
Submitted:
04 December 2023
Posted:
05 December 2023
You are already at the latest version
Abstract
The correlation between pain and emotional status in subjects with temporomandibular disorders (TMD) is known. Regardless of that up to date these findings were seldomly confronted with the objective assessment of pain using a digital algometer on the mastication muscles. The aim of the study was to investigate the relationship between the emotional status, chronic pain pain pressure threshold (PPT). 38 subjects were screened for the existence of temporomandibular disorders with the 3Q/TMD questionnaire, for chronic pain (GCPS) and emotional status (PHQ-9 and GAD-7). The results were confronted with the PPT measured with the digital algometer on the masseter muscles. Each subject was examined three times (after 1 month and after 7 months from the initial exami-nation session. Chronic pain scores (GCPS) were found to be higher in the TMD group in all three examination sessions (p<0,05). The pain, depression and anxiety levels were higher in females de-spite the existence of TMD, but only some were significant.A correlation between chronic orofacial pain scores and PPT was found in 2 out of 3 examination sessions. The PPT scores on the masseter muscles did not correlate with the emotional state in the study population.
Keywords:
algometry
; facial pain
; temporomandibular disorders
; muscle tenderness
; depression
; anxiety
; masseter muscle
1. Introduction
Emotions are an inseparable element accompanying every human in everyday life. The emotional state changes and is influenced by many factors such as quality of relationships, free time, professional, financial success, and health. Problems within these areas of life are clear factors contributing to the development of depression [1]. The latest literature states that anxiety disorders affect approximately 3,8-25,0% of the general population [2]. The WHO reports that depression is the fourth most serious disease in the world, affecting approximately 3,8% of the general population, and predicts that it will be at the top of this ranking by 2030. According to studies, from 3,0% of the Japanese population to 16,9% of people in the United States suffer from major depressive disorders [3].
For the purposes of scientific research authors mostly use tools assessing anxiety and depression to describe the emotional state of a person [4]. The most popular being The State-Trait Anxiety Inventory (STAI), Hospital Anxiety and Depression Scale (HAD) [4], Generalized Anxiety Disorder (GAD-7) and Patient Health Questionnaire (PHQ-9) are used to assess the occurrence of depression and anxiety disorders [5,6]. The last two of the above-mentioned questionnaires also form part of a broader diagnostic protocol for assessing the prevalence of temporomandibular disorders, i.e the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) [5]. It considers the physical and psycho-emotional component of the patient's health and is successfully used in many countries around the world [6].
As defined by the International Society for the Study of Pain: pain is an unpleasant, sensual, and emotional sensation related to, or described as, actual or potential tissue damage [7]. There are many categories describing pain, e.g. according to its intensity, location, duration, etc. The types of pain listed in the literature are also clinical pain and induced pain [8].
Multiple questionnaires assessing the occurrence and severity of pain in general are available: McGill Pain Questionnaire (MPQ) [8], visual-analogue scale (VAS scale), Numeric Pain Rating Scale (NPRS) [9]. Also there are more precise and widely used tools such as the Graded Chronic Pain Scale (GCPS) aimed at assessing chronic orofacial pain [10,11].
Since the sensation of pain is subjective, clinical pain is assessed on the basis of the subjective assessment of the patient, i.e. using the VAS or NPRS scale. The induced pain is defined as caused by pressure or e.g. from contact with cold water, and can be measured using an algometer. Such a measurement still has a subjective component, but the respondent does not quantify his reception of pain as this happens with the help of the researcher and specialized equipment. A widely used, relatively cheap and easy-to-use device for measuring the pain threshold is an algometer [12,13,14].
The pain examination using a digital algometer is based on the term of pain pressure threshold (PPT) that refers to a stimulus with the lowest possible intensity and is perceived as painful [15]. Another definition, mentioned in the context of the use of an algometer, refers to the stimulus with the lowest intensity, which causes the sensation to change from pressure to pain [12].
Available data show high intra-examiner reliability when using a digital algometer which makes it a valuable diagnostic tool for scientific research [16].
According to the latest reports, 90% of Americans claim that mental health is as equally important as physical health2. Scientific literature says that pain is associated with emotional reactions and cognitive processes [17]. It is also emphasized that the pain stimulus itself is also a source of fear [17]. In accordance with the research, people with an optimistic approach to life do not feel pain as strongly as pessimists, and are less prone to catastrophize their pain sensations [8]. Moreover, research proves that intense, negative emotions are associated with greater sensitivity to pain stimuli [18]. People with a neurotic personality have a lower pain threshold, which, reported by others, is correlated with the occurrence of greater clinical pain [8].
In the field of orofacial pain multiple studies have shown a higher prevalence of depression and anxiety in subjects with TMD [6]. Moreover, others found that there is a strong correlation between the level of pain and psycho-emotional status measured by the levels of depression and somatization (based on the axis II of the RDC/TMD). Another very interesting conclusion is that pain level is independent from structural symptoms concerning the muscles of mastication, temporomandibular joint (TMJ) or the disc inside the TMJ (all together consisted in the axis I of the RDC/TMD) [19]. All these psycho-emotional factors contribute to the lowering of quality of life (QOL) affecting both personal and professional life of subjects with temporomandibular disorders (TMD) symptoms [20].
The literature review showed that in the past ten years only few reports examining PPT in the TMD population were published. None of which tried to compare the PPT results in the TMD population with the psycho-emotional status. Based on the cited observation, it seems justified to test the pain threshold in patients not only in any part of the body, for example on the phalanx, but also in the masseter or the temporal muscle, whose pain is associated with temporomandibular disorders and the patient's emotional state. The location of the tender points for the above-mentioned muscles is described in the DC/TMD diagnostic protocol [5].
