
Submitted:
29 November 2023
Posted:
30 November 2023
You are already at the latest version
Abstract
To evaluate whether the extent of cardiac damage in severe aortic stenosis (AS) might be associated with the occurrence of conduction system disorders after TAVI. A total of 153 symptomatic patients with severe AS who had a TAVI were categorized before the procedure according to the extent of cardiac damage: stage 1 (13.5%): no or LV damage; stage 2 (58.8%): left atrial/mitral valve damage, atrial fibrillation (AF); stage 3 (27.7%): low-flow state, pulmonary vasculature/tricuspid valve/RV damage. After TAVI, 34% of patients exhibited LBBB and 10% high-degree atrioventricular block (HD-AVB). No patient in group 1 developed HD-AVD whereas new LBBB was frequent in groups 2 and 3. Twenty-one patients presented with resolutive paroxysmal AF with a higher rate for each group increment (group 1: n=0, 0%; group 2: n=11,15.7%; group 3: n=10, 30.3%) (p = 0.012). Patients in group 3 had the higher rate of permanent pacemaker implantation (PPMI) (group 1: n=1, 6.3%; group 2: n=7,10%; group 3: n=9, 27.3%) (p=0.012). No patient in group 1 died during the hospital stay. In conclusion, cardiac damage staging of AS might help identify patients at higher risk of conduction disorders and PPMI requirement after TAVI.
Keywords:
TAVI
; Cardiac damage
; conduction disorders
; risk stratification
INTRODUCTION
Transcatheter aortic valve implantation (TAVI) has become the therapeutic standard of care for patients with severe symptomatic aortic stenosis (AS) across all surgical risk categories [1]. In the European guidelines, TAVI should be offered to patients aged ≥75 years with a suitable transfemoral approach or to those at high surgical risk (STS-PROM/EuroSCORE II > 8%) [2]. Nevertheless, although TAVI is less invasive than surgical aortic valve replacement (SAVR), patients require demanding care monitoring. TAVI-related conduction disturbances, mainly new-onset left bundle-branch block (LBBB) and high-degree atrioventricular block (HD-AVB) necessitating permanent pacemaker implantation (PPMI), remain the most common complication of this procedure, which may have a significant detrimental association with patients’ prognosis [3,4,5,6]. The proximity between the aortic valve and the conduction system explains the genesis of periprocedural conduction disturbances during TAVI. Several factors have been associated with an increased risk of conduction disturbances and PPMI, with prior right bundle-branch block (RBBB) and transcatheter valve type and implantation depth being the most frequently reported [7,8,9,10]. However, apart from the mechanical interaction between the transcatheter valve and the conduction system, there is evidence supporting the association between AS and conduction disturbances. Calcium deposition on the conduction system and left ventricular (LV) dysfunction have been both associated with the occurrence of LBBB and HD-AVB in patients with AS [11,12,13]. Delayed intervention in AS may lead to irreversible myocardial damage that may also increase peri-procedural risks and affect long-term clinical outcomes. Recently, a staging system using 4 grades has been proposed to quantify the extent of cardiac damage associated with AS, which is not strictly limited to the aortic valve and the left ventricle (LV), but also extends to the left atrium, pulmonary circulation, and to the right ventricle (RV) and right atrium. Progressive stages of cardiac damage are independently associated with all-cause mortality and important clinical outcomes, such as post-TAVI readmission rates [14,15]. In the present study, we hypothesised that the extent of cardiac damage might be associated with the occurrence of conduction system disorders after TAVI.
METHODS
Study population
The study population consisted of 153 patients with symptomatic severe AS who underwent a TAVI procedure with a self-expandable valve (CoreValve EvolutR®, Medtronic Inc., Minneapolis, Minnesota, USA) between January 2018 and December 2020 at the University of Liège Hospital. Data were collected from the patient hospital records or via the Walloon health network. The decision to perform TAVR was reached by consensus of the institutional heart team. Patients with pre-existing intracardiac devices (PPM) or undergoing a valve in valve procedure were excluded (n=34). A total of 119 patients were finally included. The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Liege University Hospital (protocol code: 2021/306, date of approval: 12 October 2021).
Echocardiography and cardiac staging
A pre-TAVI procedure TTE was performed in all patients. The presence of severe AS, the chambers dimensions, LV and RV function and valvular regurgitation evaluation were defined according to current guidelines. Patients were categorized into five stages according to the extent of extra-aortic valve cardiac damage: stage 0: no cardiac damage; stage 1, LV damage: LV hypertrophy (LV mass index >95 g/m2 for women, >115 g/m2 for men), and/or LV diastolic dysfunction ≥ grade 2 and/or LV systolic dysfunction (LV ejection fraction <60%); stage 2, left atrial and/or mitral valve damage: left atrial enlargement (left atrium volume index >34 mL/m2) and/or ≥ moderate mitral regurgitation, and/or atrial fibrillation; stage 3, pulmonary vasculature or tricuspid valve damage: PH defined as sPAP ≥60 mmHg, and/or ≥ moderate tricuspid regurgitation; stage 4, RV damage and/or subclinical heart failure: RV dysfunction based on a multiparametric evaluation (TAPSE <17 mm and s’ <9.5 cm/s and fractional area change <35%) and/or low-flow state (stroke volume index <30 mL/m2). Patients were hierarchically classified in a given stage (worst stage) if at least one of the proposed criteria was satisfied. Given the small number of patients observed in stages 0-1 and 4, we categorized our population in 3 groups by merging stages 0-1 (group 1), and stages 3-4 (group 3) [14,15,16].
