
Submitted:
10 December 2023
Posted:
11 December 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Depression is one of the most severe sequelae of COVID-19, with major depressive disorder often characterized by disruption in white matter (WM) connectivity , stemming from changes in brain myelination. This study aimed to quantitatively assess brain myelination in clinically diagnosed post-COVID depression using recently proposed MRI method, macromolecular proton fraction (MPF) mapping. The study involved 63 recovered COVID-19 patients (52 mild, 11 moderate, 2 severe) at 13.5±10.0 months post-recovery, with matched controls without prior COVID-19 history (n=19). A post-COVID depression group (PCD, n=25) was identified based on psychiatric diagnosis, while a comparison group (noPCD, n=38) included participants with neurological COVID-19 complications, excluding clinical depression. Fast MPF mapping revealed extensive demyelination in PCD patients, particularly in juxtacortical WM (predominantly occipital lobe and medial surface), WM tracts (inferior fronto-occipital fasciculus (IFOF), posterior thalamic radiation, external capsule, sagittal stratum, tapetum), and grey matter (GM) structures (hippocampus, putamen, globus pallidus, and amygdala). The noPCD group also displayed notable demyelination but with less magnitude and propagation. Multiple regression analysis highlighted IFOF demyelination as the primary predictor of PCD presence and severity according to Hamilton scores. The number of post-COVID symptoms was a significant predictor of PCD presence while the number acute of symptoms was a significant predictor of PCD severity. This study, for the first time, reveals extensive demyelination in numerous WM and GM structures in PCD, outlining IFOF demyelination as a key biomarker.
Keywords:
COVID-19
; post-COVD
; long COVID
; depression
; demyelination
; white matter
; magnetic reso-nance imaging
; MRI
; macromolecular proton fraction
; MPF
; major depressive disorder
1. Introduction
An outbreak of a coronavirus in late 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection quickly became pandemic. Based on the World Health Organization statistics, there have been 771,820,937 confirmed cases of COVID-19 globally by November 2023, including 6,978,175 deaths (WHO Coronavirus (COVID-19) Dashboard). Many studies indicate the persistence of COVID-19 symptoms following recovery of the acute infection despite clearance of the virus from the body [1,2,3]. This phenomenon of the COVID-19 symptoms persistence more than 12 weeks following the infection has been characterized as post-COVID-19 syndrome or long-COVID-19 syndrome.
The long-term neurological and psychiatric complications of COVID-19 infection are being intensively studied. Complications of the COVID-19 include “brain fog”, fatigue, headache, sleep disorders, cognitive impairment, impaired sense of smell and taste, depression, anxiety, sleep disturbances, post-traumatic disorder and obsessive–compulsive symptoms [4,5,6,7,8,9,10,11,12,13,14].
Among the complications related to COVID-19, depression represents one of the major public health concerns; it decreases quality-of-life outcomes and may cause disability [15]. People who survived the acute phase of COVID-19 have been found to be at increased risk of mental health disorders, including being diagnosed with major depressive disorder (MDD) more often [16]. There are still too few studies to confidently judge whether PCD has any specific features compared to MDD. Some publications described differences in symptoms of PCD and MDD. Simonetti et al. [17] found high level of excitatory symptoms in post-COVID-19 syndrome, which is more likely corresponded to a mixed form of depression. In contrast, the comparative analysis of biomarkers suggested a similar etiopathogenesis and inflammatory hypothesis for post-COVID depression and MDD [18].
The etiology of MDD is commonly considered to be multifactorial [19]. The pathological mechanisms underlying post-COVID depressive symptoms are mainly related to the inflammation triggered by the peripheral immune-inflammatory response to the viral infection [18,20]. Several studies have also demonstrated neuroinflammation [21,22] in post-COVID syndrome. Neuroinflammation-associated reactivation of microglia and astrocytes is accompanied by the release of cytokines, pro-inflammatory and cytotoxic factors. This change in the extracellular environment negatively affects the functions of myelinating oligodendrocytes and oligodendrocyte precursors [23,24,25]. This leads to the hypothesis that neuroinflammation and subsequent demyelination may be a major cause of post-COVID depression.
Several studies of brain demyelination in post-COVID patients support this hypothesis. White matter damage was seen in 57% of 4342 hospitalized COVID-19 patients [26]. Reports indicated effect of COVID-19 infection in triggering demyelinating diseases, such as multiple sclerosis [27], acute disseminated encephalomyelitis [28], Guillain Barré syndrome [29,30]. The neurotoxic action of the virus is mediated by binding to angiotensin-converting enzyme-2 (ACE2) receptors or indirectly by inducing cytokine storm leading to disruption of the blood-brain barrier, immunological mediation, increasing blood coagulation and as a trigger for autoimmune-mediated demyelinating injuries in the CNS [31,32]. Recent MRI studies had shown a widespread alterations of white matter (WM) microstructure in the brain after COVID-19 and increase in radial diffusivity is indicative of demyelination and axonal damage [33,34,35,36,37,38,39].
Considering the similarities between MDD and PCD symptoms [40], another argument in favor of the significant role of demyelination in PCD is that MDD is often considered as a disorder of WM connectivity, which is caused by changes in brain myelination. Impaired WM integrity and demyelination in patients with MDD has been shown in several neuroimaging studies [41,42,43,44,45,46,47].
Despite the large number of publications. related to brain demyelination in post-COVID-19 patients, we have not encountered a single study that systematically assessed demyelination in patients with diagnosed clinical depression [36]. In this work, we applied the quantitative MRI method called macromolecular proton fraction (MPF) mapping to assess brain demyelination as a possible cause of post-COVID depression. MPF mapping is standing out among other MRI methods sensitive to myelin due its improved specificity to myelin, fewer physiological confounders based on diffusion, relaxation, and susceptibility [48,49,50]. MPF has strongest correlations with myelin content assessed with histology [51,52,53,54,55]. MPF values are independent of the magnetic field strength and provide solid method for myelin measurements across a variety of human and animal MRI platforms [56,57]. Finally, MPF maps can be obtained without modification of original manufacturers’ pulse sequences available on the standard clinical MRI scanners [58,59,60] including for assessing demyelination in mental disorders [58].
The current study aim was to quantify the degree of brain myelination in patients with clinically diagnosed post-COVID depression. We hypothesize that depression in post COVID-19 period is directly related to the decrease in brain myelination.
2. Materials and Methods
2.1. Study participants
Eighty seven participants were recruited by Mental Health Research Institute (Tomsk, Russia), Medica Diagnostic and Treatment Center (Tomsk, Russia), and Tomsk State University (Tomsk, Russia) between September 2022 and June 2023. The inclusion criteria were the following: age from 18 to 60 years, previous positive to COVID-19 PCR test and persistence of post-COVID complications (except for the control group), the absence of the history of traumatic brain injury, and the absence of any diagnosed neurologic or psychiatric condition prior to COVID-19. The exclusion criteria were: pregnancy, symptoms of acute infectious and somatic diseases, contraindications to MRI, inability to tolerate the MRI procedure, and self-withdrawal from the study. Written informed consent was obtained from all participants. The study design was approved by the local Ethical Committee of the Mental Health Research Institute (protocol №15/8.2022) and Bioethics Committee of Tomsk State University (№12/06.2022) following the guidelines of the Declaration of Helsinki
Patients with post-COVID complications were recruited by a neurologist at the Medica Diagnostic and Treatment Center and a psychiatrist at the Mental Health Research Institute. The control group was formed from employees and students of Tomsk State University, as well as their relatives and friends, who had not prior COVID-19 history. Patients and healthy volunteers were interviewed regarding eligibility for inclusion and exclusion criteria. Those who met these criteria signed an informed consent form and completed the questionnaire (Supplementary Materials). A few days later, participants underwent an MRI scanning. Data acquired from 5 participants who were newly diagnosed with brain pathologies based on MRI (cavernoma, glioma, vascular anomalies) were excluded from further analysis.
The severity of depressive symptoms was assessed using two scales, Hospital Anxiety and Depression Scale (HADS and Hamilton Depression Rating Scale (HDRS) [61]. The screening testing with HADS was carried out by a clinical psychologist. the HDRS testing was carried out by a qualified clinical psychiatrist during a clinical interview. After that, the participants who scored higher (>8) on the HADS were assessed by a psychiatrist. A group of patients with PCD was formed by a psychiatrist based on a structured clinical interview for the International Classification of Diseases (ICD-10) and baseline assessment report, including socio-demographic characteristics, medical history, questionnaire regarding COVID-19, clinical and psychometric examination. The severity of the current depressive episode was assessed before the start of drug therapy using the Hamilton Rating Scale for Depression (HDRS) [62,63]. The total score is interpreted as follows: no depression (0-7); mild depression (8-16); moderate depression (17-23); and severe depression (≥24).
Twenty five individuals with diagnosed clinical depression (moderate depressive episode - F32.1, severe depressive episode without psychotic symptoms – F32.2, recurrent depressive disorder (first diagnosed at the time of the study), current episode moderate – F33.1, according to ICD-10) were included in the post-COVID depression (PCD) group. The participants (n=38) with neurological complications of COVID-19 and without clinical depression were included in the comparison group (noPCD group). The control group (n=19) included healthy volunteers who were not COVID-19 positive and did not experience symptoms of COVID-19 from the start of the pandemic until the time of examination. The demographic characteristics of participants are shown in Table 1. The groups did not differ significantly in age, gender, and severity of COVID-19 (PCD and noPCD groups) according to Chi-square criteria.
2.3. Patient survey
All participants filled out a questionnaire regarding COVID-19 (Supplementary Materials). The questionnaire included questions about the number, severity, and date of illnesses, the PCR tests, vaccination, symptoms of the acute and post-COVID phases. As symptoms of the acute phase, patients were asked to note the presence or absence of anosmia, ageusia, fever, difficulty breathing, cough, muscle weakness, myalgia, headache, and dizziness. As symptoms of the post-COVID phase, patients were asked to note the presence or absence of headache, dizziness, brain fog, anosmia, ageusia, sensitivity, hypertensia/hypotensia, insomnia, fatigue, attention and memory deficit, myalgia, depression, panic attacks. Based on the results of the answers, the number of symptoms in the acute and post-COVID phases was calculated as the sum of symptoms (1 symptom – 1 point), for which positive answers were given for all diseases. This parameter has proven itself well as a predictor of post-COVID complications and for assessing the severity of post-COVID [64,65,66,67].
2.2. MRI data acquisition
All participants underwent MR imaging using 1.5T clinical scanner Magnetom Essenza (Siemens, Erlangen, Germany). The fast MPF mapping protocol [58] included three 3D spoiled gradient-echo pulse sequences with following acquisition parameters:
- − Magnetization-transfer-weighted: TR = 20 ms, echo time (TE) = 4.76 ms, flip angle (FA) = 8°, scan time 5 min 40 s;
- − T1-weighted: TR =16 ms, TE = 4.76 ms, FA =18°, scan time 4 min 32 s;
− Proton-density-weighted: TR= 16 ms, TE = 4.76 ms, FA= 3°, scan time 4 min 32 s.
- In addition, the following sequences were included in the protocol:
- − 3D FLAIR: TR = 5000 ms, TE = 390 ms, TI = 1800 ms;
- − 3D T1-weighted: TR = 16 ms, TE = 4.76 ms;
- − 3D T2-weighted: TR=3000ms, TE=335ms.
All scans were acquired in the sagittal plane with a voxel size of 1.25 × 1.25 × 1.25 mm3 (matrix 192 × 192 × 160, field of view 240 × 240 × 200 mm3), single signal averaging.
The total scanning time was about 35 minutes.
2.3. Image processing
MPF maps were reconstructed using the previously developed software in the C++ language (available at https://www.macromolecularmri.org/), which implements a single-point algorithm with a synthetic reference image [68,69].
Regional WM and GM segmentation was carried out using Advanced Normalization Tools (ANTs) [70,71] and Eve anatomical atlas [72] as described in [73]. T1 template image of Eve atlas was registered to individual MPF maps using antsRegistrationSyNQuick algorithm. Then the obtained deformation field was applied to Type-III Eve atlas segmentation [72] to register the template atlas labels to individual MPF maps ( Figure 1).
