
Submitted:
05 December 2023
Posted:
06 December 2023
You are already at the latest version
Abstract
This study evaluated the influence of methotrexate (MTX) and non-surgical periodontal treatment (NSPT) on the composition of the oral-gut microbiota in patients with rheumatoid arthritis (RA). Assessments were performed at baseline (T0), 6 months after MTX treatment (T1), and 45 days after NSPT (T2). The composition of the oral and gut microbiota was assessed by amplifying the V4 region of the 16S gene from subgingival plaques and stools. The results of the analysis of continuous variables were presented descriptively and non-parametric tests were adopted. Thirty-seven patients (27 with periodontitis) were evaluated at T0; 32 patients (24 with periodontitis) at T1; and 28 patients (17 with periodontitis) at T2. Nine individuals were lost to follow-up. MTX tended to reduce the alpha diversity of the oral-gut microbiota, while NSPT appeared to increase the number of different species of oral microbiota. MTX and NSPT influenced beta diversity in the oral microbiota. The relative abundance of oral microbiota was directly influenced by periodontal status. MTX did not affect the periodontal condition but modified the interactions between clinical parameters and the oral-gut microbiota. MTX and NSPT directly affected the composition and richness of the oral-gut microbiota. However, MTX did not influence periodontal clinical parameters.
Keywords:
gut microbiome
; methotrexate
; microbiota
; periodontitis
; rheumatoid arthritis
; mouth
1. Introduction
Rheumatoid arthritis (RA) is an autoimmune disease characterized by synovial inflammation and bone erosion, resulting in joint damage [1]. The etiology of the disease involves genetic and environmental factors, as well as immune system dysfunction [2]. Interactions between microorganisms and the immune system are also implicated in the progression of RA [3]. Individuals with RA have an increased incidence of periodontitis [4]. Periodontitis is a multifaceted and dynamic inflammatory condition influenced by multiple factors, among them microbial dysbiosis, host response, environmental influences, tissue remodeling, systemic connections, and patient-centered impacts, resulting in the disruption of the supportive structures surrounding the teeth [1,5]. Previous studies have proposed a two-way model where RA exacerbates periodontal destruction and the resulting inflammatory response worsens RA progression [6,7].
Recent literature has reported dysbiosis of oral [8,9,10,11] and gut [8,12,13] microbiota in individuals with RA. In turn, the increase in alpha diversity is more common in the oral cavity, while a decrease or stability of diversity is observed in the gut microbiota [13]. These findings support the theory that RA represents a chronic inflammatory state that can be triggered or exacerbated by the overgrowth of pathogenic bacteria which are often able to modulate the immune response [3,8,13].
Disturbances in the oral and gut microbiomes in RA have also been associated with a loss of tolerance against autoantigens and an increase in inflammatory events that promote joint damage [14]. Among the numerous bacterial pathogens potentially involved in RA, the Gram-negative bacterium Porphyromonas gingivalis plays an important role due to its ability to induce citrullination, which elicits or modifies the host immune response [15]. Other periodontal pathogens, including Aggregatibacter actinomycetemcomitans and Prevotella intermedia, play a role in the pathogenesis of RA by inducing hypercitrullinization [16,17], and can be identified both in subgingival plaque and in the serum of individuals with RA [18]. Within the context of the gut microbiota, Prevotella copri is also immune-relevant in RA pathogenesis [19].
The folic acid antagonist methotrexate (MTX) is currently the anchor drug for RA treatment—either as a single agent or in combination with other disease-modifying antirheumatic drugs (DMARD) [20]. Oral MTX can be partially metabolized by the gut microbiota; in turn, the microbiome may be useful to predict the response to MTX and may also be a potential target in the attempt to improve the response to this drug [21]. Studies in mice have revealed that MTX affects the abundance of some species in the gut and protects against the periodontal bone loss associated with arthritis and periodontal infection [22,23]. However, the combined effects of MTX and of short- and long-term non-surgical periodontal treatment (NSPT) on the oral-gut microbiota in individuals with RA, along with the association with clinical parameters, are unknown. The scarcity of literature highlights the need for more comprehensive studies investigating the simultaneous effects of MTX on the oral-gut microbiota in individuals with RA. Specific changes in microbial diversity, composition, and function in response to MTX treatment and how these changes may correlate with clinical outcomes and disease progression have been barely explored [8,13].
The purpose of the present longitudinal study was to investigate the effects of MTX and NSPT on the oral-gut microbiota composition of individuals with RA and their relationship with clinical and biochemical parameters in a Brazilian cohort. Our hypothesis was that MTX and NSPT have a direct impact on the diversity of the oral-gut microbiota.
2. Materials and Methods
2.1. Study design, setting, and ethical clearance
This was a prospective longitudinal study performed at the Rheumatology Outpatient Clinic of the Ribeirão Preto Medical School Hospital, São Paulo, Brazil, between August 2018 and December 2019. The guidelines for Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) were followed [24] and the study was approved by the Institutional Ethics Committee (#05934818.3.0000.5440). Patients gave written informed consent to participate in the study and their anonymity was preserved in accordance with the Declaration of Helsinki.
2.2. Participants and RA diagnostic criteria
Individuals aged ≥18 years and who had at least eight teeth, diagnosed with RA based on 2010 ACR/EULAR classification criteria [25], were included in the study. The patient should have experienced arthralgia for at least six weeks and clinically detected synovitis in at least one joint to be classified as having RA. The diagnosis is made when the patient achieves a total score of ≥6 (out of a possible 10) based on the number of painful and swollen joints, inflammatory markers (e.g., C-reactive protein [CRP] and erythrocyte sedimentation rate [ESR]), as well as the presence of autoantibodies (e.g., rheumatoid factor and anti-citrullinated protein antibodies [ACPA]) in the absence of an alternative diagnosis that would better explains the synovitis [25]. Individuals with symptom duration ≤24 months were classified as “early RA” and those with >24 months of symptoms were classified as “established RA” [26].
The exclusion criteria were: individuals diagnosed with another rheumatic disease (e.g., Sjögren’s syndrome, systemic lupus erythematosus, or primary osteoarthritis), individuals who received DMARD other than MTX as the initial treatment or who were already undergoing treatment with MTX or any other DMARD before the first assessment, and individuals with diabetes mellitus or malignant neoplasms. Individuals undergoing treatment for periodontal disease within the last 6 months, individuals wearing orthodontic appliances, those who took antibiotics within the last 3 months, and pregnant or lactating women were also excluded [27].
2.3. Data assessment and collection
The patients were evaluated at three time points. The first assessment (T0) was performed before starting MTX treatment and the second (T1) was performed six months after starting MTX treatment; at T1, after the second evaluation, the patients underwent NSPT. The third evaluation (T2) was performed 45 days after NSPT (Figure 1).
2.4. Clinical and laboratory RA assessment
The following data were collected from patients’ records: rheumatoid factor, ESR, CRP, ACPA, pain measured with a visual analogue scale (VAS), time of symptoms, and time of treatment. RA disease activity was determined by calculating the ESR-DAS 28 score (disease activity score 28) and was assessed at T0 and T1. At T1, the responsiveness of individuals to MTX treatment was also evaluated. Individuals who regularly used MTX orally for at least three months at a dose ≥15 mg/week and who exhibited a decrease in DAS 28 ≥1.2, and a final DAS 28 ≤3.2 were considered to be responsive to treatment. Individuals who did not meet these criteria were considered to be unresponsive [28].
2.5. Periodontal evaluation and treatment
Periodontal status was evaluated by two calibrated examiners (V.F.C. and T.A.S.), who used a periodontal probe (model PCP15, Hu-Friedy®; Chicago, IL, USA) at three time points (T0, T1, and T2). Weighted kappa agreement tests for periodontal clinical parameters revealed intra- and inter-examiner values ≥92%. The following parameters were recorded: plaque index, probing depth, clinical attachment loss (CAL), and bleeding on probing (BOP). Participants were classified according to the 2018 periodontitis classification [29] and assigned to two groups: individuals without periodontitis (periodontal health or gingivitis) and individuals with periodontitis (stages I, II, III, or IV). Participants were further classified as individuals without periodontitis or with mild, moderate, and severe periodontitis [30]. In T1, a single session of NSPT (full-mouth scaling and root planing) was performed with ultrasound and manual Gracey curettes in all individuals. Oral hygiene instructions were also provided.
2.6. Subgingival plaque and stool samples for microbiome analysis
Subgingival plaque samples were collected with sterile absorbent paper points (Dentsply Sirona; New York, PA, USA) inserted for 1 minute at five sites with the deepest probing depth. Next, all material was pooled, stored in a sterile tube containing 500 µL of sterile distilled water, and centrifuged at 3,000 g for 5 minutes. The paper points were discarded, and the pellet was kept at -80 °C until DNA extraction [9]. Fresh stool samples were collected from patients using an OMNI gene® GUT | OM-200 kit (DNA Genotek Inc.; Ottawa, ON, Canada) for gut microbiome profiling according to manufacturer’s instructions. Samples were stored at 8 °C until DNA extraction.
2.6.1. DNA extraction and 16S rRNA amplicon library preparation and sequencing
DNA was extracted from subgingival and stool samples using the DNeasy PowerSoil Pro kit (QIAGEN; Hilden, Germany). DNA concentration was evaluated spectrophotometrically using a NanoDrop™ spectrophotometer (Thermo Fisher; Waltham, MA, USA). The resulting purified DNA was stored at -20 °C until use.
For the subgingival samples, the V4 hypervariable region of the 16S rDNA gene was amplified using the 341F and 806R primer pair [31,32]. The primers were modified to obtain an overhang sequence complementary to the Nextera XT DNA Library Prep Kit (Illumina, San Diego, CA, USA) and were applied to a final volume of 25 μL containing 1X NEBNext® Q5 Hot Start HiFi PCR Master Mix (New England Biolabs; Ipswich, MA, USA), a 0.2 μM primer, and 12.5 ng of DNA. Cycling conditions were 95 °C for 3 minutes followed by 30 cycles of 95 °C (30 seconds), 55 °C (30 seconds) and 72 °C (30 seconds), and a final extension at 72 °C (5 minutes).
