Submitted:
27 November 2023
Posted:
28 November 2023
You are already at the latest version
Abstract
This rapid review aims to present a comprehensive overview of barriers and facilitators or factors, and, effective interventions that promote immunisation uptake by older people in the Asia-Pacific region. Rapid review methodology was applied using two databases (PubMed, Embase). Articles were included if studies were conduced in Australia, Singapore, Indonesia and the Philippines, included human population ≥50 years old, used original data, adopted quantitative, qualitative, and mixed-method designs, and published from 2016 to August 2022. The study selection yielded 1424 articles. A total 23 papers met the inclusion criteria, of which 19 reported on barriers and facilitators, while, 4 articles reported on effective interventions to promote vaccination uptake. Among the 19 studies that identified barriers and facilitators to vaccination uptake, the more common factors were social influences (n=8/19), perceived benefits of vaccine (n=7/19), and perceived vaccine safety (n=6/19). Strategies that focussed on supporting clinicians were found to be effective in leading them to recommend vaccinations among older adults such as creating awareness on the low baseline vaccination rates among older adults, provision of structured health assessment, and nurse reminders. More studies are needed ascertain the factors, and effective interventions influencing vaccine uptake among older people in the Asia-Pacific region.
Keywords:
vaccine uptake
; immunisation
; adults
; older people
; elderly
; Asia-Pacific
; barriers
; facilitators
; factors
; interventions
Introduction
Saving millions of lives globally each year, immunization is now considered fundamental to primary health care and public health. The World Health Organization (WHO) has adopted a life-course approach to immunization and healthy ageing in the WHO Immunization Agenda 2030 and the UN Decade of Healthy Ageing program [1]. Life-course immunization is particularly important in Asia-Pacific as its population ages at an unprecedented pace. In 2020, 13.6% of the population in Asia-Pacific was aged 60 years or over [2]. The number of older adults (aged 65 years or older) in the region is estimated to increase more than twofold, from 535 million in 2015 to about 1.3 billion in 2050 [3]. Despite the widespread benefits of vaccines, vaccination uptake in this population segment remains low across Asia-Pacific [4]. For instance, only 37.3% individuals who are in high-risk group that included older adults reported to take influenza vaccination. This is far below the WHO target of 75% for older adults [4].
To improve vaccination uptake among older adults in Asia-Pacific, it is essential to understand the related factors, as well as the interventions that have been shown to be effective, specific to this context. Several reviews have reported on factors influencing vaccination uptake among older adults. Among the factors were storage of vaccines, funding and costs (healthcare systems factor); accessibility, vaccination settings (policy and operational factor); knowledge of vaccines and mechanisms of action, failure to assume the responsibility for vaccination, incomplete or inaccessible documentation of previous vaccinations (healthcare provider factor); perception vaccine is ineffective or harmful, and mistrust in healthcare system (patient and caregiver factor) [5,6,7]. Some of the reviews covered diverse geographical areas [5,6] or concentrated on a single country [7], with none looking specifically at the Asia-Pacific region.
Various interventions for promoting vaccination uptake have been reported in the literature. A review of interventions aimed at addressing barriers to vaccination uptake among adults aged 18 years or older such as lack of knowledge about, and the need for vaccination, lack of recommendation from healthcare providers (HCPs), poor access to vaccines, financial considerations, and racial and ethnic disparities highlighted that interventions such as educational and financial strategies, providing access, and reminders can improve vaccination uptake [8]. In a recent review, provider-led educational initiatives and provider recommendations were shown to be more effective than less interactive interventions, such as posters and reminder-recall letters. Interventions targeting HCPs, including awareness campaigns, incentives, affordability efforts, and vaccination site expansion also showed positive associations [9]. Both reviews above covered diverse geographical areas, however, the understanding of effective interventions at overcoming barriers related to older adults’ uptake of vaccination specifically in the Asia-Pacific setting is still lacking.
This rapid review aims to provide an overview of the known factors related to, as well as effective interventions at promoting vaccination uptake by older adults in Asia-Pacific. More specifically, this review focused on four countries: Australia, Singapore, Indonesia and the Philippines. These four countries were selected because they represent the diverse nations across the Asia-Pacific region in terms of socio-economic development, healthcare structures and policies, and culture. Australia and Singapore have rapidly ageing societies with older adults (aged 65 years or above) constituting 17% and 14% of the population, respectively [10]. Even though Indonesia and Philippines have 7% or less of their population aged 65 years or above at present [11], these countries are also expecting to become ageing societies by 2030 [12]. The findings of this review will help to identify missed opportunities and promote vaccination uptake among older adults, as part of building strengthened and sustainable health systems in Asia-Pacific communities.
Methods
Search strategy
A literature search was conducted in August 2022, searching PubMed and EMBASE electronically. The following concepts were used in the literature search: “older people”, “vaccination”, “barriers”, “facilitators”, “intervention”, “strategy”, “Australia”, “Singapore”, “Indonesia”, “Philippines”, and their synonyms or alternative spelling. Keywords of barriers and facilitators pertaining to vaccination among older adults that had been identified in the literature such as "knowledge", "internet access", "information", "funding", "cost", "financial", "infrastructure", "policy", "politics", "affordability”, and "coverage" were also included in the search strategy for comprehensiveness.
Both keywords and MeSH terms were used. The search strategy can be found in supplementary materials: (Table S1. Search strategy).
Literature selection
All titles retrieved were imported into the bibliographic management software, EndNote X21. Duplicates were removed. The screening process was guided by recommendations for conducting rapid review by the Cochrane Rapid Reviews Methods Group [13]. Article screening involved two of the authors (AS and AL) screening 20% of all the titles/abstracts, with conflict resolution. AS then screened the remaining titles/abstracts. Excluded titles/abstracts were screened by another author (WTT). This is followed by four authors working in pairs (AS & WTT; MPEN & SCT) to assess the full text of resultant articles (n=104; 52 each pair), with the articles divided up equally between pairs (an author in the pair was assigned either 20 or 21 articles). Each author independently assessed the articles assigned to their pair and cross-checked their partner’s excluded articles. Discrepancies were resolved through discussions. Articles assessed were included in or excluded from the review according to the inclusion and exclusion criteria outlined below (Figure 1).
Figure 1.
Article inclusion and exclusion criteria.
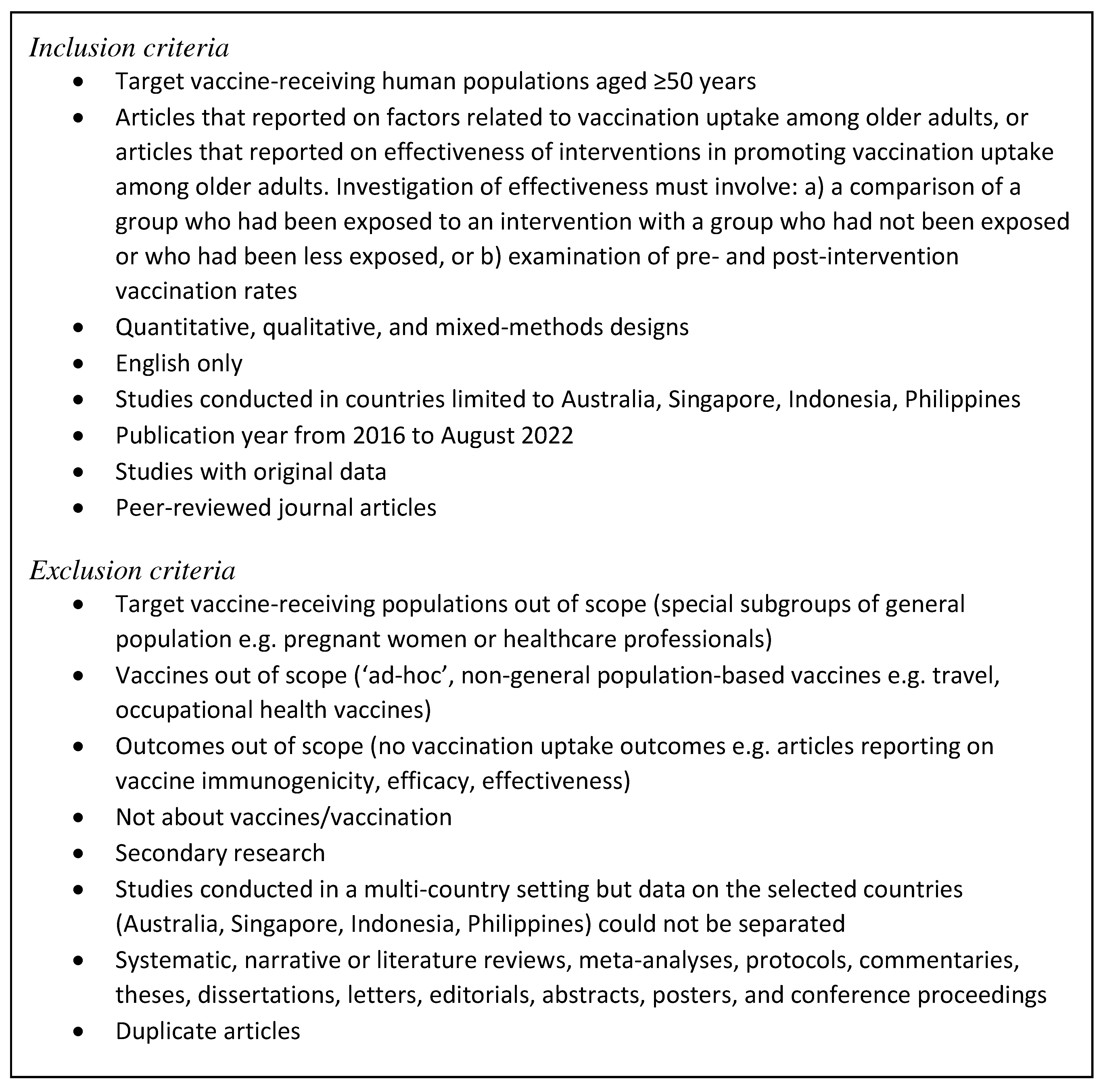
The target study populations aged ≥50 years was used because older adults particularly those aged 50 years and above are at a higher risk of severe outcomes for diseases such as covid-19, influenza, pneumococcal and shingles. Consequently, national immunization programmes target the age group for recommended vaccines, and in some cases provide free vaccines to eligible sub-groups. In Australia, for instance, pneumococcal vaccine is free for Aboriginal and Torres Strait Islander adult populations over 50 years and above [14]. In Singapore, adults over 50 years were prioritised in the Covid-19 vaccine campaign [15].
