
Submitted:
29 November 2023
Posted:
30 November 2023
You are already at the latest version
Abstract
(1) Background: National health system databases represent one of the most obvious sources of information about epidemiology of adverse drug reactions including drug-induced allergy and anaphylaxis. (2) Methods: Retrospective analysis of data from national database of pharmacovigilance in the Russian Federation (analyzed period 02.04.2019 - 21.06.2023) was performed. The prevalence of anaphylactic reactions (ARs) was determined, the structure of drugs involved was estimated together with patients’ characteristics. (3) Results: ARs were reported in 8.3% of drug-induced allergic reactions (2304/27,727), mean age of patients was 48.2 ± 15.8 years, 53.2% were females. Main causative groups of drugs were antibiotics, ABs (44.62%), local anesthetics, (19.97%), and cyclooxygenase (COX)-inhibitors (10.07%). Fatal ARs was reported in 9.5% (218/2304), mean age 48.0 ± 16.7 years, 56.2% females. Pediatric population accounted for 5.8% (133/2304), mean age 11.8± 4.5 years, 51.9% females. Elderly population accounted for 2.8% (65/2304), mean age 73.0±5.3 years, 43.5% (27/65) females. ABs were the leading causative groups of ARs in the elderly (40%), children (42.86%), and among fatal cases (50%). (4) Conclusions: ARs accounted for 8.3% of all drug-induced allergic reactions, and ABs were the most common causative agents. Females predominated in all groups except elderly patients.
Keywords:
drug-induced allergy
; anaphylaxis
; antibiotics
; local anesthetics
; cyclooxygenase (COX)-inhibitors
1. Introduction
Prevalence of severe allergic reactions, including anaphylaxis, is increasing worldwide with the most frequent elicitor groups including food, insect venom, and drugs [1-4]. Drug allergy may affect up to one third of patients in emergency departments [5]. The prevalence of self-reported drug allergy was estimated in a systematic review and meta-analysis of 53 studies (n - 26,306), which results revealed the value of 8.3% (range across studies 0.7-38.5%) [6]. Anaphylaxis is one of most severe forms of allergy, representing acute, potentially fatal reaction. A cross-sectional study based on a screening of medical records (from January 2015 to August 2017) identified the prevalence of anaphylaxis among emergency department admissions at the level of 0.00026%, and the pediatric population (age 1–16 years) was the most affected (60.9%). Anaphylaxis was triggered by drugs in 17.4% [7]. A retrospective 10-year study of practice in a tertiary hospital revealed drugs to be the most common cause of anaphylaxis in an emergency department (33%) [8]. Analysis of electronic health records from a large United States healthcare system described epidemiology of drug-induced hypersensitivity reactions (HSRs): they were reported in 13.8% (377,474 out of 2.7 million patients), of which 53.1% were immediate type reactions, and 46.9% - delayed [9].
Anaphylactic reactions are among the most dangerous immediate type HSRs, and Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are considered as the most severe delayed-type HSRs [10]. Dhopeshwarkar N et al (2019) performed electronic health records analysis and revealed that 1.1% of patients report drug-induced anaphylaxis, and ABs, nonsteroidal anti-inflammatory drugs (NSAIDs) and opiates were the main causative pharmacological groups [11]. Retrospective analysis based on the National Adverse Drug Reaction Monitoring System in China found the incidence of anaphylaxis to be 0.03%, and ABs, antineoplastic drugs, and contrast media were the most prevalent allergens [12]. ABs are also the most common triggers of delayed HSRs (SJS and TEN) [13, 14].
The aim of our study was to estimate proportion of SRsAs among SRsDIAs, proportion of pediatric SRsAs, elderly SRsAs, and fatal SRsAs among SRsAs, to detect the structure of drugs involved in anaphylaxis and to assess patients’ characteristics (sex, age) using Russian National Pharmacovigilance database - Automatized Information System “Pharmacovigilance” (AIS).
2. Results
2.1. Analysis of SRsAs
A total of 27,727 SRsDIAs were detected in the electronic database during the study period (02.04.2019 - 21.06.2023). Of these, SRsAs accounted for 8.3% (n – 2304). Mean age of patients (SRsAs) was 48.2 ± 15.8 years (min - 1 day, max - 89 years), 53.2% (n - 1226) were females.
Analysis of outcomes among SRsAs revealed recovery in 90.54% (n - 2086), and death in 9.46% (n - 218).
SRsAs assessment revealed seven main pharmacological groups involved in anaphylaxis: ABs (44.6%, n - 1028), local anesthetics, LAs (20%, n - 460), COX-inhibitors (10.0%, n - 232), iodine-containing contrast medium, ICCM (6.6%, n - 153), cardiovascular (CV) drugs (6.2%, n - 143), central nervous system (CNS)-active drugs (1.5%, n - 35), and neuromuscular blocking agents, NMBAs (1.4%, n - 33). Other drugs accounted for 9.5% (n - 220).
2.1.1. Analysis of ABs Involved in Anaphylaxis
The mean age of patients with anaphylaxis due to ABs was 55.0±14.9 years (min – 1 day, max – 89 years), females were – 63.8% (n - 655). The number of SRsAs where ABs were causative agents was 1028 (46.7%), and beta-lactam antibiotics were the most prevalent group (87.74%, n - 902). Ceftriaxone was the most common among all ABs (63.3%, n - 687). The structure of ABs involved in anaphylaxis is shown in the Table 1. Lethal outcomes were reported in 109 cases of SRsAs caused by ABs (10.6%).
2.1.2. Analysis of LAs Involved in Anaphylaxis
LAs were identified as a main cause of anaphylaxis in 20% of SRsAs (n - 460). The mean age of patients with anaphylaxis due to LAs was 44.3±14.9 years (min – 5 months, max – 84 years). Females were 53.7% (n - 247). The absolute leader was lidocaine (63.7%, n - 293). The structure of LAs is indicated in the Table 2.
2.1.3. Analysis of COX-Inhibitors Involved in Anaphylaxis.
The mean age of patients listed in SRsAs with COX-inhibitors as a main cause was 44.9±14.5 (min – 10, max – 81) years, and 62.1% (n - 144) were females.
The number of SRsAs with causative agents COX-inhibitors was 232 accounting for 10.07% of SRsAs. Among COX-inhibitors we did consider NSAIDs, acetaminophen, and metamizole. Acetaminophen inhibits COX in the brain structures with analgesic and antipyretic effects [15]. Acetaminophen was the cause of SRsAs in the vast majority of cases – 49 (21.1%). Nearly the same value was revealed for metamizole, another COX inhibitor without anti-inflammatory activity but with potent analgesic action [16]. It was detected in 48 cases (20.69%). Detailed information about COX-inhibitors involved in anaphylaxis is presented in the Table 3.
2.1.4. Analysis of ICCM Involved in Anaphylaxis.
ICCM were causative agents in 6.6% of SRsAs (n - 153). The mean age of patients was 55.4±12.0 years (min – 8.5 months, max – 86 years), 47.1% (n - 72) were females. The structure of ICCM involved is presented in the Table 4. Lethal outcome was reported in 8 cases (5.2%).
2.1.5. Analysis of CV Drugs Involved in Anaphylaxis
SRsAs with CV drugs being causative agents accounted for 6.2% (n - 143) of SRsAs. The mean age of patients was 57.7±16.2 (min –19, max - 86), females were 76,9% (n-110). The highest frequency was reported for angiotensin-converting enzyme inhibitors, ACEIs (20.3%, n - 29), followed by beta-blockers (15.4%, n - 22) and calcium channel blockers (14.7%, n - 21). Table 5 contains data on the structure of CV drugs involved in anaphylaxis.
2.1.6. Analysis of CNS-Active Drugs Involved in Anaphylaxis
SRsAs analysis revealed CNS-active drugs being causative agents in 35 (1.5%). The mean age of patients was 54.6±17.8 years (min –23, max - 82). The structure of drugs involved in anaphylaxis is indicated in the Table 6. Among the CNS-active drugs the highest prevalence was reported for synthetic opioid, fentanyl (57.1%, n - 20).
2.1.7. Analysis of NMBAs Involved in Anaphylaxis
NMBAs were detected as causative drugs in 1.2% of SRsAs (n – 28). The mean age of patients was 47.4 ± 14.3 years (min –22, max - 71). The highest prevalence was reported for rocuronium (n - 10) – 30.3%. NMBAs involved in anaphylaxis are presented in the Table 7.
2.2. Analysis of Fatal SRsAs
The total number of fatal SRsAs was 218 (9.5%). Reports analysis revealed 56.2% were women, mean age was 48.0 ± 16.7 (min - 1 month, max - 86 years). Two cases of death were observed in pregnant women (1.4%), 17 cases in children (11.5%), and 65 (29.8%) – in the elderly. The leading causative groups were ABs (50%, n - 109), LAs (13.3%, n - 29), and CV drugs (6.0%, n - 13). The total structure of drugs detected in fatal SRsAs is shown in the Table 8.
The mean age of patients in fatal SRsAs depending on causative group of drugs is listed in the Table 9 together with sex distribution (%). The youngest age was reported in fatal SRsAs where LAs were causative drugs, the oldest – where CV drugs were the cause. Females predominated in all groups except fatal SRsAs with CV drugs, where 69.2% (n - 9) were males.
The highest proportion of fatal SRsAs was revealed in SRsAs, where NMBAs and CNS-active drugs were causative agents notwithstanding the fact that SRsAs caused by these pharmacological groups accounted for only 1.2 and 1.5% in the total structure, respectively (Figure 1).
