
Submitted:
30 November 2023
Posted:
04 December 2023
You are already at the latest version
Abstract
Treatment-emergent sexual dysfunction (TESD) is one of the most frequent and persistent adverse effects of antidepressant medication. Sexual dysfunction (SD) secondary to SSRIs occurs in >60% of sexually active patients and >80% of healthy volunteers, with this causing treatment discontinuation in >35% of patients. However, this factor is rarely addressed in routine examinations, and only 15%-30% of these events are spontaneously reported. A strategy of switching to a different non-serotonergic antidepressant could involve a risk of relapse or clinical worsening due to a lack of serotonergic activity. Vortioxetine appears to have less impact on sexual function due to its multimodal mechanism of action. No studies have been published on the effectiveness of switching to vortioxetine in patients with poorly tolerated long-term antidepressant-related SD at naturalistic settings.
Study objectives: To determine the effectiveness of switching to vortioxetine due to SD in a routine clinical practice setting.
Methodology: observational pragmatic and naturalistic study to determinate the effectiveness of the switch to vortioxetine (mean dosage 13.11±4.03) in 74 patients aged 43.1 ± 12.65 ( 54% males) at risk of discontinuing treatment due to sexual dysfunction. The SALSEX Scale was applied at two moments: baseline visit and after 3 months of follow-up.
Results. The global Sexual Dysfunction (SD) measured with the SALSEX Scale, decreased significantly from baseline visit (10.32; SD 2.73) to follow-up visit (3.78; SD 3.68) p<0.001. There was a significant improvement ( p<0.001) at the endpoint including decreased libido, delay of orgasm, anorgasmia and arousal difficulties in both sexes. After switching to Vortioxetine, 83.81% of patients experienced sexual function improvement (43.2% felt greatly improved). Most patients (83.3%) who switched to vortioxetine continued treatment after the follow-up visit. 58.1% of patients showed an improvement in depressive symptoms from baseline visit. Conclusion. Switching to vortioxetine is an effective and reliable strategy to treat patients with poor tolerated previous antidepressant -related sexual dysfunction in the real-life clinical settings.
Keywords:
Sexual Dysfunction
; antidepressant
; vortioxetine
; depression
; sexuality
1. Introduction
Antidepressants are frequently associated with sexual dysfunction (SD), particularly SSRI serotonergic agents, dual-action drugs, and clomipramine [1]. Other drugs with different mechanisms of action appear to cause fewer sexual adverse effects (mirtazapine, bupropion, moclobemide). Unfortunately, the real incidence of SD is underestimated, and specific questionnaires must be used. Spontaneous reporting of this adverse effect is around 15%-20%, while real figures exceed 60%-80%, [2,3]. The problem is significant and it is closely associated with treatment dropout, particularly in the case of long-term treatments, and has a negative impact on the quality of life of patients and their partners [4].
Vortioxetine (VOR)] seems to have better profile in terms of SD, although most data comes from clinical trials with registration purposes that may have some methodological limitations, such as the depressive population examined and short-term data [5]. SD rates vary between 0.9% and 45%, depending on the study methodology. Since the serotonergic mechanism of action seems to be closely linked with the etiology and pathogenesis of depression [6], drugs increasing serotonin availability are generally associated with high rates of SD, as this neurotransmitter is very closely involved with inhibition of sexual function, impulsivity, and appetite among others.
The physio pathogenic mechanisms of these phenomena appear to be multifactorial and complex [7]. One mechanism is the increase in circulating serotonin and the activation of serotonin 5-HT2A receptors that could affect orgasmic function and sexual interest. Erectile dysfunction appears to be caused by changes in nitric oxide functioning and activation of peripheral adrenergic receptors.
Management of SD has been attempted using various approaches [8]: waiting for spontaneous remission, dose reduction, or switching to another drug with a lower profile of impact on sexual functioning or use of "antidotes” such as sildenafil or other similar compounds [4,9]. Given the high rates of sexual dysfunction nowadays usually left unaddressed by clinicians, its impact on patients’ quality of life and treatment discontinuation (estimated at over 35%), this problem must be directly investigated in all patients who receive antidepressants.
In the last 10 years, a very significant increase has been observed in the number of publications addressing this topic, and rising rates of SD have been detected with the use of specific questionnaires [10,11,12], compared to the initial estimates obtained from spontaneous patient reports. Initial data on the incidence of SD obtained retrospectively ranged widely: between 5% and 75% depending on the study methodology used.
In previous studies using the validated questionnaire Psychotropic-Related Sexual Dysfunction Questionnaire [10] the mean incidence of SD with SSRIs and dual-action agents was as high as 80% among sexually active patients [3]. The questionnaire analyses the following variables on a scale of severity or frequency: 1) lower libido; 2) delayed orgasm/ejaculation; 3) absent orgasm/ejaculation; 4) erectile/vaginal lubrication dysfunction; and 5) patient’s tolerability of sexual dysfunction and risk of discontinuing treatment. The author and the working group have published numerous studies that use this method to evaluate frequency of SD, risk of discontinuation, impact on quality of life, studies in healthy volunteers, clinical management procedures, and global review studies, such as that of World Psychiatry 2018 [4].
The questionnaire has been translated into multiple languages including French, English, Italian, German, Portuguese, Greek, Swedish, Finnish, Polish and Japanese, and has recently also been validated in Mandarin Chinese.
The mean incidence of SD among patients receiving SSRIs was 62.9%, although only 14%-22% [13,14] of these patients spontaneously reported any dysfunction. Although this is a common side effect of all SSRIs and dual-action drugs, the highest rates were reported with paroxetine for several reasons: its powerful serotonergic action, its effect on increasing prolactin and inhibiting nitric oxide, and its greater anticholinergic effect. The most common problems were reduced desire and delay in achieving orgasm. Erectile dysfunction is less common, although rates associated with paroxetine, citalopram, and venlafaxine at standard therapeutic doses were around 30%-40%. Absent orgasm or ejaculation is clearly the most poorly tolerated side effect in patients of both genders.
In contrast, the rates of SD caused by mirtazapine, bupropion, and agomelatine are lower than those of SSRIs [1], due to their different mechanisms of action: mirtazapine blocks postsynaptic 5- HT2 receptors (the stimulation of which has been closely related with the development of ejaculation and orgasm changes); bupropion has a dopaminergic/adrenergic action; and agomelatine is a melatonin receptor agonist and HT2C antagonist.
An American group led by Anita Clayton (University of Virginia) also used a specific questionnaire, the Changes in Sexual Function Questionnaire (CSFQ) [12]. After screening a population sample with inclusion and exclusion criteria, their results were similar to the Spanish series, and contributed data on the low prevalence of bupropion associated SD, lower than 10% [15].
There appear to be differences between genders. Males over 40 years of age generally tolerate SD worse than females [3], but this is not observed in younger individuals, and at least one third of patients considered discontinuing treatment for this reason. In contrast, other patients, such as those with premature ejaculation, accepted their SD well: the delay in achieving ejaculation experienced after starting antidepressant treatment “normalized” their ejaculatory time. Surveys conducted in large patient series report discontinuation figures between 41.7% and 50.8% [14].
Although reports from medical records of antidepressant use refer to a very low incidence of SD (2%-16%) [16], the real incidence almost always goes unnoticed unless targeted interviews are conducted to explore this adverse effect. In studies in which patients were directly asked about their sexual functioning after starting treatment, only 14%-20% reported SD spontaneously, and the rest concealed it from their doctor, even if they suspected that this could be due to the medication [13,14].
In clinical practice, doctors are often unaware and unable to manage the appearance of these side effects. This approach would avoid the possibility of patients discontinuing treatment, particularly among those who require it at long-term.
With regards to clinical management, the treatment of SD caused by antidepressants has not been examined using controlled and extensive studies. Scant data are available to guide clinicians on the most appropriate choice in each case, and no controlled clinical trials have been performed in this area.
In the ELIXIR study [17] clinicians were asked about their treatment choice in cases of SD due to antidepressants. The results indicated that most psychiatrists opted for no intervention, and preferred to wait for spontaneous remission, and a small percentage chose to switch treatment or to add an antidote. In Spain, [3] a clinical study with more than 2,000 patients found a rate of SD of over 80% in patients who were receiving SSRIs or dual-action agents. Spanish doctors opted to wait for spontaneous remission in 25% of cases or else switched to bupropion or agomelatine in 30% of cases. Results were better for agomelatine (80% reduction in SALSEX scores [18,19]. The use of PDE5 inhibitors, such as sildenafil or weekend drug holidays, was very rare.
The experience in our country shows that while patients with at least 3 months following can benefit from switching to other non-serotonergic antidepressants in order to Improve SD, they can be at risk of clinical deterioration or depressive relapses in one in three cases. Therefore, new therapeutic alternatives must be found. In the absence of meta-analyses and specifically designed clinical trials, the recommendations obtained from analyzed data from published studies [18] suggest different levels of evidence including switching to another antidepressant (agomelatine, bupropion or mirtazapine), weekend drug holidays (useful in the absence of orgasm), and PD5 Inhibitors among others.
Due to the lack of an effective treatment with favorable, persistent results in antidepressant treatment- emergent SD, newer products with different mechanisms of action that could have less effect on sexual functioning must be explored. One of them is vortioxetine, which has a multimodal mechanism of action on different receptors, with full agonist effect on 5-HT1A, partial antagonism on 5-HT1B, and antagonist effects on 5HT1D, 5-HT3 and 5-HT7, in addition to displaying a dopaminergic, adrenergic, histaminergic, and cholinergic effects. Given the lack of current evidence regarding this topic, specific studies in routine clinical practice and in carefully selected populations are required to confirm these preliminary data.
2. Study Rationale:
Vortioxetine is a recently developed antidepressant with a novel mechanism of action. Data from clinical trials for registration purposes suggest a neutral, or even beneficial, effect on sexual functioning in depressive patients receiving vortioxetine [20,21], which has since been proved again in a recent phase IV randomized study [22]. A switching study showed that vortioxetine is a safe and effective switch therapy for treating SSRI-induced sexual dysfunction in adults with well-treated MDD [23]. Also, improvement in sexual dysfunction with vortioxetine or escitalopram may be influenced by prior SSRI usage, sex, age (≤45 years, women) and history of one to three major depressive episodes [24]. For example, a recent study in postmenopausal transition women observed less antidepressant induced SD with vortioxetine when compared to paroxetine [25], although the exact dose was not specified. However, overall limited data have been published to date regarding the effects of this antidepressant on sexual functioning.
