Submitted:
08 December 2023
Posted:
08 December 2023
You are already at the latest version
Abstract
Intestinal failure (IF) is characterized by a critical reduction of functional gut mass below the minimum needed for optimal growth in children. It requires parenteral nutrition (PN) and home-PN (HPN) which is challenging in terms of meeting nutritional needs according to age, growth velocity, clinical situation, and rapid changes in fluid and electrolyte requirements. Due to these complex requirements, age-adapted multi-chamber bags (MCBs) are important additions to the nutrition armamentarium. The launch of composite fish oil (FO)-containing intravenous lipid emulsions (ILEs) heralded the development of MCBs containing these ILEs in combination with a crystalline amino acids solution (CAAS) adapted for pediatric use. The safety and efficacy of lipid and amino acid components in this context have been widely documented in numerous published studies. This manuscript includes a review of the articles published in PubMed, Embase, and Google Scholar until June 2022, exploring studies in the age groups from term infants to children and adolescents. Preterm infants with their highly specific demands are not included. It aims to offer an overview of the clinical experience regarding the use of a composite FO-based ILE and a specific CAAS developed
Keywords:
intestinal failure
; parenteral nutrition
; home parenteral nutrition
; fish oil based intravenous lipid emulsion
; crystalline amino acids solution
; multi-chamber bags
1. Introduction
Adequate nutrient supply is of greater relevance during childhood than at any other period in life. Due to their high basal and anabolic requirements and limited metabolic reserves, pediatric patients are particularly sensitive to energy and protein restriction [1]. Sufficient nutrients must be provided not only for the maintenance of body tissue, but also for growth, while starvation, even for few days, may be detrimental [1,2,3].
Parenteral nutrition (PN) has become a valid therapeutic option for patients with intestinal failure (IF) who require long-term PN and home-PN (HPN) [1,4,5]. The provision of PN to pediatric patients represents a distinct clinical challenge, as metabolic demands and nutritional needs change according to age, growth velocity, and clinical situations [3]. Moreover, the complex and rapidly changing fluid and electrolyte requirement is a major challenge to PN delivery [6].
In children, IF is defined as a critical reduction of functional gut mass below the minimum needed for adequate growth [7,8]. The leading cause of IF in childhood is short bowel syndrome (SBS) as a consequence of extensive small bowel resection. Other conditions of IF are neuromuscular disorders (chronic intestinal pseudo-obstruction and long segment Hirschsprung disease) and mucosal intestinal diseases [8]. Intestinal failure may be reversible or irreversible, depending on the underlying cause.
Long-term PN and home PN (HPN) are the mainstay for the management of chronic IF, that allow children to grow in their familiar environment [9].
This article is based on the sourcing of PubMed (without time restriction), Embase (since 2016), and Google Scholar (since 2018), with the last search conducted in June 2022. This narrative review paper aims to give an overview of the specific quantitative and qualitative nutritional intake in pediatric patients including term newborn infants, infants/toddlers, children, and adolescents receiving PN. Preterm infants with their highly specific demands are not included, as this would be beyond the scope of the present article. Of note, this specific population provided important data not only for developing crystalline amino acids solutions (CAASs) specifically designed for preterms as well as for the demonstration of safety and efficiency of the composite intravenous lipid emulsion (ILE) containing fish oil (FO). Moreover, this article explores the clinical experience regarding the use of a composite ILE containing FO (SMOFlipid®, Fresenius Kabi Bad Homburg, Germany) and a pediatric CAAS (Vaminolact®, Fresenius Kabi Bad Homburg, Germany) in the management of pediatric patients with acute or chronic IF depending on PN.
2. Provision of Energy and Macronutrients in Pediatric Patients on PN
Energy
Generally, energy supply should meet the requirements to cover the resting energy expenditure (REE), plus those for physical activity, growth, diet induced thermogenesis and the correction of pre-existing malnutrition when present [3,10]. ESPGHAN/ESPEN/ESPR guidelines recommend calculating total parenteral energy requirements of stable patients from the REE that may be either measured by indirect calorimetry or estimated from Schofield’s formula, which are based on gender, age, body weight, and length [11]. Energy intake must cover energy expenditure for physical activity and growth (including catch-up growth) and must be adjusted according to age and disease states [3].
In clinical practice, PN intake must be adapted to the degree of intestinal insufficiency in pediatric patients. It may be estimated by the level of PN required for normal or catch-up growth. The PN dependency index (PNDI) has been defined as the ratio of non-protein-energy intake (NPEI) provided by PN for achieving optimal growth to REE calculated by using the Schofield formula, expressed as a percentage and validated from several papers [12,13,14,15]. In clinical practice, the PNDI corresponds to the caloric requirements from PN to achieve normal growth. It reflects the degree of intestinal insufficiency more accurately than other criteria, such as the ratio of parenteral versus enteral intakes or the addition of PN and enteral intake when compared to recommended dietary allowances (RDA). The PNDI for estimating the PN requirements for optimal growth makes sense by considering the final nutritional efficiency. Based on the PNDI expressed in percentage, it can be considered as high when >120% and even higher for achieving catch-up growth and low when <50% [12,13,14,15].
Excess energy intake may increase the risk of hyperglycemia, infections, and fat deposition (fat body mass and liver steatosis). Underfeeding may result in failure to thrive, poor development, impaired immune responses, increasing the risks of morbidity, and mortality in newborn infants, infants/toddlers, and children [3]. In acute critical illness, energy provision should be reduced compared to stable patients while overfeeding (glucose) increases ventilatory workload and potentially prolongs the need for mechanical ventilation and the length of hospital stay [3,16]. During the stable phase of critical illness, requirements are approximately 1.3 times the REE and further increase in the recovery phase for catch-up growth [3]. Therefore, energy provision must be carefully managed to ensure that energy needs are met but not exceeded.
Glucose
D-glucose (dextrose) is the main source of calories in PN, but also accounts for a major part of the osmolarity in PN solutions. All body cells and organs utilize glucose and for the brain, renal medulla and erythrocytes, glucose is an obligatory energy substrate [17].
Factors guiding glucose intake with PN include age, disease status, nutritional status, the concomitant provision of other macronutrients (lipids and amino acids). The rate of glucose delivery should not exceed the maximum rate of glucose oxidation. Studies have shown a maximal oxidation rate of about 12 mg/kg body weight (BW) per min (17.2 g/kg BW per day) in term infants after surgery or infants on long-term PN [17,18,19].
The higher the glucose delivery rate, the higher is hyperinsulinism favoring a costly lipid synthesis from glucose (lipogenesis) with subsequent lipid deposition in adipose tissue and liver. Moreover glucose overfeeding induces hyperglycemia and increased CO2 production and minute ventilation [17]. In critically ill children with insulin resistance and beta-cell dysfunction, risk of hyperglycemia is a particular concern [17,20] and represents an independent risk factor for morbidity and mortality [21,22].
Lipids
Quantitative requirements
Intravenous lipid emulsions are an integral component of pediatric PN [23]. ILEs are a low osmolarity and energy-dense source of calories. In addition, they serve as a source of essential fatty acids (EFAs) and facilitate the delivery of fat-soluble vitamins [24,25]. According to the ESPPGHAN/ESPEN/ESPR guidelines [23], lipid intake should provide 25–50% of the non-protein calories in pediatric patients on total PN. As for glucose, the maximal lipid oxidation rate has been established [26]. It decreases with age, from approximately 3 g/kg/day in young children to 1.7-2.5 g/kg/day in adults. According to ESPGHAN/ESPEN/ESPR guidelines [23], parenteral lipid intake in children should be limited to a maximum of 3 g/kg/day. (LoE 3e4, RG 0, conditional recommendation for, strong consensus).
Qualitative fatty acids requirements
Not only the quantity of lipids but also the fatty acid (FA) composition of the ILE used as part of PN is critical, as it may influence clinical outcomes in pediatric patients [27]. To prevent biochemical evidence of EFA deficiency, parenteral lipid intake should include 0.1 g/kg BW/day of the omega-6 polyunsaturated fatty acid (PUFA) linoleic acid (LA) in term infants and children [23]. The “historical” ILEs, subsequently referred to as “first generation”, were derived from pure soybean oil (SO) rich in LA. A potential disadvantage with pure SO ILEs is that high contents of omega-6 PUFAs, in particular of LA, have been attributed to pro-inflammatory and immunosuppressive properties. This led to the development of more advanced ILEs containing mixtures of SO with alternative oil sources such as medium-chain triglycerides (MCT) from coconut/palm kernel oil, olive oil (OO) and/or FO [25,28]. In particular, FO representing a source of omega-3 PUFAs with anti-inflammatory properties [29] has become an important component of the last generation of composite ILEs containing FO [28,30]. The long-chain omega-3 PUFAs docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) and the omega-6 PUFA arachidonic acid (ARA) modulate key metabolic pathways, including inflammatory and immune responses, coagulation, and cell signaling [28,31]. DHA and ARA are also required for an optimal development of brain as well as for cognition and visual acuity [32,33,34]. In order to prevent EFA deficiency in term infants to children, a lipid emulsion dosage providing a minimum LA intake of 0.1 g/kg/day can be given, which also provides an adequate intake of linolenic acid (LNA) with all 20% ILEs currently registered for pediatric use (LoE 3-4, RG 0, conditional recommendation for, strong consensus). In critically ill pediatric patients, ILE should also be an integral part of PN. Composite ILEs containing FO may be used as the first-choice treatment. Available evidence raises the important question on the best timing to provide PN support in critically ill children, but do not allow to differentiate potential effects on outcomes of the timing of introducing ILE (LoE 4, GPP, conditional recommendation for, strong consensus) [21].
The ESPGHAN/ESPEN/ESPR guidelines [23] support that in newborn infants and older children on short-term PN, pure SO ILEs may provide a less balanced FA profile than composite ILEs. For PN lasting longer than a few days, the use of pure SO-ILE is discouraged and composite ILEs with or without FO are recommended as first-line treatment [23.35]. Of note, to date there are no quantitative recommendations for the supply of EPA, DHA, or ARA in pediatric patients.
Intestinal failure associated liver disease (IFALD) is the most prevalent complication affecting children with IF receiving long-term PN [24,36,37]. The diagnosis of IFALD is usually based on the onset of cholestasis, generally defined as an elevation in conjugated serum bilirubin (CBil) concentration (≥2 mg/dL) [24,37]. Effects of pure FO based ILEs (Omegaven®, Fresenius Kabi Bad Homburg, Germany) for reversing cholestasis in children receiving a SO based ILE (Intralipid®, Fresenius Kabi Bad Homburg, Germany) have first been reported by Gura et al [38]. Ten years later, the same group reported data of patients treated with pure FO from 2004 to 2014. Most of the time, cholestasis appeared very early during the first year of life. Resolution of cholestasis was defined as sustained direct bilirubin (DBil) <2 mg/dL, and treatment failure as liver transplantation or death while DBil was >2 mg/dL. Among 182 patients treated with FO, 86% achieved resolution of cholestasis and 14% failed therapy. Factors significantly associated with therapy failure included lower birth weight, patients older than 20.4 weeks (9.9, 38.6 weeks) compared with 11.7 weeks (7.3, 21.4 weeks), and more advanced liver disease at therapy initiation compared to patients whose cholestasis resolved [39].
Provision of high amounts of the omega-6 PUFA LA with pure SO ILEs results in the endogenous formation of ARA, a precursor of lipid mediators with more pro-inflammatory properties [28,40]. Excessive intake of LA may thus promote an inflammatory state contributing to cholestasis and liver fibrosis [31,40]. Moreover, pure SO ILEs are relatively low in vitamin E (alpha-tocopherol) as antioxidant substrate and, thus, are prone to the formation of lipid peroxidation products, which may lead to macrophage activation and hepatocyte damage [24,41,42]. Finally, pure SO based ILEs also contain much higher concentrations of phytosterols compared with any of the other ILEs, especially composite ILEs containing FO. There is evidence that phytosterols may accumulate in the liver, thereby reducing bile secretion while promoting liver damage in children with IF [24,43]. Recent discovery of farnesoid X receptor (FXR) as possible target mediating altered bile secretion in SBS patients has opened new field of research for IFALD prevention [44,45].
In this regard, composite ILEs with FO offer several advantages, including high concentrations of the anti-inflammatory omega-3 PUFAs DHA and EPA and the antioxidant alpha-tocopherol (200 mg/L), reduced omega-6 PUFA content, and a reduced phytosterol load [23,24,40]. Moreover, some composite ILEs, containing FO, also provide rapidly oxidizable MCTs [46,47] while the diversity of oils ensures a balanced intake of FA and prevents EFA deficiency [36,37].
To reverse IFALD in pediatric patients, ESPGHAN recommends a discontinuation of SO ILE, a reduction of other ILE dosage and/or the use of composite ILE with FO, along with the treatment and management of other risk factors (LoE 2b, RG B, strong recommendation). The use of pure FO ILE is not recommended for general use in pediatric patients but may be used for short-term rescue treatment in patients with progression to severe IFALD, based on case reports (LoE 3e4, GPP, conditional recommendation for, strong consensus).
Amino acids and protein synthesis
Quantitative requirements
In any patient receiving PN, proteins have to be administered in the form of free amino acids (AAs). Pediatric CAASs are currently available. Their primary goal is to promote anabolism (protein synthesis and positive nitrogen balance) for cells and tissue building (e.g., muscle, skeleton) consistent with the normal growth and development typical of healthy peers [48]. Due to additional needs for growth, the protein requirements based on weight are higher in newborn infants, infants/toddlers, and children than in adults and the timely provision of adequate amounts of AAs with PN is particularly critical [1].
Generally, the total AA requirement is lower in parenterally fed newborn infants, infants/toddlers, and children than in enterally fed patients because the intestinal and hepatic “first-pass” metabolism is bypassed [49]. The ESPGHAN/ESPEN/ESPR guidelines [49] recommend a minimum AA intake of 1.0 g/kg/d for stable infants and children from 1 month to 3 years to avoid negative balance (LOE 1¡, moderate quality, RG B, strong recommendation, strong consensus). In stable children aged 3-12 years an AA intake of 1.0-2.0 g/kg per day may be considered. (LOE 4, RG GPP, conditional recommendation, strong consensus) [47]. The maximum AA intake should not exceed 3.0 g/kg BW/day in term newborn infants and 2.0 g/kg BW/day in stable children and adolescents [49]. Excessive AA intake has been shown to increase oxidation, in turn promoting high blood urea concentrations and metabolic acidosis [50]. In very low birth weight (VLBW) newborn infants, high AA and energy intakes from birth onwards result in a more anabolic state but may cause higher urea concentrations, reflecting a higher AA oxidation [51]. Of note, AA must always be co-administered with sufficient amounts of energy in the form of glucose and lipid to prevent wasting of AAs for endogenous glucose production. The optimal ratio of NPEI in kcal to 1 gr of nitrogen (N) decreases with age, from approximately 250:1 in infants below 1 year of age to 150:1 in adolescents [13].