2.3. Analysis of Pediatric SRsAs
Pediatric SRsAs (reports of patients ≤ 18 years) accounted for 5.8% (n - 133) of the total SRsAs structure. The mean age was 11.8± 4.5 years (min – 1 day, max – 18 years), females were 51.9% (n - 69). Outcome analysis revealed recovery in 87.2% (n - 116), and death in 12.8% (n - 17).
The most prevalent groups of drugs involved in anaphylaxis in children were ABs (42.9%, n - 57), LAs (12.8%, n - 17), and COX-inhibitors (6.0%, n - 8). Other drugs accounted for 38.3 (n - 51).
ABs were the leading causative pharmacological group in children and the absolute majority of reactions (87.7%) were due to ABs (Table 6). The mean age of children with anaphylaxis due to ABs was 16.0 ± 12.6 years (min – 1 day, max -18 years), females were 51.2% (n-29). The structure of ABs involved in anaphylaxis in children is given in the Table 10.
Lethal outcome due to ABs was reported in 8 cases (14.0%, 8/57), mean age was 7.4± 5.4 (min – 15 months, max – 16 years), males were 85.7% (n - 6). Ceftriaxone was detected in 7 cases, amoxicillin clavulanate – in 1.
Among LAs the leading agent was lidocaine, responsible for 52.9% of cases (Table 11). The mean age of children in SRsAs with LAs was 9.9±4.6 (min – 5 months, max – 17 years), males were 64.7% (n - 11). Fatal SRsAs included only lidocaine (3/17, 17.6%), mean age was 10.0±3.3 (min - 5, max -13) years, males were 66.7% (n - 2).
There were only 8 SRsAs with COX-inhibitors in pediatric population (acetaminophen – 50% (n - 4), ketorolac – 25% (n - 2) and metamizole – 25% (n – 2)). The mean age was 15.0±2.0 (min - 10, max - 18) years, females were 62,5% (n-5). There were no lethal outcomes among SRsAs with COX-inhibitors as causative agents in children.
2.4. Analysis of SRsAs in the Elderly
SRsAs of patients ≥65 years accounted for 2.8% (n - 65). The mean age was 73.0±5.3 (min - 65, max - 89) years, females were 43.5% (n - 27). Outcomes analysis revealed recovery in 53.8% (n - 35), and death in 46.2% (n - 30).
The most common causative pharmacological groups were ABs (40%, n - 26), CV drugs (20%, n - 13), and ICCM (12.3%, n - 8). The structure of drugs involved in anaphylaxis in the elderly is demonstrated in the Table 12.
Among the records with lethal outcomes in the elderly 53.3% (16/30) were reported in females. The majority of fatal SRsAs revealed ABs as causative agents (the only drug was ceftriaxone) – 31.4% (n - 16). ICCM were reported in 15.7% (n - 8), pentoxifylline - in 3.9% (n - 2), amiodarone - in 2.0% (n - 1), bupivacaine - in 2.0% (n - 1), and cisplatin - in 3.9% (n - 2).
3. Discussion
Our results revealed anaphylaxis in 8.3% of SRsDIAs registered in the AIS “Pharmacovigilance” database (2304/27,727) during the study period 02.04.2019 - 21.0 6.2023. Fatal SRsAs were reported in 9.5% (n - 218). There were close age and sex characteristics in the records of survived and died patients according to the SRsAs analysis (48.2 ± 15.8 years, females - 53.2% vs. 48.0 ± 16.7 years, females - 56.2%).
Based on the results of an 8-year post hoc analysis on the MEREAFaPS Study database (2012–2019) the mean age of population with anaphylaxis was 55.7 ± 17.7 years, and females were 52.4% [17]. The mean age of patients with drug-induced anaphylaxis in China was determined as 47.6 years (Beijing Pharmacovigilance Database analysis), and 52.7% were females [18]. Analysis of records with drug-induced anaphylaxis in Poland, West Pomerania, revealed the mean age of population to be 40.5 years, and 54.4% were females [19]. Female dominance in the structure of patients with drug-induced anaphylaxis (57.9%) was also proved by the results of an analysis of electronic health records (EHRs) of a large United States healthcare system [11] and by the results of a Tunisian retrospective study (males/female ratio was 0.6)), in the last study patients were younger than in most of other published works: the mean age was 33.52 years [20]. An analysis of drug-induced anaphylaxis in a Vietnamese Pharmacovigilance Database revealed 51.8% patients between 20 and 60 years old, 53.2% were female [21]. Korean Health Insurance Review and Assessment Service (HIRA) database analysis (period - January 2011to December 2019) indicated that the mean age of patients with drug-induced anaphylaxis was 52 years, 55.2% were female [22].
ABs are among the most common triggers of drug-induced anaphylaxis. Their leading role was proved both by retrospective and prospective studies [8, 24, 25]. Our results revealed ABs to be the main cause of anaphylaxis in all age groups (44.6% (n - 1028) in total SRsAs, 42.9% (n - 57) in pediatric SRsAs, and 40.0% (n – 26) in the elderly), and among fatal SRsAs (50% (n - 109)). According to our study the absolute leader among ABs causing anaphylaxis was ceftriaxone.
Zhao Y et al (2018) revealed ABs to be the main group in the structure of drugs involved in anaphylaxis (39.3%), followed by traditional Chinese medicines (11.9%), radiocontrast agents (11.9%), and antineoplastic agents (10.3%) [18]. Among all the drugs analyzed cephalosporins were leading agents, accounted for 34.5% [18].
Based on the FDA Adverse Event Reporting System (FAERS) analysis drug-induced anaphylaxis was reported in 0.27% of all adverse drug events (47,496/17,506,002), and causative drugs included ABs (14.87%)), monoclonal antibodies (13.06%), and COX-inhibitors (NSAIDs and acetaminophen – 8.83%). Anaphylaxis deaths were associated with ABs, radiocontrast agents and intraoperative agents, and the rate of fatal cases was 6.28% (2984/47,496) [23].
Pagani S et al (2022) defined the leading role of ABs in ARs development (53.78%), and penicillins were the most prevalent (66.67%) followed by cephalosporins (21.10%), and fluoroquinolones (8.56%) [17]. Penicillins were the cause of ARs in 50% according to the data of Wong A et al (2019), and sulfonamides and cephalosporines were other common causes [9].
Cephalosporins are proved to be common triggers of ARs in adults and children [26 - 29], and a 3rd generation agent including ceftriaxone were among main inducers of allergic reactions reported in hospitals of South Korea [30]. Analysis of the Korean Adverse Event Reporting System (KAERS) and HIRA database revealed incidence rates for hypersensitivity reactions including anaphylaxis to cefaclor, other 2nd generation cephalosporins, and 3rd generation cephalosporins to be 1.17/10,000 persons (0.38/10,000 persons), 3.57/10,000 persons (0.38/10,000 persons), and 5.82/10,000 persons (0.61/10,000 persons), respectively [31]. Another Korean study revealed five common medication risk factors for drug-induced anaphylaxis including cephalosporine cefaclor, ICCM (iopromide, iohexol, iomeprol), and tolperisone [22]. Cephalosporines were defined as the most common ABs causing ARs based on the results of China Hospital Pharmacovigilance System analysis [12]. Third generation cephalosporines were determined as the main cause of drug-induced anaphylaxis based on the results of a Vietnamese Pharmacovigilance Database [21].
LAs in our study were reported in 20.0% of SRsAs (n - 460). They were ranked second in the list of causative agents among total SRsAs, pediatric SRsAs, and among fatal SRsAs. LAs are typically considered to be anaphylaxis triggers prevalent in dentistry practice [32], though the risk of true IgE-mediated allergy was shown to be lower than 1% [33 - 37]. Amide local anesthetics are less involved in hypersensitivity reactions compared with ethers, and among amides lidocaine is known to be the most associated with severe allergic reactions. Other amides are safer in this respect, though published data demonstrated their ability to cause anaphylactic shock, that was shown for mepivacaine [38] and bupivacaine [39]. French Pharmacovigilance Database System analysis revealed a twentyfold growth of reports on anaphylactic reactions involving local anesthetics from 1985 to 2020 year, and lidocaine was reported to be the most common cause (81.49%) [40]. Leading role of lidocaine in severe HSRs and in anaphylaxis development in dental practice was stated in the work by Matveev AV et al (2020) [41]. Anesthetics (first, lidocaine, second – bupivacaine) were reported among top eight pharmacotherapeutic groups involved in anaphylaxis based on results of Vietnamese Pharmacovigilance Database analysis [21].
NSAIDs are a common cause of hypersensitivity [25] responsible for a significant proportion of anaphylaxis in clinical practice of tertiary care hospitals and emergency departments [8, 21, 24, 42]. Our data revealed COX-inhibitors (NSAIDs, acetaminophen and metamizole) to be the third causative group among total (10.1%, main drug - acetaminophen) and pediatric SRsAS (6.0%, main drug - acetaminophen), and the fourth - among elderly SRsAs (7.7%, main drug - diclofenac). Fatal SRsAs analysis revealed COX-inhibitors only in 1.8% (two cases - diclofenac, one case - ibuprofen). In the USA NSAIDs (ibuprofen and naproxen) were the second cause of anaphylactic reactions (13.0%) after ABs (61%) [11], while in Poland NSAIDs were the main causative pharmacological group (acetylsalicylic acid, ketoprofen, metamizole and ibuprofen) [19]. These results are supported by the FAERS database analysis (study period 1999 to 2019) by Yu RJ et al (2021), which revealed acetaminophen and NSAIDs (acetylsalicylic acid, celecoxib, diclofenac) among top 50 drugs causing anaphylaxis [23]. Based on the analysis of a Vietnamese Pharmacovigilance Database NSAIDs were found to be a second pharmacological group involved in drug-induced anaphylaxis [21]. Published data indicate that in children NSAIDs are a second significant pharmacological group causing anaphylaxis after ABs [43]. Our results revealed acetaminophen to be the leader among COX-inhibitor in total SRsAs and pediatric SRsAs., and no fatal cases involving acetaminophen were detected. EudraVigilance Database analysis (2007–2018) found that acetaminophen-induced anaphylaxis was most common at age group 18–64 years, and among acetaminophen-induced ARs anaphylaxis was the second cause of death after hepatic failure with shock [44]. A systematic review of 85 studies reporting hypersensitivity reactions to acetaminophen revealed that acetaminophen hypersensitivity reaction prevalence among children was 10.1% (95% confidence interval 4.5-15.5) [45]. A retrospective analysis of 159 validated spontaneous reports in children (database of German Federal Institute for Drugs and Medical Devices) revealed another COX-inhibitor, ibuprofen, to be the main drug responsible for anaphylaxis development [46].
