
Submitted:
10 December 2023
Posted:
12 December 2023
You are already at the latest version
Abstract
Aim. The analysis of incidence, clinical and morphological manifestations, and the prognosis of IgA nephropathy in the Northeastern Europe (NEE). Materials and methods. We enrolled cases with primary IgA nephropathy (IgAN) from 2005 to 2020 in the single-center retrospective study. Demographic and clinical parameters, histology data, and the treatment were analyzed. The outcomes were the occurrence of complete (PR) or partial remission (CR), renal replacement therapy (RRT), eGFR<15 ml/min/1.73m2 and eGFR decrease ≥ 50%. The composite endpoint included all renal outcomes and was used to evaluate the risk of IgAN progression and associated factors. Results. The incidence of IgAN cases was 23.6% of all indication biopsies and 41.2% of primary immune glomerulopathies. At the time of the kidney biopsy, the proteinuria was 2.5 (1.5-5.0) g/24h, eGFR - 69 ± 32 ml/min/1.73 m2. Proportions of cases with arterial hypertension and eGFR <60 ml / min / 1.73 m2 were 75% and 36%, respectively. The prevalence of histological changes in accordance with the Oxford (MEST-C) classification was M1 - 40.5%, E1 -22.9%, S1-70.2%, T1-22%, T2 - 9%, C1-16.7%, C2 - 4.4%. In the follow-up of 27 (11; 61) months, 6 deaths occured (1.7%). The 10-year cumulative dialysis-free survival was 80% and progression-free survival was 56%. Remissions registered in 50% of cases, being more frequent in patients who received immunosuppression vs renoprotection (60% vs. 40%, p = 0.001). In multivariable Cox regression, the independent factors associated with the increased probability of IgAN progression were male gender, a younger age, higher blood pressure and hematuria, lower eGFR, interstitial fibrosis/ tubular atrophy (≥50%), the presence of peritubular capillaritis and any crescents. Compared to the cohorts of other ethnic or geographical origin, IgAN in the studied cohort were found to have more severe clinical and morphological presentations and faster progression rate. Conclusion. Being the most common glomerulopathy in the NEE population, IgAN has more pronounced clinical and morphological presentations. Considering the distinctive features of the disease, further research is warranted in order to establish approaches for enhancing risk stratification and treatment efficacy.
Keywords:
Immunoglobulin A nephropathy
; Northeastern Europe
; clinical manifestations
; morphology
; renal survival
; progression
; prognosis
; associated factors
1. Introduction
Immunoglobulin A nephropathy (IgAN) is the most common immune glomerulopathy worldwide [1]. The disease represents specific damage to the kidney due to alterations in the mucosal immune response. A critical factor underlying the disease progression is the occurrence of minor molecular rearrangements within the hinge region of secretory immunoglobulin A1 (IgA1) [2,3]. These rearrangements result in a deficiency of galactosylation in the O-glycan structure, consequently causing conformational changes in the molecule and leading to the acquisition of autoantigenic properties [4]. A prerequisite for hyperproduction of galactose-deficient IgA1 (Gd-IgA1) is the activation of mucosa associated lymphoid tissue (MALT) immune response and impaired IgA1 secretion [5,6]. Increased circulating pool of Gd-IgA1 leads to the formation of immune complexes (IC). The latter comprises anti-glycan autoantibodies represented by either class of immunoglobulin (IgG, IgA or IgM) targeting Gd-IgA1, and CD89 (FcαRI) and complement [7,8]. Gd-IgA1-containing IC cannot undergo natural clearance in hepatocytes [9], leading to its glomerular deposition, mainly in the mesangial area. An interaction with CD71, transferrin receptor on mesangial cells, causes their proliferation with subsequent activation of the complement and inflammation, which associated with organ damage and formation of a typical morphological pattern of the disease [10,11].
The prevalence, clinical and morphologic manifestations, and prognosis of IgA-nephropathy have significant geographic and racial differences [12,13,14,15,16]. Long-term clinical observations of the course of IgA-nephropathy cases enabled us to assume that the disease in the Northeastern Europe (NEE) population may have considerable peculiarities of incidence, clinical and morphologic manifestations, and prognosis. To explore this hypothesis, we conducted the initial extensive large-scale study of IgAN in this specific geographical location.
2. Materials and Methods
2.1. Study design
Cases diagnosed with primary IgA nephropathy at the Renal Clinic of the Research Institute of Nephrology, Pavlov University in the period from 01.05.2005 to 01.08.2020, were enrolled in this retrospective single-centre cohort study with unrestricted criteria at entry. This clinic is a major renal centre serving Northwest Russia with a population of about 18 million since 1987. A brief scheme of the study design is presented in Figure 1.
2.2. Baseline data at the time of kidney biopsy
Demographic and clinical data
The following parameters were recorded at the time of diagnosis: sex, age, height, body mass index (BMI), estimated glomerular filtration rate (eGFR), erythrocyturia, daily proteinuria (DP), serum albumin, total serum IgA, serum C3- and C4- complement fractions, systolic, diastolic and mean arterial blood pressure (ABP), and the presence of nephrotic syndrome (NS). NS was defined at DP >3.5 g/day and serum albumin <30 g/l. The clinically significant chronic infection of mucous membranes of various localizations was also recorded: upper and lower respiratory, gastrointestinal (GI), urinary and genital. We also collected the data on the clinical manifestations of the disease and the period elapsed until the verification of the diagnosis.
Histologic data
The light microscopy and immunomorphology data were analysed. For light microscopy, we used 4-6 μm thick tissue sections and standard stainings (PAS, trichome, haematoxylin-eosin and silver-methenamine) [17]. The prevalence of histologic changes of various structures within the area of the kidney biopsy specimen was evaluated. The global and segmental glomerular sclerosis, cellular, fibro-cellular and fibrous crescents were evaluated quantitatively (as a percentage of the total number of glomeruli in the biopsy specimen). We used a semi-quantitative assessment of interstitial fibrosis and tubular atrophy (IFTA), interstitial inflammation and peritubular capillaritis (PTC) (grade 0, <5%; grade 1, 6-24%; grade 2, 25-49%; grade 3, ≥50%). At immunofluorescence studies, the intensity of glomerular and extra glomerular deposits of immunoglobulins G, M, A, C3-component of complement (C3) and fibrinogen was also evaluated semi-quantitatively in scores from 0 to 3.
Histologic alterations were also evaluated according to the Oxford classification [18,19]: mesangial proliferation (M0, <50% of the tubules; M1, >50% or more), endocapillary proliferation (E0 - absent, E1 - present) and segmental sclerosis or adhesion of capillary loops to the tubular capsule (S0 - absent, S1 - present), tubular atrophy/interstitial fibrosis ( T0, < 25% of cortical area; T1, 26-50% of cortical area; T2, > 50% of cortical area; cellular or fibro-cellular crescents (C0 - none; C1, < 25% of the tubules; C2, ≥ 25% of the glomeruli).
2.3. Follow-up and outcomes
Dynamic clinical data
The changes in DP, erythrocyturia, serum albumin and eGFR were evaluated at follow-up.
Therapy
We registered the data on tonsillectomy and pharmacological therapies, including angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers and immunosuppressive therapies (IST) using corticosteroids, cyclosporine, cyclophosphamide (CP), mycophenolic acid (MMF), and azathioprine.
Outcomes
The outcomes were all-cause death, end-stage kidney disease (ESKD) with eGFR<15 ml/min/1.73 m2, start of renal replacement therapy (RRT), and decrease of eGFR ≥50% of baseline. Disease progression was assessed by a composite endpoint that included all renal outcomes. At the end of follow-up, we assessed complete or partial remissions of the disease. Complete remission was defined as DP <0.5 g/day and erythrocyturia <5 cells in the field of view (FOV). Partial remission was defined as proteinuria decrease by >50% of the baseline level with its absolute value <3.5 g/day, provided that haematuria regressed by at least 70% from baseline.