Qualitative requirements
In the sixties at the early phase of PN development, newborn infants received protein hydrolysates as a source of nitrogen [52,53]. These protein hydrolysates were not only nutritionally unadapted but raised the risk of severe allergic reactions and were therefore abandoned. With the advent of technology for the production of pure L-AAs, a second generation of CAAS was developed, but much more adapted for adult than pediatric patients and especially for VLBW newborn infants. Extrapolation from data on oral nutrition was often unsatisfactory for the adequate formulation of such mixtures. Intestinal metabolism of specific AAs is highly variable and may also change with age [49]. For example, the parenteral requirements for the branched-chain amino acids (BCAAs) leucine, valine, and isoleucine are considerably lower compared to enteral requirements, as losses due to first-pass metabolism with enteral administration were shown to be substantial both in the newborn state [54] and in older children [55]. On the other hand, parenteral arginine requirements are higher than with enteral nutrition, as intestinal metabolism results in a net synthesis of arginine [56]. Moreover, parenteral requirements for tyrosine and cysteine are increased due to the lacking conversion of phenylalanine and methionine in the intestine that would occur after enteral intake [56]. Accordingly, the composition of CAASs for pediatric use should ideally be adapted to the specific requirements resulting from the lack of intestinal “first-pass” metabolism. In other words, composition of AAs solution for PN cannot copy the enteral intake.
In the 80’s, great attention has been given to AA supply in VLBW infants from the first day of life in order to avoid catabolism, establish anabolism, achieve in utero protein accretion rates, and promote linear growth. Numerous studies have been performed for developing CAASs with the aim of resembling the plasma AA patterns of normally growing, breast fed infants, or resembling the AA profile of cord blood and achieving positive nitrogen balance. The direct study of the parenterally nourished patient led to the third generation of CAASs providing all nine essential AAs and a varying composition of non-essential AAs. Studies have been published on the clinical efficacy of altered doses of arginine, BCAAs, cysteine, or taurine supplementation of PN [57,58,59,60,61,62,63,64,65,66].
Today, most currently used AA mixtures contain AA amounts that result from this model. These pediatric AA mixtures provide more essential and less non-essential AAs. Specificities of those mixtures such as Vaminolact or Primene® (Baxter Maurepas, France) are nowadays well established.
An AA that should be included in pediatric AA solutions is taurine. Plasma, platelet, and urinary taurine levels have been shown to be significantly decreased in children on long-term HPN compared to those in normal children of similar age [67]. It has even been suggested that taurine may be conditionally essential in pediatric patients on long-term PN [68]. ESPGHAN/ESPEN/ESPR guidelines [49] recommend that AA solutions for infants and children should contain taurine, a recommendation that is based on data indicating that adequate taurine may prevent cholestasis in newborn infants.
3. PN with SMOFlipid in Newborn Infants, Infants/Toddlers, Children, and Adolescents – Clinical Experience
Special features of SMOFlipid
SMOFlipid is a composite ILE containing SO (30%), MCTs (30%), OO (25%), and FO (15%) and is supplemented with alpha-tocopherol (200 mg/L) to counteract lipid peroxidation and oxidative stress [22]. A key feature of SMOFlipid is its specific FA pattern resulting from the combination of these four different oils. In comparison to SO, SO/MCT or OO/SO-based ILEs, the pattern is more similar to human umbilical cord blood and breast milk, respectively, with regard to proportions of saturated fatty acids (SFAs), monounsaturated fatty acids (MUFAs), EFAs, and the omega-3 PUFAs EPA and DHA (Figure 1) [71,72,73]. Such a balanced FA supply is of relevance, especially for newborn infants, to maintain plasma and tissue FA patterns equivalent to those seen in breast-fed infants [32].
Several randomized clinical trials have been performed in VLBW infants comparing SO based ILEs and SMOFlipid [51,77,78,79,80,81].
In these studies, growth was not different between treatment groups, but those who received composite ILEs with FO had higher circulating EPA and DHA levels in both plasma and red blood cells (RBCs). Moreover, liver function tests (ALAT, ASAT, GGT, alkaline phosphatase) are less modified in those receiving FO based ILEs. This suggest that the reduced content of n-6 PUFAs and phytosterols in SMOFlipid can contribute to counteract inflammation and liver damages while the supply of adequate amounts of DHA supports visual, neural, and mental development [27,28,31,32,33].
In numerous clinical trials conducted in term newborn infants, infants and toddlers, older children and adolescents, SMOFlipid provided as a component of PN has been evaluated in comparison to other types of ILEs, especially SO based ILEs, in terms of effects on plasma and tissue FA patterns, inflammation and infections, cholestasis and liver function, growth and nutritional status as well as EFA status (see Table 1).
Table 1: Studies investigating PN with SMOFlipid in newborn infants, infants/toddlers, children, and adolescents [9,15,47,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107]
Effects on fatty acid patterns
Several studies evaluated effects of HPN with SMOFlipid on FA patterns in pediatric patients (Table 1). Goulet et al. conducted the first double blind RCT including infants and children on HPN receiving either SMOFlipid or a SO-based ILE [47]. Both ILEs were administered at a mean dose of 1.4 g lipids/kg BW/day. After 4 weeks, EPA and DHA contents in RBC and plasma phospholipids (PL) were significantly increased in the SMOFlipid group compared to controls. Moreover, the ratio of n-3 to n-6 FAs in plasma and RBC-PL was significantly elevated with SMOFlipid compared to SO-ILE [47]. Similar results have been published by Lezo et al. [86] from a study involving 38 pediatric patients with a median age of 5.56 (0.9-21.9) years on long-term PN receiving composite FO containing ILE (SMOFlipid) (n=23) or OO based ILE (Clinoleic) (n=15) at a dose of 1.3 g lipids/kg BW/day. Patients on SMOFlipid showed significantly higher levels of EPA and DHA as well as lower levels of ARA and Mead acid (MA)/ARA ratio in plasma and RBC compared with patients on Clinoleic and with healthy controls. Patients did not differ between groups for growth and liver status.
Potential risk of essential fatty acid deficiency
It has been claimed that pure FO based ILEs (e.g., Omegaven) were safe for achieving a normal EFA status [108]. Yet, ESPGHAN does not recommend the long-term use of Omegaven as the sole source of IV lipid [23]. As a corollary, effects of long-term use of SMOFlipid for children on long-term HPN receiving a composite FO based ILE, on the RBC FA profile and EFA status also remain to be clarified. With that aim, 46 children highly dependent on PN (median PNDI 120% and daily ILE dose of 1.5-2 g/kg BW) for ≥1 year were included in a prospective study when they had received the composite FO ILE for >6 month. Out of this baseline group, only 25 children remained highly PN dependent (SMOF1, n = 25) and could be assessed a second time, 2.4 years later (SMOF2, n = 25). An independent control group (“weaned off PN” group; n = 24) included children who had been weaned off PN for >2 years (median: 4 years). No differences for growth parameters, citrulline, and bilirubin were observed between the SMOF groups (0.2 < P < 0.8). The weaned-off group did not differ from the SMOF groups for growth parameters (0.2 < P < 0.4) but citrulline was higher (P < 0.0001), reflecting intestinal sufficiency. SMOFlipid induced higher percentages of EPA (20:5n–3) (8.4% ±2.9%) and DHA (22:6n–3) (11.7% ±2.2%) in RBC profiles in the SMOF2 group compared to weaned-off children (0.8% ± 0.4% and 6.6% ± 2.3%, respectively) but lower proportions of ARA (20:4n–6). However, the Holman index, a marker of EFA deficiency, did not vary between groups (P = 0.9). Authors concluded that long-term (>2.4 years) use of SMOFlipid was well tolerated in HPN-dependent children. The RBC-FA profile alterations were consistent with the omega-3 PUFA–enriched composition of this emulsion without evidence of EFA deficiency (see Table 1) [15].
Likewise, Lezo et al. found no significant differences in Holman index between pediatric patients of all age groups receiving HPN with SMOFlipid or OO/SO-ILE (Clinoleic) compared to healthy controls; there were no signs of EFA deficiency (Holman index ≥ 0.21) with either ILE [86].
Effects on inflammation and infections
Evidence on the effects of PN with SMOFlipid on parameters of inflammation and infections in hospitalized patients receiving PN is limited and lacking for patients receiving HPN. In a small RCT measuring levels of pro-inflammatory cytokines in 14 newborn infants receiving SMOFlipid (dose range 1-4 g lipids/kg BW/day) for 72 hours post gastrointestinal (GI) surgery, serum levels of IL-6 decreased from baseline to day 3 whereas there was an increase in IL-6 levels in controls receiving SO/MCT-ILE (p=0.007 for change between groups) [90]. The authors concluded that SMOFlipid was beneficial to ameliorate the inflammatory response post GI-surgery [90]. In a larger RCT including 160 newborn infants receiving either SMOFlipid or SO/MCT-ILE for 4-5 days after GI surgery (lipid dose 1-3 g/kg BW/day), no significant differences in pro-inflammatory cytokines or incidence of sepsis between groups were seen at 2 and 4 weeks post-surgery [95].
Effects on cholestasis/liver function
Hospitalized patients
In hospitalized newborn infants, infants/toddlers, children, and/or adolescents receiving PN with SMOFlipid administered at doses of up to 3 g lipids/kg BW/day for periods of 1 to 9 weeks, studies report significantly lower incidences of cholestasis and IFALD as reflected by significantly lower plasma conjugated bilirubin (CBil), total bilirubin (TBil), and direct bilirubin (DBil) levels compared to controls receiving SO-ILE [82,85,93,94,96,99]. Moreover, administration of SMOFlipid resulted in improved liver function as indicated by significantly lower levels of the liver enzymes alanine aminotransferase (ALT), aspartate aminotransferase (AST), and DBil levels compared to SO/MCT-ILE [95,102,105].
HPN patients
In 2010, a double blind RCT investigated the effects of SMOFlipid (lipid dose 1.4 g/kg BW/day) compared to the same dose of SO-ILE, on RBC FA profiles, and liver status in children receiving HPN over a period of 4 weeks. Parameters of liver function (ALAT, ASAT, GGT, alkaline phosphatase) were below critical values and tended to be lower after the 4 weeks study period compared to controls receiving SO-ILE. Total bilirubin decreased significantly with SMOFlipid whereas it increased with SO-ILE over the observation period, the change being significant between the treatment groups [47]. Muhammed et al. [107] published a cohort comparing serum bilirubin during 6 months in children with PN-associated jaundice who changed from SO based ILE Intralipid (n=9) to SMOFlipid (n=8). After 6 months, 5 of 8 children in the SMOFlipid and 2 of 9 children in the Intralipid group had total resolution of jaundice. The median bilirubin fell by 99 μmol/L in the SMOFlipid group but increased by 79 μmol/L in the Intralipid group (P=0.02). Belza et al. conducted a retrospective cohort study in infants with IF and found that SMOFlipid administered at doses between 2-3 g lipid/kg BW/day resulted in a lower incidence and decreased severity of IFALD over the first 12 months of administration compared with a historical cohort who received SO-ILE. Infants receiving SMOFlipid were less likely to reach critical CBil levels, and no infant receiving SMOFlipid required “rescue treatment” with pure FO-ILE for salvage of liver function [94]. In a large cross-sectional study including 578 pediatric patients enrolled in HPN centers in France between 2014 and 2019, it was reported that the use of SMOFlipid for these patients significantly increased within this period from 67.4% to 88.3%. Overall, the prevalence of cholestasis (Conjugated Bilirubin > 20mmole/L) was low and remained stable between 4.1 and 5.9% during the study period [9]. In a recent prospective cross-sectional study including 46 children on HPN who were highly dependent upon PN as indicated by the PNDI (median 120%), these investigators evaluated the clinical safety of SMOFlipid long-term administration (average duration 2.4 years) at doses between 1.5–2.0 g/kg BW/day [15]. Liver function tests (ALAT, ASAT, GGT, alkaline phosphatase) and indicators of cholestasis, especially CBil, were close to the normal range in the group receiving SMOFlipid. These results provide further evidence that PN with SMOFlipid reduces the risk of cholestasis and IFALD in the long-term [15].
Overall, studies investigating effects of HPN with SMOFlipid (doses up to 3 g lipids/kg BW/day) for varying durations ranging from 4 weeks to 6.6 years consistently report benefits in terms of correction or prevention of liver disease following SMOFlipid administration [47,84,88,107].
Effects on growth and nutritional status
Hospitalized patients
In studies evaluating effects of PN with SMOFlipid, administered in doses up to 3 g lipids /kg BW/day for 2 to 9 weeks to hospitalized pediatric patients of all age groups, no significant differences in weight gain and parameters of growth as compared to SO-ILE [82,96,105] or SO/MCT-ILE [95,102] were reported (see Table 1), indicating that SMOFlipid is at least equally effective as SO-based ILEs with regard to supporting adequate growth in these patients.
HPN patients
Several studies evaluated effects of long-term HPN with SMOFlipid on growth parameters (see Table 1). Goulet et al. found that after receiving SMOFlipid for more than 6 months, highly PN-dependent children (median age 5.8 years) on HPN showed normal body weight and height relative to growth charts for healthy children. After an extended PN duration of 2.4 years, growth parameters between patients still receiving PN with SMOFlipid and those weaned from PN did not show any significant differences and were consistent with normal growth rates [15]. Ho et al. retrospectively evaluated growth parameters in children on HPN from initiation of SMOFlipid up to 1.5 years post SMOFlipid initiation and found slight increases in body mass index (BMI) z-scores over this period that were, however, not significant [88]. In newborn infants with IF receiving PN with SMOFlipid (2-3 g lipids/kg BW/day) for an average of 421 days, Belza et al. reported significantly improved weight z-scores after 3 and 6 months compared to historic controls receiving SO-ILE. Anthropometric parameters including weight, height, and head circumference remained within the normal range with both ILEs [94]. Lezo et al. conducted a prospective multicenter study including pediatric patients of all age groups receiving HPN with SMOFlipid or OO/SO-ILE (median lipid dose 1.3 g/kg BW/day) for a mean duration of 22 and 21 months, respectively [86]. Median Z-scores of weight, height or BMI for age were not statistically significant between groups [86]. The authors concluded that both ILEs ensured adequate growth – despite the lower plasma levels of ARA seen in this study.
4. Crystalline Amino Acid Solutions for Newborn Infants, Infants/Toddlers, Children, and Adolescents – Clinical Experience
Special features
Vaminolact is a pediatric CAAS providing essential (49%) and non-essential (51%) AAs in a pattern similar to human milk (Figure 2). The AA composition of Vaminolact has a special focus on AAs that are critical for pediatric patients (Table 2). It supplies adequate amounts of cysteine and tyrosine to compensate for the insufficient synthetic capacity in newborn and young infants. Moreover, it provides higher amounts of arginine to account for reduced intestinal synthesis and lower amounts of methionine, phenylalanine, valine, and isoleucine to account for the lack of intestinal “first-pass” metabolism [54,55,56]. This helps to avoid plasma AAs imbalances in pediatric patients receiving PN.
