
Submitted:
12 December 2023
Posted:
14 December 2023
You are already at the latest version
Abstract
Implantation of two electrical stimulators of different cranial nerves in one patient is rare. We report the case of a forty-seven-year-old patient already implanted with a trigeminus nerve stimulator. In addition, this patient suffered from hearing problems. In one ear, the patient was deaf. On the other side, the patient wore a bone conduction hearing aid to improve hearing. In this complex situation, we decided to check the possibility of cochlear implantation on the deaf side. Finally, we managed to provide electrical stimulation of the auditory pathway of the deaf ear to improve the patient’s hearing tests. In addition, this case report shows how the trigeminus stimulator interferes with the electrical stimulation in auditory evoked potentials measurements of the auditory brainstem and cortex via EABR (evoked auditory brainstem response) resp. EALR (evoked auditory late response).
Keywords:
cochlear implant
; EABR
; EALR
; trigeminal nerve stimulator
1. Introduction
Today, cochlear implantation in deaf patients is regularly a straightforward procedure [1]. In the herein presented case rare circumstances made it difficult to find a good solution using electrical stimulation of the auditory pathway. Besides the bone conduction hearing aid contralateral to the deaf ear, our patient was implanted with an electrical stimulator that aims to stimulate the trigeminal nerve to minimize the patient’s pain. Due to possible electrical interferences between the trigeminal nerve stimulator and the cochlear implant that was planned to be implanted several checks needed to be done pre-operatively. Our patient was therefore not only suffering from pain but also from deafness on one side and hearing loss on the other ear. In this case report, we describe how cochlear implantation was made possible, how the patient performed clinical measurements, and what special issues were recognized.
2. Case Presentation
A forty-seven-year-old patient presented himself to our clinic asking for rehabilitation of hearing. In childhood, the patient reported a temporal bone fracture on both sides. He underwent cholesteatoma surgery in both ears. In 1997, on the right side, he received a trigeminal nerve stimulator system (stimulator + electrode) because of diagnosed trigeminal neuropathy for pain control after a skull base fracture. Since the first implantation of the trigeminal nerve stimulator system, the stimulator unit has been exchanged multiple times due to battery exhaustion. Related to his hearing situation, the patient reported deafness for about 40 years in the right ear, and on the left side, the patient reported a (combined) hearing loss for around 40 years. On the left side, he used a hearing aid until BAHA implantation. This hearing aid was still in use in 2001 when he received the BAHA. On the right ear, he never used a hearing aid. Furthermore, in February 2012, the patient was diagnosed with borreliosis and meningitis.
Diagnostics confirmed deafness of the right ear and profound hearing impairment of the left ear. This finding resulted in a WHO grade 4 of hearing impairment [2,3].
At that time, the patient had the trigeminal nerve stimulator system “ACTIVA SC/PC” of the manufacturer Medtronic implanted.
Our first hearing tests (see Figure 1) on the left ear stated an unaided 500 to 4k pure tone audiogram of 88.0 dB HL air conduction and 57.0 dB SPL bone conduction. Using the BAHA system resulted in an aided pure tone audiogram of 50.0 dB HL for 500 Hz to 4 kHz and the aided monosyllabic word understanding of 85% at 65dB SPL in the Freiburg speech test. We did not find hearing via air or bone conduction and also did not find speech understanding in the right ear.
Considering cochlear implantation of the right ear, we needed to check possible electrical interactions between two electrically stimulating devices, interference, or cross-stimulation. I.e., the question was whether the existing electrical stimulation system for the trigeminal nerve would be compatible with an additional electrical stimulation pulse of a cochlear implant system (usually monopolar stimulation for most modern CI devices) for the auditory nerve. Due to the release specifications for the existing Medtronic trigeminal nerve stimulator system, only bipolar pulses had been allowed. Thus, the only compatible CI system that fulfilled the requirements according to Medtronic specifications of compatibility to be implanted legally and that was available to us with the safety considerations to the brain electrode was the CI500 series from Cochlear Ltd. The CI500 series was able to fulfill the compatibility requirements of Medtronic. One major request from Medtronic was that the cochlear implant system had to only stimulate inside the cochlea. Thus, only bipolar stimulation was allowed. However, in today’s cochlear implants, monopolar stimulation against common ground or bipolar stimulation mode has become the standard. The earlier stimulation modes, the old-fashioned stimulation modes, are no longer standard due to a lower chance of auditory nerve response recording, potentially lower speech understanding, and higher power consumption [4,5,6,7,8]. Modern cochlear implant systems either do not offer such a stimulation mode or do not use it by default. Cochlear Ltd offers such a stimulation called bipolar stimulation [9]. The bipolar stimulation mode is abbreviated as BP. Therefore, we were able to offer cochlear implantation to the patient.
In 2018, the patient’s deaf right ear was implanted with a cochlear implant offering bipolar stimuli (electrode Cochlear Profile Slim Straight (CI522) offering 22 intra-cochlear electrodes for stimulation of the auditory nerve and two reference electrodes) to enable hearing (see Figure 2).
