
Submitted:
14 December 2023
Posted:
15 December 2023
You are already at the latest version
Abstract
Breast cancer-related lymphedema (BCRL) affects approximately 20% of women after breast cancer therapy. Advances in treatment have increased life expectancy, thus the prevalence of BCRL will continue to rise with the number of cancer survivors. Hence the need to develop strategies to prevent this condition. We provide a systematic review of the literature on primary prevention of BCRL by prophylactic lymphatic surgery (PLS).
Between June and August 2022, we conducted a search of PubMed, Google Scholar and Cochrane. In the end a total of eighteen papers were selected.
The eleven studies without a control group reported only 15 of 342 patients who developed lymphedema at least six months after PLS (4.59%). The seven studies with a control group included 569 patients, 328 cases and 241 controls. Among the cases, 36 (10%) developed lymphedema. In contrast, the incidence of lymphedema in controls was 40% (98 of 241 patients).
Formulation of definite recommendations in favour of PLS is hindered by low-quality studies. There is no consensus on which technique should be preferred, nor on whether adjuvant radiotherapy might affect the efficacy of PLS. Randomized controlled trials are mandatory to conceive evidence-based recommendations.
Keywords:
Breast cancer- related lymphedema
; lymphatic surgery
; microsurgery
; primary prevention
; lymphedema
Introduction
Lymphedema is characterized by cumulative tissue swelling caused by impaired drainage function of the lymphatic vessels. It may be the result of aberrant lymphatic development, as in primary cases, or be secondary to traumatic or iatrogenic injury to lymph nodes or lymphatic vessels [1].
The condition is both physically and psychologically distressing, as patients suffer from chronic pain and decreased strength and function of the affected limbs [2].
In the western world, lymphedema is most commonly associated with secondary cases related to breast cancer treatment [3].
The incidence of BCRL after axillary lymph node dissection (ALND) varies widely, ranging from 14.1% to 33.4%, with the highest rates reported in patients undergoing adjuvant radiotherapy [4]. Several conservative strategies have been implemented to reduce the risk of developing lymphedema in breast cancer patients after ALND or to treat it, once it has occurred [5,6].
The most commonly used options include exercise, manual lymph drainage, compression therapy and lymph taping (kinesio tape). Although there is currently no consensus on the most effective conservative treatment option or combination of options, surgery has emerged as a “last-ditch” effort when lymphedema reoccurs after all other measures have failed [7].
Surgical techniques currently utilized in the treatment of lymphedema include liposuction, vascularized lymph node transfer (VLNT) and lymphatic-venous anastomosis (LVA) [8].
The former directly aims to reduce the volume of the affected limb, whereas VLNT affects lymphatic drainage by potentially inducing the formation of lymphatic vessels over time. LVA, on the other hand, diverts lymphatics directly into the venous circulation of the arm, bypassing the impaired lymphatic drainage. The clinical efficacy of the above options varies greatly, whether conservative or surgical, with most findings reporting only marginal improvements or none whatsoever [9]. In 2010, prophylactic LVA following ALND was conceived as a strategy for the primary prevention of lymphedema, under the protocol known as the Lymphatic Microsurgical Preventing Healing Approach (LYMPHA) [3,10].
Few studies have quantitatively assessed the impact and clinical outcomes of this intervention in the primary prevention of BCRL. This manuscript aims to present a systematic review of the state of the art and the most current evidence supporting the use of PLS.
MATERIALS AND METHODS
Literature search
A review of the literature was carried out according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. An electronic search was conducted through PubMed/Medline, Google Scholar and Cochrane Database between June and August 2022 by two independent reviewers (DP and FG). The databases were searched using the following Medical Subject Headings (MeSH) terms “lymphatic venous anastomosis”;” lymphaticovenular anastomosis“;“ breast-cancer-related- lymphedema”; ”lymphaticovenular bypass”; ”prophylaxis”; ”vascularized lymph node transplant”; “lymphovenous bypass”, in combination with AND or OR. A manual search of references was also conducted to identify any other potentially relevant additional studies. Inclusion criteria for manuscripts, used for full-text assessment and data extraction, were English-based original papers exclusively discussing PLS and, specifically, randomized clinical trials, retrospective comparative studies, retrospective case series of at least three patients and prospective studies. Studies addressing lymphatic mapping alone or single case reports were discarded. Prophylaxis was defined as therapeutic interventions directed towards the prevention of disease from occurring; hence, manuscripts discussing subjects with clinical or subclinical evidence of lymphedema were excluded.
Data extraction
Data extraction was performed by the same two independent reviewers (DP and FG) who reported the extracted data in a spreadsheet where all the relevant information was included. Any case of divergent opinions was solved either through consensus-based discussion or through the intervention of a third independent investigator (CR) and a majority-based vote. For all included studies, the following data was documented: type of study, year of publication, authors, number of patients, type of microsurgical technique, operating time, follow-up period, complications, presence of a control group, method of lymphedema diagnosis, lymphedema outcome, whether patients received adjuvant therapy and follow-up time. The Oxford Centre for Evidence-Based Medicine (OCEBM) and the JADAD scale were used to provide a critical appraisal of the level of evidence.