2.4. Statistical analysis
Frequencies (fractions, percentages) were used for descriptive statistics of qualitative variables. Continuous variables were expressed as mean with its standard deviation (M±SD) or as median with interquartile range (Me (25%;75%)), depending on the variable distribution. Intergroup differences were evaluated using Student’s t-test, Mann-Whitney U-test, Pearson’s χ2 test, and analysis of variance. Spearman’s correlation analysis was used to assess the relationships between the study parameters. The cumulative proportions of survivors who reached a particular outcome were calculated by the Kaplan-Meier method with the assessment of intergroup differences by the Mantel-Cox criterion. Cases that reached the outcome were included in the analysis as complete observations, and other cases were censored at the end of the observation period. Univariable and multivariable Cox regression models were used to analyze the associations of the studied parameters with the probability of outcome. For subsequent use in multiple regression, independent variables (baseline clinical and morphologic indices) were pre-selected in the univariable analysis. First, applying univariable Cox models, we selected clinical variables with a p-value <0.05 for the regression coefficient. Second, only these clinical variables were included in the multiple regression model to identify those independently associated with the probability of outcome. Next, we selected morphological indices by including each of them in a regression models adjusted for a set of previously identified independent clinical factors. Finally, we constructed a regression model by the inclusion of all pre-selected clinical and morphological variables. For the final model building, we used variable stepwise exclusion and bootstrapping procedures. Variables with skewed distribution could be logarithmically transformed before inclusion in the analysis. Differences, correlation, or regression coefficients were considered significant at p-values <0.05. Statistical analyses were performed using SPSS 20.0 software (IBM Corporation, Armonk, NY, USA) and R programming software (version 4.3.1).
3. Results
The prevalence of IgAN cases among all indication biopsies and morphologically confirmed primary immune glomerulopathies was 23.6% and 41.2%, respectively.
3.1. Clinical presentation
The IgAN patients were predominantly of male sex and young in age, and the disease expectedly manifested with urinary abnormalities and/or episodes of macro haematuria. The median period from the first symptoms to kidney biopsy was 3.4 years. At the baseline, most of the patients had significant erythrocyturia and proteinuria. Nephrotic syndrome was registered in nearly every tenth case. One third of patients had eGFR level <60ml/min/1.73m2. The serum complement and total IgA mainly corresponded to the reference values. A significant proportion of patients had clinically evident chronic mucosal inflammatory diseases. Arterial hypertension was also prevalent for the analysed cohort (Table 1).
Histology of IgA nephropathy
Light microscopy showed a high prevalence of glomerular fibroplastic alterations, tubular atrophy and interstitial fibrosis. Among inflammatory lesions, diffuse mesangial proliferation was detected more frequently, followed by endocapillary hypercellularity and crescents. Among the histologic changes not included in the Oxford criteria, a significant incidence of interstitial infiltration and PTC was noticeable (Table 2).
Mesangial deposits of IgA and C3 could be combined with their deposits in the glomerular capillary walls and, less frequently, in small arteries and peritubular capillaries. Co-deposition of IgA and IgM was a typical finding in the study cohort, with a smaller proportion of cases having both IgA and IgG positivity at immunofluorescence. Deposits of C3 and fibrinogen were infrequently found extraglomerularly (Table 3).
Clinical and morphologic correlations
Correlations between major clinical and histologic indices are represented in the Table 4. Haematuria, a typical clinical sign of the disease, was associated with histologic indices of active glomerular and interstitial inflammation. Proteinuria and eGFR had significant correlations with all major histologic alterations, both fibroplastic and inflammatory. Mean BP was positively associated with IFTA, endocapillary hypercellularity, interstitial inflammation, and PTC. The intensity of IgA and C3 deposits in glomerular capillary walls and peritubular vessels correlated with proteinuria, but not with haematuria (Table 4).
3.2. Follow-up and outcomes
Overall and renal survival
Patients with follow-up differed significantly from cases without follow-up in a number of clinical and morphologic manifestations of IgAN: severity of proteinuria and haematuria, eGFR level, prevalence of NS, segmental glomerulosclerosis, endo- and extracapillary proliferation (Table S1).
The median follow-up period was 27 (11; 61) months. Median annual decrease in e GFR was -2.3 (-11.4; -1.9) ml/min/1.73m2. A total of 6 all-cause deaths (1.7%) were registered. During the follow-up period, 72 patients (17.9%) reached the composite endpoint, of which dialysis was initiated in 47.2%. The cumulative dialysis-free and progression-free survival probabilities are shown on Figure 1 (A, B).
Treatment and remissions
Most patients (95%) were treated with renin-angiotensin system blockers according to current guidelines [20]. IST was administered to 29% of patients. Steroids monotherapy or steroids in combination with other immunosuppressants, mainly cyclophosphamide, MMF and azathioprine, were used in 23% and 9% of patients, respectively. The proportion of cases on IST in those with follow-up (n=403) was 46% (steroids monotherapy - 31%, combined IST - 15%). By the end of follow-up, we registered remissions in 50% of cases: PR in 26%, CR in 24%. Remissions were observed more frequently in patients who received IST compared to those on symptomatic therapy (60% vs. 40%, p=0.001), including CR (31% and 16%) and PR (29% and 24%).
Notwithstanding a higher remission rate, renal survival did not differ between the groups of patients who did not receive and those who received IST (Figure 3C). However, the group of patients undergone IST had more pronounced clinical and morphologic manifestations of IgAN. These differences were related to proteinuria and NS, as well as fibrous and proliferative alterations of the glomeruli and interstitium (Table S2).
3.3. Factors associated with prognosis
Comparative analysis showed significant differences between cases with progression of IgA nephropathy compared with patients who did not reach the composite prognostic endpoint for many of the clinical and morphologic parameters studied (Table S3).
In a Cox regression model, including only clinical variables at the time of biopsy, sex, age, mean ABP, eGFR, and severity of haematuria were independently associated with the risk of IgAN progression. Among morphologic indices, severe IFTA (T2), PTC, interstitial infiltration, the presence of any crescents, and the proportion of global glomerulosclerosis were significantly associated with the probability of reaching the composite end-point. In the final model using both clinical and morphologic parameters, the independent factors associated with a negative prognosis were male sex, younger age, increased mean BP, lower eGFR, higher haematuria, IFTA ≥50%, severe PTC, and the presence of any crescents. No other parameters had an independent association with the risk of IgAN progression (Table 5).
4. Discussion
There is a notable disparity in the prevalence of IgAN among various regions and ethnicities, characterised by a geographical gradient from the Southwest to the Northeast [1,12,21,22]. The disease is most prevalent in people of East Asia ancestry (45–58% of primary glomerulonephritis), followed by Caucasians and relatively rare in individuals of African descent. It has been estimated to account for approximately 40% of all native biopsies in Japan, 25% in Europe, 12% in the USA and less than 5% in Central Africa [1,21,22,23,24].
Here, we present the first cohort study that has provided detailed information on the clinical, morphologic, and prognostic aspects of IgAN in NEE, assuming higher frequency and more severe course. Indeed, we demonstrated that IgAN was the most frequent variant of immune glomerulopathies and the most prevalent kidney disease by clinical and morphologic examination in this region. Moreover, the prevalence of IgAN in NEE seems to be ahead of most regions in Europe and America and comparable to Asian countries [1,16,21,22,23,25,26].
Clinical manifestations of IgAN were expectedly represented by a combination of proteinuria and haematuria. However, the studied IgAN cohort differed from the European and Asian cohorts in the severity of urine protein loss, renal dysfunction, and hypertension. Compared to European data, histologic lesions associated with active inflammation were also more pronounced in the study cohort [16] (Table S4).
