
Submitted:
11 December 2023
Posted:
12 December 2023
You are already at the latest version
Abstract
(1) Background: Emotion regulation is a critical determinant of adaptive functioning during adolescence, exerting profound influence on psychological well-being. This study seeks to deepen our understanding of the intricate interplay between emotion regulation and maladaptive psychological symptoms, examining these dynamics through a cross-countries comparison; (2) Methods: A total of 224 adolescents, aged 13 to 21 years, from both Iran and Belgium, participated in a cross-sectional comparative study. The study aimed to elucidate the relationship between emotion regulation and mental health functioning, assessing internalizing symptoms, externalizing symptoms, and self-injury. A demographic questionnaire, the Emotion Regulation Inventory, Strengths and Difficulties Questionnaire, and Self-Harm Inventory, were administered. Data analysis incorporated correlation assessments, Multivariate Analysis of Variance, and Structured Equation Modeling; (3) Results: The findings revealed a positive association between emotional dysregulation and psychological symptoms across the entire sample. Conversely, emotional suppression, more prevalent in Iran, showed no significant link with maladaptive symptoms but was associated with self-harm in the Belgian sample. Cultural disparities were evident, with internalizing problems more prevalent in Iran and externalizing issues more common in Belgium; (4) Conclusion: Emotional dysregulation emerged as a common factor compromising mental health. It emphasizes the necessity of considering cultural nuances when developing intervention and prevention programs and calls for further research in this field.
Keywords:
Emotion Regulation
; Internalizing Symptoms
; Externalizing Symptoms
; NSSI
; Adolescent
; Culture
1. Introduction
Emotion regulation (ER) – which involves the internal or external process of monitoring, evaluating, and modulating emotional experiences [1,2] – is a key psychological resource and has a major impact on mental health and social adjustment [3,4,5]. Although the importance of ER is widely recognized [6,7,8,9], there is little consensus on the different dimensions of ER and their differential association with psychopathology [10].
Based on the Self-Determination Theory (SDT), Roth et al [11], introduced the concept of Integrative Emotion Regulation (IER). SDT is a comprehensive motivational theory aimed at elucidating the relationship between psychological development and social adaptation [12]. Within the SDT taxonomy of ER styles, IER is characterized by an inclination toward openness and receptivity to one's own emotional states. This approach involves the impartial processing of emotions and the deliberate cultivation of full emotional awareness. In contrast, Suppressive Emotion Regulation (SER) represents a controlled form of ER that hinges on the avoidance of emotional experiences with the goal of mitigating the impact of emotional inputs. The third mode of ER is referred to as Dysregulated Emotion Regulation (DER), wherein emotions are perceived as overwhelming, and the individual grapples with difficulties in effectively managing these emotional states [13]. These distinctions within ER styles, particularly the introduction of IER, contribute significantly to our understanding of how individuals navigate their emotional landscapes and how these approaches may impact mental health and social adaptation.
ER has been considered to play a particularly salient role in the context of adolescence mental health [14], a developmental phase distinguished by heightened emotional intensity and heightened moment-to-moment variability in emotional experiences [15,16]. Research has consistently documented the detrimental effect of maladaptive ER strategies (i.e., SER and DER) on the adolescents’ mental health [17,18,19]. In contrast, IER has been shown to decrease the risk for developing psychopathology in adolescents [20,21,22]. This emerging body of research highlights the importance of further exploring of the distinctive role of ER styles in adolescent psychopathology.
Among the most prevalent mental health problems among adolescence is non-suicidal self-injury (NSSI), which has been shown to be strongly related to difficulties in ER [23,24,25]. NSSI is defined as "the deliberate, non-fatal self-infliction of body tissue damage without suicidal intent" [26], and is associated with a range of adverse outcomes, including diminished academic performance, peer-related difficulties, and an elevated risk of suicidal behaviours [27,28,29].
Theoretical frameworks propose that challenges in ER are also pivotal in the development of internalizing symptoms among adolescents [30,31,32]. Building on this notion, research consistently indicates that difficulties in ER predict the emergence of both internalizing and externalizing symptoms in adolescents [33,34,35]. Moreover, extending our understanding of adolescent mental health, previous studies have established a clear link between NSSI and internalizing and externalizing symptoms [36,37]. As proposed in the Four-function Model by Nock and Prinstein [38], NSSI is considered as a maladaptive means of coping with negative emotions and thoughts. Difficulty tolerating intense emotions can lead to a tendency to internalize emotional distress, which in turn increases susceptibility to non-suicidal self-injury (NSSI). Delving deeper into the dynamics of ER and its impact, it has been observed that the frequency of NSSI is closely associated with emotion dysregulation. Importantly, this relationship is assumed to be mediated by the presence of internalizing symptoms [39]. However, the role of internalizing and externalizing symptoms as underlying mechanisms in the relationship between integrative, suppressive, and dysregulated ER with NSSI has not yet been examined. Furthermore, the vast majority of studies in this area are limited to Western adolescents.
Previous studies, distinct from the novel SDT taxonomy, have elucidated cultural disparities in ER and emotional expression [40,41]. Nevertheless, it is essential to highlight that, so far, only Benita et al.'s study [20] has delved into the SDT taxonomy of ER, encompassing the examination of integrative, suppressive, and dysregulated ER as universal constructs. As emphasized in a meta-analysis review by Hu et al [42], examining the relationship between ER and mental health, it is very important to consider culture as a moderator in this regard. It is noteworthy that Western cultures, in general, tend to exhibit a leaning toward individualism when compared to Eastern cultures, with Iran occupying an intermediary position between the individualistic and collectivist cultural spectrums [43,44]. Iranian families exhibit a profound cultural inclination toward the socialization of their offspring, instilling a deeply ingrained reverence for elder family members. Moreover, they emphasize the preservation of familial harmony by nurturing a strong sense of filial respect toward parents and other kin. Within this cultural context, children are subtly discouraged from openly expressing dissenting opinions or disagreements within the family dynamic [45,46].
The present study
The present study aims to investigate the cross-cultural relevance of ER styles in the context of adolescent psychopathology. To achieve this goal, we have formulated three main objectives: First, we examined the relationship between three different ER styles (IER, SER, and DER) and adolescent psychopathology (internalizing and externalizing problems and NSSI), as well as cultural differences in these relationships. Following Ryan and Deci's [47] theoretical framework, we expected a significant negative relationship between IER and psychological symptoms and a significant positive relationship between DER and SER and psychological symptoms in the two cultural groups. Moreover, given previous research (e.g., [42]) indicating a stronger correlation between expressive suppression and negative mental health indicators in Western cultural groups, we expect potential cross-cultural differences in the correlation between SER and psychological symptoms. Second, we examined the mediating role of internalizing and externalizing problems in the association between ER styles and NSSI. Based on the study by Kranzler et al. [39], we hypothesized that internalizing and externalizing problems would mediate the relationship between ER styles and NSSI in both cultural groups. Third, we examined the role of ER styles in predicting internalizing and externalizing problems and NSSI, controlling for age, gender, and country. In light of previous research describing age-related differences in ER (or a review, see [48]), increased incidence of internalizing symptoms in women (for a review, see [50]) and cultural differences in ER and adolescent psychopathology [50,51,52], we considered the potential effects of age, gender, and country on the relationship between ER styles and psychopathology.