RESULTS
Study characteristic
A total of 5028 articles were identified in the Cochrane, Google scholar and Pubmed search.
After the removal of duplicates, the literature search retrieved 2698 studies, of which only 55 full-text papers were assessed for eligibility. Six abstracts, ten overviews, three systematic reviews, one meta-analysis and one case report were excluded, identifying 34 eligible full-text articles. After the full-text screening, an additional 16 articles were eliminated either because of population overlap, or due to the management of upper or lower lymphedema already diagnosed or because of no surgical prophylactic techniques. In the end, 18 studies were included (Figure 1).
An overview of each study is summarized in Table 1 and Table 2. Nine studies were observational cohort studies, five were case-control, two were randomized trials and two were case series.
The OCEBM level of evidence for the articles was as follows: eleven articles had a level of 4, five a level of 3 and two a level of 2. The JADAD level score was 5 for two articles, 4 for six articles, and 3 for ten articles.
Patient characteristics
The qualitative analysis comprised 911 patients who had received ALND for breast cancer treatment. Among the overall eighteen studies, eleven had no a control group, while seven had a control group. The eleven studies without a control group reported only 15 patients out of 327 who developed lymphedema (4.59%) after at least six months from PLS. Of these, eight had received radiotherapy exclusively, one had received adjuvant radiotherapy and neo-adjuvant chemotherapy and had a body mass index (BMI) of 38, one had received radiotherapy and had a concomitant axillary surgical site infection and seven had received neo-adjuvant chemotherapy and adjuvant radiotherapy [11,12,13,14,15].
The seven studies with a control group comprised 569 patients, of which 328 cases and 241 controls. Among the cases, 36 (10%) developed lymphedema. Those patients had either received adjuvant radiotherapy, had an increased number of positive nodes removed, or had been treated with adjuvant chemotherapy and radiotherapy and had a BMI > 40 [16,17,18,19].
Among the controls, instead, the rate of lymphedema was 40% (98 patients out of 241). All the lymphedemas diagnosed within the six months of their final oncologic treatment (chemotherapy, radiotherapy and surgery) were defined as transient and thus not taken into account. The follow-up period ranged from three to eighty-four months, during which, besides lymphedema, only one complication was registered: an infected axillary seroma treated with aspiration and intravenous antibiotics [12].
The methods used to detect lymphedema differed among studies. Fourteen studies applied circumferential arm measurements (CA) [12,13,14,15,18,19,20,21,22,23,24,25,26,27].
Four papers used volumetry (V) and calculated the relative volume change by dividing the pre-and post-operative difference by the preoperative value [11,16,17,28].
Estimated limb volume was calculated using the following formula: V = (d)(A2 + Aa + a2)/12(π), where “A” is the circumference measurement of the distal section, “a” is the circumference measurement of the proximal section, and “d” is the distance between the distal and the proximal section [29]. Nevertheless, seven studies also used, but not exclusively, bioimpedance spectroscopy (BS) [12,13,18,19,24,25,26,27].
Some works also used lymphoscintigraphy as a tool to diagnose lymphedema, in addition to other methods [11,15,20].
Only one study applied the Lymphedema Life Impact Score and/or Lymphedema Quality of Life Questionnaire carried out by a certified lymphedema therapist [25,30].
Almost all the studies performed LVA as primary prophylaxis isotopic to the lymphadenectomy procedure. Telescopic end-to-end anastomosis of several lymphatics inserted together into a single vein was reported in ten studies [11,14,15,16,17,18,20,21,24,27].
Two studies opted for super microsurgical LVA exclusively and two studies for a combination of both techniques [12,13,24,26].
Two studies used both an end-to-end LVA and a telescopic end-to-side technique of multiple lymphatics on the same vein [19,23].
Only one study performed multiple distal LVA between the proximal end of the vein and the distal end of the lymphatic duct, as a primary prophylaxis ectopic to the lymphadenectomy procedure [24].
One paper described autologous breast reconstruction using the deep inferior epigastric perforator (DIEP) flap and the lymphatic superficial circumflex iliac artery perforator (SCIP) flap procured separately from the Zone 4 region [28].
Another paper accounted for a vascularized serratus anterior fascia flap during concurrent latissimus dorsi flap harvest (for breast or chest wall reconstruction) [22]. In terms of feasibility, all techniques were reported highly feasible, with a pooled feasibility rate varying from 75% up to 100%.
DISCUSSION
Considering the high morbidity of ALND in breast cancer patients, several techniques attempting to reduce the lymphedema rate have been implemented over recent decades.
In 2007, Thompson and Nos described, in two different studies, the axillary reverse mapping (ARM) technique, demonstrating that arm and breast lymphatic drainages can be identified separately [31,32].