During the literature search process, it was found that there no articles on Indonesia or Philippines. To ensure that articles on these two countries were not missed, the search was run again but with the publication timeframe backtracked to year 2012 for the two countries. However, the same was found. Subsequently, e-mails seeking literature recommendations were sent to experts on immunization known to the authors in these two countries, but none was proposed.
Data extraction
Data extraction was divided into two parts based on the aims of this review. The first part focused on factors related to vaccination uptake among older adults. The second part focused on effectiveness of interventions for promoting vaccination uptake among older adults. Two sets of data extraction forms were created correspondingly.
Similar to the process of full-text assessment of articles for inclusion, data extraction was conducted by four authors working in pairs (AS & MPEN; AL & WTT), with the articles divided up between pairs (n=23; 11 or 12 articles for one of the pairs). Each author independently extract the articles assigned to their pair (an author in the pair was assigned either 5 or 6 articles). Data on the following were extracted from the included articles: author name, publication year, study country, vaccine type, study setting, study design, study population, data analysis methods, factors related to vaccination uptake (where applicable), intervention description and effectiveness for promoting vaccination uptake (where applicable). Once an author finished their share of the data extraction work, their partner cross-checked for correctness and completeness of the extracted data.
Risk of bias assessment
The Mixed Methods Appraisal Tool [16] was used to appraise the quality of included articles. The quality appraisal was again conducted by four authors working in pairs (AS, WT; MPEN, SCT). Each author cross-checked the appraisal done by their partner, and disagreements were resolved through discussions.
Data analysis and reporting
Regarding factors related to vaccination uptake among older adults, the data analysis process involved WTT classifying emerging barriers and facilitators into broader themes. The themes were constructed using a data-driven approach. Using the inductive approach, barriers and facilitators reported in both quantitative and qualitative studies were extracted, similar factors were then grouped together and categorised into broader themes.
In this review, quantitative, qualitative, and mixed-methods studies were included. For studies that quantified the association between factors and vaccination uptake, odds ratios and p-values were extracted when the data is available. For studies that only presented frequencies of factors, the top three most frequent factors reported were included [17]. For qualitative studies, unique factors that were not identified in quantitative studies were also included. Whether a factor was deemed negative (barrier) or positive (facilitator) depended on how the descriptions were phrased in the qualitative article. For example, “Seven refusers and defaulters cited being not vulnerable to influenza as a reason for not having the vaccine. Most felt they were not vulnerable because they seldom got influenza. This was reinforced by previous encounters with mild episodes of influenza.” [18] was extracted as a negative factor for (barrier to) vaccination. Where factors similar to those identified in quantitative studies were found, they were used to confirm or add a perspective to the findings from quantitative studies.
Regarding effectiveness of interventions for promoting vaccination uptake among older adults, interventions identified were classified according to the nine categories defined by the Expert Recommendations for Implementing Change (ERIC) project [19]. The effectiveness of the interventions reported was based the effect of the interventions in influencing the uptake of the specific vaccination in the studies. Where available, p-values and odds ratios were reported.
Results
Literature selection
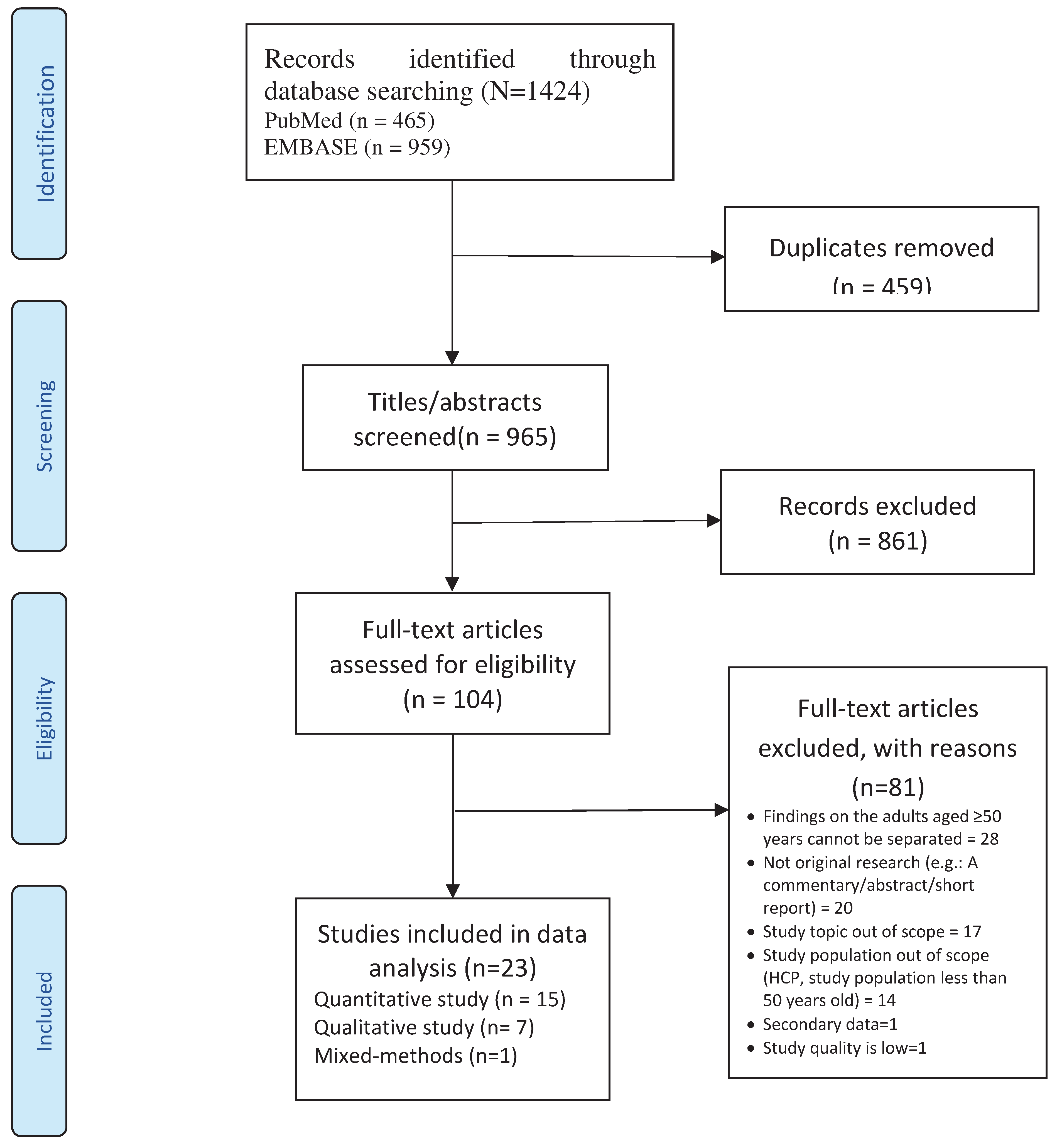
A total of 1424 records were retrieved from the databases. After removal of 459 duplicates, 965 records were put through title and abstract screening, which excluded 861 articles. After full-text assessment of the remaining 104 articles, 23 articles were included in the review (19 on factors related to vaccination uptake, and four on effectiveness of interventions for promoting vaccination uptake). Figure 2 illustrates the literature selection process.
