
Submitted:
05 December 2023
Posted:
06 December 2023
You are already at the latest version
Abstract
Background: Idiopathic Toe Walking (ITW) is the persistence of a forefoot strike pattern at initial contact while walking beyond the age of three years, in the absence of other justifiable causes. This review aims to consolidate the current knowledge on the subject and to highlight recent advancements in literature. Methods: We conducted an electronic search in the following databases up to June 2023: Ovid MEDLINE, EBSCO, Embase, CINAHL Plus, and PubMed. The PICO framework was employed to define search terms. Results: Despite considerable methodological heterogeneity among studies, we found a stronger inclination toward investigating etiological and prognostic factors. There is a trend for a higher prevalence in boys with a positive family history. Novel classifications have been proposed to improve differential diagnosis. Among conservative treatment options, there is stronger evidence for gait improvement with the use of serial casting followed by orthoses. Severe cases may benefit from surgical Zone III gastrocsoleus lengthening. Conclusion: Further studies with standardized methodologies are required to clarify questions about the etiology, classification, and treatment of this condition. Nonetheless, there is a higher level of evidence supporting conservative treatments with serial casting and orthoses, as well as gastrocsoleus Zone III surgical lengthening for severe cases in the second decade of life.
Keywords:
Idiopathic Toe Walking
; Equinus Gait
; Tip Toe Walking
; Toe Walking Behavior
; Treatment
; Narrative Review.
1. Introduction
Idiopathic Toe Walking (ITW) is a gait deviation characterized by the persistence of a forefoot strike pattern at initial contact throughout most of the gait cycles beyond the age of 3 years, without an apparent cause [1,2]. It is a diagnosis of exclusion, so one must rule out neurological, neuromuscular and primary orthopedic abnormalities, therefore the assessment of strength, reflexes, and selectivity needs to be normal [3,4].
Genetic syndromes like McArdle syndrome, muscular dystrophies, autism spectrum disorder (ASD), peripheral neuropathies - such as Charcot-Marie-Tooth disease - and cerebral palsy are highlighted among the differential diagnoses. Children with mild spastic diplegic cerebral palsy bear considerable resemblance to ITW [5]. However, in idiopathic toe walking, there is adequate knee extension at initial contact and at the end of terminal swing in the gait cycle. These characteristics indicate good selective motor control, which stands as a primary distinctive factor from cerebral palsy [5,6].
The natural history of ITW remains uncertain, and further studies with higher levels of evidence are required to support decisions on when and how to intervene [7]. Divergence among authors is substantial, with some citing spontaneous resolution for the majority of children [8,9], while others suggest persistence of toe walking in approximately 20% to 50% of untreated cases, varying with the severity of the condition [10].
The prevalence also lacks consensus, with some citing ITW in approximately 5% [8,11] of children, while others point to as much as 24% [5] in the preschool population.
The first publication on the subject was made by Hall and colleagues in 1967 [10], describing it as a congenital contracture of the Achilles tendon, commonly referred to as congenital short Achilles tendon, a theory that prevailed until the early 21st century, influencing generations of orthopedic surgeons. However, over the last two decades, the subject gained new approaches, nomenclatures, and different classifications were proposed. Currently, the term Idiopathic Toe Walking is the most widely accepted and used.
Several etiological hypotheses have gained visibility, such as the theory of sensory processing dysfunction (SPD), with studies suggesting a possible association with vestibular dysfunctions [12]. Additionally, genetic etiology has been considered, with the possible presence of an autosomal dominant variable expression characteristic [13]. A positive family history is frequently observed, ranging from 30% [14] to 88% [13].
The main consequences of persistent toe walking include the development of plano-valgus feet, increased external tibial torsion, pain, fatigue, imbalance, and psychological impact [15].
Various severity classification methods have been proposed. In 2007, Alvarez proposed categorizing severity into mild, moderate, and severe based on the presence or absence of three primary criteria identified in three-dimensional gait analysis. These criteria include the presence of the first ankle rocker, the presence of an early third rocker, and the predominance of the first wave of ankle plantar flexor moment [16] (Table 1) (Figure 1).
In 2021, Westberry et al [17] proposed a modification to the Alvarez classification, replacing the kinematic assessment of the first ankle rocker with the use of sagittal ankle kinetics. They introduced the presence of a dorsiflexor moment within the initial 10% of the gait cycle as the defining criterion for the first ankle rocker (Figure 2).
Three-dimensional gait analysis adds diagnostic and prognostic value to ITW. Efforts are being made to correlate the most effective treatments for each level of severity. However, criticism exists regarding this analysis method, as the environment in which the gait is performed may lead the child to walk differently from their habitual gait. Studies are investigating alternative methods, such as using inertial sensor garments (wearables) [18], though this technique is still under investigation.
The most common treatment methods described in the literature include physical therapy, sensory therapy, serial casting, botulinum toxin A (BoNT-A) injections, orthotic use (2-10 weeks), pyramid insoles, and surgical gastrocsoleus lengthening with or without the use of casting and orthotics.
This study aims to organize the new information available on this subject, providing a critical overview and identifying areas for potential future research.
2. Materials and Methods
This literature review was conducted following PICO (Population, Intervention, Comparison, and Outcome) model as the search framework for terms. The following databases were searched from September 2022 to June 2023: Ovid MEDLINE, EBSCO, Embase, CINAHL Plus, and PubMed. The keywords were: idiopathic toe walking, tiptoe walking, tiptoe gait, gait and toe walking gait. Inclusion criteria comprised studies involving children diagnosed with ITW discussing diagnosis, risk factors, classifications, treatment, and prognosis. We analyzed data published in peer-reviewed journals in English. Case reports and studies exclusively focused on patients with cerebral palsy or primary Achilles tendon contractures were excluded. The selection process involved reading abstracts, and if they did not meet the exclusion criteria, full articles were assessed.
3. Results
3.1. Age
Kelly (1997) [1] and Sutherland [2] consider idiopathic toe walking (ITW) to be the persistence of toe walking beyond the age of three. Sobel (1997) [14], when evaluating children who predominantly walked on their toes since the initiation of walking, observed that 35% of children continued this pattern until age two, and 7% between 9 and 15 years. Engstrom (2018) [8] noted that 79% of children with idiopathic toe walking ceased toe walking naturally by the age of ten.
Despite the evident spontaneous improvement in the majority of children, studies by Sobel et al. (1997) [14] and Engelbert (2011) [5] demonstrate that children who persist with idiopathic toe walking without undergoing treatment have higher rates of shortening and contracture of the calf muscles.

Table 2.
