
Submitted:
14 December 2023
Posted:
15 December 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The official recommendations to manage COVID-19 in the outpatient setting focus on high-cost drugs (remdesivir, nirmatrelvir-ritonavir, molnupiravir), suffering from many problems.
Therefore, one may consider also other treatments meeting these criteria:
• promising effectiveness, based on favorable randomized controlled trials (RCTs) of sufficient validity. Even without definitive evidence, physicians and informed patients can consider them if they are also:
• safe, to the state of knowledge
• with a very favorable opportunity cost
• biologically plausible/not implausible
• accessible
• without major commercial sponsors in the trials promoting them, and with researchers without major conflicts of interests.
The main focus is on a limited group of functional foods and some their active ingredients, with further mention of other substances of different origin, yet fully meeting all the aforementioned criteria.
The functional foods and substances described and discussed certainly do not cover all the known effective therapies for COVID-19 (in one case also for Long-COVID), but the only therapies proposed in this paper currently satisfy all the above criteria.
The supporting scientific evidence will favor meta-analyses of RCTs that include the most definitive outcome: all-cause mortality, i.e. the outcome that most fully informed people tend to prioritize. Furthermore, the reported evidence favors clinical studies of the most valid design, i.e. RCTs.
Keywords:
EB functional foods in COVID-19 early therapy
; EB active ingredients of foods in COVID-19 therapy
; EB active substance in Long-COVID-19 therapy
; EB active substance for Post-COVID sequelae.
1. Introduction
1.1. Current gaps and problems
Strategies to manage COVID-19, mainly in the outpatient setting, evolve as new data emerge about newer treatments. However, the official recommendations (e.g., by World Health Organization/WHO [1], or by American College of Physicians [2]) are chiefly focused on high-cost drugs, as remdesivir, but only for patients with high risk of hospitalization [1], or as nirmatrelvir-ritonavir and molnupiravir [1,2], to be taken within 5 days of the onset of symptoms and only by people at risk of progressing to severe disease.
Anyway, these drugs have several problems in addition to the very high cost. In particular, as regards remdesivir, the difficult and inconvenient administration, making it unsuitable for home therapy. As regards molnupiravir, the web site of European Medicine Agency (EMA) [3] reported that, on 21 June 2023, Merck Sharp & Dohme (MSD) withdrew its application for a marketing authorisation concerning this drug (Lagevrio) for the treatment of COVID-19 in adults. MSD stated that its decision was based on the view of the Committee for Medicinal Products for Human Use (CHMP) of EMA, that the data provided by MSD itself do not allow to conclude on a positive benefit-risk balance for Lagevrio. Indeed, based on the totality of data, CHMP was unable to conclude that Lagevrio either can reduce the risk of hospitalisation or death or shorten the duration of illness or time to recovery in adults at risk of severe disease. Furthermore, it was not possible to identify a specific group of patients for whom a clinically relevant benefit of Lagevrio had been demonstrated.
As regards nirmatrelvir-ritonavir, in addition to the numerous pharmacological interactions limiting its use [4], there are also other problems. E.g., its effectiveness was lowered during the Omicron surge [5]: it remained significant against hospitalization and death due to Covid-19 among patients 65 years of age or older, but no evidence of benefit was found in younger adults of 40 to 64 years [5], neither versus hospitalization among patients with previous immunity (Adjusted Hazard Ratio 1.13; 95% CI, 0.50 to 2.58), nor versus death due to Covid-19 (AHR 1.32; 95% CI, 0.16 to 10.75). It showed also a high virologic rebound: in a recent large cohort study [6,7], more than 1 in 5 people taking nirmatrelvir-ritonavir had a rebound, often without symptom, but associated with shedding of replication-competent viruses. Even the hypothesized effectiveness of nirmatrelvir-ritonavir against the development of Post-COVID-19 conditions (PCCs) was questioned, because it seems to reduce only combined thromboembolic events out of 31 potential PCCs [8] in a target trial emulation in US Veterans (82.5% vaccinated).
Highly specific monoclonal antibodies showed initial clinical trials evidence, soon becoming no longer applicable to covid-19 caused by the SARS-CoV-2 variants and subvariants that are currently circulating globally [1].
So, it is also useful to take into account less specific treatments, with potentially more durable and affordable effectiveness.
1.2. Materials and Methods - Inclusion criteria for proposed therapies
The products or active substances addressed by this paper expand the range of COVID-19 remedies, effective also in the home setting. Of course, after having discussed them with one own’s physician.
Such products or active substances have been chosen and included according the following criteria:
- very promising effectiveness, based on favorable randomized controlled trials (RCTs) of sufficient validity,* complemented by consistent observational studies, available on the major databases of biomedical literature. Even if the evidence is not definitive, attending physicians and informed patients can consider them to the extent that they are at the same time also:
- safe (primum non nocere!), to the state of knowledge
- affordable, with a very favorable opportunity cost, allowing resources to be saved for other valuable healthcare uses
- biologically plausible (or at least not clearly implausible)
- accessible (or capable of quickly granting accessibility)
- without major commercial sponsors in the trials promoting them, and realized by researchers without major conflicts of interests.

The main focus is on a limited group of functional foods and related active substances, with mention also of other substances of different origin, yet fully meeting all the aforementioned criteria, including also a product with valid evidence of efficacy against long-COVID
(but also by closing the list with a negative didactic example, of an active ingredient among the most used and recommended worldwide, although it does not meet five of the six aforementioned golden criteria).
The substances that will be described and discussed in this review manuscript certainly do not cover all the known effective therapies against COVID-19 (including those approved or pending approval), but the only therapies proposed in this paper are those that currently satisfy all the above criteria.
Among the treated substances, the paper set a special focus on functional foods and on some of their active ingredients.
The supporting scientific evidence will favor meta-analyses of clinical trials that include the most definitive of outcomes, all-cause mortality. This is also the outcome that most fully informed people tend to prioritize. Furthermore, the scientific evidence reported will favor clinical studies of the most valid design, i.e., randomized controlled trials, as already specified in the inclusion criteria.
* Note that some cited references come from preprint articles. When there is also a good number of RCTs with favorable results on a substance, the choice was not to exclude preprint articles adding consistent information on the topic. It should be noted that there are also reasons other than the quality of scientific information why major biomedical journals do not publish or heavily delay the publication of some articles. There is an ongoing debate on this topic, and some authors with very high H Indexes have chosen to publish elsewere their scientific production [9].
2. Curcumin
Curcumin is a polyphenolic compound derived from the rhizomes of turmeric (Curcuma Longa). Its spices’ yellow pigment has shown anti-inflammatory, antioxidant, immune modulating and anti-viral properties [10,11]. Its antiviral activity was observed against multiple viruses including hepatitis viruses, influenza viruses and arboviruses like the Zika or chikungunya virus; it has also been reported to inhibit human immunodeficiency virus, herpes simplex virus 2 and human papillomavirus [12]. Curcumin also favors fibrinolysis [13].
Both a systematic review and dose–response meta-analysis [14] and an umbrella meta-analysis [15] of randomized clinical trials (on nearly 6,000 participants) have suggested that turmeric/curcumin supplementation may be useful for improving inflammatory/oxidative status, and that curcumin is a promising agent in reducing inflammation as an adjunctive therapy in diseases with a high level of infammatory biomarkers. Indeed, curcumin supplementation significantly decreased levels of C-reactive protein (CRP), interleukin 6 (IL-6), and tumour necrosis factor α (TNF-α) levels.
A problem may be caused by the low bioavailability of traditional forms of curcumin and turmeric, first of all related to their poor solubility [16], requiring bio-enhancers like piperine to considerably improve its absorption. RCTs has successfully used a dosage of about 500 mg or curcumin with piperine (2,5 mg) twice a day (e.g., [17]). Another substance substantially increasing the absorption of curcumin after oral administration is bromelain, isolated from the pineapple stem [13], in turn accredited with anti-inflammatory, fibrinolytic and anticoagulant properties, but affecting the absorption rate of several medications, potentially leading to drug interactions.
Both curcumin and bromelain might also inhibit viral entry into cells, with possible multiple synergistic actions. The absorption of curcumin is also favored by nano or liposomal formulations, available as over-the-counter oral supplements.
Curcumin has shown high safety and tolerability in clinical trials, even at high doses [18]; its potential adverse effects include diarrhea, headache, rash, and yellow stool, but no serious adverse effects have been reported to date [19]. 500 mg twice a day has shown
to be a safe and common dosage regardless of curcumin type [20].
Given that curcumin is about 10% in weight of curcuma, and that piperine is about 5%-8% in weight of black pepper, a home made dosage could consider (in agreement with one’s doctor) about 5 grams of curcuma with 1-2 well-chewed black peppercorns twice a day.
A real time analysis of COVID-19 early (and late) treatments [21] shows for curcumin the following mortality results, all coming from single o double blind randomized controlled trials (RCTs)(Figure 1):
Note the consistency of the results of all the RCTs. They are not large, but some have a highly valid design (double blind), with very good results both in early and in advanced treatment phases.
Moreover, Figure 2 shows all the curcumin RCTs in COVID-19, studying several other outcomes in addition to mortality (hospitalization, ventilation, numbers of recovery or recovery time, progression of the disease, oxigen saturation, viral positivity, in both early and late treatments):
Interestingly, curcumin has offered antiinflammatory and prophylactic benefits also in healthy individuals with a history of prior COVID-19 infection who received the COVID-19 vaccine [41].
3. Nigella Sativa (Black Seed)
Nigella (N.) sativa, also known as black seed or black cumin seed, is a food spice with a medicinal value, with several active compounds, including thymoquinone and a radical scavenging property. The safety profile of thymoquinone has been documented in clinical trials (e.g., one in asthmatic patients [42]). A systematic review of RCTs that used N. sativa showed no serious adverse effects on hepatic and renal function [43]. Several preclinical and clinical studies have documented the antiviral activities of N. sativa against several viruses [44]. Some N. sativa compounds demonstrated potential inhibition of coronavirus replication in in silico models [45]. In several studies N. sativa has shown immunostimulant effects through the induction of multiple cellular mediators and immune responses to eradicate infections [45]. In studies on inflammatory conditions, N. sativa L. has demonstrated anti-inflammatory and immunomodulatory activities, reducing pro-inflammatory mediators [46]. It has also analgesic and antipyretic properties [47].
A real time analysis of COVID-19 early (and late) treatments [21] shows for nigella sativa the following mortality results, all coming from RCTs (Figure 3).
Figure 4 shows all the nigella sativa RCTs in COVID-19, studying several other outcomes in addition to mortality (hospitalization, recovery, cases/viral positivity, symptomatic cases, both in early and in late treatments):
However, only in one case the RCT is double blind, and the quality of some black seed trials is poor.
Doses of N. Sativa typically used in the RCTs have been 0.5 g twice daily of black seed oil for about two weeks, or 2-5 g of black seed, about 40 mg per kilogram of weight.
4. Quercetin
Quercetin is a plant flavonol, of the flavonoid class of phenolic compounds, with potent antioxidant activity, studied for its immunomodulatory and immune-boosting properties. It has been approved by the US Food and Drug Administration as GRAS (Generally Recognized As Safe) for use as an ingredient at levels up to 500 mg per serving.
Important sources of quercetin, approximately expressed in mg per 100 g of each food, are: capers (200 mg); lovage (levisticum) leaves (170); eidelberry (sambucus) juice concentrate (110 mg); dill weed (anethum), fresh (55 mg); cilantro (coriandrum), fresh (55 mg); banana peppers (50 mg); juniper berries (50); onions (40 mg); radicchio and read leaf lettuce (30 mg); asparagus, kale, okra, bee pollen, cocoa powder, apples skin, chia seeds (20-25 mg).
Quercetin, like other flavonoids, reduces the production of pro-inflammatory mediators (Bhaskar, 57), promotes the relaxation of cardiovascular muscles, and neuroprotection (Khan, 58). Moreover, quercetin protects against both non-communicable diseases as cancer, coronary heart disease, atherosclerosis and hypercholesterolemia, rheumatic diseases, and infections thanks to its antioxidant properties and the regulation of cellular homeostasis (Batiha 59). It may benefit people with comorbidities like hypertension, diabetes mellitus, obesity, chronic obstructive pulmonary disease, coagulopathy and cytokine storm, all associated with COVID-19 seriousness (60 Xu). Quercetin also have shown a strong association with reduction in frailty onset in the 12 years follow-up of a prospective cohort study of individuals from the Framingham Heart Study without frailty at baseline (61). Every 10 mg/d of higher quercetin intake was associated with 35% lower odds of frailty onset (OR: 0.65; 95% CI: 0.48–0.88).
Antibacterial and antiviral activity of Quercetin has been known for decades [62].
In in vitro studies quercetin has inhibited the replication of various respiratory viruses, among which influenza virus [63], and severe acute respiratory syndrome (SARS) viruses [64]. This suggested possible clinical efficacy in COVID-19 [65,66,67,68].
A systematic review and meta-analysis of quercetin for COVID-19 patients [69] have found that quercetin significantly decreased the risk of intensive care unit admission (OR = 0.31; 95% confidence interval (CI) 0.10–0.99) and the incidence of hospitalisation (OR = 0.25; 95% CI 0.10–0.62), but did not [significantly] decrease the risk of all-cause mortality (OR 0.39; 0.10 to 1.54) and the rate of no recovery (0.55; 0.28 to 1.07). However, one should consider that even for these outcomes the tendency is in the direction of a benefit. The Authors [69] conclude: “Quercetin may
be of benefit in COVID-19 patients, especially if administered in its phytosome formulation which greatly enhances its bioavailability, but large-scale RCTs are needed to confirm these findings”.
The already cited real time analysis of COVID-19 early (and late) treatments [21] shows for quercetin the following mortality results, all coming from single blind RCTs (Figure 5):
Figure 6 shows all the quercetin RCTs in COVID-19, studying several other outcomes in addition to mortality (hospitalization, recovery, cases/viral positivity, symptomatic cases, both in early and in late treatments):
5. L-arginine
L-arginine is an amino acid that participates in the formation of almost all proteins. It is a semi-essential amino acid, i.e., produced by the body but also taken in from the outside with food (nuts, especially pine nuts, seeds, legumes…). It is a substrate for endothelial nitric oxide synthase, a key enzyme in endothelial cells [77,78], and it showed to significantly improve the endothelial function. It stimulates the synthesis of glutathione, thus preventing oxidative stress. L-arginine also showed beneficial effects on the regulation of immune responses [79].
Preclinical and clinical evidence shows that the endothelium is a target organ in COVID-19, explaining many of its systemic manifestations. In severe COVID-19 decreased plasma levels of L-arginine, and more arginase activity [80,81] have been reported.
L-arginine has beneficial effects on the endothelial function [78]. Therefore, in a double-blind RCT [82] on patients hospitalized for COVID-19 requiring oxigen support, after a mean of 7.8 days since the symptoms onset the standard therapy was supplemented with oral vials containing 1.66 g of L-arginine, twice a day (48 patients), or with an identical placebo (53 patients). The dose was the same as that used in a study in which this regimen was safe and effective in improving the oxidative metabolism in sportsmen [83]. The adherence was 100%.
The primary outcome of the reduction in respiratory support was significantly reached 10 days after randomization in the L-arginine group, but the result was no longer significant at 20 days (however, nearly twice the participants in the L-arginine group were already discharged at 20 days, and in hospital there remained only the sicker patients of their group). Indeed, the time to hospital discharge was significantly shorter with L-arginine (25 days) than with placebo (46 days), even in a fully adjusted multivariable analysis. Moreover, in the per protocol analysis 3 patients (6.7%) died in the placebo arm, vs no deaths in the L-arginine arm; in the intention to treat analysis the placebo group had 20.8% deaths, L-arginine 6.3%; p = 0.035.
Three serious adverse events were reported in the placebo arm and 1 in the L-arginine arm, though the investigators considered them unrelated to the study treatment.
It is noteworthy that L-arginine had no significant effect in the time to negativization of RT-PCR for SARS-CoV-2 on nasopharyngeal swab. This suggests that L-arginine acts improving the endothelial function, not against virus replication, which affects the negativization of RT-PCR for SARS-CoV-2. The COVID-19 pathogenesis includes first a viral injury, then an inflammatory immune response, which could culminate in a disfunctional hyperinflammation, leading to endothelitis, thromboembolism, and intravascular coagulation. L-arginine depletion has shown to increase the production of reactive oxygen species and to exaggerate the inflammatory response [84].
The promising results of this RCT indicate that L-arginine added to standard therapy in patients with severe COVID-19 can significantly improve their late treatment, leading to the conjecture of its possible use to treat Long-COVID symptoms.
5.1. Long-COVID treatment
Long COVID, also known as Post COVID-19 condition (PCC), or post-acute sequelae of SARS-CoV-2 infection (PASC), is the continuation or development of new symptoms in the period after acute infection with SARS-CoV-2. The World Health Organization (WHO) definition of PCC [85] states that these symptoms should be present three months after the initial SARS-CoV-2 infection and last for at least two months with no other explanation.
COVID-19 affects both the epithelial cells of the lung, and the endothelial cells in the whole body, causing a generalized endothelial damage.
Endothelial dysfunction, caused by the viral infection or by the resulting high inflammation, can increase permeabilization, tissue edema, possibly leading to thromboembolism. Endothelial dysfunction may affect smokers and subjects with hypertension, obesity, diabetes and cardiovascular disease, notoriously more prone to adverse outcomes in COVID-19. The favorable interim results of the RCT testing oral supplementation of L-arginine in COVID-19 hospitalized patients [82] led to the survey LINCOLN [86]. The aim was to verify wether L-arginine and Vitamin C could improve Long-COVID symptoms, administering a questionnaire to 1390 patients, with these inclusion criteria: COVID-19 diagnosis confirmed by RT-qPCR; its negativization confirmed by RT-qPCR from at least 4 weeks; COVID-19 sequelae extended more than four weeks after initial infection. The first group (521 patients) included patients who had received 2 vials/day of L-arginine 1.66 g associated with 500 mg of liposomal Vitamin C. The second group (alternative treatment) had been treated with a multivitamin combination of B Vitamins. At the questionnaire administration, both groups had already completed 30 days of treatment. The investigators asked to physicians administering the survey to maintain about a 2:1 ratio (L-Arginine + Vitamin C vs alternative treatment); therefore, they were not blinded. The physicians assessed 10 typical Long-COVID symptoms on a scale from 1 to 3 (1 means absence of the symptom, 2 presence of a mild symptom, 3 presence of a severe symptom). The results, shown in Table 1, were excellent:
A prospective study has demonstrated that endothelial dysfunction in COVID-19 patients remains significantly impaired compared to healthy controls even at a 6-month follow-up [87]. Circulating endothelial cells, probably detached from the vessels, correlate with the severity of COVID-19 outcome [88]. The non-respiratory symptoms of Long-COVID are strongly correlated to persistent endothelial dysfunction [89]. An already cited research demonstrated that reduced levels of L-arginine increase the generation of reactive oxigen species (ROS), worsening inflammation [84]. L-arginine level showed an inverse correlation with platelet activation [90], contributing to COVID-19 thromboembolic events.
