Submitted:
11 December 2023
Posted:
12 December 2023
You are already at the latest version
Abstract
Premortem clinical diagnoses and postmortem autopsy findings do not match throughout history. These clinicopathological discrepancies are expected to be raised during the coronavirus disease 2019 (COVID-19) pandemic due to increased pressure on healthcare. At the same time, autopsies and clinicopathological discrepancies accurately display the quality of the healthcare system. To assess that, we examined the relevant works of literature according to the PRISMA-based protocol. As discrepancy rate changes in the correlation to the length of stay in the hospital, we also checked whether studies with patients from the intensive care unit (ICU) differed in discrepancies significantly. We found overall risk differences pretty much alike in "pre-COVID" and "during the pandemic" groups of studies. Based on that, we concluded that healthcare quality did not drop significantly during the pandemic. Be it as it may, the pandemic exposed some shortcomings in mortem healthcare regarding consensus to the autopsy, organ retention, burial, and the postponed burial or the digitalization of post mortem healthcare. All of these issues should be addressed in the future.
Keywords:
autopsy
; discrepancy
; post mortem healthcare
Modern burden
Since the first medicolegal autopsies in 13th century Italy, they have always been accompanied by a specific rate of cases where autopsy reveals significant disease unknown to the clinicians before death - clinicopathological discrepancies [1]. Since the coronavirus disease 2019 (COVID-19) brought about a significant challenge to healthcare, autopsies are an excellent quality marker and a valuable educational tool [2,3,4]. With that in mind, we set out this research to find out how much (if it did) COVID-19 influenced clinicopathological discrepancies and, thus, healthcare quality. Aside from that, some new approaches to the earliest paradigm of autopsy have been presented, considering the post-COVID era and some modern developments.
Although autopsy remains an essential tool for quality assurance at the same time, it reveals or confirms the cause of death and provides information that may differ significantly from the premortem clinical impression. At times, it happens in 1 of 3 autopsies [2]. Zehr and colleagues found a somewhat smaller proportion. They claim that autopsy found over 20% of discrepancies compared to premortem clinical impression [5,6]. Discrepancies had decreased significantly over time, but their rate was still high in 2010 [2], and in "COVID era" circumstances, it nonetheless accounts for approximately one-third of all postmortems.
Discrepancies
Despite its discrepancies compared to clinical records, Autopsy remains the gold standard as the ultimate diagnostic procedure [7,8]. It is a standard of post-mortem healthcare and an important tool to advance medical knowledge [8].
The diagnostic discrepancy does not equal diagnostic error (see Table 1 for the classification). Diagnostic error is a condition that could harm the patient, with no acceptable grounds and no scientific data for defense. Discrepancy refers to a reasonable difference or a divergence of opinion about a finding or diagnosis [9].
Premortem clinical diagnoses and postmortem findings do not match throughout history, constantly underscoring the need for enhanced surveillance, monitoring, and treatment. In 2003, a Command Paper by "Luce's group" was presented to Parliament in the UK. That report established the lack of evidence about the utility and justification for coroners' autopsies in 18%. That was the proportion of coroners' autopsies where
findings did not support the clinical course. Nevertheless, the results of most analyses nowadays indicate that discrepancies remain at a 10% rate, even in the face of advances in diagnostic techniques; these findings are sustained when data are adjusted for time and geography. Clinical history was given in the autopsy report in 76% of cases. Tissue samples for histopathology were retained in only 13% of the coronial autopsy cases; this increased to 19-55% in the subsequent reports [10,11]. For instance, from the initial 50% of autopsies findings that were unsuspected before death and 18% did not support the clinical course [10,12], in 2017, significant findings that had not been clinically detected were found in19.5% [13]. Conversely, the study of Sonderegger-lseli et al. from 2000 noticed a substantial decline in the frequency of major discrepancies increase in the rate of minor diagnostic errors [14].
The trend line for the plot in Figure 1 should help visualize a tendency of the constant presence of clinicopathological discrepancies.
Standards and Apophenic vs. Evidence-based Forensic Medicine
Perhaps the perennial persistence of discrepancies rests in the practice of forensic pathologists to rely on experience and individual customary practice in formulating their opinion. Such a feature might be a potential source of error in formulating conclusions. Case reports, found so dear in forensic medicine, are detailed descriptions the of the circumstances, physical presentations, medical features, treatments, and unique features of an individual case that advance medical and forensic sciences. Moreover, it has educational value [23]. On the other hand, forensic pathology is a major discipline of forensic medicine. It provides evidence to determine the effects of injury, toxic substances, and disease, focusing on criminal law. Since reports of that practice vary considerably in quality between individuals and between centers, the fact that no internationally accepted recommendations exist certainly does not provide for it [24].
Relying on experience and customary practice will make room for the tendency to perceive meaningful connections between unrelated things and recognize patterns that do not meaningfully exist – apophenia [25,26]. Although the word has a negative connotation, I firmly believe that the reliability of expert opinions originates in evidence-based practice. The methodology by which forensic pathologists formulate their opinions and recommendations on reporting and communicating is not always transparent and reflects the differences in the scope and role of forensic medical services and local settings.
We must also consider the methodology of work and report creation by pathologists in a hospital environment. Pathologists take tissue/histological samples during autopsies and formulate the main disease and the immediate cause of death in their reports, based on which they submit data to the central statistical institute, which is all regulated by the rulebook on filling out the death certificate, which in turn is established as part of the law on health care (a specific example in Croatia [27]). Pathologists "arrange" their diagnoses pathophysiologically, and the order is often not within the "expectations" of clinicians. The main disease is not necessarily COD; the pathologist places it first. Clinicians often disagree due to a simple misunderstanding of the pathohistological methodology. Sometimes, they simply name it differently. For example, a pathologist will not name respiratory insufficiency as such. Why is that? They cannot say that the patient does not breathe well - they examine a dead body, not a living patient. The pathologist could name it pulmonary edema if he finds reddish homogeneous content in the alveoli and blood vessels filled with blood in the septal area of the alveolar tissue. The clinician could see that very strange and say that the patient did not have symptoms of pulmonary edema. In that case, the pathologist understands that the clinician is not wrong, but the clinician hears a different statement, often an incriminatory one. Therefore, sometimes it is necessary to understand and incorporate the human side (ego), when we observe a lack of cooperation between the pathologist and the clinician if the pathologist "points out a mistake". Fortunately, there are fewer such cases, given that those pathologists were brought up in the manner that "our mistakes are kept in paraffin blocks and can be proven". During professional training of pathologists, it is expected to make mistakes. It is usual for a colleague to show his mistakes and emphasize them to teach colleagues around him not to repeat the same mistakes. As far as statistics are concerned, it is also essential to emphasize the increasingly clear trend of decreasing the number of autopsies due to better diagnostics before death and at the expense of the fact that the end is often determined as part of a long-standing malignant disease. In hospitals, it is illogical that material, time, and human resources are spent, relatively speaking, on the dead when they can be used for the living. As a result, autopsies are often not performed when the cause of death is clear, when the clinician, pathologist, family, and director of the institution agree that the autopsy is not necessary. It is important to emphasize that this does not result in a loss of quality but a loss of accuracy and completeness of the statistics. That is why statistical data on the cause of death are often based on clinical knowledge, not on the autopsy report, and it is not possible to speak about the discrepancy between the clinical opinion and the autopsy report. The statistics are also affected by the number of patients who do not die in hospitals but who die at home. In some European countries, there is no coroner`s office linked to the police department, and often, even forensic pathology departments are not related to the police departments. The lack of medical staff is seen in these countries also in this field, and the coroner that fills out the death certificate needs not to be a doctor but a specially trained nurse or even not even a nurse. On the one side, the teaching facilities are constantly confronted with the needs of" students; on the other side, there are pathology or forensic medicine departments with available human material from postmortems. In between are many legal challenges related to the substantial commodity value of bodily material [28,29,30]. Teaching, laboratory quality control, and research rely on human tissue [3]. So, the data from 2006 shocks. In 2006, 65% of autopsy reports in the UK did not indicate whether histology samples were obtained - even though these were formally retained in no more than 13% of the cases of coronial autopsy [10,31,32,33]. With time, this number is 19-55% due to implementing a "new" consent process [34]. Partly, persistency is a consequence of the COVID-19 chrissis, but with the origin as long ago as in the margins of organ retention controversy (from Bristol's first organ scandal [35,36] in 1998, the Alder Hey organs scandal" in the UK, or a case of New Zealand's hospital [37,38,39]. Reacting to the Alder Hey organs scandal, another Act of the Parliament of Great Britain was brought about in 2004 – known for its colloquial name "The Human Tissue Act 2004" [40,41,42]. In that same vein, the British Anatomy Act of 1977 was modified for the territory of Australia into The Human Tissue and Anatomy Legislation Amendment Act in 2003 [43,44]. Rigorously, this regulation permits the retention of human tissue post-mortem. That refers to cases of non-coronial autopsies [45], and only if an adult deceased had given consent to such use [46], unambiguously and without revocation, though [47,48]. Post mortem management of organs (or body parts) needed regulation throughout the past, so to sustain the integrity of this review, it will be started with "the Murder Act 1751," an Act of the Parliament of Great Britain that defines that only the corpses of executed murderers could be used for dissection [49,50]. It remained so for over eighty years, when another Act of Parliament was passed, permitting medical students and teachers in general, but particularly in anatomy, to dissect donated bodies.
