
Submitted:
17 December 2023
Posted:
18 December 2023
You are already at the latest version
Abstract
The advent of AI in medicine has transformed various medical specialties, including orthodontics. AI has shown promising results in enhancing the accuracy of diagnoses, treatment planning, and predicting treatment outcomes. With the growing number of AI applications and commercially available tools, there is an increase in their usage in orthodontic practices worldwide. This review aims to explore the principles of artificial intelligence (AI), its applications in the diagnostic process of modern orthodontic practices, and concerns associated with the implementation of AI algorithms in clinical practice. A comprehensive review of the literature was conducted, focusing on five categories where AI has been applied in orthodontics: dental diagnostics, cephalometric evaluation, skeletal age determination, temporomandibular joint (TMJ) evaluation, and extraction decision making. AI has demonstrated high efficacy in all those fields. However, variations in performance and the necessity of manual supervision indicate that AI should be used cautiously in clinical settings. Nevertheless, the high complexity and potential unpredictability of AI algorithms call for cautious implementation and regular manual validation of results. Continuous AI learning, proper governance, and addressing privacy and ethical concerns are crucial for the successful integration of AI into orthodontic practice.
Keywords:
orthodontics
; artificial intelligence
; deep learning
; cephalometric analysis
; radiology
; CBCT
; skeletal age
; treatment planning
1. Introduction
Artificial intelligence (AI), a term first introduced in 1955 by John McCarthy, describes the ability of machines to perform tasks classified as intelligent [1]. Over the past nearly 70 years since the coining of the term AI, there have been cycles of significant optimism associated with the development of AI, interspersed with periods of failures, reductions in research funding, and pessimism [2]. The breakthrough that sparked renewed widespread interest in AI and heralded the current boom in this technology was a victory of AlphaGo, a Deep Learning (DL)-based program developed by Google over the world champion in the board game Go in 2015 [2]. This event, accompanied by the introduction of Chat-GPT in 2022, foreshadowed the incredible growth of numerous AI applications in everyday life and medicine, which we are familiar with today.
AI algorithms have already proven their effectiveness in a variety of tasks across different medical specialties, even demonstrating the potential to outperform experienced clinicians [3,4,5,6]. Currently, AI enables the analysis, arrangement, depiction, and classification of healthcare data. The development of AI algorithms in medicine has especially occurred in recent years, particularly in radiology; medical imaging currently constitutes approximately 85% of FDA-approved AI programs (data for 2023) [7]. There are three main domains of AI in diagnostic imaging: operational AI improves healthcare delivery, diagnostic AI assists in interpreting clinical images, and predictive AI forecasts future outcomes [8]. Currently, the primary objectives of AI are to detect and segment structures, and classify pathologies [9]. The AI tools can analyze images acquired in all radiological modalities from X-ray to MRI [10,11,12,13,14]. The specific nature of orthodontics, associated with cephalometric analysis and pretreatment imaging, predisposes orthodontics to the field where AI is being implemented most rapidly. However, AI is being utilized in orthodontics in many other applications beyond cephalometric analysis. The current body of literature regarding the use of AI in orthodontics can be divided into five categories: diagnosis and treatment planning, automated landmark detection and cephalometric analysis, assessment of growth and development, treatment outcome evaluation, and a miscellaneous category [15].
The number of AI companies in the healthcare industry has increased exponentially, indicating a significant growth in commercial prospects for AI [8]. Currently, AI tools, in addition to being available to a specific group of researchers and scientists involved in particular research and development projects, are now accessible through commercially available web-based products. The adoption of AI in orthodontics has led to the development of several AI-based programs, such as WeDoCeph (Audax, Ljubljana, Slovenia), WebCeph (Assemble Circle, Gyeonggi-do, Korea), and CephX (ORCA Dental AI, Las Vegas, NV). These systems automatically identify cephalometric landmarks, compute angles and distances, and generate cephalometric reports with significant findings. This enables access to AI programs even from mobile devices and promotes the "democratization" of access to AI tools and their widespread availability to all those interested in implementing them. This, in turn, leads to a significant increase in the number of orthodontic practices and the number of scientific researchers globally who are engaged in AI applications. It also raises growing concerns related to patient safety, where AI is involved in diagnosis and treatment.
The main objectives of this article are: to elucidate the principles of AI, outline its applications in diagnostic process of modern orthodontic practices, and discuss the concerns associated with implementation of the AI algorithms in clinical practice.
2. AI categories
AI can be classified into two main categories: symbolic AI and machine learning. Symbolic AI involves structuring the algorithm in a human-readable symbolic manner. This approach was dominant in AI research until the late 1980s and is known as GOFAI (Good Old-Fashioned AI) [16]. Symbolic AI is still useful for solving problems with limited outcomes, limited computational power, or when human explainability is important. However, the efficiency of GOFAI in healthcare is low, mainly due to the complexity of problems, multiple variables, and limited sets of rules [17]. Therefore, with advancements in technology and computer sciences, the new powerful iterations of AI are becoming more prevalent, replacing GOFAI in medical applications. The schematic representation of AI in Figure 1.
2.1. Machine Learning
Machine learning (ML) is the predominant paradigm in the field of artificial intelligence. Coined by Arthur Samuel in 1952, ML differs from symbolic AI in that it relies on models learning from examples rather than predefined rules set by humans [18]. By leveraging statistical and probabilistic techniques, machines can improve their performance by learning from previous models and adapting their actions when new data is introduced. This can involve making predictions, identifying new patterns, or classifying new data.
ML can be categorized into three types based on the algorithm's learning approach and the desired outcome. The first type is supervised learning, which is used for classification or prediction tasks where the outcome is already known. Here, the algorithm learns from a labeled dataset and generalizes its knowledge to make accurate predictions on unseen data. The second type is unsupervised learning, which aims to discover hidden patterns and structures in data without any prior knowledge of the outcome. This type of learning is useful for tasks such as clustering and anomaly detection. Lastly, reinforcement learning involves the machine developing an algorithm that maximizes a predefined reward based on previous versions of itself. This type of learning is often used in scenarios where an agent interacts with an environment and learns through trial and error [19].
2.2. Deep Learning
Deep learning (DL) refers to a subset of machine learning (ML) in which the machine is capable of independently computing the specific characteristics of an input. The foundation of DL can be traced back to artificial neural networks (ANN), which were developed in the 1990s. However, with advancements in computational technology and increased computing power, researchers have been able to construct more intricate and "deeper" neural networks to tackle increasingly complex tasks. Currently, in the field of medical imaging, DL algorithms predominantly employ convolutional neural networks (CNNs) with high diagnostic accuracy [20,21,22]. DL differs from traditional ML approaches in that it allows the machine to automatically extract relevant features from input data. Instead of relying on human engineers to manually engineer these features, DL models have the ability to learn and recognize patterns directly from the raw data. Moreover, DL algorithms do not require time consuming feature dentification and extraction [22]. This has proven to be particularly useful in imaging, where DL tools are starting to surpass experienced readers in diagnostic accuracy [20,23,24]. However, the DL is not limited only to image analysis tasks, it has shown promise in tasks such as medical disease diagnosis, and personalized treatment recommendation [25,26,27,28].
3. AI applications in Orthodontics
3.1. Dental Diagnostics
The use of radiological diagnostic methods is fundamental in dental patient care. Recently, these methods have served as a basic tool aiding the clinical diagnosis of pathologies associated with teeth and their surrounding structures. They have also been a valuable tool in the assessment of treatment outcomes [29,30,31]. Besides the standard pre-orthodontic treatment evaluation in lateral cephalograms, orthopantomograms (OPG) remain valuable tools for orthodontic diagnosis, treatment planning, and monitoring [32]. Although its role and indications are still being discussed, CBCT plays an important role in decision making for orthodontic patients, where conventional radiography fails to provide an accurate diagnosis of the pathology [32,33]. However, due to the increasing number of examinations performed [34], there is a need for a tool that would comprehensively support the process of radiological diagnosis. The response to such a market demand was the emergence of multi-modular diagnostic systems based on AI. These systems are used for the analysis of both CBCT and OPG, as well as periapical radiographs (PR). The tool created by Diagnocat Ltd. (San Francisco, CA, USA), based on CNN, would ideally serve for precise, comprehensive dental diagnostics, allowing for teeth segmentation and enumeration, oral pathologies diagnosis (for example, periapical lesions, caries), and volumetric assessment. Scientific papers validating the diagnostic performance of the program have proved its high efficacy and accuracy [35,36,37,38,39]. The study by Orhan et al [35], found that the AI system achieved 92.8% accuracy in periapical lesions detection in CBCT images, and no statistically significant difference in volumetric measurements compared to manual methods. Comparable results were achieved in a study assessing the program's diagnostic accuracy in periapical lesion detection on PRs [36]. However, there are also studies revealing conflicting results, showing unacceptable accuracy of AI in OPG assessment of periapical lesions [40]. The study by Ezhov (2021) [41], compared the overall diagnostic performance of two groups of AI-aided and unaided clinicians in oral CBCT evaluation. The AI system was equipped with teeth and jaw segmentation, tooth-localization and enumeration, periodontitis, caries, and periapical lesion-detection modules. The results of the study showed that the AI system significantly improved the diagnostic capabilities of dentists (AI-aided vs unaided group sensitivity values were 0.8537 and 0.7672, specificity values were 0.9672 and 0.9616 respectively). These results suggest that such multimodal AI programs may serve as first-line diagnostic aids and decision support systems, improving patient care on many levels. Sample Diagnocat report in Figure 2.