The measurements on MPF maps were performed for 118 GM and WM structures (including measurements in the right and left hemispheres) using ITK-snap software. The list of structures included:
- 1)
- juxtacortical (superficial) WM: superior parietal, superior, middle, and inferior frontal; precentral; postcentral; angular; pre-cuneus; cuneus; lingual; fusiform; superior, inferior, and middle occipital; superior, inferior, and middle temporal; lateral and middle fronto-orbital, supramarginal, rectus, cingulum (parts of cingulate gyrus and hippocampus);
- 2)
- WM pathways and fasciculi: corticospinal tract (CST); medial lemniscus; anterior limb, posterior limb, and retrolenticular part of internal capsule (IC); inferior, superior, and middle cerebellar peduncles (CP); cerebral peduncles; posterior thalamic radiation; anterior, superior, and posterior corona radiata (CR); fornix (FX) (stria terminalis, column and body); superior longitudinal (SL) fasciculus; superior (SFO) and inferior fronto-occipital (IFO) fasciculi; uncinate fasciculus; sagittal stratum; external capsule; pontine crossing tract; genu, body, and splenium of corpus callosum (CC); tapetum;
- 3)
- subcortical and allocortical GM structures: amygdala; hippocampus; entorhinal area; caudate nucleus; putamen; globus pallidus; thalamus;
- 4)
- brainstem structures: midbrain; pons; medulla.
The measurements for left and right hemispheres were averaged for the midbrain, pons, and medulla. Other brain structures were analyzed, taking into account whether they belonged to the left or right hemisphere.
2.5. Statistical analysis
Statistical analysis was performed using Statistica 10.0 software. Differences in MPF between the PCD, noPCD, and control groups for each brain structure were analyzed using the repeated measures analysis of variance (ANOVA) following by post-hoc Fisher LSD tests. One-way ANOVA was used to assess between-group differences in MPF of brainstem structures, results of psychological tests, and parameters associated with COVID-19, such as severity, time after recovery, number of acute and post-COVID symptoms. Post-hoc Fisher LSD tests were performed to clarify differences between groups.
Multiple regression analysis was performed to identify the best predictors of clinical post-COVID depression. First, for all patients of the PCD and noPCD groups for all studied brain structures, the percentage of change in MPF relative to the control group was calculated using the formula: (MPFind - MPFcontrol) / MPFcontrol x 100, where MPFind is the individual MPF value for each brain structure, MPFcontrol is the average MPF for the same structure in the control group. 115 variables were obtained corresponding to the percentage changes in the MPF of 59 structures of the left and right hemispheres. To avoid errors associated with multicollinearity of data for multiple regression analysis, the values of percentage changes in MPF were examined using factor analysis. As a result, principal component analysis allowed to identify 19 independent factors with eigenvalues >1 that explained 87.3% of the variance in total. To interpret the obtained factors, the percentage changes in the MPF of structures with factor loadings >0.7 were considered. The individual factor scores were used for multiple regression analyses. The multiple regression analysis was performed for the PCD and noPCD groups separately and for the total sample of post-COVID patients. HDRS score was used as the dependent variable. Independent variables included 19 variables of individual factor scores, age, gender, time since the acute phase of the first and last disease, the number of symptoms of the acute and post-COVID phase. The quality of regression models was assessed using multiple R correlation coefficient and R2 determination coefficient. The contribution and significance of predictors were assessed using beta-coefficient and p-value.
The differences were considered statistically significant at p<0.05.
3. Results
3.1. Acute and post-COVID symptoms
Group characteristics related to disease severity, time since first and last COVID-19, symptoms in the acute and post-COVID phases are presented in Table 2.
Patients of the PCD group with depression differed significantly from the noPCD group on several symptoms in both the acute phase of the disease and the post-COVID phase. In the acute phase, the PCD patients significantly more often than the noPCD noted ageusia, cough and headache, however, these differences were on the borderline of statistical significance. The total number of symptoms in the PCD group in the acute phase was also higher compared to the noPCD group. In the post-COVID phase, the differences between the groups were more essential. In the PCD group, more than half of the patients experienced anosmia and ageusia (64% and 56% correspondingly), while in the noPCD group only 29 and 21% reported these symptoms. Almost all patients in the PCD group reported sleep disturbances, fatigue, attention deficits, and depression, in contrast to the noPCD group, in which about half or fewer patients reported these symptoms. The average number of symptoms of patients in the PCD group is 1.7 times higher than in the noPCD group (Table 2).
3.2. Neuropsychological results
Table 3 demonstrates the results of neuropsychological testing of the study participants based on the medical diagnosis.
As expected, patients with clinical post-COVID depression showed significantly higher scores on the HDRS and HADS depression-related scales not only compared to controls, but also compared to the noPSD group. Hamilton scores in the PSD group were 4.6 times higher than in the control group and 3.0 times higher than in the noPSD group. The total HADS score for the PSD group was 2.7 times higher than in the control group and 2.3 times higher than in the noPSD group. The noPSD group is also showed significantly higher HDRS and HADS scores in comparison with controls. The noPSD group also showed significantly higher HDRS and HADS scores compared to the control group, but the differences between groups were smaller (1.5 and 1.2 times, respectively).
3.3. Brain demyelination in the patients with post-COVID depression
Brain images obtained from the study participants using multiple MRI techniques did not show visible differences between healthy control, PCD and no-PCD groups.. Example MPF maps, T1w, T2w and T2-FLAIR images of the participants of similar age from all groups are shown on Figure 2.
Quantitative MPF mapping was more sensitive in detecting differences in myelination of brain structures in study participants. Figure 3 demonstrates a significant decrease in myelination in large number of WM as well as GM brain structures and brainstem in the PSD group in comparison to the control and the noPSD group. The Figure 4 shows percentage differences in MPF for the PCD and noPCD groups relative to the level of controls. Specifically, a significant myelination decrease was observed in the juxtacortical regions of the WM(Figure 3a). The regions of the occipital and frontal lobes, as well as regions of medial brain surface were most affected. A 2-4% decrease in MPF was observed in all parts of the occipital lobe (inferior, superior, and middle occipital WM) of both hemispheres in the PSD group compared to controls. Inferior occipital WM also showed myelination decrease in the PSD group relative to the control group. For the frontal lobe, a significant decrease in MPF in the PСD group compared to controls was found for the superior frontal WM of both hemispheres, the lateral fronto-orbital WM of the left hemisphere, and the precentral WM of the right hemisphere. A significant myelination decrease in the PCD group compared to controls was found for the superior parietal WM of both hemispheres and the left superior temporal WM. In addition, a significant demyelination in the PCD group compared to controls was found for medial surface: right cuneus, left cingulate and fusiform WM. For the lateral fronto-orbital and cuneus WM, a decrease in MPF was found in the noPСD group, although of a smaller magnitude than in the PСD group (3.3% and 4.2%, respectively, Figure 4a). Among all juxtacortical structures the largest decrease in MPF (5%) was found for the fusiform WM (medial part of juxtacortical WM).
Subcortical WM pathways, including association, projection, and commissural, also revealed a significant decrease in myelination in the PCD group compared to the control group ( Figure 3b). The most prominent demyelination was observed for the association WM pathways. The inferior fronto-occipital fasciculus (IFOF) and sagittal stratum of both hemispheres, and left external capsule showed a significant decrease for the PCD group compared to controls. Additionally, the CST of both hemispheres and the right medial lemniscus showed a significant PMF decrease for the PCD group compared to the noPCD group. MPF decrease was also observed in the projection WM pathway, the posterior thalamic radiation of both hemispheres in the PCD patients compared to controls. Among the commissural WM pathways only left tapetum showed a significant decrease compared to controls. Among all WM pathways, the greatest MPF reduction was observed for IFOF (3%, Figure 4b), association WM pathway. No significant differences in myelination was observed in WM pathways between the noPCD comparison group and controls.
Decrease in myelination was also observed in the allocortex and deep GM structures of the PSD cohort (Figure 3c) in comparison to controls and noPSD group. The MPF decrease was observed in the hippocampus and putamen of both hemispheres, as well as in the amygdala and globus pallidus of the left hemisphere. The largest MPF differences of 3% and more were found in the amygdala and hippocampus, which are part of the allocortex (Figure 4c).
A few brain structures of the PCD cohort patients exhibited differences in MPF with both noPCD and control. Specific structures are the putamen, IFOF of both hemispheres, the right hippocampus and superior occipital WM. For the CST of both hemispheres and the left medial lemniscus, a decrease in MPF was observed for the PCD group compared to the noPCD group with no significant differences with control.
Brainstem structures did not reveal any significant differences between groups ( Figure 3d).
Figure 5 was built based on the Eve anatomical atlas, which was used for segmentation, and indicates the regions for which significant differences in MPF were obtained. It shows the spatial differences for each ROI between groups, shown in detail in Figure 3. The significant (p<0.05) or near significant (p<0.1) differences in myelination are shown between groups at the levels of superior juxtacortical WM, basal ganglia, and brainstem of axial views (Figure 5a) and sagittal views of the left (Figure 5b) and right (Figure 5c) hemispheres. Extensive demyelination was detected in PCD patients compared to controls. The reduction in myelination was less extensive in the noPCD group compared to controls. A significant decrease in MPF was observed in a large number of GM and WM brain structures in the PCD group compared to noPCD and controls. A significant or nearly significant decrease in myelination was observed only in brainstem structures of the PCD group compared to noPCD, in the absence of differences with controls.
3.4. Specifiсity of demyelination in the patients with post-COVID depression
Multiple regression analysis was used to identify brain structures where changes in myelination are closely related to manifestation of clinical post-COVID depression. A factor analysis was applied to exclude multicollinearity of independent variables – potential predictors of multiple regression. As a result, 19 factors were identified that explained 87% of the MPF variability in the post-COVID patients (Table 4). The factors that could be uniquely linked to the specific brain structures were examined further. The identified factors did not correlate with each other, which confirmed their unique contribution to the data variance.
The 19 factors associated with the percentage change of MPF, along with age, gender, disease severity, time since recovery, and the number of symptoms in the acute and long phases, were included in multiple regression analyzes as potential predictors of Hamilton scores. The results of the analysis are shown in Table 5. Factor 7, associated with IFOF and uncinate fasciculus, was identified as the most highly significant predictor for classification between post-COVID and PCD patient groups.is (Table 4). The number of post-COVID symptoms was significant in the regression equation for the total sample and noPCD groups. The number of acute symptoms was significant in the regression equation only for the PCD group. Factors 12 and 15 were significant in the regression equation for the PCD group. The highest scores for Factor 12 corresponded to left lingual WM. For factor 15, none of the structures studied showed high factor scores. This factor shows weak (r < 0.04), although significant negative correlations with superior and middle occipital, middle frontal WM and medulla, and weak (p < 0.04) significant positive correlations with the angular, inferior, and superior temporal WM.
4. Discussion
In this work, brain demyelination was investigated as a possible cause of post-COVID depression. Patients with newly diagnosed post-COVID-19 clinical depression showed extensive brain demyelination. Changes in myelination were statistically significant in comparison of the post-COVID patients with depression (PCD) and controls without previous COVID-19 as well as in comparison with the patients with long-term complications after COVID-19 but without diagnosed depression. Patients in the PCD group showed extensive demyelination of the juxtacortical WM, most pronounced in the occipital lobe, but also including the frontal, parietal and temporal lobes. In addition, patients in this group showed demyelination of the WM tracts, the most prominent for the association pathways including the IFOF, sagittal stratum, and left external capsule. Projection (posterior thalamic radiation) and commissural (left tapetum) WM pathways also were affected. Besides, we found GM demyelination, including the hippocampus, putamen, left globus pallidus and amygdala. Significant demyelination was also observed in the noPCD group compared to the control group, but with lower magnitude and smaller affected area than for the PCD group.
