Submitted:
06 December 2023
Posted:
13 December 2023
You are already at the latest version
Abstract
Delivery of drugs through the nasal route provides an alternative, yet highly efficacious modality for administering both large and small pharmaceutic molecules. This method proves particularly advantageous for drugs that are unstable during oral administration, as they undergo significant degradation in the gastrointestinal tract or metabolization through the first-pass effect in the liver. Nasal administration stands as a viable alternative to parenteral therapy and is also suitable for long-term medical management. The nasal mucosa, characterized by high vascularity and permeability, facilitates rapid pharmaceutical absorption, ensuring a swift onset of therapeutic action. Despite its noninvasive nature, the nasal delivery technique finds broad applicability for both local treatment and systemic therapy, as the drug directly enters systemic circulation. This article explores the feasibility of a novel spray delivery mechanism for intranasal drug deposition. The study aims to determine whether users can correctly follow the state-of-the-art application instructions for a nasal spray with an optimal nozzle placement angle (namely, 12-15°) at the nostril while maintaining sufficient safety and efficacy, and without engaging in preventable usage errors that could harm the user. Additionally, the study evaluates the effectiveness of device labeling, instructions for use, and a short video in supporting the correct application of the nasal spray at the optimal angle (12-15°) and assesses whether users can differentiate the product from others with similar appearances. We have also performed physical spray tests to experimentally evaluate drug penetration to the nasopharynx (a key target site for viral infections) for two different nozzle placements – one for current package instructions coming with over-the-counter spray products and the other for the optimal spray usage procedure to enhance targeted drug delivery. Human Factors (HF) validation studies were also conducted, instructing users to follow the application instructions of the nasal spray bottle with the nozzle placed at the optimal angle to target the nasopharynx. The experimental tests consistently confirmed improved penetration with the 12-15° nozzle placement, with visual cues proving effective when used in tandem with written instructions for guiding the study participants to adhere to the recommended usage procedures.
Keywords:
intranasal spray
; drug delivery
; respiratory transport modeling
; respiratory diseases
; upper airway physiology
; targeted nasal therapy
; gentlemistTM technology
1. Introduction
The concept of nasal drug delivery has evolved significantly since its initial use for local drug applications. In the early 1980s, the nasal route emerged as a promising systemic delivery alternative, challenging the dominance of conventional drug delivery methods [1,2]. Its appeal lies in the nasal cavity’s unique features, comprising an easily accessible, highly vascularized, and permeable mucosa that facilitates rapid absorption of compounds into the systemic circulation. This bypasses hepatic first-pass elimination, a substantial advantage over oral drug administration. Intranasal drug delivery allows for dose reduction, rapid attainment of therapeutic levels in the blood, quicker onset of pharmacological activity, and fewer side effects [3,4]. The low metabolic environment of the nose has the potential to overcome the limitations of the oral route and replicate the benefits of intravenous administration. Additionally, nasal administration minimizes the lag time associated with oral drug delivery and offers noninvasiveness, self-administration, patient comfort, and patient compliance, thus overcoming the hurdles in intravenous drug therapy [5]. Lipophilic drugs exhibit especially favorable absorption profiles through the nasal route with pharmacokinetic profiles that are often identical to those obtained after intravenous injection with a bioavailability approaching 100% [1]; on the other hand, absorption of hydrophilic drugs can be increased utilizing absorption enhancers [2]. Drugs ranging from small chemicals to large macromolecules, including peptide/protein therapeutics, hormones, and vaccines, are being delivered through the nasal cavity [6]. Intranasal delivery poses a favorable way to circumvent the obstacles to the blood-brain barrier, enabling direct drug delivery to the central nervous system [7,8]. It has also been considered for the administration of vaccines [9,10,11]. Peptides such as buserelin, desmopressin, calcitonin, insulin, luteinizing hormone-releasing hormone, growth hormone, and adrenocorticotrophic hormone have been successfully administered through the nasal route [12,13]. In addition, steroids (corticosteroids, estradiol, progesterone, testosterone, etc.) [14,15], antihypertensives (nifedipine, nitroglycerine, propranolol, hydralazine, etc.), analgesics (buprenorphine), antibiotics and antivirals [16] have been shown to produce considerable systemic effects when administered via the nasal cavity. Various systems for nasal drug delivery, such as nasal spray, nasal pumps, gels, microemulsions, suspensions, powders, and thermo-reversible mucoadhesive gels, have been studied [17].
In the past decade, pharmaceutical scientists and clinicians have increasingly focused on the feasibility of drug delivery via the nasal route for viral diseases. Regions in the upper respiratory tract often serve as the initial dominant sites of airborne viral infection, replication, and transmission in the human body [18,19]. Consequently, nasally inhaled drugs and vaccines may offer a promising alternative for managing allergies and viral diseases in addition to other routes of drugs and vaccine administration.
Despite the above benefits, challenges persist in maximizing the efficacy of intranasal drug delivery, with optimal drug penetration to targeted sites within the nasal cavity being a key concern. This study addresses this gap by exploring the feasibility of a novel nasal spray delivery mechanism, specifically designed to enhance intranasal therapeutic penetration for treating respiratory illnesses. The research is structured into two distinct parts. Part I involves physical spray tests performed in a 3D-printed anatomically accurate nasal cast designed to assess drug penetration using different nozzle orientations. Part II comprises Human Factors (HF) Validation Studies to evaluate the ease of use and effectiveness of the nasal spray device and its optimal usage instructions in a real-world setting. This comprehensive approach aims to determine the practicality and efficiency of the nasal spray device when used at an optimal angle (12-15°) and assess the effectiveness of accompanying instructional materials in guiding correct usage. By focusing on these aspects, the study endeavors to contribute significantly to the field of nasal drug delivery, with potential implications for enhanced drug administration and patient outcomes in treating respiratory illnesses.
