
Submitted:
13 December 2023
Posted:
14 December 2023
You are already at the latest version
Abstract
(1) Background If placenta percreta (PP) is suspected, one should take into account ultrasound and MRI data, which allow one to assess not only the depth of invasion of the placenta into the myometrium, but also the degree of involvement of the blood vessels of the uteroplacental region and the pelvis, the formation of adhesions and collaterals between organs as well; (2) Methods: The patient with suspected PP was examined by ultrasound and Magnetic Resonance Imaging (MRI) examination. Histological study was performed on paraffin sections (hematoxylin & eosin, Mallory staining); cytotrophoblast was detected with antibodies to cytokeratin-8; (3) Results MRI and ultrasound examinations showed placental invasion extending beyond the serous lining of the uterus involving the posterior wall of the bladder. Elective abdominal delivery was performed at 37 weeks. Surgical excision of the uterine wall with invaded villi and involved fibrous bladder wall were performed. Histological study revealed invasive cytotrophoblast cells in the uterine wall located up to adventitia of the uterine subserosal vessels only. Thinning of the uterine wall up to the serous membrane was detected; (4) Conclusions: Placental villi and trophoblast extended beyond the uterus is not histology equivalent to placenta percreta. To diagnose PP instrumental visualization methods should be used.
Keywords:
caesarean section
; uterine scar
; healing of the uterine wall
; placenta accreta spectrum
; placenta percreta
; invasion
1. Introduction
The term “placenta accreta” was proposed in the last century, when scientists Irving and Hertig first defined it as “abnormal partial or complete attachment of the placenta to the wall of the uterus” [1]. Abnormal attachment and invasion of the placenta villi is manifested in its inability to separate from the wall of the uterus.
As in the FIGO system [2] the proposed subcategories of PAS are designated as grades based on the degree of grossly assessed invasion and local tissue destruction: Grade 1 – Abnormally adherent placenta (pl. accreta) when the villi adhere directly to the myometrium without a decidual interface. Grade 2 – Abnormally invasive placentation (Pl. increta) when the villi invade into the myometrium. Grade 3 – Abnormally invasive placentation (Pl. percreta) when the villi invade the full thickness of the uterine wall either to the serosa or beyond. They are subdivided into: Grade 3a, limited to and including the uterine serosa; Grade 3b, when there is urinary bladder invasion; Grade 3c, when there is invasion of other pelvic tissue. PAS is a dangerous complication of pregnancy leading to maternal morbidity and mortality, associated with a high risk of massive blood loss.
Recently, PAS increased significantly from 1:1200 [3] to 1: 250 - 1:500 in all countries [4,5,6]. Observational studies in United States reported about 1: 272 in 2016 [7]. The most studied and proven factor leading to an increase in the incidence of PAS is number of previous caesarean sections (CS) [2,8,9]. Risk factors for PAS are the previous CS is 3%, 11%, 40%, 61% and 67% for one, two, three, four and five previous CS [5], respectively Uterine scar dehiscence represents an incomplete disruption of the uterine wall at the site of prior cesarean delivery, typically occurs within the anterior lower uterine segment overlying the bladder [10,11].
Risk factors for PAS includes as well the patient’s history of multiple surgical interventions on the uterus (myomectomy, hysteroscopy, curettage), uterine artery embolization, placenta previa and PAS [12], metabolic disorders [13,14,15], which probably initiates inflammation and incomplete regeneration for damaged tissues in the future [4].
2. Сase Report
Patient O*., 37 years old, was admitted to the Pregnancy Pathology Department of the Vidnovsky Perinatal Center in 2022. Singleton pregnancy. Placenta previa. The fetus was in cephalic presentation at 33 weeks and 2 days.
The patient was admitted to Vidnovsky Perinatal Center for therapy aimed at prolonging pregnancy at the period of 33 weeks and 2 days.
Recent pregnancy was the fifth, after the fourth birth. Incompetent scar on the uterus after two CS with the formation of the uterine prolapse or «hernia». Given that ultrasound examination placenta invaded into the uterine scar after previous CS surgery and the wall of bladder, placenta previa was revealed also.
The parity and anamnesis: This is the fifth pregnancy occurred in a natural cycle, no using high reproductive technologies. The first baby was born in 2007 after with spontaneous labor at 38 weeks. A healthy girl was born at 2900 grams. Second pregnancy was in 2012. A healthy boy was born weighing 2690 grams after urgent spontaneous birth. In 2013, the third pregnancy ended in emergency surgical delivery at 38 weeks due to clinically narrow pelvis, a boy was born, (the weight was 4200 g), healthy. The fourth pregnancy was in 2020. There was operative labor at 35 weeks due to severe preeclampsia. The girl was born, 2600 grams, healthy.
The first trimester proceeded without complications. When conducting a screening ultrasound at 13 weeks and 6 days, chorionic presentation on the uterine scar niche was diagnosed. No markers of preeclampsia were identified. Ultrasound examination performed at 19 weeks and 6 days, the myometrium in the area of the uterine scar dehiscence was 1.6 mm. Placenta рrevia was revealed as well. At 33 weeks the pregnant was admitted to the hospital because of elevated risk of premature labor. Ultrasound examination revealed a high risk of PAS as well. Ultrasound examination was performed using transabdominal and transvaginal devises (MEDISON ACCUVIX A30-RUS 2014, Korea and ultrasound diagnostic device of expert class WS80A-RUS 2019, Korea). It was found that the retroplacental myometrium is not visible by ultrasound examination on over 158x133 mm). Aberrant vessels were identified that penetrated to the serosa of the bladder (Figure 1). The placenta was diffusely thickened up to 46 mm, located along the anterior wall, the lower edge of the placenta overlaped the area of the internal os. Ultrasound signs were revealed formation of the uterine prolapse so-called «uterine hernia». High risk of placental invasion into the bladder was detected.
Magnetic resonance imaging (MRI) examination was performed by Siemens MAGNETOM Verio with magnetic field induction 3 T, using standard surface coils. Scanning was performed according to the routine protocol [16,17] with T2-weighted images obtained in three mutually perpendicular planes. А slice thickness of 3-4 mm, field of view of 32-42 cm. T2-weighted images with signal suppression from adipose tissue in the axial plane. T1-weighted images in sagittal and axial planes. T1-weighted images with suppression of MR signal intensity from adipose tissue in any plane, and also with obtaining diffusion-weighted images.
The study performed with a moderately full bladder, when the patient lying on her back. The interpretation of the results was carried out on the basis of the developed unified scoring system for the obtained MAPI data – RADS (Morbidly Adherent Placenta Imaging Reporting and Data System) [18] (Figure 2, Table 1). The developed MAPI-RADS system makes it possible to identify, systematize and quantify the signs of pathological PAS obtained during the study, which makes it possible to establish a class corresponding to the PAS grade and correlating with intraoperative view.
Considering the depth of placental invasion and the high risk of intraoperative massive blood loss, аutoplasma was prepared as the preparation for delivery. Three sessions of donor plasmapheresis were conducted. А result of this 1500 ml of autoplasma were prepared [19].
