Submitted:
29 November 2023
Posted:
30 November 2023
You are already at the latest version
Abstract
(1) Background: It is crucial to provide safe and knowledgeable healthcare practices because no research has been done on the knowledge and usage patterns of NSAIDs among the Hail population. (2) Method: Structured questionnaires were utilized to gather data from 399 individuals in Hail, Saudi Arabia for the cross-sectional analysis. The study assessed participants' knowledge regarding NSAIDs, patterns of use, reasons for use, and awareness of potential side effects. (3) Results: In the study, the gender distribution indicated that 170 participants (42.61%) were male, while 229 (57.39%) were female. Gender, occupation, and marital status showed non-significant associations (p>0.01), except for menstrual cycle and joint pain, where marital status displayed significant associations. Age had significant associations with muscle pain, menstrual cycle, and joint pain (p<0.01). Education and monthly income exhibited non-significant associations for all the reasons. The regression analysis demonstrated that gender played a significant role, with females having higher odds of knowledge (AOR = 1.75, 95% CI 1.10-2.88) than males. Age also had a notable impact, with individuals aged 50-59 (AOR = 0.21, 95% CI 0.07-0.66) exhibiting lower odds of knowledge. Education holding a Ph.D (AOR = 3.50, 95% CI 0.54-22.51) and business as an occupation (AOR = 6.12, 95% CI 1.10-35.10) had significantly higher odds of knowledge while housewives (AOR = 0.76, 95% CI 0.25-2.27) had lower odds. Meanwhile, >50% of the participants had knowledge of adverse events related to the use of NSAIDs while 25% had no knowledge. Moreover, 59 (25.766%) participants reported discomfort with the use of NSAIDs. In addition, 50% and >75% of participants’ considered NSAIDs can cause peptic ulcers and damage kidneys, respectively (4) Conclusions: This study shed light on the knowledge and patterns of NSAIDs use in the population of Hail, Saudi Arabia. While NSAIDs are commonly utilized for pain management, there exists a need for improved public awareness regarding potential risks and safe usage practices. Healthcare providers and policymakers should consider these insights to develop targeted educational initiatives and healthcare interventions to promote safe and informed NSAID utilization in the region.
Keywords:
KAP
; NSAIDS
; pain treatment
; muskosceletonal pain
; complications
1. Introduction
Nonsteroidal anti-inflammatory drugs (NSAIDs) are a widely recognized group of medicines that possess fever-reducing, pain-relieving, and anti-inflammatory properties [1]. From the ancient utilization of willow leaves containing salicylates to the more recent fluctuations in the popularity of highly selective cyclooxygenase-2 (COX-2) inhibitors and the emergence of the latest dual-acting anti-inflammatory compounds, there has been a continuous and dynamic evolution in this field [2]. Approximately 30 million individuals worldwide are believed to use NSAIDs daily [3] and ranked among the most frequently utilized pharmaceuticals worldwide, encompassing about 5% of all prescribed and over-the-counter (OTC) medications [4,5]. A significant number of individuals with chronic kidney disease (CKD) in the United States are using NSAIDs, with an observed prevalence of 8% for stages 1 and 2 and 9% for stages 3 and 4, in contrast to patients without CKD, where the prevalence was 5% [6]. In Saudi Arabia, diclofenac, an NSAID, is the most frequently utilized medication, accounting for 67% of all medicines used in the country from 2010 to 2015 [7].
NSAIDs effectively treat a range of conditions, such as osteoarthritis, rheumatoid arthritis, ankylosing spondylitis, menstrual pain, and postoperative discomfort [8]. Furthermore, they are under scrutiny for their potential protective role in combating significant diseases like cancer and cardiovascular disorders [9]. Moreover, earlier studies demonstrated the potential advantages of NSAIDs in reducing the likelihood of delirium and mortality [10]. Despite the significant progress made over the past two decades, researchers continue to seek ways to design and develop more effective and safer therapies for treating inflammatory conditions [2]. This quest has become particularly compelling due to recognizing inflammation as a shared underlying factor and a unifying mechanism in most chronic diseases [2]. However, the ubiquitous nature of NSAIDs and their availability OTC has led to their frequent use without strict medical supervision. This widespread accessibility and usage have raised concerns regarding the knowledge and awareness of the general population regarding the safe and appropriate utilization of NSAIDs. Nevertheless, NSAIDs come with potential negative impacts on the gastrointestinal (GI) [11], cardiovascular (CV) [12], and renal systems [13]. Additionally, the likelihood of GI bleeding rises with advancing age and in individuals with a history of stomach ulcers and bleeding disorders [14]. For instance, in USA, NSAID usage among CKD patients raises concerns about the potential for nephrotoxicity and the progression of CKD due to insufficient knowledge regarding the safe use of NSAIDs [15]. Similarly, in Saudi Arabia, the population that used NSAIDs encountered adverse effects associated with these medications. Among these complications, peptic ulcer disease and heartburn emerged as the most prevalent issues [16]. Therefore, it is crucial to explore the level of awareness and understanding the general population possesses about these medications and their associated risks. This multifaceted exploration encompasses a comprehensive assessment of the general public's knowledge, attitudes, and behaviors concerning NSAID use, focusing on the potential gaps in awareness that could ultimately impact their health and well-being [17].
The knowledge and awareness of the general population regarding NSAID use are critical factors in ensuring safe and responsible medication practices [18]. Understanding the appropriate dosages, potential side effects, and interactions with other medications or medical conditions is vital for informed decision-making [19]. Moreover, being aware of alternative pain management strategies and when to seek medical advice can contribute to better health outcomes and reduce the risk of adverse effects associated with NSAIDs. Various factors, including the accessibility of information, cultural norms, and individual beliefs, influence the general population's awareness of NSAIDs [20]. In an era of readily available information through the internet and media, many individuals rely on online sources and self-diagnosis for their healthcare decisions. This can be both advantageous and risky, as misinformation or misinterpretation of medical information can lead to inappropriate NSAID use or avoidance of necessary treatments [21]. Thus, promoting accurate, evidence-based information on NSAID use and its potential risks is essential in today's information age.
The utilization of NSAIDs and the awareness of the general population about their use represent a critically important area of study, particularly within the context of Ha'il Province. NSAIDs are a class of medications widely employed for their pain-relieving and anti-inflammatory properties, making them some of the most commonly used pharmaceuticals worldwide. They are easily accessible over-the-counter in many regions, making them a go-to choice for managing various types of pain and inflammation, from mild headaches to chronic arthritic conditions. However, the benefits of NSAIDs often come with a trade-off, as their use is associated with a range of potential side effects and risks, particularly when taken inappropriately or for extended periods. Understanding the patterns of NSAID utilization within the specific regional context of Ha'il Province is essential to comprehending the broader implications for public health, as usage trends and associated risks can vary significantly from one area to another due to cultural, social, and economic factors. Thus, the present study was designed to investigate the use and knowledge regarding NSAIDs.