Vortioxetine with this novel mechanism of action could have some implications in less sexual dysfunction. In a recent randomized, double-blind trial with vortioxetine (15–20 mg/day), treatment-emergent sexual dysfunction symptoms were not significantly different versus placebo using the ASEX Scale [20]. In addition, in another short (8 weeks) randomized, double blind clinical trial with vortioxetine 10–15 mg/day in depressed patients ASEX total scores were similar across groups [26]. In an open-label, flexible-dose (2.5–10 mg/day), 52-week extension study that evaluated the long-term safety and tolerability of vortioxetine, the rate of adverse events related to sexual dysfunction was low [27]. Moreover, a recent prospective epidemiological study shows that females (but not males) treated with vortioxetine presented better sexual function than those treated with SSRIs or Duals and a lower risk of sexual dysfunction. [28]
In a recent review [29], authors stated that vortioxetine is well tolerated, but is associated with significantly increased sexual dysfunction at a dosage of 20 mg; however, vortioxetine was shown to improve previous-treatment-emergent sexual dysfunction in patients with well- treated MDD to a greater degree than escitalopram. These studies show some limitations when studying this topic, such as lack of a control group with sexually active patients in a naturalistic setting, so further specific studies are needed.
Therefore, the aim of this study is to determine the frequency and intensity of sexual dysfunction (SD) after a switching to vortioxetine from another antidepressant due to TESD.
3. Study Objectives:
3.1. Primary Objective:
- To analyze the effectiveness of the antidepressant switch strategy to vortioxetine for the improvement of sexual dysfunction (measured as Total SALSEX Score) after 3 months of follow-up in patients with poor tolerance or risk of treatment discontinuation (the risk of discontinuation is defined as a score ≥ 2 in item 5 of the SALSEX).
3.2. Secondary Objectives:
- □
- To study the individual tolerance and risk of treatment discontinuation using the PSRSexDQ-SALSEX questionnaire at baseline and to the endpoint.
- □
- To determine differences in SD between males and females at baseline and to the endpoint.
- □
- To determine differences in SD between different age groups at baseline and to the endpoint.
- □
- To determine differences in SD between different levels of severity of depression at baseline and to the endpoint.
- □
- To determine differences in SD between different dosages of vortioxetine (10-20 mg)
4. Methodology
4.1. Design
This is a naturalistic, prospective, pragmatic, open label, one group study design in a routine clinical practice setting measuring the outcomes of the antidepressant switching to vortioxetine in patients with previous antidepressant -related poorly tolerated SD.
4.2. Study Subjects
4.2.1. Sample Size Calculation
To analyse the effectiveness of the antidepressant switch strategy to vortioxetine for the improvement of sexual dysfunction and considering the frequency of SD of different antidepressants of previous studies, the sample size necessary for the difference between proportions was calculated. Assuming a 95% confidence level and a power of 80%, according to data from previous studies in which the proportion of patients with SD on SSRIs (70%) and 45% on the dual-action drugs [2,3,39] and based on recent studies with the same design, prospective open label one group study, in patients with SD switched to desvenlafaxine showing 44% of SD after the switching [31], the required sample size is 124 patients, with a sample size of 62 males and 62 females patients in each group in order to observe possible gender differences.
4.2.2. Inclusion Criteria:
- □
- Patients who showed at least moderate intensity in the total score of SALSEX ≥6 (including ≥ 2 in item 5, tolerance of sexual dysfunction).
- □
- Patients with normal sexual function prior to taking antidepressants (Normal sexual function was defined as an absence of habitual dysfunctions of sufficient intensity to cause subjective discomfort in the patient in the areas of desire, orgasm or sexual arousal that would require specialized attention, with previous regular, satisfactory sexual and/or autoerotic practices).
- □
- Patients sexually active treated with an antidepressant for at least 2 months. This time requirement was included to avoid false negatives, as some symptoms do not appear until after this period (loss of sexual desire or erectile/vaginal lubrication dysfunction).
- □
- Previous antidepressant-related sexual dysfunction. Patients were switched to vortioxetine only if there were symptoms of sexual dysfunction that were considered associated with the previous antidepressant.
- □
- Treatment exclusively with antidepressants used within approved label (including SSRIs, SNRIs). Combined treatment with benzodiazepines at low clinical doses was permitted (less than 20 mg clorazepate or equivalent).
- □
- Patients with at least partial response with a maximum score on the Clinical Global Impression Scale of Depression (CGI-D) ≤ 3- mild depression.
4.2.3. Exclusion Criteria:
- □
- SD prior to starting administration of the antidepressant. (Only a mild decrease in libido before starting antidepressant treatment was permitted, as this is considered a symptom of depression itself, although worsening of libido because of treatment was considered as an adverse effect).
- □
- Combination of the antidepressant with antipsychotic drugs or mood stabilizers.
- □
- Use of hormones or any other medication with known capacity to interfere in sexual relationships (antiepileptic drugs, H2 antagonists, recent introduction of contraceptives as concomitant therapy, β-blockers, opiates, and antihypertensive drugs).
- □
- Medically significant intercurrent diseases clearly affecting sexual function.
4.2.4. Switching Procedures:
Switching from previous antidepressant therapy (SSRI, SNRI) was made with no abrupt interruptions. Doses were increased up to 10 mg/day during the first week and , following a naturalistic design, an increase up to 15-20 mg/day of vortioxetine was allowed after the first week. Previous antidepressants were simultaneously gradually tapered down by halving the dose for the first week before complete withdrawal.
4.2.5. Sites
All patients were attended by psychiatrists working in Salamanca's (Spain) complete outpatient network, which comprises five outpatient units in total.
4.3. Variables
4.3.1. Primary Variable:
- □
- The Severity of global SD was measured using the SALSEX total score (scoring from 0= no sexual dysfunction to 15= maximum sexual dysfunction) at baseline and to the endpoint. The severity of each individual dimension of sexual functioning (reduced sexual desire, delay of orgasm, anorgasmia and arousal difficulties such as erectile dysfunction or vaginal lubrication) was measured with a Likert scale (0= no SD; 3= maximum SD) of the items 1-4 of the SALSEX questionnaire) at baseline and at endpoint visit.
4.3.2. Secondary Variables:
- □
- To study the individual acceptance of SD and risk of treatment discontinuation, we used the score of the item 5 of the SALSEX questionnaire (0= no risk of discontinuation; 3= maximum risk) at baseline and at endpoint visit.
- □
- To determine differences in SD that varied across the severity of depression we used the Clinical Global Impression-Improvement (CGI-I) scale for depression, and the CGI-S for sexual functioning at baseline and at endpoint visit.
4.4. Data Collection and Analysis
4.4.1. Measurement Scales
PRSexDQ- SALSEX Questionnaire:
The SALSEX questionnaire for the Evaluation of Psychotropic-Related Sexual Dysfunction was used to measure and evaluate the prevalence and severity of SD (validated in 2008 by Montejo et al. [10]). in a population with depressive disorders). This questionnaire was administered at baseline and during the follow-up period (within 3 months after the initial visit). It is included in an annex at the end of this paper. The SALSEX questionnaire is meant to be administered during a direct clinical interview to collect information on whether treatment-related SD is detected, and if it is present, note whether the patient reported the SD spontaneously or not. The degree of SD is evaluated according to 4 items, for each of the possible manifestations of SD: 1) sexual desire; 2) delayed orgasm; 3) absent orgasm; 4) erection-lubrication. A fifth item evaluates the acceptance of SD, if present. Each of these items is scored between 0 (no problem) and 3 (maximum intolerance).
The presence and severity of SD is evaluated according to the total score and individual item scores of the questionnaire, using the following criteria:
- ○
- No SD: Total score of 0 or 1, only if item 1 is evaluated as a slight loss of libido (which is equivalent to a score of 1 on that item).
- ○
- SD present: Total score of 2-15, or total score of 1 if any item except for item 1 (desire) is scored 1.
- □
- Mild SD: 1-5 points, provided no item scores ≥2 points and item 5 (tolerability) is not >1.
- □
- Moderate SD: 6-10 points, provided that no item scores ≥3 points or else <6 points if any item = 2 and provided that item 5 (tolerability) is not >2.
- □
- Severe SD: 11-15 or <11 points if any item = 3 or whenever item 5 (tolerability) = 3.
Clinical Global Impression Scale, severity subscale, applied to sexual dysfunction (CGI-S-SD) to assess the DS severity at baseline
Clinical Global Impression Scale, improvement subscale, applied to sexual dysfunction (CGI-I-SD) to assess the clinical effectiveness of the intervention, administered in the follow-up visit (performed within 3 months after the baseline visit)
Clinical Global Impression scale, severity subscale (CGI-S), applied to the psychiatric disease for which the antidepressant treatment is administered, to assess severity at baseline
Clinical Global Impression scale, improvement subscale, CGI-I) to assess the clinical effectiveness of the intervention, administered in the follow-up visit (performed within 3 months after the baseline visit)
Adverse Events Assessments:
Adverse events (including pre-treatment adverse events) had to be recorded on an Adverse Event Form. The investigator had to provide information on the adverse event, preferably with a diagnosis, or at least with signs and symptoms; start and stop dates (and start and stop time if the adverse event lasted less than 24 hours); severity; causal relationship to the IMP; action taken; and outcome. If the adverse event was not related to the IMP, an alternative etiology had to be recorded, if available. If the adverse event was an overdose, the nature of the overdose had to be stated (for example, medication error, accidental overdose, or intentional overdose). If the adverse event was serious, this had to be indicated on the Adverse Event Form. The sponsor/investigator had to comply with all national rules and regulations concerning the reporting of Serious Adverse Events as defined in the ICH GCP guidelines and forward a copy of any such reports to Lundbeck, and to report all AE/ADRs to Lundbeck immediately. ICH.
4.4.2. Visits
Information will be collected on two visits:
- □
- Baseline visit (V1): treatment initiation switch if prompted by poorly tolerated SD
- □
- Visit 2 (V2) conducted within 3 months of follow-up after after switching antidepressant at baseline visit
4.4.3. Treatment
Patients switched treatments only if the clinician and/or the patient considered that some treatment modification was necessary to improve SD due to the use of the current antidepressant, which was replaced by vortioxetine with the patient's consent.
4.4.4. Ethical and Legal Considerations
Patient Information
Informed consent was obtained from the patient, and the physician involved the patient and his/her partner in the study, since their collaboration was deemed essential.
