Submitted:
28 November 2023
Posted:
29 November 2023
You are already at the latest version
Abstract
(1) Background: This manuscript introduces the "Lines and Dots" (LAD) technique, a novel method for administering Botulinum Toxin Type A (BoNT-A) in treating horizontal forehead lines. This technique emphasizes precision in targeting nerve endplates, considering individual anatomical variations, and optimizing treatment efficacy. (2) Methods: The LAD technique focus on using the frontalis muscle contraction dynamics to identify the specific distribution of the supraorbital and supratrochlear nerves It involves creating a grid of predetermined lines and points on the forehead that align with nerve paths and motor endplate zones. (3) Results: By targeting injections along these precise lines and points, the LAD technique ensures more effective utilization of BoNT-A. This approach not only enhances the toxin's effect but also allows for a reduction in the overall dosage. The strategic placement of injections results in a more natural, symmetrical, and sustained therapeutic effect, ensuring an improved aesthetic outcome. (4) Conclusions: The LAD technique represents a significant advancement in the realm of cosmetic injectables. It offers a tailored, patient-specific approach, maximizing the effectiveness of BoNT-A injections for treating forehead lines while minimizing risks and enhancing patient satisfaction. This method underscores the importance of a deep anatomical understanding and precision in cosmetic procedures.
Keywords:
Botulinum Toxin Type A (BoNT-A)
; Cosmetic Dermatology
; Frontalis Muscle
; Forehead Lines
; Supraorbital Nerve
; Supratrochlear Nerve
1. Introduction
Horizontal forehead lines are among the most prominent signs of aging and can significantly affect an individual’s facial expressions and perceived emotions [1,2,3]. As a result, the aesthetic treatment of these lines is a common procedure within the field of cosmetic dermatology and plastic surgery [4,5,6].
Traditionally, these treatments have included a range of approaches from topical creams to more invasive techniques such as surgical lifts. However, the emergence of botulinum toxin type A (BoNT-A) injections has revolutionized this domain by offering a non-surgical, minimally invasive solution that can temporarily reduce the appearance of forehead wrinkles [7,8,9].
BoNT-A, a neurotoxin produced by Clostridium botulinum, acts by blocking the nerve signals responsible for muscle contraction, thereby smoothing the skin above the muscles and reducing the visibility of wrinkles. The frontalis muscle, extending across the forehead and responsible for raising the eyebrows, is the primary target in treating horizontal forehead lines [10]. Current BoNT-A formulations, including Onabotulinumtoxin-A (ONA; BoNT-A®), Abobotulinumtoxin-A (ABO; Dysport®), Prabotulinumtoxin-A (Nuceiva®), and Incobotulinumtoxin-A (INCO; Xeomin®), each have unique properties and applications in aesthetic treatments [11].
Despite its widespread use and generally high efficacy, BoNT-A treatment is not without its limitations. When not optimally applied, it can lead to undesirable effects such as asymmetry, an unnatural facial expression, or, in some cases, ptosis. To achieve optimal results, precision in the administration of BoNT-A is paramount [12,13]. This necessitates a deep understanding of an individual’s muscle anatomy and contraction patterns, especially the varied anatomical shapes of the frontalis muscle, which directly correlate with different forehead line patterns [14,15].
The frontalis muscle, part of the occipitofrontalis muscle complex, plays a crucial role in facial expressions, especially in the upper face. It originates from the galea aponeurotica and inserts into the skin above the supraorbital ridge [16]. This muscle facilitates the elevation of the eyebrows and the formation of horizontal rhytids (wrinkles). The supraorbital (SON) and supratrochlear (SOT) nerves, branches of the ophthalmic division of the trigeminal nerve, innervate the frontalis muscle. The SON and SOT nerves emerge from the supraorbital foramen and notch, respectively, providing sensory innervation to the forehead and the overlying scalp. The SON has four branches: deep, lateral, intermediate, and medial, While the SOT has two branches: medial and lateral [17,18] as shown in Figure 1.
BoNT-A’s efficacy is significantly enhanced when injected close to the nerve endplates [19,20,21]. These endplates are the regions where nerve terminals meet the muscle and are crucial for neurotransmitter release. By targeting these areas, BoNT-A can more effectively block the release of neurotransmitters, leading to better muscle relaxation. Identifying nerve endplates for BoNT-A injections may help optimize the efficacy and safety of the treatment. Here are several methods used to locate these nerve endplates. While Electromyography (EMG) can significantly enhance the precision of BoNT-A injections. However, their utility in the cosmetic field is considerably limited due to high cost [22,23,24].
To address this issue, we introduce the “Lines and Dots” technique, a novel method of BoNT-A application rooted in a detailed understanding of the frontalis muscle’s anatomy, the specific distribution of the supraorbital and supratrochlear nerves, and the dynamics of muscle contraction. The Lines and Dots (LAD) technique aims to deliver BoNT-A along predetermined lines and points that align with these nerve paths, targeting the muscle’s motor endplate zones. This strategic approach enhances the toxin’s effect while allowing for a reduction in the overall dosage, yielding a more natural, symmetrical, and sustained therapeutic effect, ensuring an improved aesthetic outcome for patients seeking treatment for horizontal forehead lines.
This technique also considers the significant variations in forehead structure between different ethnicities and genders, as well as the impact of aging processes like forehead flattening and skin elasticity loss. Furthermore, the shape and position of the eyebrows, key elements in expressing emotions and personality, are taken into account to ensure a more tailored and effective treatment.
2. Materials and Methods
2.1. Assessment Frontalis Muscle and Horizontal Lines
Before initiating the LAD technique, a comprehensive assessment is conducted for each patient to ensure optimal outcomes in the treatment of forehead wrinkles using BoNT-A. This meticulous assessment process begins with evaluating patient eligibility for BoNT-A treatment, where factors such as the severity and type of forehead wrinkles, muscle hyperactivity, and potential contraindications to BoNT-A use are carefully examined. The patient’s facial anatomy is then thoroughly analyzed, with a particular focus on the frontalis muscle. This involves studying the muscle’s strength, contraction patterns, and the presence of asymmetries or static lines at rest, essential for determining the precise placement of injections as per the LAD methodology.
During the consultation, the patient’s aesthetic goals and expectations are discussed in depth. This step is pivotal in customizing the treatment plan to achieve the desired outcome while ensuring a natural appearance. Photographic documentation of the patient’s face, captured from multiple angles, is employed as a vital tool for assessing the pre-treatment condition and aiding in the communication process with the patient.