2. Materials and Methods
2.1. Study design, Sampling and Data collection
A cross-sectional study was conducted within the municipality of Hail in Saudi Arabia. This study utilized an online questionnaire administered between August and September 2022 to assess the level of awareness and knowledge among the Hail population regarding the appropriate utilization of NSAIDs and the associated complications. Multiple social media platforms, including Twitter, Snapchat, WhatsApp, and Instagram, were employed as dissemination channels for our questionnaire to reach the target population.
2.2. Questionnaire description
The questionnaire was structured into five distinct sections comprising 25 questions. The initial section pertains to collecting demographic data from the study participants, encompassing age, gender, socioeconomic status, marital status, education level, and occupation. The second section was dedicated to eliciting the medical history of the participants, including inquiries related to any chronic diseases they may have experienced, occurrences of GI upset, and the frequency of pain episodes they have encountered. The third section focused on discerning the specific types of NSAIDs employed by the participants. In the fourth section, participants were probed about their NSAID usage habits, encompassing aspects such as the rationale behind their NSAID utilization, the timing of NSAID ingestion, the duration over which these medications were taken, the number of tablets consumed per day, and the sources from which they acquire information about NSAIDs. The fifth and final section of the questionnaire was dedicated to evaluating the knowledge possessed by the participants regarding potential complications associated with NSAID usage.
2.3. Pilot study
The validity and accuracy of the questionnaire were rigorously assessed through a pilot study, ensuring that the instrument is reliable and effectively captures the intended information for the research.
2.4. Sample size calculation
We employed the Raosoft® sample size calculator, with a specified margin of error of 5% and a confidence level set at 95% and after calculations 377 sample size was obtained, furthermore, sampling error was taken into account by calculating 377 * 1.058 that corresponds to 399.
2.5. Statistical analysis
The data collected were subjected to encoding and preprocessing procedures before statistical analysis, which involved employing MS Excel for data manipulation and organization. Subsequent statistical analyses were performed using SPSS-21 software. Descriptive statistical metrics, specifically frequencies, and proportions represented as percentages, were computed to examine an array of qualitative variables encompassing socio-demographic attributes and factors pertaining to NSAIDS utilization. In the subsequent multiple logistic regression analysis, independent variables were subjected to a rigorous selection process, employing a significance threshold set at a p-value < 0.05 for screening and inclusion.
3. Results
3.1. Demographic characteristics
The gender distribution indicated that 170 participants (42.61%) were male, while 229 (57.39%) were female. In terms of age, 73 participants (18.43%) fell within the 18-20 age range, 124 (30.96%) were between the ages of 21-29, 54 (13.51%) were aged 30-39, and 85 (21.13%) were in the 40-49 age group. Education levels varied, with 79 participants (19.9%) having completed high school or less, 44 (11.12%) with a diploma, 261 (65.6%) holding a bachelor's degree, 18 (4.45%) having a master's degree, and 9 (2.36%) possessing a PhD. In terms of occupation, 26 participants (6.52%) worked in the private sector, 123 (30.83%) held government jobs, 12 (3.01%) were involved in business, 42 (10.53%) were housewives, 25 (6.27%) were unemployed, 24 (6.02%) were retired, 3 (1%) worked from home, and 143 (35.84%) were students. Regarding monthly income, 133 participants (33.34%) reported earnings above the average, 195 (48.9%) had an average income, and 73 (18.3%) earned below the average. Marital status revealed that 7 participants (1.8%) were divorced, 202 (50.6%) were married, 188 (47.1%) were single, and 2 (0.5%) were widowed (Table 1). In terms of reasons, muscle pain was reported by 53 (13.34%) participants, while headaches were a concern for 109 (27.4%) participants. Fever was experienced by 33 (8.23%) participants, and toothache affected 68 (17.2%) participants. Menstrual cycle-related issues were reported by 60 (14.92%) participants, and joint pain was observed in 52 (13.2%) of the cases. The remaining health issues, categorized as "Others," were reported by 20 (5.1%) of the cases (Table 1).
Additionally, association between demographic variables and reasons for using NSAIDs, such as muscle pain, headache, fever, toothache, menstrual cycle, joint pain, and others, were presented with associated p-values, indicating the level of significance. Gender, occupation, and marital status had non-significant association (p>0.01) except for menstrual cycle and joint pain while marital status also had significant association with other reasons. While age had significant association with muscle pain, menstrual cycle, and joint pain (p<0.01). Meanwhile, education and monthly income had non-significant associations with all the reasons (Table 2).