Another author notes the coexistence of migraines, depression and anxiety disorders as well as the lowered pain threshold, which once again emphasizes the importance of further exploring this area of interest [21].
It is interesting that the interaction between pain and emotions is two-sided. The occurrence of pain affects the deterioration of mood and the appearance of stress, while negative emotions and a lowered emotional state seem to increase pain perception. Half of people with depression report pain [22]. At the same time, approximately 30-60% of people suffering from chronic pain suffer from depression as well [23]. Based on many articles suggesting the coexistence of pain experiences or a lowered pain threshold with depression or anxiety disorders and stress, it seems justified to deepen this topic by conducting further studies analyzing this relationship in depth.
Thus the aim of this study was to investigate the relationship between the psycho-emotional state, chronic pain and pain pressure threshold measured on the masseter muscle.
2. Materials and Methods
2.1. Materials
The study group consisted of 38 subjects (23 women, and 15 men). Ultimately, the study group consisted of 38 subjects who were examined three times (Figure 3). All of the participants were students of the physiotherapy degree at the Józef Piłsudski University of Physical Education in Warsaw, Poland. The age of the subjects ranged from 21 to 25 years (22,42±0,89). The participants reported good general health.
The following inclusion criteria were used:
- -
- age between 20 and 25 years old,
- -
- good general health.
Exclusion criteria:
- -
- chronic systemic diseases
- -
- past injury or surgery in the head or face area,
- -
- good oral health - no presence of any ongoing dental pain.
Before each examination the participants were divided into two groups according to the 3Q/TMD questionnaire. Subjects who gave at least one positive answer to the 3Q/TMD were qualified to the TMD group. Others were assigned as controls.
2.2. Method
All the measurements were performed by one researcher. Details on the group size and time schedule of the examination sessions are presented in Figure 1. The first session of the study was performed in a less stressful period for the participants, during the academic year. The second session was carried out a month later - during the examination period, and another session was conducted 7 months later during the next examination period. The tests performed in each series did not differ from each other and consisted of two parts; filling out the questionnaires and measuring the pressure pain threshold (PPT) using the digital algometer.
The explanation of the examination procedure was followed by obtaining a written consent from the participants. Afterwards the subjects were asked to fill in all the below mentioned questionnaires. The study protocol obtained approval from the university's Ethical Committee (SKE 01-03/2022).
2.2.1. Emotional state assessment
The participants were asked to fill in the following questionnaires: 3Q/TMD as a temporomandibular disorders screening tool, then to describe the emotional state with the PHQ-9 (Patient Health Questionnaire) and the GAD-7 (Generalized Anxiety Disorder) and finally with the GCPS (Graded Chronic Pain Scale v.2) for occurrence of chronic orofacial pain.
2.2.2. Pain Pressure Threshold Assessment
The PPT examination was performed with the patient in the prone position, with the head rotated 30° to the contralateral side from the examined muscle.
The test was performed on both masseter muscles (first right and secondly the left muscle). Each muscle was divided into nine parts or points according to the DC/TMD clinical examination guidelines as presented (Figure 2) [5].
The operator using the digital algometer pressed each point until the subject felt that the sensation of pressure was becoming painful. Before the examination, the subject received verbal instructions explaining that the signal indicating that change of the sensation of pressure to the feeling of pain (the first pain felt) would be to point the thumb up of the hand resting on the abdomen, so that it was visible for the researcher.
Each masseter muscle was examined twice (i.e all nine points on each muscle), and the result was the average of the measurements taken – separately on the right and on the left side. To standardize the velocity of force application a metronome set at 60 bpm was used. Thus the pressure force was increased at the rate of 0,25 kg/cm2/s. The researcher was looking at the algometer screen and increasing the pressure with the appropriate pace as indicated elsewhere [13]. The peak value displayed on the screen of the device was recorded and the algometer was reset to zero for subsequent measurements. The participants of the study were informed that the study may be stopped at any time.
2.3. Statistical analysis
The statistical analysis was performed using the STATISTICA (v.13.0) software. The Friedman test was used to compare the results of repeated measurements. Detailed comparisons were made post-hoc using Wilcoxon tests with Bonferroni correction.
The interdependence of the variables was assessed with the Spearman correlation coefficient. The effect size (ES) was measured with the Kendall’s coefficient (Friedman's test) and an equivalent correlation coefficient (Wilcoxon test). The ES scale proposed by Fritz25 was used. The level of significance was set at alpha=0,05.
3. Results
3.1. Results
Before each examination session the same subjects were asked to fill in the 3Q/TMD questionnaire, which was the main criteria for group allocation. Therefore a different number of participants within the groups during the final analysis (see Table 1).
The results of the 3Q/TMD questionnaire divided the participants into a group of people with and without TMD symptoms. The results regarding chronic pain measured with the GCPS questionnaire were significantly higher in the TMD group (p<0,001) than in the control in each examination session with the effect size being large (R>0,50). At the same time, no significant differences were found between the groups regarding the emotional state assessed with the PHQ-9 and the GAD-7 questionnaires (Table 2).
Analyzing the dimorphic differences between the participants it was observed that women had significantly higher scores in the GCPS questionnaire in the first session (p<0,05, R=0,35), in the GAD-7 questionnaire in the second session (p<0,05, R=0,39), and in the PHQ-9 questionnaire in the third session (p<0,05, R=0,47). The effect size being medium regarding the GCPS and GAD-7 and large regarding the PHQ-9. The rest of the results obtained from the questionnaires did not differ between the sexes (see Table 3).
There were statistically significant differences in the PPT result on the right masseter muscle between the first and the third (p<0,05) and also the second and the third examination sessions (p<0,05). In the first case the effect size was medium (R=0,41) and in the second it was large (R=0,52). Such a correlation was not found for the left masseter muscle (Table 4).
