
Submitted:
30 November 2023
Posted:
01 December 2023
You are already at the latest version
Abstract
In colorectal cancer (CRC) patients, apart from fatigue, psychological and physical symptoms often converge, affecting their quality of life and ability to work. Our objective was to ascertain symptom clusters within a year following CRC treatment and their longitudinal association with persistent fatigue and reduced work ability at the 3-month follow-up. We used data from MIRANDA, a multicenter cohort study enrolling adult CRC patients who are starting a 3-week in-patient rehabilitation within a year post-curative CRC treatment. Participants completed questionnaires evaluating symptoms at the start of rehabilitation (baseline) and after three months. We performed an exploratory factor analysis to analyze the clustering of symptoms at baseline. Longitudinal analysis was performed using a multivariable linear regression model with dichotomized symptoms at baseline as independent variables, and the change of fatigue and ability to work from baseline to 3-month-follow-up as separate outcomes, adjusted for covariates. We identified six symptom clusters: fatigue, gastrointestinal symptoms, pain, psychosocial symptoms, urinary symptoms, and chemotherapy side effects. At least one symptom from each factor was associated with higher fatigue or reduced ability to work at the 3-month follow-up. This study highlights the interplay of multiple symptoms in influencing fatigue and work ability among CRC patients post rehabilitation.
Keywords:
colorectal cancer
; rehabilitation
; fatigue
; ability to work
; symptom clusters
1. Introduction
Cancer-related fatigue is a pervasive and debilitating symptom experienced by many colorectal cancer (CRC) patients, which can persist for months or even years after primary cancer therapy [1]. Besides fatigue, CRC survivors also commonly report other symptoms, such as depression, anxiety, pain, sleep disturbance, digestive tract symptoms, and sexual dysfunction [2,3,4]. These symptoms stem from the physical and psychological sequelae of CRC and its treatments.
Chemotherapy is one of the vital treatment components in stage II or III CRC patients. However, the inherent nature of chemotherapy results in not only the destruction of cancer cells but also the damage to healthy cells, leading to various adverse effects [5]. CRC patients undergoing chemotherapy experience adverse effects that impact their physical health, overall quality of life [4,5,6], and emotional state [6]. A study from Australia examining the adverse effects of chemotherapy in routine care found that CRC patients had the highest prevalence of fatigue (88%), with 89% of CRC patients having at least one adverse effect [7].
Radiotherapy has become an integral part of managing rectal cancer, contributing to a significant reduction in the rate of local recurrences when paired with total mesorectal excision surgery in stage II and III CRC patients [8]. Notably, neoadjuvant radiotherapy, administered before surgery, has been associated with lower local recurrence rates and fewer toxic effects than adjuvant therapy given after the operation [9]. While radiotherapy is an effective treatment strategy for rectal cancer, it is not without potential side effects due to the impact on surrounding organs. Locally, patients may experience diarrhea, frequent urination, gas and bloating, cramping, skin irritation, and constipation [10]. In addition, systemic side effects like fatigue and loss of appetite might significantly impact the patient’s well-being [11].
Previous studies have reported that multiple symptoms cluster together in CRC survivors, suggesting that these symptoms may be interconnected and share underlying mechanisms [12]. For example, one study identified four distinctive symptom clusters (psychological, digestive and urinary, low energy, and pain) in CRC patients during the first year after surgery [13]. Functional status and quality of life are often significantly impaired among CRC survivors who experience these adverse symptoms simultaneously [14,15]. Therefore, modifying the traditional single-symptom approach and addressing symptom clusters when treating CRC patients might be beneficial.
Return to work of cancer patients is an essential milestone in rehabilitation after primary treatment. Patients who return to work report regaining a sense of normalcy and purpose, which is closely linked to the ability to provide for oneself and economic independence [16,17]. However, only 57% of cancer patients have been reported to return to work after treatment [18]. The symptoms of primary disease and adverse effects stemming from associated treatments often form significant barriers to resuming professional activities. Fatigue and depression can cause decreased productivity, while physical symptoms lead to lower employment rates [19]. Therefore, the challenges do not solely arise from the cancer diagnosis but are also intricately related to the treatment side effects, further complicating the patient’s ability to reintegrate into the pre-diagnosis work environment.
As fatigue commonly co-occurs with various adverse effects of CRC treatment, it is crucial to investigate the association between adverse symptoms and persistent cancer-related fatigue and low ability to work with a longitudinal study design. With a better understanding of the temporal relationship, it can be better estimated whether such adverse symptoms are causally related to fatigue and ability to work or are simply bystanders of the associations of CRC treatments and fatigue.
The first aim of this study was to determine whether there are clusters of symptoms in CRC patients undergoing in-patient rehabilitation. The investigated symptoms include psychological, physical, and fatigue-related symptoms and issues impacting daily life and social interactions. The second aim was to explore which of these symptoms are also associated with changes in fatigue and the ability to work in the first three months after rehabilitation.
2. Materials and Methods
2.1. Study design and participants
The MIRANDA study is a multicentric, prospective cohort study with the aim to investigate risk, preventive, and prognostic factors of fatigue, QoL, ability to work, and other health-related outcomes among CRC patients during and after in-patient rehabilitation [20]. Participants are recruited in 6 rehabilitation clinics located in different regions in Germany to ensure a representative sample of the German rehabilitation setting. Besides an age of 18 years and older, the inclusion criteria for the MIRANDA study were CRC diagnosis, CRC therapy (surgery, radiation, and/or chemotherapy) in last 12 months and sufficient knowledge of the German language. No written informed consent was the only exclusion criterion. Recruitment started in September 2020 and will last at least until January 2025, with the aim to recruit approximately 1000 participants.
At baseline (first week during in-patient rehabilitation), the participants fill out a questionnaire and provide blood and stool samples. The participants are asked to complete a self-administered follow-up questionnaire every three months in the first year, and after 3, 5, 7, and 10 years.
MIRANDA study participants with 25-hydroxyvitamin D levels < 60 nmol/L and no contraindication for vitamin D supplementation are invited to take part in the “Personalized Vitamin D supplementation for reducing or preventing fatigue and enhancing the quality of life of patients with colorectal tumor – randomized intervention trial “(VICTORIA) [21]. Approximately half of the MIRANDA participants also participate in the VICTORIA trial and are randomly assigned to receive either vitamin D3 or a placebo for 12 weeks.
2.2. Study measurements
2.2.1. Demographic, lifestyle and clinical data
Sociodemographic, lifestyle, and clinical data were collected from the participant’s baseline questionnaires. Sociodemographic data include sex, age, and lifestyle data physical activity levels, smoking status, and the body mass index (BMI). Clinical data encompass the stage of disease, mode of treatment (surgery, chemotherapy, or radiotherapy), months since CRC surgery, and the number of comorbidities. All of the sociodemographic, lifestyle, and clinical data are self-reported, apart from weight and height, which were measured at baseline and cancer stage, which was physician-reported.
2.2.2. Symptom scales
Fatigue and the ability to work were estimated using the Functional Assessment of Chronic Illness Therapy – Fatigue – Fatigue Scale (FACIT-F-FS) score and the FACIT-F- Functional Well-Being – Ability to Work (FACIT-F-FWB-AW) item, respectively [22]. FACIT-F-FS is scaled from 0 to 52, with a higher score denoting less fatigue. Cancer-related fatigue was defined as having a score of less than 34 on the FACIT-F-FS, previously established as clinically relevant fatigue [23]. FACIT-F-FWB-AW item is scored from 1 to 5, with a higher score denoting better ability to work. A low-to-moderate ability to work was defined by the response categories “Not at all” and “A little bit” to the FACIT-F-FWB-AW item (“I am able to work, including work at home”) (score ≤ 2 points) [20].
Pain, fatigue, nausea/vomiting, dyspnea, insomnia, appetite loss, constipation, financial difficulties, and diarrhea were ascertained using the European Organization for the Research and Treatment of Cancer – Quality of Life Questionnaire – Core 30 (EORTC-QLQ-C30) symptoms scale [24]. Symptoms are scaled from 0 to 100, with a higher score indicating greater symptom presence. The following cut-off values were used to define a clinically significant symptom presence: fatigue > 39 points, pain > 25 points, nausea/vomiting > 8 points, insomnia > 50 points, dyspnea > 17 points, appetite loss > 50 points, constipation > 50 points, diarrhea > 17 points and financial difficulties > 17 points [24].
Urinary frequency, blood and mucus in stool, stool frequency, urinary incontinence, dysuria, abdominal pain, buttock pain, bloating, dry mouth, hair loss, taste, flatulence, fecal incontinence, sore skin, embarrassment, and impotence/dyspareunia were assessed using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Colorectal Cancer Module (EORTC QLQ-CR29) [25]. Each symptom was rated how often it appeared during the previous week, ranging from 1 (not at all) to 4 (very much), and transformed into a linear scale from 0 to 100. For the current study, the EORTC QLQ-CR29 symptoms were dichotomized into none or a little bit (answer category 1 or 2) versus moderate and a lot (answer category 3 or 4). For those symptoms where the number of participants in the second category was below 20%, the answer category a little bit was merged with the moderate and a lot categories.