The Standard Evaluation of the Patient (The Merz Scale), depicted in Figure 2, provides a standardized method to objectively assess the severity of forehead wrinkles [25,26,27]. It is a 5-point photonumeric rating system specifically designed to differentiate between resting (static) and hyperkinetic (dynamic) forehead lines. This scale enables clinicians and researchers to evaluate the presence and depth of forehead lines both when the face is at rest and during facial expressions. A score of 0 indicates the absence of wrinkles, while a score of 1 signifies that no wrinkles are visible at rest, yet fine lines appear with facial movements. A score of 2 denotes fine lines at rest that evolve into pronounced lines upon facial expressions. The presence of fine wrinkles at rest that transition into deeper lines with movement is graded as a 3. The highest score of 4 is reserved for those with deeper wrinkles while the face is at rest, which further deepen into pronounced furrows during facial expressions. This grading scale is pivotal in evaluating the progression of forehead lines and the effectiveness of various dermatological treatments.
This comprehensive evaluation, encompassing both clinical and aesthetic aspects, is integral to the success of the LAD technique, ensuring that each treatment is uniquely adapted to the patient’s individual anatomical and functional characteristics.
2.2. The Lines and Dots Technique
Locating the Supraorbital and Supratrochlear Nerve
The LAD technique employs a systematic approach to target the motor endplate zones of the frontalis muscle. The methodology begins by identifying the following horizontal and vertical lines on the forehead as shown in Figure 3.
Draw Six Vertical Lines
- Medial Canthus (MC): Draw a vertical line upwards from the medial corner of the eye.
- Medial Limbus (ML): Draw a vertical line upwards from the medial edge of the iris.
- Mid-Pupil (MP): Draw another vertical line upwards from the midpoint of the pupil when the subject is looking straight ahead.
- Lateral Limbus (LL): Draw a vertical line upwards from the lateral edge of the iris.
- Lateral Canthus (LC): Draw a vertical line upwards from the lateral corner of the eye.
- Medial line: This represents the mid-sagittal symmetry line between the right and left sides of the face.
Draw Four Horizontal Lines
- Suborbital Ridge (SOR): This horizontal line runs along the bony ridge of the eye socket.
- Lowest Horizontal Line (LHL): Draw the lowest horizontal forehead crease visible when the eyebrows are elevated.
- C-line: Draw a horizontal line along the second prominent horizontal forehead wrinkle.
- Uppermost Horizontal Line (UHL): Draw the highest visible line on the forehead when the eyebrows are elevated.
Identify Intersection Points
- O: Intersection of SOR and ML.
- D: Intersection of UHL and LC.
- L: Intersection of UHL and LL.
- I: Intersection of UHL and MP.
- M1: Intersection of UHL and ML.
- M2: Intersection of UHL and MC.
- M3: Intersection of UHL and the Medial line.
- Nerve Path Connections
- Deep SON (D-SON) Branch Path: Connect O to D, illustrating the path of the deep branch.
- Lateral SON (L-SON) Branch Path: Draw a line from O to L, representing the SON lateral branch.
- Intermediate SON (I-SON) Branch Path: Connect O to I, showing the path of the intermediate branch.
- Medial SON (M-SON) Branch Path: Connect O to M1, indicating the SON medial branch.
- Lateral SOT (L-SOT) Branch Path: Connect O to M2, indicating the SOT medial branch.
- Medial SOT (M-SOT) Branch Path: Connect O to M3, indicating the SOT lateral branch.
Ensuring the accuracy of the nerve pathway identification is critical for the success of the LAD technique. To validate the paths of the Supraorbital Nerve (SON) and Supratrochlear Nerve (SOT), we employed an innovative approach by using an electronic acupuncture pen (Electronic LY-508B Acupuncture Pen, ACUPRESSURE HEALTH CARE SYSTEM, China), as a surrogate for a conventional EMG device. This portable and accessible instrument was utilized to locate and validate the nerve paths. The procedure involved placing a grounding electrode in the patient’s hand, while the tip of the acupuncture pen was applied to the marked points on the forehead. As the pen approached the vicinity of a nerve, it produced an audible buzzing sound and a numerical reading indicative of nerve proximity. The intensity of the response correlated with the closeness to the nerve path, providing a practical and immediate means of verification. Due to the short distance between the points, the sensitivity was set at level 2 out of 10 to improve accuracy and decrease false positivity, as shown in Video 1.
2.3. BoNT-A Reconstitution
A-100 united of freeze-dried ONA (BoNT-A, Allergan) was reconstituted with 4 ml of sterile solution of 0.9% sodium chloride for injection following common aseptic techniques. This dilution yields 5 units/0.2 ml. The high dilution allows practitioners to distribute low dose of BoNT-A in large area.
2.4. Injection Technique
The injection follows the paths illustrated by the white vectors in the accompanying figure, using a 1mL Luer-lock, low-dead-space syringe (HENKE-JECT, HENKE SASS WOLF, Tuttlingen, Germany) and low-dead-space 0.2 mm Guage x 9 mm needles (The Invisible Needle TM, TSK Laboratory, Tochigi-Kan, Japan). The procedure begins from the lateral aspect of the forehead and progresses medially. The initial injection, starting at point D, follows the path of the deep branch of the Supraorbital Nerve (SON). Utilizing the full length of the needle, the practitioner advances the BoNT-A along this nerve path until reaching the C-line, angling the needle at approximately 15 degrees to facilitate intradermal delivery.
Subsequent injections follow a similar protocol, beginning from the endpoint of the preceding injection at the C-line and continuing along the same nerve path, terminating at the Lowest Horizontal Line (LHL). The remaining injections, starting respectively from points L, I, M1, M2, and M3, are administered with careful consideration of the direction and depth to remain consistent with the nerve path trajectory. For areas below the LHL, the LAD technique incorporates a microdose pinpoint approach as shown in Video 2.
2.5. Customized BoNT-A Dose
The General rule for the LAD techniques is that the dose increases lateral to medial and decrease upper to lower. While the injection depth increases medial to lateral as shown in Figure 4.
Therefore, injections from point D will have the lowest dose and deepest injection. While injections at point M3 will have the highest does, but the most superficial injection. The lines originating from the equivalent points, on the right and left and side, should receive equal dose, unless the practitioner aims to fix some asymmetry. The total dose of BoNT-A should be customized for each patient depending on several factors such as the size of the forehead, the severity of the lines and the patient’s expectations. Our average total dose was 10 units, distributed as following:
- 0.5 U for the line starting from point D to target the D-SON.
- 0.5 U for the line starting from point L to target the L-SON.
- 0.75 U for the line starting from point L to target the I-SON.
- 0.75 U for the line starting from point M1 to target the M-SON.
- 1 U for the line starting from point M2 to target the L-SOT.
- 1.5 U for the line starting from point M3 to target M-SOT.
