
Submitted:
11 December 2023
Posted:
12 December 2023
You are already at the latest version
Abstract
Background and Objectives: Cardiovascular events are the leading cause of morbidity and mortal-ity in hemodialysis (HD) patients. Identifying risk factors can help in the effort to reduce cardi-ovascular risk and improve life expectancy. The purpose of this study was to evaluate the ability of CHA2DS2-VASc score [risk index of stroke in atrial fibrillation (AF)] in patients with end stage kidney disease, to predict stroke, major cardiovascular events and mortality. Materials and Meth-ods: CHA2DS2-VASc and HAS-BLED (bleeding risk from use of anticoagulation in AF) scores were calculated in 237 HD patients, [99 women, median age 76 (15) years], at time they com-menced on HD. The scores’ ability to predict long term cardiovascular morbidity and mortality was estimated, both in those with and without AF. Results: CHA2DS2-VASc score was signifi-cantly increased in AF (n=69) compared to non-AF (n=168) patients, 5 (2.5) versus 4 (2), p<0.0001, respectively. Increased CHA2DS2-VASc score was associated with heart failure (p=0.007, p=0.024), stroke (p<0.0001, p<0.0001) and risk of all-cause mortality (p<0.0001, p<0.0001), in both groups, respectively. C statistics indicated that CHA2DS2-VASc score performed modest discrimination in this HD population with and without AF for heart failure, stroke, and all-cause mortality, but for cardiovascular mortality in AF group only. Conclusions: Increased CHA2DS2-VASc score at time starting on HD, can predict stroke, heart failure and all-cause mortality in HD patients in-dependent of the presence of AF. Risk of cardiovascular mortality could be predicted only on patients with AF.
Keywords:
stroke
; atrial fibrillation
; hemodialysis
; CHA2DS2-VASc score
1. Introduction
The need to determine cardiovascular composite end points in clinical studies led to the term major adverse cardiovascular events (MACE). In mid-90’s, its use was initially restricted to describe a composite of clinical events in-hospital complications following percutaneous coronary interventions. During the following years, the definition of MACE was widely applied in cardiovascular research, however with great heterogeneity, which finally revealed the practical difficulties in using a broadly comprehensive end point to describe cardiovascular complications, and forced researchers to substitute it with separate end points [1]. According to World Health Organization, cardiovascular diseases include: coronary heart disease, cerebrovascular disease, peripheral arterial disease, rheumatic heart disease, congenital heart disease, deep vein thrombosis and pulmonary embolism [2]. Stroke is the second leading cause of death and one of the principal causes of disability worldwide. Although ischemic stroke is more common, hemorrhagic stroke accounts for more deaths and disability-adjusted life-years lost [3]. Atrial fibrillation (AF) is the most common clinically recognized cardiac arrhythmia, and consists a major cause of morbidity and mortality. Its incidence in people aged 60-65 is less than 1%, but that raises to 8-10% among those over 80. Being the responsible cause for 15% of stroke events, it is considered to fivefold increase the risk of stroke [4].
CHA2DS2-VASc score has been designed and broadly applied as a useful a tool that calculates the risk of stroke in patients with AF. Patients receive 1 or 2 points for each criterion, which are: congestive heart failure, arterial hypertension, age (over 75 years or 65-74 years), diabetes mellitus, previous stroke/transient ischemic attack/thromboembolism, vascular disease and gender. Patients are classified as low, intermediate or high risk to predict the annual risk of stroke (0.2-12.2%). In the high-risk patients, use of oral anticoagulant treatment is recommended, while in intermediate risk patients, it should be considered as a possible treatment [5]. Supplement table S1 describes the parameters that consist and determine CHA2DS2-VASc score.
Furthermore, HAS-BLED score has been described to predict bleeding risk from the use of anticoagulation in patients with AF. The HAS-BLED score includes the presence of systolic blood pressure over 160 mmHg, impaired renal function, with serum creatinine above 2.26 mg/dl or need for dialysis, liver disease (cirrhosis, serum bilirubin levels 2 times above normal, serum transaminases levels 3 times above normal), history of stroke, previous bleeding/predisposition to bleeding, age over 65 years, irregular International Normalized Ratio (INR), medication that predisposes to bleeding and alcohol use. It is classified into low, intermediate and high risk for bleeding, as described on Supplement Table S2. Its use is aimed at trying to reduce the risk of bleeding with appropriate measures [6].
The aim of this study was to evaluate the ability of CHA2DS2-VASc score in patients with end stage kidney disease (ESKD) measured at time started on hemodialysis (HD), to predict not only stroke, but also, major cardiovascular events and mortality. In fact, the study not only tried to repurpose this risk score, and expand its use as predictive indices of cardiovascular events, in patients on HD, but this was applied not only in patients with AF, but also in those without AF.
2. Materials and Methods
2.1. Study Population
Patient Inclusion and Exclusion Criteria
Patients included in the study should be adults, above 18 years old, with ESKD, on HD for at least 12 months prior to participation, in order to have a follow up of at least one year and to avoid cases of acute renal failure temporally requiring HD [7,8,9].
Exclusion criteria were: change of dialysis method (peritoneal dialysis or transplantation) during the last 12 months, incompliance with medical and diet instructions and HD rules, patients who could not achieve adequate dialysis or lost to follow up.