Confidentiality
Collection, processing, and transfer of study data were conducted in compliance with the provisions of the Spanish Organic Law 15/1999 on Personal Data Protection. All information on the identity of participating patients was treated as confidential for all purposes. The identity of the patients was not to be disclosed or shared, except when necessary for their treatment, evaluation, follow-up, and safety. The patient was identified in the data collection forms with a patient number. The collected data were entered in a database following a procedure that ensured total dissociation between these data and the identity of the patient.
5. Data Analysis
5.1. Evaluation Criteria and Data Management
Case report forms (CRFs) were individually reviewed to ensure that all data had been collected or otherwise a reason had been provided. Numerical values were assigned to the open text fields, particularly for adverse reactions. Incorrect and incomplete CRFs, and those that had not been completed according to the protocol were rejected or returned to the corresponding investigator for review and correction.
CRF data considered valid was entered in a database created for this purpose with appropriate safety measures and internal coherence rules, after which any cases with anomalous or inconsistent values were reviewed.
5.2. Evaluation Criteria
Cases rejected due to serious inconsistencies, or incorrect or incomplete data were not evaluated. All patients were to be described in the participant's biodemographic characteristics section, indicating the total number of patients included, the total number of patients excluded or who had discontinued treatment early (along with the reason), and the total number of evaluable patients. Pharmacovigilance assessment was based on all recruited patients, except for those cases rejected due to incorrect data or those who did not return to any visit after baseline.
Evaluations Performed:
General characteristics of patients included in the study, including biodemographic data and their psychiatric diagnosis were described. The primary analysis was conducted by describing the percentage of patients who had SD during previous treatment and after switching to vortioxetine with their respective confidence intervals. Total SALSEX score, frequency and intensity of each item of the SALSEX (Items 1-5) was compared at endpoint vs baseline.
Testing of the hypothesis were considered significant when the corresponding p-value was less than 5% (α=0.05) for two-tailed tests. All operations were performed on PC-type compatible computers, protected by strict measures controlling for access and quality, using the SPSS package, version 23.0 for Windows or a subsequent version.
Measures of central tendency and dispersion for quantitative variables were determined throughout the study. Normality of distribution of continuous variables were tested using the Kolmogorov-Smirnov test for one sample, so that the data were subsequently analyzed based on the results obtained. The descriptive analysis included categorical qualitative variables measured using frequencies and percentages.
For the inferential statistical analysis, testing of the hypothesis were evaluated using the appropriate parametric test for variables with normal distribution, or non-parametric tests for those with non-normal distribution. Throughout the study, it was of interest to examine differences between the patient groups in the characteristics evaluated. When experimental data were measured using continuous scales that follow a normal distribution, the appropriate procedure was the Student's t test for 2 independent samples. If these scales did not have a normal distribution, a non-parametric Mann-Whitney U test was used. If the difference of means was to be studied between more than 2 groups, the corresponding parametric or non- parametric test was used.
The Pearson Chi-square test for independence and Fisher’s exact test were used to compare independence between categorical variables.
6. Project Development Stages
The study was conducted in the Department of Psychiatry of the Hospital Universitario de Salamanca, with the participation of 10 investigators from 5 Mental Health outpatient Units located in Salamanca, which provides care for a population close to 300,000 inhabitants.
The study was performed in 3 phases between July 2019 and September 2022. The recruitment was delayed due to COVID 19.
All administrative permissions, including submission of the protocol for qualification by the Spanish Agency of Medicines, agreement from the Research Ethics Committee of the Salamanca Health Area, and agreement from the Government of Castile and Leon were obtained in 2019. Investigators’ meeting was carried out in January 2020 for an explanation of the protocol, standardization of procedures, training, and practical administration of the SALSEX questionnaire to reduce inter-investigator variability. The collection of baseline socio-demographic data was obtained and included in the CRF, as well as all selection criteria, presence, and severity of the psychiatric disease (measured using the CGI-S scale), presence and severity of SD (measured with the SALSEX questionnaire and the CGI-S-SD), and randomized therapeutic strategy of antidepressant switch for the management of SD associated with antidepressant treatment.
Clinical follow-up of patients with SD detected at baseline visit included the measurement, within 3 months after baseline, of the effectiveness of the intervention using the SALSEX scale (lower scores indicate improvement), and a Clinical Global Impression-Improvement for depression (CGI-IDep) and for sexual functioning (CGI-ISex) after intervention. A determination of the number of patients withdrawing from the study due to lack of efficacy, adverse effects or loss to follow-up was performed.
7. Results
103 patients treated with an antidepressant who had poorly tolerated sexual dysfunction after initiation of treatment and who met the inclusion and exclusion criteria of the protocol were switched to vortioxetine. The response to the SALSEX scale was analyzed in 74 patients from whom data were obtained at the follow-up visit (3 months after the baseline). 29 out of 103 patients (28,15%) were lost to the study with no data at Visit 2.

Table 1.
Clinical and sociodemographic characteristics of patients switched to vortioxetine.
| n=74 | |
| Age (years) | 43.1 ± 12.65 |
| < 30 , n (%) | 14 (18.9) |
| 30-40, n (%) | 21 (28.4) |
| 40-50, n (%) | 17 (23.0) |
| > 50, n (%) | 22 (29.7) |
| Gender (Males), n (%) | 40 (54.1) |
| Gender (Females), n (%) | 34 (45.9) |
| Duration of treatment (months) (Baseline) | 19.53 ± 37.27 |
| Duration of treatment (meses) (Follow-up) | 3.21 ± 1.17 |
| Dosage (mg/d) (Follow-up) | 13.11±4.03 |
| SALSEX Total Score at Baseline | 10.32 ± 2.73 |
| SALSEX Total Score at Follow-up | 3.78 ± 3.68 |
7.1. Previous Antidepressant Treatment at Baseline
At baseline, patients with sexual dysfuntion were taking venlafaxine 6.8%, mean dosage 177 mg/day ± 73.02; escitalopram 25.7%, 14.74mg/day ± 3.90; citalopram 5.4%, 23.75 mg/day ± 7.50 ; paroxetine 9.5%, 22.86 mg/day ± 7.56 ; sertraline 18.9%, 78.57 mg/day ± 37.80; fluoxetine 8%, 23.33 mg/day ± 8.17; duloxetine 10.8%, 67.50 mg/day ± 21.21; clomipramine 4.1% , 75.00 mg/day ± 0.000 and desvenlafaxine 10.8%, 78.57 mg/day ± 56.70 ( Figure 1)
7.2. SALSEX Scale Total Score of Sexual Dysfunction.
The total score of Sexual Dysfunction (SD) measured with the SALSEX scale (ranging from 0= no sexual dysfunction to 15= strong SD) at baseline visit in which patients were taking an antidepressant was 10.32 (SD 2.73). The total score of SALSEX scale in Follow-up visit (3 months after switching to vortioxetine) was 3.78 (SD 3.68). Highly significant differences were found between the global SALSEX score at baseline and after switching to vortioxetine (t=12.279, p<0.001),
At baseline, 4 % of patients had mild sexual dysfunction (SD) (n=3), 20.3% of patients with moderate (n=15) and 75.7% of patients with severe DS (n=56).
SD was spontaneously reported in 47.3% of patients (n=35), compared to 52.7% (n=39) who did not.
Significant differences were found in the total score of the SALSEX scale between males and females, higher in female at baseline (p=0.021), and also after follow-up (p=0.021) (Table 2). There were no differences in age, treatment time to baseline, treatment time to visit 2 or dose.
7.3. Clinical Global Impression of Severity of Depression (CGI-D)
Analyzing the CGI-D at baseline, 81.1% of the patients switched to vortioxetine felt depressed (35.1% mildly ill, 20.3% borderline, 20.3% moderately ill and 5.4% markedly ill). After treatment with vortioxetine, 39.2% felt no change, but 58.1% of patients showed an improvement (Figure 2).
7.4. Clinical Global Impression of Severity of Sexual Dysfunction (CGI-SEx)
Analyzing the CGI-Sex at baseline, 100% of patients had sexual dysfunction (6,9% borderline ill, 6.8% mildly ill, 43.8% moderately ill, 28.8% markedly ill, 9.6% severely ill and 4.1% extremely sick). After switching to Vortioxetine, 83.81% of patients felt an improvement (43.2% felt greatly improved). (Figure 3)
After switching to vortioxetine, 18.9% did not show SD (n=14), 44.6% had mild SD (n=33), 14.9% moderate (n=11) and 14.9% severe (n=11). 5 patients (6,7%) did not respond to item 5 of tolerability and that is why they were not classified in any group of the scale, although they presented values of 0 points in the rest of the items.
7.5. SALSEX Scale by Items from Baseline to Follow-Up
Analyzing the items of SALSEX at baseline, 85% of moderate/severe decreases in sexual desire were observed, 86.5% showed moderate/intense orgasm delay, 51.4% showed anorgasmia frequently and 17.6% always/almost always. A similar issue happened with arousal difficulties (Figure 4)
At the follow-up visit after taking vortioxetine 43.2% of patients no longer showed any problem of sexual desire and 36.5% showed a mild decrease. A similar improvement in orgasm delay, anorgasmia and arousal dysfunction was observed at follow-up. (Figure 5 and Table 3)
At Follow-up visit, a general tendency to decrease the severity of sexual dysfunction from moderate/severe to becoming mild or absent in all items of the SALSEX was observed in all items (Table 4).
After switching to vortioxetine, a clinically significant improvement (p<0.001) was observed in sexual desire, delayed orgasm, anorgasmia, and arousal difficulties. Additionally, tolerability of sexual dysfunction improved significantly in patients who maintained some degree of sexual dysfunction at the follow-up visit. (Figure 6)
7.6. Sexual Dysfunction and Dosages of Vortioxetine
Regarding differences in the total SALSEX score in the Follow-up for patients switched to vortioxetine, no significant differences were found comparing the dose administered to patients, although it could be observed at the descriptive level that there was an increase in the SALSEX score as the dose increased. (Figure 7)
7.7. Clinical Outcomes after Switching to Vortioxetine
Of those switched to vortioxetine (n=103) , 70.7% of them continued treatment (n=65) after three months, 2 patients voluntarily abandoned due to lack of efficacy, the investigator decided to withdraw the treatment due to lack of efficacy in 2 patients. Five patients voluntarily abandoned due to adverse effects and in 2 patients the investigator withdrew the treatment for one or more side effects. Fourteen patients (15.2%) received were not evaluable due to lack of sexual activity. There is no information on the outcome of the strategy of 13 patients. Finally, 65/74 patients switched to vortioxetine continued treatment after the follow-up visit (83.3%).