Physical fatigue, emotional fatigue, cognitive fatigue, interference with daily life, and social sequelae were assessed using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire - Fatigue Module 12 (EORTC QLQ-FA12) questionnaire [26]. In order to determine the cut-off values for the EORTC QLQ-FA12 subscales, the General Fatigue Index was calculated using physical, emotional, and cognitive fatigue scales, ranging from 0 to 30 points, with ≥12 points denoting fatigue levels that require clinical assistance [27]. Given that the prevalence of clinically relevant fatigue was close to 50% (57% using the FACIT-F-FS scale and 53% using the Global Fatigue Index), we used the median (50 points) as a cut-off value for the EORTC-QLQ-FA12 subscales.
Psychosocial distress was estimated using the Questionnaire on Stress in Cancer Patients (QSC-R10). The QSC-R10 uses a five-point Likert scale ranging from 0 (not at all) to 4 (very much) to assess the frequency and intensity of distress experienced by cancer patients. The total score ranges from 0 to 40, with higher scores indicating higher levels of distress. A cut-off score of >14 points has been established to determine the need for psychosocial support [28].
2.3. Statistical analysis
Participants who completed their baseline questionnaires between 09/2020 and 10/2023 were included in the analyses. For the longitudinal analyses, a subset of participants who have completed 3-month follow-up was selected.
Descriptive statistical measures were used to characterize the baseline characteristics of the participants and their fatigue and ability to work at baseline and 3-month follow-up. Pearson’s chi-squared test was used to compare the participants who completed the 3-month follow-up, those who did not respond, and those who were recruited late.
Symptom clusters were identified through exploratory factor analysis. All symptom scales from the validated FACIT-F-FS, FACIT-F-FWB-AW, EORCT-QLQ-C30, EORTC QLQ-CR29, EORTC-QLQ-FA12, and QSC-R10 were used as defined in chapter 2.2.2 with only few exceptions. Impotence/dyspareunia and stoma care were not included due to a high number of participants who preferred not to answer this question. Fatigue from the EORCT-QLQ-C30 and physical fatigue from the EORCT-QLQ-FA12 were excluded due to high correlation with the FACIT-F-FS fatigue item (r = -0.86 and r = -0.86, respectively). The final number of symptoms included in the exploratory factor analysis was 32. The Kaiser-Meyer-Olkin measure was employed to assess the dataset’s suitability for factor analysis. Oblique rotation with the promax option was applied to simplify the factor structure. The final number of factors was determined using the Minimum Average Partial and Parallel Analysis methods.
The longitudinal analysis was performed with a multiple linear regression model. Assumptions of multiple linear regression (linearity, independence, multicollinearity, homoscedasticity) were tested prior the analysis and were met for all analyses [29]. Symptoms that exhibited factor loadings above 0.3 in the exploratory factor analysis were dichotomized and selected as independent variables. Longitudinal changes in fatigue (defined as FACIT-F-FS 3-month follow-up scale subtracted by its baseline value) and ability to work (defined as FACIT-F-FWB-AW score at the 3-month follow-up subtracted by its baseline value) were used as dependent variables. The regression models for these two outcomes were adjusted for baseline FACIT-F-FS and FACIT-F-FWB-AW scales, respectively. Furthermore, all models were adjusted for age, sex, CRC stage, months since CRC surgery, chemotherapy and/or radiotherapy in the last 12 months, BMI, baseline smoking status, physical activity before surgery, and number of comorbidities. In subgroup analysis, analyses were stratified by sex, age groups (<65 years/ ≥65 years), and additional participation in the VICTORIA trial to corroborate if this potentially impacted the results.
To impute missing values of covariates at baseline, multiple imputation by the Markov Chain Monte Carlo method was applied. Twenty-five data sets were imputed separately with the SAS procedure PROC MI. To our knowledge, missing values of other covariates are missing at random. All longitudinal analyses were performed in the 25 imputed data sets, and results were combined by the SAS procedure PROC MIANALYZE. The covariate matrix for the exploratory factor analysis was imputed using the “mifa” package in R [30].
All analyses were done using SAS software version 9.4, except for the exploratory factor analysis performed in R, version 4.2.3 (package “psych). A two-sided significance level of p < 0.05 was used for all tests.
3. Results
3.1. Baseline characteristics
In total, 394 participants filled out the baseline questionnaire, of whom 279 returned a 3-month follow-up questionnaire. Among the non-responders, 64 were recruited in the last 3 months and did not have a chance to respond yet. By not counting these study participants results in a response rate at the 3-month follow-up of 84.5%. When comparing the participants who completed the 3-month follow-up questionnaire to those who were later recruited and those who did not respond by age, sex, and cancer stage, no significant differences were found (Suppl. Table S1).
The mean age of the study participants was 63 years, and 57.9% were male (Table 1). While the CRC stages I-III were approximately equally distributed (31.2%, 32%, and 26.4%, respectively), only 6.1% of participants had stage IV disease. Almost all participants had surgery (99.2%), 46.1% had chemotherapy and 20.9% had radiotherapy. Start of rehabilitation was most frequently initiated up to 1 month after CRC surgery (42.3%) and only a few participants have had their surgery more than 1 year ago (3.9%). The latter are CRC patients who needed rehabilitation after a recurrence of the cancer and its treatment.
The majority of study participants had overweight or obesity (59.1%; BMI ≥ 25 kg/m²) and was not engaged in a healthy level of physical activity prior to the CRC diagnosis (52.5%) and had 2 or more comorbidities (53.2%). Hypertension (52.7%) and diabetes mellitus (17.3%) were common whereas few participants had a history of myocardial infarction or stroke (< 4% each). Furthermore, 14.2% of study participants were current smokers.
Almost half of the participants were fully employed (48.7%) prior CRC treatment. More than one-third were in retirement (38.9%), while the rest were either part-time employed (9.3%) or unemployed (3.1%).
3.2. Symptom clusters
Symptom clusters were identified using exploratory factor analysis. The total number of items included in the analysis was 32. The Keyser-Meier-Olkin measure of sampling adequacy was 0.87. The Minimum Average Partial test suggested three factors as the optimal solution, while the Parallel Analysis suggested six factors. Using the criteria above, solutions with three, four, five, and six factors were explored. The six-factor solution was chosen because it explained the biggest proportion of the variance and had a clear conceptual structure. Apart from dry mouth, all symptoms had at least one factor loading greater than 0.30.
Factor 1 included fatigue, interference with daily life, emotional fatigue, depression, cognitive fatigue, dyspnea, social functioning, ability to work, and appetite loss. Factor 2 included fecal incontinence, stool frequency, sore skin, embarrassment, diarrhea, flatulence, and blood/mucus in stool. Factor 3 included pain, abdominal pain, buttock pain, bloating, and dysuria. Factor 4 included psychosocial stress, anxiety, and financial difficulties. Factor 5 included urinary frequency, urinary incontinence, and sleep disturbance. Factor 6 included taste alteration, hair loss, nausea or vomiting, and constipation. Upon examining the items loaded on each factor, we have named factors 1 to 6 as fatigue factor, gastrointestinal symptoms factor, pain factor, psychosocial symptoms factor, urinary symptoms factor, and chemotherapy side-effects factor, respectively. Factor loadings, eigenvalues, and explained variance can be found in Table 2. Since the oblique rotation was used, factors are correlated with each other (Suppl. Table S2). However, the correlations between factors are low to moderate, with the highest correlation between the fatigue factor and urinary symptoms factor (r = 0.56).
3.3. Longitudinal analyses
3.3.1. Longitudinal association of baseline symptoms with fatigue
150 (54%) study participants had clinical fatigue (FACIT-F-FS < 34 points) at baseline and n= 82 (29.3%) at 3-month follow-up. The median FACIT-F-FS increased from 31 points (interquartile range (IQR): 22 - 42) to 40 points (IQR: 29-47) in this time, which translates to less fatigue. On average, the mean FACIT-F-FS improved by 5.9 points (standard deviation (SD): 9.7 points). The distribution of this change in FACIT-F-FS points was approximately normally distributed (Figure 1).
The results of the multivariable linear regression analysis evaluating the association between covariates and the change of fatigue from baseline to 3-months follow-up are displayed in Suppl. Table S3. Having received chemotherapy or radiotherapy within one year before rehabilitation was the factor with the highest reduction in fatigue with a β coefficient (95% CI) of 4.71 (1.93; 7.48).