Removal, retention, and disposal of human tissue that was unapproved during the period 1988 to 199 caused a profound crisis in organ handling postmortem [51,52]. That crisis could have had implications for the care of any patient [53], but publicity was especially stroked by the fact that many of these cases were children's organs [54]. Over 2,000 containers with children's body parts were revealed at the hospital in Liverpool [41,55]. As a result of organ shortage in medical education [56,57], there have been many discussions in past years worldwide. Explaining tissue from the living patients is covered by practical laws from a healthcare d. domain, and always requires consent. In the context of post mortem healthcare, it is different; it is almost grotesque to insist on informed consent to perform an autopsy [58,59]. Generally, next of kin are not well informed when consenting. Consent is repeatedly required to remove tissue from the body of a deceased person and store or use it for research, including when the removal for this purpose has taken place during a coroner's postmortem examination. Nowadays, the worldwide trend in handling human organs is consent. Not only does it help to encourage trust and respect between researchers and grieving families, but it is legally required to store and use 'relevant material from the living or deceased for a 'scheduled purpose' such as research. It is indeed a global standard. In Zambian children, the rate of consenting autopsy was merely 25% [60]; on the other hand, a Jamaican study reports a consent rate of 65% [61].
In spite the consent for an autopsy, next of kin's permission for the use of organs/tissue for scientific research and education seem to exhibit persistent falling rate. removal of The guidelines from the European Parliament and Council advised that postmortem consent forms should include a section explicitly addressing the issue of organ retention [62,63]. Hospital and mortuary staff should be educated on brain and spinal cord donations programs, with a prerogative of availability of such. These are cases where consent is usually specific to the project itself, however in more vague cases-more generic consent to include storage and future use. If seeking generic consent, researchers should prudently weight how much information to provide to potential participants of a certain study so that they could easily understand the significance of their contribution' scope and its future use. Briefly, researchers should foresee how samples might be used in the future. Fortunately, rigorous standards on required consent do not apply for education or training.
So, as there are neither independent guidelines nor a federal law on postmortem examination practices, the authority to conduct an autopsy comes from the state law. Moreover, it rests totally in the authority of a coroner or medical examiner to decide whether a postmortem will be requested. However, only a few states' Statutes address the issue of retention of remains verbatim.
However, by no means can the answer to the organ retention question be considered vague or incomplete. This issue is regulated under the common law, which originates from the seventeenth-century England and is summarized in the Restatements of the Law series for the Court use. However, due to the absence of any federal law and national guidelines on postmortem examination practices), cases of unconsented" collection/retention of organs" come to the public occasionally. So, the case law, is ambiguous and outdated [64].
The impact of COVID-19
At the end of 2019, few acute respiratory syndrome cases were reported in, Chinese Wuhan City, Hubei province, which was the beginning of more than three years of a worldwide catastrophe. After asymptomatic transmission, sometimes disease escalates up to the risk of death (in case of co-morbidities). As no effective control options or widespread diagnostic testing were available, social distancing or even generalized lockdowns were introduced [65,66].
As overall mortality increased worldwide and disease presented an excess burden to healthcare, our study aims to compare the rate of clinicopathological discrešamcies of cases referred for Autopsy during the period of the COVID-19 pandemic versus the cases referred before the pandemic.
Literature search
Literature databases–PubMed, Web of Sciemce amd the Scopus were searched for "discrepancy" and "autopsy", in two separate searches. The first search covered all published work before March 11th, 2020 [when World Health Organization (WHO) declared a COVID-19 pandemic].The other search(see Figure 2) covered all published studies between March 11th, 2020 and May 5th, 2023, when WHO ended the global emergency status for COVID-19. We removed duplicates, single-case reports, and non-English articles in both searches. We also eliminated articles on intensive care unit (ICU) patients only, as ICUs are known for meticulously scrutinizing their patients [67].
Scrutiny of intensive care unit as an exclusion criterion
End-of-life care in the ICU and subsequent postmortem healthcare (the Autopsy) have been made challenging to quantify by poor documentation in the medical record [68,69]. Patients who stay longer are more likely to develop and, subsequently, have a major error discovered post-mortem [70]. After a short hospital stay, it is reasonable to expect the surprising findings at the Autopsy [71]. Discrepancies that follow ICU. stay are interesting as time spent in the ICU. before death means a great scrutiny. A word is that longer ICU stay may increase the chance of developing g an infectious process, only to be uncovered at post-mortem examination [70,72].
Unfortunately, not even being critically ill and under the scrutiny that follows ICU. makes patients proof to common diagnostic errors. Though, Pastores et al. in 2007 reported of 26% of patients had major missed diagnoses. Regarding discrepancies of premortem clinical diagnoses and postmortem autopsy findings in critically ill, class I discrepancies were due to opportunistic infections (67%) and cardiac complications (33%), whereas class II discrepancies were due to cardiopulmonary complications (70%) and opportunistic infections (30%) [73]. To avoid this "scrutiny bias", we randomly selected 5 ICU-patients (Figure 4) only studies that turned out to be pretty heterogenous (Tau² = 0.02; Chi² = 27.47, df = 4 (P < 0.0001); I² = 85%, for overall effect Z = 7.62 (P < 0.00001) (see Figure 3).