They proposed, a few minutes before proceeding with sentinel lymph node biopsy (SLNB) or ALND, the injection of a colorant (blue dye) into the upper arm to make visible during the dissection the lymphatics draining exclusively the arm, and not the breast, and preserve them. Thompson and Nos showed that their technique was feasible, with a detection rate of blue lymphatics of 61–71% and a preservation rate of 47%. Introducing ARM, the incidence of upper extremity lymphedema went from 33.4% to 4% [14,33,34,35].
Unfortunately, the ARM technique couldn’t guarantee an oncological radicality, since blue lymphnodes were considered part of the arm lymphatic pathway, and thus were not originally removed, not knowing if they were metastatic or not.
Another point of controversy was the removal of the lymphatics departing from the blue nodes when exiting the axillary basin and joining the common lymphatic pathway draining the breast. According to Boneti et al, their preservation was considered not safe in terms of oncological radicality [36].
Therefore, aiming to find a technique able to prevent secondary arm lymphedema and, at the same time, maintain the oncological radicality, Boccardo et al developed the lymphatic microsurgical preventing healing approach (LYMPHA) [19].
The microsurgical operation, also known as the “sleeve technique” consisted of a telescopic end-to-end anastomosis: blue lymphatics found at the lateral pillar of the axillary dissection (AD) after the blue dye injection were placed together into the vein with a U-shaped stitch. The lymphatics were then stabilized inside the vein with additional stitches between the vein border and the perilymphatic tissue. As a matter of fact, Boccardo implemented the ARM technique, not saving the blue nodes and the lymphatics coming from them, and adding the LYMPHA procedure, counting zero cases of lymphedema within 12 months in an 18 patient population [20].
After Boccardo et al, Casabona also applied the ARM and the LYMPHA technique reporting no cases of lymphedema in 8 patients in a 9-month follow-up [21].
In 2015, Boccardo extended the use of LYMPHA and ARM to 74 patients of which only 3 developed lymphedema within 48 months of follow-up (4%) [11].
An inferior rate was reported by Johnson: out of 32 patients treated, only 1 developed lymphedema (3.1%) within 12 months [14].
Applying the same procedure and in the same time frame, Cook registered a 9% rate of lymphedema (3 out of 33 patients) [15].
In their study, Scharwz et al tried to prevent lymphedema occurrence in 58 patients by applying an end-to-end micro anastomosis between a tributary of the lateral thoracic vein or the thoracodorsal vein and a single transected lymphatic, in the instance of its precise size match and availability [12].
When significant size discrepancy existed between lymphatic and recipient vein (1:3), or if there were multiple transected lymphatics in proximity to a recipient’s vein, they utilized the sleeve technique already described by Boccardo [20]. Unfortunately, the surgical procedure used for the two patients who developed lymphedema, reported in the study, was not registered, thus it was not possible to detect the more effective type of anastomosis.
In 2020, Shaffer et al applied the same scheme as Scharwz to 88 patients with a rate of lymphedema of 6% (5 out of 88) and also in this case it was not possible to detect the relation between the type of anastomosis and the onset of lymphedema [12,13].
In 2021, Chuan et al in three patients with locally advanced breast cancer, requiring mastectomy and axillary clearance, harvested a vascularized serratus anterior fascia flap during concurrent latissimus dorsi flap dissection (for breast or chest wall reconstruction) and then wrapped it around the axillary vessels [22].
In this way, they provided a conduit for lymphatic regeneration, protecting the axillary vessels from radiotherapy and reducing scarring and axillary cording. Within 48 months, none of them experienced upper limb lymphedema or cording.
A similar concept was applied by Yoshimatsu et al in 2022 [28].
They described a novel method in which the afferent lymphatic vessels were harvested with their lymph nodes from the Zone 4 region as a separate flap, the superficial circumflex iliac artery perforator (SCIP) flap, in the context of autologous breast reconstruction with the deep inferior epigastric artery perforator (DIEP) flap. Of the four patients who did not have lymphedema at the time of reconstruction, none developed it in a 48-month follow-up.
In 2022, Lipman et al applied the LYMPHA procedure to 19 patients using indistinctly end-to-end or end-to-side LVA, and having only one case of lymphedema in an average of 10 months follow-up period. Moreover, they reported about one patient who simultaneously underwent immediate breast reconstruction with an omental-free flap [23].
As a result, in this case, it may be difficult to determine the relative contributions of LYMPHA versus omental transfer on lymphedema prevention. In fact, in the intra-abdominal space, the omentum is known to serve a critical role in immune response and lymphatic drainage. Though the omental transfer for breast reconstruction did not involve the transfer of the gastric nodal basin or lymphovenous anastomosis of the efferent lymphatic that sometimes accompanies the gastroepiploic vessels, the omentum-associated lymph tissue (OALT) within the flap may have contributed partially to improve lymphatic drainage postoperatively [37].
Finally, in 2022, Pierazzi et al evaluated 5 patients who underwent prophylactic LVA distally to the axillary region and after the conclusion of adjuvant radiotherapy [24].