Multiple regression analysis revealed only one factor as the main predictor of post-COVID depression: factor 7, which with the highest level of significance was included in both the regression equation for the total sample, which differentiates the PCD and noPCD groups (R2 = 0.41, p < 0.001), and in the regression equation predicting the severity of depression by Hamilton score in the PCD group (R2 = 0.68, p < 0.001). Factor 7 included two structures with the highest factor loadings: IFOF and the uncinate fasciculus of both hemispheres. IFOF also showed significant demyelination in the PCD group compared with both the non-PCD group and the control according to ANOVA results. The uncinate fasciculus showed only a trend (p = 0.08) toward decreased MPF for the PCD group compared with the noPCD group and no significant differences with the control group. Thus, according to the results of two types of analysis, IFOF demyelination can be considered as the best predictor of clinical post-COVID depression.
The regression equation for the total sample did not include any other MPF-related variables other than Factor 7, while the regression equation for the PCD group also included factor 12 and factor 15. Factor 12 was associated with left lingual WM, which showed no significant differences between groups according to ANOVA results. Factor 15 was not strictly associated with any of the studied structures (factor loadings < 0.7 for all structures) and demonstrated weak, although significant, correlations with changes in myelination in multiple regions of juxtacortical WM (superior and middle occipital, middle frontal, angular, inferior and superior temporal WM) and medulla. Most of these juxtacortical WM regions (superior and middle occipital, angular, superior temporal WM) showed significant decrease in MPF in the PCD group compared to controls.
The number of symptoms in the acute and post-COVID phases were also important for group classification. The equations for the total sample and noPCD group included the number of symptoms in the post-COVID phase, and this variable was the only significant predictor for the noPCD group. In contrast, the regression equation for the PCD group included the number of symptoms in the acute phase.
According to the literature, depression is often considered as a disorder of WM connectivity [41,42,43,44,45,46,47] in which IFOF plays a significant role [45,46,47]. The IFOF connects early visual processing in the cuneus and lingual gyrus as well as parts of the parietal lobe to frontal lobe regions and plays a critical role in semantic language processing, goal-oriented behavior, and visual switching tasks [74,75]. In addition, the tract includes the connections between the cingulo-opercular and frontoparietal networks related to executive function and goal-oriented behavior [75,76]. High angle diffusion spectrum imaging analysis identified five subcomponents of the IFOF, which primarily included connections from the frontal or fronto-orbital cortex to inferior, superior, and middle occipital lobes [77]. The IFOF degeneration has been demonstrated in patients with Alzheimer's disease and neuropsychological behavioral disorders, including antisocial personality disorder and obsessive compulsive disorder [78,79,80].
Demyelination of IFOF along with other brain structures has been described in MDD patients [45,47,81,82]. Lai et al. [45] found lower fractional anisotropy (FA) in the bilateral IFOF, SLF, inferior longitudinal fasciculi, and CC in MDD patients compared to controls. Changes in FA were found in the left IFOF, uncinate fasciculus, anterior thalamic radiation, and bilateral CC compared to the patients with panic disorder. Liang et al. [82] identified 3 subgroups of MDD patients based on the spatial localization of reduced FA: the first group with widespread WM disruption (decrease in 8 of 20 studied tracts, including IFOF), the second group with a predominant decreased FA in the CC and left cingulate, and the third group with no statistically significant tract disruption. Reduced FA in the genu of the corpus callosum, IFOF, and posterior thalamic radiation in MDD patients was found by Coloigner et al [47].
Different studies reported different number of WM-demyelinated brain structures in MDD patients [42,43,44,45,47,81,82,83,84]. Thus, Reppermund et al. [85] found a significant decrease in FA in 45 brain regions, while the study by Hollocks et al. [86] found no significant association between our WM parameters and depressive symptoms. Demyelination in MDD patients was observed most often in the CR [42,87], IFOF [42,45,47,81,82,87], uncinate fasciculus [45,87], posterior thalamic radiation [47,85,88], cingulum [42,82,84,87], sagittal stratum [42,43,87], IC [42,43,47], and frontal lobe [44,85],which was confirmed by our results. Other demyelinated brain structured in MDD were CC [42,45,47,82,83,85], SLF [85,87,88], and FX [42,43,83]; in which we did not find significant changes compared to controls. Perhaps the reason for these discrepancies lies in the differences in the etiology of MDD and post-COVID depression.
The etiology of MDD is commonly considered as multifactorial, in other words, it might be caused by the interaction of biological, genetic, environmental, and psychosocial factors [19]. Results of our current study point to COVID-19 as the main factor causing recent depressive episode. The multiple regression results identified that the number of symptoms of the acute and post-COVID phase as significant predictors of the presence and severity of clinical depression. Patients in the PCD group were significantly more likely to report ageusia, cough, and headache in the acute phase, as well as anosmia, ageusia, insomnia, fatigue, and attention deficit in the post-COVID phase compared to patients in the noPCD group. At the same time, factors such as age, gender and severity of COVID-19 were not among the significant predictors of post-COVID depression, although previous studies have shown these factors as predictors of post-COVID complications [64,67,89,90,91,92].
In addition to WM demyelination, we found MPF decrease in PCD patients for GM structures: hippocampus, left amygdala, putamen and left globus pallidus. Since all published studies measured only WM myelination, we cannot compare our results describing demyelination of GM brain structures in MDD patients, although some evidence suggests the involvement of the amygdala, hippocampus, and deep GM in depressive disorders [42,93]. Application of MPF mapping to myelin quantification was important advantage of our study in comparison with data published with use of DTI and other MRI methods. MPF mapping allows reliable quantification of weak GM myelination [51,52,53,55,58] and is independent of iron accumulation in the basal ganglia [94].
A few studies systematically examined myelination in post-COVID patients [33,34,35,36,37,38,39]. The works by Huang et al. examined WM changes in the longitudinal MRI (DTI, DKI, NODDI) studies one [34] and two [33] years after COVID-19 recovery. They found abnormal diffusion metrics in the corona radiata, genu of the CC and left SLF in one year after recovery and in the CC, CR, CP, IC, posterior thalamic radiation, sagittal stratum, left external capsule, SLF, and CST in two years after recovery. Lower FA in the body of the corpus callosum was observed in the acute phase of COVID-19. Inflammation levels in the acute stage positively correlated with white matter abnormalities and negatively with cognitive function. Qin et al. [37] revealed significant changes in the volumes of numerous WM structures and in FA in severe compared to mild patients, and in mild patients compared to controls patients. FA differences were found in the following WM tracts: anterior thalamic radiation, SLF, optic radiation, ILF, inferior longitudinal fasciculus, forceps minor, right IFOF, left FX, acoustic radiation, cingulum, and frontal aslant tract. MRI study by Bispo et al. [35], in patients about 3 months after COVID-19 recovery, showed no changes in GM and lower fiber-specific apparent fiber density in the corona radiata, CST, CC, arcuate fasciculus, cingulate, fornix, IFOF, inferior longitudinal fasciculus, SLF, and uncinate fasciculus. Thus, there was a significant overlap of our results and the literature data regarding a number of brain structures affected by the disease, in particular, the IFOF, cingulum, corona radiata, IC, posterior thalamic radiation, sagittal stratum, external capsule, and uncinate fasciculus. The differences in results can be explained by variability in COVID-19 complications among patients.
We found only one work by Benedetti et al. [36] that examined associations between the manifestations of post-COVID depression, brain myelination and functional connectivity. The study included voxel-based morphometry, DTI, and resting-state fMRI on 42 patients imaged 3 months after COVID-19. Self-rated depression inversely correlated with GM volumes in anterior cingulate cortex and insula, axial diffusivity, and was associated with functional connectivity. In this study, depressive psychopathology was self-rated on the Zung Self-Rating Depression Scale and high scores (>9) were observed in only 9 of 42 patients. This situation is critically different from our study of a homogeneous group with a clinical diagnosis of depression made by a psychiatrist. Unfortunately, in the study by Benedetti et al. the control group was missing. Our results partially overlap with the above in terms of decreased connectivity in singular WM, but differences in samples and the lack of a control group do not allow us to draw a clear conclusion.
5. Conclusions
To date, very few studies have been carried out on changes in myelination in post-COVID complications and, in particular, in post-COVID depression. The present study is the first to show widespread demyelination in WM and GM brain structures in patients with clinically diagnosed depression caused by COVID-19. These changes were observed both in comparison with controls, as well as in comparison with patients with post-COVID complications, but without diagnosed depression. the IFOF, has been identified as a key structure, where the presence of demyelination was the best predictor of the presence and severity of post-COVID depression. Future studies will clarify whether IFOF demyelination is a specific feature associated with the effects of Sars-CoV-2 infection or is a general feature of the depressive disorders.
6. Study limitations
Our study is limited by using the age from 18 to 60; older individuals with PCD were not studied. Only two psychiatric scales, HDRS and HADS, for assessing the severity and symptoms of depression. Testing with other psychiatric scales, as well as survey of the family members and the caregivers may provide additional objective information about symptoms of depression [95]. Future studies in other age ranges, using other MRI modalities in combination with testing for depressive symptoms, will help to better understand the features and mechanisms of post-COVID depression.
Author Contributions
Conceptualization, writing—original draft preparation, M.Kh.; Data curation, project administration, software M..S.; writing—review and editing, A.V.N.; investigation, D.K.; data acquisition, A.U.; formal analysis, T.A.; formal analysis, I.V.; formal analysis, M.K.; formal analysis, V.P.; formal analysis, M.M.; investigation, V.O.; investigation, N.K.; investigation, A.L.; resources, Y.T, investigation, S.V.; investigation, E.S. All authors reviewed and approved the final version of the manuscript.
Funding
The study was funded by the Russian Science Foundation (project No. 22-15-00481). M. Khodanovich, T. Anan’ina, and M. Moshkina received partial support for their activities from a state assignment of the Ministry of Science and Higher Education of the Russian Federation “Priority 2030”. Software for MPF map reconstruction was distributed under support of the NIH High-Impact Neuroscience Research Resource grant R24NS104098.
Institutional Review Board Statement
The study design was approved by the local Ethical Committee of the Mental Health Research Institute (№15/8.2022) and Bioethics Committee of Tomsk State University (№12/06.2022) in accordance with Helsinki ethics committee guidelines.