Studies evaluating spontaneous resolution of ITW.
| Article | Authors (Publication Year) | Journal, Publication year (impact factor 22/23) | Number of ITW in the sample/Number of the population in the study | Average age at the beginning of the study (years) | Conclusions of the study |
|---|---|---|---|---|---|
| Idiopathic Toe-Walking: Prevalence and Natural History from Birth to Ten Years of Age | Engstrom P, Tedroff K (2018) [8] | The Journal of Bone and Joint Surgery (5,3) | 63/1401 |
5.5 | - 79% of children with ITW ceased toe walking by age 10. - Among 4 cases of Achilles tendon contractures (defined as <10°of ankle dorsiflexion), 2 maintained 5°, one worsened from 10° to 5°, and one progressed from 10/15° to 0° bilaterally. |
| Effect of Persistent Toe Walking on Ankle Equinus |
Sobel E, Caselli M. A, Velez Z (1997) [14] | Journal of the American Podiatric Medical Association (0,7) |
60/- | 3.5 | - There was a male predominance in ITW cases (non-significant p-value). - ITW begins right from the onset of a child's walking, which differs from cases of cerebral palsy. - Approximately 30% of cases have a positive family history. - The average dorsiflexion angle measures 6.2°. - 35% of children exhibited ITW at the age of 2, and 7% between 9 and 15 years. - The presence of ITW decreases with increasing age, accompanied by a decrease in dorsiflexion angle. |
3.2. Etiology and Risk Factors
Regarding etiology and potential risk factors, there is ongoing research into family history. In Sobel's study (1997) [14], a positive family history was present in 30% of cases, while Fox et al (2006) [19] reported 43.3%, Hirsh and Wagner (2004) [20] reported 57%, and Katz and Mubarak (1984) [13] reported 88%. It is important to note that Katz and Mubarak (1984) [13] identified an autosomal dominant condition in the investigation of Achilles tendon contracture. Although these are different conditions, it is not a factor that can be completely ignored.
Pomarino and colleagues conducted two studies [21,22] on genetic influence on the development of this condition. They observed a higher predominance in male children, raising the question of whether this pathology could have an X-linked recessive autosomal cause, associated with 30% to 42% paternal family history presence.
Table 3.
Studies demonstrating a possible genetic association in children with ITW.
| Authors (Publication Year) | Journal (Impact Factor 22/23) | Percentage of children with positive family history |
|---|---|---|
| Katz and Mubarak (1984) [13] | Journal of Pediatric Orthopaedics (1,7) | (88%) |
| Sobel (1997) [14] | Journal of the American Podiatric Medical Association (0.678) | (30%) |
| Fox (2006) [19] | Acta Orthopædica Belgica (0,35) | (43,3%) |
| Hirsh and Wagner (2004) [20] | International Journal of Pediatrics (5) | (57%) |
| Pomarino (2012) [21] | Foot and Ankle Specialist (0,562) | (30-42%) |
Furthermore, some studies have proposed an association of ITW with SPD [12,23]. It is known that patients diagnosed with Autism Spectrum Disorder (ASD) might have a higher prevalence of ITW - up to 20.1% - with a high rate of tight heel cords (12%) [24,25]. Since patients with ASD frequently present higher rates of SPD, one might take this into account as a possible target in the treatment of ITW.
New studies are also investigating neurological changes between children with and without ITW. Donne et al. (2022) [26] found differences in the neural pathway activation in their study, as the toe walking group showed lower activation in the left frontal lobe region, which indicates a somatosensory difference between groups. However, more studies are needed to determine the true impact of these differences.
3.3. Classification of ITW
One of the first reference points to define treatment approaches in different clinical conditions is the severity classification. The most widely used classification for ITW is Alvarez's (2007) [16], which is based on the presence or absence of the three ankle rocker mechanisms. This classification has been considered highly sensitive according to the Cochrane systematic review by Caserta et al (2019) [27].
Other aspects have formed the basis for additional classifications. For instance, O’Sullivan's proposal (2018) [28] divides children into typical and ITW, based on differences in gait analysis. Additionally, there are classifications based on anatomical features, as described by Pomarino [29], highlighting differences in calf shape, forefoot, and Achilles tendon, among others.
Bauer et al (2022) [30] introduced a descriptive classification for children who walk on their toes. In a straightforward manner, they divided it into toe walking during developmental stages, ITW with autism, congenital tendon contracture, habitual persistent ITW (without contracture), and finally, persistent ITW with contracture (Figure 3).
3.4. Treatment
The literature shows different management options for ITW, including conservative methods such as physiotherapy, orthotics, serial casting, and foot orthoses. Invasive approaches, such as surgical procedures (percutaneous or open), are also considered (Table 4).
Table 4.
Studies that investigated treatment options for ITW.
| Article (Publication Year) | Authors | Journal (Impact Factor) | Number of ITW sample | Mean age at the beginning of intervention (years) | Mean time of follow-up (years) | Conclusions of the study |
|---|---|---|---|---|---|---|
| Outcomes of Noninvasively Treated Idiopathic Toe Walkers (2017) |
Radke K, Karch N, Goede F, Vaske B, Von Lewinsky G, Noll Y, Thren A [11] | Foot & Ankle Specialist (0.562) | 101 | 7.75 (2-17) |
1.94 | Pyramidal insoles: - 95.5% were used in conjunction with physiotherapy. - 60% were used in conjunction with orthotics. → Resulted in a 95.8% cessation of ITW. |
| Surgical Outcomes for Severe Idiopathic Toe Walkers (2021) | Westberry D. E, Carpenter A. M, Brandt A, Barre A, Hilton S. B, Sarawat P, Davids J. R [17] | Journal of Pediatric Orthopaedics (1,7) | 26 | 9 (6.7-16.8) | 3.6 | Surgery: - 100% improvement in ITW for those operated on in zone III, and 88% for those in zone II. |
| Serial casting in the treatment of idiopathic toe-walkers and review of the literature (2006) |
Fox A, Deakin S, Petigrew G, Paton R [19] | Acta Orthopædica Belgica (0,35) | 44 | 6.08 (2-14.3) | 1.1 | Serial casting + stretching: → Among 44 cases, 29 (66%) showed a reduction or cessation of ITW and an increase in dorsiflexion |
| The natural history of idiopathic toe-walking: a long-term follow-up of fourteen conservatively treated children (2004) |
Hirsch G, Wagner B [20] | Acta Paediatrica (3,8) | 14 | 6.45 (3-9.9) | 14.5 | Combination of physiotherapy, stretching, casting, orthotics: - 100% combined with stretching. - 35.7% used in conjunction with orthotics or casting. → Among 14 cases, 8 (57.1%) children ceased ITW. |
| Idiopathic Toe-Walking: Does Treatment Alter the Natural History? (2000) | Eastwood D. M, Menelaus M.B, Dickens R.V.D, Broughton N. S, Cole W. S, Se M [32] | Journal of Pediatric (2,99) | 136 | Group: Observational: 4 (1.5-10) Group: Casting: 3.5 (1.5-10.3) Group: Surgical: 6.5 (2.5-14.5) |