TAVI procedure and ECG assessment
Most TAVI procedures were completed through transfemoral access under locoregional anaesthesia combined with sedation. The selection of valve size (23 to 34 mm) was made by the heart team based on preoperative cardiac computed tomography (CT) analysis. Patients had continuous ECG monitoring in the first 24 hours post-TAVI. This period was extended if significant conduction abnormalities were detected. Thereafter, patients had a daily ECG including on the day of discharge. ECGs were used to determine new conduction abnormalities that persisted until PPMI or discharge. New onset LBBB and RBBB were determined according to standard criteria. HD-AVB included second-degree type 2 (BAV 2 type 2) and third-degree (BAV 3) atrioventricular blocks. Those that developed indications for PPMI had the device implanted during the same admission. The decision to do so was made by the structural intervention and electrophysiology teams, in conjunction with the patient.
Statistical analysis
Variables are presented as the number with the percentage or as the median with the interquartile range. The comparison of clinical data between groups was performed by the Kruskal-Wallis test for continuous variables, with the DSCF test for post-hoc comparison. The evolution of electrocardiographic parameters was analysed by the paired Wilcoxon test. The association between periprocedural death and other variables was analysed by univariate logistic regression. Odds ratios (OR) are calculated with their 95% confidence intervals. The association between PPM implantation during follow-up, mortality and cardiovascular mortality and other variables was performed by univariate Cox regression. Hazard ratios (HR) are calculated with their 95% confidence intervals. All tests are two-tailed and a p-value < 0.05 is considered significant. All statistical analyses were performed in SAS 9.4 (SAS Institute, Cary NC).
RESULTS
Baseline characteristics of the study population
Baseline pre-TAVI data according to the stage of cardiac involvement (group 1: 13.5%; group 2: 58.8%; group 3:27.7%) are summarized in Table 1. Overall, the general characteristics, except for age (p = 0.017) and the presence of atrial fibrillation (AF) (p = 0.003), were similar between the groups. Patients in group 1 were younger (78 years median age) compared to those in groups 2 and 3 (median age: 78 vs. 83.5 vs. 85 years; p = 0.046, p=0.009, respectively). The rate of AF (group 1: 18.8%, group 2: 35.7%, group 3: 60.6%) as the PR interval increased with each stage increment. At pre-TAVI ECG, the duration of the PR interval increased with the staging severity (p=0.02). A PR interval ≥ 240 ms was only seen in groups 2 and 3.
Staging and ECG outcomes after TAVI
The median duration of hospitalization was 8 days (range 6-13 days). Mean duration of the procedure was 122 minutes (range 101-140 minutes). After TAVI, 47% of patients exhibited new conduction disturbances with new LBBB (n=41, 34%) being the most frequent, new RBB in 2.5% (n=3) and HD-AVB in 10% (n=12) (Table 2). Overall, 17 patients (14.7%) required PPMI and 6 patients (5%) died of cardiovascular cause. No patient in group 1 developed HD-AVD whereas new LBBB was frequent in groups 2 and 3. PR interval increased in group 2 (p=0.006) whereas QRS duration increased after TAVI in each group (p<0.0001). Only 1 patient in group 1 had a PR interval ≥ 240 ms and none of them had a QRS ≥ 150 ms. The rate of permanent AF remained similar after TAVI and did not change between groups. However, 21 patients (17.65%) presented with resolutive paroxysmal AF with a higher rate for each group increment (group 1: n=0, 0%; group 2: n=11,15.7%; group 3: n=10, 30.3%) (p = 0.012). Patients in group 3 had the higher rate of PPMI (group 1: n=1, 6.3%; group 2: n=7,10%; group 3: n=9, 27.3%) (p = 0.012). No patient in group 1 died during the hospital stay (Figure 1).
Predictors of PPMI and in-hospital mortality
Several factors were associated with an increased risk of PPMI (Table 3): a) before TAVI: AF as a comorbidity (p=0.023), low pre-TAVI heart rate (p=0.047); b) during TAVI: sedation with local anesthesia (p=0.028), development of HD-AVB (p=0.0005), use of a size 34 mm prosthesis (p=0.012); c) after TAVI: a PR interval > 200 ms (p=0.027), a QRS ≥ 150 ms (p<0.0001), a higher QRS delta from baseline ECG (p=0.001), and a new BBB (p<0.01). Factors associated with in-hospital mortality were: a large QRS (p=0.022), a pre-TAVI QRS ≥ 150 ms (p=0.009), a HD-AVB immediately after implantation (p=0.002), and the duration of the procedure (p=0.003).