3.2. Association between demographic variables and pain frequency
In terms of gender, a significant association (p=0.01) was found as 99 males (47.6%) experienced irregular pain, 7 (30.4%) had daily pain, 25 (53.2%) reported weekly pain, and 39 (32.2%) experienced monthly pain. Among females, 109 (52.4%) experienced irregular pain, 16 (69.6%) had daily pain, 22 (46.8%) reported weekly pain, and 82 (67.8%) experienced monthly pain. When considering age, individuals aged 18-20 experienced irregular pain in 30 cases (14.4%), daily pain in 5 cases (21.7%), weekly pain in 14 cases (29.8%), and monthly pain in 26 cases (21.5%). In the 21-29 age group, 67 participants (32.2%) experienced irregular pain, 5 (21.7%) had daily pain, 12 (25.5%) reported weekly pain, and 42 (34.7%) experienced monthly pain. The 30-39 age group had 29 individuals (13.9%) with irregular pain, 6 (26.1%) with daily pain, 4 (8.5%) with weekly pain, and 16 (13.2%) with monthly pain. In the 40-49 age group, 46 participants (22.1%) experienced irregular pain, 2 (8.7%) had daily pain, 7 (14.9%) had weekly pain, and 31 (25.6%) experienced monthly pain. For those aged 50-59, 30 individuals (14.4%) experienced irregular pain, 4 (17.4%) had daily pain, 8 (17.0%) had weekly pain, and 4 (3.3%) experienced monthly pain. In the age group above 60, 6 individuals (2.9%) experienced irregular pain, 1 (4.3%) had daily pain, 2 (4.3%) reported weekly pain, and 2 (1.7%) experienced monthly pain, with a non-significant association (p=0.03). Education level also played a significant role, with participants with a high school education or less having 39 participants (18.8%) experiencing irregular pain, 5 (21.7%) having daily pain, 13 (27.7%) having weekly pain, and 20 (16.5%) experiencing monthly pain. Those with a diploma had 25 participants (12.0%) experiencing irregular pain, 2 (8.7%) with daily pain, 5 (10.6%) with weekly pain, and 12 (9.9%) with monthly pain. Individuals with a bachelor's degree had 136 (65.4%) with irregular pain, 10 (43.5%) with daily pain, 26 (55.3%) with weekly pain, and 85 (70.2%) with monthly pain. Those with a master's degree had 6 participants (2.9%) experiencing irregular pain, 3 (13.0%) with daily pain, 1 (2.1%) with weekly pain, and 4 (3.3%) with monthly pain. Lastly, participants with a PhD had 2 (1.0%) experiencing irregular pain, 3 (13.0%) with daily pain, 2 (4.3%) with weekly pain, and none with monthly pain, with a significant association (p=0.001). In terms of occupation, those in the private sector had 14 participants (6.7%) experiencing irregular pain, 3 (6.4%) with weekly pain, and 9 (7.4%) with monthly pain. Individuals with a government job had 68 (32.7%) experiencing irregular pain, 8 (34.8%) with daily pain, 14 (29.8%) with weekly pain, and 33 (27.3%) with monthly pain. Business professionals had 2 (1.0%) experiencing irregular pain, 1 (4.3%) with daily pain, 2 (4.3%) with weekly pain, and 7 (5.8%) with monthly pain. Housewives had 25 participants (12.0%) with irregular pain, 3 (8.5%) with weekly pain, and 10 (8.3%) with monthly pain. Unemployed individuals had 13 (6.3%) with irregular pain, 2 (8.7%) with daily pain, and 10 (8.3%) with monthly pain. Retired participants had 14 (6.7%) with irregular pain, 2 (8.7%) with daily pain, 4 (8.5%) with weekly pain, and 4 (3.3%) with monthly pain. Those who worked from home had 1 (0.5%) with irregular pain and 3 (2.5%) with monthly pain, while students had 71 (34.1%) with irregular pain, 7 (30.4%) with daily pain, 20 (42.6%) with weekly pain, and 45 (37.2%) with monthly pain and non-significant (p=0.43) association was found. When considering monthly income, those above the average had 63 participants (30.3%) experiencing irregular pain, 8 (34.8%) with daily pain, 23 (48.9%) with weekly pain, and 36 (29.8%) with monthly pain. Those with average income had 101 (48.6%) experiencing irregular pain, 9 (39.1%) with daily pain, 19 (40.4%) with weekly pain, and 66 (54.5%) with monthly pain. Participants with below-average income had 44 (21.2%) with irregular pain, 6 (26.1%) with daily pain, 5 (10.6%) with weekly pain, and 19 (15.7%) with monthly pain, with non-significant association (p=0.12). Lastly, regarding marital status, a non-significant association with a p-value of 0.20 was observed as divorced respondents had 2 (1.0%) with irregular pain and 5 (4.1%) with monthly pain. Married individuals had 111 (53.4%) with irregular pain, 12 (52.2%) with daily pain, 22 (46.8%) with weekly pain, and 57 (47.1%) with monthly pain. Singles had 95 (45.7%) with irregular pain, 10 (43.5%) with daily pain, 25 (53.2%) with weekly pain, and 58 (47.9%) with monthly pain, while widowed participants had 1 (4.3%) with daily pain and none with weekly or monthly pain (Table 3).
In Table 4, the regression analysis revealed that gender played a significant role, with females having higher odds of knowledge (AOR = 1.75, 95% CI 1.10-2.88) than males. Age also had a notable impact, with individuals aged 50-59 (AOR = 0.21, 95% CI 0.07-0.66) and those above 60 (AOR = 0.30, 95% CI 0.05-1.92) showing lower odds of knowledge compared to the reference group (18-20 years). Education had varied effects, where individuals with a PhD (AOR = 3.50, 95% CI 0.54-22.51) exhibited the highest odds of knowledge among the education categories. Occupation-wise, those in business (AOR = 6.12, 95% CI 1.10-35.10) had significantly higher odds of knowledge than those in the private sector, while housewives (AOR = 0.76, 95% CI 0.25-2.27) had lower odds. Monthly income did not show significant associations with knowledge.
In Table 5, the bifurcation of medications concerning gender revealed differences in the use of various medications between females and males. When it came to aspirin, 202 females (56.6%) answered "No," while 27 females (64.3%) answered "Yes," compared to 155 males (43.4%) answering "No" and 15 males (35.7%) answering "Yes," with a p-value of 0.34. For diclofenac, 110 females (50.2%) answered "No," and 119 females (66.1%) answered "Yes," while 109 males (49.8%) answered "No," and 61 males (33.9%) answered "Yes," with a significant p-value of 0.001. Similar differences were observed with ibuprofen (p-value = 0.01), celecoxib (p-value = 0.004), and mefenamic acid (p-value = 0.08). However, ketoprofen, meloxicam, naproxen, and piroxicam did not show statistically significant differences between the genders, with p-values of 0.58, 0.76, 1.00, and 0.36, respectively.
Meanwhile, >50% of the participants had knowledge of adverse events related to the use of NSAIDs while 25% had no knowledge. Moreover, 59 (25.766%) participants reported discomfort with the use of NSAIDs. In addition, 50% and >75% of participants considered NSAIDs can cause peptic ulcers and damage kidneys, respectively (Figure 1). Meanwhile, 39.3% of participants wanted all NSAIDs to be available without prescription.
In the present study, it was found that regarding the sources of information about the use of NSAIDs concerning gender, several significant differences were observed. Regarding information from physicians, a p-value of 0.12 indicated non-statistical significant difference between females and males, with 75.5% of females and 81.8% of males responding negatively. In comparison, 24.5% of females and 18.2% of males responded positively. However, information from pharmacists yielded a notable difference with a p-value of 0.01, suggesting that more females (69.4%) received information negatively compared to males (80.6%), where 30.6% of females and 19.4% of males received positive information. Information from relatives also showed a significant disparity with a p-value of 0.001, as 82.1% of females and 94.1% of males did not receive information from relatives. In comparison, 17.9% of females and 5.9% of males did. Information from friends, social media, and other sources did not exhibit significant differences between females and males, as indicated by their p-values of 0.86, 0.13, and 0.60. Moreover, the frequency of Non-steroidal anti-inflammatory drug usage revealed a significant discrepancy with a p-value of 0.001, demonstrating that more females (33.2%) did not use the tablets compared to males (55.3%), and the usage pattern varied across the categories (Table 6).