According to our results ICCM were identified in 6.6% of SRsAs (n - 153), with the most common agents iopromide and iohexol. ICCM were on the third place among causative drugs in the elderly SRsAs (12.3%). This group of agents is known to mediate severe hypersensitivity reactions which may lead to a lethal outcome [47, 48]. ICCM group was reported to be a leader among drugs involved in anaphylaxis due to the results of 13-year period analysis of Japanese Adverse Drug Event Report (JADER) database [49]. Based on the results of a 10-year study in China, total radiocontrast agents accounted for 11.9%, ICCM - for 9.5% [18]. Pagani S et al (2022) demonstrated association of anaphylaxis with radiology contrast agents in 6.92% [17]. Nguyen KD et al (2019) reported contrast media to be on the fourth place among all pharmacological groups caused drug-induced anaphylaxis [21]. FAERS database analysis reported iohexol, iopamidol and iopromide among top 50 drugs involved in anaphylaxis [23]. Published studies suggest that anaphylaxis due to radiocontrast medium is more common in older age and on repeated drug exposure [50].
Our study reported CV-drugs to be the fourth significant group involved in anaphylaxis in total SRsAs (6.2%, n - 143) with next most common groups: ACEIs (enalapril, captopril, perindopril), beta-blockers (bisoprolol, metoprolol, atenolol), and calcium channel blockers (nifedipine, amlodipine, verapamil). In the elderly CV-drugs were the second group caused anaphylaxis (20%, n - 13). ACEIs and beta-blockers are known causes of anaphylaxis in clinical practice [51]. A systematic review and meta-analysis of observational studies stated that beta-blockers and ACEIs increase the severity of anaphylaxis (beta-blockers, odds ratio [OR] 2.19, 95% confidence interval [CI] 1.25-3.84; ACEIs, OR 1.56, 95% CI 1.12-2.16) [52]. Anaphylaxis severity was shown to be increased with ACEIs intake along with presence of such factors as mastocytosis, and high fever prior to anaphylaxis [53]. Published studies based on pharmacovigilance databases revealed less significance of CV-drugs in anaphylaxis compared with our results. FAERS analysis reported no CV-agents among top-50 drugs causing anaphylaxis [23]. Vietnamese Pharmacovigilance Database analysis revealed cardiac therapy agents on the 22nd place among drugs involved in anaphylaxis [21], a 10 year retrospective analysis of the Beijing Pharmacovigilance Database reported cardiovascular medications accounted for 0.9% of drug-induced anaphylaxis [18].
The total number of SRsAs with causative agents being CNS-active drugs in our study was 35 (1.5%) with the leading role of fentanyl, diazepam, and tramadol. Published clinical studies revealed relatively low incidence of fentanyl-associated anaphylaxis [54, 55], mainly cases are reported [56 - 59]. Low frequency of anaphylaxis is also known for benzodiazepines [60], though diazepam is considered to be more common cause of allergy compared with midazolam [61]. Pagani S et al (2022) indicated a frequency of anaphylaxis due to tramadol equal to 0.32%, 2/608 [17], and literature analysis revealed only several cases of tramadol-induced anaphylaxis [62 - 64]. From the other hand, some studies based on pharmacovigilance database analysis revealed a significant role for several drugs affecting CNS. FAERS database analysis reported fentanyl, midazolam, propofol, and sufentanyl among top-50 drugs involved in anaphylaxis [23], Vietnamese Pharmacovigilance Database analysis indicated analgesic opioids and psychostimulants were on the 18th and 19th positions among groups involved in anaphylaxis [21].
NMBAs in our study accounted for 1.43% (n - 33), and the most prevalent were rocuronium and suxamethonium. NMBAs are the most frequent allergens responsible for acute hypersensitivity reactions during anaesthesia [65 - 67], and leading causative agents for perioperative anaphylaxis [68]. A French pharmacovigilance survey from 2000 to 2012 revealed suxamethonium and rocuronium to be the most common NMBAs causing ARs [69]. Atracurium, rocuronium, and succinylcholine were listed among top 50 drugs involved in anaphylaxis based on FAERS analysis [23].
According to fatal SRsAs analysis most of cases were due to ABs (and beta-lactams among ABs), which is in complete accordance with published data. Beta-lactam antibiotics, muscle relaxants, and injected radiocontrast medium were the main triggers of fatal drug anaphylaxis based on analysis made by Turner PJ et al (2017) [70] and the higher prevalence of ABs among drugs involved in total ARs and fatal ARs is also proved by the vast majority of reported studies in adults and children [11, 17, 18, 23, 43, 71, 72].
Published data indicate that drug-induced anaphylaxis is associated with more lethal cases than food-induced and venom-induced [73]. Actuality of the problem is supported by increasing number of fatal cases reported in modern studies. A systematic review of 46 observational studies reported increased frequency of deaths due to drug-induced anaphylaxis during the study period (IRR per year, 1.02; 95% CI, 1.00-1.04), and the highest rates were detected for Australian region [74]. Jerschow E et al (2014) stated a significant increase in fatal drug-induced anaphylaxis over 12 years (from 0.27 (95% CI, 0.23-0.30) per million in 1999 to 2001 to 0.51 (95% CI, 0.47-0.56) per million in 2008 to 2010 (p< 0.001) [75]. Fatal SRsAs percentage reported in our study (9.5%) exceeds published values. FAERS database analysis revealed 6.28% (2,984/47,496) reports of anaphylaxis followed by death [23], Brazilian Hospital Information System – 5.8% [76], Beijing Pharmacovigilance Database – 3.3% (39/1,189) [18], Vietnamese Pharmacovigilance Database analysis - about 2.3% (111/4,873) [21]. The rate of fatal drug-induced anaphylaxis in Spain was 1.02% [77], and Latin American anaphylaxis registry revealed that only 0.3% of cases were fatal [78].
Our study has some limitations. First, retrospective design of the study based on the analysis of SRsAs entered in the AIS “Pharmacovigilance” made it impossible to evaluate the effect of concomitant medications and comorbidities, laboratory tests performed, and to estimate risks of anaphylaxis in different populations.
It is worth to note, that the number of SRsAs reported in our study was based on the analysis of spontaneous reporting records and thus cannot completely reflect the prevalence of anaphylaxis in a real clinical practice. Reported proportions of drugs involved in anaphylaxis described in our study may be determined not by their true safety profile, but by a frequency of their prescribing. E.g.: an absolute leader determined in our study was ceftriaxone, and it is one of the most prescribed drugs to treat various infectious diseases worldwide, ranging from 2.5% of therapeutic prescriptions in Northern Europe to 24.8% in Eastern Europe; also it is the most prescribed AB for a surgical prophylaxis (34.4% of ABs prescriptions in Eastern Europe, 24.8% in Southern Europe, 23.6% in West and Central Asia, and 19.7% in Northern Africa) [79]. A promising approach to assess real world prevalence of ARs due to a drug may be based on a parallel assessment of a drug consumption rates.
4. Materials and Methods
4.1. Data Source
Federal Service for Surveillance in Healthcare (Roszdravnadzor) is responsible for drug safety and effectiveness monitoring in the Russian Federation. Spontaneous/voluntary adverse reaction (AR) reporting is regulated by legislation in the Russian Federation. All reports are directed to the AIS “Pharmacovigilance” database which is a national pharmacovigilance database. It was established in 2008 and its structure, functioning and management comply with ICH E2B (R3) standard [80]. AIS “Pharmacovigilance” uses MedDRA version 25.0 as a reference tool [81]. Drugs are identified by brand name and international nonproprietary names (INN), which are both selected automatically by reporters when they fill out the official reporting form. Drug categories are determined in accordance with ATC classification. Causality assessment is made in AIS “Pharmacovigilance” by built-in WHO algorithm and Naranjo algorithm. Signal detection is performed using built-in quantitative statistical methods (proportional reporting ratio, PRR; reporting odds ratio, ROR; reduced rank regression, RRR). AIS “Pharmacovigilance” receives ARs reports on all drugs registered and approved for use in the Russian Federation, and cases occurred abroad. SRs may come from medical professionals, pharmaceutical companies, patients, and their representatives. In June 2023 the total number of individual case safety reports in AIS was >2 100 000 and no cases of reports made by patients, or their representatives were presented. Most of reports were generated by healthcare workers (mainly from hospitals).
4.2. Definitions
For this study, we used the following definitions [82]:
- “Adverse reaction - a response to a medicinal product, which is noxious and unintended. Adverse reaction may arise from use of the product within or outside the terms of the marketing authorization or from occupational exposure. Use outside the marketing authorization includes off-label use, overdose, misuse, abuse and medication errors”.