There is no data available for supporting the use of adult CAASs such as Vamin® (Fresenius Kabi Bad Homburg, Germany) in infants, toddlers, children and adolescents. As a matter of fact, even designed for neonatology according to the value of CAASs, there is no worry to use them also in infants/toddlers, children, and adolescents. The literature reports valuable data supporting the safety and efficiency of those pediatric AAs mixtures on the short as well as the long-term (Table 1). Moreover, Vaminolact supplies taurine, an AA that may be conditionally essential in pediatric patients requiring long-term PN [68,111]. Taurine deficiency during the neonatal period may result in retinal dysfunction [112] as well as long-term neurodevelopmental impairment [113]. Additionally, available evidence suggests that adequate taurine provision may prevent cholestasis in newborn infants [112,114]. According to ESPGHAN/ESPEN/ESPR guidelines [49], taurine should be part of AA solutions for administration to the pediatric age group.
Clinical experience with Vaminolact
Nutritional efficacy and tolerance of Vaminolact has been proven by extensive clinical experience since its introduction to the market in 1989 and demonstrated by clinical studies showing adequate weight gain, positive or improved nitrogen balance, and normal development in pediatric patients receiving PN with Vaminolact in doses in line with ESPGHAN/ESPEN/ESPR guidelines (Table 3) [49].
Table 3: Studies investigating PN with Vaminolact in newborn infants, infants/toddlers, children [13,14,47,115,116,117,118,119,120,121,122,123]
In 1989, Puntis et al. reported results from the first published study comparing Vaminolact in parenterally fed surgical newborn infants and infants/toddlers to a conventional adult CAAS based on the AA pattern of egg protein (Vamin) [123]. Vaminolact was initiated at 0.5 g AA/kg BW/day and advanced to a maximum of 2.5 g AA/kg/day during the 6 days study period. Plasma concentrations of all AAs except threonine, lysine, histidine, and cysteine/cystine were closer to the reference plasma AA pattern of breast-fed infants than with the adult AA solution. In particular, infants receiving Vaminolact had a reduced risk of developing hyperphenylalaninemia, and hypotyrosinemia that have been associated with neurotoxicity in parenterally fed newborn infants [124]. From this short term study, no significant differences in growth or nitrogen retention were seen between the two groups and no hematological or biochemical measurements changed significantly in either group. Authors concluded that Vaminolact would be likely to lessen the risk of neurotoxicity resulting from AA imbalance [123].
In a subsequent study comparing these two CAASs (Vaminolact vs. Vamin) in critically ill newborn infants, Thornton et al found that taurine levels recovered more rapidly with Vaminolact (n.s.) while phenylalanine levels were significantly lower at day 1 and day 3. Moreover, administration of Vaminolact at a mean dose of 2.3 g AAs/kg BW/day from days 3 for a mean total duration of 12 days also resulted in substantially improved nitrogen balance when compared to the adult CAAS [122].
A clinical study involving hospitalized infants recovering from severe malnutrition receiving Vaminolact as part of total PN has shown a body weight gain after the 28 days study period was 110 ± 5% of optimal weight gain for age. In this study, the mean NPEI from PN was 104.3 ± 8.0 kcal/kg BW/d with a mean ratio of NPEI over REE (PNDI) of 210 ± 20%. Authors concluded that a NPEI twice the REE was optimal to achieve the targeted body weight gain in this population of malnourished infants on TPN [14].
A retrospective study by Abi Nader [13] investigated parameters of growth and nutritional status among infants/toddlers and children on HPN receiving Vaminolact or a similar AA solution adapted to the specific requirements of infants (Primene) at a mean dose of 2.9 g AAs/kg BW/day for a mean duration of 1.9 years [14]. Growth velocity for both body weight gain and size was within the normal range.
Nowadays, one should consider these pediatric CAASs as more adapted than any adult CAAS for short as well as for long-term use from birth to adolescence. They achieve normal body weight and size growth without any reported metabolic disorder.
The role for commercial multi-chamber bags inpediatric PN
PN formulations for pediatric patients can either be individualized, tailored to meet the specific requirements of the patient, or standardized which may be suitable for a broad range of patients [125,126]. Individualized PN formulations are prescribed and prepared, usually on a daily basis, in the hospital pharmacy or in specialized compounding centers [126]. Individualized PN has long been regarded as the standard for PN in term infants, infants/toddlers, children, and adolescents. Nowadays there are concerns about hospital compounded bags regarding the adequacy of nutrient delivery as well as prescribing and compounding errors [127]. Individualizing PN in pediatric patients entails a large number of calculations and numerous patient-specific characteristics must be accounted for. It is, therefore, particularly prone to errors, in particular concentration errors with a reported error rate of 6% in a neonatal/pediatric ICU [128]. It is moreover unlikely that an expert in pediatric nutrition is readily available in each center [129].
With standardized PN formulations, in particular with ready-to-use, commercially manufactured multi-chamber bags (MCBs), this problem may be overcome since an expert nutrition care team can order the most common and suitable bags in advance [129]. Commercial MCBs can reduce infection risk, provide an adequate supply of nutrients, support adequate growth, provide ease of use, decrease prescription errors, and potentially reduce costs compared to individually compounded bags [130,131]. Thus, they can provide important benefits in pediatric patients, particularly in smaller centers where automated compounding facilities are not available. A major advantage of standardized PN bags vs. individualized PN is related to their immediate availability on demand due to easy storage and longer shelf life of approximately 2 years, while individualized formulations cannot be prepared at any time and require highly aseptic conditions, specifically trained staff, and a longer lead time for provision [132,133]. Indeed, roles for commercial MCBs have been proposed during emergency situations that make it impossible to acquire supplies, during power failures interrupting the cooling chain, travel, or shortages of single PN components have been proposed [134,135].
According to current ESPGHAN/ESPEN/ESPR guidelines [125], standard PN solutions should generally be chosen over individualized PN solutions in the majority of pediatric and newborn patients [125]. Yet, although a wide variety of commercial MCBs are available for adults, these are not optimal for infants and children as their metabolic demands and nutritional needs differ significantly, depending on age, weight, underlying disease, nutritional and hydration status, and environmental factors [3,126,136]. Accordingly, standard PN formulations designed specifically to meet the varying nutritional requirements of newborn infants, infants/toddlers, children, and adolescents have been developed and made commercially available [126]. These modern commercial MCBs contain fixed amounts of nutrients conform to current guidelines, thus, enabling an improved compliance with guidelines [125,133]. These MCBs should contain last generation ILEs and AA solutions adapted for pediatric use.
However, there seem to be pediatric patients whose requirements cannot be met by standard regimes, especially among patients requiring PN for longer periods. As described in the current literature, only few children receive standard formulas in the HPN setting. According to a large national survey form France, only 0.3 to 7.2% of HPN patients received standardized formulations between 2014 and 2019, mostly during holidays or during the period of the process of weaning from PN [9]. A European survey of 61 IF teams from 20 countries found that HPN was provided in form of individually age- and weight-specific customized bags in 78% of the IF teams, as commercial MCBs without adaptations in 25% of teams and as commercial MCBs customized by the pharmacy in 31% of teams (multiple answers per team possible) [137]. Indeed, customizing commercial MCBs by individual additions of electrolytes when required may represent a promising strategy to increase the number of HPN patients that could benefit from standardized PN formulations.
5. Summary and Conclusion
With the evolution of practices and extended use of PN in hospitalized as well as HPN pediatric patients, MCBs adapted to this age group are needed. The safety and efficacy of lipid and AA components are well documented from many reported studies, most of which are reviewed in this article. The onset of composite FO-based ILEs (SMOFlipid) calls for the development of MCBs containing these ILEs in combination with CAAS adapted for use in pediatric patients. Overall, the available evidence clearly supports the benefits of SMOFlipid administered at doses in line with ESPGHAN/ESPEN/ESPR guidelines [23] in terms of improving the RBC-FA profile without an increased risk of essential fatty acid deficiency (EFAD), of reducing or reversing IFALD, while ensuring adequate growth, both in hospitalized or HPN pediatric patients (see Table 1). The advantages of MCBs have been underlined especially in hospitalized pediatric patients while open discussion should be promoted for its use for HPN pediatric patients.
Funding
Fresenius Kabi GmbH provided financial support for the development of this review.
Acknowledgments
The authors are grateful to Fresenius Kabi for their support in the production of this review.
Abbreviations
- -
- AA: amino acid
- -
- ALA: alpha-linolenic acid
- -
- ALT: alanine aminotransferase
- -
- ARA: arachidonic acid
- -
- AST: aspartate aminotransferase
- -
- BW: body weight
- -
- CAAS: crystalline amino acids solution
- -
- CBil: conjugated bilirubin
- -
- DBil: direct bilirubin
- -
- DHA: docosahexaenoic acid
- -
- EFA: essential fatty acid
- -
- EFAD: essential fatty acid deficiency
- -
- EPA: eicosapentaenoic acid
- -
- FA: fatty acid
- -
- FO: fish oil
- -
- GGT: gamma-glutamyl transferase
- -
- HPN: home parenteral nutrition
- -
- IF: intestinal failure
- -
- IFALD: intestinal failure associated liver disease
- -
- ILE: intravenous lipid emulsion
- -
- LA: linoleic acid
- -
- LCPUFA: long-chain polyunsaturated fatty acid
- -
- LNA: linolenic acid
- -
- MCB: multi-chamber bags
- -
- MCT: medium-chain triglyceride
- -
- NPEI: non-protein-energy intake
- -
- OO: olive oil
- -
- PN: parenteral nutrition
- -
- PNDI: parenteral nutrition dependency index
- -
- PUFA: polyunsaturated fatty acid
- -
- RBC: red blood cell
- -
- RDA: recommended dietary allowance
- -
- REE: resting energy expenditure
- -
- SBS: short bowel syndrome
- -
- SO: soybean oil
- -
- TBil: total bilirubin
- -
- VLBW: very low birth weight
References
- Worthington, P.; Balint, J.; Bechtold, M.; Bingham, A.; Chan, L.-N.; Durfee, S.; Jevenn, A.K.; Malone, A.; Mascarenhas, M.; Robinson, D.T. When Is Parenteral Nutrition Appropriate? JPEN J Parenter Enteral Nutr 2017, 41, 324-377. [CrossRef]
- Koletzko, B.; Goulet, O.; Hunt, J.; Krohn, K.; Shamir, R. 1. Guidelines on Paediatric Parenteral Nutrition of the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) and the European Society for Clinical Nutrition and Metabolism (ESPEN), Supported by the European Society of Paediatric Research (ESPR). J Pediatr Gastroenterol Nutr 2005, 41 Suppl 2, S1-87. [CrossRef]
- Joosten, K.; Embleton, N.; Yan, W.; Senterre, T. ESPGHAN/ESPEN/ESPR guidelines on pediatric parenteral nutrition: Energy. Clin Nutr 2018, 37, 2309-2314. [CrossRef]
- Ayers, P.; Boullata, J.; Sacks, G. Parenteral nutrition safety: the story continues. Nutr Clin Pract 2018, 33, 46-52. [CrossRef]
- Singer, P. Advances in Medical Nutrition Therapy: Parenteral Nutrition. Nutrients 2020, 12, 717. [CrossRef]
- Keady, S.; Morgan, C.; Ozzard, A.; Chauhan, B. Effect of a neonatal standard aqueous parenteral nutrition formulation on aseptic unit capacity planning. e-SPEN 2010, 5, e14-e17. [CrossRef]
- Goulet, O.; Ruemmele, F. Causes and management of intestinal failure in children. Gastroenterology 2006, 130, S16-S28. [CrossRef]
- Vlug, L.E.; Nagelkerke, S.C.J.; Jonkers-Schuitema, C.F.; Rings, E.; Tabbers, M.M. The Role of a Nutrition Support Team in the Management of Intestinal Failure Patients. Nutrients 2020, 12, 172. [CrossRef]
- Goulet, O.; Breton, A.; Coste, M.E.; Dubern, B.; Ecochard-Dugelay, E.; Guimber, D.; Loras-Duclaux, I.; Abi Nader, E.; Marinier, E.; Peretti, N.; et al. Pediatric Home Parenteral Nutrition in France: A six years national survey. Clin Nutr 2021, 40, 5278-5287. [CrossRef]
- Elia, M. Changing concepts of nutrient requirements in disease: implications for artificial nutritional support. Lancet 1995, 345, 1279-1284. [CrossRef]
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum Nutr Clin Nutr 1985, 39 Suppl 1, 5-41.