4. Discussion
NSAIDs are among the most commonly used medications due to their anti-inflammatory, anti-pyretic, and analgesic properties. However, improper use of NSAIDs in the long term is associated with GI, cardiovascular, and renal toxicity. The widespread use of NSAIDs worldwide and their serious adverse effects cause the severe problem of NSAIDs [4]. This study was the first to assess the people's awareness of NSAIDs use in the Hail region, Saudi Arabia.
In the present study, age, gender, occupation, and marital status had a significant association (p<0.01) with menstrual cycle and joint pain while age also had significant association with muscle pain. The significant associations between age, gender, occupation, and marital status with menstrual cycle and joint pain could be attributed to various factors. Age, being a significant factor in the use of NSAIDs for muscle pain, might suggest that as individuals age, they are more likely to experience muscle pain, thereby leading to NSAID use and most used drugs in elderly people [22]. Gender differences may be linked to variations in pain thresholds and reporting, with women potentially experiencing menstrual cycle and joint pain more frequently [23]. Occupational and marital status may influence the physical demands of a person's work and their social support network, which in turn can impact the experience of joint pain. These findings underscore the complex interplay of demographic variables in shaping individuals' pain experiences and subsequent use of NSAIDs. Moreover, it was also observed that 57.4% of the participants had utilized NSAIDs, signifying that NSAID usage within the Hail region is prevalent and readily accessible. Our study further revealed that the predominant NSAID used was diclofenac, which aligns with prior research conducted in Saudi Arabia, where diclofenac was reported as the most frequently used drug within the country across all drug classes [24]. Additionally, consistent with findings from a study in Turkey, diclofenac emerged as the most commonly used NSAID [25]. In contrast, a study conducted in Saudi Arabia found that the prevalent type of NSAID was ibuprofen [26]. These observations underscore the variability in NSAID utilization patterns, which can be attributed to regional and cultural distinctions in drug preferences.
Our study shows that a notable proportion of participants use NSAIDs without a prescription, reflecting a relatively permissive attitude toward their utilization, and 39.3% of participants believed in the accessibility of NSAIDs without any prescription. Notably, this finding aligns with the opinions of around one-third of the participants, who opined that such medications should be available without needing a prescription. Similarly, without a prescription, NSAIDs were taken by 83.7% of medical students and 84.7% of non-medical students in Karachi, Pakistan [27].
Furthermore, our results indicate that a substantial proportion of NSAID users, approximately >50%, reported an absence of discomfort, side effects, or problems associated with their usage. While approximately 50% of participants reported a history of GI upset (peptic ulcer), it remains challenging to conclusively attribute this to using NSAIDs alone, as other contributing factors may be at play. Moreover, a breakdown of NSAID usage patterns revealed that about 62% of participants employed NSAIDs for 1 to 3 days, while roughly 22% extended usage to 4 to 7 days. Of note, it is imperative to acknowledge that even from the inception of use, all NSAIDs engender an elevated risk of adverse effects, including GI bleeding, myocardial infarction, and stroke [28,29]. Notably, NSAIDs are associated with a rise in systolic blood pressure by approximately 5 mmHg and an increase in fluid retention. In patients administered coxibs, diclofenac, and higher-dose ibuprofen, these effects contribute to an excess risk of approximately 7 to 9 non-fatal and 2 fatal cardiovascular events per 1000 patients annually. This underlines the heightened risk of developing adverse effects due to NSAIDs from the very onset of usage [30].
Our study also revealed that the participants (male and female) sourced information about NSAIDs from physicians and pharmacists, indicating the significant role played by pharmacists in patient counseling. This observation aligns with the findings of two studies conducted in Saudi Arabia [26]. Concerning perceptions of NSAIDs, over 60% of the participants believed that NSAIDs could lead to developing diseases, whereas around 25% perceived them as not causing any diseases. A notable percentage, approximately 41%, expressed uncertainty regarding the relationship between NSAIDs and peptic ulcers, with roughly 10% of participants asserting that NSAIDs did not cause peptic ulcers at all. These findings underscore a lack of awareness among nearly half of the participants regarding the gastrointestinal complications associated with NSAIDs, which may potentially progress to more severe conditions, such as cancer. Furthermore, our study indicates that about 77% of participants concurred that NSAIDs could contribute to kidney damage. Notably, almost half of the participants admitted to being uninformed about the potential side effects of NSAIDs, highlighting a significant knowledge gap concerning the adverse effects of NSAIDs, which can result in severe systemic repercussions. These findings align with a study conducted in Poland, which reported that approximately 57% of individuals were unaware of the side effects associated with NSAIDs [31].
5. Conclusions
The findings of our investigation underscore a notable deficiency in the participants' understanding of NSAIDs usage and its associated complications. This highlights a pressing imperative for comprehensive public education initiatives in several respects. Enhancing public awareness concerning alternative pharmaceutical options characterized by comparably reduced adverse effects relative to widely utilized drugs is imperative. Furthermore, healthcare practitioners are pivotal in disseminating pertinent information regarding medication usage and its attendant implications to patients. Community pharmacists, in particular, are responsible for providing guidance to individuals procuring medications without prior medical consultation. The discerned inadequacy concerning NSAIDs utilization and associated risks necessitates immediate and extensive public enlightenment efforts to promote judicious NSAIDs utilization.
Author Contributions
Conceptualization, S.A.; methodology, A.T.A, W.S.A, S.F.A.; software, S.A.; validation, S.A..; data curation, S.A.A, N.F.A, S.Al.; writing—original draft preparation, A.T.A, W.S.A.; writing—review and editing, S.A.; supervision, S.A.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical clearance was secured from the University's Ethics Committee under the reference number (H-2022-315). Stringent measures were implemented to uphold the confidentiality of participants' personal information.
Informed Consent Statement
Before administering the questionnaire, informed consent was duly obtained from each participant. Furthermore, a written statement was explicitly presented to participants, articulating the exclusive intent of the collected data for scientific research purposes.