2.2. Study methodology and data extraction
The present retrospective study included patients commencing on HD during the period 2/2010 until 1/2021, and staying on a regular HD method for at least 12 months. CHA2DS2-VASc and HAS-BLED scores were calculated at time of commencing on HD. In addition, in the same time of initiating HD, demographic, clinical and laboratory data, comorbidities and information regarding medication and HD prescription were collected from patients’ records.
Major cardiovascular events and deaths were recorded during their follow up treatment on HD. Laboratory indices, such as serum total cholesterol, high- and low-density lipoprotein cholesterol (HDL-C, LDL-C), triglycerides and high sensitivity troponin T (TnT-hs) were also recorded at the end of follow up.
2.3. Statistical Analysis
The statistical processing and analysis of the data, frequencies and results was done with the statistical package for social sciences (SPSS) 26 for Windows. The level of statistical significance (p) was set below 0.05. The qualitative variables were described using absolute (n) and relative frequency (%). Kolmogorov Smirnov and Shapiro tests were used to estimate normality of variables. In the description of the quantitative variables, the normally distributed parameters were expressed as numerical average value (mean) ± standard deviation (SD), while the non-normally distributed parameters were expressed as median (interquartile range, IQR). Means were compared with Pearson’s chi square test (x2), while medians with Mann-Whitney test. The calculation of discrimination of CHA2DS2-VASc score, made by using C statistics for each outcome. Receiver Operating Characteristics (ROC) curves were applied to estimate the incidence of CHA2DS2-VASc score in cardiovascular diseases (CVD), cardiovascular morbidity and mortality.
3. Results
3.1. Description of patient data
Three hundred eighty-three Caucasian patients were initially evaluated, 146 of them were eliminated either because of the presence of exclusion criteria or because of non-compliance during follow up, resulting in a final number of 237 patients. The median age of the patients was 76 (15) years, most of them 197/237 (83.1%) being elderly, ≥ 65 years old. The mean value of body mass index was 24.99±5.12 kg/m2. Approximately half of the patients (n=132/237, 55.7%) were alive at the data collection cut-off date. The median value of total serum cholesterol, LDL-C and triglycerides were within normal levels. most of the patients however, being on treatment with statins, ezetimibe or omega 3 fatty acids. The patients’ demographics are condensed in Table 1.
3.2. Cardiovascular events during follow up
About the same proportion of patients (almost one third of them) had acute myocardial infarction and peripheral arterial disease. In the majority of them, diagnosis of the cardiovascular event was made before the initiation of HD. Approximately 1 in 4 patients (n=63, 26.6%) had a stroke, with the majority of these having an ischemic stroke, while 35 patients developed some complication or neurologic residual. AF was present in 29.1% of patients, and nearly 1 in 10 developed this arrhythmia after starting dialysis, in the first three months. Almost 6% of patients developed venous thromboembolic disease, in most of them occurring before start of HD and in the form of deep vein thrombosis. The cardiovascular events characteristics are summarized in Table 2.
3.3. Correlation with morbidity and mortality
All patients with AF had an abnormal CHA2DS2-VASc and HAS-BLED score, as seen in Table 3. CHA2DS2-VASc score was 5 (2.5) versus 4 (2), p<0.0001, in AF and non-AF, respectively. No significant difference between AF and non-AF patients, was demonstrated regarding the HAS-BLED score.
In addition, in Table 4, the causes of death as reported in the Service for Coordination and Control of the End Stage Chronic Kidney Failure Program are listed. One third of the 105 patients who died had an underlying cardiovascular cause of death. Higher mortality was depicted in AF group, 40/69, 58%, in comparison to non-AF group, 65/168, 38.7%, chi-square=7.36, p=0.006.
Table 5 depicts the association of CHA2DS2-VASc score with cardiovascular events and mortality in the two groups of patients (with and without AF, n=69 and n=168 patients, respectively). In our study population, increased CHA2DS2-VASc score was associated with heart failure (p=0.007, p=0.024) and stroke (p<0.0001, p<0.0001), respectively. This score may forecast the risk of all-cause mortality in both groups, p<0.0001, p<0.0001, respectively.
C statistics indicate that the CHA2DS2-VASc score performed modestly in this HD population with and without AF for events that occurred after the initiation of HD; for acute myocardial infarction 0.681 (95% confidence interval [CI], 0.335-1) p=0.227, and 0.442 (95% CI, 0.314-0.571) p=0.523, for heart failure, 0.79 (95% CI, 0.613-0.967) p=0.008 and 0.825 (95% CI, 0.722-0.929) p=0.026, for peripheral arterial disease 0.65 (95% CI, 0.499-0.801) p=0.071 and 0.524 (95% CI, 0.39-0.658) p=0.76, for stroke, 0.864 (95% CI, 0.77-0.958) p<0.0001 and 0.811 (95% CI, 0.726-0.896) p<0.001, for cardiovascular mortality 0.713 (95% CI, 0.581-0.845) p=0.012 and 0.629 (95% CI, 0.514-0.745) p=0.067 and all-cause mortality 0.771 (95% CI, 0.654-0.887) p<0.0001 and 0.682 (95% CI, 0.602-0.763) p<0.0001, respectively. Figure 1, shows only the above relations which are statistically significant.
Subsequently, the stroke and AF studied were correlated with various parameters, either demographic, clinical or laboratory or with HD characteristics. A marginally statistically significant relationship was observed between stroke and patients with high HAS-BLED score (p=0.049). AF was correlated with death (p=0.007). Increased CHA2DS2-VASc score was correlated with stroke (p<0.001), cardiovascular mortality (p=0.047) and central venous catheter (p=0.047).
