
Submitted:
15 December 2023
Posted:
18 December 2023
You are already at the latest version
Abstract
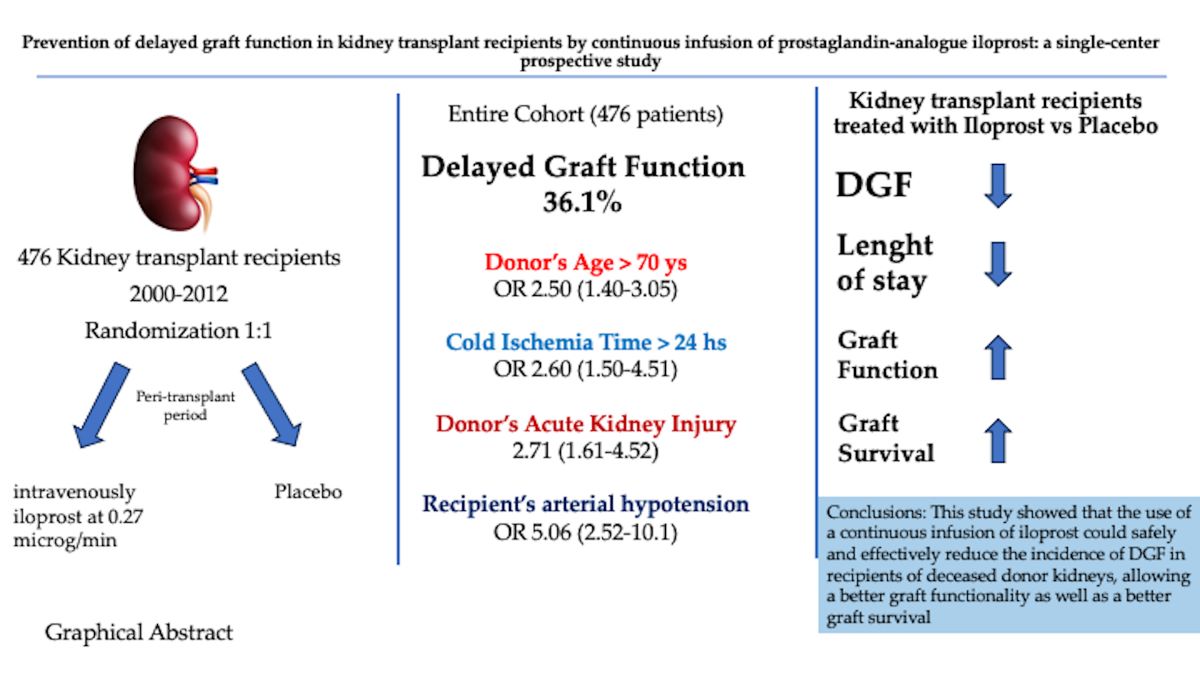
Background: Delayed graft function (DGF) is common after kidney transplantation from de-ceased donor and may significantly affect post-transplant outcomes. This study aimed to evaluating whether an innovative approach, based on the administration of intravenous prostaglandin-analogue iloprost, could be beneficial in reducing the incidence of DGF occurring after kidney transplantation from deceased donors. Methods: This prospective, randomised (1:1), place-bo-controlled study enrolled all consecutive patients who received a kidney transplantation from a deceased donor from January 2000 to December 2012 and who were treated in the peri-transplant period with the prostaglandin-analogue iloprost at 0.27 μg/min through elastomeric pump (treatment group) or placebo (control group). Results: A total of 476 patients were included : DGF was reported in 172 (36.1%) patients in the entire cohort. The multivariate analysis showed that donor’s age > 70 years (OR 2.50, 95% Confidence Interval (CI) 1.40-3.05, p < .001), cold ischemia time > 24 h (OR 2.60, 95 CI 1.50-4.51, p < .001), donor’s AKI (OR 2.71, 95% CI 1.61-4.52, p = .021) and, above all, recipient’s arterial hypotension (OR 5.06, 95% CI 2.52-10.1, p < .0001) were the strongest risk factors for developing post-transplant DGF. The incidence of DGF was 21.4% in the treatment group and 50.9% in the control group (p< .001). Interestingly, among patients who developed DGF, those who received iloprost had a shorter duration of post-transplant DGF (10.58.3 v s13.46.7, days, p= .016). Conclusions: This study showed that the use of a continuous infusion of iloprost could safely and effectively reduce the incidence of DGF in recipients of deceased donor kidneys, allowing a better graft functionality as well as a better graft survival.
