
Submitted:
30 November 2023
Posted:
30 November 2023
You are already at the latest version
Abstract
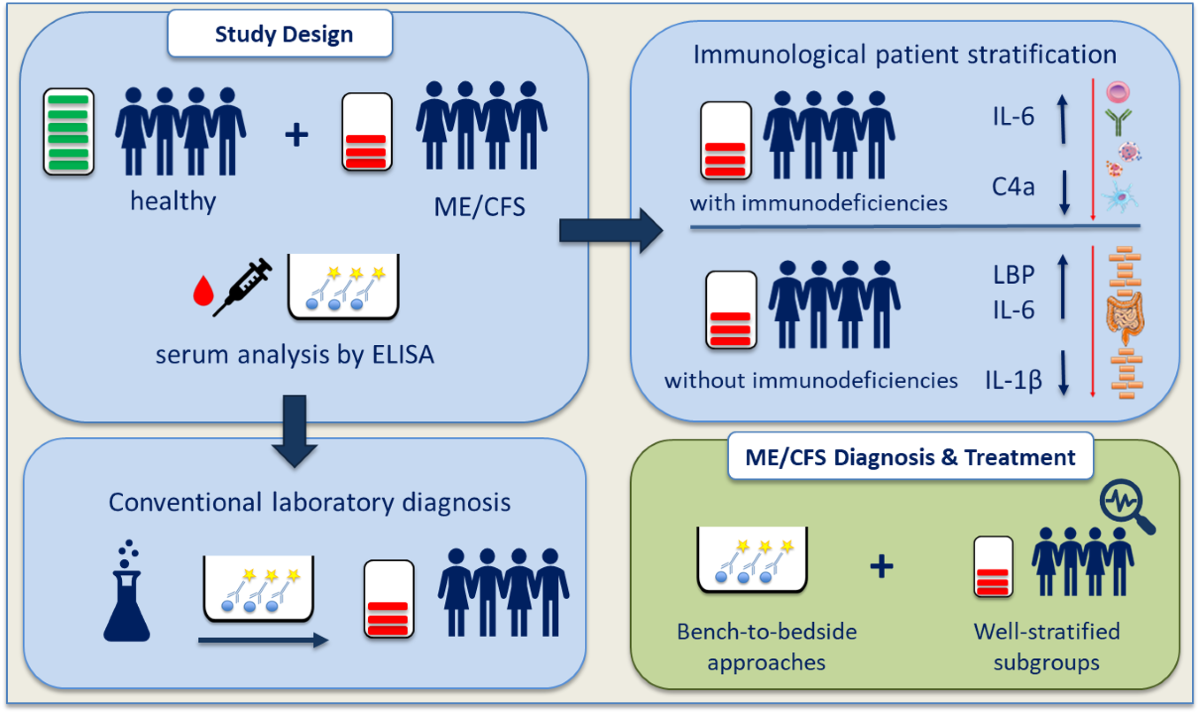
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is a complex disease characterized by profound fatigue, post-exertional malaise (PEM), and neurocognitive dysfunction. Immune dysregulation and gastrointestinal symptoms are commonly observed in ME/CFS patients. Despite affecting approximately 0.89% of the general population, the underlying pathophysiological mechanisms remain poorly understood. This study aimed to elucidate the relationship between immunological characteristics and intestinal barrier function in ME/CFS patients. ME/CFS patients were stratified into two groups based on their immune competence. After documentation of detailed medical records, serum and plasma samples were collected for assessment of inflammatory immune mediators and biomarkers for intestinal barrier integrity by ELISA. We found reduced complement protein C4a levels in immunodeficient ME/CFS patients suggesting a sub-group specific innate immune dysregulation. ME/CFS patients without immunodeficiencies exhibit a mucosal barrier leakage, as indicated by elevated levels of Lipopolysaccharide-binding protein (LBP). Stratifying ME/CFS patients based on immune competence enabled the distinction of two subgroups with different pathophysiological patterns. The study highlights the importance of emphasizing precise patient stratification in ME/CFS, particularly in the context of defining suitable treatment strategies. Given the substantial health and socioeconomic burden associated with ME/CFS, urgent attention and research efforts are needed to define causative treatment approaches.
Keywords:
myalgic encephalomyelitis
; chronic fatigue syndrome
; immunology
; immunodeficiencies
; mucosal barrier function
; patient stratification
; post-viral fatigue
; intestinal barrier leakage
; debilitating disease
1. Introduction
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a multifactorial disease associated with a profound and disabling fatigue, a systemic exercise intolerance and worsening of symptoms after physical or mental exertion, which is termed post-exertional malaise (PEM), as well as neurological and/or cognitive dysfunction. Besides, immune dysregulation, autoimmunity or immunodeficiencies (IDs) are also frequently observed in ME/CFS patients [1]. Based on data from public databases, 0.89% of the general population are estimated to suffer from ME/CFS, with approximately 1.5- to 2-fold higher prevalence in women [2]. Diverse mechanisms of disease development are discussed ranging from metabolic and endocrinological disorders to immune related mechanisms. While a subset of patients develops ME/CFS over a long-time span without being able to name a certain disease initiating event, a large subgroup of patients develops post-infectious ME/CFS, mentioning especially viral infections as the main trigger [3]. Hypotheses on disease trigger range from asymptomatic viral infections, explaining the subgroup of patients, who are not able to identify the disease initiating event, to a genetically greater host susceptibility to infections, where latent infected cells are associated with immune dysfunction and post-viral fatigue [4]. However, a definite disease trigger has not been described yet, leaving definition of pathomechanisms challenging.
With the outbreak of the COVID-19 pandemic, we are in the unique situation to monitor and investigate the mechanisms of early post-viral fatigue, which might ultimately lead to ME/CFS. SARS-CoV-2 infection, independent of the severity of the acute phase, results in 1 – 10% of cases in sequelae termed Long-COVID (LC) or post-acute sequelae of COVID-19 (PASC) [5]. While some LC symptoms are associated with organ damage due to viral host invasion [6], a sizeable subgroup of patients develops post-viral fatigue. Alarmingly, first estimations predict a doubling of ME/CFS patients due to SARS-CoV-2 within the next years [7], making an increase in ME/CFS research effort a matter of uttermost importance. Translating LC research into ME/CFS research will be crucial to improve patient health care and improve definition of disease onset and pathogenesis in ME/CFS,
Despite huge knowledge gaps in disease onset and fatigue development, similarities in ME/CFS and LC are documented. Both ME/CFS and LC are often associated with altered immune functions and a dysregulated mucosal barrier. In ME/CFS a dysregulated natural killer (NK) cell function leads to reduced cytotoxicity and increased levels of pro-inflammatory cytokines, especially, tumor necrosis factor alpha (TNF-alpha). After exertion, reduced levels of complement system components as well as elevated markers of oxidative stress were detected and the concentrations of interleukin (IL)-10 and toll-like receptor 4 (TLR4) were found to be elevated [8,9]. Furthermore, TNF-alpha, IL-6 and IL-8 were previously shown to be related to fatigue severity in ME/CFS [10]. However, results are often inconsistent through out literature depending on the study design and subsequent ME/CFS patient stratification. In LC, patient stratification and subsequent data interpretation are less challenging as the disease trigger and time of infection are known. Here, an inadequate immune function was also identified to predispose to post-viral fatigue [11]. A higher prevalence of Mannose-binding lectin (MBL) deficiency is found among LC patients with persistent severe fatigue and PEM [12]. This is also in line with ME/CFS patients developing the disease after EBV infection [1,13]. Noteworthy, MBL is essential for the innate immune response, which acts as a first line defense to prevent viral invasion or replication. It has been suggested to regulate NK cell function [14] and works as a pattern recognition receptor [15] by binding and opsonizing viral proteins, i.e. the S and N proteins of SARS-CoV-2 [16,17]. Low MBL level are associated with release of several cytokines, including TNF-alpha and IL-6 [14,18,19]. High concentrations of MBL drastically reduce IL-6 and TNF-alpha production by monocytes, as seen in response to meningococcal infection [20], which highlights the importance of well-regulated MBL level during an acute infection. Furthermore, MBL deficiency is associated to an increased susceptibility to infection and genetically determined low levels of MBL can predispose to viral diseases, such as COVID-19 [15]. Also, LC patients showed altered humoral responses to distinct herpesviruses including EBV. In accordance with these data, our group recently demonstrated an association between EBV-reactivation and LC fatigue, with presence of EBV DNA in 50% of LC fatigue patients and only 20% in fully convalescent COVID-19 patients [21]. These mechanisms tempt to hypothesize, that in a sub-set of ME/CSF and post-infectious syndrome patients, an inadequate immune activation during a viral acute phase may contribute to the disease development.