2. Materials and Methods
Participants
The study included a total of 224 participants from secondary school students in Iran (Tehran, n = 117, 38% (44 of 117) female) and Belgium (Antwerp, n = 107, 52% (56 of 107) female). The age range in the Iranian sample spanned from 13 to 15 years, with a mean age of 13.85 (SD = 0.62), while in the Belgian sample the age range was from 14 to 19 years, with a mean age of 15.23 (SD = 1.20). It is important to note that in Belgium, given the considerable ethnic diversity, only adolescents with both parents born in Belgium were included in the study. They made up 30.83% (n = 107) of the total sample of 347 Belgian participants.
Measures
Demographic questions included age (13-19 years), sex (male and female), country of origin, parents’ place of birth, and religious orientation (Muslim, Christian, Hindu and other).
The self-report version of the Strengths and Difficulties Questionnaire [53] for ages 11-17 years was used to measure internalizing and externalizing symptoms. Goodman & Goodman [54] recommended the use of three subscales in non-clinical samples: Internalizing Problems (emotional symptoms (e.g., “I worry a lot”) and peer problems (e.g., “I am usually on my own”), 10 items), Externalizing Problems (conduct problems (e.g., “I fight a lot”) and hyperactivity symptoms (e.g., “I am constantly fidgeting”), 10 items), and the Prosocial Subscale (e.g., “I try to be nice to other people”; 5 items). Each item is rated on a 3-point Likert scale, where 0 = not true, 1 = somewhat true, and 2 = definitely true. Only the total score and the subscales of internalizing and externalizing problems were used in this study. Previous studies have reported satisfactory psychometric properties for the Dutch [55] and the Persian versions [56] of the self-reported SDQ of the self-report version of the SDQ. In the study by Goodman [57], the internal consistency for the total score was 0.73 and good construct validity (r = 0.70 for the total score) was reported. In the current study, the Cronbach’s alpha for the total score, internalizing and externalizing problems was 0.68, 0.71 and 0.72 respectively.
Emotion Regulation Inventory [58]. This questionnaire includes three styles of ER: 1) Dysregulated (6 items, e.g., “When I am angry, I feel I have little control over my behaviour”), 2) Suppressive (6 items, e.g., “I almost always try to not express my anger ”), and 3) Integrative (6 items, e.g., “When I am angry, I usually try to understand why I am angry”). These items are rated on a 5-point Likert scale ranging from 1 (not at all) to 5 (very much). Roth et al. [58] found evidence for the validity and internal consistency of all three subscales. Using the Dutch version of the ERI, Brenning et al. [59] found Cronbach’s alphas of 0.69 for dysregulated and 0.72 for suppressive ER. The Cronbach’s alphas in the current study were 0.76, 0.73 and 0.85 for DER, SER, and IER, respectively. For the Iranian sample, the English version of the ERI [58] was translated into Persian by a Persian-speaking researcher and then back-translated by another researcher. The Cronbach’s alpha for this Persian version was 0.63, 0.80 and 0.67 for the DER, SER and IER subscales respectively.
Self-Harm Inventory [60]. This measure assesses the respondent’s history of indirect self-injurious behaviours, NSSI, and suicidal self-injurious (SSI) behaviours with a 23-item (yes/no) questionnaire. Each item is preceded by a question: “Have you ever intentionally, or on purpose…”. In this study, we used only the 8 items examining NSSI methods (including methods such as cutting, banging, scratching, and burning) and a single SSI item (i.e., “Have you ever intentionally, or on purpose, attempted suicide?”). In the current study, the Cronbach’s alpha for the NSSI subscale was 0.69.
Procedure
A convenience sampling approach was used to select the participants in both countries. For the Belgian sample, students were recruited from three different schools in the Flanders region. The first step was to send an information letter to the parents via the students. Parents who wished their adolescents to participate in the study were asked to return a signed consent form to the school via the adolescent, thereby establishing a passive consent procedure. Subsequently, before completing the questionnaires by the students, they provided active informed consent. A parallel procedure was followed in Iran for two schools in Tehran. The questionnaires were administrated to the adolescents during their regular school hours under the supervision of a research assistant. It is important to note that the research protocol was approved by the Medical Ethics Committee of UZ Brussels (2019/073) and was also approved by Yazd Shahid Sadoughi University of Medical Sciences (IR.SSU.REC.1400.159) in Iran.
Statistical Analyses
The statistical analyses in this study were conducted using SPSS (version 25) and Amos software (version 24). In the first step, a thorough check for missing data was performed before conducting analyses, and one participant’s data was excluded due to an excessive number of unanswered questions. After these initial data checks, descriptive statistics were then calculated. Second, correlation analyses were conducted to examine the relationship between the three modes of ER, internalizing and externalizing problems and NSSI. These correlations were calculated for the entire group of participants and separately for the Iranian and Belgian samples, allowing a comprehensive examination of the relationships between these variables within different cultural contexts. Cohen’s q effect sizes were calculated to examine the differences in correlations between two countries and were interpreted according to Cohen [61]: 0.10 = small effects, 0.30 = moderate effects, and 0.50 = large effects. Third, a Multivariate Analysis of Variance (MANOVA) was performed to explore potential differences between the Belgian and Iranian samples with regard to the mean scores of the ER modes and internalizing and externalizing problems. Fourth, a hierarchical regression analysis was conducted to examine if ER modes predict NSSI and internalizing and externalizing problems controlling for demographic variables (age, gender, and country). Finally, Structural Equation Modelling (SEM) was employed to examine the direct effects between the variables and the indirect effects of ER modes on NSSI through internalizing and externalizing problems separately in the Belgian and Iranian samples. This advanced analytical method allows for a more in-depth examination of the complex interactions and pathways between these variables, facilitating a comprehensive understanding of their associations.
3. Results
3.1. Preliminary analysis
Descriptive analyses (mean and standard deviations) and the correlation between ER modes, internalizing and externalizing problems and NSSI are presented in Table 1. Pearson correlation results showed that both DER and SER were positively correlated with internalizing problems. In addition, DER was also positively correlated with externalizing problems and NSSI. SER, inversely, showed a negative correlation with externalizing problems and NSSI. However, IER showed no statistically significant correlations with internalizing and externalizing problems and NSSI. In terms of the correlation between internalizing and externalizing problems and NSSI, both internalizing and externalizing problems were positively associated with NSSI. It is worth noting that the most robust correlation is observed between externalizing problems and NSSI (r = 0. 54, p < 0.01).
Table 2 presents the descriptive statistics and bivariate correlations between ER modes, internalizing and externalizing problems and NSSI in the two different samples, each representing a different cultural context. In the Belgian sample, Pearson correlation results indicated that the maladaptive ER modes (SER and DER) were positively and significantly correlated with NSSI, while IER was negatively correlated with NSSI. Additionally, DER was positively correlated with both internalizing and externalizing problems. However, SER and IER were not significantly associated with internalizing and externalizing problems. In the Iranian sample, DER was positively significantly associated with all maladaptive symptoms (internalizing and externalizing problems and NSSI). SER was positively significantly associated with internalizing problems and unexpectedly negatively associated with externalizing problems. The correlation between SER and NSSI was not significant (r = -0.13, p > 0.05). IER showed no significant correlation with maladaptive symptoms (p > 0.05). Notably, internalizing and externalizing problems were strongly positively correlated with NSSI in both countries.