Standard surgery through classical access (mastoidectomy, Facial Recess Approach, cochleostomy) was uneventful despite the skull base fracture. Intra-operatively, standard tests were performed: Impedance test, auditory nerve response test, and electrically evoked stapedius reflex test. First, the impedance test measurement allows the measurement of the impedances of all 22 intra-cochlear electrodes. The auditory nerve response test checks for compound action potentials (ECAP) while electrical stimulation by the cochlear implant. These early responses of the auditory pathway are equivalent to electrocochleography, where acoustic stimulation evokes the compound action potential. The electrically evoked stapedius reflex test (ESR), in contrast to the other two intra-operative standard measurements in cochlear implants, can check the auditory pathway up to the brainstem. On the other side, stapedius reflex measurement is a semi-objective test, unlike impedance and ECAP. Objective stapedius reflex detection is currently not part of the clinical routine but is evaluated in studies [11]. Stimulation is provided by the cochlear implant using a 0.5-second-long burst stimulus. The stapedius reflex path is a chain of the auditory nerve, the cochlear nucleus, the superior olivary complex, and the nucleus of the facial nerve [12: Auditory System, Central].
For this patient, we were able to perform impedance and ECAP measurements. ESR test was not possible. According to the anatomical findings, the surgeon couldn’t visualize the stapedius reflex, as the stapes and its tendon were missing. Also, the surgeon could not expose the stapedius muscle in this patient. Impedances and ECAP were in the normal range.
Post-operatively, we recorded an x-ray to control the position of the cochlear implant (see Figure 3). The radiologic department proved no disconnections, correct positioning of the cochlear implant, and an insertion depth of the intra-cochlear stimulation electrode of around 360°. At a later stage, we estimated the cochlear parameters from the preoperative CT scan using the OTOPLAN software (of diameter = 10.1mm, height = 4.8mm, width = 7.5mm, and cochlear duct length = 39.6mm using OTOPLAN 3 (see Figure 4; according to [13]).
For safety considerations, we proceeded with the initial activation of the cochlear implant system comparable to ABI first fitting procedures (intermediated care unit, monitoring, anesthesia team on standby) for being aware of a theoretical possible interference of the two neuro-stimulators running simultaneously. In addition, we invited external specialists from the manufacturer to attend since there are no reports of experience of a combination of these two devices. Thus, we performed the first activation and fitting of the cochlear implant system. According to the recommendation of the trigeminus nerve stimulator manufacturer, only the bipolar stimulation mode was selected for the cochlear implant fitting using only intra-cochlear electrodes on the intra-cochlear electrode array. After testing different electrode configurations and distances for this stimulation mode, we found confident results for BP+3 (BP+3 means that the reference electrode is always three electrodes away next to the stimulation electrode). Using BP+3, we could provide a small dynamic range (= DR) for electrical stimulation without interference between the two neuro-stimulators. DR is the difference between the threshold and loud but not uncomfortable stimulation limits (compare [14]). The DR was around 15CL (= manufacturer-specific current level). It can be converted to microampere using the following equation given by Cochlear [15].
I [μA] = 17.5 * 100 ^ (I[CL] / 255),
Based on the cochlear implant manufacturer’s standard values for lower and upper stimulation levels, the reference DR is around 45CL. Such a small DR is uncommon and results mostly in lower performance in speech understanding. Besides these optimizations of fitting values, we selected a pulse width of 150µs and a stimulation frequency of 250Hz.
One month after the initial activation of the cochlear implant system, an electrically evoked auditory brainstem response (= EABR) was successfully recorded using clinical software and hardware. We chose this method as it is known to also be reliable in difficult-to-record responses like patients with malformations. For EABR stimulation, we selected electrode number 11 in the middle segment of the active electrode array using bipolar stimulation mode (BP+3) at a subjectively loud sensation. Due to continuously appearing strong artifacts and spontaneously appearing strong artifacts, we used 8000 instead of the usually recorded 1000 averages. In contrast to pre-operative EABR recordings, no myogenic artifacts hardened the recording of waveforms [16]. Like in pre-operative EABR recordings, we observed a much stronger stimulus artifact than in other patients. Apart from this setting, we used the default EABR setting from [16] for intra-operative EABR. Therefore, we applied surface recording electrodes to the contralateral mastoid (inverting), high forehead (noninverting), and lower forehead (ground). In both evoked potential devices, we set the recording window to 10 ms and the bandpass filter to 50–3000 Hz. We set the amplifier range to 500 mV, and the rejection threshold to ±150µV, and we strictly monitored the patient’s movements. Figure 5 documents the recorded brainstem responses. Both essential responses, eIII and eV, were securely reproduced. Latencies of wave eV are higher than in typical EABR. In this patient, we observed a value of around 5.15ms while the reference value is 3.98 +- 0.24 ms [17]. Prolonged latencies of eV are known in cases of deprivation [18,19] or in autism [20].