Planned abdominal delivery was performed at 37 weeks of pregnancy according to author’s technique. [20,21]. Briefly, further improvement of the methodology of organ preserving operations was reflected in the research “Method of operative delivery patients with placenta accretion into the uterine scar"[21]. Briefly, the essence of the technique is to combine tourniquet hemostasis with balloon tamponed of the vagina using a Zhukovsky catheter. The method was presented on Figure 3A-E.
An inferomedial laparotomy was performed with bypass of the umbilicus on the left Сaesarean section was carry out in the area of the uterine fundus. The fetus was removed from the uterine cavity and divided the umbilical cord and immersed in the uterus, the placenta was not separated. Incision on the uterus sewed up in two rows with separate vicryl sutures.
The operation was conducted under long-term epidural anesthesia (at the stage of Cesarean section) with subsequent transition to endotracheal anesthesia (at the stage of metroplasty). After inferomedian laparotomy, the lower uterine segment was examined. Local prolapse of uterine wall (sizes 200x200 mm) with a pronounced vascular network was visualized (Figure 3A).
A caesarean section was performed. A live born full-term boy, with the Apgar score of 7-8 points, was extracted at 6 minutes (the weight =3890 g, the body length =51 cm). After administration of uterotonics there were no signs of placental separation. The umbilical cord was tied and immersed in the uterine cavity. The uterus was with two rows with separate vicryl sutures. Next, the first tourniquet was applied above the «uterine hernia». In the area of the trigonum vesicae (trigonum Lieto). Mobilization was difficult due to placental invasion and severe tissue fibrosis. Below the uterine prolapse, the second uterine tourniquet was placed to capture the bladder in the area of the trigonum vesicae. The «uterine hernia» with an area of placental invasion was excised. The posterior wall of the bladder was resected over the length of 60 mm (Figure 3 B). The uterus with stitches in two rows with separate vicryl sutures. The bladder was sutured in two rows with a continuous vicryl suture. In order to reduce the volume of blood loss, vaginal balloon tamponade was performed using Zhukovsky vaginal catheter.
Intraoperative blood loss was 1547 ml. Two doses of autoplasma equivalent as1000 ml were transfused. 1281 ml of blood were collected intraoperatively, followed by reinfused autologous red blood cells in a volume of 336 ml. The postoperative period proceeded without complications. Postoperative period lasted 7 days.
Placenta and myometrium for morphological research was obtained after Caesarian section. Fragments of the myometrium in the uteroplacental region in PAS zone were excised according to the surgical method researched at the Vidnovsky Perinatal Center [21].
Gross examination: placental weigh was 420 g, dimensions corresponded 18x14x2.5 cm. At one of the edge was revealed area of grayish-red tissue (looks like myometrium) dimensions were 60x40 mm, attached to the maternal surface of the placenta. Thickness this segment varied from 15 mm with thinning up to serous layer (less than 1 mm). Adjacent to this fragment was a grayish area similar to the mucous membrane (of the bladder).
Histological examination. For histological examination, tissue samples were fixed with 10% buffered formalin (#60-001/S, LLC «BioVitrum» Russia). After 24 hours of fixation, the material was washed, dehydrated, and embedded in Histomix Extra paraffin (#10342, LLC «BioVitrum», Russia). Sections from paraffin blocks with a thickness of 4 μm were obtained on a Sakura rotary microtome Accu-Cut SRM200 (Sakura, Japan), stained with hematoxylin and eosin (#07-006, LLC «BioVitrum», Russia), Mallory trichrome kit (#21-036, LLC «BioVitrum», Russia). Microsections placed on glass slides were deparaffinized and re-hydrated in a graded ethanol series, then washed in water and stained with hematoxylin and eosin (LLC «BioVitrum», article: 07-006) or Mallory trichrome kit (#21-036, LLC «BioVitrum», Russia) for detection of connective tissue according to Mallory (LLC «BioVitrum», article: 21-036), then next they were dehydrated and placed in Vitrogel (LLC «BioVitrum», article 12-005) for further microscopic examination.
Immunohistochemical study. Sections from the paraffin blocks were mounted on lysine-coated glass slides (Menzel-Glaser Polysine®), rehydrated, followed by heat-mediated antigen retrieval in citrate solution (pH 6.0), blocked [1 h at RT in 10% goat serum + 0.1% Tween-20 in Tris-buffered saline (TBS)] and incubated overnight at 4˚C with primary antibodies specifically interacting with the antigen on the section, then washed using phosphate buffer. The products of interaction primary antibodies with the antigen were revealed using the horseradish peroxidase conjugate specifically bound to secondary anti-species antibodies. Novolink ™ Polymer Reagent Kit was used to detect bound primary antibodies (#RE7150, Leica, UK) followed by counter-staining with Mayer’s hematoxylin solution (LLC «BioVitrum», article: 05-002/S), dehydration in a graded ethanol series, and mounting with Vitrogel (LLC «BioVitrum», article 12-005). An aqueous solution of 3,3-diaminobenzidine tetrahydrochloride (DAB) was used to stain the product of the immunohistochemical reactions. Products of the positive immunohistochemical reaction were determined as brown staining of the membrane and cytoplasm of cells. For the negative control, the sections were subjected to standard immunohistochemical procedure without incubation with primary antibodies. The positive control was selected according to the specifications manufacturer.
We used mouse monoclonal antibody to cytokeratin 8 (cat# DB098-RTU, DB Biotech) for the detection of epithelial cells. Specimen microscopy was performed using Leica microscope system, consisting of Leica DM2500 microscope, Leica DFC290 video camera image microscopy and analysis software, Image Scope M (Leica, Germany) as well.
All procedures performed in this study involving all patients comply with the ethical standards of the institutions ethics committee and the 1964 Declaration of Helsinki and its subsequent amendments or comparable Ethical standards. This research was approved by the Bioethics Committee at FSBI (protocol No 35 (11) dated 03/23/2022). All included women gave voluntary Agreement to participate in the study, in accordance with the Declaration of Helsinki on the conduct of biomedical research.
As the results of the histological examinations, thinning of the lower segment to a serose membrane with invaded villi presented by an uneven layer of borderline fibrinoid. In myometrium of uteroplacental region multiple villi with dystrophic changes and necrosis, including loss of basophilia of nuclei coated in fibrinoid (“villi - shadows”), with cytotrophoblast remnants were revealed (Figure 4 and Figure 5). The placental villous tree was represented by intermediate villi, angiogenesis with predominantly of branching vessels with unevenly expressed blood supply. Decidual lamina with vast deposits of fibrinoid, and few decidual cells (Figure 4).
In the described structures, moderate lymphoid infiltration with the formation of nodules and vasculitis (chronic cystitis signs). Small foci of squamous metaplasia of the transitional epithelium were observed. Separated muscle bundles and edematous serous membrane with local microvascular thrombosis and/or adjacent retroplacental hematoma zone were detected. There was a large retrochorial hematoma several days old, reaching serous uterine membrane (Figure 4 and Figure 5).