- “Causality: In accordance with ICH-E2A, the definition of an adverse reaction implies at least a reasonable possibility of a causal relationship between a suspected medicinal product and an adverse event. An adverse reaction, in contrast to an adverse event, is characterized by the fact that a causal relationship between a medicinal product and an occurrence is suspected. For regulatory reporting purposes, as detailed in ICH-E2D, if an event is spontaneously reported, even if the relationship is unknown or unstated, it meets the definition of an adverse reaction. Therefore all spontaneous reports notified by healthcare professionals or consumers are considered suspected adverse reactions, since they convey the suspicions of the primary sources, unless the reporters specifically state that they believe the events to be unrelated or that a causal relationship can be excluded”.
- “A spontaneous report is an unsolicited communication by a healthcare professional, or consumer to a competent authority, marketing authorisation holder or other organisation (e.g. regional pharmacovigilance centre, poison control centre) that describes one or more suspected adverse reactions in a patient who was given one or more medicinal products. It does not derive from a study or any organised data collection systems”.
4.3. Study Design and Data Selection
Study design: a retrospective, descriptive study of SRs accumulated in AIS “Pharmacovigilance” database. Study period: 02.04.2019 - 21.06.2023.
Data selection was made using several steps described at Figure 2. First, from the total number of reports in AIS “Pharmacovigilance” SRs from the Russian Federation only were extracted with obligative inclusion criterion - high probability of a causal relationship (“certain”, “probable”, “possible”). Probability assessment was performed automatically in AIS “Pharmacovigilance” using built-in Naranjo algorithm. Second, using MedDRA high level group term (HLGT) «Allergic conditions» we defined the total number of SRs describing drug-induced allergy (SRsDIAs). Then we excluded duplicate and invalid reports getting exact number of SRsDIAs occurred in the Russian Federation. Validity was determined according to paragraph VI.B.2 of the EMA “Guideline on good pharmacovigilance practices” and paragraph 407 of the Eurasian Economic Union “Good pharmacovigilance practice”, which state that information in a SR must contain at least 4 elements: identifiable reporter; identifiable patient; at least one suspected drug; at least one suspected ADR. If any of these 4 elements is absent, the report is considered invalid [82, 83]. Next step we used MedDRA HLGT – «Anaphylactic reaction and anaphylactic shock» to detect SRs with anaphylaxis (SRsAs).
4.4. Drug Identification and Analyzed Categories
For this study, we used INN of suspected drugs, groups were distinguished according to the ATC classification. Drug identification did not distinguish between dosage forms or routes of administration.
Patient demographic information and data on causative drugs were extracted from the sample including SRsAs. All identified SRsAs were first analyzed. Then two age categories were defined: elderly (SRsA describing patients ≥65 years) and pediatric (SRsAs describing patients ≤18 years). The reported age was described in days, weeks, and years. Also, fatal SRsAs were estimated (SRsAs with a lethal outcome due to anaphylaxis).
4.5. Statistical Analysis
Descriptive statistics was used for all analyzed parameters; qualitative variables were described using absolute (n) and relative (%) values. All statistical analyses were performed using Microsoft Excel 2019. The percentage of SRsAs among SRsDIAs was estimated, mean age and sex differences were analyzed, the structure of causative drugs was detected.
5. Conclusions
SRs analysis performed in our work revealed anaphylaxis accounting for 8.3% of all drug-induced allergic reactions. In the structure of drugs involved leaders were ABs, LAs, ICCM, COX-inhibitors, CV drugs and CNS-active drugs. The number of pediatric SRsAs was almost twice as high as the number of SRsAs in the elderly (5.8% vs. 2.8%). Our results proved a higher prevalence of females with drug-induced anaphylaxis in all analyzed categories of SRsAs except the elderly (43.5%). Fatal SRsAs were reported in 9.5%, they were mainly caused by ABs, LAs, and CV-drugs. The highest percentage of deaths was observed in the elderly (46.2% (n - 30)), while in children it was 3.6 times less (12.78% (n – 17)). National pharmacovigilance databases and EHRs are important tools to assess the structure of drugs involved in various ARs including HSRs and to get information on demographic characteristics of patients [84], though a higher objectivity level of results may be obtained taking into account data on the actual drug consumption in real clinical practice.
Author Contributions
Conceptualization, O.I.B., S.K.Z..; resources, O.I.B., A.A.G., I.L.A. and V.A.P.; data curation, S.K.Z. and O.I.B.; search of data sources—O.I.B., V.A.P. and I.L.A.; writing—original draft preparation, O.I.B. and A.A.G.; writing—review and editing, O.I.B.; supervision, S.K.Z. and O.I.B. All authors have read and agreed to the published version of the manuscript.
Funding
“This research received no external funding”.
Institutional Review Board Statement
“Not applicable”.
Informed Consent Statement
“Not applicable”.
Data Availability Statement
Data were gained from https://newmimn.roszdravnadzor.gov.ru/.
Conflicts of Interest
“The authors declare no conflict of interest.”
References
- Cardona V, Ansotegui IJ, Ebisawa M, et al. World allergy organization anaphylaxis guidance 2020. World Allergy Organ J. 2020;13(10):100472. Published 2020 Oct 30. [CrossRef]
- Regateiro FS, Marques ML, Gomes ER. Drug-Induced Anaphylaxis: An Update on Epidemiology and Risk Factors. Int Arch Allergy Immunol. 2020;181(7):481-487. [CrossRef]
- Villarreal-González RV, Canel-Paredes A, Arias-Cruz A, et al. Alergia a medicamentos: aspectos fundamentales en el diagnóstico y tratamiento. Reporte de grupo del Colegio Mexicano de Inmunología Clínica y Alergia [Drug allergy: Fundamental aspects in diagnosis and treatment.]. Rev Alerg Mex. 2023;69(4):195-213. Published 2023 Apr 19. [CrossRef]
- Bruhns P, Chollet-Martin S. Mechanisms of human drug-induced anaphylaxis. J Allergy Clin Immunol. 2021;147(4):1133-1142. [CrossRef]
- Kiechle ES, McKenna CM, Carter H, et al. Medication Allergy and Adverse Drug Reaction Documentation Discrepancies in an Urban, Academic Emergency Department. J Med Toxicol. 2018;14(4):272-277. [CrossRef]
- Yu TC, Cunneen J. Prevalence of Antibiotic Allergy at a Spinal Cord Injury Center. Fed Pract. 2023;40(5):142-145. [CrossRef]
- Alkanhal R, Alhoshan I, Aldakhil S, et al. Prevalence triggers and clinical severity associated with anaphylaxis at a tertiary care facility in Saudi Arabia: A cross-sectional study. Medicine (Baltimore). 2018;97(31):e11582. [CrossRef]
- Alen Coutinho I, Ferreira D, Regateiro FS, et al. Anaphylaxis in an emergency department: a retrospective 10-year study in a tertiary hospital. Eur Ann Allergy Clin Immunol. 2020;52(1):23-34. [CrossRef]
- Wong A, Seger DL, Lai KH, Goss FR, Blumenthal KG, Zhou L. Drug Hypersensitivity Reactions Documented in Electronic Health Records within a Large Health System. J Allergy Clin Immunol Pract. 2019;7(4):1253-1260.e3. [CrossRef]
- Lerch M, Mainetti C, Terziroli Beretta-Piccoli B, Harr T. Current Perspectives on Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis. Clin Rev Allergy Immunol. 2018;54(1):147-176. [CrossRef]
- Dhopeshwarkar N, Sheikh A, Doan R, et al. Drug-Induced Anaphylaxis Documented in Electronic Health Records. J Allergy Clin Immunol Pract. 2019;7(1):103-111. [CrossRef]
- Wang C, Li Z, Yu Y, Feng M, Liu A. Active surveillance and clinical analysis of anaphylaxis based on the China Hospital Pharmacovigilance System. Front Pharmacol. 2023;14:1180685. Published 2023 Jul 11. [CrossRef]
- Yang SC, Hu S, Zhang SZ, et al. The Epidemiology of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis in China [published correction appears in J Immunol Res. 2018 Jun 28;2018:4154507]. J Immunol Res. 2018;2018:4320195. Published 2018 Feb 11. [CrossRef]
- Lee EY, Knox C, Phillips EJ. Worldwide Prevalence of Antibiotic-Associated Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Systematic Review and Meta-analysis. JAMA Dermatol. 2023;159(4):384–392. [CrossRef]
- Esh CJ, Chrismas BCR, Mauger AR, Taylor L. Pharmacological hypotheses: Is acetaminophen selective in its cyclooxygenase inhibition?. Pharmacol Res Perspect. 2021;9(4):e00835. [CrossRef]
- van Diepen ATN, Simons P, Bos JM, Kramers C. Pijnbestrijding met metamizol in de Nederlandse praktijk [Metamizol: current status in Dutch practice]. Ned Tijdschr Geneeskd. 2022;166:D6182. Published 2022 Jan 19.