These are only general guidelines, and it should be modified as required after the individual assessment.
3. Results
Validation of the Nerve Path
The validation of the LAD technique for predicting the paths of the Supraorbital Nerve (SON) and Supratrochlear Nerve (SOT) using an electronic acupuncture pen yielded excellent results. Upon application of the pen to the points outlined by the LAD grid, there was a consistent production of an audible buzzing sound along with corresponding numerical readings. These readings were indicative of nerve proximity, with higher intensities marking the precise locations of the SON and SOT nerve paths as predicted by the LAD technique.
Conversely, points that fell outside the LAD grid showed little to no pen readings, signaling a lack of proximity to the nerve paths. This clear distinction in pen readings between the targeted and non-targeted areas provided substantial evidence of the technique’s accuracy.
The electronic acupuncture pen, set at a sensitivity level of 2 out of 10, proved to be a reliable instrument for this application, demonstrating the LAD technique’s success in identifying the correct nerve paths, which is crucial for the efficacy and safety of BoNT-A injections.
Comparison of Pre- and Post-BoNT-A Treatment Using the Lines and Dots Technique (LAD)
After administering the Lines and Dots technique (LAD) for BoNT-A treatment, we conducted a comprehensive evaluation of the patient’s pre- and post-treatment images. This assessment utilized the Merz Aesthetics Scale (MAS) to objectively compare the severity of forehead wrinkles before and after the intervention. The results of this evaluation are exemplified in one patient’s, as depicted in Figure 5.
Before BoNT-A Treatment:
At Rest: The pre-treatment relaxed state of the forehead showed fine lines, which were classified as Grade 1 on the MAS. These lines were just perceptible, indicating the early signs of wrinkle formation without any significant depth.
During Contraction: The contracted state prior to treatment revealed shallow wrinkles consistent with a Grade 2 classification. This indicated a moderate development of dynamic lines that became more pronounced with facial movements but were not deeply set.
After BoNT-A Treatment:
At Rest: Post-treatment images in a relaxed state showed no visible wrinkles, which aligns with a Grade 0 on the MAS. This demonstrates a significant improvement, as the forehead appeared smooth, indicating an effective response to the BoNT-A treatment.
During Contraction: Similarly, the contracted state after BoNT-A treatment exhibited no visible wrinkles. The patient’s forehead-maintained smoothness under contraction, maintaining a Grade 0 on the MAS. This suggests a successful neuromodulation of the frontalis muscle, with the elimination of dynamic wrinkles typically formed during muscle contraction.
Patient Satisfaction:
The patient reported a high level of satisfaction with the treatment outcome. The absence of visible wrinkles in both relaxed and contracted states signified not only a reduction in the signs of aging but also the preservation of a natural-looking forehead movement.
Aesthetic Improvement
A notable aesthetic improvement was observed, with the patient achieving a more youthful and refreshed appearance. The post-treatment results showed no evidence of the “frozen” look often associated with botulinum toxin treatments, indicating that the LAD technique’s precision in targeting specific muscle areas was successful.
| https://drive.google.com/file/d/1m2MCYqw_h46qwZP00LMkVu4zeNFwffMX/view?usp=sharing |
| Video 1: This video demonstrates the innovative use of the Electronic LY-508B Acupuncture Pen as a method for validating the nerve pathways critical to the Lines and Dots (LAD) technique. The procedure showcases the placement of a grounding electrode in the patient’s hand and the application of the acupuncture pen on specific marked points on the forehead. Notably, as the pen approaches a nerve, it emits an audible buzzing sound accompanied by a numerical reading, indicative of nerve proximity. The video highlights the pen’s response intensity, correlating to nerve closeness, with the sensitivity set at level 2 out of 10 for enhanced accuracy and reduced false positives. |
| https://drive.google.com/file/d/1cxwg_63YrYaRviMPjDG0F6-6lGxzEnFq/view?usp=sharing |
| Video 2: This video illustrates the precise application of Botulinum Toxin Type A (BoNT-A) following the Lines and Dots (LAD) technique. The process begins from the lateral aspect of the forehead, using a 1mL Luer-lock, low-dead-space syringe and ultra-fine needles for accurate delivery. The initial injection starts at point D, targeting the deep branch of the Supraorbital Nerve (SON), with the needle angled at approximately 15 degrees for optimal intradermal injection. The video showcases the methodical progression of injections from the endpoint of one nerve path at the C-line to the next, adhering to the illustrated paths for precise targeting. Special attention is given to the direction and depth of injections to ensure alignment with the nerve pathways, culminating in the microdose pinpoint approach for areas below the Lowest Horizontal Line (LHL), demonstrating the meticulous nature of the LAD technique. |
4. Discussion
The “Lines and Dots” (LAD) technique introduces a groundbreaking approach in the realm of cosmetic injectables, primarily focusing on the precise identification of nerve paths. This technique is a significant advancement in aesthetic treatments, as it is the first to prioritize locating nerve endplates for BoNT-A injections. By mapping out these nerve paths with meticulous accuracy, the LAD technique elevates the precision of BoNT-A administration, ensuring that the injections are as close as possible to the nerve endplates.
A central aspect of the LAD method is its ability to maximize the effect of BoNT-A while minimizing the required dose. This efficiency is achieved through the strategic placement of injections near the nerve paths. By concentrating on these key areas, the LAD technique ensures that smaller doses of BoNT-A are used more effectively, leading to optimal results without the need for excessive quantities of the toxin.
The LAD technique is an advanced procedure that necessitates a high level of skill and expertise from the practitioner. It requires a nuanced understanding of needle direction and depth, as well as the ability to place multiple injections within a relatively confined area on the forehead. This level of control is crucial to target the nerve paths accurately and to achieve the desired aesthetic outcomes.
A unique benefit of the LAD technique is its ability to avoid common complications associated with BoNT-A injections, such as the lowering of the eyebrows. By possibly using a lower dose and targeting specific nerve endplates, the technique minimizes the risk of affecting areas that could lead to undesired drooping of the eyebrows. This precision ensures that the natural movement and expression of the forehead are maintained, enhancing patient satisfaction.
5. Conclusions
The LAD technique presents several distinct advantages in BoNT-A aesthetic treatments for forehead lines. Its primary strength lies in the precise identification of nerve paths, a pioneering approach in this field. This focus on targeting nerve endplates allows for increased effectiveness of BoNT-A injections, ensuring significant results even with possible reduced dosages. Consequently, LAD minimizes the risk of common side effects such as eyebrow ptosis. However, The technique demands a high degree of expertise from practitioners, emphasizing the importance of skillful application to achieve optimal aesthetic outcomes. By combining precision in nerve path targeting with strategic injection placement, the LAD method enhances treatment efficacy, offering a more tailored and patient-specific approach in cosmetic dermatology.