Diagnosis of IgAN is established by the presence of immunoglobulin A1 (IgA1) as the dominant or co-dominant immunoglobulin in the glomerular mesangium [18,19]. While the mesangial IgA deposition is a defining disease feature, we found no associations of mesangial IgA staining with the clinical indices of the disease severity (see Table 4). One might suggest that distinct processes are being responsible for mesangial IgA deposition and glomerular inflammation.
Contrariwise, IgA deposits in the glomerular capillary walls, detected in one of six cases, correlated to proteinuria, ABP and eGFR levels, likely mirroring the course of more severe forms of the disease with the formation of a membranoproliferative pattern [32] and worse prognosis [33].
In addition, we found the significant prevalence of extra-glomerular changes in IgAN. In particular, the significance of interstitial inflammation and peritubular capillaritis was apparent. Both lesions closely correlated with hypertension, renal dysfunction, proteinuria and haematuria, the major clinical manifestations. The interaction of immunocytes with peritubular capillary walls, along with occasionally detectable deposits of IgA, C3, and fibrinogen may indicate that a proportion of IgAN cases had with histologic features of renal-limited interstitial vasculitis. Such patients may have an unfavourable prognosis, as PTC was identified as an independent factor associated with the higher probability of disease progression (see Table 5).
IgAN has often been considered a disease with a benign prognosis. Such perceptions have been largely based on large cohort studies conducted in Asia, where the 10- and 20-year renal survival rates in these studies are 82-84% and 64-70%, respectively [1,13,14,15,34,35]. Contrariwise, the pooled European data in multicenter retrospective VALIGA study [16] showed significantly lower survival rates (see Table S4), suggesting a less favourable course of the disease in the Caucasian population. Our data definitely showed that dialysis-free survival in the NEE population is lower than in Asian regions. A cumulative rate of disease progression (ESKD, RRT or decrease in eGFR>50%) was also inferior compared to the European population [16].
The likely explanation for such findings could be the delayed recognition of IgAN, acquiring a more pronounced glomerular and tubulointerstitial fibrotic lesions [21,22]. However, there were no apparent differences in the prevalence of glomerulosclerosis and IFTA in both cohorts (Table S4). Therefore, given the comparable treatment [16], these data could suggest a more aggressive course of the disease in the NEE region (Table S4). Therefore, given the comparable treatment [16], these data could suggest a more aggressive course of the disease in the NEE region.
Our study was also focused on the evaluation of clinical and morphologic factors associated with the IgAN outcomes. Among the major clinical indices, proteinuria is considered a significant predictor of IgAN prognosis and treatment [13,16]. However, in this study, baseline proteinuria was not an independent predictor of IgAN progression. One explanation could rely on the small proportion of cases in our cohort with proteinuria <1 g/day known to be associated with a more favourable prognosis [38,39]. A link between proteinuria and the progression of IgAN is thought to be influenced by a range of histological alterations that also exhibit strong correlations with urinary protein loss (see Table 4).
In addition, baseline proteinuria and histologic indices of current disease activity can be modified by therapy [16,40,41]. Consequently, an average proteinuria during in follow-up period seems to be more important for predicting IgAN outcomes [16,42]. Next, in the patients with higher proteinuria, one can also assume that other clinical and morphologic parameters have a greater prognostic value. Particularly, this refers to haematuria that was independently related to IgA progression, consistent with prior data [42]. Judging by the close relationship with histologic and clinical activity indices (see Table 4), haematuria seemed to be a significant biomarker of disease activity, requiring clinical monitoring at the background of therapy.
In our study, the prognostic value of the Oxford classification indices (MEST-C [18,19]) differed significantly from the original data and the results of validation studies [35,43,44,45,46,47,48]. Of these, only IFTA was significantly associated with long-term prognosis in models adjusted for baseline clinical parameters and treatment. Consequently, we do not exclude that the MEST-C classification may be of limited use in patients with higher proteinuria levels, which exceeded 1 g/day in almost ¾ of cases of the entire cohort.
Like several other studies [49,50,51], we have found independent and significant associations with prognosis for some morphologic indices not included in the MEST-C classification. Among them, are PTC and the occurrence of any crescents in the renal biopsy. It is likely that further development of the MEST-C classification, along with clarification of the prognostic value of other histologic changes [52], will allow a more accurate assessment of IgAN prognosis. So far, our findings leave open the issue on the reliability of using MEST-C for predicting the IgAN outcomes [38,53,54,55,56,57] in the NEE population, requiring additional validation studies.
The substantial prevalence, severity of course and unfavourable prognosis of IgAN in NEE suggest the existence of predisposing specific, yet unknown, population-level factors. Future research should be focused on assessments of genetic predisposition and environmental factors, including dietary patterns and infections affecting the mucosal immune system [27,28,29,36,37].
This retrospective study was not designed to analyse the efficacy of currently recommended therapies [20]. As the natural evolution of clinical and morphologic manifestations of IgAN can be influenced by treatment [42,58,59,60,61,62,63,64,65], we accounted for treatment in the construction of regression models.
Almost half of the patients in the analyzed cohort received some variant of IST. In the analysis of outcomes and associated factors, there were no differences in renal survival between patients receiving symptomatic therapy alone (based on renin-angiotensin system blockers) and its combination with IST. The subgroup of patients receiving IST had significantly more severe clinical and morphological manifestations of IgA nephropathy, having a less favourable prognosis. These observations probably do not mirror the ineffectiveness of immunosuppression in IgAN, however, further studies appropriately designed for the high-risk disease are warranted.
Short-term efficacy of treatment is assessed by the development of remission, an important modifier of prognosis (39). Within the follow-up period, complete or partial remissions were reported in 50% of cases and occurred more frequently in patients on IST compared to symptomatic renoprotection. These data are consistent with the results of prospective studies, where remission rates on IST were only 25 - 62% (including complete remissions of 7.8 - 55.3%) [63,64,65,66,67,68,69]. Notably, we applied a more strict definition of remission, including the regress of haematuria beyond the fall in urine protein. Haematuria, a hallmark of IgAN, correlated mostly with active inflammatory lesions. The persistence of proteinuria may resulted from either active disease or glomerular and tubulointerstitial fibrosis. Haematuria can help to separate the latter cases, avoiding unnecessary IST. Moreover, urine blood cell count
Overall, the unsatisfactory remission rate in IgAN definitely calls for an intensification of research on approaches to therapy of IgAN. Beyond IST, these approaches should be focused on targeting the known nodal hits of the disease pathogenesis [27,28,29,59].
The main limitation of the study was its retrospective nature. This did not allow to determine causal relationships between clinical and morphologic parameters and disease outcomes. Next, patients with follow-up had more pronounced clinical and morphologic manifestations at the baseline. As a result, the renal survival may be underestimated, because it was estimated for a group of patients at higher risk of progression. Furthermore, the relatively small number of cases that reached the endpoint precluded multivariable analysis of potential prognostic predictors in groups with different therapies, which can significantly affect the prognostic impact of morphologic and clinical parameters [58]. However, to reduce potential bias, all prognostic models were adjusted for IST.