Another analyzed aspect concerning the relationship between chronic orofacial pain assessed with the GCPS (subjective perception of pain) and the PPT measured on the masseter muscle with the algometer (objective assessment of pain). A statistically significant relationship was found between the results of the GCPS questionnaire and PPT. Such a correlation existed in the first and second examination sessions, but not in the third one. All the results are shown in Table 5.
The data showed no significant correlation between the emotional state assessed with PHQ-9 and GAD-7 and the PPT in the studied sample.
3.2. Figures, Tables and Schemes
3.2.1. Figures:
- Group size and time schedule of the examination sessions. [source: own project]……………….3
- Localization of the points on the masseter muscle for PPT examination. [source: Schiffman et al., 2014]..………………………………………………………….…………….………………………...4
3.2.2. Tables:
- Number of participants in TMD and control groups during each examination session…………5
- Results of chronic pain (GCPS) and the emotional state (PHQ-9 and GAD-7) questionnaires in the TMD and control groups in all three examination sessions…..……………….………………..5
- Dimorphic differences between the results of chronic pain (GCPS) and the emotional state (PHQ-9 and GAD-7) questionnaires…………………..……………………………………………….6
- Pressure pain threshold (PPT) changes between the sessions (1, 2 or 3) for the right (MR) and the left masseter muscle (ML)…………………………………………………………………………..7
- Correlation between chronic orofacial pain questionnaire (GCPS) and pressure pain threshold (PPT) between the three examination sessions. Right (MR) and left (ML) masseter muscles…...7
4. Discussion
Up to date the relationship between the emotional state and pain pressure threshold (PPT) in the TMD population was barely investigated. Thus the current pilot study was an attempt to clarify if the relationship even exists. The authors wanted to check whether the relationship between the emotional state and orofacial pain and the tenderness of the masseter muscle occurs in people with and without TMD signs and symptoms or orofacial pain.
The relationship of the emotional state and pain has been widely described in the literature. TMD subjects show higher levels of depression and anxiety than the general population [26]. One of the main symptoms of TMD is pain, thus this premise was the main factor for choosing the material and methods for this paper. The most common methods of assessing pain in people with TMD are self-report pain questionnaires [27,28].
In the literature on the relationship between pain and emotions, this relationship is often noticed in the group of pain patients with TMD [12,29]. The authors of this article examined the existence of this relationship in a group of people with and without TMD.
In the current study we can observe differences in GCPS results between the groups − TMD and control − assessed with 3Q/TMD. In all three sessions the results of GCPS were significantly higher in the TMD group compared with controls. At the same time the results of the questionnaires assessing the emotional state (PHQ-9 and GAD-7) did not differ between the groups. Based on these results it is possible to conclude that the self-declared pain levels in GCPS were more pronounced in the TMD group, but at the same time the levels of depression and anxiety did not show any differences between the groups.
The relationship between TMD and declared chronic orofacial pain is widely described in the literature. Some authors found correlation between the existence of TMD and GCPS as those shown in the current study [28], on the contrary others didn’t [30]. Lack of a significant correlation between TMD and emotional state differ from the current study’s results from those which we generally can observe elsewhere. It may be due to the small sample with extremely low or extremely high scores regarding depression or anxiety assessment. Such a conclusion was drawn because in the literature where the existence of that relationship was observed, the number of participants was higher [19].
Another aspect is that in the current study, no significant relationship was found between the emotional state and chronic orofacial pain reported in the GCPS questionnaire. There are studies showing the opposite, but they often examine only participants with facial pain or only with TMD and not both as in the current study [27,29]. The authors examined a young population of students and in this group there were both subjects with orofacial pain and/or TMD, and also without it. It allows us to create an interesting hypothesis that the mere presence of orofacial pain is not correlated with emotions, but its intensity depends on emotions [27,29].
The last possible aspect is the examined time frame coverage within the GPCS and the PHQ-9/GAD-7 questionnaires, 6 months and 2 weeks respectively. The difference mentioned may be the reason why the significance was not found between groups. The solution for further studies may be the use of similar tools regarding the examined time frame.
Regarding the depression and anxiety levels between sexes, there have been found statistically significant differences between women and men.
The pain regulatory mechanisms connected with TMD are different between the genders [30]. In many studies the authors decided to include only women in the examined group [31]. There are many factors that contribute to the differences in pain mechanisms between men and women. There are psychosocial, social, hormonal and biological factors [33], but in general most research show that women experience more facial pain than men [19]. This phenomenon could be due to a lower pain threshold in women which was shown by others [34].
In the current study women had higher scores than men in all of the questionnaires, but only the following differences were significant: GCPS - in the first session, GAD-7 in the second session and PHQ-9 in the third examination session. Other authors also reported gender differences in emotional state and pain levels [19,35].
The literature shows that women suffer from anxiety disorders and depression more often than men [19,35], but at the same time other authors claim that this difference sometimes is very small or even doesn’t exist [36].
The results obtained from this study are in accordance with the latter statement. The results of the PHQ-9 questionnaire completed during each session showed that results during the first and the second rounds did not show significant differences between women and men. Only in the third round the results showed significantly higher scores in women. The same tendency applied for anxiety disorders. In the first and the third sessions of the study, no differences in the results of the GAD-7 questionnaire were noticed between genders, but only in the second session, anxiety disorders were significantly higher in women.
The examination sessions were planned and performed three times - the initial examination, the second after 1 month and the third after 7 months. The aim of this procedure was to check the pressure pain threshold (PPT) in conjunction with the changes in the emotional state. The chosen timeframe was set to be in agreement with the academic year.