For each patient, the microsurgical technique was the same standard technique for the LVA procedure and four anastomoses were performed between the proximal end of a subdermal vein and the distal end of a lymphatic duct. None of them developed lymphedema within 12 months [38].
However, the real proof of the LYMPHA technique is manifest through case-control studies.
Two randomized case-control papers showed a rate of 30% (7/23) and 18.8% (9/48) respectively among patients who did not receive LVA, while it was 4% and 0% respectively among patients who received LVA [16,26].
All the other non-randomized case-control studies showed a rate even higher of lymphedema among controls, going from 8% (19) up to 68%, while among cases the rate of lymphedema was significantly lower, from 0% in Yoon’s study, up to 16% in Ozmen’s study. The follow-up rate period was 14.5 months on average [19,26,27].
The relation between the LVA shunting technique used and the rate of cases with lymphedema is worthy of note. The lowest rate appeared in Yoon’s study in which end-to-end LVA was performed on 21 patients with a lymphedema rate of 0% within 6 months of follow-up, while the highest rate appeared in Ozmen’s study, in which, among 110 patients treated with a simplified version of LYMPHA technique, 18 developed lymphedema within 84 months.
Despite the lower rate of lymphedema registered in all the mentioned papers, scepticism has emerged over the years on the cost incurred of an additional procedure that requires microsurgical expertise. To solve this controversy, in 2019 Johnson et al evaluated the cost-utility of a surgical procedure performed for the prevention of lymphedema in a patient population undergoing ALND or ALND with regional lymph node radiotherapy (RLNR) [39].
Their findings demonstrated that the addition of LYMPHA to ALND and ALND with RLNR was more cost-effective than ALND and ALND with RLNR alone, with favourable cost-utility ratios (ICURs) of $1587.73/quality-adjusted life years (QALY) and $699.48/QALY, respectively. The substantial clinical benefit of LYMPHA easily overcame the cost disadvantage, which is why ICUR in both scenarios had a relatively low amount per QALY. The huge bias of Johnson’s paper, though, was the exclusive analysis of the LYMPHA procedure at the time of ALND. As we have emphasized in this review, the LYMPHA technique is not the only option in the prophylactic surgical BCRL scenario [39].
Other surgical alternatives exist and the effectiveness of the ones performed at the time of ALND has yet to be proved. In fact, after ALND, patients might require RLNR, which per se represents an independent risk factor for lymphedema development [40,41,42].
No studies have been published yet regarding the safety of adjuvant radiotherapy on the long-term patency of anastomoses. In our review, though, we have registered more cases of lymphedema among the patients who received RLNR after prophylactic surgery, 15 patients out of 253 (5.93%) (Table 1 and Table 2).
Nowadays, Pierazzi et al (24) reported the only series in which LVA was performed distally to the irradiated area after axillary lymphadenectomy and after adjuvant radiotherapy, although this promising idea was previously described by Chen [24,43].
However, the five cases reported in their paper do not allow us to ensure a lower lymphedema rate, compared with all the other studies whose patients received adjuvant radiotherapy after PLS.
CONCLUSIONS
Low-quality studies with great heterogeneity, short follow-up periods, and variability among diagnostic modalities hamper the formulation of strong recommendations in favour of PLS.
Nonetheless, there is no consensus on which PLS technique should be considered preferable and it is not clear if adjuvant radiotherapy might hinder its effectiveness. For this reason and for its feasibility, delayed LVA might be considered a standard procedure for the primary prevention of BCRL. High-quality randomized controlled trials are mandatory to determine evidence-based recommendations.