3.2. Cephalometric Analysis
Cephalometric analysis (CA), first introduced in 1931, has evolved into a key diagnostic instrument for cranial examination in orthodontics [42]. Advancements in technology have led to the substitution of time-consuming manual assessments with digital CA software, simplifying the measurement process and automatically displaying the results of the analysis. The results of automated CA have proven to be relatively stable and repeatable compared with the highly operator-dependent manual analysis with significant variability in landmark identification [43,44,45,46]. The accuracy and repeatability of landmark identification are crucial for determining CA outcomes. Numerous studies have been conducted to demonstrate the effectiveness of AI in identifying cephalometric landmarks. Despite lateral radiography being the most widely used method in CA, recent advancements in AI have brought the utilization of cone-beam computed tomography (CBCT) back into discussion [47].
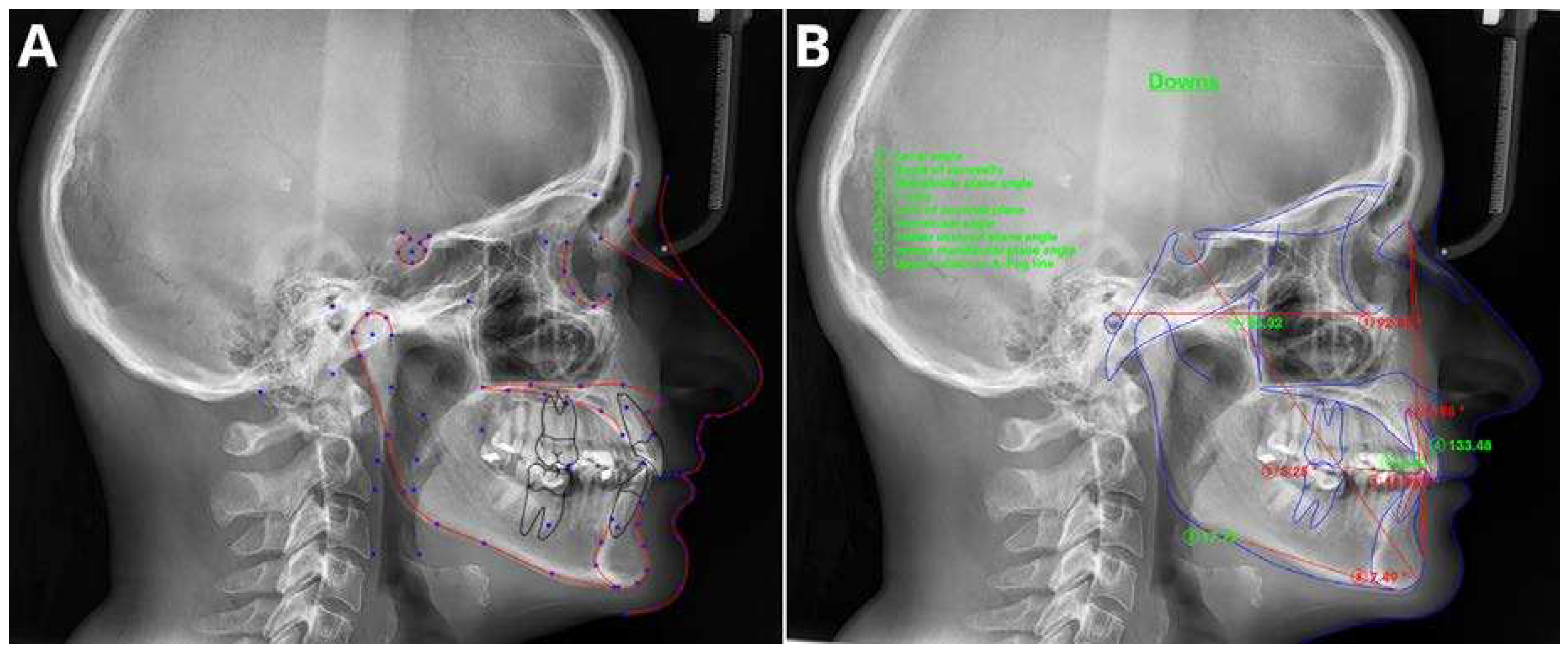
Initial attempts to evaluate the effectiveness of AI in identifying cephalometric landmarks can be traced back to 1998 [48]. The authors found no statistical differences in the mean landmark identification errors between the manual and automated methods. These results were supported by multiple other studies using different automated methods of cephalometric landmark identification, with high levels of accuracy [45,46,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63]. In a recent study conducted by Hwang et al. (2020) [46], the authors concluded that automated cephalometric landmark identification can be as reliable as an experienced human reader. Similar results, with accuracy in landmark definition between 88% and 92%, were achieved by Kim et al [53], Lee et al [62], and Dobratulin et al [49]. These authors concluded that AI demonstrated greater accuracy in landmark detection and reduced the time and human labor spent on anatomic landmark identification compared to manual methods. In other studies by be Hwang et al [45], and Yu et al [60], the authors showed that the results of automated CA were not statistically different from those calculated from manually identified landmarks. Moreover, AI can significantly improve the workflow of the practices, reducing the analysis time by up to 80 times compared to manual analysis [63]. Figure 3 presents sample cephalometric landmark definition.
The first reports regarding the utilization of Cone Beam Computed Tomography (CBCT) in CA can be traced back to the 2000s. However, due to the ineffective and time-consuming nature of this method, it did not spread widely [64]. Recent advancements in the AI field, with the possibility of automated assessment of the cranium in three dimensions, have revived the idea of CBCT-based CA. Numerous studies [65,66,67,68,69,70,71,72] leveraging AI for automatic landmark identification and analysis have demonstrated the accuracy and efficiency of these techniques compared to traditional, manual analysis. The study by Kim et al [71] showed higher repeatability of the results than those achieved by human readers. Muraev et al [72] found that ANNs could achieve accuracy in landmark identification comparable to humans and even outperform inexperienced readers in this task. However, a recent study by Bao et al (2023) [73] revealed that AI-automated analysis cannot completely replace manual tracing, and manual supervision is crucial to increase the accuracy of the results.
3.3. Determination of Skeletal Age
Growth and maturation are critical factors in the field of orthodontics, as they are closely linked to the effectiveness of orthodontic devices, which are often timed to coincide with periods of rapid growth and natural changes in facial structure. As previous studies have shown, the effectiveness of treatment can be increased by tailoring treatments to align with the patient's growth phases [74,75]. The rate of growth and the stage of facial development are crucial elements for achieving lasting results in orthodontic treatment, and precise assessment of these factors is necessary to minimize the risk of post-treatment changes resulting from ongoing facial growth [76]. The dynamics of growth in adolescence vary significantly among individuals, making chronological age alone insufficient for estimating the extent of remaining growth [77,78]. Skeletal age is a more suitable and well-established parameter for individual growth assessment with the two leading methods: cervical vertebral maturation (CVM) and wrist X-rays [74,79,80,81,82]. Since CVM can be assessed on lateral cephalometric x-rays, wrist X-rays are contraindicated in standard diagnostic orthodontic routine [32].