DISCUSSION
To the best of our knowledge, this is the first study to specifically evaluate the relationship between AS staging and ECG changes after TAVI. The main findings are as follows: a) conduction disorders are frequent after TAVI with new LBBB being the most common, especially in advanced AS stages; b) patients with AS stage 1 are relatively free of HD-AVD, PPMI and peri-procedural paroxysmal AF, the latter occurring in one-third of patients in group 3; c) unlike HD-AVB immediately after implantation, the occurrence of new LBBB had no impact on hospital outcomes.
Cardiac damage and post-TAVI conduction disorders
In AS, not only the severity of the stenosis but also the extent of cardiac damage has a significant impact on the patient’s prognosis. The more severe the extra-valvular lesions, the more the outcome is compromised with a progressive increase in mortality for each stage increment [14,15,27]. It is known that cardiac electrophysiology can be altered by chronic changes in loading conditions, as in AS [28]. Therefore, with disease progression, the vulnerability of conductive tissues to any mechanical stress, as in the case of TAVI, may increase as extravalvular damage increases. In our study, we reported that the likelihood of conduction disturbances differed depending on the extent of AS-related cardiac damage prior to TAVI. After TAVI, the increase in PR interval and in QRS duration was more pronounced in advanced AS stages. Only 1 patient in group 1 had a PR interval ≥ 240 ms and none of them had a QRS ≥ 150 ms. The incidence of new LBBB and HD-AVB increased progressively for each stage increment. As a result, the rate of PPMI was the highest in advanced stages with 27.3% in group 3, 10% in group 2 compared to only 6% in group 1. Although rhythm type did not change significantly after TAVI, the rate of paroxysmal AF increased with higher stage. No patient in group 1 developed paroxysmal AF. Overall, these results indicate that the greater the extent of cardiac damage before TAVI, the higher the likelihood of tissue conduction disturbances after the procedure. Thus, staging of cardiac lesions appears to be effective in identifying a population at low risk for arrhythmias or PPMI after TAVI. These results could help 1) identify patients who could benefit from the use of the pacing over the wire technique or in whom rapid removal of the right ventricular pacing lead after the procedure could be performed, 2) monitor preferentially stage 1 patients in a cardiology room rather than in an intensive care unit.
Limitations
Our study contains some limitations. The number of patients examined was relatively low, especially with initial stages 0-1 or 3-4, which is why they were logically grouped in stage 1 or 3, corresponding to left chamber cardiac involvement or upstream repercussions of AS on the pulmonary circulation and the right ventricle. Even if this study only concerned self-expandable prostheses, it is likely that our results could also be transposed to balloon expandable prostheses.
Conclusion
Despite technological advancements, increased operator experience and improvements in terms of efficiency and safety of the TAVI procedure, the incidence of peri- and post-procedure conduction abnormalities remain high. Cardiac damage staging of AS seems to be a way to detect patients at low risk of conduction disorders and PPMI requirement and could also provide valuable assistance in the patient monitoring strategy. Future prospective studies in larger cohort of patients are needed to confirm these results.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Rosseel, L.; Mylotte, D.; Cosyns, B.; Vanhaverbeke, M.; Zweiker, D.; Teles, R.C.; Angerås, O.; Neylon, A.; Rudolph, T.K.; Wykrzykowska, J.J.; et al. Contemporary European practice in transcatheter aortic valve implantation: results from the 2022 European TAVI Pathway Registry. Front. Cardiovasc. Med. 2023, 10, 1227217. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Karyofillis, P.; Kostopoulou, A.; Thomopoulou, S.; Habibi, M.; Livanis, E.; Karavolias, G.; Voudris, V. Conduction abnormalities after transcatheter aortic valve implantation. J. Geriatr. Cardiol. 2018, 15, 105–112. [Google Scholar] [CrossRef]