The first round of examination was conducted during the semester, the second round during the examination period and the third during the next examination period. The latter is often described by students as the most stressful and the most difficult one because of the number of exams included.
The pressure pain threshold was measured using nine points on each of the masseter muscles and not only on one point on the masseter which we can observe in literature [13,24,37].
PPT scores on the right masseter muscle differed significantly between first and third and between second and third sessions, which shows that the time between series of examinations performed on the same group of people is significant. This is an important conclusion because the authors found only few other studies that tested PPT in the same group of people at intervals without subjecting them to any interventions, e.g. physiotherapy treatment. In the study found the authors used an eight-month interval [38].
No such relationship was found for the left masseter muscle. The reason for that could be the fact that TMD symptoms often are one-sided [39]. The lack of symmetry shows that in future research it is worth noting the painful side in the TMD group. Another reason explaining why this asymmetry occurred is that the examination protocol of PPT always started with the right masseter muscle. Future protocols should consist of random selection of the muscle to be tested to diminish this factor.
Another aspect worth mentioning is a try of an improvement of the accuracy of the PPT examination of the masseter muscle. In the current study the pressure pain threshold was measured using nine points on each of the masseter muscles and not only on one point which we can observe in literature [13,24,37]. Additionally the nine point scheme adopted from the DC/TMD protocol reproduces the most recommended guidelines of the clinical examination of the temporomandibular disorders [5].
The authors of this study used an algometer to test the pressure pain threshold (PPT) with an aim to objectify pain assessment and to find out if it correlates with patients' emotional state and also with self-declared pain levels in the questionnaires. Up to date a negative correlation between PPT on the left masseter and severity of TMD was found by different authors but there was a lack of similar observation on the right masseter [13]. It shows that this correlation is not constant. In the current study both a digital algometer and the GCPS questionnaire were used with an aim to assess both the subjective perception of pain (GCPS) and also an objective measurement such as PPT. This protocol allowed us to gather more information about the duration of pain in the long term (i.e. the last 6 months) and also at the moment of examination. The literature reports that pain sensitivity often predisposes to the occurrence of the phenomenon of pain chronicity reported by the patients, especially among women [40].
The data shows that during the first two sessions the relationship between the chronic orofacial pain experienced and declared in the GCPS questionnaire (subjective assessment), and the tenderness of the masseter muscle tested by means of PPT measured using a digital algometer. This tendency was proven by a correlation between PPT and both, the right and the left masseter muscles and GCPS results in the first and the second session.
In this study, no significant correlation between the emotional state and the PPT in the masseter muscle was found. This finding is fundamental because it complies with recent reports that stated that there is no correlation between the structure and pain, depression and somatization intensity. In other words the level of pain is independent from the muscles, the temporomandibular joint position etc. On the other hand pain is strictly correlated with the levels of depression and somatization in TMD patients [19].
The results from this pilot study show that there are reasons to continue exploring this subject by conducting further research on larger and more representative study samples.
5. Conclusions
- The orofacial pain scores were higher in the TMD group compared with the control subjects.
- The prevalence of pain, depression and anxiety was higher in female subjects, but only some were significant.
- The PPT (only of the right masseter) correlates with the incidence and intensity of chronic orofacial pain assessed by the GCPS questionnaire results, but not in all cases.
- The PPT tested with an algometer on the masseter muscles does not correlate with the emotional state measured with PHQ-9 and GAD-7 in the study population.
Study Advantages
The protocol consisted of both the subjective (GCPS) and objective pain assessment (PPT) tools to have a better understanding of the patients symptoms and complaints. This pilot study was a try to investigate the pain-emotions relation that seems to be a clinically important topic.
Study Limitations
A small study sample that is not representative of the general population.
Author Contributions
Conceptualization, W.K.-M. and T.M.; methodology, W.K.-M. and T.M.; software, W.K.-M. and T.M.; validation, W.K.-M. and T.M.; formal analysis, W.K.-M. and T.M.; investigation, W.K.-M. and T.M.; resources, W.K.-M. and T.M.; data curation, W.K.-M. and T.M.; writing—original draft preparation, W.K.-M. and T.M.; writing—review and editing, W.K.-M. and T.M.; visualization, W.K.-M. and T.M.; supervision, W.K.-M. and T.M.; project administration, W.K.-M. and T.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Józef Piłsudski University of Physical Education in Warsaw (SKE 01-03/2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We would like to express our deepest gratitude to Dr Katarzyna Kaczmarczyk.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kessler, R. C., de Jonge, P., Shahly, V., van Loo, H. M., Wang, P. S. E., & Wilcox, M. A. Epidemiology of depression. Annu Rev Public Health. 2014; 34:119–138. [CrossRef]
- Athanas, A., McCorrison, J., Campistron, J., Bender, N., Price, J., Smalley, S., & Schork, N. J. Characterizing Emotional State Transitions During Prolonged Use of a Mindfulness and Meditation App: Observational Study, JMIR Mental Health, 2021; 8(3). [CrossRef]
- Yang, Y., Ligthart, L., Terwindt, G. M., Boomsma, D. I., Rodriguez-Acevedo, A. J., & Nyholt, D. R. Genetic epidemiology of migraine and depression, Cephalalgia, 2016; 36(7), 679-691. [CrossRef]
- Farnik, M., & Pierzchała, W., Stan emocjonalny, funkcje poznawcze i jakość życia u chorych na OBPS, Pneumonologia i Alergologia Polska, 2007, 75 (supl 1), 77-79. Polish. [CrossRef]
- Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet J-P, List T, Svensson P, Gonzales Y. Diagnostic criteria for Temporomandibular Disorders (DC-TMD) for clinical and research applications: Recommendations of the International RDC-TMD Consortium Network and Orofacial Pain Special Interest Group. J Oral Facial Pain headache; 2014; 28(1):6-27. [CrossRef]
- Simoen, L., Van den Berghe, L., Jacquet, W., & Marks, L. Depression and anxiety levels in patients with temporomandibular disorders: Comparison with the general population, Clinical oral investigations, 2020; 24(11), 3939-3945. [CrossRef]
- Morley S., Psychologiczne koncepcje bólu Dobrogowski J. Wardliczek J. (red) Terapie uzupełniające w leczeniu bólu, Elsevier Urban & Partner Wrocław, 2010.