Figure 2.
Flow diagram detailing the database searches, the number of abstracts screened and the full texts retrieved.
Figure 2.
Flow diagram detailing the database searches, the number of abstracts screened and the full texts retrieved.
Study characteristics
The characteristics of the included articles are summarized in Table 1.
Studies on intervention effectiveness
There were four studies that tested interventions aimed at increasing vaccination uptake among older adults. The vaccines of focus were influenza (2/4 studies), influenza and pneumococcal (1/4 studies), and herpes zoster (1/4 studies). In terms of study design, two studies were randomized controlled trials, one was a before-and-after study, and one was a retrospective analysis. Three studies were conducted in Singapore, and one in Australia.
Risk of bias in studies
Overall, the quality of the studies was found to be acceptable, except one, which was therefore removed from the review. The details on each study’s appraisal can be found in supplementary materials: (Table S2. Study appraisal).
Individual characteristics
The individual characteristics related to vaccination uptake among older adults included age, sex, knowledge, past vaccination experience, perceived health status, comorbidities, income, marital status, smoking status, education, employment status, housing type, ethnicity, and engagement in physical activity.
Knowledge and awareness of vaccine and immunization
Knowledge was one of the most commonly reported factors related to vaccination uptake. There was a lack of knowledge about the influenza vaccine [25,30], and some older adults had not heard of the pneumococcal vaccine [36]. There were also various misconceptions about the influenza vaccine, such as it is only needed before travel, the interval for vaccination, vaccine as a cure or treatment for flu, the effect of ageing on bodies made older people not suitable for vaccine, that antibiotics could replace the need to have the influenza vaccine, and proper lifestyle and diet is adequate to prevent getting flu [18].
Awareness of the types of vaccine available for their specific age group [31], and awareness of free vaccination (Trent et al., 2020) was related to older adults receiving vaccination.
Past vaccination experience or infection
The lack of experience with influenza influenced older adults to not pay much attention to the need for influenza vaccination [18].
Vaccination uptake was positively related to having been vaccinated in the past. Older adults who had received an either influenza vaccine in the previous 12 months [36] or a pneumococcal vaccine [24] were more receptive to vaccination. Previous experience of protective health effects of influenza vaccination for themselves and their families was also a predictor of influenza vaccination uptake [18]. Participants referred to their experience of disease such as diphtheria, or having chronic diseases, or being immunocompromised, and having vaccination over their lifetime when expressing their appreciation that the COVID-19 vaccine existed to reduce their vulnerability to COVID [32].
Perceived health status and co-morbidities
Three Singapore-based studies reported that participants’ self-perceived health status was related to various vaccinations uptake such as influenza, pneumococcal, and COVID-19. Perceived poor health was related to lower uptake [20,21,35], while perceived good health status was related to higher vaccination uptake [35].
Attitudes and beliefs
Perceived benefits of vaccine
Another driver for older adults to go for vaccination was their perceived benefits of vaccines. Older adults reported the health benefits of vaccines in terms of protection of oneself [18], and the community from diseases [31,32], and promoting longevity [28,29]. Older adults also reported a belief that vaccines contain vitamins [25] and can lead to a stronger body in terms of being able to eat without fear of falling sick [30]. Another perceived benefit of getting vaccinated was having the personal freedom to travel and socialize with others [29,31].
Perceived vaccine safety and effectiveness
Another major theme that emerged from the studies was the perceived characteristics of the vaccine, including side effects and effectiveness of the vaccine. A commonly reported factor negatively related to vaccination uptake was the belief that COVID-19 vaccines are not safe [28,29]. There are also studies that found that uptake is negatively related to fear of short and long-term side effects of the vaccine [31], and worry of pain associated with vaccination [18,25,30].
Social responsibility
In Australia, perceived social responsibility emerged as both positively and negatively related to vaccination uptake. A concern for the health and livelihood of family members emerged as a factor regarding vaccination decisions. Older adults in close contact with children below five years of age reported highest recall rates of adult pertussis vaccination over time [22]. Individuals also reported perceived social responsibility towards the community [24], protecting the public and having a moral obligation to get vaccinated for the safety and protection of others, as a reason to opt for Covid-19 vaccination [29].
Trust
Studies reported levels of trust in vaccines, healthcare workers and sources of information as related to vaccination uptake. In Australia, a general distrust of vaccines was a predictor for not taking pneumococcal vaccine [36], with a lack of trust in vaccine development processes related to general distrust towards the government. There were misconceptions such as remote indigenous communities being used as test dummies for vaccines [28]. In Singapore, among the barriers to influenza uptake was mistrust in the doctor’s advice [18], including their recommendations being informed by profit considerations [25].
Older adults with trust in formal sources of information such as government sources, as well as local news on the television or radio, were significantly more likely to get vaccinated [35].
Perceived susceptibility
A low perceived risk and severity of disease was related to low vaccination uptake [36]. In Singapore, a low perceived risk of contracting influenza, reinforced by previous experience of mild episodes of influenza influenced older adults to not get influenza vaccinations [18]. Thus, older adults were less willing to get vaccinated if they did not see the disease as a threat.
Personal health beliefs and practices
Religion and fatalism
Interpersonal
Social influence
Studies found that recommendations by physicians and other healthcare personnel, as well as family members, were related to vaccination uptake. Social influences came in the forms of recommendations by doctors and nurses, or personal recommendations by friends and family. In both Australia and Singapore, a lack of advice and encouragement from healthcare workers was a deterrent to vaccination uptake [18,24,25]. In Singapore, a lack of encouragement and reminders from immediate social networks such as friends and family was another reason for not going for influenza vaccination (Teo et al., 2019).
Having a regular family doctor/GP
Community
Among older adults, a lack of mobility or transportation was related to non-uptake of vaccination. In Australia, pneumococcal vaccination uptake was lower among patients whose general practitioner’s clinic was located in outer and remote areas compared to inner regional or major cities [27]. Vaccination coverage among older adults varied by remoteness and was highest in major cities [33]. Living in a higher socio-economic status area was positively related to vaccination uptake [26], while vaccination rates were low for those living in lower socio-economic status areas [27,33]. Access to vaccines was a predictor of uptake in both countries [23,25]. In Singapore, older adults reported that the need to travel to vaccination sites, and the long waiting times at clinics as inconvenient, and these deterred them to go for influenza vaccination [25]. Complying with pre-travel vaccination was also related to higher influenza vaccination uptake among Singapore older adults [18].
Vaccine-related
The high cost of vaccine was reported as a barrier for vaccine uptake in general [30]. A fear of injections prevented some older adults from receiving vaccination [18,25].

Table 2.
Factors related to vaccination uptake among older adults in Australia and Singapore.