Acknowledgments
Authors acknowledge the support from College of Pharmacy, University of Hail, Saudi Arabia.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Silva, F.; Costa, G.; Veiga, F.; Cardoso, C.; Paiva-Santos, A.C. Parenteral Ready-to-Use Fixed-Dose Combinations Including NSAIDs with Paracetamol or Metamizole for Multimodal Analgesia—Approved Products and Challenges. Pharm. 2023, 16, 1084. [Google Scholar] [CrossRef]
- Ozleyen, A.; Yilmaz, Y.B.; Donmez, S.; Atalay, H.N.; Antika, G.; Tumer, T.B. Looking at NSAIDs from a historical perspective and their current status in drug repurposing for cancer treatment and prevention. J. Cancer Res. Clin. Oncol. 2023, 149, 2095–2113. [Google Scholar] [CrossRef]
- Bhala, N.; Emberson, J.; Merhi, A.; Abramson, S.; Arber, N.; Baron, J.A.; Bombardier, C.; Cannon, C.; Farkouh, M.E.; FitzGerald, G.A.; et al. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomised trials. Lancet (London, England) 2013, 382, 769–779. [Google Scholar] [CrossRef]
- Bindu, S.; Mazumder, S.; Bandyopadhyay, U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: A current perspective. Biochem. Pharmacol. 2020, 180, 114147. [Google Scholar] [CrossRef]
- Conaghan, P.G. A turbulent decade for NSAIDs: update on current concepts of classification, epidemiology, comparative efficacy, and toxicity. Rheumatol. Int. 2012, 32, 1491–1502. [Google Scholar] [CrossRef]
- CDC. Percentage of U.S. Adults Using Prescribed NSAIDs. Available online: https://nccd.cdc.gov/ckd/detail.aspx?Qnum=Q700 (accessed on 11-1).
- AlKhamees, O.A.; AlNemer, K.A.; Bin Maneea, M.W.; AlSugair, F.A.; AlEnizi, B.H.; Alharf, A.A. Top 10 most used drugs in the Kingdom of Saudi Arabia 2010-2015. Saudi. Pharm. J. 2018, 26, 211–216. [Google Scholar] [CrossRef]
- Ali, K.A.; Maity, A.; Roy, S.D.; Das Pramanik, S.; Pratim Das, P.; Shaharyar, M.A. Chapter 4 - Insight into the mechanism of steroidal and non-steroidal anti-inflammatory drugs. In How Synthetic Drugs Work; Kazmi, I., Karmakar, S., Shaharyar, M.A., Afzal, M., Al-Abbasi, F.A., Eds.; Academic Press, 2023; pp. 61–94. [Google Scholar]
- Panchal, N.K.; Prince Sabina, E. Non-steroidal anti-inflammatory drugs (NSAIDs): A current insight into its molecular mechanism eliciting organ toxicities. Food Chem. Toxicol. 2023, 172, 113598. [Google Scholar] [CrossRef]
- Marra, P.S.; Nishizawa, Y.; Yamanashi, T.; Sullivan, E.J.; Comp, K.R.; Crutchley, K.J.; Wahba, N.E.; Shibata, K.; Nishiguchi, T.; Yamanishi, K.; et al. NSAIDs use history: impact on the genome-wide DNA methylation profile and possible mechanisms of action. Clin. Exp. Med. 2023, 23, 3509–3516. [Google Scholar] [CrossRef]
- Sohail, R.; Mathew, M.; Patel, K.K.; Reddy, S.A.; Haider, Z.; Naria, M.; Habib, A.; Abdin, Z.U.; Chaudhry, W.R.; Akbar, A. Effects of Non-steroidal Anti-inflammatory Drugs (NSAIDs) and Gastroprotective NSAIDs on the Gastrointestinal Tract: A Narrative Review. Cureus 2023, 15. [Google Scholar] [CrossRef]
- Wan, E.Y.F.; Yu, E.Y.T.; Chan, L.; Mok, A.H.Y.; Wang, Y.; Chan, E.W.Y.; Wong, I.C.K.; Lam, C.L.K. Comparative Risks of Nonsteroidal Anti-inflammatory Drugs on Cardiovascular Diseases: A Population-Based Cohort Study. J. Clin. Pharmacol. 2023, 63, 126–134. [Google Scholar] [CrossRef]
- LaForge, J.M.; Urso, K.; Day, J.M.; Bourgeois, C.W.; Ross, M.M.; Ahmadzadeh, S.; Shekoohi, S.; Cornett, E.M.; Kaye, A.M.; Kaye, A.D. Non-steroidal Anti-inflammatory Drugs: Clinical Implications, Renal Impairment Risks, and AKI. Adv. Ther. 2023, 40, 2082–2096. [Google Scholar] [CrossRef]
- Martin, J.R.; Yu, M.; Erstad, B.L. Adverse effects of nonsteroidal anti-inflammatory drugs in critically ill patients: A scoping review. AJHP 2023, 80, 348–358. [Google Scholar] [CrossRef]
- Baker, M.; Perazella, M.A. NSAIDs in CKD: Are They Safe? Am. J. Kidney. Dis. 2020, 76, 546–557. [Google Scholar] [CrossRef]
- Asiri, O. , Alzahrani AA, Alshehri KM, Althomali OW, Alameen AAI, Serwah MA. . Prevalence of non-steroidal anti-inflammatory drugs usage and assessment of knowledge related to its complications among Saudi population; a cross-sectional study IJMDC 2020, 4, 296–302. [Google Scholar]