REFERENCES
- Maclellan RA, Greene AK. Lymphedema. Semin Pediatr Surg. 2014;23(4):191-197. [CrossRef]
- Taghian NR, Miller CL, Jammallo LS, O'Toole J, Skolny MN. Lymphedema following breast cancer treatment and impact on quality of life: a review. Crit Rev Oncol Hematol. 2014;92(3):227-234. [CrossRef]
- Jørgensen MG, Toyserkani NM, Sørensen JA. The effect of prophylactic lymphovenous anastomosis and shunts for preventing cancer-related lymphedema: a systematic review and meta-analysis. Microsurgery. 2018;38(5):576-585. [CrossRef]
- Johnson AR, Kimball S, Epstein S, et al. Lymphedema Incidence After Axillary Lymph Node Dissection: Quantifying the Impact of Radiation and the Lymphatic Microsurgical Preventive Healing Approach. Ann Plast Surg. 2019;82(4S Suppl 3): S234-S241. [CrossRef]
- Stuiver MM, ten Tusscher MR, Agasi-Idenburg CS, Lucas C, Aaronson NK, Bossuyt PM. Conservative interventions for preventing clinically detectable upper-limb lymphoedema in patients who are at risk of developing lymphoedema after breast cancer therapy. Cochrane Database Syst Rev. 2015;(2):CD009765. Published 2015 Feb 13. [CrossRef]
- Badger C, Preston N, Seers K, Mortimer P. Physical therapies for reducing and controlling lymphoedema of the limbs. Cochrane Database Syst Rev. 2004;(4):CD003141. Published 2004 Oct 18. [CrossRef]
- Markkula SP, Leung N, Allen VB, Furniss D. Surgical interventions for the prevention or treatment of lymphoedema after breast cancer treatment. Cochrane Database Syst Rev. 2019;2(2):CD011433. Published 2019 Feb 19. [CrossRef]
- Granzow JW, Soderberg JM, Kaji AH, Dauphine C. Review of current surgical treatments for lymphedema. Ann Surg Oncol. 2014;21(4):1195-1201. [CrossRef]
- Kung TA, Champaneria MC, Maki JH, Neligan PC. Current Concepts in the Surgical Management of Lymphedema. Plast Reconstr Surg. 2017;139(4):1003e-1013e. [CrossRef]
- Campisi CC, Ryan M, Boccardo F, Campisi C. LyMPHA and the prevention of lymphatic injuries: a rationale for early microsurgical intervention. J Reconstr Microsurg. 2014;30(1):71-72. [CrossRef]
- Boccardo F, Casabona F, De Cian F, et al. Lymphatic microsurgical preventing healing approach (LYMPHA) for primary surgical prevention of breast cancer-related lymphedema: over 4 years follow-up [published correction appears in Microsurgery. 2015 Jan;35(1):83. DeCian, Franco [corrected to De Cian, Franco]. Microsurgery. [CrossRef]
- Schwarz GS, Grobmyer SR, Djohan RS, et al. Axillary reverse mapping and lymphaticovenous bypass: Lymphedema prevention through enhanced lymphatic visualization and restoration of flow. J Surg Oncol. 2019;120(2):160-167. [CrossRef]
- Shaffer K, Cakmakoglu C, Schwarz GS, et al. Lymphedema Prevention Surgery: Improved Operating Efficiency Over Time. Ann Surg Oncol. 2020;27(12):4695-4701. [CrossRef]
- Johnson AR, Fleishman A, Granoff MD, et al. Evaluating the Impact of Immediate Lymphatic Reconstruction for the Surgical Prevention of Lymphedema. Plast Reconstr Surg. 2021;147(3):373e-381e. [CrossRef]
- Cook JA, Sasor SE, Loewenstein SN, et al. Immediate Lymphatic Reconstruction after Axillary Lymphadenectomy: A Single-Institution Early Experience. Ann Surg Oncol. 2021;28(3):1381-1387. [CrossRef]
- Boccardo FM, Casabona F, Friedman D, et al. Surgical prevention of arm lymphedema after breast cancer treatment. Ann Surg Oncol. 2011;18(9):2500-2505. [CrossRef]
- Feldman S, Bansil H, Ascherman J, et al. Single Institution Experience with Lymphatic Microsurgical Preventive Healing Approach (LYMPHA) for the Primary Prevention of Lymphedema. Ann Surg Oncol. 2015;22(10):3296-3301. [CrossRef]
- Herremans KM, Cribbin MP, Riner AN, et al. Five-Year Breast Surgeon Experience in LYMPHA at Time of ALND for Treatment of Clinical T1-4N1-3M0 Breast Cancer. Ann Surg Oncol. 2021;28(10):5775-5787. [CrossRef]
- Weinstein B, Le NK, Robertson E, et al. Reverse Lymphatic Mapping and Immediate Microsurgical Lymphatic Reconstruction Reduces Early Risk of Breast Cancer-Related Lymphedema. Plast Reconstr Surg. 2022;149(5):1061-1069. [CrossRef]
- Boccardo F, Casabona F, De Cian F, et al. Lymphedema microsurgical preventive healing approach: a new technique for primary prevention of arm lymphedema after mastectomy. Ann Surg Oncol. 2009;16(3):703-708. [CrossRef]
- Casabona F, Bogliolo S, Valenzano Menada M, Sala P, Villa G, Ferrero S. Feasibility of axillary reverse mapping during sentinel lymph node biopsy in breast cancer patients. Ann Surg Oncol. 2009;16(9):2459-2463. [CrossRef]