| Australia | Singapore | No. of studies (out of 19) | |||
|---|---|---|---|---|---|
| Domain and factor | Barrier | Facilitator | Barrier | Facilitator | |
| Individual characteristics | |||||
| Age | Higher age (OR: 2.01 (95% CI 1.77-2.77)) (Enticott et al., 2018) [26]; Those aged 75–84 (PR = 1.42; 95% CI = 1.20–1.69, p < 0.01) (Trent et al., 2020) [36]; Qualitative findings: Those aged 85 plus (Briggs et al., 2019) [24]; Older people (those aged 70 and over) were very supportive of vaccines (Lupton et al., 2022) [32] |
Individuals aged ≥50 (OR=1.30 [1.02; 1.67], p=0.036) (Ang et al., 2017 [21]) | 5 | ||
|
Sex |
Men: SARSCoV- 2 vaccine intention to uptake (OR: 1.37 (95% CI 1.08-1.72)) (Enticott et al., 2018) [26] Women: Pneumococcal vaccine uptake (69.1% (95% CI: 68.6;69.6)) (Frank et al., 2020 [27]; (PR = 1.21, 95% CI = 1.02–1.45, p = 0.03) (Trent et al., 2020) [36]; Herpes zoster vaccine uptake (adjusted OR: 1.1, 95% CI: 1.1–1.2) (Lin et al., 2020) [33] |
Women (OR: 0.83, p < .05) (Tan et al., 2022 [35]) | 5 | ||
| Knowledge and awareness | Never having heard of the pneumococcal vaccine (PR = 0.07; 95 %CI = 0. 03–0.18; p < 0.01) (Trent et al., 2020) |
Awareness of the eligibility of the free pneumococcal vaccination under the National Immunisation Programme (PR = 5.02; 95% CI = 2.34– 10.77; p < 0.01) (Trent et al., 2020) [36] Qualitative findings: Awareness of the availability of vaccine for specific age group for older people (Kaufman et al., 2022) [31] |
Qualitative findings: Misconceptions of influenza vaccines (Teo et al., 2019 [18]) Lack of knowledge about the influenza vaccine (Cummings et al., 2020 [25]; Ho et al., 2017 [30]) |
5 | |
| Past vaccination experience or infection |
Had influenza vaccination in the previous 12 months (PR = 4.28; 95% CI = 2.85–6.44, p < 0.01) (Trent et al., 2022) [36] Qualitative findings: Participants who had been immunised against pneumococcal disease were also receptive to influenza vaccination (Briggs et al., 2019) [24]. Older people referred to their experience of disease and vaccination over their lifetimes when expressing their appreciation that COVID vaccines existed (Lupton et al., 2022) [32] |
Qualitative findings: The lack of experience with influenza also caused participants to not pay much attention to the need for vaccination (Teo et al., 2019 [18]) |
Qualitative findings: Previous positive experience with influenza vaccines (Teo et al., 2019 [18]) |
4 | |
| Perceived health status | Poorer perceived health (moderate, aOR=0.68 [0.55; 0.83], p<0.0005); bad, aOR=0.17 [0.07;0.40], p<0.0005) (Ang et al., 2017 [21]) (moderate, aOR=0.55 [0.41; 0.75] p<0.0005; bad, aOR=0.28 [0.11;0.66] p=0.004) (Ang et al., 2018 [20]) (p < .0.001) (Tan et al., 2022 [35]) |
Positive perceived of health status (OR: 1.26, p < 0.001)(Tan et al., 2022 [35]) | 3 | ||
| Comorbidities | Individuals with comorbidities (95% CI: 71.3-72.3, p < 0.001) (Frank et al., 2020) [27] such as lung disease (PR = 1.36, 95% CI = 1.11– 1.67, p < 0.01) (Trent et al., 2022) [36] |
Individuals with comorbidities (aOR=1.43 [1.14; 1.80], p=0.002) (Ang et al., 2017 [21]) | 3 | ||
| Income | High monthly household income (>$6000): (">6000$": OR=3.18 [1.98; 5.09], p<0.0005) (Ang et al., 2018 [20]) (>$6000: OR=1.59 [1.17; 2.17], p=0.002) (Ang et al., 2017 [21]) |
2 | |||
| Marital status | Married (aOR=0.61 [0.44; 0.86], p=0.005) (Ang et al., 2017 [21]) | Separated, divorced or widowed (aOR=2.53, 95% CI 1.16–5.54, p=0.020) (Ang et al., 2018 [20]) |
2 | ||
| Smoking status | Being a tobacco smoker (PR = 0.69, 95% CI = 0.48–0.98; p = 0.04) (Trent et al., 2020) | Being an ex-smoker compared to non-smoker or smoker (71.2 (95% CI 70.6-71.8, p < 0.001)) (Frank et al., 2020) [27] | 2 | ||
| Education | Higher education level (A-level/diploma/degree) (aOR=1.56 [1.08; 2.27] p=0.019) (Ang et al., 2018 [20]) | 1 | |||
| Employment status | Working in the last 12 months (aOR=0.72 [0.59; 0.89], p=0.002) (Ang et al., 2017 [21]) | 1 | |||
| Housing type | Lived in wealthier house types 4–5 room flats or condominiums: (OR: 1.28, p< 0.05) compared to those who lived in less wealthy house types (e.g.: 1–3 room flats) (Tan et al., 2022 [35]) |
1 | |||
| Ethnicity | Indian (OR: 0.66, p< 0.05) (Tan et al., 2022 [35]) | 1 | |||
| Engagement in physical activity | Sufficient total physical activity (aOR=3.04 [2.38-3.90], p<0.0005) (Ang et al., 2017 [21]) | 1 | |||
| Attitudes and beliefs | |||||
| Perceived benefits of vaccine |
Qualitative findings: Benefits of vaccination in relation to health, longevity (Graham et al., 2022) [28]; Hamilton et al., 2022 [29]) Individual and community protection (Kaufman et al., 2022 [31]; Lupton et al., 2022 [32]) Having personal freedoms that one would gain from vaccination (e.g.: freedom to travel, socialise) (Hamilton et al., 2022 [29]; Kaufman et al., 2022 [31]) |
Qualitative findings: Protect oneself from influenza infection (Teo et al., 2019 [18]) Believed that vaccine contains vitamins (Cummings et al., 2020 [25]) Belief that vaccine can lead to having a stronger body, being able to eat anything without fear of falling ill and that prevention is better than cure (Ho et al., 2017 [30]) |
7 | ||
| Perceived vaccine safety |
Qualitative findings: Belief that vaccine is not safe (Graham et al., 2022; Hamilton et al., 2022) Fear of short- and/or long-term side effects (Kaufman et al., 2022) |
Qualitative findings: Worry of side effects and pain (Teo et al., 2019 [18]; Cummings et al., 2020; Ho et al., 2017 [30]) and that it could affect their ability to work (Teo et al., 2019 [38]) Vaccine would weaken bodies (Ho et al., 2017 [30]) |
Qualitative findings: Trust in safety of vaccines (Teo et al., 2019 [18]) |
6 | |
| Social responsibility | Adult populations without regular contact with young children (Bayliss et al., 2021) Being a healthcare worker: (OR: 0.5 (95% CI 0.3-0.8) (for general vaccine); OR: 0.5 (95% CI 0.3-0.8) (for SARS- CoV- 2 vaccines)) (Enticott et al., 2018) |
Individuals in close contact with children <5 years old (parents, grandparents and carers of children). Mothers and grandmothers consistently reported higher rates of pertussis vaccination than fathers and grandfathers (Bayliss et al., 2021)[22] Qualitative findings: Concern for the health and livelihood of grandchildren and other family members pervaded the data, followed by responsibility for the community in general (Briggs et al., 2019)[24] Protecting people in the public and having a moral obligation to be vaccinated. (“safety of everyone else”, “protection of others”) (Hamilton et al., 2022) [29] |
Qualitative findings: Protecting loved ones (Teo et al., 2019 [18]) |
5 | |
| Trust | General distrust of vaccines (PR = 0.50; 95% CI = 0.28–0.89; p = 0.02) (Trent et al., 2020) |
Qualitative findings Lack of trust in governments (Graham et al., 2022)[28] |
Qualitative findings: Mistrust in doctor’s advice (Teo et al., 2019 [18]) Do not trust doctors - doctors may held profit interests (Cummings et al., 2020 [25]) |
Trust in formal sources of information government sources, local news on television and local news on the radio (OR: 1.28; p < .001) were significantly more likely to have received at least 1 dose of the COVID-19 vaccine in June 2021 (Tan et al., 2022 [35]) |
5 |
| Perceived susceptibility | Low perceived susceptibility to disease (PR = 0.73; 95% CI = 0.58–0.92; p = 0.01) (Trent et al., 2020) |
High perceived severity to disease (PR = 1.62; 95% CI = 1.29–2.95; p < 0.01). (Trent et al., 2020) [36] Belief that they had a health condition that would increase their risk of pneumonia (PR = 1.79; 95% CI = 1.47–2.18; p < 0.01) (Trent et al., 2020) Qualitative findings: High perceived severity to disease (Lupton et al., 2022)[32] |
Qualitative findings: Perceived low risk to getting influenza. This was reinforced by previous encounters with mild episodes of influenza (Teo et al., 2019 [18]) |
Qualitative findings: Perceived vulnerability was evidenced by frequent influenza episodes previously and the notion that a vaccine would reduce the severity of infection (Teo et al., 2019 [18]) Belief that pneumonia is an illness that is more serious than influenza (Ho et al., 2017 [30]) |
4 |
| Perceived effectiveness of vaccine | Positive perception of the effectiveness of vaccine (Burke et al., 2021 [23]; Enticott et al., 2018 [26]) (PR = 4.37; 95% CI = 2.05–9.32; p < 0.01) (Trent et al., 2020 [36]) (OR=14.6 (95% CI 10.9 to 19.5) for general vaccine and 14.0 (95% CI 10.4 to 18.9) for SARS- CoV- 2 vaccine) (Enticott et al., 2018 [26]) |