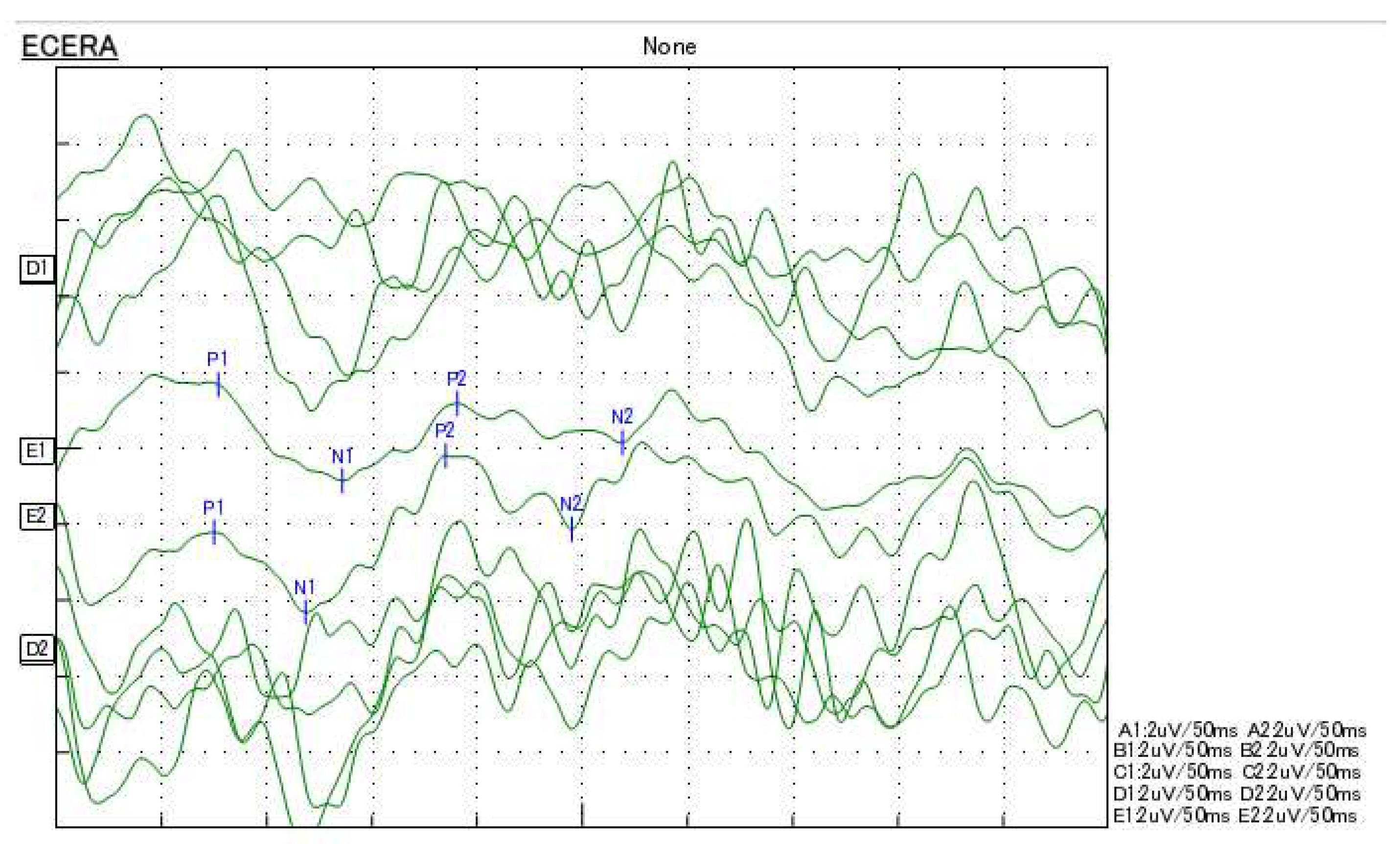
In addition, electrically evoked auditory late response (= EALR) was recorded to evaluate the cortical auditory area. This measurement is important as only that way we could test the whole auditory pathway up to the auditory cortex [21]. We selected the default settings for post-operative EALR [22]. We used a band-pass filter from 0.5 Hz to 100 Hz, collecting 50. We applied rejection for sweeps with an amplitude higher than +/- 100 μV. Other settings were identical to those for the EABR. In contrast to pre-operative EALR, we didn’t have to handle high CI stimulation or myogenic artifacts [23]. In this patient, continuous and spontaneous stimulation noise led to challenging recording circumstances, as seen in the EABR. Therefore, we averaged four recordings with default settings. Figure 6 documents the recorded cortical responses. All essential responses, P1, N1, P2, and N2 were securely reproduced.
During the follow-up appointments over the next three months, it was possible to enlarge the DR to around 20cl after switching to a pulse width of 200µs. But only two months later, DR had to be set to around 10cl.
Half a year after activation of the CI system, audiometric tests showed/confirmed a hearing threshold of 69.3dB HL (pure-tone audiogram; mean of frequencies 500 Hz to 4 kHz). Additionally, we performed a loudness scaling using a broad-band noise signal. Results showed/confirmed linear loudness increase from a threshold of 60dB SPL to medium sound sensation at 80dB SPL. The patient’s speech understanding in Freiburg numbers was 0% at 65dB SPL and 20% at 80dB SPL (contralateral ear masked). In the Freiburg monosyllable test, no understanding was possible. Till today, the patient uses the CI system around 13 hours a day and is satisfied with the hearing.
3. Discussion
The extraordinary case of cochlear implantation illustrated in this case report shows how complex it could be to check CI indication. The existing trigeminal nerve stimulator system brought us many obstacles. However, we found a solution for this patient by allowing cochlear implantation. The electrophysiological measurements of the auditory pathway objectively confirmed hearing in this patient. In the audiometry results, our patient accomplished a little speech understanding. In summary, this report shows that cochlear implantation can be done and can improve hearing in patients with an existing trigeminal nerve stimulator system when considering the need to modify settings in the CI system to avoid interaction between the trigeminal nerve stimulator system and the cochlear implant system.