By immunohistochemical examination studies with primary antibody to cytokeratin-8, invasive cytotrophoblast cells were detected in the uterine wall located up to the subserosal layer, including those reaching the adventitia of the walls of subserosal vessels. In the same area, multinucleated giant cells were detected (Figure 5). Multinucleated giant cells were associated to invasion arrested, because in cases of physiological pregnancy they were located at the border of invasion [22].
Moreover, large deposits of fibrinoid were detected in the uteroplacental region. It that fibrinoid is known to be combined product created as a result of both coagulation of plasma proteins and trophoblastic secretion. [23]. We detected increased fibrinoid amount, multiple hemorrhages, areas of dystrophy and necrosis of the myometrium in the uteroplacental region, which significantly disrupted the usual structure of the myometrium, which made the diagnosis unclear.
3. Conclusions
How to interpret these changes according to the latest FIGO classification? So performed study raises a number of questions. How to interpret these changes according to the latest FIGO classification? According to ultrasound and intraoperative data, we show close interactions between the wall of the uterus and the bladder. Assessment of the placental villi invasion depth do not confirm their presence in the bladder wall or parametrium. The formation of adhesions between the placenta and the uterine wall and bladder may be one of the options for PP.
Perhaps, the wall of the bladder is attached to the wall of the uterus through the proliferation of connective tissue, which may be regarded as a variant of pelvic adhesive disease. Should these lesions be classified as a controversial form PP?
Although histological examination considered to be the «gold standard» for verifying the diagnosis, when studying patients with PAS, an integrated approach should be used, taking into account data from visual diagnostic methods (ultrasound, MRI) and intraoperative view. Our study presented a new comprehensive approach to the morphological verification of PP. A detailed analysis in the same cases is necessary. In the future this may require additions and clarifications to the speculated PAS classification.
Author Contributions
Author Contributions: “Conceptualization, N.V.N., I.A.K. and A.P.M.; methodology, T.V.F. and A.P.M.; validation, E.R.M. and E.I.B.; formal analysis, T.N.B. and I.A.G.; investigation, N.B.T.; resources, T.N.B.; data curation, E.R.M.; writing—original draft preparation, N.V.N.; writing—review and editing, N.V.N. and K.A.A.; visualization, A.P.M.; supervision, Yu.E.D; project administration, L.M.M. All authors have read and agreed to the published version of the manuscript.”.
Funding
This research was carried out within the framework of the state assignment FSBI “Petrovsky National Research Centre of Surgery”, 119991 Moscow, Russian Federation, No. 123030700104- 3.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee at Avtsyn Research Institute of Human Morphology (protocol No 35 (11) dated 23 March 2022.
Informed Consent Statement
Written consent for the publication of pictures and personal information was obtained from the patient described in this case report.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Irving, C.; Hertig, A.T. A study of placenta accreta. Surg. Gynecol. Obstet. 1937, 64, 178–200. [Google Scholar]
- Jauniaux, E.; Ayres-de-Campos, D.; Langhoff-Roos, J.; Fox, K.A.; Collins, S. FIGO Placenta Accreta Diagnosis and Management Expert Consensus Panel. FIGO classification for the clinical diagnosis of placenta accreta spectrum disorders. Int. J. Gynaecol. Obstet. 2019, 146, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Morlando, M.; Sarno, L.; Napolitano, R.; Capone, A.; Tessitore, G.; Maruotti, G.M; Martinelli, P. Placenta accreta: Incidence and risk factors in an area with a particularly high rate of cesarean section. Acta Obstet. Gynecol. Scand. 2013, 9, 457–460. [Google Scholar] [CrossRef] [PubMed]
- Carusi, D.A. The placenta accreta spectrum: Epidemiology and risk factors. Clin. Obstet. Gynecol. 2018, 61, 733–42. [Google Scholar] [CrossRef] [PubMed]
- Silver, R.M.; Landon, M.B.; Rouse, D.J.; Leveno, K.J.; Spong, C.Y.; Thom, E.A.; Moawad, A.H.; Caritis, S.N.; Harper, M.; Wapner, R.J.; Sorokin, Y.; Miodovnik, M.; Carpenter, M.; Peaceman, A.M.; O'Sullivan, M.J.; Sibai, B.; Langer, O.; Thorp, J.M.; Ramin, S.M.; Mercer, B.M. , National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Maternal morbidity associated with multiple repeat cesarean deliveries. Obstet. Gynecol. 2006, 107, 1226–32. [Google Scholar] [CrossRef] [PubMed]
- Upson, K.; Silver, R.M.; Greene, R.; Lutomski, J.; Holt, V.L. Placenta accreta and maternal morbidity in the Republic of Ireland, 2005-2010. J Matern. Fetal Neonatal Med. 2014, 27, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Obstetric Care Consensus, No. Obstetric Care Consensus No. 7: placenta accreta spectrum. Obstet Gynecol. 2018, 132, e259–e275. [Google Scholar] [CrossRef]
- Milovanov, A.P.; Aksenenko, V.A.; Lukashevich, A.A.; Fokina, T.V.; Stepanova, I.I.; Tikhonova, N.B. The leading role of scars after the caesarian section in the pathogenesis of placenta previa accreta. Clin. exp. morphology (In Russ.). 2019, 8, 10–18. [Google Scholar] [CrossRef]
- Milovanov, A.P.; Bushtarev, A.V.; Fokina, T.V. Special features of cytotrophoblastic invasion in complete placenta previa and increta. Arkh Pathol. Arkh Pathol. (In Russ.). 2017, 79, 30–35. [Google Scholar] [CrossRef]
- Hecht, J.L.; Baergen, R.; Ernst, L.M.; Katzman, P.J.; Jacques, S.M.; Jauniaux, E.; Khong, T.Y.; Metlay, L.A.; Poder, L.; Qureshi, F.; Rabban JT 3rd, Roberts, D.J.; Shainker, S.; Heller, D.S. Classification and reporting guidelines for the pathology diagnosis of placenta accreta spectrum (PAS) disorders: recommendations from an expert panel. Mod Pathol. 2020 Dec;33, 2382-2396. [CrossRef]
- Zhu, Z.; Li, H.; Zhang, J. Uterine dehiscence in pregnant with previous caesarean delivery. Ann Med. 2021, 53, 1265–1269. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Bhide, A. Prenatal ultrasound diagnosis and outcome of placenta previa accreta after cesarean delivery: a systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2017, 217, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Habek, D.; Cerovac, A.; Luetić, A.; Marton, I.; Prka, M.; Kulaš, T.; Ujević, B. Modified Stark's (Misgav Ladach) caesarean section: 15 – year experience of the own techniques of caesarean section. Eur J Obstet Gynecol Reprod Biol. 2020, 247, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Antila-Långsjö, R.M.; Mäenpää, J.U.; Huhtala, H.S.; Tomás, E.I.; Staff, S.M. Cesarean scar defect: A prospective study on risk factors. Am J Obstet Gynecol. 2018, 219, 458–e1. [Google Scholar] [CrossRef]
- Markaryan, N.M.; Vandysheva, R.A.; Nizyaeva, N.V.; Gioeva, Z.V.; Mikhalev, S.A.; Khamoshina, M.B.; Mikhaleva, L.M. Clinical and morphological assessment of uterine scars after caesarean section in patients with gynecological and extragenital diseases. Clin. exp. morphology (In Russ.). 2023, 12, 34–45. [Google Scholar] [CrossRef]
- Jha, P.; Pōder, L.; Bourgioti, C.; Bharwani, N.; Lewis, S.; Kamath, A.; Nougaret, S.; Soyer, P.; Weston, M.; Castillo, R.P.; Kido, A.; Forstner, R.; Masselli, G. Society of Abdominal Radiology (SAR) and European Society of Urogenital Radiology (ESUR) joint consensus statement for MR imaging of placenta accreta spectrum disorders. Eur Radiol. 2020, 30, 2604–2615. [Google Scholar] [CrossRef]
- Dighe, M. MR Imaging of Abnormal Placentation. Magn Reson Imaging Clin N Am. 2017 Aug;25, 601-610 ;25. [CrossRef]
- Uchevatkina, P.V.; Bychenko, V.G.; Kulabukhova, E.A.; Luzhin, I.A.; Shmakov, R.G. System of a unified approach to interpretation of magnetic resonance tomography in diagnostics of pathological placental attachment "MAPI-RADS" (morbidly adherent placenta imaging reporting and data system). REJR 2021, 11, 174–190. [Google Scholar] [CrossRef]
- Patent for invention. Method of correction of blood loss during surgical resolution of pregnant women with placenta ingrowth. Plakhotina, E.N.; Belousova, T.N.; Kulikov, I.A.; Pavlyutina, K.M.; Latyshev RV RU 2 704 464 C1, Russia, 2019 Application number: 2019119021. Registration date: 2019.06.19.