3 | |||
| Personal health beliefs and practices | A preference to develop immunity ‘naturally’ (PR = 0.37; 95% CI = 0.24–0.57; p < 0.01) (Trent et al., 2020) Use of naturopath/herbalist or other alternative health practitioners (p < 0.05; OR = 0.78; 95% CI: 0.65, 0.93) (Wardle et al., 2017) Having practiced yoga often: influenza vaccination (p < 0.05; OR = 0.79; 95% CI: 0.66, 0.95) pneumococcal vaccination (p < 0.05; OR = 0.78; 95% CI: 0.60, 1.02) (Wardle et al., 2017) |
Use of vitamins/minerals: Use at least sometimes (OR = 1.17; 95% CI: 1.00, 1.36) or often (1.22; 95% CI: 1.08, 1.38) were more likely to have received the influenza vaccination. Use vitamins often (OR = 1.24; 95% CI: 1.06, 1.44) were more likely to have received a pneumococcal vaccination (Wardle et al., 2017 [37]) |
Qualitative findings: Dislike for taking any form of medication (Cummings et al., 2020 [25]) |
3 | |
| Perceived severity |
Qualitative findings: Believed that influenza is not a serious illness which warranted a vaccine (Teo et al., 2019 [18]) |
1 | |||
| Perceived importance of being vaccinated |
Qualitative findings: There are more pressing issues such as other chronic health problems and heavy work commitments (Teo et al., 2019 [18]) |
1 | |||
| Religion |
Qualitative findings: Religious objections (Cummings et al., 2020 [25]) |
1 | |||
| Fatalism |
Qualitative findings: Perceived inevitability of illness in old age and belief in predestination (Teo et al., 2019 [18]) |
1 | |||
| Interpersonal | |||||
| Social influences |
Qualitative findings Health practitioners acted as deterrents to vaccine uptake behaviours (Briggs et al., 2019) |
Recommendation to go for vaccine from doctor (PR = 10.25; 95% CI = 6.06–17.33; p < 0.01) (Trent et al., 2020 [36]) Qualitative findings Recommendation to go for vaccine from doctor (Kaufman et al., 2022 [31]; Briggs et al., 2019 [24]; Hamilton et al., 2022 [29]) |
Qualitative findings: Lack of advice and encouragement from healthcare workers (Teo et al., 2019 [18]; Cummings et al., 2020 [25]) Lack of encouragement from family members (Teo et al., 2019 [18]) Vaccine was deemed unnecessary as surrounding low vaccine uptake rates is low (Teo et al., 2019 [18]) |
Qualitative findings: Encouragement from friends and family (Teo et al., 2019 [18]; Cummings et al., 2020 [25]; Ho et al., 2017 [30]) Family and friends also helped to remind participants to have annual vaccination (Teo et al., 2019) Encouragement from both doctors and nurses (Teo et al., 2019; Ho et al., 2017) |
8 |
| Having a regular family doctor/GP | Having a regular family doctor/GP: (aOR=1.28 [1.06; 1.55], p=0.012) (Ang et al., 2017 [21]) (aOR=2.19 [1.67; 2.88]) (Ang et al., 2018 [20]) |
2 | |||
| Community | |||||
| Socio-economic status | Living in low SES area: (Frank et al., 2020); (aOR = 0.7, (0.6–0.8)) (Lin et al., 2020)) | Living in higher SES area; residing in the least disadvantaged areas SES quintile (OR: 2.1 (95% CI 1.4-3.2) for general vaccine and (OR: 2.7, 95% CI 1.5-3.4) for SARSCoV- 2 vaccines (Enticott et al., 2018 [26]) | 3 | ||
| Locality | Pneumococcal vaccine uptake among patients was lower among general practices located in outer/remote/very remote areas compared to inner regional or major cities: (95% CI 64.9-7.4) (Frank et al., 2020); (Lin et al., 2020)) |
Coverage also varied by remoteness status and was highest in major cities (aOR = 0.7, (0.6–0.8), p < 0.05.) (Lin et al., 2020 [33]) | 2 | ||
| Access to vaccine | Vaccines are easily available (Burke et al., 2021 [23]) |
Qualitative findings: Inconvenient to travel to vaccine site and the long waiting hours at polyclinics (Cummings et al., 2020 [25]) |
2 | ||
| Complying to regulations |
Qualitative findings: Complying with official recommendation to vaccinate before travel (Teo et al., 2019 [18]) |
1 | |||
| Vaccine-related | |||||
| Vaccine procedure |
Qualitative findings: Fear of injections (Teo et al., 2019 [18]; Cummings et al., 2020 [25]) |
2 | |||
| Cost |
Qualitative findings: Expensive (Ho et al., 2017 [30]) |
1 | |||
Effectiveness of interventions for promoting vaccination uptake
Interventions that focused on supporting doctors, such as creating awareness on the low baseline vaccination rates among older adults [40] and facilitating doctors in providing structured health assessment [39], led to vaccination uptake among patients. Nurse reminders for patients to go for vaccination can also increase vaccination uptake [40]. While financial strategies such as providing monetary incentives (SGD20 = USD 14.70 ) could improve influenza vaccination uptake, increasing the amount (to SGD 30 = USD 22) was reported to be ineffective. However, this finding was reported to be different for older adults who were working and not working, with the former not sensitive to the increased amount offered given the time barrier to go for vaccination [41]. Lastly, the intervention of engaging consumers through provision of informational flyers and posters was found to have mixed effectiveness [38,40]. Table 3 provides an overview of the interventions and their effectiveness.
Table 3.
Effectiveness of interventions for promoting vaccination uptake among older adults.
| Intervention category (Intervention description) | Effective | Not effective | No of studies (out of 4) |
|---|---|---|---|
| Engage consumers (Involving, preparing, and intervening with patients and the market to involve them and increase demand for the clinical innovation) | Patients who visited the clinic during the intervention (informational flyers and posters) period were more likely to receive influenza vaccination (AOR=1.43; 95% CI=0.99, 2.07; P=.06) than were those who visited during the control period. They were also more likely to receive pneumococcal vaccination (AOR=1.78; 95% CI=1.28, 2.48; P< .01) (Ho et al., 2019 [38]). An additional 34 patients (12.1%) received their vaccinations as a result of nurses’ reminders (Li et al., 2019 [40])* |
None of the patients attributed their updated vaccination status to the patient education posters (Li et al., 2019 [40])* | 3 |
| Support clinicians (Supporting clinical staff performance) | When structured health assessments were provided, patients eligible for free vaccine were more likely to receive a zoster vaccine (adjusted OR = 3.0; 95% CI: 2.8–3.2) than in encounters where this health assessment was not provided (Lin et al., 2022 [39]). While the vaccination card reminders on the computers and the newly minted electronic health record system influenced practices, the main impetus for change was the realisation that current vaccination rates were low (intervention: department briefing to the physicians was conducted highlighting the baseline influenza vaccination rates (Li et al., 2019 [40])* |
2 | |
| Use financial strategies (Changing the patient billing systems, fee structures, reimbursement policies, research funding, and clinician incentives) | Increasing the total monetary incentive for vaccination and reporting from 10 to 20 SGD increased participation in vaccination from 4.5% to 7.5% (P<0.001) (Yue et al., 2020 [41]) | 1 |
*The study by Li et al., 2019 is a multifaceted intervention study which comprised of several discrete strategies including education posters, vaccination card reminders, utilising electronic healthcare record system, department briefing to the physicians, and nurse reminders. Overall, the entire intervention was effective at improving vaccination (Baseline influenza vaccination rate among the preintervention group was 47.7% (166 out of 348 patients). In the post-intervention group, the influenza vaccination rate improved significantly to 80.7% (281 out of 348 patients) (p<0.001) [40].
Discussions
This rapid review presents a thorough overview of barriers and facilitator or factors influencing uptake of vaccinations among older people aged 50 years and older in Australia and Singapore. The more prevalent factors influencing vaccine uptake among older adults found in this review were related to interpersonal (social influences), attitudes (perceived benefits of vaccine, perceived vaccine safety, social responsibility, trust), and individual characteristics (age, sex, knowledge). Apart from this, strategies that were found to be effective in improving vaccine uptake was also reported and these were to engage consumers, support clinicians, and use financial strategies.