The results of the Cohen’s q for the assessment of the differences in the correlations between two countries revealed small effect sizes for the correlation between externalizing problems with SER (r = 0.229) and IER (r = 0.256) and also the correlation between NSSI with DER (r = 0.114) and IER (r = 0.175). Medium effect sized were observed for the association between SER and NSSI (r = 0.256) and also the association between NSSI and externalizing problems (r = 0.256).
3.2. Multivariate Analysis of Variance
The results of the MANOVA showed significant differences between Belgian and Iranian adolescents in terms of SER (F = 95.9, p < 0.01), IER (F = 15.04, p < 0.01), internalizing (F = 27.03, p < 0.01), and externalizing problems (F = 67.5, p < 0.01). More specifically, the Belgian adolescents scored significantly lower on SER and internalizing problems and higher on IER and externalizing problems compared to the Iranian adolescents (see Table 3). However, there were no significant differences in DER scores between the two countries (p > 0.05).
3.3. Hierarchical Regression Analyses
The results of the hierarchical regression analysis showed that in the first step (Model 1), the combined impact of the control variables (i.e., age, gender, and country) accounted for a modest 4% of the variance in internalizing and externalizing problems and a substantial 16% of the variance in NSSI scores (see Table 4). However, when we introduced the ER modes in the next step (Model 2), there was a noticeable increase in the explained variance. Specifically, the cumulative variance explained for internalizing and externalizing problems increased to 27% and for NSSI to 30%. Both increments were statistically significant (p < 0.01). Among the ER modes, only DER emerged as a statistically significant predictor of both internalizing and externalizing problems (β = 0.49, p < 0.01) and NSSI (β = 0.35, p < 0.01) in Model 2. Among the control variables, country had a significant effect on NSSI (β = 5.698, p < 0.01) and DER (β = 5.598, p < 0.01). None of the other variables examined played a significant role in predicting internalizing and externalizing problems and NSSI (see Table 4).
3.3. Mediation Analysis
The structural model with all significant paths for the mediating role of internalizing and externalizing problems in the association between ER modes and NSSI for the Belgian sample is shown in Figure 1. As the initially proposed model did not fit the data well, all insignificant paths were removed (i.e., the paths from SER and IER to externalizing problems and the path from DER to NSSI). The model fit indices for the presented model were satisfactory (χ2/df = 1.25, p = 0.02, CFI = 0.92, IFI = 0. 93, RMSEA = 0.04). The values of the standardized regression weights for direct effects were statistically significant for all paths in the model, except for the path from SER to NSSI (β = 0.126, p > 0.05). The results of the standardized indirect effects indicated a significant mediating role of internalizing and externalizing problems in the relationship between DER (β = 0.35, p > 0.05) and SER modes and NSSI (β = 0.07, p > 0.05). However, the association between IER and NSSI was only mediated by internalizing problems (β = 0.07, p > 0.05).
The structural model with all significant paths for the mediating role of internalizing and externalizing problems in the association between ER modes and NSSI for the Iranian sample is presented in Figure 2. As the initially proposed model did not fit the data well, all insignificant paths were removed (i.e., the path from DER to NSSI, the path from internalizing problems to NSSI, and IER to internalizing and externalizing problems and NSSI). The model fit indices for the presented model were satisfactory (χ2/df = 1.2, p = 0.06, CFI = 0.93, IFI = 0. 94, RMSEA = 0.04). The values of the standardized regression weights for direct effects were statistically significant for all paths in the model, except for the path from SER to NSSI (β = 0.18, p > 0.05). The results of the standardized indirect effects revealed a significant mediating role of externalizing problems in the relationship between DER (β = 0.6, p > 0.05) and SER (β = -0.33, p > 0.05) modes and NSSI.
4. Discussion
The primary objective of this study was to illuminate cultural differences in the relationship between distinct ER modes and adolescent psychopathology based on the SDT framework and to examine the mediating role of internalizing and externalizing problems in the association between ER modes and NSSI in two different cultural groups. To achieve this goal, we compared two distinct samples: Iranian adolescents, serving as a representative sample of a more collectivist culture, and Belgian adolescents, as proxies for a more individualistic cultural context.
In line with the insights from Mesquita [62], highlighting the pivotal role of cultural values, norms, and ideas in the development of psychological symptoms, emotion regulation (ER), and normative behavior, our study brought to light distinct patterns within the Iranian and Belgian samples. Notably, the Iranian cohort exhibited higher occurrences of internalizing symptoms, coupled with a prevalent use of Suppressive Emotion Regulation (SER) modes. This finding echoes prior research by Dadkhah and Shirinbayan [63], indicating a substantial incidence of emotional suppression among Iranian adolescents. The prevalence of SER in this population underscores the robust influence of cultural norms on emotion regulation, particularly in collectivistic societies.
Conversely, the Belgian sample displayed higher frequencies of externalizing symptoms and a greater inclination toward Intrusive Emotion Regulation (IER). This aligns with the broader cultural context in Belgium, characterized by individualistic tendencies, as identified by Hofstede insights country comparison tool [64]. The observed higher prevalence of IER among Belgians reflects the cultural emphasis on self-expression, self-reliance, and the pursuit of individual goals. In contrast to the collectivistic approach, the deliberate engagement with one's emotional experiences, seeking to integrate them into personal aspirations and values, aligns harmoniously with the individualistic cultural framework in Belgium.
Our findings further corroborate these cultural variations, revealing that Iranian adolescents scored significantly higher in suppressive regulation, consistent with prior studies [41,65,66] a higher prevalence of emotional suppression in collectivist/non-Western cultures. This resonates with the broader pattern observed in Asian/Eastern cultures, where greater control over emotions is encouraged, potentially contributing to a higher incidence of internalizing problems [41]. Tahmouresi et al.'s [67] cross-cultural study, comparing Iranian and German children, similarly found a greater tendency toward emotional suppression in the Iranian context, highlighting the enduring influence of culture on emotion regulation strategies and their impact on psychological well-being.
These associations underscores the interplay between cultural values and ER strategies, contributing to a deeper understanding of the observed variations between the Belgian and Iranian samples in our study. Additionally, our findings underscore the notion that emotion dysregulation appears to exert adverse effects on adolescent mental health across diverse cultural contexts. This is evidenced by the strong associations identified between DER and internalizing and externalizing symptoms, as well as NSSI in both cultural groups.
Next, The results of the hierarchical regression indicated that DER positively predicted NSSI and internalizing and externalizing problems above and beyond age, gender, and culture. This finding further supports our bivariate correlation results indicating robust correlation between DER and psychological symptoms in both countries and little or no difference in the correlations.
Emotion dysregulation is linked to an increased reliance on negative coping mechanisms, commonly observed in both internalizing and externalizing disorder [68]. Our findings support the conceptualization proposed by Clapham & Brausch [69], indicating that adolescents may manifest internalizing symptoms in response to insufficient emotion regulation.