5. Conclusions
The present study showed that in NEE population IgAN is the most common glomerulopathy. The disease is characterized by more severe clinical and morphological manifestations and a faster progression compared to cohorts of other ethnicities or geographic regions. Considering specific features of a disease in NEE, additional research is required to ascertain approaches to the risk stratification and effective treatment.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1. Clinical and morphological data in patients with and without follow-up; Notes: ABP - arterial blood pressure; eGFR - estimated glomerular filtration rate; M1 - mesangial proliferation ≥50%; E1 - endocapillary hypercellularity; S1 - segmental sclerosis/adhesions; C1 - cellular/fibrocellular crescents <25%; C2 - cellular/fibrocellular crescents≥25%; values are presented as fractions/percentages or as mean with its standard deviation (M±SD) or as median with interquartile range (25%;75%); Table S2. Clinical and demographic parameters in patients who received and not received immunosupression in the follow-up period; Notes: ABP – arterial blood pressure; eGFR – estimated glomerular filtration rate; IgA – immunoglobulin A; RASB – renin-angiotensin system blockers; PTC –peritubular capillaritis; M1 – mesangial proliferation ≥50%; E1 – endocapillary hypercellularity; S1 – segmental sclerosis/adhesions; C1 – cellular/fibrocellular crescents <25%; C2 – cellular/fibrocellular crescents ≥25%; IST – immunosuppressive therapy; values are presented as fractions/percentages or as mean with its standard deviation (M±SD) or as median with interquartile range (25%;75%); Table S3. Clinical and morphological data in patients with and without progression of IgA-nephropathy; Note: BP – blood pressure, eGFR – estimated glomerular filtration rate, M1 – mesangial proliferation ≥50%; E1 – endocapillary hypercellularity; S1 – segmental sclerosis/adhesions; T1 – tubular atrophy/interstitial fibrosis 26-50% of the cortical area, T2 – tubular atrophy/interstitial fibrosis >50% of the cortical area, C – cellular and fibrotic-cellular crescents; C1 – cellular/fibrotic-cellular crescents <25%; C2 – >25% of the tubules, PTC – peritubular capillaritis; RASB – renin-angiotensin system blockers; values are presented as fractions/percentages or as mean with its standard deviation (M±SD) or as median with interquartile range (Me (25%;75%)); Table S4. Clinical and morphological presentation of IgAN in Northeastern Europe and other world regions; Note: eGFR – estimated glomerular filtration rate, ND – no data; values are presented as fractions/percentages or as mean with its standard deviation (M±SD) or as median with interquartile range (Me (25%;75%)); *, n=403; superscripts are references to original studies.
Author Contributions
conceptualization, methodology, T.M., V.D., Z.K., E.B.; formal analysis, T.M., V.D.; resources, E.B., V.D.; data curation, Z.K.; writing—original draft preparation, V.D., T.M., Z.K., E.B.; writing—review and editing, V.D.; visualization, T.M., Z.K., E.B.; supervision, V.D.; project administration, V.D.; funding acquisition, V.D., E.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Russian Science Foundation, grant number 23-15-00510.
Institutional Review Board Statement
The study protocol was approved by the local Ethics Committee of Pavlov University (Project identification code №250, June 28, 2021).
Informed Consent Statement
Not applicable.
Data Availability Statement
All data presented in this study are available from the corresponding author on reasonable request.
Conflicts of Interest
V.D. has received consulting fees from AstraZeneca, Bayer and honoraria for lectures from AstraZeneca, CSL Vifor, Novartis, Bayer. Other authors declare no conflict of interest. The funders had no role in the design of the study, in the collection, analysis, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
References
- Schena FP, Nistor I. Epidemiology of IgA Nephropathy: A Global Perspective. Semin Nephrol 2018; 38: 435 – 442. [CrossRef]
- Reily C, Ueda H, Huang ZQ et al. Cellular Signaling and Production of Galactose-Deficient IgA1 in IgA Nephropathy, an Autoimmune Disease. Journal of Immunology Research 2014. [CrossRef]
- Hiki Y, Odani H, Takahashi M et al. Mass spectrometry proves under-O-glycosylation of glomerular IgA1 in IgA nephropathy. Kidney Int. 2001 Mar; 59(3): 1077 – 1085. [CrossRef]
- Tomana M, Novak J, Julian B et al. Circulating immune complexes in IgA nephropathy consist of IgA1 with galactose-deficient hinge region and antiglycan antibodies. J Clin Invest. 1999 Jul; 104 (1): 73 - 81. [CrossRef]
- Boyaka, PN. Inducing Mucosal IgA: A Challenge for Vaccine Adjuvants and Delivery Systems. J Immunol 2017; 199: 9 - 16. [CrossRef]
- Muto M, Manfroi B, Suzuki H et al. Toll-Like Receptor 9 Stimulation Induces Aberrant Expression of a Proliferation-Inducing Ligand by Tonsillar Germinal Center B Cells in IgA Nephropathy. J Am Soc Nephrol 2017; 28 (4): 1227 – 1238. [CrossRef]
- Robert T, Berthelot L, Cambier A et al. Molecular Insights into the Pathogenesis of IgA Nephropathy. Trend Mol Med. 2015; 12: 762 – 775. [CrossRef]
- Ben Mkaddem S, Benhamou M, Monteiro RC. Understanding Fc Receptor Involvement in Inflammatory Diseases: From Mechanisms to New Therapeutic Tools. Front Immunol. 2019; 10: 1 - 12. [CrossRef]
- Novak J, Julian BA, Tomana M et al. IgA Glycosylation and IgA Immune Complexes in the Pathogenesis of IgA Nephropathy. Semin Nephrol 2008; 28 (1): 78 – 87. [CrossRef]
- Wyatt RJ, Julian BA. IgA Nephropathy. N Engl J Med 2013; 368: 2402 - 2414. [CrossRef]
- Novak J, Tomana M, Matousovic K, et al. IgA1-containing immune complexes in IgA nephropathy differentially affect proliferation of mesangial cells. Kidney Int. 2005; 67: 504–513. [CrossRef]
- Kiryluk K, Li Y, Sanna-Cherchi S et al. Geographic Differences in Genetic Susceptibility to IgA Nephropathy: GWAS Replication Study and Geospatial Risk Analysis. PLoS Genet 8(6): e1002765. [CrossRef]
- Moriyama T, Tanaka K, Iwasaki C et al. Prognosis in IgA Nephropathy: 30-Year Analysis of 1,012 Patients at a Single Center in Japan. PLOS ONE 2014; 9 (3). [CrossRef]
- Lee H, Kim DK, Oh KH et al. Mortality of IgA Nephropathy Patients: A Single Center in Korea. Experience over 30 Years. PLoS ONE 7(12): e51225. [CrossRef]
- Le W, Liang S, Hu Y et al. Long-term renal survival and related risk factors in patients with IgA nephropathy: results from a cohort of 1155 cases in a Chinese adult population. Nephrol Dial Transplant 2012; 27: 1479–1485. [CrossRef]
- Coppo R, Troyanov S, Bellur S et al. Validation of the Oxford classification of IgA-nephropathy in cohorts with different presentations and treatments. Kidney Int. 2014; 86: 828–836. [CrossRef]
- Roberts, IS. Pathology of IgA nephropathy. Nat. Rev. Nephrol 2014; 10: 445 – 454. [CrossRef]
- Cattran DC, Coppo R, Cook HT et al. The Oxford classification of IgA nephropathy: rationale, clinicopathological correlations, and classification. A Working Group of the International IgA Nephropathy Network and the Renal Pathology Society. Kidney Int. 2009; 76(5): 534 - 545. [CrossRef]
- Trimarchi H, Barratt J, Cattran DC et al. IgAN Classification Working Group of the International IgA Nephropathy Network and the Renal Pathology Society; Conference Participants. Oxford Classification of IgA nephropathy 2016: an update from the IgA Nephropathy Classification Working Group. Kidney Int. 2017; 91(5): 1014 - 1021. [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int. 2021 Oct;100(4S):S1-S276. [CrossRef]
- Yeo SC, Goh SM, Barratt J. Is immunoglobulin A nephropathy different in different ethnic populations? Nephrology (Carlton). 2019 Sep;24(9):885-895. [CrossRef]