- Kulikov, I.A.; Shmakov, R.G.; Belousova, T.N.; Plakhotina, E.N.; Nizyaeva, N.V.; Geilis, I.A.; et al. Efficacy of the tourniquet hemostasis combined with vaginal balloon tamponade using a Zhukovsky vaginal catheter during delivery in placenta accreta spectrum. Obstetrics and Gynegology. 2022, 10, 58–66. (In Russian) [Google Scholar] [CrossRef]
- Patent for invention Method of surgical delivery of patients with placenta ingrowth in the uterine scar. Kulikov, I.A.; Belousova, T.N.; Sovaev, N.I.; Plakhotina, E.N.; Musaeva, S.V.; Pavlyutina, K.M.; Petrov AE RU 2706368 C1, Russia, 2019 Application number: 2019118817. Registration date: 06.18.2019.
- Milovanov, A.P. Cytotrophoblastic invasion is the most important mechanism of placement and pregnancy progression (in Russian only). Arkhiv Pathologii. 2019, 81, 5 10. (In Russ.). [CrossRef]
- Benirschke, K.; Burton, G.J.; Baergen, R. Pathology of the human placenta. 6th edition. Berlin, Heidelberg: Springer-Verlag . 2012. 939 p. ISBN: 0-387-26738-7.
- Tikhonova, N.B.; Milovanov, A.P.; Aleksankina, V.V.; Fokina, T.V.; Boltovskaya, M.N.; Aleksankin, A.P. The role of adipose tissue in the healing of the rat uterine wall after a full-thickness surgical incision. Clin. exp. morphology 2021, 10, 72–80, (In Russ.). [Google Scholar] [CrossRef]
Figure 1.
Ultrasound sings of placenta percreta. A. «Uterine hernia»: Protrusion of the placenta beyond the uterine wall, absence of retroplacental myometrium. B. Aberrant vessels located perpendicular to the wall of the bladder.
Figure 1.
Ultrasound sings of placenta percreta. A. «Uterine hernia»: Protrusion of the placenta beyond the uterine wall, absence of retroplacental myometrium. B. Aberrant vessels located perpendicular to the wall of the bladder.
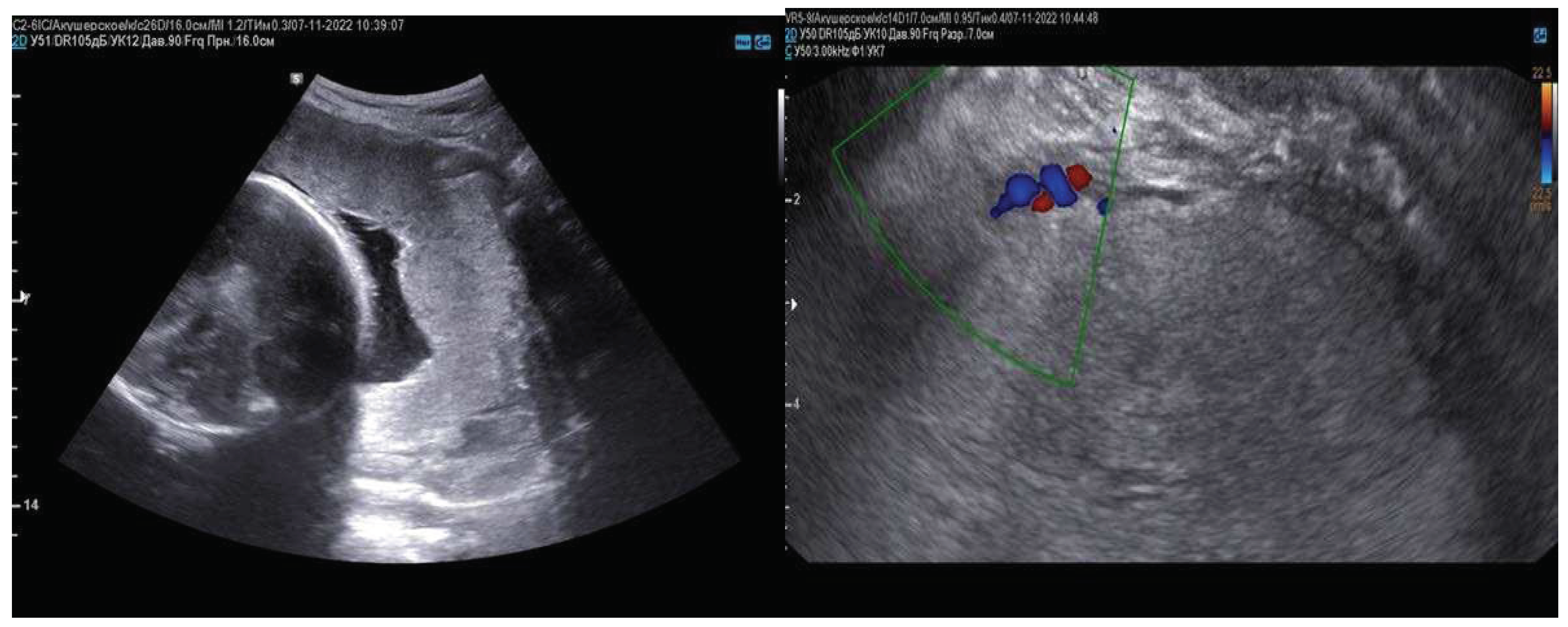
Figure 2.