- Pagani S, Lombardi N, Crescioli G, et al. Drug-Related Hypersensitivity Reactions Leading to Emergency Department: Original Data and Systematic Review. J Clin Med. 2022;11(10):2811. Published 2022 May 16. [CrossRef]
- Zhao Y, Sun S, Li X, et al. Drug-induced anaphylaxis in China: a 10 year retrospective analysis of the Beijing Pharmacovigilance Database. Int J Clin Pharm. 2018;40(5):1349-1358. [CrossRef]
- Poziomkowska-Gęsicka I, Kurek M. Clinical Manifestations and Causes of Anaphylaxis. Analysis of 382 Cases from the Anaphylaxis Registry in West Pomerania Province in Poland. Int J Environ Res Public Health. 2020;17(8):2787. Published 2020 Apr 17. [CrossRef]
- Ben Mansour, A. , Daghfous H., Ben Saad S., Slim A., Bellali H., Tritar F. Drug related severe anaphylaxis investigation: A Tunisian retrospective study. Revue Française d'Allergologie. 2023;63(2):103309. [CrossRef]
- Nguyen KD, Nguyen HA, Vu DH, et al. Drug-Induced Anaphylaxis in a Vietnamese Pharmacovigilance Database: Trends and Specific Signals from a Disproportionality Analysis. Drug Saf. 2019;42(5):671-682. [CrossRef]
- Ahn KM, Kim BK, Yang MS. Risk factors of anaphylaxis in Korea: Identifying drug-induced anaphylaxis culprits using big data. Medicine (Baltimore). 2022;101(35):e30224. [CrossRef]
- Yu RJ, Krantz MS, Phillips EJ, Stone CA Jr. Emerging Causes of Drug-Induced Anaphylaxis: A Review of Anaphylaxis-Associated Reports in the FDA Adverse Event Reporting System (FAERS). J Allergy Clin Immunol Pract. 2021;9(2):819-829.e2. [CrossRef]
- Sari Dogan F, Ozaydin V. Drug-induced anaphylaxis in the emergency department: A prospective observational study. North Clin Istanb. 2021;8(6):595-600. Published 2021 Dec 31. [CrossRef]
- Demir S, Erdenen F, Gelincik A, et al. Evaluation of the Potential Risk Factors for Drug-Induced Anaphylaxis in Adult Patients. Int Arch Allergy Immunol. 2019;178(2):167-176. [CrossRef]
- Khan DA, Banerji A, Bernstein JA, et al. Cephalosporin Allergy: Current Understanding and Future Challenges. J Allergy Clin Immunol Pract. 2019;7(7):2105-2114. [CrossRef]
- D'Errico S, Frati P, Zanon M, et al. Cephalosporins' Cross-Reactivity and the High Degree of Required Knowledge. Case Report and Review of the Literature. Antibiotics (Basel). 2020;9(5):209. Published 2020 Apr 25. [CrossRef]
- Romano A, Valluzzi RL, Caruso C, Zaffiro A, Quaratino D, Gaeta F. Evaluating Immediate Reactions to Cephalosporins: Time Is of the Essence. J Allergy Clin Immunol Pract. 2021;9(4):1648-1657.e1. [CrossRef]
- Mori F, Liccioli G, Piccorossi A, et al. The Diagnosis of Ceftriaxone Hypersensitivity in a Paediatric Population. Int Arch Allergy Immunol. 2019;178(3):272-276. [CrossRef]
- Jung IY, Kim JJ, Lee SJ, et al. Antibiotic-Related Adverse Drug Reactions at a Tertiary Care Hospital in South Korea. Biomed Res Int. 2017;2017:4304973. [CrossRef]
- Rhyou HI, Nam YH, Kim SC, et al. Cefaclor-induced hypersensitivity: Differences in the incidence of anaphylaxis relative to other 2nd and 3rd generation cephalosporins. PLoS One. 2021;16(7):e0254898. Published 2021 Jul 22. [CrossRef]
- Jevon P, Shamsi S. Management of anaphylaxis in the dental practice: an update. Br Dent J. 2020;229(11):721-728. [CrossRef]
- Zuo J, Gong R, Liu X, Zhao J. Risk of True Allergy to Local Anesthetics: 10-Year Experience from an Anesthesia Allergy Clinic in China. Ther Clin Risk Manag. 2020;16:1297-1303. Published 2020 Dec 29. [CrossRef]
- Liu, X., Gong, R., Xin, X. et al. Clinical characteristics and allergen detection of perioperative anaphylaxis: a 12-year retrospective analysis from an anesthesia clinic in China. Perioper Med 11, 5 (2022). [CrossRef]
- Park KK, Sharon VR. A Review of Local Anesthetics: Minimizing Risk and Side Effects in Cutaneous Surgery. Dermatol Surg. 2017;43(2):173-187. [CrossRef]
- Bhole MV, Manson AL, Seneviratne SL, Misbah SA. IgE-mediated allergy to local anaesthetics: separating fact from perception: a UK perspective [published correction appears in Br J Anaesth. 2012 Oct;109(4):669]. Br J Anaesth. 2012;108(6):903-911. [CrossRef]
- Cherobin ACFP, Tavares GT. Safety of local anesthetics. An Bras Dermatol. 2020;95(1):82-90. [CrossRef]
- Takahashi, M., Hotta, K., Inoue, S. et al. Mepivacaine-induced anaphylactic shock in a pregnant woman undergoing combined spinal and epidural anesthesia for cesarean delivery: a case report. JA Clin Rep 5, 84 (2019). [CrossRef]
- Simionescu AA, Danciu BM, Stanescu AMA. Severe Anaphylaxis in Pregnancy: A Systematic Review of Clinical Presentation to Determine Outcomes. Journal of Personalized Medicine. 2021; 11(11):1060. [CrossRef]
- Hascoët E, Mahé J, Meillard H, Théophile H, Cloitre A, Lesclous P. Anaphylactic reac-tions to local anesthetics in dental practice: a nationwide French retrospective study. Clin Oral Investig. 2022;26(2):1667-1676. [CrossRef]
- Matveev AV, Krasheninnikov AE, Yagudina RI, Egorova EA, Konyaeva EI. Nezhelatel'nye reaktsii na mestnye anestetiki pri ikh primenenii v stomatologii [Adverse drug reactions of local anesthetics used in dentistry]. Stomatologiia (Mosk). 2020;99(6):82-88. [CrossRef]
- Blanca-Lopez N, Soriano V, Garcia-Martin E, Canto G, Blanca M. NSAID-induced reactions: classification, prevalence, impact, and management strategies. J Asthma Allergy. 2019;12:217-233. Published 2019 Aug 8. [CrossRef]
- Cimen SS, Suleyman A, Yucel E, Guler N, Tamay Z. Evaluation of the triggers and the treatment models of anaphylaxis in pediatric patients. North Clin Istanb. 2023;10(5):609-617. Published 2023 Aug 25. [CrossRef]
- Popiołek I, Piotrowicz-Wójcik K, Porebski G. Hypersensitivity Reactions in Serious Adverse Events Reported for Paracetamol in the EudraVigilance Database, 2007⁻2018. Pharmacy (Basel). 2019;7(1):12. Published 2019 Jan 17. [CrossRef]
- Gabrielli S, Langlois A, Ben-Shoshan M. Prevalence of Hypersensitivity Reactions in Children Associated with Acetaminophen: A Systematic Review and Meta-Analysis. Int Arch Allergy Immunol. 2018;176(2):106-114. [CrossRef]
- Sachs B, Dubrall D, Fischer-Barth W, Schmid M, Stingl J. Drug-induced anaphylactic reactions in children: A retrospective analysis of 159 validated spontaneous reports. Pharmacoepidemiol Drug Saf. 2019;28(3):377-388. [CrossRef]
- Qiu L, Cui Q, Gong X, Zhou H. Anaphylaxis Following Contrast-Enhanced CT with Iodixanol: A Case Report and Literature Review [published correction appears in J Asthma Allergy. 2023 Mar 02;16:239-240]. J Asthma Allergy. 2023;16:195-200. Published 2023 Jan 25. [CrossRef]
- Fukushima Y, Taketomi-Takahashi A, Suto T, Hirasawa H, Tsushima Y. Clinical features and risk factors of iodinated contrast media (ICM)-induced anaphylaxis. Eur J Radiol. 2023;164:110880. [CrossRef]
- Sugizaki C, Sato S, Yanagida N, Ebisawa M. Analysis of drug-induced anaphylaxis cases using the Japanese Adverse Drug Event Report (JADER) database - secondary publication. Allergol Int. 2023;72(4):580-587. [CrossRef]
- Kim MH, Lee SY, Lee SE, et al. Anaphylaxis to iodinated contrast media: clinical characteristics related with development of anaphylactic shock. PLoS One. 2014;9(6):e100154. Published 2014 Jun 16. [CrossRef]