6. Patents
The author has applied for a trademark registration for the ‘Lines and Dots’ (LAD) technique, underlining its uniqueness and proprietary status in the field of cosmetic dermatology.
Funding
This research received no external funding
Institutional Review Board Statement
The study did not require ethical approval.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The author would like to express my sincere gratitude to R.N. Dima Omran, Dr. Salem Tomi, and Dr. Adel Abdulhafid at Albany Cosmetic and Laser Centre for their invaluable contributions and support throughout the development of this research. Their expertise, insights, and dedication have been instrumental in the advancement and refinement of the “Lines and Dots” (LAD) technique. Their commitment to excellence in the field of cosmetic dermatology has greatly enriched this work, and their collaborative efforts have been a cornerstone of its success.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Swift, A.; Liew, S.; Weinkle, S.; Garcia, J.K.; Silberberg, M.B. The facial aging process from the “inside out”. Aesthetic surgery journal 2021, 41, 1107–1119. [Google Scholar] [CrossRef] [PubMed]
- Diego-Mas, J.A.; Fuentes-Hurtado, F.; Naranjo, V.; Alcañiz, M. The influence of each facial feature on how we perceive and interpret human faces. i-Perception 2020, 11, 2041669520961123. [Google Scholar] [CrossRef] [PubMed]
- Marini, M.; Ansani, A.; Paglieri, F.; Caruana, F.; Viola, M. The impact of facemasks on emotion recognition, trust attribution and re-identification. Scientific Reports 2021, 11, 5577. [Google Scholar] [CrossRef] [PubMed]
- Fabi, S.; Alexiades, M.; Chatrath, V.; Colucci, L.; Sherber, N.; Heydenrych, I.; Jagdeo, J.; Dayan, S.; Swift, A.; Chantrey, J. Facial aesthetic priorities and concerns: a physician and patient perception global survey. Aesthetic surgery journal 2022, 42, NP218–NP229. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.L.; Goodman, G.J.; De Almeida, A.T.; Jones, D.; Carruthers, J.; Grimes, P.E.; de Maio, M.; Swift, A.; Solish, N.; Fagien, S. Decades of beauty: Achieving aesthetic goals throughout the lifespan. Journal of Cosmetic Dermatology 2023, 22, 2889–2901. [Google Scholar] [CrossRef] [PubMed]
- Braccini, F.; Catoni, I.; Belfkira, F.; Lagier, J.; Roze, E.; Paris, J.; Huth, J.; Bronsard, V.; Cartier, H.; David, M. SAMCEP Society consensus on the treatment of upper facial lines with botulinum neurotoxin type A: A tailored approach. Journal of Cosmetic Dermatology 2023, 22, 2692–2704. [Google Scholar] [CrossRef]
- Sever, L. Nonsurgical aesthetic procedures. University of Zagreb. School of Medicine. Department of Surgery, 2020.
- Walker, B.; Hand, M.; Chesnut, C. Forehead Movement Discrepancies After Botulinum Toxin Injections: A Review of Etiology, Correction, and Prevention. Dermatologic Surgery 2022, 48, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Cai, L.; Yang, M.; Li, F.; Han, X. Botulinum toxin to treat horizontal forehead lines: a refined injection pattern accommodating the lower frontalis. Aesthetic Surgery Journal 2020, 40, 668–678. [Google Scholar] [CrossRef] [PubMed]
- Omran, D.; Tomi, S.; Abdulhafid, A.; Alhallak, K. Expert opinion on non-surgical eyebrow lifting and shaping procedures. Cosmetics 2022, 9, 116. [Google Scholar] [CrossRef]
- Patil, A.; Kassir, M.; Wollina, U.; Goldust, M. New botulinum toxins for aesthetic dermatology: A comprehensive review. Der Hautarzt 2021, 72, 393–402. [Google Scholar] [CrossRef]
- de Sanctis Pecora, C.; Ventura Ferreira, K.; Amante Miot, H. ONE21 technique for an individualized assessment and treatment of upper face wrinkles in five pairs of identical twins with IncobotulinumtoxinA. Journal of Cosmetic Dermatology 2022, 21, 1940–1947. [Google Scholar] [CrossRef] [PubMed]
- de Sanctis Pecora, C. One21: a novel, customizable injection protocol for treatment of the forehead with IncobotulinumtoxinA. Clinical, Cosmetic and Investigational Dermatology, 2020; 127–136. [Google Scholar]
- Barbarino, S.C.; van Loghem, J.A.; Burgess, C.M.; Corduff, N. Evaluating the Effect of Incobotulinumtoxin A for Glabellar, Forehead, and Crow’s Feet Lines Using A High Dilution. The Journal of Clinical and Aesthetic Dermatology 2021, 14, 34. [Google Scholar] [PubMed]
- Bertucci, V.; Carruthers, J.D.; Sherman, D.D.; Gallagher, C.J.; Brown, J. Integrative assessment for optimizing aesthetic outcomes when treating glabellar lines with botulinum toxin type A: an appreciation of the role of the frontalis. Aesthetic Surgery Journal 2022, sjac267. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Z.; Qi, Z. The Impact of Upper Face Botulinum Toxin Injections on Eyebrow Height and Forehead Lines: A Randomized Controlled Trial and an Algorithmic Approach to Forehead Injection. Plastic and Reconstructive Surgery 2019, 144, 510e. [Google Scholar] [CrossRef] [PubMed]
- Gil, Y.-C.; Lee, S.-H.; Shin, K.-J.; Song, W.-C.; Koh, K.-S.; Shin, H.J. Three-dimensional topography of the supratrochlear nerve with reference to the lacrimal caruncle, and its danger zone in Asians. Dermatologic Surgery 2017, 43, 1458–1465. [Google Scholar] [CrossRef]