The last few years have seen a rise in scientific evidence supporting the diagnostic accuracy and effectiveness of AI in skeletal age assessment, based on both wrist X-rays [83,84] and CVM [85,86,87,88]. Although AI has already proven its diagnostic accuracy in skeletal age assessment, exceeding that of experienced readers in wrist X-rays [83,84] and even index finger X-rays [89], the accuracy of CVM-based models remains a concern [90,91]. Studies published on this topic have shown heterogeneous results, with agreement rates with human observers ranging from 58% to over 90% [90,92,93,94,95]. In the recent study by Seo et al. (2021) [92], the authors achieved over 90% accuracy with each of the tested CNN-based models in CVM assessment. They concluded that automatic diagnosis using lateral cephalometric radiographs can provide clinicians with accurate information on skeletal maturity. However, the results of the other above-mentioned studies call for caution when evaluating the outcomes of AI in CVM assessment and indicate significant discrepancies, especially during the critical for orthodontic treatment stages around the growth peak, which generally show lower accuracy [78,93].
We advise considering the results of AI CVM assessment studies with caution, as the gold standard was established by evaluations from a few expert readers. Therefore, the results of the studies might partially stem from errors made by the readers and their influence on AI algorithms. However, consider those results as highly encouraging, and believe that future advancements in AI technology will lead to an increase in the diagnostic accuracy of CVM tools, comparable to that of wrist X-ray skeletal maturity assessments.
3.4. TMJ Evaluation
Osteoarthritis (OA) is a condition that affects joints and is characterized by the gradual deterioration of joint cartilage associated with bone remodeling and the formation of osteoproliferative bodies. Temporomandibular joint osteoarthritis (TMJOA) is a specific type of temporomandibular disorder that can cause significant joint pain, dysfunction, dental malocclusion, and a decrease in overall quality of life [96]. The examination of TMJ function and morphology is an important part of every orthodontic or dental treatment [97], as the presence of TMJOA is one of the causes of malocclusion and facial asymmetries [98,99]. The presence of TMJOA is confirmed by bony changes observed on radiographic (OPG/CBCT) examination [100], whereas MRI remains the modality of choice in joint disc evaluation [97].
There is growing scientific evidence proving that AI applications demonstrate high diagnostic performance in the detection and staging of TMJOA [100,101,102,103,104]. The studies have shown the potential for automated, detailed assessment of joint morphology using various imaging techniques such as OPG, CBCT, and MRI. The authors anticipate that the utilization of AI systems for diagnostic imaging of the TMJ will enhance future research on early detection and personalized treatments for OA. They believe that the development of these AI systems, along with the proposed algorithms, will contribute to the establishment of a comprehensive diagnostic system for the maxillofacial region.
3.5. Extraction Decision Making
One of the most challenging issues during orthodontic treatment is deciding whether extraction is mandatory in a particular case. A variety of factors associated with the identified orthodontic defect, patient preferences, expected outcomes, sociocultural factors, and the professional position of the orthodontist, influence the patient's attitude towards the proposed orthodontic extraction therapy [105,106,107]. Additionally, on the other hand, decisions related to extractions are influenced by the experience, training, and philosophy of the orthodontist [108,109,110,111]. All these factors make the extraction decision during the orthodontic treatment very challenging, even for an experienced practitioner. Furthermore, conclusions regarding the treatment undertaken can greatly vary among experts, especially in borderline cases [112,113,114,115].
In recent years, several AI tools have been introduced, designed to support therapeutic decision-making in orthodontics [77,116,117]. Initial studies evaluating the assistance of extraction decision aids have shown promising results, with AI algorithms achieving more than 80% agreement with decisions made by experts [118,119,120,121,122]. The study by Xie (2010) [122] demonstrated an 80% concurrence in decisions related to extractions between AI and experts; however, the study only analyzed a mere 20 cases. The ANN system evaluated by Jung & King [120] showed a 93% success rate for diagnosing extraction versus non-extraction cases based on 12 cephalometric variables and 84% for the detailed diagnosis of specific extraction patterns. Similar results were achieved by Li et al. (2019) [121] with a 94% accuracy rate for extraction versus non-extraction predictions, 84.2% for extraction patterns, and 92.8% for anchorage patterns. The studies identified several features for predicting treatment, among which crowding of the upper arch, the position of anterior teeth, lower incisors inclination, overjet, overbite, and capability for lip closure were most important for the extraction decision. However, significant limitations that substantially affect the risk of bias of the selected AI models in the mentioned studies were pointed out [59]. In the majority of the manuscripts, the AI systems were trained on the examples provided by limited number of experts, therefore they were based on treatment philosophies of the examiners. Correctness of these approaches were not established. Moreover, the occurrence of important dental findings such as the large dental fillings, periapical lesions, periodontal damage, previous endodontic treatment and missing teeths were not considered [107,119,120,121,122].
Considering the aforementioned limitations, it is crucial to acknowledge that, particularly in borderline scenarios, a clear-cut decision regarding the implementation or avoidance of orthodontic extraction therapy is often elusive. Clinicians must meticulously evaluate the pros and cons of each treatment approach, considering `the entire clinical scenario. Moreover, the incorporation of extraction decision-making tools into clinical practice carries the risk of a specific treatment philosophy influencing patient care. Practitioners should strive to develop individualized treatment plans for their patients and not be influenced by rigid treatment 'philosophies' [106].
4. Implementation Considerations
While the potential of AI to improve patient management in orthodontics is vast, its impact has only been proven in a limited number of cases. Most of the literature on this subject consists of retrospective studies, without support from large randomized controlled trials. However, we might expect such studies in the coming years due to the exciting nature of this topic and the increasing supply of AI solutions. Financial investments and the number of introduced AI technologies are rapidly growing - in 2022, there were 69 new FDA-approved products associated with $4.8 billion in funding. By 2035, product-year funding is projected to reach $30.8 billion, resulting in 350 new AI products [7].
Despite many optimistic studies demonstrating the high performance of AI algorithms in a variety of tasks, the further incorporation of AI algorithms into everyday clinical practice remains a matter for the future. Most of the programs described above were launched in the last 2-3 years, and as studies have shown, the average time for the introduction of innovation in medicine to application in clinical practice is 17 years [123,124]. The process of implementing AI in workflows and clinical practice requires meeting a number of requirements to ensure sufficient clinical quality and patient safety. As indicated by Pianykh [8], here are still important issues to overcome. The first issue is the lack of reproducibility, as AI models are typically developed using a limited number of specific datasets and struggle to perform well on a wide range of data. The second issue is the lack of adaptivity, as existing AI models are not designed to constantly adjust to changes in their environment. The third issue is the absence of robust quality control mechanisms for AI, making it more susceptible to data errors, outliers, and sudden shifts in trends. Lastly, there is a lack of integration between AI algorithms and the workflow, preventing them from effectively adapting to changes in the data environment. The solution to these issues is the creation of continuous learning AI, enabling the AI tool to adapt continuously to changes in the data [8]. This would allow for live adjustments of the AI algorithms, preventing performance deterioration.
Like any technology used in medicine, there is a need for a sufficient AI governance process to maintain the quality of results and ensure patients' safety [125]. The need for continuous evaluation of algorithm quality should be kept in mind to prevent degradation in performance and allow for appropriate early intervention. Moreover, privacy issues, safety concerns, and health inequities (such as AI algorithms exacerbating racial or income disparities) are a few more general issues related to the application of AI in medicine, which have recently been highlighted in The Lancet [126].
Despite the availability of a wide range of products, there is still limited scientific evidence regarding the validation and effectiveness of AI products in general medicine and in a narrow field such as orthodontics [127]. Despite generally optimistic test results of various AI tools, the issues highlighted above underscore the necessity of exercising considerable caution when introducing AI into daily practice.
5. Conclusions
Undoubtedly, AI has the potential to revolutionize medicine, particularly in the field of diagnostic imaging, including orthodontics. The continuous advancement of AI algorithms supporting pre-treatment diagnostic processes, allowing visualization of outcomes, and facilitating decision-making during treatment, places orthodontics among the disciplines benefiting the most from the introduction of AI technology. However, due to the high complexity and associated unpredictability of AI, these tools should be treated with caution and their results should be regularly manually validated.