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Acknowledgments
The authors thank Dr.Vasily L. Yarnykh for providing the software for MPF map reconstruction.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M. V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-Acute COVID-19 Syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Nasserie, T.; Hittle, M.; Goodman, S.N. Assessment of the Frequency and Variety of Persistent Symptoms among Patients with COVID-19: A Systematic Review. JAMA Netw. Open 2021, 4, 1–19. [Google Scholar] [CrossRef]
- Huang, Y.; Pinto, M.D.; Borelli, J.L.; Mehrabadi, M.A.; Dutt, N.; Lambert, N.; Nurmi, E.L.; Chakraborty, R.; Amir, M. COVID Symptoms, Symptom Clusters, and Predictors for Becoming a Long-Hauler: Looking for Clarity in the Haze of the Pandemic. Clin. Nurs. Res. 2022, 31, 1390–1398. [Google Scholar] [CrossRef]
- de Erausquin, G.A.; Snyder, H.; Carrillo, M.; Hosseini, A.A.; Brugha, T.S.; Seshadri, S. The Chronic Neuropsychiatric Sequelae of COVID-19: The Need for a Prospective Study of Viral Impact on Brain Functioning. Alzheimer’s Dement. 2021, 17, 1056–1065. [Google Scholar] [CrossRef]
- Graham, E.L.; Clark, J.R.; Orban, Z.S.; Lim, P.H.; Szymanski, A.L.; Taylor, C.; DiBiase, R.M.; Jia, D.T.; Balabanov, R.; Ho, S.U.; et al. Persistent Neurologic Symptoms and Cognitive Dysfunction in Non-Hospitalized Covid-19 “Long Haulers. ” Ann. Clin. Transl. Neurol. 2021, 8, 1073–1085. [Google Scholar] [CrossRef]
- Khodanovich, M.Y.; Kamaeva, D.A.; Naumova, A. V. Role of Demyelination in the Persistence of Neurological and Mental Impairments after COVID-19. Int. J. Mol. Sci. 2022, 23. [Google Scholar] [CrossRef]
- Varatharaj, A.; Thomas, N.; Ellul, M.A.; Davies, N.W.S.; Pollak, T.A.; Tenorio, E.L.; Sultan, M.; Easton, A.; Breen, G.; Zandi, M.; et al. Neurological and Neuropsychiatric Complications of COVID-19 in 153 Patients: A UK-Wide Surveillance Study. The Lancet Psychiatry 2020, 7, 875–882. [Google Scholar] [CrossRef]
- Miskowiak, K.W.; Johnsen, S.; Sattler, S.M.; Nielsen, S.; Kunalan, K.; Rungby, J.; Lapperre, T.; Porsberg, C.M. Cognitive Impairments Four Months after COVID-19 Hospital Discharge: Pattern, Severity and Association with Illness Variables. Eur. Neuropsychopharmacol. 2021, 46, 39–48. [Google Scholar] [CrossRef]
- Daroische, R.; Hemminghyth, M.S.; Eilertsen, T.H.; Breitve, M.H.; Chwiszczuk, L.J. Cognitive Impairment After COVID-19—A Review on Objective Test Data. Front. Neurol. 2021, 12. [Google Scholar] [CrossRef]
- Woo, M.S.; Malsy, J.; Pöttgen, J.; Seddiq Zai, S.; Ufer, F.; Hadjilaou, A.; Schmiedel, S.; Addo, M.M.; Gerloff, C.; Heesen, C.; et al. Frequent Neurocognitive Deficits after Recovery from Mild COVID-19. Brain Commun. 2020, 2, 1–9. [Google Scholar] [CrossRef]
- Stefanou, M.I.; Palaiodimou, L.; Bakola, E.; Smyrnis, N.; Papadopoulou, M.; Paraskevas, G.P.; Rizos, E.; Boutati, E.; Grigoriadis, N.; Krogias, C.; et al. Neurological Manifestations of Long-COVID Syndrome: A Narrative Review. Ther. Adv. Chronic Dis. 2022, 13, 1–21. [Google Scholar] [CrossRef]
- Peterson, C.J.; Sarangi, A.; Bangash, F. Neurological Sequelae of COVID-19: A Review. Egypt. J. Neurol. Psychiatry Neurosurg. 2021, 57. [Google Scholar] [CrossRef]
- Efstathiou, V.; Stefanou, M.-I.; Demetriou, M.; Siafakas, N.; Makris, M.; Tsivgoulis, G.; Zoumpourlis, V.; Kympouropoulos, S.; Tsoporis, J.; Spandidos, D.; et al. Long COVID and Neuropsychiatric Manifestations (Review). Exp. Ther. Med. 2022, 23, 1–12. [Google Scholar] [CrossRef]
- Bhola, S.; Trisal, J.; Thakur, V.; Kaur, P.; Kulshrestha, S.; Bhatia, S.K.; Kumar, P. Neurological Toll of COVID-19. Neurol. Sci. 2022, 43, 2171–2186. [Google Scholar] [CrossRef]
- Naphade, P.; Singh, P.; Rao, P.; Rohatgi, S.; Chaudhury, S.; Nirhale, S. Psychiatric Symptoms and Fatigue in COVID-19 Survivors. Cureus 2023, 15, 0–7. [Google Scholar] [CrossRef]
- Xie, Y.; Xu, E.; Al-Aly, Z. Risks of Mental Health Outcomes in People with Covid-19: Cohort Study. BMJ 2022, 376, 1–13. [Google Scholar] [CrossRef]
- Simonetti, A.; Bernardi, E.; Margoni, S.; Catinari, A.; Restaino, A.; Ieritano, V.; Palazzetti, M.; Mastrantonio, F.; Janiri, D.; Tosato, M.; et al. Mixed Depression in the Post-COVID-19 Syndrome: Correlation between Excitatory Symptoms in Depression and Physical Burden after COVID-19. Brain Sci. 2023, 13. [Google Scholar] [CrossRef]
- Lorkiewicz, P.; Waszkiewicz, N. Biomarkers of Post-COVID Depression. J. Clin. Med. 2021, 10, 4142. [Google Scholar] [CrossRef]
- Li, Z.; Ruan, M.; Chen, J.; Fang, Y. Major Depressive Disorder: Advances in Neuroscience Research and Translational Applications. Neurosci. Bull. 2021, 37, 863–880. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Braga, J.; Lepra, M.; Kish, S.J.; Rusjan, P.M.; Nasser, Z.; Verhoeff, N.; Vasdev, N.; Bagby, M.; Boileau, I.; Husain, M.I.; et al. Neuroinflammation after COVID-19 with Persistent Depressive and Cognitive Symptoms. JAMA Psychiatry 2023, 80, 787–795. [Google Scholar] [CrossRef]
- Sriwastava, S.; Tandon, M.; Podury, S.; Prasad, A.; Wen, S.; Guthrie, G.; Kakara, M.; Jaiswal, S.; Subedi, R.; Elkhooly, M.; et al. COVID-19 and Neuroinflammation: A Literature Review of Relevant Neuroimaging and CSF Markers in Central Nervous System Inflammatory Disorders from SARS-COV2. J. Neurol. 2021, 268, 4448–4478. [Google Scholar] [CrossRef]
- Chapman, T.W.; Hill, R.A. Myelin Plasticity in Adulthood and Aging. Neurosci. Lett. 2020, 715, 134645. [Google Scholar] [CrossRef]
- Sams, E.C. Oligodendrocytes in the Aging Brain. Neuronal Signal. 2021, 5, 1–24. [Google Scholar] [CrossRef]
- Kohama, S.G.; Rosene, D.L.; Sherman, L.S. Age-Related Changes in Human and Non-Human Primate White Matter: From Myelination Disturbances to Cognitive Decline. Age (Omaha). 2012, 34, 1093–1110. [Google Scholar] [CrossRef]
- Faro, S.H.; Manmatharayan, A.; Leiby, B.; Jain, N.; Mohamed, F.B.; Talekar, K.S.; Doshi, A.; Jambor, I.; Chang, S.; Finkelstein, M.; et al. Neuroimaging Findings in 4342 Hospitalized COVID-19 Subjects: A Multicenter Report from the United States and Europe. J. Neuroimaging 2023, 11–14. [Google Scholar] [CrossRef]
- Erdoğan, T.; Koçer, B.; Şen, S.; Petek Balci, B.; Terzi, M. Newly Diagnosed Tumefactive Demyelinating Lesion and Multiple Sclerosis After COVID-19 Infection. Noropsikiyatri Ars. 2023, 60, 223–230. [Google Scholar] [CrossRef]
- Bezold, A.; Hussain, H.; Nwanze, J.; Roberts, J.T.; Hsieh, K.J. Radiologic-Pathologic Correlation of COVID-19-Associated Acute Disseminated Encephalomyelitis. Cureus 2023, 15. [Google Scholar] [CrossRef]
- Sharma, V.; Chhabra, T.; Singh, T.G. Correlation of Covid-19 and Guillain-Barré Syndrome: A Mechanistic Perspective. Obes. Med. 2023, 40. [Google Scholar] [CrossRef]
- Malekpour, M.; Khanmohammadi, S.; Meybodi, M.J.E.; Shekouh, D.; Rahmanian, M.R.; Kardeh, S.; Azarpira, N. COVID-19 as a Trigger of Guillain-Barré Syndrome: A Review of the Molecular Mechanism. Immunity, Inflamm. Dis. 2023, 11. [Google Scholar] [CrossRef]
- Sklinda, K.; Dorobek, M.; Wasilewski, P.G.; Dreżewski, K.; Dȩbicka, M.; Walecki, J.; Mruk, B. Radiological Manifestation of Neurological Complications in the Course of SARS-CoV-2 Infection. Front. Neurol. 2021, 12. [Google Scholar] [CrossRef]
- Bhardwaj, A.; Mishra, H.P.; Goel, A.; Gupta, A. COVID-19 – a Potential Trigger for MOGAD-Associated Optic Neuritis: A Case Report and Literature Review. Ther. Adv. Ophthalmol. 2023, 15, 1–9. [Google Scholar] [CrossRef]
- Huang, S.; Zhou, X.; Zhao, W.; Du, Y.; Yang, D.; Huang, Y.; Chen, Y.; Zhang, H.; Yang, G.; Liu, J.; et al. Dynamic White Matter Changes in Recovered COVID-19 Patients: A Two-Year Follow-up Study. Theranostics 2023, 13, 724–735. [Google Scholar] [CrossRef]
- Huang, S.; Zhou, Z.; Yang, D.; Zhao, W.; Zeng, M.; Xie, X.; Du, Y.; Jiang, Y.; Zhou, X.; Yang, W.; et al. Persistent White Matter Changes in Recovered COVID-19 Patients at the 1-Year Follow-Up. Brain 2022, 145, 1830–1838. [Google Scholar] [CrossRef]
- Bispo, D.D. de C.; Brandão, P.R. de P.; Pereira, D.A.; Maluf, F.B.; Dias, B.A.; Paranhos, H.R.; von Glehn, F.; de Oliveira, A.C.P.; Regattieri, N.A.T.; Silva, L.S.; et al. Brain Microstructural Changes and Fatigue after COVID-19. Front. Neurol. 2022, 13. [Google Scholar] [CrossRef]