The majority of the findings of this review are similar to two reviews conducted among older adults in the Western societies (Europe and North America), where income, education level, living in deprived areas [42], attitudes and beliefs regarding vaccination, healthcare providers’ and family and friends’ influences, vaccine’s side effects and effectiveness, perceived susceptibility [17] were found to be key factors influencing vaccine uptake. This indicates that many of the factors influencing vaccine uptake among older adults are universal among high-income countries that have clear guidance on these vaccines in their national immunization schedules. Australia and Singapore provide vaccines free of costs, or subsidised vaccines for older adults. Australia’s National Immunization Program also provides clear guidance for adult vaccines. Under the program, free vaccines are provided for adults and seniors. These include pneumococcal, influenza and shingles vaccines [43]. As a result, 74.6% of the population aged 65 years and above were vaccinated against seasonal influenza and 54.4% against pneumococcal disease in 2009. Singapore’s National Adult Immunisation Schedule (NAIS) provides guidance on 11 important vaccinations for adults. MEDISAVE, the national medical savings scheme, can be used to pay for vaccinations recommended under the NAIS [44]. Since the introduction of this scheme, around 24% of adults between 65 to 79 took up the vaccinations [45]. Singapore is currently implementing a new strategy aimed at healthy ageing in 2023, which will provide full subsidies for vaccines for older adults [46].
The finding of this review adds to the body of literature on effective interventions in increasing vaccination uptake rates among countries in the Asia-Pacific region. In addition to interventions that have been found to be effective in other countries in Asia-Pacific such as government-funded vaccination programs (Japan, Korea and Australia, China), provider-led education (i.e., face-to-face discussions about vaccination) (China and Hong Kong), recommendation from a provider to be vaccinated (Japan and China), and expanding vaccination sites and vaccinators that were evidenced to increase vaccination rates (Japan, Korea) [9], this review shows that using informational flyers and posters, nurse reminders, highlighting the baseline influenza vaccination rates among HCPs, and having structured health assessments could also increase vaccination uptake. The barriers and facilitators identified in this study such as perceived benefits of vaccine, perceived vaccine safety, trust, and knowledge indicates that investing in educational strategies is the key to promote vaccination uptake among older adults in Australia and Singapore. Other educational intervention such as pharmacist-led interventions have been shown to be effective in increasing vaccination uptake [47,48].
In this review, social influences was the most commonly reported factor influencing vaccine uptake among older adults. Healthcare providers, family, friends and the community can affect older person’s decision on whether to go for vaccination. In the Asian setting, this is not surprising as older people tend to defer their health decision making to physicians and children, whom they see as more knowledgeable [49]. Strategies to promote vaccine uptake that leverage on social influences should be developed especially getting healthcare providers to encourage older people to go for vaccinations. This current review highlighted that nurse reminders was effective in getting older adults to go for vaccination [40]. HCP’s recommendation has consistently shown to be the strongest motivator to encourage vaccination [17,50,51]. However, HCPs faced a myriad of challenges to offer vaccination (Srivastav, 2018). Strategies such as provider education with or without the support of a designated immunisation champion, implementation of a recall/reminder through clinical decision support system, or collaboration through public-private collaboration were reported to be effective solutions to address HCP’s challenges to offer vaccination [8]. This current review also highlighted that having structured health assessment for HCPs was effective in getting older adults to go for free vaccination [39].
One of the lesser reported factors influencing vaccination uptake in the literature is religion. In the review by Jain et al., 2017, religion as a factor influencing vaccine uptake was only studied in two studies, in which both showed inconsistent findings [42]. In this current review, religious objection was reported as a barrier to influenza vaccine uptake in a Singapore study. Asia-Pacific, where Hindus, Muslims, and Buddhists formed the larger religious groups in the region, religion plays an important role in influencing one’s way of life, including health decision making such as vaccination uptake. Among the more prominent religious barriers to vaccinations were related to concern of ingredients content of vaccines for Muslims, and religious taboos among Hinduism and Sikhism [52]. Religion tends to become more important as an individual gets older [53], and given the increasing ageing population in various countries in Asia-Pacific such as Singapore, more studies are needed to determine if religion is a determinant to vaccination uptake among older adults.
This review has several strengths. This review is the first review that provides an overview of barriers and facilitators, and effective interventions that can promote vaccine uptake among older adults in the Asia-Pacific setting. Despite being a rapid review, the process of appraising the quality of the studies to be included in the review was conducted to ensure quality studies are included. This findings of this review needs to be interpreted with caution. Firstly, the studies within this review were only from Australia and Singapore. Only two databases were used, and only five years were applied when searching for relevant literature. This could have led to the lack of comprehensiveness in the search that might have resulted in missed studies. This may also be the reason why studies from Indonesia and Philippines were not found. Secondly, the significance of each factor presented by comparing their presence as significant and non-significant findings in the studies may not truly reflect the most crucial factor, given that only number of studies were calculated rather than performing a meta-analysis due to the insufficient number of studies, and the diversity of the study designs. Thirdly, only studies in English was included, which may have excluded some data.
Conclusion
This review highlighted the major factors influencing older people’s uptake of vaccination in Singapore and Australia, and they were interpersonal, attitudes, and individual characteristics. While strategies such as engage consumers, support clinicians, and financial incentives were found to be effective, strategies that target the major influencing factors identified should also be considered. More studies are needed ascertain the relative importance of the factors influencing vaccine uptake among older people in the Asia-Pacific region.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Search strategy; Table S2: Study appraisal.
Author Contributions
Conceptualization, WTT, AS, MPEN, SCT, SEO, JYSY; Methodology, WTT, AS, MPEN, SCT, SEO, JYSY; Software, WTT, AS, MPEN, SCT, AL; validation, WTT, AS, MPEN, SCT, AL, TYTC, SEO, JYSY; formal analysis, WTT, AS, MPEN, SCT, AL; investigation, WTT, AS, MPEN, SCT, AL; data curation, WTT, AS; writing—original draft preparation, WTT, AS; writing—review and editing, WTT, AS, TYTC, JYSY; visualization, X.X.; WTT, AS, TYTC; project administration, WTT, AS; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding, and the APC was funded by the.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results”.
References
- World Health Organisation. WHO's work on the UN Decade of Healthy Ageing (2021–2030) 2023 [Available from: https://www.who.int/initiatives/decade-of-healthy-ageing.
- United Nations Economic and Social Commission for Asia and the Pacific. Population ageing: A human success story 2023 [Available from: https://www.population-trends-asiapacific.org/population-ageing.
- United Nations ESCAP. Addressing the Challenges of Population Ageing in Asia and the Pacific. Bangkok; 2017.
- Seth, A., Pangestu, T. Promoting older adults immunisation. A pathway to healthy ageing in Asia Pacific. 2022.
- Bhanu, C., Gopal, D.P., Walters, K., Chaudhry, U.A.R. Vaccination uptake amongst older adults from minority ethnic backgrounds: A systematic review. PLoS Med. 2021, 18(11), e1003826. [CrossRef]
- Kan, T., Zhang, J. Factors influencing seasonal influenza vaccination behaviour among elderly people: a systematic review. Public Health. 2018, 156, 67-78. [CrossRef]
- Nguyen, M.H., Li Chen, L., Lim, K.W., Chang, W.T., Mamun, K. Vaccination in Older Adults in Singapore: A Summary of Recent Literature. Proceedings of Singapore Healthcare. 2015, 24(2), 94-102. [CrossRef]
- Bach, A.T., Kang, A.Y., Lewis, J., Xavioer, S., Portillo, I., Goad, J.A. Addressing common barriers in adult immunizations: a review of interventions. Expert Rev Vaccines. 2019, 18(11), 1167-85. [CrossRef]
- Eiden, A.L., Barratt, J., Nyaku, M.K. A review of factors influencing vaccination policies and programs for older adults globally. Hum Vaccin Immunother. 2023, 19(1), 2157164. [CrossRef]
- United Nations. Ageing in the Asian and Pacific Region: An overview. Bangkok; 2017.
- The World Bank. Population ages 65 and above (% of total population) - Malaysia, Singapore, Thailand, Vietnam, Philippines, Indonesia 2019 [Available from: https://data.worldbank.org/indicator/SP.POP.65UP.TO.ZS?contextual=default&end=2019&locations=MY-SG-TH-VNPH-ID&start=2019&view=bar.
- Western Pacific Pharmaceutical Forum. The Decade of Healthy Ageing in ASEAN: Role of Life-course Immunisation. 2019.
- Garritty, C., Gartlehner, G., Nussbaumer-Streit, B., King, V.J., Hamel, C., Kamel, C., Affengruber, L., Stevens, A. Cochrane Rapid Reviews Methods Group offers evidence-informed guidance to conduct rapid reviews. J Clin Epidemiol. 2021, 130, 13-22. [CrossRef]
- Australia Department of Health and Aged Care. Immunisation for adults 2023 [Available from: https://www.health.gov.au/topics/immunisation/when-to-get-vaccinated/immunisation-for-adults.