- Coop CA, Schapira RS, Freeman TM. Are ACE Inhibitors and Beta-blockers Dangerous in Patients at Risk for Anaphylaxis?. J Allergy Clin Immunol Pract. 2017;5(5):1207-1211. [CrossRef]
- Tejedor-Alonso MA, Farias-Aquino E, Pérez-Fernández E, Grifol-Clar E, Moro-Moro M, Rosado-Ingelmo A. Relationship Between Anaphylaxis and Use of Beta-Blockers and Angiotensin-Converting Enzyme Inhibitors: A Systematic Review and Meta-Analysis of Observational Studies. J Allergy Clin Immunol Pract. 2019;7(3):879-897.e5. [CrossRef]
- Yeğit OO, Aslan AF, Coşkun R, et al. Comparison of recent anaphylaxis diagnostic criteria in real life: Can more patients be diagnosed as having anaphylaxis?. World Allergy Organ J. 2023;16(8):100810. Published 2023 Aug 26. [CrossRef]
- Teshigawara A, Nishibe S, Horie S, et al. Fentanyl-associated anaphylaxis in an infant with tetralogy of Fallot: a case report. JA Clin Rep. 2019;5(1):34. Published 2019 May 21. [CrossRef]
- Laguna JJ, Archilla J, Doña I, et al. Practical Guidelines for Perioperative Hypersensitivity Reactions. J Investig Allergol Clin Immunol. 2018;28(4):216-232. [CrossRef]
- Teshigawara A, Nishibe S, Horie S, et al. Fentanyl-associated anaphylaxis in an infant with tetralogy of Fallot: a case report. JA Clin Rep. 2019;5(1):34. Published 2019 May 21. [CrossRef]
- Tomar GS, Tiwari AK, Chawla S, Mukherjee A, Ganguly S. Anaphylaxis related to fentanyl citrate. J Emerg Trauma Shock. 2012;5(3):257-261. [CrossRef]
- Joo J, Bae H, Lee J. Intraoperative allergic reaction to fentanyl: A case report. Korean J Anesthesiol. 2009;57(6):776-779. [CrossRef]
- Belso N, Kui R, Szegesdi I, et al. Propofol and fentanyl induced perioperative anaphylaxis. Br J Anaesth. 2011;106(2):283-284. [CrossRef]
- Haybarger E, Young AS, Giovannitti JA Jr. Benzodiazepine Allergy With Anesthesia Administration: A Review of Current Literature. Anesth Prog. 2016;63(3):160-167. [CrossRef]
- Mali S. Anaphylaxis during the perioperative period. Anesth Essays Res. 2012;6(2):124-133. [CrossRef]
- Mori F, Barni S, Manfredi M, et al. Anaphylaxis to Intravenous Tramadol in a Child. Pharmacology. 2015;96(5-6):256-258. [CrossRef]
- Hallberg P., Brenning G. Angioedema induced by tramadol—a potentially life-threatening condition. European Journal of Clinical Pharmacology. 2005;60: 901-903. [CrossRef]
- Arslan K. Tramadol-Induced Anaphylaxis: A Rare Case. Türkiye Klinikleri Journal of Case Reports. 2022;30(4): 238 – 241. [CrossRef]
- Dejoux A, de Chaisemartin L, Bruhns P, Longrois D, Gouel-Chéron A. Neuromuscular blocking agent induced hypersensitivity reaction exploration: an update. Eur J Anaesthesiol. 2023;40(2):95-104. [CrossRef]
- Di Leo E, Delle Donne P, Calogiuri GF, Macchia L, Nettis E. Focus on the agents most frequently responsible for perioperative anaphylaxis. Clin Mol Allergy. 2018;16:16. Published 2018 Jul 9. [CrossRef]
- Misbah SA, Krishna MT. Peri-Operative Anaphylaxis-An Investigational Challenge. Front Immunol. 2019;10:1117. Published 2019 May 29. [CrossRef]
- Zou Y, Shao LJ, Xue FS. Perioperative anaphylaxis: a potential hazard to the safety of surgical patients. Chin Med J (Engl). 2020;133(5):609-612. [CrossRef]
- Petitpain N, Argoullon L, Masmoudi K, et al. Neuromuscular blocking agents induced anaphylaxis: Results and trends of a French pharmacovigilance survey from 2000 to 2012. Allergy. 2018;73(11):2224-2233. [CrossRef]
- Turner PJ, Jerschow E, Umasunthar T, Lin R, Campbell DE, Boyle RJ. Fatal Anaphylaxis: Mortality Rate and Risk Factors. J Allergy Clin Immunol Pract. 2017;5(5):1169-1178. [CrossRef]
- Xing Y, Zhang H, Sun S, et al. Clinical features and treatment of pediatric patients with drug-induced anaphylaxis: a study based on pharmacovigilance data. Eur J Pediatr. 2018;177(1):145-154. [CrossRef]
- Cavkaytar O, Karaatmaca B, Cetinkaya PG, et al. Characteristics of drug-induced anaphylaxis in children and adolescents. Allergy Asthma Proc. 2017;38(5):56-63. [CrossRef]
- Bilò MB, Corsi A, Martini M, Penza E, Grippo F, Bignardi D. Fatal anaphylaxis in Italy: Analysis of cause-of-death national data, 2004-2016. Allergy. 2020;75(10):2644-2652. [CrossRef]
- Perez-Codesido S, Rosado-Ingelmo A, Privitera-Torres M, et al. Incidence of Fatal Anaphylaxis: A Systematic Review of Observational Studies. J Investig Allergol Clin Immunol. 2022;32(4):245-260. [CrossRef]
- Jerschow E, Lin RY, Scaperotti MM, McGinn AP. Fatal anaphylaxis in the United States, 1999-2010: temporal patterns and demographic associations. J Allergy Clin Immunol. 2014;134(6):1318-1328.e7. [CrossRef]
- Tanno LK, Molinari N, Annesi-Maesano I, Demoly P, Bierrenbach AL. Anaphylaxis in Brazil between 2011 and 2019. Clin Exp Allergy. 2022;52(9):1071-1078. [CrossRef]
- Tejedor-Alonso MA, Martínez-Fernandez P, Vallejo-de-Torres G, Navarro-Escayola E, Moro-Moro M, Alberti-Masgrau N. Clinical and demographic characteristics of fatal anaphylaxis in Spain (1998-2011): A comparison between a series from the hospital system and a national forensic series. Clin Exp Allergy. 2019;49(1):82-91. [CrossRef]
- Jares EJ, Cardona V, Gómez RM, et al. Latin American anaphylaxis registry. World Allergy Organ J. 2023;16(2):100748. Published 2023 Feb 5. [CrossRef]
- Pauwels I, Versporten A, Drapier N, Vlieghe E, Goossens H; Global-PPS network. Hospital antibiotic prescribing patterns in adult patients according to the WHO Access, Watch and Reserve classification (AWaRe): results from a worldwide point prevalence survey in 69 countries. J Antimicrob Chemother. 2021;76(6):1614-1624. [CrossRef]
- European Medicines Agency. ICH E2B (R3) Electronic transmission of individual case safety reports (ICSRs) – data elements and message specification – implementation guide – Scientific guideline. Available online: https://www.ema.europa.eu/en/ich-e2b-r3-electronic-transmission-individual-case-safety-reports-icsrs-data-elements-message (Accessed 18 November 2023).
- MedDRA. Available online: https://www.meddra.org/how-to-use/support-documentation/english (Accessed 18 November 2023).
- European Medicines Agency. Guideline on good pharmacovigilance practices (GVP) Module VI – Collection, management and submission of reports of suspected adverse reactions to medicinal products (Rev 2). Available online: https://www.ema.europa.eu/en/documents/regulatory-procedural-guideline/guideline-good-pharmacovigilance-practices-gvp-module-vi-collection-management-submission-reports_en.pdf (Accessed 18 November 2023).
- Eurasian Economic Union “Good pharmacovigilance practice” guideline (edition No. 2 dated 05/19/2022). Available online: https://docs.eaeunion.org/docs/ru-ru/01433831/err_09062022_81 (Accessed 18 Nov 2023).
- Bassir F, Varghese S, Wang L, Chin YP, Zhou L. The Use of Electronic Health Records to Study Drug-Induced Hypersensitivity Reactions from 2000 to 2021: A Systematic Re-view. Immunol Allergy Clin North Am. 2022;42(2):453-497. [CrossRef]
Figure 1.
Prevalence (%) of fatal ARs among pharmacological groups compared with the structure of pharmacological groups involved in ARs.
Figure 1.
Prevalence (%) of fatal ARs among pharmacological groups compared with the structure of pharmacological groups involved in ARs.
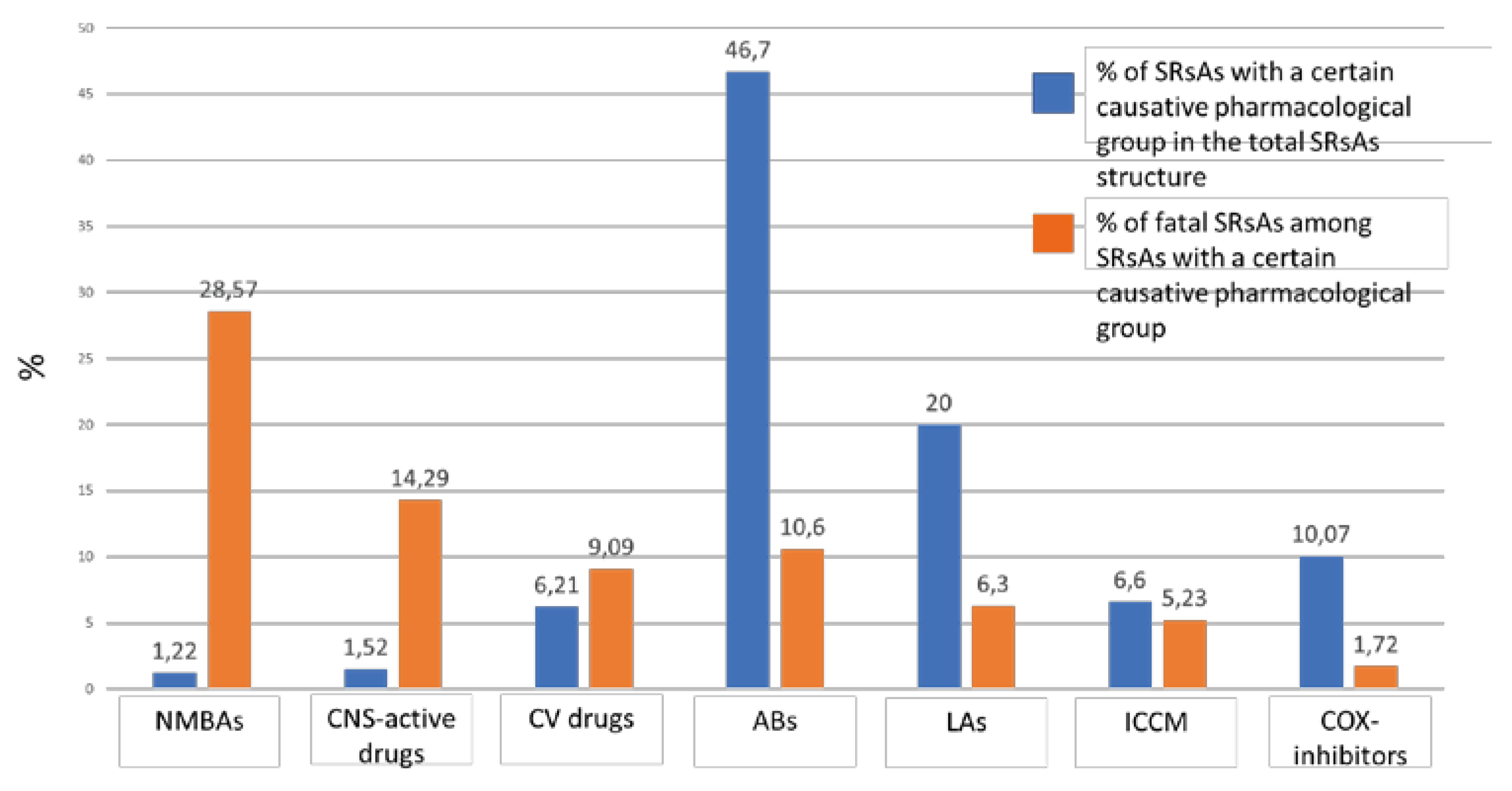
Figure 2.