Until the end of 2022, no research of valid design (RCT) had been published in the biomedical literature on a medicine capable of treating the symptoms of Long-COVID. The above survey stimulated the execution of a single-blind RCT on Long-COVID adult patients with persistent fatigue, attending a post-acute COVID-19 outpatient clinic [91].
The participants were randomized either to an oral combination of vials containing 1.66 g L-arginine plus 500 mg liposomal vitamin C twice-daily, or to an indistinguishable placebo for four weeks. Primary outcome: the distance paced on the 6 min walk test. Secondary outcomes: handgrip strength, fatigue persistence, flow-mediated dilation. 23 participants per group received the intervention and completed the study.
Results at 28 days showed significant improvement in 6 min walk distance (intervention +30 m, vs. placebo +0; p = 0.001), handgrip strength (+3.4 kg vs. +1 kg; p = 0.03), flow-mediated dilation (14.3% vs. 9.4%; p = 0.03). Above all, it reduced fatigue, reported only by two participants (8.7%) in the L-arginine vs 21 (80.1%) in the placebo group (p < 0.0001).
A systematic critical assessment [92] of the current evidence for the
management of long COVID rated “moderated evidence” for important benefits only for respiratory training for respiratory symptoms. The Authors cite a Living Systematic Review of Therapeutic Options for Post COVID-19 Condition [93]; last subsequent publication in August 2023], rating L-arginine + Vitamin C among some therapeutic options for PCC-related asthenia or fatigue, with a disappointing summary of findings: “Uncertainty in potential benefits and harms. Further research is needed”, similar to the findings regarding Coenzime Q10, which really showed unsatisfactory results in a well conducted RCT [94].
However, as regards to L-arginine, I disagree, for the following reasons:
- it is true that the RCT [91] is not double blind, has only 4 weeks of follow-up and it is very small, with the possibility that a larger RCT would not confirm its excellent results, however
- one does not see valid reasons to speak of “uncertainty about potential harms”, which the trial’s results do not allow to hypothesize, even more so given that the active ingredients are introduced daily even with a healthy diet, albeit at doses lower than those effectively administered in the RCT. Moreover, the review [93] states “Adverse events and Severe adverse events: No information”, but this is not true, because the Authors [91] report that “L-arginine plus vitamin C supplementation was safe and well tolerated, and no adverse events were recorded”; even more so because the retention was complete in both groups
- the problem of Long-COVID is widespread and socially very relevant, and currently lacks therapeutic options confirmed by valid research
- the product used in the RCT [91] still satisfies all the “Inclusion criteria for proposed therapies”, and, although awaiting more definitive research, there are good reasons to inform doctors and to offer it to patients with persistent COVID-19 sequelae.
Furthermore, it is plausible that the results of this research [91], suggesting important benefits of a safe molecule such as L-arginine on endothelial disfunction, will also stimulate similar research in other pathologies where endothelial disfunction is believed to have an important pathogenetic role.
6. Povidone-iodine (and other antiseptics for local use)
The SARS-CoV-2 virus is usually transmitted in the air and settles in the nose (and in the pharynx, and/or in the ocular mucosa), and multiplies for days before it invades the body. The virus can be killed in those locations, and in any case the viral load can be significantly reduced with early targeted local interventions. Some studies have suggested that mouthwash and/or gargling with povidone-iodine (PVP–I) may have an antiseptic effect for SARS-CoV-2, reducing its viral load [95].
PVP-I is a water-soluble iodine compound that has long been used as a skin antiseptic and mouthwash. After free iodine dissociates from polyvinylpyrrolidone, it quickly enters microorganisms and destroys them by disrupting proteins and oxidizing nucleic acid structures [95]. No germ resists it or develops resistance to it.
PVP–I has previously been shown to have an antiseptic effect on SARS-CoV and MERS in vitro [96,97], and it was also effective against SARS-CoV-2 [98]. A single in vitro gargle with PVP–I reduced the salivary viral load in patients with a high salivary viral load [99].
It is now one of the most studied antiseptics against SARS-CoV-2, with overall excellent results.
The repeatedly cited living real-time analysis of over 3,500 studies [21] reports only two studies with mortality results for PVP-I: one is a retrospective observational study, with good results in late treatment [100]; the other is a rather large RCT, in early treatment, with excellent results [101], published in 2021.
Figure 7.
Random effects meta-analysis for RCTs with mortality results about povidone-iodine in COVID-19 [100,101].
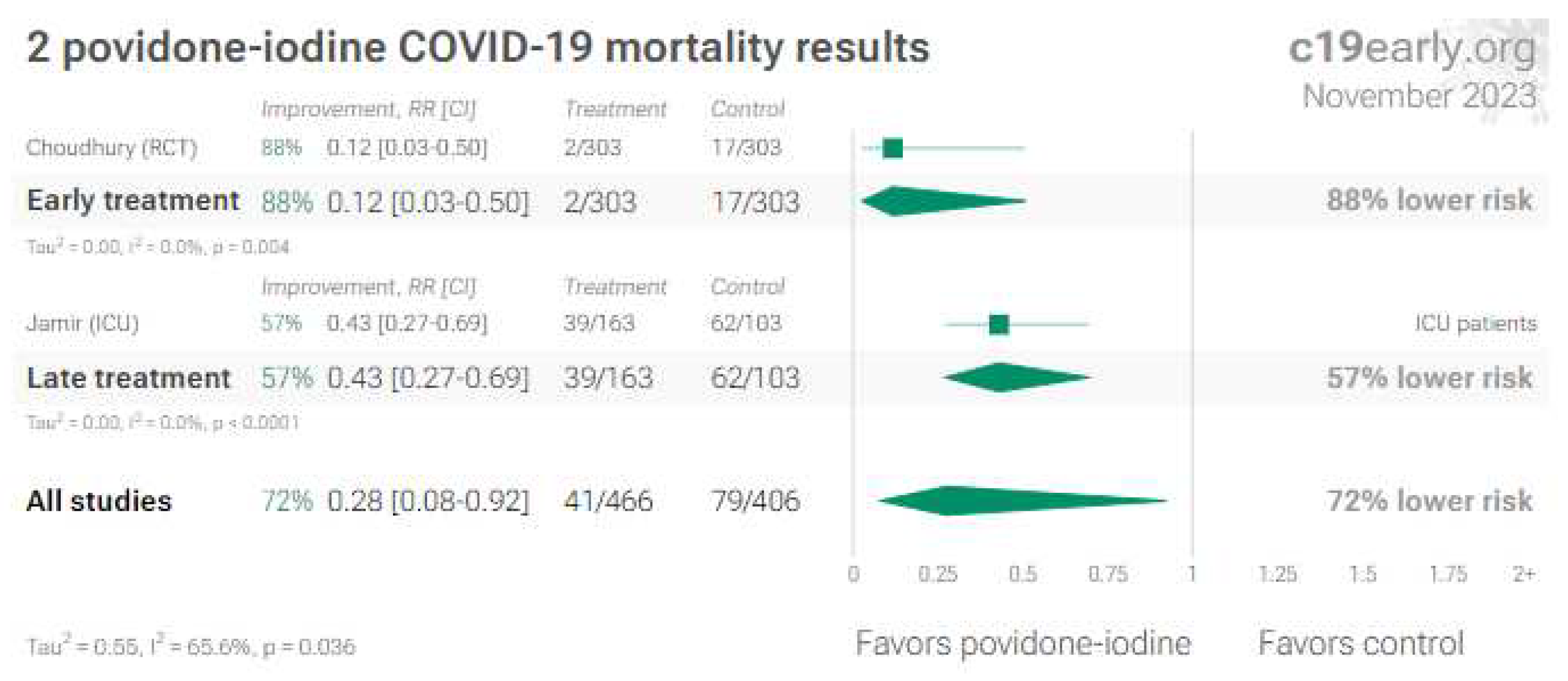
In the Choudhury’s RCT [101] in Bangladesh, 606 COVID-19 middle class patients were enrolled and randomized in 2 groups after taken consents. About 40% of patients were in the 31-50 years age group, and 35% in the 51-70 years age group. The treatment was taken at home.
The 303 patients in the experimental group underwent mouthwash/gargle, nasal drops and eye drops with 1% PVP-I every four hours for 4 weeks (but now we know that about ten days/two weeks can be more than enough for the large majority of patients) as well as symptomatic treatment according to need. In the control group, 303 patients were advised to do mouthwash/gargle, nasal cavity and eye wash with lukewarm water 4 hourly for 4 weeks and symptomatic treatment according to need. In Bangladesh 10% PVP-I was found all over the country, but 1% commercially available PVP-I was found only in a few cities. Most of the 1% PVP-I was formed from 10% PVP-I, diluting 1 mL of it in 10mL of purified water. The instructions were to introduce 1% PVP-I as mouth wash, distributing the solution throughout the oral cavity for 30 seconds and then gently gargled, or holding at the back of the throat for another 30 seconds before spitting out. Then 4-5 drops of 1% PVP-I were introduced to wash the nostrils by dropper and 2 drops in each eye. This application was done every 4 hours for 4 weeks. The same instructions were given for the control group, but with lukewarm water.
RT-PCR test was done every 3rd, 5th and 7th day and thyroid hormone level (TSH, T3, T4, FT4) was measured at 4th week for follow up, but excluding patients with thyroid diseases.
Results: on the 7th day only 2.64% (N. 8) of PVP-I patients were RT-PCR positive, whereas in the control group 70.30% (N. 213) were RT-PCR positive (p>0.05). Only 3.30% (N. 10) hospitalized patients of group A needed oxygen support (by mechanical ventilator and/or high flow nasal cannula and/or non rebreather mask and/or face mask and/or nasal cannula). On the contrary, 20.79% (N. 63) patients of group B needed oxygen support. Mortality rate was high 5.6% (N. 17) in the control group, and only 0.66% (N. 2) in PVP-I group (P<0.05) [101].
Therefore, the PVP-I group has dramatically reduced mortality, morbidity and hospitalization, as well as financial burden. Indeed, nose has the highest expression of ACE2, the main receptor of COVID-19 virus. Local use of PVP-I 1% as drops in the nostrils, in the eyes, and as mouth wash/gargling showed to be a simple, rapid and cost effective treatment in reducing mortality and morbidity by COVID-19.
The fact that an RCT like this has not been replicated since then, and that this extremely effective, economical, affordable, convenient and safe treatment has not been disseminated worldwide suggests the weight and influences of commercial interests in health strategies and policies.
Figure 8 shows all the povidone-iodine RCTs in COVID-19, studying several other outcomes in addition to mortality (hospitalization, recovery, viral positivity, viral load, symptomatic cases, both in early and in late treatments):
6.1. Nose/oropharyngeal treatments
Under this denomination the living real-time analysis c19early.org [21] lists other products in addition to PVP-I: alkalinization (with sodium bicarbonate, saline irrigation…), chlorhexidine, hydrogen peroxide, iota-carrageenan, and some others. The results are consistently good.
At least one systematic review and meta-analysis comparing PVP-I and chlorhexidine (CHX) deserves mention here [118]. It included 10 studies concerning 1,339 patients with COVID-19. Compared with the control group, both CHX and PVP-I reduced significantly the viral load in the COVID-19 patients. In subgroup analysis, compared with the control group, CHX had a pooled medium-to-large effect size of 0.69 (95% CI=0.02–1.37; p=0.04) for reducing the viral load, without evidence of heterogeneity across the studies (I2=0.00). Similarly, the pooled effect size of PVP-I was 0.66 (95%
CI=0.04–1.27; p=0.04) for decreasing the viral load, without evidence of heterogeneity across the studies (I2=0.00). PPVP-I was safe, and it does not cause tooth or tongue discoloration or taste disturbance. CHX can have adverse effects if used for 4 weeks or longer. Specifically, CHX mouthwash causes brown discoloration on the surface of the teeth which may be removed by a dental expert after scaling and polishing. CHX mouthwash causes no or minimal discoloration after 1 or 2 weeks of treatment, but may have taste disruption and mouth lining pain, albeit temporary and reversible after use has ceased. Therefore, both CHX and PVD-I seem similarly effective, but for longer time usage PVP-I seems to be safer.
Finally, early alkalization interventions (nasal irrigation and gargle and spit with sodium bicarbonate or simple saltwater) also deserve mention, for their effectiveness, simplicity, safety, cost-effectiveness and affordability.
Figure 9.
Random effects meta-analysis for RCTs with mortality results about alkalinization in COVID-19 [119,120,121,122,123].
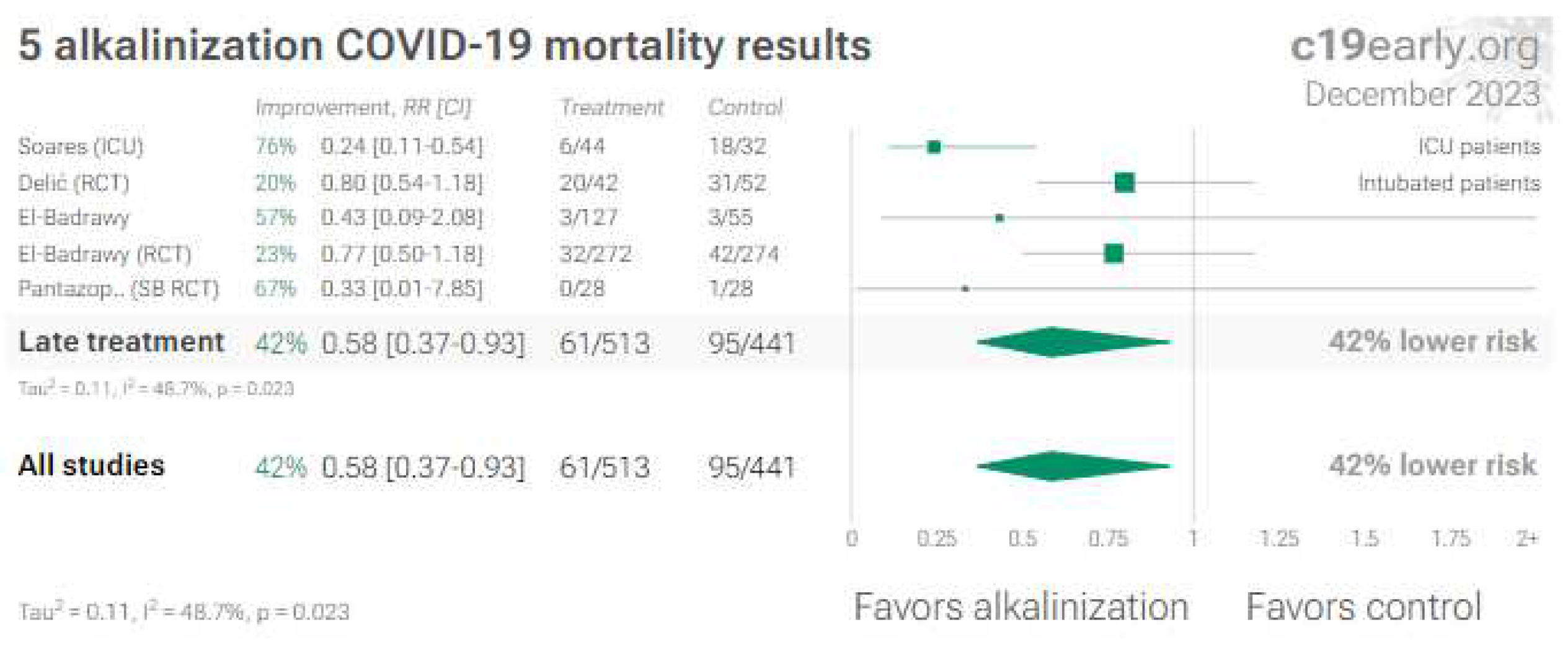
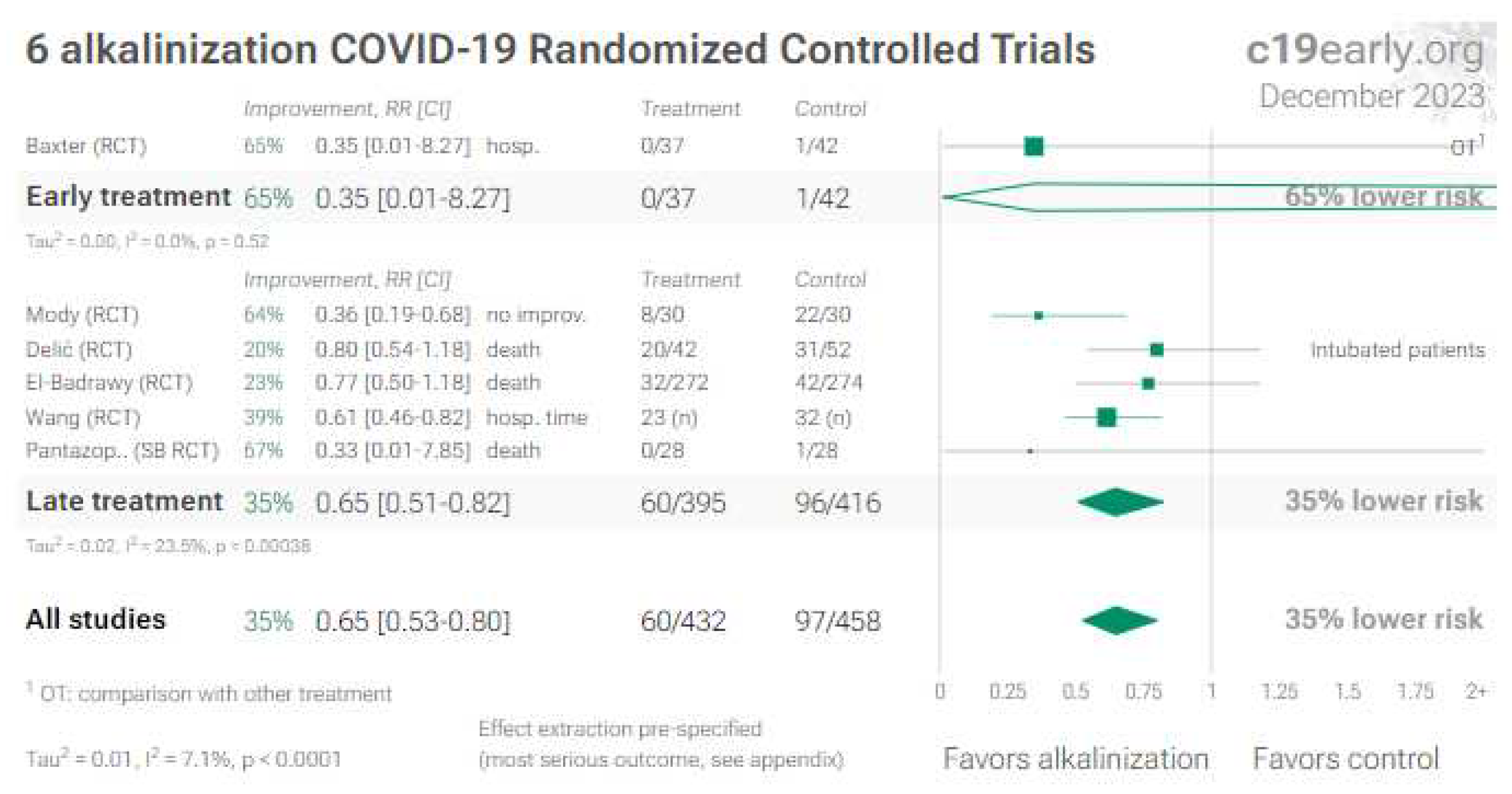
Figure 10.