Placenta percreta. MRI T2VI in the Sag, Cor, Ax plane. А–С–Zone of deep placenta increta. MRI visual view was shown the spread lesions placenta beyond the serous membrane of the uterus with the involvement of the posterior wall of the bladder. Above mentioned changes were associated to areas of neoangio- and vasculogenesis including large retroplacental blood vessels (indicated by an arrow) in the combination with local thinning of the uterine wall in this area and protrusion like a “uterine hernia” or “uterine window” (A-C).
Figure 2.
Placenta percreta. MRI T2VI in the Sag, Cor, Ax plane. А–С–Zone of deep placenta increta. MRI visual view was shown the spread lesions placenta beyond the serous membrane of the uterus with the involvement of the posterior wall of the bladder. Above mentioned changes were associated to areas of neoangio- and vasculogenesis including large retroplacental blood vessels (indicated by an arrow) in the combination with local thinning of the uterine wall in this area and protrusion like a “uterine hernia” or “uterine window” (A-C).
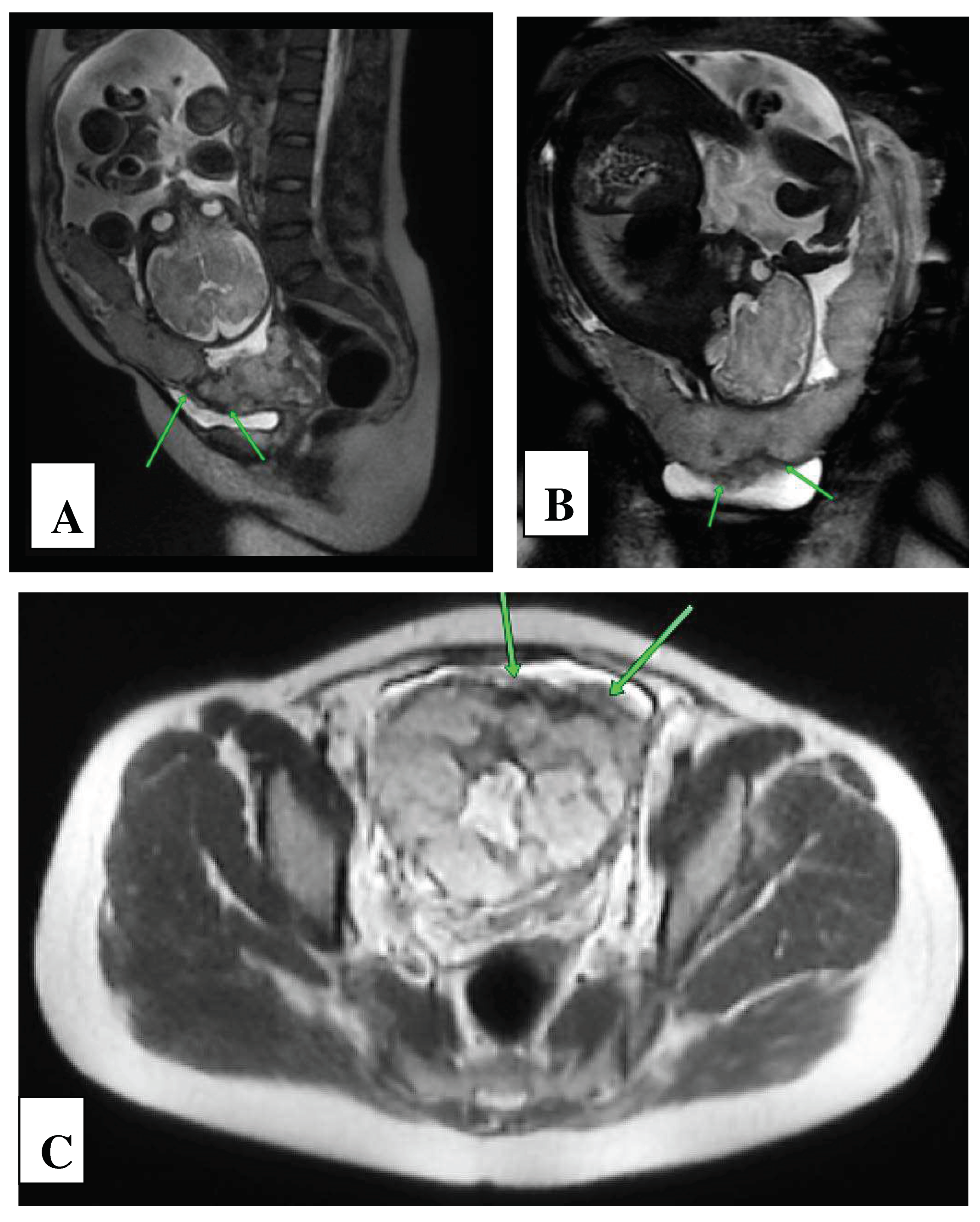
Figure 3.
Intraoperative view in case of placenta percreta. А–Intraoperative view of «hernia of uterine wall». В – Intraoperative view: Application of the first uterine tourniquet along the upper edge of the uterine hernia after completion of the bottom cesarean section. С, D – The second uterine tourniquet application. Excision of the uterine hernia along the lower edge of one after mobilization of the bladder completed. Е– Maternal surface of the placenta with attached myometrium zone (placental villi invaded into the altered myometrium), as well as a resected area of the bladder as well (yellow marker shows the posterior wall of the bladder; black marker shows mucous membrane of the bladder).
Figure 3.
Intraoperative view in case of placenta percreta. А–Intraoperative view of «hernia of uterine wall». В – Intraoperative view: Application of the first uterine tourniquet along the upper edge of the uterine hernia after completion of the bottom cesarean section. С, D – The second uterine tourniquet application. Excision of the uterine hernia along the lower edge of one after mobilization of the bladder completed. Е– Maternal surface of the placenta with attached myometrium zone (placental villi invaded into the altered myometrium), as well as a resected area of the bladder as well (yellow marker shows the posterior wall of the bladder; black marker shows mucous membrane of the bladder).