The association between baseline symptoms and the change in fatigue until the 3-month follow-up are displayed in Figure 2. In total, 14 out of 30 symptoms were significantly associated with the change in the fatigue score until the 3-month follow-up. Their ß-coefficients were negative indicating that subjects with these symptoms improved less in the extent of their fatigue symptoms than those without these symptoms. At least one of the symptoms from each factor was longitudinally associated with fatigue. Abdominal pain from the pain factor had the strongest association with fatigue, with a β coefficient (95% CI) of -5.11 (-7.86; -2.37). The β coefficients with 95% CIs and p values of all symptoms shown in Figure 2 can be found in Suppl. Table S4.
Subgroup analyses by age and sex showed several potential differences, which need to be interpreted with caution because all confidence intervals overlapped. We would like to highlight potential subgroup differences, with effect estimates that were statistically significant and among which one was at least twice as strong as another when comparing the subgroups. With respect to potential sex differences, sore skin, faecal incontinence, all pain-related symptoms except abdominal pain, financial difficulties, psychological stress and hair loss were stronger associated with the change in fatigue scores in females then in males (Suppl. Table S5). Dyspnea and social sequelae were stronger associated with the change in fatigue scores in males than females. The subgroup analysis by age groups found that many symptoms from the gastrointestinal, pain and psychosocial symptom clusters were stronger associated with the change in fatigue scores in study participants younger than 65 years than in older patients (Suppl. Table S6). Moreover, urinary incontinence and constipation were stronger associated with the change of fatigue in younger study participants. In participants 65 years or older, only appetite loss was stronger associated with the change of fatigue than among younger CRC patients (Suppl. Table S6). Subgroup analysis by participation in the VICTORIA trial did not show relevant differences in the results because all confidence intervals overlapped (data not shown).
3.3.2. Longitudinal association of baseline symptoms with ability to work
111 (40%) study participants had a low-to-moderate ability to work (FACIT-F-FWB-AW score ≤ 2 points) at baseline and 72 (25.8%) participants at 3-month follow-up. The median FACIT-F-FWB-AW increased from 3 points (interquartile range (IQR: 2 - 4) to 4 points (IQR: 2 - 4) in this time, which translates to higher ability to work. On average, the mean FACIT-F-FWB-AW score improved by 0.57 points (standard deviation (SD): 1.2 points). The distribution of this change in FACIT-F-FWB-AW score points was approximately normally distributed (Figure 3).
The results of the multivariable linear regression analysis evaluating the association between covariates and the change of the ability to work from baseline to 3-month follow-up are displayed in Suppl. Table S7. A higher baseline ability to work and having received chemotherapy or radiotherapy within the year before rehabilitation were significantly associated with improved ability to work at the 3-month follow-up, whereas all other factors were not associated with this outcome.
The association between baseline symptoms and the change in ability to work until the 3-month follow-up are displayed in Figure 4. Overall, 24 out of 30 symptoms were significantly associated with the change in ability to work until the 3-month follow-up. At least one of the symptoms from each factor was associated with the change of ability to work at the 3-month follow-up. Their ß-coefficients were negative indicating that subjects with these symptoms improved less in the ability to work than those without these symptoms. All of the symptoms stemming from the fatigue-, pain-, and psychosocial symptoms- factors were associated with the ability to work at the 3-month follow-up. Nausea or vomiting had the strongest association with work ability, with a β coefficient (95% CI) of -0.83 (-1.12; -0.53). The β coefficients with 95% CIs and p values for all symptoms shown in Figure 4 can be found in Suppl. Table S8.
In the subgroup analyses on the ability to work we focus again on potential subgroup differences, with statistically significant effect estimate among which one was at least twice as strong compared to the other. However, it needs to be noted that all confidence intervals overlapped. Subgroup analysis by sex found that sore skin and dysuria were stronger associated with the change in the ability to work among female than male participants. In contrast, several symptoms from the fatigue cluster (fatigue, appetite loss, social sequelae, and dyspnea) and diarrhea were stronger associated with the change in the ability to work in male than in female CRC patients (Suppl. Table S9). Subgroup analysis by age showed comparable findings for the associations of most symptoms with the change in the ability to work with the exceptions of social sequelae, bloating, and constipation being stronger associated with the change in the ability to work among patients younger than 65 years (Suppl. Table S10). Only dyspnea had a stronger effect estimate among older subjects. Subgroup analysis by participation in the VICTORIA study did not reveal differences in the results for the outcome “change in the ability to work” (data not shown).
4. Discussion
The primary objective of this study was to identify symptom clusters in CRC patients within a year of completing primary CRC treatment using exploratory factor analysis. The second aim was to investigate which symptoms were longitudinally associated with the change of fatigue or ability to work from baseline to the 3-month follow-up using multivariable linear regression. We have identified six symptom clusters: fatigue, gastrointestinal symptoms, pain, psychosocial symptoms, urinary symptoms, and chemotherapy side effects clusters. Out of 30 symptoms with significant factor loadings, 14 symptoms were longitudinally associated with fatigue and 24 symptoms with the ability to work.
The fatigue cluster consisted of the following symptoms: fatigue (FACIT-F-FS), interference with daily life, emotional fatigue, depression, cognitive fatigue, dyspnea, social sequelae, appetite loss and ability to work. Fatigue is one of the most frequent symptoms of CRC patients, caused by primary disease or affiliated treatment. It is characterized as “physical, social and/or cognitive tiredness or exhaustion related to cancer or cancer treatment that is not proportional to recent activity and interferes with functioning “[31], and all of the symptoms included in this cluster, apart from dyspnea, could be interpreted as manifestations of cancer-related fatigue. Lack of appetite has been identified as a correlate of cancer-related fatigue [32]. Dyspnea, or the feeling of difficulty breathing, could be present during everyday physical activities such as walking or climbing the stairs. Cancer-related anemia, often present in CRC patients due to the chronic character of the disease or occult bleeding, can be a cause of both dyspnea and fatigue [33]. The fatigue cluster was often identified in previous studies on symptom clusters, irrespective of the type of malignancy [13,34]. In a network analysis of symptom clusters among a diverse group of cancer survivors, fatigue emerged as the most central symptom across all networks [35]. This finding highlights the crucial need to address fatigue early in the rehabilitation process.
The gastrointestinal symptoms cluster consisted of fecal incontinence, stool frequency, sore skin, embarrassment, diarrhea, flatulence, and blood/mucus in stool. Most of these symptoms can be directly linked to treatment side effects. Local radiotherapy can cause diarrhea, bloating, skin erythema, and fecal incontinence [10]. Due to the nature of these symptoms, patients can have accompanying embarrassment in social settings. The gastrointestinal symptoms cluster, often characterized as “digestive symptoms cluster”, is frequently identified in previous literature in CRC patients [13,36] and patients with other cancer types [35].
The pain cluster consisted of pain, abdominal pain, buttock pain, bloating, and dysuria. Pain is one of the symptoms present at the time of the diagnosis and before treatment and can often be aggravated by subsequent treatments [37]. Oxaliplatin-induced neuropathy has emerged as a common side effect of chemotherapy for CRC patients [38]. Chronic pain can be a long-term side effect of CRC surgery. A Danish study found that 40% of CRC patients reported having chronic abdominal or pelvic pain after rectal surgery [39]. The pain cluster is commonly identified in cancer populations, irrespective of tumor localization [13,15,40].
The psychosocial symptoms cluster consisted of anxiety, financial difficulties, and psychosocial distress. During therapy, many patients need to take an absence from work. A previous study in the Netherlands found that CRC patients had a median return-to-work time of 423 days from the beginning of their absence leave [41]. The temporary absence from work can be a cause of financial difficulties as well as worry and anxiety for CRC patients. Anxiety is also frequent at the start of the treatment and can persevere after the completion of the treatment [42]. In some previous studies, anxiety has clustered with depression and other emotional symptoms [36,43]. However, in our study, anxiety coupled with psychosocial distress and financial difficulties. It is possible that the absence from work and its financial implications may have amplified the interconnectedness of anxiety, financial strain, and broader psychosocial distress in CRC patients in our study.
The urinary symptoms cluster consisted of urinary incontinence, urinary frequency, and sleep disturbance. Sleep disturbances are not unusual in patients with frequent urination during the night. A previous study found that late urinary side effects affect up to 41% of CRC patients following brachytherapy for colorectal cancer. Symptoms included obstructive and irritative symptoms [44]. The urinary symptoms have been described in previous studies of CRC symptom clusters.
The chemotherapy side effects cluster included nausea or vomiting, taste alteration, constipation, and hair loss. These symptoms have been described as common post-chemotherapy side effects in the literature [45]. Though nausea and vomiting are sometimes grouped as a gastrointestinal cluster in previous literature [46], they constitute their own cluster alongside other prevalent chemotherapy side effects in our study. These findings indicate the complexity of CRC symptomatology after treatment and variability in patient experience.