4. Discussion
CHA2DS2-VASc score is a very useful tool, initially described and widely applied for the calculation of ischemic stroke risk in patients with AF and also, to recognize and distinguish patients who can take oral anticoagulation [5]. The score has not been widely used in patients on HD, and in validation showed only poor performance, possibly attributed to chronic inflammation and vascular calcification, commonly seen in HD patients [10]. In the present study we assessed CHA2DS2-VASc score in patients with ESKD undergoing HD, and estimated its efficacy to predict major cardiovascular events and cardiovascular and all-cause mortality. CHA2DS2-VASc score was calculated in the whole cohort of HD patients, while its predictive ability was separately estimated for patients with AF and without AF.
CHA2DS2-VASc score was associated with all-cause mortality in both groups, AF and non-AF, but with cardiovascular mortality only on patients with AF. Previous studies have shown that this score is used for the estimation of cardiovascular and all-cause mortality in patients with chronic kidney disease (CKD) with and without AF [11,12,13]. Moreover, it was used as a predictor of three year all-cause and cardiovascular mortality in patients on HD [14]. Furthermore, CHA2DS2-VASc score above 3.5 and the presence of central venous catheter at the commencement of HD may predict one-year mortality in this population [15].
In our study, CHA2DS2-VASc score may predict the risk of stroke and heart failure. It was found that each one point increase in this score was related with increased risk for myocardial infarction and stroke within the first year, in patients on HD [16]. In the same population, this score was associated with stroke in patients without AF. Furthermore, CHA2DS2-VASc score above or equal to four, related with a highest risk for cardiovascular outcomes, namely stroke, myocardial infarction and peripheral ischemia [17]. However, it was found that previous ischemic strokes are non-inferior for prognosticating future ones, than the whole CHA2DS2-VASc score in patients on HD. This score is less predictive in those patients without history of cerebrovascular accident or transient ischemic attack [18].
In the present study, one third of the deceased patients had an underlying cardiovascular cause of death, following by infectious diseases and cancer, with a higher mortality in AF group. A Japanese study, in patients on HD, found similar results, with sudden death, pulmonary infection and lung cancer being the most ordinary cause of death in each category [19]. A Chinese study had almost similar results, with major causes of death being cardiovascular disease, sudden death, infection, and cerebrovascular disease [20]. AF at the commencement of HD related with increased mortality risk of ESKD patients in all age groups [21]. AF was a risk factor for outcomes on HD population, such as death from any cause, hospitalization, and hemorrhagic stroke [22].
Stroke was associated with decreased survival, AF and approximately half had some neurological residual after the event. In a meta-analysis, an inverse linear relationship was found between glomerular filtration rate and stroke. The risk of this occurrence increases by 7% for every 10 ml/min/1.73 m2 reduction in glomerular filtration rate [23]. CKD patients on HD have an increased risk of ischemic stroke compared to the general population, with AF being the main risk factor. There is also increased mortality after stroke in this population [24]. While in patients with CKD stage 2 the risk of occurrence and incidence of AF is 6%, on HD it may exceed 25%. In patients with CKD undergoing HD, the relative risk of stroke is three times higher in the presence of AF compared to its absence [4]. A Scottish study concluded that the leading risk factors of stroke were old age, AF, history of stroke, diabetes mellitus, elevated serum phosphorus levels, low body weight and increased systolic blood pressure [25]. Another study showed that diabetic nephropathy was a statistically significant risk factor [26]. Stroke was correlated with a reduction in functional capacity and an increment in mortality. Also, the presence of AF and abnormal CHA2DS2-VASc score [27] were common. Moreover, it has been observed that in patients with AF, a high CHA2DS2-VASc score has been associated with an increased risk of development of CKD and ESKD [28]. Most patients had high HAS-BLED score, regardless of AF. However, this score showed poor predictive abilities in this population [29] and had poor discriminatory performance in patients with ESKD on HD [30].
Our results are based on a retrospective analysis of patients dialyzed in a single center, which however covers an extended area. However, we believe that the large number of patients, with adequate follow up and the strict inclusion and exclusion criteria may overwhelm this limitation and highlight the importance of newer applications of CHA2DS2-VASc score.
5. Conclusions
In the present study, stroke coexisted with AF in HD patients, highlighting its potential causality. The majority of patients had increased CHA2DS2-VASc and HAS-BLED score, making it necessary not only to receive appropriate treatment, but also to try to reduce the high bleeding risk.
CHA2DS2-VASc score may predict the risk of stroke, heart failure and all-cause mortality in HD patients with and without AF. However, the risk of cardiovascular mortality may be predicted only in patients with AF.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: CHA2DS2-VASc score, Table S2: HAS-BLED score.