This finding is aligns with the overarching consensus that emotion dysregulation serves as a risk factor for adolescent psychopathology, as highlighted in previous research such as McLaughlin et al [70]. Also consistent with a recent study- drawing upon data derived from 49 distinct sources- showing that people who struggle to regulate their emotions are more likely to engage in self-harm throughout their lives and emotion dysregulation is strongest predictor of NSSI [71]. Nevertheless, our findings revealed that even when accounting for gender and age and country differences, emotion dysregulation remained correlated with NSSI. This supports the findings of Wolf et al [71], indicating that heightened challenges in emotion regulation are connected to an increased probability of engaging in NSSI across individuals, regardless of age or gender. These results differ from studies such as Chen & Chun [72] and Thomas & Bonnaire [73], which have suggested gender differences in this association. The present study stands as a distinctive contribution by demonstrating the association between emotion dysregulation and psychopathology across diverse countries.
Mediation analysis revealed that both internalizing and externalizing problems served as mediating factors in the association between DER and NSSI in the Belgian sample, with internalizing problems demonstrated a more pronounced influence. In the Iranian model, only externalizing problems acted as a mediator in the relationship between DER and NSSI. This finding aligns with the results of Kranzler et al.'s study [39], which evidenced the mediating role of internalizing problems in the relationship between emotion dysregulation and NSSI. Furthermore, SER was indirectly related to NSSI primarily through internalizing problems in the Belgian sample. While, in the Iranian sample, the association between SER and NSSI was only mediated by externalizing problems. These outcomes are consistent with previous research demonstrating links between emotion dysregulation and internalizing problems [70,74], as well as between internalizing problems and NSSI (e.g., [75]). The observation that NSSI was correlated with heightened SER is particularly noteworthy in the context of the Belgian adolescents. This finding aligns with prevailing Western theories which consider NSSI as a means to evade or suppress intense emotions and thoughts, as evidenced by Hooley and Franklin [76]. However, intriguingly, this correlation between NSSI and SER was not observed in the Iranian sample, which may suggest cultural disparities in the expressions of NSSI, as previously indicated by Gholamrezaei et al [77]. Their research revealed lower incidence rates of NSSI in an Iranian sample and limited support for NSSI as an ER strategy, particularly among men, when compared to Western samples.
5. Conclusions
Our study contributes to the growing body of research on ER modes and their impact on adolescent psychopathology from an SDT perspective. Our study underscores some cultural differences in the links between ER modes and psychological symptoms in adolescents. The most noteworthy cultural differences are the variations in levels of internalizing symptoms and emotional suppression between Iranian and Belgian adolescents. These results underscore the significance of considering cultural nuances in understanding the interplay between ER modes and adolescent psychopathology, further emphasizing the need for more extensive cross-cultural research to build a more comprehensive understanding of these phenomena.
Acknowledgments
We express our sincere gratitude to all the participants who participated in this study.
Conflicts of Interest
The author(s) have stated that there are no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
References
- Gross, J.J. Emotion Regulation: Current Status and Future Prospects. Psychological Inquiry 2015, 26, 1–26. [Google Scholar] [CrossRef]
- McRae, K.; Gross, J.J. Emotion Regulation. Emotion 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Lincoln, T.; Schulze, L.; Renneberg, B. The Role of Emotion Regulation in the Characterization, Development and Treatment of Psychopathology. Nature Reviews Psychology 2022, 1, 1–15. [Google Scholar] [CrossRef]
- Compas, B.E.; Jaser, S.S.; Bettis, A.H.; Watson, K.H.; Gruhn, M.A.; Dunbar, J.P.; Williams, E.; Thigpen, J.C. Coping, Emotion Regulation, and Psychopathology in Childhood and Adolescence: A Meta-Analysis and Narrative Review. Psychological Bulletin 2017, 143, 939–991. [Google Scholar] [CrossRef] [PubMed]
- Werner, K.; Gross, J.J. Emotion Regulation and Psychopathology: A Conceptual Framework. In Emotion regulation and psychopathology: A transdiagnostic approach to etiology and treatment.; The Guilford Press: New York, NY, US, 2010; pp. 13–37. [Google Scholar]
- DeSteno, D.; Gross, J.J.; Kubzansky, L. Affective Science and Health: The Importance of Emotion and Emotion Regulation. Health Psychology 2013, 32, 474. [Google Scholar] [CrossRef]
- Gardner, S.E.; Betts, L.R.; Stiller, J.; Coates, J. The Role of Emotion Regulation for Coping with School-Based Peer-Victimisation in Late Childhood. Personality and Individual Differences 2017, 107, 108–113. [Google Scholar] [CrossRef]
- Klein, R.; Nguyen, N.; Gyorda, J.; Jacobson, N. Adolescent Emotion Regulation and Future Psychopathology: A Prospective Transdiagnostic Analysis. Journal of Youth and Adolescence 2022, 32. [Google Scholar] [CrossRef]
- Thomas, C.; Zolkoski, S. Preventing Stress Among Undergraduate Learners: The Importance of Emotional Intelligence, Resilience, and Emotion Regulation. Frontiers in Education 2020, 5, 94. [Google Scholar] [CrossRef]
- Bonanno, G.; Burton, C. Regulatory Flexibility: An Individual Differences Perspective on Coping and Emotion Regulation. Perspectives on Psychological Science 2013, 8, 591–612. [Google Scholar] [CrossRef]
- Roth, G.; Benita, M.; Amrani, C.; Shahar, B.; Asoulin, H.; Moed, A.; Bibi, U.; Kanat-Maymon, Y. Integration of Negative Emotional Experience Versus Suppression: Addressing the Question of Adaptive Functioning.; Emotion: Washington, D.C., 2014; Volume 14. [Google Scholar]
- Ryan, R.; Deci, E. Self-Regulation and the Problem of Human Autonomy: Does Psychology Need Choice, Self-Determination, and Will? Journal of personality 2006, 74, 1557–1585. [Google Scholar] [CrossRef]
- Roth, G.; Vansteenkiste, M.; Ryan, R. Integrative Emotion Regulation: Process and Development from a Self-Determination Theory Perspective. Development and Psychopathology 2019, 31, 1–12. [Google Scholar] [CrossRef]
- Silvers, J. Adolescence as a Pivotal Period for Emotion Regulation Development For Consideration at Current Opinion in Psychology. Current Opinion in Psychology 2021, 44. [Google Scholar]
- Bailen, N.H.; Green, L.M.; Thompson, R.J. Understanding Emotion in Adolescents: A Review of Emotional Frequency, Intensity, Instability, and Clarity. Emotion Review 2019, 11, 63–73. [Google Scholar] [CrossRef]