Meta-analysis of findings
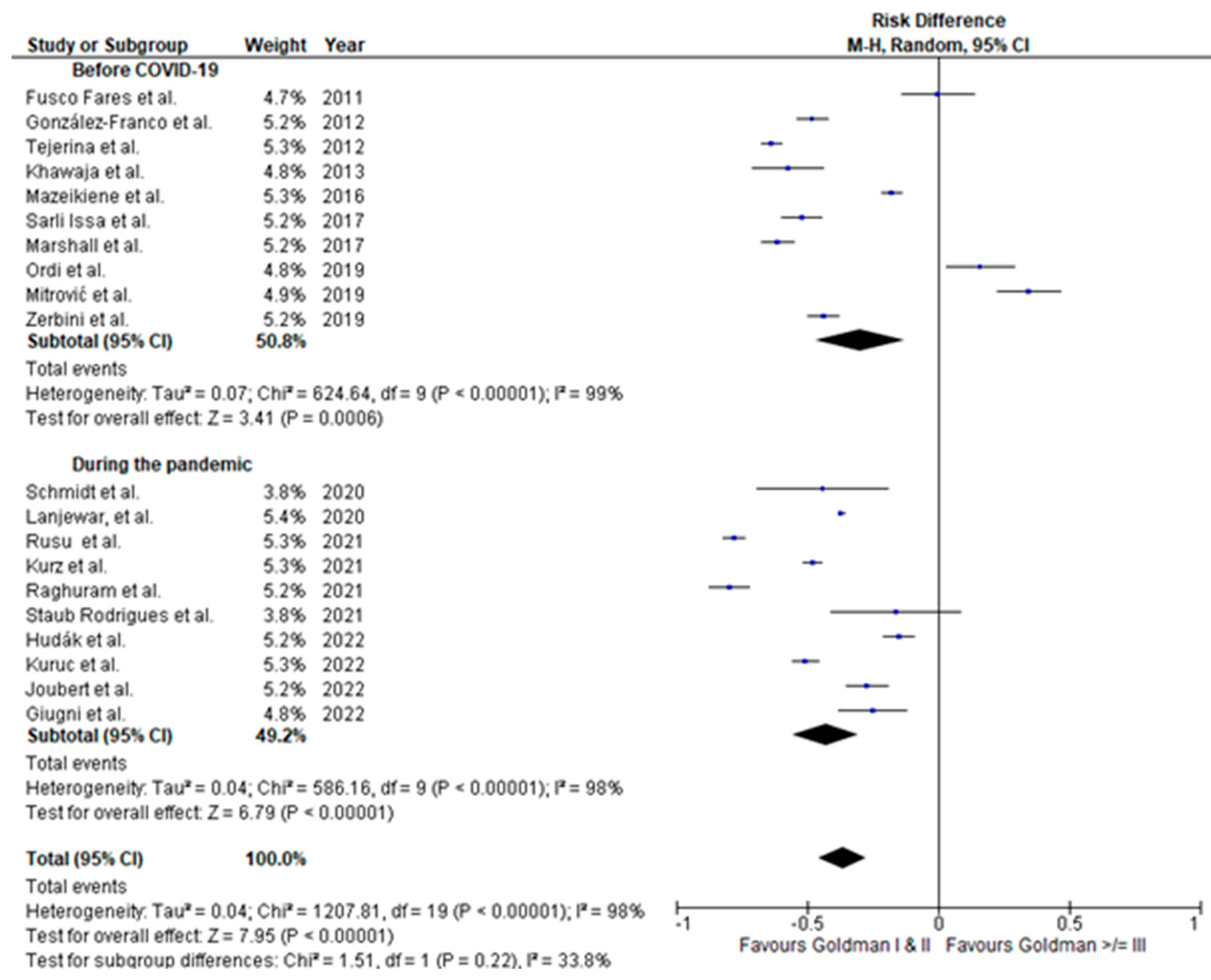
Overall heterogeneity for all studies from the "pre-COVID" and the time during the COVID-19 was very high (tau² = 0.04; ᵡ² = 1207.81, df = 19 (P < 0.00001); I² = 98%) with overall effect Z = 7.95 (P < 0.00001). Test for subgroup differences: Chi² = 1.51, df = 1 (P = 0.22), I² = 33.8%. As per subgroups, the "pre-COVID" subgroup exhibited heterogeneity of tau² = 0.07; ᵡ² = 624.64, df = 9 (P < 0.00001); I² = 99%; compared to tau² = 0.04; ᵡ² = 586.16, df = 9 (P < 0.00001); I² = 98% in a "during the pandemic" subgroup. On the level of a effect, it is Z = 3.41 (P = 0.0006) in the "pre-COVID" subgroup vs. Z = 6.79 (P < 0.00001) in the a "during the pandemic" subgroup (see Figure 4).
Figure 4.
Forest plot of comparison of clinicopathological discrepancies before and during the pandemic; plot for risk differences with random effect sizes.
Figure 4.
Forest plot of comparison of clinicopathological discrepancies before and during the pandemic; plot for risk differences with random effect sizes.
Forensics in the Society 5.0
The highly new concept of Society 5.0 is like a guide to social development and can profoundly impact all points of society. It emphasizes the potential of the individual–technology relationship [74]. This leap forward furthers the upgrade of the quality of life of all people in a sustainable world [75].
Machine learning (ML) and artificial intelligence (AI) approaches are indispensable components of this concept and have revolutionized multiple disciplines; therefore, they might revolutionize even post mortem healthcare [76,77]. AI has the potential to outperform most forensic pathologists and may soon automate and standardize some processes [78]. For instance, an AI-augmented forensic laboratory offers the most elegant method of dodging space limitations. We are all aware of how needed space is in the forensic laboratory as there is a requirement to store several thousands of images and physical archives [79,80]. In this context, demands for data storage make artificial neural networks (ANNs) and AI as supreme acquisitions [81,82,83,84].
On the other hand, progress in computing programming has ignited diligence for learning the AI-constructed machines built for the high-dimensional output of data [85]. A model for the near future comprises the forensic medicine specialist skilled in toxicology enhanced by a real-time artificial intelligence system's second review [4,86].
Machines should be trained and validated by toxicology, in subjects that cover diverse and representative clinical cases, as seen usually in everyday practice [87]. This would result in an AI system that can handle large numbers of toxicological reports without the potential disturbances commonly experienced by professionals in the field (space or time limitations, for instance) [88,89]. Such a system would drastically alleviate daily work's heavy clinical burden and be a generalizable tool for other professions with similar background knowledge.
Basically, deep learning AI models are currently used in analytical procedures as an assessment tool to help with efficiency, consistency, and decision-making. This all leaves a more professional outlook of an organized environment. Unfortunately, a human - specialist still needs to be at the center of the assessment. By all accounts, this will remain so, at least for the near future [90,91].
Documentation and Professional Approach
To maintain the efficiency of the organ or entire body donation process, there must be asserted communication among all the participants. Standardized templates must be available, and effective process management must be assured [92,93,94]. With fewer autopsies performed worldwide in recent times and with a reduced influx of tissue for research and education, delayed and incomplete autopsy reports undercut trust and respect between clinicians and families, as both do not receive information in a timely fashion [95,96].
Improvements in the autopsy reporting system and the coronial system's management are To be completely honest, waiting for the tissue to be processed or document to be signed are all significant sources of delay and ineffectiveness [97,98]. This refers especially to families, whose trust needs to be upheld at the first place.
Instead of experiencing heightened anxiety waiting for report and documents regarding body handover, some guidelines mandated by meritorious society.
Together with improvements of the consent process, this should all prepare families to consent to retain organs and the possibility of their return. Ultimately, this would provide teaching aids for the anatomy curriculum. In favor of that go individualized tracking sheets and other improvements on autopsy reporting system, as part of the continuous performance improvement (CPI) [98,99].
Improving willingness to donate (to consent) and appreciate greater professionalism would help establish a set of intermediate deadlines for each case, corresponding to the various stages in the reporting process. It seems practical to advocate flexible deadlines to accommodate he work schedules of involved staff and the office. Loose-leaf binders for each case with outside flow sheet and interior pockets, as those created by Siebert sound helpful in tracking deadlines. including wall-mounted status board to display the progress of each case. Professional notion of the institution, and consequently willingness to donate organ, certainly heighten a weekly, 1-hour autopsy conference where cases are reviewed. Not only does this raise clinical significance of each presented case, but scientific aspects of the case are also addressed. Also, this is a great opportunity to discuss approaching deadlines.
Factors that influence donation willingness relevant for transplantable organs (such as–mistrust in the healthcare system, perceptions about organ donation, and respect for the corpse, religious beliefs, and family factors), seldom apply for materials retained at the Autopsy. In these cases, generally no consenting process was acknowledged, whatsoever. Aside well conceptualized, however not popular enough body (Department of Anatomy) and tissue (Department of General Pathology) donation/retention programs at the University of Rijeka Faculty of Medicine, Croatia lacks well well-established program of this kind.
During the Autopsy, as a part of checklist, it should be recognized that organ retention might be necessary. And when it is required, a form in that sense is sent to the coroner, who asks for written confirmation from the family regarding disposition by either cremation or return.