Author Contributions
All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- McCarthy, J.; Minsky, M.L.; Rochester, N.; Shannon, C.E. A Proposal for the Dartmouth Summer Research Project on Artificial Intelligence. AI Mag 2006, 27. [Google Scholar]
- Haenlein, M.; Kaplan, A. A Brief History of Artificial Intelligence: On the Past, Present, and Future of Artificial Intelligence. Calif Manage Rev 2019, 61. [Google Scholar] [CrossRef]
- Schwendicke, F.; Golla, T.; Dreher, M.; Krois, J. Convolutional Neural Networks for Dental Image Diagnostics: A Scoping Review. J Dent 2019, 91. [Google Scholar] [CrossRef] [PubMed]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-Level Classification of Skin Cancer with Deep Neural Networks. Nature 2017, 542. [Google Scholar] [CrossRef] [PubMed]
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J.; et al. Development and Validation of a Deep Learning Algorithm for Detection of Diabetic Retinopathy in Retinal Fundus Photographs. JAMA - Journal of the American Medical Association 2016, 316. [Google Scholar] [CrossRef] [PubMed]
- Mazurowski, M.A.; Buda, M.; Saha, A.; Bashir, M.R. Deep Learning in Radiology: An Overview of the Concepts and a Survey of the State of the Art with Focus on MRI. Journal of Magnetic Resonance Imaging 2019, 49. [Google Scholar] [CrossRef] [PubMed]
- McNabb, N.K.; Christensen, E.W.; Rula, E.Y.; Coombs, L.; Dreyer, K.; Wald, C.; Treml, C. Projected Growth in FDA-Approved Artificial Intelligence Products Given Venture Capital Funding. Journal of the American College of Radiology 2023. [Google Scholar] [CrossRef] [PubMed]
- Pianykh, O.S.; Langs, G.; Dewey, M.; Enzmann, D.R.; Herold, C.J.; Schoenberg, S.O.; Brink, J.A. Continuous Learning AI in Radiology: Implementation Principles and Early Applications. Radiology 2020, 297. [Google Scholar] [CrossRef] [PubMed]
- Milam, M.E.; Koo, C.W. The Current Status and Future of FDA-Approved Artificial Intelligence Tools in Chest Radiology in the United States. Clin Radiol 2023, 78. [Google Scholar] [CrossRef]
- Giełczyk, A.; Marciniak, A.; Tarczewska, M.; Kloska, S.M.; Harmoza, A.; Serafin, Z.; Woźniak, M. A Novel Lightweight Approach to COVID-19 Diagnostics Based on Chest X-Ray Images. J Clin Med 2022, 11. [Google Scholar] [CrossRef]
- Kloska, A.; Tarczewska, M.; Giełczyk, A.; Kloska, S.M.; Michalski, A.; Serafin, Z.; Woźniak, M. Influence of Augmentation on the Performance of the Double ResNet-Based Model for Chest X-Ray Classification. Pol J Radiol 2023, 88. [Google Scholar] [CrossRef] [PubMed]
- Fujima, N.; Kamagata, K.; Ueda, D.; Fujita, S.; Fushimi, Y.; Yanagawa, M.; Ito, R.; Tsuboyama, T.; Kawamura, M.; Nakaura, T.; et al. Current State of Artificial Intelligence in Clinical Applications for Head and Neck MR Imaging. Magnetic Resonance in Medical Sciences 2023. [Google Scholar] [CrossRef]
- Matsubara, K.; Ibaraki, M.; Nemoto, M.; Watabe, H.; Kimura, Y. A Review on AI in PET Imaging. Ann Nucl Med 2022, 36. [Google Scholar] [CrossRef]
- Wang, B.; Jin, S.; Yan, Q.; Xu, H.; Luo, C.; Wei, L.; Zhao, W.; Hou, X.; Ma, W.; Xu, Z.; et al. AI-Assisted CT Imaging Analysis for COVID-19 Screening: Building and Deploying a Medical AI System. Appl Soft Comput 2021, 98. [Google Scholar] [CrossRef] [PubMed]
- Bichu, Y.M.; Hansa, I.; Bichu, A.Y.; Premjani, P.; Flores-Mir, C.; Vaid, N.R. Applications of Artificial Intelligence and Machine Learning in Orthodontics: A Scoping Review. Prog Orthod 2021, 22. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.; Haugeland, J. Artificial Intelligence: The Very Idea. Technol Cult 1987, 28. [Google Scholar] [CrossRef]
- Schwartz, W.B.; Patil, R.S.; Szolovits, P. Artificial Intelligence in Medicine. Where Do We Stand? N Engl J Med 1987, 316. [Google Scholar] [CrossRef]
- Faber, J.; Faber, C.; Faber, P. Artificial Intelligence in Orthodontics. APOS Trends in Orthodontics 2019, 9. [Google Scholar] [CrossRef]
- Bishop, C. Pattern Recognition and Machine Learning; Springer, 2007; Volume 16. [Google Scholar]
- Rajpurkar, P.; Irvin, J.; Ball, R.L.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T.; Ding, D.; Bagul, A.; Langlotz, C.P.; et al. Deep Learning for Chest Radiograph Diagnosis: A Retrospective Comparison of the CheXNeXt Algorithm to Practicing Radiologists. PLoS Med 2018, 15. [Google Scholar] [CrossRef]
- Chilamkurthy, S.; Ghosh, R.; Tanamala, S.; Biviji, M.; Campeau, N.G.; Venugopal, V.K.; Mahajan, V.; Rao, P.; Warier, P. Deep Learning Algorithms for Detection of Critical Findings in Head CT Scans: A Retrospective Study. The Lancet 2018, 392. [Google Scholar] [CrossRef]
- Yu, A.C.; Mohajer, B.; Eng, J. External Validation of Deep Learning Algorithms for Radiologic Diagnosis: A Systematic Review. Radiol Artif Intell 2022, 4. [Google Scholar] [CrossRef] [PubMed]
- Wu, N.; Phang, J.; Park, J.; Shen, Y.; Huang, Z.; Zorin, M.; Jastrzebski, S.; Fevry, T.; Katsnelson, J.; Kim, E.; et al. Deep Neural Networks Improve Radiologists’ Performance in Breast Cancer Screening. IEEE Trans Med Imaging 2020, 39. [Google Scholar] [CrossRef]
- Kuo, W.; Hӓne, C.; Mukherjee, P.; Malik, J.; Yuh, E.L. Expert-Level Detection of Acute Intracranial Hemorrhage on Head Computed Tomography Using Deep Learning. Proc Natl Acad Sci U S A 2019, 116. [Google Scholar] [CrossRef] [PubMed]
- Bulten, W.; Pinckaers, H.; van Boven, H.; Vink, R.; de Bel, T.; van Ginneken, B.; van der Laak, J.; Hulsbergen-van de Kaa, C.; Litjens, G. Automated Deep-Learning System for Gleason Grading of Prostate Cancer Using Biopsies: A Diagnostic Study. Lancet Oncol 2020, 21. [Google Scholar] [CrossRef] [PubMed]
- Hosny, A.; Aerts, H.J.; Mak, R.H. Handcrafted versus Deep Learning Radiomics for Prediction of Cancer Therapy Response. Lancet Digit Health 2019, 1. [Google Scholar] [CrossRef]
- Lou, B.; Doken, S.; Zhuang, T.; Wingerter, D.; Gidwani, M.; Mistry, N.; Ladic, L.; Kamen, A.; Abazeed, M.E. An Image-Based Deep Learning Framework for Individualising Radiotherapy Dose: A Retrospective Analysis of Outcome Prediction. Lancet Digit Health 2019, 1. [Google Scholar] [CrossRef]
- Haug, C.J.; Drazen, J.M. Artificial Intelligence and Machine Learning in Clinical Medicine, 2023. New England Journal of Medicine 2023, 388. [Google Scholar] [CrossRef] [PubMed]
- Vandenberghe, B.; Jacobs, R.; Bosmans, H. Modern Dental Imaging: A Review of the Current Technology and Clinical Applications in Dental Practice. Eur Radiol 2010, 20. [Google Scholar] [CrossRef]