For the stool samples, the V4 region of the 16S rDNA gene was amplified with the region-specific 515F primers [33] and 806R [34] constructed with barcodes according to the method proposed by the Earth Microbiome Project (https://earthmicrobiome.org/protocols-and-standards/16s/). PCR was performed in a final 25 μL volume containing 1X PCR buffer, 0.2 mM dNTP, 2 mM MgSO4, 0.2 μM of primers, 1U Platinum™ Taq DNA Polymerase High Fidelity (Thermo Fisher; Waltham, MA, USA), and 20–30 ng of DNA. Cycling conditions were 94 °C for 3 minutes followed by 30 cycles at 94 °C (45 seconds), 57 °C (60 seconds), and 68 °C (45 seconds), and a final extension at 68 °C (10 minutes).
All libraries were purified using AMPure XP beads (Beckman Coulter; Brea, CA, USA) according to the Illumina 16S metagenomic sequencing library protocol (https://www.illumina.com/content/dam/illuminasupport/documents/documentation/chemistry_documentation/16s/16s-metagenomic-library-prep-guide-15044223-b.pdf). The size of the libraries was checked by the Bioanalyzer DNA 1000 Assay (Agilent; Santa Clara, CA, USA). Quantifications were performed with the KAPA Library Quantification Kit Illumina (Roche; Basel, Switzerland) and further DNA libraries were normalized and pooled. The libraries were paired end sequenced (2×300) in a single run on the Miseq platform (Illumina; San Diego, CA USA). All sequencing was performed on the Next Generation Sequencing platform of the René Rachou Institute (CPqRR/FIOCRUZ, Belo Horizonte, Brazil).
2.6.2. Read processing and taxonomic classification
The raw read files were processed in the R environment using the DADA2 package [35]. The forward and reverse sequences were trimmed to 180 and 130 bases, respectively. Readings containing more than two expected errors were removed. The errors of the filtered sequences were corrected by the algorithm and were joined to form the Amplicon Sequence Variants. The chimeric sequences were also removed and a sample count table was generated. Taxonomic classification was performed using the TAG.ME package and 515F-806R model [36].
2.6.3. Data analysis
The environmental beta diversity was measured using the principal coordinate analysis function of the “ade4 R” package [37] based on the Jensen-Shannon divergence calculated by the philentropy R package [38]. PERMANOVA was performed using 999 permutations to test the impact of categorical variables on beta diversity, and alpha diversity was measured by the Shannon and Simpson indices. The PERMANOVA test and alpha diversity calculations were performed using the vegan R package. Differential abundance between groups was tested with the DESeq2 R package [39] using the absolute read counts for each taxonomic entry in a Wald test. Differences supported by adjusted values of p < 0.01 were selected for discussion. Spearman’s correlation coefficient was used to measure the correlation between bacterial content and quantitative variables.
2.7. Statistical analysis
The Statistical Package for the Social Sciences (SPSS) (version 25.0, Armonk, USA) and the GraphPad Prism (version 7.00, La Jolla, CA, USA) were employed for the statistical analyses. Descriptive analysis was applied to clinicodemographic aspects and periodontal data. The Shapiro-Wilk test revealed that the data exhibited a non-normal distribution (p ≤ 0.001). The results of the analysis of continuous variables were presented as median, minimum, and maximum. Non-parametric tests (Wilcoxon test and chi-square test) were adopted for data analysis. For all analyses, the level of significance was set at <0.05.
3. Results
3.1. Clinicodemographic data
A total of 37 individuals diagnosed with RA were included in this study; of these, 22 were in the early stage of the disease and 15 in the established stage. Median age was 51 years, with most individuals being females (89.2%) who had never smoked (59.5%) or consumed alcohol (83.8%). Regarding RA disease activity, the median DAS 28 observed was 4.99 and many individuals had high disease activity. The median treatment time was three months. Among the individuals included, most had a diagnosis of periodontitis regardless of the classification used. The clinicodemographic characteristics of the included individuals are presented in Table 1.
3.2. NSPT modified periodontal parameters
At T0, 37 individuals were evaluated. After 6-month of treatment with MTX alone (T1), 32 individuals were reevaluated. There were no significant reductions in isolated periodontal parameters and no changes in periodontitis severity (p˃0.05), except for BOP, for which a significant increase was observed at T1 (p < 0.05). Regarding disease activity, a reduction in DAS 28 was observed after treatment with MTX (T1), albeit not significant (p˃0.05). At T1, 24 individuals with periodontitis and eight without periodontitis received NSPT. Forty-five days after NSPT (T2), 28 individuals were reevaluated; of these, 17 exhibited periodontitis and 11 did not. There was a significant reduction in periodontal parameters, such as probing depth, CAL, BOP, and plaque index, in addition to a significant reduction in the number of individuals with moderate-stage periodontitis (p < 0.05) (Table 2). Individuals who had missed the follow-up appointment (n = 5), who had undergone NSPT periodontal treatment at another service (n = 3), and those who had used a systemic antibiotic during the study (n = 1) were excluded.
3.3. MTX and NSPT affected subgingival microbial richness and diversity
Comparisons of subgingival microbial diversity were performed for individuals with RA at recruitment and at two follow-up times (T1 and T2). A trend towards decreased alpha diversity was observed after MTX treatment. In contrast, successful NSPT appeared to also influence alpha diversity, as shown by an increase in the number of different species of oral microbiota (Figure 2A). In comparisons related to beta diversity (i.e., alteration in the structure of the oral microbiota), MTX and NSPT seemed to have an influence on the bacterial composition of individuals. However, no clustering of microbiota samples was observed among the three different assessments (Figure 2B).
3.4. Periodontitis influenced the relative abundance of different genera in the oral microbiota
The composition of the oral microbiota differed significantly between groups of individuals according to their periodontal status. Among individuals with severe periodontitis, there was an increase in the relative abundance of the genera Anaeroglobus, Eubacterium.saphenum, Defluviitaleaceae.UCG.011, Eubacterium.yurii, Pseudoramibacter, unclassified.Bacteroidaceae, Selenomonas, Desulfobulbus, Eubacterium.nodatum, and Mycoplasma. Also, Dialister bacteria were increased in both moderate and severe periodontitis. Among individuals with moderate periodontitis, a genus of unclassified Archaea, Eikenella, and Staphylococcus showed increased relative abundance. In contrast, among individuals without periodontitis, only an increase in the unclassified Weeksellaceae was observed (Figure 3). Conversely, the severity of periodontitis did not significantly influence the gut microbiota (data not shown).
s3.5. MTX treatment and gut microbiome diversity
Similar to what was observed in the oral microbiota, MTX treatment decreased alpha diversity in the gut microbiota (Figure 4A). Regarding beta diversity, MTX treatment punctually altered the structure of the gut microbiota (Figure 4B). Individuals who did not respond to MTX treatment had a significantly higher relative abundance of Abiotrophia compared to those who responded to treatment (Supplementary Figure S1). No additional differential abundance within taxonomic groups of the gut microbiota was associated with MTX treatment.
3.6. Periodontal parameters and RA activity influenced the oral and gut microbiota
At the baseline evaluation of the participants, correlations of the oral and gut microbiome with the periodontal clinical parameters were observed (Figure 5). The plaque index was positively correlated with Prevotella.2 and Campylobacter, and negatively correlated with Alloprevotella. BOP was positively correlated with Fusobacterium and probing depth was positively correlated with Prevotella. On the other hand, the number of teeth was negatively correlated with Aggregatibacter and Prevotella.2. There was a positive correlation between DAS 28 and Campylobacter. Also, treatment time showed a negative correlation with Leptotrichia and Veillonella. A positive correlation between CRP and Leptotrichia was also observed.
Regarding the gut microbiome, there was a negative correlation between BOP and the unclassified Clostridiales, Ruminococcaceae.UCG.002, and Ruminococcaceae.UCG.005. Probing depth correlated positively with Bacteroides and negatively with Ruminococcaceae.UCG.005, Desulfovibrio, and the Ruminococcaceae.NK4A214.group.
CAL and bacteria of the genera Bacteroides and Agathobacter were also positively correlated. Positive correlations of rheumatoid factor and time of symptoms with the Lachnospiraceae.NK4A136.group were observed. Time of symptoms exhibited a positive correlation with the Ruminococcaceae.UCG.003 and with the Eubacterium.eligens.group. In contrast, a negative correlation was observed between time of treatment and Tyzzerella. Positive correlations of CRP with Butyricimonas, Eubacterium.eligens, and unclassified Lachnospiraceae were observed. All correlations observed were statistically significant (p < 0.05).
3.7. MTX treatment defined new associations of periodontal and RA parameters with oral and gut bacteria
Six months after MTX treatment, a change in correlations between clinical parameters and oral and gut bacteria was observed, with the emergence of new correlations (Figure 6). BOP was positively correlated with oral bacteria of the genus Streptococcus and Capnocytophaga. Plaque index was also positively correlated with Streptococcus and negatively correlated with Porphyromonas and Fusobacterium. Number of teeth was negatively correlated with Capnocytophaga.