Group: Observational: 3.2 Group: Casting: 3.7 Group: Surgical: 7.9 |
Three groups (observational, casting, and surgical): - Observational: Improvement of ITW in 45% and cessation in 12%. - Casting: Improvement of ITW in 41% and cessation in 22%. - Surgical: Reduction of ITW by 50% and cessation by 37%. |
| Does botulinum toxin A improve the walking pattern in children with idiopathic toe-walking? (2010) |
Engstrom P, Gutierrez-Farewik E. M, Bartonek A, Tedroff K, Orefelt C, Haglund-A˚kerlind Y [33] | Journal of Children's Orthopaedics (1,38) | 15 | (5-13), Median 9 | 1 | BoNT-A+ stretching: → Improvement in 4 out of 11 cases (36.4%) and cessation in 3 out of 11 cases (27.3%) |
| Serial ankle casts for patients with idiopathic toewalking: effects on functional gait parameters (2019) |
Thielemann F, Rockstroh G, Mehrholz J, Druschel C [34] | Journal of Children Orthopaedics (1,38) | 10 | (5-15) | < 1 | Casting: - Improvement in gait analysis criteria. |
| Habitual toe-walkers. A clinical and electromyographic gait analysis (1977) | Griffin P. P, Wheelhouse W. W, Shiavi R, Bass W [36] | Journal of Bone and Joint Surgery (5,3) | 6 | 6 (5-9) | <1 | Casting: → Improvement of ITW in 100% |
| Long-term gait outcomes following conservative management of idiopathic toe walking (2018) Group: Casting + BoNT-A : 7.2 (4.3-12.2) |
Davies K, Black A, Hunt M, Holsti L [37] | Gait & Posture (2,4) | 34 | Group: Casting + BoNT-A : 7.2 (4.3-12.2) Group: Stretching: 8.7 (4.9-13) Group: Stretching: 8.7 (4.9-13) |
13.4 |
Two groups: Casting + BoNT-A ; Stretching - Casting + BoNT-A : Improvement of ITW in 74%. - Stretching: Improvement of ITW in 35%. - Improvement in gait analysis criteria observed in both groups. |
| IncobotulinumtoxinA Injection for Treating Children with Idiopathic Toe Walking: A Retrospective Efficacy and Safety Study (2022) |
Fillipetti M, Picelli A, Di Censo R, Vantim S, Randazzo P. N, Sandrini G, Tassorelli C, De Icco R, Smania N, Tamburin S [38] |
Toxins (4,2) |
28 | 8.3 (Standard Deviation 3.1) |
<1 | Incobotulinumtoxin A: → Improvement in dorsiflexion |
| Botulinum Toxin A Does Not Improve the Results of Cast Treatment for Idiopathic Toe-Walking (2013) |
Engstrom P, Bartonek A, Tedroff K, Orefelt C, Haglund-A˚kerlind Y, Gutierrez-Farewik E. M [39] | Journal of Bone and Joint Surgery-American (5,3) | 47 | 9.4 (5-14.5) | 1 | Casting with and without BoNT-A: → No improvement in gait analysis parameters was observed with the addition of BoNT-A. |
| Orthotic treatment of idiopathic toe walking with a lower leg orthosis with circular subtalar blocking (2021) |
Berger N, Bauer M, Hapfelmeier A, Salzmann M, Prodinge P. M [42] | BMC Musculoskeletal Disorders (2,3) | 22 | 7 (2.5-13.1) | 2 | Orthoses: - Improvement of ITW by 73% in 1 year, and 64% in 2 years |
| Effects of wearing a foot orthosis on ankle function in children with idiopathic toe walking during gait (2022) | Brasiliano P, Alvini M, Di Stanislao E, Vannozzi G, Di Rosa G, Camomilla V [43] | Heliyon (3,7) | 21 | 8.3 (5-12) | 1.3 | Orthosis: - Improvement of ITW by 82% - Enhancement of gait analysis criteria |
| A comparison of orthoses in the treatment of idiopathic toe walking: A randomized controlled trial (2015) |
Herrin K, Geil M [44] | Prosthetics and Orthotics International (1,6) | 18 | Group: Ankle and Foot Orthosis: 5.4 Group: Foot Orthosis: 4.6 |
<1 | 2 groups (ankle-foot and foot orthoses): - Ankle-foot orthosis group: 63% improvement in ITW - Foot orthosis group: 38% improvement in ITW |
| Outcome after conservative and operative treatment of children with idiopathic toe walking: a systematic review of literature (2014) |
Van Bemmel A. F, Van de Graaf, V. A, Van den Bekeom M. P. J, Vergroesen D. A [45] | Musculoskeletal Surgery (0,67) | 298 | Group: Casting 4.9 (3.3-6.8) Group: Surgical 9 (3.9-12.1) |
Group: Casting 3.4 Group: Surgical 4.2 |
Surgery vs. Serial Casting: - Surgery resulted in higher dorsiflexion values. Gait improvement in 52.5% - Serial casting led to an improvement of 47.9% |
| Long term gait outcomes of surgically treated idiopathic toe walkers (2016) | McMulking M. L, Gordon A. B, Tompkins B. J, Caskey P. M, Baird G. O [46] | Gait & Posture (2,4) | 8 | 9 (6.4-11.3) | 5 | Surgery: - 87.5% improvement in ITW (7 out of 8 with first rocker) - Enhancement of gait analysis criteria |
| Outcome of Patients After Achilles Tendon Lengtheningfor Treatment of Idiopathic Toe Walking (2006) | Hemo Y, Macdessi S. J, Pierce R. A, Aiona M. D, Sussman M. D [47] | Journal of Children's Orthopaedics (1,38) | 15 | 9 (4.2-13.1) | 2.9 | Surgery: - Enhancement of gait analysis criteria - May lead to knee hyperextension (recurvatum) |
Conservative therapies (physiotherapy, serial casting, orthotics, and BoNT-A)
Evaluation of the effectiveness of stretching and physiotherapy sessions as a curative approach to equinus gait was discussed and their efficacy was compared to more invasive techniques. When used in isolation, these methods did not show effectiveness [31].
Other techniques have also been investigated, including the use of pyramidal insoles, serial casting, botulinum toxin (BoNT-A) injections, and orthotics. To date, there's only one study published in English evaluating the outcomes of the use of pyramidal insoles [11] and one review [29] where the main author cites 4 other studies published in German, reporting a success rate of this approach to be between 70%-95,8% [11,29]. Despite these studies demonstrating positive results, they often combined insoles with other therapies involving orthotics, BoNT-A injections, and physiotherapy. Furthermore, they did not have a control group, making it challenging to assess the actual effectiveness of the treatment or whether the good outcomes were not related to the natural history of the disease.
The use of serial casting has shown favorable outcomes in some studies [19,20,32], including increased ankle dorsiflexion, cessation of idiopathic toe walking, and parental satisfaction with the final results. These positive effects have been observed even in older patients [35,36]. However, some authors still question whether these outcomes could be a result of the natural progression of the condition [32,35,36]. Eastwood (2000) suggests that 50% of children might experience spontaneous improvement [32].
A notable point in serial casting studies is the proposal by Fox et al. (2006) [19] to measure ankle dorsiflexion with the knee flexed, as this seems to be a more accurate indicator of improvement in idiopathic toe walking than measuring with the knee in extension. Fox's study showed that while 100% of participants improved ankle dorsiflexion with the knee in extension, only 66% experienced improvement in flexion. Additionally, Davies' study (2018) [37] highlighted compensatory changes observed in older children, such as greater restriction of passive ankle dorsiflexion and compensatory knee hyperextension in both groups. These changes could be due to increased skeletal maturity or longer follow-up periods.