When focusing on an inadequate immune response during an acute infection, it is important to elucidate the role of mucosal barrier function. As mucosae protect the human body from the outside environment, a failed protection has been suggested to be involved in disease mechanisms of post-infectious syndromes. This hypothesis is based on frequently observed gastrointestinal complaints in ME/CFS patients. While recurring infections can be associated to inadequate host defense, most gastrointestinal affected patients suffer from symptoms similar to irritable bowel syndrome (IBS) or gastrointestinal mast cell activation disorders [22,23], without being diagnosed with inflammatory bowel disease (IBD) or other detectable inflammatory gastrointestinal disorders. The gut microbiome gained much attention in ME/CFS research with proposed pathomechanisms regarding gut dysbiosis and subsequent altered gut-brain-axis activity, but also increased gut permeability with concomitant bacterial translocation enabling a chronic, low-grade gastrointestinal inflammation. SARS-CoV-2 has been demonstrated to affect gastrointestinal barrier function via ACE-2 receptor binding, and viral particles are found in patients with gastrointestinal inflammation [24] providing a possible mechanism for intestinally triggered post-viral fatigue. Also, other discussed viral triggers of ME/CFS, like influenza virus A, coxsackievirus and several members of the Herpesviridae family are known to break mucosal tissue barriers and impair epithelial and microbial barrier functions [25,26].
Although ME/CFS has been described as a disease by the WHO more than 50 years ago and ME/CFS prevalence is increasing due to SARS-CoV-2, the exact causes of the disease remain elusive. The lack of well-characterized patient stratification not only hinders identification of biomarkers, which are urgently needed in diagnostics, but also ultimately impairs the definition of causative treatment approaches. Most intervention approaches with diverse compounds such as antivirals and monoclonal antibody rituximab have not shown promising results [27,28,29]. Thus, ME/CFS patients rely on symptomatic treatment, partially with off-label use of medication, and energy management (pacing) [30], which enables patients to successfully manage their disease. However, symptomatic treatment is highly individual and often poorly documented. In contrast, pacing prevents PEM and sustainable disease improvement might also be explained by the prevention of de-conditioning [31]. Until today, there is no cure or approved treatment strategy for ME/CFS [31].
In this study, we aim to evaluate immunological and mucosal barrier related insights in an Austrian ME/CFS cohort. Understanding immune dysfunction and the impact of related factors, like immunodeficiency and mucosal barrier disruption, can lead to targeted interventions and therapies to alleviate symptoms and improve patient outcomes. We offer insights into ME/CFS subgroups, with the ultimate goal of improving the medical care situation of ME/CFS and post-infectious fatigue patients.
2. Materials and Methods
2.1. Study Cohort and Sampling Procedure
All participants provided written informed consent before study inclusion. As shown in Figure 1, 39 ME/CFS patients and 19 healthy sex- and age matched control participants were recruited. ME/CFS was diagnosed based on the Institute of Medicine (IOM) criteria [32] which define that following three symptoms and at least one of two additional manifestations are required for diagnosis. The three required symptoms are: (1) a substantial reduction/impairment in the ability to engage in pre-illness levels of activity, (2) PEM and (3) unrefreshing sleep. Additional manifestations include cognitive impairment and/or orthostatic intolerance. ME/CFS patients were further divided in a group of patients without immunodeficiencies (ME/CFS – ID, n=19) and patients with immunodeficiencies (ME/CFS + ID, n=20). The immunological stratification of the ME/CFS patients (Figure 1) was conducted during diagnostic evaluations prior to study participation. Before sampling of biological material, participants were asked to give a detailed medical record on background and individual symptoms. The information was collected to enable detailed stratification after the analyses of disease markers. ME/CFS patients with immunodeficiencies were in average 41.2 years old (± 12.6 years) and 75% female, while ME/CFS patients without immunodeficiencies were in average 38.4 years old (± 10.8 years) and 84.2% female. Healthy control participants were in average 43.1 years old (± 13.0 years) and 73.7% female (Table 1). Besides one severely affected patient in the ME/CFS – ID group, all ME/CFS patients were mild to moderate affected by the disease. Healthy controls were excluded when suffering from neurological, immunological or psychiatric pre-existing conditions. Blood was collected in serum and plasma/EDTA vials on the day of study participation at the Institute for Pathophysiology and Allergy Research, Medical University of Vienna. After centrifugation with 2000 x g for 10 minutes, serum and plasma were retrieved and stored at -20°C until further analysis.
2.2. Measurement of Disease-Related Parameters
As an important aspect of the study was to improve ME/CFS diagnosis and patient health care, we focused on parameters feasible in routine diagnostics. All parameters were obtained from plasma or serum samples and measured by commercially available Enzyme-linked immunosorbent assays (ELISAs). Markers of interest were chosen to determine (1) chronic, low-grade inflammation and immune dysfunction, (2) mucosal barrier disruption and (3) mast cell related disorders. All markers and respective ELISA Kits are listed in the supplementary materials (Table A1). ELISAs were performed according to the respective manufacturer’s protocols. Briefly summarized, 96-well microplates were coated with an antigen-specific capture antibody. After incubation and washing, serum or plasma samples were applied. All used detection antibodies were biotinylated and detected by a streptavidin/horse radish peroxidase conjugate. Tetramethylbenzidine and an acidic stopping solution was used for the colorimetric reaction. Absorbance was measured at 450 nm using ELISA Reader Infinite m200 PRO (Tecan, Männedorf, Switzerland). A four-parameter logistic (4PL) curve was used to analyze antibody concentrations after subtracting levels detected in blank wells as background values.
2.3. Statistical Analyses
Quantitative variables are reported as mean ± standard deviation (SD) if not stated otherwise. All acquired data sets were tested for normal distribution by using the Kolmogorov-Smirnov test. If normally distributed, data sets were compared by one-way ANOVA. The confidence level was adjusted by Tukey’s multiple comparison test and variances were computed for each comparison. If normal distribution was not given, data sets were compared by Kruskal-Wallis test. The confidence level was adjusted by Dunn’s multiple comparisons of all columns and individual variances were computed for each comparison. Multiplicity adjusted P-values <0.05 were considered statistically significant. Data analysis was done by GraphPad Prism 9 software (GraphPad, San Diego, USA).
3. Results
3.1. Evaluation of Pro-Inflammatory Immune Mediators
To detect signs of chronic low-grade inflammation and evaluate respective markers in ME/CFS patients, pro-inflammatory and mucosal barrier integrity related cytokines IFN-gamma, TNF-alpha, IL-6, IL-1-beta, IL-8 and IL-33 were measured in serum samples, as well as complement factor protein C4a and fibroblast growth factor FGF21, which is exported into the circulation by the liver in response to stress. There were no notable statistical variances detected in plasma C4a levels when comparing individuals with ME/CFS to healthy participants (Figure 2A). However, upon stratifying patients based on their immunological status, a noteworthy, statistically significant decrease in plasma C4a concentrations was observed in individuals with ME/CFS and immunodeficiencies (ME/CFS + ID) in contrast to those with ME/CFS but no immunodeficiencies (ME/CFS – ID) and the healthy control group (Figure 2B). A significant reduction in serum IL-1-beta levels was observed when comparing ME/CFS patients without immunodeficiencies to the healthy control group (Figure 3A). Serum IL-33 levels were increased in ME/CFS patients without immunodeficiencies when compared to healthy control participants, but also slightly increased when compared to ME/CFS patients with immunodeficiencies. (Table 2). A similar trend was observed in serum levels of IL-6 as shown in Figure 3B, with a statistically significant difference in the ME/CFS - ID group compared to healthy controls. Evaluation of TNF-alpha, IL-8 and FGF21 serum did not show statistically significant differences between the tested groups as described in Table 2. The data on IFN-gamma level is not shown, as all measured values were below the limit of detection (LOD) stated in the manufacturer’s protocol.