- Auffret, V.; Puri, R.; Urena, M.; Chamandi, C.; Rodriguez-Gabella, T.; Philippon, F.; Rodés-Cabau, J. Conduction Disturbances After Transcatheter Aortic Valve Replacement. Circ. 2017, 136, 1049–1069. [Google Scholar] [CrossRef]
- Mangieri, A.; Montalto, C.; Pagnesi, M.; Lanzillo, G.; Demir, O.; Testa, L.; Colombo, A.; Latib, A. TAVI and Post Procedural Cardiac Conduction Abnormalities. Front. Cardiovasc. Med. 2018, 5, 85. [Google Scholar] [CrossRef] [PubMed]
- Scarsini, R.; De Maria, G.L.; Joseph, J.; Fan, L.; Cahill, T.J.; Kotronias, R.A.; Burzotta, F.; Newton, J.D.; Kharbanda, R.; Prendergast, B.; et al. Impact of Complications During Transfemoral Transcatheter Aortic Valve Replacement: How Can They Be Avoided and Managed? J. Am. Hear. Assoc. 2019, 8, e013801. [Google Scholar] [CrossRef] [PubMed]
- Sammour, Y.; Krishnaswamy, A.; Kumar, A.; Puri, R.; Tarakji, K.G.; Bazarbashi, N.; Harb, S.; Griffin, B.; Svensson, L.; Wazni, O.; et al. Incidence, Predictors, and Implications of Permanent Pacemaker Requirement After Transcatheter Aortic Valve Replacement. JACC: Cardiovasc. Interv. 2021, 14, 115–134. [Google Scholar] [CrossRef]
- Auffret, V.; Webb, J.G.; Eltchaninoff, H.; Muñoz-García, A.J.; Himbert, D.; Tamburino, C.; Nombela-Franco, L.; Nietlispach, F.; Morís, C.; Ruel, M.; et al. Clinical Impact of Baseline Right Bundle Branch Block in Patients Undergoing Transcatheter Aortic Valve Replacement. JACC: Cardiovasc. Interv. 2017, 10, 1564–1574. [Google Scholar] [CrossRef] [PubMed]
- van Rosendael, P.J.; Delgado, V.; Bax, J.J. Pacemaker implantation rate after transcatheter aortic valve implantation with early and new-generation devices: a systematic review. Eur. Hear. J. 2018, 39, 2003–2013. [Google Scholar] [CrossRef]
- Lenders, G.D.; Collas, V.; Hernandez, J.M.; Legrand, V.; Danenberg, H.D.; Heijer, P.D.; Rodrigus, I.E.; Paelinck, B.P.; Vrints, C.J.; Bosmans, J.M. Depth of valve implantation, conduction disturbances and pacemaker implantation with CoreValve and CoreValve Accutrak system for Transcatheter Aortic Valve Implantation, a multi-center study. Int. J. Cardiol. 2014, 176, 771–775. [Google Scholar] [CrossRef]
- Prihadi, E.A.; Leung, M.; Vollema, E.M.; Ng, A.C.; Marsan, N.A.; Bax, J.J.; Delgado, V. Prevalence and Prognostic Relevance of Ventricular Conduction Disturbances in Patients With Aortic Stenosis. Am. J. Cardiol. 2017, 120, 2226–2232. [Google Scholar] [CrossRef] [PubMed]
- Sebag, F.A.; Lellouche, N.; Chaachoui, N.; Dubois-Rande, J.; Gueret, P.; Monin, J. Prevalence and clinical impact of QRS duration in patients with low-flow/low-gradient aortic stenosis due to left ventricular systolic dysfunction. Eur. J. Hear. Fail. 2014, 16, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Dhingra, R.C.; Amat-Y-Leon, F.; Pietras, R.J.; Wyndham, C.; Deedwania, P.C.; Wu, D.; Denes, P.; Rosen, K.M. Sites of Conduction Disease in Aortic Stenosis. Ann. Intern. Med. 1977, 87, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Généreux, P.; Pibarot, P.; Redfors, B.; Mack, M.J.; Makkar, R.R.; A Jaber, W.; Svensson, L.G.; Kapadia, S.; Tuzcu, E.M.; Thourani, V.H.; et al. Staging classification of aortic stenosis based on the extent of cardiac damage. Eur. Hear. J. 2017, 38, 3351–3358. [Google Scholar] [CrossRef] [PubMed]
- Tastet, L.; Tribouilloy, C.; Maréchaux, S.; Vollema, E.M.; Delgado, V.; Salaun, E.; Shen, M.; Capoulade, R.; Clavel, M.-A.; Arsenault, M.; et al. Staging Cardiac Damage in Patients With Asymptomatic Aortic Valve Stenosis. J. Am. Coll. Cardiol. 2019, 74, 550–563. [Google Scholar] [CrossRef]
- Viva, T.; Postolache, A.; Trung, M.-L.N.; Danthine, P.; Petitjean, H.; Bruno, V.D.; Martinez, C.; Lempereur, M.; Guazzi, M.; Aghezzaf, S.; et al. A new integrative approach combining right heart catheterization and echocardiography to stage aortic stenosis-related cardiac damage. Front. Cardiovasc. Med. 2023, 10, 1184308. [Google Scholar] [CrossRef] [PubMed]