Author Contributions
Conceptualization, D.P.; methodology, D.P.; validation, D.P., M.N., S.S., and J.M.; formal analysis, D.P. investigation, D.P.; resources, D.P.; data curation, D.P.; writing—original draft preparation, D.P.; writing—review and editing, D.P., J.M., and M.N.; visualization, D.P and S.S..; supervision, J.M.; project administration, D.P.; funding acquisition, no funding. All authors have read and agreed to the published version of the manuscript. Contributor roles are described according to the CRediT taxonomy.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to solely retrospective analysis for this case report.
Informed Consent Statement
Patient consent was waived due to solely retrospective analysis for this case report.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hochmair, I., Nopp, P., Jolly, C., Schmidt, M., Schößer, H., Garnham, C., & Anderson, I. (2006). MED-EL cochlear implants: state of the art and a glimpse into the future. Trends in amplification, 10(4), 201-219. [CrossRef]
- WHO (1991). Report of the Informal Working Group on Prevention of Deafness and Hearing Impairment Programme Planning, Geneva, 18-21 June 1991. URL: https://apps.who.int/iris/handle/10665/58839.
- Olusanya, B. O., Davis, A. C., & Hoffman, H. J. (2019). Hearing loss grades and the International classification of functioning, disability and health. Bulletin of the World Health Organization, 97(10), 725–728. [CrossRef]
- Zwolan, T. A., Kileny, P. R., Ashbaugh, C., & Telian, S. A. (1996). Patient performance with the Cochlear Corporation “20+ 2” implant: bipolar versus monopolar activation. Otology & Neurotology, 17(5), 717-723.
- Brown, Carolyn J.; Abbas, Paul J.; Gantz, Bruce J.. Preliminary Experience With Neural Response Telemetry in the Nucleus CI24M Cochlear Implant. The American Journal of Otology 19(3):p 320-327, May 1998.
- Lai, W, 1999. an NRT Cookbook: Guidelines for making 157 ™ measurements. Version 2.04.
- Zhu, Z., Tang, Q., Zeng, F. G., Guan, T., & Ye, D. (2012). Cochlear-implant spatial selectivity with monopolar, bipolar, and tripolar stimulation. Hearing research, 283(1-2), 45-58. [CrossRef]
- Mesnildrey, Q., & Macherey, O. (2015). Simulating the dual-peak excitation pattern produced by bipolar stimulation of a cochlear implant: effects on speech intelligibility. Hearing Research, 319, 32-47. [CrossRef]
- Wesarg, T., Arndt, S., Aschendorff, A., Laszig, R., & Zirn, S. (2014). Intraoperative audiological-technical diagnostics during cochlear implant surgery. HNO, 62(10), 725-734. [CrossRef]
- Parreño M, Di Lella FA, Fernandez F, Boccio CM and Ausili SA (2020) Toward Self-Measures in Cochlear Implants: Daily and “Homemade” Impedance Assessment. Front. Digit. Health 2:582562. [CrossRef]
- Weiss, B. G., Söchting, F., Bertlich, M., Busch, M., Blum, J., Ihler, F., & Canis, M. (2018). An objective method to determine the electrically evoked stapedius reflex threshold during cochlea implantation. Otology & Neurotology, 39(1), e5-e11. [CrossRef]
- Middlebrooks, J. C. (2015). Auditory system: Central pathways. [CrossRef]
- Spiegel, J. L., Polterauer, D., Hempel, J. M., Canis, M., Spiro, J. E., & Müller, J. (2022). Variation of the cochlear anatomy and cochlea duct length: analysis with a new tablet-based software. European Archives of Oto-rhino-laryngology, 279(4), 1851-1861. [CrossRef]
- Müller J. & Schön F. (1994). Category Scaling of Loudness in Cochlear Implant Patient Evaluation. Laryngorhinootologie 1994; 73(3): 128-131. [CrossRef]
- Cochlear Limited (2006). NIC V2 SOFTWARE INTERFACE SPECIFICATION. E11318RD Issue: 1.
- Polterauer, D., Mandruzzato, G., Neuling, M., Polak, M., Müller, J., & Hempel, J. M. (2022a). Evaluation of auditory pathway excitability using a pre-operative trans-tympanic electrically evoked auditory brainstem response under local anesthesia in cochlear implant candidates. International Journal of Audiology, 1-11. [CrossRef]
- Polterauer, D. Intraoperative and postoperative measurement of brainstem responses through electrical stimulation of the auditory nerve via implantable neurostimulators eABR by PATH MEDICAL SENTIERO ADVANCED. [CrossRef]
- Leake, P. A., Hradek, G. T., Bonham, B. H. & Snyder, R. L., 2008. Topography of auditory nerve projections to the cochlear nucleus in cats after neonatal deafness and electrical stimulation by a cochlear implant. Journal of the Association for Research in Otolaryngology, 9(3), pp. 349-372. [CrossRef]
- Lammers, M. J. et al., 2015. Delayed auditory brainstem responses in prelingually deaf and late implanted cochlear implant users. Journal of the Association for Research in Otolaryngology, Jul, Band 16, pp. 669-678. [CrossRef]
- Minami, S. B. et al., 2015. Usefulness of measuring electrically evoked auditory brainstem responses in children with inner ear malformations during cochlear implantation. Acta Oto-Laryngologica, 135(10), pp. 1007-1015. [CrossRef]
- Firszt, J. B., Chambers, R. D. & Kraus, N., 2002. Neurophysiology of cochlear implant users II: comparison among speech perception, dynamic range, and physiological measures. Ear Hear, 12, Band 23, pp. 516-531.