Flowchart of SRsAs selection from AIS “Pharmacovigilance”.
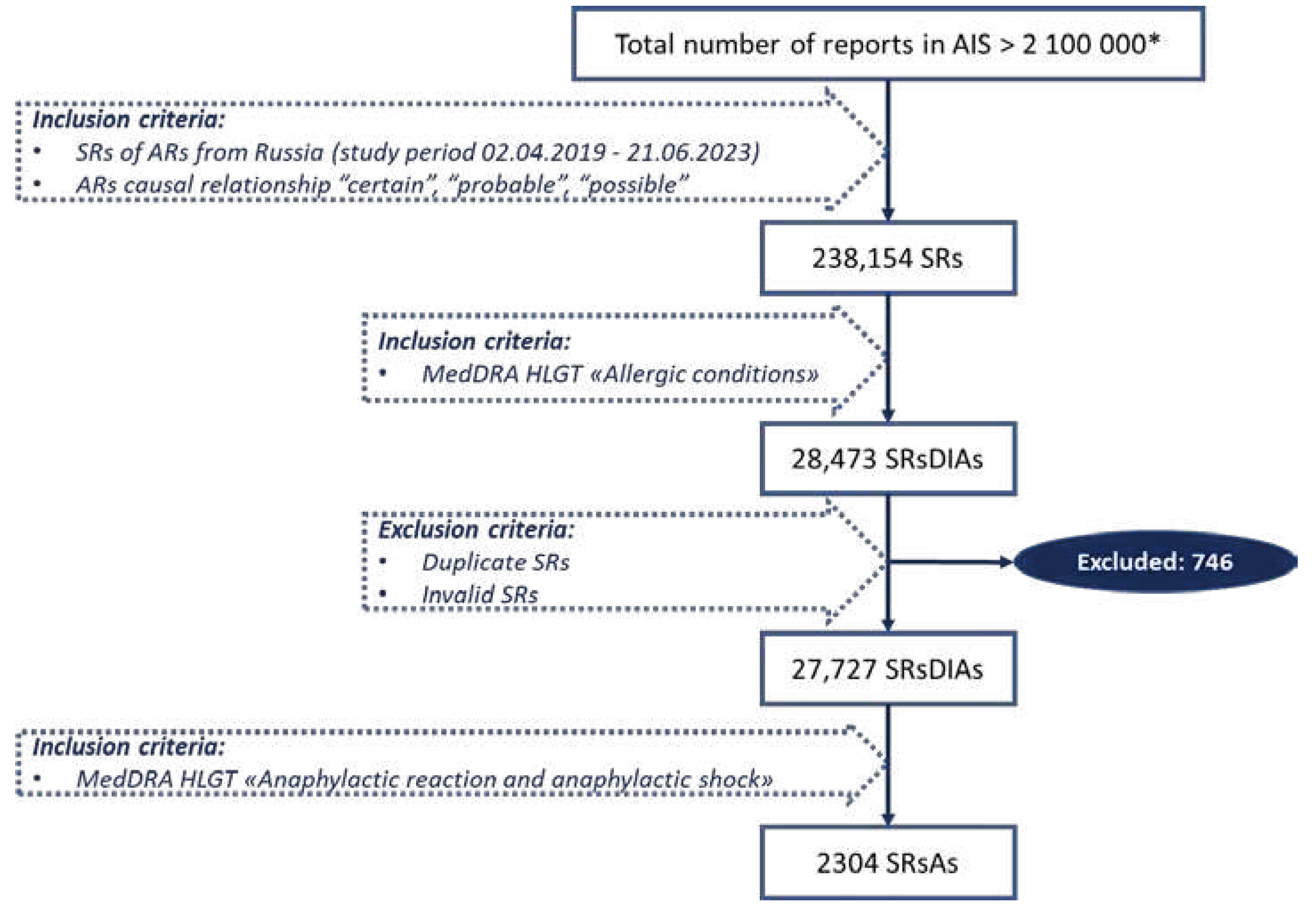

Table 1.
The Structure of ABs involved in anaphylaxis.
| ABs | N (Total - 1028) |
% |
|---|---|---|
| Beta-lactams | 902 | 87.7 |
| Ceftriaxone | 687 | 66.8 |
| Cefotaxime | 87 | 8.5 |
| Cefazolin | 39 | 3.8 |
| Ampicillin sulbactam | 17 | 1.7 |
| Cefepime | 15 | 1.5 |
| Cefuroxime | 10 | 1.0 |
| Meropenem | 10 | 1.0 |
| Amoxicillin clavulanate | 8 | 0.8 |
| Cefoperazone sulbactam | 7 | 0.7 |
| Ertapenem | 5 | 0.5 |
| Cefoperazone | 4 | 0.4 |
| Ampicillin | 4 | 0.4 |
| Cefepime sulbactam | 3 | 0.3 |
| Amoxicillin sulbactam | 2 | 0.2 |
| Piperacillin tazobactam | 2 | 0.2 |
| Cephalexin | 1 | 0.1 |
| Cefixime | 1 | 0.1 |
| Other | 126 | 12.3 |
| Vancomycin | 28 | 2.7 |
| Ciprofloxacin | 22 | 2.1 |
| Levofloxacin | 18 | 1.8 |
| Metronidazole | 14 | 1.4 |
| Linezolid | 7 | 0.7 |
| Amikacin | 7 | 0.7 |
| Nitrofurantoin | 7 | 0.7 |
| Fosfomycin | 5 | 0.5 |
| Sulfamethoxazole trimethoprim | 3 | 0.3 |
| Tigecycline | 3 | 0.3 |
| Polymyxin B | 2 | 0.2 |
| Kanamycin | 2 | 0.2 |
| Amphotericin B | 2 | 0.2 |
| Gentamicin | 1 | 0.1 |
| Ofloxacin | 1 | 0.1 |
| Erythromycin | 1 | 0.1 |
| Clindamycin | 1 | 0.1 |
| Rifampicin | 1 | 0.1 |
| Isoniazid | 1 | 0.1 |
Table 2.
The Structure of LAs involved in anaphylaxis.
| LAs | N (Total - 460) |
% |
|---|---|---|
| Lidocaine | 293 | 63.7 |
| Procaine | 68 | 14.8 |
| Articaine | 61 | 13.3 |
| Ropivacaine | 16 | 3.5 |
| Bupivacaine | 14 | 3.0 |
| Mepivacaine | 8 | 1.7 |
Among SRsAs caused by LAs lethal outcome was reported in 29 cases (6.3%).
Table 3.
The Structure of COX-inhibitors involved in anaphylaxis.
| COX-inhibitors | N (Total - 232) |
% |
|---|---|---|
| Acetaminophen | 49 | 21.1 |
| Metamizole | 48 | 20.7 |
| Ibuprofen | 35 | 15.1 |
| Diclofenac | 29 | 12.5 |
| Ketorolac | 26 | 11.2 |
| Acetylsalicylic acid | 25 | 10.8 |
| Ketoprofen | 6 | 3.0 |
| Celecoxib | 5 | 2.2 |
| Aceclofenac | 3 | 1.3 |
| Meloxicam | 3 | 1.3 |
| Lornoxicam | 2 | 0.9 |
| Nimesulide | 1 | 0.4 |
Among SRsAs where COX-inhibitors were causative drugs lethal outcome was reported in 4 cases (1.72%).
Table 4.
The Structure of ICCM involved in anaphylaxis.
| ICCM | N (Total - 153) |
% |
|---|---|---|
| Iopromide | 97 | 63.4 |
| Iohexol | 39 | 25.5 |
| Iomeprol | 13 | 8.5 |
| Iodixanol | 2 | 1.3 |
| Ioversol | 1 | 0.7 |
| Iopamidol | 1 | 0.7 |
Lethal outcome was reported in 8 cases (5.2%).
Table 5.