Author Contributions
Conceptualization, M.S. and T.T.; methodology, M.S., T.T. and E.G; software, T.T., F.S. and Z.S; validation, G.L., E.M., M.C. and S.S.; formal analysis, G.L.; investigation, F.S. and Z.S; resources, E.G.; data curation, E.M., M.C. and S.S.; writing—original draft preparation, T.T.; writing—review and editing, M.S.; visualization, M.S. and T.T; supervision, M.S.; project administration, M.S.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board. All research activities were performed with coded-anonymous tissue samples and data. Informed consent was obtained from all patients.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hermans:, W.R.; Foley, D.P.; Rensing, B.J.; Rutsch, W.; Heyndrickx, G.R.; Danchin, N.; Mast, G.; Hanet, C.; Lablanche, J.M.; Rafflenbeul, W. Usefulness of Quantitative and Qualitative Angiographic Lesion Morphology, and Clinical Characteristics in Predicting Major Adverse Cardiac Events during and after Native Coronary Balloon Angioplasty. CARPORT and MERCATOR Study Groups. Am J Cardiol 1993, 72, 14–20. [Google Scholar] [CrossRef]
- Cardiovascular Diseases (CVDs). Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 4 September 2022).
- Katan, M.; Luft, A. Global Burden of Stroke. Semin Neurol 2018, 38, 208–211. [Google Scholar] [CrossRef]
- Leung, K.C.-W.; MacRae, J.M. Anticoagulation in CKD and ESRD. J Nephrol 2019, 32, 719–731. [Google Scholar] [CrossRef]
- Joundi, R.A.; Cipriano, L.E.; Sposato, L.A.; Saposnik, G. Stroke Outcomes Research Working Group Ischemic Stroke Risk in Patients With Atrial Fibrillation and CHA2DS2-VASc Score of 1: Systematic Review and Meta-Analysis. Stroke 2016, 47, 1364–1367. [Google Scholar] [CrossRef]
- Peterson, D.; Geison, E. Pharmacist Interventions to Reduce Modifiable Bleeding Risk Factors Using HAS-BLED in Patients Taking Warfarin. Fed Pract 2017, 34, S16–S20. [Google Scholar] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group KDIGO 2020 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int 2020, 98, S1–S115. [CrossRef] [PubMed]
- Levey, A.S.; Becker, C.; Inker, L.A. Glomerular Filtration Rate and Albuminuria for Detection and Staging of Acute and Chronic Kidney Disease in Adults: A Systematic Review. JAMA 2015, 313, 837–846. [Google Scholar] [CrossRef]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef] [PubMed]
- Molnar, A.O.; Sood, M.M. Predicting in a Predicament: Stroke and Hemorrhage Risk Prediction in Dialysis Patients with Atrial Fibrillation. Semin Dial 2018, 31, 37–47. [Google Scholar] [CrossRef]
- Goudis, C.; Daios, S.; Korantzopoulos, P.; Liu, T. Does CHA2DS2-VASc Score Predict Mortality in Chronic Kidney Disease? Intern Emerg Med 2021, 16, 1737–1742. [Google Scholar] [CrossRef]
- Vodošek Hojs, N.; Ekart, R.; Bevc, S.; Piko, N.; Hojs, R. CHA2DS2-VASc Score as a Predictor of Cardiovascular and All-Cause Mortality in Chronic Kidney Disease Patients. Am J Nephrol 2021, 52, 404–411. [Google Scholar] [CrossRef]
- Hsu, P.-C.; Lee, W.-H.; Chen, S.-C.; Tsai, Y.-C.; Chen, Y.-C.; Chu, C.-Y.; Lin, T.-H.; Voon, W.-C.; Lai, W.-T.; Sheu, S.-H.; et al. Using CHADS2 and CHA2DS2-VASc Scores for Mortality Prediction in Patients with Chronic Kidney Disease. Sci Rep 2020, 10, 18942. [Google Scholar] [CrossRef] [PubMed]
- Okubo, A.; Doi, T.; Morii, K.; Nishizawa, Y.; Yamashita, K.; Shigemoto, K.; Mizuiri, S.; Usui, K.; Arita, M.; Naito, T.; et al. Utility of CHA2DS2-VASc Score to Predict Mid-Term Clinical Outcomes in Hemodialysis Patients. Am J Nephrol 2022, 53, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Abrantes, A.M.; Marques da Silva, B.; Branco, C.; Costa, C.; Peres, N.; Cardoso, A.; Sant’Ana, M.; Fonseca, J.A.; Outerelo, C.; Resina, C.; et al. One-Year Mortality after Hemodialysis Initiation: The Prognostic Role of the CHA2DS2-VASc Score. J Clin Med 2023, 12, 1011. [Google Scholar] [CrossRef] [PubMed]