Regarding BoNT-A injections, some studies indicate positive outcomes with improvements in ankle dorsiflexion and other gait parameters [33,37,38], while others do not show significant improvement in idiopathic toe walking [39,40]. Engstrom and colleagues conducted two studies [33,39]; the first showed a positive effect on idiopathic toe walking improvement when BoNT-A was used in combination with isolated physiotherapy [33], but the later study in 2013 [39] found no superiority of BoNT-A combined with serial casting over serial casting without BoNT-A. Caserta et al (2019)[27], in a Cochrane review, concluded that there aren't sufficient studies to confirm that combining BoNT-A with serial casting is superior to using serial casting alone. In addition, Satila et al. conducted a randomized controlled trial in 30 children with ITW [41], dividing them into 2 groups: (1) a conservative treatment with firm shoes, night splints, a home stretching program and physical therapy and (2) the same approach with the addition of BoNT-A injections. They reported 38 adverse effects in the BoNT-A group (16 patients treated with 30 injections) and none in the conservative group. No significant differences between the treatment groups in function or ankle range of motion ensued at 24 months posttreatment.
Positive results in the short-term follow-up have been reported [42,43,44] in the use of orthotics for ITW. However, ongoing research aims to determine the most effective types of orthotics, suitable age groups, the optimal duration of use, and how long the effects of the intervention last, among other factors. There is no evidence to prove the standalone effectiveness of orthotics as a primary treatment option for ITW.
Invasive Therapies: Surgical Procedures
There is a consensus that the surgical approach might have better outcomes in treating ITW, as has been shown in several studies [17,32,45,46]. However, there is still a lack of studies addressing the most suitable techniques for different age groups and severity levels. In the study by Westberry et al (2020) [17], which evaluated 26 patients classified as severe according to Alvarez's classification [16], an 88% improvement was observed with the triceps surae surgical lengthening in zone II, and 100% improvement was seen in those operated in zone III. Among those operated in zone III, none required re-intervention. However, not all children had their symptoms completely resolved; out of the 21 children operated using this technique, 14 were subsequently classified as moderate and 7 as mild. Among children undergoing lengthening in zone II, out of the 25 operated extremities, 6 extremities required surgical re-intervention.
Possible complications after surgery include tendonitis, wound dehiscence, and pain, among others. However, these complications have a low incidence and are easily resolved in most cases. Compensatory changes such as knee hyperextension (recurvatum) may also occur [29,47], necessitating longer follow-up studies to assess the presence of further abnormalities and the impacts of each of these changes.
4. Discussion
Despite the heterogeneity in the methodologies of the analyzed studies, certain observations can be made. The determination of relevant etiological and prognostic factors is still under analysis. A trend towards higher prevalence in boys with a positive family history exists, but the inheritance of the condition remains inconclusive, and higher-level evidence studies are required to confirm these theories. In addition, the association of ITW with SPD and ASD is well established, nonetheless not as a causative factor since many children that present with ITW do not present these conditions.
Regarding the final age of spontaneous resolution, there is variability in the reports for the percentage of children who cease ITW. Ranging from 30% to 88%, it's important to question the reference age used by each author. Engstrom (2018) [8] uses a milestone of 5.5 years, while Kelly (1997) [1] uses 3 years. Thus, some patients showing resolution in Engstrom's study might not have been considered by Kelly, making direct comparison difficult. Furthermore, the follow-up time of studies is questionable. In Engstrom's study (2018) [8], children with neurodevelopmental disorders - which were not specified - were included in the ITW cohort. Despite this finding, most of the patients ceased toe walking spontaneously, thereby possibly overestimating the value of the prevalence of ITW in the general population.
In terms of etiology and risk factors, authors such as Fox [19] and Sobel [14] did not find statistically significant evidence for correlations with other demographic data such as sex, gestational age, and age at diagnosis, among others. However, it's important to consider that the lack of statistical relevance might be due to the small sample size of the cohorts, especially since sex seems to have clinical relevance in discussions from certain studies [14,19,21,22]. As for age, there seems to be a negative correlation between ankle dorsiflexion and age, a hypothesis supported by some studies [37,48], which agree with the normative data for normal individuals shown in 2 studies [49,50].
Some authors have raised critical views about established standards of three-dimensional gait analysis, which warrant further investigation and studies to strengthen these opinions. For example, Brasiliano et al. (2023) [51] suggest increased accuracy using multi-segmented three-dimensional gait analysis incorporating foot models. Westberry et al. [17] proposed a modification to Alvarez's classification [16], utilizing the sagittal ankle moment in kinetics to define the first rocker instead of kinematic assessment, as it provides a better representation of the foot's position relative to the tibia, yielding a more precise measure. However, it is important to recognize that three-dimensional gait analysis can only recognize the children's walking pattern in a "snapshot in time", which might not reflect the habitual walking pattern of the patient since these patients can voluntarily correct their gait at their will [6]. Further studies should establish a correlation between habitual walking patterns using sensors and three-dimensional gait analysis.
Methods such as stretching, physiotherapy exercises, pyramidal insoles, and BoNT-A do not have strong evidence of effectiveness when used in isolation. Many studies have assessed these techniques in combination, making it difficult to distinguish the effect of each one in isolation [11,19,20,33]. It's important to question if the positive effects seen in conservative treatment methods are due to the small sample size, the short follow-up periods that might not account for future presentations, or if they are simply a result of the natural progression of the condition. Weighing the risks and benefits of each therapy individually may be the best approach regarding those options.
The most evidence-based conservative measure is serial casting followed by orthotics. Randomized clinical trials are needed to define optimal casting intervals and orthotic usage, given the heterogeneity across studies. Long-term effects also require investigation. Davies (2018) [37] noted greater knee hyperextension in the stance phase and reduced flexion in the swing phase of gait after serial casting, whereas Engstrom et al. (2013) [39] reported less knee hyperextension in the stance phase and increased knee flexion in the swing phase. Davies attributed these differences to the varying follow-up durations: Davies' study spanned 12 years, while Engstrom's was only 12 months. The population in the former study also had a higher average age than in the latter. Further research is necessary in this area, but serial casting seems to be a good option for gaining ankle dorsiflexion range of motion in mild contractures to improve ankle kinetics and kinematics in the short term.
There is growing evidence of the benefits of surgery in ITW, ranging from symptom reduction to complete resolution in the long term [17,32,45,46,47]. For severe cases aged near or above 10 years, the technique of open or percutaneous lengthening in zone III is considered the best choice [17]. However, there are few robust studies that adequately address these questions, demanding randomized clinical trials and better long-term follow-up of proposed interventions.
In our clinical experience, post-treatment follow-up often reveals other pre-existing orthopedic conditions such as increased tibial external rotation and flexible flat feet. This underscores the importance of conducting a thorough physical exam before treatment and emphasizes the need to educate parents and children about these issues, which might be more evident after treatment. Further research is warranted to validate these findings, highlighting the significance of early assessment and the value of informing patients and their families about these potential concerns.