The process of informing family members of the autopsy procedure and how it would affect an open casket viewing, and the process of afterward tissue sharing. Ultimately. this procedure aimed to obtain approved/signed informed-consent forms (in person, with a witness present; whenever possible), before or after the patient's death. This approach boosted consent rates over the time, and a case study by DeWire et al. confirms so. Namely from 2013 to 2018 number of autopsies performed upon such an informative approach increased arrowhead.
Postponed Burial and Retention of Organs
Autopsy rate as a percentage of all deaths declines worldwide and even though we lack national indicators, there is a reason to believe that this negative trend might be one of the reasons for organ shortage to our end [48,56,97,100]. Despite the popular understanding of autopsy as a "not so central" procedure in modern clinical practice [101] there are situations where still after an autopsy pathologists retain tissue for few says to examine its histopathological features in more detail, what can lead to an inevitable delay in burial [95,96].
Typically, at least in European culture, funerals take place within one week after death, given all arrangements can be made within that time. This depends on secular emotional, cultural, or religious considerations. Logistics informing families on organ retention and their return was found difficult and barely possible [102]. The delay was studied during inquiries in the Great Britain, and a number of days that lapsed between the date the autopsy was performed and that the autopsy report was issued was taken into account. This time varied considering whether histology samples were taken, and the median number of 4 days (range 0-255) was found to have lapsed in cases that did and [15 (0-255)] did not [2 (0-144)] take histology samples. In situations where all diagnoses, thus the cause of death, are evident from the gross examination, pathologist's report can be rapidly transmitted to the coroner. If the autopsy report is delayed, it can significantly slow down the medicolegal process, and cause distress to families who would like to know the diagnosis and see a fuller account than just the bare cause of death. On the other hand, pathologists retain tissue from an autopsy to thoroughly gross examine an organ once it is fixed or preserved with chemical treatment. Tissue retention of tissue/organs at Autopsy has probably been the most controversial of all issues around the Autopsy, especially relating to coronial autopsies. This applies to both, whole organs, and small tissue samples, as well.
The retention as a concept should be employed only for educational archives or museums for as long as the samples or specimens are held/updated. Otherwise, images from postmortem examinations and images of histological slides should be obtained. Recently, there have been major changes on issues of consent, the fundamental principle that strengthens the legislation. Although the real question is its enacting-in the complex, sensitive, and emotive area of procuring human remains.
The possible remedy for such a delay is a service that deals effectively with legal and health issues, capable of choosing a feasible test. It recognizes the space for "retention of organs" could fit only in a consolidated morgue (incorporated in the existing government-to-citizen communication channel) to a "Consolidated Administration of Death."
Conclusions
According to our findings, healthcare quality during the pandemic retained its "pre-COVID" level.
This study showed that discrepancies between clinical and postmortem examination diagnoses persist despite the medical progress. There was no evident change in the discrepancy rate during the COVID-19 pandemic. Such a finding shows the healthcare quality and efficacy of the present surveillance system/management protocols.
To overcome clinicopathological discrepancies and to improve the educational environment, a novel strategy of deep learning and AI-constructed machines should be proposed.
Consolidating morgue (incorporated in the existing government-to-citizen communication channel) to a "Consolidated Administration of Death" seems like the most promising opportunity to retain organs removed at a coroner's Autopsy lawfully instead of customary but not strictly lawful practice, thus providing a significant contribution to the discussion over changes to the retaining organs in educational purposes.
Author Contributions
IŠ and MP conceived of the presented idea. IŠ developed the experimental model and performed the computations. MP verified the analytical methods. Both authors contributed to the design and implementation of the research and discussed the results contributing to the final manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Available on request.
Acknowledgments
I.Š. acknowledges the University of Rijeka, Faculty of Medicine, for their constant support. M.P. acknowledges general hospital Pula for their constant non support.
Conflicts of Interest
The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- van den Tweel, J.G.; Taylor, C.R. The rise and fall of the autopsy. Virchows Arch 2013, 462, 371–380. [Google Scholar] [CrossRef] [PubMed]
- van den Tweel, J.G.; Wittekind, C. The medical autopsy as quality assurance tool in clinical medicine: dreams and realities. Virchows Arch 2016, 468, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Hundl, C.; Neuman, M.; Rairden, A.; Rearden, P.; Stout, P. Implementation of a Blind Quality Control Program in a Forensic Laboratory. J Forensic Sci 2020, 65, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; Group, Q.-. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Aludaat, C.; Sarsam, M.; Doguet, F.; Baste, J.M. Autopsy and clinical discrepancies in patients undergoing extracorporeal membrane oxygenation: a case series-a step towards understanding "Why"? J Thorac Dis 2019, 11, S1865–S1868. [Google Scholar] [CrossRef] [PubMed]
- Zehr, K.J.; Liddicoat, J.R.; Salazar, J.D.; Gillinov, A.M.; Hruban, R.H.; Hutchins, G.M.; Cameron, D.E. The autopsy: still important in cardiac surgery. Ann Thorac Surg 1997, 64, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Kurz, S.D.; Sido, V.; Herbst, H.; Ulm, B.; Salkic, E.; Ruschinski, T.M.; Buschmann, C.T.; Tsokos, M. Discrepancies between clinical diagnosis and hospital autopsy: A comparative retrospective analysis of 1,112 cases. PLoS One 2021, 16, e0255490. [Google Scholar] [CrossRef]
- Buja, L.M.; Barth, R.F.; Krueger, G.R.; Brodsky, S.V.; Hunter, R.L. The Importance of the Autopsy in Medicine: Perspectives of Pathology Colleagues. Acad Pathol 2019, 6, 2374289519834041. [Google Scholar] [CrossRef]
- Hall, K.K.; Shoemaker-Hunt, S.; Hoffman, L.; Richard, S.; Gall, E.; Schoyer, E.; Costar, D.; Gale, B.; Schiff, G.; Miller, K. Making healthcare safer III: a critical analysis of existing and emerging patient safety practices. 2020.