In the context of our findings, we identified six specific symptom clusters in CRC patients. Our findings point that these clusters originate from the primary disease or, more predominantly, from therapeutic interventions. Notably, the fatigue and pain clusters, which are prominently present, suggest an underlying inflammatory mechanism, a facet that requires further exploration [47]. A recent study further supports this hypothesis by reporting an association between the symptom clusters in palliative CRC patients and proinflammatory cytokines [48]. This underscores the necessity to investigate potential inflammatory mechanisms underlying these symptom clusters, emphasizing the importance of ongoing research for improved management and comprehension of CRC-associated symptoms.
In this study, we identified two groups of symptoms to be longitudinally associated with fatigue: gastrointestinal/physical symptoms (fecal incontinence, stool frequency, urinary incontinence, abdominal pain, dyspnea, and nausea or vomiting) and psychosocial symptoms (cognitive fatigue, embarrassment, anxiety, financial difficulties, and sleep disturbance). Participants who experienced any of these symptoms were more likely to have higher fatigue levels. Gastrointestinal symptoms in female CRC patients were previously shown to be associated with fatigue, as well as reduced social functions and increased daily life interference [49]. Considering psychosocial factors, a cross-sectional study identified an association between fatigue and both sleep disturbances and anxiety in CRC patients [50]. However, while this study noted a significant relationship between fatigue and depression, our findings did not corroborate this link. Possible reasons for this inconsistency might include variations in study methodologies, patient demographics, or therapeutic regimens between the two studies. Recognizing symptoms associated with fatigue is crucial for clinical practice, allowing for more targeted interventions in fatigue management for CRC patients.
We have found 24 symptoms that are longitudinally associated with the ability to work. Our findings confirm the results from the systematic review on the influence of cancer-related symptoms on the ability to work [19]. Previously, a study found that CRC patients had a 56% higher risk of losing employment due to work disability up to 4 years after CRC diagnosis, compared to the general population [51]. Symptoms related to lower ability to work stemmed from all six of the identified clusters. Out of 11 symptoms associated with improved fatigue at the 3-month follow-up, 9 were also associated with improved ability to work in the first 3 months after rehabilitation. These results reaffirm the pleiotropic influence of different symptoms on the ability to work in CRC patients, apart from the conventional predictors such as age and stage of the disease. It also underscores the importance of a holistic approach, emphasizing the need to address the entirety of symptoms rather than the traditional one-symptom focus. Understanding the clustering of symptoms and its connection to the ability to work is a central step in developing intervention strategies that could be implemented during the rehabilitation part of the convalescence of CRC patients.
The MIRANDA study possesses several strengths. Firstly, it’s a multicentric, prospective cohort study that aims to capture data from six rehabilitation clinics across different regions in Germany, ensuring a diverse and representative sample. The rigorous inclusion and exclusion criteria further ensure the consistency and reliability of the data. The study involves periodic follow-ups, which allows for a longitudinal understanding of the variables in question, such as fatigue and the ability to work. Furthermore, the study utilizes multiple well-established scales and questionnaires like the FACIT-F-FS, GDS-15, GAD-7, and EORTC-QLQ-C30, among others, to comprehensively assess various symptoms and factors.
However, there are some inherent limitations to our study. One limitation is the reliance on self-reported data for most sociodemographic, lifestyle, and clinical information, such as symptom presence. Only a few variables, such as weight, height, and stage of the disease, relied on physician reports. Additionally, the ability to work was estimated using a single-item measure. Various factors can influence the ability to work, including physical symptoms, cognitive function, environmental conditions, and social and emotional well-being. A single item might not capture all these dimensions. Lastly, almost half of the participants were recruited during the COVID-19 pandemic between Sept 2020 and Dec 2021. Consequently, there is a possibility that some of these participants might have experienced post-COVID symptoms or late effects from the virus infection [52]. This could potentially increase the prevalence of certain symptoms in our sample, making it higher than it might have been in a non-pandemic context.
5. Conclusions
Our analysis identified six unique symptom clusters in CRC patients following curative treatment: fatigue, gastrointestinal symptoms, pain, psychosocial stress, urinary symptoms, and chemotherapy side effects. These clusters offer valuable insights for clinicians, suggesting a structured approach wherein symptoms can be addressed based on the cluster from which they originate. Notably, symptoms stemming from each of these clusters have shown an association with worse fatigue and lower ability to work at the 3-month follow-up.
Despite the efforts of current rehabilitation protocols, our findings indicate that several symptoms remain significantly associated with post-rehabilitation fatigue and a low ability to work in CRC patients. This highlights an area in our care continuum that requires further investigation and optimization. Enhanced interventions, integrating both pharmacological and psychosocial modalities, may provide improved outcomes for these patients. A targeted approach is recommended to address specific symptom clusters and their relationship with fatigue. Future studies should focus on developing and testing these interventions to optimize the post-treatment phase for CRC patients.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Supplementary Table S1: Comparison of important baseline characteristics of participants who completed the 3-month follow-up, non-responding participants, and with late recruited participants who did not have a chance yet to participate in the 3-month follow-up; Supplementary Table S2: Longitudinal associations of symptoms at baseline with fatigue at the 3-month follow-up, subgroup analysis by sex; Supplementary Table S3: Longitudinal associations of symptoms at baseline with fatigue at the 3-month follow-up, subgroup analysis by age; Supplementary Table S4: Longitudinal associations of symptoms at baseline with ability to work at the 3-month follow-up, subgroup analysis by sex; Supplementary Table S5: Longitudinal associations of symptoms at baseline with ability to work at the 3-month follow-up, subgroup analysis by age.
Author Contributions
Conceptualization, B.S.; methodology B.S. and T.V., H.B., R.C.; validation, T.V., M.S., and B.S.; formal analysis, T.V. and B.S.; investigation, R.C., B.B., H.F.; data curation, B.B., H.R. M.S.; writing—original draft preparation, T.V., and B.S.; writing—review and editing, B.S., T.V., R.C., B.B., H.F., M.S., and H.B.; visualization, T.V., B.S., and R.C.; supervision, H.B., and B.S.; project administration, B.S., H.B., M.S.; funding acquisition, H.B., R.C., and B.S. All authors have read and agreed to the published version of the manuscript.
Funding
The MIRANDA study is funded by own resources at the German Cancer Research Center. This specific project was funded by the German Pension Insurance (Deutsche Rentenversicherung Bund), grant number 8011- 106-31/31.136.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and in accordance with all applicable legal and regulatory requirements in Germany. The study was approved by the responsible Ethical Committee of the Faculty of Medicine Heidelberg (ethical approval code S-905/2019, date of approval: 27 January 2020).
Informed Consent Statement
Written informed consent was obtained from all participants involved in the study.
Data Availability Statement
The data will not be published to an open-access platform. After completion of the study, interested scientists can request data use and receive pseudonymized data upon approval of this application by the principal investigator. Please contact Dr. Ben Schöttker (b.schoettker@dkfz.de).
Acknowledgments
We gratefully acknowledge the collaboration and commitment of all staff in the rehabilitation clinics involved in the MIRANDA study. We thank the documentarians at the German Cancer Research Centers’ Division of Clinical Epidemiology and Ageing Research for their work in the planning of data collection and all documentation procedures.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Hofman, M.; Ryan, J.L.; Figueroa-Moseley, C.D.; Jean-Pierre, P.; Morrow, G.R. Cancer-related fatigue: the scale of the problem. Oncologist 2007, 12 Suppl 1, 4–10. [Google Scholar] [CrossRef]
- Han, C.J.; Yang, G.S.; Syrjala, K. Symptom Experiences in Colorectal Cancer Survivors After Cancer Treatments: A Systematic Review and Meta-analysis. Cancer Nurs 2020, 43, E132–E158. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.N.; Huang, M.L.; Kao, C.H. Prevalence of Depression and Anxiety in Colorectal Cancer Patients: A Literature Review. Int J Environ Res Public Health 2019, 16. [Google Scholar] [CrossRef] [PubMed]
- Zielinska, A.; Wlodarczyk, M.; Makaro, A.; Salaga, M.; Fichna, J. Management of pain in colorectal cancer patients. Crit Rev Oncol Hematol 2021, 157, 103122. [Google Scholar] [CrossRef] [PubMed]
- Senapati, S.; Mahanta, A.K.; Kumar, S.; Maiti, P. Controlled drug delivery vehicles for cancer treatment and their performance. Signal Transduct Target Ther 2018, 3, 7. [Google Scholar] [CrossRef] [PubMed]
- Carelle, N.; Piotto, E.; Bellanger, A.; Germanaud, J.; Thuillier, A.; Khayat, D. Changing patient perceptions of the side effects of cancer chemotherapy. Cancer 2002, 95, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Pearce, A.; Haas, M.; Viney, R.; Pearson, S.A.; Haywood, P.; Brown, C.; Ward, R. Incidence and severity of self-reported chemotherapy side effects in routine care: A prospective cohort study. PLoS One 2017, 12, e0184360. [Google Scholar] [CrossRef] [PubMed]
- German Guideline Program in Oncology (German Cancer Society, German Cancer Aid, AWMF): S3-Guideline Colorectal Cancer, long version 2.1, 2019, AWMF registrationnumber: 021-007OL, Available online: http://www.leitlinienprogrammonkologie.de/leitlinien/kolorektales-karzinom/ (accessed on 18.07.2023).