- Schamroth Pravda, M.; Cohen Hagai, K.; Topaz, G.; Schamroth Pravda, N.; Makhoul, N.; Shuvy, M.; Benchetrit, S.; Assali, A.; Pereg, D. Assessment of the CHA2DS2-VASc Score in Predicting Mortality and Adverse Cardiovascular Outcomes of Patients on Hemodialysis. Am J Nephrol 2020, 51, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Sab, M.; Chelala, D.; Aoun, M.; Azar, R.; Abdel Massih, T. Stroke in Hemodialysis Patients and Its Association with CHA2DS2-VASC and HAS-BLED Scores: A Retrospective Study. Clin Kidney J 2022, 16, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Bel-Ange, A.; Itskovich, S.Z.; Avivi, L.; Stav, K.; Efrati, S.; Beberashvili, I. Prior Ischemic Strokes Are Non-Inferior for Predicting Future Ischemic Strokes than CHA2DS2-VASc Score in Hemodialysis Patients with Non-Valvular Atrial Fibrillation. BMC Nephrol 2021, 22, 179. [Google Scholar] [CrossRef]
- Hiyamuta, H.; Yamada, S.; Taniguchi, M.; Nakano, T.; Tsuruya, K.; Kitazono, T. Causes of Death in Patients Undergoing Maintenance Hemodialysis in Japan: 10-Year Outcomes of the Q-Cohort Study. Clin Exp Nephrol 2021, 25, 1121–1130. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhang, H.; Diao, Z.; Guo, W.; Huang, H.; Zuo, L.; Liu, W. Epidemiological Analysis of Death among Patients on Maintenance Hemodialysis: Results from the Beijing Blood Purification Quality Control and Improvement Center. BMC Nephrol 2023, 24, 236. [Google Scholar] [CrossRef]
- Hsieh, H.; Hsu, S.; Cheng, H.; Chen, C.; Huang, W.; Sue, Y.; Lin, F.; Shih, C.; Chen, J.; Lin, S.; et al. The Influence of Atrial Fibrillation on the Mortality of Incident ESRD Patients Undergoing Maintenance Hemodialysis. PLoS One 2020, 15, e0228405. [Google Scholar] [CrossRef]
- Kang, Y.; Choi, H.Y.; Kwon, Y.E.; Shin, J.H.; Won, E.M.; Yang, K.H.; Oh, H.J.; Ryu, D.-R. Clinical Outcomes among Hemodialysis Patients with Atrial Fibrillation: A Korean Nationwide Population-Based Study. Kidney Res Clin Pract 2021, 40, 99–108. [Google Scholar] [CrossRef]
- Masson, P.; Webster, A.C.; Hong, M.; Turner, R.; Lindley, R.I.; Craig, J.C. Chronic Kidney Disease and the Risk of Stroke: A Systematic Review and Meta-Analysis. Nephrol Dial Transplant 2015, 30, 1162–1169. [Google Scholar] [CrossRef]
- Boonpheng, B.; Thongprayoon, C.; Cheungpasitporn, W. The Comparison of Risk of Stroke in Patients with Peritoneal Dialysis and Hemodialysis: A Systematic Review and Meta-Analysis. J Evid Based Med 2018, 11, 158–168. [Google Scholar] [CrossRef]
- Findlay, M.; MacIsaac, R.; MacLeod, M.J.; Metcalfe, W.; Sood, M.M.; Traynor, J.P.; Dawson, J.; Mark, P.B. The Association of Atrial Fibrillation and Ischemic Stroke in Patients on Hemodialysis: A Competing Risk Analysis. Can J Kidney Health Dis 2019, 6, 2054358119878719. [Google Scholar] [CrossRef]
- Shinya, Y.; Miyawaki, S.; Kumagai, I.; Sugiyama, T.; Takenobu, A.; Saito, N.; Teraoka, A. Risk Factors and Outcomes of Cerebral Stroke in End-Stage Renal Disease Patients Receiving Hemodialysis. J Stroke Cerebrovasc Dis 2020, 29, 104657. [Google Scholar] [CrossRef]
- Cohen-Hagai, K.; Nacasch, N.; Rozenberg, I.; Korzets, Z.; Einbinder, Y.; Zitman-Gal, T.; Benchetrit, S. Clinical Outcomes of Stroke in Hemodialysis Patients: A Retrospective Single-Center Study. Int Urol Nephrol 2019, 51, 1435–1441. [Google Scholar] [CrossRef]
- Wang, C.-J.; Hsieh, Y.-P.; Kor, C.-T.; Chiu, P.-F. The CHA2DS2-VASc Score Predicts Chronic Kidney Disease among Patients with Atrial Fibrillation. Int Urol Nephrol 2020, 52, 1523–1531. [Google Scholar] [CrossRef]
- Ocak, G.; Ramspek, C.; Rookmaaker, M.B.; Blankestijn, P.J.; Verhaar, M.C.; Bos, W.J.W.; Dekker, F.W.; van Diepen, M. Performance of Bleeding Risk Scores in Dialysis Patients. Nephrol Dial Transplant 2019, 34, 1223–1231. [Google Scholar] [CrossRef]
- Nopp, S.; Spielvogel, C.P.; Schmaldienst, S.; Klauser-Braun, R.; Lorenz, M.; Bauer, B.N.; Pabinger, I.; Säemann, M.; Königsbrügge, O.; Ay, C. Bleeding Risk Assessment in End-Stage Kidney Disease: Validation of Existing Risk Scores and Evaluation of a Machine Learning-Based Approach. Thromb Haemost 2022, 122. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Receiver operating characteristic (ROC) curves for CHA2DS2-VASc score for relation with cardiovascular events in patients with (a), (c), (e), (g) and without (b), (d), (f) atrial fibrillation (AF).
Figure 1.
Receiver operating characteristic (ROC) curves for CHA2DS2-VASc score for relation with cardiovascular events in patients with (a), (c), (e), (g) and without (b), (d), (f) atrial fibrillation (AF).