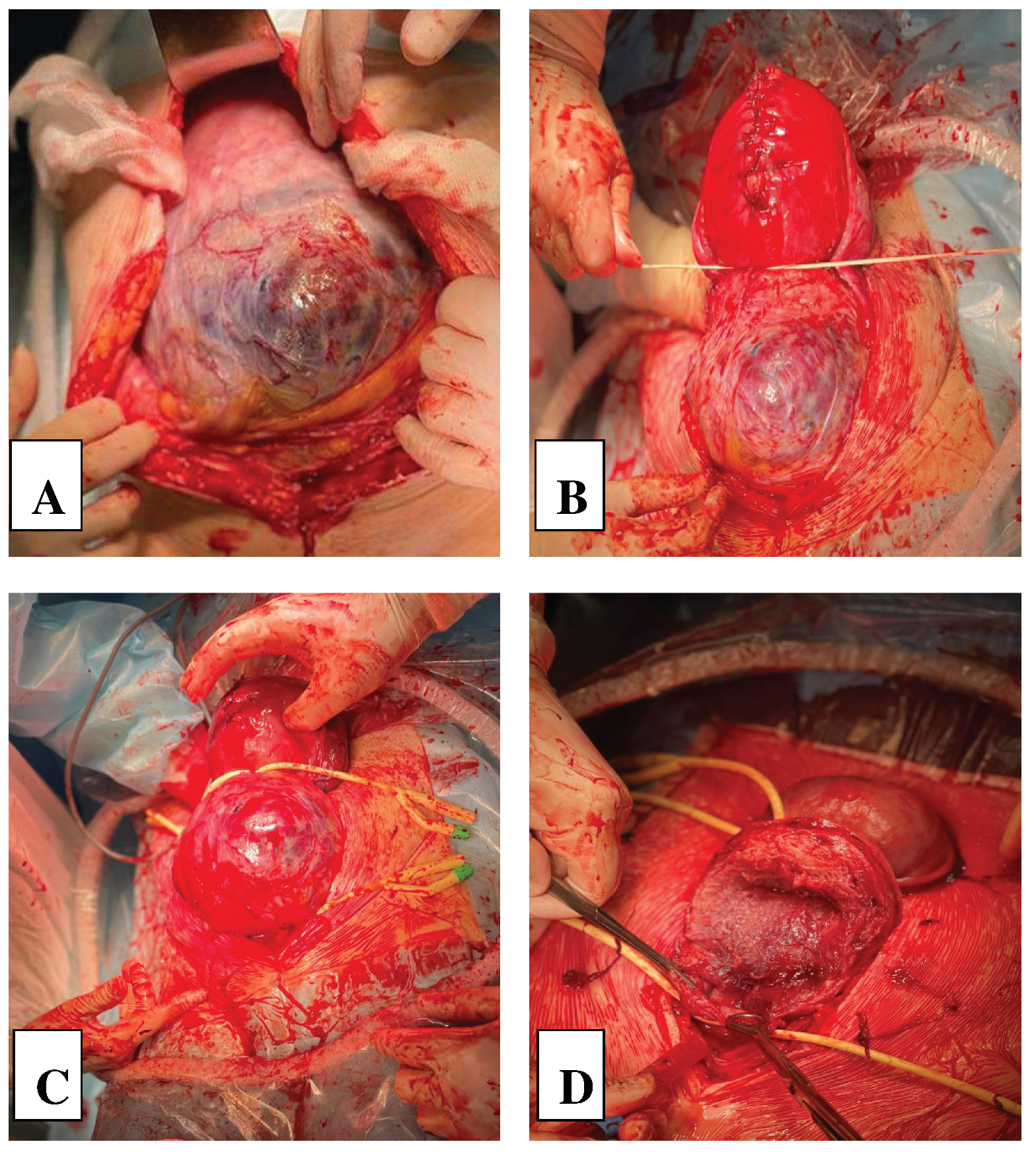
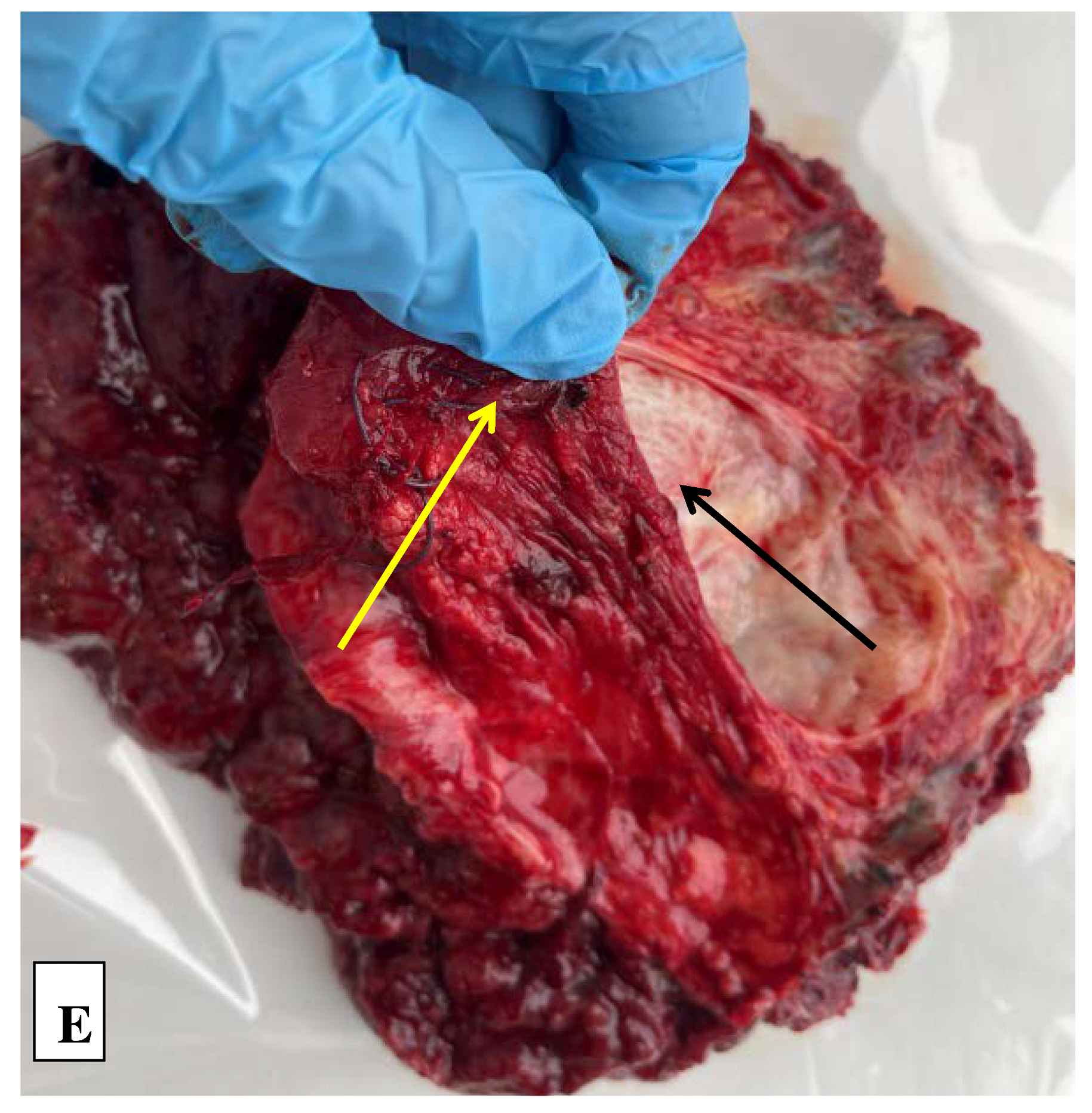
Figure 4.
Histological examination of the uteroplacental region (hematoxylin-eosin staining). A – Сollage of 6 figures of the uteroplacental region with attached bladder wall; hematoxylin and eosin staining, x50; B – The bladder wall; The bladder mucous membrane is lined to transitional type epithelium, hematoxylin and eosin staining, x50; C – The lumen of the vessel is marked with arrows, hematoxylin and eosin staining, x50; D, E – Mallory staining, x50.