- Faroux, L.; Chen, S.; Muntané-Carol, G.; Regueiro, A.; Philippon, F.; Sondergaard, L.; Jørgensen, T.H.; Lopez-Aguilera, J.; Kodali, S.; Leon, M.; et al. Clinical impact of conduction disturbances in transcatheter aortic valve replacement recipients: a systematic review and meta-analysis. Eur. Hear. J. 2020, 41, 2771–2781. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Ko, Y.-G.; Shim, C.Y.; Ryu, J.; Lee, Y.-J.; Seo, J.; Lee, S.-J.; Cho, I.; Hong, S.-J.; Ahn, C.-M.; et al. Impact of New-Onset Persistent Left Bundle Branch Block on Reverse Cardiac Remodeling and Clinical Outcomes After Transcatheter Aortic Valve Replacement. Front. Cardiovasc. Med. 2022, 9, 893878. [Google Scholar] [CrossRef]
- Jørgensen, T.H.; De Backer, O.; Gerds, T.A.; Bieliauskas, G.; Svendsen, J.H.; Søndergaard, L. Mortality and Heart Failure Hospitalization in Patients With Conduction Abnormalities After Transcatheter Aortic Valve Replacement. JACC: Cardiovasc. Interv. 2019, 12, 52–61. [Google Scholar] [CrossRef]
- Wang, B.; Mei, Z.; Ge, X.; Li, Y.; Zhou, Q.; Meng, X.; An, G. Comparison of outcomes of self-expanding versus balloon-expandable valves for transcatheter aortic valve replacement: a meta-analysis of randomized and propensity-matched studies. BMC Cardiovasc. Disord. 2023, 23, 1–18. [Google Scholar] [CrossRef]
- Smith, C.R.; Leon, M.B.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter versus Surgical Aortic-Valve Replacement in High-Risk Patients. N. Engl. J. Med. 2011, 364, 2187–2198. [Google Scholar] [CrossRef] [PubMed]
- Aladham, A.; Gada, H.; Wang, Y.; Mumtaz, M.; Sultan, I.; Mulukutla, S.; Vora, A.N. Incidence of Permanent Pacemaker Implantation Using the Cusp Overlap Technique. JACC: Cardiovasc. Interv. 2022, 15, 1006–1008. [Google Scholar] [CrossRef] [PubMed]
- Szotek, M.; Drużbicki; Sabatowski, K.; Amoroso, G.R.; De Schouwer, K.; Matusik, P.T. Transcatheter Aortic Valve Implantation and Cardiac Conduction Abnormalities: Prevalence, Risk Factors and Management. J. Clin. Med. 2023, 12, 6056. [Google Scholar] [CrossRef] [PubMed]
- Regueiro, A.; Altisent, O.A.-J.; Del Trigo, M.; Campelo-Parada, F.; Puri, R.; Urena, M.; Philippon, F.; Rodés-Cabau, J. Impact of New-Onset Left Bundle Branch Block and Periprocedural Permanent Pacemaker Implantation on Clinical Outcomes in Patients Undergoing Transcatheter Aortic Valve Replacement. Circ. Cardiovasc. Interv. 2016, 9, e003635. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Liu, S.; Han, X.; Chen, Y.; Chen, H.; Wan, Z.; Song, B. Prognostic Outcome of New-Onset Left Bundle Branch Block After Transcatheter Aortic Valve Replacement in Patients With Aortic Stenosis: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2022, 9, 842929. [Google Scholar] [CrossRef] [PubMed]
- Chamandi, C.; Barbanti, M.; Munoz-Garcia, A.; Latib, A.; Nombela-Franco, L.; Gutiérrez-Ibanez, E.; Veiga-Fernandez, G.; Cheema, A.N.; Cruz-Gonzalez, I.; Serra, V.; et al. Long-Term Outcomes in Patients With New-Onset Persistent Left Bundle Branch Block Following TAVR. JACC: Cardiovasc. Interv. 2019, 12, 1175–1184. [Google Scholar] [CrossRef] [PubMed]
- Avvedimento, M.; Franzone, A.; Leone, A.; Piccolo, R.; Castiello, D.S.; Ilardi, F.; Mariani, A.; Esposito, R.; Iapicca, C.; Angellotti, D.; et al. Extent of Cardiac Damage and Mortality in Patients Undergoing Transcatheter Aortic Valve Implantation. J. Clin. Med. 2021, 10, 4563. [Google Scholar] [CrossRef]
- Mills, R.W.; Wright, A.T.; Narayan, S.M.; McCulloch, A.D. The effects of wall stretch on ventricular conduction and refractoriness in the whole heart. In Cardiac Mechano-Electric Coupling and Arrhythmias; Kohl, P., Sachs, F., Franz, M.R., Eds.; Oxford University Press: Oxford, UK, 2011; p. 0. [Google Scholar] [CrossRef]
Figure 1.
Outcomes after TAVI between the different groups. AF: atrial fibrillation, AVB: atrioventricular block, PPMI: permanent pacemaker implantation.
Figure 1.
Outcomes after TAVI between the different groups. AF: atrial fibrillation, AVB: atrioventricular block, PPMI: permanent pacemaker implantation.