Table 1.
Evaluation of disease-related marker associated with low-grade inflammation, enhanced mast cell activity and mucosal barrier disruption. No parameter showed statistically significant difference between the groups. LOD = Limit of detection.
Table 1.
Evaluation of disease-related marker associated with low-grade inflammation, enhanced mast cell activity and mucosal barrier disruption. No parameter showed statistically significant difference between the groups. LOD = Limit of detection.
| Study Group | ME/CFS + ID | ME/CFS - ID | Healthy |
| Parameter (unit ± SD) | |||
|
TNF-alpha (pg/ml) LOD: 4 pg/ml |
2.76 (± 2.56) | 7.03 (± 9.08) | 3.63 (± 3.68) |
|
IL-8 (pg/ml) LOD: 2 pg/ml |
10.80 (± 7.78) | 10.68 (± 12.63) | 10.37 (± 8.00) |
|
IL-33 (pg/ml) LOD: 0.9 pg/ml |
35.70 (± 48.23) | 52.13 (± 77.37) | 27.77 (± 35.44) |
|
FGF21 (pg/ml) LOD: 7 pg/ml |
170.50 (± 158.90) | 149.70 (± 116.80) | 155.80 (± 90.14) |
|
ECP (ng/ml) LOD: 39 pg/ml |
11.50 (± 2.66) | 12.77 (± 9.31) | 12.34 (± 4.12) |
|
EDN (ng/ml) LOD: 0.63 ng/ml |
50.11 (± 27.60) | 52.29 (± 29.19) | 41.03 (± 17.78) |
|
Endotoxin-Core IgG (MU/ml) LOD: 0.13 MU/ml |
113.10 (± 219.30) | 77.79 (± 79.75) | 75.97 (± 46.80) |
|
sCD14 (µg/ml) LOD: 6 pg/ml |
12.23 (± 2.00) | 11.99 (± 2.20) | 11.39 (± 1.00) |
|
I-FABP (ng/ml) LOD: 25 pg/ml |
7.86 (± 17.51) | 3.90 (± 7.30) | 11.35 (± 20.29) |
3.2. Immune Marker Related to Enhanced Mast-Cell Activity and Eosinophil Activation
As chronic mast cell activation is difficult to determine, due to the acute nature and short half-life of the major mediators tryptase and histamine [33], we aimed to measure serum level of eosinophil cationic protein (ECP) and eosin-derived neurotoxin (EDN). The measurement of ECP did not reveal differences between the test groups of the study cohort. Serum EDN level were more elevated in ME/CFS patients with immunodeficiencies (50.11 ± 27.60 ng/ml) and without immunodeficiencies (52.29 ± 29.19 ng/ml) than in the healthy control group (41.03 ± 17.78 ng/ml, Table 2). Results are not statistically significant.
3.3. Biomarker Associated to Mucosal and Intestinal Barrier Integrity
When comparing ME/CFS patients to the healthy control participants (Figure 4A), there were no statistically significant differences detected in serum Lipopolysaccharide-binding protein (LBP) levels. However, following immunological patient stratification, serum LBP levels were found to be significantly increased in patients without immunodeficiencies (ME/CFS - ID) when compared to the healthy control group (Figure 4B). Soluble CD14 serum level, which is needed as a co-factor together with LBP to mediate innate immunity against LPS to the immune system, did not differ between the test groups (Table 2). Conversely, I-FABP levels were slightly reduced in ME/CFS patients without immunodeficiencies compared to healthy control participants, but results were not significant (Table 2). Endotoxin-core IgG-antibodies were highest in immunodeficient ME/CFS patients (113.10 ± 219.30 MU/ml), while ME/CFS patients without immunodeficiencies had similar Endotoxin-core IgG level like healthy control participants (Table 2), although results are not statistically significant.
4. Discussion
Previous studies on ME/CFS already investigated immunological dysregulation with the potential to trigger inflammatory processes [1,13]. In our research, we focused on investigating the mucosal intestinal barrier to gain a deeper understanding of pathological mechanisms underlying ME/CFS. Our goal was to bridge these two aspects to elucidate the link between mucosal (intestinal) barrier function and immunodeficiencies. We divided the ME/CFS patients into two subgroups based on immunological stratification. Based on our results, we defined 3 key-messages. Our data suggest that the two patient groups exhibit distinct pathophysiological mechanisms and most importantly, we show the importance of immunological stratification prior to down-stream analyses. Our findings should be considered when diagnosing ME/CFS and developing targeted medications to mitigate disease progression and improve patient health care.
It was previously demonstrated that C4a levels in ME/CFS patients were in general lower than in healthy control participants but elevated after exercise challenge and correlating with PEM-associated symptoms [34,35,36]. Interestingly, the rise in C4a levels was not observable one hour after being physically challenged [34,35,36] but only after six hours [36] and returned almost to baseline 24 hours post exercise. This suggests C4a as a potential PEM-associated biomarker and a pathophysiological marker in ME/CFS. Noteworthy, none of the above-mentioned studies examined the immune competence of the ME/CFS patients before study participation. In our study, comparing all ME/CFS patients to healthy control participants showed reduced C4a levels as well, although results were not significant. However, after stratifying ME/CFS patients based on their immune competence we found statistically reduced C4a levels in ME/CFS patients with immunodeficiencies compared to both other test groups (Figure 2). Furthermore, ME/CFS patients without immunodeficiencies showed C4a levels comparable to healthy controls. This demonstrates that not only immunological patient stratification before study inclusion is required when using C4a as marker of interest, but it also indicates a potential dysregulation in the inflammatory processes involving complement system activation. Ten percent of the ME/CFS patients with immunodeficiencies in our study suffered from a complement deficiency. C4a, which serves together with C3a and C5a as an inflammatory anaphylatoxin, plays a crucial role in histamine release from mast cells, increased vascular permeability, chemotaxis, inflammation, smooth muscle cell contraction, and the generation of cytotoxic oxygen radicals [37]. These effects may contribute to the flu-like symptoms frequently associated with PEM.
Elevated levels of the barrier marker LBP indicate mucosal barrier leakage in the ME/CFS patient group without immunodeficiencies (Figure 4B). This marker is associated with bacterial wall components that breach the intestinal barrier and enter the bloodstream [38]. LBP production is dependent on circulating LPS concentrations in the blood, as the body produces more LBP on increased LPS levels. Interestingly, we did not find sCD14 levels to be different within the whole study cohort (Table 2), although it is needed as a co-factor for LBP when mediating innate immunity [38]. In mice, it has been demonstrated that sCD14 presents protective effects in inflammatory bowel disease and that a rise of LBP/sCD14 ratio in both humans and mice is linked to an increase of plasma IL-6 [39]. Thus, it is suggested that LBP and sCD14, as well as the ratio to each other, are important factors in low-grade inflammation during metabolic diseases. In line with these data, the ME/CFS – ID group, which has the highest LBP values, also shows higher level of serum IL-6 (Figure 3B), compared to the other study groups, indicating barrier leakage and low-grade inflammation. Also, our findings regarding IL-1-beta (Figure 3A) and IL-33 levels (Table 2), which are associated with homeostasis of the gut microbiota, support the hypothesis of a mucosal barrier leakage [40,41]. Gut microbiota homeostasis is essential for maintenance and repair of the mucosal epithelial barrier. IL-1-beta production induced by mucosa-associated gut commensal bacteria promotes intestinal barrier repair, thus reduced IL-1beta levels in ME/CFS might promote barrier dysfunction. Increased IL-33, which is a member of the IL-1 cytokine family, points towards a mucosal barrier leakage in ME/CFS patients without immunodeficiencies, as it acts as an alarmin to provide acute initial protection [40]. Interestingly, I-FABP levels, which are found in elevated levels in situations of epithelial damage [42] showed an inversed pattern with the biggest reduction in the ME/CFS – ID group (Table 2). However, it is important to emphasize that intestinal barrier leakage is not necessarily induced by epithelial damage, as the gastrointestinal mucosal tissues also regulates its dynamics via intra- and inter-cellular transportation pathways [43]. With the slightly elevated endotoxin-core antibodies in the ME/CFS + ID group, we hypothesize that ME/CFS patients with immunodeficiencies have suffered an epithelial damage, while ME/CFS patients without immunodeficiencies fail to maintain mucosal barrier function resulting in leakage.