- Siddig, A.I.; Alqahtani, A.M.; AlShalawi, A.; Turkistani, M.; Binbaz, S.; Altowairqi, A. Awareness of analgesics complications in Saudi Arabia: a cross-sectional study. Future J. Pharm. Sci. 2020, 6, 6. [Google Scholar] [CrossRef]
- Babelghaith, S.D.; Alarifi, M.N.; Wajid, S.; Alhawassi, T.M.; Alqahtani, S.K.; Alghadeer, S.M. Knowledge of patients on safe medication use in relation to nonsteroidal anti-inflammatory drugs. Saudi. J. Anaesth. 2019, 13, 106–111. [Google Scholar] [CrossRef]
- Mullan, J.; Weston, K.M.; Bonney, A.; Burns, P.; Mullan, J.; Rudd, R. Consumer knowledge about over-the-counter NSAIDs: they don't know what they don't know. Aust. N. Z. J. Public. Health. 2017, 41, 210–214. [Google Scholar] [CrossRef]
- Vina, E.R.; Hannon, M.J.; Quinones, C.; Hausmann, L.R.M.; Ibrahim, S.A.; Dagnino, J.; Kwoh, C.K. The Role of Knowledge and Attitudes About Nonsteroidal Anti-inflammatory Drugs in Determining Treatment Use. ACR Open Rheumatol. 2021, 3, 154–163. [Google Scholar] [CrossRef]
- AlMuammar, S.A.; Noorsaeed, A.S.; Alafif, R.A.; Kamal, Y.F.; Daghistani, G.M. The Use of Internet and Social Media for Health Information and Its Consequences Among the Population in Saudi Arabia. Cureus 2021, 13, e18338. [Google Scholar] [CrossRef]
- Wongrakpanich, S.; Wongrakpanich, A.; Melhado, K.; Rangaswami, J. A Comprehensive Review of Non-Steroidal Anti-Inflammatory Drug Use in The Elderly. Aging Dis. 2018, 9, 143–150. [Google Scholar] [CrossRef]
- Bäckryd, E. Gender differences in dispensed analgesics in Sweden during 2006–2015–an observational, nationwide, whole-population study. Int. J. Womens. Health. 2018, 55–64. [Google Scholar] [CrossRef]
- Al-Khamees, O.A.; AlNemer, K.A.; Bin Maneea, M.W.; AlSugair, F.A.; AlEnizi, B.H.; Alharf, A.A. Top 10 most used drugs in the Kingdom of Saudi Arabia 2010–2015. Saudi. Pharm. J. 2018, 26, 211–216. [Google Scholar] [CrossRef]
- Coşkuner, İ.; Yilmaz, T.E. Awareness among patients taking oral non-steroidal anti-inflammatory drugs as analgesics: a cross-sectional study. J. Health. Sci. Med. 2021, 4, 63–70. [Google Scholar] [CrossRef]
- Asiri, O.A.; Alzahrani, A.A.; Alshehri, K.M.; Althomal, O.W.; Alameen, A.A.I.; Serwah, M.A. Prevalence of non-steroidal anti-inflammatory drugs usage and assessment of knowledge related to its complications among Saudi population; a cross-sectional study. IJMDC 2020, 68, 19–11. [Google Scholar] [CrossRef]
- Suleman, M., Ahsan Ahmed; Kamran, M.; Ashraf, H.; Subata Siddiqui, U.N.; Siddiqui, A.H. Knowledge of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) and their Adverse Effects among Medical and Non-Medical Students. Pak. J. Med. Dent. 2022, 11, 94–99. [Google Scholar]
- Bally, M.; Dendukuri, N.; Rich, B.; Nadeau, L.; Helin-Salmivaara, A.; Garbe, E.; Brophy, J.M. Risk of acute myocardial infarction with NSAIDs in real world use: bayesian meta-analysis of individual patient data. BMJ (Clinical research ed.) 2017, 357, j1909. [Google Scholar] [CrossRef]
- Schjerning Olsen, A.-M.; Gislason, G.H.; McGettigan, P.; Fosbøl, E.; Sørensen, R.; Hansen, M.L.; Køber, L.; Torp-Pedersen, C.; Lamberts, M. Association of NSAID Use With Risk of Bleeding and Cardiovascular Events in Patients Receiving Antithrombotic Therapy After Myocardial Infarction. JAMA 2015, 313, 805–814. [Google Scholar] [CrossRef]
- Bhala, N.; Emberson, J.; Merhi, A.; Abramson, S.; Arber, N.; Baron, J.; Bombardier, C.; Cannon, C.; Farkouh, M.; FitzGerald, G. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomised trials. Lancet (London, England) 2013, 382, 769–779. [Google Scholar]
- Matoulková, P.; Dosedel, M.; Růzková, B.; Kubena, A. Information and awareness concerning ibuprofen as an ingredient in over the counter analgesics: a questionnaire-based survey of residents of retirement communities. Acta. Pol. Pharm. 2013, 70, 333–338. [Google Scholar]
Figure 1.
Knowledge of adverse events related to the use of NSAIDs.
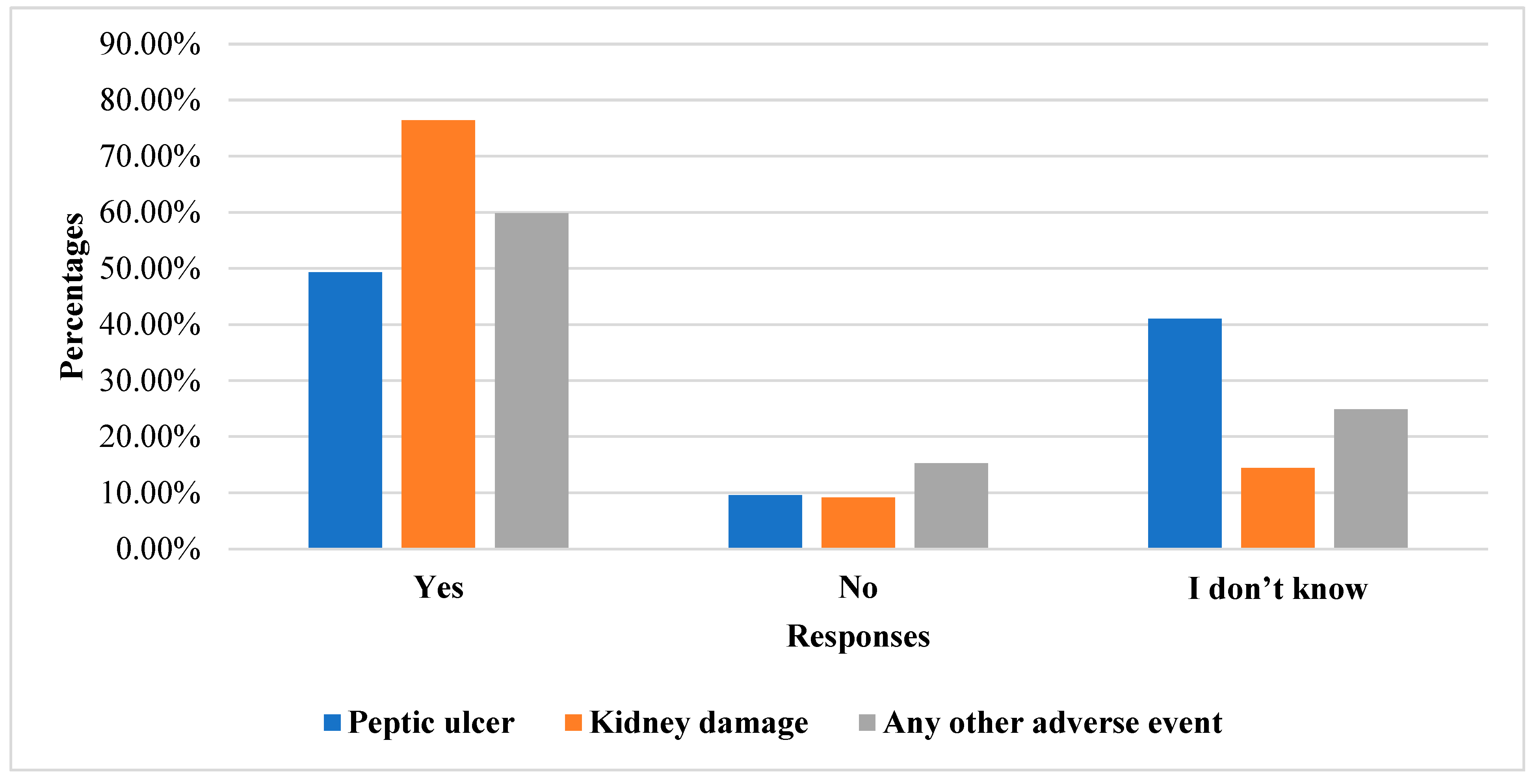

Table 1.