Finally, the lack of consensus in results is apparent due to the heterogeneity in methodologies, as discussed by Caserta et al. (2019) [40] in their systematic review of outcomes and assessment tools, as well as in Bauer’s (2022) [30] and Williams' (2020) [52] findings, which identified a lack of consensus among healthcare professionals regarding evidence-based therapies. Heterogeneity is seen in populations across studies [32,37,45], the type of severity classification used [29,32,42], previous treatments [46,47], and different exclusion criteria [19,42], among other differences, making results comparison unfeasible. For future studies, larger study populations, standardized techniques and follow-up durations, and defined outcome metrics are essential.
This study has some limitations. First, it was restricted to articles in English, excluding some studies in languages like Russian, Italian, Spanish, and others. Second, the methodological heterogeneity of the analyzed articles makes it difficult to extrapolate and compare results. Third, the evaluation included studies other than randomized clinical trials, which decreases the overall evidence levels of the studies reported.
5. Conclusions
Despite the significant heterogeneity in methodologies across studies, it was possible to note a growing trend toward investigating etiological factors, particularly genetic and neurosensory factors, as well as prognostic factors like age, Achilles tendon contractures, and gender. There appears to be a higher prevalence in boys with a positive family history, yet the genetic inheritance aspect remains inconclusive.
Novel classifications have been proposed, based on anatomical features and three-dimensional gait analysis, aiming to differentiate severity, prognosis, and differential diagnoses. Treatment options encompass both conservative and surgical alternatives. Among conservative approaches, there is stronger evidence of gait improvement in equinus gait through the use of serial casting followed by orthotics, while the addition of BoNT-A has not shown better results. There is no evidence of sustained improvement with isolated physiotherapy exercises and stretching, but these may be recommended in conjunction with other therapies. Regarding surgical procedures, they are reserved for patients with Achilles tendon contractures, with better outcomes observed in severe cases, as per Alvarez's classification, who undergo lengthening in Zone III and are nearly 10 years of age or older. However, more robust studies, preferably randomized clinical trials, are needed to establish clearer conclusions about treatment protocols to be used in patients with ITW.
Author Contributions
Conceptualization, L.D.L.S. and F.M.B.; Methodology, L.D.L.S. and F.M.B.; Writing—original draft preparation, L.D.L.S. and F.M.B.; Writing—review and editing, L.D.L.S., F.M.B., T.O.G., L.R.A.A., F.C.B.; Supervision, F.M.B.; Project administration, F.M.B.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kelly IP: Jenkinson A, Stephens M, O’Brien T. The Kinematic Patterns of Toe-Walkers. Journal of Pediatric Orthopaedics. 1997 Jul;17(4):478–80. [CrossRef]
- Sutherland D. The development of mature gait. Gait & Posture. 1997 Oct;6(2):163–70.
- Sala DA, Shulman LH, Kennedy RF, Grant AD, Chu MLY. Idiopathic toe-walking: a review. Developmental Medicine & Child Neurology. 1999 Dec;41(12):846–8.
- Haynes KB, Wimberly RL, VanPelt JM, Jo CH, Riccio AI, Delgado MR. Toe Walking: A Neurological Perspective After Referral From Pediatric Orthopaedic Surgeons. Journal of Pediatric Orthopaedics. 2018 Mar;38(3):152–6. [CrossRef]
- Engelbert R, Gorter JW, Uiterwaal C, van de Putte E, Helders P. Idiopathic toe-walking in children, adolescents and young adults: a matter of local or generalised stiffness? BMC Musculoskeletal Disorders. 2011 Mar 21;12(1).
- Westberry DE, Davids JR, Davis RB, de Morais Filho MC. Idiopathic Toe Walking. Journal of Pediatric Orthopaedics. 2008 Apr;28(3):352–8.
- Oetgen ME, Peden S. Idiopathic Toe Walking. Journal of the American Academy of Orthopaedic Surgeons. 2012 May;20(5):292–300.
- Engström P, Tedroff K. Idiopathic Toe-Walking: Prevalence and Natural History from Birth to Ten Years of Age. Journal of Bone and Joint Surgery. 2018 Apr 18;100(8):640–7. [CrossRef]
- Engström P, Tedroff K. The Prevalence and Course of Idiopathic Toe-Walking in 5-Year-Old Children. Pediatrics. 2012 Aug 1;130(2):279–84. [CrossRef]
- Hall JE, Salter RB, Bhalla SK. CONGENITAL SHORT TENDO CALCANEUS. The Journal of Bone and Joint Surgery British volume. 1967 Nov;49-B(4):695–7.
- Radtke K, Karch N, Goede F, Vaske B, von Lewinski G, Noll Y, et al. Outcomes of Noninvasively Treated Idiopathic Toe Walkers. Foot & Ankle Specialist. 2018 Mar 27;12(1):54–61. [CrossRef]
- Williams CM, Tinley P, Curtin M. Idiopathic toe walking and sensory processing dysfunction. Journal of Foot and Ankle Research. 2010 Aug 16;3(1). [CrossRef]
- Katz MM, Mubarak SJ. Hereditary Tendo Achillis Contractures. Journal of Pediatric Orthopaedics. 1984 Nov;4(6):711–4. [CrossRef]
- Sobel E, Caselli M, Velez Z. Effect of persistent toe walking on ankle equinus. Analysis of 60 idiopathic toe walkers. Journal of the American Podiatric Medical Association. 1997 Jan 1;87(1):17–22.
- Lindsay SE, Bauer J, Bouton D, Do P, Woodmark C, Sienko S, et al. Patient-Reported Outcome Measurement Information System (PROMIS) Scores in Pediatric Idiopathic Toe Walkers. Journal of Pediatric Orthopaedics. 2022 Jun 29;42(8):e878–81. [CrossRef]
- Alvarez C, De Vera M, Beauchamp R, Ward V, Black A. Classification of idiopathic toe walking based on gait analysis: Development and application of the ITW severity classification. Gait & Posture. 2007 Sep;26(3):428–35. [CrossRef]
- Westberry DE, Carpenter AM, Brandt A, Barre A, Hilton SB, Saraswat P, et al. Surgical Outcomes for Severe Idiopathic Toe Walkers. Journal of Pediatric Orthopaedics. 2020 Dec 22;41(2):e116–24. [CrossRef]
- Brasiliano P, Mascia G, Di Feo P, Di Stanislao E, Alvini M, Vannozzi G, et al. Impact of Gait Events Identification through Wearable Inertial Sensors on Clinical Gait Analysis of Children with Idiopathic Toe Walking. Micromachines. 2023 Jan 21;14(2):277. [CrossRef]
- Fox A, Deakin S, Pettigrew G, Paton R. Serial casting in the treatment of idiopathic toe-walkers and review of the literature. Acta Orthop Belg. 2006; 72(6): 722-30.
- Hirsch G, Wagner B. The natural history of idiopathic toe-walking: a long-term follow-up of fourteen conservatively treated children. Acta Paediatrica. 2007 Jan 2;93(2):196–9.