- Cooper, H.; Leigh, M.A.; Lucas, S.; Martin, I. The coroner's autopsy. The final say in establishing cause of death? Med Leg J 2007, 75, 114–119. [Google Scholar] [CrossRef]
- Ong, B.B.; Wong, J.J.; Hashim, J. A retrospective study of the accuracy between clinical and autopsy cause of death in the University of Malaya Medical Centre. Malays J Pathol 2004, 26, 35–41. [Google Scholar]
- Cooper, H.; Lucas, S.B. The value of autopsy, believe it or not. Lancet 2007, 370, 27. [Google Scholar] [CrossRef] [PubMed]
- Marshall, H.S.; Milikowski, C. Comparison of Clinical Diagnoses and Autopsy Findings: Six-Year Retrospective Study. Arch Pathol Lab Med 2017, 141, 1262–1266. [Google Scholar] [CrossRef]
- Sonderegger-Iseli, K.; Burger, S.; Muntwyler, J.; Salomon, F. Diagnostic errors in three medical eras: a necropsy study. Lancet 2000, 355, 2027–2031. [Google Scholar] [CrossRef] [PubMed]
- Tejerina, E.; Esteban, A.; Fernandez-Segoviano, P.; Maria Rodriguez-Barbero, J.; Gordo, F.; Frutos-Vivar, F.; Aramburu, J.; Algaba, A.; Gonzalo Salcedo Garcia, O.; Lorente, J.A. Clinical diagnoses and autopsy findings: discrepancies in critically ill patients*. Crit Care Med 2012, 40, 842–846. [Google Scholar] [CrossRef]
- Khawaja, O.; Khalil, M.; Zmeili, O.; Soubani, A.O. Major discrepancies between clinical and postmortem diagnoses in critically ill cancer patients: Is autopsy still useful? Avicenna J Med 2013, 3, 63–67. [Google Scholar] [CrossRef]
- Mitrovic, D.; Savic, I.; Jankovic, R. Discrepancies between clinical and autopsy diagnosis of cause of death among psychiatric patients who died due to natural causes. A retrospective autopsy study. Vojnosanitetski Pregled 2019, 76, 278–283. [Google Scholar] [CrossRef]
- Lanjewar, D.N.; Sheth, N.S.; Lanjewar, S.D.; Wagholikar, U.L. Analysis of Causes of Death as Determined at Autopsy in a Single Institute, The Grant Medical College and Sir J. J. Hospital, Mumbai, India, Between 1884 and 1966: A Retrospective Analysis of 13 024 Autopsies in Adults. Arch Pathol Lab Med 2020, 144, 644–649. [Google Scholar] [CrossRef]
- Giugni, F.R.; Salvadori, F.A.; Smeili, L.A.A.; Marcilio, I.; Perondi, B.; Mauad, T.; de Paiva, E.F.; Duarte-Neto, A.N. Discrepancies Between Clinical and Autopsy Diagnoses in Rapid Response Team-Assisted Patients: What Are We Missing? J Patient Saf 2022, 18, 653–658. [Google Scholar] [CrossRef]
- Hudak, L.; Nagy, A.C.; Molnar, S.; Mehes, G.; Nagy, K.E.; Olah, L.; Csiba, L. Discrepancies between clinical and autopsy findings in patients who had an acute stroke. Stroke Vasc Neurol 2022, 7, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Ordi, J.; Castillo, P.; Garcia-Basteiro, A.L.; Moraleda, C.; Fernandes, F.; Quintó, L.; Hurtado, J.C.; Letang, E.; Lovane, L.; Jordao, D.; et al. Clinico-pathological discrepancies in the diagnosis of causes of death in adults in Mozambique: A retrospective observational study. PLoS One 2019, 14, e0220657. [Google Scholar] [CrossRef]
- Mazeikiene, S.; Laima, S.; Chmieliauskas, S.; Fomin, D.; Andriuskeviciute, G.; Markeviciute, M.; Matuseviciute, A.; Jasulaitis, A.; Stasiuniene, J. Deontological examination: Clinical and forensic medical diagnoses discrepancies. Egyptian Journal of Forensic Sciences 2016, 6, 323–327. [Google Scholar] [CrossRef]
- Koehler, S.A. Case Reports: An Important Source of Data for Forensic Medicine and Forensic Pathology. J Crim Forensic studies 2018, 1, 180020. [Google Scholar] [CrossRef]
- Meilia, P.D.I.; Herkutanto; Atmadja, D.S.; Cordner, S.; Eriksson, A.; Kubat, B.; Kumar, A.; Payne-James, J.J.; Rubanzana, W.G.; Uhrenholt, L.; et al. The PERFORM-P (Principles of Evidence-based Reporting in FORensic Medicine-Pathology version). Forensic Sci Int 2021, 327, 110962. [Google Scholar] [CrossRef] [PubMed]
- Fyfe, S.; Williams, C.; Mason, O.J.; Pickup, G.J. Apophenia, theory of mind and schizotypy: perceiving meaning and intentionality in randomness. Cortex 2008, 44, 1316–1325. [Google Scholar] [CrossRef] [PubMed]
- Goldfarb, B.; King, A.A. Scientific apophenia in strategic management research: Significance tests & mistaken inference. Strategic Management Journal 2016, 37, 167–176. [Google Scholar] [CrossRef]
- sabor, H. Zakon o zdravstvenoj zaštiti. Available online: https://narodne-novine.nn.hr/clanci/sluzbeni/2018_11_100_1929.html (accessed on November 14th).
- Gold, E.R. Body parts: Property rights and the ownership of human biological materials; Georgetown University Press: 1996. [CrossRef]
- Seale, C.; Cavers, D.; Dixon-Woods, M. Commodification of body parts: By medicine or by media? Body & Society 2006, 12, 25–42. [Google Scholar] [CrossRef]
- Bryant, R.; Harrison, R.; Start, R.; Chetwood, A.; Chesshire, A.M.; Reed, M.; Cross, S.S. Ownership and uses of human tissue: what are the opinions of surgical in-patients? Journal of clinical pathology 2008, 61, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Mayor, S. One in four autopsy reports in UK is substandard, report finds. Bmj 2006, 333, 824. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, S.; Shafi, M.I. National Confidential Enquiry into Patient outcome and death. Obstetrics, Gynaecology & Reproductive Medicine 2007, 17, 278–279. [Google Scholar] [CrossRef]
- Lucas, S.; Cooper, H.; Emmett, S.; Hargraves, C.; Mason, M. The coroner’s autopsy: do we deserve better. London: National Confidential Enquiry into Patient Outcome and Death 2006.
- Scraton, P.; McNaull, G. Death Investigation, Coroners’ Inquests and the Rights of the Bereaved. 2021.
- Fox, R. Bristol scandal. Circulation 2001, 104, E9014–9014. [Google Scholar] [CrossRef]
- Butler, P. The Bristol royal infirmary inquiry: the issue explained. The Guardian 2002.
- Coney, S. New Zealand: organ donor registry in jeopardy. Lancet 1989, 2, 1386. [Google Scholar] [CrossRef] [PubMed]
- Streat, S.; Silvester, W. Organ donation in Australia and New Zealand--ICU perspectives. Crit Care Resusc 2001, 3, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Bauchner, H.; Vinci, R. What have we learnt from the Alder Hey affair? That monitoring physicians' performance is necessary to ensure good practice. BMJ 2001, 322, 309–310. [Google Scholar] [CrossRef] [PubMed]
- Price, D. The human tissue act 2004. The Modern Law Review 2005, 68, 798–821. [Google Scholar] [CrossRef]
- Mavroforou, A.; Giannoukas, A.; Michalodimitrakis, E. Consent for organ and tissue retention in British law in the light of the Human Tissue Act 2004. Med Law 2006, 25, 427–434. [Google Scholar] [PubMed]
- Cecchetto, G.; Bajanowski, T.; Cecchi, R.; Favretto, D.; Grabherr, S.; Ishikawa, T.; Kondo, T.; Montisci, M.; Pfeiffer, H.; Bonati, M.R.; et al. Back to the Future - Part 1. The medico-legal autopsy from ancient civilization to the post-genomic era. Int J Legal Med 2017, 131, 1069–1083. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, E.F.; Kramer, B.; Billings, B.K.; Brits, D.M.; Pather, N. The law, ethics and body donation: A tale of two bequeathal programs. Anatomical sciences education 2020, 13, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Manning, J. Changing to Deemed Consent for Deceased Organ Donation in the United Kingdom: Should Australia and New Zealand Follow? J Law Med 2020, 27, 513–526. [Google Scholar] [PubMed]
- Raut, A.; Andrici, J.; Severino, A.; Gill, A.J. The death of the hospital autopsy in Australia? The hospital autopsy rate is declining dramatically. Pathology 2016, 48, 645–649. [Google Scholar] [CrossRef]
- Forest, F.; Duband, S.; Peoc'h, M. The attitudes of patients to their own autopsy: a misconception. Journal of clinical pathology 2011. [Google Scholar] [CrossRef]