- Drage, N. Cone Beam Computed Tomography (CBCT) in General Dental Practice. Prim Dent J 2018, 7. [Google Scholar] [CrossRef]
- Gallichan, N.; Albadri, S.; Dixon, C.; Jorgenson, K. Trends in CBCT Current Practice within Three UK Paediatric Dental Departments. European Archives of Paediatric Dentistry 2020, 21. [Google Scholar] [CrossRef]
- Kapetanović, A.; Oosterkamp, B.C.M.; Lamberts, A.A.; Schols, J.G.J.H. Orthodontic Radiology: Development of a Clinical Practice Guideline. Radiologia Medica 2021, 126. [Google Scholar] [CrossRef] [PubMed]
- de Grauwe, A.; Ayaz, I.; Shujaat, S.; Dimitrov, S.; Gbadegbegnon, L.; Vannet, B. Vande; Jacobs, R. CBCT in Orthodontics: A Systematic Review on Justification of CBCT in a Paediatric Population Prior to Orthodontic Treatment. Eur J Orthod 2019, 41. [Google Scholar] [CrossRef]
- Hajem, S.; Brogårdh-Roth, S.; Nilsson, M.; Hellén-Halme, K. CBCT of Swedish Children and Adolescents at an Oral and Maxillofacial Radiology Department. A Survey of Requests and Indications. Acta Odontol Scand 2020, 78. [Google Scholar] [CrossRef] [PubMed]
- Orhan, K.; Bayrakdar, I.S.; Ezhov, M.; Kravtsov, A.; Özyürek, T. Evaluation of Artificial Intelligence for Detecting Periapical Pathosis on Cone-Beam Computed Tomography Scans. Int Endod J 2020, 53. [Google Scholar] [CrossRef]
- Issa, J.; Jaber, M.; Rifai, I.; Mozdziak, P.; Kempisty, B.; Dyszkiewicz-Konwińska, M. Diagnostic Test Accuracy of Artificial Intelligence in Detecting Periapical Periodontitis on Two-Dimensional Radiographs: A Retrospective Study and Literature Review. Medicina (Lithuania) 2023, 59. [Google Scholar] [CrossRef] [PubMed]
- Orhan, K.; Shamshiev, M.; Ezhov, M.; Plaksin, A.; Kurbanova, A.; Ünsal, G.; Gusarev, M.; Golitsyna, M.; Aksoy, S.; Mısırlı, M.; et al. AI-Based Automatic Segmentation of Craniomaxillofacial Anatomy from CBCT Scans for Automatic Detection of Pharyngeal Airway Evaluations in OSA Patients. Sci Rep 2022, 12. [Google Scholar] [CrossRef]
- Vujanovic, T.; Jagtap, R. Evaluation of Artificial Intelligence for Automatic Tooth and Periapical Pathosis Detection on Panoramic Radiography. Oral Surg Oral Med Oral Pathol Oral Radiol 2023, 135. [Google Scholar] [CrossRef]
- Brignardello-Petersen, R. Artificial Intelligence System Seems to Be Able to Detect a High Proportion of Periapical Lesions in Cone-Beam Computed Tomographic Images. Journal of the American Dental Association 2020, 151. [Google Scholar] [CrossRef]
- Zadrożny, Ł.; Regulski, P.; Brus-Sawczuk, K.; Czajkowska, M.; Parkanyi, L.; Ganz, S.; Mijiritsky, E. Artificial Intelligence Application in Assessment of Panoramic Radiographs. Diagnostics 2022, 12. [Google Scholar] [CrossRef]
- Ezhov, M.; Gusarev, M.; Golitsyna, M.; Yates, J.M.; Kushnerev, E.; Tamimi, D.; Aksoy, S.; Shumilov, E.; Sanders, A.; Orhan, K. Clinically Applicable Artificial Intelligence System for Dental Diagnosis with CBCT. Sci Rep 2021, 11. [Google Scholar] [CrossRef]
- Leonardi, R.; Giordano, D.; Maiorana, F.; Spampinato, C. Automatic Cephalometric Analysis: A Systematic Review. Angle Orthodontist 2008, 78. [Google Scholar] [CrossRef]
- Chen, Y.J.; Chen, S.K.; Yao, J.C.C.; Chang, H.F. The Effects of Differences in Landmark Identification on the Cephalometric Measurements in Traditional versus Digitized Cephalometry. Angle Orthodontist 2004, 74. [Google Scholar]
- Dias Da Silveira, H.L.; Dias Silveira, H.E. Reproducibility of Cephalometric Measurements Made by Three Radiology Clinics. Angle Orthodontist 2006, 76. [Google Scholar]
- Hwang, H.-W.; Moon, J.-H.; Kim, M.-G.; Donatelli, R.E.; Lee, S.-J. Evaluation of Automated Cephalometric Analysis Based on the Latest Deep Learning Method. Angle Orthod 2021, 91, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.W.; Park, J.H.; Moon, J.H.; Yu, Y.; Kim, H.; Her, S.B.; Srinivasan, G.; Aljanabi, M.N.A.; Donatelli, R.E.; Lee, S.J. Automated Identification of Cephalometric Landmarks: Part 2-Might It Be Better than Human? Angle Orthodontist 2020, 90. [Google Scholar] [CrossRef]
- Chung, E.J.; Yang, B.E.; Park, I.Y.; Yi, S.; On, S.W.; Kim, Y.H.; Kang, S.H.; Byun, S.H. Effectiveness of Cone-Beam Computed Tomography-Generated Cephalograms Using Artificial Intelligence Cephalometric Analysis. Sci Rep 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, D.J.; Sinclair, P.M.; Coggins, J.M. Automatic Computerized Radiographic Identification of Cephalometric Landmarks. Am J Orthod Dentofacial Orthop 1998, 113. [Google Scholar] [CrossRef] [PubMed]
- Dobratulin, K.; Gaidel, A.; Kapishnikov, A.; Ivleva, A.; Aupova, I.; Zelter, P. The Efficiency of Deep Learning Algorithms for Detecting Anatomical Reference Points on Radiological Images of the Head Profile. In Proceedings of the Proceedings of ITNT 2020 - 6th IEEE International Conference on Information Technology and Nanotechnology; 2020.
- Park, J.H.; Hwang, H.W.; Moon, J.H.; Yu, Y.; Kim, H.; Her, S.B.; Srinivasan, G.; Aljanabi, M.N.A.; Donatelli, R.E.; Lee, S.J. Automated Identification of Cephalometric Landmarks: Part 1—Comparisons between the Latest Deep-Learning Methods YOLOV3 and SSD. Angle Orthodontist 2019, 89. [Google Scholar] [CrossRef]
- Tanikawa, C.; Yamamoto, T.; Yagic, M.; Takadad, K. Automatic Recognition of Anatomic Features on Cephalograms of Preadolescent Children. Angle Orthodontist 2010, 80. [Google Scholar] [CrossRef]
- Tanikawa, C.; Yagi, M.; Takada, K. Automated Cephalometry: System Performance Reliability Using Landmark-Dependent Criteria. Angle Orthodontist 2009, 79. [Google Scholar] [CrossRef]
- Kim, H.; Shim, E.; Park, J.; Kim, Y.J.; Lee, U.; Kim, Y. Web-Based Fully Automated Cephalometric Analysis by Deep Learning. Comput Methods Programs Biomed 2020, 194. [Google Scholar] [CrossRef] [PubMed]
- Grau, V.; Alcañiz, M.; Juan, M.C.; Monserrat, C.; Knoll, C. Automatic Localization of Cephalometric Landmarks. J Biomed Inform 2001, 34. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Zeng, W.; He, T.; Zhou, S.; Zhang, Y.; Guo, J.; Tang, W. Automatic Localization of Cephalometric Landmarks Based on Convolutional Neural Network. American Journal of Orthodontics and Dentofacial Orthopedics 2022, 161. [Google Scholar] [CrossRef] [PubMed]
- Rueda, S.; Alcañiz, M. An Approach for the Automatic Cephalometric Landmark Detection Using Mathematical Morphology and Active Appearance Models. In Proceedings of the Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); 2006; Vol. 4190 LNCS-I.