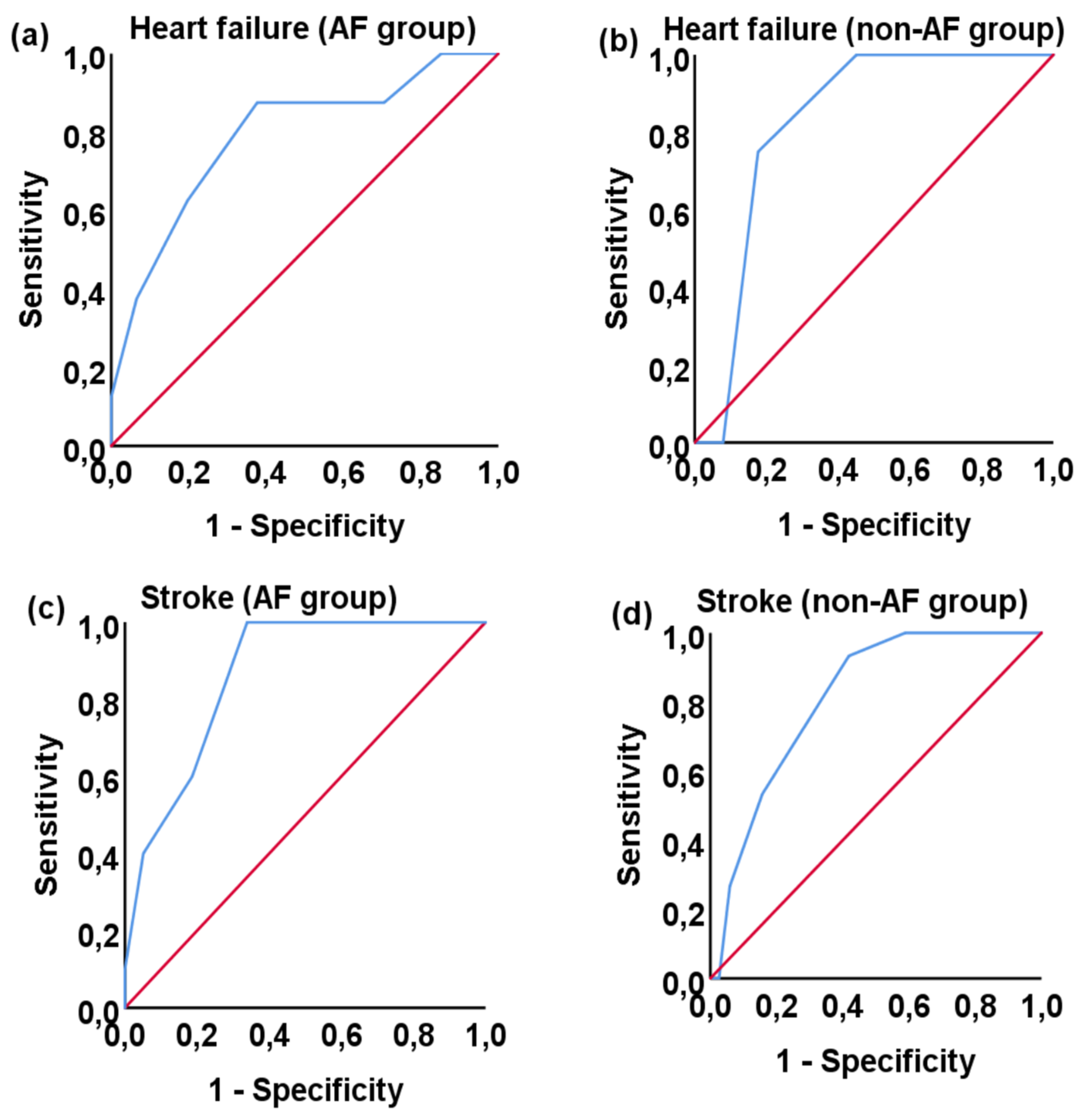
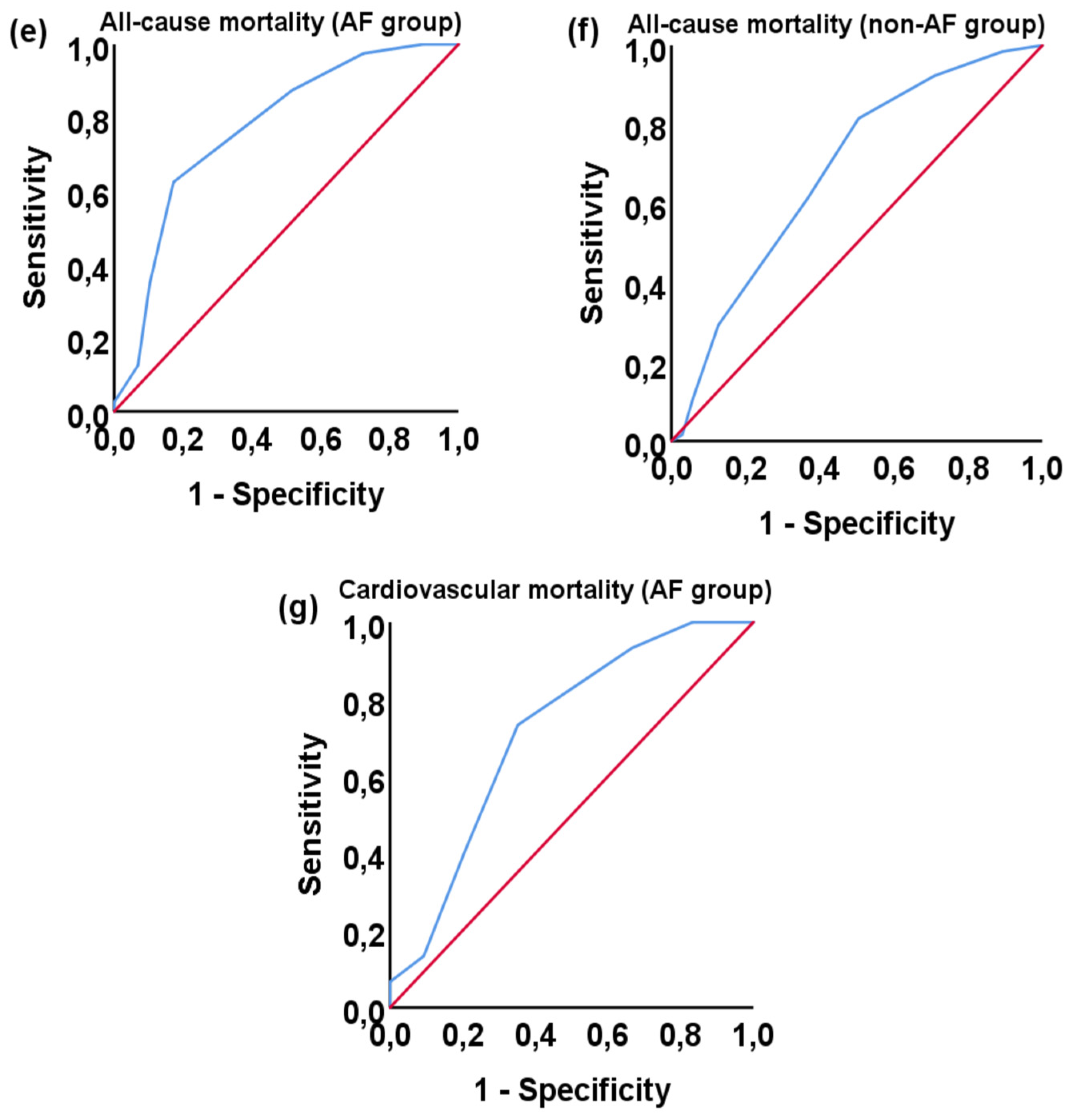

Table 1.
Patients’ demographics.
| Parameter | Total | AF group | Non-AF group | p |
|---|---|---|---|---|
| n | 237 | 69 | 168 | |
| Primary cause of end stage kidney disease | ||||
| Diabetic nephropathy (%) | 69 (29.1) | 19 (27.5) | 50 (29.8) | |
| Arterial hypertension (%) | 22 (9.3) | 9 (13) | 13 (7.7) | |
| Glomerulonephritis or vasculitis (%) | 20 (8.4) | 3 (4.3) | 17 (10.1) | |
| Polycystic kidney disease (%) | 8 (3.4) | 1 (1.4) | 7 (4.2) | |
| Obstructive cause (%) | 12 (5.1) | 2 (2.9) | 10 (6) | |
| Cardiorenal syndrome (%) | 9 (3.8) | 8 (11.6) | 1 (0.6) | |
| Cancer (%) | 4 (1.7) | 1 (1.4) | 3 (1.8) | |
| Unknown cause (%) | 93 (39.2) | 26 (37.7) | 67 (39.9) | |
| At time starting on HD | ||||
| Age (years, IQR) | 76 (15) | 79 (12) | 75 (17.75) | 0.067 |
| Gender (female/male) | 99 (41.8)/138 (58.2) | 25 (36.2)/44 (63.8) | 74 (44)/ 94 (56) | 0.268 |
| At time of evaluation | ||||
| Time since staring on HD (months, IQR) | 36 (44) | 34 (37) | 37 (46.75) | 0.032 |
| Age (years, IQR) | 73 (16) | 76 (11.5) | 72 (18.5) | 0.384 |
| BMI (kg/m2, ± SD) | 24.99 (± 5.12) | 25.31 (± 5.34) | 24.86 (± 5.04) | 0.568 |
| BMI classification (underweight/physiological/overweight/type I obesity/type II obesity/type III obesity) (%) | 41 (17.3)/90 (38)/66 (27.8)/32(13.5)/7 (3)/1 (0.4) | 13 (18.8)/22 (31.9)/20 (29)/11 (15.9)/3 (4.3)/0 (0) | 28 (16.7)/68 (40.5)/46 (27.4)/21 (12.5)/4 (2.4)/1 (0.6) | 0.76 |