- Maciejewski, D.; Lier, P.; Branje, S.; Meeus, W. A 5-Year Longitudinal Study on Mood Variability Across Adolescence Using Daily Diaries. Child Development, Advance Online Publication. 2015. [Google Scholar]
- Brenning, K.; Soenens, B.; Vansteenkiste, M.; De Clercq, B.; Antrop, I. Emotion regulation as a transdiagnostic risk factor for (non)clinical adolescents’ internalizing and externalizing psychopathology : investigating the intervening role of psychological need experiences. CHILD PSYCHIATRY & HUMAN DEVELOPMENT. 2022, 53, 124–136. [Google Scholar]
- Brenning, K.; Waterschoot, J.; Dieleman, L.; Morbée, S.; Vermote, B.; Soenens, B.; et al. The role of emotion regulation in mental health during the COVID-19 outbreak : a 10-wave longitudinal study. STRESS AND HEALTH. 2023, 39, 562–75. [Google Scholar] [CrossRef]
- Scharf, N.; Benita, M.; Benish-Weisman, M. Emotion Regulation Styles and Adolescent Adjustment Following a COVID-19 Lockdown. Stress and Health 2023. [Google Scholar] [CrossRef] [PubMed]
- Benita, M.; Benish-Weisman, M.; Matos, L.; Torres, C. Integrative and Suppressive Emotion Regulation Differentially Predict Well-Being through Basic Need Satisfaction and Frustration: A Test of Three Countries. Motivation and Emotion 2020, 44, 67–81. [Google Scholar] [CrossRef]
- Brenning, K.; Soenens, B.; Van Petegem, S.; Vansteenkiste, M. Perceived Maternal Autonomy Support and Early Adolescent Emotion Regulation: A Longitudinal Study. Social Development 2015, 24, 561–578. [Google Scholar] [CrossRef]
- Vatandoost, S.; Baetens, I.; Van Den Meersschaut, J.; Van Heel, M.; Van Hove, L. The impact of the COVID-19 pandemic on the incidence of non-suicidal self-injury; a comparison between Iran and Belgium. Clinical Medicine Insights: Psychiatry. 2023, 14. [CrossRef]
- Brausch, A.; Clapham, R.; Littlefield, A. Identifying Specific Emotion Regulation Deficits That Associate with Nonsuicidal Self-Injury and Suicide Ideation in Adolescents. Journal of Youth and Adolescence 2022, 51, 1–14. [Google Scholar] [CrossRef]
- Lan, Z.; Pau, K.; Md Yusof, H.; Huang, X. The Effect of Emotion Regulation on Non-Suicidal Self-Injury Among Adolescents: The Mediating Roles of Sleep, Exercise, and Social Support. Psychology Research and Behavior Management 2022, 15, 1451–1463. [Google Scholar] [CrossRef]
- Robinson, K.; Garisch, J.A.; Kingi, T.; Brocklesby, M.; O’Connell, A.; Langlands, R.L.; Russell, L.; Wilson, M.S. Reciprocal Risk: The Longitudinal Relationship between Emotion Regulation and Non-Suicidal Self-Injury in Adolescents. Journal of Abnormal Child Psychology 2019, 47, 325–332. [Google Scholar] [CrossRef] [PubMed]
- International Society for the Study of Self-Injury. What is self-injury? 2018. Available online: https://itriples.org/about-self-injury/what-is-self-injury.
- Baetens, I.; Greene, D.; Van Hove, L.; Van Leeuwen, K.; Wiersema, R.; Desoete, A.; et al. Predictors and consequences of non-suicidal self-injury in relation to life, peer, and school factors. JOURNAL OF ADOLESCENCE. 2021, 90, 100–8. [Google Scholar] [CrossRef]
- Cassels, M.; Wilkinson, P. Non-suicidal self-injury in adolescence. Paediatrics and Child Health. 2016, 26, 554–558. [Google Scholar] [CrossRef]
- Robinson, K.; Garisch, J.A.; Wilson, M.S. Nonsuicidal self-injury thoughts and behavioural characteristics: Associations with suicidal thoughts and behaviours among community adolescents. J Affect Disord. 2021, 282, 1247–1254. [Google Scholar] [CrossRef] [PubMed]
- Aldao, A.; Gee, D.G.; De Los Reyes, A.; Seager, I. Emotion regulation as a transdiagnostic factor in the development of internalizing and externalizing psychopathology: Current and future directions. Development and Psychopathology. 2016, 28, 927–946. [Google Scholar] [CrossRef]
- Cludius, B.; Mennin, D.; Ehring, T. Emotion Regulation as a Transdiagnostic Process. Emotion 2020, 20, 37–42. [Google Scholar] [CrossRef]
- Cole, P.M.; Hall, S.E.; Hajal, N.J.; Beauchaine, T.P.; Hinshaw, S.P. Emotion dysregulation as a vulnerability to psychopathology. Child and adolescent psychopathology. 2017, 346–386. [Google Scholar] [CrossRef]
- Cai, R.Y.; Hardan, A.Y.; Phillips, J.M.; Frazier, T.W.; Uljarević, M. Brief Report: Emotion Regulation Influences on Internalizing and Externalizing Symptoms Across the Normative-Clinical Continuum. Frontiers in Psychiatry 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Cavicchioli, M.; Stefanazzi, C.; Tobia, V.; Ogliari, A. The Role of Attachment Styles in Attention- Deficit Hyperactivity Disorder: A Meta-Analytic Review from the Perspective of a Transactional Development Model The Role of Attachment Styles in Attention-Deficit Hyperactivity Disorder: A Meta-Analytic Review from the Perspective of a Transactional Development Model. European Journal of Developmental Psychology 2022, 20. [Google Scholar] [CrossRef]
- Schneider, R.; Arch, J.; Landy, L.; Hankin, B. The Longitudinal Effect of Emotion Regulation Strategies on Anxiety Levels in Children and Adolescents. Journal of Clinical Child & Adolescent Psychology 2016, 47, 1–14. [Google Scholar] [CrossRef]
- Baetens, I.; Claes, L.; Muehlenkamp, J.; Grietens, H.; Onghena, P. Differences in Psychological Symptoms and Self-Competencies in Non-Suicidal Self-Injurious Flemish Adolescents. Journal of Adolescence 2012, 35, 753–759. [Google Scholar] [CrossRef]
- Cipriano, A.; Cella, S.; Cotrufo, P. Nonsuicidal Self-Injury: A Systematic Review. Frontiers in Psychology 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.; Prinstein, M. A Functional Approach to the Assessment of Self-Mutilative Behavior. Journal of consulting and clinical psychology 2004, 72, 885–890. [Google Scholar] [CrossRef]
- Kranzler, A.; Fehling, K.B.; Anestis, M.D.; Selby, E.A. Emotional dysregulation, internalizing symptoms, and self-injurious and suicidal behavior: Structural equation modeling analysis. Death Studies 2016, 40, 358–366. [Google Scholar] [CrossRef]
- Arens, E.A.; Balkir, N.; Barnow, S. Ethnic Variation in Emotion Regulation: Do Cultural Differences End Where Psychopathology Begins? Journal of Cross-Cultural Psychology 2013, 44, 335–351. [Google Scholar] [CrossRef]
- Matsumoto, D.; Yoo, S.H.; Nakagawa, S. ; Culture, Emotion Regulation, and Adjustment. Journal of Personality and Social Psychology 2008, 94, 925–937. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Zhang, D.; Wang, J.-L.; Mistry, R.; Ran, G.; Wang, X. Relation between Emotion Regulation and Mental Health: A Meta-Analysis Review. Psychological Reports 2014, 114, 341–362. [Google Scholar] [CrossRef] [PubMed]
- Diener, M.L.; Lucas, R.E. Adults’ Desires for Children’s Emotions Across 48 Countries: Associations with Individual and National Characteristics. Journal of Cross-Cultural Psychology 2004, 35, 525–547. [Google Scholar] [CrossRef]
- Hofstede, G. Empirical Models of Cultural Differences. In Contemporary issues in cross-cultural psychology; Swets & Zeitlinger Publishers: Lisse, Netherlands, 1991; pp. 4–20. [Google Scholar]