- Kuipers, E.J.; Grady, W.M.; Lieberman, D.; Seufferlein, T.; Sung, J.J.; Boelens, P.G.; van de Velde, C.J.; Watanabe, T. Colorectal cancer. Nat Rev Dis Primers 2015, 1, 15065. [Google Scholar] [CrossRef] [PubMed]
- Birgisson, H.; Pahlman, L.; Gunnarsson, U.; Glimelius, B. Late adverse effects of radiation therapy for rectal cancer - a systematic overview. Acta Oncol 2007, 46, 504–516. [Google Scholar] [CrossRef]
- Guren, M.G.; Dueland, S.; Skovlund, E.; Fossa, S.D.; Poulsen, J.P.; Tveit, K.M. Quality of life during radiotherapy for rectal cancer. Eur J Cancer 2003, 39, 587–594. [Google Scholar] [CrossRef]
- Li, G. A Review of the Research on Symptom Clusters in Cancer Survivors. Open Journal of Nursing 2021, 11, 423–434. [Google Scholar] [CrossRef]
- Hao, J.; Gu, L.; Liu, P.; Zhang, L.; Xu, H.; Qiu, Q.; Zhang, W. Symptom clusters in patients with colorectal cancer after colostomy: a longitudinal study in Shanghai. J Int Med Res 2021, 49, 3000605211063105. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Ryu, E. Effects of symptom clusters and depression on the quality of life in patients with advanced lung cancer. Eur J Cancer Care (Engl) 2018, 27. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.W.; Lyon, D.; Farace, E. Symptom clusters in patients with high-grade glioma. J Nurs Scholarsh 2007, 39, 61–67. [Google Scholar] [CrossRef] [PubMed]
- van Muijen, P.; Weevers, N.L.; Snels, I.A.; Duijts, S.F.; Bruinvels, D.J.; Schellart, A.J.; van der Beek, A.J. Predictors of return to work and employment in cancer survivors: a systematic review. Eur J Cancer Care (Engl) 2013, 22, 144–160. [Google Scholar] [CrossRef]
- Kane, D.; Rajacich, D.; Andary, C. Experiences of cancer patients’ return to work. Can Oncol Nurs J 2020, 30, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Tavan, H.; Azadi, A.; Veisani, Y. Return to Work in Cancer Patients: A Systematic Review and Meta-analysis. Indian J Palliat Care 2019, 25, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.J.; Yip, S.Y.C.; Chan, R.J.; Chew, L.; Chan, A. Investigating how cancer-related symptoms influence work outcomes among cancer survivors: a systematic review. J Cancer Surviv 2022, 16, 1065–1078. [Google Scholar] [CrossRef]
- Vlaski, T.; Slavic, M.; Caspari, R.; Fischer, H.; Brenner, H.; Schottker, B. Development Trajectories of Fatigue, Quality of Life, and the Ability to Work among Colorectal Cancer Patients in the First Year after Rehabilitation-First Results of the MIRANDA Study. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef]
- Schottker, B.; Kuznia, S.; Laetsch, D.C.; Czock, D.; Kopp-Schneider, A.; Caspari, R.; Brenner, H. Protocol of the VICTORIA study: personalized vitamin D supplementation for reducing or preventing fatigue and enhancing quality of life of patients with colorectal tumor - randomized intervention trial. BMC Cancer 2020, 20, 739. [Google Scholar] [CrossRef]
- Cella, D.F.; Tulsky, D.S.; Gray, G.; Sarafian, B.; Linn, E.; Bonomi, A.; Silberman, M.; Yellen, S.B.; Winicour, P.; Brannon, J.; et al. The Functional Assessment of Cancer Therapy scale: development and validation of the general measure. J Clin Oncol 1993, 11, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Van Belle, S.; Paridaens, R.; Evers, G.; Kerger, J.; Bron, D.; Foubert, J.; Ponnet, G.; Vander Steichel, D.; Heremans, C.; Rosillon, D. Comparison of proposed diagnostic criteria with FACT-F and VAS for cancer-related fatigue: proposal for use as a screening tool. Support Care Cancer 2005, 13, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Giesinger, J.M.; Loth, F.L.C.; Aaronson, N.K.; Arraras, J.I.; Caocci, G.; Efficace, F.; Groenvold, M.; van Leeuwen, M.; Petersen, M.A.; Ramage, J.; et al. Thresholds for clinical importance were established to improve interpretation of the EORTC QLQ-C30 in clinical practice and research. J Clin Epidemiol 2020, 118, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Whistance, R.N.; Conroy, T.; Chie, W.; Costantini, A.; Sezer, O.; Koller, M.; Johnson, C.D.; Pilkington, S.A.; Arraras, J.; Ben-Josef, E.; et al. Clinical and psychometric validation of the EORTC QLQ-CR29 questionnaire module to assess health-related quality of life in patients with colorectal cancer. Eur J Cancer 2009, 45, 3017–3026. [Google Scholar] [CrossRef] [PubMed]
- Weis, J.; Tomaszewski, K.A.; Hammerlid, E.; Ignacio Arraras, J.; Conroy, T.; Lanceley, A.; Schmidt, H.; Wirtz, M.; Singer, S.; Pinto, M.; et al. International Psychometric Validation of an EORTC Quality of Life Module Measuring Cancer Related Fatigue (EORTC QLQ-FA12). J Natl Cancer Inst 2017, 109. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, M.; Nowe, E.; Hofmeister, D.; Kuhnt, S.; Leuteritz, K.; Sender, A.; Stobel-Richter, Y.; Geue, K. Psychometric properties of the fatigue questionnaire EORTC QLQ-FA12 and proposal of a cut-off value for young adults with cancer. Health Qual Life Outcomes 2018, 16, 125. [Google Scholar] [CrossRef] [PubMed]
- Book, K.; Marten-Mittag, B.; Henrich, G.; Dinkel, A.; Scheddel, P.; Sehlen, S.; Haimerl, W.; Schulte, T.; Britzelmeir, I.; Herschbach, P. Distress screening in oncology-evaluation of the Questionnaire on Distress in Cancer Patients-short form (QSC-R10) in a German sample. Psychooncology 2011, 20, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.F.; Finan, C. Linear regression and the normality assumption. J Clin Epidemiol 2018, 98, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Nassiri, V.; Lovik, A.; Molenberghs, G.; Verbeke, G. On using multiple imputation for exploratory factor analysis of incomplete data. Behav Res Methods 2018, 50, 501–517. [Google Scholar] [CrossRef]