- Benedetti, F.; Palladini, M.; Paolini, M.; Melloni, E.; Vai, B.; De Lorenzo, R.; Furlan, R.; Rovere-Querini, P.; Falini, A.; Mazza, M.G. Brain Correlates of Depression, Post-Traumatic Distress, and Inflammatory Biomarkers in COVID-19 Survivors: A Multimodal Magnetic Resonance Imaging Study. Brain, Behav. Immun. - Heal. 2021, 18, 100387. [Google Scholar] [CrossRef]
- Qin, Y.; Wu, J.; Chen, T.; Li, J.; Zhang, G.; Wu, D.; Zhou, Y.; Zheng, N.; Cai, A.; Ning, Q.; et al. Long-Term Microstructure and Cerebral Blood Flow Changes in Patients Recovered from COVID-19 without Neurological Manifestations. J. Clin. Invest. 2021, 131. [Google Scholar] [CrossRef]
- Tian, T.; Wu, J.; Chen, T.; Li, J.; Yan, S.; Zhou, Y.; Peng, X.; Li, Y.; Zheng, N.; Cai, A.; et al. Long-Term Follow-up of Dynamic Brain Changes in Patients Recovered from COVID-19 without Neurological Manifestations. JCI Insight 2022, 7. [Google Scholar] [CrossRef] [PubMed]
- Boito, D.; Eklund, A.; Tisell, A.; Levi, R.; Özarslan, E.; Blystad, I. MRI with Generalized Diffusion Encoding Reveals Damaged White Matter in Patients Previously Hospitalized for COVID-19 and with Persisting Symptoms at Follow-Up. Brain Commun. 2023, 5, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Mazza, M.G.; Palladini, M.; Poletti, S.; Benedetti, F. Post-COVID-19 Depressive Symptoms: Epidemiology, Pathophysiology, and Pharmacological Treatment. CNS Drugs 2022, 36, 681–702. [Google Scholar] [CrossRef] [PubMed]
- Wise, T.; Marwood, L.; Perkins, A.M.; Herane-Vives, A.; Joules, R.; Lythgoe, D.J.; Luh, W.M.; Williams, S.C.R.; Young, A.H.; Cleare, A.J.; et al. Instability of Default Mode Network Connectivity in Major Depression: A Two-Sample Confirmation Study. Transl. Psychiatry 2017, 7. [Google Scholar] [CrossRef]
- van Velzen, L.S.; Kelly, S.; Isaev, D.; Aleman, A.; Aftanas, L.I.; Bauer, J.; Baune, B.T.; Brak, I. V.; Carballedo, A.; Connolly, C.G.; et al. White Matter Disturbances in Major Depressive Disorder: A Coordinated Analysis across 20 International Cohorts in the ENIGMA MDD Working Group. Mol. Psychiatry 2020, 25, 1511–1525. [Google Scholar] [CrossRef]
- Hou, G.; Lai, W.; Jiang, W.; Liu, X.; Qian, L.; Zhang, Y.; Zhou, Z. Myelin Deficits in Patients with Recurrent Major Depressive Disorder: An Inhomogeneous Magnetization Transfer Study. Neurosci. Lett. 2021, 750, 135768. [Google Scholar] [CrossRef]
- Sacchet, M.D.; Gotlib, I.H. Myelination of the Brain in Major Depressive Disorder: An in Vivo Quantitative Magnetic Resonance Imaging Study. Sci. Rep. 2017, 7, 1–14. [Google Scholar] [CrossRef]
- Lai, C.H.; Wu, Y. Te The White Matter Microintegrity Alterations of Neocortical and Limbic Association Fibers in Major Depressive Disorder and Panic Disorder: The Comparison. Med. (United States) 2016, 95, 1–6. [Google Scholar] [CrossRef]
- Liao, Y.; Huang, X.; Wu, Q.; Yang, C.; Kuang, W.; Du, M.; Lui, S.; Yue, Q.; Chan, R.C.K.; Kemp, G.J.; et al. Is Depression a Disconnection Syndrome? Meta- Analysis of Diffusion Tensor Imaging Studies in Patients with MDD. J. Psychiatry Neurosci. 2013, 38, 49–56. [Google Scholar] [CrossRef]
- Coloigner, J.; Batail, J.M.; Commowick, O.; Corouge, I.; Robert, G.; Barillot, C.; Drapier, D. White Matter Abnormalities in Depression: A Categorical and Phenotypic Diffusion MRI Study. NeuroImage Clin. 2019, 22. [Google Scholar] [CrossRef]
- Trujillo, P.; Summers, P.E.; Ferrari, E.; Zucca, F.A.; Sturini, M.; Mainardi, L.T.; Cerutti, S.; Smith, A.K.; Smith, S.A.; Zecca, L.; et al. Contrast Mechanisms Associated with Neuromelanin-MRI. Magn. Reson. Med. 2017, 78, 1790–1800. [Google Scholar] [CrossRef]
- Li, K.; Li, H.; Zhang, X.Y.; Stokes, A.M.; Jiang, X.; Kang, H.; Quarles, C.C.; Zu, Z.; Gochberg, D.F.; Gore, J.C.; et al. Influence of Water Compartmentation and Heterogeneous Relaxation on Quantitative Magnetization Transfer Imaging in Rodent Brain Tumors. Magn. Reson. Med. 2016, 76, 635–644. [Google Scholar] [CrossRef] [PubMed]
- Yarnykh, V.L.; Krutenkova, E.P.; Aitmagambetova, G.; Henson, L.K.J.; Piedmont, H.; Repovic, P.; Mayadev, A.; Qian, P.; Gangadharan, B. Iron-Insensitive Quantitative Assessment of Subcortical Gray Matter Demyelination in Multiple Sclerosis Using Macromolecular Proton Fraction. Am. J. Neuroradiol. 2018, 39, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Kisel, A.A.; Naumova, A. V.; Yarnykh, V.L. Macromolecular Proton Fraction as a Myelin Biomarker: Principles, Validation, and Applications. Front. Neurosci. 2022, 16, 1–10. [Google Scholar] [CrossRef]
- Khodanovich, M.Y.Y.; Sorokina, I.V.V.; Glazacheva, V.Y.Y.; Akulov, A.E.E.; Nemirovich-Danchenko, N.M.M.; Romashchenko, A.V. V.; Tolstikova, T.G.G.; Mustafina, L.R.R.; Yarnykh, V.L.L. Histological Validation of Fast Macromolecular Proton Fraction Mapping as a Quantitative Myelin Imaging Method in the Cuprizone Demyelination Model. Sci. Rep. 2017, 7, 1–12. [Google Scholar] [CrossRef]
- Khodanovich, M.Y.; Pishchelko, A.O.; Glazacheva, V.Y.; Pan, E.S.; Akulov, A.E.; Svetlik, M.V.; Tyumentseva, Y.A.; Anan’ina, T.V. ; Yarnykh Vasily Leonidovich Quantitative Imaging of White and Gray Matter Remyelination in the Cuprizone Demyelination Model Using the Macromolecular Proton Fraction. Cells 2019, 8, 1204. [Google Scholar] [CrossRef]
- Khodanovich, M.Y.; Gubskiy, I.L.; Kudabaeva, M.S.; Namestnikova, D.D.; Kisel, A.A.; Anan’ina, T. V.; Tumentceva, Y.A.; Mustafina, L.R.; Yarnykh, V.L. Long-Term Monitoring of Chronic Demyelination and Remyelination in a Rat Ischemic Stroke Model Using Macromolecular Proton Fraction Mapping. J. Cereb. Blood Flow Metab. 2021, 41, 2856–2869. [Google Scholar] [CrossRef]
- Khodanovich, M.Y.; Kisel, A.A.; Akulov, A.E.; Atochin, D.N.; Kudabaeva, M.S.; Glazacheva, V.Y.; Svetlik, M. V.; Medvednikova, Y.A.; Mustafina, L.R.; Yarnykh, V.L. Quantitative Assessment of Demyelination in Ischemic Stroke in Vivo Using Macromolecular Proton Fraction Mapping. J. Cereb. Blood Flow Metab. 2018, 38, 919–931. [Google Scholar] [CrossRef]
- Naumova, A.V.; Akulov, A.E.; Khodanovich, M.Y.; Yarnykh, V.L. High-Resolution Three-Dimensional Macromolecular Proton Fraction Mapping for Quantitative Neuroanatomical Imaging of the Rodent Brain in Ultra-High Magnetic Fields. Neuroimage 2017, 147, 985–993. [Google Scholar] [CrossRef]
- Anisimov, N.V.; Pavlova, O.S.; Pirogov, Y.A. Yarnykh Vasily Leonidovich Three-Dimensional Fast Single-Point Macromolecular Proton Fraction Mapping of the Human Brain at 0.5 Tesla. Quant. Imaging Med. Surg. 2020, 10, 1441–1449. [Google Scholar] [CrossRef]
- Smirnova, L.P.; Yarnykh, V.L.; Parshukova, D.A.; Kornetova, E.G.; Semke, A. V.; Usova, A. V.; Pishchelko, A.O.; Khodanovich, M.Y.; Ivanova, S.A. Global Hypomyelination of the Brain White and Gray Matter in Schizophrenia: Quantitative Imaging Using Macromolecular Proton Fraction. Transl. Psychiatry 2021, 11, 365. [Google Scholar] [CrossRef]
- Yarnykh, V.L.L.; Prihod’ko, I.Y.Y.; Savelov, A.A.A.; Korostyshevskaya, A.M.M. Quantitative Assessment of Normal Fetal Brain Myelination Using Fast Macromolecular Proton Fraction Mapping. Am. J. Neuroradiol. 2018, 39, 1341–1348. [Google Scholar] [CrossRef]
- Korostyshevskaya, A.M.M.; Prihod’ko, I.Y.Y.; Savelov, A.A.A.; Yarnykh, V.L.L. Direct Comparison between Apparent Diffusion Coefficient and Macromolecular Proton Fraction as Quantitative Biomarkers of the Human Fetal Brain Maturation. J. Magn. Reson. Imaging 2019, 50, 52–61. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snalth, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. [Revista En Internet] 2014 [Acceso 28 de Noviembre de 2019]; 64(5): 361-370. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Hamilton, M. A Rating Scale for Depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Hamilton, M. Development of a Rating Scale for Depressive Illness. Br. J. Soc. Clin. Psychol. 1967, 6, 278–296. [Google Scholar] [CrossRef]
- Chan Sui Ko, A.; Candellier, A.; Mercier, M.; Joseph, C.; Schmit, J.L.; Lanoix, J.P.; Andrejak, C. Number of Initial Symptoms Is More Related to Long COVID-19 than Acute Severity of Infection: A Prospective Cohort of Hospitalized Patients. Int. J. Infect. Dis. 2022, 118, 220–223. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Pellicer-Valero, O.J.; Navarro-Pardo, E.; Rodríguez-Jiménez, J.; Martín-Guerrero, J.D.; Cigarán-Méndezd, M. The Number of Symptoms at the Acute COVID-19 Phase Is Associated with Anxiety and Depressive Long-Term Post-COVID Symptoms: A Multicenter Study. J. Psychosom. Res. 2021, 150, 110625. [Google Scholar] [CrossRef]
