
Submitted:
05 December 2023
Posted:
06 December 2023
You are already at the latest version
Abstract
Burden of diseases measured as disability-adjusted life years per 100,000 people can be mined from public domain data, when they are made available by population health surveillance systems. This can be analysed to allow insightful comparisons with the national average, and to understand differences in trends between the sexes, age groups, time periods, geographic regions and sub-regions. In this illustrative case study, we have analysed the Scottish burden of disease database to understand what ailed the population of the Grampian region before the COVID-19 pandemic. We have identified selected cancers, ischaemic heart disease, Alzheimer’s disease and other dementias amongst the highest contributors to the burden; that drug use disorders and colorectal cancer are showing worsening trends and require health promotion and disease prevention measures from ages 15 and 25 respectively, especially in Aberdeen City; and that males are more vulnerable to atrial fibrillation and flutter, diabetes mellitus and oesophageal cancer, while females are to cerebrovascular disease. We demonstrate the usefulness of our analysis and methodology for the wider health system, allowing targeted medical research investments and coordinated response from public health and health service delivery. We also show the need for up-to-date surveillance data, forecasts and evidence on the impact of interventions to be made available widely.
Keywords:
burden of disease
; disability-adjusted life year (DALY)
; disease prevention
; epidemiology
; health policy
; health service
; health surveillance
; medical research
; public health
1. Introduction
The origin of quality of life and cost-effectiveness analyses can be traced back to a study on chronic renal disease published in 1968 [1], leading to quality-adjusted life years or QALYs being formally defined in 1976 as the output of a utility function ([2], c.f. Acknowledgements). This concept gained gradual acceptance over the next three decades for the economic evaluation of healthcare programmes [3], using metrics such as the incremental cost-effectiveness ratio developed at York [4], and the disability-adjusted life year (DALY) introduced in 1994 as a related term with age-weighting and discounting [3,5].
Disability-adjusted life year (DALY), the loss of equivalent of one year of full health, is a time-based measure which allows the burden of different diseases to be compared objectively [6]. DALY is a combination of years of life lost due to mortality (YLL), and years of healthy life lost due to disability or living in less than full health (YLD). DALY and DALY rate per 100,000 people in a given region can provide valuable insights to health service providers, public health departments, health economists and policy makers if data is available to compare that region (for example, Grampian in Scotland) with others and the national average – as shown in this communication. Authentic and curated sources of such data in the United Kingdom include the Fingertips for England [7], the Scottish Burden of Disease [8], etc.
2. Methods
For this work, we have used the Scottish burden of disease [8, c.f. eight references therein], a population health surveillance system which monitors how diseases, injuries and risk factors prevent the Scottish population from living longer lives in better health. The underlying raw Scottish burden of disease data used by this communication is available as Supplementary Material S1.
3. Results and Discussions
Burden of disease expressed as DALY rate per 100,000 population was calculated for Scotland versus Grampian for the latest year for which data is available (2019), separately for females (Table 1 and Table 2) and males (Table 3 and Table 4).
It is seen from Table 1 and Table 3 that by and large the top 25 diseases for Grampian are also important for Scotland, however their exact order may vary. Ischaemic heart disease, lung cancer, Alzheimer's disease and other dementias significantly affect both Grampian and Scotland (c.f. Figure 1), so it is important to focus on these national priorities.
We are able to identify those diseases where Grampian’s DALY rate exceeds the Scottish average as local priorities for the region. These include atrial fibrillation and flutter, diabetes and oesophageal cancer for males; breast cancer, cerebrovascular disease, and other cardiovascular and circulatory diseases for females; colorectal cancer and drug use disorders affecting both sexes with worsening trends since 2016 (c.f. Table 1 and Table 3). Table 2 and Table 4 identify the age groups for these diseases of concern where the burden is especially high. It is important to address these unmet needs through a combination of public health measures (e.g. health promotion, disease prevention) and interventions arising from life sciences, health and medical research and innovation.