Regarding the gut microbiome, the number of teeth showed a negative correlation with the bacteria of the genus unclassified Lachnospiraceae, Faecalibacterium, Sutterella, Odoribacter, Oscillibacter, Ruminococcaceae.UCG.002, unclassified Ruminococcaceae, Ruminococcus.torques.group, Eubacterium.coprostanoligenes.group, Butyricicoccus, Lachnoclostridium, Ruminiclostridium.9, Lachnospiraceae.NK4A136.group, and Subdoligranulum. In contrast, a positive correlation was observed between the number of teeth and Prevotella.9. A negative correlation between BOP and Ruminococcaceae.UCG.003 was also observed. DAS 28 showed a negative correlation with Tyzzerella, Coprococcus.3, Ruminococcaceae.UCG.005, and Roseburia. Importantly, after treatment with MTX, new correlation tests were performed. A priori, negative correlations between the number of teeth and oral bacteria were observed. No correlation between number of teeth and gut bacteria was observed. After the MTX regimen, numerous new negative correlations were observed between number of teeth and gut bacteria. Likewise, initially, DAS 28 only showed a positive correlation with an oral bacterium (Campylobacter). After treatment with MTX, numerous positive correlations were observed between DAS 28 and gut bacteria (e.g., Tyzzerella, Roseburia). All correlations observed after MTX treatment were statistically significant (p < 0.05).
4. Discussion
This study demonstrated that a 6-month MTX treatment reduced alpha diversity and modified the structure of the oral and gut microbiota in RA patients. NSPT influenced the diversity of the oral microbiota. Moreover, NSPT improved periodontal parameters individually, whereas MTX treatment had no impact on the periodontium. Finally, MTX modified the relationship between periodontal and RA clinical factors.
Without early and efficient treatment, RA can result in progressive disability and extra-articular symptoms, leading to increased morbidity and mortality [2]. MTX targets the inflammation pathways responsible for joint swelling and damage [20]. However, a significant non-response rate of 30 to 40%, as well as the impossibility of predicting the patient’s response to treatment, are evident impasses [40]. Recent literature has indicated multiple factors involved with MTX responsiveness, including the participation of the gut microbiota in drug metabolism and efficiency [41,42]. Understanding how the microbiota affects the response to MTX and, in turn, what impact this drug has on the microbiota is important not only because the modulation of the gut microbiota may offer a novel therapeutic or preventive approach for patients with RA, but also because it may be helpful in predicting the response to treatment. Herein, we observed that a decrease in the alpha diversity of both the oral and gut microbiota occurred after MTX treatment. Zhang et al. [8] reported that dysbiosis was detected in the gut and oral microbiomes of RA patients and was partially modified after RA treatment. Hence, these findings have not been uniform [10,15], perhaps due to the different study designs, sampling sites, or assays used. Another report also noted that the microbiota of RA patient was sensitive to MTX, to changes in gut bacterial taxa and to gene family abundance [43]. The fine line that separates this effect from dysbiosis may depend on the intrinsic ability to metabolize the drug or on factors such as the pharmacological combination, the dose administered, or the length of time the drug is prescribed [41].
At baseline, numerous positive and negative correlations were observed between oral and gut bacteria, as well as correlations with clinical parameters of both periodontitis and RA. It is interesting to note the positive correlation between the clinical parameters, namely plaque index and DAS 28, and the pathobiont oral bacterium Campylobacter, which has been previously reported to be abundant in individuals with RA and periodontitis [44]. In the present study, a negative correlation was observed between the oral pathogenic bacteria Leptotrichia and treatment time, as well as a positive correlation with CRP. In the context of systemic lupus erythematosus, we demonstrated positive correlations between Leptotrichia and levels of pro-inflammatory interleukins [45]. Sher et al. [46] demonstrated that Leptotrichia species were predominant in individuals with recent-onset RA, thus indicating a consistent role of this oral bacterium in the onset of RA [14]. Several other correlations have also been demonstrated between gut bacteria and periodontal parameters elsewhere. For example, gut bacteria of the genus Bacteroides, which have only been observed abundantly in individuals with RA and which may be associated with disease progression [47], were positively correlated with clinical parameters, probing depth, and CAL. Conversely, a negative correlation was noted between Bacteroides and the oral bacterium Capnocytophaga, which a priori was associated with lower probing depth in individuals with RA [10].
In the present study, after treatment with MTX, changes occurred in the correlation network, mainly in gut bacteria, which exhibited numerous new positive correlations with DAS 28 and negative correlations with the number of teeth. It is important to note that correlations between pathogenic bacteria such as Tannerella and Treponema have not been previously observed after MTX treatment. On the contrary, new correlations with the health-related bacteria Streptococcus, Capnocytophaga, and Tyzzerella emerged after MTX treatment. This scenario of new correlations reinforces the evidence that changes in microbiota diversity and disease parameters may occur after MTX treatment. In fact, the mechanism of response to MTX in patients with RA is likely to be associated with the catabolic capacity of the drug in the gut microbiota [42]. Although no microbiological signature regarding response to MTX was observed in our study, individual biological variations, disease parameters, and genetic susceptibility may probably explain the responsiveness to MTX treatment.
Relevant data refer to the impact of MTX treatment on periodontal parameters [22]. Contrary to the results observed in an animal model of arthritis in which MTX treatment protected against alveolar bone loss [23], in the present study there was no apparent effect of MTX on the periodontium. Other clinical studies have shown similar results, i.e., stability of periodontal parameters in individuals with moderate to severe periodontitis after 16 months of antirheumatic treatment [48]. In contrast, an improvement in periodontal inflammation parameters following treatment with conventional DMARD has been reported elsewhere [49,50]. Evidence indicates that DMARD, including MTX, are able to improve the periodontal condition of individuals with RA and periodontitis; hence, to observe such an effect on a short-term basis is unfeasible [51,52]. The short follow-up period, limited sample size, and initial 6-month period without combined professional oral prophylaxis as part of our study design certainly explain the maintenance of individual periodontal parameters before and after MTX treatment. Thus, studies with more robust samples and longer follow-up time are necessary to confirm the data.
NSPT resulted in the improvement of periodontal parameters and also influenced the diversity of our patients’ oral microbiota. Another report has also observed the effect of NSPT among individuals with RA [47]. Studies investigating the influence of NSPT on the subgingival microbiota of systemically healthy individuals with chronic periodontitis initially observed a decrease in alpha diversity after two and six weeks of NSPT, which was completely restored after 12 weeks [53]. In our study, a decrease, albeit non-significant, in microbial diversity was also demonstrated when compared to baseline. However, a change of this microbiota was noticed after NSPT when compared to the time after the antirheumatic treatment. These findings corroborate the notion that greater microbiota diversity is associated with increased ecosystem resilience and a healthier condition [54,55].
It was also observed that NSPT individually modified the structure of the oral microbiota; however, it was not possible to identify a pattern in these changes due to the non-formation of clusters. Changes in the composition of the microbiota after NSPT have also been reported in the literature. This reflects a significant decrease in the relative abundance of periodontopathogenic bacteria such as Porphyromonas and Treponema species, and an increase in health-associated bacteria, such as Streptococcus and Rothia species, shortly after NSPT, but these changes were gradually reversed within 12 weeks after treatment [53]. Other studies that analyzed the salivary microbiota after NSPT in systemically healthy individuals with aggressive periodontitis documented a trend towards reduced diversity measured by the Shannon index after three and six months of NSPT compared to baseline [56]. It has also been suggested that other adjunctive periodontal therapies such as antimicrobial photodynamic treatment may lead to a reduction in periodontopathogenic bacteria in individuals with RA [57]. Nonetheless, it is important to highlight the individuality of each patient’s oral microbiota and that there is probably no single composition that represents a healthy periodontal state. Additionally, recovery from periodontal disease appears to reflect a shift from a personalized disease state to a personalized healthy state. While there is consensus that specific communities must change with the response to disease, there may not be a “healthy amount” of these bacteria that is consistent across individuals [58].
The severity of periodontitis of the patients evaluated here was associated with a greater relative abundance of some pathogenic bacteria. In this line, changes in the subgingival microbial profile of individuals with RA directly associated with the severity of periodontitis were demonstrated [11]. Conversely, other authors have not demonstrated significant differences between the subgingival microbial profile of individuals with RA and the classification of periodontitis. Nevertheless, individual periodontal parameters such as deep periodontal pockets have been directly associated with a greater abundance of Gram-negative anaerobic pathogens such as Selenomonas [10], which was also observed more abundantly in our study. Likewise, bacteria of the genus Anaeroglobus have been associated with severe periodontitis. Bacteria of this genus have been correlated with an increase in the number of swollen and painful joints and with the levels of circulating rheumatoid factor and ACPA in individuals with RA [9,14,46]. These findings indicate a possible role of this oral bacterium, i.e., its increase in severe periodontitis, in the progression of RA [9,14,46]. We also showed that individuals with severe periodontitis had a higher abundance of the Desulfobulbus genus when compared to those without periodontitis. This aligns with former studies reporting that the Desulfobulbus genus was increased in individuals with RA and more severe periodontitis [11]. Other authors have also identified the severity of periodontitis as a determining factor in defining the diversity of the subgingival microbiota [46] and have identified pathogenic bacteria of the “red complex” associated with more severe periodontitis in individuals with RA [59]. These findings suggest that differences in relative abundance of the subgingival microbiota characterize more severe forms of periodontitis and do not represent a specific signature for the oral microbiota of RA [46].
The current study has shortcomings that should be acknowledged. The first concerns the absence of a control group of healthy individuals for comparison. The relatively small sample size and the limitations of periodontitis classifications in terms of their complex nature for implementation in clinical practice should also be highlighted. Several aspects such as lifestyle (e.g., physical activity and stress management), dietary patterns (e.g., cultural and regional differences), individual variability (e.g., genetic factors) can have a profound impact on shaping microbial communities in the oral-gut axis and cannot be ruled out [19]. Taken together, these factors underscore the need for cautious interpretation, particularly with regard to the generalizability of the results. Nonetheless, this study offers a valuable contribution to the understanding of the complex interplay among MTX treatment, periodontal health, and the oral-gut microbiota in individuals with RA. Of clinical relevance, the importance of evaluating changes at multiple time points to capture the dynamic nature of the microbiota under the influence of periodontal treatments supports the idea of performing NSPT at the beginning of RA treatment with MTX.