- Gil, Y.-C.; Shin, K.-J.; Lee, S.-H.; Song, W.-C.; Koh, K.-S.; Shin, H.J. Topography of the supraorbital nerve with reference to the lacrimal caruncle: danger zone for direct browplasty. British Journal of Ophthalmology 2017, 101, 940–945. [Google Scholar] [CrossRef] [PubMed]
- Lapatki, B.; Van Dijk, J.; Van de Warrenburg, B.; Zwarts, M. Botulinum toxin has an increased effect when targeted toward the muscle’s endplate zone: A high-density surface EMG guided study. Clinical Neurophysiology 2011, 122, 1611–1616. [Google Scholar] [CrossRef] [PubMed]
- Delnooz, C.; Veugen, L.; Pasman, J.; Lapatki, B.; Van Dijk, J.; Van De Warrenburg, B. The clinical utility of botulinum toxin injections targeted at the motor endplate zone in cervical dystonia. European Journal of Neurology 2014, 21, 1486–e1498. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, S.; Gormley, M.E.; Carey, J.R. Muscle fiber orientation in muscles commonly injected with botulinum toxin: an anatomical pilot study. Neurotoxicity research 2006, 9, 115–120. [Google Scholar] [CrossRef]
- O’Brien, C.F. Injection techniques for botulinum toxin using electromyography and electrical stimulation. Muscle & Nerve: Official Journal of the American Association of Electrodiagnostic Medicine 1997, 20, 176–180. [Google Scholar]
- Ågren, M.; Sahin, C.; Pettersson, M. The effect of botulinum toxin injections on bruxism: A systematic review. Journal of oral rehabilitation 2020, 47, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Sitnikova, V.; Kämppi, A.; Teronen, O.; Kemppainen, P. Effect of Botulinum Toxin Injection on EMG Activity and Bite Force in Masticatory Muscle Disorder: A Randomized Clinical Trial. Toxins 2022, 14, 545. [Google Scholar] [CrossRef] [PubMed]
- Chao, Y.Y.Y.; Chhabra, C.; Corduff, N.; Fabi, S.G.; Hornfeldt, C.S.; Kerscher, M.; Lam, S.; Pavicic, T.; Peng, P.H.; Pooth, R. Validation of a photonumeric assessment scale for grading the slope of the Asian forehead. Dermatologic Surgery 2019, 45, S38–S45. [Google Scholar] [CrossRef]
- Kang, E.; Kang, D.; Kim, S.; Choi, K.; Lee, W.; Cho, J. Development and Validation of Facial Line Distress Scale for Forehead Lines: FINE-FL. Aesthetic Surgery Journal 2023, sjad340. [Google Scholar] [CrossRef] [PubMed]
- da Cunha, A.L.G.; Vasconcelos, R.; Di Sessa, D.; Sampaio, G.; Ramalhoto, P.; Zampieri, B.F.; Deus, B.S.; Vasconcelos, S.; Bellote, T.; Carvalho, J. IncobotulinumtoxinA for the Treatment of Glabella and Forehead Dynamic Lines: A Real-Life Longitudinal Case Series. Clinical, Cosmetic and Investigational Dermatology 2023, 697–704. [Google Scholar] [CrossRef]
Figure 1.
This figure showcases the intricate anatomical dissection of a cadaver with the lower part of the frontalis muscle, procerus, corrugator supercilii, depressor supercilii, and orbicularis oculi muscles removed to reveal the underlying nerve pathways. The paths of the Supraorbital Nerve (SON) and Supratrochlear Nerve (SOT) are meticulously traced: D-SON (Deep branch of the Supraorbital Nerve) is visible extending upwards from the eyebrow’s medial end. L-SON (Lateral branch of the Supraorbital Nerve) runs laterally across the forehead. I-SON (Intermediate branch of the Supraorbital Nerve) is shown diverging slightly towards the center from the lateral branch. M-SON (Medial branch of the Supraorbital Nerve) is delineated moving towards the midline. L-STN (Lateral branch of the Supratrochlear Nerve) and M-STN (Medial branch of the Supratrochlear Nerve) are also visible, with their respective trajectories marked. The dotted white lines represent the boundaries of the removed muscles, highlighting the now-exposed nerve branches, allowing for a clear visualization of their natural anatomical distribution. This dissection serves as a vital reference for understanding the facial nerve anatomy relevant to aesthetic procedures.
Figure 1.
This figure showcases the intricate anatomical dissection of a cadaver with the lower part of the frontalis muscle, procerus, corrugator supercilii, depressor supercilii, and orbicularis oculi muscles removed to reveal the underlying nerve pathways. The paths of the Supraorbital Nerve (SON) and Supratrochlear Nerve (SOT) are meticulously traced: D-SON (Deep branch of the Supraorbital Nerve) is visible extending upwards from the eyebrow’s medial end. L-SON (Lateral branch of the Supraorbital Nerve) runs laterally across the forehead. I-SON (Intermediate branch of the Supraorbital Nerve) is shown diverging slightly towards the center from the lateral branch. M-SON (Medial branch of the Supraorbital Nerve) is delineated moving towards the midline. L-STN (Lateral branch of the Supratrochlear Nerve) and M-STN (Medial branch of the Supratrochlear Nerve) are also visible, with their respective trajectories marked. The dotted white lines represent the boundaries of the removed muscles, highlighting the now-exposed nerve branches, allowing for a clear visualization of their natural anatomical distribution. This dissection serves as a vital reference for understanding the facial nerve anatomy relevant to aesthetic procedures.
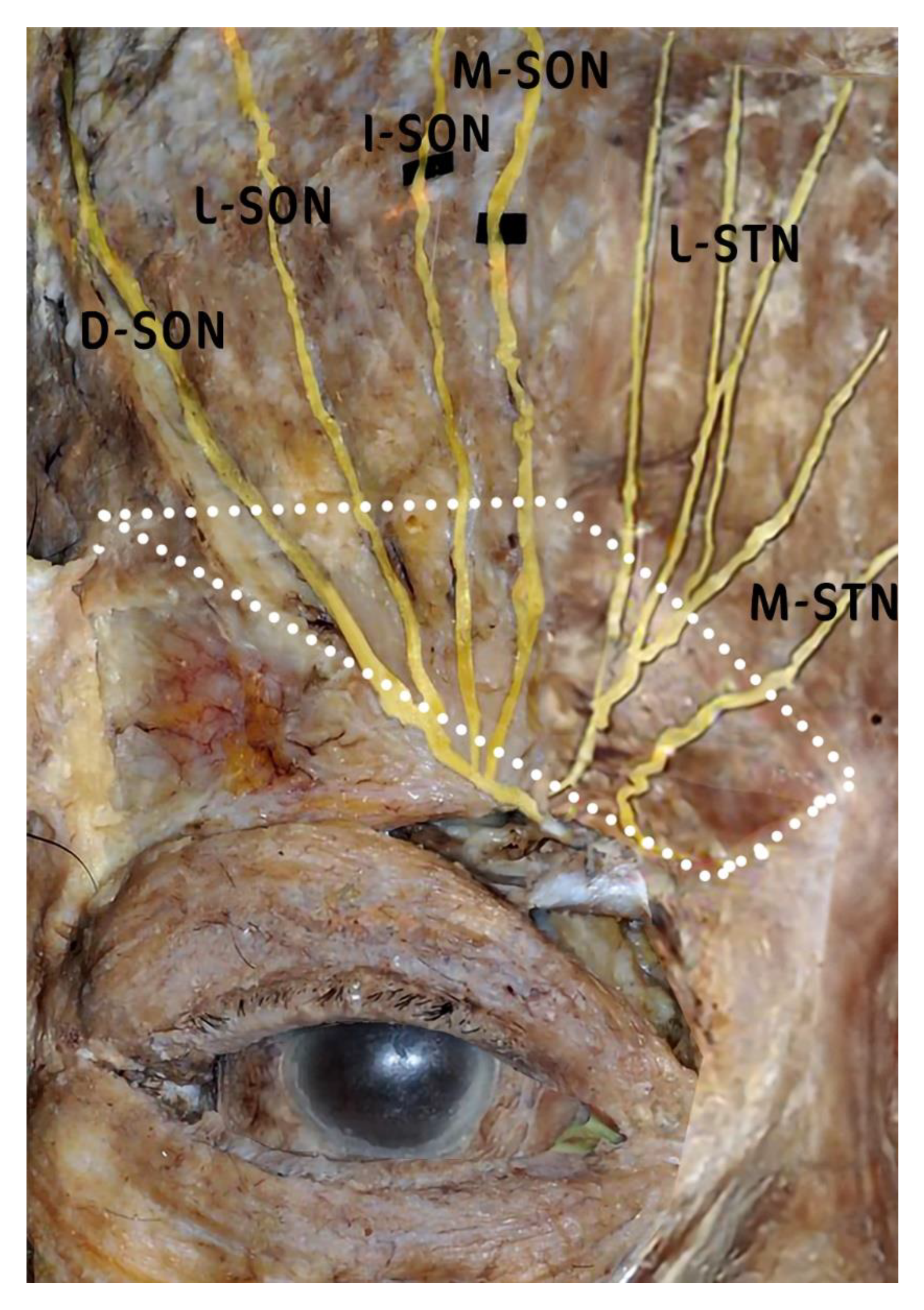
Figure 2.