Previous research on ME/CFS has often focused on altered cytokine patterns, mucosal barrier dysfunction, chronic low-grade inflammation and various other mechanisms but the results have been inconsistent. The multi-factorial nature and the still unknown disease trigger hamper research as much as the highly individual symptoms, which also differ depending on the disease severity and co-morbidities of affected patients. To support this observation, we aimed to bridge immunological and mucosal barrier dysfunction as the gut-associated lymphoid tissues represent the largest immune organ in the human body [44]. No major differences were found in most measured parameters when comparing ME/CFS patients with healthy control participants. Minor trends were found in IL-6 (p=0.049), IL-33 (not significant), EDN (not significant) and I-FABP (not significant) levels (Figure 3B and Table 2). However, an examination of larger study cohorts is needed to confirm the observed results. While IL-8, ECP and sCD14 measurements did not reveal major differences between all test groups, an interesting trend was detected when examining the other parameters. If ME/CFS patients are not stratified based on their immune competence, the measured results are averaged out and comparable to the healthy control participants (Table 2). This effect was especially prominent when evaluating the immunological marker C4a (Figure 2A) and the mucosal barrier marker LBP (Figure 4A). Thus, we provide evidence that ME/CFS patient subgroups exhibit different pathophysiological pattern. These distinct patterns represent subgroup-specific characteristics, thus might serve as target points for future diagnostic and treatment approaches. Without precise patient stratification, potential biomarker might lose discrimination power.
As patient recovery is poorly and incoherently documented [45], it is difficult to find common mechanistic pathways. Attempts to define causative treatment approaches have failed so far. From an immunological perspective, promising treatment strategies could be identified in well-characterized ME/CFS subgroups. The gavage of intravenous immunoglobulins shows good results, but the outcome strongly depends on well-stratified responders, as they must show markers of immune dysfunction [46,47]. Also, immunoadsorption to remove ß2-adrenergic receptor antibodies leads to clinical improvement in some cases, but only if the premise is given that patients show elevated ß2 autoantibodies in the first place [48]. The synthetic oligonucleotide aptamer BC-007, which was designed to neutralize antibodies against G-protein coupled receptor (GPCR) and SARS-CoV-2 autoantibodies, is currently under investigation for treatment of post-infectious disease [49,50]. When it comes to the gastrointestinal barrier function, treatment approaches are rather based on case reports and the use of off-label medication. In children with multisystemic inflammatory syndrome (MIS-C), elevated plasma zonulin levels were associated with gastrointestinal permeability after SARS-CoV-2 infection and therefore, suggested to serve as a biomarker [51]. In line, the zonulin antagonist Larazotide (AT1001) might offer potential benefit in treatment of MIS-C patients, by preventing a break-down of tight junctions and subsequent protection of gastrointestinal barrier integrity [52]. Altogether, these findings highlight the importance of well stratified ME/CFS patients in research and medical care. Promising treatment approaches can be defined on subgroup-specific characteristics but might fail if patient subgroups are too heterogenous [53].
5. Conclusion
This research investigates the relationship between immunological abnormalities and mucosal intestinal barrier function in ME/CFS patients. The study stratified ME/CFS patients into two groups based on their immunological status and presented three key findings: Reduced C4a levels in ME/CFS patients with immunodeficiencies suggested a sub-group specific disease pattern impairing innate immunity. It remains elusive if this deficiency contributes to disease onset due to a failure innate immunity in situations of (viral) host defense or is a result of the ongoing disease. ME/CFS patients without immunodeficiency exhibited mucosal barrier leakage, indicated by elevated levels of the marker LBP, potentially contributing to low-grade inflammation. The use of standardized detection methods is needed to rapidly translate research into clinics. This ensures the definition of bench-to-bedside orientated approaches to make evidence-based ME/CFS diagnosis and treatment generally available for patients. Stratifying ME/CFS patients based on their immune competence enabled distinction of ME/CFS patient sub-groups with generally accessible detection methods. This finding further highlights the importance of careful patient stratification when studying ME/CFS, especially in evaluation of novel treatment strategies, as different disease mechanisms might be involved in fatigue and PEM development.
The COVID-19 pandemic clearly demonstrated that viral infections may be of asymptomatic nature. Due to the progressing climate change novel pathogens, like the West Nile virus or tick-borne diseases, which trigger post-infectious conditions, are on the forefront [3,54]. The population of ME/CFS patients will increase and will include more patients, who experience an asymptomatic disease course and are not aware of their infection. The role of immune dysregulation and mucosal barrier disruption as disease mechanisms needs in-depth investigations as they represent promising target point in ME/CFS and post-viral treatment. When considering that in ME/CFS around 25% of patients are bedbound and 75% of patients are unable to work, it is obvious that prolonged fatigue represents an enormous health burden and socioeconomic challenge. ME/CFS is associated with yearly costs of 17-24 billion USD in the United States alone [55], highlighting the enormous impact of the disease. Noteworthy, this information is based on an estimation from 2004. Considering the drastically increasing incidences of post-virally triggered ME/CFS due to SARS-CoV-2 infections, the financial burden for health authorities, as well as individual patients needs to be counteracted as soon as possible.
Author Contributions
Conceptualization: RJ, UE; data curation: RJ, LL, UE; formal analysis: RJ, HL, LL; funding acquisition: UE; investigation: RJ, HL, LL, KL, GSA; methodology: RJ, HL, LL, KL, GSA, RD; project administration: UE; resources: SM, UE; supervision: UE; visualization: RJ, UE; writing (original draft preparation): RJ, UE; writing (review and editing): RJ, HL, LL, LL, KL, GSA, RD, SM, UE. All authors have read and agreed to the published version of the manuscript.
Funding
The study was financially supported by the WE&ME Foundation (former TEMPI - Charitable Foundation for the Support of Patients and Research of Undiagnosed Diseases).
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by Ethics Committee of the Medical University of Vienna (vote number: 1441/2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Further information is available from the corresponding authors upon reasonable request.
Acknowledgments
We like to thank all ME/CFS patients and other participants who made this scientific study possible. Your voices have added a crucial dimension to our research and your valuable insights will pave the way for better diagnosis and treatment.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Appendix A
Table A1.