- Goulet, O.; Abi Nader, E.; Pigneur, B.; Lambe, C. Short Bowel Syndrome as the Leading Cause of Intestinal Failure in Early Life: Some Insights into the Management. Pediatr Gastroenterol Hepatol Nutr 2019, 22, 303-329. [CrossRef]
- Abi Nader, E.; Lambe, C.; Talbotec, C.; Pigneur, B.; Lacaille, F.; Garnier-Lengliné, H.; Petit, L.M.; Poisson, C.; Rocha, A.; Corriol, O.; et al. Outcome of home parenteral nutrition in 251 children over a 14-y period: report of a single center. Am J Clin Nutr 2016, 103, 1327-1336. [CrossRef]
- Abi Nader, E.; Lambe, C.; Talbotec, C.; Dong, L.; Pigneur, B.; Goulet, O. A new concept to achieve optimal weight gain in malnourished infants on total parenteral nutrition. JPEN J Parenter Enteral Nutr 2018, 42, 78-86. [CrossRef]
- Goulet, O.; Lamazière, A.; Abi Nader, E.; Talbotec, C.; Wolf, C.; Lambe, C. Erythrocyte fatty acid membrane composition in children on long-term parenteral nutrition enriched with ω-3 fatty acids. Am J Clin Nutr 2022, 115, 422-431. [CrossRef]
- Mehta, N.M.; Compher, C. A.S.P.E.N. Clinical Guidelines: nutrition support of the critically ill child. JPEN J Parenter Enteral Nutr 2009, 33, 260-276. [CrossRef]
- Mesotten, D.; Joosten, K.; van Kempen, A.; Verbruggen, S. ESPGHAN/ESPEN/ESPR guidelines on pediatric parenteral nutrition: Carbohydrates. Clin Nutr 2018, 37, 2337-2343. [CrossRef]
- Bresson, J.L.; Narcy, P.; Putet, G.; Ricour, C.; Sachs, C.; Rey, J. Energy substrate utilization in infants receiving total parenteral nutrition with different glucose to fat ratios. Pediatr Res 1989, 25, 645-648. [CrossRef]
- Salas, J.; Girardet, J.P.; De Potter, S.; Martí-Henneberg, C.; Goulet, O.; Ricour, C. Glucose versus glucose-fat mixture in the course of total parenteral nutrition: effects on substrate utilisation and energy metabolism in malnourished children. Clin Nutr 1991, 10, 272-278. [CrossRef]
- Preissig, C.M.; Rigby, M.R. Hyperglycaemia results from beta-cell dysfunction in critically ill children with respiratory and cardiovascular failure: a prospective observational study. Crit Care 2009, 13, R27. [CrossRef]
- Hirshberg, E.; Larsen, G.; Van Duker, H. Alterations in glucose homeostasis in the pediatric intensive care unit: Hyperglycemia and glucose variability are associated with increased mortality and morbidity. Pediatr Crit Care Med 2008, 9, 361-366. [CrossRef]
- Dasarathy, S.; Dodig, M.; Muc, S.M.; Kalhan, S.C.; McCullough, A.J. Skeletal muscle atrophy is associated with an increased expression of myostatin and impaired satellite cell function in the portacaval anastamosis rat. Am J Physiol Gastrointest Liver Physiol 2004, 287, G1124-1130. [CrossRef]
- Lapillonne, A.; Fidler Mis, N.; Goulet, O.; van den Akker, C.H.P.; Wu, J.; Koletzko, B. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Lipids. Clin Nutr 2018, 37, 2324-2336. [CrossRef]
- Goulet, O.J.; Cai, W.; Seo, J.M. Lipid Emulsion Use in Pediatric Patients Requiring Long-Term Parenteral Nutrition. JPEN J Parenter Enteral Nutr 2020, 44 Suppl 1, S55-S67. [CrossRef]
- Martindale, R.G.; Berlana, D.; Boullata, J.I.; Cai, W.; Calder, P.C.; Deshpande, G.H.; Evans, D.; Garcia-de-Lorenzo, A.; Goulet, O.J.; Li, A.; et al. Summary of Proceedings and Expert Consensus Statements From the International Summit “Lipids in Parenteral Nutrition”. JPEN J Parenter Enteral Nutr 2020, 44 Suppl 1, S7-S20. [CrossRef]
- Salas, J.S.; Dozio, E.; Goulet, O.J.; Marti-Henneberg, C.; Moukarzel, E.; Ricour, C. Energy expenditure and substrate utilization in the course of renutrition of malnourished children. JPEN J Parenter Enteral Nutr 1991, 15, 288-293. [CrossRef]
- Deshpande, G.C.; Cai, W. Use of Lipids in Neonates Requiring Parenteral Nutrition. JPEN J Parenter Enteral Nutr 2020, 44 Suppl 1, S45-s54. [CrossRef]
- Klek, S. Omega-3 Fatty Acids in Modern Parenteral Nutrition: A Review of the Current Evidence. J Clin Med 2016, 5, 34. [CrossRef]
- Serhan, C.N.; Levy, B.D. Resolvins in inflammation: emergence of the pro-resolving superfamily of mediators. J Clin Invest 2018, 128, 2657-2669. [CrossRef]
- Calder, P.C.; Waitzberg, D.L.; Klek, S.; Martindale, R.G. Lipids in Parenteral Nutrition: Biological Aspects. JPEN J Parenter Enteral Nutr 2020, 44 Suppl 1, S21-S27. [CrossRef]
- Wanten, G.J.; Calder, P.C. Immune modulation by parenteral lipid emulsions. Am J Clin Nutr 2007, 85, 1171-1184. [CrossRef]
- Lien, E.L.; Richard, C.; Hoffman, D.R. DHA and ARA addition to infant formula: Current status and future research directions. Prostaglandins Leukot Essent Fatty Acids 2018, 128, 26-40. [CrossRef]
- Hoffman, D.R.; Boettcher, J.A.; Diersen-Schade, D.A. Toward optimizing vision and cognition in term infants by dietary docosahexaenoic and arachidonic acid supplementation: a review of randomized controlled trials. Prostaglandins Leukot Essent Fatty Acids 2009, 81, 151-158. [CrossRef]
- Qawasmi, A.; Landeros-Weisenberger, A.; Bloch, M.H. Meta-analysis of LCPUFA supplementation of infant formula and visual acuity. Pediatrics 2013, 131, e262-272. [CrossRef]
- Goulet, O.; De Potter, S.; Antebi, H.; Driss, F.; Colomb, V.; Bereziat, G.; Alcindor, L.G.; Corriol, O.; Le Brun, A.; Dutot, G.; et al. Long-term efficacy and safety of a new olive oil-based intravenous fat emulsion in pediatric patients: a double-blind randomized study. Am J Clin Nutr 1999, 70, 338-345. [CrossRef]
- Goulet, O.; Joly, F.; Corriol, O.; Colomb-Jung, V. Some new insights in intestinal failure-associated liver disease. Curr Opin Organ Transplant 2009, 14, 256-261. [CrossRef]
- Lacaille, F.; Gupte, G.; Colomb, V.; D'Antiga, L.; Hartman, C.; Hojsak, I.; Kolacek, S.; Puntis, J.; Shamir, R. Intestinal failure-associated liver disease: a position paper of the ESPGHAN Working Group of Intestinal Failure and Intestinal Transplantation. J Pediatr Gastroenterol Nutr 2015, 60, 272-283. [CrossRef]
- Gura, K.M.; Duggan, C.P.; Collier, S.B.; Jennings, R.W.; Folkman, J.; Bistrian, B.R.; Puder, M. Reversal of parenteral nutrition-associated liver disease in two infants with short bowel syndrome using parenteral fish oil: implications for future management. Pediatrics 2006, 118, e197-e201. [CrossRef]
- Nandivada, P.; Baker, M.A.; Mitchell, P.D.; O'Loughlin, A.A.; Potemkin, A.K.; Anez-Bustillos, L.; Carlson, S.J.; Dao, D.T.; Fell, G.L.; Gura, K.M.; et al. Predictors of failure of fish-oil therapy for intestinal failure-associated liver disease in children. Am J Clin Nutr 2016, 104, 663-670. [CrossRef]
- Hojsak, I.; Colomb, V.; Braegger, C.; Bronsky, J.; Campoy, C.; Domellof, M.; Embleton, N.; Fidler Mis, N.; Hulst, J.M.; Indrio, F.; et al. ESPGHAN Committee on Nutrition Position Paper. Intravenous Lipid Emulsions and Risk of Hepatotoxicity in Infants and Children: a Systematic Review and Meta-analysis. J Pediatr Gastroenterol Nutr 2016, 62, 776-792. [CrossRef]
- Dupont, I. Peroxidation of lipid emulsions: effects of changes in fatty acid pattern and α-tocopherol content on the sensitivity to peroxidative damage. Clin Nutr 1999, 18, 113-116. [CrossRef]
- Goulet, O.; Girot, R.; Maier-Redelsperger, M.; Bougle, D.; Virelizier, J.L.; Ricour, C. Hematologic disorders following prolonged use of intravenous fat emulsions in children. JPEN J Parenter Enteral Nutr 1986, 10, 284-288. [CrossRef]
- Hukkinen, M.; Mutanen, A.; Nissinen, M.; Merras-Salmio, L.; Gylling, H.; Pakarinen, M.P. Parenteral Plant Sterols Accumulate in the Liver Reflecting Their Increased Serum Levels and Portal Inflammation in Children With Intestinal Failure. JPEN J Parenter Enteral Nutr 2017, 41, 1014-1022. [CrossRef]
- Pereira-Fantini, P.M.; Lapthorne, S.; Gahan, C.G.M.; Joyce, S.A.; Charles, J.; Fuller, P.J.; Bines, J.E. Farnesoid X Receptor Agonist Treatment Alters Bile Acid Metabolism but Exacerbates Liver Damage in a Piglet Model of Short-Bowel Syndrome. Cell Mol Gastroenterol Hepatol 2017, 4, 65-74. [CrossRef]
- Cao, Y.; Xiao, Y.; Zhou, K.; Yan, J.; Wang, P.; Yan, W.; Cai, W. FXR agonist GW4064 improves liver and intestinal pathology and alters bile acid metabolism in rats undergoing small intestinal resection. Am J Physiol Gastrointest Liver Physiol 2019, 317, G108-G115. [CrossRef]
- Bach, A.C.; Babayan, V.K. Medium-chain triglycerides: an update. Am J Clin Nutr 1982, 36, 950-962. [CrossRef]
- Goulet, O.; Antebi, H.; Wolf, C.; Talbotec, C.; Alcindor, L.G.; Corriol, O.; Lamor, M.; Colomb-Jung, V. A new intravenous fat emulsion containing soybean oil, medium-chain triglycerides, olive oil, and fish oil: a single-center, double-blind randomized study on efficacy and safety in pediatric patients receiving home parenteral nutrition. JPEN J Parenter Enteral Nutr 2010, 34, 485-495. [CrossRef]
- ASPEN. Guidelines for the use of parenteral and enteral nutrition in adult and paediatric patients. JPEN J Parenter Enteral Nutr 2002, 26, 1SA-138SA. [CrossRef]
- van Goudoever, J.B.; Carnielli, V.; Darmaun, D.; Sainz de Pipaon, M. ESPGHAN/ESPEN/ESPR guidelines on pediatric parenteral nutrition: Amino acids. Clin Nutr 2018, 37, 2315-2323. [CrossRef]
- Goulet, O.; DePotter, S.; Salas, J.; Robert, J.J.; Rongier, M.; Ben Hariz, M.; Koziet, J.; Desjeux, J.F.; Ricour, C.; Darmaun, D. Leucine metabolism at graded amino acid intakes in children receiving parenteral nutrition. Am J Physiol 1993, 265, E540-546. [CrossRef]
- Vlaardingerbroek, H.; Vermeulen, M.J.; Carnielli, V.P.; Vaz, F.M.; van den Akker, C.H.; van Goudoever, J.B. Growth and fatty acid profiles of VLBW infants receiving a multicomponent lipid emulsion from birth. J Pediatr Gastroenterol Nutr 2014, 58, 417-427. [CrossRef]
- Dudrick, S.J.; Wilmore, D.W.; Vars, H.M.; Rhoads, J.E. Long-term total parenteral nutrition with growth, development, and positive nitrogen balance. Surgery 1968, 64, 134-142.
- Holt, L.E., Jr.; Snyderman, S.E. The amino acid requirements of infants. Jama 1961, 175, 100-103. [CrossRef]
- Elango, R.; Pencharz, P.B.; Ball, R.O. The branched-chain amino acid requirement of parenterally fed neonatal piglets is less than the enteral requirement. J Nutr 2002, 132, 3123-3129. [CrossRef]
- Kien, C.L.; Horswill, C.A.; Zipf, W.B.; McCoy, K.S.; Denne, S.C. Splanchnic uptake of leucine in healthy children and in children with cystic fibrosis. Pediatr Res 1999, 45, 680-683. [CrossRef]
- Heird, W.C. Amino acids in pediatric and neonatal nutrition. Curr Opin Clin Nutr Metab Care 1998, 1, 73-78. [CrossRef]
- Beganović, N.; Kok, K.; de Leeuw, R.; de Vries, I.J.; Schutgens, R. Amino acids in parenteral nutrition of preterm infants. Comparison of oral and parenteral supply. Acta Paediatr Scand 1983, 72, 421-425. [CrossRef]
- Andersen, G.E.; Bucher, D.; Friis-Hansen, B.; Nexø, E.; Olesen, H. Plasma amino acid concentrations in newborn infants during parenteral nutrition. JPEN J Parenter Enteral Nutr 1983, 7, 369-373. [CrossRef]
- Bürger, U.; Wolf, H.; Fritsch, U.; Bauer, M. Parenteral nutrition in preterm infants: influence of respiratory treatment and effect of different amino acid compositions. J Pediatr Gastroenterol Nutr 1983, 2, 644-652.
- Bell, E.F.; Filer, L.J., Jr.; Wong, A.P.; Stegink, L.D. Effects of a parenteral nutrition regimen containing dicarboxylic amino acids on plasma, erythrocyte, and urinary amino acid concentrations of young infants. Am J Clin Nutr 1983, 37, 99-107. [CrossRef]
- Coran, A.G.; Drongowski, R.A. Studies on the toxicity and efficacy of a new amino acid solution in pediatric parenteral nutrition. JPEN J Parenter Enteral Nutr 1987, 11, 368-377. [CrossRef]
- Sankaran, K.; Berscheid, B.; Verma, V.; Zakhary, G.; Tan, L. An evaluation of total parenteral nutrition using Vamin and Aminosyn as protein base in critically ill preterm infants. JPEN J Parenter Enteral Nutr 1985, 9, 439-442. [CrossRef]
- Chessex, P.; Zebiche, H.; Pineault, M.; Lepage, D.; Dallaire, L. Effect of amino acid composition of parenteral solutions on nitrogen retention and metabolic response in very-low-birth weight infants. J Pediatr 1985, 106, 111-117. [CrossRef]
- Meurling, S.; Grotte, G. Total parenteral nutrition in pediatric surgery using a new amino acid solution (Vaminolac). Acta Chir Scand Suppl 1983, 517, 79-87.
- Pineault, M.; Chessex, P.; Lepage, D.; Dallaire, L.; Brisson, G.; Qureshi, I. Total parenteral nutrition in very low birth weight infants with Travasol 10% blend C. JPEN J Parenter Enteral Nutr 1986, 10, 296-299. [CrossRef]
- Vlaardingerbroek, H.; Roelants, J.A.; Rook, D.; Dorst, K.; Schierbeek, H.; Vermes, A.; Vermeulen, M.J.; van Goudoever, J.B.; van den Akker, C.H. Adaptive regulation of amino acid metabolism on early parenteral lipid and high-dose amino acid administration in VLBW infants - a randomized, controlled trial. Clin Nutr 2014, 33, 982-990. [CrossRef]
- Vinton, N.E.; Laidlaw, S.A.; Ament, M.E.; Kopple, J.D. Taurine concentrations in plasma, blood cells, and urine of children undergoing long-term total parenteral nutrition. Pediatr Res 1987, 21, 399-403. [CrossRef]
- Laidlaw, S.A.; Kopple, J.D. Newer concepts of the indispensable amino acids. Am J Clin Nutr 1987, 46, 593-605. [CrossRef]
- Fitzgerald, K.A.; MacKay, M.W. Calcium and phosphate solubility in neonatal parenteral nutrient solutions containing TrophAmine. Am J Hosp Pharm 1986, 43, 88-93.
- Fitzgerald, K.A.; MacKay, M.W. Calcium and phosphate solubility in neonatal parenteral nutrient solutions containing Aminosyn PF. Am J Hosp Pharm 1987, 44, 1396-1400.