This figure illustrates the Forehead Lines Grading Scale. This figure is divided into two sections: (A) and (B). Section (A) demonstrates the scoring of the photonumeric scale for resting or static forehead lines, while section (B) illustrates the scoring for hyperkinetic or dynamic forehead lines. The scale is a 5-point photonumeric rating system, where each point represents a different severity of wrinkles: 0 indicates no wrinkles, 1 represents no wrinkles present at rest but fine lines with facial expression, 2 is for fine wrinkles present at rest and deep lines with facial expression, 3 signifies fine wrinkles present at rest and deeper lines with facial expression, and 4 denotes deeper wrinkles at rest and deeper furrows with facial expression. Artwork by Kamal Alhallak.
Figure 2.
This figure illustrates the Forehead Lines Grading Scale. This figure is divided into two sections: (A) and (B). Section (A) demonstrates the scoring of the photonumeric scale for resting or static forehead lines, while section (B) illustrates the scoring for hyperkinetic or dynamic forehead lines. The scale is a 5-point photonumeric rating system, where each point represents a different severity of wrinkles: 0 indicates no wrinkles, 1 represents no wrinkles present at rest but fine lines with facial expression, 2 is for fine wrinkles present at rest and deep lines with facial expression, 3 signifies fine wrinkles present at rest and deeper lines with facial expression, and 4 denotes deeper wrinkles at rest and deeper furrows with facial expression. Artwork by Kamal Alhallak.
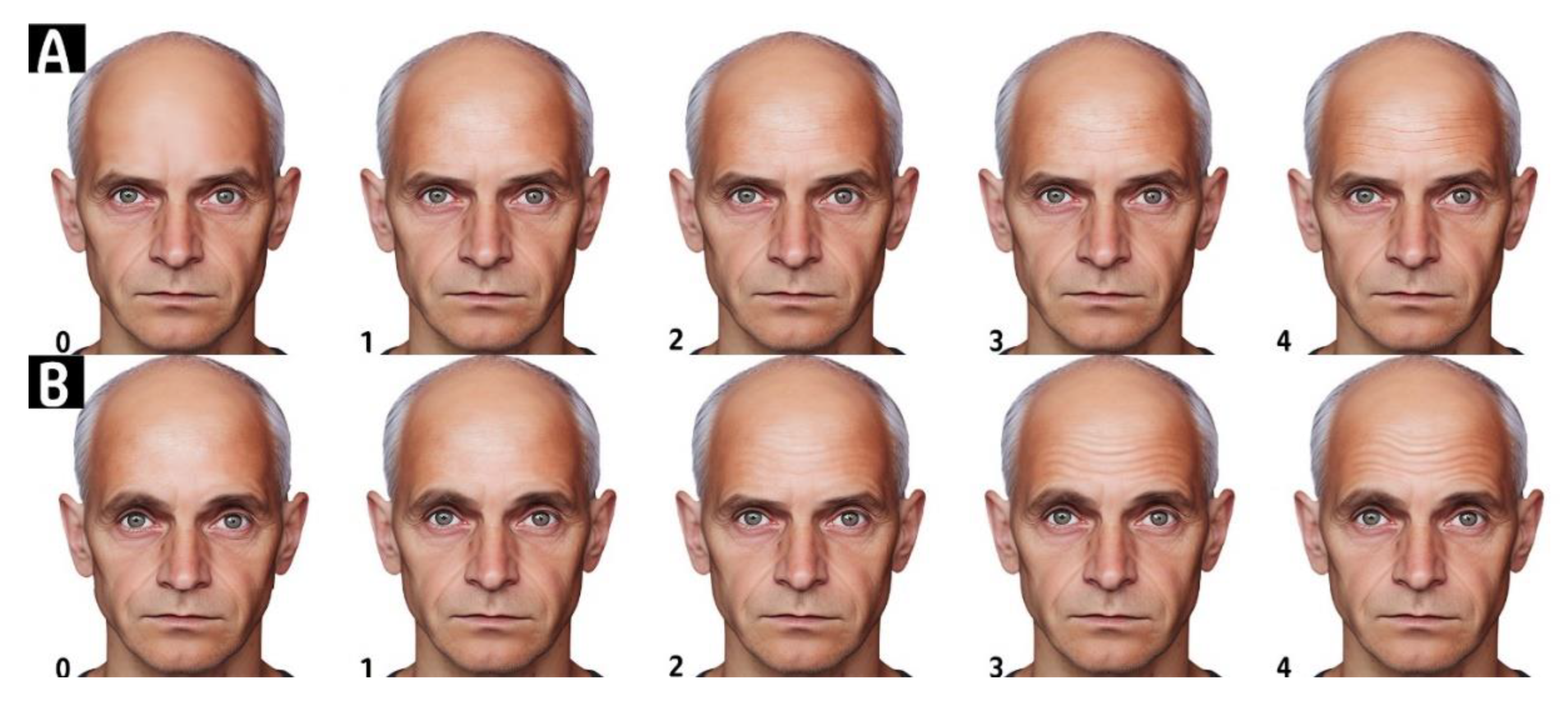
Figure 3.