The latter is very important as demonstrated by recent reviews of Australia’s hugely important Medical Research Future Fund [9,10], in which it was found that 231 grants were awarded during 2016-19 with a total value of AU$ 574.5 million [10], but when mapped against 17 disease groups in the Australian burden of disease study 2015 [11], only a weak association was observed with DALY (r2 = 0.4359) and no association was observed with disability burden YLD (r2 = 0.0009) [10]. Any life sciences, health and medical research and innovation investments into Grampian by public, private or non-profit sectors should take these considerations into account. Realistic medicine approaches [12] and regional investments should target the local burden of diseases, lest there could be higher opportunity costs and unintentional widening of inequalities. For the Grampian region, disease priorities are summarized under the mnemonic “CICADAS” (Table 5), with the worst-affected age groups identified from Table 2 and Table 4.
As shown in Figure 1, the Grampian region is in turn comprised of three Health & Social Care Partnerships (viz. Aberdeen City, Aberdeenshire and Moray), so it will be instructive to see if there are any sub-regional variations that these partnerships should be made aware of. From Table 6, it is seen that Aberdeenshire is close to the Grampian average for diseases in females listed under Table 2 (except perhaps breast cancer); Aberdeen City has higher DALY rate than Grampian for Alzheimer’s disease and other dementias, lung and colorectal cancers and drug use disorders; while Aberdeenshire has higher DALY rate than Grampian for ischaemic heart disease, cerebrovascular disease and other cardiovascular and circulatory diseases.
From Table 7, it is seen that Aberdeenshire is again tracking the Grampian average for diseases in males listed under Table 4 (except perhaps colorectal cancer, atrial fibrillation and flutter); Moray has higher DALY rate than Grampian for lung cancer, atrial fibrillation and flutter; while Aberdeen has higher DALY rate than Grampian for all but atrial fibrillation and flutter. Thus we notice that while some trends are the same for both sexes, there are significant differences too, so we need a nuanced approach.
4. Conclusions, limitation and future work
With health services under increasing pressure across the world, it is important to ensure better alignment between the long-term plans for population health, integrated health and social care. In many developed countries, we have health surveillance data on the public domain. These, especially on burden of diseases, can be mined and analysed by health service providers to serve their populations more effectively and in a targeted manner, as shown in this communication with the Grampian region case study. For example, we were able to identify which diseases have the highest DALY rate burden, which ones are of particular concern to Grampian, and those that are showing a worsening trend. We were also able to gain a nuanced understanding in terms of differences between males and females, age groups, and the three sub-regions that make up Grampian. This will allow targeted medical research investments and coordinated response from public health and health service delivery. The public domain Scottish burden of disease data ends at 2019, and we acknowledge this limitation. However, this communication does provide a useful pre-pandemic baseline for future comparisons, and our methodology and case study will still be very useful across the UK and internationally. We also demonstrate the importance of up-to-date surveillance data being available to health service providers, as well as the need for predictive trends and evidence on the impact of interventions, and it is heartening to note that such forecasting could soon be made available “to offer insights into future public health challenges in Scotland” [8].
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Scottish burden of disease underlying dataset.
Author Contributions
Conceptualization, S.S.V. and N.F.; methodology, S.S.V.; software, S.S.V.; validation, S.S.V.; formal analysis, S.S.V.; investigation, S.S.V.; resources, N.F.; data curation, S.S.V.; writing—original draft preparation, S.S.V.; writing—review and editing, S.S.V. and N.F.; visualization, S.S.V.; supervision, N.F.; project administration, S.S.V.; funding acquisition, N.F. Both authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data supporting reported results can be downloaded from the Scottish burden of disease [8] or Supplementary Material.
Acknowledgments
S.S.V. is grateful for discussions with his past collaborator and co-author Professor Donald S. Shepard of Brandeis University (see for instance [13] and [14]) on QALYs versus DALYs. Donald preferred the term QALY to quality-adjusted citizen years as the latter acronym was felt to be quacky and fowl usage. The authors thank their colleague Professor Shantini Paranjothy for her comments.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Klarman, H.E.; Francis, J.O.S.; Rosenthal, G.D. Cost-effectiveness analysis applied to the treatment of chronic renal disease. Medical Care. 1968, 6, pp. 48–54. Available online: https://journals.lww.com/lww-medicalcare/citation/1968/01000/cost_effectiveness_analysis_applied_to_the.5.aspx (accessed on 20 November 2023).