2. Materials and Methods
2.1. Experimental Setup for Physical Spray Tests
The experimental setup shown in Figure 1 is a representation of the nasal drug delivery process with a pharma-quality nasal pump sprayer manufactured by Dr. Ferrer Biopharma trademarked and patented as GentleMistTM Technology (DFB; located in Hallandale Beach, FL). The physical spray tests were designed to assess drug penetration for two different protocols characterized by the following orientations of the nozzle: (a) when the nozzle was placed at an approximately 15° angle to the horizontal and inserted at a shallow depth of 5 mm inside the airspace (see Figure 1a); this specific orientation aligned with our recent in silico findings [20,21,22,23,24] on improved usage protocols to enhance targeted delivery of drugs at key infection and inflammation sites along the airspace, e.g., the nasopharynx (for viral infections) and the ostiomeatal complex (for complications such as chronic rhinosinusitis), and (b) when the nozzle was placed at approximately 67.5° to the horizontal and inserted at a shallow depth of 5 mm inside the airspace (see Figure 1b); this latter orientation is a schematic replication of the usage instructions that come with over-the-counter nasal spray products [21].
For the experiments, we utilized a 3D-printed airway cavity cast that accurately replicates the anterior nasal passage of the human anatomy. This cast was created by reconstructing computed tomography (CT) imaging data obtained from a 41-year-old Caucasian male, with a CT-slice resolution of 0.352 mm; see Figure 2a. The soft plastic part was produced using a Connex3TM 3D printer through the polymer ink-jetting process on Tangogray FLX950 material. This choice of material helps to closely mimic the flexibility of external nares, internal tissues, and associated cartilages. The printed cavity's extent concluded just anterior to the nasopharynx, allowing for the measurement of the outflow volume (emerging from the back of the cast) of the administered spray solution, which would have (in a complete nasal anatomy) swept through the nasopharyngeal surfaces, e.g., see Figure 2b.
An adjustable angle hinge connector of a diameter of ¾’’ was used to precisely fix the nasal sprayer for the test angles. Additionally, to collect the output solution reaching the nasopharyngeal walls and to tightly hold the 3D model, we employed a standard burette holder with clamps. In the experimental tests, the administered formulation was a saline solution of density 1.3 g/ml. For experimental accuracy, we maintained a constant net output of 5 ml (i.e., the volume of solution penetrating through the anatomical cast), and we recorded the number of pumps required to achieve the specified volume output for both protocols. Subsequently, we determined the mean penetration for each orientation by dividing the net collected output discharge by the number of pumps. Note that occasional discharge through the front of the nose was collected in a separate cup, ensuring that the anterior discharge does not contaminate the measurement of the penetrating solution.
Figure 2.
(a) A perspective view of the computed tomography-based in silico reconstruction used to prepare the 3D-printed anatomic cast for the physical spray tests. (b) The 3D-printed anatomic nasal cast is virtually placed against an atypical upper airway model. The Dr. Ferrer Biopharma graphics design team has prepared the underlying airway cartoon shown in panel (b).
Figure 2.
(a) A perspective view of the computed tomography-based in silico reconstruction used to prepare the 3D-printed anatomic cast for the physical spray tests. (b) The 3D-printed anatomic nasal cast is virtually placed against an atypical upper airway model. The Dr. Ferrer Biopharma graphics design team has prepared the underlying airway cartoon shown in panel (b).
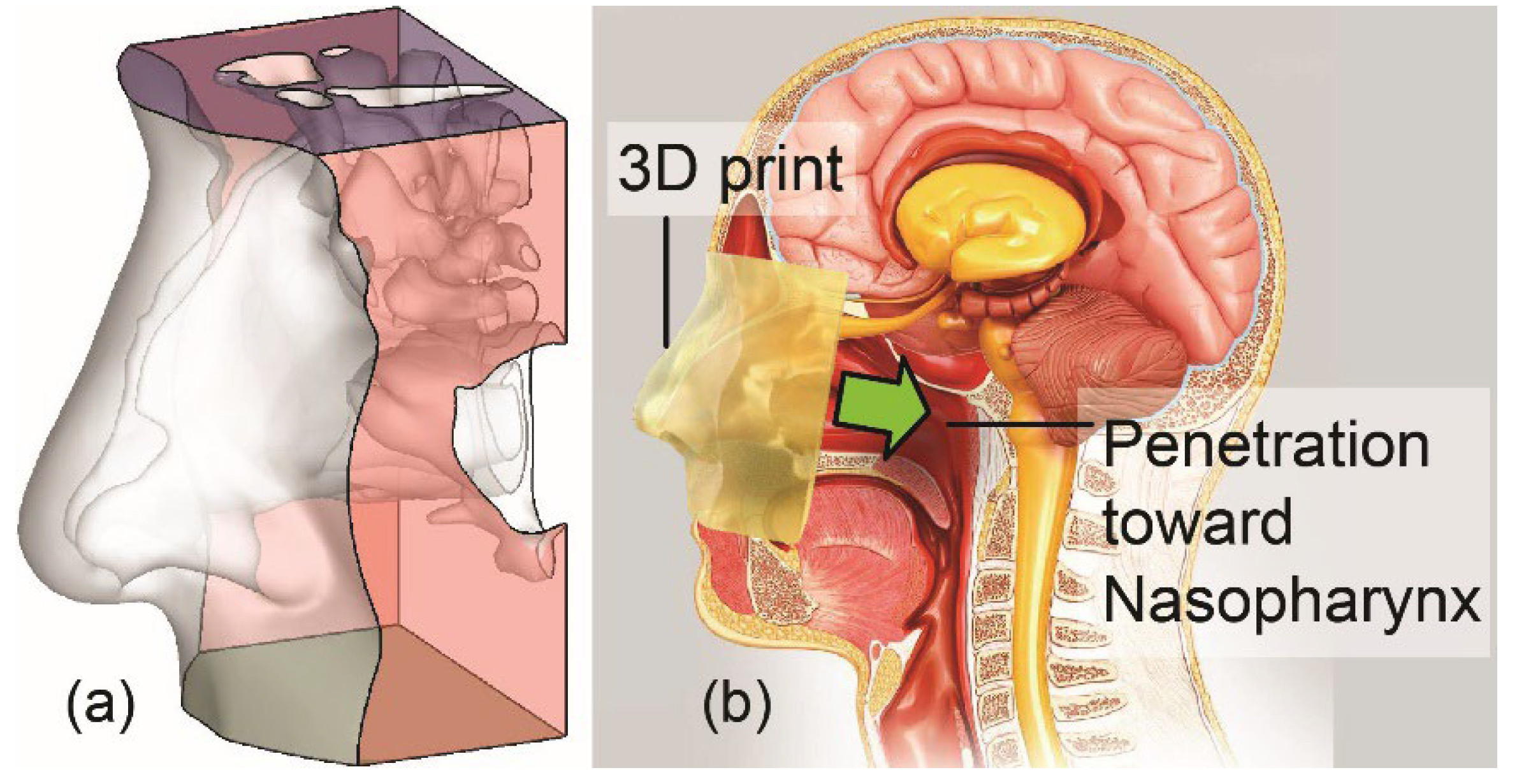
Figure 3.
Visual aid for application of nasal spray at an intended angle. The Dr. Ferrer Biopharma graphics design team prepared the airway cartoon.
Figure 3.
Visual aid for application of nasal spray at an intended angle. The Dr. Ferrer Biopharma graphics design team prepared the airway cartoon.