- Vuinić, P.; Trpovski, Z.; Ćepan, I. Automatic Landmarking of Cephalograms Using Active Appearance Models. Eur J Orthod 2010, 32. [Google Scholar] [CrossRef] [PubMed]
- Nishimoto, S.; Sotsuka, Y.; Kawai, K.; Ishise, H.; Kakibuchi, M. Personal Computer-Based Cephalometric Landmark Detection with Deep Learning, Using Cephalograms on the Internet. Journal of Craniofacial Surgery 2019, 30. [Google Scholar] [CrossRef] [PubMed]
- Kunz, F.; Stellzig-Eisenhauer, A.; Zeman, F.; Boldt, J. Artificial Intelligence in Orthodontics: Evaluation of a Fully Automated Cephalometric Analysis Using a Customized Convolutional Neural Network. Journal of Orofacial Orthopedics 2020, 81. [Google Scholar] [CrossRef]
- Yu, H.J.; Cho, S.R.; Kim, M.J.; Kim, W.H.; Kim, J.W.; Choi, J. Automated Skeletal Classification with Lateral Cephalometry Based on Artificial Intelligence. J Dent Res 2020, 99. [Google Scholar] [CrossRef]
- Mario, M.C.; Abe, J.M.; Ortega, N.R.S.; Del Santo, M. Paraconsistent Artificial Neural Network as Auxiliary in Cephalometric Diagnosis. Artif Organs 2010, 34. [Google Scholar] [CrossRef]
- Lee, J.H.; Yu, H.J.; Kim, M.J.; Kim, J.W.; Choi, J. Automated Cephalometric Landmark Detection with Confidence Regions Using Bayesian Convolutional Neural Networks. BMC Oral Health 2020, 20. [Google Scholar] [CrossRef]
- Nishimoto, S. Locating Cephalometric Landmarks with Multi-Phase Deep Learning. Journal of Dental Health and Oral Research 2023. [Google Scholar] [CrossRef]
- Palomo, J.M.; Yang, C.Y.; Hans, M.G. Clinical Application of Three-Dimensional Craniofacial Imaging in Orthodontics. Journal of Medical Sciences 2005, 25. [Google Scholar]
- Kazimierczak, N.; Kazimierczak, W.; Serafin, Z.; Nowicki, P.; Lemanowicz, A.; Nadolska, K.; Janiszewska-Olszowska, J. Correlation Analysis of Nasal Septum Deviation and Results of AI-Driven Automated 3D Cephalometric Analysis. J Clin Med 2023, 12, 6621. [Google Scholar] [CrossRef]
- Ed-Dhahraouy, M.; Riri, H.; Ezzahmouly, M.; Bourzgui, F.; El Moutaoukkil, A. A New Methodology for Automatic Detection of Reference Points in 3D Cephalometry: A Pilot Study. Int Orthod 2018, 16. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Kharbanda, O.P.; Sardana, V.; Balachandran, R.; Sardana, H.K. A Knowledge-Based Algorithm for Automatic Detection of Cephalometric Landmarks on CBCT Images. Int J Comput Assist Radiol Surg 2015, 10. [Google Scholar] [CrossRef]
- Ma, Q.; Kobayashi, E.; Fan, B.; Nakagawa, K.; Sakuma, I.; Masamune, K.; Suenaga, H. Automatic 3D Landmarking Model Using Patch-Based Deep Neural Networks for CT Image of Oral and Maxillofacial Surgery. International Journal of Medical Robotics and Computer Assisted Surgery 2020, 16. [Google Scholar] [CrossRef] [PubMed]
- Montúfar, J.; Romero, M.; Scougall-Vilchis, R.J. Hybrid Approach for Automatic Cephalometric Landmark Annotation on Cone-Beam Computed Tomography Volumes. American Journal of Orthodontics and Dentofacial Orthopedics 2018, 154. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Kharbanda, O.P.; Sardana, V.; Balachandran, R.; Sardana, H.K. Accuracy of 3D Cephalometric Measurements Based on an Automatic Knowledge-Based Landmark Detection Algorithm. Int J Comput Assist Radiol Surg 2016, 11. [Google Scholar] [CrossRef]
- Kim, M.-J.; Liu, Y.; Oh, S.H.; Ahn, H.-W.; Kim, S.-H.; Nelson, G. Evaluation of a Multi-Stage Convolutional Neural Network-Based Fully Automated Landmark Identification System Using Cone-Beam Computed Tomographysynthesized Posteroanterior Cephalometric Images. Korean J Orthod 2021, 51, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Muraev, A.A.; Tsai, P.; Kibardin, I.; Oborotistov, N.; Shirayeva, T.; Ivanov, S.; Ivanov, S.; Guseynov, N.; Aleshina, O.; Bosykh, Y.; et al. Frontal Cephalometric Landmarking: Humans vs Artificial Neural Networks. Int J Comput Dent 2020, 23. [Google Scholar]
- Bao, H.; Zhang, K.; Yu, C.; Li, H.; Cao, D.; Shu, H.; Liu, L.; Yan, B. Evaluating the Accuracy of Automated Cephalometric Analysis Based on Artificial Intelligence. BMC Oral Health 2023, 23, 191. [Google Scholar] [CrossRef]
- Baccetti, T.; Franchi, L.; McNamara, J.A. The Cervical Vertebral Maturation (CVM) Method for the Assessment of Optimal Treatment Timing in Dentofacial Orthopedics. Semin Orthod 2005, 11. [Google Scholar] [CrossRef]
- McNamara, J.A.; Bookstein, F.L.; Shaughnessy, T.G. Skeletal and Dental Changes Following Functional Regulator Therapy on Class II Patients. Am J Orthod 1985, 88. [Google Scholar] [CrossRef] [PubMed]
- Flores-Mir, C.; Nebbe, B.; Major, P.W. Use of Skeletal Maturation Based on Hand-Wrist Radiographic Analysis as a Predictor of Facial Growth: A Systematic Review. Angle Orthodontist 2004, 74. [Google Scholar]
- Khanagar, S.B.; Al-Ehaideb, A.; Vishwanathaiah, S.; Maganur, P.C.; Patil, S.; Naik, S.; Baeshen, H.A.; Sarode, S.S. Scope and Performance of Artificial Intelligence Technology in Orthodontic Diagnosis, Treatment Planning, and Clinical Decision-Making - A Systematic Review. J Dent Sci 2021, 16. [Google Scholar] [CrossRef]
- Kim, D.W.; Kim, J.; Kim, T.; Kim, T.; Kim, Y.J.; Song, I.S.; Ahn, B.; Choo, J.; Lee, D.Y. Prediction of Hand-Wrist Maturation Stages Based on Cervical Vertebrae Images Using Artificial Intelligence. Orthod Craniofac Res 2021, 24. [Google Scholar] [CrossRef] [PubMed]
- Uysal, T.; Sari, Z.; Ramoglu, S.I.; Basciftci, F.A. Relationships between Dental and Skeletal Maturity in Turkish Subjects. Angle Orthodontist 2004, 74. [Google Scholar] [CrossRef]
- Jourieh, A.; Khan, H.; Mheissen, S.; Assali, M.; Alam, M.K. The Correlation between Dental Stages and Skeletal Maturity Stages. Biomed Res Int 2021, 2021. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.M.; Park, J.H. Correlation of Dental Maturity with Skeletal Maturity from Radiographic Assessment. Journal of Clinical Pediatric Dentistry 2012, 36. [Google Scholar] [CrossRef]