- Zhang Z, Zhang Y, Zhang H. IgA Nephropathy: A Chinese Perspective. Glomerular Dis. 2021 Oct 12;2(1):30-41. PMID: 36751266; PMCID: PMC9677733.). [CrossRef]
- Lee M, Suzuki H, Nihei Y, Matsuzaki K, Suzuki Y. Ethnicity and IgA nephropathy: worldwide differences in epidemiology, timing of diagnosis, clinical manifestations, management and prognosis. Clin Kidney J. 2023 Dec 4;16(Suppl 2):ii1-ii8. [CrossRef]
- Stamellou E, Seikrit C, Tang SCW, Boor P, Tesař V, Floege J, Barratt J, Kramann R. IgA nephropathy. Nat Rev Dis Primers. 2023 Nov 30;9(1):67. [CrossRef] [PubMed]
- Chang JH, Kim DK, Kim HW, et al. Changing prevalence of glomerular diseases in Korean adults: a review of 20 years of experience. Nephrol Dial Transplant. 2009; 24(8): 2406 - 2410. [CrossRef]
- Alexander S, Varughese S, Franklin R, Roy S, Rebekah G, David VG, Mohapatra A, Valson AT, Jacob S, Koshy PM, Rajan G, Daha MR, Feehally J, Barratt J, John GT. Epidemiology, baseline characteristics and risk of progression in the first South-Asian prospective longitudinal observational IgA nephropathy cohort. Kidney Int Rep. 2020 Dec 7;6(2):414-428. [CrossRef]
- Coppo, R. The Gut-Renal Connection in IgA Nephropathy. Semin Nephrol 2018; 38(5): 504 - 512. [CrossRef]
- Zhu TT, Wang L, Wang HL et al. Helicobacter pylori participates in the pathogenesis of IgA nephropathy. Ren Fail. 2016; 38(9): 1398 – 1404. [CrossRef]
- Floege J, Feehally J. The mucosa-kidney axis in IgA nephropathy. Nat Rev Nephrol. 2016; 12(3): 147 - 156. [CrossRef]
- Heybeli C, Oktan MA et al. Clinical significance of mesangial IgM deposition in patients with IgA nephropathy. Clinical and Experimental Nephrology 2018; 23(3): 371 – 379. [CrossRef]
- Dong J, Peng T, Gao J et al. A pilot and comparative study between pathological and serological levels of immunoglobulin and complement among three kinds of primary Glomerulonephritis. BMC Immunology 2018; 19: 18. [CrossRef]
- Dobronravov VA, Smirnov AV. Etiology and clinic-morphological presentation of membranoproliferative glomerulonephritis in Russian population. Ter arh 2018; 12: 39 – 47. (In Russ.)]. [CrossRef]
- Alvarado AS, Andeen NK, Brodsky S et al. Location of glomerular immune deposits, not codeposition of immunoglobulin G, influences definitive renal outcomes in immunoglobulin A nephropathy. Nephrol Dial Transplant 2018; 33: 1168–1175. [CrossRef]
- Akio Koyama, Masaki Kobayashi. Treatment of IgA Nephropathy: Present and Future. Nephrology 1997; 3: 633 – 799.
- Zeng CH, Le W, Ni Z et al. A Multicenter Application and Evaluation of the Oxford Classification of IgA Nephropathy in Adult Chinese Patients. Am J Kidney Dis. 2012; 60: 812 - 820. [CrossRef]
- Li M, Yu X. Genetic study of immunoglobulin A nephropathy: From research to clinical application. Nephrology (Carlton) 2018; 23: 26 – 31. [CrossRef]
- Feehally J, Barratt J. The Genetics of IgA Nephropathy: An Overview from Western Countries. Kidney Dis (Basel) 2015; 1: 33 - 41. [CrossRef]
- Berthoux F, Mohey H, Laurent B et al. Predicting the Risk for Dialysis or Death in IgA Nephropathy. J Am Soc Nephrol 2011; 22: 752 - 761. [CrossRef]
- Reich HN, Troyanov S, Scholey JW et al. Remission of Proteinuria Improves Prognosis in IgA Nephropathy. J Am Soc Nephrol 2007; 18: 3177 - 3183. [CrossRef]
- Shi SF, Wang SX, Jiang L et al. Pathologic predictors of renal outcome and therapeutic efficacy in IgA nephropathy: validation of the oxford classification. Clin J Am Soc Nephrol. 2011; 6(9): 2175 – 2184. [CrossRef]
- Liu LJ, Li GT, Zhou Y et al. Clinicopathologic Features and Outcomes in Endocapillary Proliferative IgA Nephropathy. Nephron Clin Pract 2010; 115: 161 – 167. [CrossRef]
- Sevillano AM, Gutiérrez E, Yuste C et al. Remission of Hematuria Improves Renal Survival in IgA Nephropathy J Am Soc Nephrol 2017; 28(10):3089-3099. [CrossRef]
- Alamartine E, Sauron C, Laurent B et al. The Use of the Oxford Classification of IgA Nephropathy to Predict Renal Survival. Clin J Am Soc Nephrol 2011; 6: 2384 – 2388. [CrossRef]
- Yau T, Korbet SM, Schwartz MM et al. The Oxford Classification of IgA Nephropathy: A Retrospective Analysis. Am J Nephrol 2011; 34: 435 – 444. [CrossRef]
- Lee H, Sul Hee Yi, Mi Seon Seo et al. Validation of the Oxford Classification of IgA Nephropathy: A Single-Center Study in Korean Adults. Korean J Intern Med 2012; 27: 293 – 300. [CrossRef]
- Tanaka S, Ninomiya T, Katafuchi R et al. Development and Validation of a Prediction Rule Using the Oxford Classification in IgA Nephropathy. Clin J Am Soc Nephrol 2013; 8: 2082 – 2090. [CrossRef]
- Kang SH, Choi SR, Park HS et al. The Oxford classification as a predictor of prognosis in patients with IgA nephropathy. Nephrol Dial Transplant 2012; 27: 252 – 258. [CrossRef]
- Bellur SS, Roberts ISD, Troyanov S et al. Reproducibility of the Oxford classification of immunoglobulin A nephropathy, impact of biopsy scoring on treatment allocation and clinical relevance of disagreements: evidence from the Validation of IGA study cohort. Nephrol Dial Transplant 2019; 34(10): 1681 - 1690. [CrossRef]
- Rankin AJ, Kipgen D, Geddes CC et al. Assessment of active tubulointerstitial nephritis in non-scarred renal cortex improves prediction of renal outcomes in patients with IgA nephropathy. Clin Kidney J. 2018; 12: 348 - 354. [CrossRef]
- Sato R, Joh K, Komatsuda A et al. Validation of the Japanese histologic classification 2013 of immunoglobulin A nephropathy for prediction of long-term prognosis in a Japanese single-center cohort. Clin Exp Nephrol 2015; 19: 411 – 418. [CrossRef]
- Okonogi H, Kawamura T, Joh K et al. A grading system that predicts the risk of dialysis induction in IgA nephropathy patients based on the combination of the clinical and histological severity. Clin Exp Nephrol 2019; 23: 16 – 25. [CrossRef]
- Katafuchi R, Ninomiya T, Nagata M et al. Validation Study of Oxford Classification of IgA Nephropathy: The Significance of Extracapillary Proliferation. Clin J Am Soc Nephrol 2011; 6: 2806 – 2813. [CrossRef]
- Barbour SJ, Coppo R, Zhang H et al. Evaluating a New International Risk-Prediction Tool in IgA Nephropathy. JAMA Intern Med 2019; 179: 942 – 952. [CrossRef]
- Chen T, Li X, Li Y et al. Prediction and Risk Stratification of Kidney Outcomes in IgA Nephropathy. Am J Kidney Dis 2019; 74: 300 - 309. [CrossRef]
- Xie J, Kiryluk K, Wang W et al. Predicting Progression of IgA Nephropathy: New Clinical Progression Risk Score. PLoS ONE 2012; 7: e38904. [CrossRef]
- Goto M, Wakai K, Kawamura T et al. A scoring system to predict renal outcome in IgA nephropathy: a nationwide 10-year prospective cohort study. Nephrol Dial Transplant 2009; 24: 3068 – 3074. [CrossRef]
- Bartosik LP, Lajoie G, Sugar L et al. Predicting progression in IgA nephropathy. Am J Kidney Dis 2001; 38: 728 – 735. [CrossRef]
- Soares MFS, Roberts ISD. Histologic Classification of IgA Nephropathy: Past, Present, and Future. Seminars in Nephrology 2018; 38: 477 – 484. [CrossRef]
- Coppo, R. Treatment of IgA nephropathy: Recent advances and prospects. Nephrol Ther 2018; 1: 13 – 21. [CrossRef]
- Hotta O, Furuta T, Chiba S et al. Regression of IgA nephropathy: a repeat biopsy study. Am J Kidney Dis 2002; 39: 493 - 502. [CrossRef]
- Tumlin JA, Lohavichan V, Hennigar R. Crescentic, proliferative IgA nephropathy: clinical and histological response to methylprednisolone and intravenous cyclophosphamide. Nephrol Dial Transplant 2003; 18: 1321 – 1329. [CrossRef]
- McIntyre CW, Fluck RJ, Lambie SH. Steroid and cyclophosphamide therapy for IgA nephropathy associated with crescentic change: an effective treatment. Clin Nephrol 2001; 56: 193 - 198.