- Zeckhauser, R.; Shepard, D.S. Where now for saving lives? Law and Contemporary Problems 1976, 40, 5–45. [Google Scholar] [CrossRef]
- Drummond, M.F.; Sculpher, M.J.; Torrance, G.W.; O’Brien, B.J.; Stoddart, G.L. Methods for the economic evaluation of health care programmes; Oxford University Press: Oxford, UK, 2005; Available online: https://academic.oup.com/book/54294 (accessed on 20 November 2023).
- York Health Economics Consortium. Incremental Cost-Effectiveness Ratio. Available online: https://yhec.co.uk/glossary/incremental-cost-effectiveness-ratio-icer/ (accessed on 20 November 2023).
- Murray, C. Quantifying the burden of disease: the technical basis for disability-adjusted life years. Bulletin of the World Health Organization 1994, 72, 429–445. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2486718/ (accessed on 20 November 2023).
- World Health Organization. Disability-adjusted life years (DALYs). Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/158 (accessed on 20 November 2023).
- Office for Health Improvement and Disparities. Fingertips (public health data). Available online: https://fingertips.phe.org.uk (accessed on 20 November 2023).
- Public Health Scotland. Scottish burden of disease. Available online: https://scotland.shinyapps.io/phs-local-trends-scottish-burden-diseases (accessed on 20 November 2023).
- Department of Health’s Management of Financial Assistance under the Medical Research Future Fund; Australian National Audit Office: Canberra, Australia, 2021; Available online: https://www.anao.gov.au/work/performance-audit/department-health-management-financial-assistance-under-the-medical-research-future-fund (accessed on 20 November 2023).
- Gilbert, S.E.; Buchbinder, R.; Harris, I.A.; Maher, C.G. A comparison of the distribution of Medical Research Future Fund grants with disease burden in Australia. The Medical Journal of Australia 2021, 214, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Australian Burden of Disease Study 2015: interactive data on disease burden. Australian Institute of Health and Welfare: Canberra, Australia, 2019; Available online: https://www.aihw.gov.au/reports/burden-of-disease/abds-2015-interactive-data-disease-burden/data (accessed on 20 November 2023).
- Realistic Medicine. Available online: https://realisticmedicine.scot (accessed on 20 November 2023).
- Lee, H.L.; Vasan, S.S.; Birgelen, L.; Murtola, T.M.; Gong, H.F.; Field, R.W.; Mavalankar, D.V.; Ahmad, N.W.; Hakim, L.S.; Murad, S.; Ng, C.W.; Lucy, L.C.S.; Suaya, J.A.; Shepard, D.S. Immediate cost of dengue to Malaysia and Thailand: an estimate. Dengue Bulletin 2010, 34, 65–76. Available online: https://iris.who.int/handle/10665/170972 (accessed on 20 November 2023).
- Murtola, T.M.; Vasan, S.S.; Puwar, T.I.; Govil, D.; Field, R.W.; Gong, H.F.; Bhavsar-Vyas, A.; Suaya, J.A.; Howard, M.; Shepard, D.S.; Kohli, V.K.; Prajapati, P.B.; Singh, A.; Mavalankar, D.V. Preliminary estimate of immediate cost of chikungunya and dengue to Gujarat, India. Dengue Bulletin 2010, 34, 32–38. Available online: https://iris.who.int/handle/10665/170981 (accessed on 20 November 2023).
Figure 1.
Grampian is a region in Scotland, and its constituent Health & Social Care Partnerships are shown in yellow (Aberdeen City), amber (Aberdeenshire) and red (Moray). Remixed image from Wikipedia released under the GNU Free Documentation License, highlighted for clarity.
Figure 1.
Grampian is a region in Scotland, and its constituent Health & Social Care Partnerships are shown in yellow (Aberdeen City), amber (Aberdeenshire) and red (Moray). Remixed image from Wikipedia released under the GNU Free Documentation License, highlighted for clarity.