- Koletzko, B.; Rodriguez-Palmero, M.; Demmelmair, H.; Fidler, N.; Jensen, R.; Sauerwald, T. Physiological aspects of human milk lipids. Early Hum Dev 2001, 65 Suppl, S3-S18. [CrossRef]
- Gil, A.; Ramirez, M.; Gil, M. Role of long-chain polyunsaturated fatty acids in infant nutrition. Eur J Clin Nutr 2003, 57 Suppl 1, S31-S34. [CrossRef]
- Oliveira, O.R.; Santana, M.G.; Santos, F.S.; Conceição, F.D.; Sardinha, F.L.; Veiga, G.V.; Tavares do Carmo, M.G. Composition of fatty acids in the maternal and umbilical cord plasma of adolescent and adult mothers: relationship with anthropometric parameters of newborn. Lipids Health Dis 2012, 11, 157. [CrossRef]
- Agostoni, C.; Galli, C.; Riva, E.; Risé, P.; Colombo, C.; Giovannini, M.; Marangoni, F. Whole blood fatty acid composition at birth: from the maternal compartment to the infant. Clin Nutr 2011, 30, 503-505. [CrossRef]
- Koletzko, B. Human Milk Lipids. Ann Nutr Metab 2016, 69 Suppl 2, 28-40. [CrossRef]
- Koletzko, B.; Goulet, O.; Hunt, J.; Krohn, K.; Shamir, R. 1. Guidelines on Paediatric Parenteral Nutrition of the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) and the European Society for Clinical Nutrition and Metabolism (ESPEN), Supported by the European Society of Paediatric Research (ESPR). J Pediatr Gastroenterol Nutr 2005, 41 Suppl 2, S1-87. [CrossRef]
- Tomsits, E.; Pataki, M.; Tölgyesi, A.; Fekete, G.; Rischak, K.; Szollár, L. Safety and efficacy of a lipid emulsion containing a mixture of soybean oil, medium-chain triglycerides, olive oil, and fish oil: a randomised, double-blind clinical trial in premature infants requiring parenteral nutrition. J Pediatr Gastroenterol Nutr 2010, 51, 514-521. [CrossRef]
- Skouroliakou, M.; Konstantinou, D.; Koutri, K.; Kakavelaki, C.; Stathopoulou, M.; Antoniadi, M.; Xemelidis, N.; Kona, V.; Markantonis, S. A double-blind, randomized clinical trial of the effect of omega-3 fatty acids on the oxidative stress of preterm neonates fed through parenteral nutrition. Eur J Clin Nutr 2010, 64, 940-947. [CrossRef]
- Skouroliakou, M.; Konstantinou, D.; Agakidis, C.; Kaliora, A.; Kalogeropoulos, N.; Massara, P.; Antoniadi, M.; Panagiotakos, D.; Karagiozoglou-Lampoudi, T. Parenteral MCT/omega-3 Polyunsaturated Fatty Acid-Enriched Intravenous Fat Emulsion Is Associated With Cytokine and Fatty Acid Profiles Consistent With Attenuated Inflammatory Response in Preterm Neonates: A Randomized, Double-Blind Clinical Trial. Nutr Clin Pract 2016, 31, 235-244. [CrossRef]
- Rayyan, M.; Devlieger, H.; Jochum, F.; Allegaert, K. Short-term use of parenteral nutrition with a lipid emulsion containing a mixture of soybean oil, olive oil, medium-chain triglycerides, and fish oil: a randomized, double-blind study in preterm infants. JPEN J Parenter Enteral Nutr 2012, 36, 81S-94S. [CrossRef]
- Deshpande, G.; Simmer, K.; Deshmukh, M.; Mori, T.A.; Croft, K.D.; Kristensen, J. Fish Oil (SMOFlipid) and olive oil lipid (Clinoleic) in very preterm neonates. J Pediatr Gastroenterol Nutr 2014, 58, 177-182. [CrossRef]
- Navaratnarajah, N.; Girard, G.; Sant'Anna, G.; Langlois, H.; Sant'Anna, A.M. The impact of a lipid injectable emulsion (SMOF) on conjugated bilirubin levels in children receiving prolonged parenteral nutrition: A large single center experience. Clin Nutr ESPEN 2022, 49, 289-294. [CrossRef]
- Rumore, S.; McGrath, K.; Scott, A.; Sexton, E.; Wong, T. Fat soluble vitamin status in children on home parenteral nutrition in a tertiary paediatric intestinal rehabilitation unit. Clin Nutr ESPEN 2021, 46, 240-245. [CrossRef]
- Wassef, J.; Lipkin, E.; Hardigan, P.; Duro, D. Trends in liver profile and nutrition outcomes in children undergoing intestinal rehabilitation using a mixed lipid injectable emulsion. Nutr Clin Pract 2021, 37, 1180-1189. [CrossRef]
- Daniel, S.; Svoboda, L.; Chen, J. Liver Function in Pediatric Recipients: A Comparison of Intralipid and Smoflipid. J Pediatr Pharmacol Ther 2021, 26, 258-264. [CrossRef]
- Lezo, A.; D'Onofrio, V.; Puccinelli, M.P.; Capriati, T.; De Francesco, A.; Bo, S.; Massarenti, P.; Gandullia, P.; Marin, M.; Derevlean, L.; et al. Plasma and Red Blood Cell PUFAs in Home Parenteral Nutrition Paediatric Patients-Effects of Lipid Emulsions. Nutrients 2020, 12, 3748. [CrossRef]
- Nagelkerke, S.C.J.; Draijer, L.G.; Benninga, M.A.; Koot, B.G.P.; Tabbers, M.M. The prevalence of liver fibrosis according to non-invasive tools in a pediatric home parenteral nutrition cohort. Clin Nutr 2021, 40, 460-466. [CrossRef]
- Ho, B.E.; Chan, S.C.; Faino, A.V.; Mortensen, M.; Williamson, N.; Javid, P.J.; Horslen, S.P.; Wendel, D. Evaluation of SMOFlipid in Pediatric Intestinal-Failure Patients and Its Effects on Essential Fatty Acid Levels. JPEN J Parenter Enteral Nutr 2021, 45, 546-552. [CrossRef]
- Huff, K.A.; Breckler, F.; Cruse, W.; Szeszycki, E.; Vanderpool, C. Pediatric Smoflipid Therapy: Patient Response and Safety Concerns. JPEN J Parenter Enteral Nutr 2021, 45, 792-799. [CrossRef]
- Hanindita, M.H.; Widjaja, N.A.; Irawan, R.; Hidajat, B. Influence of intravenous fish oil-enriched lipid emulsion on the inflammatory response in children post gastrointestinal surgery. Pak J Nutr 2019, 18, 1036-1041. [CrossRef]
- Hanindita, M.H.; Widjaja, N.A.; Irawan, R.; Hidayat, B.; Hariastawa, I.A. Impact of Intravenous Omega-3-Enriched Lipid Emulsion on Liver Enzyme and Triglyceride Serum Levels of Children Undergoing Gastrointestinal Surgery. Pediatr Gastroenterol Hepatol Nutr 2020, 23, 98-104. [CrossRef]
- Danko, M.; Żyła-Pawlak, A.; Książyk, J.; Olszewska-Durkacz, K.; Sibilska, M.; Żydak, J.; Popińska, K. A Retrospective Analysis of the Effect of Combination of Pure Fish Oil with Third Generation Lipid Emulsion on Liver Function in Children on Long-Term Parenteral Nutrition. Nutrients 2019, 11, 2495. [CrossRef]
- Casson, C.; Nguyen, V.; Nayak, P.; Channabasappa, N.; Berris, K.; Panczuk, J.; Bhiladvala, C.; Dasgupta, T.; Piper, H.G. A Comparison of Smoflipid® and Intralipid® in the Early Management of Infants with Intestinal Failure. J Pediatr Surg 2020, 55, 153-157. [CrossRef]
- Belza, C.; Wales, J.C.; Courtney-Martin, G.; de Silva, N.; Avitzur, Y.; Wales, P.W. An Observational Study of Smoflipid vs Intralipid on the Evolution of Intestinal Failure-Associated Liver Disease in Infants With Intestinal Failure. JPEN J Parenter Enteral Nutr 2020, 44, 688-696. [CrossRef]
- Jiang, W.; Chen, G.; Zhang, J.; Lv, X.; Lu, C.; Chen, H.; Li, W.; Li, H.; Geng, Q.; Xu, X.; et al. The effects of two mixed intravenous lipid emulsions on clinical outcomes in infants after gastrointestinal surgery: a prospective, randomized study. Pediatr Surg Int 2019, 35, 347-355. [CrossRef]
- Lam, C.K.L.; Church, P.C.; Haliburton, B.; Chambers, K.; Martincevic, I.; Vresk, L.; Courtney-Martin, G.; Bandsma, R.; Avitzur, Y.; Wales, P.C.; et al. Long-term Exposure of Children to a Mixed Lipid Emulsion Is Less Hepatotoxic Than Soybean-based Lipid Emulsion. J Pediatr Gastroenterol Nutr 2018, 66, 501-504. [CrossRef]
- Olszewska, K.; Ksiazyk, J.; Kozlowski, D.; Pajdowska, M.; Janusz, M.; Jaworski, M. Nutritional therapy complications in children with ultra-short bowel syndrome include growth deficiency but not cholestasis. Acta Paediatr 2018, 107, 1088-1093. [CrossRef]
- Pereira-da-Silva, L.; Nóbrega, S.; Rosa, M.L.; Alves, M.; Pita, A.; Virella, D.; Papoila, A.L.; Serelha, M.; Cordeiro-Ferreira, G.; Koletzko, B. Parenteral nutrition-associated cholestasis and triglyceridemia in surgical term and near-term neonates: A pilot randomized controlled trial of two mixed intravenous lipid emulsions. Clin Nutr ESPEN 2017, 22, 7-12. [CrossRef]
- Diamond, I.R.; Grant, R.C.; Pencharz, P.B.; de Silva, N.; Feldman, B.M.; Fitzgerald, P.; Sigalet, D.; Dicken, B.; Turner, J.; Marchand, V.; et al. Preventing the Progression of Intestinal Failure-Associated Liver Disease in Infants Using a Composite Lipid Emulsion: A Pilot Randomized Controlled Trial of SMOFlipid. JPEN J Parenter Enteral Nutr 2017, 41, 866-877. [CrossRef]
- Pichler, J.; Watson, T.; McHugh, K.; Hill, S. Prevalence of Gallstones Compared in Children With Different Intravenous Lipids. J Pediatr Gastroenterol Nutr 2015, 61, 253-259. [CrossRef]
- De Cunto, A.; Paviotti, G.; Travan, L.; Bua, J.; Cont, G.; Demarini, S. Impact of Surgery for Neonatal Gastrointestinal Diseases on Weight and Fat Mass. J Pediatr 2015, 167, 568-571. [CrossRef]
- Pichler, J.; Simchowitz, V.; Macdonald, S.; Hill, S. Comparison of liver function with two new/mixed intravenous lipid emulsions in children with intestinal failure. Eur J Clin Nutr 2014, 68, 1161-1167. [CrossRef]
- Hoffmann, K.M.; Grabowski, M.; Rodl, S.; Deutschmann, A.; Schwantzer, G.; Sovinz, P.; Strenger, V.; Urban, C.; Muntean, W.; Hauer, A.C. Short-term intravenous fish-oil emulsions in pediatric oncologic patients--effect on liver parameters. Nutr Cancer 2014, 66, 1070-1076. [CrossRef]
- Wong, R.S.; Walker, K.; Halliday, R.; Trivedi, A. Influence of Soybean Oil or Non-Soybean Oil Based Lipid Emulsions on Parenteral Nutrition Associated Liver Disease in Late Preterm and Term Infants. International Journal of Child Health and Nutrition 2014, 3, 179-184. [CrossRef]
- Ariyawangso, U.; Puttilerpong, C.; Ratanachu-ek, S.; Anuntkosol, M. Short-term safety and efficacy of fish-oil emulsions on the prevention of parenteral nutrition-associated liver disease in surgical neonates: a randomized controlled trial. Thai Journal of Pharmaceutical Sciences 2014, 38.
- Bishay, M.; Pichler, J.; Horn, V.; MacDonald, S.; Ellmer, M.; Eaton, S.; Hill, S.; Pierro, A. Intestinal failure-associated liver disease in surgical infants requiring long-term parenteral nutrition. J Pediatr Surg 2012, 47, 359-362. [CrossRef]
- Muhammed, R.; Bremner, R.; Protheroe, S.; Johnson, T.; Holden, C.; Murphy, M.S. Resolution of parenteral nutrition-associated jaundice on changing from a soybean oil emulsion to a complex mixed-lipid emulsion. J Pediatr Gastroenterol Nutr 2012, 54, 797-802. [CrossRef]
- Anez-Bustillos, L.; Dao, D.T.; Fell, G.L.; Baker, M.A.; Gura, K.M.; Bistrian, B.R.; Puder, M. Redefining essential fatty acids in the era of novel intravenous lipid emulsions. Clin Nutr 2018, 37, 784-789. [CrossRef]
- WHO. Protein and amino acid requirements in human nutrition. WHO Technical Report Series 2007, 935.
- Stapleton, P.P.; Charles, R.P.; Redmond, H.P.; Bouchier-Hayes, D.J. Taurine and human nutrition. Clin Nutr 1997, 16, 103-108. [CrossRef]
- Chesney, R.W.; Helms, R.A.; Christensen, M.; Budreau, A.M.; Han, X.; Sturman, J.A. An updated view of the value of taurine in infant nutrition. Adv Pediatr 1998, 45, 179-200.
- Lourenco, R.; Camilo, M.E. Taurine: a conditionally essential amino acid in humans? An overview in health and disease. Nutr Hosp 2002, 17, 262-270.
- Lima, L.; Obregon, F.; Cubillos, S.; Fazzino, F.; Jaimes, I. Taurine as a micronutrient in development and regeneration of the central nervous system. Nutr Neurosci 2001, 4, 439-443. [CrossRef]
- Kumpf, V.J. Parenteral nutrition-associated liver disease in adult and pediatric patients. Nutr Clin Pract 2006, 21, 279-290. [CrossRef]
- Norsa, L.; Artru, S.; Lambe, C.; Talbotec, C.; Pigneur, B.; Ruemmele, F.; Colomb, V.; Capito, C.; Chardot, C.; Lacaille, F. Long term outcomes of intestinal rehabilitation in children with neonatal very short bowel syndrome: Parenteral nutrition or intestinal transplantation. Clin Nutr 2019, 38, 926-933. [CrossRef]
- Struijs, M.-C.; Schaible, T.; van Elburg, R.M.; Debauche, C.; te Beest, H.; Tibboel, D. Efficacy and safety of a parenteral amino acid solution containing alanyl-glutamine versus standard solution in infants: A first-in-man randomized double-blind trial. Clin Nutr 2013, 32, 331-337. [CrossRef]
- Ong, E.; Eaton, S.; Wade, A.; Horn, V.; Losty, P.; Curry, J.; Sugarman, I.; Klein, N.; Pierro, A. Randomized clinical trial of glutamine-supplemented versus standard parenteral nutrition in infants with surgical gastrointestinal disease. Br J Surg 2012, 99, 929-938. [CrossRef]
- Mohamad Ikram, I.; Quah, B.; Noraida, R.; Djokomuljanto, S.; Faris Irfan, C.; Van Rostenberghe, H. A randomised controlled trial of glutamine-enriched neonatal parenteral nutrition in Malaysia. Singapore Med J 2011, 52, 356-360.