- Tan L, Tang Y, Peng W et al. Combined Immunosuppressive Treatment May Improve Short-Term Renal Outcomes in Chinese Patients with Advanced IgA Nephropathy. Kidney Blood Press Res 2018; 43: 1333 - 1343. [CrossRef]
- Lv J, Wong MG, Hladunewich MA, Jha V, Hooi LS, Monaghan H, Zhao M, Barbour S, Jardine MJ, Reich HN, Cattran D, Glassock R, Levin A, Wheeler DC, Woodward M, Billot L, Stepien S, Rogers K, Chan TM, Liu ZH, Johnson DW, Cass A, Feehally J, Floege J, Remuzzi G, Wu Y, Agarwal R, Zhang H, Perkovic V; TESTING Study Group. Effect of Oral Methylprednisolone on Decline in Kidney Function or Kidney Failure in Patients With IgA Nephropathy: The TESTING Randomized Clinical Trial. JAMA. 2022 May 17;327(19):1888‐1898. PMID: 35579642; PMCID: PMC9115617. [CrossRef]
- Yang YZ, Chen P, Liu LJ et al. Comparison of the effects of hydroxychloroquine and corticosteroid treatment on proteinuria in IgA nephropathy: a case-control study. BMC Nephrology 2019; 20: 297. [CrossRef]
- Rauen T, Fitzner C, Eitner F et al. Effects of Two Immunosuppressive Treatment Protocols for IgA Nephropathy. J Am Soc Nephrol 2018; 29: 317 – 325. [CrossRef]
- Hou JH, Le WB, Chen N et al. Mycophenolate Mofetil Combined With Prednisone Versus Full-Dose Prednisone in IgA Nephropathy With Active Proliferative Lesions: A Randomized Controlled Trial. Am J Kidney Dis 2017; 69: 788 – 795. [CrossRef]
- Chen S, Qing Yin, Song Ren et al. A comparison of the effectiveness of cyclophosphamide, leflunomide, corticosteroids, or conservative management alone in patients with IgA nephropathy: a retrospective observational study. Scientific Reports 2018; 8: 13663. [CrossRef]
- Tatematsu M, Yasuda Y, Morita Y et al. Complete remission within 2 years predicts a good prognosis after methylprednisolone pulse therapy in patients with IgA nephropathy. Clin Exp Nephrol 2012; 16: 883 – 891. [CrossRef]
Figure 1.
Study design and patient selection; IgA - immunoglobulin A, RRT - renal replacement therapy, ↓ eGFR – decreased estimated glomerular filtration rate.
Figure 1.
Study design and patient selection; IgA - immunoglobulin A, RRT - renal replacement therapy, ↓ eGFR – decreased estimated glomerular filtration rate.
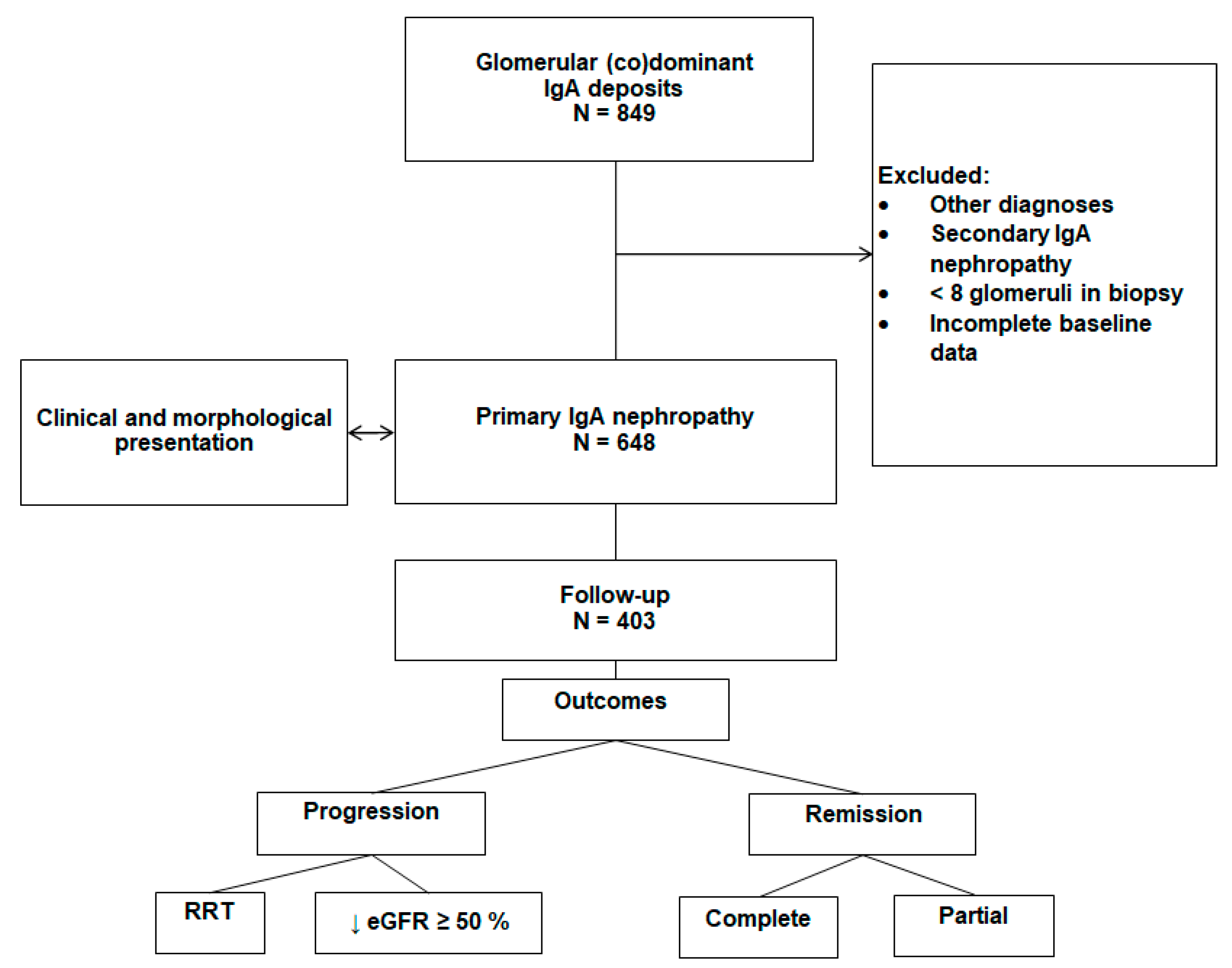
Figure 1.