Demographic variable of the respondents (n=399).
| Demographic | Variables | Number | Percentage |
|---|---|---|---|
| Gender | Male | 170 | 42.61 |
| Female | 229 | 57.39 | |
| Age | 18-20 | 73 | 18.43 |
| 21-29 | 124 | 30.96 | |
| 30-39 | 54 | 13.51 | |
| 40-49 | 85 | 21.13 | |
| Education | High School or less | 79 | 19.9 |
| Diploma | 44 | 11.12 | |
| Bachelors | 261 | 65.6 | |
| Master | 18 | 4.45 | |
| PhD | 9 | 2.36 | |
| Occupation | Private Sector | 26 | 6.52 |
| Government Job | 123 | 30.83 | |
| Business | 12 | 3.01 | |
| House Wife | 42 | 10.53 | |
| Unemployed | 25 | 6.27 | |
| Retired | 24 | 6.02 | |
| Work from home | 3 | 1 | |
| Student | 143 | 35.84 | |
| Monthly Income | Above the Average | 133 | 33.34 |
| Average | 195 | 48.9 | |
| Below the average | 73 | 18.3 | |
| Marital status | Divorced | 7 | 1.8 |
| Married | 202 | 50.6 | |
| Single | 188 | 47.1 | |
| Widowed | 2 | 0.5 | |
| Reasons for use | Muscle Pain | 53 | 13.34 |
| Headache | 109 | 27.4 | |
| Fever | 33 | 8.23 | |
| Toothache | 68 | 17.2 | |
| Menstrual Cycle | 60 | 14.92 | |
| Joint Pain | 52 | 13.2 | |
| Others | 20 | 5.1 |
Table 2.
Association between demographic variables and reasons for using NSAIDs (n=399).
| Demographic factors | ||||||
|---|---|---|---|---|---|---|
| Variables | Gender p-value | Age p-value |
Education p-value | Occupation p-value | Monthly income p-value |
Marital status p-value |
| Muscle pain | 0.34 | 0.01 | 0.24 | 0.12 | 0.55 | 0.14 |
| Headache | 0.11 | 0.31 | 0.19 | 0.85 | 0.18 | 0.18 |
| Fever | 0.16 | 0.03 | 0.63 | 0.26 | 0.34 | 0.53 |
| Toothache | 0.10 | 0.35 | 0.12 | 0.11 | 0.22 | 0.66 |
| Menstrual cycle | 0.001 | 0.001 | 0.23 | 0.01 | 0.05 | 0.01 |
| Joint pain | 0.002 | 0.001 | 0.05 | 0.001 | 0.52 | 0.001 |
| Others | 0.29 | 0.18 | 0.45 | 0.25 | 0.67 | 0.01 |
Table 3.
Association between demographic variable and pain frequency.
| Variables | Categories | Pain frequency | ||||
|---|---|---|---|---|---|---|
| Irregular | Daily | Weekly | Monthly | p-value | ||
| Gender | Male | 99 (47.6) | 7 (30.4) | 25 (53.2) | 39 (32.2) | 0.01 |
| Female | 109 (52.4) | 16 (69.6) | 22 (46.8) | 82 (67.8) | ||
| Age (years) | 18-20 | 30 (14.4) | 5 (21.7) | 14 (29.8) | 26 (21.5) | 0.03 |
| 21-29 | 67 (32.2) | 5 (21.7) | 12 (25.5) | 42 (34.7) | ||
| 30-39 | 29 (13.9) | 6 (26.1) | 4 (8.5) | 16 (13.2) | ||
| 40-49 | 46 (22.1) | 2 (8.7) | 7 (14.9) | 31 (25.6) | ||
| 50-59 | 30 (14.4) | 4 (17.4) | 8 (17.0) | 4 (3.3) | ||
| Above 60 | 6 (2.9) | 1 (4.3) | 2 (4.3) | 2 (1.7) | ||
| Education | High School or less | 39 (18.8) | 5 (21.7) | 13 (27.7) | 20 (16.5) | 0.001 |
| Diploma | 25 (12.0) | 2 (8.7) | 5 (10.6) | 12 (9.9) | ||
| Bachelors | 136 (65.4) | 10 (43.5) | 26 (55.3) | 85 (70.2) | ||
| Master | 6 (2.9) | 3 (13.0) | 1 (2.1) | 4 (3.3) | ||
| PHD | 2 (1.0) | 3 (13.0) | 2 (4.3) | - | ||
| Occupation | Private Sector | 14 (6.7) | - | 3 (6.4) | 9 (7.4) | 0.43 |
| Government Job | 68 (32.7) | 8 (34.8) | 14 (29.8) | 33 (27.3) | ||
| Business | 2 (1.0) | 1 (4.3) | 2 (4.3) | 7 (5.8) | ||
| House Wife | 25 (12.0) | 3 (13.0) | 4 (8.5) | 10 (8.3) | ||
| Unemployed | 13 (6.3) | 2 (8.7) | - | 10 (8.3) | ||
| Retired | 14 (6.7) | 2 (8.7) | 4 (8.5) | 4 (3.3) | ||
| Work from home | 1 (0.5) | - | - | 3 (2.5) | ||
| Student | 71 (34.1) | 7 (30.4) | 20 (42.6) | 45 (37.2) | ||
| Monthly Income | Above the Average | 63 (30.3) | 8 (34.8) | 23 (48.9) | 36 (29.8) | 0.12 |
| Average | 101 (48.6) | 9 (39.1) | 19 (40.4) | 66 (54.5) | ||
| Below the average | 44 (21.2) | 6 (26.1) | 5 (10.6) | 19 (15.7) | ||
| Marital status | Divorced | 2 (1.0) | - | - | 5 (4.1) | 0.20 |
| Married | 111 (53.4) | 12 (52.2) | 22 (46.8) | 57 (47.1) | ||
| Single | 95 (45.7) | 10 (43.5) | 25 (53.2) | 58 (47.9) | ||
| Widowed | - | 1 (4.3) | - | 1 (0.8) | ||
Table 4.