2.2. Human Factors Usability Study Procedure
The Human Factors (HF) usability study was conducted using a mannequin (simulated person representation) and a nasal pump sprayer (identical to the one used during the physical tests, see Section 2.1). The study environment replicated typical usage conditions, with participants given the sprayer and accompanying instructions (refer to Figure 3). Participants were directed to administer the nasal spray to the mannequin while adhering to the provided instructions. Their performance, encompassing successful applications, errors, and ease of use, was observed, and meticulously recorded.
2.4. Human Factors: Task Analysis
The HF task analysis deconstructed the application of nasal spray into four main stages: Preparation, Device Positioning, Delivery, and After Use. Each stage consisted of several specific steps crucial for the effective and accurate application of the nasal spray. Study participants were tasked with demonstrating these steps, guided by detailed instructions. To assess the efficacy of each step, we employed observational techniques, covering all recommended actions for optimal nasal spray application, as outlined in Table 1.
2.5. Knowledge Task
The HF study assessed participants' understanding of the labeling and diagrams associated with the nasal spray. Participants received the device's labeling, encompassing text instructions and visual diagrams illustrated in Figure 2. Subsequently, they were tasked with verbally articulating the steps involved in using the nasal spray and demonstrating their comprehension through a simulated application on the mannequin. Their verbal descriptions were compared to the provided instructions to gauge comprehension, while their ability to follow the visual instructions was observed and scored.
2.6. Human Factors Study Participants
The study included lay users (non-healthcare professionals) divided into the following two groups:
- • Simulation group: This group included 50 participants (38 females, average age 53.40 ± 2.58 years), with 40 having experience with a nasal spray device. In the simulation group, participants did not apply the nasal spray to themselves. Instead, they simulated the action of administering the nasal spray on a mannequin. This approach is common in studies to assess user interaction with a device without the need for actual physical usage, focusing on technique, handling, and potential errors in a controlled setting.
- • Real-use group: This group consisted of 141 participants (63 females, with an average age of 53.86 ± 18.7 years), a significant number of whom (121 participants) had prior experience using a nasal spray device. The "real-use" aspect indicates that these participants actually used the nasal spray device on themselves, in a realistic manner. This means they were applying the nasal spray as they would in a normal, everyday setting, thus providing practical insights into the usability and effectiveness of the nasal spray device under real-life conditions.
2.7. Use Environments
The study was conducted in non-clinical settings, designed to mirror the typical environments where patients would use the nasal spray.
2.8. Interventions
The intervention consisted of providing participants with the nasal spray device and the instructional materials, then instructing them on the correct use of the nasal spray, following both the written and visual guidelines.
2.9. Study Outcomes
The primary outcome was the correct self-administration of the nasal spray as per the instructions, specifically the correct application at the optimal angle of 12-15°. Secondary outcomes included the ability to distinguish the product, user-friendliness of labeling, medication error risk, and overall user confidence with the nasal spray application.
2.10. Data Analysis
Descriptive statistics were used to analyze the data from the usability study. Success rates errors, and the level of instruction comprehension were quantified, with particular attention to the correct application at the optimal angle (12- 15°). Rates were calculated to estimate the percentage of participants who completed the steps correctly, with an acceptable level of > 80%.