Keywords:
Kidney transplantation
; Marginal Donor
; Cold Ischemia Time
; Donor Age
; Acute kidney Injury
; Deceased Donor
; Graft Survival
; Patient Survival
1. Introduction
Kidney transplantation is the best available therapy for end stage renal disease. Recent improvements in short-term survival after kidney transplantation has been observed as a consequence of more effective immunosuppressive agents and improved perioperative management. However, this short-term success has not led to an equal improvement in long-term outcomes [1]. The great disparity between the organs available for kidney transplantation and the number of patients on waiting list, and the progressive increase of donor’s age, has led most transplant centers to expand their acceptance criteria, by including more and more frequently the use of expanded criteria donors, including donors with AKI [2,3,4,5,6]. The absence of immediate function known as delayed graft function (DGF), commonly defined as the need for dialysis during the first week after transplantation, is a well-known risk factor for worse graft function in kidney transplantation [7,8,9,10,11], even in absence of acute rejection [8,11,12]. DGF has an incidence ranging between 10% and 50% of deceased donor kidney transplantations [7,8,10,11,12,13,14,15,16,17], but its incidence may raise to 63% in kidney transplant from marginal donors [18]. The most important risk factors for DGF are older donor’s age, donor’s acute kidney injury, older recipient’s age, and prolonged cold ischemia time [7,8,10,11,12,13,14,15,16,17]. Donor’s age has a clear impact on the incidence of DGF and, therefore, to reduce the incidence of DGF in kidney transplantation from marginal donors, many centers have adopted a policy of local allocation of kidneys to pre-consented candidates, in most cases obviating biopsy, and by reducing the cold ischemia time, lowered the incidence of DGF [19,20]. Animal model of renal ischemia and reperfusion suggests that DGF may have an immunological basis due to an increase in endothelial lymphocyte interaction and resulting vasospasm [9]. So far, different therapeutic modalities have been proposed, ranging from the use of calcium-channel blockers to prostaglandin E1 infusion or non-selective endothelin receptors antagonists, all with debatable results [15,21]. Because of the lack of effective therapies and given the impact on graft survival of delayed graft function, this study evaluated if an innovative approach based on the administration of intravenous prostaglandin-analogue iloprost could be beneficial in reducing the incidence of DGF after kidney transplantation from deceased donors.
2. Results
A total of 476 kidney transplant recipients were collected in the study period.
The mean age was 48.5± 18.5 years with a prevalence of male recipients (301 patients, 63.2%), with a mean BMI of 26.6 Kg/m2. The most frequent cause of end-stage renal disease was autosomal dominant polycystic kidney disease (97 patients, 20.3%), followed by glomerulonephritis (49 patients, 10.2%) and diabetes (24 patients, 5%), while the cause of ESRD was unknown in 169 (35.5%) of patients. Hemodialysis was the most common renal replacement therapy (454 patients, 95.3%), while 8 patients (1.6%) received a pre-emptive kidney transplantation. Mean time on dialysis was 49± 24.3 months, while mean time on the waiting list was 19.4± 12.8 months. In the entire cohort, mean donor age was 50.8± 26.4 years and 186 recipients (39%) received a kidney graft from donors with age > 55 years. A total of 25 donors (5.2%) had diabetes and 150 (31.5%) were hypertensive. Seventy-nine donors (16.5%) had a terminal serum creatinine > 1.5 mg/dl.
Delayed graft function was reported in 172 (36.1%) patients (Table 1).
Univariate analysis showed that kidney transplant recipients who received a kidney graft from a donor with age >70 years, with a cold ischemia > 24 hours and with an acute kidney injury, were at higher risk of developing a delayed graft function. A longer time on the waiting list and a longer time on dialysis were also significant risk factors for DGF. Moreover, recipients aged > 60 years with arterial hypotension were more subjected to develop a post-transplant DGF. Both donor and recipients gender and donor’s use of vasoactive amines and the stay in ICU did not have an impact on the incidence of DGF. The multivariate analysis (Table 2) confirmed that donor’s age > 70 years ( OR 2.06, 95% CI 1.40-3-05, p < .001), cold ischemia time > 24 h ( OR 2.60, 95 CI 1.50-4.51, p < .001), donor’s AKI (OR 2.71, 95% CI 1.61-4.52, p = .021) and , above all, recipient’s arterial hypotension (OR 5.06, 95% CI 2.52-10.1, p < .0001) were the strongest risk factors for developing post-transplant DGF.