Random effects meta-analysis for all RCTs about alkalinization in COVID-19 [119,120,121,122,123,124,125,126]. This plot shows pooled effects, see the specific outcome analyses for individual outcomes, and the heterogeneity section [21] for discussion. Effect extraction is pre-specified, using the most serious outcome reported. For details of effect extraction see the appendix [21].
Figure 10.
Random effects meta-analysis for all RCTs about alkalinization in COVID-19 [119,120,121,122,123,124,125,126]. This plot shows pooled effects, see the specific outcome analyses for individual outcomes, and the heterogeneity section [21] for discussion. Effect extraction is pre-specified, using the most serious outcome reported. For details of effect extraction see the appendix [21].
Topical nasal rinses acts in multiple ways [127]. First, they physically disrupt the viscous surface layer, removing the mucus and its associated particulate matter.
Additionally, nasal saline helps to increase hydration of the deeper aqueous layer, simultaneously improving the underlying ciliary beat frequency and reducing local inflammatory mediators. This can be particularly helpful during a viral respiratory infection, in which there is resultant mucociliary dysfunction and mucostasis, secondary to the inflammatory response.
The benefit of topical nasal saline has been well established, but the optimal saline tonicity level is less clear. Isotonic saline (IS) consists of a 0.9% wt/vol sodium chloride solution, close to the physiologic salt concentration of the body; hypertonic saline (HS) solutions are greater than 0.9% wt/vol. There is supportive evidence for both IS and HS efficacy in vivo [128]. It has been theorized that HS, having higher osmolarity, pulls water out of cells resulting in increased hydration of the aqueous portion of the mucus layer, improving mucociliary clearance and also decreasing epithelial edema. Indeed, a meta-analysis evaluating both IS and HS rinses for all sinonasal diseases concluded that HS, with a sodium chloride concentration of less than 5%, was more beneficial than IS for the management of sinonasal pathology. Moreover, a RCT evaluating HS in the common cold has given evidence of reduction duration of illness, over-the-counter medication use, transmission to household members, and viral shedding [129].
However, performing irrigations of the nasal cavities require hygienic precautions, because they may increase viral shedding and transmission. There is some concern about viral contamination of the nasal rinse bottle itself, with transmission through contact-induced infections. Viral contamination of surfaces may occur via rinsing: for instance rhinovirus was detected in nasal lavage [127].
7. Melatonin
Melatonin is an endocrine molecule secreted by the pineal gland. It is also synthesized in mitochondria throughout the body, in greater quantity. Melatonin has a well-known role in sleep and circadian rhythm regulation, but it is also an anti-inflammatory, anti-oxidant, and immunomodulatory agent [130]. It is alsto a cost-effective anti-viral with minor side effects, which makes it a potential adjuvant in the COVID-19 treatment ([131].
Many studies have highlighted the link between COVID-19 severity and cytokine storm, that causes excessive production of reactive oxygen species (ROS), leading to the over-activation of neutrophils, which produce myeloperoxidase (MPO). Melatonin is both a potent ROS scavenger and a potent MPO inhibitor, and this is one of the possible mechanisms by which melatonin can cure COVID-19 [132].
A systematic review of the clinical studies on melatonin’s effects in COVID-19 patients [133] included 5 RCTs, 3 clinical trials (CTs) and 2 Cohort studies comparing the effect of melatonin in the treatment of COVID-19 with the standard of care therapy in patients older than 18. Both cohort studies were of good quality, while the others, although in theory of even more valid design, were of inferior quality, except for a good RCT [134] in patients with severe COVID-19, assessed at “low risk of bias”. In this RCT, in the melatonin group 1 of 82 patients died (1.2%), while in the control group 13 of 76 patients died (17.1%), P-value 0.000, with significant differences also in thrombosis (11% vs 23.7%) and sepsis (8.5% vs 35.5%).
The Authors’ of the systematic review [133] concluded that studies “demonstrate that melatonin supplementation at a dosage of 3–10 mg/day (or 2 mg of prolonged release in an Italian trial [135]) is associated with an improvement in clinical outcomes in COVID-19 patients”. Moreover “melatonin could be a potential adjuvant in the treatment of COVID-19 patients if administered for two weeks and can possibly help to reduce recovery time, mortality rate, and the likelihood of coagulopathy disorder or sepsis. Furthermore, it can improve patient outcomes during intubation.”. Anyway, more high-quality randomized clinical trials are needed.
The cited living real-time analysis of over 3,500 studies [21] reports the following tables:
Figure 11.
Random effects meta-analysis for RCTs with mortality results about melatonin in COVID-19 [133,134,135,136,137,138,139,140,141].
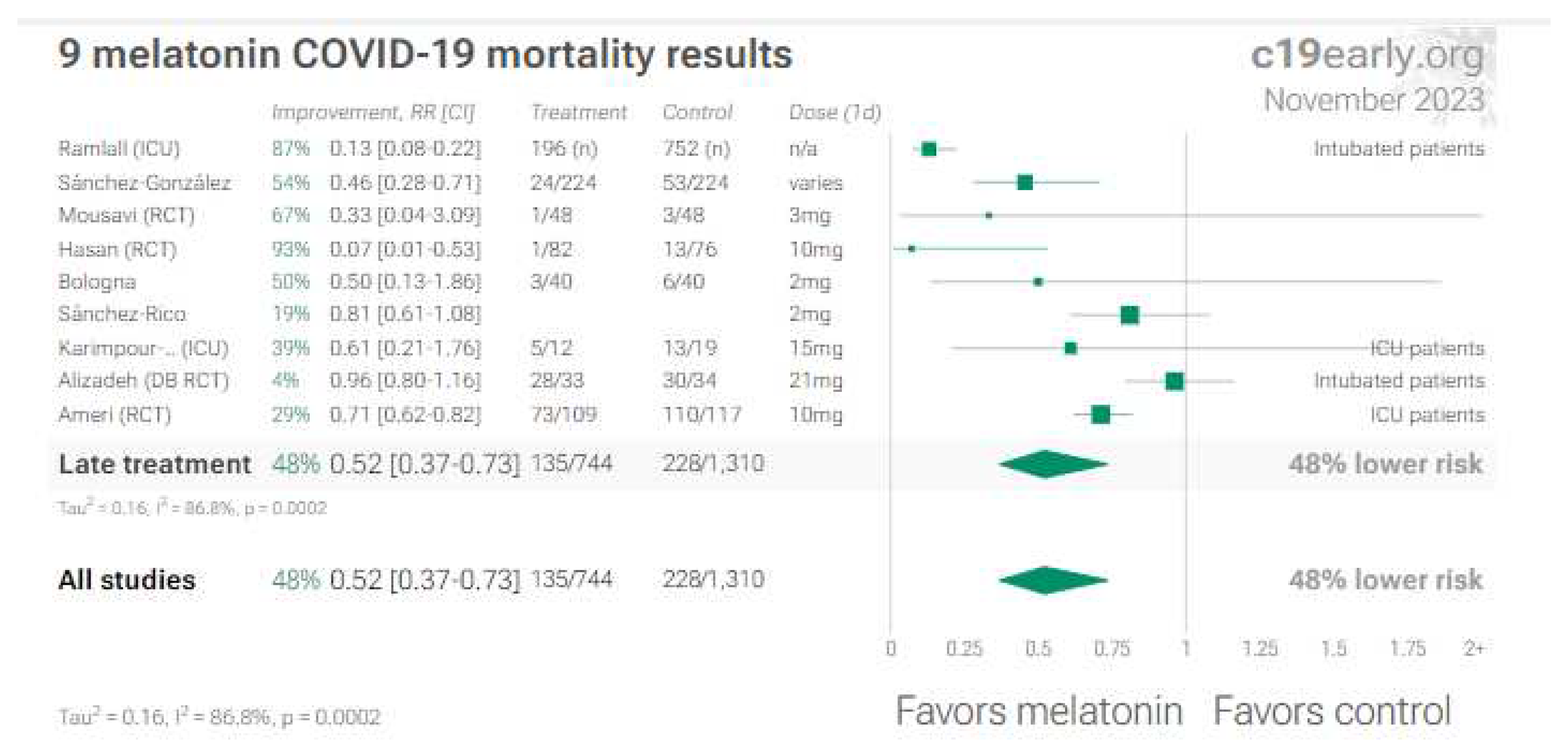
Figure 12 shows all the melatonin RCTs in COVID-19, studying several other outcomes in addition to mortality (hospitalization, recovery, symptomatic cases, progression, ICU, both in early and in late treatments):
8. Discussion
A frequent criticism of RCTs like those supporting the substances proposed in this article is that (even with valid study designs) they are small RCTs, often not double-blinded and even open-label, that is with less guarantees of avoiding confounding factors, etc. Therefore, the evidence would never be definitive, and other large confirmatory RCTs would be needed... before such substances could be recommended.
Two considerations must be made.
First, what is stated in the previous paragraph is true... except the last six words. Indeed, when the effectiveness of a therapy is not yet conclusive, it should not be recommended if: it has safety issues, and/or a high opportunity cost, and/or it is biologically implausible, and/or unaffordable, and/or it is promoted by commercial sponsors and investigators with relevant conflicts of interest, making their proposal less credible. On the contrary, a therapy can be offered legitimately if it is at the same time: safe, as far as it is known, with a favorable opportunity cost, biologically plausible, accessible and without big commercial sponsors or researchers with relevant conflicts of interest. And, above all, if there are no more effective alternatives with most of the same characteristics.
Second, is the same strictness about the absence of conclusive evidence of effectiveness always applied by the Health Authorities? The answer is no.
The teaching example of paracetamol is telling.
8.1. Acetaminophen (Paracetamol): a negative didactic example
The World Health Organization (WHO) updated November 10, 2023, its guidelines on treatments for COVID-19 [147]: “For people at low risk of hospitalization, WHO does not recommend any antiviral therapy. Symptoms like fever and pain can continue to be managed with analgesics like paracetamol.”
The European Medicine Agency (EMA) March 18, 2020 [148] wrote: “When initiating treatment for fever or pain during COVID-19 illness, patients and healthcare professionals should consider all available treatment options, including acetaminophen and NSAIDs (Nonsteroidal Antinflammatory Drugs). Each medicine has its own benefits and risks as described in the product information and which need to be taken into consideration alongside European guidelines, many of which recommend paracetamol as a first-line treatment option for fever and pain.”.
The Italian Drug Agency (Agenzia Italiana del Farmaco/AIFA) in its “Recommendations on drugs for home management of COVID-19”, Update 10/03/2023 [149], states: “Paracetamol or NSAIDs can be used in case of fever or joints or muscles pain (unless there is a clear contraindication to use)”.
Accordingly, the Italian Ministry of Health still recommend paracetamol, which appears 13 times among the 50 best-selling OTC drugs in Italy, and it occupies the 1st and 3rd position in this list [150]. This proves that, although the paracetamol is not expensive, the size of sales represents an important business for the big drug manufacturers (worldwide).
Unfortunately, there is no valid evidence of efficacy or safety for paracetamol in COVID-19. The repeatedly cited living real-time analysis of over 3,500 studies [21] reports the following Figure, showing that paracetamol has lost all comparisons, for any outcome:
Potential mechanisms of harm of paracetamol are highlighted in the box in Figure 13.
One mechanism is the induction of oxidative stress and of glutathione depletion [178], leading to damage of several organs, notably liver and lungs.
Another mechanism is even paradoxical: the insistently pursued suppression of fever, one of the best universal defenses against infections [179]. Indeed, it can slow or inhibit the replication of practically all viruses, including the latest Omicron variants [180], favoring recovery.
Moreover, paracetamol is not as safe as it is thought [181], and it is associated with incident hypertension, cardiovascular and even gastrointestinal [182] adverse events, liver damage, possible acute poisoning and fatal overdoses (with a rather narrow therapeutic window).
All considered, it is clear that recommending a drug with the risks of paracetamol during infections cannot rationally be reconciled with strict preclusions towards the very promising substances described in the chapters 2 to 7.
9. Conclusions
The official recommendations to manage COVID-19 in the outpatient setting focus on high-cost drugs, with many defects and limitations.
Therefore, one could also consider treatments meeting criteria of promising effectiveness, based on favorable RCTs of sufficient validity, safety, very favorable opportunity costs, biological plausibility, accessibility, without major commercial sponsors financially tied with the trials’ principal investigators.
A small group of functional foods and/or some of their active ingredients meet all these criteria (curcuma/curcumin, quercetin, nigella sativa/black seed; and L-arginine, this one with evidence of efficacy also against Long-COVID); besides, some other substances, among which povidone-iodine (and other local antiseptics) and melatonin deserve special consideration.
10. Future Directions
To confirm the effectiveness and safety of the highly promising substances and functional foods discussed in this paper, larger pragmatic RCTs are needed, double blind as far as possible, and with researchers independent of commercial conflicts of interest.
For treatment of the post-acute sequelae of COVID-19 (and of COVID vaccinations) much pre-clinical and clinical research is still needed, again culminating with large pragmatic confirmative RCTs.
Funding
Fondazione Allineare Sanità e Salute (Align Healthcare and Health Foundation).
Informed Consent Statement
Not applicable.
Data Availability Statement
Many data come from the living site c19early.org, expressly allowing free use of all its materials, with citation of the source.
Acknowledgments
the site c19early.org, allowing free use of all its materials (https://c19early.org/faq.html --> “Can we use your graphs? Yes. You can use any of our work free of charge.”). Moreover, the Author is grateful to his assistant Chiara Giove, for the support in bibliographic research and the drafting of the references.
Conflicts of Interest
The Author declares no conflict of interest.
References
- Agarwal, A.; Hunt, B.; Stegemann, M.; et al. A living WHO guideline on drugs for covid-19. BMJ. 2020 Sep 4;370:m3379. Update in: BMJ. 2020 Nov 19;371:m4475. Update in: BMJ. 2021 Mar 31;372:n860. Update in: BMJ. 2021 Jul 6;374:n1703. Update in: BMJ. 2021 Sep 23;374:n2219. Erratum in: BMJ. 2022 Apr 25;377:o1045. [CrossRef]
- Qaseem, A.; Yost, J.; Miller, M.C.; et al. Outpatient Treatment of Confirmed COVID-19: Living, Rapid Practice Points From the American College of Physicians (Version 1). Ann Intern Med. 2023 Jan;176(1):115-124. Epub 2022 Nov 29. Erratum in: Ann Intern Med. 2023 May;176(5):735-736. [CrossRef]
- Lagevrio: Withdrawn application | European Medicines Agency (europa.eu).
- Liverpool COVID-19 Interactions (covid19-druginteractions.org).
- Arbel, R.; Wolff Sagy, Y.; Hoshen, M.; et al. Nirmatrelvir Use and Severe Covid-19 Outcomes during the Omicron Surge. New Engl J Med 2022; 387:790-798. [CrossRef]
- Edelstein, G.E.; Boucau, J.; Uddin, R.; et al. SARS-CoV-2 Virologic Rebound With Nirmatrelvir–Ritonavir Therapy: An Observational Study. Ann Intern Med. [Epub 14 November 2023]. [CrossRef]
- Cohen, M.S.; Brown, E.R. Rebound of COVID-19 With Nirmatrelvir–Ritonavir Antiviral Therapy. Ann Intern Med. [Epub 14 November 2023]. [CrossRef]
- Ioannou, G.N.; Berry, K.; Rajeevan, N.; Li, Y.; Mutalik, P.; Yan, L.; Bui, D; Cunningham, F.; Hynes, D.M.; Rowneki, M.; et al. Effectiveness of Nirmatrelvir–Ritonavir Against the Development of Post–COVID-19 Conditions Among U.S. Veterans. Ann Intern Med. 2023;176(11):1486-1497. [CrossRef]
- Gøtzsche, P.C. Why some of us no longer want to publish in prestigious medical journals. Nov 14, 2023. 2023-Gotsche-Why-some-of-us-no-longer-want-to-publish-in-prestigious-medical-journals.docx (live.com).