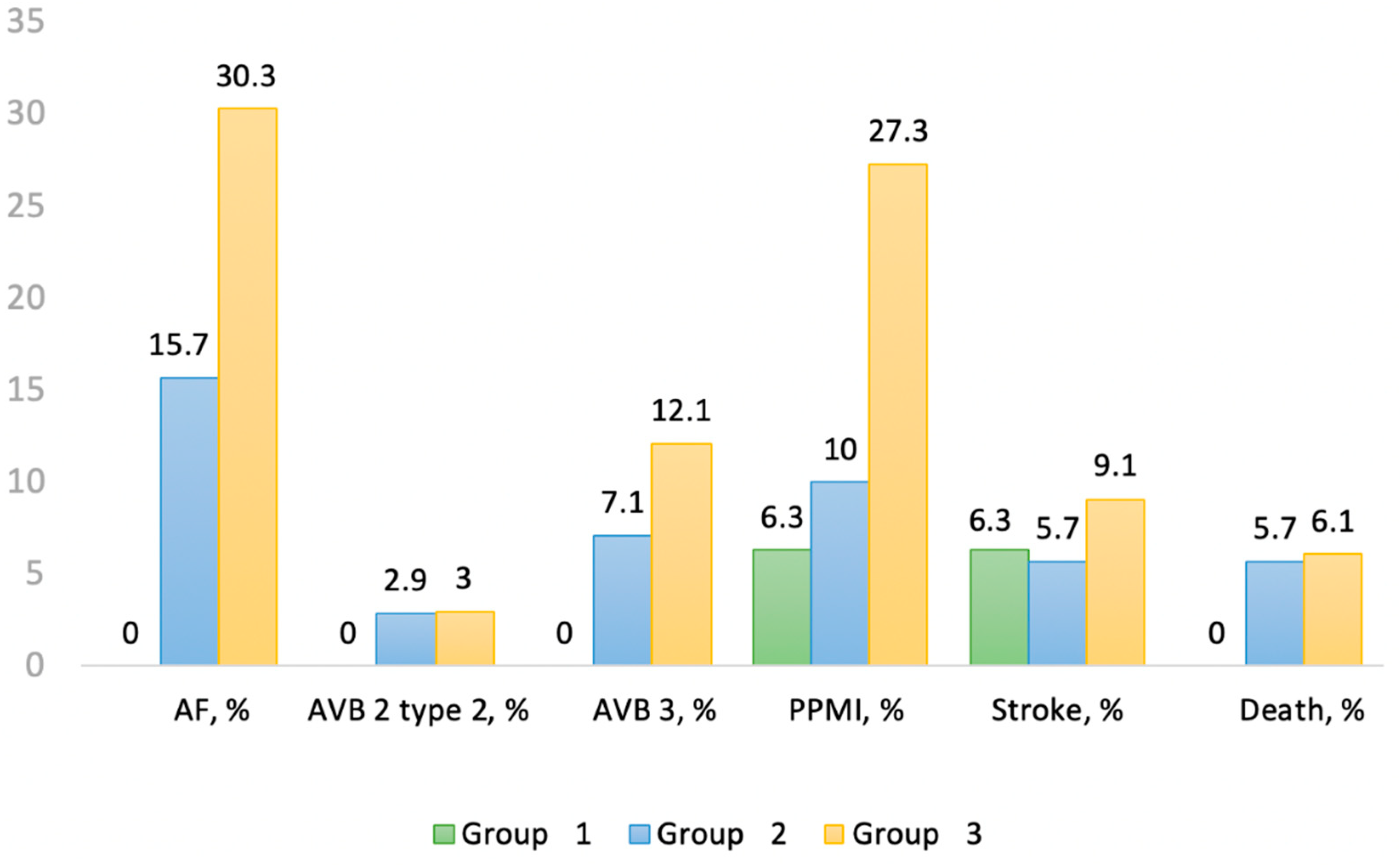

Table 1.
Baseline characteristics of the study population before TAVI.
| Total | Group 1 | Group 2 | Group 3 | p-value | |
|---|---|---|---|---|---|
| Clinical characteristics | |||||
| Number of patients (%) | 119 (100%) | 16 (13.5%) | 70 (58.8%) | 33 (27.7%) | |
| Age (years) | 84 (79 - 86) | 78 (73,5 – 84,5) | 83,5 (79 – 87) | 85 (81 – 87) | 0.017 |
| Male, (%) | 64 (53.78) | 9 (56.3) | 37 (52.9) | 18 (54.6) | 0.97 |
| Body mass index, Kg/m2 | 25.51 (23.2 – 29.6) | 27.1 (23.3-29.5) | 26.4 (23.1-30.1) | 24.9 (23.5-26.9) | 0.58 |
| Current smoker (%) | 45 (37.8) | 8 (50) | 26 (37.1) | 11 (33.3) | 0.30 |
| Hypertension n (%) | 106 (89.1) | 14 (87.5) | 62 (88.6) | 30 (90.9) | 0.82 |
| Diabetes (%) | 35 (29.4) | 6 (37.5) | 20 (28.6) | 9 (27.3) | 0.52 |
| Dyslipidemia (%) | 96 (80.7) | 14 (87.5) | 55 (78.6) | 27 (81.8) | 0.86 |
| Atrial fibrillation (%) | 48 (40.3) | 3 (18.8) | 25 (35.7) | 20 (60.6) | 0.003 |
| Stroke (%) | 22 (18.5) | 0 (0) | 15 (21.4) | 7 (21.2) | 0.19 |
| Prior peripheral vascular disease (%) | 59 (49.6) | 7 (43.8) | 37 (52.9) | 15 (45.5) | 0.90 |
| Coronary artery disease (%) | 53 (44.5) | 8 (50) | 29 (41.4) | 16 (48.5) | 0.89 |
| Chronic kidney diseases (eGFR <45 mL/min) | 50 (42.0) | 5 (31.3) | 29 (41.4) | 16 (48.5) | 0.25 |
| Medical therapy | |||||
| Beta-blockers (%) | 84 (70.6) | 9 (56.3) | 49 (70) | 26 (78.8) | 0.11 |
| Calcium antagonists (%) | 28 (23.5) | 4 (25) | 16 (22.9) | 8 (24.2) | 1.00 |
| Amiodarone (%) | 21 (17.7) | 2 (12.5) | 12 (17.1) | 7 (21.2) | 0.57 |
| Procedure | |||||
| Euroscore II (%) | 3.98 (2.51 – 6.02) | 3.92 (2.8-4.9) | 3.64 (2.35-6.06) | 4.8 (2.8-11.27) | 0.24 |
| Calcium score | 2471.45 (1652 - 3768) | 1582 (869-3197) | 2990 (1853-4111) | 2211 (1855-3117) | 0.10 |
| Pre-dilatation (%) | 38 (31.9) | 3 (18.8) | 23 (32.9) | 12 (36.4) | 0.28 |