8. Discussion
8.1. Value of the Study
Treatment-emergent sexual dysfunction (SD) is one of the most frequent and persistent adverse effects of antidepressant medication. SD secondary to SSRIs occurs in >60% in sexually active patients and >80% in healthy volunteers, this causing treatment discontinuation in >35% of patients [3]. However, this factor is rarely addressed in routine examinations, and only 15%-30% of these events are spontaneously reported. A strategy of switching to other non-serotonergic drugs (bupropion, agomelatine [32], mirtazapine) involves a potential risk of relapse or clinical worsening due to a lack of serotonergic activity, as well as new troublesome side effects [8].
New antidepressants appear to have less impact on sexual function due to their reduced serotonergic effect (desvenlafaxine) [31,33] or their multimodal mechanism of action like vilazodone [34]
Such is the case for vortioxetine, a recently developed antidepressant with a novel and promising receptor-binding profile [35]. Data from clinical trials for registration purposes suggest a neutral, or even beneficial, effect on sexual functioning in depressive patients receiving vortioxetine [20,21,36]. However, data from clinical trials are characteristically unreliable when it comes to determining SD incidence, as they are derived from biased samples, sexually inactive patients, or short treatment periods. Limited data have been published to date on the effects of this antidepressant on sexual functioning in routine clinical practice.
In our study, we wanted to find out if switching to vortioxetine proved to be an effective strategy when dealing with antidepressant induced SD. There is to our knowledge only one very recent observational study in a naturalistic setting that explored switching to other antidepressants with a non-serotoninergic mechanism of action as a measure for improving antidepressant induced SD, that included vortioxetine as a possible option [37]. This Italian retrospective cohort study tried to analyze several possible solutions for antidepressant induced SD and, among several options, found vortioxetine to be the most common and effective one, particularly at 10 mg. Although the sample was small (n=30) and was limited to male population, these results match our own: vortioxetine improved SD consistently when compared to our patient's previous antidepressants, with 83.81% of patients feeling improved (43.2% feeling greatly improved). If we compare these results to a similar switching study made by our working group with desvenlafaxine [31], which achieved and improvement rate of 17.7% after the switch, it becomes clear that vortioxetine seems to be far superior in preserving sexual function than other antidepressants.
This becomes clearer if we look at other studies with non-serotoninergic antidepressants like agomelatine. In a study comparing agomelatine to venlafaxine as a first prescribed drug to depressed patients [32], agomelatine demonstrated a lower SD incidence rate but overall differences did not exceed 8% of patients.
Regarding our secondary objectives, in our sample, we had an higher rate of SD in females than in males both in baseline and at follow-up, but no differences at all were found in SD among age groups. A recent study by Jacobsen saw greater improvement of SD in women under the age of 45 with vortioxetine [24] but our results did not match these findings.
We should also address that switching to vortioxetine did not compromise at all antidepressive efficacy either: the CGI-S for depression didn't change from baseline to follow-up, or even improved in some cases.
The degree of SD improvement with vortioxetine seems to be highly dependent on dosage: lower doses like 10 mg are more beneficial for SD than higher ones like 15 or 20 mg across several studies [23,37,38,39,40]. Numerically, our study correlated higher SALSEX scores to higher doses (but even then, lower than with the previous drug) although this was not statistically significant probably due to a lower sample number among dosing subgroups than we originally intended.
Previous studies have already shown vortioxetine having a minor rate and intensity of SD when compared to SSRI. For example, a recent double-blind clinical trial was conducted in healthy volunteers comparing the sexual dysfunction associated with the use of paroxetine (20 mg /day), versus vortioxetine 10 and 20 mg/day and placebo for 5 weeks [22], finding the 10 mg vortioxetine dose caused less SD than paroxetine. This difference was also somewhat present at 20 mg vortioxetine dose, but it did not reach statistical significance due to apparent subject noncompliance. Overall, these results are in concordance with previous comparisons done in depressed patients with vortioxetine and escitalopram [23], confirming and even improving on the previously reported SD incidence rates in the vortioxetine drug label analysis [38].
However, these studies used the CSFQ-14 and did not compare the impact of vortioxetine across several sexual dimensions to other antidepressants. But a recent study on Spanish population did [28] albeit with a different outcome measure than in this study. Our findings, measured through the SALSEX scale, point to vortioxetine having the potential to improve all the previously affected sexual dimensions, but improving decreased libido (in some cases, even restoring it completely) and delayed orgasm slightly more than anorgasmia and arousal dysfunction.
All these results probably contributed to the increase of tolerability in sexual dysfunction measured by the SALSEX score, which was observed in patients that retained some sort of SD after switching. This can lead us to believe the risk of treatment discontinuation due to SD can be greatly reduced after switching to vortioxetine.
8.2. Limitations
As this is an observational study, the data obtained may not be representative of the general population, although an attempt to minimize this bias has been made with a calculated sample size of N = 124 patients. Due to difficulties in the recruitment for COVID-19 pandemic, the initial calculated sample size was not reached out, Nevertheless, significant differences have been found with this sample of 74 patients at follow-up visit.
Information will be obtained on the decision to switch treatment; no information will be obtained on other possible therapeutic alternatives. This information will have to be obtained using different designs in subsequent phases.
9. Conclusions
According to our primary objective, the global Sexual Dysfunction measured with the SALSEX Scale, decreased significantly from baseline visit to follow-up visit (3 months). Switching to vortioxetine is an effective and reliable strategy to treat patients with poorly tolerated previous antidepressant -related sexual dysfunction and at risk of treatment discontinuation in real-life clinical settings. After switching to Vortioxetine, 83.81% of patients improved their sexual function.
All components of sexual dysfunction (decreased libido, orgasmic functioning, and arousal difficulties) improved significantly after switching to vortioxetine, especially decreased libido. Individual tolerance and risk of treatment discontinuation improved using the PSRSexDQ-SALSEX questionnaire from baseline to endpoint visit.
Both sexes improved significantly with vortioxetine, although females had a higher rate of SD than males both at baseline and at follow-up.
No significant differences in SD were found between different dosages of vortioxetine although there was an increase in the SALSEX score as the dose increased mainly with 20 mg/day.
Most patients (83.3%) who switched to vortioxetine continued treatment after the 3 months follow-up visit. Additionally, 58.1% of patients showed an improvement in depressive symptoms from baseline visit.
Author Contributions
Conceptualization A.L.M.; methodology, A.L.M., L.M. and N.G., formal analysis, N.G.; investigation, J.B., G.B., R.F.-O., M.T.G., A.J., A.P.-U., N.P. and J.L.V.; resources, A.L.M.; data curation, N.G., A.P.-U. and A.L.M.; writing original A.L.M.; draft preparation, A.L.M., N.G.; writing—review and editing, A.P.-U. , R.d.A and A.L.M.; funding acquisition, A.L.M.
Funding
This study was financed by Lundbeck by an unrestricted medical grant.
Conflicts of Interest
Angel L. Montejo has received consultancy fees or honoraria/research grants in the last 5 years from Eli Lilly, Forum Pharmaceuticals, Rovi, Servier, Lundbeck, Otsuka, Janssen Cilag, Pfizer, Roche, Instituto de Salud Carlos III, and the Junta de Castilla y León. The rests of the authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Baldwin, D.S.; Foong, T. Antidepressant Drugs and Sexual Dysfunction. Br J Psychiatry 2013, 202, 396–397. [CrossRef]
- Serretti, A.; Chiesa, A. Treatment-Emergent Sexual Dysfunction Related to Antidepressants: A Meta-Analysis. J Clin Psychopharmacol 2009, 29, 259–266. [CrossRef]
- Montejo AL, Calama J, Rico-Villademoros F, Montejo L, González-García N, Pérez J; SALSEX Working Study Group. A Real-World Study on Antidepressant-Associated Sexual Dysfunction in 2144 Outpatients: The SALSEX I Study. Arch Sex Behav. 2019 Apr;48(3):923-933. [CrossRef]
- Montejo, A.L.; Montejo, L.; Baldwin, D.S. The Impact of Severe Mental Disorders and Psychotropic Medications on Sexual Health and Its Implications for Clinical Management. World Psychiatry 2018, 17, 3–11. [CrossRef]
- Alvarez, E.; Perez, V.; Artigas, F. Pharmacology and Clinical Potential of Vortioxetine in the Treatment of Major Depressive Disorder. Neuropsychiatr Dis Treat 2014, 10, 1297–1307. [CrossRef]
- Abler, B.; Seeringer, A.; Hartmann, A.; Grön, G.; Metzger, C.; Walter, M.; Stingl, J. Neural Correlates of Antidepressant-Related Sexual Dysfunction: A Placebo-Controlled fMRI Study on Healthy Males Under Subchronic Paroxetine and Bupropion. Neuropsychopharmacology 2011, 36, 1837. [CrossRef]
- Clayton, A.H.; Croft, H.A.; Handiwala, L. Antidepressants and Sexual Dysfunction: Mechanisms and Clinical Implications. Postgrad Med 2014, 126, 91–99. [CrossRef]
- Montejo, A.L.; Prieto, N.; de Alarcón, R.; Casado-Espada, N.; de la Iglesia, J.; Montejo, L. Management Strategies for Antidepressant-Related Sexual Dysfunction: A Clinical Approach. J Clin Med 2019, 8, 1640. [CrossRef]
- Montejo, A.L.; Montejo, L.; Navarro-Cremades, F. Sexual Side-Effects of Antidepressant and Antipsychotic Drugs. Curr Opin Psychiatry 2015, 28, 418–423. [CrossRef]
- Montejo, A.L.; Rico-Villademoros, F. Psychometric Properties of the Psychotropic-Related Sexual Dysfunction Questionnaire (PRSexDQ-SALSEX) in Patients with Schizophrenia and Other Psychotic Disorders. J Sex Marital Ther 2008, 34, 227–239. [CrossRef]
- McGahuey, C.A.; Gelenberg, A.J.; Laukes, C.A.; Moreno, F.A.; Delgado, P.L.; McKnight, K.M.; Manber, R. The Arizona Sexual Experience Scale (ASEX): Reliability and Validity. J Sex Marital Ther 2000, 26, 25–40. [CrossRef]
- Clayton, A.H.; McGarvey, E.L.; Clavet, G.J. The Changes in Sexual Functioning Questionnaire (CSFQ): Development, Reliability, and Validity. Psychopharmacol Bull 1997, 33, 731–745.