- Prasad, S.; Tyagi, A.K.; Aggarwal, B.B. Recent Developments in Delivery, Bioavailability, Absorption and Metabolism of Curcumin: The Golden Pigment from Golden Spice. Cancer Res. Treat. 2014, 46, 2–18. [Google Scholar] [CrossRef]
- Kunnumakkara, A.B.; Bordoloi, D.; Padmavathi, G.; Monisha, J.; Roy, N.K.; Prasad, S.; Aggarwal, B.B. Curcumin, the golden nutraceutical: Multitargeting for multiple chronic diseases. Br. J. Pharmacol 2017, 174, 1325–1348. [Google Scholar] [CrossRef]
- Praditya D, Kirchhoff L, Brüning J, Rachmawati H, Steinmann J, Steinmann E: Anti-infective properties of 2023 Hulscher et al. Cureus 15(11): e49204. DOI 10.7759/cureus.49204 11 of 12 the golden spice curcumin. Front Microbiol. 2019, 10:912. [CrossRef]
- Karampela, I.; Kokoris, S.; Dalamaga, M. The combination of bromelain and curcumin as an immune-boosting nutraceutical in the prevention of severe COVID-19. Metabol Open. 2020 Dec;8:100066. [CrossRef]
- Dehzad, M.J.; Ghalandari, H.; Nouri, M.; Askarpour, M. Antioxidant and anti-inflammatory effects of curcumin/turmeric supplementation in adults: A GRADE-assessed systematic review and dose–response meta-analysis of randomized controlled trials. Cytokine 2023, 164, 156144. [Google Scholar] [CrossRef]
- Naghsh, N.; Musazadeh, V.; Nikpayam, O.; Kavyani, Z.; Moridpour, A.H.; Golandam, F.; Faghfouri, A.H.; Ostadrahimi, A. Profiling Inflammatory Biomarkers following Curcumin Supplementation: An Umbrella Meta-Analysis of Randomized Clinical Trials. Evid.-Based Complement. Altern. Med 2023, 2023, 4875636. [Google Scholar] [CrossRef]
- Anand, P.; Kunnumakkara, A.B.; Newman, R.A.; Aggarwal, B.B. Bioavailability of curcumin: Problems and promises. Mol. Pharm 2007, 4, 807–818. [Google Scholar] [CrossRef]
- Pawar K.S., Mastud R.N., Pawar S.K., et al. Oral Curcumin With Piperine as Adjuvant Therapy for the Treatment of COVID-19: A Randomized Clinical Trial. Frontiers in Pharmacology. 2021. https://www.frontiersin.org/articles/10.3389/fphar.2021.669362/full. [CrossRef]
- Thimmulappa, R.K.; Mudnakudu-Nagaraju, K.K.; Shivamallu, C.; Subramaniam, K.; Radhakrishnan, A.; Bhojraj, S.; Kuppusamy, G. Antiviral and immunomodulatory activity of curcumin: A case for prophylactic therapy for COVID-19. Heliyon 2021, 7, e06350. [Google Scholar] [CrossRef]
- Abdelazeem, B.; Ahmed, K. Awad, A.K.; Elbadawy, M.A.; Manasrah, N.; Malik, B.; Yousaf, A.; Alqasem, S.; Banour, S.; Abdelmohsen, S.M. The effects of curcumin as dietary supplement for patients with COVID-19: A systematic review of randomized clinical trials. Drug Discoveries & Therapeutics. 2022; 16(1):14-22. [CrossRef]
- Hegde M; Girisa, S.; BharathwajChetty, B.; Vishwa, R.; and B. Kunnumakkara, A.B. Curcumin formulations for better bioavailability: what we learned from clinical trials thus far?. ACS Omega. 2023, 8:10713-46. [CrossRef]
- COVID-19 early treatment: real-time analysis of 3,492 studies. COVID-19 early treatment: real-time analysis of 3,492 studies (c19early.org).
- Sankhe A.P., Memane N.S., Gawali V.P. et al., A prospective, multi center, single blind, randomized controlled study evaluating “AyurCoro3” as an adjuvant in the treatment of mild to moderate COVID, Journal of Ayurveda and Integrated Medical Sciences, 2021. https://jaims.in/jaims/article/view/1386/1425. [CrossRef]
- Valizadeh H., Abdolmohammadi-Vahid S., Danshina S., et al., Nano-curcumin therapy, a promising method in modulating inflammatory cytokines in COVID-19 patients, Int. Immunopharmacol. 2020. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7574843/. [CrossRef]
- Tahmasebi S., Saeed B.Q., Temirgalieva E. et al., Nanocurcumin improves Treg cell responses in patients with mild and severe SARS-CoV2, Life Sciences, 2021. https://www.sciencedirect.com/scie../article/abs/pii/S0024320521004227. [CrossRef]
- Asadirad A., Nashibi R., Khodadadi A., et al., Antiinflammatory potential of nano-curcumin as an alternative therapeutic agent for the treatment of mild-to-moderate hospitalized COVID-19 patients in a placebo-controlled clinical trial, Phytotherapy Research, 2023. https://onlinelibrary.wiley.com/doi/10.1002/ptr.7375. [CrossRef]
- Sankhe (B) A.P., Memane N.S., Gawali V.P. et al., A Randomized, Controlled, Blinded, Parallel Group, Clinical Trial to study the role of Ayurcov (AyurCoro3), one day regimen as an adjuvant therapy for COVID-19 disease management, at dedicated Covid Hospital (DCH) in India, Complementary Therapies in Medicine, 2022. https://www.sciencedirect.com/science/article/pii/S0965229922000267. [CrossRef]
- Abbaspour-Aghdam S., Hazrati A., Abdolmohammadi-Vahid S., et al., Immunomodulatory role of Nanocurcumin in COVID-19 patients with dropped natural killer cells frequency and function, European Journal of Pharmacology, 2022. https://www.sciencedirect.com/science/article/pii/S0014299922005283. [CrossRef]
- Gérain J., Uebelhoer M., Costes B. et al., NASAFYTOL® supplementation in adults hospitalized with COVID-19 infection: results from an exploratory open-label randomized controlled trial, Frontiers in Nutrition, 2023 . https://www.frontiersin.org/articles/10.3389/fnut.2023.1137407/full. [CrossRef]
- Ahmadi R., Salari S., Sharifi M.D. et al., Oral nano-curcumin formulation efficacy in the management of mild to moderate outpatient COVID-19: A randomized triple-blind placebo-controlled clinical trial, Food Science and Nutrition, 2021. https://onlinelibrary.wiley.com/doi/full/10.1002/fsn3.2226. [CrossRef]
- Majeed M., Nagabhushanam K., Shah K. et al., A Randomized, Double-Blind, Placebo-Controlled Study to Assess the Efficacy and Safety of a Nutritional Supplement (ImmuActive) for COVID-19 Patients, Evidence-Based Complementary and Alternative Medicine, 2021. https://www.hindawi.com/journals/ecam/2021/8447545/. [CrossRef]
- Khan A., Iqtadar S., Mumtaz S.U., et al., Oral Co-Supplementation of Curcumin, Quercetin, and Vitamin D3 as an Adjuvant Therapy for Mild to Moderate Symptoms of COVID-19—Results From a Pilot Open-Label, Randomized Controlled Trial, Frontiers in Pharmacology, 2022. https://www.frontiersin.org/articles/10.3389/fphar.2022.898062/full. [CrossRef]
- Askari G., Sahebkar A., Soleimani D. et al., The efficacy of curcumin-piperine co-supplementation on clinical symptoms, duration, severity, and inflammatory factors in COVID-19 outpatients: a randomized double-blind, placebo-controlled trial, Trials, 2022 . https://trialsjournal.biomedcentra..rticles/10.1186/s13063-022-06375-w. [CrossRef]
- Chitre D., Nadkarni S., Jagtap N et al., Phase III randomized clinical trial of BV-4051, an Ayurvedic polyherbal formulation in moderate SARS-CoV-2 infections and its impact on inflammatory biomarkers, Phytotherapy Research, 2023. https://onlinelibrary.wiley.com/doi/10.1002/ptr.7683. [CrossRef]
- Ujjan I.D., Khan S., Nigar R. et al., The possible therapeutic role of curcumin and quercetin in the early-stage of COVID-19—Results from a pragmatic randomized clinical trial, Frontiers in Nutrition, 2022. https://www.frontiersin.org/articles/10.3389/fnut.2022.1023997/full. [CrossRef]
- Hassaniazad M., Eftekhar E., Inchehsablagh B.R. et al., A triple-blind, placebo-controlled, randomized clinical trial to evaluate the effect of curcumin-containing nanomicelles on cellular immune responses subtypes and clinical outcome in COVID-19 patients, Phytotherapy Research, 2021. https://onlinelibrary.wiley.com/doi/full/10.1002/ptr.7294. [CrossRef]
- Hartono B., Suryawati Y. Sari A. et al., The Effect of Curcumin and Virgin Coconut Oil Towards Cytokines Levels in COVID-19 Patients at Universitas Sebelas Maret Hospital, Surakarta, Indonesia, Pharmacognosy Journal, 2022. https://phcogj.com/article/1755. [CrossRef]
- Thomas R., Williams M., Aldous J., et al., A Randomised, Double-Blind, Placebo-Controlled Trial Evaluating Concentrated Phytochemical-Rich Nutritional Capsule in Addition to a Probiotic Capsule on Clinical Outcomes among Individuals with COVID-19—The UK Phyto-V Study, COVID, 2022. https://www.mdpi.com/2673-8112/2/4/31. [CrossRef]
- Hellou E., Mohsin J., Elemy A., et al., Effect of ArtemiC in patients with COVID-19: A Phase II prospective study, Journal of Cellular and Molecular Medicine, 2022 . https://onlinelibrary.wiley.com/doi/10.1111/jcmm.17337. [CrossRef]
- Sadeghizadeh M., Asadollahi E., Jahangiri B. et al., Promising clinical outcomes of nano-curcumin treatment as an adjunct therapy in hospitalized COVID-19 patients: A randomized, double-blinded, placebo-controlled trial, Phytotherapy Research, 2023 . https://onlinelibrary.wiley.com/doi/10.1002/ptr.7844. [CrossRef]
- Ahmadi (B) S., Mehrabi Z., Zare M. et al., Efficacy of Nanocurcumin as an Add-On Treatment for Patients Hospitalized with COVID-19: A Double-Blind, Randomized Clinical Trial, International Journal of Clinical Practice, 2023 hindawi.com, doi.org.
- Fessler, S.N.; Chang, Y.; Liu, L.; Johnston, C.S. Curcumin Confers Anti-Inflammatory Effects in Adults Who Recovered from COVID-19 and Were Subsequently Vaccinated: A Randomized Controlled Trial. Nutrients 2023, 15, 1548. [Google Scholar] [CrossRef]
- Koshak A, Wei L, Koshak E, et al. Nigella sativa supplementation improves asthma control and biomarkers: a randomized, double-blind, placebo-controlled trial. Phyther Res. 2017;(January). [CrossRef]
- Razmpoosh E, Safi S, Abdollahi N, et al. The effect of Nigella sativa on the measures of liver and kidney parameters: a systematic review and meta-analysis of randomized-controlled trials. Pharmacol Res. 2020;156:104767. [CrossRef]
- Molla S, Abul M, Azad K, et al. A review on antiviral effects of Nigella Sativa L. Pharmacologyonline. 2019;2:47–53 (Accessed 18 March 2020). http://pharmacologyo nline.silae.it.
- Koshak AE, Koshak EA. Nigella sativa L as a potential phytotherapy for coronavirus disease 2019: a mini review of in silico studies. Curr Ther Res - Clin Exp. 2020;93: 100602. [CrossRef]
- Majdalawieh AF, Fayyad MW. Immunomodulatory and anti-inflammatory action of Nigella sativa and thymoquinone: a comprehensive review. Int Immunopharmacol. 2015;28(1):295–304. [CrossRef]
- Al-Ghamdi MS. The anti-inflammatory, analgesic and antipyretic activity of Nigella sativa. J Ethnopharmacol. 2001;76(1):45–48. [CrossRef]
- Ashraf S., Ashraf S., Ashraf M. et al., Honey and Nigella sativa against COVID-19 in Pakistan (HNS-COVID-PK): A multi-center placebo-controlled randomized clinical trial, Phytotherapy Research, 2023 (preprint 11/3/2020). https://onlinelibrary.wiley.com/doi/10.1002/ptr.7640. [CrossRef]
- Al-Haidari K.A., Faiq T.N., Ghareeb O. A. et al., Clinical Trial of Black Seeds Against COVID – 19 in Kirkuk City / Iraq, Indian Journal of Forensic Medicine & Toxicology, 15:3 (preprint 1/2021). https://www.researchgate.net/publi..inst_COVID_-19_in_Kirkuk_City_Iraq.
- Karimi M., Zarei A., Soleymani S. et al., Efficacy of Persian medicine herbal formulations (capsules and decoction) compared to standard care in patients with COVID-19, a multicenter open-labeled, randomized, controlled clinical trial, Phytotherapy Research, 2021 . https://onlinelibrary.wiley.com/doi/10.1002/ptr.7277. [CrossRef]
- Setayesh M., Karimi M., Zargaran A. et al., Efficacy of a Persian herbal medicine compound on coronavirus disease 2019 (COVID-19): a randomized clinical trial, Integrative Medicine Research, 2022. https://www.sciencedirect.com/science/article/pii/S2213422022000373. [CrossRef]
- Koshak A.E., Koshak E.A., Mobeireek A.F. et al., Nigella sativa for the treatment of COVID-19: An open-label randomized controlled clinical trial, Complementary Therapies in Medicine, 2021 . https://www.sciencedirect.com/science/article/pii/S0965229921001102. [CrossRef]
- Bencheqroun H., Ahmed Y., Kocak M. et al., A Randomized, Double-Blind, Placebo-Controlled, Multicenter Study to Evaluate the Safety and Efficacy of ThymoQuinone Formula (TQF) for Treating Outpatient SARS-CoV-2, Pathogens, 2022. https://www.mdpi.com/2076-0817/11/5/551. [CrossRef]
- Said S.A., Abdulbaset A., El-Kholy A.A. et al., The effect of Nigella sativa and vitamin D3 supplementation on the clinical outcome in COVID-19 patients: A randomized controlled clinical trial, Frontiers in Pharmacology, 2022 . https://www.frontiersin.org/articles/10.3389/fphar.2022.1011522/full. [CrossRef]
- Chandra K., Das A.K., Banday S., et al., Efficacy of polyherbal formulations for prevention of COVID-19 infection in high-risk subjects: A randomized open-label controlled clinical trial, Phytotherapy Research, 2022. https://onlinelibrary.wiley.com/doi/10.1002/ptr.7531. [CrossRef]
- Daneshfard B., Aghanouri R., Kazemnejad A. et al., Effect of Sinamaz nasal drop on asymptomatic family members of COVID 19 patients: An open-label randomized controlled trial, Phytotherapy Research, 2023. https://onlinelibrary.wiley.com/doi/epdf/10.1002/ptr.7915. [CrossRef]
- Bhaskar S., Kumar K. S., Krishnan K., Antony H. (2013). Quercetin alleviates hypercholesterolemic diet induced inflammation during progression and regression of atherosclerosis in rabbits. Nutrition (Burbank, Los Angeles County, Calif.), 29(1), 219–229. [CrossRef]
- Khan, H., Ullah, H., Aschner, M., Cheang, W. S., & Akkol, E. K. (2019). Neuroprotective effects of quercetin in Alzheimer’s disease. Biomolecules, 10(1), 59. [CrossRef]
- Batiha GE, Beshbishy AM, Ikram M, et al. (2020). The pharmacological activity, biochemical properties, and pharmacokinetics of the major natural polyphenolic flavonoid: Quercetin. Foods (Basel, Switzerland), 9(3), 374. [CrossRef]
- Xu Z, Shi L, Wang Y, et al. (2020). Pathological findings of COVID-19 associated with acute respiratory distress syndrome. The Lancet Respiratory Medicine, 8(4), 420–422. [CrossRef]
- Oei S, Millar CL, Nguyen Lily TN, et al. Higher intake of dietary flavonols, specifically dietary quercetin, is associated with lower odds of frailty onset over 12 years of follow-up among adults in the Framingham Heart Study. Am J Clin Nutr. 2023 Jul;118(1):27-33. [CrossRef]
- Brito J, Lima WG, Cordeiro L, da Cruz Nizer WS. (2021). Effectiveness of supplementation with quercetin-type flavonols for treatment of viral lower respiratory tract infections: Systematic review and metaanalysis of preclinical studies. Phytotherapy Research: PTR, 35(9), 4930–4942. [CrossRef]
- Mehrbod P, Abdalla MA, Fotouhi F, et al. Immunomodulatory properties of quercetin-3-O-α-L-rhamnopyranoside from Rapanea melanophloeos against influenza a virus. BMC Complementary and Alternative Medicine 2018, 18, 184. [Google Scholar] [CrossRef]
- Derosa G, Maffioli P, D’Angelo A, Di Pierro F (2021). A role for quercetin in coronavirus disease 2019 (COVID-19). Phytotherapy Research: PTR, 35(3), 1230–1236. [CrossRef]
- Di Pierro, F, Derosa, G, Maffioli, P, et al. (2021). Possible therapeutic effects of adjuvant quercetin supplementation against early-stage COVID-19 infection: A prospective, randomized, controlled, and open-label study. International Journal of General Medicine, 14, 2359–2366. [CrossRef]
- Di Pierro F., Khan A., Iqtadar S., et al., Quercetin as a possible complementary agent for early-stage COVID-19: Concluding results of a randomized clinical trial, Frontiers in Pharmacology, 2022. https://www.frontiersin.org/articles/10.3389/fphar.2022.1096853/full. [CrossRef]
- Di Pierro F, Iqtadar S, Khan A, et al. (2021). Potential clinical benefits of quercetin in the early stage of COVID-19: Results of a second, pilot, randomized, controlled and open-label clinical trial. International Journal of General Medicine, 14, 2807–2816. [CrossRef]
- Shohan M, Nashibi R, Mahmoudian-Sani MR, et al. (2022). The therapeutic efficacy of quercetin in combination with antiviral drugs in hospitalized COVID-19 patients: A randomized controlled trial. European Journal of Pharmacology, 914, 174615. [CrossRef]
- Cheema HA, Sohail A, Fatima A, et al. Quercetin for the treatment of COVID-19 patients: A systematic review and meta-analysis. Rev Med Virol. 2023 Mar;33(2):e2427. Epub 2023 Feb 13. [CrossRef] [PubMed]
- Onal et al., Treatment of COVID-19 patients with quercetin: a prospective, single center, randomized, controlled trial, Turk. J. Biol., 45:518-529 (preprint 1/19/2021). https://journals.tubitak.gov.tr/biology/vol45/iss7/13/.