- Berger, A.M.; Mooney, K.; Alvarez-Perez, A.; Breitbart, W.S.; Carpenter, K.M.; Cella, D.; Cleeland, C.; Dotan, E.; Eisenberger, M.A.; Escalante, C.P.; et al. Cancer-Related Fatigue, Version 2.2015. J Natl Compr Canc Netw 2015, 13, 1012–1039. [Google Scholar] [CrossRef]
- Oh, H.S.; Seo, W.S. Systematic review and meta-analysis of the correlates of cancer-related fatigue. Worldviews Evid Based Nurs 2011, 8, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Chardalias, L.; Papaconstantinou, I.; Gklavas, A.; Politou, M.; Theodosopoulos, T. Iron Deficiency Anemia in Colorectal Cancer Patients: Is Preoperative Intravenous Iron Infusion Indicated? A Narrative Review of the Literature. Cancer Diagn Progn 2023, 3, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Agasi-Idenburg, S.C.; Thong, M.S.; Punt, C.J.; Stuiver, M.M.; Aaronson, N.K. Comparison of symptom clusters associated with fatigue in older and younger survivors of colorectal cancer. Support Care Cancer 2017, 25, 625–632. [Google Scholar] [CrossRef] [PubMed]
- de Rooij, B.H.; Oerlemans, S.; van Deun, K.; Mols, F.; de Ligt, K.M.; Husson, O.; Ezendam, N.P.M.; Hoedjes, M.; van de Poll-Franse, L.V.; Schoormans, D. Symptom clusters in 1330 survivors of 7 cancer types from the PROFILES registry: A network analysis. Cancer 2021, 127, 4665–4674. [Google Scholar] [CrossRef] [PubMed]
- Storey, S.; Luo, X.; Ren, J.; Huang, K.; Von Ah, D. Symptom Clusters in Patients With Colorectal Cancer and Diabetes Over Time. Oncol Nurs Forum 2023, 50, 475–485. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Garzon, M.; Postigo-Martin, P.; Gonzalez-Santos, A.; Arroyo-Morales, M.; Achalandabaso-Ochoa, A.; Fernandez-Perez, A.M.; Cantarero-Villanueva, I. Colorectal cancer pain upon diagnosis and after treatment: a cross-sectional comparison with healthy matched controls. Support Care Cancer 2022, 30, 3573–3584. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, K.; Lyleroehr, M.; Shaunfield, S.; Lacson, L.; Corona, M.; Kircher, S.; Nittve, M.; Cella, D. Neuropathy experienced by colorectal cancer patients receiving oxaliplatin: A qualitative study to validate the Functional Assessment of Cancer Therapy/Gynecologic Oncology Group-Neurotoxicity scale. World J Gastrointest Oncol 2020, 12, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, A.R.; Thyo, A.; Emmertsen, K.J.; Laurberg, S. Chronic pain after rectal cancer surgery - development and validation of a scoring system. Colorectal Dis 2019, 21, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Dong, S.T.; Butow, P.N.; Costa, D.S.; Lovell, M.R.; Agar, M. Symptom clusters in patients with advanced cancer: a systematic review of observational studies. J Pain Symptom Manage 2014, 48, 411–450. [Google Scholar] [CrossRef]
- den Bakker, C.M.; Anema, J.R.; Huirne, J.A.F.; Twisk, J.; Bonjer, H.J.; Schaafsma, F.G. Predicting return to work among patients with colorectal cancer. Br J Surg 2020, 107, 140–148. [Google Scholar] [CrossRef]
- Abd El Aleem, E.M.; Selim, N.F.M.; Abdallah, A.M.; Amin, S.I. Assessment of Depression and Anxiety in Colorectal Cancer Patients: Review Article. The Egyptian Journal of Hospital Medicine 2023, 92, 2630–2633. [Google Scholar] [CrossRef]
- Potosky, A.L.; Graves, K.D.; Lin, L.; Pan, W.; Fall-Dickson, J.M.; Ahn, J.; Ferguson, K.M.; Keegan, T.H.M.; Paddock, L.E.; Wu, X.C.; et al. The prevalence and risk of symptom and function clusters in colorectal cancer survivors. J Cancer Surviv 2022, 16, 1449–1460. [Google Scholar] [CrossRef] [PubMed]
- Liberman, D.; Mehus, B.; Elliott, S.P. Urinary adverse effects of pelvic radiotherapy. Transl Androl Urol 2014, 3, 186–195. [Google Scholar] [CrossRef] [PubMed]
- İnsaf ALTUN, A.S. The Most Common Side Effects Experienced by Patients Were Receiving First Cycle of Chemotherapy. Iran J Public Health 2018, 47, 1218–1219. [Google Scholar]
- Fan, G.; Filipczak, L.; Chow, E. Symptom clusters in cancer patients: a review of the literature. Curr Oncol 2007, 14, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Dong, S.T.; Costa, D.S.; Butow, P.N.; Lovell, M.R.; Agar, M.; Velikova, G.; Teckle, P.; Tong, A.; Tebbutt, N.C.; Clarke, S.J.; et al. Symptom Clusters in Advanced Cancer Patients: An Empirical Comparison of Statistical Methods and the Impact on Quality of Life. J Pain Symptom Manage 2016, 51, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Nilsberth, C.; Sackmann, V.; Fransson, K.; Jakobsson, M.; Karlsson, M.; Milberg, A. Symptom clusters in palliative-stage cancer correlate with proinflammatory cytokine cluster. Ann Palliat Med 2023, 12, 458–471. [Google Scholar] [CrossRef]
- Han, C.J.; Reding, K.W.; Kalady, M.F.; Yung, R.; Greenlee, H.; Paskett, E.D. Factors associated with long-term gastrointestinal symptoms in colorectal cancer survivors in the women’s health initiatives (WHI study). PLoS One 2023, 18, e0286058. [Google Scholar] [CrossRef]
- Mota, D.D.; Pimenta, C.A.; Caponero, R. Fatigue in colorectal cancer patients: prevalence and associated factors. Rev Lat Am Enfermagem 2012, 20, 495–503. [Google Scholar] [CrossRef]
- de Wind, A.; Tamminga, S.J.; Bony, C.A.G.; Diether, M.; Ludwig, M.; Velthuis, M.J.; Duijts, S.F.A.; de Boer, A.G.E.M. Loss of Paid Employment up to 4 Years after Colorectal Cancer Diagnosis—A Nationwide Register-Based Study with a Population-Based Reference Group. Cancers 2021, 13. [Google Scholar] [CrossRef]
- Han, Q.; Zheng, B.; Daines, L.; Sheikh, A. Long-Term Sequelae of COVID-19: A Systematic Review and Meta-Analysis of One-Year Follow-Up Studies on Post-COVID Symptoms. Pathogens 2022, 11. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Histogram of change of FACIT-F-FS points from baseline to 3-month follow-up.
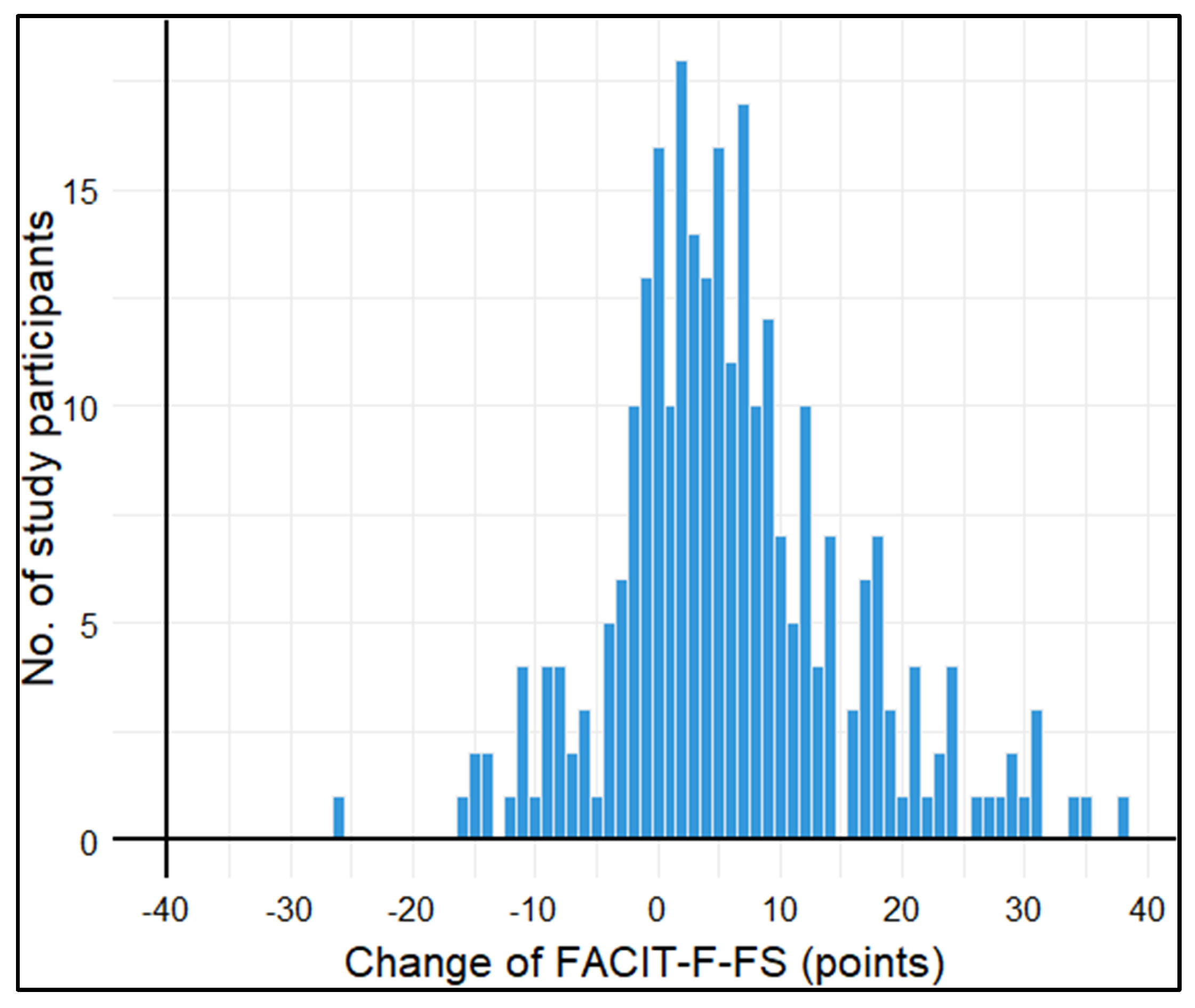
Figure 2.