- Pomarino D, Ramírez Llamas J, Pomarino A. Idiopathic Toe Walking. Foot & Ankle Specialist. 2016 Jul 7;9(5):417–22.
- Pomarino D, Thren A, Morigeau S, Thren JR, Emelina AA. Genetic Factors Associated with Toe Walking in Children. Current Pediatrics. 2020 Jun 21;19(2):146–9. [CrossRef]
- Williams CM, Tinley P, Curtin M, Wakefield S, Nielsen S. Is Idiopathic Toe Walking Really Idiopathic? The Motor Skills and Sensory Processing Abilities Associated With Idiopathic Toe Walking Gait. Journal of Child Neurology. 2013 Jan 24;29(1):71–8. [CrossRef]
- Barrow WJ, Jaworski M, Accardo PJ. Persistent Toe Walking in Autism. Journal of Child Neurology. 2011 Jan 31;26(5):619–21. [CrossRef]
- Leyden J, Fung L, Frick S. Autism and toe-walking: Are they related? Trends and treatment patterns between 2005 and 2016. Journal of Children’s Orthopaedics. 2019 Aug;13(4):340–5. [CrossRef]
- Donne J, Farrell MJ, Kolic J, Powell J, Fahey M, Williams C. Two-point discrimination responses in children with idiopathic toe walking: A feasibility fMRI study. Science Progress. 2022 Oct;105(4):003685042211321. [CrossRef]
- Caserta AJ, Pacey V, Fahey MC, Gray K, Engelbert RH, Williams CM. Interventions for idiopathic toe walking. Cochrane Database of Systematic Reviews. 2019 Oct 6;
- O’Sullivan R, Munir K, Keating L. Idiopathic toe walking—A follow-up survey of gait analysis assessment. Gait & Posture. 2019 Feb;68:300–4. [CrossRef]
- Pomarino D, Ramírez Llamas J, Martin S, Pomarino A. Literature Review of Idiopathic Toe Walking: Etiology, Prevalence, Classification, and Treatment. Foot & Ankle Specialist. 2017 Jan 16;10(4):337–42. [CrossRef]
- Bauer JP, Sienko S, Davids JR. Idiopathic Toe Walking: An Update on Natural History, Diagnosis, and Treatment. Journal of the American Academy of Orthopaedic Surgeons. 2022 Sep 7;30(22):e1419–30.
- Clark E, Sweeney JK, Yocum A, McCoy SW. Effects of Motor Control Intervention for Children With Idiopathic Toe Walking. Pediatric Physical Therapy. 2010;22(4):417–26. [CrossRef]
- Eastwood DM, Menelaus MB, Dickens RDV, Broughton NS, Cole WG. Idiopathic Toe-Walking: Does Treatment Alter the Natural History? Journal of Pediatric Orthopaedics, Part B. 2000 Jan;9(1):47–9.
- Engström P, Gutierrez-Farewik EM, Bartonek Å, Tedroff K, Orefelt C, Haglund-Åkerlind Y. Does botulinum toxin A improve the walking pattern in children with idiopathic toe-walking? Journal of Children’s Orthopaedics. 2010 Aug;4(4):301–8.
- Thielemann F, Rockstroh G, Mehrholz J, Druschel C. Serial ankle casts for patients with idiopathic toe walking: Effects on functional gait parameters. Journal of Children’s Orthopaedics. 2019 Apr;13(2):147–54. [CrossRef]
- Brouwer B, Davidson LK, Olney SJ. Serial Casting in Idiopathic Toe-Walkers and Children with Spastic Cerebral Palsy. Journal of Pediatric Orthopaedics. 2000 Mar;20(2):221–5. [CrossRef]
- Griffin P, Wheelhouse W, Shiavi R, Bass W. Habitual toe-walkers. A clinical and electromyographic gait analysis. The Journal of Bone & Joint Surgery. 1977 Jan;59(1):97–101. [CrossRef]
- Davies K, Black A, Hunt M, Holsti L. Long-term gait outcomes following conservative management of idiopathic toe walking. Gait & Posture. 2018 May;62:214–9. [CrossRef]
- Filippetti M, Picelli A, Di Censo R, Vantin S, Randazzo PN, Sandrini G, et al. IncobotulinumtoxinA Injection for Treating Children with Idiopathic Toe Walking: A Retrospective Efficacy and Safety Study. Toxins. 2022 Nov 13;14(11):792. [CrossRef]
- Engström P, Bartonek Å, Tedroff K, Orefelt C, Haglund-Åkerlind Y, Gutierrez-Farewik EM. Botulinum Toxin A Does Not Improve the Results of Cast Treatment for Idiopathic Toe-Walking. Journal of Bone and Joint Surgery. 2013 Mar 6;95(5):400–7. [CrossRef]
- Caserta A, Morgan P, Williams C. Identifying methods for quantifying lower limb changes in children with idiopathic toe walking: A systematic review. Gait Posture. 2019;67:181–6. [CrossRef]
- Sätilä H, Beilmann A, Olsén P, Helander H, Eskelinen M, Huhtala H. Does Botulinum Toxin A Treatment Enhance the Walking Pattern in Idiopathic Toe-Walking? Neuropediatrics. 2016;47(3):162–8.
- Berger N, Bauer M, Hapfelmeier A, Salzmann M, Prodinger PM. Orthotic treatment of idiopathic toe walking with a lower leg orthosis with circular subtalar blocking. BMC Musculoskeletal Disorders. 2021 Jun 7;22(1).
- Brasiliano P, Alvini M, Di Stanislao E, Vannozzi G, Di Rosa G, Camomilla V. Effects of wearing a foot orthosis on ankle function in children with idiopathic toe walking during gait. Heliyon. 2022 Oct;8(10):e11021.
- Herrin K, Geil M. A comparison of orthoses in the treatment of idiopathic toe walking. Prosthetics & Orthotics International. 2016 Apr;40(2):262–9. [CrossRef]
- van Bemmel AF, van de Graaf VA, van den Bekerom MPJ, Vergroesen DA. Outcome after conservative and operative treatment of children with idiopathic toe walking: a systematic review of literature. MUSCULOSKELETAL SURGERY. 2014 Jan 12;98(2):87–93. [CrossRef]
- McMulkin ML, Baird GO, Caskey PM, Ferguson RL. Comprehensive Outcomes of Surgically Treated Idiopathic Toe Walkers. Journal of Pediatric Orthopaedics. 2006 Sep;26(5):606–11. [CrossRef]
- Hemo Y, Macdessi SJ, Pierce RA, Aiona MD, Sussman MD. Outcome of Patients After Achilles Tendon Lengthening for Treatment of Idiopathic Toe Walking. Journal of Pediatric Orthopaedics. 2006 May;26(3):336–40. [CrossRef]
- Shulman LH, Sala DA, Chu MLY, McCaul PR, Sandler BJ. Developmental implications of idiopathic toe walking. The Journal of Pediatrics. 1997 Apr;130(4):541–6. [CrossRef]
- Soucie JM, Wang C, Forsyth A, Funk S, Denny M, Roach KE, et al. Range of motion measurements: reference values and a database for comparison studies. Haemophilia. 2010 Nov 11;17(3):500–7. [CrossRef]
- Liyanarachi S, Hulleberg G, Foss OA. Is Gastrocnemius Tightness a Normal Finding in Children? Journal of Bone and Joint Surgery. 2021 Aug 25;103(20):1872–9.