- Durstenfeld, M.S.; Peluso, M.J.; Peyser, N.D.; Lin, F.; Knight, S.J.; Djibo, A.; Khatib, R.; Kitzman, H.; O’Brien, E.; Williams, N.; et al. Factors Associated with Long COVID Symptoms in an Online Cohort Study. Open Forum Infect. Dis. 2023, 10, 1–10. [Google Scholar] [CrossRef]
- Asadi-Pooya, A.A.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Nemati, H.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; Farjoud-Kouhanjani, M.; et al. Risk Factors Associated with Long Covid Syndrome: A Retrospective Study. Iran. J. Med. Sci. 2021, 46, 428–436. [Google Scholar] [CrossRef]
- Yarnykh, V.L. Time-Efficient, High-Resolution, Whole Brain Three-Dimensional Macromolecular Proton Fraction Mapping. Magn. Reson. Med. 2016, 75, 2100–2106. [Google Scholar] [CrossRef]
- Yarnykh, V.L.; Tartaglione, E. V.; Ioannou, G.N. Fast Macromolecular Proton Fraction Mapping of the Human Liver in Vivo for Quantitative Assessment of Hepatic Fibrosis. NMR Biomed. 2015, 28, 1716–1725. [Google Scholar] [CrossRef]
- Avants, B.B.; Tustison, N.J.; Song, G.; Cook, P.A.; Klein, A.; Gee, J.C. NeuroImage A Reproducible Evaluation of ANTs Similarity Metric Performance in Brain Image Registration. Neuroimage 2011, 54, 2033–2044. [Google Scholar] [CrossRef]
- Avants, B.B.; Yushkevich, P.; Pluta, J.; Minkoff, D.; Korczykowski, M.; Detre, J.; Gee, J.C. NeuroImage The Optimal Template Effect in Hippocampus Studies of Diseased Populations. Neuroimage 2010, 49, 2457–2466. [Google Scholar] [CrossRef]
- Oishi, K.; Faria, A.; Jiang, H.; Li, X.; Akhter, K.; Zhang, J.; Hsu, J.T.; Miller, M.I.; Zijl, P.C.M. Van; Albert, M.; et al. NeuroImage Atlas-Based Whole Brain White Matter Analysis Using Large Deformation Diffeomorphic Metric Mapping : Application to Normal Elderly and Alzheimer ’ s Disease Participants. Neuroimage 2009, 46, 486–499. [Google Scholar] [CrossRef]
- Khodanovich, M.; Svetlik, M.; Naumova, A.; Kamaeva, D.; Usova, A.; Kudabaeva, M.; Wasserlauf, I.; Pashkevich, V.; Moshkina, M.; Obukhovskaya, V.; et al. Age-Related Decline in Brain Myelination : Quantitative Macromolecular Proton Fraction Mapping, T2-FLAIR Hyperintensity Volume, and Anti-Myelin Antibodies 7 Years Apart. Biomedicines 2023, Preprint. [Google Scholar] [CrossRef]
- Caverzasi, E.; Papinutto, N.; Amirbekian, B.; Berger, M.S.; Henry, R.G. Q-Ball of Inferior Fronto-Occipital Fasciculus and Beyond. PLoS One 2014, 9. [Google Scholar] [CrossRef]
- Conner, A.K.; Briggs, R.G.; Sali, G.; Rahimi, M.; Baker, C.M.; Burks, J.D.; Glenn, C.A.; Battiste, J.D.; Sughrue, M.E. A Connectomic Atlas of the Human Cerebrum-Chapter 13: Tractographic Description of the Inferior Fronto-Occipital Fasciculus. Oper. Neurosurg. 2018, 15, 5436–5443. [Google Scholar] [CrossRef]
- Hausman, H.K.; Hardcastle, C.; Albizu, A.; Kraft, J.N.; Evangelista, N.D.; Boutzoukas, E.M.; Langer, K.; O’Shea, A.; Van Etten, E.J.; Bharadwaj, P.K.; et al. Cingulo-Opercular and Frontoparietal Control Network Connectivity and Executive Functioning in Older Adults. GeroScience 2022, 44, 847–866. [Google Scholar] [CrossRef]
- Wu, Y.; Sun, D.; Wang, Y.; Wang, Y. Subcomponents and Connectivity of the Inferior Fronto-Occipital Fasciculus Revealed by Diffusion Spectrum Imaging Fiber Tracking. Front. Neuroanat. 2016, 10, 1–13. [Google Scholar] [CrossRef]
- Agosta, F.; Pievani, M.; Sala, S.; Geroldi, C.; Galluzzi, S.; Frisoni, G.B.; Filippi, M. White Matter Damage in Alzheimer Disease and Its Relationship to Gray Matter Atrophy. Radiology 2011, 258, 853–863. [Google Scholar] [CrossRef]
- Waller, R.; Dotterer, H.L.; Murray, L.; Maxwell, A.M.; Hyde, L.W. White-Matter Tract Abnormalities and Antisocial Behavior: A Systematic Review of Diffusion Tensor Imaging Studies across Development. NeuroImage Clin. 2017, 14, 201–215. [Google Scholar] [CrossRef]
- Peng, Z.W.; Lui, S.S.Y.; Cheung, E.F.C.; Jin, Z.; Miao, G.D.; Jing, J.; Chan, R.C.K. Brain Structural Abnormalities in Obsessive-Compulsive Disorder: Converging Evidence from White Matter and Grey Matter. Asian J. Psychiatr. 2012, 5, 290–296. [Google Scholar] [CrossRef]
- Cheng, Y.; Xu, J.; Yu, H.; Nie, B.; Li, N.; Luo, C.; Li, H.; Liu, F.; Bai, Y.; Shan, B.; et al. Delineation of Early and Later Adult Onset Depression by Diffusion Tensor Imaging. PLoS One 2014, 9. [Google Scholar] [CrossRef]
- Liang, S.; Wang, Q.; Kong, X.; Deng, W.; Yang, X.; Li, X.; Zhang, Z.; Zhang, J.; Zhang, C.; Li, X. min; et al. White Matter Abnormalities in Major Depression Biotypes Identified by Diffusion Tensor Imaging. Neurosci. Bull. 2019, 35, 867–876. [Google Scholar] [CrossRef]
- Williams, M.R.; Sharma, P.; Macdonald, C.; Pearce, R.K.B.; Hirsch, S.R.; Maier, M. Axonal Myelin Decrease in the Splenium in Major Depressive Disorder. Eur. Arch. Psychiatry Clin. Neurosci. 2019, 269, 387–395. [Google Scholar] [CrossRef]
- Baranger, D.A.A.; Halchenko, Y.O.; Satz, S.; Ragozzino, R.; Iyengar, S.; Swartz, H.A.; Manelis, A. Aberrant Levels of Cortical Myelin Distinguish Individuals with Depressive Disorders from Healthy Controls. NeuroImage Clin. 2021, 32, 102790. [Google Scholar] [CrossRef]
- Reppermund, S.; Zhuang, L.; Wen, W.; Slavin, M.J.; Trollor, J.N.; Brodaty, H.; Sachdev, P.S. White Matter Integrity and Late-Life Depression in Community-Dwelling Individuals: Diffusion Tensor Imaging Study Using Tract-Based Spatial Statistics. Br. J. Psychiatry 2014, 205, 315–320. [Google Scholar] [CrossRef]
- Hollocks, M.J.; Lawrence, A.J.; Brookes, R.L.; Barrick, T.R.; Morris, R.G.; Husain, M.; Markus, H.S. Differential Relationships between Apathy and Depression with White Matter Microstructural Changes and Functional Outcomes. Brain 2015, 138, 3803–3815. [Google Scholar] [CrossRef]
- Wu, J.Y.; Zhang, Y.; Wu, W.B.; Hu, G.; Xu, Y. Impaired Long Contact White Matter Fibers Integrity Is Related to Depression in Parkinson’s Disease. CNS Neurosci. Ther. 2018, 24, 108–114. [Google Scholar] [CrossRef]
- Shen, X.; Reus, L.M.; Cox, S.R.; Adams, M.J.; Liewald, D.C.; Bastin, M.E.; Smith, D.J.; Deary, I.J.; Whalley, H.C.; McIntosh, A.M. Subcortical Volume and White Matter Integrity Abnormalities in Major Depressive Disorder: Findings from UK Biobank Imaging Data. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and Predictors of Long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-Month Consequences of COVID-19 in Patients Discharged from Hospital: A Cohort Study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Bahmer, T.; Borzikowsky, C.; Lieb, W.; Horn, A.; Krist, L.; Fricke, J.; Scheibenbogen, C.; Rabe, K.F.; Maetzler, W.; Maetzler, C.; et al. Severity, Predictors and Clinical Correlates of Post-COVID Syndrome (PCS) in Germany: A Prospective, Multi-Centre, Population-Based Cohort Study. EClinicalMedicine 2022, 51, 101549. [Google Scholar] [CrossRef]
- Pilotto, A.; Cristillo, V.; Cotti Piccinelli, S.; Zoppi, N.; Bonzi, G.; Sattin, D.; Schiavolin, S.; Raggi, A.; Canale, A.; Gipponi, S.; et al. Long-Term Neurological Manifestations of COVID-19: Prevalence and Predictive Factors. Neurol. Sci. 2021, 42, 4903–4907. [Google Scholar] [CrossRef]
- Ramasubbu, R.; Konduru, N.; Cortese, F.; Bray, S.; Gaxiola-Valdez, I.; Goodyear, B. Reduced Intrinsic Connectivity of Amygdala in Adults with Major Depressive Disorder. Front. Psychiatry 2014, 5, 1–11. [Google Scholar] [CrossRef]
- Krutenkova, E.P.; Khodanovich, M.; Bowen, J.; Gangadharan; Henson, L.K.J.; Mayadev, A.; Repovic, P.; Qian, P.Q.; Yarnykh, V.L. Demyelination and Iron Accumulation in Subcortical Gray Matter (GM) in Multiple Sclerosis (MS). Ann. Neurol. 2015, 78. [Google Scholar]
- Giannouli, V. Predictive Factors of Depressive Symptoms of Elderly Patients with Cancer: A Critical Comment. Psychooncology. 2017, 26, 870. [Google Scholar] [CrossRef]
Figure 1.
An example of T1 Eve template [72] registration with segmentation (a) to individual MPF map (b). Slices are shown in similar axial, sagittal, and coronal projections.
Figure 1.
An example of T1 Eve template [72] registration with segmentation (a) to individual MPF map (b). Slices are shown in similar axial, sagittal, and coronal projections.
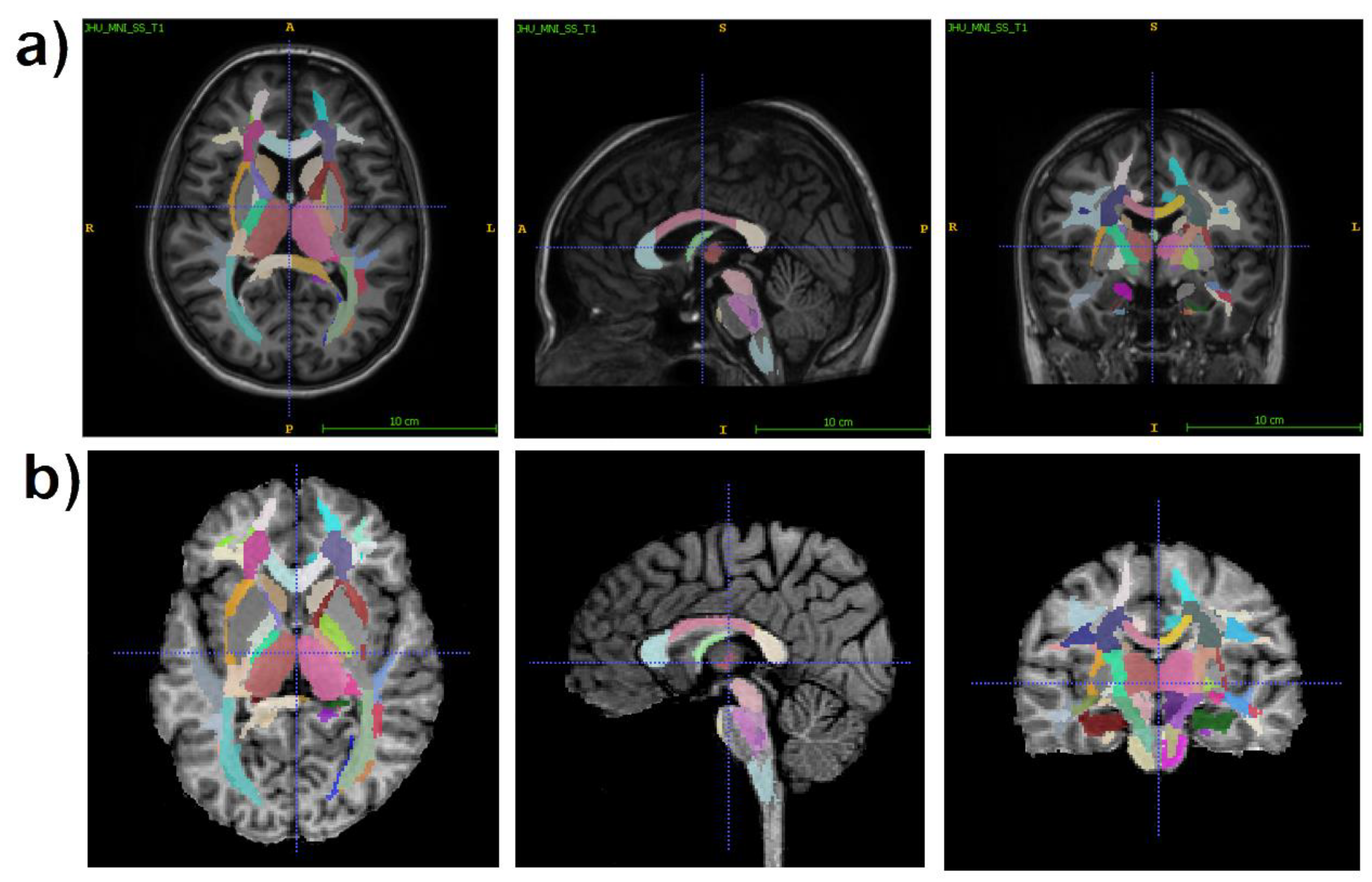
Figure 2.
Example MPF maps, T1, T2, and T2-FLAIR images of the participants from the PCD (44 years, female), noPCD (48 years, male), and control (44 years, female) group.
Figure 2.
Example MPF maps, T1, T2, and T2-FLAIR images of the participants from the PCD (44 years, female), noPCD (48 years, male), and control (44 years, female) group.