- Montejo-González, A.L.; Llorca, G.; Izquierdo, J.A.; Ledesma, A.; Bousoño, M.; Calcedo, A.; Carrasco, J.L.; Ciudad, J.; Daniel, E.; De la Gandara, J.; et al. SSRI-Induced Sexual Dysfunction: Fluoxetine, Paroxetine, Sertraline, and Fluvoxamine in a Prospective, Multicenter, and Descriptive Clinical Study of 344 Patients. J Sex Marital Ther 1997, 23, 176–194. [CrossRef]
- Montejo, A.L.; Llorca, G.; Izquierdo, J.A.; Rico-Villademoros, F. Incidence of Sexual Dysfunction Associated with Antidepressant Agents: A Prospective Multicenter Study of 1022 Outpatients. Spanish Working Group for the Study of Psychotropic-Related Sexual Dysfunction. J Clin Psychiatry 2001, 62 Suppl 3, 10–21.
- Clayton, A.H.; Warnock, J.K.; Kornstein, S.G.; Pinkerton, R.; Sheldon-Keller, A.; McGarvey, E.L. A Placebo-Controlled Trial of Bupropion SR as an Antidote for Selective Serotonin Reuptake Inhibitor-Induced Sexual Dysfunction. J Clin Psychiatry 2004, 65, 62–67. [CrossRef]
- FDA Selective Serotonin Reuptake Inhibitors (SSRIs) Information. [(accessed on 01 November 2023)]; Available online: https://www.fda.gov/drugs/information-drug-class/selective-serotonin-reuptake-inhibitors-ssris-information.
- Bonierbale, M.; Lançon, C.; Tignol, J. The ELIXIR Study: Evaluation of Sexual Dysfunction in 4557 Depressed Patients in France. Curr Med Res Opin 2003, 19, 114–124. [CrossRef]
- Montejo, A.L.; Deakin, J.F.W.; Gaillard, R.; Harmer, C.; Meyniel, F.; Jabourian, A.; Gabriel, C.; Gruget, C.; Klinge, C.; MacFayden, C.; et al. Better Sexual Acceptability of Agomelatine (25 and 50 Mg) Compared to Escitalopram (20 Mg) in Healthy Volunteers. A 9-Week, Placebo-Controlled Study Using the PRSexDQ Scale. J Psychopharmacol 2015, 29, 1119–1128. [CrossRef]
- Montejo, A.L.; Prieto, N.; Terleira, A.; Matias, J.; Alonso, S.; Paniagua, G.; Naval, S.; Parra, D.G.; Gabriel, C.; Mocaër, E.; et al. Better Sexual Acceptability of Agomelatine (25 and 50 Mg) Compared with Paroxetine (20 Mg) in Healthy Male Volunteers. An 8-Week, Placebo-Controlled Study Using the PRSEXDQ-SALSEX Scale. J Psychopharmacol 2010, 24, 111–120. [CrossRef]
- Jacobsen, P.L.; Mahableshwarkar, A.R.; Serenko, M.; Chan, S.; Trivedi, M.H. A Randomized, Double-Blind, Placebo-Controlled Study of the Efficacy and Safety of Vortioxetine 10 Mg and 20 Mg in Adults with Major Depressive Disorder. J Clin Psychiatry 2015, 76, 575–582. [CrossRef]
- Jacobsen, P.L.; Mahableshwarkar, A.R.; Palo, W.A.; Chen, Y.; Dragheim, M.; Clayton, A.H. Treatment-Emergent Sexual Dysfunction in Randomized Trials of Vortioxetine for Major Depressive Disorder or Generalized Anxiety Disorder: A Pooled Analysis. CNS Spectr 2016, 21, 367–378. [CrossRef]
- Jacobsen, P.; Zhong, W.; Nomikos, G.; Clayton, A. Paroxetine, but Not Vortioxetine, Impairs Sexual Functioning Compared With Placebo in Healthy Adults: A Randomized, Controlled Trial. J Sex Med 2019, 16, 1638–1649. [CrossRef]
- Jacobsen PL, Mahableshwarkar AR, Chen Y, Chrones L, Clayton AH. Effect of Vortioxetine vs. Escitalopram on Sexual Functioning in Adults with Well-Treated Major Depressive Disorder Experiencing SSRI-Induced Sexual Dysfunction. J Sex Med. 2015 Oct;12(10):2036-48. [CrossRef]
- Jacobsen, P.L.; Nomikos, G.G.; Zhong, W.; Cutler, A.J.; Affinito, J.; Clayton, A. Clinical Implications of Directly Switching Antidepressants in Well-Treated Depressed Patients with Treatment-Emergent Sexual Dysfunction: A Comparison between Vortioxetine and Escitalopram. CNS Spectr 2020, 25, 50–63. [CrossRef]
- Callegari, C.; Ielmini, M.; Caselli, I.; Lucca, G.; Isella, C.; Diurni, M.; Pettenon, F.; Poloni, N. Paroxetine versus Vortioxetine for Depressive Symptoms in Postmenopausal Transition: A Preliminary Study. Psychopharmacol Bull 2019, 49, 28–43.
- Mahableshwarkar, A.R.; Jacobsen, P.L.; Serenko, M.; Chen, Y.; Trivedi, M.H. A Randomized, Double-Blind, Placebo-Controlled Study of the Efficacy and Safety of 2 Doses of Vortioxetine in Adults with Major Depressive Disorder. J Clin Psychiatry 2015, 76, 583–591. [CrossRef]
- Alam, M.Y.; Jacobsen, P.L.; Chen, Y.; Serenko, M.; Mahableshwarkar, A.R. Safety, Tolerability, and Efficacy of Vortioxetine (Lu AA21004) in Major Depressive Disorder: Results of an Open-Label, Flexible-Dose, 52-Week Extension Study. Int Clin Psychopharmacol 2014, 29, 36–44. [CrossRef]
- Sánchez-Sánchez F, Ponce-Buj B, Montejo-González AL, Sipán-Sarrión Y, Gimeno-Marqués A, Merino-Gámez A. Repercusión de vortioxetina sobre la función sexual frente a otros antidepresivos [Impact of vortioxetine on sexual function compared to other antidepressants]. Semergen. 2023 Jun 15;49(7):101997. Spanish. [CrossRef]
- Garnock-Jones, K.P. Vortioxetine: A Review of Its Use in Major Depressive Disorder. CNS Drugs 2014, 28, 855–874. [CrossRef]
- Clayton, A.H.; Montejo, A.L. Major Depressive Disorder, Antidepressants, and Sexual Dysfunction. J Clin Psychiatry 2006, 67 Suppl 6, 33–37.
- Montejo, A.L.; Becker, J.; Bueno, G.; Fernández-Ovejero, R.; Gallego, M.T.; González, N.; Juanes, A.; Montejo, L.; Pérez-Urdániz, A.; Prieto, N.; et al. Frequency of Sexual Dysfunction in Patients Treated with Desvenlafaxine: A Prospective Naturalistic Study. J Clin Med 2019, 8, 719. [CrossRef]
- Kennedy, S.H.; Rizvi, S.; Fulton, K.; Rasmussen, J. A Double-Blind Comparison of Sexual Functioning, Antidepressant Efficacy, and Tolerability between Agomelatine and Venlafaxine XR. J Clin Psychopharmacol 2008, 28, 329–333. [CrossRef]
- Clayton, A.H.; Reddy, S.; Focht, K.; Musgnung, J.; Fayyad, R. An Evaluation of Sexual Functioning in Employed Outpatients with Major Depressive Disorder Treated with Desvenlafaxine 50 Mg or Placebo. J Sex Med 2013, 10, 768–776. [CrossRef]
- Deardorff, W.J.; Grossberg, G.T. A Review of the Clinical Efficacy, Safety and Tolerability of the Antidepressants Vilazodone, Levomilnacipran and Vortioxetine. Expert Opin Pharmacother 2014, 15, 2525–2542. [CrossRef]
- D’Agostino, A.; English, C.D.; Rey, J.A. Vortioxetine (Brintellix): A New Serotonergic Antidepressant. Pharmacy and Therapeutics 2015, 40, 36.
- Baldwin, D.S.; Chrones, L.; Florea, I.; Nielsen, R.; Nomikos, G.G.; Palo, W.; Reines, E. The Safety and Tolerability of Vortioxetine: Analysis of Data from Randomized Placebo-Controlled Trials and Open-Label Extension Studies. J Psychopharmacol 2016, 30, 242–252. [CrossRef]
- De Luca, R.; Bonanno, M.; Manuli, A.; Calabrò, R.S. Cutting the First Turf to Heal Post-SSRI Sexual Dysfunction: A Male Retrospective Cohort Study. Medicines (Basel) 2022, 9, 45. [CrossRef]
- Kelliny, M.; Croarkin, P.E.; Moore, K.M.; Bobo, W.V. Profile of Vortioxetine in the Treatment of Major Depressive Disorder: An Overview of the Primary and Secondary Literature. Ther Clin Risk Manag 2015, 11, 1193–1212. [CrossRef]
- Takeda A Randomized, Double-Blind, Parallel Group, Placebo- and Active-Controlled, Phase 4 Study Evaluating the Effect of Vortioxetine 10 and 20 Mg/Day vs Paroxetine 20 Mg/Day on Sexual Functioning in Healthy Subjects; clinicaltrials.gov, 2018 [(accessed on 02 November 2023)]. Available online: https://clinicaltrials.gov/study/NCT02932904.
- Mattingly, G.; Brunner, E.; Chrones, L.; Lawrence, D.F.; Simonsen, K.; Ren, H. Effectiveness of Vortioxetine for Major Depressive Disorder in Real-World Clinical Practice: US Cohort Results from the Global RELIEVE Study. Front Psychiatry 2023, 13, 977560. [CrossRef]
Figure 1.
Initial antidepressant treatment at baseline.