List of used ELISA Kits.
| Kit | Manufacturer | Cat.-Number |
|---|---|---|
| Human IL-1-beta Uncoated ELSIA | ThermoFisher Scientific, Waltham, USA | 88-7261 |
| Human IL-6 Uncoated ELISA Kit | ThermoFisher Scientific, Waltham, USA | 88-7066 |
| Human TNF-alpha Uncoated ELISA | ThermoFisher Scientific, Waltham, USA | 88-7346 |
| Human IL-8 Uncoated ELISA Kit | ThermoFisher Scientific, Waltham, USA | 88-8086 |
| Human IL-33 ELISA Kit | ThermoFisher Scientific, Waltham, USA | BMS2048 |
| Human IFN-gamma Uncoated ELISA | ThermoFisher Scientific, Waltham, USA | 88-7316 |
| BD OptEIA Human C4a ELISA Kit | BD Biosciences, Franklin Lakes, USA | 550947 |
| Fibroblast Growth Factor 21 Human ELISA | BioVendor, Brno, Czech Republic | RD191108200R |
| Human RNASE3/ECP (Ribonuclease A3/Eosinophil cationic Protein) ELISA Kit | Elabscience, Houston, USA | E-EL-H1379 |
| Human EDN (Eosinophil-Derived Neurotoxin) ELISA Kit | Elabscience, Houston, USA | E-EL-H2341 |
| Human LBP ELISA Kit | ThermoFisher Scientific, Waltham, USA | EH297RB |
| EndoCAb IgG, Human, ELISA Kit | Hycult Biotech, Wayne, USA | HK504-IGG |
| Human CD14 ELISA Kit | ThermoFisher Scientific, Waltham, USA | EHCD14 |
| Human FABP-2 (intestinal) ELISA Kit | ThermoFisher Scientific, Waltham, USA | EHFABP2 |
References
- Lutz, L., et al., Evaluation of Immune Dysregulation in an Austrian Patient Cohort Suffering from Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Biomolecules, 2021. 11(9): p. 1359. [CrossRef]
- Lim, E.J., et al., Systematic review and meta-analysis of the prevalence of chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME). J Transl Med, 2020. 18(1): p. 100. [CrossRef]
- Tschopp, R., et al., Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): A preliminary survey among patients in Switzerland. Heliyon, 2023. 9(5): p. e15595. [CrossRef]
- Ruiz-Pablos, M., et al., Epstein-Barr Virus and the Origin of Myalgic Encephalomyelitis or Chronic Fatigue Syndrome. Frontiers in Immunology, 2021. 12. [CrossRef]
- Komaroff, A.L. and L. Bateman, Will COVID-19 Lead to Myalgic Encephalomyelitis/Chronic Fatigue Syndrome? Frontiers in Medicine, 2021. 7(1132). [CrossRef]
- Altmann, D.M., et al., The immunology of long COVID. Nature Reviews Immunology, 2023. [CrossRef]
- Renz-Polster, H. and C. Scheibenbogen, [Post-COVID syndrome with fatigue and exercise intolerance: myalgic encephalomyelitis/chronic fatigue syndrome]. Inn Med (Heidelb), 2022. 63(8): p. 830-839. [CrossRef]
- Nguyen, T., et al., Novel characterisation of mast cell phenotypes from peripheral blood mononuclear cells in chronic fatigue syndrome/myalgic encephalomyelitis patients. Asian Pac J Allergy Immunol, 2017. 35(2): p. 75-81. [CrossRef]
- Nijs, J., et al., Altered immune response to exercise in patients with chronic fatigue syndrome/myalgic encephalomyelitis: a systematic literature review. Exerc Immunol Rev, 2014. 20: p. 94-116.
- Jonsjö, M.A., et al., The role of low-grade inflammation in ME/CFS (Myalgic Encephalomyelitis/Chronic Fatigue Syndrome) - associations with symptoms. Psychoneuroendocrinology, 2020. 113: p. 104578. [CrossRef]
- Gang, J., et al., Microbiota and COVID-19: Long-term and complex influencing factors. Front Microbiol, 2022. 13: p. 963488. [CrossRef]
- Kedor, C., et al., A prospective observational study of post-COVID-19 chronic fatigue syndrome following the first pandemic wave in Germany and biomarkers associated with symptom severity. Nature Communications, 2022. 13(1): p. 5104. [CrossRef]
- Guenther, S., et al., Frequent IgG subclass and mannose binding lectin deficiency in patients with chronic fatigue syndrome. Hum Immunol, 2015. 76(10): p. 729-35. [CrossRef]
- Jack, D.L., et al., Mannose-binding lectin regulates the inflammatory response of human professional phagocytes to Neisseria meningitidis serogroup B. J Infect Dis, 2001. 184(9): p. 1152-62. [CrossRef]
- Gupta, A. and G.S. Gupta, Status of mannose-binding lectin (MBL) and complement system in COVID-19 patients and therapeutic applications of antiviral plant MBLs. Molecular and Cellular Biochemistry, 2021. 476(8): p. 2917-2942. [CrossRef]
- Ali, Y.M., et al., Lectin Pathway Mediates Complement Activation by SARS-CoV-2 Proteins. Frontiers in Immunology, 2021. 12. [CrossRef]
- Gao, T., et al., Highly pathogenic coronavirus N protein aggravates inflammation by MASP-2-mediated lectin complement pathway overactivation. Signal Transduction and Targeted Therapy, 2022. 7(1): p. 318. [CrossRef]
- Liu, H., et al., Mannan binding lectin attenuates double-stranded RNA-mediated TLR3 activation and innate immunity. FEBS Lett, 2014. 588(6): p. 866-72. [CrossRef]
- Zhou, J., et al., Mannan-Binding Lectin Regulates Inflammatory Cytokine Production, Proliferation, and Cytotoxicity of Human Peripheral Natural Killer Cells. Mediators of Inflammation, 2019. 2019: p. 6738286. [CrossRef]
- Tang, Y., et al., Mannan-binding lectin reduces CpG DNA-induced inflammatory cytokine production by human monocytes. Microbiol Immunol, 2015. 59(4): p. 231-7. [CrossRef]
- Rohrhofer, J., et al., Association between EBV reactivation and development of Long-COVID fatigue. Allergy, 2022. n/a(n/a). [CrossRef]
- König, R.S., et al., The Gut Microbiome in Myalgic Encephalomyelitis (ME)/Chronic Fatigue Syndrome (CFS). Front Immunol, 2021. 12: p. 628741. [CrossRef]
- Wirth, K.J. and M. Löhn, Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and Comorbidities: Linked by Vascular Pathomechanisms and Vasoactive Mediators? Medicina (Kaunas), 2023. 59(5). [CrossRef]
- Zollner, A., et al., Postacute COVID-19 is Characterized by Gut Viral Antigen Persistence in Inflammatory Bowel Diseases. Gastroenterology, 2022. 163(2): p. 495-506.e8. [CrossRef]
- Sencio, V., et al., Influenza Virus Infection Impairs the Gut's Barrier Properties and Favors Secondary Enteric Bacterial Infection through Reduced Production of Short-Chain Fatty Acids. Infect Immun, 2021. 89(9): p. e0073420. [CrossRef]
- Tugizov, S., Virus-associated disruption of mucosal epithelial tight junctions and its role in viral transmission and spread. Tissue Barriers, 2021. 9(4): p. 1943274. [CrossRef]
- Kim, D.Y., et al., Systematic review of randomized controlled trials for chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME). J Transl Med, 2020. 18(1): p. 7. [CrossRef]
- Fluge, Ø., et al., B-Lymphocyte Depletion in Myalgic Encephalopathy/ Chronic Fatigue Syndrome. An Open-Label Phase II Study with Rituximab Maintenance Treatment. PLoS One, 2015. 10(7): p. e0129898. [CrossRef]
- Fluge, Ø., et al., B-Lymphocyte Depletion in Patients With Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. Ann Intern Med, 2019. 170(9): p. 585-593. [CrossRef]
- Goudsmit, E.M., et al., Pacing as a strategy to improve energy management in myalgic encephalomyelitis/chronic fatigue syndrome: a consensus document. Disabil Rehabil, 2012. 34(13): p. 1140-7. [CrossRef]
- Rowe, K., Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (CFS/ME) in Adolescents: Practical Guidance and Management Challenges. Adolesc Health Med Ther, 2023. 14: p. 13-26. [CrossRef]
- Committee on the Diagnostic Criteria for Myalgic Encephalomyelitis/Chronic Fatigue, S., P. Board on the Health of Select, and M. Institute of, The National Academies Collection: Reports funded by National Institutes of Health, in Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. 2015, National Academies Press (US).
- Copyright 2015 by the National Academy of Sciences. All rights reserved.: Washington (DC).