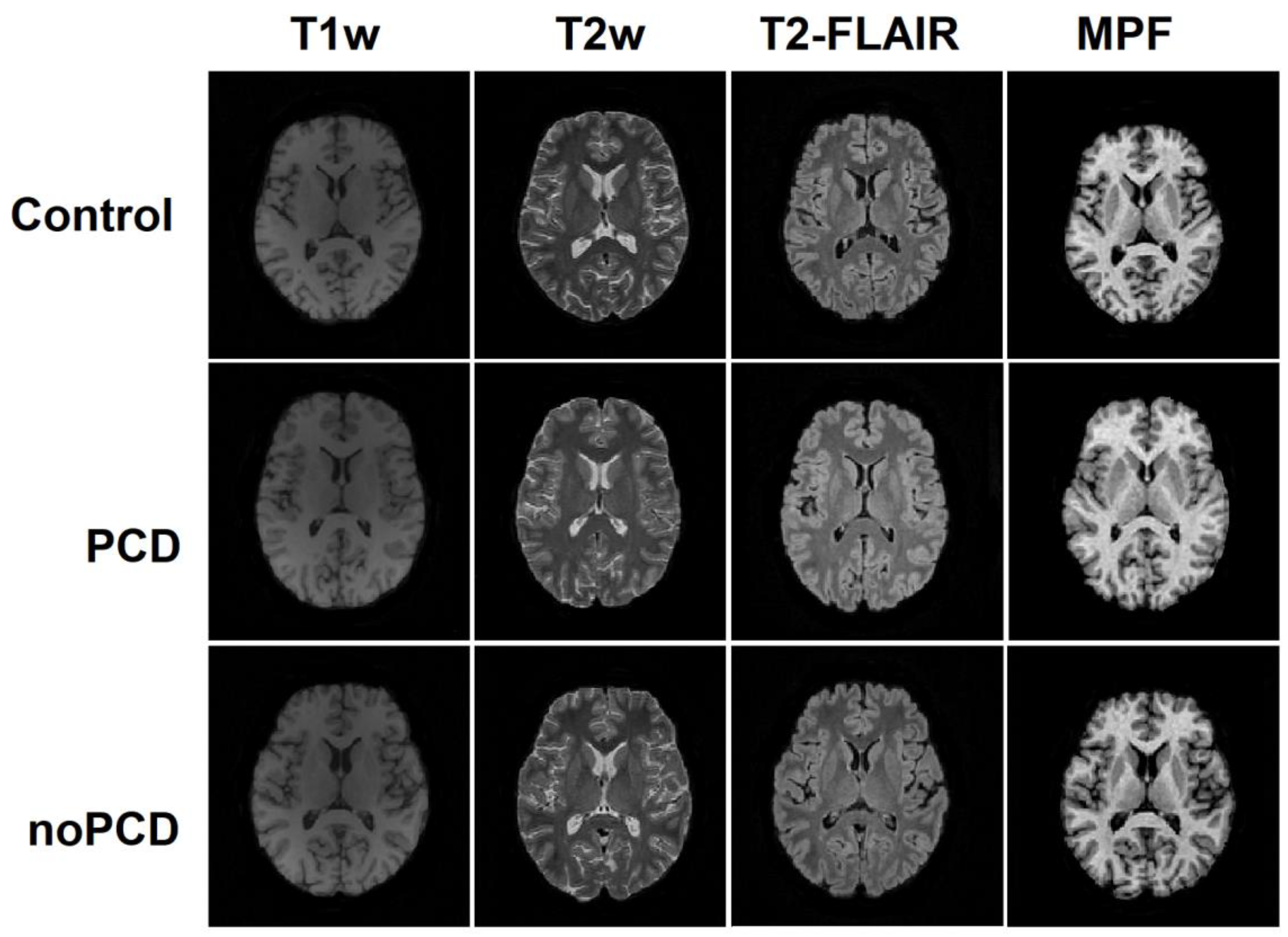
Figure 3.
Differences in MPF measurements between the PCD, noPCD, and control group for the separate brain regions: (a) juxtacortical WM, (b) WM pathways, (c) allocortex and deep GM, (d) brainstem. Significant differences relative to controls: * - p < 0.05, ** - p < 0.01. Significant differences relative to the noPCD group: ♦ - p < 0.05, ♦♦ - p < 0.01. Error bars correspond to SD.
Figure 3.
Differences in MPF measurements between the PCD, noPCD, and control group for the separate brain regions: (a) juxtacortical WM, (b) WM pathways, (c) allocortex and deep GM, (d) brainstem. Significant differences relative to controls: * - p < 0.05, ** - p < 0.01. Significant differences relative to the noPCD group: ♦ - p < 0.05, ♦♦ - p < 0.01. Error bars correspond to SD.
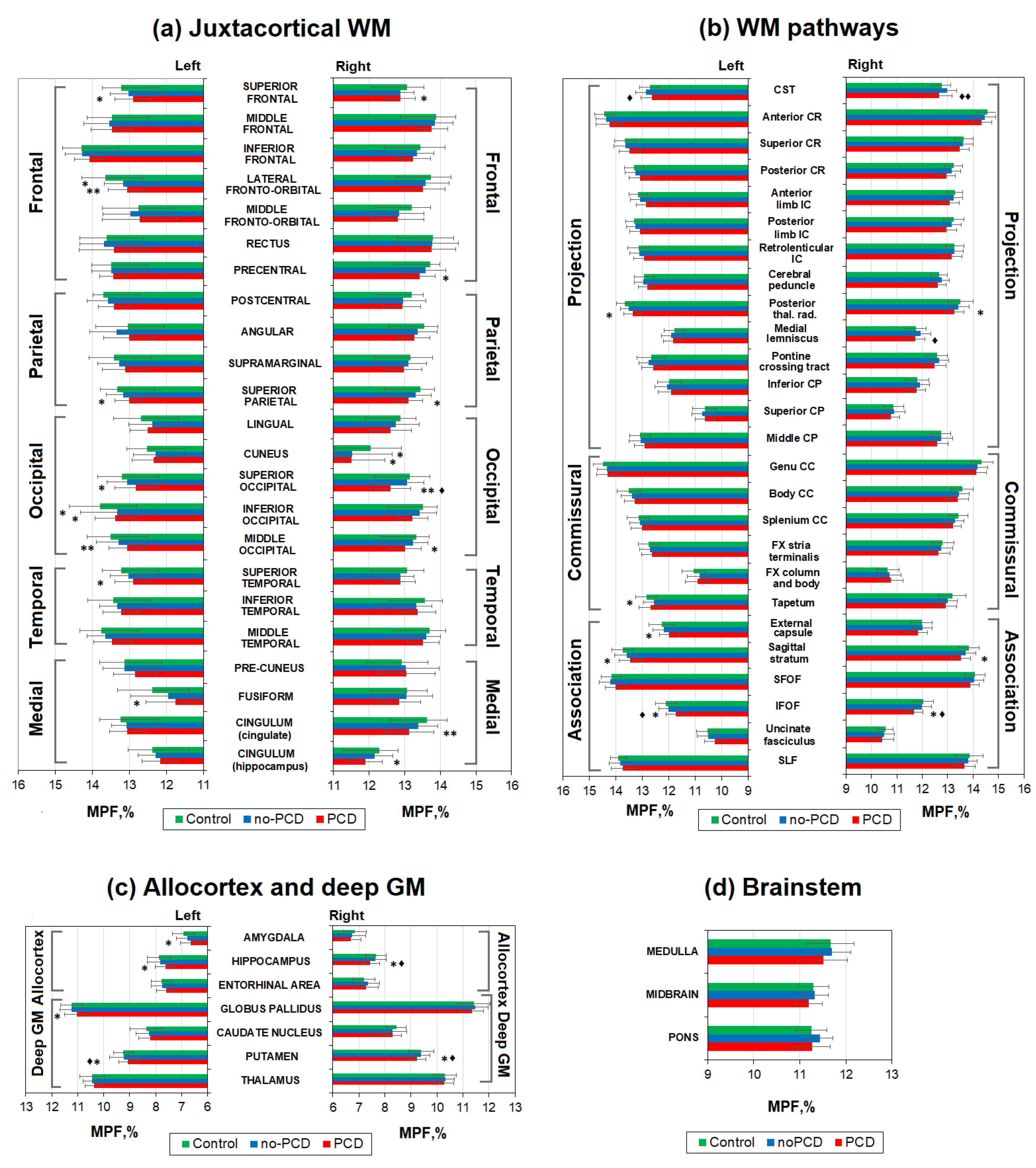
Figure 4.
Examples of the brain slices of Eve template [72] that illustrates significant (p<0.05) and near significant (p<0.1) differences between groups at the levels of superior juxtacortical WM, basal ganglia, and brainstem of axial views (a) and sagittal views of the left (b) and right (c) hemispheres.
Figure 4.
Examples of the brain slices of Eve template [72] that illustrates significant (p<0.05) and near significant (p<0.1) differences between groups at the levels of superior juxtacortical WM, basal ganglia, and brainstem of axial views (a) and sagittal views of the left (b) and right (c) hemispheres.
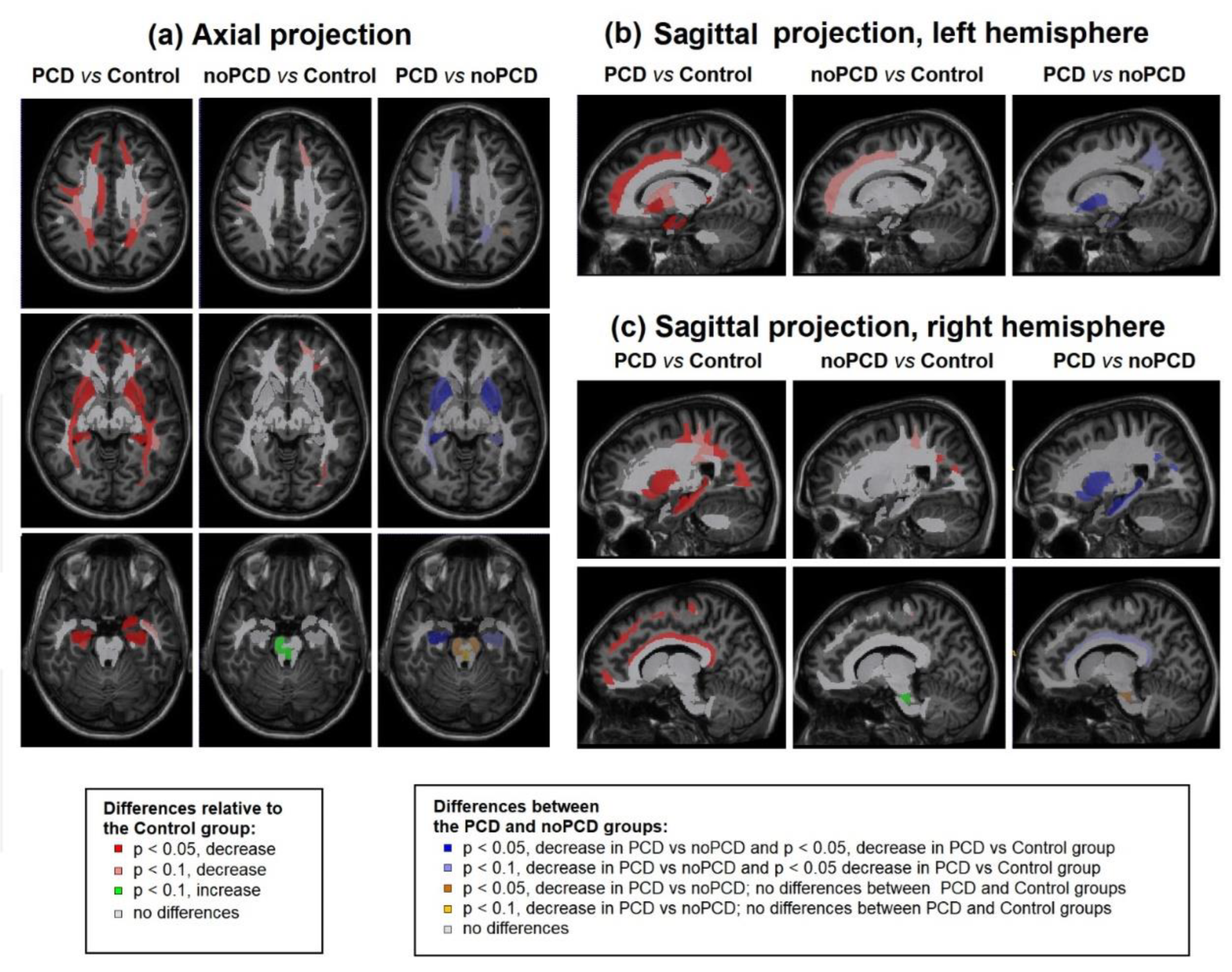
Figure 5.
The percentage changes between MPF measurements obtained in the PCD, noPCD, and control groups: (a) juxtacortical WM, (b) WM pathways, (c) allocortex and deep GM, (d) brainstem.
Figure 5.
The percentage changes between MPF measurements obtained in the PCD, noPCD, and control groups: (a) juxtacortical WM, (b) WM pathways, (c) allocortex and deep GM, (d) brainstem.