- Doldissen, A.; Severino, A.; Bourne, D.; Gill, A. 8. The hospital autopsy rate has fallen dramatically. Pathology 2011, 43, S91–S92. [Google Scholar] [CrossRef]
- Davies, D.J.; Graves, D.J.; Landgren, A.J.; Lawrence, C.H.; Lipsett, J.; MacGregor, D.P.; Sage, M.D. The decline of the hospital autopsy: a safety and quality issue for healthcare in Australia. Medical Journal of Australia 2004, 180, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Warner, J.H.; Rizzolo, L.J. Anatomical instruction and training for professionalism from the 19th to the 21st centuries. Clinical Anatomy 2006, 19, 403–414. [Google Scholar] [CrossRef] [PubMed]
- King, L.S.; Meehan, M.C. A history of the autopsy. A review. The American journal of pathology 1973, 73, 514–544. [Google Scholar] [PubMed]
- Bauchner, H.; Vinci, R. What have we learnt from the Alder Hey affair? That monitoring physicians' performance is necessary to ensure good practice. BMJ (Clinical research ed.) 2001, 322, 309–310. [Google Scholar] [CrossRef]
- Tomasini, F. Remembering and disremembering the dead: Posthumous punishment, harm and redemption over time; Springer Nature: 2017. [CrossRef]
- Castledine, G. The repercussions of the organ retention scandal. British Journal of Nursing 2001, 10, 275. [Google Scholar] [CrossRef] [PubMed]
- Seale, C.; Cavers, D.; Dixon-Woods, M. Commodification of body parts: by medicine or by media? Body & Society 2006, 12, 25–42. [Google Scholar] [CrossRef]
- Ellis, I. Beyond organ retention: the new human tissue bill. Lancet 2004, 364 Suppl 1, s42–43. [Google Scholar] [CrossRef]
- Radunz, S.; Benkö, T.; Stern, S.; Saner, F.H.; Paul, A.; Kaiser, G.M. Medical students’ education on organ donation and its evaluation during six consecutive years: results of a voluntary, anonymous educational intervention study. European Journal of Medical Research 2015, 20, 23. [Google Scholar] [CrossRef]
- Akkas, M.; Anık, E.G.; Demir, M.C.; İlhan, B.; Akman, C.; Ozmen, M.M.; Aksu, N.M. Changing Attitudes of Medical Students Regarding Organ Donation from a University Medical School in Turkey. Med Sci Monit 2018, 24, 6918–6924. [Google Scholar] [CrossRef]
- Khiani, R.; Shingler, S.; Hasleton, P. Consent for autopsy. Journal of the Royal Society of Medicine 2003, 96, 53–53. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, G.E.; Burns, J.; Johnson, J.; Mitchell, C.; Robinson, M.; Truog, R.D. Autopsy consent practice at US teaching hospitals: results of a national survey. Archives of internal medicine 2000, 160, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Lishimpi, K.; Chintu, C.; Lucas, S.; Mudenda, V.; Kaluwaji, J.; Story, A.; Maswahu, D.; Bhat, G.; Nunn, A.J.; Zumla, A. Necropsies in African children: consent dilemmas for parents and guardians. Archives of disease in childhood 2001, 84, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Gibson, T.N.; Escoffery, C.T.; Shirley, S.E. Necropsy request practices in Jamaica: a study from the University Hospital of the West Indies. Journal of clinical pathology 2002, 55, 608–612. [Google Scholar] [CrossRef] [PubMed]
- Elger, B.S.; Hofner, M.-C.; Mangin, P. Research involving biological material from forensic autopsies: legal and ethical issues. Pathobiology 2009, 76, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sarnacka, E. Models of the Legal Construct of Consent for Post Mortem organ Transplantation Illustrated by the Example of Poland, Norway and USA. Review of European and Comparative Law 2017, 29, 47–83. [Google Scholar] [CrossRef]
- Lynch, M.J.; Woodford, N.W. Objections to medico-legal autopsy--recent developments in case law. J Law Med 2007, 14, 463–468. [Google Scholar]
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19). In StatPearls; StatPearls Publishing.
- Copyright © 2023, StatPearls Publishing LLC.: Treasure Island (FL), 2023.
- Nguyen, T.; Duong Bang, D.; Wolff, A. 2019 Novel Coronavirus Disease (COVID-19): Paving the Road for Rapid Detection and Point-of-Care Diagnostics. Micromachines (Basel) 2020, 11, 306. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Gong, Y. Teamwork and Patient Safety in Intensive Care Units: Challenges and Opportunities. Stud Health Technol Inform 2022, 290, 469–473. [Google Scholar] [CrossRef]
- Esper, A.M.; Arabi, Y.M.; Cecconi, M.; Du, B.; Giamarellos-Bourboulis, E.J.; Juffermans, N.; Machado, F.; Peake, S.; Phua, J.; Rowan, K.; et al. Systematized and efficient: organization of critical care in the future. Crit Care 2022, 26, 366. [Google Scholar] [CrossRef]
- Conley, C.E. Student nurses' end-of-life and post mortem care self-efficacy: A descriptive study. Nurse Educ Today 2023, 121, 105698. [Google Scholar] [CrossRef] [PubMed]
- Mort, T.C.; Yeston, N.S. The relationship of pre mortem diagnoses and post mortem findings in a surgical intensive care unit. Crit Care Med 1999, 27, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Rusu, S.; Lavis, P.; Domingues Salgado, V.; Van Craynest, M.P.; Creteur, J.; Salmon, I.; Brasseur, A.; Remmelink, M. Comparison of antemortem clinical diagnosis and post-mortem findings in intensive care unit patients. Virchows Arch 2021, 479, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulos, G.; Piagnerelli, M.; Berre, J.; Salmon, I.; Vincent, J.L. Post mortem examination in the intensive care unit: still useful? Intensive Care Med 2004, 30, 2080–2085. [Google Scholar] [CrossRef] [PubMed]
- Pastores, S.M.; Dulu, A.; Voigt, L.; Raoof, N.; Alicea, M.; Halpern, N.A. Premortem clinical diagnoses and postmortem autopsy findings: discrepancies in critically ill cancer patients. Crit Care 2007, 11, R48. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, H.; Sasajima, H.; Takayanagi, Y.; Kanamaru, H. International standardization for smarter society in the field of measurement, control and automation. In Proceedings of the 2017 56th Annual Conference of the Society of Instrument and Control Engineers of Japan (SICE), 2017; pp. 263-266. [CrossRef]
- Carayannis, E.G.; Morawska-Jancelewicz, J. The Futures of Europe: Society 5.0 and Industry 5.0 as Driving Forces of Future Universities. Journal of the Knowledge Economy 2022, 13, 3445–3471. [Google Scholar] [CrossRef]
- Xu, Y.; Liu, X.; Cao, X.; Huang, C.; Liu, E.; Qian, S.; Liu, X.; Wu, Y.; Dong, F.; Qiu, C.W.; et al. Artificial intelligence: A powerful paradigm for scientific research. Innovation (Camb) 2021, 2, 100179. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Wang, Y.; Byrne, R.; Schneider, G.; Yang, S. Concepts of Artificial Intelligence for Computer-Assisted Drug Discovery. Chem Rev 2019, 119, 10520–10594. [Google Scholar] [CrossRef]
- Sergi, C.M. Digital pathology: the time is now to bridge the gap between medicine and technological singularity. In Interactive Multimedia-Multimedia Production and Digital Storytelling; IntechOpen London, UK: 2019. [CrossRef]
- Jaillant, L.; Caputo, A. Unlocking digital archives: cross-disciplinary perspectives on AI and born-digital data. AI Soc 2022, 37, 823–835. [Google Scholar] [CrossRef]
- Ries, T.; Palkó, G. Born-digital archives. 2019, 1, 1-11.
- Ahmed Alaa El-Din, E. ARTIFICIAL INTELLIGENCE IN FORENSIC SCIENCE: INVASION OR REVOLUTION? Egyptian Society of Clinical Toxicology Journal 2022, 10, 20–32. [Google Scholar] [CrossRef]
- Jones, A. Biochemical and physiological research on the disposition and fate of ethanol in the body. Medico legal aspects of alcohol, 5th edition, Lawyers and Judges publishing company, Tucson 2008.