- Baljić, I., Müller, A., Fröhlich, L., Polterauer, D. & Dziemba, O. (2021). Elektrisch evozierte Potentiale des auditorischen Systems - Teil 2. Zeitschrift für Audiologie (Audiological Acoustics) 60(2):71-75.
- Polterauer, D., Mandruzzato, G., Neuling, M., Polak, M., Müller, J., & Hempel, J. M. (2022b). LA-TT-EALR/PromCERA: Comparison of preoperatively performed electrically evoked auditory potentials at the brainstem and cortical level during local anesthesia. Current Directions in Biomedical Engineering, 8(2), 233-236. [CrossRef]
Figure 1.
Hearing tests using tone and speech audiometry of the right and left ear at the first consultation: unaided tone-audiometry (top left ear in blue and right ear in red) and aided tone and Freiburg mono-syllable speech audiometry for the left ear (bottom) using the BAHA hearing aid (The copyright of these figures belongs to INNOFORCE Est.).
Figure 1.
Hearing tests using tone and speech audiometry of the right and left ear at the first consultation: unaided tone-audiometry (top left ear in blue and right ear in red) and aided tone and Freiburg mono-syllable speech audiometry for the left ear (bottom) using the BAHA hearing aid (The copyright of these figures belongs to INNOFORCE Est.).
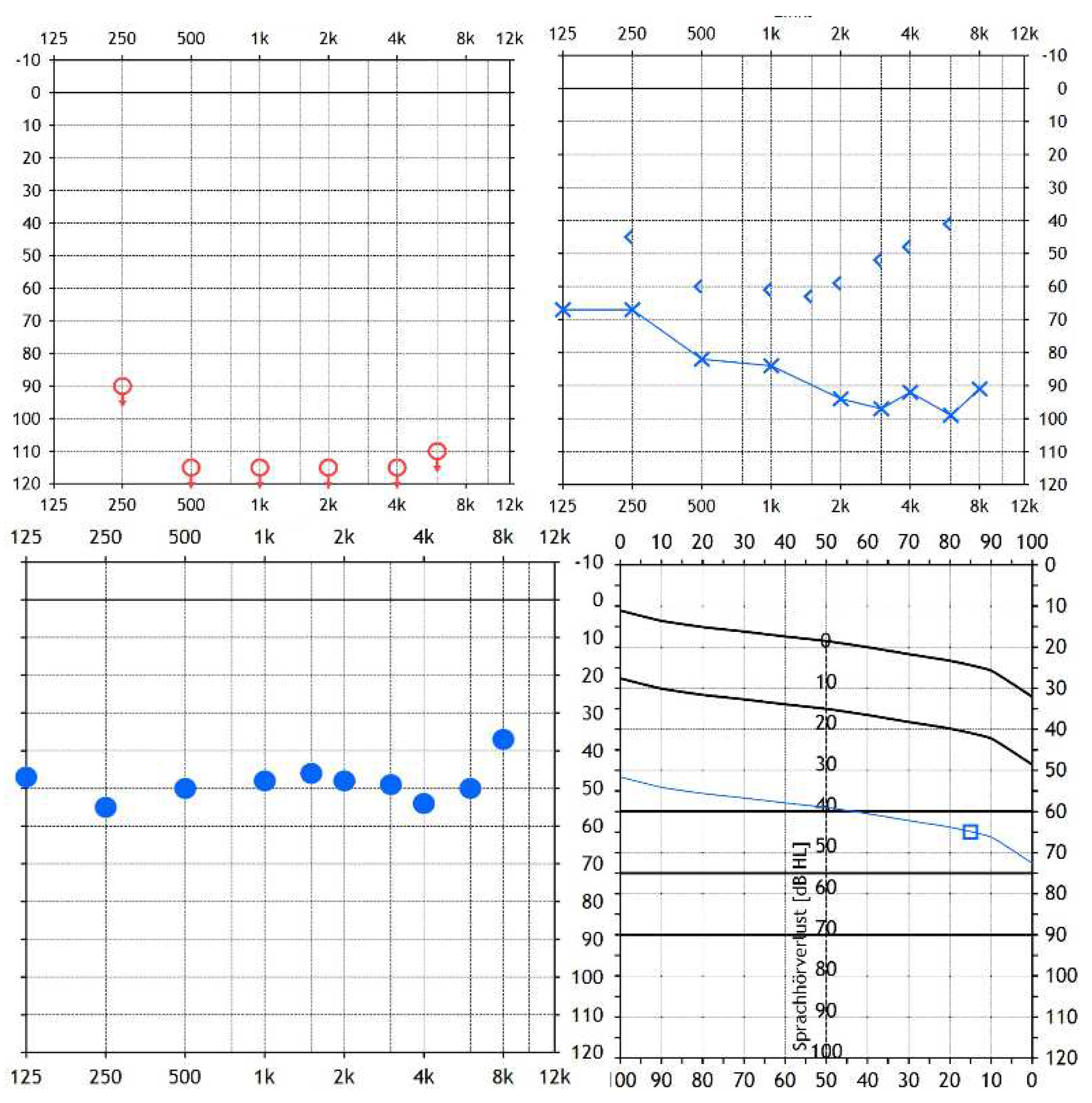
Figure 2.