- Albers, M.J.; Steyerberg, E.W.; Hazebroek, F.W.; Mourik, M.; Borsboom, G.J.; Rietveld, T.; Huijmans, J.G.; Tibboel, D. Glutamine Supplementation of Parenteral Nutrition Does Not Improve Intestinal Permeability, Nitrogen Balance, or Outcome in Newborns and Infants Undergoing Digestive-Tract Surgery: Results From a Double-Blind, Randomized, Controlled Trial. Ann Surg 2005, 241, 599-606. [CrossRef]
- Cruccetti, A.; Pierro, A.; Uronen, H.; Klein, N. Surgical infants on total parenteral nutrition have impaired cytokine responses to microbial challenge. J Pediatr Surg 2003, 38, 138-142. [CrossRef]
- Guimber, D.; Michaud, L.; Ategbo, S.; Turck, D.; Gottrand, F. Experience of parenteral nutrition for nutritional rescue in children with severe liver disease following failure of enteral nutrition. Pediatr Transplant 1999, 3, 139-145. [CrossRef]
- Thornton, L.; Griffin, E. Evaluation of a taurine containing amino acid solution in parenteral nutrition. Arch Dis Child 1991, 66, 21-25. [CrossRef]
- Puntis, J.; Ball, P.; Preece, M.; Green, A.; Brown, G.; Booth, I. Egg and breast milk based nitrogen sources compared. Arch Dis Child 1989, 64, 1472-1477. [CrossRef]
- Puntis, J.W.; Edwards, M.A.; Green, A.; Morgan, I.; Booth, I.W.; Ball, P.A. Hyperphenylalaninaemia in parenterally fed newborn babies. Lancet 1986, 2, 1105-1106. [CrossRef]
- Riskin, A.; Picaud, J.C.; Shamir, R. ESPGHAN/ESPEN/ESPR guidelines on pediatric parenteral nutrition: Standard versus individualized parenteral nutrition. Clin Nutr 2018, 37, 2409-2417. [CrossRef]
- Ferreira, M.; Guerra, P.; Ferreras, C.; Espinheira, M.D.C.; Trindade, E.; Dias, J.A. Could Commercial Formulations Replace Individualized Prescription in Pediatric Home Parenteral Nutrition? J Pediatr Gastroenterol Nutr 2021, 73, 548-554. [CrossRef]
- Meyer, R.; Timmermann, M.; Schulzke, S.; Kiss, C.; Sidler, M.; Furlano, R. Developing and implementing all-in-one standard paediatric parenteral nutrition. Nutrients 2013, 5, 2006-2018. [CrossRef]
- Hermanspann, T.; Schoberer, M.; Robel-Tillig, E.; Hartel, C.; Goelz, R.; Orlikowsky, T.; Eisert, A. Incidence and Severity of Prescribing Errors in Parenteral Nutrition for Pediatric Inpatients at a Neonatal and Pediatric Intensive Care Unit. Front Pediatr 2017, 5, 149. [CrossRef]
- Riskin, A.; Shiff, Y.; Shamir, R. Parenteral nutrition in neonatology--to standardize or individualize? Isr Med Assoc J 2006, 8, 641-645.
- Mena, K.D.R.; Espitia, O.L.P.; Vergara, J.A.D. Management of Ready-to-Use Parenteral Nutrition in Newborns: Systematic Review. JPEN J Parenter Enteral Nutr 2018, 42, 1123-1132. [CrossRef]
- Simmer, K.; Rakshasbhuvankar, A.; Deshpande, G. Standardised parenteral nutrition. Nutrients 2013, 5, 1058-1070. [CrossRef]
- Adamkin, D.H.; Radmacher, P.G. Current trends and future challenges in neonatal parenteral nutrition. J Neonatal Perinatal Med 2014, 7, 157-164. [CrossRef]
- Lapillonne, A.; Berleur, M.P.; Brasseur, Y.; Calvez, S. Safety of parenteral nutrition in newborns: Results from a nationwide prospective cohort study. Clin Nutr 2018, 37, 624-629. [CrossRef]
- Kumpf, V.J. Challenges and Obstacles of Long-Term Home Parenteral Nutrition. Nutr Clin Pract 2019, 34, 196-203. [CrossRef]
- Holcombe, B.; Mattox, T.W.; Plogsted, S. Drug shortages: effect on parenteral nutrition therapy. Nutr Clin Pract 2018, 33, 53-61. [CrossRef]
- Hill, S.; Ksiazyk, J.; Prell, C.; Tabbers, M. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Home parenteral nutrition. Clin Nutr 2018, 37, 2401-2408. [CrossRef]
- Neelis, E.; de Koning, B.; van Winckel, M.; Tabbers, M.; Hill, S.; Hulst, J. Wide variation in organisation and clinical practice of paediatric intestinal failure teams: an international survey. Clin Nutr 2018, 37, 2271-2279. [CrossRef]
Figure 1.
Fatty Acid Pattern of Lipid Emulsions vs. Human Umbilical Cord Blood and Human Breast Milk. Compiled from * Agostoni 2011 [74], ** Oliveira et al. 2012 [73], *** Koletzko et al 2016 [75] § Goulet et al. 2010 [47], $ Koletzko et al. 2005 [76].
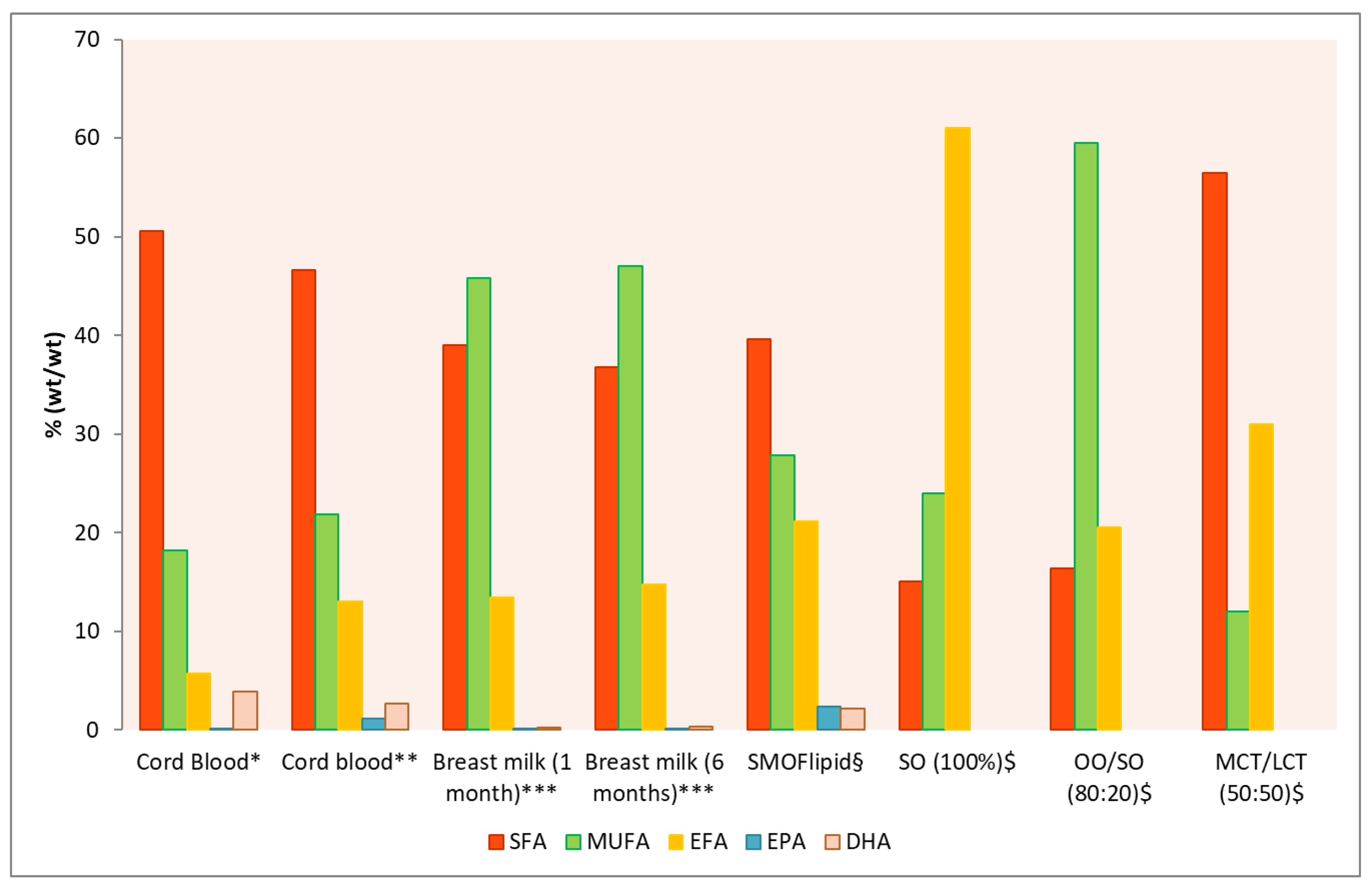
Figure 2.
Amino acid (AA) supply to infants with human milk* or Vaminolact. * derived from WHO 2007 [109] and Stapleton 1997 [110].
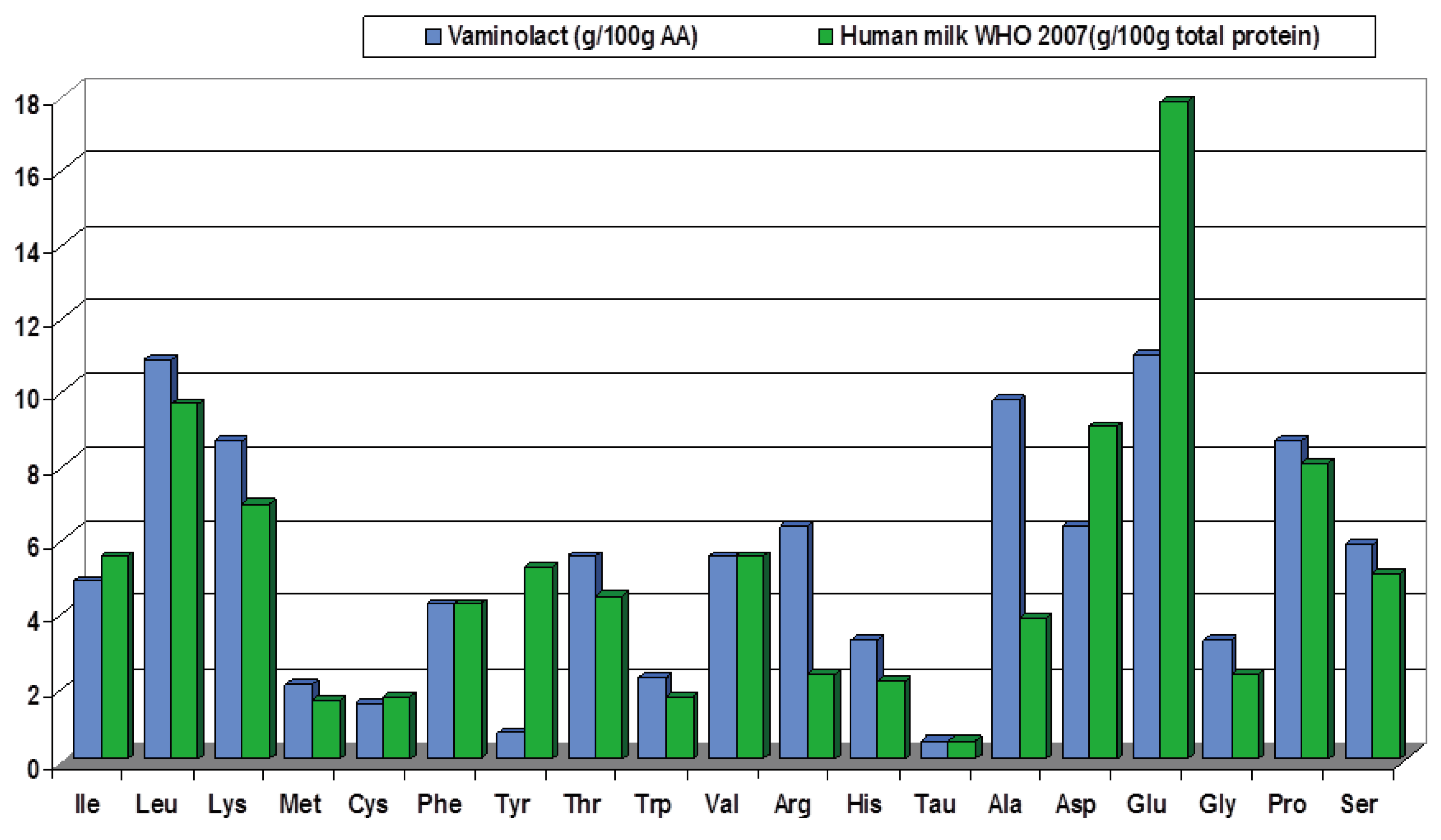

Table 1.
Parenteral nutrition with SMOFlipid in newborn infants, infants/toddlers, children, and adolescents.
Table 1.
Parenteral nutrition with SMOFlipid in newborn infants, infants/toddlers, children, and adolescents.