2.11. Use-related risk analysis
During the risk assessment phase, medication delivery was identified as a critical task. It was determined that if a patient failed to successfully self-administer the nasal spray as per instructions, it could result in excess dosing, under-dosing, or inability to deliver a dose. Additionally, proper delivery at the optimal angle (12-15° angle) is crucial for patients with viral infections to ensure maximum drug deposition at the nasopharynx, which is the target site of viral infection onset [24,25,26,27]. Improper delivery techniques could lead to inadequate drug transmission as well as nasal irritation and discomfort if the spray axis directly hits the septum wall. Another important factor in risk assessment is the ability of the patient to distinguish a product from others with similar appearances. Failure to recognize the difference could result in the delivery of incorrect medication. Furthermore, environmental conditions that may lead to use errors were also considered, such as confusion between the nasal spray and other medications stored in the same location, especially if they had a similar appearance. This could potentially lead to accidental use of the wrong medication.
3. Results
The pump sprayers used in the experiment could administer 0.01 ml of solution with each pump. By comparing the penetration data from the two spray protocols, we quantitatively assessed the improvements in nasal penetration. Table 2 and Table 3 show the values from the experiments with the sprayer placed at 15° to the horizontal plane for the right and left nostrils, respectively. Table 3 and Table 4 similarly record the data for the currently used protocol, i.e., for the nozzle placement angle of 67.5° with the horizontal, for right and left nostrils, respectively.

Table 2.
Right airway penetration data for 15° nozzle alignment with respect to horizontal: The first column lists the trial numbers, with the subsequent columns listing the number of pumps and the volume penetration to the nasopharynx per spray application. Symbols: M, sample mean; SD, standard deviation; CV, coefficient of variation (calculated as 100 × |SD|/M, in percentage).
Table 2.
Right airway penetration data for 15° nozzle alignment with respect to horizontal: The first column lists the trial numbers, with the subsequent columns listing the number of pumps and the volume penetration to the nasopharynx per spray application. Symbols: M, sample mean; SD, standard deviation; CV, coefficient of variation (calculated as 100 × |SD|/M, in percentage).
| Trial No. | Number of spray pumping action | Mean volume penetration to the nasopharynx per spray application (ml) | ||||
|---|---|---|---|---|---|---|
| 1 | 80 | 0.0625 | ||||
| 2 | 77 | 0.0649 | ||||
| 3 | 81 | 0.0617 | ||||
| 4 | 75 | 0.0666 | ||||
| 5 | 72 | 0.0694 | ||||
| M 77.0 |
SD ± 3.6742 |
CV % 4.77 |
M 0.0650 |
SD ± 0.0031 |
CV 4.76% |
|
Table 3.
Left airway penetration data for 15° nozzle alignment with respect to horizontal: The first column lists the trial numbers, with the subsequent columns listing the number of pumps and the volume penetration to the nasopharynx per spray application. Symbols: M, sample mean; SD, standard deviation; CV, coefficient of variation (calculated as 100 × |SD|/M, in percentage).
Table 3.
Left airway penetration data for 15° nozzle alignment with respect to horizontal: The first column lists the trial numbers, with the subsequent columns listing the number of pumps and the volume penetration to the nasopharynx per spray application. Symbols: M, sample mean; SD, standard deviation; CV, coefficient of variation (calculated as 100 × |SD|/M, in percentage).
| Trial No. | Number of spray pumping action | Mean volume penetration to the nasopharynx per spray application (ml) | ||||
|---|---|---|---|---|---|---|
| 1 | 83 | 0.0625 | ||||
| 2 | 96 | 0.0649 | ||||
| 3 | 94 | 0.0617 | ||||
| 4 | 85 | 0.0588 | ||||
| 5 | 86 | 0.0581 | ||||
| M 88.8 |
SD ± 5.8052 |
CV 6.54 % |
M 0.0612 |
SD ± 0.0028 |
CV 4.58 % |
|
Table 4.
Right airway penetration data for the 67.5° nozzle alignment with respect to horizontal: The first column lists the trial numbers, with the subsequent columns listing the number of pumps and the volume penetration to the nasopharynx per spray application. Symbols: M, sample mean; SD, standard deviation; CV, coefficient of variation (calculated as 100 × |SD|/M, in percentage).
Table 4.
Right airway penetration data for the 67.5° nozzle alignment with respect to horizontal: The first column lists the trial numbers, with the subsequent columns listing the number of pumps and the volume penetration to the nasopharynx per spray application. Symbols: M, sample mean; SD, standard deviation; CV, coefficient of variation (calculated as 100 × |SD|/M, in percentage).
| Trial No. | Number of spray pumping action | Mean volume penetration to the nasopharynx per spray application (ml) | ||||
|---|---|---|---|---|---|---|
| 1 | 160 | 0.0312 | ||||
| 2 | 157 | 0.0318 | ||||
| 3 | 175 | 0.0285 | ||||
| 4 | 174 | 0.0287 | ||||
| 5 | 169 | 0.0295 | ||||
| M 167.0 |
SD ± 8.1548 |
CV 4.88 % |
M 0.0299 |
SD 0.0015 |
CV 5.02 % |
|
Table 5.
Left airway penetration data for 67.5° nozzle alignment with respect to horizontal: The first column lists the trial numbers, with the subsequent columns listing the number of pumps and the volume penetration to the nasopharynx per spray application. Symbols: M, sample mean; SD, standard deviation; CV, coefficient of variation (calculated as 100 × |SD|/M, in percentage).
Table 5.