Figure 4.
Histological examination of the uteroplacental region (hematoxylin-eosin staining). A – Сollage of 6 figures of the uteroplacental region with attached bladder wall; hematoxylin and eosin staining, x50; B – The bladder wall; The bladder mucous membrane is lined to transitional type epithelium, hematoxylin and eosin staining, x50; C – The lumen of the vessel is marked with arrows, hematoxylin and eosin staining, x50; D, E – Mallory staining, x50.
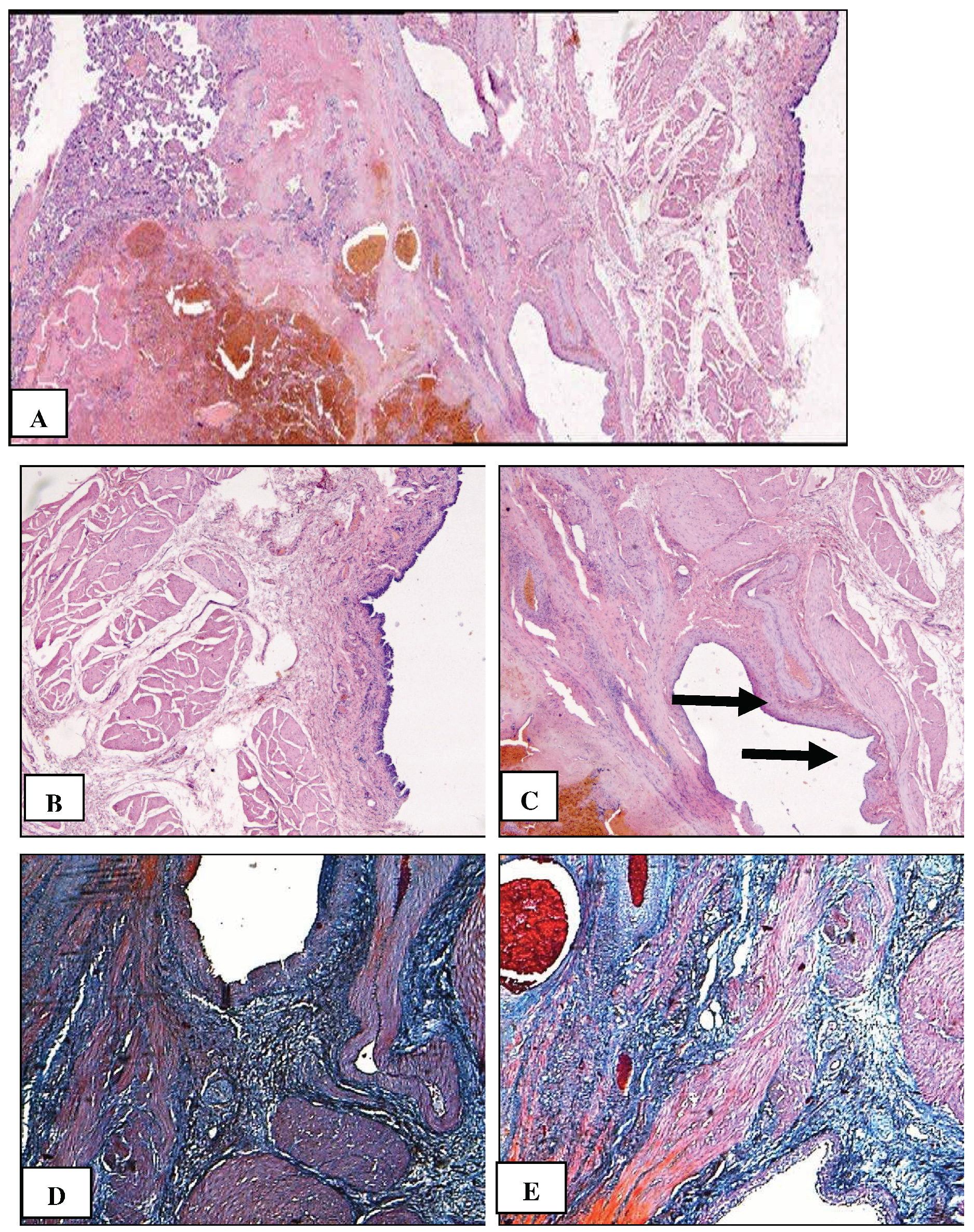
Figure 5.
Immunohistochemical staining using primary antibodies to cytokeratin-8 (CK8). A – Сollage of 9 figures: Uteroplacental region in case of placenta percreta. Invasive trophoblast at the border between the uterus and bladder; B – The wall of bladder (the transitional epithelium, a type of stratified epithelium composed of several layers of cells, lines the bladder mucosa are stained brown), x100; C – Аdhesion of the bladder to the uterine wall. Cytokeratin 8+ trophoblast cells do not penetrate into the lumen of the vessel (there is a blood vessel in the center), x50; D, E – Survival of trophoblast cells converted in fibrinoid in the uterine wall, Dx100, Ex200; E, G – CK8+ trophoblast cells and multinucleated cells (brown staining) in the vessel wall of myometrium, F x100, G, x400 5.
Figure 5.
Immunohistochemical staining using primary antibodies to cytokeratin-8 (CK8). A – Сollage of 9 figures: Uteroplacental region in case of placenta percreta. Invasive trophoblast at the border between the uterus and bladder; B – The wall of bladder (the transitional epithelium, a type of stratified epithelium composed of several layers of cells, lines the bladder mucosa are stained brown), x100; C – Аdhesion of the bladder to the uterine wall. Cytokeratin 8+ trophoblast cells do not penetrate into the lumen of the vessel (there is a blood vessel in the center), x50; D, E – Survival of trophoblast cells converted in fibrinoid in the uterine wall, Dx100, Ex200; E, G – CK8+ trophoblast cells and multinucleated cells (brown staining) in the vessel wall of myometrium, F x100, G, x400 5.