- Gérain J., Uebelhoer M., Costes B. et al., NASAFYTOL® supplementation in adults hospitalized with COVID-19 infection: results from an exploratory open-label randomized controlled trial, Frontiers in Nutrition, 2023 . https://www.frontiersin.org/articles/10.3389/fnut.2023.1137407/full. [CrossRef]
- Zupanets I.A., Holubovska О.А., Tarasenko O.O. et al., Quercetin effectiveness in patients with COVID-19 associated pneumonia, Zaporozhye Med. J., 2021. http://zmj.zsmu.edu.ua/article/view/231714. [CrossRef]
- Ujjan I.D., Khan S., Nigar R. et al., The possible therapeutic role of curcumin and quercetin in the early-stage of COVID-19—Results from a pragmatic randomized clinical trial, Frontiers in Nutrition, 2022 . https://www.frontiersin.org/articles/10.3389/fnut.2022.1023997/full. [CrossRef]
- Khan A., Iqtadar S. , Sami Ullah Mumtaz S.U. et al., Oral Co-Supplementation of Curcumin, Quercetin, and Vitamin D3 as an Adjuvant Therapy for Mild to Moderate Symptoms of COVID-19—Results From a Pilot Open-Label, Randomized Controlled Trial, Frontiers in Pharmacology, 2022 . https://www.frontiersin.org/articles/10.3389/fphar.2022.898062/full. [CrossRef]
- Rondanelli M., Perna S., Gasparri C., et al., Promising Effects of 3-Month Period of Quercetin Phytosome® Supplementation in the Prevention of Symptomatic COVID-19 Disease in Healthcare Workers: A Pilot Study, Life, 2022 . https://www.mdpi.com/2075-1729/12/1/66/htm. [CrossRef]
- Arslan B., Ergun N.U., Topuz S. et al., et al., Synergistic Effect of Quercetin and Vitamin C Against COVID-19: Is a Possible Guard for Front Liners, SSRN, 2020 . https://europepmc.org/article/ppr/ppr239932. [CrossRef]
- Wu G., Meininger C.J., McNeal C.J., Bazer F.W., Rhoads J.M. Role of L-Arginine in nitric oxide synthesis and health in humans, Adv. Exp. Med. Biol. 1332 (2021) 167–187. [CrossRef]
- Gambardella J, Khondkar W, Morelli MB, Wang X, Santulli G, Trimarco V. Arginine and endothelial function. Biomedicines 2020;8(8):277. [CrossRef]
- Wijnands K.A., Castermans T.M., Hommen M.P., Meesters D.M., Poeze M. Arginine and citrulline and the immune response in sepsis, Nutrients 7 (2015) 1426–1463. [CrossRef]
- Rees CA, Rostad CA, Mantus G, et al. Altered amino acid profile in patients with SARS-CoV-2 infection. Proc Natl Acad Sci USA 2021, 118, e2101708118. [Google Scholar]
- Reizine F, Lesouhaitier M, Gregoire M, et al. SARS-CoV-2-induced ARDS associates with MDSC expansion, lymphocyte dysfunction, and arginine shortage. J Clin Immunol 2021, 41, 515–25. [Google Scholar] [CrossRef]
- Fiorentino G, Coppola A, Izzo R, et al. Effects of adding L-arginine orally to standard therapy in patients with COVID-19: A randomized, double-blind, placebo-controlled, parallel-group trial. Results of the first interim analysis. EClinicalMedicine. 2021 Oct;40:101125. [CrossRef]
- Gambardella J, Fiordelisi A, Spigno L, et al. Effects of chronic supplementation of Larginine on physical fitness in water polo players. Oxid Med Cell Longev 2021, 2021, 6684568. [Google Scholar]
- Lucas R, Czikora I, Sridhar S, et al. Arginase 1: an unexpected mediator of pulmonary capillary barrier dysfunction in models of acute lung injury. Front Immunol 2013;4:228. [CrossRef]
- WHO. A clinical case definition of post COVID-19 condition by a Delphi consensus. 6 October, 2021. Available from: https://apps.who.int/iris/rest/bitstreams/1376291/retrieve 85′. WHO. A clinical case definition for post COVID-19 condition in children and adolescents by expert consensus (16 February 2023). Available from. https://www.who.int/publications/i/item/WHO-2019-nCoV-Post-COVID-19-condition-CA-Clinical-case-definition-2023-1.
- Izzo R, Trimarco V, Mone P, et al. Combining L-Arginine with vitamin C improves long-COVID symptoms: The LINCOLN Survey. Pharmacol Res. 2022 Sep;183:106360. [CrossRef]
- Oikonomou E., Souvaliotis N., Lampsas S., et al., Endothelial dysfunction in acute and long standing COVID- 19: a prospective cohort study, Vasc. Pharm. 144 (2022), 106975. [CrossRef]
- Guervilly C., et al., Circulating endothelial cells as a marker of endothelial injury in severe COVID -19, J. Infect. Dis. 222 (2020) 1789–1793. [CrossRef]
- Charfeddine S, Ibn Hadj Amor H., Jdidi J., et al., Long COVID 19 syndrome: is it related to microcirculation and endothelial dysfunction? Insights from TUN-EndCOV study, Front Cardiovasc. Med. 8 (2021), 745758. [CrossRef]
- Sacchi A., Grassi G., Notari S., et al., Expansion of myeloid derived suppressor cells contributes to platelet activation by L-Arginine deprivation during SARS-CoV-2 infection, Cells 10 (2021). [CrossRef]
- Tosato M, Calvani R, Picca A, et al. Effects of l-Arginine Plus Vitamin C Supplementation on Physical Performance, Endothelial Function, and Persistent Fatigue in Adults with Long COVID: A Single-Blind Randomized Controlled Trial. Nutrients. 2022 Nov 23;14(23):4984. [CrossRef]
- Peiris S, Izcovich A, Ordunez P, et al. Challenges to delivering evidence-based management for long COVID. BMJ Evidence-Based Medicine 2023, 28, 295–298. [Google Scholar] [CrossRef]
- PAHO/IMS/EIH/COVID-19/23-0024. Living Systematic Review of Therapeutic Options for Post Acute or Post COVID-19 Condition, 25 August 2023. https://iris.paho.org/bitstream/handle/10665.2/57278/PAHOIMSEIHCOVID19230024_eng.pdf?sequence=18&isAllowed=y.
- Hansen KS, Mogensen TH, Agergaard J, et al. High-dose coenzyme Q10 therapy versus placebo in patients with post COVID-19 condition: a randomized, phase 2, crossover trial. Lancet Reg Health Eur. 2023 Jan;24:100539. [CrossRef]
- Mateos-Moreno MV, Mira A, Ausina-Marquez V, and Ferrer MD. Oral antiseptics against coronavirus: In-vitro and clinical evidence. J. Hosp. Infect. 2021, 113, 30–43. [Google Scholar] [CrossRef]
- Kariwa H, Fujii N, Takashima I. Inactivation of SARS coronavirus by means of povidone-iodine, physical conditions, and chemical reagents. Jpn. J. Vet. Res. 2004, 52, 105–112. [Google Scholar]
- Eggers M, Eickmann M, Zorn J. Rapid and effective virucidal activity of povidone-iodine products against Middle East respiratory syndrome coronavirus (MERS-CoV) and modified vaccinia virus Ankara (MVA). Infect. Dis. Ther 2015, 4, 491–501. [Google Scholar] [CrossRef]
- Anderson DE, et al. Povidone-iodine demonstrates rapid in vitro virucidal activity against SARS-CoV-2, the virus causing COVID-19 disease. Infect. Dis. Ther. 2020, 9, 669–675. [Google Scholar] [CrossRef]
- Martinez Lamas, L. et al. Is povidone iodine mouthwash effective against SARS-CoV-2? First in vivo tests. Oral Dis. 2020. [Google Scholar] [CrossRef]
- (Observational) Jamir L., Tripathi M., Shankar S. et al. Determinants of Outcome Among Critically Ill Police Personnel With COVID-19: A Retrospective Observational Study From Andhra Pradesh, India. Cureus cureus.com, doi.org. 2021. [Google Scholar]
- Choudhury I. M., Shabnam, N., Ahsan, T. et al. Effect of 1% Povidone Iodine Mouthwash/Gargle, Nasal and Eye Drop in COVID-19 patient. Bioresearch Communications banglajol.info, doi.org. 2021. [Google Scholar]
- Mohamed N.A., Baharom N., Sulaiman W.S. et al. Early viral clearance among COVID-19 patients when gargling with povidone-iodine and essential oils: a pilot clinical trial. medRxiv, medrxiv.org, doi.org. 2020. [Google Scholar]
- Guenezan J., Garcia M., Strasters D. et al. Povidone Iodine Mouthwash, Gargle, and Nasal Spray to Reduce Nasopharyngeal Viral Load in Patients With COVID-19: A Randomized Clinical Trial. JAMA Otolaryngol Head Neck Surg jamanetwork.com, doi.org. 2021. [Google Scholar]
- Elzein R., Abdel-Sater F., Fakhreddine S. et al. In vivo evaluation of the virucidal efficacy of chlorhexidine and povidone-iodine mouthwashes against salivary SARS-CoV-2. A randomized-controlled clinical trial. Journal of Evidence Based Dental Practice sciencedirect.com, doi.org. 2021. [Google Scholar]
- Arefin M.K., Rumi S.K.N.F., Uddin A.K.M.N. et al. Virucidal effect of povidone iodine on COVID-19 in the nasopharynx: an open-label randomized clinical trial. Indian Journal of Otolaryngology and Head & Neck Surgery springer.com, doi.org. 2022. [Google Scholar]
- Baxter A.L., Schwartz K.R., Johnson R.W. et al. Rapid initiation of nasal saline irrigation to reduce severity in high-risk COVID+ outpatients. Ear, Nose & Throat Journal sagepub.com, doi.org. 2022. [Google Scholar]
- Sulistyani L.D., Julia V., Soeprapto A., et al. The effects of mouth rinsing and gargling with mouthwash containing povidone-iodine and hydrogen peroxide on the cycle threshold value of Severe Acute Respiratory Syndrome Coronavirus 2: A randomized controlled trial of asymptomatic and mildly symptomatic patients, F1000Research f1000research.com, doi.org. 2022. [Google Scholar]
- Elsersy H.E., Zahran M.A.H., Elbakry A.E. et al. Combined Nasal, Oropharyngeal Povidone Iodine Plus Glycyrrhizic Acid Sprays, Accelerate Clinical and Laboratory Recovery and Reduces Household Transmission of SARS-CoV-2: A Randomized Placebo-Controlled Clinical Trial. Frontiers in Medicine frontiersin.org, doi.org. 2022. [Google Scholar]
- Sevinç Gül S.N., Dilsiz A., Sağlık İ., et al. Effect of oral antiseptics on the viral load of SARS-CoV-2: A randomized controlled trial. Dental and Medical Problems edu.pl, doi.org. 2022. [Google Scholar]
- Natto Z.S., Bakhrebah M.A., Afeef M. et al. The short-term effect of different chlorhexidine forms versus povidone iodine mouth rinse in minimizing the oral SARS-CoV-2 viral load: An open label randomized controlled clinical trial study. Medicine, lww.com, doi.org. 2022. [Google Scholar]
- Batioglu-Karaaltin A., Yigit O., Cakan D. et al. Effect of the povidone iodine, hypertonic alkaline solution and saline nasal lavage on nasopharyngeal viral load in COVID-19. Authorea, Inc authorea.com, doi.org. 2022. [Google Scholar]
- Matsuyama A., Okura H., Hashimoto S. et al., A prospective, randomized, open-label trial of early versus late povidone-iodine gargling in patients with COVID-19, Scientific Reports, 2022 nature.com. [CrossRef]
- Seneviratne C.J., Balan P., Ko KKK. et al. Efficacy of commercial mouth-rinses on SARS-CoV-2 viral load in saliva: randomized control trial in Singapore. Infection springer.com, doi.org. 2021. [Google Scholar]
- Zarabanda D., Vukkadala N., Phillips K.M., et al. The Effect of Povidone-Iodine Nasal Spray on COVID-19 Nasopharyngeal Viral Load in Patients: A Randomized Control Trial, Laryngoscope wiley.com, doi.org. 2022. [Google Scholar]
- Ferrer M.D., Barrueco, Á.S., Martinez-Beneyto, Y. et al. Clinical evaluation of antiseptic mouth rinses to reduce salivary load of SARS-CoV-2. Scientific Reports nature.com, doi.org. 2021. [Google Scholar]
- Fantozzi P.J., Pampena E., Pierangeli A., et al. Efficacy of antiseptic mouthrinses against SARS-CoV-2: A prospective randomized placebo-controlled pilot study. American Journal of Otolaryngology sciencedirect.com, doi.org. 2022. [Google Scholar]
- Seet R.C.S., Quek A.M.L., Ooi D.S.Q. et al. Positive impact of oral hydroxychloroquine and povidone-iodine throat spray for COVID-19 prophylaxis: an open-label randomized trial. International Journal of Infectious Diseases ijidonline.com, doi.org. 2021. [Google Scholar]
- Hasan F, Chiu HY, Salamanca E, et al. Effects of Chlorhexidine and Povidone-Iodine on the SARS-CoV-2 Load: A Systematic Review and Meta-analysis. Eur J Dent. 2023 Jul;17(3):587-601. [CrossRef]
- Baxter A.L., Schwartz K.R., Johnson R.W. et al. Rapid initiation of nasal saline irrigation to reduce severity in high-risk COVID+ outpatients. Ear, Nose & Throat Journal. 2022;0(0). [CrossRef]
- Mody, K., et al. Effect of 8.4% Soda-Bicarbonate Steam Inhalation on the Course of Disease in Mild to Moderate Cases of Covid-19, Acta Scientific Orthopaedics, 4:4, actascientific.com.
- Delić N., Matetic A., Domjanović J. et al. Effects of Different Inhalation Therapy on Ventilator-Associated Pneumonia in Ventilated COVID-19 Patients: A Randomized Controlled Trial. Microorganisms. 2022; 10(6):1118. [CrossRef]
- El-Badrawy M., Elmorsey R., Shehta M. et al. A randomized controlled trial of adjuvant inhalable sodium bicarbonate role in treatment of COVID-19, 18 November 2022, PREPRINT (Version 1) available at Research Square. [CrossRef]
- Wang T., Zhang Y., Zhang R. et al. Efficacy of nasal irrigation and oral rinse with sodium bicarbonate solution on virus clearance for COVID-19 patients. Front Public Health. 2023 Mar 15;11:1145669. [CrossRef]
- Pantazopoulos I., Chalkias A., Miziou A.,et al. A Hypertonic Seawater Nasal Irrigation Solution Containing Algal and Herbal Natural Ingredients Reduces Viral Load and SARS-CoV-2 Detection Time in the Nasal Cavity. Journal of Personalized Medicine. 2023; 13(7):1093. [CrossRef]
- Soares, C. P., da Silva, S. A. F., Soares, F. F.,et al. Preliminary observation of the use of sodium bicarbonate solution as an adjunct in the treatment of coronavirus 2019 disease (COVID-19): prognosis improvement in patients requiring intensive care / Observação preliminar do uso de solução de bicarbonato de sódio como coadjuvante no tratamento da doença coronavírus 2019 (COVID-19): melhora do prognóstico na necessidade de terapia intensiva. Brazilian Journal of Development, 7(12), 110698–110708. [CrossRef]
- El-Badrawy M. K., Saleh A. M., El-Badrawy A. et al. Role of Sodium Bicarbonate as Adjuvant Treatment of Nonsevere Computed Tomography-identified COVID-19 Pneumonia: A Preliminary Report. Indian Journal of Respiratory Care ; 10(3):318-325, 2022.
- Farrell NF, Klatt-Cromwell C, Schneider JS. Benefits and Safety of Nasal Saline Irrigations in a Pandemic-Washing COVID-19 Away. JAMA Otolaryngol Head Neck Surg. 2020;146(9):787-788. [CrossRef]
- Kanjanawasee D, Seresirikachorn K, Chitsuthipakorn W, Snidvongs K. Hypertonic Saline Versus Isotonic Saline Nasal Irrigation: Systematic Review and Meta-analysis. Am J Rhinol Allergy. 2018 Jul;32(4):269-279. [CrossRef]
- Ramalingam S., Graham C., Dove J., et al. A pilot, open labelled, randomised controlled trial of hypertonic saline nasal irrigation and gargling for the common cold. Sci Rep. 2019 Jan 31;9(1):1015. [CrossRef]
- Vlachou, M., Siamidi, A., Dedeloudi, A., Konstantinidou, S.K., Papanastasiou, I.P., 2021. Pineal hormone melatonin as an adjuvant treatment for COVID-19 (Review). Int. J. Mol. Med. 47 (4). [CrossRef]
- Bahrampour Juybari, K., Pourhanifeh, M.H., Hosseinzadeh, A., Hemati, K., Mehrzadi, S. Melatonin potentials against viral infections including COVID-19: Current evidence and new findings. Virus Res 2020, 287, 198108. [Google Scholar] [CrossRef]
- Camp, O.G.; Bai, D.; Gonullu, D.C.; Nayak, N.; Abu-Soud, H.M. Melatonin interferes with COVID-19 at several distinct ROS-related steps. J. Inorg. Biochem 2021, 223, 111546. [Google Scholar] [CrossRef]
- Faridzadeh A, Tabashiri A, Miri HH, Mahmoudi M. The role of melatonin as an adjuvant in the treatment of COVID-19: A systematic review. Heliyon. 2022 Oct;8(10):e10906. [CrossRef]
- Hasan Z.T., Atrakji D.M.Q.Y.M.A.A., Mehuaiden D.A.K., The Effect of Melatonin on Thrombosis, Sepsis and Mortality Rate in COVID-19 Patients, International Journal of Infectious Diseases, 2021 . https://www.sciencedirect.com/science/article/pii/S1201971221007980. [CrossRef]
- Bologna C., Madonna P., Pone E. et al., Efficacy of Prolonged-Release Melatonin 2 mg (PRM 2 mg) Prescribed for Insomnia in Hospitalized Patients for COVID-19: A Retrospective Observational Study, Journal of Clinical Medicine, 2021 . https://www.mdpi.com/2077-0383/10/24/5857. [CrossRef]
- Vijendra Ramlall V., Zucker J., Tatonetti N., Melatonin is significantly associated with survival of intubated COVID-19 patients, medRxiv, 020. https://www.medrxiv.org/content/10.1101/2020.10.15.20213546v1. [CrossRef]
- Sánchez-González M., Mahıllo-Fernandez I., Villar-Alvarez F., et al., What if melatonin could help COVID-19 severe patients?, 2022 . https://jcsm.aasm.org/doi/10.5664/jcsm.9554.
- Mousavi S.A., Heydari K., Mehravaran H., et al., Melatonin effects on sleep quality and outcomes of COVID-19 patients: An open-label, randomized, controlled trial, Journal of Medical Virology, 2022 . https://onlinelibrary.wiley.com/doi/full/10.1002/jmv.27312. [CrossRef]
- Sánchez-Rico M., de la Muela P., Herrera-Morueco J.J. et al., Melatonin does not reduce mortality in adult hospitalized patients with COVID-19: a multicenter retrospective observational study, Journal of Travel Medicine, 2022 . https://academic.oup.com/jtm/advan..le/doi/10.1093/jtm/taab195/6523003. [CrossRef]
- Karimpour-razkenari E., Naderi-Behdani F., Salahshoor A., et al., Melatonin as adjunctive therapy in patients admitted to the Covid-19, Annals of Medicine and Surgery, 2022 . https://www.sciencedirect.com/science/article/pii/S2049080122002527. [CrossRef]
- Alizadeh Z., Keyhanian N., Ghaderkhani S., et al., A Pilot Study on Controlling Coronavirus Disease 2019 (COVID-19) Inflammation Using Melatonin Supplement, Iranian Journal of Allergy, Asthma and Immunology, 2021 . https://ijaai.tums.ac.ir/index.php/ijaai/article/view/3086.