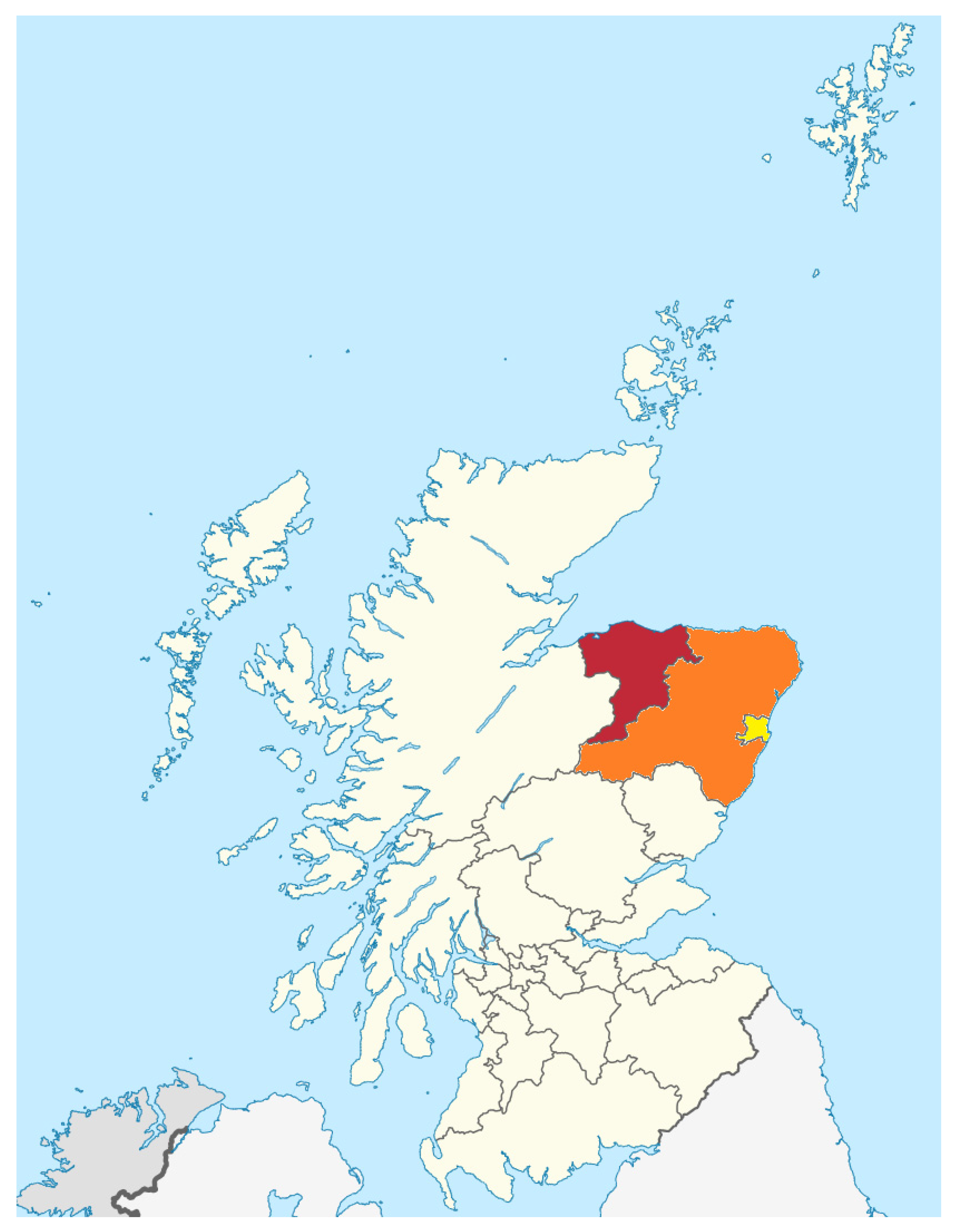

Table 1.
Disability-adjusted life year (DALY) rate per 100,000 people – females in Scotland versus Grampian (across time).
Table 1.