| Post-dilatation (%) | 15 (12.6) | 1 (6.3) | 12 (17.1) | 2 (6.1) | 0.66 |
| Prosthesis size | 0.55 | ||||
| 23 mm (%) | 8 (6.72) | 0 (0) | 4 (5.7) | 4 (12.1) | |
| 26 mm (%) | 33 (27.7) | 5 (31.3) | 19 (27.1) | 9 (27.3) | |
| 29 mm (%) | 45 (37.8) | 7 (43.8) | 27 (38.6) | 11 (33.3) | |
| 34 mm (%) | 33 (27.7) | 4 (25) | 20 (28.6) | 9 (27.3) | |
| Approach (%) | 0.32 | ||||
| Femoral | 103 (86.6) | 14 (87.5) | 60 (85.7) | (87.9) | |
| Trans-Axillary | 15 (12.6) | 2 (12.5) | 10 (14.3) | (9.1) | |
| Carotid | 1 (0.84) | 0 (0) | 0 (0) | 1 (3) | |
| General anesthesia (%) | 0.42 | ||||
| General | 80 (67.2) | 7 (43.8) | 52 (74.3) | 21 (63.6) | |
| Local anesthesia + sedation | 39 (32.8) | 9 (56.3) | 18 (25.7) | 12 (36.4) | |
| Procedure time(min) | 122 (101 - 140) | 123.5 (102.5-132.5) | 123 (102-140) | 115 (99-147) | 0.84 |
| Electrocardiogram | |||||
| Heart rate (bpm) | 71 (62 – 81) | 73.5 (65-85) | 69 (60-80) | 72 (62-81) | 0.59 |
| Rhythm | < 0.0001 | ||||
| Sinus (%) | 94 (78.99) | 16 (100) | 61 (87.1) | 17 (51.5) | |
| Atrial fibrillation (%) | 25 (21.01) | 0 (0) | 9 (12.9) | 16 (48.5) | |
| PR interval (ms) | 180 (164 – 204) | 165 (161-177) | 180 (164-204) | 202 (180-214) | 0.020 |
| < 200 ms (%) | 63 (67.0) | 15 (93.8) | 40 (57.1) | 8 (24.2) | |
| 200-239 ms (%) | 20 (21.3) | 1 (6.3) | 13 (18.6) | (18.2) | |
| ≥ 240 ms (%) | 11 (11.70) | 0 (0) | 8 (11.4) | 3 (9.1) | |
| QRS (ms) | 96 (84 – 112) | 89 (78-98) | 96 (86-119) | 94 (84-110) | 0.13 |
| < 120 ms (%) | 96 (80.7) | 14 (87.5) | 54 (77.1) | 28 (84.9) | |
| 120-149 ms (%) | 17 (14.3) | 2 (12.5) | 10 (14.3) | (15.1) | |
| ≥ 150 ms (%) | 6 (5.04) | 0 (0) | 6 (8.6) | 0 (0) | |
| Prior bundle branch block | 0.47 | ||||
| Left (%) | 10 (8.4) | 1 (6.3) | 7 (10) | 2 (6.1) | |
| Right (%) | 6 (5.04) | 1 (6.3) | 5 (7.1) | 0 (0) |
Table 2.