5. Conclusions
Based on the findings of the present study, MTX treatment reduced the diversity and richness of the oral and gut microbiota and also modified the correlations between the bacterial and clinical parameters of RA and periodontitis. Periodontal treatment resulted in changes in the oral microbiota and the severity of periodontitis influenced the relative abundance of oral bacteria. However, antirheumatic treatment had no effect on periodontal clinical parameters. Defining the mechanisms by which MTX alters the oral and gut microbiota may be useful for predicting and monitoring the response to treatment. Future studies on robust samples with a suitable experimental design are necessary to detect subtle effects and validate our data.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1. Relative abundance of gut microbiota after methotrexate treatment.
Author Contributions
TAS and FQC conceived the presented idea. PLJ, RDRO, and DCC proposed and verified the analytical methods. JAAA, JDC, VFC, JDM, AHS, LFD, GRF, and CCM performed the experiments. MTJ and SFA conducted the analyses. SRO took the lead in writing the manuscript and performed the experiments. LGA contributed to the interpretation of the results and statistical analysis. All authors provided critical feedback and helped shape the research and analysis and contributed to the final version of this manuscript.
Funding
Fundação de Amparo à Pesquisa do Estado de São Paulo (Centro de Pesquisa em Doenças Inflamatórias) (#2013/08216-2), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (Finance code 001), and Conselho Nacional de Desenvolvimento Científico e Tecnológico (#305077/2021-0), Brazil.
Data Availability Statement
Data are contained within the article or Supplementary Material.
Acknowledgments
We would like to thank Mrs. Lívia Ambrósio (HC-USP), Mrs. Katia Santos (FMRP-USP), Mrs. Anna Christina Salim (FIOCRUZ), and Mr. Emerson Santos (Multi-User Nucleic Acid Sequencing Laboratory- LMSeq) for technical laboratory support. Mrs. E. Greene provided English editing of the manuscript.
References
- Potempa J, Mydel P, Koziel J. The case for periodontitis in the pathogenesis of rheumatoid arthritis. Nat Rev Rheumatol. 2017;13(10):606-620. [CrossRef]
- Smolen JS, Aletaha D, Barton A, Burmester GR, Emery P, Firestein GS, Kavanaugh A, McInnes IB, Solomon DH, Strand V, Yamamoto K. Rheumatoid arthritis. Nat Rev Dis Primers. 2018;4:18001. [CrossRef]
- Maeda Y, Takeda K. Role of Gut microbiota in rheumatoid arthritis. J Clin Med. 2017;6(6):60. [CrossRef]
- Bolstad AI, Fevang BS, Lie SA. Increased risk of periodontitis in patients with rheumatoid arthritis: a nationwide register study in Norway. J Clin Periodontol. 2023;50(8):1022-1032. [CrossRef]
- Krutyhołowa A, Strzelec K, Dziedzic A, Bereta GP, Łazarz-Bartyzel K, Potempa J, Gawron K. Host and bacterial factors linking periodontitis and rheumatoid arthritis. Front Immunol. 2022;13:980805. [CrossRef]
- Farquharson D, Butcher JP, Culshaw S. Periodontitis, Porphyromonas, and the pathogenesis of rheumatoid arthritis. Mucosal Immunol. 2012;5(2):112-120. [CrossRef]
- Ebbers M, Lübcke PM, Volzke J, Kriebel K, Hieke C, Engelmann R, Lang H, Kreikemeyer B, Müller-Hilke B. Interplay between P. gingivalis, F. nucleatum and A. actinomycetemcomitans in murine alveolar bone loss, arthritis onset and progression. Sci Rep. 2018;8(1):15129. [CrossRef]
- Zhang X, Zhang D, Jia H, Feng Q, Wang D, Liang D, Wu X, Li J, Tang L, Li Y, Lan Z, Chen B, Li Y, Zhong H, Xie H, Jie Z, Chen W, Tang S, Xu X, Wang X, Cai X, Liu S, Xia Y, Li J, Qiao X, Al-Aama JY, Chen H, Wang L, Wu QJ, Zhang F, Zheng W, Li Y, Zhang M, Luo G, Xue W, Xiao L, Li J, Chen W, Xu X, Yin Y, Yang H, Wang J, Kristiansen K, Liu L, Li T, Huang Q, Li Y, Wang J. The oral and gut microbiomes are perturbed in rheumatoid arthritis and partly normalized after treatment. Nat Med. 2015;21(8):895-905. [CrossRef]
- Corrêa JD, Fernandes GR, Calderaro DC, Mendonça SMS, Silva JM, Albiero ML, Cunha FQ, Xiao E, Ferreira GA, Teixeira AL, Mukherjee C, Leys EJ, Silva TA, Graves DT. Oral microbial dysbiosis linked to worsened periodontal condition in rheumatoid arthritis patients. Sci Rep. 2019;9(1):8379. [CrossRef]
- Beyer K, Zaura E, Brandt BW, Buijs MJ, Brun JG, Crielaard W, Bolstad AI. Subgingival microbiome of rheumatoid arthritis patients in relation to their disease status and periodontal health. PLoS One. 2018;13(9):e0202278. [CrossRef]
- Eriksson K, Fei G, Lundmark A, Benchimol D, Lee L, Hu YOO, Kats A, Saevarsdottir S, Catrina AI, Klinge B, Andersson AF, Klareskog L, Lundberg K, Jansson L, Yucel-Lindberg T. Periodontal health and oral microbiota in patients with rheumatoid arthritis. J Clin Med. 2019;8(5):630. [CrossRef]
- Sun Y, Chen Q, Lin P, Xu R, He D, Ji W, Bian Y, Shen Y, Li Q, Liu C, Dong K, Tang YW, Pei Z, Yang L, Lu H, Guo X, Xiao L. Characteristics of gut microbiota in patients with rheumatoid arthritis in Shanghai, China. Front Cell Infect Microbiol. 2019;9:369. [CrossRef]
- Chu XJ, Cao NW, Zhou HY, Meng X, Guo B, Zhang HY, Li BZ. The oral and gut microbiome in rheumatoid arthritis patients: a systematic review. Rheumatology (Oxford). 2021;60(3):1054-1066. [CrossRef]
- du Teil Espina M, Gabarrini G, Harmsen HJM, Westra J, van Winkelhoff AJ, van Dijl JM. Talk to your gut: the oral-gut microbiome axis and its immunomodulatory role in the etiology of rheumatoid arthritis. FEMS Microbiol Rev. 2019;43(1):1-18. [CrossRef]
- Mikuls TR, Thiele GM, Deane KD, Payne JB, O’Dell JR, Yu F, Sayles H, Weisman MH, Gregersen PK, Buckner JH, Keating RM, Derber LA, Robinson WH, Holers VM, Norris JM. Porphyromonas gingivalis and disease-related autoantibodies in individuals at increased risk of rheumatoid arthritis. Arthritis Rheum. 2012;64(11):3522-3530. [CrossRef]
- Konig MF, Abusleme L, Reinholdt J, Palmer RJ, Teles RP, Sampson K, Rosen A, Nigrovic PA, Sokolove J, Giles JT, Moutsopoulos NM, Andrade F. Aggregatibacter actinomycetemcomitans-induced hypercitrullination links periodontal infection to autoimmunity in rheumatoid arthritis. Sci Transl Med. 2016;8(369):369ra176. [CrossRef]
- Schwenzer A, Quirke AM, Marzeda AM, Wong A, Montgomery AB, Sayles HR, Eick S, Gawron K, Chomyszyn-Gajewska M, Łazarz-Bartyzel K, Davis S, Potempa J, Kessler BM, Fischer R, Venables PJ, Payne JB, Mikuls TR, Midwood KS. Association of distinct fine specificities of anti-citrullinated peptide antibodies with elevated immune responses to Prevotella intermedia in a subgroup of patients with rheumatoid arthritis and periodontitis. Arthritis Rheumatol. 2017;69(12):2303-2313. [CrossRef]
- Martu MA, Solomon SM, Sufaru IG, Jelihovschi I, Martu S, Rezus E, Surdu AE, Onea RM, Grecu GP, Foia L. Study on the prevalence of periodontopathogenic bacteria in serum and subgingival bacterial plaque in patients with rheumatoid arthritis. Rev Chim 2017;68(8):1946-1950. [CrossRef]
- Möller B, Kollert F, Sculean A, Villiger PM. Infectious triggers in periodontitis and the gut in rheumatoid arthritis (RA): a complex story about association and causality. Front Immunol. 2020;11:1108. [CrossRef]
- Giollo A, Fuzzi E, Doria A. Methotrexate in early rheumatoid arthritis: is the anchor drug still holding? Autoimmun Rev. 2022;21(4):103031. [CrossRef]
- Bodkhe R, Balakrishnan B, Taneja V. The role of microbiome in rheumatoid arthritis treatment. Ther Adv Musculoskelet Dis. 2019;11:1759720X19844632. [CrossRef]
- Lübcke PM, Ebbers MNB, Volzke J, Bull J, Kneitz S, Engelmann R, Lang H, Kreikemeyer B, Müller-Hilke B. Periodontal treatment prevents arthritis in mice and methotrexate ameliorates periodontal bone loss. Sci Rep. 2019;9(1):8128. [CrossRef]
- de Arruda JAA, Corrêa JD, Singh Y, Oliveira SR, Machado CC, Schneider AH, Medeiros JD, Fernandes GR, Macari S, Barrioni BR, Santos MS, Duffles LF, Nakaya HTI, Fukada SY, Graves DT, Cunha FQ, Silva TA. Methotrexate promotes recovery of arthritis-induced alveolar bone loss and modifies the composition of the oral-gut microbiota. Anaerobe. 2022;75:102577. [CrossRef]