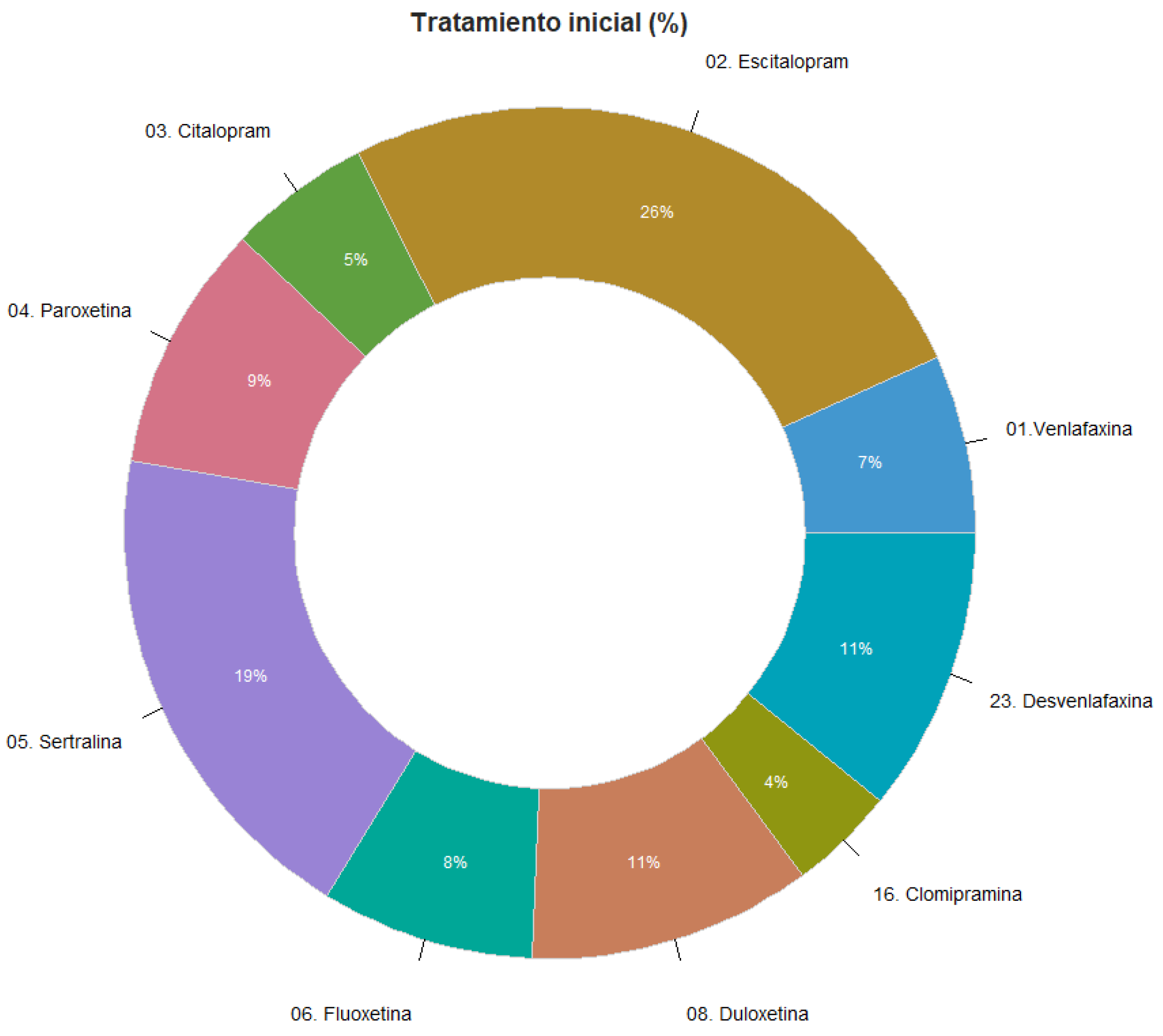
Figure 2.
Changes of the Clinical Global Impression of severity of depression (CGI-D). Baseline-Follow-up.
Figure 2.
Changes of the Clinical Global Impression of severity of depression (CGI-D). Baseline-Follow-up.
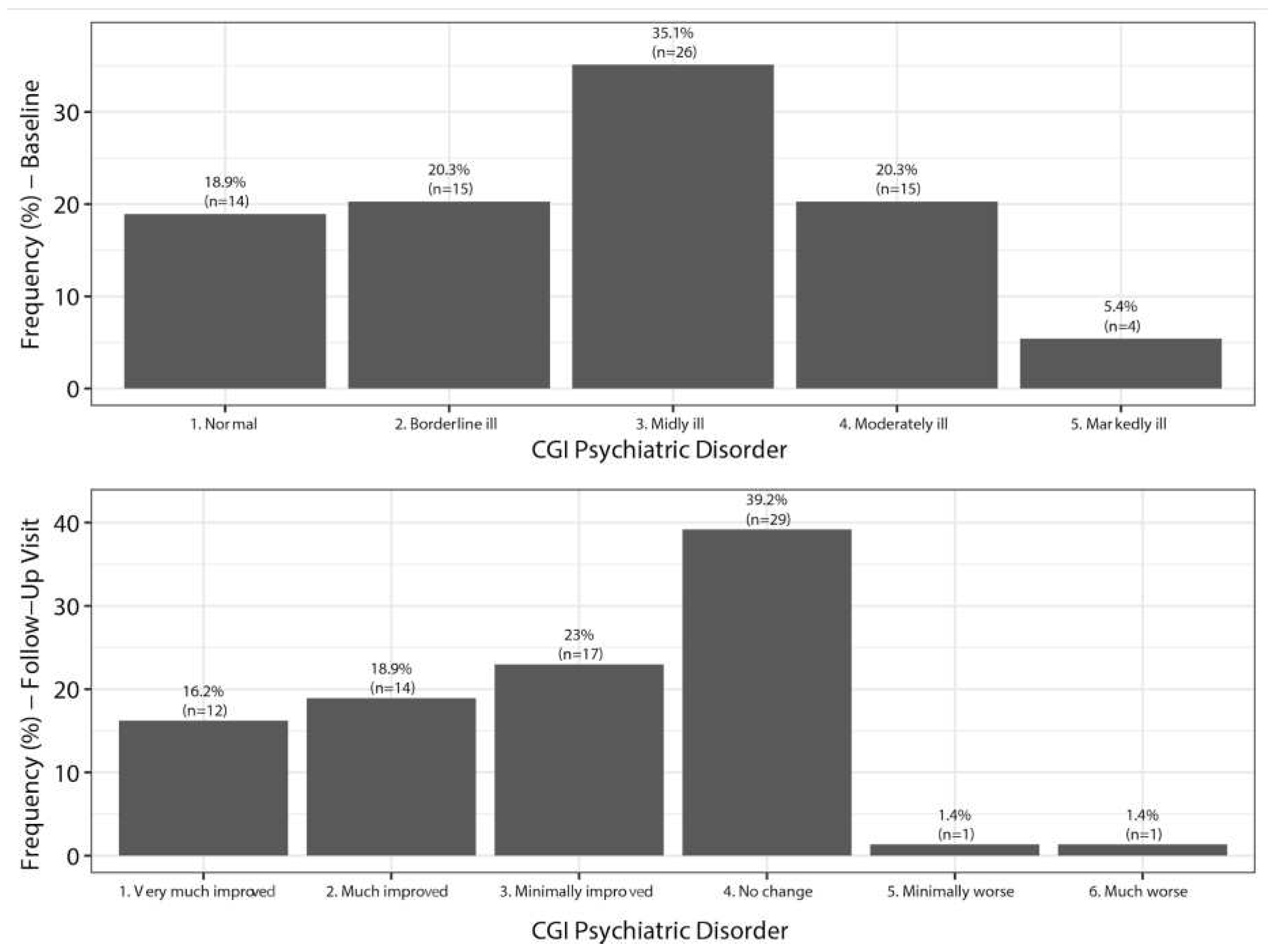
Figure 3.
Changes of the Clinical Global Impression of severity of sexual Dysfunction (CGI-Sex). Baseline-Follow-up.
Figure 3.
Changes of the Clinical Global Impression of severity of sexual Dysfunction (CGI-Sex). Baseline-Follow-up.
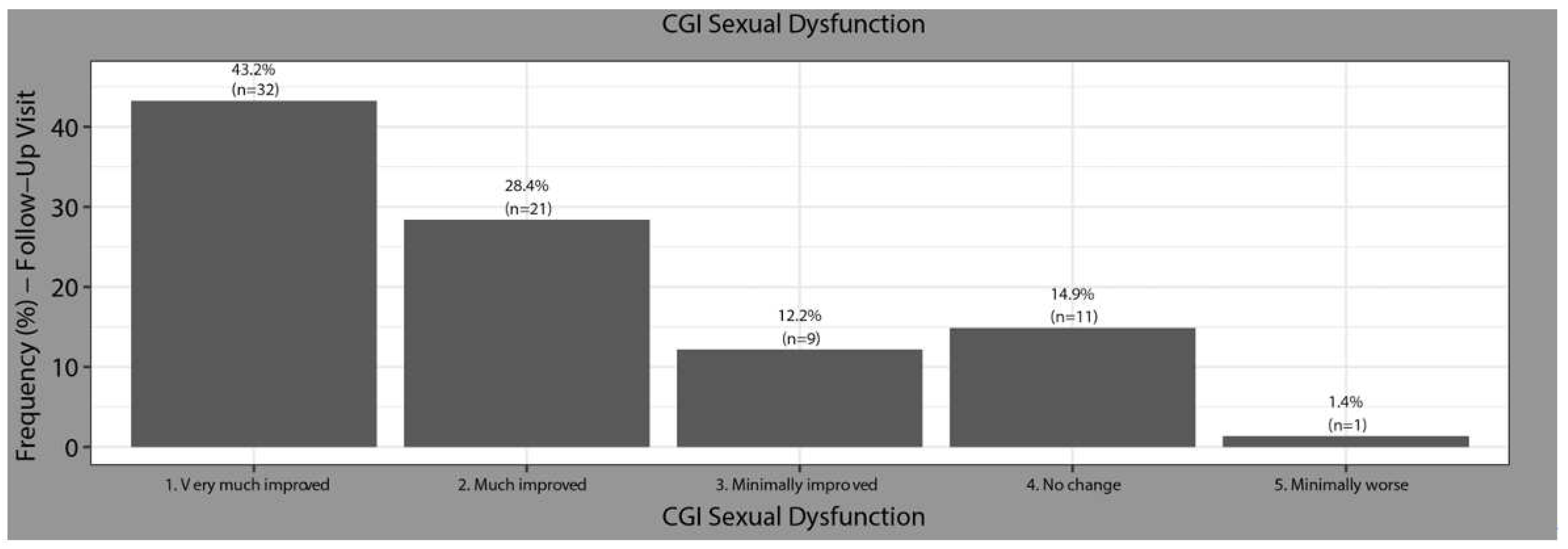
Figure 4.