Hardware setup for CI measurements and electrode illustration [10]: Figure 1, modified text “Research Audio Processor”  “Audio Processor”, licensed CC 4.0].
“Audio Processor”, licensed CC 4.0].
“Audio Processor”, licensed CC 4.0].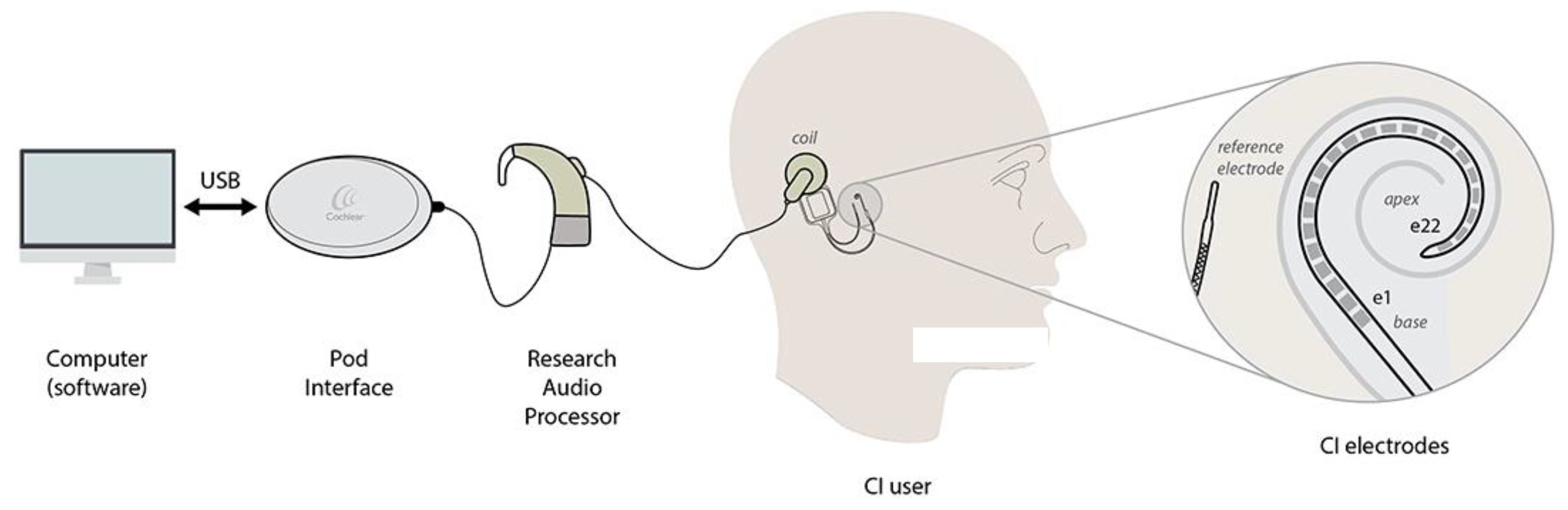
Figure 3.
X-ray, one day after surgery, for position control of the cochlear implant. Besides the cochlear implant, the stimulation electrode and the electrode lead of the trigeminus nerve stimulator are visible on the right side of this image.
Figure 3.
X-ray, one day after surgery, for position control of the cochlear implant. Besides the cochlear implant, the stimulation electrode and the electrode lead of the trigeminus nerve stimulator are visible on the right side of this image.