Forest plot showing longitudinal associations of symptoms at baseline with the change in fatigue symptoms from baseline to 3-month follow-up.
Figure 2.
Forest plot showing longitudinal associations of symptoms at baseline with the change in fatigue symptoms from baseline to 3-month follow-up.
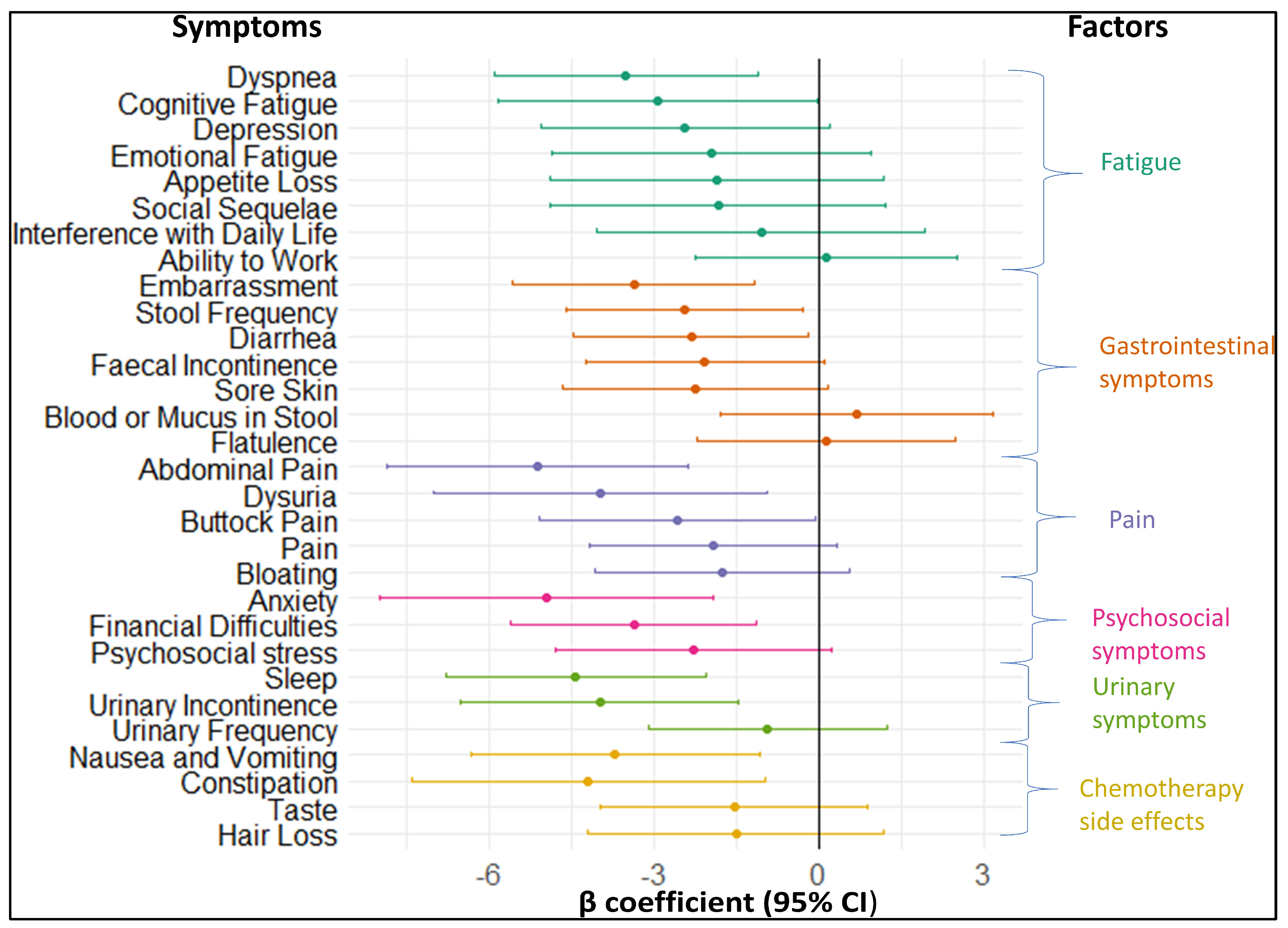
Figure 3.
Histogram of change of FACIT-F-FWB Ability to Work score points from baseline to 3-month follow-up.
Figure 3.
Histogram of change of FACIT-F-FWB Ability to Work score points from baseline to 3-month follow-up.
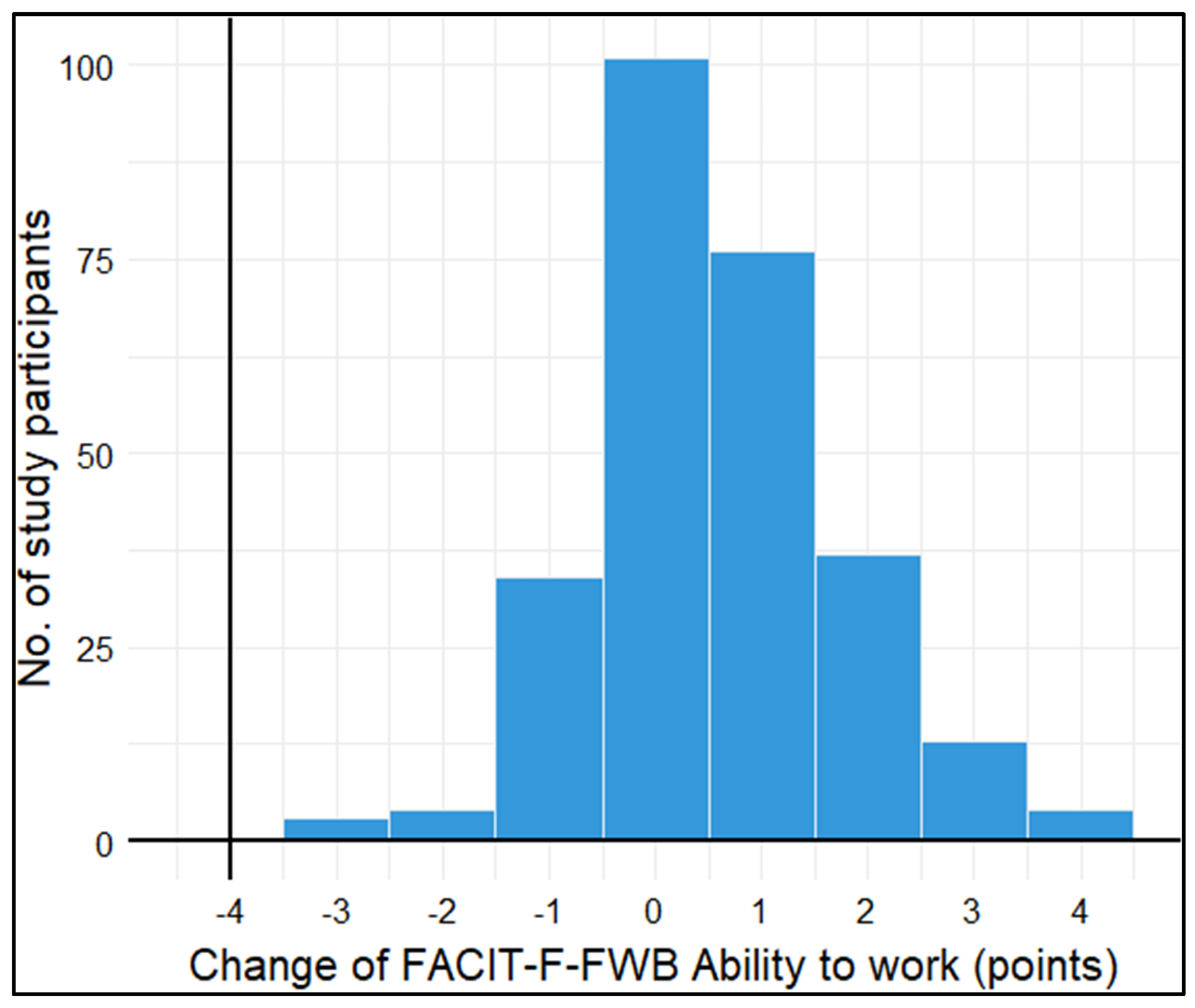
Figure 4.
Forest plot showing longitudinal associations of symptoms at baseline with the change in the ability to work from baseline to 3-month follow-up.
Figure 4.
Forest plot showing longitudinal associations of symptoms at baseline with the change in the ability to work from baseline to 3-month follow-up.