Frequency of decreased libido, orgasm delay, anorgasmia, and arousal dysfunction at baseline.
Figure 4.
Frequency of decreased libido, orgasm delay, anorgasmia, and arousal dysfunction at baseline.
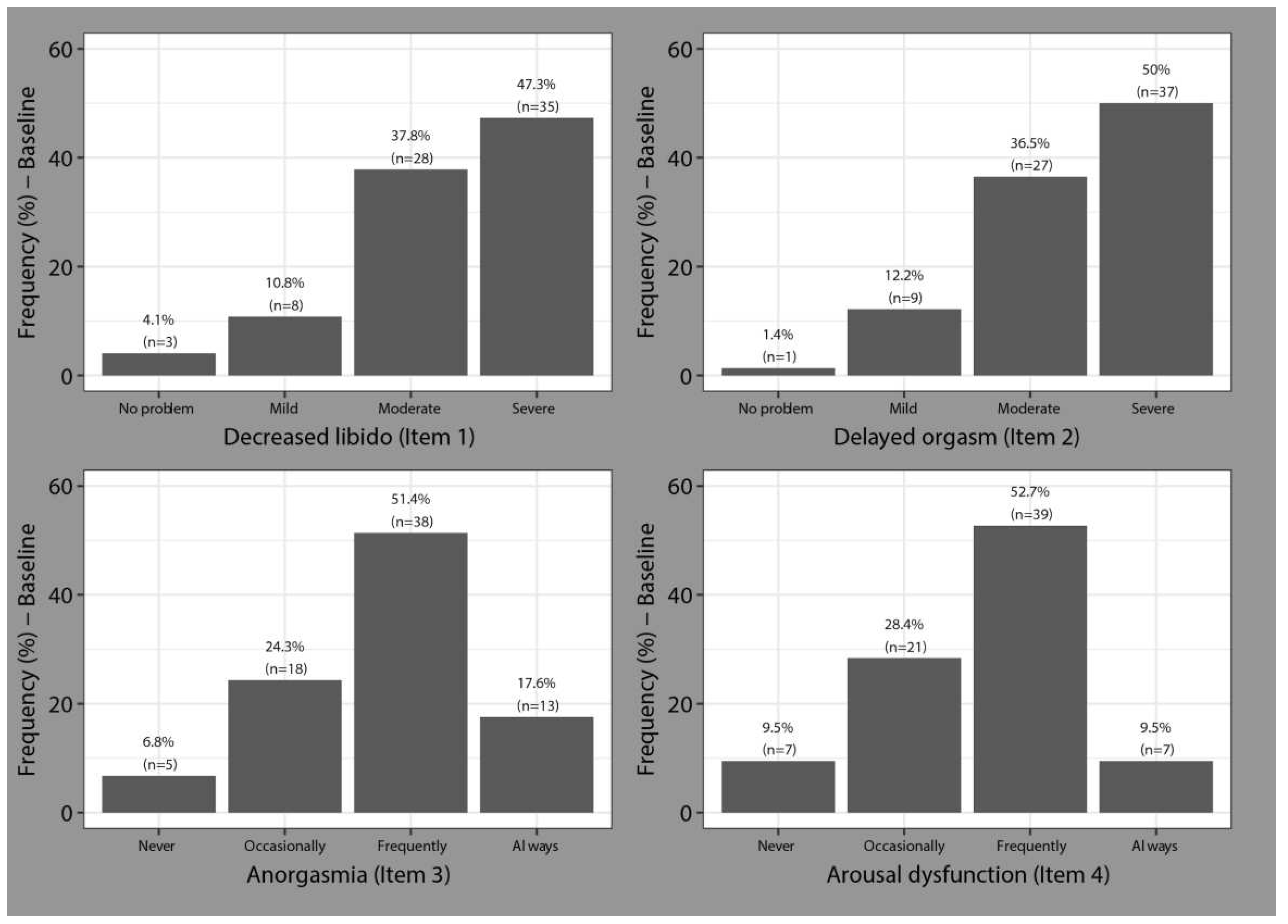
Figure 5.
Frequency of decreased libido, orgasm delay, anorgasmia, and arousal dysfunction at Follow-up.
Figure 5.
Frequency of decreased libido, orgasm delay, anorgasmia, and arousal dysfunction at Follow-up.
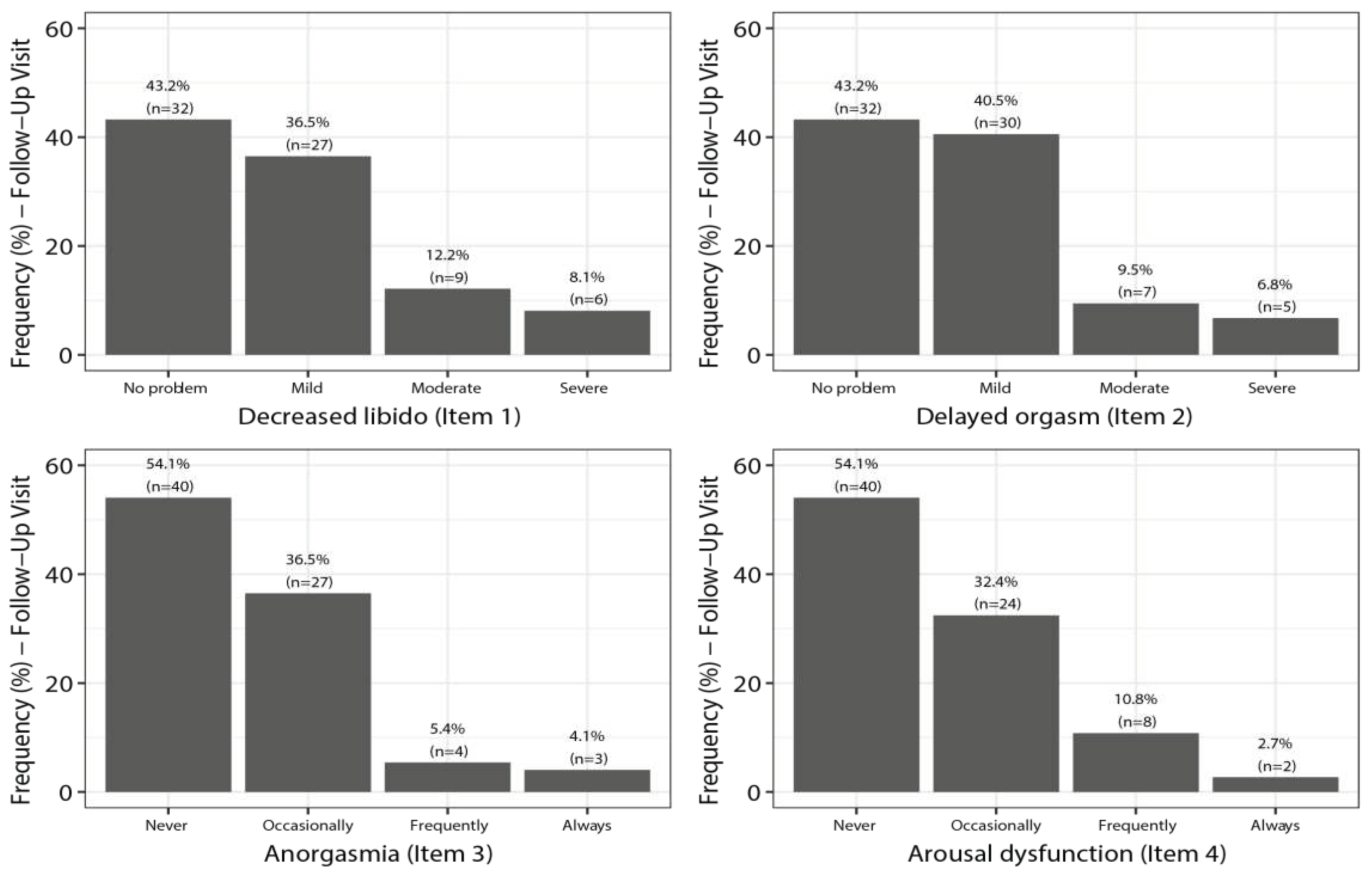
Figure 6.
SALSEX Score by items. Comparison from Baseline to Follow-up.
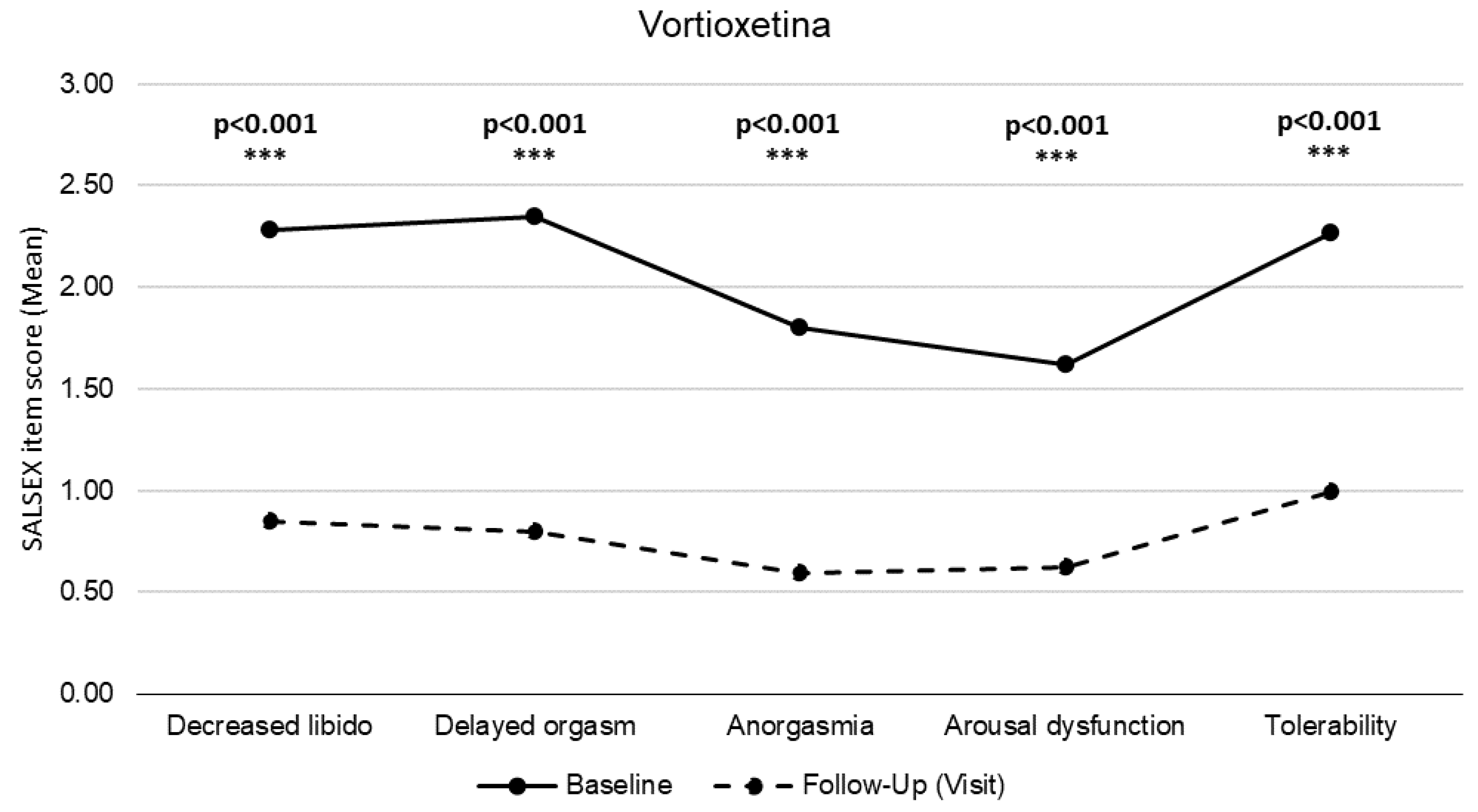
Figure 7.