- Brasiliano P, Alvini M, Di Stanislao E, Vannozzi G, Di Rosa G, Camomilla V. Ankle Kinematics Characterization in Children with Idiopathic Toe Walking: Does the Foot Model Change the Clinical Evaluation? Healthcare. 2023 Mar 16;11(6):873.
- Williams C, Gray K, Davies N, Barkocy M, Fahey M, Simmonds J, et al. Exploring health professionals understanding of evidence based treatment for idiopathic toe walking: a cross-sectional study. [Internet]. Research Square Platform LLC; 2019 Jun [cited 2023 Oct 19]. Available from:. [CrossRef]
Figure 1.
Representation of ankle kinematics and kinetics graphs, illustrating the assessed parameters for Alvarez classification. (Reproduced from Alvarez C, De Vera M, Beauchamp R, Ward V, Black A. Classification of idiopathic toe walking based on gait analysis: Development and application of the ITW severity classification. Gait Posture. 2007;26(3):428–35.) [1.6].
Figure 1.
Representation of ankle kinematics and kinetics graphs, illustrating the assessed parameters for Alvarez classification. (Reproduced from Alvarez C, De Vera M, Beauchamp R, Ward V, Black A. Classification of idiopathic toe walking based on gait analysis: Development and application of the ITW severity classification. Gait Posture. 2007;26(3):428–35.) [1.6].
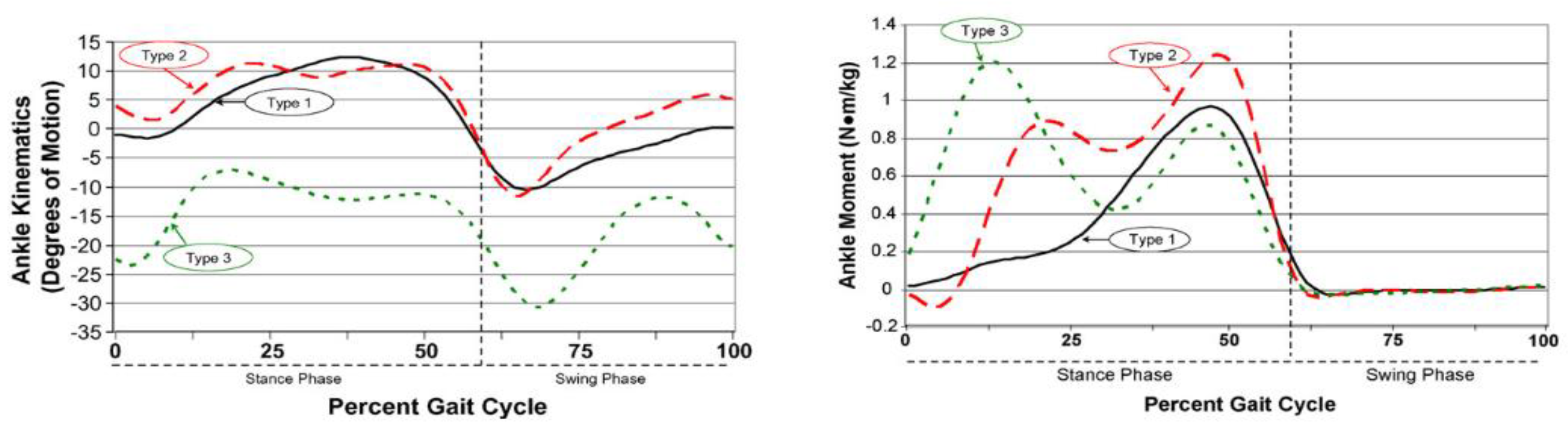
Figure 2.
Representation of the proposed modification by Westberry to the Alvarez first ankle rocker classification, based on the presence of a dorsiflexor moment within the initial 10% of the gait cycle in the sagittal plane ankle kinetics. (Replicated from Westberry DE, Carpenter AM, Brandt A, Barre A, Hilton SB, Saraswat P, Davids JR. Surgical Outcomes for Severe Idiopathic Toe Walkers. J Pediatr Orthop. 2021 Feb 1;41(2):e116-e124. doi: 10.1097/BPO.0000000000001677. PMID: 33405465.) [1.7].
Figure 2.
Representation of the proposed modification by Westberry to the Alvarez first ankle rocker classification, based on the presence of a dorsiflexor moment within the initial 10% of the gait cycle in the sagittal plane ankle kinetics. (Replicated from Westberry DE, Carpenter AM, Brandt A, Barre A, Hilton SB, Saraswat P, Davids JR. Surgical Outcomes for Severe Idiopathic Toe Walkers. J Pediatr Orthop. 2021 Feb 1;41(2):e116-e124. doi: 10.1097/BPO.0000000000001677. PMID: 33405465.) [1.7].