- Ameri A., Frouz Asadi, M., Ziaei et al., Efficacy and safety of oral melatonin in patients with severe COVID-19: a randomized controlled trial, Inflammopharmacology, 2023 . https://link.springer.com/10.1007/s10787-022-01096-7. [CrossRef]
- Darban M., Malek F., Memarian M., et al., Efficacy of High Dose Vitamin C, Melatonin and Zinc in Iranian Patients with Acute Respiratory Syndrome due to Coronavirus Infection: A Pilot Randomized Trial, Journal of Cellular & Molecular Anesthesia, 2021 . https://journals.sbmu.ac.ir/jcma/article/view/32182. [CrossRef]
- Farnoosh G., Akbariqomi M., Badriet T. et al., Efficacy of a Low Dose of Melatonin as an Adjunctive Therapy in Hospitalized Patients with COVID-19: A Randomized, Double-blind Clinical Trial, Archives of Medical Research, 2021 . https://www.sciencedirect.com/science/article/pii/S0188440921001417. [CrossRef]
- Fogleman C., Cohen D., Mercier A. et al., A Pilot of a Randomized Control Trial of Melatonin and Vitamin C for Mild-to-Moderate COVID-19, The Journal of the American Board of Family Medicine, 2022 . http://www.jabfm.org/lookup/doi/10.3122/jabfm.2022.04.210529. [CrossRef]
- García-García I.; Seco-Meseguer, E.; Ruiz-Seco, P. et al., Melatonin in the Prophylaxis of SARS-CoV-2 Infection in Healthcare Workers (MeCOVID): A Randomised Clinical Trial, Journal of Clinical Medicine, 2022 . https://www.mdpi.com/2077-0383/11/4/1139. [CrossRef]
- WHO updates guidelines on treatments for COVID-19. WHO updates guidelines on treatments for COVID-19.
- European Medicine Agency, March 18, 2020. L’EMA fornisce indicazioni sull’uso degli antinfiammatori non steroidei per COVID-19 (aifa.gov.it).
- Italian Drug Agency/AIFA. AIFA recommendations on drugs for home management of COVID-19 Vers. 10 – Update 10/03/2023. https://www.aifa.gov.it/documents/20142/1616529/IT_Raccomandazioni_AIFA_gestione_domiciliare_COVID-19_Vers10_10.03.2023.pdf.
- Ministry of Health - Italy. Open Data - Data - Drugs, 50 Sop and Otc best sellers in the 2nd half of the year 2022 - www.dati.salute.gov.it.
- Rinott E., Kozer E., Shapira Y., et al. Ibuprofen use and clinical outcomes in COVID-19 patients. Clin Microbiol Infect. 2020 Sep;26(9):1259.e5-1259.e7. [CrossRef]
- Lapi F., Marconi E., Grattagliano I., et al. To clarify the safety profile of paracetamol for home-care patients with COVID-19: a real-world cohort study, with nested case-control analysis, in primary care. Intern Emerg Med. 2022 Nov;17(8):2237-2244. [CrossRef]
- Sharif N., Opu R.R., Khan A., et al. Impact of Zinc, Vitamins C and D on Disease Prognosis among Patients with COVID-19 in Bangladesh: A Cross-Sectional Study. Nutrients. 2022 Nov 26;14(23):5029. [CrossRef]
- Chen C., Parthasarathy S., Leung J.M., et al. Distinct temporal trajectories and risk factors for Post-acute sequelae of SARS-CoV-2 infection. Front Med (Lausanne). 2023 Oct 16;10:1227883. [CrossRef]
- Ravichandran R., Mohan S.K., Sukumaran S.K., et al. An open label randomized clinical trial of Indomethacin for mild and moderate hospitalised Covid-19 patients. Sci Rep. 2022 Apr 19;12(1):6413. Erratum in: Sci Rep. 2022 Jun 20;12(1):10389. [CrossRef]
- Manjani l., Desai n., Kohli A.,et al. Effects of acetaminophen on outcomes in patients hospitalized with covid-19. Chest. 2021 Oct;160(4):A1072. [CrossRef]
- Lerner I., Serret-Larmande A., Rance B., et al. Mining Electronic Health Records for Drugs Associated With 28-day Mortality in COVID-19: Pharmacopoeia-wide Association Study (PharmWAS). JMIR Med Inform. 2022 Mar 30;10(3):e35190. Erratum in: JMIR Med Inform. 2022 Apr 12;10(4):e38505. [CrossRef]
- Ravichandran R., Mohan S.K., Sukumaran S.K., et al. An open label randomized clinical trial of Indomethacin for mild and moderate hospitalised Covid-19 patients. Sci Rep. 2022 Apr 19;12(1):6413. Erratum in: Sci Rep. 2022 Jun 20;12(1):10389. [CrossRef]
- Stufano A., Isgrò C., Palese L.L., et al. Oxidative Damage and Post-COVID Syndrome: A Cross-Sectional Study in a Cohort of Italian Workers. Int J Mol Sci. 2023 Apr 18;24(8):7445. [CrossRef]
- Abolhassani H., Delavari S., Landegren N., et al. Genetic and immunologic evaluation of children with inborn errors of immunity and severe or critical COVID-19. J Allergy Clin Immunol. 2022 Nov;150(5):1059-1073. [CrossRef]
- Baldia P.H., Wernly B., Flaatten H., et al. The association of prior paracetamol intake with outcome of very old intensive care patients with COVID-19: results from an international prospective multicentre trial. BMC Geriatr. 2022 Dec 27;22(1):1000. [CrossRef]
- Blanc F., Waechter C., Vogel T., et al. Interest of Proton Pump Inhibitors in Reducing the Occurrence of COVID-19: A Case-Control Study. Preprints 2020, 2020050016. [CrossRef]
- Sobhy A., Saleh L. A., Abdelatty M. E. L. Early Use of Ibuprofen in Moderate Cases of COVID-19 Might be a Promising Agent to Attenuate the Severity of Disease: A Randomized Controlled Trial. Open Anesthesia Journal; 17 (no pagination), 2023.
- Kolin D.A., Kulm S., Christos P.J.,et al. Clinical, regional, and genetic characteristics of Covid-19 patients from UK Biobank. PLoS One. 2020 Nov 17;15(11):e0241264. [CrossRef]
- Leal N.S., Yu Y., Chen Y., et al. Paracetamol Is Associated with a Lower Risk of COVID-19 Infection and Decreased ACE2 Protein Expression: A Retrospective Analysis. COVID. 2021; 1(1):218-229. [CrossRef]
- Park J., Lee S.H., You S.C., et al. Non-steroidal anti-inflammatory agent use may not be associated with mortality of coronavirus disease 19. Sci Rep. 2021 Mar 3;11(1):5087. [CrossRef]
- Gálvez-Barrón C., Arroyo-Huidobro M., Miňarro A., et al. COVID-19: Clinical Presentation and Prognostic Factors of Severe Disease and Mortality in the Oldest-Old Population: A Cohort Study. Gerontology. 2022;68(1):30-43. [CrossRef]
- Reese J.T., Coleman B., Chan L., et al. Cyclooxygenase inhibitor use is associated with increased COVID-19 severity. medRxiv 2021.04.13.21255438. [CrossRef]
- Chandan J.S., Zemedikun D.T., Thayakaran R., et al. . Nonsteroidal Antiinflammatory Drugs and Susceptibility to COVID-19. Arthritis Rheumatol. 2021 May;73(5):731-739. [CrossRef]
- Oh T.K., Song I.A., Lee J., et al. Musculoskeletal Disorders, Pain Medication, and in-Hospital Mortality among Patients with COVID-19 in South Korea: A Population-Based Cohort Study. Int J Environ Res Public Health. 2021 Jun 24;18(13):6804. [CrossRef]
- Moreno-Martos D., Verhamme K., Ostropolets A., et al. Characteristics and outcomes of COVID-19 patients with COPD from the United States, South Korea, and Europe. Wellcome Open Res. 2022 Mar 24;7:22. [CrossRef]
- MacFadden D.R., Brown K., Buchan S.A., et al. Screening Large Population Health Databases for Potential Coronavirus Disease 2019 Therapeutics: A Pharmacopeia-Wide Association Study of Commonly Prescribed Medications. Open Forum Infect Dis. 2022 Mar 29;9(5):ofac156. [CrossRef]
- Kim J.W., Yoon S., Lee J., et al.Serious Clinical Outcomes of COVID-19 Related to Acetaminophen or NSAIDs from a Nationwide Population-Based Cohort Study. Int J Environ Res Public Health. 2023 Feb 21;20(5):3832. [CrossRef]
- Campbell H.M., Murata A.E., Conner T.A., et al. Chronic use of non-steroidal anti-inflammatory drugs (NSAIDs) or acetaminophen and relationship with mortality among United States Veterans after testing positive for COVID-19. PLoS One. 2022 May 5;17(5):e0267462. [CrossRef]
- Xie J., Brash J.T., Turkmen C., et al. Risk of COVID-19 Diagnosis and Hospitalisation in Patients with Osteoarthritis or Back Pain Treated with Ibuprofen Compared to Other NSAIDs or Paracetamol: A Network Cohort Study. Drugs. 2023 Feb;83(3):249-263. [CrossRef]
- Kim J.W., Yoon S, Lee J., Lee S. Serious Clinical Outcomes of COVID-19 Related to Acetaminophen or NSAIDs from a Nationwide Population-Based Cohort Study. Int J Environ Res Public Health. 2023 Feb 21;20(5):3832. [CrossRef]
- Ritsinger V., Bodegård J., Kristofi R., et al. A. History of heart failure and chronic kidney disease and risk of all-cause death after COVID-19 during the first three waves of the pandemic in comparison with influenza outbreaks in Sweden: a registry-based, retrospective, case-control study. BMJ Open. 2023 Apr 28;13(4):e069037. [CrossRef]
- Sestili P., Fimognari C. Paracetamol-Induced Glutathione Consumption: Is There a Link With Severe COVID-19 Illness? Front Pharmacol. 2020 Oct 7;11:579944. [CrossRef]
- Haddad F., Soliman A.M., Wong M.E., et al. Fever integrates antimicrobial defences, inflammation control, and tissue repair in a cold-blooded vertebrate. Elife. 2023 Mar 14;12:e83644. [CrossRef]
- Muramoto Y., Takahashi S., Halfmann P.J., et al. Replicative capacity of SARS-CoV-2 omicron variants BA.5 and BQ.1.1 at elevated temperatures. Lancet Microbe. 2023 Jul;4(7):e486. [CrossRef]
- Roberts E., Delgado Nunes V., Buckner S., et al.Paracetamol: not as safe as we thought? A systematic literature review of observational studies. Ann Rheum Dis. 2016 Mar;75(3):552-9. [CrossRef]
- Doherty M., Hawkey C., Goulder M.,et al. A randomised controlled trial of ibuprofen, paracetamol or a combination tablet of ibuprofen/paracetamol in community-derived people with knee pain. Ann Rheum Dis. 2011 Sep;70(9):1534-41. [CrossRef]
- Baker B.H., Lugo-Candelas C., Wu H., et al. Association of Prenatal Acetaminophen Exposure Measured in Meconium With Risk of Attention-Deficit/Hyperactivity Disorder Mediated by Frontoparietal Network Brain Connectivity. JAMA Pediatr. 2020 Nov 1;174(11):1073-1081. [CrossRef]
Figure 1.
Random effects meta-analysis for all RCTs about curcumin mortality results in COVID-19 [17,22,23,24,25,26,27,28].
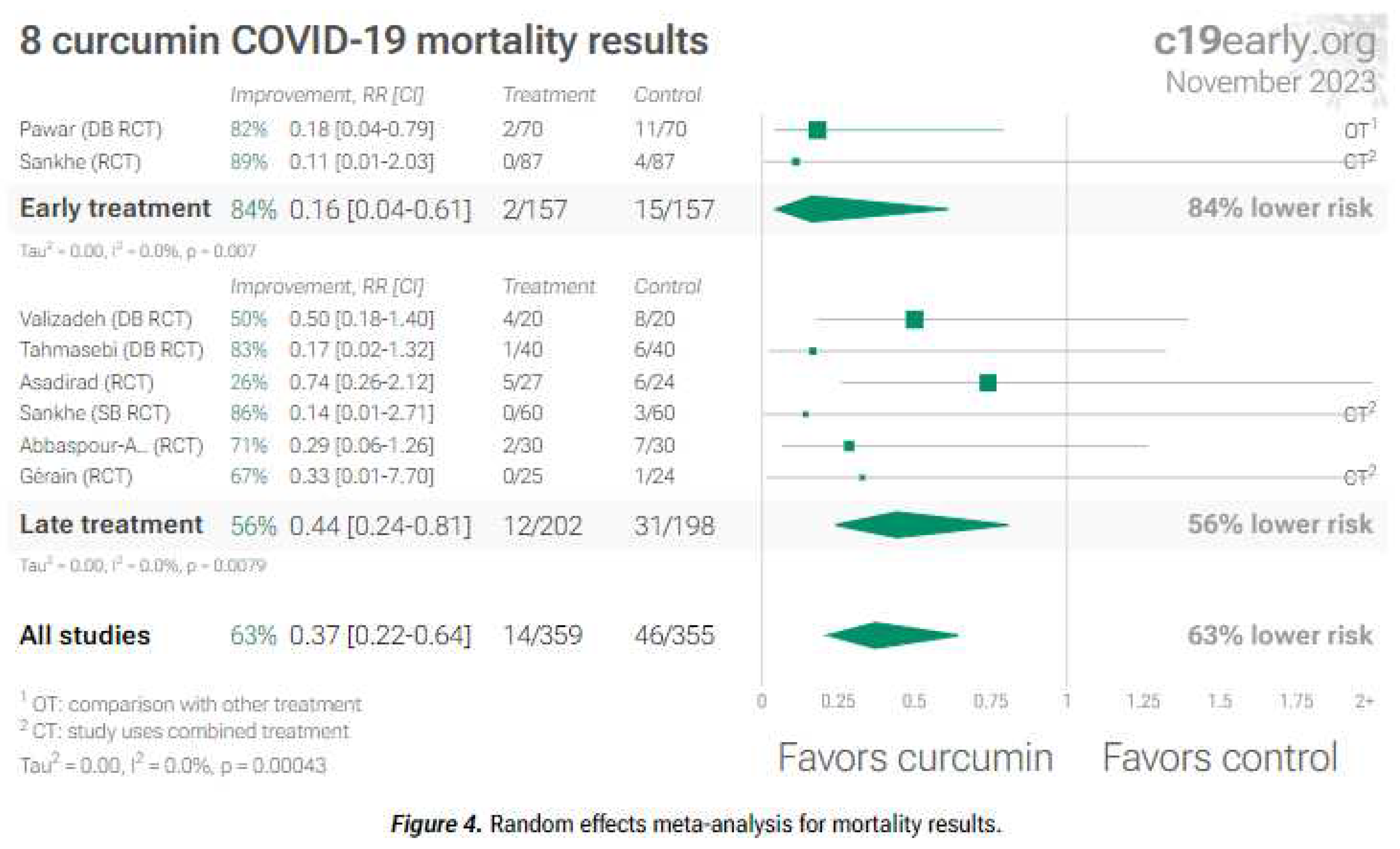
Figure 2.
Random effects meta-analysis for all RCTs about curcumin in COVID-19 [17,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40]. This plot shows pooled effects, see the specific outcome analyses for individual outcomes, and the heterogeneity section [21] for discussion. Effect extraction is pre-specified, using the most serious outcome reported. For details of effect extraction see the appendix [21].
Figure 2.
Random effects meta-analysis for all RCTs about curcumin in COVID-19 [17,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40]. This plot shows pooled effects, see the specific outcome analyses for individual outcomes, and the heterogeneity section [21] for discussion. Effect extraction is pre-specified, using the most serious outcome reported. For details of effect extraction see the appendix [21].
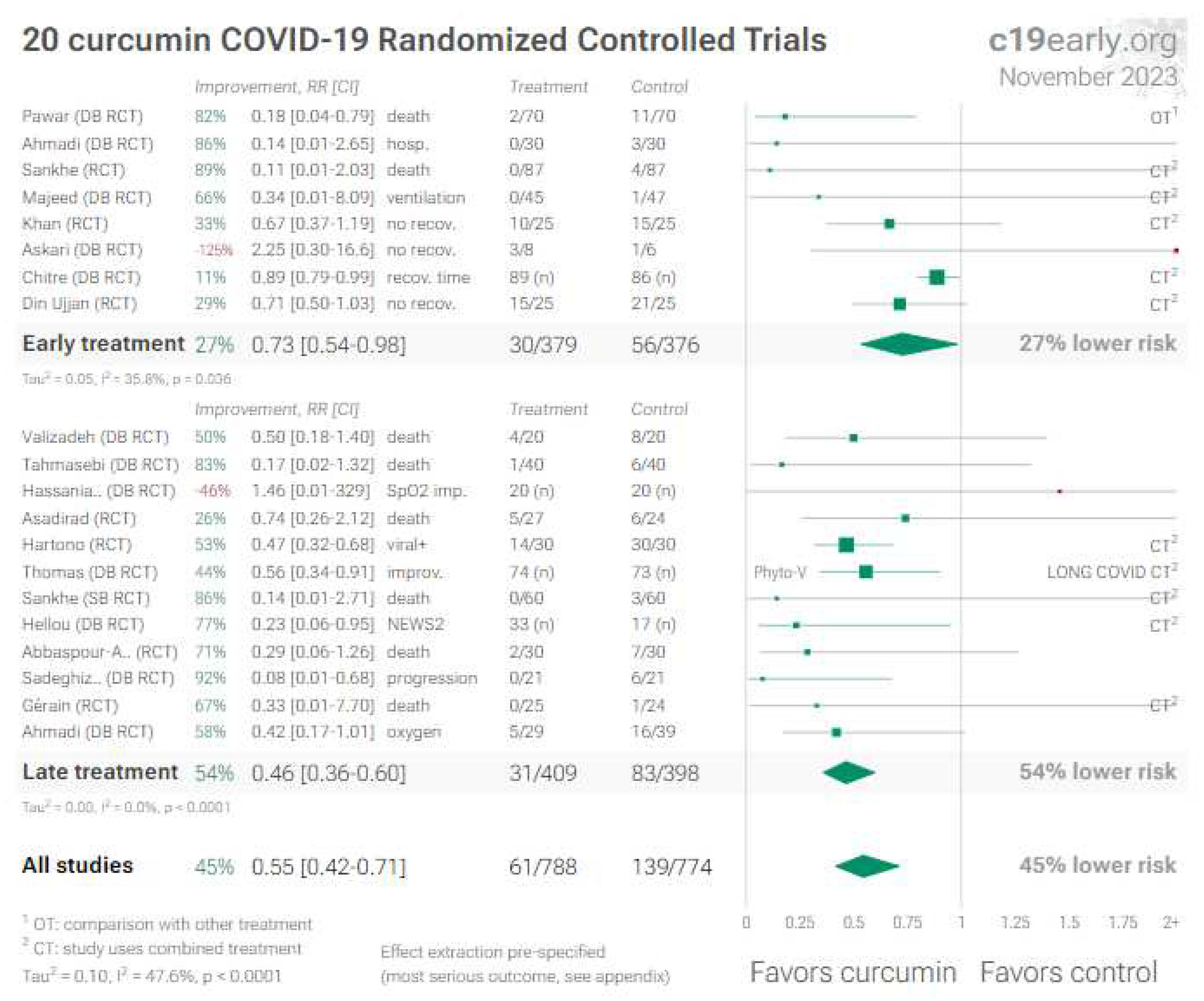
Figure 3.