Disability-adjusted life year (DALY) rate per 100,000 people – females in Scotland versus Grampian (across time).
| Disease | Scotland | Grampian | Difference | CAGR 6 | |||
|---|---|---|---|---|---|---|---|
| Time period→ | 2019 | 2019 | 2018 | 2017 | 2016 | 2019 | 2016-19 |
| Alzheimer's disease1 | 1827 | 1693 | 1675 | 1655 | 1616 | -134 | 1.6% |
| Ischaemic heart disease | 1605 | 1489 | 1635 | 1639 | 1525 | -116 | -0.8% |
| Cerebrovascular disease | 1379 | 1414 | 1391 | 1521 | 1508 | 35 | -2.1% |
| Low back and neck pain | 1452 | 1390 | 1391 | 1391 | 1370 | -62 | 0.5% |
| Lung cancer | 1474 | 1366 | 1287 | 1110 | 1163 | -108 | 5.5% |
| Headache disorders | 1333 | 1337 | 1337 | 1337 | 1327 | 4 | 0.3% |
| COPD 2 | 1301 | 1087 | 952 | 1144 | 1060 | -214 | 0.8% |
| Breast cancer | 1027 | 1077 | 846 | 1092 | 1106 | 50 | -0.9% |
| Depression | 1215 | 1067 | 1068 | 1068 | 1044 | -148 | 0.7% |
| Anxiety disorders | 1045 | 918 | 919 | 919 | 898 | -127 | 0.7% |
| Other cancers | 1094 | 911 | 1169 | 1153 | 930 | -183 | -0.7% |
| Other cardiovascular3 | 763 | 850 | 679 | 865 | 837 | 87 | 0.5% |
| Colorectal cancer | 648 | 726 | 668 | 681 | 638 | 78 | 4.4% |
| Drug use disorders | 1003 | 677 | 522 | 683 | 553 | -326 | 7.0% |
| Lower respiratory infections | 622 | 528 | 691 | 800 | 612 | -94 | -4.8% |
| Diabetes mellitus | 586 | 487 | 551 | 600 | 555 | -99 | -4.3% |
| Other musculoskeletal disorders | 462 | 445 | 478 | 475 | 467 | -17 | -1.5% |
| Osteoarthritis | 457 | 441 | 442 | 442 | 438 | -16 | 0.3% |
| Cirrhosis 4 | 510 | 421 | 429 | 396 | 445 | -89 | -1.8% |
| Chronic kidney disease | 382 | 396 | 423 | 499 | 376 | 14 | 1.8% |
| Skin and subcutaneous diseases | 406 | 391 | 407 | 386 | 364 | -15 | 2.5% |
| Other digestive diseases | 440 | 368 | 344 | 378 | 387 | -72 | -1.7% |
| Gynecological diseases | 368 | 360 | 360 | 360 | 367 | -8 | -0.6% |
| Asthma | 330 | 335 | 317 | 393 | 351 | 5 | -1.5% |
| Self-harm 5 | 399 | 332 | 291 | 311 | 289 | -67 | 4.8% |
| Falls | 380 | 332 | 287 | 316 | 277 | -48 | 6.1% |
1 and other dementias; 2 Chronic obstructive pulmonary disease; 3 and circulatory diseases; 4 and other chronic liver diseases; 5 and interpersonal violence; 6 Compound annual growth rate in percentage. Bold font indicates areas of concern.
Table 2.
Disability-adjusted life year (DALY) rate per 100,000 people – females in Grampian 2019 (for selected diseases, age groups).
Table 2.
Disability-adjusted life year (DALY) rate per 100,000 people – females in Grampian 2019 (for selected diseases, age groups).
| Selected diseases of concern | Grampian 2019 | ||||||
|---|---|---|---|---|---|---|---|
| Age groups→ | All | <15 | 15-24 | 25-44 | 45-64 | 65-84 | 85+ |
| Alzheimer's disease 1 | 1693 | 0 | 0 | 2 | 72 | 4489 | 36399 |
| Ischaemic heart disease | 1489 | 1 | 1 | 81 | 1012 | 4929 | 14448 |
| Cerebrovascular disease | 1414 | 186 | 9 | 113 | 913 | 3878 | 18098 |
| Lung cancer | 1366 | 0 | 0 | 73 | 1765 | 4778 | 2660 |
| Breast cancer | 1077 | 0 | 18 | 743 | 1774 | 1926 | 3218 |
| Other cardiovascular 2 | 850 | 26 | 37 | 300 | 872 | 2250 | 5948 |
| Colorectal cancer | 726 | 5 | 7 | 383 | 530 | 2271 | 3851 |
| Drug use disorders | 677 | 0 | 430 | 1763 | 561 | 65 | 8 |
1 and other dementias; 2 and circulatory diseases. Bold font indicates areas of concern.