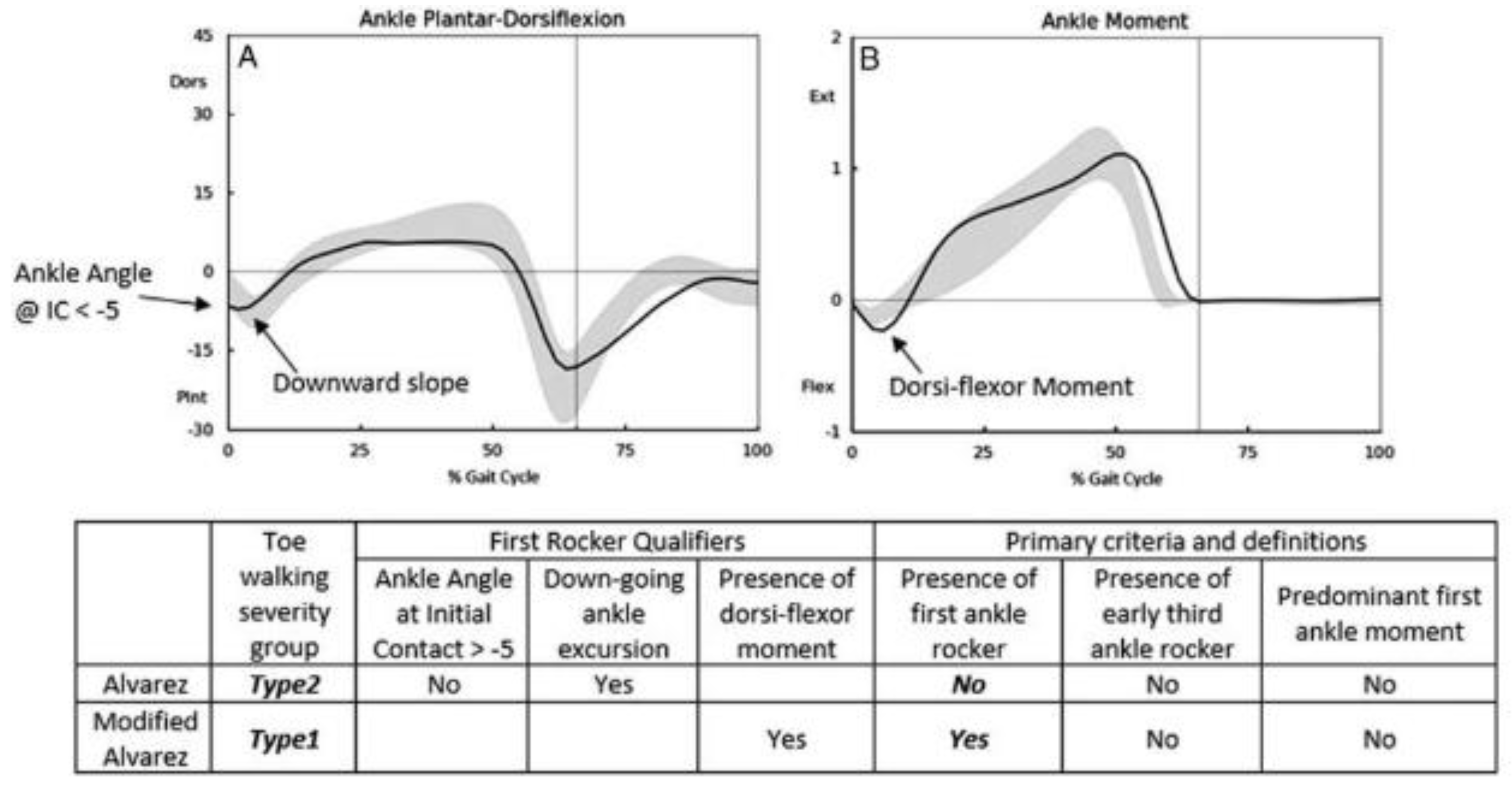
Figure 3.
Idiopathic Toe Walking classification, by Bauer. (Replicated from Bauer, J., Sienko, S. & Davids, J. (2022). Idiopathic Toe Walking: An Update on Natural History, Diagnosis, and Treatment. Journal of the American Academy of Orthopaedic Surgeons, 30 (22), e1419-e1430.) [30].
Figure 3.
Idiopathic Toe Walking classification, by Bauer. (Replicated from Bauer, J., Sienko, S. & Davids, J. (2022). Idiopathic Toe Walking: An Update on Natural History, Diagnosis, and Treatment. Journal of the American Academy of Orthopaedic Surgeons, 30 (22), e1419-e1430.) [30].
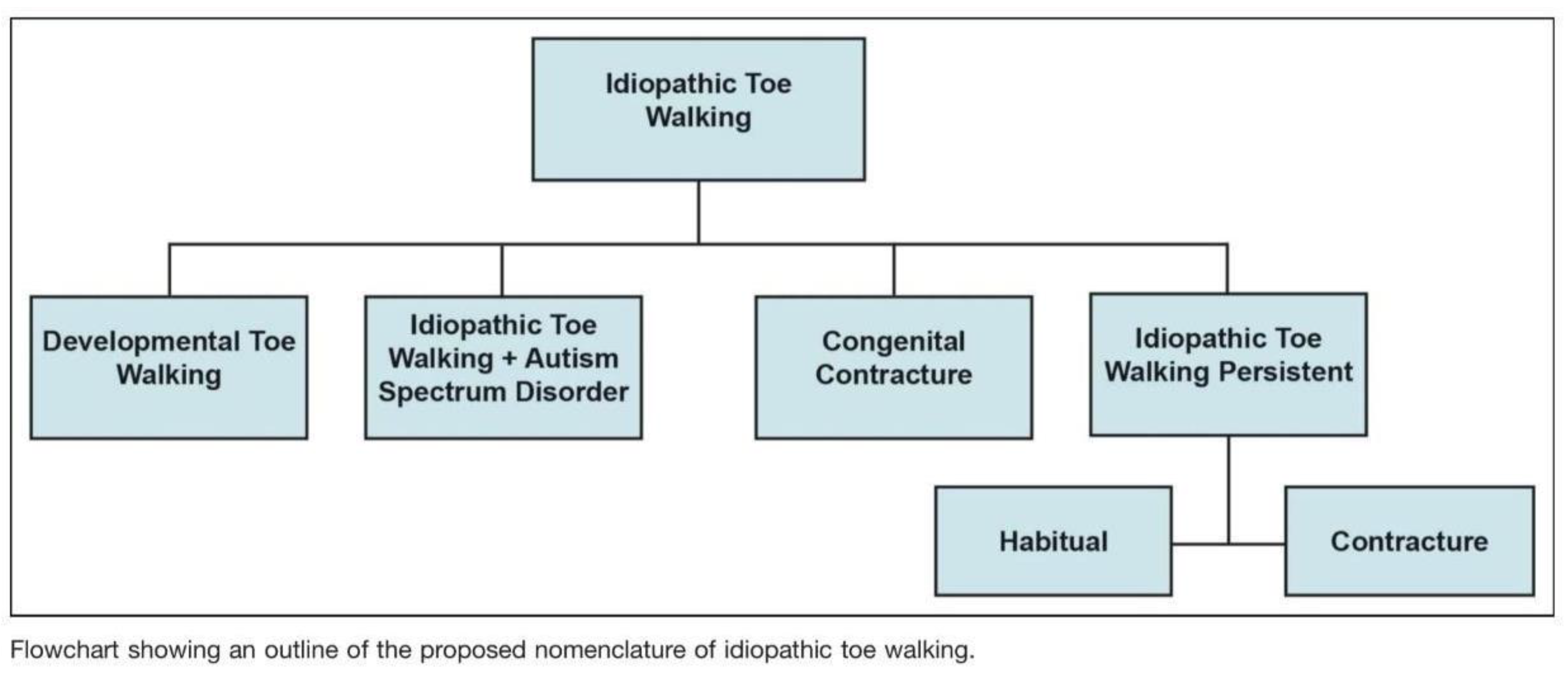
Table 1.
Criteria for ITW Classification. Adapted from Alvarez C, De Vera M, Beauchamp R, Ward V, Black A. (Classification of idiopathic toe walking based on gait analysis: Development and application of the ITW severity classification. Gait Posture. 2007;26(3):428–35.) [16].
Table 1.
Criteria for ITW Classification. Adapted from Alvarez C, De Vera M, Beauchamp R, Ward V, Black A. (Classification of idiopathic toe walking based on gait analysis: Development and application of the ITW severity classification. Gait Posture. 2007;26(3):428–35.) [16].
| Idiopathic Toe Walking: Primary Criteria and Definitions | |||
|---|---|---|---|
| First ankle rocker | Early third rocker | Predominance of the first wave of ankle plantar flexor moment | |
| Type 1 | Yes | No | No |
| Type 2 | Yes/No | Yes/No | No |
| Type 3 | No | Yes | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