- Ghorbani, N.; Bing, M.N.; Watson, P.J.; Davison, H.K.; LeBreton, D.L. Individualist and Collectivist Values: Evidence of Compatibility in Iran and the United States. Personality and Individual Differences 2003, 35, 431–447. [Google Scholar] [CrossRef]
- Sharifzadeh, V. Middle Eastern-rooted families. In Developing Cross-Cultural Competence, 3rd ed.; Lynch, E., Hanson, M., Eds.; Brookes: Baltimore, MD, 2004; pp. 373–410. [Google Scholar]
- Ryan, R. M.; Deci, E. L. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness.; Self-determination theory: Basic psychological needs in motivation, development, and wellness.; The Guilford Press: New York, NY, US 2017; pp xii, 756. [CrossRef]
- Allen, V.; Windsor, T. PSYCHO-SOCIAL MODERATORS OF THE COUPLING OF STRESS AND NEGATIVE AFFECT: A MICRO-LONGITUDINAL STUDY. Innovation in Aging 2017, 1 (suppl_1), 863–863. [Google Scholar] [CrossRef]
- Keyes, K.; Platt, J. Annual Research Review: Sex, Gender, and Internalizing Conditions among Adolescents in the 21st Century - Trends, Causes, Consequences. Journal of child psychology and psychiatry, and allied disciplines 2023. [Google Scholar] [CrossRef]
- Aka, B.T. Cultural Dimensions of Emotion Regulation. Psikiyatride Guncel Yaklasimlar - Current Approaches in Psychiatry 2023, 15, 441–450. [Google Scholar] [CrossRef]
- Potthoff, S.; Garnefski, N.; Miklósi, M.; Ubbiali, A.; Domínguez-Sánchez, F.J.; Martins, E.C.; Witthöft, M.; Kraaij, V. Cognitive Emotion Regulation and Psychopathology across Cultures: A Comparison between Six European Countries. Personality and Individual Differences 2016, 98, 218–224. [Google Scholar] [CrossRef]
- Weiss, N.H.; Kiefer, R.; Goncharenko, S.; et al. Emotion regulation and substance use: A meta-analysis. Drug Alcohol Depend 2022, 230, 109131. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R.; Meltzer, H.; Bailey, V. The Strengths and Difficulties Questionnaire: a pilot study on the validity of the self-report version. Eur Child Adolesc Psychiatry 1998, 7, 125–130. [Google Scholar] [CrossRef]
- Goodman, A.; Goodman, R. Strengths and Difficulties Questionnaire as a Dimensional Measure of Child Mental Health. Journal of the American Academy of Child and Adolescent Psychiatry 2009, 48, 400–403. [Google Scholar] [CrossRef]
- Muris, P.; Meesters, C.; van den Berg, F. The Strengths and Difficulties Questionnaire (SDQ)--further evidence for its reliability and validity in a community sample of Dutch children and adolescents. Eur Child Adolesc Psychiatry 2003, 12, 1–8. [Google Scholar] [CrossRef]
- Alavi, M.; Mohammadi, M.R.; Md, J.; Tehranidoost, M.; Shahrivar, Z.; Saadat, S. The Farsi Version of the Strength and Difficulties Questionnaire Selfreport Form: The Normative Data and Scale Properties. iranian Journal of child neurology 2009, 3. [Google Scholar]
- Goodman, R. Psychometric Properties of the Strengths and Difficulties Questionnaire. Journal of the American Academy of Child & Adolescent Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef]
- Roth, G.; Assor, A.; Niemiec, C.P.; Ryan, R.M.; Deci, E.L. The Emotional and Academic Consequences of Parental Conditional Regard: Comparing Conditional Positive Regard, Conditional Negative Regard, and Autonomy Support as Parenting Practices. Developmental Psychology 2009, 45, 1119–1142. [Google Scholar] [CrossRef]
- Brenning, K.; Soenens, B.; Braet, C.; Bosmans, G. Attachment and depressive symptoms in middle childhood and early adolescence: testing the validity of the emotion regulation model of attachment. PERSONAL RELATIONSHIPS 2012, 19, 445–64. [Google Scholar] [CrossRef]
- Sansone, R.A.; Wiederman, M.W.; Sansone, L.A. The Self-Harm Inventory (SHI): Development of a Scale for Identifying Self-Destructive Behaviors and Borderline Personality Disorder. Journal of Clinical Psychology 1998, 54, 973–983. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge, 1998. [Google Scholar] [CrossRef]
- Mesquita, B.; Boiger, M. Emotions in Context: A Sociodynamic Model of Emotions. Emotion Review 2014, 6, 298–302. [Google Scholar] [CrossRef]
- Dadkhah, A.; Shirinbayan, P. Emotion Regulation Characteristics Development in Iranian Primary School Pupils. Iranian Rehabilitation Journal 2014, 12, 17–21. [Google Scholar]
- Insights, H. Hofstede insights country comparison tool 2020.
- Butler, E.A.; Lee, T.L.; Gross, J.J. Emotion Regulation and Culture: Are the Social Consequences of Emotion Suppression Culture-Specific? Emotion 2007, 7, 30–48. [Google Scholar] [CrossRef]
- Soto, J.A.; Levenson, R.W.; Ebling, R. Cultures of Moderation and Expression: Emotional Experience, Behavior, and Physiology in Chinese Americans and Mexican Americans. Emotion 2005, 5, 154–165. [Google Scholar] [CrossRef]
- Tahmouresi, N.; Bender, C.; Schmitz, J.; Baleshzar, A.; Tuschen-Caffier, B. Similarities and Differences in Emotion Regulation and Psychopathology in Iranian and German School-Children: A Cross-Cultural Study. International journal of preventive medicine 2014, 5, 52–60. [Google Scholar]
- McLaughlin, K.A.; Sheridan, M.A.; Tibu, F.; Fox, N.A.; Zeanah, C.H.; Nelson, C.A. Causal Effects of the Early Caregiving Environment on Development of Stress Response Systems in Children. Proceedings of the National Academy of Sciences 2015, 112, 5637–5642. [Google Scholar] [CrossRef]
- Clapham, R.; Brausch, A. Internalizing and Externalizing Symptoms Moderate the Relationship Between Emotion Dysregulation and Suicide Ideation in Adolescents. Child Psychiatry & Human Development 2022. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, K.A.; Hatzenbuehler, M.L.; Mennin, D.S.; Nolen-Hoeksema, S. Emotion dysregulation and adolescent psychopathology: a prospective study. Behav Res Ther 2011, 49, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Wolff, J.C.; Thompson, E.; Thomas, S.A.; et al. Emotion dysregulation and non-suicidal self-injury: A systematic review and meta-analysis. Eur Psychiatry 2019. [Google Scholar] [CrossRef]
- Chen, W.-L.; Chun, C.-C. Association between Emotion Dysregulation and Distinct Groups of Non-Suicidal Self-Injury in Taiwanese Female Adolescents. Int. J. Environ. Res. Public Health 2019, 16, 3361. [Google Scholar] [CrossRef]
- Thomas, D.; Bonnaire, C. Relationship Between Non-Suicidal Self-Injury and Emotion Dysregulation Among Male and Female Young Adults. Psychol Rep 2023. [Google Scholar] [CrossRef]
- Abela, J.R.; Brozina, K.; Haigh, E.P. An examination of the response styles theory of depression in third- and seventh-grade children: a short-term longitudinal study. J Abnorm Child Psychol 2002, 30, 515–527. [Google Scholar] [CrossRef]
- Ross, S.; Heath, N. A Study of the Frequency of Self-Mutilation in a Community Sample of Adolescents. Journal of Youth and Adolescence 2002, 31, 67–77. [Google Scholar] [CrossRef]
- Hooley, J.M.; Franklin, J.C. Why Do People Hurt Themselves? A New Conceptual Model of Nonsuicidal Self-Injury. Clinical Psychological Science 2018, 6, 428–451. [Google Scholar] [CrossRef]
- Gholamrezaei, M.; De Stefano, J.; Heath, N.L. Nonsuicidal self-injury across cultures and ethnic and racial minorities: A review. Int J Psychol 2017, 52, 316–326. [Google Scholar] [CrossRef]
Figure 1.