- Knottnerus A, Tugwell P. 2008. STROBE--a checklist to Strengthen the Reporting of Observational Studies in Epidemiology. J Clin Epidemiol 61(4):323. [CrossRef]
- Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO 3rd, Birnbaum NS, Burmester GR, Bykerk VP, Cohen MD, Combe B, Costenbader KH, Dougados M, Emery P, Ferraccioli G, Hazes JM, Hobbs K, Huizinga TW, Kavanaugh A, Kay J, Kvien TK, Laing T, Mease P, Ménard HA, Moreland LW, Naden RL, Pincus T, Smolen JS, Stanislawska-Biernat E, Symmons D, Tak PP, Upchurch KS, Vencovský J, Wolfe F, Hawker G. 2010. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum 62(9):2569-2581. [CrossRef]
- Mitchell KL, Pisetsky DS. Early rheumatoid arthritis. Curr Opin Rheumatol. 2007;19(3):278-283. [CrossRef]
- Oliveira SR, de Arruda JAA, Schneider AH, Carvalho VF, Machado CC, Corrêa JD, Moura MF, Duffles LF, de Souza FFL, Ferreira GA, Costa FO, Abreu LG, Taba Júnior M, Fukada SY, de Oliveira RDR, Louzada-Júnior P, Cunha FQ, Silva TA. Are neutrophil extracellular traps the link for the cross-talk between periodontitis and rheumatoid arthritis physiopathology? Rheumatology (Oxford). 2021;61(1):174-184. [CrossRef]
- Aletaha D, Smolen JS. Diagnosis and management of rheumatoid arthritis: a review. JAMA. 2018;320(13):1360-1372. [CrossRef]
- Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: framework and proposal of a new classification and case definition. J Clin Periodontol. 2018;45 Suppl 20:S149-S161. [CrossRef]
- Eke PI, Page RC, Wei L, Thornton-Evans G, Genco RJ. Update of the case definitions for population-based surveillance of periodontitis. J Periodontol. 2012;83(12):1449-1454. [CrossRef]
- Klindworth A, Pruesse E, Schweer T, Peplies J, Quast C, Horn M, Glöckner FO. Evaluation of general 16S ribosomal RNA gene PCR primers for classical and next-generation sequencing-based diversity studies. Nucleic Acids Res. 2013;41(1):e1. [CrossRef]
- de Paula ACL, Medeiros JD, Fernandes GR, da Silva VL, Diniz CG. Microbiome of industrialized Minas frescal cheese reveals high prevalence of putative bacteria: a concern in the one health context. LWT. 2021;139:110791. [CrossRef]
- Parada AE, Needham DM, Fuhrman JA. Every base matters: assessing small subunit rRNA primers for marine microbiomes with mock communities, time series and global field samples. Environ Microbiol. 2016;18(5):1403-1414. [CrossRef]
- Apprill A, McNally S, Parsons R, Weber L. Minor revision to V4 region SSU rRNA 806R gene primer greatly increases detection of SAR11 bacterioplankton. Aquat Microb Ecol. 2015;75:129-137. [CrossRef]
- Callahan BJ, McMurdie PJ, Rosen MJ, Han AW, Johnson AJ, Holmes SP. DADA2: high-resolution sample inference from illumina amplicon data. Nat Methods. 2016;13(7):581-583. [CrossRef]
- Pires DEV, Oliveira FS, Correa FB, Morais DK, Fernandes GB. TAG.ME: taxonomic assignment of genetic markers for ecology. bioRxiv. 2018;263293. [CrossRef]
- Dray S, Dufour AB. The ade4 package: implementing the duality diagram for ecologists. J Stat Soft. 2007;22(4):1-20. [CrossRef]
- Drost HG. 2018. Philentropy: information theory and distance quantification with R. Journal of Open Source Software. 2018;3(26):765. [CrossRef]
- Love MI, Huber W, Anders S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 2014;15(12):550. [CrossRef]
- Maciejewski M, Sands C, Nair N, Ling S, Verstappen S, Hyrich K, Barton A, Ziemek D, Lewis MR, Plant D. Prediction of response of methotrexate in patients with rheumatoid arthritis using serum lipidomics. Sci Rep. 2021;11(1):7266. [CrossRef]
- Zaragoza-García O, Castro-Alarcón N, Pérez-Rubio G, Guzmán-Guzmán IP. DMARDs-Gut microbiota feedback: implications in the response to therapy. Biomolecules. 2020;10(11):1479. [CrossRef]
- Han M, Zhang N, Mao Y, Huang B, Ren M, Peng Z, Bai Z, Chen L, Liu Y, Wang S, Huang S, Cheng Z. The potential of gut microbiota metabolic capability to detect drug response in rheumatoid arthritis patients. Front Microbiol. 2022;13:839015. [CrossRef]
- Nayak RR, Alexander M, Deshpande I, Stapleton-Gray K, Rimal B, Patterson AD, Ubeda C, Scher JU, Turnbaugh PJ. Methotrexate impacts conserved pathways in diverse human gut bacteria leading to decreased host immune activation. Cell Host Microbe. 2021;29(3):362-377.e11. [CrossRef]
- Kawamoto D, Borges R, Ribeiro RA, de Souza RF, Amado PPP, Saraiva L, Horliana ACRT, Faveri M, Mayer MPA. Oral dysbiosis in severe forms of periodontitis is associated with gut dysbiosis and correlated with salivary inflammatory mediators: a preliminary study. Front Oral Health. 2021;2:722495. [CrossRef]
- Corrêa JD, Calderaro DC, Ferreira GA, Mendonça SM, Fernandes GR, Xiao E, Teixeira AL, Leys EJ, Graves DT, Silva TA. Subgingival microbiota dysbiosis in systemic lupus erythematosus: association with periodontal status. Microbiome. 2017;5(1):34. [CrossRef]
- Scher JU, Ubeda C, Equinda M, Khanin R, Buischi Y, Viale A, Lipuma L, Attur M, Pillinger MH, Weissmann G, Littman DR, Pamer EG, Bretz WA, Abramson SB. Periodontal disease and the oral microbiota in new-onset rheumatoid arthritis. Arthritis Rheum. 2012;64(10):3083-3094. [CrossRef]
- Sun J, Zheng Y, Bian X, Ge H, Wang J, Zhang Z. Non-surgical periodontal treatment improves rheumatoid arthritis disease activity: a meta-analysis. Clin Oral Investig. 2021;25(8):4975-4985. [CrossRef]
- Äyräväinen L, Leirisalo-Repo M, Kuuliala A, Ahola K, Koivuniemi R, Meurman JH, Heikkinen AM. Periodontitis in early and chronic rheumatoid arthritis: a prospective follow-up study in Finnish population. BMJ Open. 2017;7(1):e011916. [CrossRef]
- Kordtabar S, Aghaie M, Fakhari E, Vakili MA. Periodontal condition in patients with rheumatoid arthritis: effect of anti-rheumatic Drugs. J Dent (Shiraz). 2019;20(3):190-194. [CrossRef]
- Jung GU, Han JY, Hwang KG, Park CJ, Stathopoulou PG, Fiorellini JP. Effects of conventional synthetic disease-modifying antirheumatic drugs on response to periodontal treatment in patients with rheumatoid arthritis. Biomed Res Int. 2018;2018:1465402. [CrossRef]
- Zhang J, Xu C, Gao L, Zhang D, Li C, Liu J. Influence of anti-rheumatic agents on the periodontal condition of patients with rheumatoid arthritis and periodontitis: a systematic review and meta-analysis. J Periodontal Res. 2021;56(6):1099-1115. [CrossRef]
- Balta MG, Papathanasiou E, Blix IJ, Van Dyke TE. Host modulation and treatment of periodontal disease. J Dent Res. 2021;100(8):798-809. [CrossRef]
- Belstrøm D, Grande MA, Sembler-Møller ML, Kirkby N, Cotton SL, Paster BJ, Holmstrup P. Influence of periodontal treatment on subgingival and salivary microbiotas. J Periodontol. 2018;89(5):531-539. [CrossRef]
- Liu G, Luan Q, Chen F, Chen Z, Zhang Q, Yu X. Shift in the subgingival microbiome following scaling and root planing in generalized aggressive periodontitis. J Clin Periodontol. 2018;45(4):440-452. [CrossRef]
- Schulz S, Porsch M, Grosse I, Hoffmann K, Schaller HG, Reichert S. Comparison of the oral microbiome of patients with generalized aggressive periodontitis and periodontitis-free subjects. Arch Oral Biol. 2019;99:169-176. [CrossRef]
- Greenwood D, Afacan B, Emingil G, Bostanci N, Belibasakis GN. Salivary microbiome shifts in response to periodontal treatment outcome. Proteomics Clin Appl. 2020;14(3):e2000011. [CrossRef]
- Martu MA, Luchian I, Mares M, Solomon S, Ciurcanu O, Danila V, Rezus E, Foia L. The effectiveness of laser applications and photodynamic therapy on relevant periodontal pathogens (Aggregatibacter actinomycetemcomitans) associated with immunomodulating anti-rheumatic drugs. Bioengineering (Basel). 2023;10(1):61. [CrossRef]
- Schwarzberg K, Le R, Bharti B, Lindsay S, Casaburi G, Salvatore F, Saber MH, Alonaizan F, Slots J, Gottlieb RA, Caporaso JG, Kelley ST. The personal human oral microbiome obscures the effects of treatment on periodontal disease. PLoS One. 2014;9(1):e86708. [CrossRef]
- Ziebolz D, Pabel SO, Lange K, Krohn-Grimberghe B, Hornecker E, Mausberg RF. Clinical periodontal and microbiologic parameters in patients with rheumatoid arthritis. J Periodontol. 2011;82(10):1424-1432. [CrossRef]
Figure 1.
Diagram representing data collection.