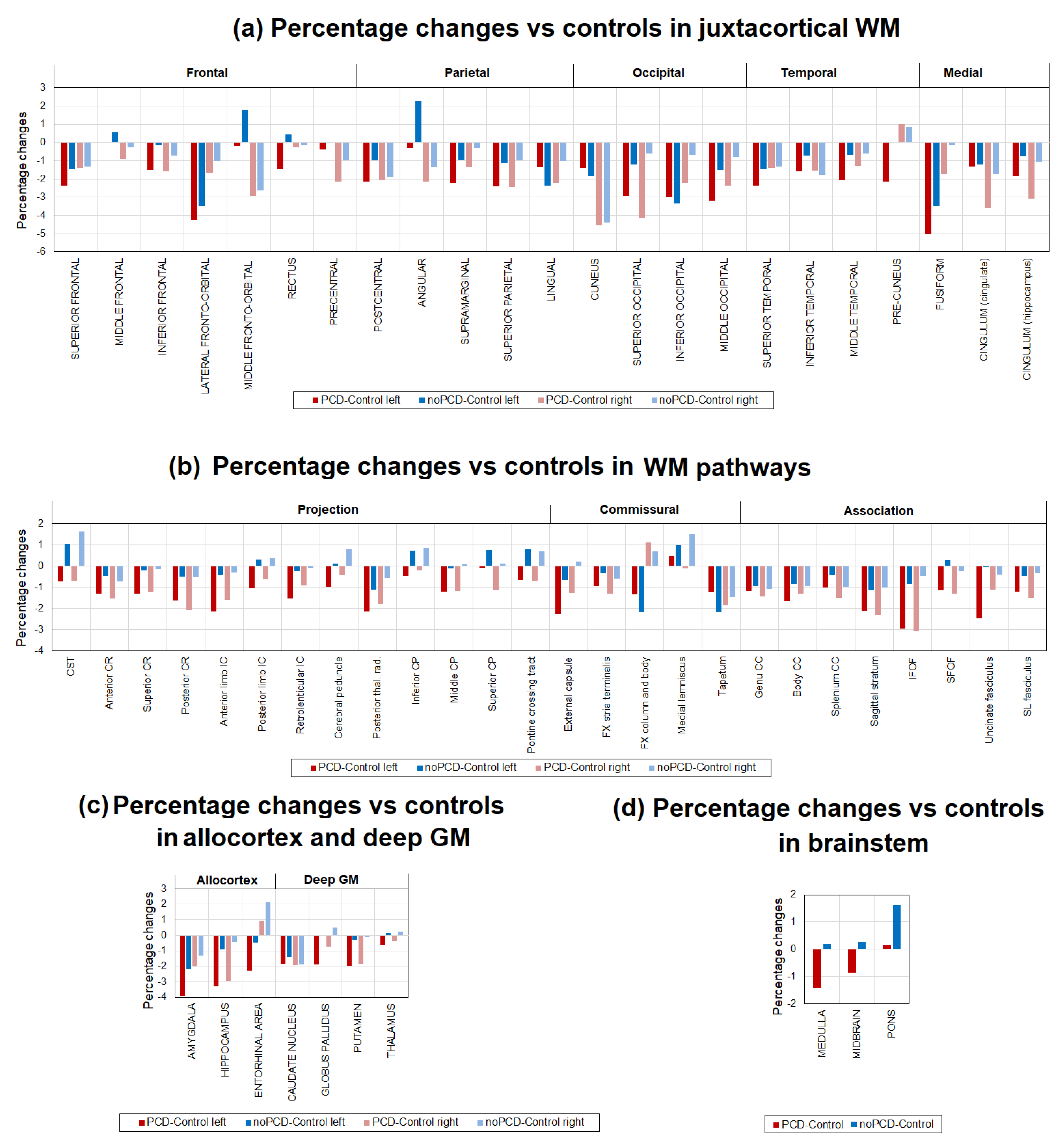

Table 1.
The demographic characteristics of participants of the study.
| Parameter | PCD | No-PCD | Control |
|---|---|---|---|
| Sample size | 25 | 38 | 19 |
| Male (%) | 4(16) | 14(29) | 8(42.1) |
| Female (%) | 21(84) | 24(71) | 11(57.9) |
| Age, years±SD | 36.96±13.7 | 42.05±9.17 | 38.53±10.57 |
| Age, median (min-max) | 42 (19-59) | 42(21-58) | 37(20-56) |
Table 2.
The severity of COVID-19, acute and post-COVID symptoms of participants of the study, according to the health questionnaire.
Table 2.
The severity of COVID-19, acute and post-COVID symptoms of participants of the study, according to the health questionnaire.
| Parameter | PCD | noPCD | Statistics |
|---|---|---|---|
| Severity, mild/moderate/severe (%) | 88/8/4 | 73/24/3 | F(2, 79)=1.74, p=0.18 |
| Number of COVID-19 episodes, mean±SD | 1.6±0.7 | 1.5±0.7 | F(1, 61)=0.33, p=0.56 |
| Time after the first COVID-19, months±SD | 20.3±8.2 | 19.7±9.8 | F(1, 61)=0.06, p=0.81 |
| Time after last COVID-19, months±SD | 13.1±10.3 | 13.8±9.9 | F(1, 61)=0.07, p=0.79 |
| Acute symptoms | |||
| Anosmia, n (%) | 22(88%) | 29(76%) | Chi sq, p= 0.25 |
| Ageusia, n (%) | 19(76%)* | 19(50%) | Chi sq, p= 0.04 |
| Fever, n (%) | 22(88%) | 36(95%) | Chi sq, p= 0.33 |
| Difficulty breathing, n (%) | 14 (56%) | 17(45%) | Chi sq, p= 0.38 |
| Cough, n (%) | 22(88%)* | 24(65%) | Chi sq, p= 0.04 |
| Muscle weakness, n (%) | 24(96%) | 35(92%) | Chi sq, p= 0.53 |
| Myalgia, n (%) | 20 (80%) | 22(58%) | Chi sq, p= 0.07 |
| Headache, n (%) | 22(88%)* | 25(66%) | Chi sq, p= 0.047 |
| Dizziness, n (%) | 14 (56%) | 15(39%) | Chi sq, p= 0.20 |
| Number of acute symptoms | 7.24± 1.85** | 5.82±2.13 | F(1, 61)=7.45, p=0.008 |
| Post-COVID symptoms | |||
| Headache, n (%) | 7 (28%) | 4 (11%) | Chi sq, p= 0.07 |
| Dizziness, n (%) | 10 (40%) | 13 (34%) | Chi sq, p= 0.64 |
| Brain fog, n (%) | 14 (56%) | 16 (42%) | Chi sq, p= 0.28 |
| Anosmia, n (%) | 16 (64%)** | 11(29%) | Chi sq, p= 0.006 |
| Ageusia, n (%) | 14 (56%)** | 8(21%) | Chi sq, p= 0.004 |
| Sensitivity, n (%) | 3 (12%) | 4(11%) | Chi sq, p= 0.86 |
| Hypertensia/hypotensia, n (%) | 7 (28%) | 15(39%) | Chi sq, p= 0.35 |
| Insomnia, n (%) | 20 (80%)* | 19(50%) | Chi sq, p= 0.02 |
| Fatigue, n (%) | 24(96%)** | 25(66%) | Chi sq, p= 0.005 |
| Attention deficit, n (%) | 23(92%)*** | 19(50%) | Chi sq, p= 0.0005 |
| Memory deficit, n (%) | 19(76%) | 22(58%) | Chi sq, p= 0.14 |
| Myalgia, n (%) | 15(60%) | 14(37%) | Chi sq, p= 0.07 |
| Depression1, n (%) | 24(96%)*** | 13(34%) | Chi sq, p= 0.000 |
| Panic attacks, n (%) | 5(20%)* | 1(3%) | Chi sq, p= 0.03 |
| Number of post-COVID symptoms | 8.04±2.23*** | 4.84±3.50 | F(1, 61)=16.45, p=0.000 |
Data are presented as mean ± SD. Significant differences between groups: * - p<0.05, ** - p<0.01, *** - p<0.001. 1 The “depression” parameter in the table refers to self-reported depression as reported by participants on the questionnaire, as opposed to depression diagnosed by a psychiatrist.
Table 3.
The results of psychiatric testing.
| Test | Parameter | Control | PCD | noPCD |
|---|---|---|---|---|
| HDRS | Hamilton score | 4.0±3.40 | 18.36±3.66 *** ### | 6.11±3.52 * |
| HADS | Anxiety | 4.42±2.41 | 10.84±3.25 *** ### | 5.32±3.59 *** |
| Depression | 3.47±2.44 | 10.36±4.78 *** ### | 4.05±2.89 *** | |
| Total score | 7.89±3.75 | 21.04±7.40 *** ### | 9.18±4.73 *** |
Data are presented as mean±SD. Significant differences relative the Control group: * - p<0.05, ** - p<0.01, *** - p<0.001. Significant differences between the PCD and noPCD groups: # - p<0.05, ### - p<0.001.
Table 4.
The factor structure in relation to the MPF percentage changes in post-COVID patients.
| Factor | Eigenvalue | % Total Variance | Cumulative % | Brain structures with scores > 0.7 |
| Factor 1 | 55.77 | 48.50 | 48.50 | Anterior, Superior, and Posterior CR (L+R); Genu, Body, and Splenium of CC (L+R); Posterior thal. rad.(L+R); Tapetum (L+R); SLF (L+R); Superior Frontal WM (L+R); Inferior Frontal WM (L); Superior Parietal WM (L+R); Middle Occipital WM (R); Superior Occipital (L); Middle Temporal WM (R) |
| Factor 2 | 8.84 | 7.69 | 56.19 | CST (L+R); Cerebral peduncle (L+R); Medial lemniscus (L+R); Pontine crossing tract (L+R); Inferior, Superior, and Middle CP (L+R); Midbrain, Pons, Medulla |
| Factor 3 | 4.92 | 4.28 | 60.46 | Middle Fronto-Orbital (R); Rectus (L+R) |
| Factor 4 | 4.20 | 3.65 | 64.12 | Amygdala (L+R) |
| Factor 5 | 3.26 | 2.83 | 66.95 | Cuneus (R) |
| Factor 6 | 2.85 | 2.48 | 69.42 | Globus Pallidus (R); Putamen (R) |
| Factor 7 | 2.49 | 2.16 | 71.584 | IFOF (L+R); Uncinate fasciculus (L+R) |
| Factor 8 | 2.22 | 1.93 | 73.52 | Entorhynal area (L) |
| Factor 9 | 2.01 | 1.75 | 75.27 | Caudate Nucleus (L+R) |
| Factor 10 | 1.94 | 1.68 | 76.95 | Fusiform WM (L) |
| Factor 11 | 1.75 | 1.52 | 78.48 | Pre-cuneus WM (R) |
| Factor 12 | 1.60 | 1.39 | 79.87 | Lingual WM (L) |
| Factor 13 | 1.40 | 1.21 | 81.08 | Postcentral WM (L+R) |
| Factor 14 | 1.31 | 1.14 | 82.23 | Hippocampus (R+L) |
| Factor 15 | 1.28 | 1.11 | 83.34 | - |
| Factor 16 | 1.20 | 1.04 | 84.38 | FX column and body (L) |
| Factor 17 | 1.16 | 1.01 | 85.39 | Middle Fronto-Orbital (R) |
| Factor 18 | 1.09 | 0.95 | 86.34 | - |
| Factor 19 | 1.08 | 0.94 | 87.28 | - |
Table 5.
The parameters of multiple regressions predicting Hamilton scores in post-COVID patients.
| Parameter | Total | PCD | noPCD | |||
|---|---|---|---|---|---|---|
| Multiple R | 0.64 | 0.82 | 0.36 | |||
| Multiple R2 | 0.41 | 0.68 | 0.123 | |||
| F | 20.53 | 10.53 | 5.24 | |||
| p | 0.0000 | 0.0000 | 0.0281 | |||
| Variables in the model | β coefficient | p | β coefficient | p | β coefficient | p |
| Number of acute symptoms | 0.48 | 0.0016 | ||||
| Number of post-COVID symptoms | 0.56 | 0.0000 | 0.36 | 0.0281 | ||
| Factor 7 | -0.34 | 0.0010 | -0.58 | 0.0002 | ||
| Factor 15 | -0.40 | 0.0068 | ||||
| Factor 12 | 0.29 | 0.0393 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