- Han Ang C, Wong M. Incorporation of the Vascularized Serratus Fascia Flap during Latissimus Dorsi Flap Harvest to Minimize Morbidity after Axillary Clearance. Journal of Plastic and Reconstructive Surgery 2022; 1(2):58-62. [CrossRef]
- Lipman K, Luan A, Stone K, Wapnir I, Karin M, Nguyen D. Lymphatic Microsurgical Preventive Healing Approach (LYMPHA) for Lymphedema Prevention after Axillary Lymph Node Dissection-A Single Institution Experience and Feasibility of Technique. J Clin Med. 2021;11(1):92. Published 2021 Dec 24. [CrossRef]
- Pierazzi DM, Arleo S, Faini G. Distally Prophylactic Lymphaticovenular Anastomoses after Axillary or Inguinal Complete Lymph Node Dissection Followed by Radiotherapy: A Case Series. Medicina (Kaunas). 2022;58(2):207. Published 2022 Jan 29. [CrossRef]
- Hahamoff M, Gupta N, Munoz D, et al. A Lymphedema Surveillance Program for Breast Cancer Patients Reveals the Promise of Surgical Prevention. J Surg Res. 2019;244:604-611. [CrossRef]
- Yoon JA, Lee HS, Lee JW, Kim JH. Six-Month Follow-up for Investigating the Effect of Prophylactic Lymphovenous Anastomosis on the Prevention of Breast Cancer-Related Lymphedema: A Preliminary Study in a Single Institution. Archives of Hand and Microsurgery. 2021;26(4):276-84. [CrossRef]
- Ozmen T, Layton C, Friedman-Eldar O, et al. Evaluation of Simplified Lymphatic Microsurgical Preventing Healing Approach (SLYMPHA) for the prevention of breast cancer-related lymphedema after axillary lymph node dissection using bioimpedance spectroscopy. Eur J Surg Oncol. 2022;48(8):1713-1717. [CrossRef]
- Yoshimatsu H, Karakawa R, Fuse Y, Yano T. Simultaneous Lymphatic Superficial Circumflex Iliac Artery Perforator Flap Transfer from the Zone 4 Region in Autologous Breast Reconstruction Using the Deep Inferior Epigastric Artery Perforator Flap: A Proof-of-Concept Study. J Clin Med. 2022;11(3):534. [CrossRef]
- Casley-Smith JR. Measuring and representing peripheral oedema and its alterations. Lymphology. 1994;27(2):56-70.
- Kleinhans E, Baumeister RG, Hahn D, Siuda S, Büll U, Moser E. Evaluation of transport kinetics in lymphoscintigraphy: follow-up study in patients with transplanted lymphatic vessels. Eur J Nucl Med. 1985;10(7-8):349-352. [CrossRef]
- Thompson M, Korourian S, Henry-Tillman R, et al. Axillary reverse mapping (ARM): a new concept to identify and enhance lymphatic preservation. Ann Surg Oncol. 2007;14(6):1890-1895. [CrossRef]
- Nos C, Lesieur B, Clough KB, Lecuru F. Blue dye injection in the arm in order to conserve the lymphatic drainage of the arm in breast cancer patients requiring an axillary dissection. Ann Surg Oncol. 2007;14(9):2490-2496. [CrossRef]
- Ochoa D, Korourian S, Boneti C, Adkins L, Badgwell B, Klimberg VS. Axillary reverse mapping: five-year experience. Surgery. 2014;156(5):1261-1268. [CrossRef]
- Tummel E, Ochoa D, Korourian S, et al. Does Axillary Reverse Mapping Prevent Lymphedema After Lymphadenectomy?. Ann Surg. 2017;265(5):987-992. [CrossRef]
- Yue T, Zhuang D, Zhou P, et al. A Prospective Study to Assess the Feasibility of Axillary Reverse Mapping and Evaluate Its Effect on Preventing Lymphedema in Breast Cancer Patients. Clin Breast Cancer. 2015;15(4):301-306. [CrossRef]
- Boneti C, Korourian S, Bland K, et al. Axillary reverse mapping: mapping and preserving arm lymphatics may be important in preventing lymphedema during sentinel lymph node biopsy. J Am Coll Surg. 2008;206(5):1038-1044. [CrossRef]
- Shimotsuma M, Shields JW, Simpson-Morgan MW, et al. Morpho-physiological function and role of omental milky spots as omentum-associated lymphoid tissue (OALT) in the peritoneal cavity. Lymphology. 1993;26(2):90-101.
- Chen WF. How to Get Started Performing Supermicrosurgical Lymphaticovenular Anastomosis to Treat Lymphedema. Ann Plast Surg. 2018;81(6S Suppl 1):S15-S20. [CrossRef]
- Johnson AR, Asban A, Granoff MD, et al. Is Immediate Lymphatic Reconstruction Cost-effective?. Ann Surg. 2021;274(6):e581-e588. [CrossRef]
- Fu MR. Breast cancer-related lymphedema: Symptoms, diagnosis, risk reduction, and management. World J Clin Oncol. 2014;5(3):241-247. [CrossRef]
- DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 2013;14(6):500-515. [CrossRef]
- Basta MN, Wu LC, Kanchwala SK, et al. Reliable prediction of postmastectomy lymphedema: The Risk Assessment Tool Evaluating Lymphedema. Am J Surg. 2017;213(6):1125-1133.e1. [CrossRef]
- Chen WF, Knackstedt R. Delayed Distally Based Prophylactic Lymphaticovenular Anastomosis: Improved Functionality, Feasibility, and Oncologic Safety?. J Reconstr Microsurg. 2020;36(9):e1-e2. [CrossRef]
Figure 1.
PRISMA flow chart.