Structural model for the mediating role of internalizing and externalizing problems in the relationship between ER modes and NSSI in the Belgian sample.
Figure 1.
Structural model for the mediating role of internalizing and externalizing problems in the relationship between ER modes and NSSI in the Belgian sample.
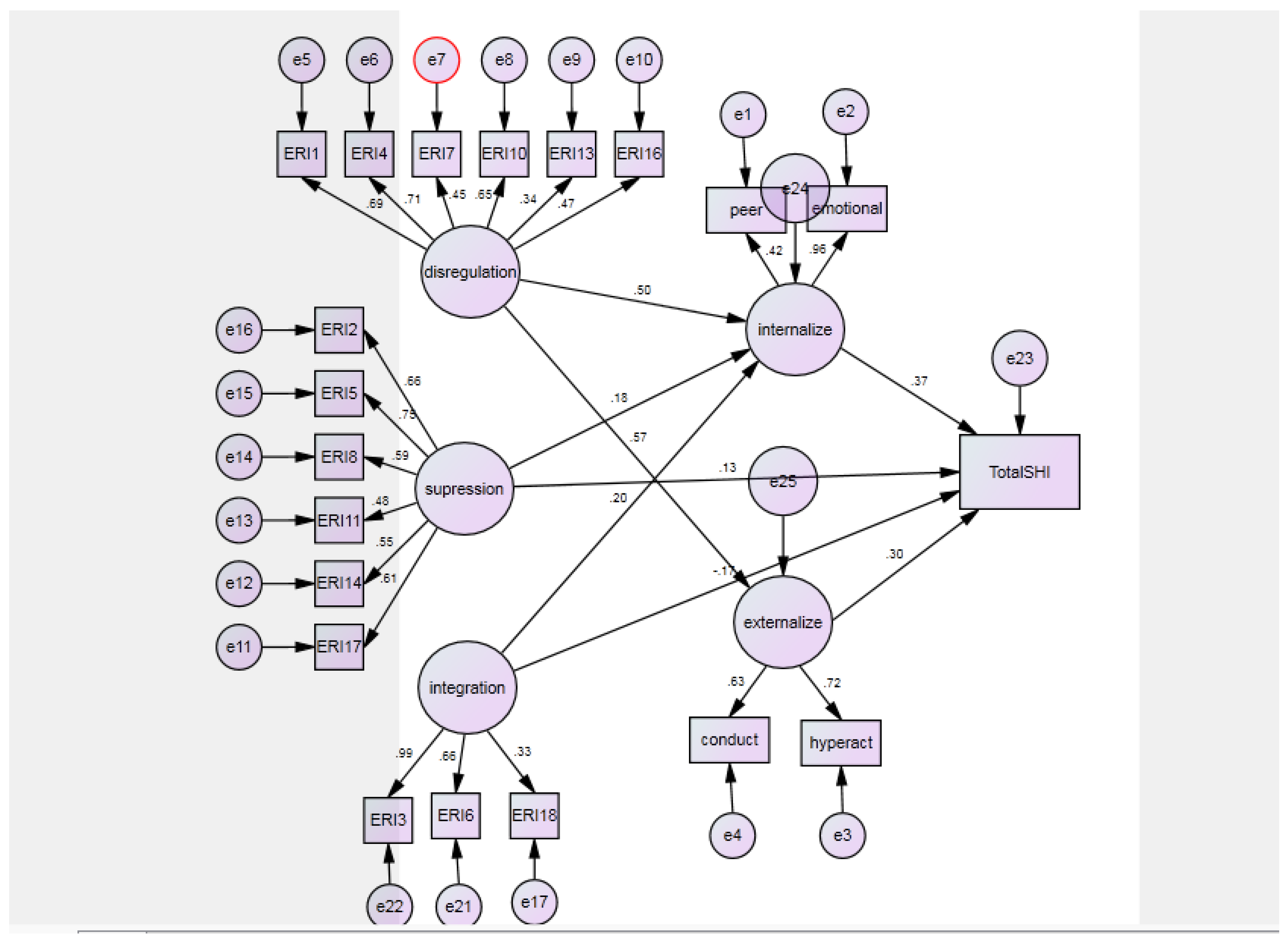
Figure 2.
Structural model for the mediating role of internalizing and externalizing problems in the relationship between ER modes and NSSI in the Iranian sample.
Figure 2.
Structural model for the mediating role of internalizing and externalizing problems in the relationship between ER modes and NSSI in the Iranian sample.