Cumulative renal survival: dialysis-free survival (A); progression-free survival (В); progression-free survival who received and not received immunosuppression (C); IST - immunosuppressive therapy.
Figure 1.
Cumulative renal survival: dialysis-free survival (A); progression-free survival (В); progression-free survival who received and not received immunosuppression (C); IST - immunosuppressive therapy.
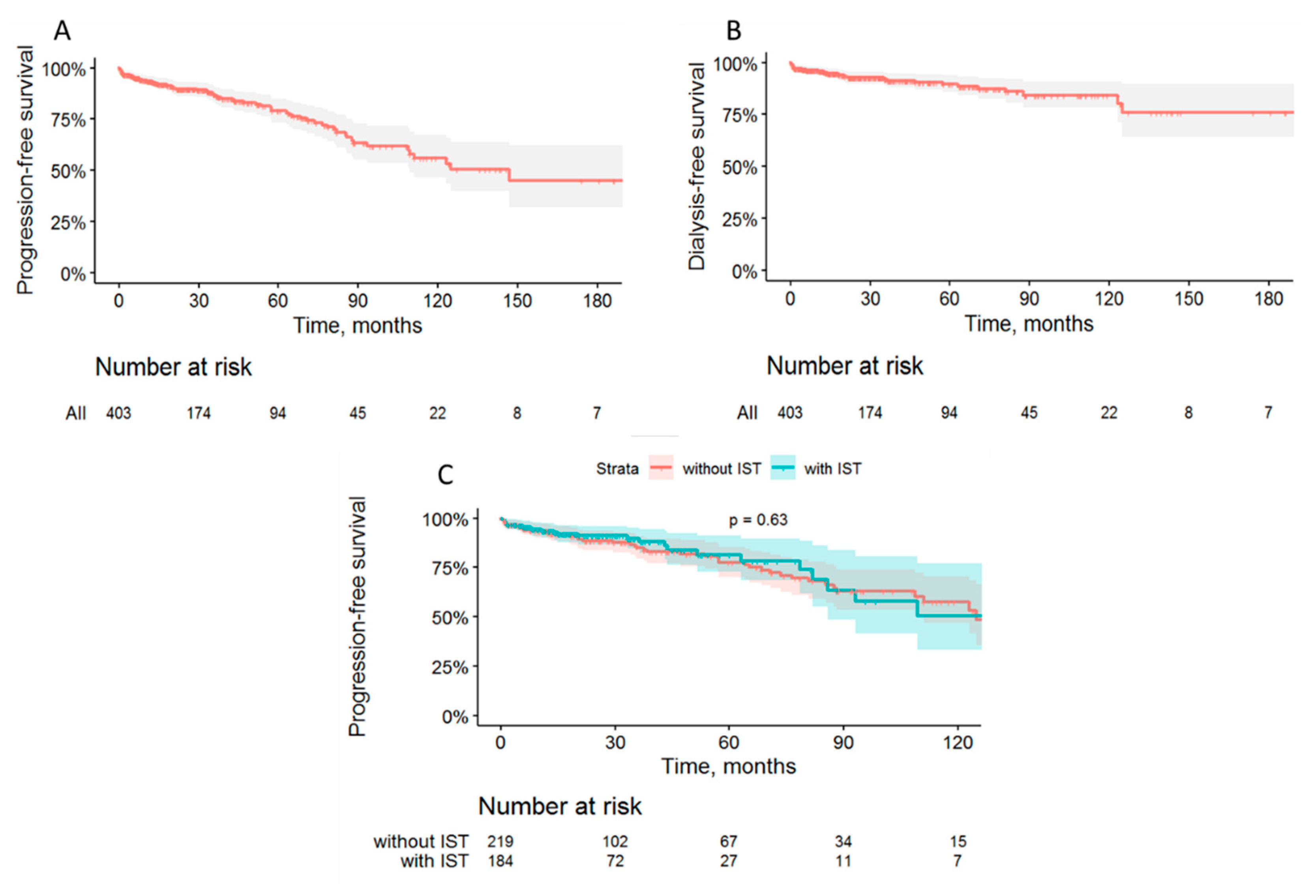

Table 1.
Baseline clinical data of IgA-nephropathy patients (n=648).
| Indicator | Value* |
|---|---|
| Age, years | 34±12 |
| male gender, % | 55 |
| BMI, kg/m2 | 25.5±5 |
| Months from first IgAN manifestations to biopsy | 41 (10;116) |
| Proteinuria, g/24h | 2.5 (1.5-5.0) |
| Proteinuria >1 g/24h, % | 76 |
| Proteinuria>3.5 g/24h, % | 30 |
| Serum albumin, g/L | 35.7±5.6 |
| Nephrotic syndrome, % | 9.3 |
| Macrohematuria before biopsy, % | 41 |
| Erythrocyturia, cells per field of view | 9 (4;19) |
| Creatinine, mmol/L | 0.106 (0.082;0.140) |
| eGFR, ml/min/1.73 m2 | 71±32 |
| CKD stages 1/2/3AB/4/5, % | 31/32/25/7/4 |
| Total serum IgA, g/L | 3.5±1.3 |
| Serum IgA elevation, % | 10.6 |
| Serum C3, g/L | 1.08±0.24 |
| Serum C4, g/L | 0.24±0.07 |
| Mean ABP (maximal), mm Hg | 116±20 |
| Mean ABP (at admission), mm Hg | 99±20 |
| Arterial hypertension, % | 75 |
| Inflammatory diseases of upper respiratory tract, % | 55 |
| Tonsillitis, % | 49 |
| Inflammatory diseases of lower respiratory tract, % | 8 |
| Inflammatory diseases of gastrointestinal tract, % | 48 |
| Inflammatory diseases of lower urinary tract, % | 10 |
| Vaginitis/cervicitis,% | 7** |
Notes: BMI, body mass index; IgA-immunoglobulin A; C3-C3 complement fraction; C4-C4 complement fraction; eGFR, estimated glomerular filtration rate; CKD, chronic kidney disease; ABP, arterial blood pressure; GI tract, gastrointestinal tract; *values are presented as fractions/percentages or as mean with its standard deviation (M±SD), or as median with interquartile range (Me (25%;75%)); ** among females.
Table 2.
Prevalence of histological alterations.
| Indices | Values* |
|---|---|
|
Oxford classification (MEST-C): Mesangial proliferation (M1),% Endocapillary hypercellularity (E1) , % Segmental sclerosis or adhesions (S1) , % Tubular atrophy/interstitial fibrosis (T1+T2),% T0, % T1, % T2, % Cellular/fibro-cellular crescents, % C1, % C2, % |
40.5 22.9 70.2 31 69 22 9 16,7 12,3 4,4 |
|
Other changes: Global sclerosis, % of glomeruli Segmental sclerosis, % of glomeruli Fibrous crescents, % Interstitial infiltration, % >25% of interstitial area, % Peritubular capillaritis, % |
13 (5;30) 9 (0;17) 7.7 50.5 14.8 30.1 |
Notes: M1, mesangial proliferation ≥50% of the tubules; E1, presence of endocapillary proliferation; S1, presence of segmental sclerosis/adhesions; T1, tubular atrophy/interstitial fibrosis 26-50% of the cortical area, T2, tubular atrophy/interstitial fibrosis >50% of the cortical area; C1, cellular/fibro-cellular crescents <25%; C2, ≥25% of the glomeruli. * Values are presented as fractions/percentages or as medians with interquartile range (25%;75%).
Table 3.
Prevalence of deposits of immunoglobulins, C3 complement and fibrinogen in sub-structures of kidney (immunofluorescence).
Table 3.