- Ministry of Health Singapore. Expert committee on Covid-19 vaccination recommends a booster dose of MRNA Covid-19 vaccine for persons aged between 50 and 59 years, six months after completion of their primary series 2021 [Available from: https://www.moh.gov.sg/news-highlights/details/expert-committee-on-covid-19-vaccination-recommends-a-booster-dose-of-mrna-covid-19-vaccine-for-persons-aged-between-50-and-59-years-six-months-after-completion-of-their-primary-series_24September2021.
- Hong, Q.N. , Pluye, P., Fàbregues, S., Bartlett, G., Boardman, F., Cargo, M., Dagenais, P., Gagnon, M.P., Griffiths, F., Nicolau, B., et al. Mixed Methods Appraisal Tool (MMAT) v2018. 2018.
- Eilers, R., Krabbe, P.F., de Melker, H.E. Factors affecting the uptake of vaccination by the elderly in Western society. Prev Med. 2014, 69, 224-34. [CrossRef]
- Teo, L.M., Smith, H.E., Lwin, M.O., Tang, W.E. Attitudes and perception of influenza vaccines among older people in Singapore: A qualitative study. Vaccine. 2019, 37(44), 6665-72. [CrossRef]
- Waltz, T.J., Powell, B.J., Matthieu, M.M., Damschroder, L.J., Chinman, M.J., Smith, J.L., Proctor, E.K., Kirchner, J.E. Use of concept mapping to characterize relationships among implementation strategies and assess their feasibility and importance: results from the Expert Recommendations for Implementing Change (ERIC) study. Implementation Science. 2015, 10(1), 109. [CrossRef]
- Ang, L.W., Cutter, J., James, L., Goh, K.T. Epidemiological characteristics associated with uptake of pneumococcal vaccine among older adults living in the community in Singapore: Results from the National Health Surveillance Survey 2013. Scandinavian journal of public health. 2018, 46(2), 175-81. [CrossRef]
- Ang, L.W., Cutter, J., James, L., Goh, K.T. Factors associated with influenza vaccine uptake in older adults living in the community in Singapore. Epidemiology and Infection. 2017, 145(4), 775-86. [CrossRef]
- Bayliss, J., Randhawa, R., Oh, K.B., Kandeil, W., Jenkins, V.A., Turriani, E., Nissen, M. Perceptions of vaccine preventable diseases in Australian healthcare: focus on pertussis. Hum Vaccin Immunother. 2021, 17(2), 344-50. [CrossRef]
- Burke, P.F., Masters, D., Massey, G. Enablers and barriers to COVID-19 vaccine uptake: An international study of perceptions and intentions. Vaccine. 2021, 39(36), 5116-28. [CrossRef]
- Briggs, L., Fronek, P., Quinn, V., Wilde, T. Perceptions of influenza and pneumococcal vaccine uptake by older persons in Australia. Vaccine. 2019, 37(32), 4454-9. [CrossRef]
- Cummings, C.L., Kong, W.Y., Orminski, J. A typology of beliefs and misperceptions about the influenza disease and vaccine among older adults in Singapore. PLoS One. 2020, 15(5), e0232472. [CrossRef]
- Enticott, J., Gill, J.S., Bacon, S.L., Lavoie, K.L., Epstein, D.S., Dawadi, S., Teede, H.J., Boyle, J. Attitudes towards vaccines and intention to vaccinate against COVID-19: a cross-sectional analysis - implications for public health communications in Australia. BMJ Open. 2022, 12(1). [CrossRef]
- Frank, O., De Oliveira Bernardo, C., González-Chica, D.A., Macartney, K., Menzies, R., Stocks, N. Pneumococcal vaccination uptake among patients aged 65 years or over in Australian general practice. Human Vaccines and Immunotherapeutics. 2020, 16(4), 965-71. [CrossRef]
- Graham, S., Blaxland, M., Bolt, R., Beadman, M., Gardner, K., Martin, K., Doyle, M., Beetson, K., Murphy, D., Bell, S., et al. Aboriginal peoples' perspectives about COVID-19 vaccines and motivations to seek vaccination: a qualitative study. BMJ Global Health. 2022, 7(7). [CrossRef]
- Hamilton, E.M., Oversby, S., Ratsch, A., Kitchener, S. COVID-19 Vaccination: An Exploratory Study of the Motivations and Concerns Detailed in the Medical Records of a Regional Australian Population. Vaccines. 2022, 10(5). [CrossRef]
- Ho, H.J., Chan, Y.Y., Ibrahim, M.A.B., Wagle, A.A., Wong, C.M., Chow, A. A formative research-guided educational intervention to improve the knowledge and attitudes of seniors towards influenza and pneumococcal vaccinations. Vaccine. 2017, 35(47), 6367-74. [CrossRef]
- Kaufman, J., Bagot, K.L., Tuckerman, J., Biezen, R., Oliver, J., Jos, C., Ong, D.S., Manski-Nankervis, J.A., Seale, H., Sanci, L., et al. Qualitative exploration of intentions, concerns and information needs of vaccine-hesitant adults initially prioritised to receive COVID-19 vaccines in Australia. Aust N Z J Public Health. 2022, 46(1), 16-24.
- Lupton, D. Understandings and practices related to risk, immunity and vaccination during the Delta variant COVID-19 outbreak in Australia: An interview study. Vaccine: X. 2022, 11. [CrossRef]
- Lin, J., Wood, J.G., Bernardo, C., Stocks, N.P., Liu, B. Herpes zoster vaccine coverage in Australia before and after introduction of a national vaccination program. Vaccine. 2020, 38(20), 3646-52. [CrossRef]
- Moosa, A.S., Wee, Y.M.S., Jaw, M.H., Tan, Q.F., Tse, W.L.D., Loke, C.Y., Ee, G.L.A., Ng, C.C.D., Aau, W.K., Koh, Y.L.E., et al. A multidisciplinary effort to increase COVID-19 vaccination among the older adults. Frontiers in public health. 2022, 10, 904161. [CrossRef]
- Tan, M., Straughan, P.T., Cheong, G. Information trust and COVID-19 vaccine hesitancy amongst middle-aged and older adults in Singapore: A latent class analysis Approach. Social Science and Medicine. 2022, 296. [CrossRef]
- Trent, M.J., Salmon, D.A., MacIntyre, C.R. Predictors of pneumococcal vaccination among Australian adults at high risk of pneumococcal disease. Vaccine. 2022, 40(8), 1152-61. [CrossRef]
- Wardle, J., Frawley, J., Adams, J., Sibbritt, D., Steel, A., Lauche, R. Associations between complementary medicine utilization and influenza/pneumococcal vaccination: Results of a national cross-sectional survey of 9151 Australian women. Preventive Medicine. 2017, 105, 184-9. [CrossRef]
- Ho, H.J., Tan, Y.R., Cook, A.R., Koh, G., Tham, T.Y., Anwar, E., Hui Chiang, G.S., Lwin, M.O., Chen, M.I. Increasing Influenza and Pneumococcal Vaccination Uptake in Seniors Using Point-of-Care Informational Interventions in Primary Care in Singapore: A Pragmatic, Cluster-Randomized Crossover Trial. American journal of public health. 2019, 109(12), 1776-83. [CrossRef]
- Lin, J., Dobbins, T., Wood, J.G., Hall, J.J., Liu, B. Impact of a structured older persons health assessment on herpes zoster vaccine uptake in Australian primary care. Preventive Medicine. 2022, 155. [CrossRef]
- Li, A., Chan, Y.H., Liew, M.F., Pandey, R., Phua, J. Improving Influenza Vaccination Coverage Among Patients With COPD: A Pilot Project. Int J Chron Obstruct Pulmon Dis. 2019, 14, 2527-33. [CrossRef]
- Yue, M., Wang, Y., Low, C.K., Yoong, J.S.Y., Cook, A.R. Optimal Design of Population-Level Financial Incentives of Influenza Vaccination for the Elderly. Value in Health. 2020, 23(2), 200-8. [CrossRef]
- Jain, A., van Hoek, A.J., Boccia, D., Thomas, S.L. Lower vaccine uptake amongst older individuals living alone: A systematic review and meta-analysis of social determinants of vaccine uptake. Vaccine. 2017, 35(18), 2315-28. [CrossRef]
- Australian Government Department of Health and Aged. Immunisation for Adults and Seniors: Australian Government Department of Health and Aged Care; 2017 [Available from: https://www.health.gov.au/health-topics/immunisation/when-to-get-vaccinated/immunisation-for-adults-and-seniors.
