111] | PDB (6VSB) | S protein | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| Robson[112] | GenBank and the Protein Data Bank | S protein | ✔ | ● | ● | ● | ● | ● |
| Enayatkhani et al. [113] | NCBI | First S, E, M, N, ORF10, ORF8, ORF3a; then after the antigenicity test N, ORF3a, and M | ✔ | ✔ | ✔ | ● | ✔ | ● |
| Sarkar et al.[114] | NCBI | N, M, S, ORF3a | ✔ | ✔ | ✔ | ● | ● | ✔ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