ECG outcomes after TAVI.
| Total | Group 1 N=16 (13.5%) |
Group 2 N=70 (58.8%) |
Group 3 N=33 (27.7%) |
p value | |
|---|---|---|---|---|---|
| Electrocardiogram | |||||
| Heart rate (bpm) | 73 (65 – 86) | 72 (61-95) | 72 (65-81) | 79 (67.5-88.5) | 0.41 |
| Rhythm | |||||
| Atrial fibrillation (%) | 25 (21.7) | 0 (0) | 9 (12.9) | 16 (48.5) | < 0.0001 |
| PR interval (ms) | 190 (166 – 214) | 170 (162-194) | 192 (172-215) | 214 (168-226) | 0.052 |
| < 200 ms (%) | 55 (63.2) | 13 (81.3) | 36 (51.4) | (18.2) | |
| 200-239 ms (%) | 19 (21.8) | 2 (12.5) | 11 (15.7) | (18.2) | |
| ≥ 240 ms (%) | 13 (14.9) | 1 (6.3) | 9 (12.9) | 3 (9.1) | |
| Delta PR | 8 (-6 - 20) | 4 (-3 – 23)* | 8 (-6 – 18)* | 2 (-22 – 26) | 0.71 |
| QRS (ms) | 122 (96 – 140) | 101 (88-129) | 122 (94- 140) | 124.5 (103-142) | 0.13 |
| < 120 ms (%) | 54 (47.4) | 10 (62.5) | 30 (42.9) | 14 (42.4) | |
| 120-149 ms (%) | 42 (36.8) | 6 (37.5) | 23 (32.9) | 13 (39.4) | |
| ≥ 150 ms (%) | 18 (15.8) | 0 (0) | 13 (18.6) | 5 (15.2) | |
| Delta QRS | 8 (2-36) | 11 (6 – 24)* | 5 (0 – 33)* | 19 (4 – 54)* | 0.082 |
| New bundle branch block | 0.17 | ||||
| Left (%) | 41 (34.5) | 4 (25) | 24 (34.3) | (39.4) | |
| Right (%) | 3 (2.52) | 0 (0) | 1 (1.4) | 2 (6.1) | |
| Complications | |||||
| Paroxysmal atrial fibrillation (%) | 21 (17.7) | 0 (0) | 11 (15.7) | 10 (30.3) | 0.012 |
| High degree AV block (%) | 12 (10) | 0 (0) | 7 (10) | 5 (15) | 0.38 |
| Permanent pacemaker implantation (%) | 17 (14.3) | 1 (6.3) | 7 (10) | 9 (27.3) | 0.022 |
| Stroke (%) | 8 (6.7) | 1 (6.3) | 4 (5.7) | 3 (9.1) | 0.32 |
| Death (%) | 6 (5) | 0 (0) | 4 (5.7) | 2 (6.1) | 0.52 |
*P<0.05, difference between post and pre-TAVI.
Table 3.
Variables associated with PPMI.
| Variables | HR (LCL – UCL) | p-value | Units |
|---|---|---|---|
| Local vs general anesthesia | 2.77 (1.11 – 6.89) | 0.028 | |
| Heart rate ECG pre-TAVI | 0.96 (0.93 – 1) | 0.047 | 1 beat |
| Duration QRS ECG pre-TAVI | 1.16 (1 – 1.34) | 0.051 | 10 ms |
| PR pre-TAVI 200-239 ms vs < 200 ms | 3.35 (0.97 – 11.59) | 0.056 | |
| Per-procedure: AV block 2 type 2 vs No AV block | 142.6 (8.71 – 2333.5) | 0.0005 | |
| Per-procedure: AV block 3 vs No AV block | 6.2 (2.19 – 17.54) | 0.0006 | |
| Prosthesis size 34 vs 29 | 5.27 (1.45 – 19.17) | 0.012 | |
| Atrial fibrillation | 2.95 (1.16 – 7.51) | 0.023 | |
| Heart rate ECG post-TAVI | 0.97 (0.94 – 1) | 0.082 | 1 beat |
| Interval PR ECG post-TAVI | 1.20 (1.06 – 1.36) | 0.004 | 10 ms |
| Delta PR | 1.02 (1 – 1.04) | 0.11 | 1 ms |
| Duration QRS ECG post-TAVI | 1.55 (1.26 – 1.91) | <0.0001 | 10 ms |
| Delta QRS | 1.03 (1.01 – 1.05) | 0.001 | 1 ms |
| ECG post-TAVI: left bundle-branch block vs No bundle-branch block | 5.76 (1.62 – 20.44) | 0.007 | |
| ECG post-TAVI: right bundle-branch block vs No bundle-branch block | 7.15 (1.44 – 35.49) | 0.016 | |
| PR post-TAVI < 200 ms vs ≥ 240 ms | 0.13 (0.02 – 0.79) | 0.027 | |
| PR post-TAVI 200-239 ms vs < 200 ms | 6.59 (1.2 – 35.99) | 0.030 | |
| QRS post-TAVI ≥ 150 ms vs < 120 ms | 16.97 (4.55 – 63.29) | <0.0001 | |
| QRS post-TAVI 120-149 ms vs ≥ 150 ms | 0.17 (0.06 – 0.48) | 0.0009 | |
| Post-TAVI: AV block 3 vs No AV block | 9.95 (3.67 – 26.92) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