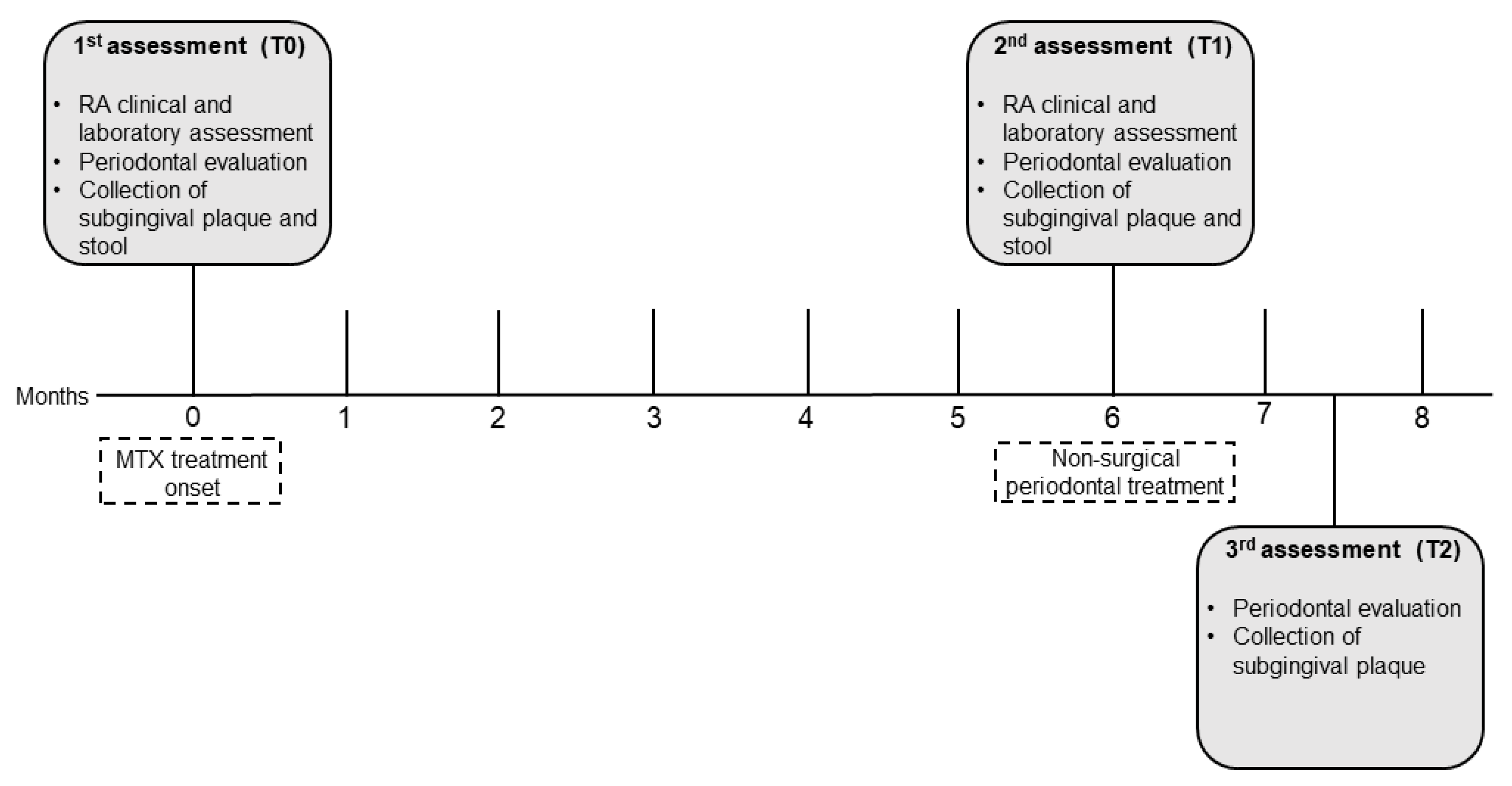
Figure 2.
Diversity of oral microbiota. (A) Shannon alpha diversity index. (B) Beta diversity index. The blue dashed lines connect the samples that showed increased diversity in relation to the immediately previous assessment (T1 ˃ T0; T2 ˃ T1) and the red dashed lines demonstrate the decrease in diversity in relation to the immediately previous assessment (T1 < T0; T2 < T1).
Figure 2.
Diversity of oral microbiota. (A) Shannon alpha diversity index. (B) Beta diversity index. The blue dashed lines connect the samples that showed increased diversity in relation to the immediately previous assessment (T1 ˃ T0; T2 ˃ T1) and the red dashed lines demonstrate the decrease in diversity in relation to the immediately previous assessment (T1 < T0; T2 < T1).
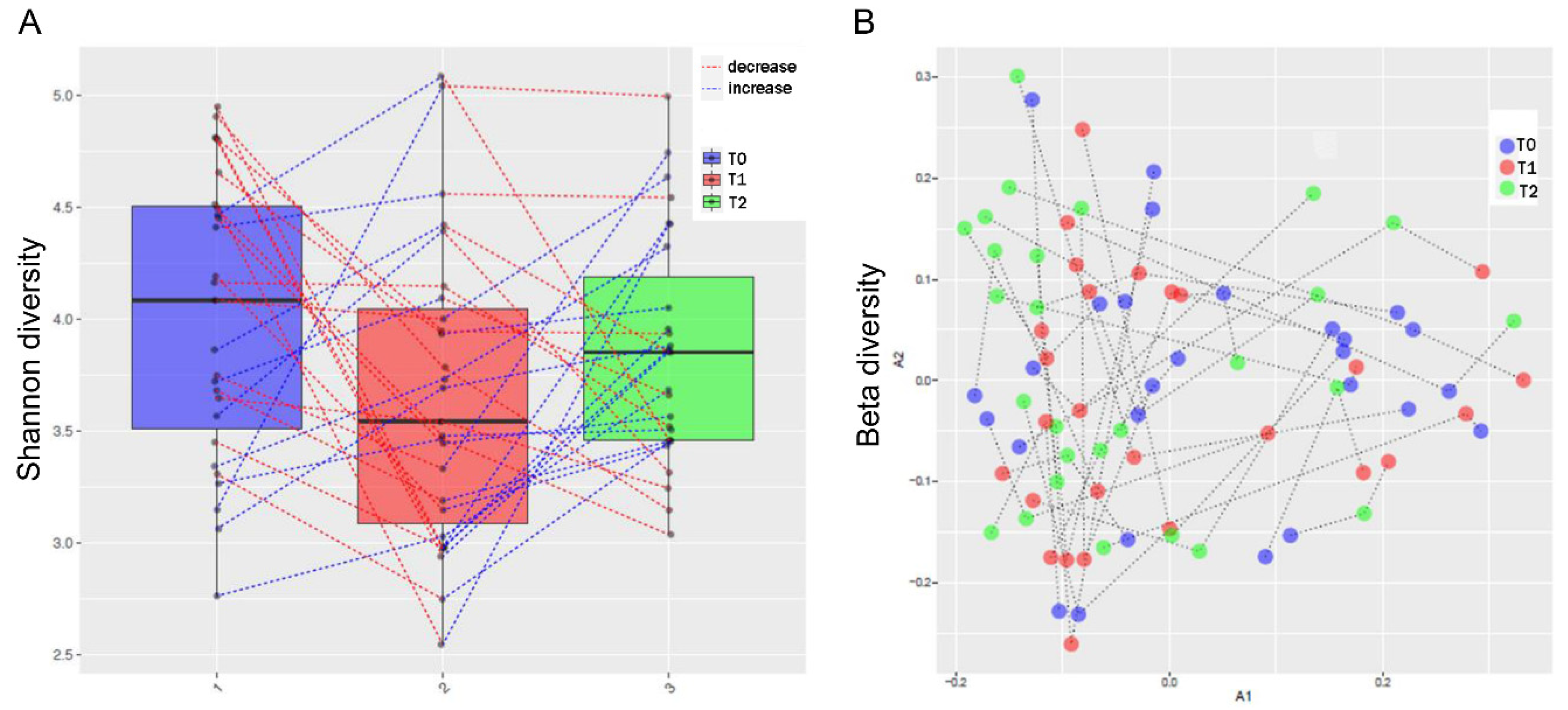
Figure 3.
Genus abundance that differed between periodontal status groups (DESeq2).
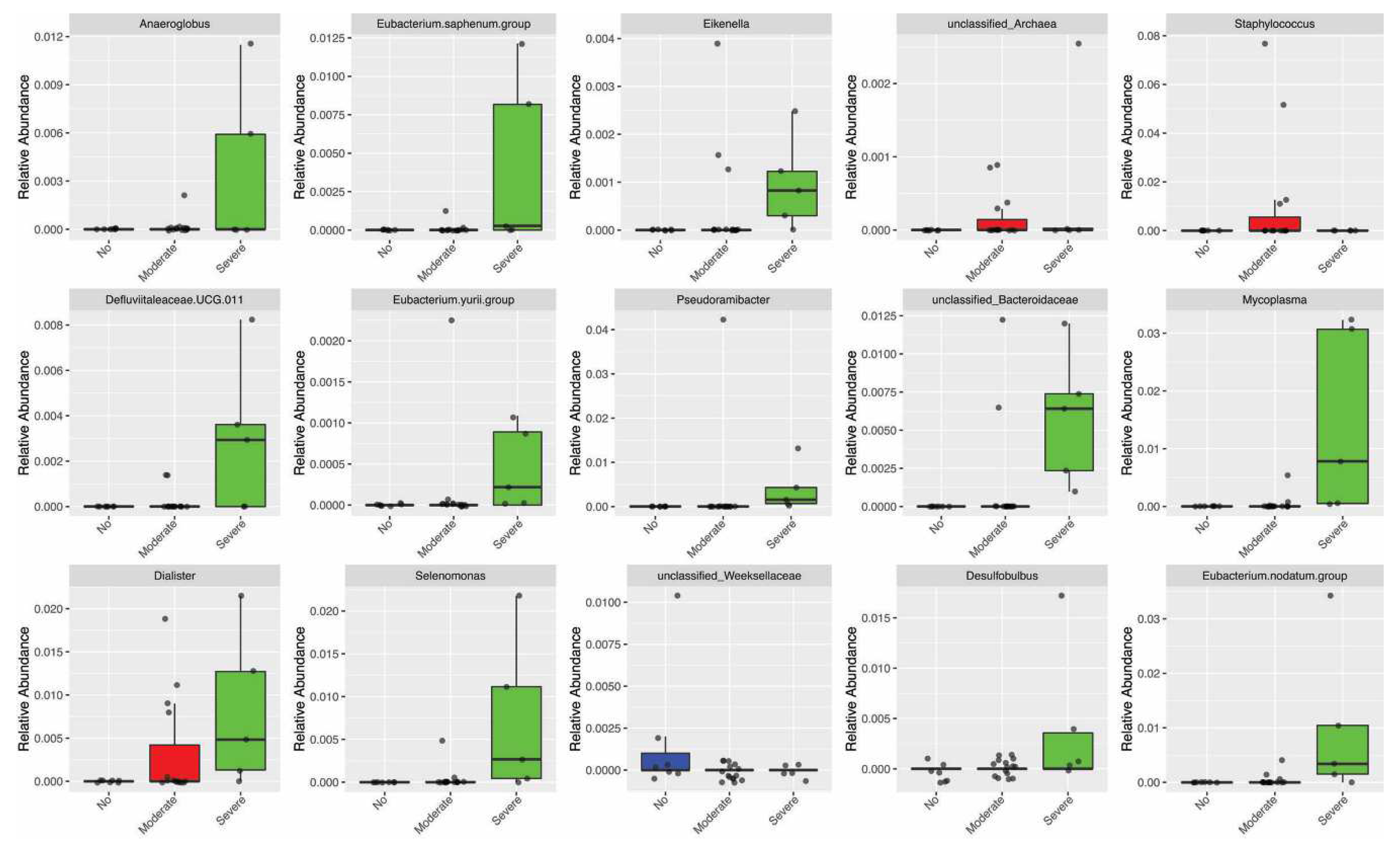
Figure 4.