This figure is a visualization of the Lines and Dots Technique (LAD) for Botulinum Toxin Injection. (A) Vertical lines are drawn corresponding to key facial landmarks: Lateral Canthus (LC), Mid-Pupil (MP), Medial Limbus (ML), and Medial Canthus (MC), establishing a framework for injection planning. (B) Horizontal lines are added: the Upper Horizontal Line (UHL), the C-line marking the central forehead crease, and the Lowest Horizontal Line (LHL), providing additional structure to the injection grid. (C) The intersection of the vertical and horizontal lines creates the grid points, which serve as potential injection sites for the LAD technique. (D) The nerve paths are identified, with blue lines tracing the expected courses of the Supraorbital Nerve (SON) and Supratrochlear Nerve (SOT) branches. (E) The upper injection pattern marked with white arrows, with blue dots indicating where injections are made to target the upper portions of the forehead along the nerve paths. (F) The lower injection pattern marked with white arrows, with blue dots marking the injection sites below the C-line to address the lower forehead and eyebrow region. (G) Intradermal injection points are indicated, demonstrating the precise locations for the BoNT-A to be administered. (H) An overlay of the LAD grid is superimposed over a cadaver dissection image to illustrate the correlation between the theoretical grid and the actual anatomical nerve locations, validating the LAD technique’s anatomical accuracy. Artwork by Kamal Alhallak.
Figure 3.
This figure is a visualization of the Lines and Dots Technique (LAD) for Botulinum Toxin Injection. (A) Vertical lines are drawn corresponding to key facial landmarks: Lateral Canthus (LC), Mid-Pupil (MP), Medial Limbus (ML), and Medial Canthus (MC), establishing a framework for injection planning. (B) Horizontal lines are added: the Upper Horizontal Line (UHL), the C-line marking the central forehead crease, and the Lowest Horizontal Line (LHL), providing additional structure to the injection grid. (C) The intersection of the vertical and horizontal lines creates the grid points, which serve as potential injection sites for the LAD technique. (D) The nerve paths are identified, with blue lines tracing the expected courses of the Supraorbital Nerve (SON) and Supratrochlear Nerve (SOT) branches. (E) The upper injection pattern marked with white arrows, with blue dots indicating where injections are made to target the upper portions of the forehead along the nerve paths. (F) The lower injection pattern marked with white arrows, with blue dots marking the injection sites below the C-line to address the lower forehead and eyebrow region. (G) Intradermal injection points are indicated, demonstrating the precise locations for the BoNT-A to be administered. (H) An overlay of the LAD grid is superimposed over a cadaver dissection image to illustrate the correlation between the theoretical grid and the actual anatomical nerve locations, validating the LAD technique’s anatomical accuracy. Artwork by Kamal Alhallak.
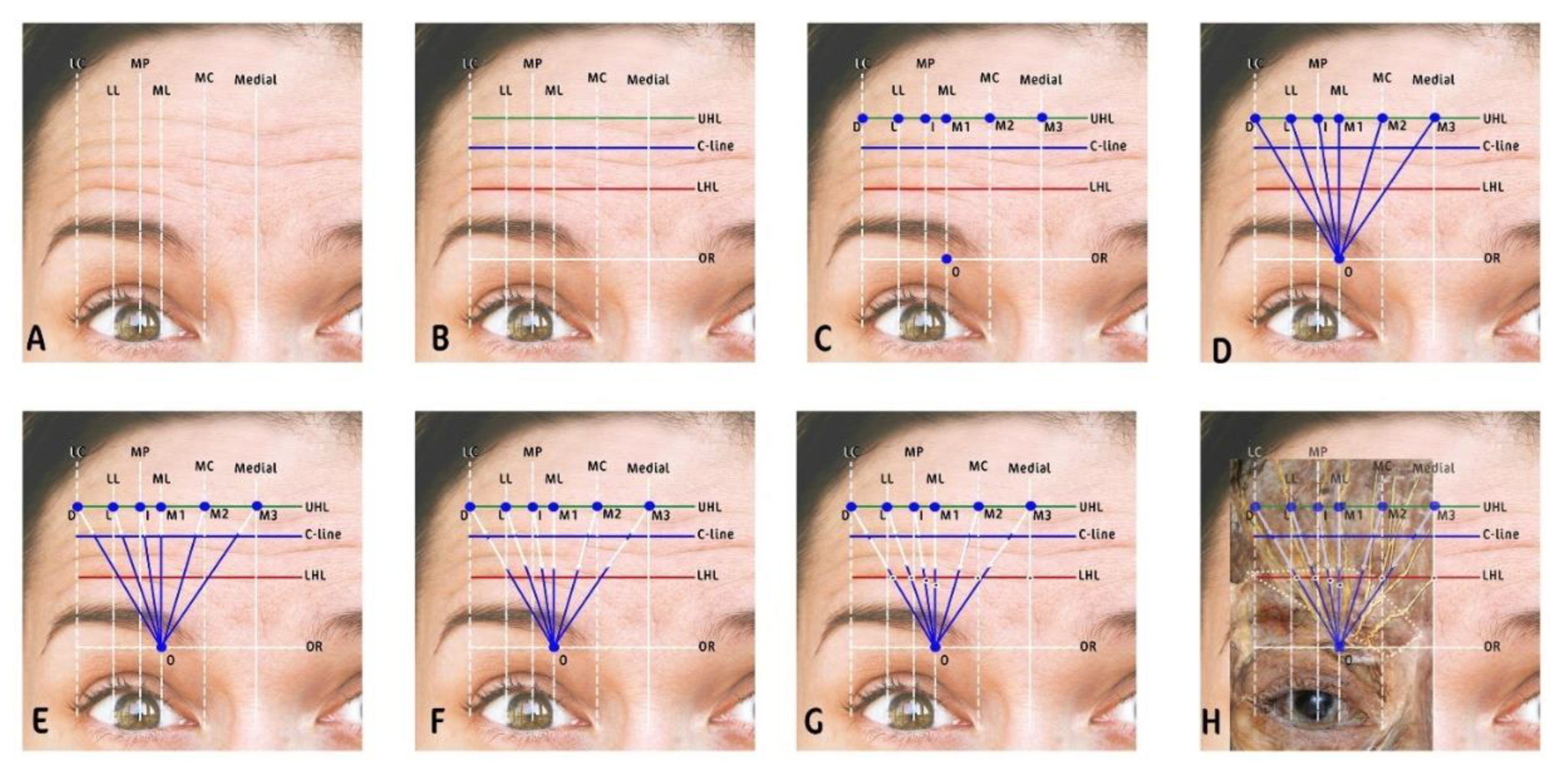
Figure 4.