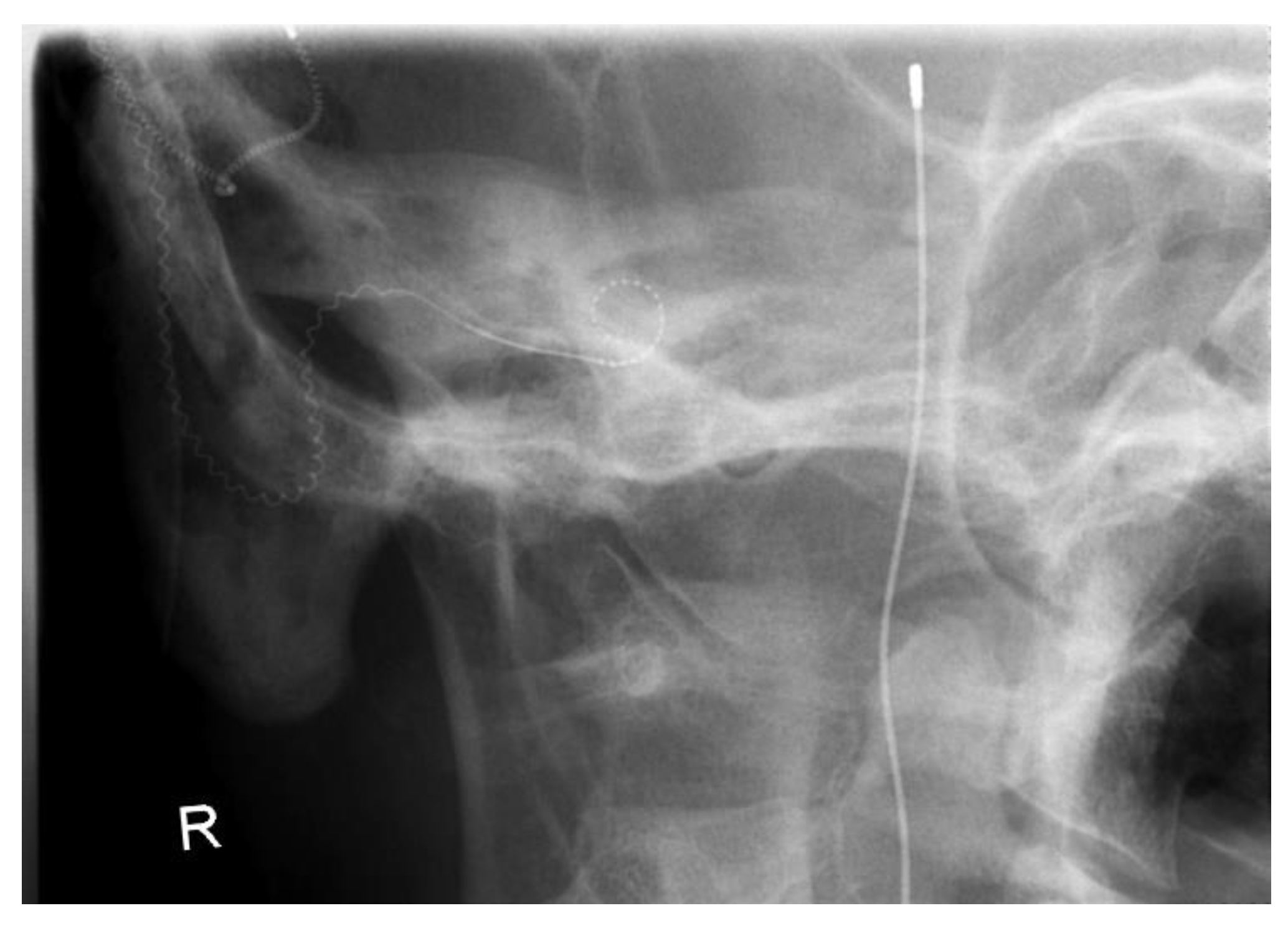
Figure 4.
Cochlear analyzation of the right ear (CI ear) pre-operatively using CASCINATION OTOPLAN 3 (in axial, coronal, and sagittal view).
Figure 4.
Cochlear analyzation of the right ear (CI ear) pre-operatively using CASCINATION OTOPLAN 3 (in axial, coronal, and sagittal view).
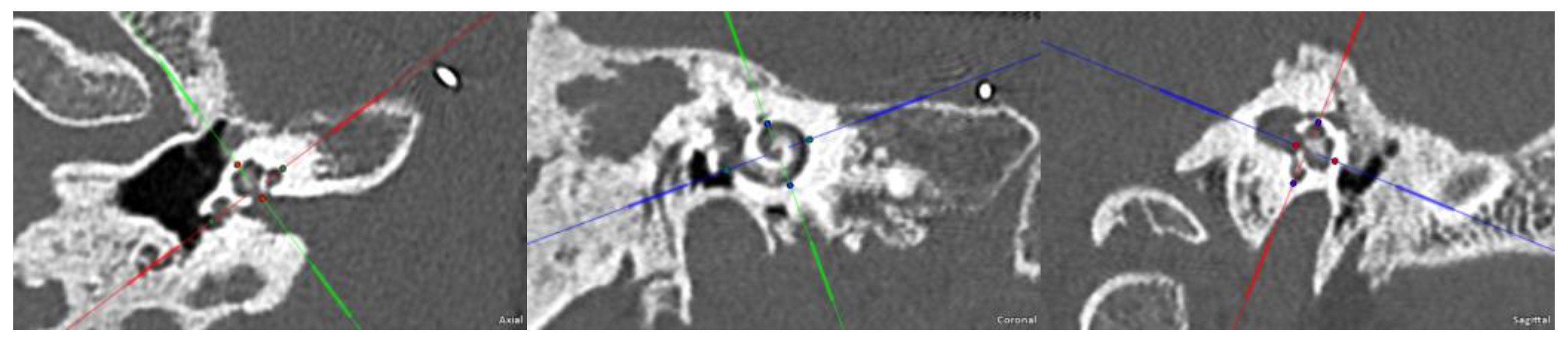
Figure 5.
EABR at medial electrode stimulation was recorded one month after the initial activation of the cochlear implant system. The first recordings (B1/B2) failed. After setting the number of averages from 1000 (default value) to 8000 (maximum value), we could record and reproduce the brainstem responses eIII and eV. A, B, C, D, and E show the recording order of these responses. 1 and 2 are the two recording channels for the right and left mastoids. Waveform illustrations by Nihon Kohden Neuropack S1 (Nihon Kohden Corporation, Japan) with kind permission of NIHON KOHDEN EUROPE GmbH.
Figure 5.