Diversity of gut microbiota. (A) Shannon alpha diversity index. (B) Beta diversity index. The blue dashed lines connect the samples with increased diversity compared to the immediately previous assessment (T1 ˃ T0; T2 ˃ T1), and the red dashed lines demonstrate the decrease in diversity compared to the immediately previous assessment (T1 < T0; T2 < T1).
Figure 4.
Diversity of gut microbiota. (A) Shannon alpha diversity index. (B) Beta diversity index. The blue dashed lines connect the samples with increased diversity compared to the immediately previous assessment (T1 ˃ T0; T2 ˃ T1), and the red dashed lines demonstrate the decrease in diversity compared to the immediately previous assessment (T1 < T0; T2 < T1).
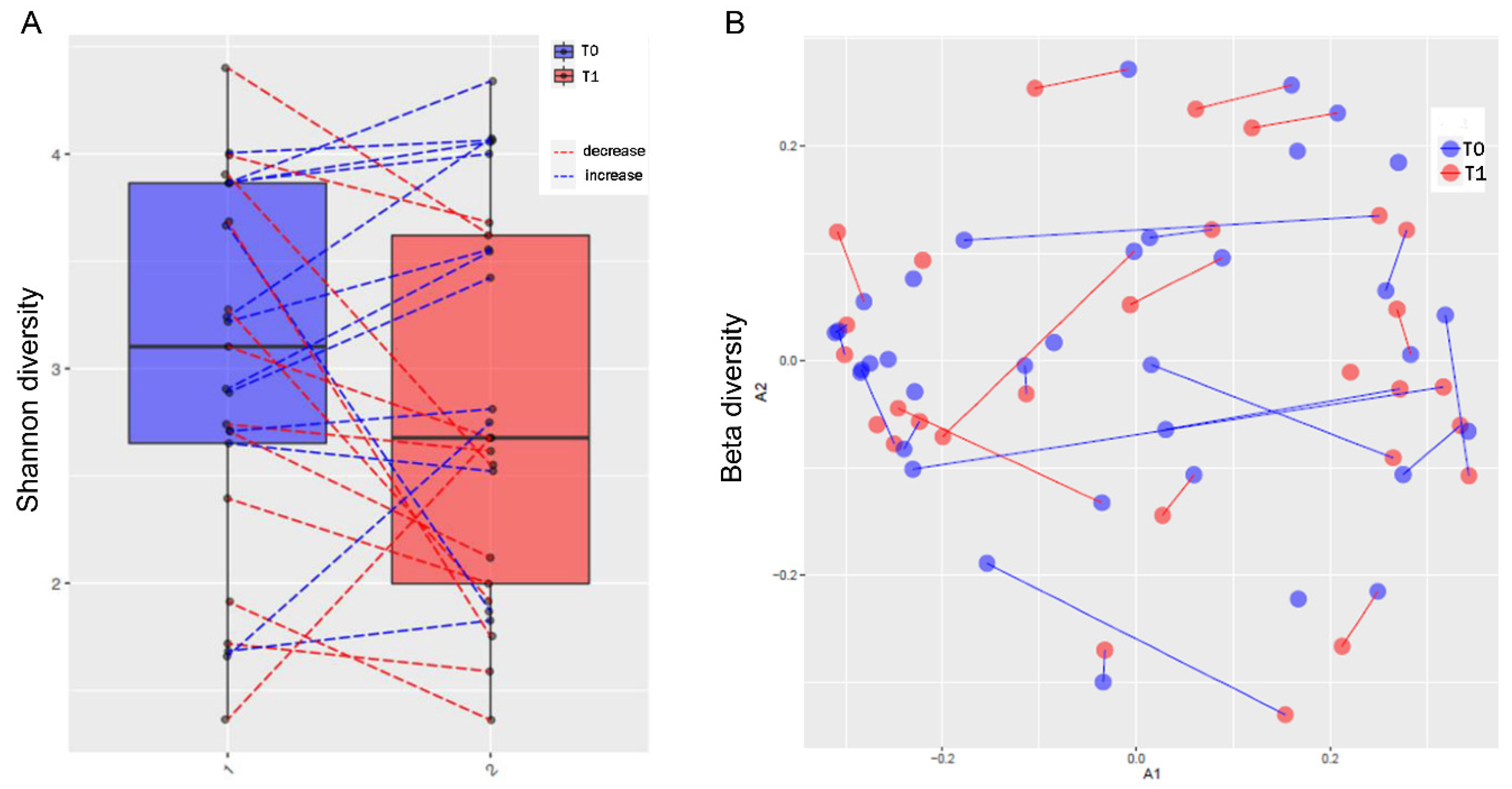
Figure 5.
Intercorrelations between oral and gut microbiota and clinical data before methotrexate (MTX) treatment. Spearman’s correlation coefficient was used to measure the correlation between bacterial content and quantitative variables. The blue lines represent positive correlations, and the red lines represent negative correlations. Yellow circles represent oral bacteria, green circles represent gut bacteria, and pink circles represent metadata.
Figure 5.
Intercorrelations between oral and gut microbiota and clinical data before methotrexate (MTX) treatment. Spearman’s correlation coefficient was used to measure the correlation between bacterial content and quantitative variables. The blue lines represent positive correlations, and the red lines represent negative correlations. Yellow circles represent oral bacteria, green circles represent gut bacteria, and pink circles represent metadata.
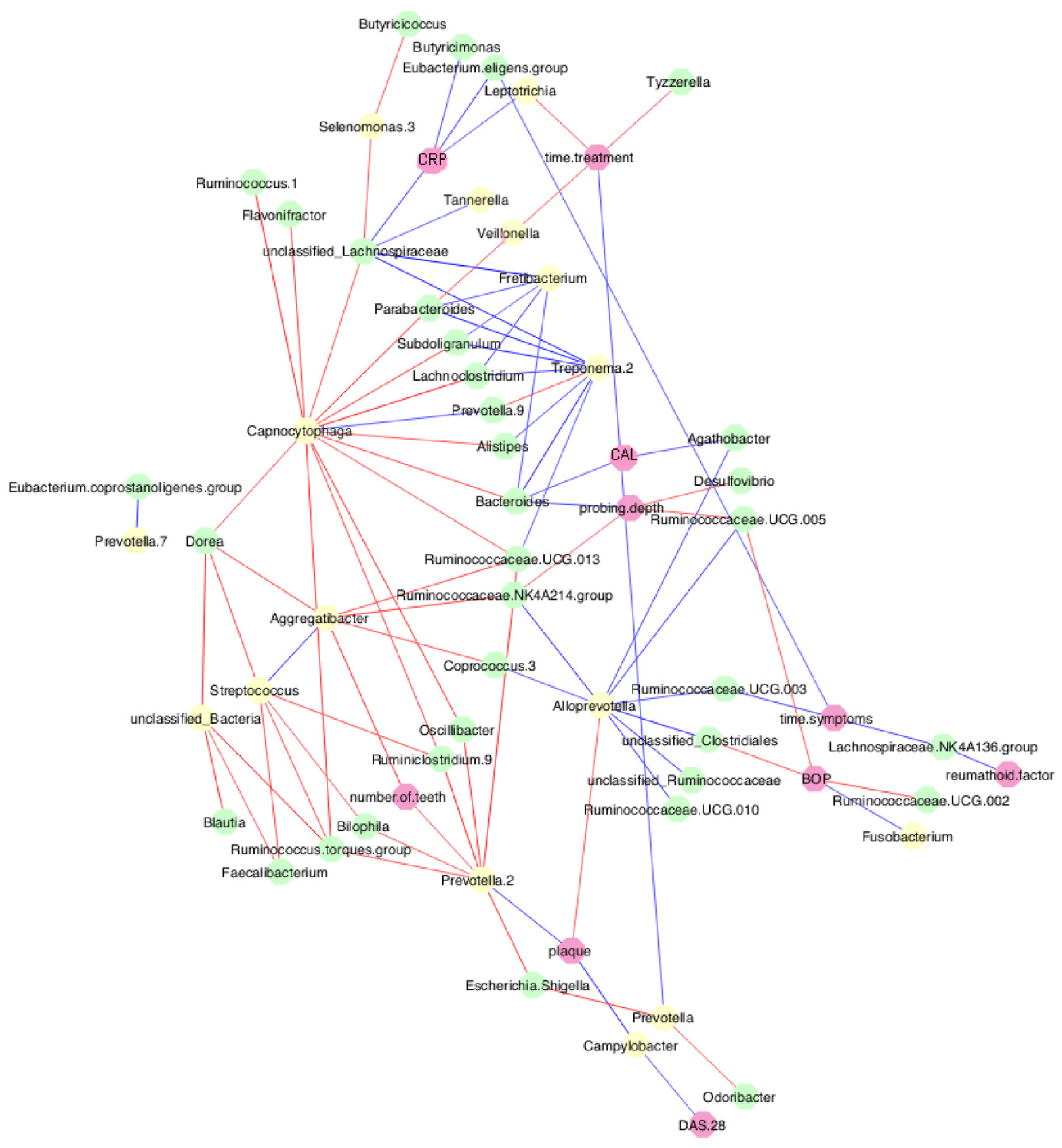
Figure 6.