- Szemraj, A.; Wojtaszek-Słomińska, A.; Racka-Pilszak, B. Is the Cervical Vertebral Maturation (CVM) Method Effective Enough to Replace the Hand-Wrist Maturation (HWM) Method in Determining Skeletal Maturation?—A Systematic Review. Eur J Radiol 2018, 102. [Google Scholar] [CrossRef]
- Nguyen, T.; Hermann, A.L.; Ventre, J.; Ducarouge, A.; Pourchot, A.; Marty, V.; Regnard, N.E.; Guermazi, A. High Performance for Bone Age Estimation with an Artificial Intelligence Solution. Diagn Interv Imaging 2023, 104. [Google Scholar] [CrossRef]
- Eng, D.K.; Khandwala, N.B.; Long, J.; Fefferman, N.R.; Lala, S.V.; Strubel, N.A.; Milla, S.S.; Filice, R.W.; Sharp, S.E.; Towbin, A.J.; et al. Artificial Intelligence Algorithm Improves Radiologist Performance in Skeletal Age Assessment: A Prospective Multicenter Randomized Controlled Trial. Radiology 2021, 301. [Google Scholar] [CrossRef] [PubMed]
- Amasya, H.; Cesur, E.; Yıldırım, D.; Orhan, K. Validation of Cervical Vertebral Maturation Stages: Artificial Intelligence vs Human Observer Visual Analysis. American Journal of Orthodontics and Dentofacial Orthopedics 2020, 158. [Google Scholar] [CrossRef]
- Zhou, J.; Zhou, H.; Pu, L.; Gao, Y.; Tang, Z.; Yang, Y.; You, M.; Yang, Z.; Lai, W.; Long, H. Development of an Artificial Intelligence System for the Automatic Evaluation of Cervical Vertebral Maturation Status. Diagnostics 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Mathew, R.; Palatinus, S.; Padala, S.; Alshehri, A.; Awadh, W.; Bhandi, S.; Thomas, J.; Patil, S. Neural Networks for Classification of Cervical Vertebrae Maturation: A Systematic Review. Angle Orthod 2022, 92. [Google Scholar] [CrossRef]
- Radwan, M.T.; Sin, Ç.; Akkaya, N.; Vahdettin, L. Artificial Intelligence-Based Algorithm for Cervical Vertebrae Maturation Stage Assessment. Orthod Craniofac Res 2023, 26. [Google Scholar] [CrossRef]
- Reddy, N.E.; Rayan, J.C.; Annapragada, A.V.; Mahmood, N.F.; Scheslinger, A.E.; Zhang, W.; Kan, J.H. Bone Age Determination Using Only the Index Finger: A Novel Approach Using a Convolutional Neural Network Compared with Human Radiologists. Pediatr Radiol 2020, 50. [Google Scholar] [CrossRef]
- Amasya, H.; Yildirim, D.; Aydogan, T.; Kemaloglu, N.; Orhan, K. Cervical Vertebral Maturation Assessment on Lateral Cephalometric Radiographs Using Artificial Intelligence: Comparison of Machine Learning Classifier Models. Dentomaxillofacial Radiology 2020, 49. [Google Scholar] [CrossRef] [PubMed]
- Rana, S.S.; Nath, B.; Chaudhari, P.K.; Vichare, S. Cervical Vertebral Maturation Assessment Using Various Machine Learning Techniques on Lateral Cephalogram: A Systematic Literature Review. J Oral Biol Craniofac Res 2023, 13. [Google Scholar] [CrossRef] [PubMed]
- Seo, H.; Hwang, J.; Jeong, T.; Shin, J. Comparison of Deep Learning Models for Cervical Vertebral Maturation Stage Classification on Lateral Cephalometric Radiographs. J Clin Med 2021, 10. [Google Scholar] [CrossRef]
- Kök, H.; Acilar, A.M.; İzgi, M.S. Usage and Comparison of Artificial Intelligence Algorithms for Determination of Growth and Development by Cervical Vertebrae Stages in Orthodontics. Prog Orthod 2019, 20. [Google Scholar] [CrossRef]
- Mohammad-Rahimi, H.; Motamadian, S.R.; Nadimi, M.; Hassanzadeh-Samani, S.; Minabi, M.A.S.; Mahmoudinia, E.; Lee, V.Y.; Rohban, M.H. Deep Learning for the Classification of Cervical Maturation Degree and Pubertal Growth Spurts: A Pilot Study. Korean J Orthod 2022, 52. [Google Scholar] [CrossRef]
- Tajmir, S.H.; Lee, H.; Shailam, R.; Gale, H.I.; Nguyen, J.C.; Westra, S.J.; Lim, R.; Yune, S.; Gee, M.S.; Do, S. Artificial Intelligence-Assisted Interpretation of Bone Age Radiographs Improves Accuracy and Decreases Variability. Skeletal Radiol 2019, 48. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.D.; Zhang, J.N.; Gan, Y.H.; Zhou, Y.H. Current Understanding of Pathogenesis and Treatment of TMJ Osteoarthritis. J Dent Res 2015, 94. [Google Scholar] [CrossRef] [PubMed]
- Derwich, M.; Mitus-Kenig, M.; Pawlowska, E. Interdisciplinary Approach to the Temporomandibular Joint Osteoarthritis—Review of the Literature. Medicina (Lithuania) 2020, 56. [Google Scholar] [CrossRef]
- Crincoli, V.; Cortelazzi, R.; De Biase, C.; Cazzolla, A.P.; Campobasso, A.; Dioguardi, M.; Piancino, M.G.; Mattia, L.; Di Comite, M. The Loss of Symmetry in Unilateral Bony Syngnathia: Case Report and Literature Review. Symmetry (Basel) 2022, 14, 2008. [Google Scholar] [CrossRef]
- Andrade, N.N.; Mathai, P.; Aggarwal, N. Facial Asymmetry. In Oral and Maxillofacial Surgery for the Clinician; Springer Nature Singapore: Singapore, 2021; pp. 1549–1576. [Google Scholar]
- Choi, E.; Kim, D.; Lee, J.Y.; Park, H.K. Artificial Intelligence in Detecting Temporomandibular Joint Osteoarthritis on Orthopantomogram. Sci Rep 2021, 11. [Google Scholar] [CrossRef]
- de Dumast, P.; Mirabel, C.; Cevidanes, L.; Ruellas, A.; Yatabe, M.; Ioshida, M.; Ribera, N.T.; Michoud, L.; Gomes, L.; Huang, C.; et al. A Web-Based System for Neural Network Based Classification in Temporomandibular Joint Osteoarthritis. Computerized Medical Imaging and Graphics 2018, 67. [Google Scholar] [CrossRef]
- Bianchi, J.; de Oliveira Ruellas, A.C.; Gonçalves, J.R.; Paniagua, B.; Prieto, J.C.; Styner, M.; Li, T.; Zhu, H.; Sugai, J.; Giannobile, W.; et al. Osteoarthritis of the Temporomandibular Joint Can Be Diagnosed Earlier Using Biomarkers and Machine Learning. Sci Rep 2020, 10. [Google Scholar] [CrossRef]
- Shoukri, B.; Prieto, J.C.; Ruellas, A.; Yatabe, M.; Sugai, J.; Styner, M.; Zhu, H.; Huang, C.; Paniagua, B.; Aronovich, S.; et al. Minimally Invasive Approach for Diagnosing TMJ Osteoarthritis. J Dent Res 2019, 98. [Google Scholar] [CrossRef]
- Ito, S.; Mine, Y.; Yoshimi, Y.; Takeda, S.; Tanaka, A.; Onishi, A.; Peng, T.Y.; Nakamoto, T.; Nagasaki, T.; Kakimoto, N.; et al. Automated Segmentation of Articular Disc of the Temporomandibular Joint on Magnetic Resonance Images Using Deep Learning. Sci Rep 2022, 12. [Google Scholar] [CrossRef]
- Al-Ani, M.H.; Mageet, A.O. Extraction Planning in Orthodontics. Journal of Contemporary Dental Practice 2018, 19. [Google Scholar] [CrossRef]