EABR at medial electrode stimulation was recorded one month after the initial activation of the cochlear implant system. The first recordings (B1/B2) failed. After setting the number of averages from 1000 (default value) to 8000 (maximum value), we could record and reproduce the brainstem responses eIII and eV. A, B, C, D, and E show the recording order of these responses. 1 and 2 are the two recording channels for the right and left mastoids. Waveform illustrations by Nihon Kohden Neuropack S1 (Nihon Kohden Corporation, Japan) with kind permission of NIHON KOHDEN EUROPE GmbH.
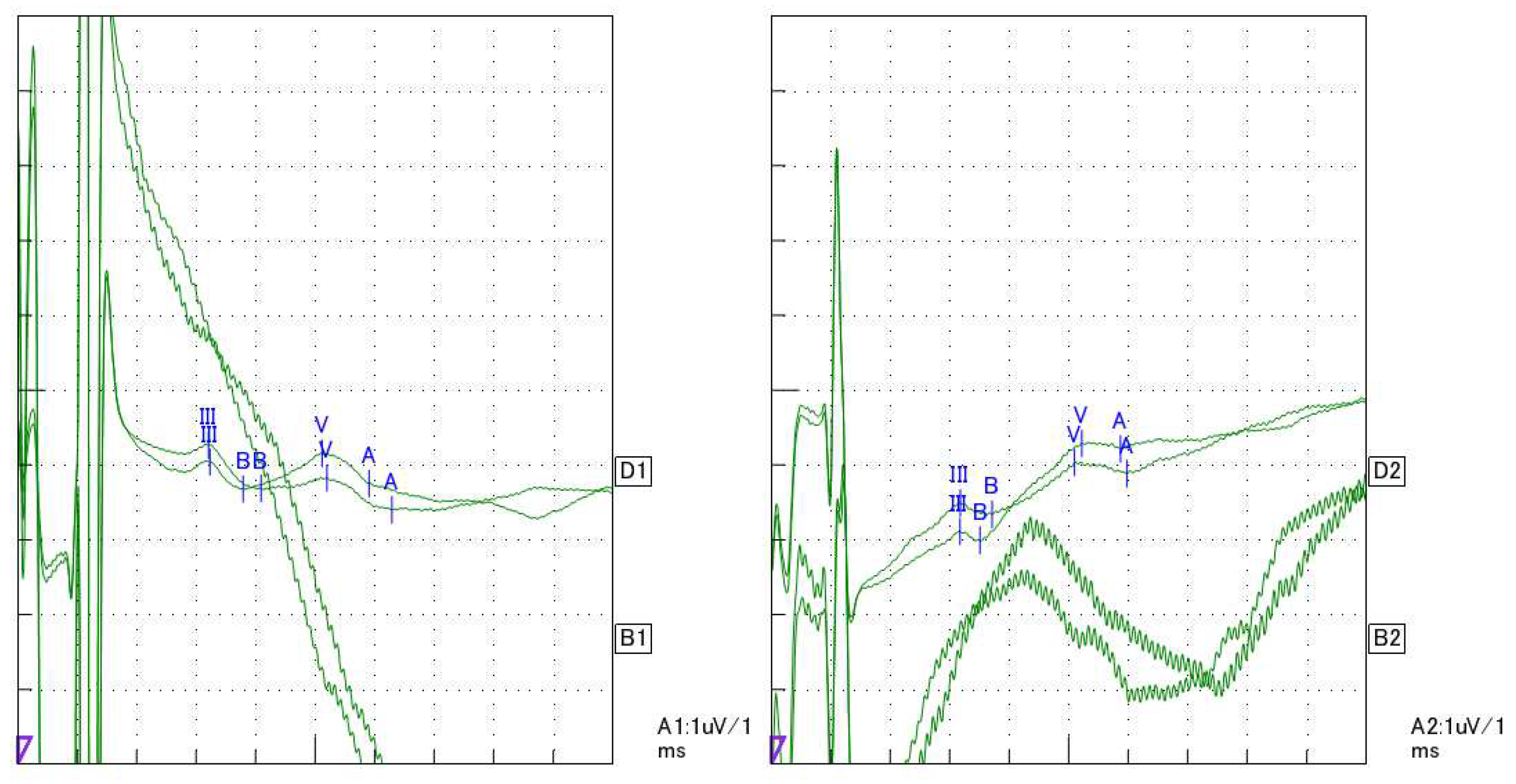
Figure 6.
EALR at medial electrode stimulation was recorded one month after the initial activation of the cochlear implant system. The first recordings (A, B, C, and D) failed. We averaged these four recorded waveforms. By this, we could record and reproduce the cortical responses P1-N1-P2-N2. A, B, C, D, and E show the recording order of these responses. 1 and 2 are the two recording channels for the right and left mastoids. Waveform illustrations by Nihon Kohden Neuropack S1 (Nihon Kohden Corporation, Japan) with kind permission of NIHON KOHDEN EUROPE GmbH.
Figure 6.
EALR at medial electrode stimulation was recorded one month after the initial activation of the cochlear implant system. The first recordings (A, B, C, and D) failed. We averaged these four recorded waveforms. By this, we could record and reproduce the cortical responses P1-N1-P2-N2. A, B, C, D, and E show the recording order of these responses. 1 and 2 are the two recording channels for the right and left mastoids. Waveform illustrations by Nihon Kohden Neuropack S1 (Nihon Kohden Corporation, Japan) with kind permission of NIHON KOHDEN EUROPE GmbH.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