- Jones, A.W. Alcohol, its analysis in blood and breath for forensic purposes, impairment effects, and acute toxicity. Wiley Interdisciplinary Reviews: Forensic Science 2019, 1, e1353. [Google Scholar] [CrossRef]
- Jones, A.W. Driving under the influence of alcohol. Handbook of Forensic Medicine 2022, 3, 1387–1408. [Google Scholar] [CrossRef]
- Aggarwal, K.; Mijwil, M.M.; Al-Mistarehi, A.-H.; Alomari, S.; Gök, M.; Alaabdin, A.M.Z.; Abdulrhman, S.H. Has the Future Started? The Current Growth of Artificial Intelligence, Machine Learning, and Deep Learning. Iraqi Journal for Computer Science and Mathematics 2022, 3, 115–123. [Google Scholar] [CrossRef]
- Svensson, A.M.; Jotterand, F. Doctor ex machina: A critical assessment of the use of artificial intelligence in health care. In Proceedings of the The Journal of Medicine and Philosophy: A Forum for Bioethics and Philosophy of Medicine; 2022; pp. 155–178. [Google Scholar] [CrossRef]
- Pantic, I.; Paunovic, J.; Cumic, J.; Valjarevic, S.; Petroianu, G.A.; Corridon, P.R. Artificial neural networks in contemporary toxicology research. Chem Biol Interact 2023, 369, 110269. [Google Scholar] [CrossRef]
- Mehrvar, S.; Himmel, L.E.; Babburi, P.; Goldberg, A.L.; Guffroy, M.; Janardhan, K.; Krempley, A.L.; Bawa, B. Deep Learning Approaches and Applications in Toxicologic Histopathology: Current Status and Future Perspectives. J Pathol Inform 2021, 12, 42. [Google Scholar] [CrossRef]
- Raju, B.; Jumah, F.; Ashraf, O.; Narayan, V.; Gupta, G.; Sun, H.; Hilden, P.; Nanda, A. Big data, machine learning, and artificial intelligence: a field guide for neurosurgeons. J Neurosurg 2020, 1, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Katz, P.S. Expert Robot: Using Artificial Intelligence to Assist Judges in Admitting Scientific Expert Testimony. Albany Law Journal of Science & Technology 2014, 24. [Google Scholar]
- Whitford, A.B.; Yates, J.; Burchfield, A.; Anastasopoulos, J.L.; Anderson, D.M. The Adoption of Robotics by Government Agencies: Evidence from Crime Labs. Public Administration Review 2020, 80, 976–988. [Google Scholar] [CrossRef]
- Mujtaba, G.; Shuib, L.; Raj, R.G.; Rajandram, R.; Shaikh, K.; Al-Garadi, M.A. Automatic ICD-10 multi-class classification of cause of death from plaintext autopsy reports through expert-driven feature selection. PloS one 2017, 12, e0170242. [Google Scholar] [CrossRef]
- Jeon, M.; Cho, H.N.; Bhang, S.Y.; Hwang, J.W.; Park, E.J.; Lee, Y.J. Development and a Pilot Application Process of the Korean Psychological Autopsy Checklist for Adolescents. Psychiatry Investig 2018, 15, 490–498. [Google Scholar] [CrossRef]
- Shkrum, M.J.; Kent, J. An Autopsy Checklist: A Monitor of Safety and Risk Management. Am J Forensic Med Pathol 2016, 37, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Burton, J.L.; Underwood, J. Clinical, educational, and epidemiological value of autopsy. The Lancet 2007, 369, 1471–1480. [Google Scholar] [CrossRef] [PubMed]
- Beukes, C. The Autopsy in the 21st Century. 2012. [CrossRef]
- Chariot, P.; Witt, K.; Pautot, V.; Porcher, R.; Thomas, G.; Zafrani, E.S.; Lemaire, F. Declining autopsy rate in a French hospital: physicians' attitudes to the autopsy and use of autopsy material in research publications. Archives of pathology & laboratory medicine 2000, 124, 739–745. [Google Scholar] [CrossRef]
- Siebert, J.R. Increasing the efficiency of autopsy reporting. Arch Pathol Lab Med 2009, 133, 1932–1937. [Google Scholar] [CrossRef]
- . [CrossRef]
- Rokoske, F.S.; Schenck, A.P.; Hanson, L.C. The potential use of autopsy for continuous quality improvement in hospice and palliative care. The Medscape Journal of Medicine 2008, 10, 289. [Google Scholar]
- Loughrey, M.; McCluggage, W.; Toner, P. The declining autopsy rate and clinicians' attitudes. The Ulster medical journal 2000, 69, 83. [Google Scholar]
- Ayoub, T.; Chow, J. The conventional autopsy in modern medicine. Journal of the Royal Society of Medicine 2008, 101, 177–181. [Google Scholar] [CrossRef]
- McDermott, A.J.; Field, C.L.; Hoopes, L.A.; Clauss, T.M. Medical Management of Coelomic Distention, Abnormal Swimming, Substrate Retention, and Hematologic Changes in a Reef Manta Ray (Manta Alfredi). J Zoo Wildl Med 2016, 47, 927–930. [Google Scholar] [CrossRef]
Figure 1.
Proportion of clinicopathological discrepancies before and during the coronavirus disease 2019 (COVID-19) pandemic according to studies by Tejerina et al.,2012; Khawaja et al., 2013; Mazeikiene et al., 2016; Marshall et al., 2017; Ordi et al., 2019; Mitrović et al., 2019; Lanjewar et al., 2020; Kurz et al.,2021; Giugni et al., 2022; Hudák et al.,2022 [7,13,15,16,17,18,19,20,21,22].
Figure 1.
Proportion of clinicopathological discrepancies before and during the coronavirus disease 2019 (COVID-19) pandemic according to studies by Tejerina et al.,2012; Khawaja et al., 2013; Mazeikiene et al., 2016; Marshall et al., 2017; Ordi et al., 2019; Mitrović et al., 2019; Lanjewar et al., 2020; Kurz et al.,2021; Giugni et al., 2022; Hudák et al.,2022 [7,13,15,16,17,18,19,20,21,22].
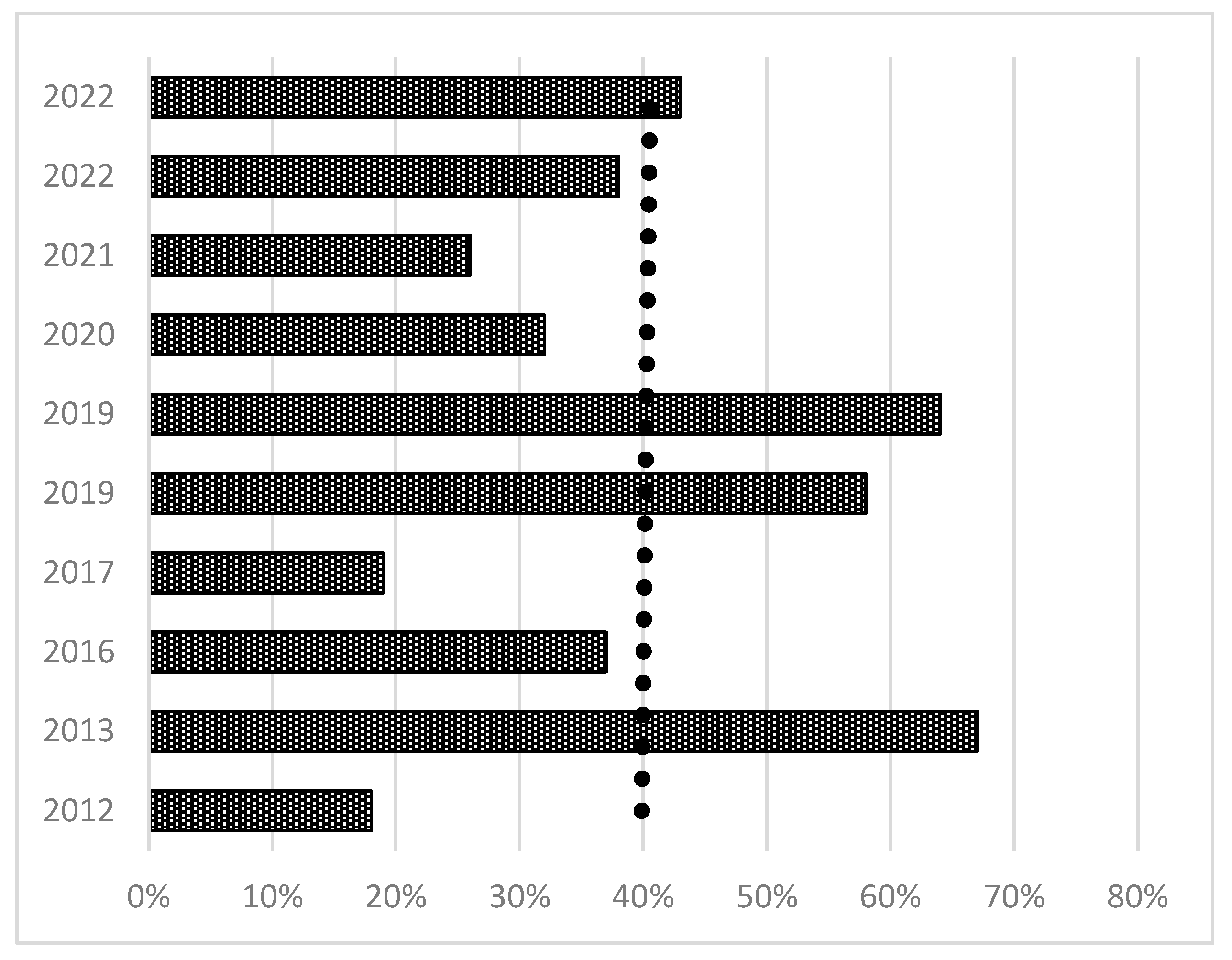
Figure 2.