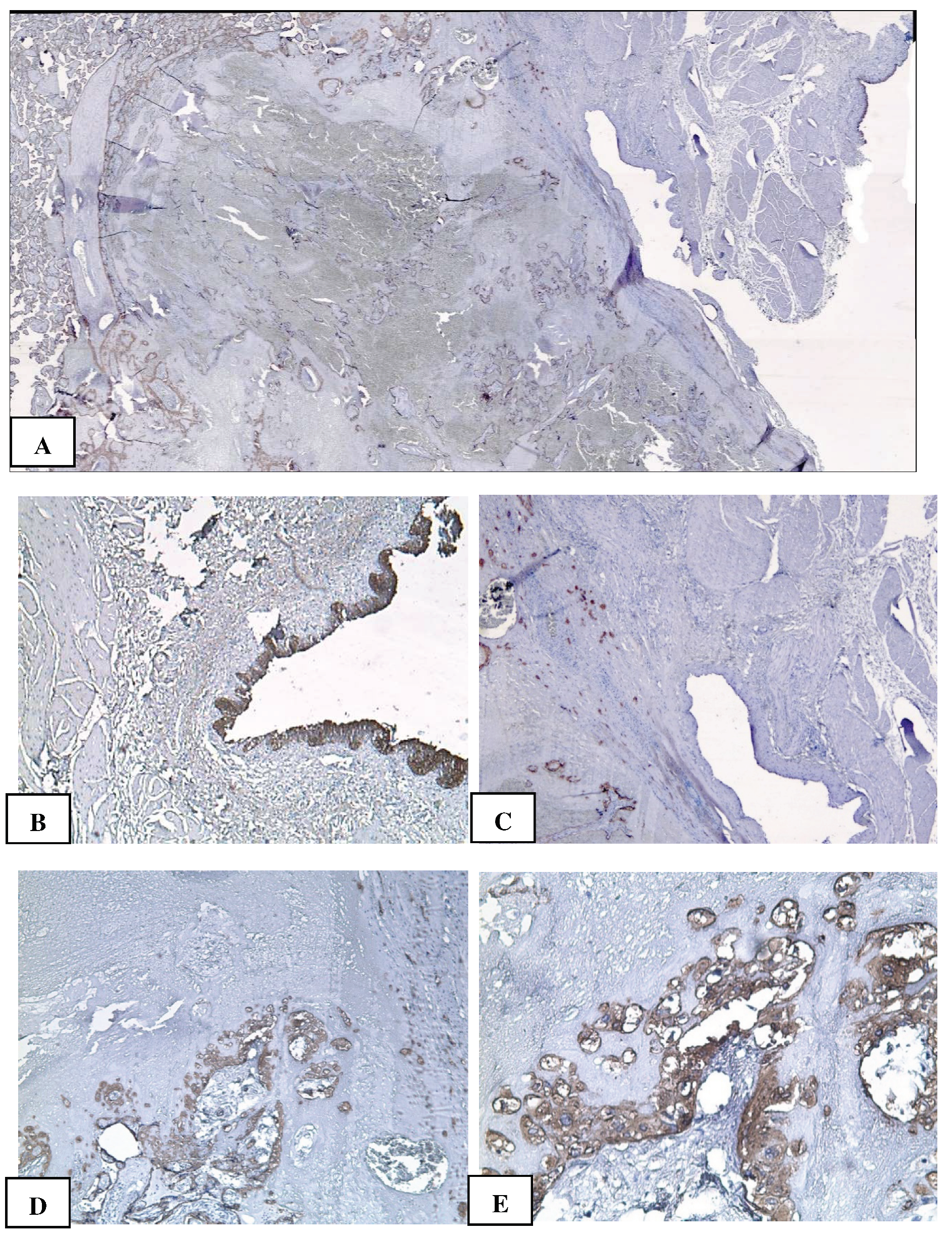
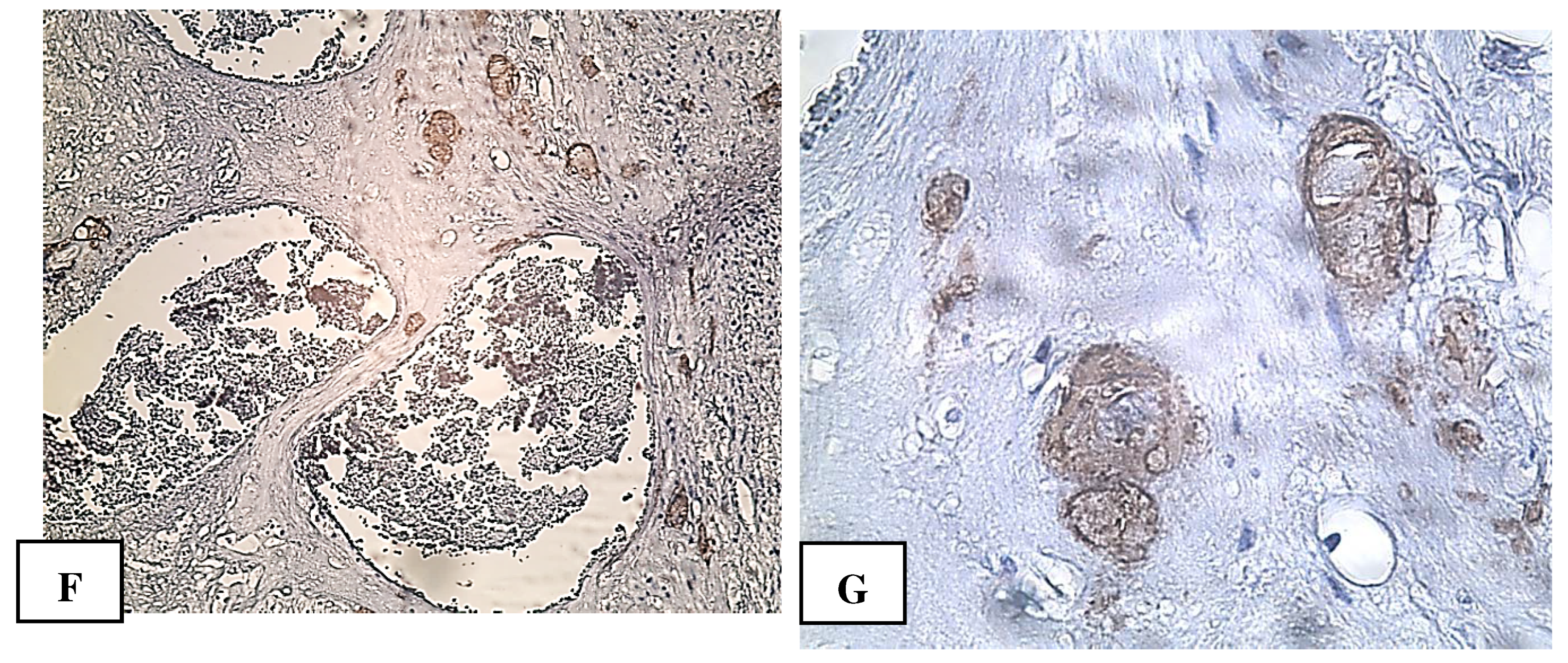

Table 1.
MRI signs assessment scale: basic and additional.
| Basic signs: | Availability | MAPI Scores - RADS |
|---|---|---|
| Local prolapse of the uterine wall («uterine hernia») | present | 2 |
| Thinning of the myometrium in the area where the placenta adjacent | present | 2 |
| MRI vascular lacuna visualization in the structure of the placenta | present | 2 |
| Vascular band MRI visualization in the structure of the placenta | present | 2 |
| Retroplacental hypointense “shadow” | present | 2 |
| Additional signs: | ||
| Varicose veins of the uterine wall and parametrium | Yes | 1 |
| Central/marginal placenta previa | Yes | 1 |
| Spread of the placenta beyond the walls of the uterus | Yes | 3 |
| Sum of points: | 15 | |
*(according to «MAPI-RADS» (Morbidly Adherent Placenta Imaging Reporting and Data System) [18]. Given MRI examination data it was revealed PP (class 5 according to MAPI - RADS).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