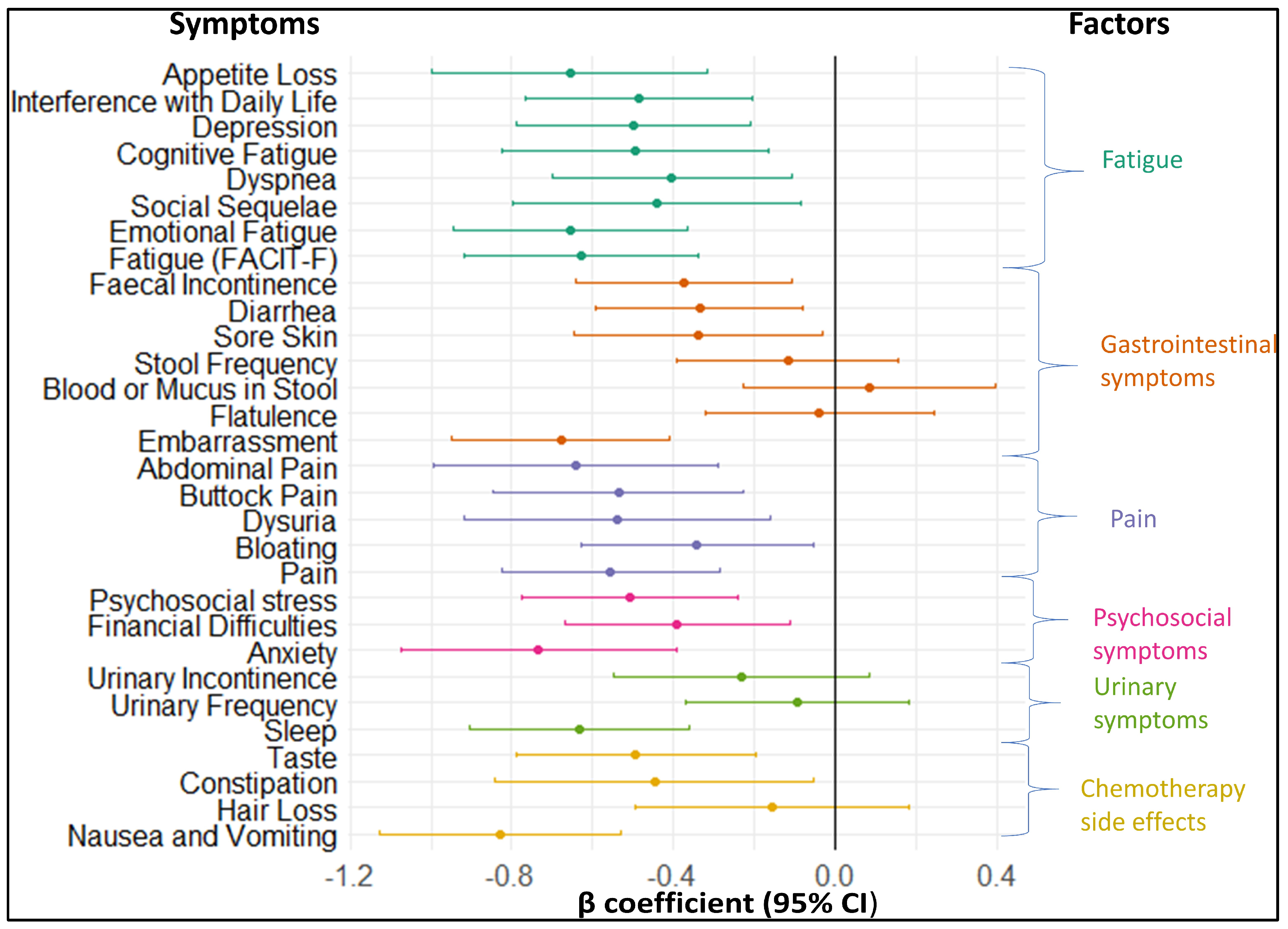

Table 1.
Baseline characteristics of the participants (N=394).
| Baseline characteristics | Ntotal | Proportion (%) | Median (Q1-Q3) |
|---|---|---|---|
| Age (years) | 394 | 62 (56 - 71) | |
| <65 | 222 (56.3) | ||
| ≥65 | 172 (43.7) | ||
| Sex | 394 | ||
| Female | 166 (42.1) | ||
| Male | 228 (57.9) | ||
| Cancer stage | 375 | ||
| I | 117 (31.2) | ||
| II | 120 (32.0) | ||
| III | 99 (26.4) | ||
| IV | 23 (6.1) | ||
| Unknown | 16 (4.3) | ||
| Type of CRC treatment | |||
| Surgery | 389 | 386 (99.2) | |
| Chemotherapy | 382 | 176 (46.1) | |
| Radiotherapy | 378 | 79 (20.9) | |
| Months since CRC surgery | 383 | ||
| 0–1 | 162 (42.3) | ||
| 2–3 | 62 (16.2) | ||
| 4–6 | 48 (12.5) | ||
| 7–9 | 62 (16.2) | ||
| 10–12 | 34 (8.9) | ||
| >12 | 15 (3.9) | ||
| Body Mass Index (kg/m²) | 394 | 26.2 (23.1 – 29.6) | |
| <25 | 161 (40.9) | ||
| 25 to <30 | 144 (36.5) | ||
| ≥30 | 89 (22.6) | ||
| Smoking status | 373 | ||
| Never smoked | 159 (42.6) | ||
| Former smoker | 161 (43.2) | ||
| Current smoker | 53 (14.2) | ||
| Healthy physical activity level a | 368 | 175 (47.5) | |
| Comorbidities | |||
| Diabetes mellitus | 371 | 64 (17.3) | |
| Hypertension | 368 | 194 (52.7) | |
| History of myocardial infarction | 370 | 13 (3.5) | |
| History of stroke | 371 | 14 (3.8) | |
| Number of comorbidities | 374 | 2 (1 – 2) | |
| 0 | 66 (17.7) | ||
| 1 | 109 (29.1) | ||
| ≥ 2 | 199 (53.2) | ||
| Employment status | 386 | ||
| Fully employed | 188 (48.7) | ||
| Part-time employed | 36 (9.3) | ||
| Retired | 150 (38.9) | ||
| Unemployed | 12 (3.1) |
Abbreviations: CRC, colorectal cancer; Q1, 1st Quartile (25th percentile); Q3, 3rd Quartile (75th percentile). a Healthy physical activity was defined as at least 150 min of moderate-intensity or 75 min of vigorous-intensity aerobic physical activity throughout the week or an equivalent combination of moderate-intensity physical activity during the year before the CRC diagnosis.
Table 2.
Allocation of 32 colorectal cancer symptoms to six factors.
| Symptoms | Factor 1 “Fatigue” |
Factor 2 “Gastro- intestinal symptoms” |
Factor 3 “Pain” |
Factor 4 “Psycho- social symptoms” |
Factor 5 “Urinary symptoms” |
Factor 6 “Chemotherapy side effects” |
|---|---|---|---|---|---|---|
| Highest factor loading | ||||||
| Fatigue (FACIT F) | -0.97 | |||||
| Interference with Daily Life | 0.94 | |||||
| Emotional Fatigue | 0.80 | |||||
| Depression | 0.68 | |||||
| Cognitive Fatigue | 0.61 | |||||
| Dyspnea | 0.49 | |||||
| Social Functioning | 0.46 | |||||
| Ability to Work | -0.39 | |||||
| Appetite Loss | 0.31 | |||||
| Faecal Incontinence | 0.82 | |||||
| Stool Frequency | 0.80 | |||||
| Sore Skin | 0.65 | |||||
| Embarrassment | 0.51 | |||||
| Diarrhea | 0.45 | |||||
| Flatulence | 0.36 | |||||
| Blood/Mucus in Stool | 0.33 | |||||
| Abdominal Pain | 0.79 | |||||
| Pain | 0.73 | |||||
| Buttock Pain | 0.52 | |||||
| Bloating | 0.43 | |||||
| Dysuria | 0.35 | |||||
| Psychosocial Stress | 0.58 | |||||
| Anxiety | 0.48 | |||||
| Financial Difficulties | 0.40 | |||||
| Urinary Frequency | 0.70 | |||||
| Urinary Incontinence | 0.50 | |||||
| Sleep Disturbance | 0.33 | |||||
| Dry Mouth | 0.20 | |||||
| Taste Alteration | 0.61 | |||||
| Hair Loss | 0.44 | |||||
| Constipation | 0.32 | |||||
| Nausea or Vomiting | 0.30 | |||||
| Eigenvalue | 4.96 | 2.67 | 2.17 | 1.99 | 1.12 | 0.95 |
| Variance explained | 0.15 | 0.08 | 0.07 | 0.06 | 0.04 | 0.03 |
| Proportion explained (%) | 36 | 19 | 16 | 14 | 8 | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