The Kaplan-Meier analysis demonstrated a significant better survival among patients with immediate graft function compared with patients who developed a DGF (p < .05) (Figure 1).
A subsequent analysis was performed to evaluate if the intravenous treatment with iloprost could reduce the incidence of DGF compared to placebo: 238 patients in the treatment group and 238 in the control group were included in the analysis (Table 3).
There was no significant difference in term of donor characteristics (age, gender, terminal serum creatinine, incidence of diabetes and arterial hypertension, stay in ICU and cause of brain death) between the two groups, but the treatment group had a longer cold ischemia time. Recipient’s characteristics (age, gender, time on dialysis, rate of primary non function and acute rejection) and type of immunosuppression were similar between the two groups, but recipients in the treatment group had a longer time on the waiting list (23.9±21 vs 15±12 months, p < .001) compared with control group.
The incidence of DGF was 21.4% in the treatment group and 50.9% in the control group (p< .001), suggesting that the use of iloprost could significantly reduce the incidence of such a complication. The use of iloprost was well tolerated and only four patients (1.6%) required a treatment discontinuation: two patients reported flushing and headache, while in two patients the treatment was stopped due to severe arterial hypotension. Interestingly, among patients who developed DGF, patients receiving iloprost had a shorter duration of post-transplant DGF (10.5±8.3 v s13.4±6.7, days, p= .016)
Patients in the treatment group had a significant lower hospital stay (10.5±4.4 vs 13.3±6.4, p <.05) and a better 1-y (1.41±0.61 vs 1.60±0.65 mg/dL, p=.008) and 5-y (1.50±0.62 vs 1.66±0.81mg/dL, p= .045) serum creatine, but 10-y serum creatinine was similar between the two groups. One-year (93.3% vs 88%, p < .05) and 5-y (83% vs 79%, p < .05) graft survival was significantly better in treatment group compared with controls, respectively. One-year, 5-y and 10-y patient survival was similar between the two groups.
3. Discussion
This prospective study showed that the use of prostaglandin-analogue iloprost was safely and effectively in reducing the incidence of DGF in kidney transplant recipients, by acting on its development mechanisms. Delayed graft function is still a common complication after kidney transplantation and the increasing donor’s and recipient’s age observed in the last decade may render transplant programs reluctant to utilize kidneys at higher risk of developing DGF. The full mechanism of DGF is not still clear in detail. The tubular damage resulting from ischemia/reperfusion injury seems the basis of the decreased glomerular impairment of DGF. Tubular epithelial cell degeneration, tubular cell exfoliation, interstitial edema, and interstitial cellular infiltration may cause, in the early phase, a tubular obstruction, resulting in a low net filtration pressure. Later, decreased sodium reabsorption results in afferent vasoconstriction and diminished glomerular filtration pressure through the tubuloglomerular feedback mechanism [6,10,15]. A recent meta-analysis showed [10] that DGF is associated with significantly worse short- and long-term outcomes posttransplant, including increased graft failure (OR 3.38; 95% CI, 1.85-6.17; P < 0.01), acute allograft rejection (OR 1.84; 95% CI, 1.30-2.61; P < 0.01) and, in single-center studies, 1-y mortality. Moreover, kidney transplant recipients who experienced DGF had an overall reduction of 5.46 mL/min in eGFR at 1-y posttransplant compared with those who did not experience DGF. Several studies suggested that the presence of DGF implies a poor outcome, and this could be amplified when receiving a kidney from a marginal donor, suggesting that the effect donor-dependent damage may be amplified by the ischemia reperfusion injury [9]. This was confirmed in this study: overall incidence of DGF in this cohort was 36.1% and the incidence of DGF was higher in patients receiving an older graft with a long ischemia time and with kidney injury, suggesting that these grafts may be more vulnerable to the ischemia-reperfusion injury, which may further reduce the nephron mass. The multivariate analysis further demonstrated that donor’s age > 70 years ( OR 2.06, 95% CI 1.40-3-05, p < .001), cold ischemia time > 24 h ( OR 2.60, 95 CI 1.50-4.51, p < .001) and donor’s AKI (OR 2.71, 95% CI 1.61-4.52, p = .021) were significantly associated with an increased risk of developing a DGF. Interestingly, the recipient’s hypotension, especially when receiving a kidney from a hypertensive donor, is an independent risk factor for DGF (OR 5.06, 95% CI 2.52-10.1, p < .0001). Indeed, hypertensive marginal donors present frequently atherosclerotic stenosis of the renal arteries, so that a low mean arterial pressure in the recipient could not be able to ensure a stable and viable perfusion of the graft, amplifying the ischaemic damage of the ischemia/reperfusion injury. Therefore, a special care must be taken in the allocation of marginal