Table 3.
Disability-adjusted life year (DALY) rate per 100,000 people – males in Scotland versus Grampian (across time).
Table 3.
Disability-adjusted life year (DALY) rate per 100,000 people – males in Scotland versus Grampian (across time).
| Disease | Scotland | Grampian | Difference | CAGR 6 | |||
|---|---|---|---|---|---|---|---|
| Time period→ | 2019 | 2019 | 2018 | 2017 | 2016 | 2019 | 2016-19 |
| Ischaemic heart disease | 3713 | 3488 | 3422 | 3495 | 3311 | -225 | 1.7% |
| Lung cancer | 1749 | 1605 | 1738 | 1737 | 1842 | -144 | -4.5% |
| Alzheimer's disease1 | 1639 | 1592 | 1578 | 1536 | 1370 | -47 | 5.1% |
| Cerebrovascular disease | 1516 | 1291 | 1763 | 1720 | 1800 | -225 | -10.5% |
| Drug use disorders | 2367 | 1233 | 1308 | 1337 | 1007 | -1134 | 7.0% |
| COPD 2 | 1296 | 1208 | 1093 | 1385 | 1209 | -88 | 0.0% |
| Other cancers | 1295 | 1142 | 1108 | 1235 | 1259 | -153 | -3.2% |
| Depression | 1277 | 1090 | 1091 | 1092 | 1059 | -187 | 1.0% |
| Low back and neck pain | 1075 | 1040 | 1041 | 1041 | 1029 | -35 | 0.4% |
| Diabetes mellitus | 923 | 973 | 935 | 924 | 816 | 50 | 6.0% |
| Colorectal cancer | 878 | 960 | 1083 | 1012 | 808 | 82 | 5.9% |
| Self-harm 3 | 1194 | 934 | 972 | 895 | 930 | -260 | 0.2% |
| Other cardiovascular 4 | 1077 | 925 | 1146 | 1241 | 1219 | -152 | -8.8% |
| Lower respiratory infections | 801 | 774 | 737 | 884 | 671 | -27 | 4.9% |
| Prostate cancer | 821 | 758 | 761 | 830 | 773 | -63 | -0.7% |
| Headache disorders | 617 | 623 | 623 | 623 | 619 | 6 | 0.2% |
| Oesophageal cancer | 483 | 617 | 498 | 545 | 491 | 134 | 7.9% |
| Alcohol use disorders | 863 | 607 | 714 | 720 | 637 | -256 | -1.6% |
| Anxiety disorders | 646 | 552 | 553 | 553 | 536 | -94 | 1.0% |
| Cirrhosis 5 | 752 | 496 | 596 | 592 | 747 | -256 | -12.8% |
| Atrial fibrillation and flutter | 430 | 454 | 412 | 493 | 447 | 24 | 0.5% |
| Chronic kidney disease | 394 | 388 | 385 | 389 | 394 | -6 | -0.5% |
| Other musculoskeletal disorders | 385 | 387 | 379 | 356 | 374 | 2 | 1.1% |
| Other digestive diseases | 412 | 368 | 351 | 327 | 376 | -44 | -0.7% |
| Pancreatic cancer | 372 | 366 | 436 | 383 | 285 | -6 | 8.7% |
| Other chronic respiratory diseases | 395 | 360 | 428 | 353 | 323 | -35 | 3.7% |
| Falls | 466 | 366 | 424 | 353 | 455 | -100 | -7.0% |
1 and other dementias; 2 Chronic obstructive pulmonary disease; 3 and interpersonal violence; 4 and circulatory diseases; 5 and other chronic liver diseases 6 Compound annual growth rate in percentage. Bold font indicates areas of concern.
Table 4.
Disability-adjusted life year (DALY) rate per 100,000 people – males in Grampian 2019 (for selected diseases, age groups).