SALSEX Score and dosages of Vortioxetine. Vortioxetine 5mg n=2 (2.70%); 10mg n=37 (50.00%); 15mg n=22 (29.73%) ; 20mg n=13 (17.57%).
Figure 7.
SALSEX Score and dosages of Vortioxetine. Vortioxetine 5mg n=2 (2.70%); 10mg n=37 (50.00%); 15mg n=22 (29.73%) ; 20mg n=13 (17.57%).
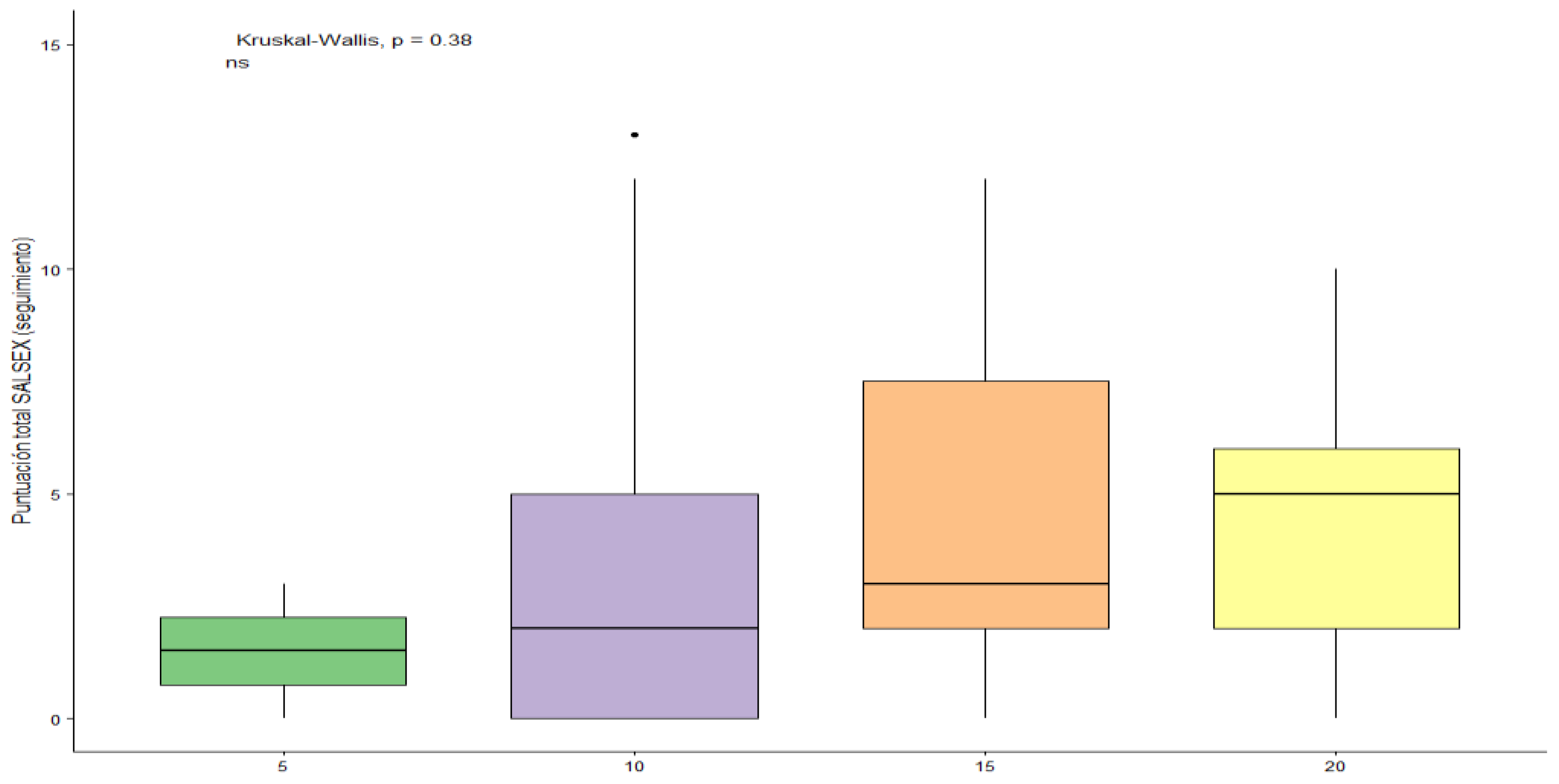
Table 2.
Comparison between sexes in sociodemographic and clinical characteristics of patients switched to Vortioxetine.
Table 2.
Comparison between sexes in sociodemographic and clinical characteristics of patients switched to Vortioxetine.
| Characteristic | Males (n=40) |
Females (n=34) |
P-Value | |
| Age (y.o) | 41.28 ± 13.60 | 45.18 ± 11.26 | 0.188 | t=1.329 |
| < 30 n (%) | 11 (27.5) | 3 (8.8) | ||
| 30-40, n (%) | 10 (25.0) | 11 (32.4) | ||
| 40-50, n (%) | 7 (17.5) | 10 (29.4) | ||
| > 50, n (%) | 12 (30.0) | 10 (29.4) | ||
| Treatment duration at baseline (months) | 14.55 ± 24.02 | 25.38 ± 48.22 | 0.129 | W=819.5 |
| Treatment duration ( baseline-follow-up) | 3.28 ± 1.41 | 3.15 ± 0.86 | 0.900 | W=399 |
| Vortioxetine dosage (mg/d) (at follow-up)) | 12.5 ± 4.08 | 13.82 ± 3.9 | 0.151 | W=802 |
| Total score SALSEX - Baseline | 9.68 ± 3.16 | 11.09 ± 1.9 | 0.021 | t=2.372 |
| Total score SALSEX – Follow-up | 2.85 ± 2.8 | 4.88 ± 4.29 | 0.021 | t=2.367 |
Table 3.
Frequency of sexual dysfunction from baseline to follow-up in Salsex items.
| No Dysfunction | Mild | Moderate | Severe | |||||
| Baseline | F-up | Baseline | F-up | Baseline | F-up | Baseline | F-up | |
| Libido decreased | 4.1 | 43.2 | 10.8 | 36.5 | 37.8 | 12.2 | 47.3 | 8.1 |
| Orgasm delayed | 1.4 | 43.2 | 12.2 | 40.5 | 36.5 | 9.5 | 50.0 | 6.8 |
| Never | Sometimes | Often | Allways | |||||
| Baseline | F-up | Baseline | F-up | Baseline | F-up | Baseline | F-up | |
| Anorgasmia | 6.8 | 54.1 | 24.3 | 36.5 | 51.4 | 5.4 | 17.6 | 4.1 |
| Arousal difficulties | 9.5 | 54.1 | 28.4 | 32.4 | 52.7 | 10.8 | 9.5 | 2.7 |
| No sex dysfunction | Good | Moderate | Poor | |||||
| Baseline | F-up | Baseline | F-up | Baseline | F-up | Baseline | F-up | |
| Acceptability of SD | 1.4 | 34.8 | 10.8 | 39.1 | 47.3 | 18.8 | 40.5 | 7.2 |
Table 4.
Comparison between baseline and Follow-up in Salsex items . Intensity of SD (%).
| No sex dysfunction | MIld | Moderate | Severe | |||||
| Baseline | F-up | Baseline | F-up | Baseline | F-up | Baseline | F-up | |
| Libido decreased | ||||||||
| No problem | 21,4 | 100,0 | 14,3 | - | 35,7 | - | 28,6 | - |
| Moderate/severe | - | 4,5 | 9,1 | 27,3 | 31,8 | 40,9 | 59,1 | 27,3 |
| Orgasm delayed | ||||||||
| No problem | 7,1 | 100,0 | 7,1 | - | 21,4 | - | 64,3 | - |
| Moderate/severe | - | - | 22,7 | 45,5 | 13,6 | 31,8 | 63,6 | 22,7 |
| Never | Sometimes | Often | Allways | |||||
| Baseline | F-up | Baseline | F-up | Baseline | F-up | Baseline | F-up | |
| Anorgasmia | ||||||||
| No problem | 21,4 | 100,0 | 21,4 | - | 35,7 | - | 21,4 | - |
| Moderate/severe | 4,5 | 9,1 | 27,3 | 59,1 | 45,5 | 18,2 | 22,7 | 13,6 |
| Arousal difficulties | ||||||||
| No problem | 28,6 | 100,0 | 42,9 | - | 28,6 | - | - | - |
| Moderate/severe | - | 9,1 | 22,7 | 45,5 | 63,6 | 36,4 | 13,6 | 9,1 |
| No sex dysfunction | Good | Moderate | Poor | |||||
| Baseline | F-up | Baseline | F-up | Baseline | F-up | Baseline | F-up | |
| Acceptability of SD | ||||||||
| No problem | - | 100,0 | 14,3 | - | 35,7 | - | 50,0 | - |
| Poor | - | - | 9,1 | 18,2 | 50,0 | 59,1 | 40,9 | 22,7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