| Study | Design Number of patients (N) |
Patients Age at inclusion |
Intervention | Control | PN Lipid dose (g/kg BW/day) |
In line with ESPGHAN | PN Duration | Main outcomes and conclusions |
|---|---|---|---|---|---|---|---|---|
| Navaratnarajah et al. 2022 [82] | Retrospective chart review N=160 |
Hospitalized infants/toddlers on prolonged PN < 1 year |
SMOF (n=88) | SO (n=72) |
SMOF: 2.5 [1.7-2.8] SO 2.5 [1.9-2.8] |
☑ | ≥28 days | SMOF vs. SO: Cholestasis/liver function Lower incidence of cholestasis (CBil >3.0 µmol/L): 4.5% vs. 20% during the study period Lower log-transformed CBil at the end of the ILE administration (p<0.02) Growth No significant differences (NSD) |
| Goulet et al. 2022 [15] | Prospective cross-sectional N=70 |
Children on HPN SMOF: 5.9 [4.1–8.4] years Weaned: 6.9 [4.0–8.7] years |
SMOF (n=46) 25 children remained PN dependent and were assessed a 2° time 2.4 years later (SMOF 2, n=25). |
Weaned off PN (n=24) |
SMOF: 1.9 [1.4-2.0] |
☑ | 2.4 ± 0.9 years | SMOF vs. weaned: Growth/nutritional status NSD Cholestasis/liver function Higher CBil (p<0.0001) and liver enzymes (all p<0.01), but close to the normal FA profile Higher proportions of EPA and DHA but lower proportions of MA and ARA incorporated in RBC (all p<0.0001) Indices of EFAD No significant difference in Holman index |
| Goulet et al. 2021 [9] | Retrospective cross-sectional Multicenter N=268 in 2014 N=385 in 2019 |
Children on HPN Median age per year over the 5 year observation period: 62.5 – 84.1 months |
HPN with different types of ILEs (OO/SO, SO, SMOF, MCT/SO or pure FO in case of cholestasis) | - | 1.02 -1.5 | ☑ | 5 years | 2014 vs. 2019: The use of a SMOF increased from 67.4% to 88.3% (p < 0.001) Blood stream infections CRBSIs dropped from 1.04 CRSBIs per 1000 days HPN to 0.61 (p<0.001) Cholestasis/liver function Prevalence of cholestasis (CBil ≥ 20 μmol/l) low and stable between 4.1 and 5.9% during the study period. |
| Rumore et al. 2021 [83] | Retrospective N=92 |
Infants/toddlers and children on HPN Range 3-223 months, (median 11 months) |
SMOF (n=79) Switch to SMOF (n=13) |
Non-SMOF (SO or OO/SO) (n=19) | n.a. To be deleted ??? |
- | n.a. | SMOF vs. non-SMOF Clinical and biological outcome Lower overall transplantation rate (7.6% vs. 21.9%; p<0.05) Lower mortality rate (14.1% vs. 21.9% n.s.) Higher vitamin E level and vitamin E:lipid ratio, both p<0.001 Higher vitamin D level (p<0.001) |
| Wassef et al. 2021 [84] | Prospective observational N=16 |
Infants/toddlers, children and adolescents with IF | SMOF (n=16) | - | Mean dose at initiation: 1.5 (range 1-2.5) Mean dose at study end: 1.6 (range 1-2.5) |
☑ | 16.4 [4-33] months | End of study vs. baseline: Cholestasis/liver function Decrease in mean TBil by 67.08% (p<0.05) normalization of DBil in all patients No significant changes in AST or ALT Significant change in mean TBil after 4-5 months (p<0.01; stable TBil at around 0.6 mg/dL thereafter) No new cases of IFALD EFAD No EFAD |
| Daniel et al. 2021 [85] | Retrospective N=101 |
Hospitalized newborn infants (preterm/term), infants/toddlers, children and adolescents SMOF: 300 [0- 1095] days SO: 31 [0-795] days |
SMOF (n=60) | SO (n=41) | Initiated: 0.5-1.0 Increased up to 2.0-3.0 |
☑ | SMOF: 28.5 [20.75, 44] days SO: 32 [23, 55] days |
SMOF vs. SO Cholestasis/liver function Significantly lower incidence of IFALD (12% vs. 32%; p<0.05) No significant difference ay onset of IFALD Subgroup of patients with IFALD (n=20), over 6 months: Significantly lower bilirubin (p<0.05) |
| Lezo et al. 2020 [86] | Prospective observational Multicenter N=38 |
Infants/toddlers, children and adolescents on HPN SMOF; 3.3 [0.9–16.9] years OO/SO: 8.4 [1.6–18.6] years |
SMOF (n=23) | OO/SO (n=15) | SMOF: 1.3 [0.5-2.5] OO/SO: 1.3 [0.5-1.7] |
☑ | SMOF: 22.2 [9.8–202] months OO/SO: 21.1 [7.0–104.0] months |
FA pattern SMOF vs. OO/SO and vs. healthy reference range: - Higher EPA and DHA and lower MA in plasma and RBC membranes (all p<0.01) - Lower ARA in plasma (both both is strange ??? p<0.01) With both ILEs vs. healthy reference range: - Lower ARA in RBC membranes (both p<0.01); n.s. between ILEs Indices of EFAD With both ILEs vs. healthy reference range: - NoNSD in Holman index; no EFAD with both ILEs Cholestasis/liver function Absence of liver fibrosis with both ILEs Growth/nutritional status SMOF vs. OO/SO: - Higher proportion of patients malnourished according to BMI or WFL z-scores (≤2) (5/23) vs. (0/15) (p<0.05) - NSD between groups for Median Z-score of weight, height or BMI for age were |
| Nagelkerke et al. 2020 [87] | Prospective cross-sectional N=32 |
Infants/toddlers, children and adolescents on HPN Median 8.0 (range 0.3-17.8) years |
SMOF (n=23) or OO/SO (n=6) |
- | Median 1.0 (range 0-2.6) | ☑ | Median 45 months |
Cholestasis/liver function Transient elastography (TE), ASAT-to platelet-ratio-index (APRI) and enhanced liver fibrosis (ELF) score showed a varying, but substantial proportion of subjects with fibrosis in the cohort: - Significant fibrosis (TE and ELF): n=6 and 10, respectively - Fibrosis (APRI): n=12 - Moderate fibrosis (ELF): n=17 |
| Ho 2020 [88] | Retrospective N=20 |
Children on HPN Median 6.2 years |
SMOF | Pre-SMOF (SO or SO/FO combination) |
2.0 [1.6-2.0] | ☑ | 1.5 years | From SMOF initiation to 1.5 years post SMOF initiation: FA pattern Increases in ARA, LA, DHA and ALA, all p<0.01 Cholestasis/liver function Decreases in ALT and GGT; both p<0.005 Growth/nutritional status Slight increases in BMI z-score; n.s. EFAD NSD in MA or Homan ratio |
| Huff 2020 [89] | Retrospective N=47 |
Newborn infants, infants/toddlers and children with IF and cholestasis (n=42) 45 [4–1623] days |
SMOF | - | Median 2.1 (range 0.8-3.0) | ☑ | Median 53 days (range 1-432 days) |
Cholestasis/liver function 16/42 cholestatic patients (38%) had resolution with SMOF, 7/42 (17%) improved, 19/42 (45%) showed no response Patients with resolution of cholestasis were older at start of SMOF therapy (p=0.010), treated with SMOF longer (p=0.001), and had lower DBil at SMOF initiation (p=0.035) EFAD Biochemical signs of EFAD (T:T ratio range 0.05-0.151) were observed in 15/28 patients with measurements available; EFAD was mild in all patients; without clinical symptoms of EFAD |
| Hanindita 2019 [90], 2020 [91] | RCT N=14 |
Newborn infants post surgery SMOF: 14.1±17.1 days MCT/SO: 14.0±12.1 days |
SMOF (n not reported) | SO/MCT (n not reported) | 1.0-4.0 | ☑ | SMOF: 29.0±34.8 days MCT/SO: 30.0±20.3 (18.2±15.7 days reported in the 2019 study) |
SMOF vs. SO/MCT group: Inflammation Decrease with SMOF vs. increase of serum IL-6 from baseline to POD 3 Significant differences in IL-6 levels before surgery (p=0.048), on POD 3 (p=0.013), and in changes within 3 days (p=0.003) NSD in TNF-α levels between groups |
| Danko 2019 [92] | Retrospective N=40 |
Children on long-term PN Median 38 months (range 1.5–200) |
SMOF + FO (Omegaven) To be deleted because of this combination that does not fit with our aim |
- | SMOF: median 1.0 (range 0.5-2.0) Omegaven dose not reported |
☑ | Median 149 days (range 28-418) | End of treatment vs baseline: Cholestasis/liver function Significant reduction in TBil, CBil, ALT, AST, and GGT in the total group and in cholestatic patients (n=13; all p<0.05) 11/40 patients had increasing or unchanged bilirubin levels (nonresponders), but no patient with initial CBil <34.2 µmol/L (<2 mg/dL) became cholestatic |
| Casson et al. 2019 [93] | Retrospective Two centers N=44 |
Newborn infants and infants/toddlers during the first 8 weeks of intestinal rehabilitation SMOF: mean 7 (range 4–50) days SO: mean 8 (range 4–47) days |
SMOF (n=21) | SO (n=23) | SMOF: week 1: 3.0 [2.0-3.0] week 4: 3.0 [1.3-3.0] week 8: 2.0 [1.5-3.0] SO: week 1: 2.0 [1.5-3.0] week 4: 2.0 [1.5-3.0] week 8: 1.5 [1.0-3.4] |
☑ | > 8 weeks | SMOF vs. SO: Cholestasis/liver function: During the 8 weeks observation period, cholestasis occurred in 76% vs. 91% of infants (p=0.18) CBil levels normalized more quickly (p=0.04) Subset of infants without any EN tolerance: Lower incidence of cholestasis (78% vs. 92%, p=0.057) |
| Belza 2019 [94] | Retrospective N=37 |
Infants/toddlers with IF < 12 months |
SMOF (n=17) | SO (n=20) | 2.0-3.0 | ☑ | SMOF: 421 [203-822] days SO: 213 [104-364] days |
SMOF vs. SO: Cholestasis/liver function Lower likelihood to reach a serum CBil of 34 µmol/L or 50 µmol/L; both p≤0.05) With SMOF: no need for Omegaven to resolve IFALD (0% vs. 30%, p=0.014) Lower median CBil 3 months after PN initiation (p=0.023) Growth /nutritional status Improved weight z-scores at 3 and 6 months (both p<0.05) Anthropometrics (weight, height, head circumference) remained within the normal range in both groups |
| Jiang 2019 [95] | RCT N=160 |
Newborn infants after GI surgery Mean 4-5 days |
SMOF (n=74) | SO/MCT (n=86) | 1.0-3.0 | ☑ | >2 weeks (22/24 patients >4 weeks) | SMOF vs. SO/MCT: Cholestasis/liver function NSD in liver enzymes and DBil at end of weeks 1 and 2 Infants who received lipids for >4 weeks: -Lower ALT, AST and DBil levels at end of week 4 (all p<0.05) Growth/nutritional status NSD in weight gain or nutrition indices at end of weeks 2 and 4 months |
| Lam 2018 [96] | Retrospective N=40 |
Hospitalized newborn infants and infants/toddlers/children SMOF: 0.6 (0.1–28) months SO: 0.8 (0.1–33) months |
SMOF (n=20) | SO (n=20) | SMOF: 2.2 (1.8-2.5] SO: 2.1 [1.6-2.3] |
☑ | SMOF: 9 [5-13] weeks SO: 6 [4-13] weeks |
SMOF vs. SO: Cholestasis/liver function Significantly lower trajectory of CBil (p<0.001) NSDin AST, ALT, or ALP trajectories (sensitivity analysis excluding outliers showed lower AST and ALT trajectories for the SMOF group (both p<0.001) Growth/nutritional status NSD between groups |
| Olszewska 2018 [97] | Prospective observational N=17 |
Infants, children and adolescents with ultra-short bowel syndrome Range 0.8-14.2 years |
SMOF (n=10) or SMOF/FO (Omegaven) (n=5) or SO/MCT (n=2) |
- | n.a. | - | median duration of PN 6.6 years (range 0.8-14.2 years) | During the 1 year observation period: Growth/nutritional status Body mass deficits were found in the cohort with a median standard deviation score (SDS) of -1.2 for body mass according to chronological age, -1.72 according to height and -0.59 according to height for age Cholestasis/liver function None of the patients had elevated CBil levels above 34.2 µmol/L |
| Pereira-da-Silva 2018 [98] | RCT N=49 |
Newborn infants (term/preterm) undergoing major surgery <48 hours |
SMOF (n=22) | SO/MCT (n=27) | Median cumulative dose: SMOF: 14.7 g/kg SO/MCT: 12.5 g/kg Such high doses should be verified | ☑ | SMOF: median 16 days SO/MCT: median 18 days |
SMOF vs. SO/MCT: Cholestasis/liver function Similar cumulative incidence rates of CBil >1 mg/dL or >20% of TBil between groups Triglycerides Cumulative incidence of hypertriglyceridemia >250 mg/dL was lower (p=0.0024) Mean serum TG increase was lower (p=0.013) |
| Diamond 2017 [99] | RCT Multicenter N=24 |
Infants/toddlers with early IFALD SMOF: mean 6.5 weeks (range 4.3-8.7) SO: mean 5.3 weeks (range 3.5-7.2) |
SMOF (n=11) | SO (n=13) | 2.0-3.0 | ☑ | SMOF: 8 [5.5-10.5] weeks SO: 8 [5.7-10.7] weeks |
SMOF vs. SO: Cholestasis/liver function Lower serum CBil at trial completion (primary endpoint, p=0.001) Higher likeliness to have a decrease in serum CBil to 0 µmol/L over the entire study period (p = 0.006) Less patients with serum CBil >50 µmol/L at primary endpoint (p = 0.04) Higher GGT at trial completion (p=0.04) |
| Pichler 2015 [100] | Controlled trial non-randomized N=67 |
Newborn infants (preterm/term), infants/toddlers, children and adolescents with IF 0.7 [0.01-15.1] years |
Mixed ILE: SMOF or OO/SO (n=27) | SO or SO/MCT (n=40) | n.a. | - | 2-3 times per week Duration n.a. |
Mixed ILE vs. SO: Cholestasis/liver function Lower frequency of sludge and/or gallstones (p=0.05). Lower incidence of liver echogenicity (p=0.003). Overall, in 7 (10%) children, sludge and/or gallstones resolved spontaneously without further intervention. Five of the 7 children were receiving mixed ILE. |
| De Cunto 2015 [101] | Retrospective N=42 |
Newborn infants (preterm/term) undergoing GI surgery 1-82 days Matched controls (n=21, thereof 5 receiving PN due to prematurity) |
SMOF (surgical group, n=21) | 0.5-3.0 | ☑ | Mean 40 days | Surgical infants vs. matched controls: Growth/nutritional status Postsurgical infants were shorter (p=0.001), lighter (p<0.001), and had lower fat mass content (p<0.0001) than their peers at similar corrected age (43 [4] weeks). Cholestasis/liver function Nine infants in the surgical group and 1 in the control group had PN-associated cholestasis. |
|
| Pichler 2014 [102] | Retrospective N=177 |
Hospitalized infants/toddlers, children and adolescents changing to or starting PN with a FO-ILE Median 0.6 (range 0-16) years |
SMOF (n=71) | SO/MCT (n=56) | SMOF: 2.3±0.8 SO/OO/FO: 2.2±0.9 |
☑ | SMOF: median 41 (range 3-311) days SO/OO/FO: median 30 (range 3-436) days SO: median 73 (range 19-154) days |
Cholestasis/liver function With SMOF (baseline vs. end of treatment): - Reduced ALT (p=0.006), ALP (p=0.008) and GGT (p=0.01) - Hyperbilirubinaemia incidence decreased from 34% to 24% (p<0.05). SMOF vs. SO/MCT: - Lower ALT at end of treatment (p=0.01) Growth/nutritional status No adverse effects were detected and significant weight gain was achieved with both FO-ILEs (p<0.05) |
| Hoffmann 2014 [103] | Retrospective N=30 |
Children with haemato-oncologic disease during CT 10.69±7.11 years (mean±SD) |
SMOF (n=15) | SO (n=15) | SMOF: 0.9 SO: 1.0 |
☑ | > 14 days |
Cholestasis/liver function No significant changes vs. baseline at day 7 and day 14 in TBil, GGT, AST, ALT, and AP in the SMOF group GGT increased in the SO group (p<0.05) No patient in either group developed cholestasis Other Decrease in lactate dehydrogenase levels (marker of cell damage) with SMOF vs increase in the SO group (p=0.016) |
| Wong 2014 [104] | Retrospective N=208 | Newborn infants (preterm/term) and infants Age not reported |
Mixed ILEs: SMOF or SO/OO (n=54) | SO (n=154) | n.a. | - | Mixed ILEs: mean 19 days SO: mean 21 days |
Cholestasis/liver function Mixed ILEs vs. SO: Lower prevalence of IFALD (17% vs. 21%; p=0.315) |
| Ariyawangso 2014 [105] | RCT N=42 |
Surgical newborn infants (preterm/term) Age not reported |
SMOF (n=21) | SO (n=21) | SMOF: 2.6 ± 0.3 SO: 2.6 ± 0.2 |
☑ | SMOF: 22.5 ± 8.5 days SO: 20.9 ± 5.5 days |
SMOF vs. SO: Cholestasis/liver function Lower plasma TBil (p<0.001)] and DBil (p<0.001)] Increase in TBil and DBil in the control group(p=0.02 and p<0.001) Decrease in TBil (p<0.001) and unchanged DBil with SMOF Growth/nutritional status NSD at day 22 Other Laboratory safety parameters (liver enzymes, lipid profiles, renal function and hematological parameters): n.s. between groups |
| Bishay 2012 [106] | Retrospective N=87 | Infants post surgery with and without IFALD Non-IFALD: mean 19 (range: 1-347) days IFALD: mean 45 (range: 4-270) days |
SMOF or SO/OO/FO |
- | n.a. | - | Non-IFALD: mean 48 (range 28-310) days IFALD: mean 77 (range 30-276) days |
Cholestasis/liver function IFALD occurred in 33% (n=29) whatever they received SMO or SO/OO/FO IFALD was associated with Ionger PN duration (p=0.002) female sex (overall [p=0.04] and trend for increasing severity [p=0.006]) Other 61 children receiving long-term PN (70%) have achieved enteral autonomy, whereas 12 (14%) required HPN |
| Muhammed 2012 [107] | Retrospective N=17 |
Infants/toddlers and children with PN-associated jaundice SMOF: 12-164 weeks SO: 8-64 weeks |
SMOF (n=8) | SO (n=9) | SMOF: 0.6–3.5 SO: 2.5-3.5 |
☑ | SMOF: 12-148 weeks SO: 8-64 weeks |
Cholestasis/liver function After 6 months, 5 of 8 children in the SMOF and 2 of 9 children in the SO group had total resolution of jaundice Median TBil decreased in the SMOF group and increased in the Intralipid group (p=0.02) |
| Goulet 2010 [47] | RCT N=28 |
Infants/toddlers and children on HPN SMOF: 30.3±23.9 months SO: 38.8 ± 35.5 months |
SMOF (n=15) | SO (n=13) | SMOF: 1.4 ± 0.5 SO: 1.4 ± 0.5 |
☑ | SMOF: 27.3±0.6 days SO: 27.5±0.5 days |
Baseline vs. end of study: Cholestasis/liver function TBil values were significantly decreased with SMOF (p<0.01) FA pattern In RBC and in plasma phospholipids, EPA and DHA were significantly increased in the SMOF group N3-/n6-FA ratio in plasma and RBC was significantly elevated with SMOF compared to SO (both p<0.01) Other Plasma α-tocopherol levels increased significantly more with SMOF vs. SO (p<0.05). |
NSD: No significant difference; ALA: alpha-linolenic acid; ALT: alanine aminotransferase; AP: alkaline phosphatase; ARA: arachidonic acid; AST: aspartate aminotransferase; BMI: body mass index; CBil: conjugated bilirubin; CRP: C-reactive protein; DBil: direct bilirubin; DHA: docosahexaenoic acid; EFAD: essential fatty acid deficiency; EPA: eicosapentaenoic acid; FA: fatty acid; FO: fish oil; GGT: gamma-glutamyl transferase; GI: gastrointestinal; HPN: home parenteral nutrition; IF: intestinal failure; IFALD: intestinal failure associated liver disease; ILE: intravenous lipid emulsion; LA: linoleic acid; MA: mead acid; MCT: medium-chain triglycerides; n.a.: not available; OO: olive oil; PN: parenteral nutrition; POD: post-operative day; RBC: red blood cell; RCT: randomized controlled trial; SMOF: soybean oil/medium-chain triglycerides/olive oil/fish oil; SO: soybean oil; TBil: total bilirubin, TG: triglycerides; T:T: triene:tetraene; WFL: weight for length. Data are reported as median [IQR] unless otherwise indicated.