Left airway penetration data for 67.5° nozzle alignment with respect to horizontal: The first column lists the trial numbers, with the subsequent columns listing the number of pumps and the volume penetration to the nasopharynx per spray application. Symbols: M, sample mean; SD, standard deviation; CV, coefficient of variation (calculated as 100 × |SD|/M, in percentage).
| Trial No. | Number of spray pumping action | Mean volume penetration to the nasopharynx per spray application (ml) | ||||
|---|---|---|---|---|---|---|
| 1 | 95 | 0.0526 | ||||
| 2 | 96 | 0.0520 | ||||
| 3 | 110 | 0.0454 | ||||
| 4 | 98 | 0.0510 | ||||
| 5 | 99 | 0.0505 | ||||
| M 99.6 |
SD 6.0249 |
CV 6.05 % |
M 0.0503 |
SD 0.0029 |
CV 5.77 % |
|
For the right nostril (see Table 2 and Table 4) in the 3D-printed anatomic cast used in the physical spray experiments, the average volumes penetrating to the nasopharynx per spray application were 0.0650 ml and 0.0299 ml, with the sprayer at approximate angles of 15°and 67.5° to the horizontal, respectively. Similarly, the corresponding average values for the left nostril were 0.0612 ml and 0.0503 ml. Therefore, the percentage increase (say, ∈1) in nasopharyngeal targeting for the right nostril is:
Furthermore, from the data reported in Table 3 and Table 5, the percentage increase (say, ∈2) in nasopharyngeal targeting for the left nostril is therefore:
In the second part of this study, the application of the presented steps was analyzed (see Table 6). Overall, the test participants (i.e., the users) followed the instruction without significant difficulties in all the steps with a score of 90.44 ± 14.9 and 86.1 ± 11.0% for the simulated and real portions of the study, respectively (acceptance level was set at > 80%). The educational level of the patients was not a determining factor for not performing the task correctly.
4. Discussion
Direct intranasal delivery to the nasopharynx, which is the primary site of viral infection onset along the upper respiratory tract owing to the propensity of ciliated epithelial cells with surface receptors, appears to be a reasonable design choice for next-generation targeted pharmaceutics and prophylactics. The tortuosity of the human airway passage coupled with its general morphological complexity can, however, render targeted delivery and durable coverage difficult. As shown in this work, a better delivery dose to the intended location, in this case the nasopharyngeal wall, can be achieved from minor modifications in administration practices, e.g., by changing the spray axis angle to approximately 15° with respect to horizontal. While the resulting mean improvement in spray penetration to the nasopharynx was clearly statistically significant, as exemplified in Figure 4 (also see Table 2, Table 3, Table 4 and Table 5) on both sides of the 3D-printed nose, the improvement for the left airway was somewhat subdued. We conjecture this to be the result of a distinct septal deviation observable in the test subject’s nasal anatomy (in the 3D-printed replica). Also, it should be noted that the pump sprayers that were used each had a projected design lifetime of 1500 pumps. The reader should also note that the experimental setup had the limitation of no ambient airflow to simulate any possible breathing effects on the spatiotemporal dynamics of the pharmaceutic aerosols. The experimental process however allowed for a perturbation of approximately +1.5° (on the 15° spray axis alignment with respect to the horizontal) to realistically replicate subjective usage variabilities.
5. Conclusions
The new intranasal delivery device assessed in our study has demonstrated promising results, ensuring continuous and consistent drug delivery to the clinically relevant target region along the upper airway. In this study, the specific focus was on the nasopharynx as the trigger site for respiratory viral infections, guaranteeing maximum surface area exposure and a higher probability of therapeutic absorption. The noteworthy discovery that participants achieved self-administration of the nasal spray with over 80% accuracy, delivering the medication at the optimal angle (12-15°), reflects the functional suitability of the device and the clarity of its instructional materials. The effectiveness of the instructions is further emphasized by the majority of users comprehending the diagrams provided in the labeling.
The presented outcomes affirm the efficacy of enhanced drug delivery protocols for targeting the upper respiratory tract and underscore the potential for increased patient comfort, satisfaction, and compliance with intranasal drug administration. Recognizing the significance of device design and user education in optimizing drug delivery, our study suggests that future research should explore the personalization of nasal spray devices to accommodate anatomical diversity, thereby enhancing the precision and efficacy of drug delivery to the nasopharynx and other clinically relevant sites, such as the ostiomeatal complex for treating sinus inflammations. The implications of such advancements could be particularly significant in the management of respiratory viral illnesses, indicating a broader application for the findings of this study in current clinical practice.
Supplementary Materials
Not applicable.
Author Contributions
Conceptualization: G.F. and S.B.; methodology: M.L.T., A.M., S.A.A.R, M.M.H.A., G.F., S.B.; software: A.M., S.B.; validation: M.L.T., A.M., S.B.; formal analysis: M.L.T., S.A.A.R, S.B.; investigation: M.L.T., A.M., G.F., S.B.; resources: G.F., S.B.; data curation: M.L.T., A.M., S.B.; writing—original draft preparation: M.L.T., A.M., S.B.; writing—review and editing: M.L.T., A.M., S.A.A.R, M.M.H.A., G.F., S.B.; visualization: M.L.T., A.M., S.B.; supervision: G.F., S.B.; project administration: G.F., S.B.; funding acquisition: G.F., S.B. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon request.
Conflicts of Interest
Dr. Ferrer owns the patent for GentleMistTM Technology.
References
- Hicke, A.J. Pharmaceutical Inhalation Aerosol Technology, 2nd Ed Marcel Dekker, Inc: NewYork, 2004.