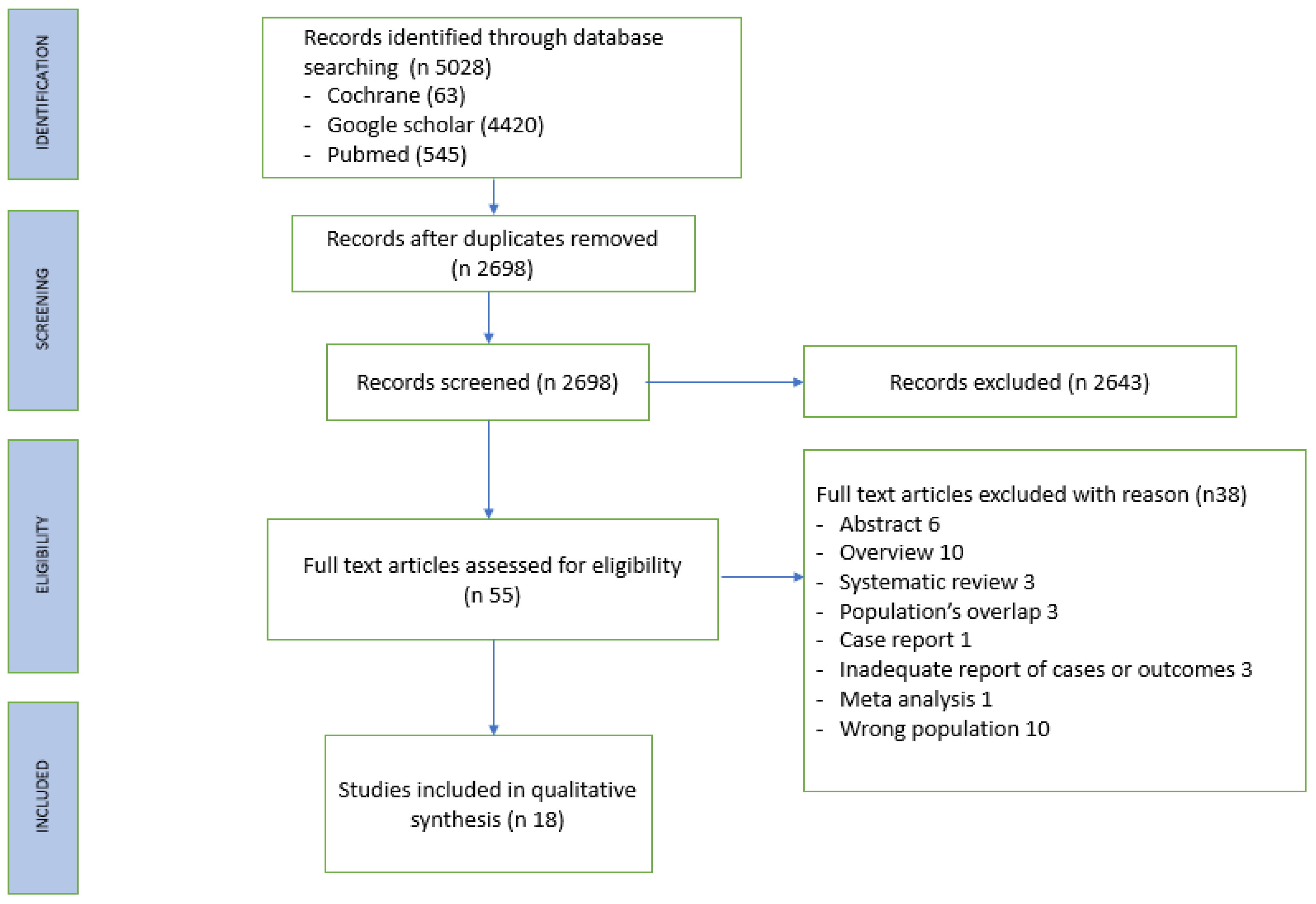

Table 1.
Studies with a control group.