| Survival (alive/dead) (%) | 132 (55.7)/105 (44.3) | 29 (42)/40 (58) | 103 (61.3)/65 (38.7) | 0.007 |
| Comorbidities | ||||
| Diabetes mellitus (%) | 121 (51.1) | 43 (62.3) | 78 (46.4) | 0.026 |
| Arterial hypertension (%) | 212 (89.5) | 63 (91.3) | 149 (88.7) | 0.552 |
| Dyslipidemia (%) | 161 (67.9) | 47 (68.1) | 114 (67.9) | 0.969 |
| Cancer (%) | 66 (27.8) | 22 (31.9) | 44 (26.2) | 0.374 |
| Chronic obstructive pulmonary disease (%) | 35 (14.8) | 11 (15.9) | 24 (14.3) | 0.744 |
| Hypothyroidism (%) | 43 (18.1) | 7 (10.1) | 36 (21.4) | 0.041 |
| Secondary hyperparathyroidism (%) | 59 (24.9) | 16 (23.2) | 43 (25.6) | 0.697 |
| Cholesterol (mg/dl, IQR) | 152 (54.5) | 147 (63.5) | 152 (49.5) | 0.122 |
| HDL-C (mg/dl, IQR) | 42 (18) | 39 (18) | 43.5 (17) | 0.113 |
| HDL-C (mg/dl) (< 40 / ≥ 40) | 105 (44,3)/132 (55,7) | 40 (58)/29 (42) | 65 (38.7)/103 (61.3) | 0.007 |
| LDL-C (mg/dl, IQR) | 80 (47) | 80 (54.1) | 80.1 (43.75) | 0.346 |
| Triglycerides (mg/dl, IQR) | 140 (85.5) | 142 (91.5) | 139.5 (80) | 0.569 |
| TnT-hs (ng/l, IQR) | 63 (64.85) | 79.9 (63.25) | 59.05 (62.03) | 0.004 |
Atrial fibrillation (AF); standard deviation (SD); interquartile range (IQR); hemodialysis (HD); body mass index (BMI); high density lipoprotein cholesterol (HDL-C); low density lipoprotein cholesterol (LDL-C); troponin T high sensitivity (TnT-hs).