- Illum, L. Nasal drug delivery-possibilities, problems and solutions. J. Control Release 2003, 87, 187–198. [Google Scholar] [CrossRef] [PubMed]
- Ugwoke, M.I.; Verbek, N.; Kinget, R. The biopharmaceutical aspects of nasal mucoadhesion drug delivery. J. Pharm. Pharmacol. 2001, 59, 3–22. [Google Scholar]
- Arora, P. Sharma; Gary, S. Permeability issues in nasal drug delivery. Drug Discov. Today 2002, 7, 967–975. [Google Scholar] [CrossRef] [PubMed]
- Marttin, E.; Nicolaas, G.M.; Schipper, J.; Coos, V.; Frans, W.H. Nasal mucociliary clearance as a factor in nasal drug delivery. Adv. Drug Deliv. Rev. 1997, 29, 13–38. [Google Scholar] [CrossRef] [PubMed]
- Alabsi, W.; Eedara, B.B.; Encinas-Basurto, D.; Polt, R.; Mansour, H.M. Nose-to-Brain Delivery of Therapeutic Peptides as Nasal Aerosols. Pharmaceutics 2022, 14, 1870. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.R.; Liu, M.; Khan, M.W.; Zhai, G. Progress in brain targeting drug delivery system by nasal route. J. Control. Release 2017, 268, 364–389. [Google Scholar] [CrossRef] [PubMed]
- Formica, M.L.; Real, D.A.; Picchio, M.L.; Catlin, E.; Donnelly, R.F.; Paredes, A.J. On a highway to the brain: A review on nose-to-brain drug delivery using nanoparticles. Appl. Mater. Today 2022, 29, 101631. [Google Scholar] [CrossRef]
- Illum, L. Nasal drug delivery: new developments and strategies. Drug Discov. Today 2002, 7, 1184–1189. [Google Scholar] [CrossRef] [PubMed]
- Graff, L.C.; Pollock, G.M. Nasal drug administration: potential for targeted central nervous system delivery. J. Pharm. Sci. 2005, 94, 1187–1195. [Google Scholar] [CrossRef]
- Malakar, A.; Borojeni, A.; Basu, S. Parametric numerical analysis of targeted drug delivery for intranasal sprays inside the upper respiratory airspace. Bull. Am. Phys. Soc. 2023. [Google Scholar]
- Bruno, B.J.; Miller, G.D.; Lim, C.S. Basics and recent advances in peptide and protein drug delivery. Ther. Deliv. 2013, 4, 1443–1467. [Google Scholar] [CrossRef]
- Pontiroli, A.E.; Pozza, G. Intranasal administration of peptide hormones: Factors affecting transmucosal absorption. Diabet. Med. 1990, 7, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Lipworth, B.J.; Jackson, C.M. Safety of inhaled and intranasal corticosteroids: lessons for the new millennium. Drug Saf. 2000, 23, 11–33. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, J.W. Steroid hormone enhancement of gene delivery to a human airway epithelial cell line in vitro and mouse airways in vivo. Gene Ther. 2001, 8, 1562–1571. [Google Scholar] [CrossRef] [PubMed]
- Krishnamoorthy, R.; Mitra, N.K. Prodrugs for nasal drug delivery. Adv. Drug Deliv. Rev. 1998, 29, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Duquesnoy, C.; Mamet, J.P.; Sumner, D.; Fuseau, E. Comparative clinical pharmacokinetics of single doses of sumatriptan following subcutaneous, oral, rectal and intranasal administration. Eur. J. Pharm. Sci. 1998, 6, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Mittal, R.; Ni, R.; Seo, J.H. The flow physics of COVID-19. J. Fluid Mech. 2020, 894, F2. [Google Scholar] [CrossRef]
- Williams, G.; Suman, J.D. In vitro anatomical models for nasal drug delivery. Pharmaceutics 2022, 14, 1353. [Google Scholar] [CrossRef] [PubMed]
- Akash, M.M.; Mituniewicz, A.; Lao, Y.; Balivada, P.; Ato, P.; Ka, N.; Silfen, Z.; Chakravarty, A.; Joseph-McCarthy, D.; Basu, S. A better way to spray?-a model-based optimization of nasal spray use protocols. APS Division of Fluid Dynamics Meeting Abstracts. 2021; pp. Q14-007).
- Basu, S.; Holbrook, L.T.; Kudlaty, K.; Fasanmade, O.; Wu, J.; Burke, A.; Langworthy, B.W.; Mamdani, M.; Farzal, Z.; Bennett, W.D.; et al. Numerical evaluation of spray position for improved nasal drug delivery. Sci. Rep. 2020, 10, 10568. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Khawaja, U.A.; Rizvi, S.A.A.; Sanchez-Gonzalez, M.A.; Ferrer, G. Evaluation of Patient Experience for a Computationally-Guided Intranasal Spray Protocol to Augment Therapeutic Penetration: Implications for Effective Treatments for COVID-19, Rhinitis, and Sinusitis. Med. Res. Arch. 2022, 10. [Google Scholar] [CrossRef]
- Treat, S.; Ebert Jr, C.S.; Farzal, Z.; Basu, S.; Kimbell, J.S.; Senior, B.A.; Shockley, W.W.; Madison Clark, J. Intranasal corticosteroids: patient administration angles and impact of education. Rhinology Online. 2020;3:160.