- Strachan, E., Poeschla, B., Dansie, E., Succop, A., Chopko, L., & Afari, N. Clinical and evoked pain, personality traits, and emotional states: Can familial confounding explain the associations?, Journal of psychosomatic research, 2015; 78(1), 58-63. [CrossRef]
- Khedr, M. A., El Sayed, H. G., & El Wakil, A. Perceived stress in multiple sclerosis patients: Relationship with mood states and pain experience. Multiple sclerosis and related disorders, 2022; 59,103650. Advance online publication. [CrossRef]
- Von Korff, M. (2011). Assessment of chronic pain in epidemiological and health services research: Empirical bases and new directions. In D. C. Turk & R. Melzack (Eds.), Handbook of pain assessment (pp. 455–473). The Guilford Press.
- Lövgren, A., Parvaneh, H., Lobbezoo, F., Häggman-Henrikson, B., Wänman, A., & Visscher, C. M. Diagnostic accuracy of three screening questions (3Q/TMD) in relation to the DC/TMD in a specialized orofacial pain clinic, Acta Odontologica Scandinavica, 2018; 76(6), 380-386. [CrossRef]
- Ramalho, D., Macedo, L., Goffredo Filho, G., Goes, C., & Tesch, R. Correlation between the levels of non-specific physical symptoms and pressure pain thresholds measured by algometry in patients with temporomandibular disorders, Journal of oral rehabilitation, 2015; 42(2), 120-126. [CrossRef]
- Herpich CM, Gomes CAFP, Dibai-Filho AV, Politti F, Souza CDS, Biasotto-Gonzalez DA, Correlation Between Severity of Temporomandibular Disorder, Pain Intensity, and Pressure Pain Threshold, J Manipulative Physiol Ther, 2017; Jan;41(1):47-51. [CrossRef]
- Tesch, R. D. S., Fernandes, F. S., Favilla, E. E., De Goffredo Filho, G. S., & Goes Differences in non-specific physical symptom levels and pressure pain thresholds between patients with masticatory myofascial pain and arthralgia, Cranio : the journal of craniomandibular practice, 2018; 38(6), 389–395. [CrossRef]
- Argoff, C. E., Dubin, A., Pilitsis, J., & McCleane, G., Pain management secrets E-Book. Elsevier Health Sciences; 2009.
- Jerez-Mayorga, D., Dos Anjos, C. F., Macedo, M. C., Fernandes, I. G., Aedo-Muñoz, E., Intelangelo, L., & Barbosa, A. C. Instrumental validity and intra/inter-rater reliability of a novel low-cost digital pressure algometer. PeerJ, 2020; 8, e10162. [CrossRef]
- Suchocka L. Psychologia Bólu, Warszawa, Wydawnictwo Difin; 2008.
- Sibille, K. T., Kindler, L. L., Glover, T. L., Staud, R., Riley III, J. L., & Fillingim, R. B. Affect balance style, experimental pain sensitivity, and pain-related responses, The Clinical journal of pain, 2012; 28(5), 410. [CrossRef]
- De la Torre Canales, G., Bonjardim, L. R., Poluha, R. L., Soares, F. F. C., Guarda-Nardini, L., Conti, P. R., & Manfredini, D. Correlation between physical and psychosocial findings in a population of temporomandibular disorder patients, Int J Prosthodont, 2020; 33(2), 155-9. [CrossRef]
- Bitiniene D, Zamaliauskiene R, Kubilius R, Leketas M, Gailius T, Smirnovaite K. Quality of life in patients with temporomandibular disorders. A systematic review. Stomatologija. 2018;20(1):3-9.