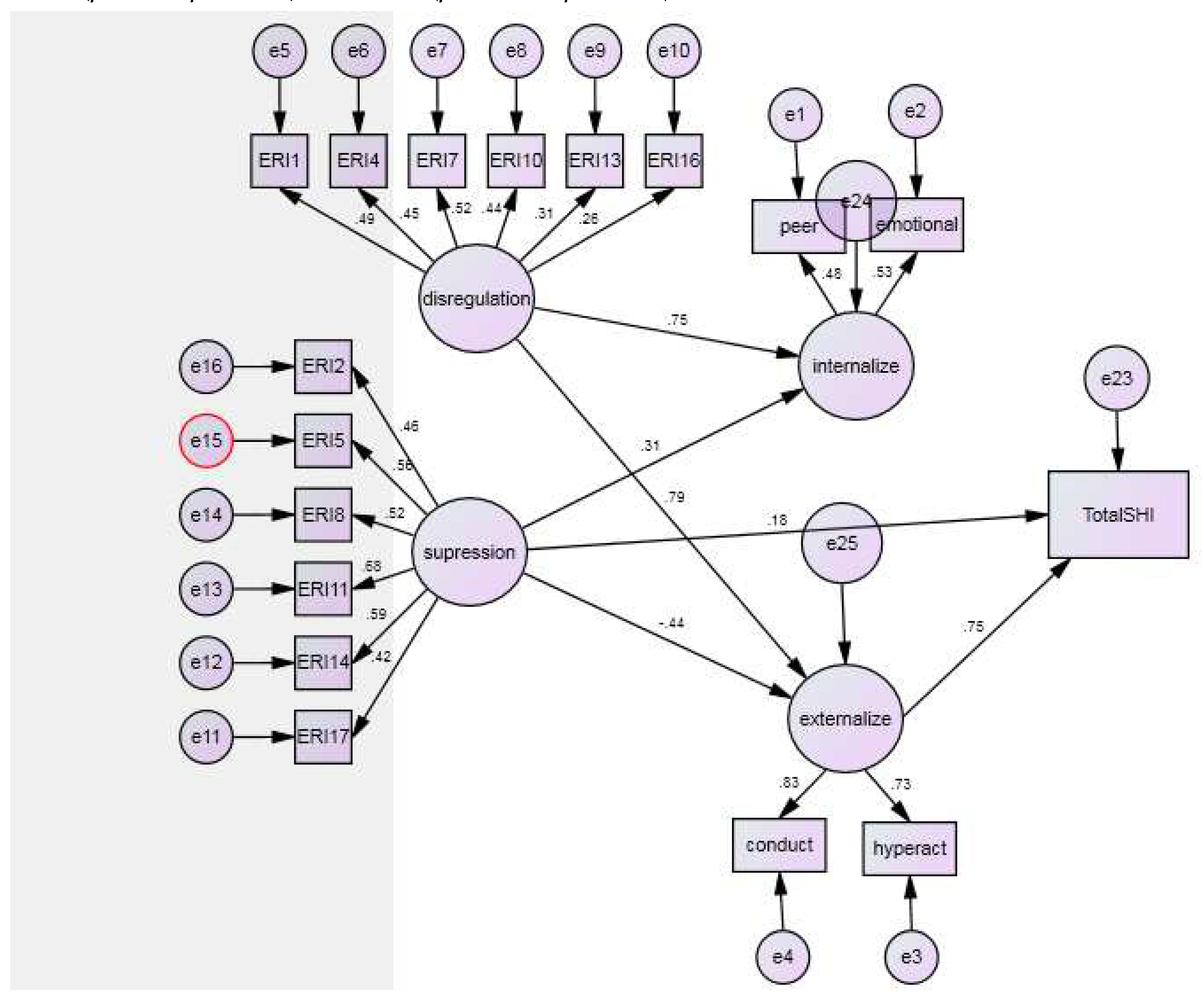

Table 1.
Correlation, Means, and Standard Deviations for ER and Maladaptive Symptoms.
| Variables | M (SD) | 1 | 2 | 3 | 4 | 5 | 6 |
| 1.INT | 7.52 (3.26) | 1 | |||||
| 2.EXT | 5.65 (3.83) | 0.06 | 1 | ||||
| 3.NSSI | 2.10 (2.09) | 0.16** | 0.54** | 1 | |||
| 4.DER | 2.77 (.75) | 0.29** | 0.43** | 0.38** | 1 | ||
| 5.SER | 3.21 (.84) | 0.32** | -0.37** | -0.18** | -0.07 | 1 | |
| 6.IER | 2.98 (.79) | -0.09 | 0.11 | 0.001 | 0.14* | -0.19** | 1 |
Note. INT = Internalizing problems and EXT = Externalizing problems. ** Correlation is significant at the 0.01 level. * Correlation is significant at the 0.05 level.
Table 2.
Means, Standard Deviations, and bivariate correlations between the variables for Iranian (n = 117) and Belgian (n = 107) samples.
Table 2.
Means, Standard Deviations, and bivariate correlations between the variables for Iranian (n = 117) and Belgian (n = 107) samples.
| Variables | M (SD) Belgium | M (SD) Iran | 1 | 2 | 3 | 4 | 5 | 6 |
| 1.INT | 1 | 0.32** | 0.27** | 0.31** | 0.21* | -0.03 | ||
| 2.EXT | 0.22* | 1 | 0.57** | 0.48** | -0.26** | 0.11 | ||
| 3.NSSI | 0.39** | 0.33** | 1 | 0.42** | -0.13 | -0.03 | ||
| 4.DER | 0.39** | 0.38** | 0.32** | 1 | 0.04 | 0.13 | ||
| 5.SER | 0.15 | -0.03 | 0.19* | -0.04 | 1 | 0.05 | ||
| 6.IER | 0.02 | -0.14 | -0.2* | 0.09 | -0.19* | 1 |
Note. INT = Internalizing problems, EXT = Externalizing problems, Upper half correlations = Iran, Lower half correlations = Belgium. ** Correlation is significant at the 0.01 level. * Correlation is significant at the 0.05 level.
Table 3.
Means differences for ER modes and internalizing and externalizing problems between two countries.
Table 3.
Means differences for ER modes and internalizing and externalizing problems between two countries.
| Variables | Iran (n = 117) | Belgium (n = 107) | F |
| M (SD) | M (SD) | ||
| DER | 2.68 (0.74) | 2.86 (0.76) | 3.215 |
| SER | 3.65 (0.71) | 2.72 (0.71) | 95.9** |
| IER | 2.79 (0.82) | 3.19 (0.69) | 15.04** |
| Internalizing | 8.55 (2.6) | 6.39 (3.55) | 27.03** |
| Externalizing | 3.81 (3.3) | 7.57 (3.53) | 67.5** |
** Difference is significant at the 0.01 level. * Difference is significant at the 0.05 level.
Table 4.
Hierarchical regression analysis for the role of age, gender, country, and ER modes in the prediction of NSSI and internalizing and externalizing problems.
Table 4.
Hierarchical regression analysis for the role of age, gender, country, and ER modes in the prediction of NSSI and internalizing and externalizing problems.
| NSSI | ||||||
| β | SE | B | T | |||
| Model 1 | Age | -0.07 | 0.13 | -0.13 | -0.99 | |
| Gender | -0.02 | 0.26 | -0.09 | -0.36 | ||
| Country | -0.44 | 0.32 | -1.85 | -5.76** | ||
| Model 2 | Age | -0.04 | 0.12 | -.080 | -0.62 | |
| Gender | -0.02 | 0.24 | -1.13 | 0.46 | ||
| Country | -0.46 | 0.33 | -1.92 | -5.69** | ||
| DER | 0.35 | 0.16 | 0.97 | 5.96** | ||
| SER | 0.05 | 0.16 | 0.13 | 0.81 | ||
| IER | -0.15 | 0.16 | -0.41 | -2.59 | ||
| Internalizing and Externalizing problems | ||||||
| β | SE | B | T | |||
| Model 1 | Age | -0.07 | 0.37 | -0.33 | -0.89 | |
| Gender | -0.13 | 0.70 | -1.42 | -.2.01 | ||
| Country | -0.17 | 0.86 | -1.86 | -2.14 | ||
| Model 2 | Age | -0.06 | 0.33 | -0.28 | -0.84 | |
| Gender | -0.60 | 0.63 | -0.63 | -1.00 | ||
| Country | -0.14 | 0.87 | -1.49 | -1.71 | ||
| DER | 0.49 | 0.42 | 3.45 | 8.18** | ||
| SER | 0.00 | 0.43 | 0.01 | 0.04 | ||
| IER | -0.05 | 0.41 | -0.36 | -0.88 | ||
Note. NSSI Model: F = 14.56**, R2 = 0.16, Adjusted R2 = 0.15 (Model 1), F = 15.30**, R2= 0.30, Adjusted R2 = 0.28 (Model 2). Internalizing and Externalizing Model: F = 3.44, R2 = 0.04, Adjusted R2 = 0.03 (Model 1), F=13.41**, R2 = 0.27, Adjusted R2 = 0.27 (Model 2).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