- Galvan-Blasco, P., J. Gil-Serrano, and A. Sala-Cunill, New Biomarkers in Anaphylaxis (Beyond Tryptase). Curr Treat Options Allergy, 2022. 9(4): p. 303-322. [CrossRef]
- Nijs, J., et al., Unravelling the nature of postexertional malaise in myalgic encephalomyelitis/chronic fatigue syndrome: the role of elastase, complement C4a and interleukin-1β. Journal of Internal Medicine, 2010. 267(4): p. 418-435. [CrossRef]
- Polli, A., et al., Exercise-induce hyperalgesia, complement system and elastase activation in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome - a secondary analysis of experimental comparative studies. Scand J Pain, 2019. 19(1): p. 183-192. [CrossRef]
- Sorensen, B., et al., Complement activation in a model of chronic fatigue syndrome. J Allergy Clin Immunol, 2003. 112(2): p. 397-403. [CrossRef]
- Wang, H. and M. Liu, Complement C4, Infections, and Autoimmune Diseases. Frontiers in Immunology, 2021. 12. [CrossRef]
- Kitchens, R.L. and P.A. Thompson, Modulatory effects of sCD14 and LBP on LPS-host cell interactions. J Endotoxin Res, 2005. 11(4): p. 225-9. [CrossRef]
- Laugerette, F., et al., Postprandial Endotoxin Transporters LBP and sCD14 Differ in Obese vs. Overweight and Normal Weight Men during Fat-Rich Meal Digestion. Nutrients, 2020. 12(6). [CrossRef]
- Hodzic, Z., et al., IL-33 and the intestine: The good, the bad, and the inflammatory. Cytokine, 2017. 100: p. 1-10. [CrossRef]
- Wu, W.H., et al., Interleukin-1β secretion induced by mucosa-associated gut commensal bacteria promotes intestinal barrier repair. Gut Microbes, 2022. 14(1): p. 2014772. [CrossRef]
- Lau, E., et al., The role of I-FABP as a biomarker of intestinal barrier dysfunction driven by gut microbiota changes in obesity. Nutr Metab (Lond), 2016. 13: p. 31. [CrossRef]
- Chelakkot, C., J. Ghim, and S.H. Ryu, Mechanisms regulating intestinal barrier integrity and its pathological implications. Experimental & Molecular Medicine, 2018. 50(8): p. 1-9. [CrossRef]
- Chakaroun, R.M., L. Massier, and P. Kovacs, Gut Microbiome, Intestinal Permeability, and Tissue Bacteria in Metabolic Disease: Perpetrators or Bystanders? Nutrients, 2020. 12(4): p. 1082. [CrossRef]
- Adamowicz, J.L., I. Caikauskaite, and F. Friedberg, Defining recovery in chronic fatigue syndrome: a critical review. Qual Life Res, 2014. 23(9): p. 2407-16. [CrossRef]
- Rowe, K.S., Double-blind randomized controlled trial to assess the efficacy of intravenous gammaglobulin for the management of chronic fatigue syndrome in adolescents. J Psychiatr Res, 1997. 31(1): p. 133-47. [CrossRef]
- Brownlie, H. and N. Speight, Back to the Future? Immunoglobulin Therapy for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Healthcare (Basel), 2021. 9(11). [CrossRef]
- Scheibenbogen, C., et al., Immunoadsorption to remove ß2 adrenergic receptor antibodies in Chronic Fatigue Syndrome CFS/ME. PLOS ONE, 2018. 13(3): p. e0193672. [CrossRef]
- Haberland, A., et al., Aptamer BC 007's Affinity to Specific and Less-Specific Anti-SARS-CoV-2 Neutralizing Antibodies. Viruses, 2021. 13(5). [CrossRef]
- Haberland, A., et al., Aptamer BC 007 - A broad spectrum neutralizer of pathogenic autoantibodies against G-protein-coupled receptors. Eur J Pharmacol, 2016. 789: p. 37-45. [CrossRef]
- Hensley-McBain, T. and J.A. Manuzak, Zonulin as a biomarker and potential therapeutic target in multisystem inflammatory syndrome in children. J Clin Invest, 2021. 131(14). [CrossRef]
- Yonker, L.M., et al., Zonulin Antagonist, Larazotide (AT1001), As an Adjuvant Treatment for Multisystem Inflammatory Syndrome in Children: A Case Series. Crit Care Explor, 2022. 10(2): p. e0641. [CrossRef]
- Scheibenbogen, C., et al., Fighting Post-COVID and ME/CFS - development of curative therapies. Front Med (Lausanne), 2023. 10: p. 1194754. [CrossRef]
- Fulton, C.D.M., et al., Long-term, West Nile virus-induced neurological changes: A comparison of patients and rodent models. Brain Behav Immun Health, 2020. 7: p. 100105. [CrossRef]
- Reynolds, K.J., et al., The economic impact of chronic fatigue syndrome. Cost effectiveness and resource allocation : C/E, 2004. 2(1): p. 4-4. [CrossRef]
Figure 1.
Patient stratification based on immunological parameters. The information on immunodeficiencies of patients was obtained during medical examinations of already diagnosed ME/CFS patients prior to study participation. All patients were recruited in the doctor’s office of Assoc.-Prof. Eva Untersmayr, MD, PhD.
Figure 1.
Patient stratification based on immunological parameters. The information on immunodeficiencies of patients was obtained during medical examinations of already diagnosed ME/CFS patients prior to study participation. All patients were recruited in the doctor’s office of Assoc.-Prof. Eva Untersmayr, MD, PhD.
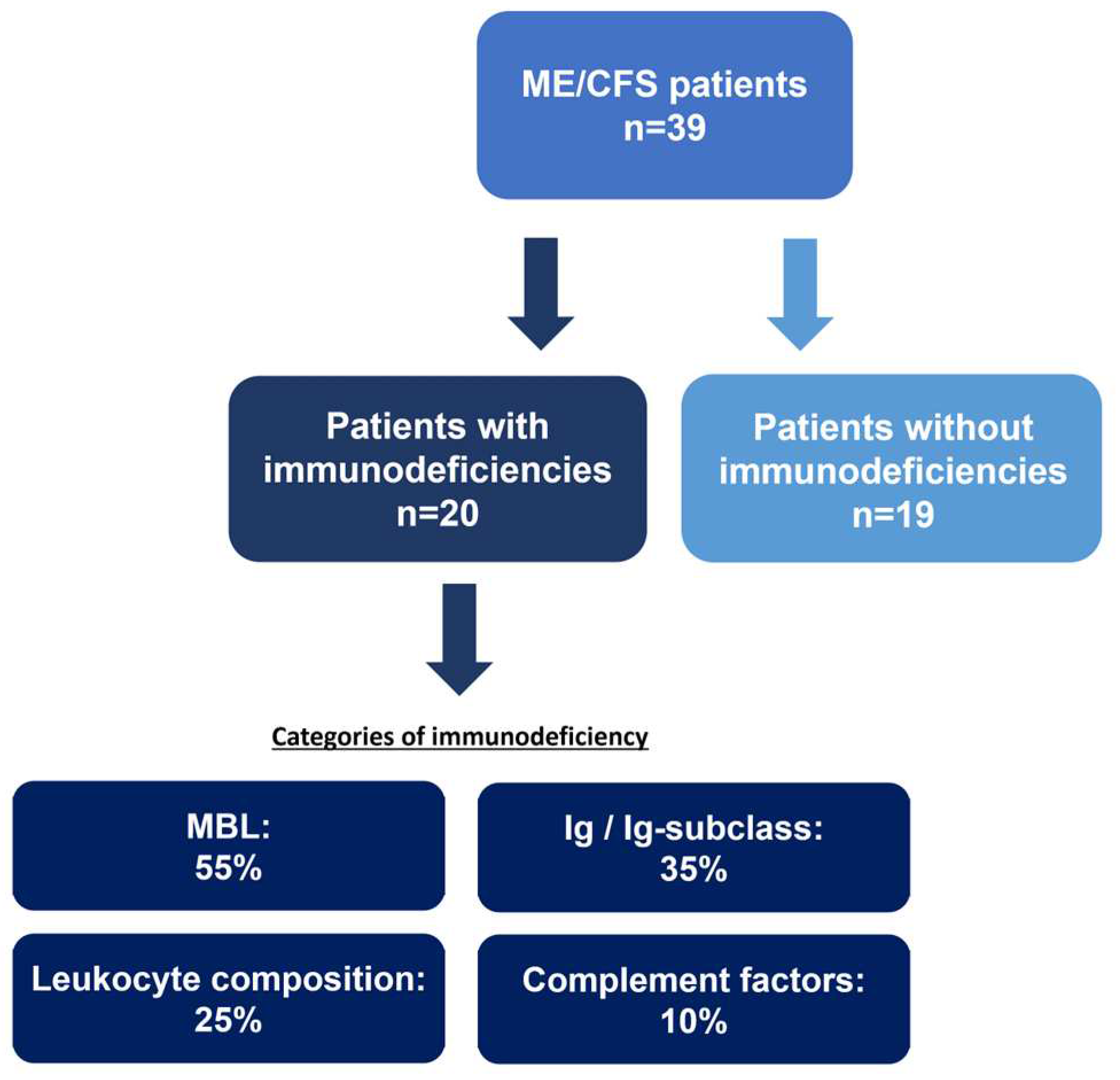
Figure 2.