- Baldacci, F., Lucchesi, C., Cafalli, M., Poletti, M., Ulivi, M., Vedovello, M. & Gori, S. Migraine features in migraineurs with and without anxiety–depression symptoms: A hospital-based study, Clinical neurology and neurosurgery, 2015; 132, 74-78. [CrossRef]
- Crofford, L. J. Psychological aspects of chronic musculoskeletal pain. Best practice & research Clinical rheumatology, 2015; 29(1), 147-155. [CrossRef]
- Goesling, J., Clauw, D. J., & Hassett, A. L. Pain and depression: an integrative review of neurobiological and psychological factors, Current psychiatry reports, 2013, 15(12), 421. [CrossRef]
- Rodriguez-Blanco, C., Cocera-Morata, F. M., Heredia-Rizo, A. M., Ricard, F., Almazán-Campos, G., & Oliva-Pascual-Vaca, Á. Immediate effects of combining local techniques in the craniomandibular area and hamstring muscle stretching in subjects with temporomandibular disorders: a randomized controlled study, The journal of alternative and complementary medicine, 2015; 21(8), 451-459. [CrossRef]
- Fritz, C. O., Morris, P. E., & Richler, J. J. Effect size estimates: Current use, calculations, and interpretation. Journal of Experimental Psychology: General, 2012; 141(1), 2–18. [CrossRef]
- Sójka, A., Stelcer, B., Roy, M., Mojs, E., & Pryliński, M. Is there a relationship between psychological factors and TMD?. Brain and behavior, 2019; 9(9), e01360. [CrossRef]
- Kotiranta, U., Forssell, H., & Kauppila, T. Painful temporomandibular disorders (TMD) and comorbidities in primary care: associations with pain-related disability. Acta odontologica Scandinavica, 2019, 77(1), 22–27. [CrossRef]
- Stålnacke C, Ganzer N, Liv P, Wänman A, Lövgren A. Prevalence of temporomandibular disorder in adult patients with chronic pain. Scand J Pain. 2020 Sep 24;21(1):41-47. [CrossRef]
- Osiewicz, M., Lobbezoo, F., Ciapała, B., Pytko-Polończyk, J., & Manfredini, D. Pain Predictors in a Population of Temporomandibular Disorders Patients. Journal of clinical medicine, 2020; 9(2), 452. [CrossRef]
- Chantaracherd, P., John, M. T., Hodges, J. S., & Schiffman, E. L. Temporomandibular joint disorders' impact on pain, function, and disability. Journal of dental research, 2015; 94(3 Suppl), 79S–86S. [CrossRef]
- Knuutila, J., Kivipuro, J., Näpänkangas, R., Auvinen, J., Pesonen, P., Karppinen, J., Paananen, M., Pirttiniemi, P., Raustia, A., & Sipilä, K. Association of temporomandibular disorders with pain sensitivity: A cohort study. European journal of pain (London, England), 2022; 26(1), 143–153. [CrossRef]
- Mohn, C., Vassend, O., & Knardahl, S. Experimental pain sensitivity in women with temporomandibular disorders and pain-free controls: the relationship to orofacial muscular contraction and cardiovascular responses. The Clinical journal of pain, 2008; 24(4), 343–352. [CrossRef]
- Miettinen, O., Lahti, S., & Sipilä, K. Psychosocial aspects of temporomandibular disorders and oral health-related quality-of-life. Acta odontologica Scandinavica, 2012; 70(4), 331–336. [CrossRef]
- Nozaki-Taguchi, N., Hayashida, T., & Isono, S. Qualitative measurement of opioid effects on pain and dyspnea: gender difference in the sensitivity. JA clinical reports, 2020; 6(1), 85. [CrossRef]
- Moutinho, I. L., Maddalena, N. C., Roland, R. K., Lucchetti, A. L., Tibiriçá, S. H., Ezequiel, O. D., & Lucchetti, G. Depression, stress and anxiety in medical students: A cross-sectional comparison between students from different semesters. Revista da Associacao Medica Brasileira (1992), 2017; 63(1), 21–28. [CrossRef]
- Tysiąc-Miśta, M. K., Pudlo, R., Nitsze-Wierzba, M., & Fischer, P. Badanie poziomu lęku i depresji wśród lekarzy dentystów z terenu województwa śląskiego na podstawie skali HADS. Psychiatria, 2022. [CrossRef]
- de Araújo Vitor, C. A., de Oliveira Lira Ortega, A., Ferreira, A. C. F. M., Da Silva, C. A., Gallottini, M. H. C., & Santos, M. T. B. R. Pressure pain threshold of masticatory muscles in children and adolescents with and without intellectual disability: A pilot study, European Archives of Paediatric Dentistry, 2021; 22(4), 587-593. [CrossRef]
- Slade, G. D., Sanders, A. E., Ohrbach, R., Fillingim, R. B., Dubner, R., Gracely, R. H., & Greenspan, J. D., Pressure pain thresholds fluctuate with, but do not usefully predict, the clinical course of painful temporomandibular disorder, PAIN, 2014; 155(10), 2134-2143. [CrossRef]
- Shao, B., Teng, H., Dong, S., & Liu, Z. Finite element contact stress analysis of the temporomandibular joints of patients with temporomandibular disorders under mastication. Computer methods and programs in biomedicine, 2022; 213, 106526. [CrossRef]
- Rollman, G. B., & Lautenbacher, S. Sex differences in musculoskeletal pain. The Clinical journal of pain, 2001; 17(1), . [CrossRef]
Figure 1.
Group size and time schedule of the examination sessions. [source: own project].