Random effects meta-analysis for RCTs with mortality results about nigella sativa [48,49,50,51].
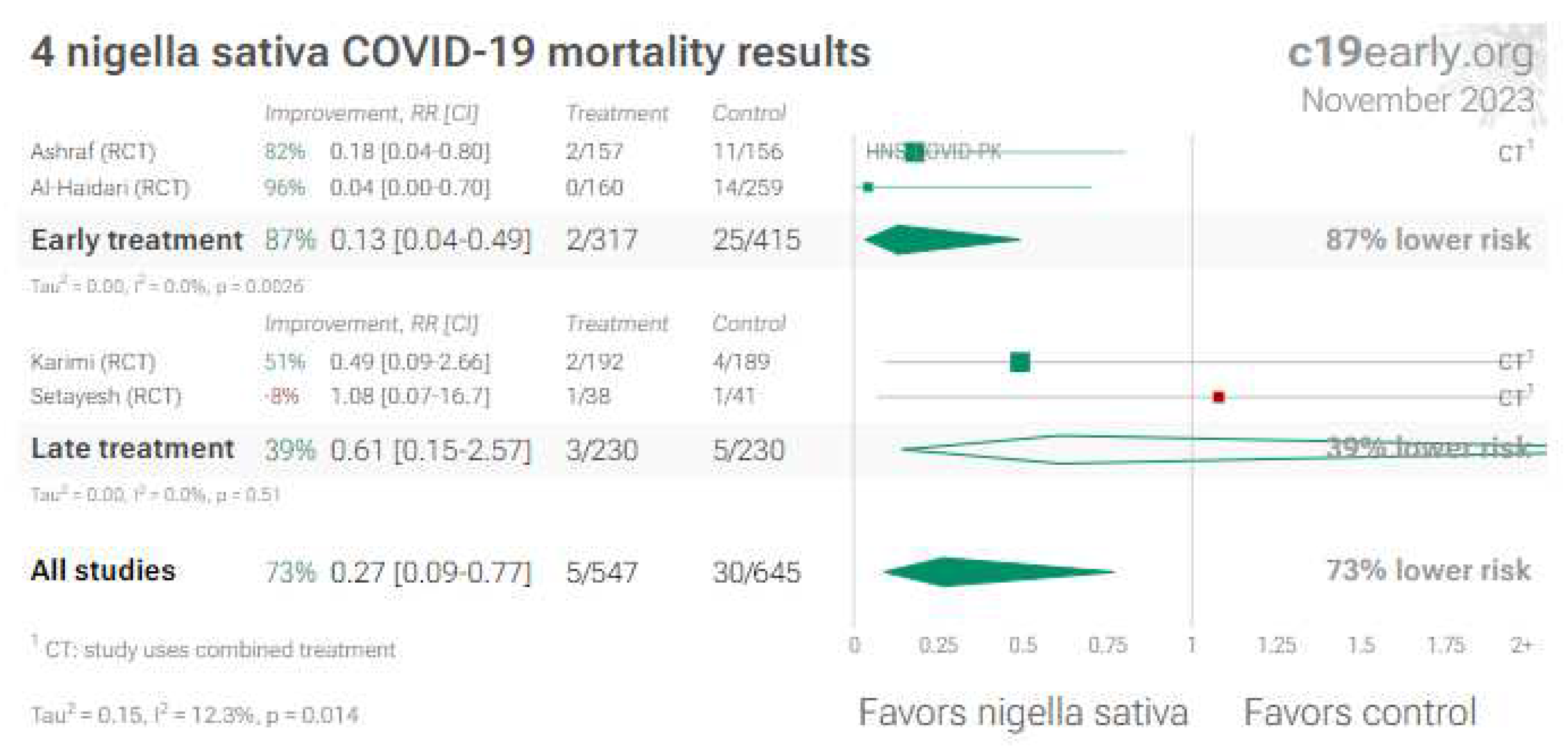
Figure 4.
Random effects meta-analysis for all RCTs about nigella sativa [48,49,50,51,52,53,54,55,56]. This plot shows pooled effects, see the specific outcome analyses for individual outcomes, and the heterogeneity section [21] for discussion. Effect extraction is pre-specified, using the most serious outcome reported. For details of effect extraction see the appendix [21].
Figure 4.
Random effects meta-analysis for all RCTs about nigella sativa [48,49,50,51,52,53,54,55,56]. This plot shows pooled effects, see the specific outcome analyses for individual outcomes, and the heterogeneity section [21] for discussion. Effect extraction is pre-specified, using the most serious outcome reported. For details of effect extraction see the appendix [21].
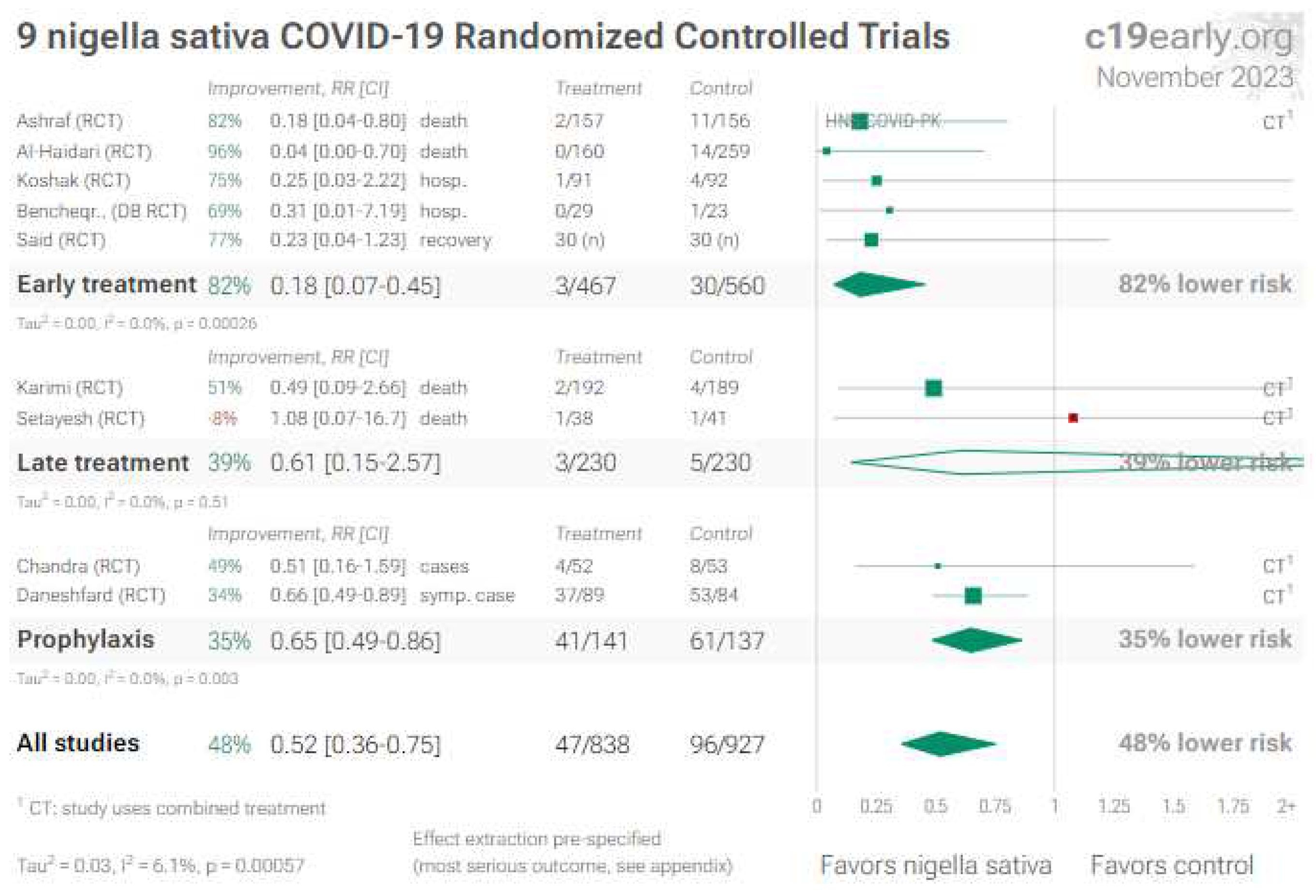
Figure 5.
Random effects meta-analysis for RCTs with mortality results about quercetin [66,67,68,70,71].
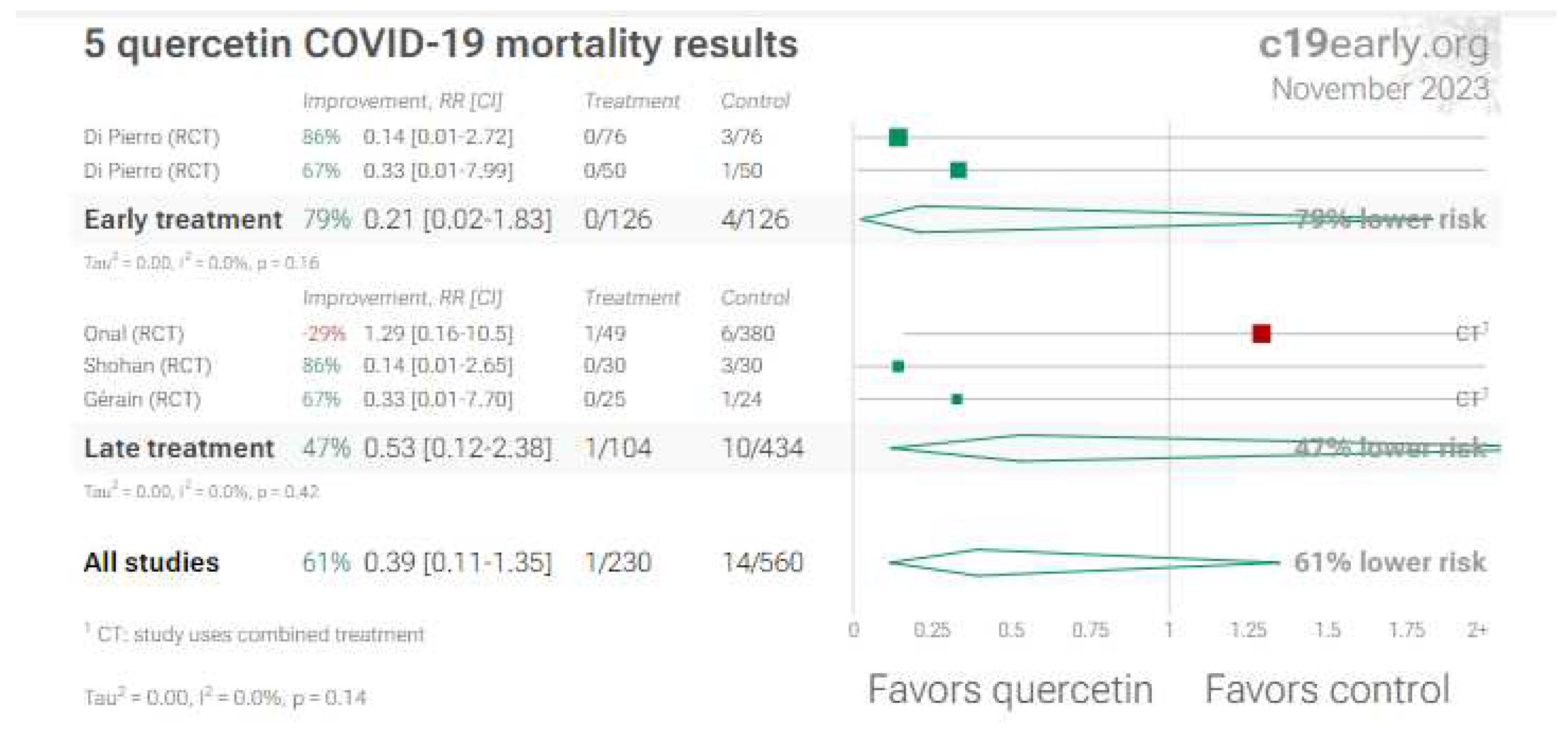
Figure 6.
Random effects meta-analysis for all RCTs about quercetin in COVID-19 [66,67,68,70,71,72,73,74,75,76]. This plot shows pooled effects, see the specific outcome analyses for individual outcomes, and the heterogeneity section [21] for discussion. Effect extraction is pre-specified, using the most serious outcome reported. For details of effect extraction see the appendix [21].
Figure 6.
Random effects meta-analysis for all RCTs about quercetin in COVID-19 [66,67,68,70,71,72,73,74,75,76]. This plot shows pooled effects, see the specific outcome analyses for individual outcomes, and the heterogeneity section [21] for discussion. Effect extraction is pre-specified, using the most serious outcome reported. For details of effect extraction see the appendix [21].
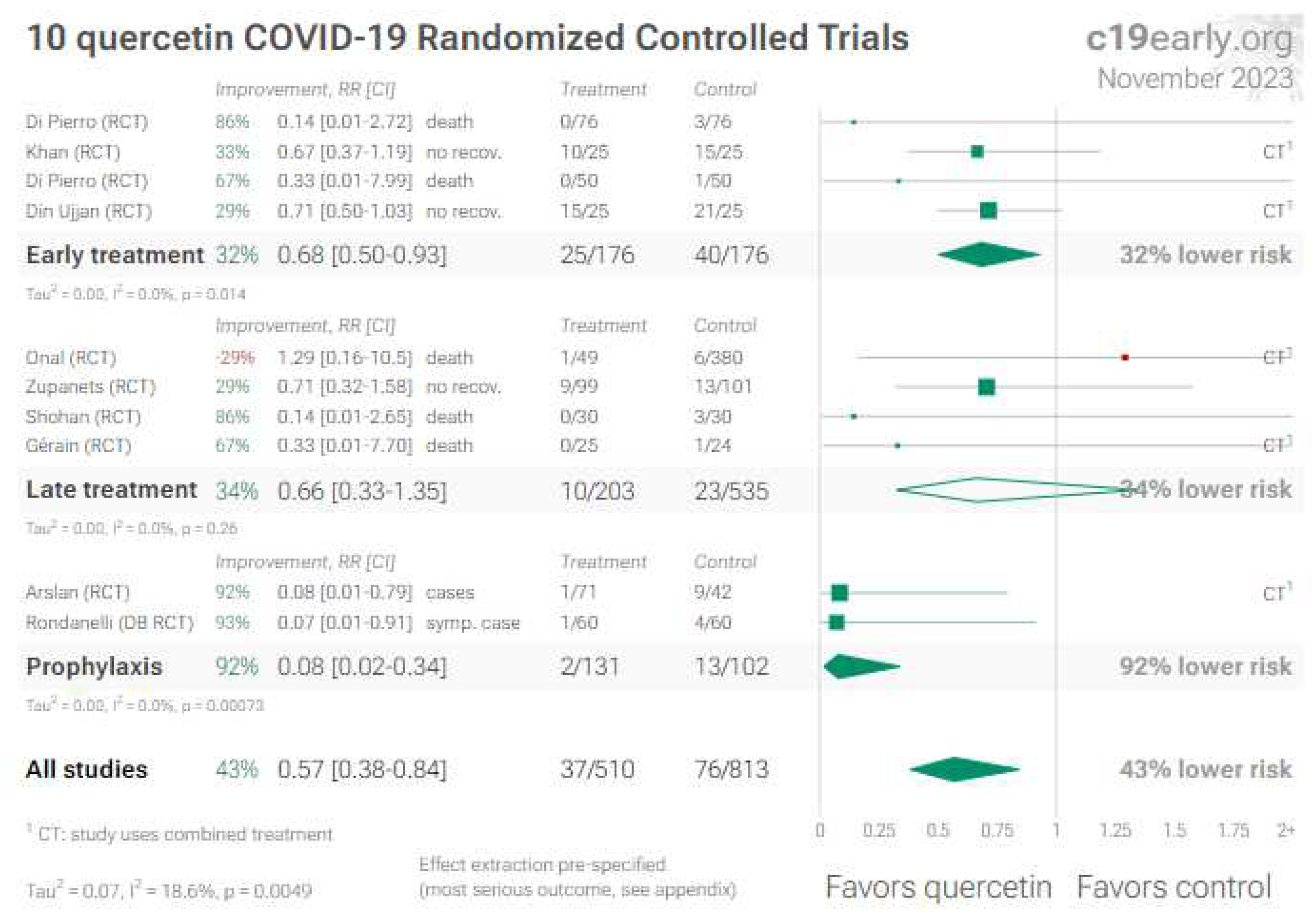
Figure 8.
Random effects meta-analysis for all RCTs about povidone-iodine in COVID-19 [100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117]. This plot shows pooled effects, see the specific outcome analyses for individual outcomes, and the heterogeneity section [21] for discussion. Effect extraction is pre-specified, using the most serious outcome reported. For details of effect extraction see the appendix [21].
Figure 8.
Random effects meta-analysis for all RCTs about povidone-iodine in COVID-19 [100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117]. This plot shows pooled effects, see the specific outcome analyses for individual outcomes, and the heterogeneity section [21] for discussion. Effect extraction is pre-specified, using the most serious outcome reported. For details of effect extraction see the appendix [21].