Regression model for demographic variables and knowledge (n=399).
| Variables | Categories | Regression Model | |
|---|---|---|---|
| COR (95% CI) | AOR (95% CI) | ||
| Gender | Male | 1 | 1 |
| Female | 1.53 (1.10, 2.30) | 1.75 (1.10, 2.88) | |
| Age (years) | 18-20 | 1 | 1 |
| 21-29 | 0.60 (0.33, 1.05) | 0.68 (0.34, 1.37) | |
| 30-39 | 0.59 (0.29, 1.21) | 0.50 (0.17, 1.34) | |
| 40-49 | 0.58 (0.31, 1.08) | 0.39 (0.15, 1.05) | |
| 50-59 | 0.36 (0.17, 0.76) | 0.21 (0.07, 0.66) | |
| Above 60 | 0.56 (0.15, 1.98) | 0.30 (0.05, 1.92) | |
| Education | High School or less | 1 | 1 |
| Diploma | 0.78 (0.37, 1.64) | 0.94 (0.40, 2.22) | |
| Bachelors | 0.91 (0.43, 4.32) | 0.92 (0.52, 1.64) | |
| Master | 1.37 (0.43, 4.32) | 1.42 (0.41, 4.94) | |
| PHD | 2.60 (0.46, 14.04) | 3.50 (0.54, 22.51) | |
| Occupation | Private Sector | 1 | 1 |
| Government Job | 0.94 (0.40, 2.21) | 1.15 (0.44, 2.97) | |
| Business | 5.83 (1.06, 32.02) | 6.12 (1.10, 35.10) | |
| House Wife | 0.79 (0.30, 2.13) | 0.76 (0.25, 2.27) | |
| Unemployed | 1.10 (0.35, 3.23) | 1.16 (0.37, 3.63) | |
| Retired | 0.83 (0.27, 2.55) | 1.52 (0.35, 6.45) | |
| Work from home | 3.50 (0.32, 38.23) | 3.53 (0.29, 42.70) | |
| Student | 1.20 (0.51, 2.73) | 0.76 (0.29, 1.97) | |
| Monthly Income | Above the Average | 1 | 1 |
| Average | 0.87 (0.56, 1.36) | 0.77 (0.47, 1.25) | |
| Below the average | 0.64 (0.36, 1.14) | 0.65 (0.34, 1.22) | |
Table 5.
Bifurcation of medications with respect to gender.
| Variables | Categories | Regression Model | |
|---|---|---|---|
| COR (95% CI) | AOR (95% CI) | ||
| Gender | Male | 1 | 1 |
| Female | 1.53 (1.10, 2.30) | 1.75 (1.10, 2.88) | |
| Age (years) | 18-20 | 1 | 1 |
| 21-29 | 0.60 (0.33, 1.05) | 0.68 (0.34, 1.37) | |
| 30-39 | 0.59 (0.29, 1.21) | 0.50 (0.17, 1.34) | |
| 40-49 | 0.58 (0.31, 1.08) | 0.39 (0.15, 1.05) | |
| 50-59 | 0.36 (0.17, 0.76) | 0.21 (0.07, 0.66) | |
| Above 60 | 0.56 (0.15, 1.98) | 0.30 (0.05, 1.92) | |
| Education | High School or less | 1 | 1 |
| Diploma | 0.78 (0.37, 1.64) | 0.94 (0.40, 2.22) | |
| Bachelors | 0.91 (0.43, 4.32) | 0.92 (0.52, 1.64) | |
| Master | 1.37 (0.43, 4.32) | 1.42 (0.41, 4.94) | |
| PHD | 2.60 (0.46, 14.04) | 3.50 (0.54, 22.51) | |
| Occupation | Private Sector | 1 | 1 |
| Government Job | 0.94 (0.40, 2.21) | 1.15 (0.44, 2.97) | |
| Business | 5.83 (1.06, 32.02) | 6.12 (1.10, 35.10) | |
| House Wife | 0.79 (0.30, 2.13) | 0.76 (0.25, 2.27) | |
| Unemployed | 1.10 (0.35, 3.23) | 1.16 (0.37, 3.63) | |
| Retired | 0.83 (0.27, 2.55) | 1.52 (0.35, 6.45) | |
| Work from home | 3.50 (0.32, 38.23) | 3.53 (0.29, 42.70) | |
| Student | 1.20 (0.51, 2.73) | 0.76 (0.29, 1.97) | |
| Monthly Income | Above the Average | 1 | 1 |
| Average | 0.87 (0.56, 1.36) | 0.77 (0.47, 1.25) | |
| Below the average | 0.64 (0.36, 1.14) | 0.65 (0.34, 1.22) | |
Table 6.
Bifurcation of Sources of information about the use of Non-steroidal anti-inflammatory drugs with respect to gender.
Table 6.
Bifurcation of Sources of information about the use of Non-steroidal anti-inflammatory drugs with respect to gender.
| Variables | Categories | Female | Male | P-value |
|---|---|---|---|---|
| Physician | ||||
| No | 173 (75.5) | 139 (81.8) | 0.12 | |
| Yes | 56 (24.5) | 31 (18.2) | ||
| Pharmacist | ||||
| No | 159 (69.4) | 137 (80.6) | 0.01 | |
| Yes | 70 (30.6) | 33 (19.4) | ||
| Relatives | ||||
| No | 188 (82.1) | 160 (94.1) | 0.001 | |
| Yes | 41 (17.9) | 10 (5.9) | ||
| Friends | ||||
| No | 209 (91.3) | 156 (91.8) | 0.86 | |
| Yes | 20 (8.7) | 14 (8.2) | ||
| Social media | ||||
| No | 213 (93.0) | 164 (96.5) | 0.13 | |
| Yes | 16 (7.0) | 6 (3.5) | ||
| Others | ||||
| No | 217 (94.8) | 159 (93.5) | 0.60 | |
| Yes | 12 (5.2) | 11 (6.5) | ||
| Frequency | ||||
| Not used | 76 (33.2) | 94 (55.3) | 0.001 | |
| 1 | 82 (35.8) | 42 (24.7) | ||
| 2 | 49 (21.4) | 25 (14.7) | ||
| 3 | 16 (7.0) | 6 (3.5) | ||
| 4 | 2 (0.9) | 1 (0.6) | ||
| More than 4 tablets | 4 (1.7) | 2 (1.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