The Structure of CV Drugs involved in Anaphylaxis.
| CV drug | N (Total – 143) |
% |
|---|---|---|
| ACEIs | 29 | 20.3 |
| Enalapril | 17 | 11.9 |
| Captopril | 11 | 7.8 |
| Perindopril | 1 | 0.7 |
| Beta-blockers | 22 | 15.4 |
| Bisoprolol | 13 | 9.1 |
| Metoprolol | 5 | 3.5 |
| Atenolol | 3 | 2.1 |
| Propranolol | 1 | 0.7 |
| Calcium Channel Blockers | 21 | 14.7 |
| Nifedipine | 9 | 6.3 |
| Amlodipine | 8 | 5.6 |
| Verapamil | 4 | 2.8 |
| Potassium-magnesium-asparaginate | 19 | 13.3 |
| Antiarrhythmics | 12 | 8.4 |
| Amiodarone | 10 | 7.0 |
| Digoxin | 1 | 0.7 |
| Propafenone | 1 | 0.7 |
| Diuretics | 11 | 7.7 |
| Furosemide | 7 | 4.9 |
| Spironolactone | 3 | 2.1 |
| Hydrochlorothiazide | 1 | 0.7 |
| Sartans (Losartan) | 8 | 5.6 |
| Statins | 6 | 4.2 |
| Rosuvastatin | 4 | 2.8 |
| Atorvastatin | 2 | 1.4 |
| Alpha-2 adrenergic receptor agonist (Clonidine) | 4 | 2.8 |
| Indirect oral anticoagulant (Warfarin) | 4 | 2.8 |
| Direct oral anticoagulants | 2 | 1.4 |
| Rivaroxaban | 1 | 0.7 |
| Apixaban | 1 | 0.7 |
| Unfractionated heparin | 2 | 1.4 |
| Antiplatelet drugs | 2 | 1.4 |
| Clopidogrel | 1 | 0.7 |
| Ticagrelor | 1 | 0.7 |
| Thrombolytic agent (Alteplase) | 1 | 0.7 |
Among SRsAs due to CV drugs lethal outcome was detected in 13 cases (9.1%).
Table 6.
The Structure of CNS-active Drugs involved in Anaphylaxis.
| CNS-active drugs | N (Total - 35) |
% |
|---|---|---|
| Fentanyl | 20 | 57.1 |
| Diazepam | 4 | 11.4 |
| Tramadol | 4 | 11.4 |
| Midazolam | 3 | 8.6 |
| Venlafaxine | 1 | 2.9 |
| Droperidol | 1 | 2.9 |
| Carbamazepine | 1 | 2.9 |
| Levetiracetam | 1 | 2.9 |
Lethal outcome was reported in 5 cases (14.3%).
Table 7.
The Structure of NMBAs involved in Anaphylaxis.
| NMBAs | N (Total - 28) |
% |
|---|---|---|
| Rocuronium | 10 | 35.7 |
| Atracurium | 8 | 28.6 |
| Suxamethonium | 5 | 17.9 |
| Cisatracurium | 5 | 17.9 |
Lethal outcome was detected in 28.6% (n-8) cases.
Table 8.
The Structure of Drugs involved in Fatal SRsAs.
| Drug | N (Total - 218) |
% |
|---|---|---|
| ABs | 109 | 50.00 |
| Ceftriaxone | 68 | 31.2 |
| Cefotaxime | 13 | 6.0 |
| Fosfomycin | 5 | 2.3 |
| Amoxicillin clavulanate | 3 | 1.4 |
| Levofloxacin | 3 | 1.4 |
| Ciprofloxacin | 3 | 1.4 |
| Cefazolin | 3 | 1.4 |
| Ampicillin sulbactam | 2 | 0.9 |
| Ertapenem | 2 | 0.9 |
| Amphotericin B | 1 | 0.5 |
| Meropenem | 1 | 0.5 |
| Tigecycline | 1 | 0.5 |
| Sulfamethoxazole trimethoprim | 1 | 0.5 |
| Vancomycin | 1 | 0.5 |
| Metronidazole | 1 | 0.5 |
| LAs | 29 | 13.3 |
| Lidocaine | 19 | 8.7 |
| Bupivacaine | 7 | 3.2 |
| Articaine | 1 | 0.5 |
| Procaine | 1 | 0.5 |
| Ropivacaine | 1 | 0.5 |
| CV drugs | 13 | 6.0 |
| Beta blockers | 3 | 1.4 |
| Bisoprolol | 2 | 0.9 |
| Metoprolol | 1 | 0.5 |
| ACEi (Enalapril) | 3 | 1.4 |
| Sartans (Losartan) | 1 | 0.5 |
| Calcium Channel Blockers (Amlodipine) | 2 | 0.9 |
| Antiarrhythmics (Amiodorone) | 1 | 0.5 |
| Statins (Rosuvastatin) | 1 | 0.5 |
| Antiplatelet drugs (Ticagrelor) | 1 | 0.5 |
| Alpha-2 adrenergic receptor agonist (Clonidine) | 1 | 0.5 |
| NMBAs | 8 | 3.7 |
| Rocuronium | 4 | 1.8 |
| Suxamethonium | 2 | 0.9 |
| Atracurium | 1 | 0.5 |
| Cisatracurium | 1 | 0.5 |
| ICCM | 8 | 3.7 |
| Iopromide | 4 | 1.8 |
| Iohexol | 3 | 1.4 |
| Iomeprol | 1 | 0.5 |
| CNS-active drugs | 5 | 2.3 |
| Fentanyl | 2 | 0.9 |
| Diazepam | 1 | 0.5 |
| Levetiracetam | 1 | 0.5 |
| Midazolam | 1 | 0.5 |
| COX-inhibitors | 4 | 1.8 |
| Diclofenac | 2 | 0.9 |
| Ibuprofen | 1 | 0.5 |
| Acetylsalicylic acid | 1 | 0.5 |
| Other drugs | 42 | 19.3 |
Table 9.
Data on Age and Sex of Patients in Fatal SRsAs.
| Causative Group of Drugs | Age | Females | |
|---|---|---|---|
| Mean (SD) | Min; Max | % (N) | |
| ABs | 48.2 (16.1) | 15 months; 85 years | 53.8 (50) |
| LAs | 39.4 (14.4) | 5 months; 68 years | 55.1 (16) |
| CV drugs | 62.6 (10.6) | 48 years; 86 years | 30.8 (4) |
| ICCM | 74.0 (8.2) | 65 years; 86 years | 62.5 (5) |
| NMBAs | 37.0 (12.7) | 22 years; 61 years | 75.0 (6) |
| COX-inhibitors | 50.7 (0.4) | 50 years; 51 years | 75.0 (3) |
| CNS-active drugs | 45.6 (7.7) | 32 years; 55 years | 60.0 (3) |
| Other drugs | 51.4 (15.2) | 1 month; 80 years | 57.8 (41) |
SD – standard deviation.
Table 10.
The Structure of ABs involved in Anaphylaxis in Children.
| ABs | N (Total - 57) |
% |
|---|---|---|
| Beta-lactams | 50 | 87.7 |
| Ceftriaxone | 29 | 50.9 |
| Cefotaxime | 7 | 12.3 |
| Cefazolin | 5 | 8.8 |
| Ampicillin sulbactam | 4 | 7.0 |
| Cefepime | 2 | 3.5 |
| Cefoperazone sulbactam | 1 | 1.8 |
| Meropenem | 1 | 1.8 |
| Amoxicillin clavulanate | 1 | 1.8 |
| Other | 7 | 12.3 |
| Vancomycin | 4 | 7.0 |
| Metronidazole | 2 | 3.5 |
| Linezolid | 1 | 1.8 |
Table 11.
The Structure of LAs involved in Anaphylaxis in Children.
| LAs | N (Total - 17) |
% |
|---|---|---|
| Lidocaine | 9 | 52.9 |
| Articaine | 6 | 35.3 |
| Mepivacaine | 2 | 11.8 |
Table 12.
The Structure of Drugs involved in SRsAs in the elderly.
| Drug | N (Total - 65) |
% |
|---|---|---|
| ABs | 26 | 40.0 |
| Ceftriaxone | 23 | 35.4 |
| Amoxicillin clavulanate | 2 | 3.1 |
| Cefixime | 1 | 1.5 |
| CV-drugs | 13 | 20.0 |
| Antiarrhythmic (Amiodarone) | 3 | 4.6 |
| Unfractionated heparin | 2 | 3.1 |
| Beta-blockers (Bisoprolol) | 2 | 3.1 |
| Calcium Channels Blockers | 3 | 4.6 |
| Amlodipine | 2 | 3.1 |
| Nifedipine | 1 | 1.5 |
| Diuretics | 2 | 3.1 |
| Furosemide | 1 | 1.5 |
| Hydrochlorothiazide | 1 | 1.5 |
| Thrombolytic agent (Alteplase) | 1 | 1.5 |
| ICCM | 8 | 12.3 |
| Iopromide | 4 | 6.2 |
| Iohexol | 3 | 4.6 |
| Iomeprol | 1 | 1.5 |
| COX-inhibitors | 5 | 7.7 |
| Diclofenac | 3 | 4.6 |
| Lornoxicam | 1 | 1.5 |
| Metamozole | 1 | 1.5 |
| NMBAs | 4 | 6.2 |
| Rocuronium | 2 | 3.1 |
| Atracurium | 1 | 1.5 |
| Cisatracurium | 1 | 1.5 |
| LAs | 2 | 3.1 |
| Bupivacaine | 1 | 1.5 |
| Procaine | 1 | 1.5 |
| Other drugs | 7 | 10.8 |
| Prednisolone | 1 | 1.5 |
| Iron formulations | 2 | 3.1 |
| Ethyl-methyl-hydroxypyridine succinate | 1 | 1.5 |
| Venlafaxine | 1 | 1.5 |
| Oxaliplatin | 1 | 1.5 |
| Pentoxifylline | 1 | 1.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