Table 4.
Disability-adjusted life year (DALY) rate per 100,000 people – males in Grampian 2019 (for selected diseases, age groups).
| Selected diseases of concern | Grampian 2019 | ||||||
|---|---|---|---|---|---|---|---|
| Age groups→ | All | <15 | 15-24 | 25-44 | 45-64 | 65-84 | 85+ |
| Ischaemic heart disease | 3488 | 1 | 3 | 391 | 3577 | 11196 | 21317 |
| Lung cancer | 1605 | 0 | 0 | 141 | 1574 | 5874 | 6083 |
| Alzheimer's disease 1 | 1592 | 0 | 0 | 1 | 204 | 4632 | 29994 |
| Drug use disorders | 1233 | 0 | 884 | 2671 | 1564 | 21 | 193 |
| Diabetes mellitus | 973 | 19 | 62 | 286 | 1266 | 2802 | 3015 |
| Colorectal cancer | 960 | 6 | 11 | 94 | 872 | 3327 | 5437 |
| Oesophageal cancer | 617 | 0 | 1 | 70 | 734 | 2235 | 954 |
| Atrial fibrillation and flutter | 454 | 0 | 3 | 20 | 229 | 1601 | 4630 |
1 and other dementias. Bold font indicates areas of concern.
Table 5.
Selected disease conditions of concern to Grampian and age groups worst affected.
| Acronym | Disease condition(s) of concern | Age groups worst affected |
|---|---|---|
| C | Cancer – Breast, Colorectal, Lung, Oesophageal (especially amongst males) | 25+ |
| I | Ischaemic heart disease; Other cardiovascular and circulatory diseases | 25+ |
| C | Cerebrovascular disease (especially amongst females) | 45+ |
| A | Alzheimer's disease and other dementias | 65+ |
| D | Drug use disorders | 15-64 |
| A | Atrial fibrillation and flutter (especially amongst males) | 45+ |
| S | Sugar (Diabetes mellitus, especially amongst males) | 25+ |
Table 6.
Disability-adjusted life year (DALY) rate per 100,000 people – females (2019, for selected diseases in Table 2, sub-regions).
Table 6.
Disability-adjusted life year (DALY) rate per 100,000 people – females (2019, for selected diseases in Table 2, sub-regions).
| Selected diseases of concern | Grampian | Aberdeen | Aberdeenshire | Moray |
|---|---|---|---|---|
| Alzheimer's disease 1 | 1693 | 1821 | 1660 | 1526 |
| Ischaemic heart disease | 1489 | 1460 | 1477 | 1597 |
| Cerebrovascular disease | 1414 | 1493 | 1252 | 1683 |
| Lung cancer | 1366 | 1603 | 1207 | 1334 |
| Breast cancer | 1077 | 1068 | 1113 | 1012 |
| Other cardiovascular 2 | 850 | 797 | 850 | 874 |
| Colorectal cancer | 726 | 960 | 674 | 438 |
| Drug use disorders | 677 | 830 | 638 | 449 |
1 and other dementias; 2 and circulatory diseases. Bold font indicates areas of concern.
Table 7.
Disability-adjusted life year (DALY) rate per 100,000 people – males (2019, for selected diseases in Table 4, sub-regions).
Table 7.
Disability-adjusted life year (DALY) rate per 100,000 people – males (2019, for selected diseases in Table 4, sub-regions).
| Selected diseases of concern | Grampian | Aberdeen | Aberdeenshire | Moray |
|---|---|---|---|---|
| Ischaemic heart disease | 3488 | 4166 | 3109 | 3231 |
| Lung cancer | 1605 | 1910 | 1287 | 1898 |
| Alzheimer's disease 1 | 1592 | 1732 | 1556 | 1440 |
| Drug use disorders | 1233 | 1665 | 949 | 1153 |
| Diabetes mellitus | 973 | 1153 | 869 | 930 |
| Colorectal cancer | 960 | 1103 | 980 | 682 |
| Oesophageal cancer | 617 | 823 | 538 | 449 |
| Atrial fibrillation and flutter | 454 | 399 | 478 | 503 |
1 and other dementias. Bold font indicates areas of concern.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