(A) No statistically significant differences in plasma C4a level were found comparing ME/CFS patients with healthy controls. (B) After immunological patient stratification, concentrations of plasma C4a samples are significantly reduced in patients with immunodeficiencies (ME/CFS + ID) compared to patients without immunodeficiencies (ME/CFS – ID) and healthy control participants. LOD: 6 pg/ml; * p<0.05. * *p<0.01.
Figure 2.
(A) No statistically significant differences in plasma C4a level were found comparing ME/CFS patients with healthy controls. (B) After immunological patient stratification, concentrations of plasma C4a samples are significantly reduced in patients with immunodeficiencies (ME/CFS + ID) compared to patients without immunodeficiencies (ME/CFS – ID) and healthy control participants. LOD: 6 pg/ml; * p<0.05. * *p<0.01.
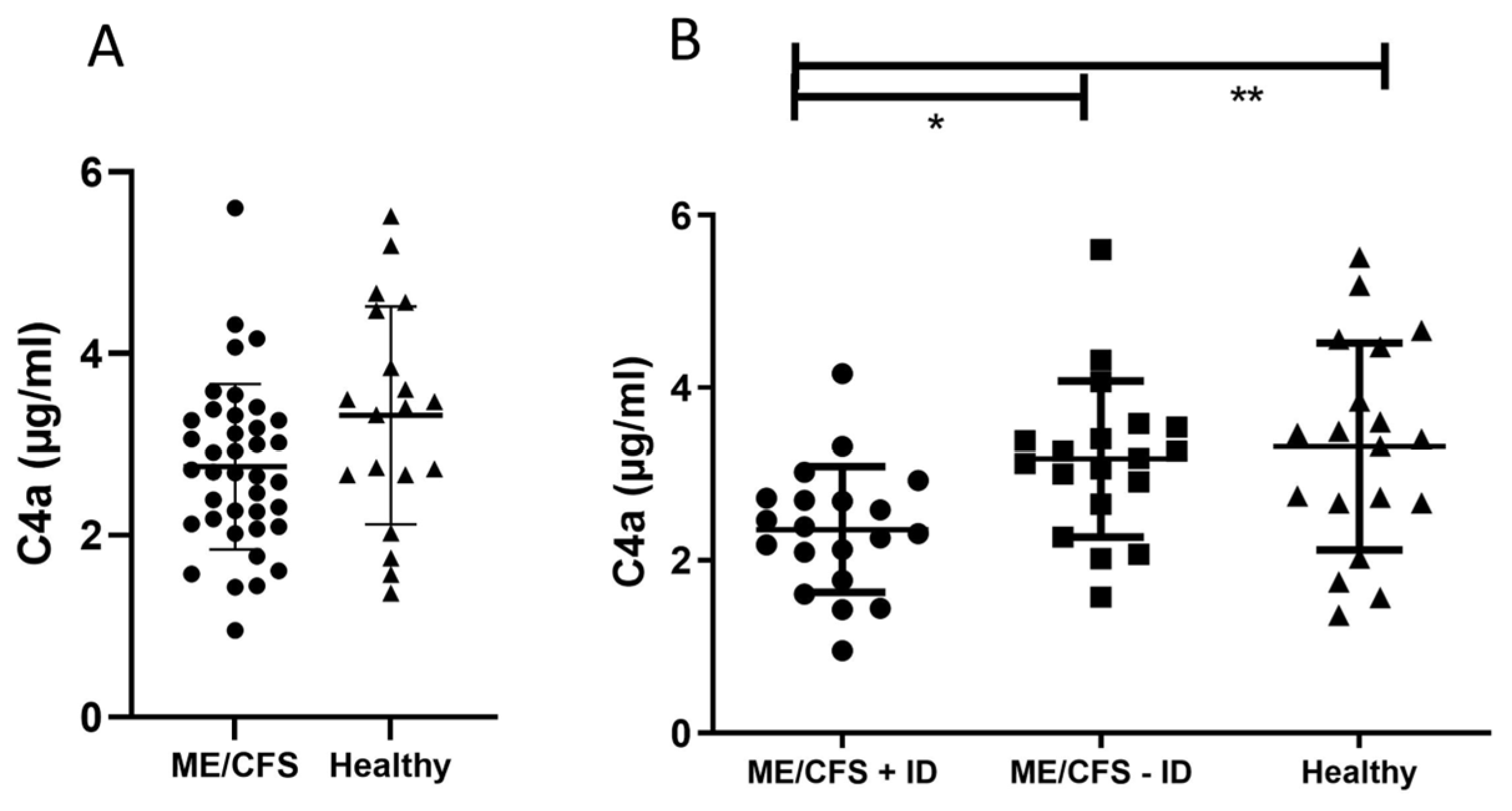
Figure 3.
(A) Significantly reduced serum IL-1-beta level were found when comparing of ME/CFS patients without immunodeficiencies to healthy control participants. (B) Serum IL-6 level were significantly elevated in ME/CFS patients without immunodeficiencies compared to healthy control participants. LOD: 2 pg/ml; * p<0.05.
Figure 3.
(A) Significantly reduced serum IL-1-beta level were found when comparing of ME/CFS patients without immunodeficiencies to healthy control participants. (B) Serum IL-6 level were significantly elevated in ME/CFS patients without immunodeficiencies compared to healthy control participants. LOD: 2 pg/ml; * p<0.05.