| Article | Adjuvant therapy | LVA shunting technique | LVA feasibility | Follow-up (months) | Operating time (minutes) | Method of lymphedema diagnosis | Cases with lymphedema | Controls with lymphedema | Cases with lymphedema who received adjuvant radiotherapy | OCEBM and JADAD |
|---|---|---|---|---|---|---|---|---|---|---|
| Boccardo 2011 | Cases: RT (11/23) Controls: RT (12/23) |
Sleeve | 23/23 | 18 | 15-20 | V | 1/23 (4%) | 7/23 (30%) | 1/1 | 2 and 5 |
| Feldman 2015 | Cases: RT (15/24), CT (23/24) Controls: RT (6/8), CT (7/8) |
Sleeve | 24/32 | From 3 to 24 | 45 | V | 3/24 (13%) | 4/8 (50%) | 3/3 | 3 and 3 |
| Hahamoff 2019 | Cases: RT (8/8),neoCT (5/8), adCT (4/8); Controls: RT (6/10), neoCT (4/10), adCT (4/10) |
Sleeve | 8/8 | From 15 to 20 | From 32 to 95 | CA, BS | 0/8 (0%) | 4/10 (40%) | 0/0 | 3 and 3 |
| Herremans 2021 | Cases: RT (67/76), CT (58/76), neoCT (36/76) Controls: RT (50/56), CT (42/56), neoCT (20/56) |
Sleeve | 76/84 | 60 | nr | CA, BS, LQOLQ | 10/76 (13.2%) | 16/56 (28.6%) | nr | 3 and 4 |
| Yoon 2021 | Cases: RT (17/21), CT (16/21); Controls: RT (36/48), CT (38/48) |
ETE LVA | 21/21 | 6 | From 30 to 60 | CA, BS | 0/21 (0%) | 9/48 (18.8%) | 0/0 | 2 and 5 |
| Ozmen 2022 | Cases: RT (89/110); Controls: RT (68/84) |
Sleeve | Nr | From 10 to 84 | nr | CA, BS | 18/110 (16%) | 57/84 (68%) | nr | 3 and 4 |
| Weinstein 2022 | Cases: RT (46/66), neoCT (56/66) adCT (26/66); Controls: RT (8/12), neoCT (8/12), adCT (8/12) | ETE or ETS LVA | Nr | 8 on average | nr | CA, BS | 4/66 (6%) | 1/12 (8%) | 3/4 | 3 and 4 |
RT: radiotherapy, adRT: adjuvant radiotherapy, CT: chemotherapy, neoCT: neoadjuvant chemotherapy, adCT: adjuvant chemotherapy, ETE LVA: end-to-end lymphatic-venous anastomosis, ETS LVA: end-to-side lymphatic-venous-anastomosis, nr: not reported, V: volumetry, CA: circumferential arm measurements, BS: bioimpedance spectrometry, LQOLQ: Lymphedema Quality of Life Questionnaire,.
Table 2.
Studies without a control group.
| Article | Adjuvant therapy | LVA shunting technique | LVA feasibility | Follow-up (months) | Operating time (minutes) | Method of lymphedema diagnosis | Cases with lymphedema | Cases with lymphedema who received adjuvant radiotherapy | OCEBM and JADAD |
|---|---|---|---|---|---|---|---|---|---|
| Boccardo 2009 | RT (7/18) | Sleeve | 18/19 (95%) | 12 | 15 | CA, LS | 0/18 (0%) | 0/0 | 4 and 3 |
| Casabona | RT (8/8), CT (0/8) | Sleeve | 8/9 (89%) | 9 | 17 | CA | 0/8 (0%) | 0/0 | 4 and 3 |
| Boccardo 2014 | RT (35/74) | Sleeve | 74/78(95%) | 48 | 48 | V, LS | 3/74(4%) | 3/3 | 4 and 3 |
| Johnson 2019 | RT (26/32), CT (19/32) | Sleeve | nr | 12 | nr | CA, BS | 1/32 (3.1%) | 1/32 | 4 and 4 |
| Scharwz 2019 | RT (52/58), neoCT (43/58), adCT (10/58) | 37/58 ETE LVA, 21/58 sleeve | 58/60 (97%) | 29 | 95 | CA, BS | 2/43 (4.6%) | 2/2 | 4 and 3 |
| Cook 2020 | RT (22/33), neoCT (24/33) | Sleeve | 33/33 (100%) | 12 | nr | CA, LS | 3/33(9%) | 3/3 | 4 and 4 |
| Shaffer 2020 | RT (82/88), neoCT (61/88), adCT (20/88), neo + adCT (1/88) | ETE LVA or sleeve | 88/88 (100%) | 14.6 on average | From 161 to 253 | CA, BS | 5/88(6%) | 4/5 | 4 and 4 |
| Chuan 2021 | RT (3/3), neo CT (2/3) | Vascularized serratus anterior fascia flap | nr | 48 | nr | CA | 0/3(0%) | 0/0 | 4 and 3 |
| Lipman 2022 | RT (16/19) | ETE or ETS LVA | nr | 10 on average | From 32 to 95 | CA,BS | 1/19(5%) | nr | 4 and 3 |
| Pierazzi 2022 | RT (5/5) | DLVA | 5/5 (100%) | 12 | nr | CA | 0/5(0%) | 0/0 | 4 and 3 |
| Yoshimatsu 2022 | RT (2/4) | SCIP flap with DIEP | 4/4 (100%) | From 24 to 48 | nr | V | 0/4(0%) | 0/0 | 4 and 3 |
RT: radiotherapy, adRT: adjuvant radiotherapy, CT: chemotherapy, neoCT: neoadjuvant chemotherapy, adCT: adjuvant chemotherapy, ETE LVA: end-to-end lymphatic-venous anastomosis, ETS LVA: end-to-side lymphatic-venous-anastomosis, DLVA: distal lymphatic-venous anastomosis, nr: not reported, V: volumetry, CA: circumferential arm measurements, BS: bioimpedance spectrometry, LQOLQ: Lymphedema Quality of Life Questionnaire.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