Methodology of literature search for discrepancies during the COVID-19.
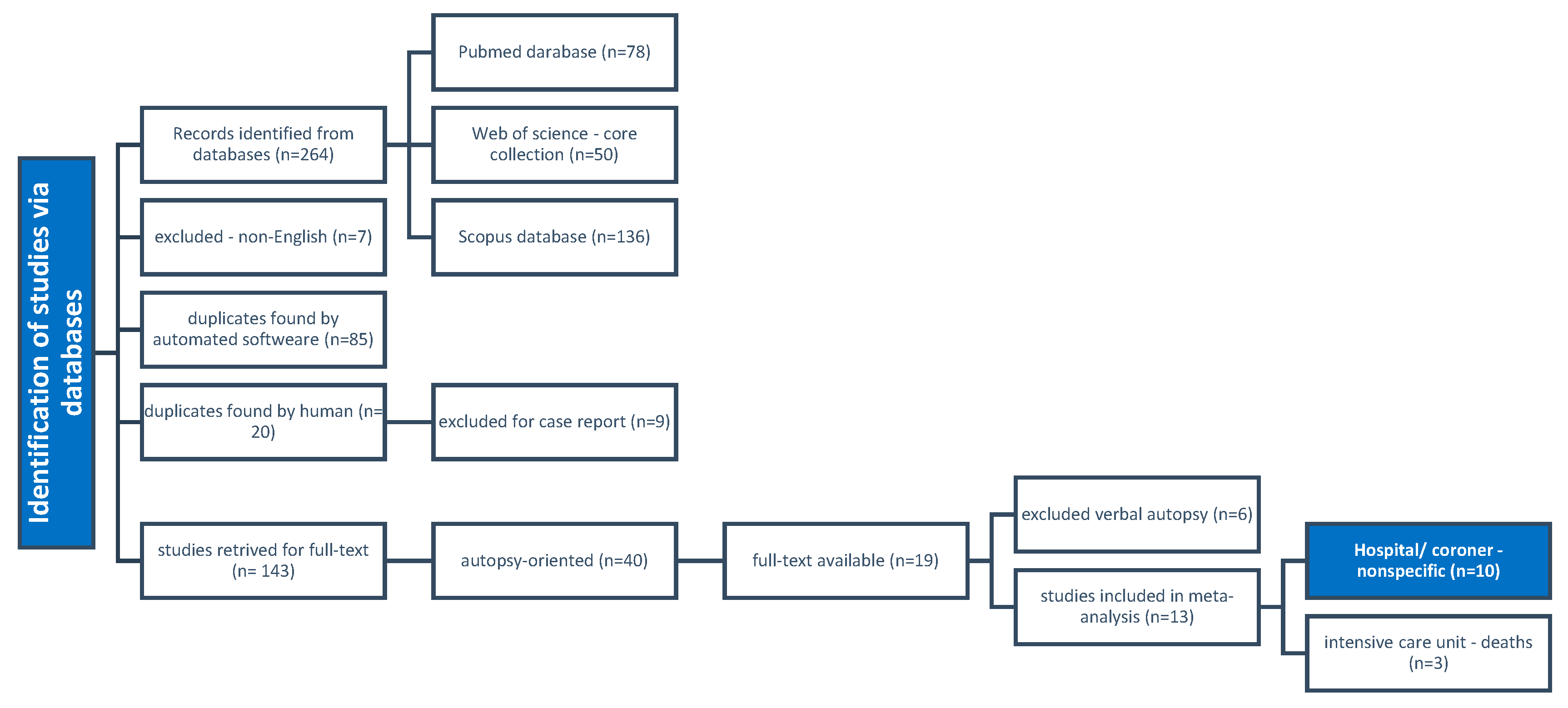
Figure 3.
Discrepancies among intensive care patients; plot for risk differences with random effect sizes.
Figure 3.
Discrepancies among intensive care patients; plot for risk differences with random effect sizes.
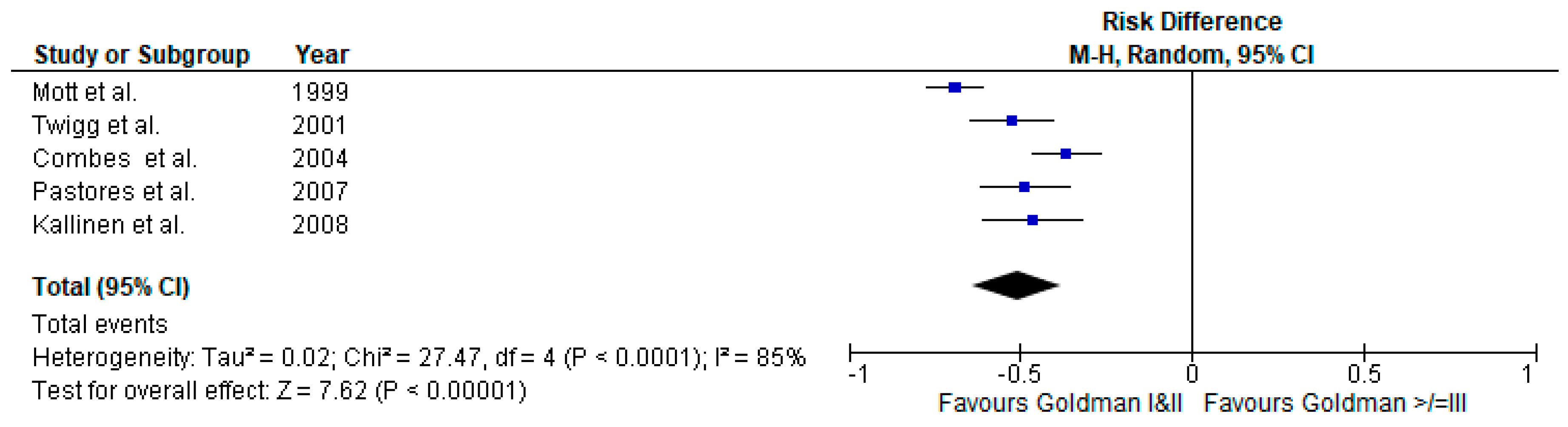

Table 1.
Goldman's system of clinicopathological discrepancies.
| major discrepancies | class l | discrepancies in primary diagnoses with relation to cause of death - detection would have led to changes in management and therapy |
| class ll | discrepancies in major diagnoses about the cause of death - detection and adjusted therapy (management changes) could have prolonged survival or cured the patient. | |
| minor discrepancies | class all | Symptoms should have been treated or would have eventually affected the prognosis. |
| class IV | Non-diagnosable (occult) diseases with possible genetic or epidemiological importance. | |
| class V | non-classifiable cases |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