Prevalence of deposits of immunoglobulins, C3 complement and fibrinogen in sub-structures of kidney (immunofluorescence).
| Indices | Frequency, % |
|---|---|
| IgA in the mesangium | 100.0 |
| IgA n glomerular capillary wall | 17.1 |
| IgA in atreries | 4.0 |
| IgA in in peritubular capillaries | 5.7 |
| IgM in mesangium | 71.1 |
| IgG in mesangium | 9.6 |
| C3 in mesangium | 98.0 |
| C3 in glomerular capillary wall | 13.8 |
| C3 in arteries | 4.5 |
| C3 in peritubular capillaries | 6.6 |
| Fibrinogen in mesangium | 21.4 |
| Fibrinogen n glomerular capillary wall | 6.2 |
| Fibrinogen in peritubular capillaries | 12.2 |
Note: IgA, immunoglobulin A; IgM, immunoglobulin M; IgG, immunoglobulin G; C3, C3 complement fraction.
Table 4.
Clinical and morphological correlations.
| Histologic indices, units | Mean ABP | eGFR | Daily proteinuria | Hematuria |
|---|---|---|---|---|
| Global glomerular sclerosis, % | 0.29 p<0.001 |
-0.47 p<0.001) |
0.39 p <0.001 |
-0.03 NS |
| Segmental glomerular sclerosis, % | 0.16 p <0.001 |
-0.20 p<0.001 |
0.35 p<0.001 |
0.00 NS |
| Crescents (any), % | 0.04 NS |
-0.10 p=0.024 |
0.25 p<0.001 |
0.15 p<0.001 |
| Cellular/fibrocellular crescents,% | 0.05 NS |
-0.11 p<0.001 |
0.28 p<0.001 |
0.17 p<0.001 |
| IFTA, grades | 0.36 p<0.001 |
-0.57 p <0.001 |
0.39 p <0.001 |
-0.02 NS |
| Interstitial infiltration, grades | 0.29 p<0.001 |
-0.51 p <0.001 |
0.35 p <0.001 |
0.118 p =0.005 |
| Mesangium proliferation, grades | 0.07 NS |
-0.15 p <0.001 |
0.19 p <0.001 |
0.14 p =0.001 |
| Endocapillary hypercellularity, no vs yes | 0.15 p<0.001 |
-0.25 p<0.001 |
0.30 p<0.001 |
0.12 p=0.004 |
| PTC, grades | 0.20 p<0.001 |
-0.41 p<0.001 |
0.37 p<0.001 |
0.11 p=0.009 |
| IgA glomerular capillaries, grades | 0.13 p<0.001 |
-0.10 p=0.009 |
0.16 p <0.001 |
0.01 NS |
| IgA mesangium, grades | -0.12 p =0.002 |
0.06 NS |
0.00 NS |
0.04 NS |
| IgA peritubular capillaries, grades | 0.07 NS |
-0.20 p<0.001) |
0.16 p<0.001 |
0.01 NS |
| IgM mesangium, grades | -0.04 NS |
0.03 NS |
0.12 p=0.002 |
0.01 NS |
| IgG mesangium, grades | -0.07 p=0.042 |
0.05 NS |
-0.04 NS |
-0.01 NS |
| C3 glomerular capillaries, grades | 0.15 p<0.001 |
-0.11 p=0.005 |
0.18 p<0.001 |
0.02 NS |
| C3 mesangium, grades | -0.054 NS |
0.01 NS |
-0.01 NS |
0.01 NS |
Notes: IFTA, interstitial fibrosis and tubular atrophy; PTC, peritubular capillaritis; eGFR, estimated glomerular filtration rate; ABP, blood pressure; IgA, immunoglobulin A; C3, C3 complement fraction; IgM, immunoglobulin M; IgG, immunoglobulin G; NS, non-significant correlation at p>0.05; values are Spearmen R (p-values).
Table 5.
Clinical and histologic factors associated with the progression of IgA-nephropathy (Multivariable Cox regression models).
Table 5.
Clinical and histologic factors associated with the progression of IgA-nephropathy (Multivariable Cox regression models).
| Models | Factors (unit change) | Expβ (95% CI) | Р-value |
|---|---|---|---|
| Clinical parametersa | Age (1 year) | 0.974 (0.949-0.999) | 0.041 |
| Male sex (vs female) | 1.956 (1.131-3.382) | 0.016 | |
| Mean BP maximal (1 mmHg) | 1.015 (1.002-1.029) | 0.025 | |
| eGFR (1 ml/min/1.73m2) | 0.950 (0.937-0.963) | <0.001 | |
| Ln (Hematuria) (1 unit) | 1.406 (1.121-1.762) | 0.003 | |
| Ln (Proteinuria) (1 unit) | 1.237 (0.893-1.714) | 0.20 | |
| Morphological parameters | M (M1 vs М0) b | 1.679 (0.984-2.864) | 0.06 |
| Е (Е1 vs Е0) b | 0.920 (0.502-1.685) | 0.67 | |
| S (S1 vs S0) b | 1.472 (0.746-2.905) | 0.26 | |
| Т (Т1 vs Т0) b | 1.021 (0.452-2.309) | 0.95 | |
| Т (Т2 vs Т0) b | 4.579 (1.835-11.462) | 0.001 | |
| С (С1 vs С0) b | 1.851 (0.960-3.569) | 0.07 | |
| С (С2 vs С0) b | 1.068 (0.400-2.855) | 0.89 | |
| Global glomerular sclerosis (1%) b | 1.014 (1.001-1.027) | 0.029 | |
| Any crescents (vs no crescents) b | 1.939 (1.110-3.389) | 0.02 | |
| Interstitial infiltration (1-24% vs 0%) b | 1.418 (0.624-3.222) | 0.40 | |
| Interstitial infiltration (≥25% vs <25%) b | 2.465 (1.097-5.539) | 0.029 | |
| PTC (moderate vs none) b | 1.321 (0.630-2.770) | 0.46 | |
| PTC (severe vs none) b | 2.590 (1.206-5.560) | 0.015 | |
| Clinical and morphological parameters с | Age (1 year) | 0.964 (0.939-0.990) | 0.006 |
| Male gender (vs. female) | 2.566 (1.448-4.548) | 0.001 | |
| eGFR (1 ml/min/1.73m2) | 0.966 (0.953-0.979) | <0.001 | |
| Ln(Hematuria) (1 unit) | 1.482 (1.166-1.884) | 0.001 | |
| Mean BP (maximal) (1 mm Hg) | 1.024 (1.010-1.040) | 0.001 | |
| PTC (severe vs none/moderate) | 2.422 (1.262-4.648) | 0.008 | |
| Tubular atrophy/interstitial fibrosis (T2 vs T0-1) | 6.738 (3.542-12.817) | <0.001 | |
| Any crescents (vs no crescents) | 2.078 (1.200-3.596) | 0.009 |
Note: ABP - blood pressure, eGFR - estimated glomerular filtration rate, M0 - mesangial proliferation <50%,M1 - mesangial proliferation ≥50%; E - endocapillary hypercellularity; E0 - no endocapillary hypercellularity, E1 - presence of endocapillary hypercellularity; S0 - no segmental sclerosis,S1 - presence of segmental sclerosis; T0 - tubular atrophy less than 25% of the cortical area, T1 - tubular atrophy/interstitial fibrosis 26-50% of the cortical area, T2 - tubular atrophy/interstitial fibrosis > 50% of the cortical area, C - cellular and fibrocellular crescents; C0 - no cellular and fibrocellular crescents, C1 - cellular and fibrocellular crescents <25%; C2 - >25% of tubules, PTC - peritubular capillaritis, CI-confidence interval. a - forced inclusion of variables with adjusted for immunosuppressive therapy – (forced inclusion of variables). b - adjusted for all clinical variables and immunosuppressive therapy. c - adjusted for all clinical and morphological variables and immunosuppressive therapy (backward stepwise regression).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