Intercorrelations between oral and gut microbiota and clinical data after MTX treatment. Spearman’s correlation coefficient was used to measure the correlation between bacterial content and quantitative variables. The blue lines represent positive correlations and the red lines represent negative correlations. Yellow circles represent oral bacteria, green circles represent gut bacteria, and pink circles represent metadata.
Figure 6.
Intercorrelations between oral and gut microbiota and clinical data after MTX treatment. Spearman’s correlation coefficient was used to measure the correlation between bacterial content and quantitative variables. The blue lines represent positive correlations and the red lines represent negative correlations. Yellow circles represent oral bacteria, green circles represent gut bacteria, and pink circles represent metadata.
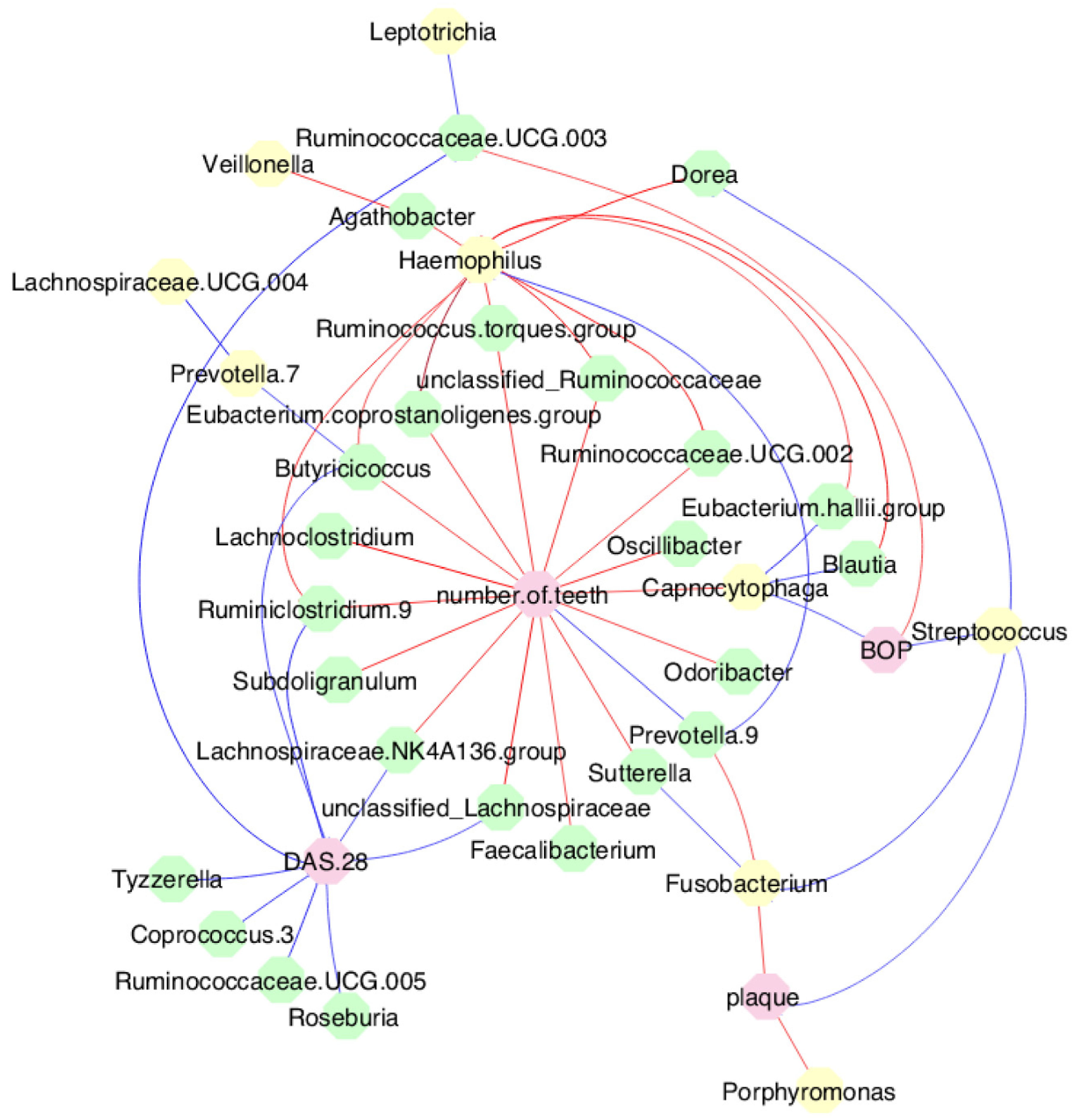

Table 1.
Clinicodemographic data of the individuals with rheumatoid arthritis (RA) included in the study (n = 37).
Table 1.
Clinicodemographic data of the individuals with rheumatoid arthritis (RA) included in the study (n = 37).
| Variables | n (%) |
|---|---|
| Age, median (min-max) | 51 (22–70) |
| Sex | |
| Female | 33 (89.2) |
| Male | 4 (10.8) |
| RA | |
| Early | 22 (59.5) |
| Established | 15 (40.5) |
| Tobacco smoking | |
| Never | 22 (59.5) |
| Still | 8 (21.6) |
| Stopped | 7 (18.9) |
| Alcohol consumption | |
| Never | 31 (83.8) |
| Still | 2 (5.4) |
| Stopped | 4 (10.8) |
| RF (IU/mL), median (min-max) | 15.00 (0–1890) |
| ACPA (IU/mL), median (min-max) | 69.75 (0–340) |
| CRP (mg/dL), median (min-max) | 0.77 (0–14) |
| VAS (mm), median (min-max) | 60 (0–100) |
| ESR (mm/h), median (min-max) | 18.00 (2–85) |
| DAS 28, median (min-max) | 4.99 (0.63–8.06) |
| Disease activity | |
| Remission | 7 (18.9) |
| Low | 6 (16.2) |
| Moderate | 11 (29.7) |
| High | 13 (35.1) |
| MTX treatment * (n, %) | |
| Failure | 16 (43.2) |
| Responsive | 17 (45.9) |
| Adverse events | 2 (5.4) |
| NA | 2 (5.4) |
| Time of treatment α, median (min-max) | 3 (0–408) |
| Periodontitis ¶ (n, %) | |
| No (periodontal health and gingivitis) | 10 (27.0) |
| Yes (stages I, II, III, IV) | 27 (73.0) |
| Periodontitis ∞ (n, %) | |
| None | 10 (27.0) |
| Mild | - |
| Moderate | 21 (56.8) |
| Severe | 6 (16.2) |
Note: ACPA, anti-citrullinated protein antibody; CRP, C-reactive protein; DAS 28, disease activity score 28; ESR, erythrocyte sedimentation rate; MTX, methotrexate; NA, not available; RF, rheumatoid factor; VAS, visual analogue scale for pain. * Response to MTX treatment assessed at T1. α Time of treatment in months. ¶ Adapted according to the 2018 classification for periodontitis (Tonetti, Greenwell and Kornman, J Clin Periodontol 2018;20:S149-161). ∞ Based on the study by Eke et al. (Eke et al., J Periodontol 2012;83:1449–54).
Table 2.
Periodontal parameters, disease activity and response to methotrexate treatment at T0, T1 and T2.
Table 2.
Periodontal parameters, disease activity and response to methotrexate treatment at T0, T1 and T2.
| Variables | T0, n = 37 | T1, n = 32 | T2, n = 28 | p value |
|---|---|---|---|---|
| Probing depth (mm), median (min-max) | 1.92 (0.86-3.16) | 1.70 (0.64-3.70) | 1.55 a,b (0.52-2.98) | <0.001 § |
| CAL (mm), median (min-max) | 2.05 (1.06-5.15) | 1.89 (0.83-7.14) | 1.83 a (0.78-6.92) | 0.026 § |
| BOP (%), median (min-max) | 9.00 (0-53) | 24.00 a (6-85) | 10.00 b (0-35) | <0.001 § |
| Plaque index (%), median (min-max) | 42.00 (0-100) | 37.50 (6-92) | 18.00 a,b (3-50) | <0.001 § |
| Periodontitis (n, %) | ||||
| None | 10 (27.0) | 8 (21.6) | 11 (29.7) | <0.05 ¶ |
| Mild | 0 (0.0) | 1 (2.7) | 0 (0.0) | |
| Moderate | 21 (56.8) | 17 (45.9) | 13 a,b (35.1) | |
| Severe | 6 (16.2) | 6 (16.2) | 4 (10.8) | |
| NA | - | 5 (13.6) | 9 (24.4) | |
| DAS 28, median (min-max) | 4.99 (0.63-8.06) | 4.49 (0.14-7.76) | - | 0.082 § |
Note: BOP, Bleeding on probing; CAL, Clinical attachment loss; DAS 28, disease activity score 28; NA, not available; T0: first assessment; T1: second assessment; T2: third assessment. a Difference compared to T0; b Difference compared to T1. § Wilcoxon test; ¶ Chi-square test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