- Akash, M.M.; Lao, Y.; Balivada, P.A.; Ato, P.; Ka, N.K.; Mituniewicz, A.; Silfen, Z.; Suman, J.D.; Chakravarty, A.; Joseph-McCarthy, D.; et al. On a model-based approach to improve intranasal spray targeting for respiratory viral infections. Frontiers in Drug Delivery, Sec. Respir. Drug Deliv. 2023, 3, 1164671. [Google Scholar]
- Basu, S. Computational characterization of inhaled droplet transport to the nasopharynx. Sci. Rep. 2021, 11, 6652. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.J.; Okuda, K.; Edwards, C.E.; Martinez, D.R.; Asakura, T.; Dinnon, K.H.; Kato, T.; Lee, R.E.; Yount, B.L.; Mascenik, T.M.; et al. SARS-CoV-2 reverse genetics reveals a variable infection gradient in the respiratory tract. Cell 2020, 182, 429–446. [Google Scholar] [CrossRef] [PubMed]
- Matheson, N.J.; Lehner, P.J. How does SARS-CoV-2 cause COVID-19? Science 2020, 369, 510–1. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(a) Experimental setup for controlled spray administration into an anatomic 3D-printed nose cast at approximately 15° to the horizontal. (b) Experimental setup for controlled spray administration into the 3D-printed nose cast at approximately 67.5° to the horizontal. The latter replicates the currently prescribed spray usage parameters available as package instructions with over-the-counter spray products.
Figure 1.
(a) Experimental setup for controlled spray administration into an anatomic 3D-printed nose cast at approximately 15° to the horizontal. (b) Experimental setup for controlled spray administration into the 3D-printed nose cast at approximately 67.5° to the horizontal. The latter replicates the currently prescribed spray usage parameters available as package instructions with over-the-counter spray products.
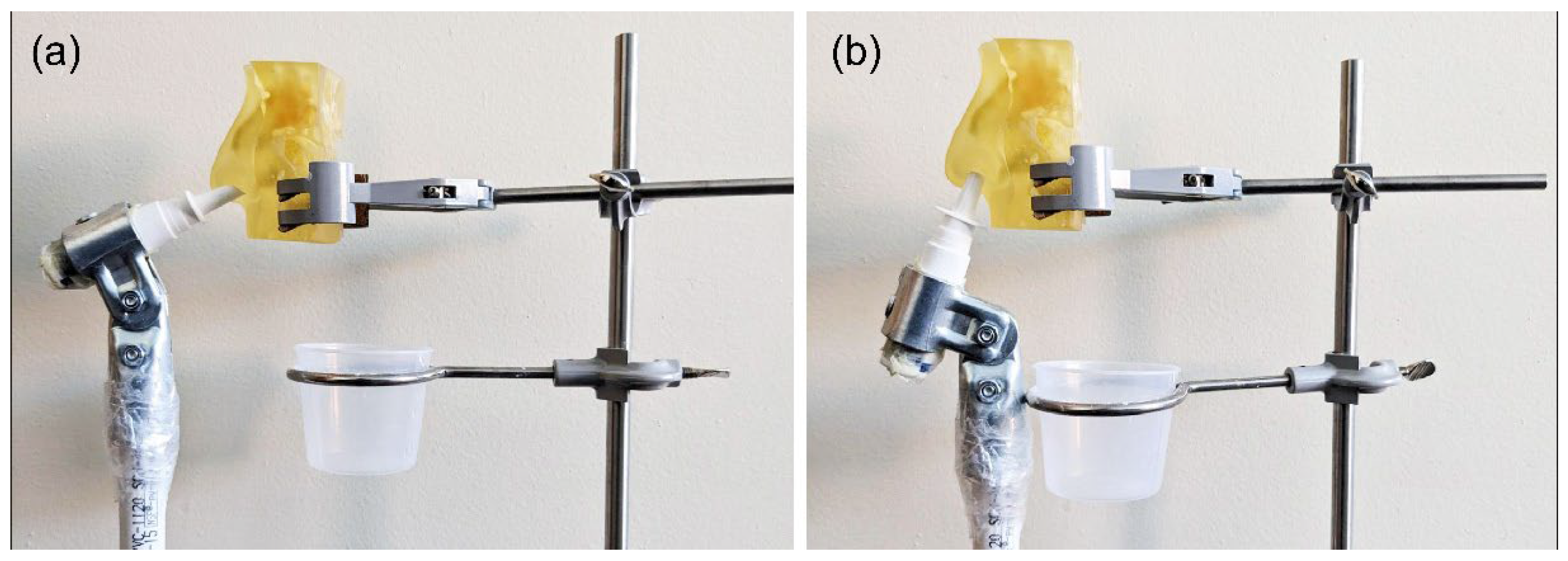
Figure 4.
Combining the data from Table 2 and Table 3, bar A demonstrates the range of spray penetration data (with the error bars representing standard deviations from the mean), in terms of the globally averaged output solution volume reaching the nasopharynx in each pumping action of the spray, corresponding to the 15° protocol. On similar lines, combining the data from Table 3 and Table 4, bar B demonstrates the range of averaged spray penetration data for the nasopharynx with the 67.5° spray placement protocol.
Figure 4.
Combining the data from Table 2 and Table 3, bar A demonstrates the range of spray penetration data (with the error bars representing standard deviations from the mean), in terms of the globally averaged output solution volume reaching the nasopharynx in each pumping action of the spray, corresponding to the 15° protocol. On similar lines, combining the data from Table 3 and Table 4, bar B demonstrates the range of averaged spray penetration data for the nasopharynx with the 67.5° spray placement protocol.