Table 2.
Supply of critical amino acids with Vaminolact calculated based on dosage recommendations for total amino acids according to ESPGHAN/ESPEN/ESPR guidelines [49].
Table 2.
Supply of critical amino acids with Vaminolact calculated based on dosage recommendations for total amino acids according to ESPGHAN/ESPEN/ESPR guidelines [49].
| Age group | Term newborn infants up to 1 month |
Infants/ Toddlers 1 month - 3 years |
Children and adolescents 3-18 years |
|---|---|---|---|
|
Recommended total amino acid dose range acc. to ESPGHAN (g/kg BW/day) |
1.5-3 | 1-2.5 | 1-2 |
| Cysteine/cysteine (mg/kg/day) | 23-46 | 15-38 | 15-31 |
| Tyrosine(mg/kg/day) | 11-23 | 8-19 | 8-15 |
| Taurine(mg/kg/day) | 7-14 | 5-14 | 5-9 |
| Arginine(mg/kg/day) | 94-188 | 63-157 | 63-126 |
| Phenylalanine(mg/kg/day) | 62-124 | 41-103 | 41-83 |
| Valine(mg/kg/day) | 83-165 | 55-138 | 55-110 |
| Isoleucine(mg/kg/day) | 71-142 | 47-119 | 47-95 |
Table 3.
Parenteral nutrition with Vaminolact in term newborn infants, infants/toddlers and children.
Table 3.
Parenteral nutrition with Vaminolact in term newborn infants, infants/toddlers and children.
| Study | Design Number of patients (N) |
Patients Age at inclusion |
Intervention | Control | Amino acid dose (g/kg BW/day) |
In line with ESPGHAN* | PN Duration | Main outcomes |
|---|---|---|---|---|---|---|---|---|
| Norsa et al. 2019 [115] | Retrospective Cross-sectional N=36 |
Infants/toddlers and children with neonatal short bowel syndrome Median 9 (3-73) months |
PN with Vaminolact or Primene (n=16) Remained on long-term PN (n=16) or Received intestinal transplantation after 2.5 -9 years (n=20) |
- | n.a. | - | Follow-up: median 17 (9-20) years |
Clinical outcomes 16 children remained on long-term PN - 6 were weaned off PN after a mean of 8 years - All children were alive at a mean age of 16 years (9-20) 20 children underwent intestinal transplantation and outcome - 8 died 29 months (0-127) - 12 were weaned off PN 73 days (13-330) after transplantation. Growth/nutritional status At latest follow-up NSD in Z-score for height, weight and BMI in alive patients between both groups |
| Abi Nader et al. 2017 [14] | Retrospective N=17 |
Infants/toddlers with severe malnutrition treated with PN for IF 4.5±2.2 (range 2–9) months |
PN with Vaminolact or Primene | - | 2.9±0.3 | ☑ | 1.9±0.4 years |
Growth/nutritional status Weight gain after 28 days of PN was 110 ± 5% of optimal weight gain for age The mean NPEI from PN was 104.3±8.0 kcal/kg/d The mean ratio of NPEI over REE was 2.1±0.2 |
| Abi Nader et al. 2016 [13] | Retrospective N=251 |
Infants/toddlers on HPN Age 8.4±3.6 months |
HPN with Vaminolact or Primene or Vintene | - | n.a. | - | Mean duration: 1.9±0.4 years |
Clinical outcomes 19 children with primary digestive diseases underwent intestinal transplantation, thereof 3 children died because of uncontrollable acute rejection 24 children died while receiving HPN (10%) 91 children with SBS were weaned off HPN at a mean age of 2.9±0.6 years The major complications of HPN were CRBSIs: 1.7/1000 days of PN and cholestasis (51 children; 20% of cohort) Growth/nutritional status Patients weaned off HPN: - NSD in weight for-age and height-for-age z scores at weaning off HPN and follow-up visits (P = 0.23 and 0.16, respectively) Children with SBS still receiving HPN at the end of the study period (n = 45): - Weight for-age and height-for-age z scores were not significantly different from those of weaned patients - The level of PN dependency assessed by the NPEI:REE ratio was 1.31±0.2 |
| Struijs et al. 2013 [116] | RCT N=23 |
Surgical newborn infants Gln-AA:1 [1-3] days Standard-AA: 2 [1-3] days |
GLN-AA: Pediatric AA solution with glycyl-tyrosine, Ala-Gln and acetyl-cysteine, higher in arginine and taurine vs. control (n=17) | Standard-AA: Vaminolact (n=6) | GLN-AA: 2.1±0.5 Standard-AA: 2.1±0.2 Requirements based on ESPGHAN 2005 |
☑ | GLN-AA: 7.5±3.1 days Standard-AA: 8.9±2.1 days |
Gln-AA vs. standard AA: Growth/nutritional status NSD for body weight, head circumference and pre-albumin AA profiles Plasma AA-profiles were closer to the normal ranges Clinical laboratory and safety No significant differences were found between groups for hematological and biochemical laboratory values, adverse events, and safety parameters |
| Ong et al. 2012 [117] | RCT Multicenter N=164 |
Surgical newborn infants and infants/toddlers Ala-Gln group: 5 (1–47) days Control: 5 (1-51) days |
PN + Ala-Gln (n=82) AA solution not specified |
Standard PN (n=82) Vaminolact in 12 centers and Primene in 2 centers |
1.5 | ☑ | Control:15.0 (13.3–16.8) days Ala-Gln: 19.0 (14.6–23.4) days |
PN with Ala-Gln vs. standard PN: Clinical outcomes During exclusive PN: significantly decreased incidence of sepsis (p=0.005) No effect on the overall incidence of sepsis or septicaemia Growth/nutritional status NSD in weight centile change between groupsHead circumference centiles were maintained in each group Clinical laboratory and safety No side-effects were reported in either group No documented abnormal levels of serum ammonia Other NSD in time to full enteral feeding or time to first enteral feeding between groups |
| Ikram et al. 2011 [118] | RCT N=132 |
Newborn infants (preterm/term) requiring PN Age <72 hours |
PN + Ala-Gln (n=132) Prepared with Vaminolact |
Standard PN (n=138) Prepared with Vaminolact |
Ala-Gln 0.6 Vaminolact dose not reported |
- | n.a. | PN with Ala-Gln vs. standard PN: Clinical outcomes NSD for Clinical outcomes: (NEC, clinical sepsis and culture-proven sepsis, duration of ventilation, duration of NICU stay) Other NSD in the median time to reach full enteral nutrition (6 days |
| Goulet et al. 2010 [47] | RCT N=28 |
Infants/toddlers and children on HPN SMOF: 30.3±23.9 months SO: 38.8 ± 35.5 |
SMOF (n=15) Vaminolact for children <3 years (n=8) |
SO (n=13) Vaminolact for children <3 years (n=7) |
1.8 | ☑ | SMOF: 27.3±0.6 days SO: 27.5±0.5 days |
Clinical laboratory and safety Treatment groups were comparable with respect to clinical indices, vital signs, biological safety parameters, including BUN, glucose, creatinine, and plasma electrolytes and growth parameters |
| Albers et al. 2005 [119] | RCT N=80 |
Newborn infants (preterm/term) and infants/toddlers Standard PN: 14.0 (2.3–54.0) days Gln-PN: 8.0 (2.8–94.0) days |
Gln-PN (n=41) AA solution not specified Article to be deleted ?? |
Standard PN (n=31) 2CB with Vaminolact |
1.5-2.5 | ☑ | n.a. | Gln-AA vs. standard AA: Protein metabolism No significant differences in nitrogen excretion and 3MH-creatinine excretion Serum ammonia levels were higher at study end (p=0.008) (not clinically relevant) Clinical outcomes No significant differences in mortality rate, length of stay in the ICU/hospital and in septic episodes Other No significant differences in intestinal permeability between groups |
| Cruccetti et al. 2003 [120] | Controlled study (not randomized) N=24 |
(a) newborn infants and infants/toddlers post surgery on PN Age: 101 (14-168) days (b) newborn infants and infants/toddlers on enteral formula 53.5 (13-172) days |
PN with Vaminolact (a) (n=9) | Formula (b) (n=8) Formula means that the two groups are not on PN To be deleted ??? |
0.5-3 | ☑/ ⊠ (for intakes <1.5) |
Mean 20 (10-106) days | PN with Vaminolact vs. formula group: Inflammation PS stimulation ex vivo: - Impaired cytokine response - Lower percentage of monocytes producing IL-6 and TNF-α (p<0.05) indicating reduced inflammatory response |
| Guimber et al. 1999 [121] | Retrospective N=7 |
Newborn infants, infants/toddlers and children with severe liver disease 2.5 years (4 days - 11.5 years) |
PN with Vaminolact or Primene | - | 1.7±0.5 | ☑/ ⊠ (for intakes <1.5) |
105 days (1 day-6 months) |
After PN vs. before PN: Growth/nutritional status Weight/height Z-score increased significantly (p<0.05) Height/age Z-score showed a trend to worsen (ns) Clinical laboratory and safety No significant differences in serum transaminases, serum albumin, serum ammonia, prothrombin time, and Factor V were noted |
| Thornton et al. 1991 [122] | Controlled study (not randomized) N=25 |
Critically ill newborn infants requiring PN 0-4 days |
PN with Vaminolact (n=15) | PN with Vamin glucose (n=10) Without taurine |
Vaminolact: 1.8±0.2 at day 1 2.3±0.2 from day 3 Vamin glucose: 1.9±0.1 at day 1 2.3±0.1 from day 3 |
☑ | Vaminolact: 12±5 days Vamin glucose: 10±3 days |
Vaminolact vs. Vamin glucose: AA profiles No serious abnormalities in AA concentrations in either group Taurine levels recovered more rapidly (n.s.) Phenylalanine levels were significantly lower at day 1 and day 3 Protein metabolism Nitrogen retention on day 1 was significantly higher Measurements n.a. on day 3 Growth With Vaminolact infants regained their birth weight faster than with Vamin glucose Clinical laboratory and safety Metabolic acidosis, which occurred in several subjects in each group, was not a serious problem Liver function tests remained satisfactory in both groups |
| Puntis et al. 1989 [123] | RCT N=14 |
Surgical newborn infants and infants/toddlers Vaminolact group: 36 days (11-84) Vamin 9 glucose group: 16 days (11-29) |
Vaminolact (n=7) | Vamin 9 glucose (n=7) Without taurine |
0.5-2.5 | ☑/⊠ (for intakes <1.5) | 6 days | Vaminolact vs. Vamin 9 glucose: AA profiles Lower PHE, TYR and total cystine/cysteine concentrations (p=0.0028, p=0.0004, p<0.05, respectively) Mean concentrations of all AA except THRE, LYS, HIST, and CYST closer to mean of the target range Growth and protein metabolism No significant difference in growth or nitrogen retention Clinical laboratory and safety No haematological or biochemical measurements changed significantly. Neither evidence of liver dysfunction |
AA: amino acid; Ala-Gln: L-alanyl-L-glutamine; BMI: body mass index; BUN: blood urea nitrogen; CRBSIs: catheter-related bloodstream infections; CT: computed tomography; GI: gastrointestinal; HPN: home parenteral nutrition; IF: intestinal failure; IFALD: intestinal failure associated liver disease; i.v.: intravenous; n.a.: not available; NPEI: non-protein energy intake; PN: parenteral nutrition; REE: resting energy expenditure; SBS: short bowel syndrome; SMOF: soybean oil/medium-chain triglycerides/olive oil/fish oil; SO: soybean oil; 2CB: 2-chamber bag. Data are reported as median (range) or median [IQR] or mean±SD unless otherwise indicated. * Amino acid dose supplied with Vaminolact in line with ESPGHAN recommendation [49].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