- Peck, S. Extractions, Retention and Stability: The Search for Orthodontic Truth. Eur J Orthod 2017, 39. [Google Scholar] [CrossRef]
- Del Real, A.; Del Real, O.; Sardina, S.; Oyonarte, R. Use of Automated Artificial Intelligence to Predict the Need for Orthodontic Extractions. Korean J Orthod 2022, 52. [Google Scholar] [CrossRef]
- Ribarevski, R.; Vig, P.; Dryland Vig, K.; Weyant, R.; O’Brien, K. Consistency of Orthodontic Extraction Decisions. Eur J Orthod 1996, 18. [Google Scholar] [CrossRef]
- Proffit, W.R. Forty-Year Review of Extraction Frequencies at a University Orthodontic Clinic. Angle Orthodontist 1994, 64. [Google Scholar] [CrossRef]
- Jackson, T.H.; Guez, C.; Lin, F.C.; Proffit, W.R.; Ko, C.C. Extraction Frequencies at a University Orthodontic Clinic in the 21st Century: Demographic and Diagnostic Factors Affecting the Likelihood of Extraction. American Journal of Orthodontics and Dentofacial Orthopedics 2017, 151. [Google Scholar] [CrossRef]
- Evrard, A.S.; Tepedino, M.; Cattaneo, P.M.; Cornelis, M.A. Which Factors Influence Orthodontists in Their Decision to Extract? A Questionnaire Survey. J Clin Exp Dent 2019, 11. [Google Scholar] [CrossRef]
- Chambers, D.W.; Thakkar, D. Consistency of Orthodontists’ Clinical Decisions: A Systematic Review, Meta-Analysis, and Theory Development. American Journal of Orthodontics and Dentofacial Orthopedics 2022, 161. [Google Scholar] [CrossRef]
- Saghafi, N.; Heaton, L.J.; Bayirli, B.; Turpin, D.L.; Khosravi, R.; Bollen, A.M. Influence of Clinicians’ Experience and Gender on Extraction Decision in Orthodontics. Angle Orthodontist 2017, 87. [Google Scholar] [CrossRef]
- Baumrind, S.; Korn, E.L.; Boyd, R.L.; Maxwell, R. The Decision to Extract: Part 1--Interclinician Agreement. Am J Orthod Dentofacial Orthop 1996, 109. [Google Scholar] [CrossRef]
- Konstantonis, D.; Anthopoulou, C.; Makou, M. Extraction Decision and Identification of Treatment Predictors in Class I Malocclusions. Prog Orthod 2013, 14. [Google Scholar] [CrossRef]
- Evangelista, K.; de Freitas Silva, B.S.; Yamamoto-Silva, F.P.; Valladares-Neto, J.; Silva, M.A.G.; Cevidanes, L.H.S.; de Luca Canto, G.; Massignan, C. Accuracy of Artificial Intelligence for Tooth Extraction Decision-Making in Orthodontics: A Systematic Review and Meta-Analysis. Clin Oral Investig 2022, 26. [Google Scholar] [CrossRef]
- Liu, J.; Chen, Y.; Li, S.; Zhao, Z.; Wu, Z. Machine Learning in Orthodontics: Challenges and Perspectives. Advances in Clinical and Experimental Medicine 2021, 30. [Google Scholar] [CrossRef]
- Choi, H. Il; Jung, S.K.; Baek, S.H.; Lim, W.H.; Ahn, S.J.; Yang, I.H.; Kim, T.W. Artificial Intelligent Model with Neural Network Machine Learning for the Diagnosis of Orthognathic Surgery. Journal of Craniofacial Surgery 2019, 30. [Google Scholar] [CrossRef] [PubMed]
- Takada, K. Artificial Intelligence Expert Systems with Neural Network Machine Learning May Assist Decision-Making for Extractions in Orthodontic Treatment Planning. Journal of Evidence-Based Dental Practice 2016, 16. [Google Scholar] [CrossRef]
- Jung, S.K.; Kim, T.W. New Approach for the Diagnosis of Extractions with Neural Network Machine Learning. American Journal of Orthodontics and Dentofacial Orthopedics 2016, 149. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Kong, D.; Tang, T.; Su, D.; Yang, P.; Wang, H.; Zhao, Z.; Liu, Y. Orthodontic Treatment Planning Based on Artificial Neural Networks. Sci Rep 2019, 9. [Google Scholar] [CrossRef]
- Xie, X.; Wang, L.; Wang, A. Artificial Neural Network Modeling for Deciding If Extractions Are Necessary Prior to Orthodontic Treatment. Angle Orthodontist 2010, 80. [Google Scholar] [CrossRef]
- van Leeuwen, K.G.; de Rooij, M.; Schalekamp, S.; van Ginneken, B.; Rutten, M.J.C.M. How Does Artificial Intelligence in Radiology Improve Efficiency and Health Outcomes? Pediatr Radiol 2022, 52. [Google Scholar] [CrossRef] [PubMed]
- Tolle, K.M.; Tansley, D.S.W.; Hey, A.J.G. The Fourth Paradigm: Data-Intensive Scientific Discovery. In Proceedings of the Proceedings of the IEEE; 2011; Vol. 99.
- Dania, D.; Walter, F.W.; Matthew, P.L.; Tarik, A.; Nina, K.; Bibb, A.; Christopher, J.R.; Bernardo, C.B.; Kimberly, D.; James, A.B.; et al. Implementation of Clinical Artificial Intelligence in Radiology: Who Decides and How? Radiology 2022, 305. [Google Scholar] [CrossRef]
- The Lancet AI in Medicine: Creating a Safe and Equitable Future. The Lancet 2023, 402.
- van Leeuwen, K.G.; Schalekamp, S.; Rutten, M.J.C.M.; van Ginneken, B.; de Rooij, M. Artificial Intelligence in Radiology: 100 Commercially Available Products and Their Scientific Evidence. Eur Radiol 2021, 31. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Simplified AI diagram.
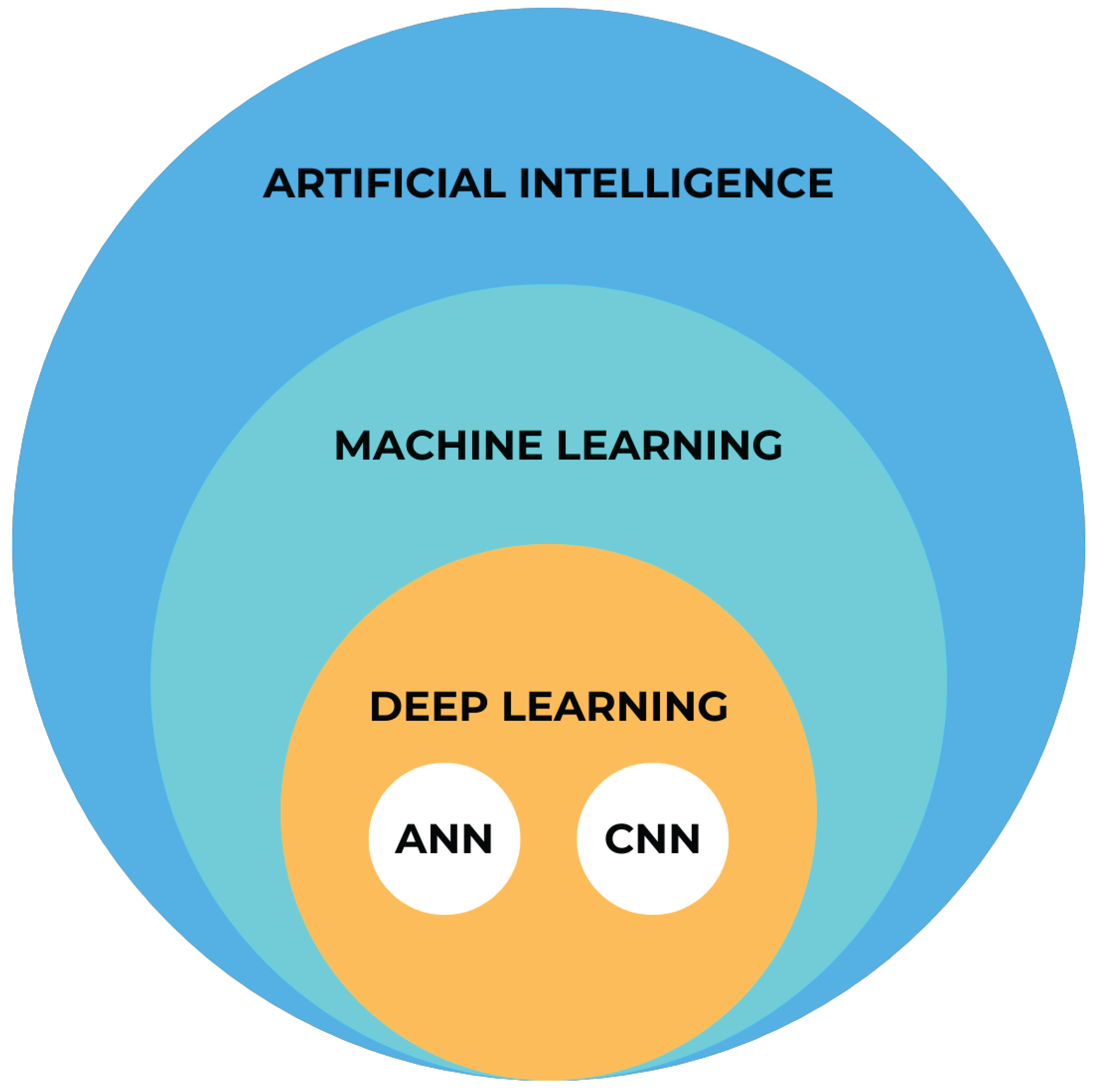
Figure 2.
Part of automatic diagnostic report from a CBCT scan, conducted prior to orthodontic treatment on a 24-year-old male. The software has automatically identified the absence of teeth 18 and 28, as well as changes in the remaining teeth, primarily consisting of attrition and the presence of dental fillings. The program has recommended further consultations as necessary.
Figure 2.
Part of automatic diagnostic report from a CBCT scan, conducted prior to orthodontic treatment on a 24-year-old male. The software has automatically identified the absence of teeth 18 and 28, as well as changes in the remaining teeth, primarily consisting of attrition and the presence of dental fillings. The program has recommended further consultations as necessary.

Figure 3.
Sample of automatic cephalometric landmarks tracings performed by Cephx (A) and WebCeph (B) on 18-year-old male. Results of Downs cephalometric analysis superimposed on tracings (B).
Figure 3.
Sample of automatic cephalometric landmarks tracings performed by Cephx (A) and WebCeph (B) on 18-year-old male. Results of Downs cephalometric analysis superimposed on tracings (B).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