- Ministry of Health Singapore. Nationally Recommended Vaccines 2021 [Available from: https://www.moh.gov.sg/resources-statistics/nationally-recommended-vaccines.
- Ministry of Health Singapore. Adult immunisation vaccinations take-up rate 2020 [Available from: https://www.moh.gov.sg/news-highlights/details/adult-immunisation-vaccinations-take-up-rate.
- Ministry of Health Singapore. White paper on healthier SG. Singapore; 2022.
- Abu-Rish, E.Y., Barakat, N.A. The impact of pharmacist-led educational intervention on pneumococcal vaccine awareness and acceptance among elderly in Jordan. Hum Vaccin Immunother. 2021, 17(4), 1181-9. [CrossRef]
- Pizzi, L.T., Prioli, K.M., Fields Harris, L., Cannon-Dang, E., Marthol-Clark, M., Alcusky, M., McCoy, M., Schafer, J.J. Knowledge, Activation, and Costs of the Pharmacists' Pneumonia Prevention Program (PPPP): A Novel Senior Center Model to Promote Vaccination. Ann Pharmacother. 2018, 52(5), 446-53.
- Dutta, O., Lall, P., Patinadan, P.V., Car, J., Low, C.K., Tan, W.S., Ho, A.H.Y. Patient autonomy and participation in end-of-life decision-making: An interpretive-systemic focus group study on perspectives of Asian healthcare professionals. Palliat Support Care. 2020, 18(4), 425-30. [CrossRef]
- Kamimura, A., Trinh, H.N., Weaver, S., Chernenko, A., Wright, L., Stoddard, M., Nourian, M.M., Nguyen, H. Knowledge and beliefs about HPV among college students in Vietnam and the United States. J Infect Public Health. 2018, 11(1), 120-5. [CrossRef]
- Magee, L., Knights, F., McKechnie, D.G.J., Al-Bedaery, R., Razai, M.S. Facilitators and barriers to COVID-19 vaccination uptake among ethnic minorities: A qualitative study in primary care. PLoS One. 2022, 17(7), e0270504. [CrossRef]
- Sheikh, A., Iqbal, B., Ehtamam, A., Rahim, M., Shaikh, H.A., Usmani, H.A., Nasir, J., Ali, S., Zaki, M., Wahab, T.A., et al. Reasons for non-vaccination in pediatric patients visiting tertiary care centers in a polio-prone country. Arch Public Health. 2013, 71(1), 19. [CrossRef]
- Malone, J., Dadswell, A. The Role of Religion, Spirituality and/or Belief in Positive Ageing for Older Adults. Geriatrics (Basel). 2018, 3(2). [CrossRef]
Table 1.
Characteristics of studies reviewed.
| No | Author, year of publication (reference no) | Country where the study was conducted | Vaccine | Setting | Study population | Study design | Data analysis |
|---|---|---|---|---|---|---|---|
| Studies that identified factors related to vaccination uptake among older adults | |||||||
| 1 | Ang et al., 2018 [20] |
Singapore | Pneumococcal | Community | n=3672 Individuals ≥50 years |
Cross-sectional | Multivariate logistic regression |
| 2 | Ang et al., 2017 [21] | Singapore | Influenza | Community | n=3700 Individuals >50 years |
Cross-sectional (Retrospective analysis of the 2013 National Health Surveillance Survey (NHSS) | Multivariate logistic regression |
| 3 | Bayliss et al., 2021 [22] |
Australia | Pertussis | Community | n=6529 Individuals ≥50 years |
Cross-sectional (online survey) | t-tests, Wilcoxon Rank Sum, Fisher’s exact test, ANOVA, Kruskal-Wallis tests |
| 4 | Burke et al., 2021 [23] |
Multicountry study: Australia, United States, England, Canada, New Zealand |
Covid-19 | Community | n=1678 (Australian respondents) Median adult age for the Australian sample is 59.5 years |
Cross-sectional | Exploratory factor analysis (EFA), confirmatory factor analysis (CFA) |
| 5 | Briggs et al., 2019 [24] | Australia | Influenza & Pneumococcal | Community | n=36 Individuals ≥65 years |
Qualitative study | Thematic analysis |
| 6 | Cummings et al., 2020 [25] |
Singapore | Influenza | Community | n=76 Individuals ≥65 years |
Qualitative study | Grounded theory |
| 7 | Enticott et al., 2018 [26] |
Australia | Covid-19 | Community | n=1158 Mean age of participants is 52 years |
Cross-sectional (online survey) | Multivariate logistic regression |
| 8 | Frank et al., 2020 [27] |
Australia | Pneumococcal | Electronic medical records: Hospital/clinic | n=58549 Individuals age between 60-65 years |
Retrospective cohort analysis | Logistic regression |
| 9 | Graham et al., 2022 [28] |
Australia | COVID-19 | Community | n=35 Aboriginal and/or Torres Strait Islanders age ranged from 15-80 years old |
Qualitative study | Thematic analysis |
| 10 | Hamilton et al., 2022 [29] |
Australia | Covid-19 | Clinic | n=102 (<50=6; 50–59=13, 60–69=42, 70–79=28, ≥80=13) 80 % of study population is more than 60 years old |
Qualitative study | Thematic analysis |
| 11 | Ho et al., 2017 [30] |
Singapore | Influenza & Pneumococcal | Community | n=32 Individuals ≥60 years |
Mixed-method study Qualitative study in a larger intervention study |
Logistic regression model Thematic analysis |
| 12 | Kaufman et al., 2022 [31] |
Australia | Covid-19 | Community | n=19 Individuals aged ≥70 years |
Qualitative study | Descriptive thematic analysis |
| 13 | Lupton., 2022 [32] |
Australia | Covid-19 | Community | n=20 Individuals ≥50 years |
Qualitative study | Thematic analysis |
| 14 | Lin et al., 2020 [33] |
Australia | Herpes Zoster | Electronic medical records: Clinic | n=52,229 (2016 cohort), N=55,034 (2017 cohort), and N=57,316 (2018 cohort) Individuals age between 50-90 years |
Retrospective cohort study | Multivariate logistic regression |
| 15 | Moosa et al., 2022 [34] |
Singapore | Covid-19 | Community | n=21663 Unvaccinated older adults ≥60 years |
Cohort study | Descriptive analysis |
| 16 | Tan et al., 2022 [35] |
Singapore | Covid-19 | Community | n=6094 Individuals aged 56-75 years old |
Cross sectional study (Retrospective analysis of data from the Singapore Life Panel population survey of Singaporeans aged 56–75) | Logistic regression |
| 17 | Trent et al., 2020 [36] |
Australia | Pneumococcal | Community | n=744 Individuals ≥65 years |
Cross-sectional (Retrospective analysis of three surveys: The Australian Adult Immunisation Survey, BREATH study, and survey on mask use during the COVID-19 pandemic (MUS). | Modified Poisson regression |
| 18 | Teo et al., 2019 [18] |
Singapore | Influenza | Clinic | n=15 Individuals aged 66-85 years |
Qualitative study | Thematic analysis |
| 19 | Wardle et al., 2017 [37] |
Australia | Influenza & Pneumococcal | Electronic medical records: Community | n=9151 Women age 62-67 years |
Cross-sectional (Retrospective analysis of the Australian Longitudinal Study on Women's Health (ALSWH) survey) |
Multivariate logistic regression |
| Studies that tested interventions for promoting uptake of vaccination among older adults | |||||||
| 22 | Ho et al., 2019 [38] |
Singapore | Influenza & Pneumococcal | Clinic | n=4378 Individuals ≥ 65 years (Intervention), 4459 (Control) |
A Pragmatic Cluster-Randomized Crossover Trial | Multilevel logistic regression |
| 20 | Lin et al., 2022 [39] |
Australia | Herpes Zoster | Clinic | n=31,876 Patients aged 75–79 years |
Retrospective analysis of data from the Australian national general practice electronic medical records | Generalized estimating equations for binary outcomes with logit link |
| 23 | Li et al., 2019 [40] |
Singapore | Influenza | Hospital | n=384 COPD patients. The mean age of the participants was 72.8 years |
Before–after study | Descriptive statistics, chi-square test |
| 21 | Yue et al., 2020 [41] |
Singapore | Influenza | Community | n=373 Individuals ≥ 65 years Arm 1: 166 Arm 2: 44 Arm 3: 73 Arm 4: 90 |
Randomised controlled experiment | Likelihood ratio test. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