This figure shows (A) Demonstration of Botulinum toxin A (BoNT-A) dose distribution, indicating an increasing pattern from lateral to medial and from lower to upper regions of the forehead. (B) Illustration of the BoNT-A injection depth progression, showing an increase from medial to lateral across the forehead.
Figure 4.
This figure shows (A) Demonstration of Botulinum toxin A (BoNT-A) dose distribution, indicating an increasing pattern from lateral to medial and from lower to upper regions of the forehead. (B) Illustration of the BoNT-A injection depth progression, showing an increase from medial to lateral across the forehead.
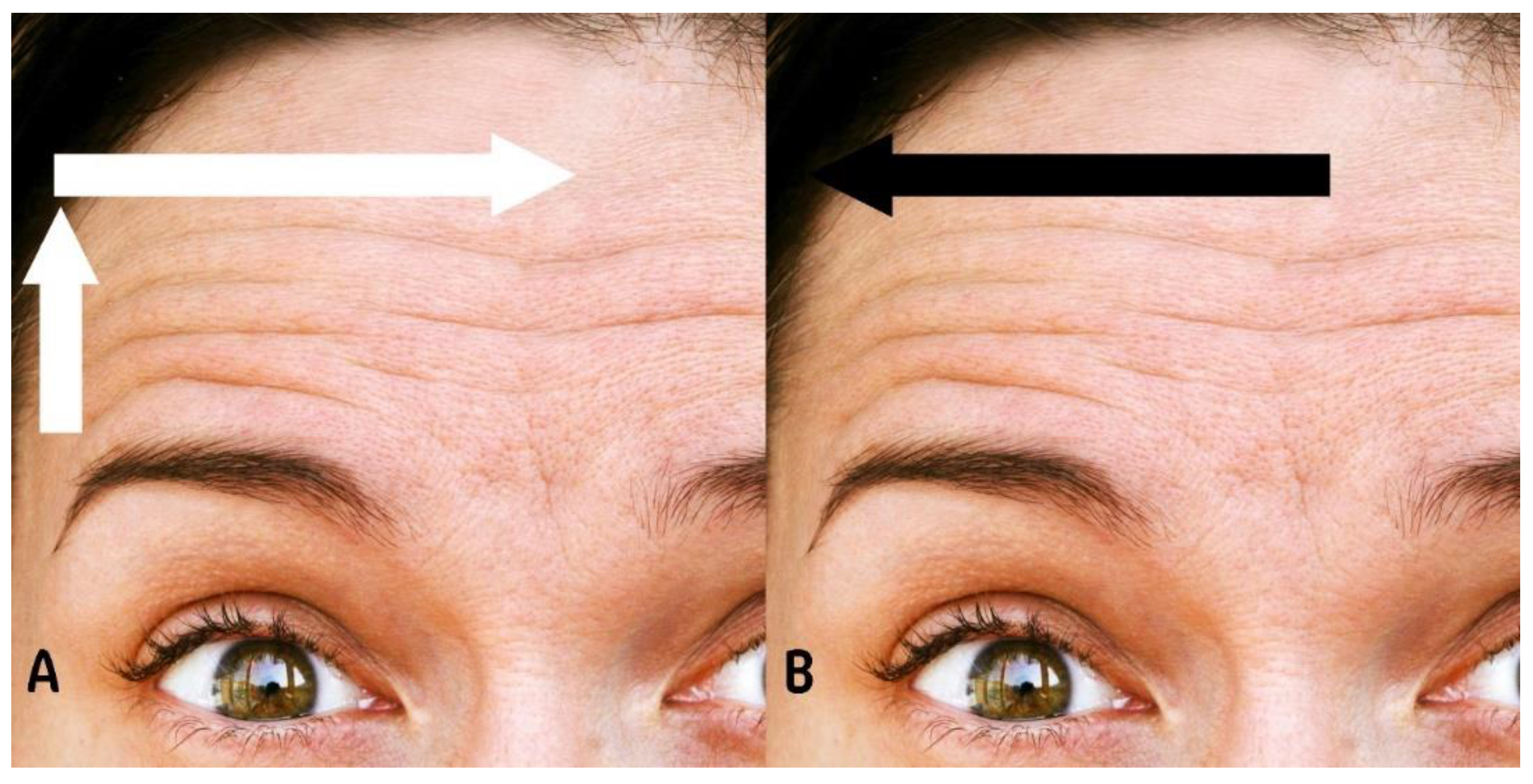
Figure 5.
this is a comparative analysis of forehead wrinkles pre- and post BoNT-A treatment using the Lines and Dots Technique (LAD): (A) LAD Grid Overlay: Pre-treatment frontal view of the patient with the LAD technique grid superimposed to guide treatment areas. (B) Maximal Forehead Contraction Pre-Treatment: Display of forehead at maximum contraction before BoNT-A, showing Grade 2 wrinkles as per MAS. (C) Relaxed Forehead Pre-Treatment: The patient’s forehead at rest before BoNT-A, exhibiting fine lines corresponding to Grade 1 on the MAS. (D) Maximal Forehead Contraction Post-Treatment: Forehead appearance at maximum contraction 2 weeks following BoNT-A, showing no visible wrinkles, achieving Grade 0 on the MAS. (E) Relaxed Forehead Post-Treatment: Post-BoNT-A relaxed state of the forehead with no visible lines, maintaining a Grade 0 on the MAS, indicative of excellent treatment response.
Figure 5.
this is a comparative analysis of forehead wrinkles pre- and post BoNT-A treatment using the Lines and Dots Technique (LAD): (A) LAD Grid Overlay: Pre-treatment frontal view of the patient with the LAD technique grid superimposed to guide treatment areas. (B) Maximal Forehead Contraction Pre-Treatment: Display of forehead at maximum contraction before BoNT-A, showing Grade 2 wrinkles as per MAS. (C) Relaxed Forehead Pre-Treatment: The patient’s forehead at rest before BoNT-A, exhibiting fine lines corresponding to Grade 1 on the MAS. (D) Maximal Forehead Contraction Post-Treatment: Forehead appearance at maximum contraction 2 weeks following BoNT-A, showing no visible wrinkles, achieving Grade 0 on the MAS. (E) Relaxed Forehead Post-Treatment: Post-BoNT-A relaxed state of the forehead with no visible lines, maintaining a Grade 0 on the MAS, indicative of excellent treatment response.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