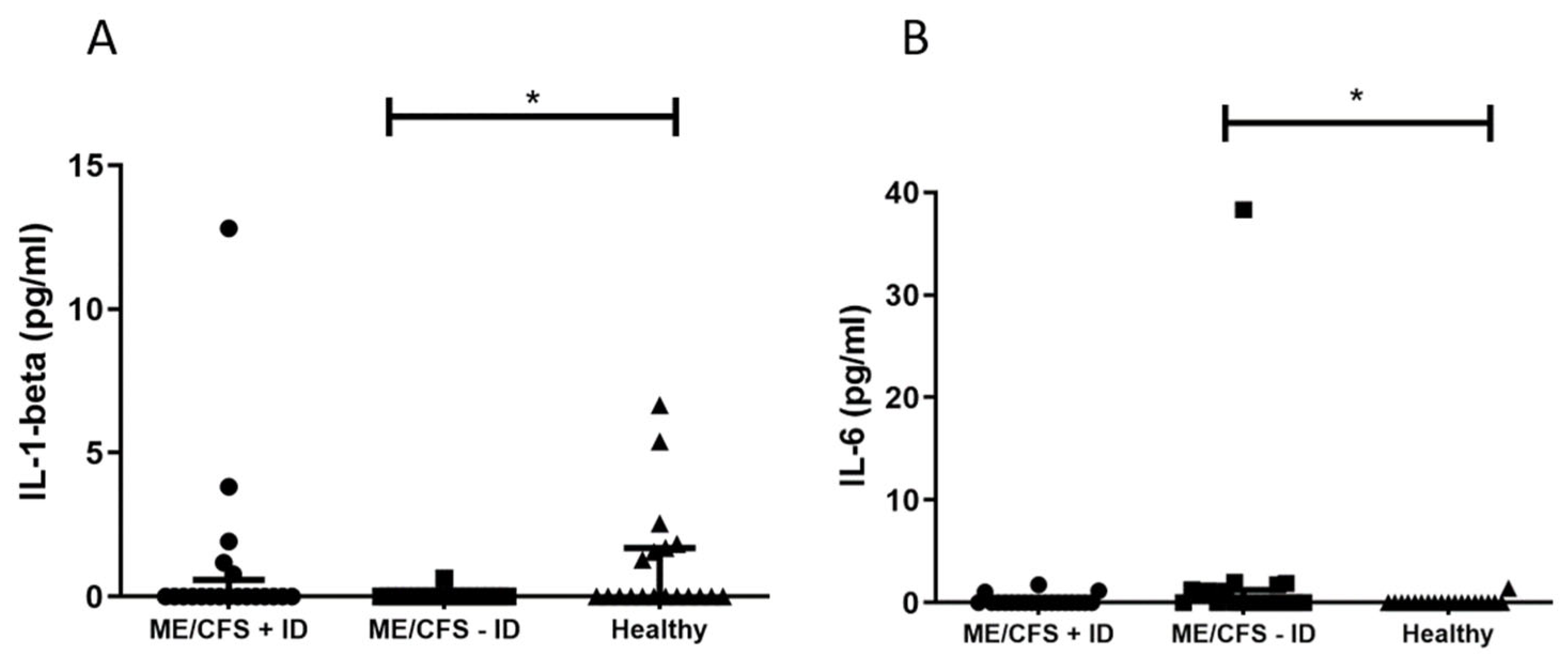
Figure 4.
(A) When comparing ME/CFS patients to healthy control participants no statistically significant differences in serum LBP level were found. (B) Only after immunological patient stratification, serum LBP level are significantly elevated in patients without immunodeficiencies (ME/CFS - ID) compared to healthy control participants. LOD: 0.82 ng/ml; * p<0.05.
Figure 4.
(A) When comparing ME/CFS patients to healthy control participants no statistically significant differences in serum LBP level were found. (B) Only after immunological patient stratification, serum LBP level are significantly elevated in patients without immunodeficiencies (ME/CFS - ID) compared to healthy control participants. LOD: 0.82 ng/ml; * p<0.05.
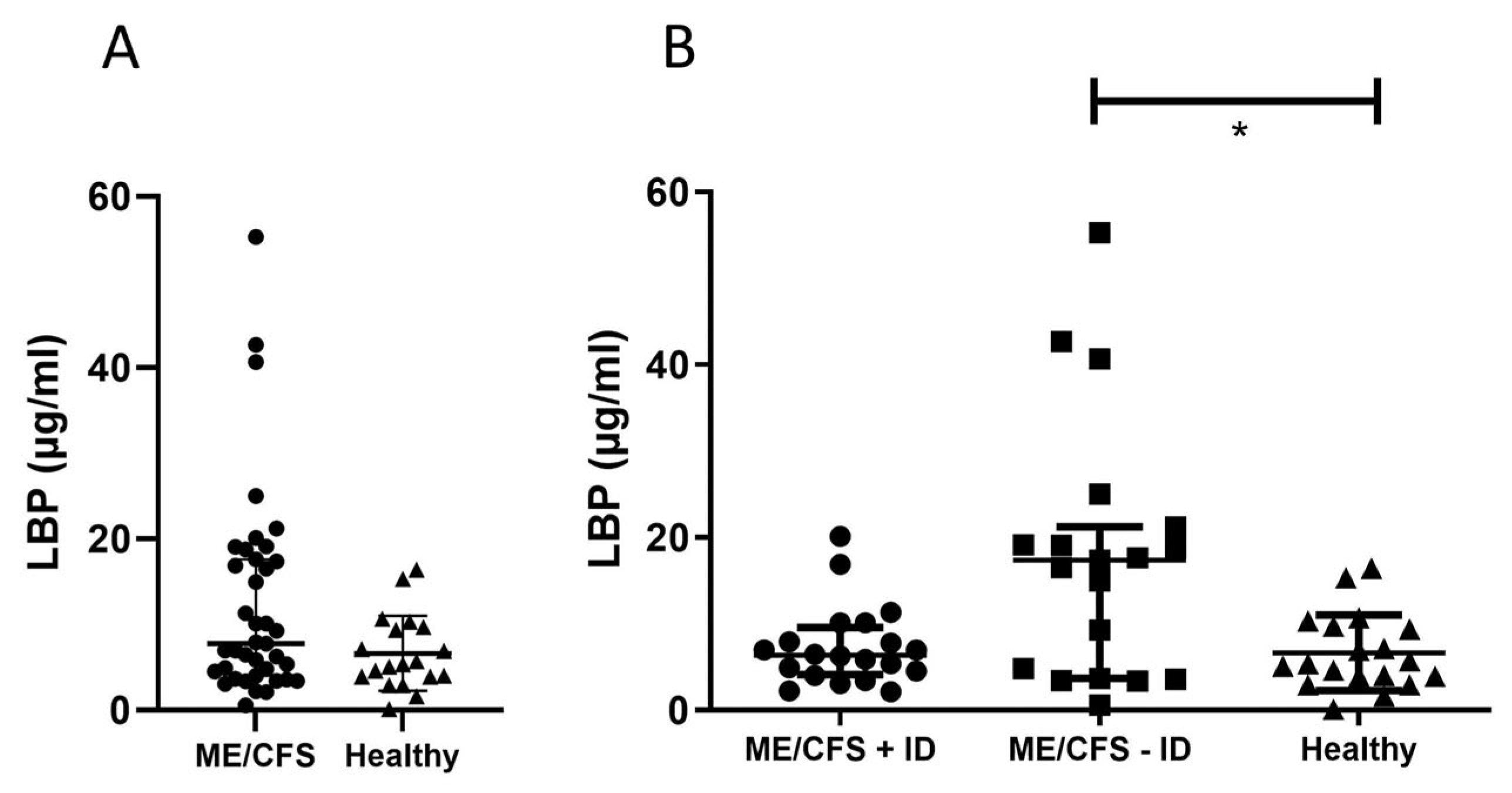
Table 1.
Demographics and in-/exclusion criteria of the study cohort. * ME/CFS was diagnosed based on the IOM criteria (Committee on the Diagnostic Criteria for Myalgic Encephalomyelitis/Chronic Fatigue, Board on the Health of Select et al. 2015) and includes a profound and debilitating fatigue, PEM, unrefreshing sleep and at least one of the two following manifestations: cognitive impairment and/or orthostatic intolerance.
Table 1.
Demographics and in-/exclusion criteria of the study cohort. * ME/CFS was diagnosed based on the IOM criteria (Committee on the Diagnostic Criteria for Myalgic Encephalomyelitis/Chronic Fatigue, Board on the Health of Select et al. 2015) and includes a profound and debilitating fatigue, PEM, unrefreshing sleep and at least one of the two following manifestations: cognitive impairment and/or orthostatic intolerance.
| Study Group | ME/CFS + ID | ME/CFS - ID | Healthy |
| Demographic Data | |||
| Mean age in years (± SD) | 41.2 (± 12.6) | 38.4 (± 10.8) | 43.1 (± 13.0) |
| Female sex in percentage (n) | 75 (15) | 84.2 (16) | 73.7 (14) |
| Inclusion criteria | |||
| Immunodeficiency (ID) | yes | no | no |
| ME/CFS (IOM criteria)* | yes | yes | no |
| Exclusion criteria | |||
| Neurological/psychiatric co-morbidities | no | no | yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