Table 2.
Characteristics of cardiovascular events on patients.
| Cardiovascular event | Total | AF group | Non-AF group | p |
|---|---|---|---|---|
| Acute myocardial infarction | 82 | 35 | 47 | 0.001 |
| Occurrence of acute myocardial infarction after start of dialysis | 15 | 4 | 11 | 0.829 |
| Heart failure | 50 | 30 | 20 | <0.001 |
| Occurrence of heart failure after start of dialysis | 12 | 8 | 4 | 0.003 |
| Peripheral arterial disease | 80 | 32 | 48 | 0.008 |
| Occurrence of peripheral arterial disease after start of dialysis | 31 | 16 | 15 | 0.003 |
| Stroke (ischemic/hemorrhagic) | 60/3 | 22/3 | 38/0 | 0.031 |
| Complication or neurological residual from stroke | 35 | 15 | 20 | 0.053 |
| Occurrence of stroke after start of dialysis | 25 | 10 | 15 | 0.207 |
| Venous thromboembolic disease | 14 | 4 | 10 | 0.963 |
| Pacemaker or defibrillator | 13 | 8 | 5 | 0.008 |
| Prosthetic valve | 4 | 3 | 1 | 0.042 |
Atrial fibrillation (AF).
Table 3.
CHA2DS2-VASc and HAS-BLED score of population study.
| Parameter | All | AF (+) | AF (-) | p |
|---|---|---|---|---|
| CHA2DS2-VASc score | 5 (3) | 5 (2.5) | 4 (2) | <0.0001 |
| classification of CHA2DS2-VASc score (low/intermediate/high) | 2/11/224 | 0/1/68 | 2/10/156 | 0.209 |
| HAS-BLED score | 4 (1) | 4 (1) | 4 (1) | 0.204 |
| classification of HAS-BLED score (low/intermediate/high) | 0/16/221 | 0/2/67 | 0/14/154 | 0.13 |
Atrial fibrillation (AF)
Table 4.
Causes of death of study patients.
| Parameter | Total | AF group | Non-AF group |
|---|---|---|---|
| cancer | 19 | 4 | 15 |
| infection | 4 | 1 | 3 |
| septicemia | 18 | 6 | 12 |
| surgical | 5 | 3 | 2 |
| cachexia | 1 | 0 | 1 |
| dementia | 1 | 1 | 0 |
| chronic obstructive pulmonary disease | 1 | 1 | 0 |
| other | 11 | 5 | 6 |
| unknown | 11 | 4 | 7 |
| cardiovascular (cardiac arrest/AMI/ stroke/HF/APE/ruptured aneurysm/PE) |
(13/6/11/1/1/1/1) | (6/2/6/1/0/0/0) | (7/4/5/0/1/1/1) |
Atrial fibrillation (AF); acute myocardial infarction (AMI); heart failure (HF); acute pulmonary edema (APE); pulmonary embolism (PE).
Table 5.
Association of CHA2DS2-VASc score with cardiovascular events and mortality in patients with and without atrial fibrillation after start of hemodialysis. *
Table 5.
Association of CHA2DS2-VASc score with cardiovascular events and mortality in patients with and without atrial fibrillation after start of hemodialysis. *
| AF group | Non-AF group | |||||
|---|---|---|---|---|---|---|
| Event | Yes | No | p | Yes | No | p |
| Acute myocardial infarction | 7 (4-7.75) | 5 (4-6) | 0.218 | 4 (3-5) | 4 (3-5) | 0.516 |
| Heart failure | 7 (6-8) | 5 (4-6) | 0.007 | 6 (5.25-6) | 4 (3-5) | 0.024 |
| Peripheral arterial disease | 6 (5-7) | 5 (4-6) | 0.066 | 4 (3-5) | 4 (3-5) | 0.756 |
| Stroke | 7 (6-8) | 5 (4-6) | <0.0001 | 6 (5-7) | 4 (3-5) | <0.0001 |
| Cardiovascular mortality | 6 (5-7) | 6 (5-7) | 0.33 | 5 (4-5) | 5 (4-6) | 0.988 |
| All-cause mortality | 6 (5-7) | 5 (3-5) | <0.0001 | 5 (4-6) | 4 (2-5) | <0.0001 |
Atrial fibrillation (AF). *The numbers are the median value of CHA2DS2-VASc score. The numbers in parentheses indicate the lower and upper interquartile range.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