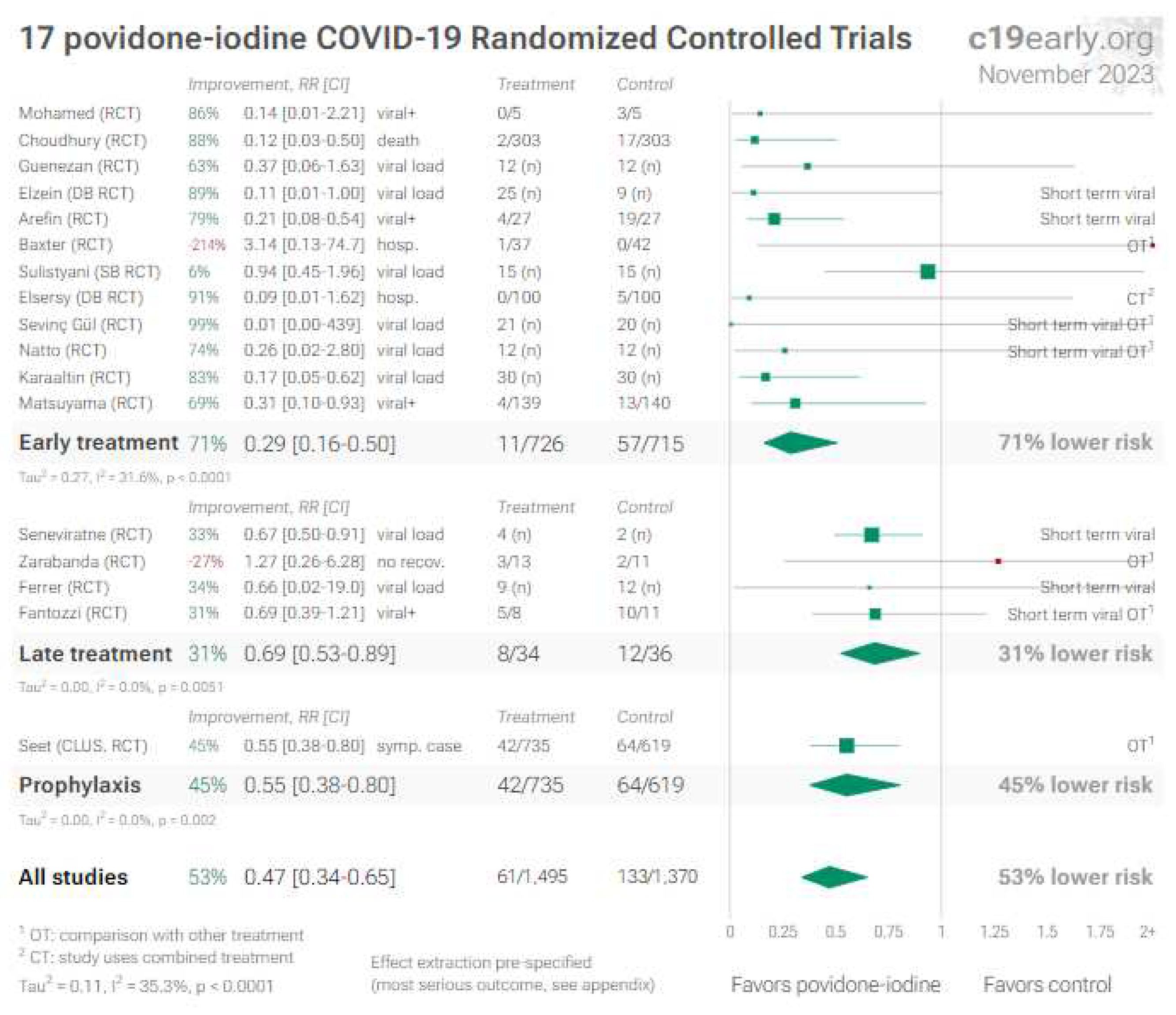
Figure 12.
Random effects meta-analysis for all RCTs about melatonin in COVID-19 [133,134,135,136,137,138,139,140,141,142,143,144,145,146]. This plot shows pooled effects, see the specific outcome analyses for individual outcomes, and the heterogeneity section [21] for discussion. Effect extraction is pre-specified, using the most serious outcome reported. For details of effect extraction see the appendix [21].
Figure 12.
Random effects meta-analysis for all RCTs about melatonin in COVID-19 [133,134,135,136,137,138,139,140,141,142,143,144,145,146]. This plot shows pooled effects, see the specific outcome analyses for individual outcomes, and the heterogeneity section [21] for discussion. Effect extraction is pre-specified, using the most serious outcome reported. For details of effect extraction see the appendix [21].
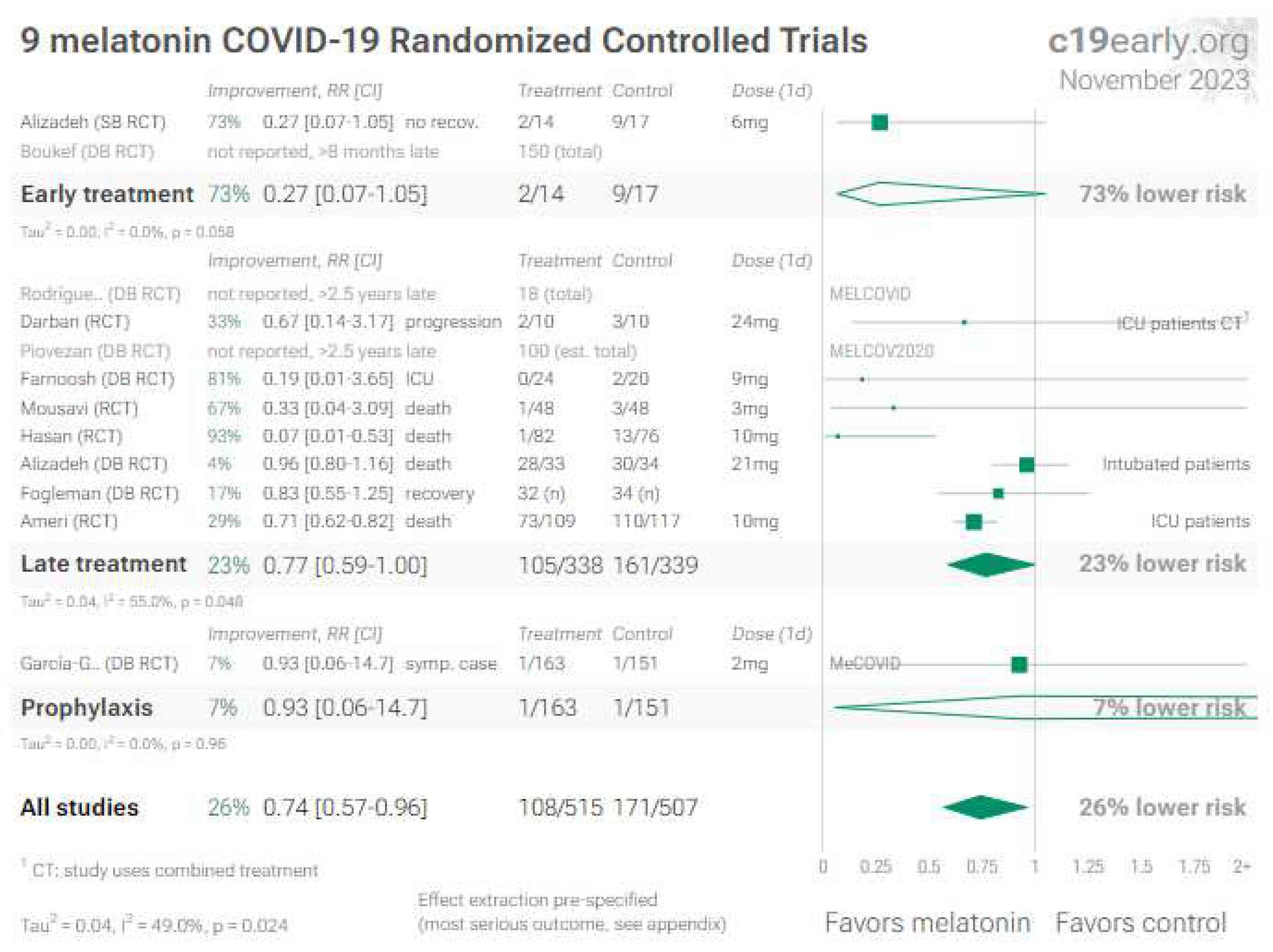
Figure 13.
No RCT (i.e., study of high validity design) reported mortality results for acetaminophen versus other comparators. Figure 14 gives the references of the various studies, showing its poor performance in virtually every comparison.
Figure 13.
No RCT (i.e., study of high validity design) reported mortality results for acetaminophen versus other comparators. Figure 14 gives the references of the various studies, showing its poor performance in virtually every comparison.
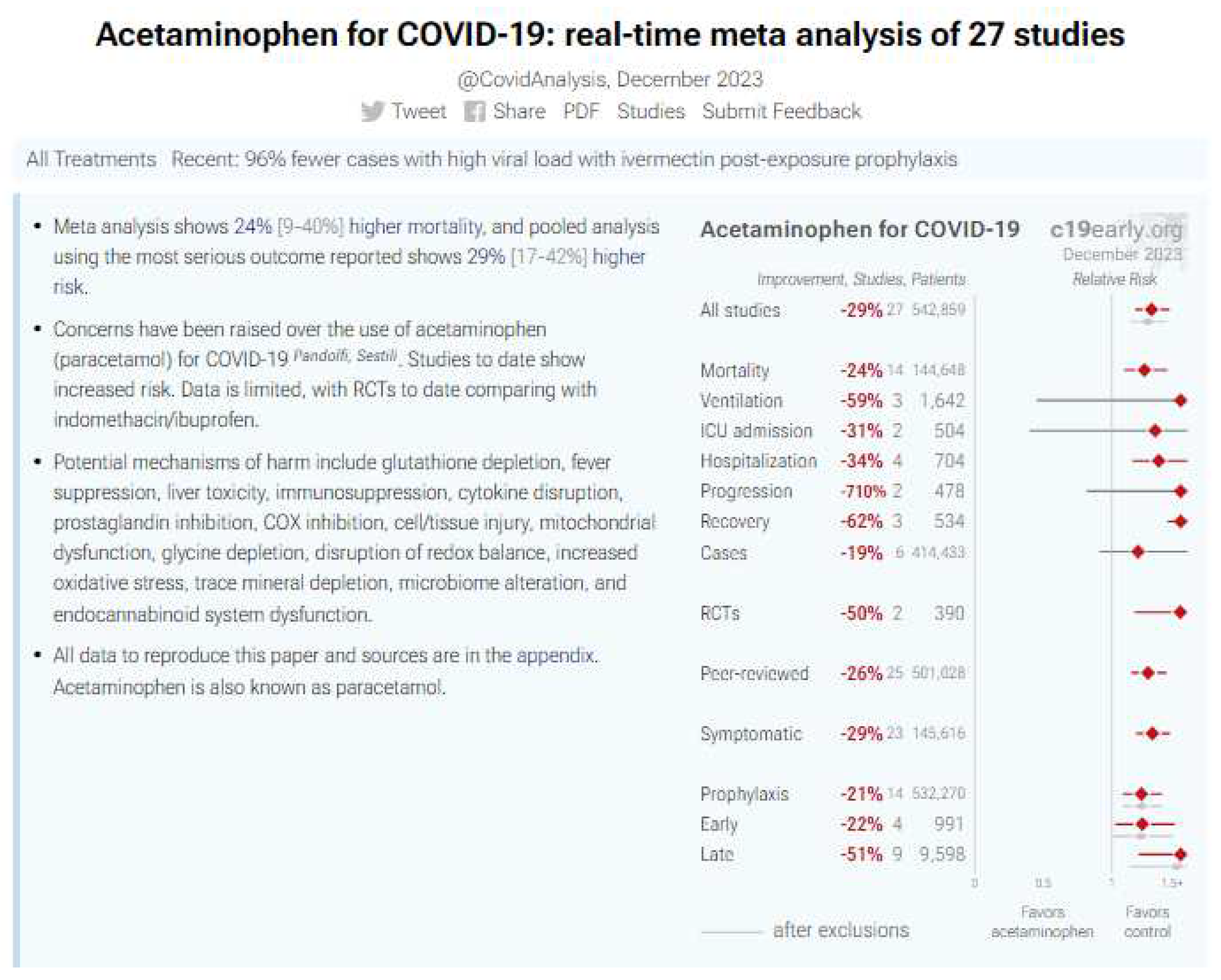
Figure 14.
Random effects meta-analysis for studies about acetaminophen in COVID-19 [151,152,153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168,169,170,171,172,173,174,175,176,177].
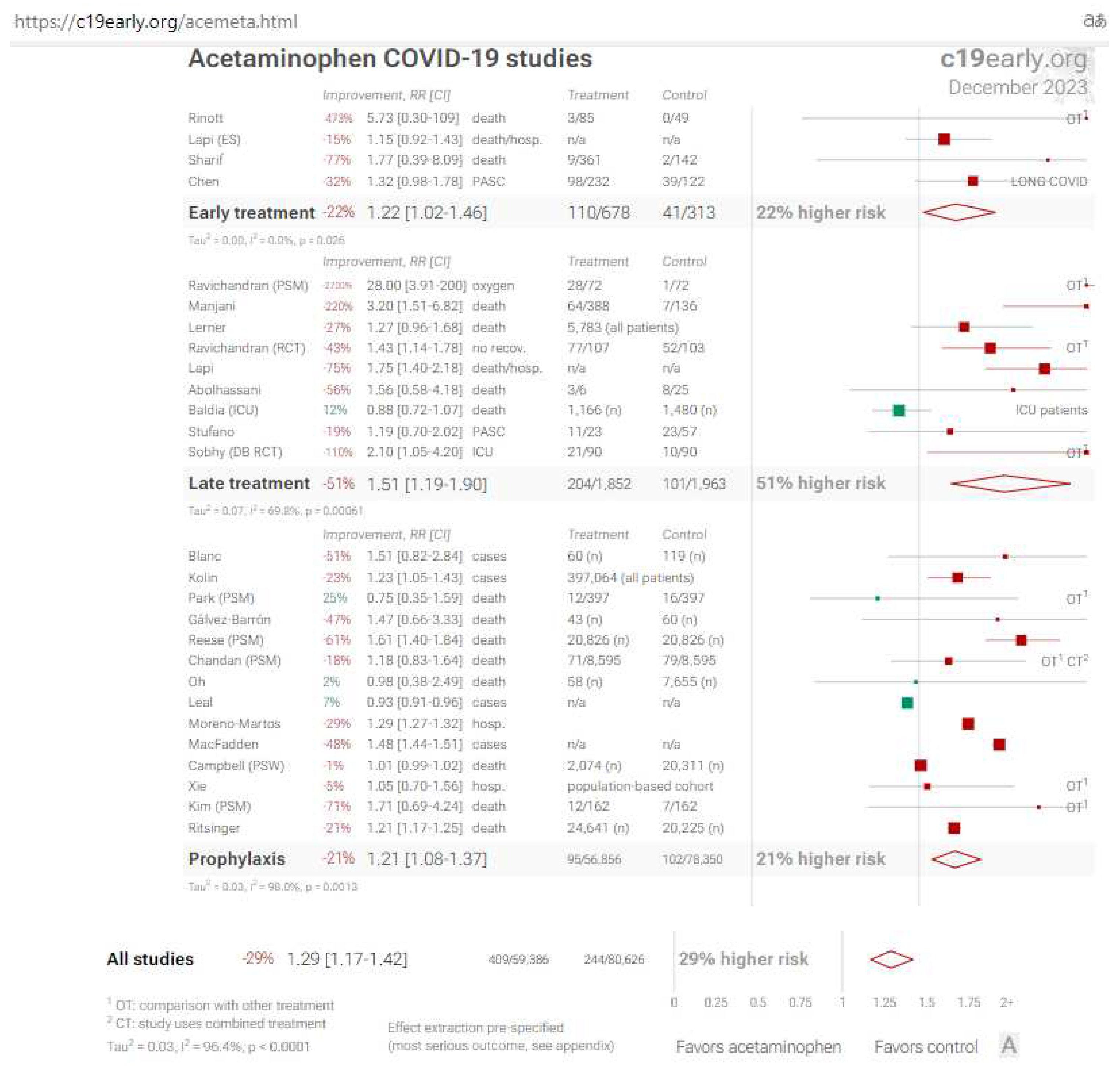

Table 1.
Survey results in the two groups of patients treated with multivitamin or L-Arginine + Vit. C [21].
Table 1.
Survey results in the two groups of patients treated with multivitamin or L-Arginine + Vit. C [21].
| Outcome | Alternative Treatment (N=521) | L-Arginine + Vitamin C (N=869) | p | |
|---|---|---|---|---|
| Asthenia | absent (%) | 0,4 | 94,9 | |
| mild (%) | 5,2 | 4,0 | <0.0001 | |
| severe (%) | 94,4 | 1,1 | ||
| Dyspnea | absent (%) | 5,4 | 74,2 | |
| mild (%) | 55,1 | 25,4 | <0.0001 | |
| severe (%) | 39,5 | 0,4 | ||
| Chest tightness | absent (%) | 26,3 | 86,1 | |
| mild (%) | 50,9 | 13,4 | <0.0001 | |
| severe (%) | 22,8 | 0,5 | ||
| Dizziness | absent (%) | 66,6 | 87,3 | |
| mild (%) | 25,9 | 11,6 | <0.0001 | |
| severe (%) | 7,5 | 1,1 | ||
| Gastrointestinal disorders | absent (%) | 63,3 | 87,7 | |
| mild (%) | 26,7 | 11,7 | <0.0001 | |
| severe (%) | 10,0 | 0,6 | ||
| Headache | absent (%) | 39,2 | 81,8 | |
| mild (%) | 44,1 | 16,8 | <0.0001 | |
| severe (%) | 16,7 | 1,4 | ||
| Anosmia | absent (%) | 52,0 | 87,2 | |
| mild (%) | 34,0 | 11,0 | <0.0001 | |
| severe (%) | 14,0 | 1,8 | ||
| Concentration difficulty | absent (%) | 32,8 | 79,1 | |
| mild (%)(%) | 46,8 | 19,4 | <0.0001 | |
| severe (%) | 20,4 | 1,5 | ||
| Sleeplessness | absent (%) | 39,5 | 80,7 | |
| mild (%) | 42,6 | 17,5 | <0.0001 | |
| severe (%) | 17,9 | 1,8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