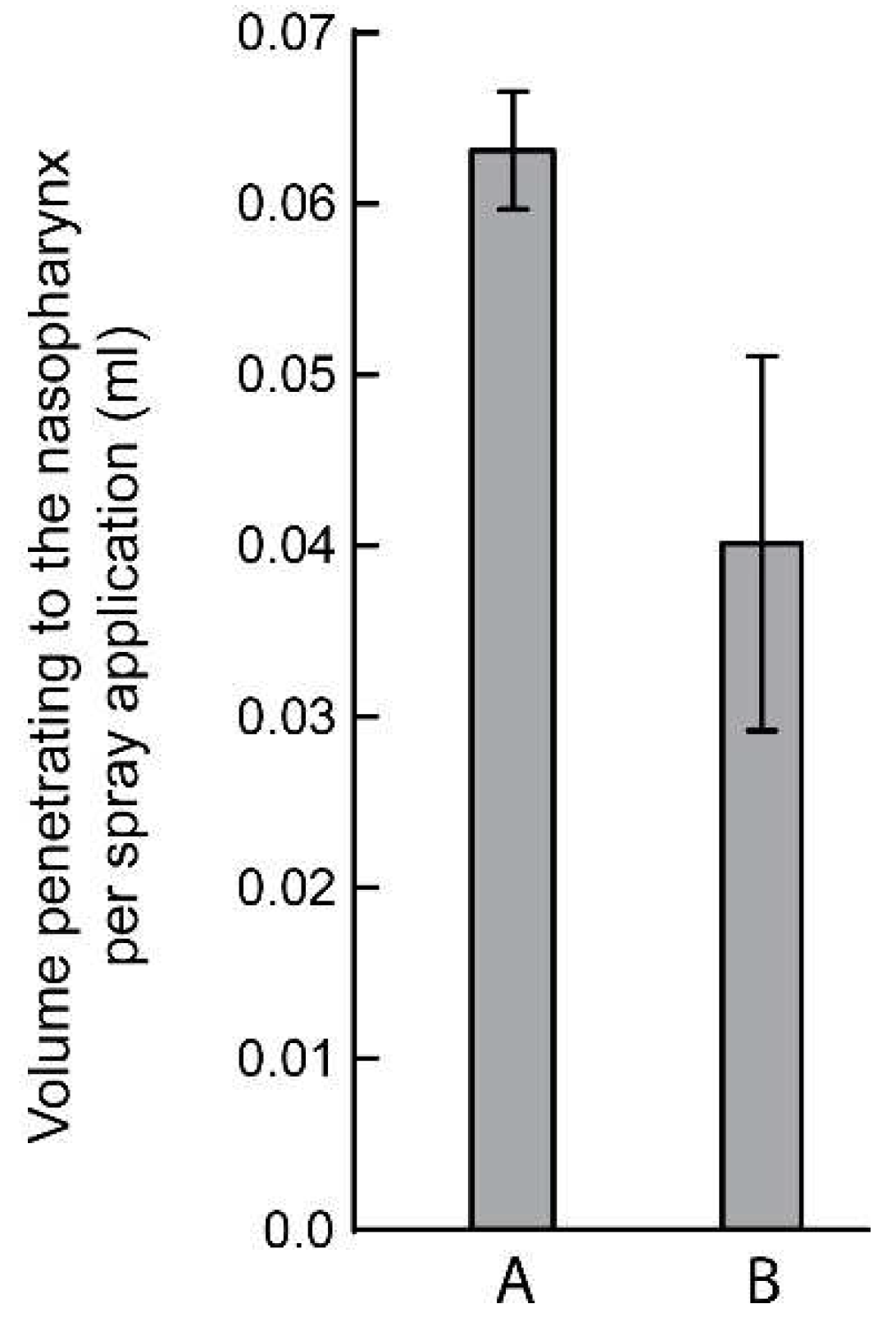
Table 1.
Steps for optimal nasal spray.
| Stages | Step | Instruction |
|---|---|---|
| Preparation | Step 1 | Shake spray bottle for 2-5 seconds. |
| Step 2 | Remove by twisting the plastic cap from the bottle. | |
| Step 3: Hand Position | Hold the bottle upright with 2 fingers on the shoulders of the spray pump and thumb on the bottom of the bottle. | |
| Step 4: Priming | Spray two times into the air away from the face. | |
| Device Positioning | Step 5: Head Position | Do not tilt your head back or front. |
| Step 6: Closing Nostril | Place the nasal spray at 12-15° angle to the head, as illustrated in the picture. | |
| Delivery | Step 7 | Spray two (2) sprays on each nostril. |
| After Use | Step 8 | Wipe the nozzle with a tissue and replace the cap. |
| Step 9 | Store the bottle in an upright position. |
Table 6.
Human factors task results: simulation and real patients’ study.
| Step | Instruction Carried Out N=50 Simulation (%) |
Instruction Carried Out N=141 Real (%) |
Principal Root Causes of Failure if missed |
|---|---|---|---|
| 1 | 88.0 | 83.6 | > 90% of missing did not read the instructions. |
| 2 | 98.0 | 80.9 | > 80% of missing was associated with not reading the instructions or left-handed patients twisting in the wrong direction. |
| 3 | 98.0 | 92.2 | |
| 4 | 82.2 | 62.4 | The patient felt confident because of prior experience did not prime the spray. |
| 5 (essential) | 100 | 95.7 | |
| 6 (essential) | 81.0 | 85.1 | |
| 7 (essential) | 82.0 | 97.2 | |
| 8 | 88.0 | 81.0 | |
| 9 | 100.0 | 96.5 | |
| Mean ± SD | 90.8 ± 8.2% | 86.1 ± 11.1% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions, or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