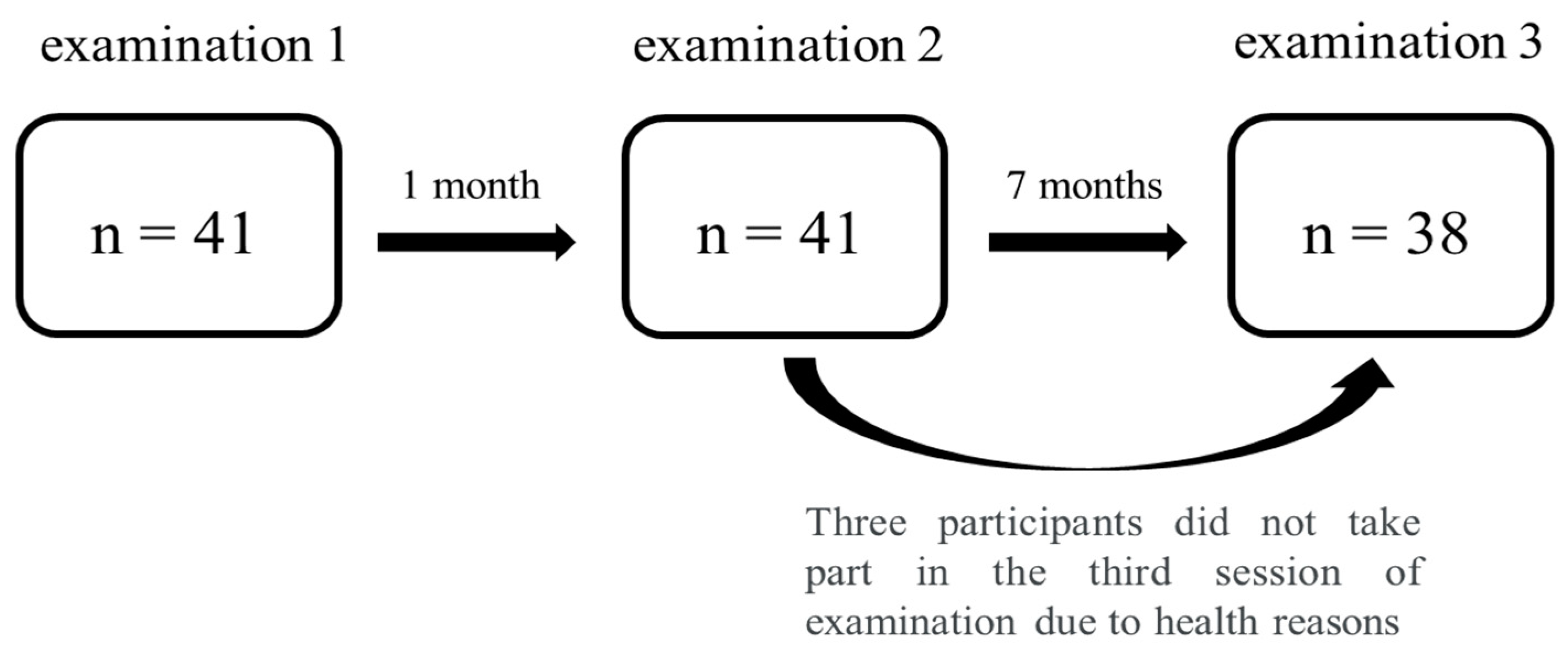
Figure 2.
Localization of the points on the masseter muscle for PPT examination [source: Schiffman et al., 2014].
Figure 2.
Localization of the points on the masseter muscle for PPT examination [source: Schiffman et al., 2014].
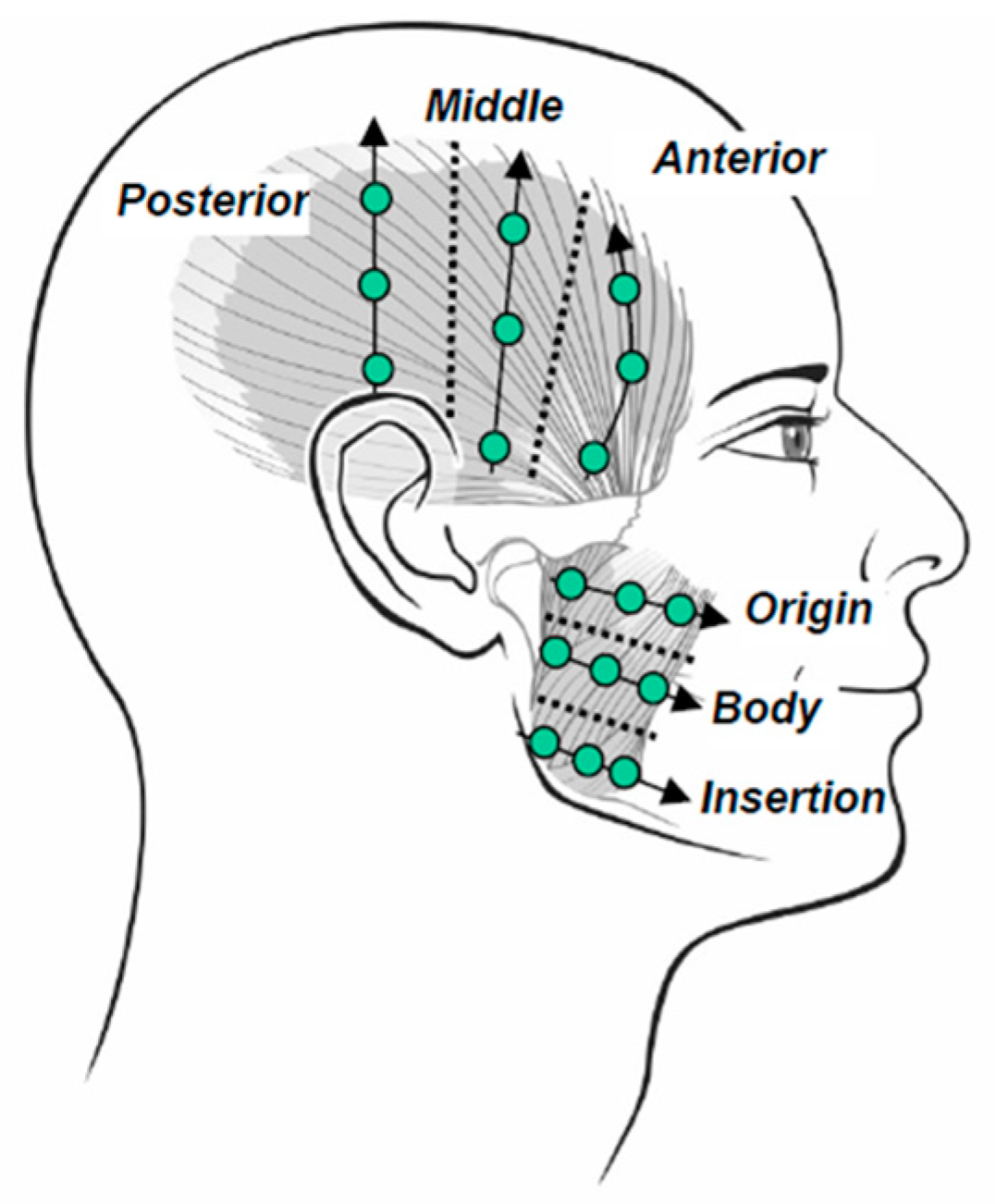

Table 1.
Number of participants in TMD and control groups during each examination session.
| Group (n=38) | Examination 1 | Examination 2 | Examination 3 |
| TMD | 24 (f14, m10) | 22 (f12, m10) | 21 (f12, m9) |
| control | 14 (f9, m5) | 16 (f11, m5) | 17 (f11, m6) |
Table 2.
Results of chronic pain (GCPS) and the emotional state (PHQ-9 and GAD-7) questionnaires in the TMD and control groups in all three examination sessions.
Table 2.
Results of chronic pain (GCPS) and the emotional state (PHQ-9 and GAD-7) questionnaires in the TMD and control groups in all three examination sessions.
| Questionnaire | TMD group | Control group | p value | Effect Size (R) | ||||
| mean | median | Interquartile range |
mean | median | interquartile range | |||
| GCPS1 | 0,95±0,95 | 1,00 | 1,00 | 0,71±0,27 | 0,00 | 0,00 | <0,001* | 0,61 |
| GCPS2 | 1,18±1,01 | 1,00 | 2,00 | 0,00±0,00 | 0,00 | 0,00 | <0,001* | 0,73 |
| GCPS3 | 1,19±1,12 | 1,00 | 3,00 | 0,12±0,48 | 0,00 | 0,00 | <0,001* | 0,64 |
| PHQ-91 | 8,75±4,71 | 8,50 | 6,00 | 6,71±4,71 | 5,00 | 7,00 | 0,187 | 0,26 |
| PHQ-92 | 8,27±4,62 | 8,00 | 6,00 | 11,44±5,12 | 10,50 | 10,50 | 0,202 | -0,07 |
| PHQ-93 | 9,10±6,39 | 8,00 | 8,00 | 11,76±8,02 | 10,00 | 10,00 | 0,310 | -0,20 |
| GAD-71 | 9,00±4,94 | 7,00 | 6,00 | 7,07±5,20 | 5,00 | 8,00 | 0,202 | 0,25 |
| GAD-72 | 8,05±4,40 | 6,50 | 6,00 | 11,94±4,40 | 13,00 | 11,00 | 0,523 | -0,13 |
| GAD-73 | 8,57±5,32 | 7,00 | 8,00 | 11,47±7,37 | 13,00 | 14,00 | 0,257 | -0,22 |
Table 3.
Dimorphic differences between the results of chronic pain (GCPS) and the emotional state (PHQ-9 and GAD-7) questionnaires.
Table 3.
Dimorphic differences between the results of chronic pain (GCPS) and the emotional state (PHQ-9 and GAD-7) questionnaires.
| Questionnaire | TMD group | Control group | p value | Effect Size (R) | ||||
| mean | median | interquartile range | mean | median | interquartile range | |||
| GCPS1 | 0,87±1,01 | 1,00 | 1,00 | 0,27±0,46 | 0,00 | 1,00 | 0,048* | 0,35 |
| GCPS2 | 0,83±1,11 | 0,00 | 2,00 | 0,47±0,64 | 0,00 | 1,00 | 0,502 | 0,12 |
| GCPS3 | 0,91±1,24 | 0,00 | 2,00 | 0,40±0,51 | 0,00 | 1,00 | 0,429 | 0,14 |
| PHQ-91 | 8,74±4,47 | 8,00 | 7,00 | 6,87±5,10 | 5,00 | 7,00 | 0,178 | 0,26 |
| PHQ-92 | 9,96±5,80 | 9,00 | 9,00 | 7,20±5,06 | 6,00 | 9,00 | 0,198 | 0,25 |
| PHQ-93 | 12,22±7,60 | 10,00 | 10,00 | 7,33±5,51 | 7,00 | 10,00 | 0,047* | 0,39 |
| GAD-71 | 9,70±5,30 | 8,00 | 9,00 | 6,13±3,89 | 6,00 | 5,00 | 0,059 | 0,37 |
| GAD-72 | 10,48±5,43 | 10,00 | 10,00 | 6,27±4,27 | 5,00 | 8,00 | 0,016* | 0,47 |
| GAD-73 | 11,22±6,32 | 10,00 | 11,00 | 7,80±6,13 | 7,00 | 11,00 | 0,088 | 0,33 |
Table 4.
Pressure pain threshold (PPT) changes between the sessions (1, 2 or 3) for the right (MR) and the left masseter muscle (ML).
Table 4.
Pressure pain threshold (PPT) changes between the sessions (1, 2 or 3) for the right (MR) and the left masseter muscle (ML).
| PPT | p value | Effect Size (R) |
| MR1 − MR2 | 1,000 | 0,03 |
| MR1 − MR3 | 0,032* | 0,41 |
| MR2 − MR3 | 0,004* | 0,52 |
| ML1 − ML2 | 1,000 | 0,08 |
| ML1 − ML3 | 0,729 | 0,19 |
| ML2 − ML3 | 0,969 | 0,16 |
Table 5.
Correlation between chronic orofacial pain questionnaire (GCPS) and pressure pain threshold (PPT) between the three examination sessions. Right (MR) and left (ML) masseter muscles.
Table 5.
Correlation between chronic orofacial pain questionnaire (GCPS) and pressure pain threshold (PPT) between the three examination sessions. Right (MR) and left (ML) masseter muscles.
| MR/ML examination 1 |
MR/ML examination 2 |
MR/ML examination 2 |
|
| GCPS1 | -0,421*/-0,437* | - | - |
| GCPS2 | - | -0,484*/-0,455* | - |
| GCPS3 | - | - | -0,315/-0,185 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