kidneys from hypertensive donors, by avoiding, if feasible, recipients with a low mean arterial pressure. DGF may, alternatively, through an increased expression of MHC antigen, determine an inflammatory response, with release of pro-inflammatory cytokines in tubular cells, which may finally contribute to an increased rate of rejection in ischaemically injured kidneys [15], and this may reflect a worse outcome [10,29,30]. In this regard, it has been shown in an experimental model [31] that the development of ischemia-reperfusion injury is closely related to cold preservation which may increase vasoconstriction, and that the addiction of anti-ischemic drugs, may prevent renal injury and had a significant beneficial effect in the renal function. The prostaglandin I2- stable analogue iloprost has been approved for therapy of lower-limb critical ischemia secondary to peripheral obliterative disease [25], and it exhibits a protective effect from renal ischemia-reperfusion injury in rabbit models [32,33]. The ischemia/reperfusion injury results in the release of free radicals and induces increase in renal tissue levels of tumor necrosis factor alpha and cytokine-induced neutrophil chemoattractant. This may lead to an activated neutrophil –induced endothelial cell injury which finally might lead to ischemia of the proximal tubules [6,15]. Iloprost has demonstrated cytoprotective properties by inhibiting intracellular lysosome distribution, which is implicated in membrane destabilization and release of free radicals [34,35]. Moreover, Iloprost, by inhibiting platelet aggregation, oxygen-free radical production and neutrophil activation could improve the ischemia reperfusion- induced injury by improving renal microcirculation [32,33]. In clinical settings, iloprost failed to improve cyclosporin-induced renal hypoperfusion in stable renal transplant recipients [36], but in a prospective randomized trial in association with diltiazem, iloprost determined a reduction of delayed graft function in cadaveric kidney transplants [34]. This prospective study confers some new insights: first, it was conducted on a selected population of deceased donor kidneys recipients; second, this is the first study in which iloprost was administered in a continuous IV infusion way through an elastomeric pump, so that the drug may have consistent and prolonged action throughout the entire 24-hour period.
The rationale of this study was that by inducing a vasodilatation of micro- and macrocirculation of the renal vasculature, we might reduce the ischemical damage resulting from the ischemia/reperfusion injury. The results of this study seem confirm such an assumption, because the incidence of DGF was significantly reduced in kidney transplant recipients who received iloprost compared with controls (21.4% vs 50.9%, respectively, p< .001). This aspect is particularly useful when transplanting kidneys from marginal donors, in whom DGF is associated with a more complicated postoperative management and, finally, with a worse outcome [9,10,11]. The treatment with iloprost resulted in a significant shorter hospital stay (10.5±4.4 vs 13.3±6.4, p <.05) and a significant better 1-y (1.41±0.61 vs 1.60±0.65 mg/dL, p=.008) and 5-y (1.50±0.62 vs 1.66±0.81mg/dL, p= .045) graft function compared with patients who received placebo. Interestingly, among patients who developed a DGF after transplantation, patients treated with iloprost had a significant shorted duration of post-transplant DGF, suggesting that iloprost could have a beneficial effect in the repair mechanism after ischemia-reperfusion injury, since graft survival and rate of acute rejection may be linked to the duration of DGF [8]. Patients treated with iloprost had a significant better 1-y and 5-y graft survival compared with control group, confirming that prevention of DGF may have a beneficial effect on graft survival [10,11,36]. This study has some limitation: data were analyzed retrospectively, but the study was performed in a prospective fashion, so that this is one of the largest studies evaluating the long-term impact of DGF on post-transplant outcomes; second, the two groups were not completely matched and this may cause differences in data analysis. In conclusion, this study suggested that iloprost could safely reduce the incidence of delayed graft function in recipients of deceased donor kidneys. This would reflect in a better graft functionality and a better graft survival. To further reduce the incidence of delayed graft function, some risk factors, such as prolonged cold ischemia time and low recipient’s mean arterial pressure should be minimised through a better allocation of deceased donor kidneys.
4. Materials and Methods
4.1. Study population
In this prospective, randomised (1:1), placebo-controlled study we evaluated retrospectively the incidence of DGF and the long-term outcomes in a cohort of consecutive patients who received a kidney transplantation from a deceased donor and who were treated in the peri-transplant period with the prostaglandin analogue iloprost (Italfarmaco, Milan, Italy) (Treatment Group) or placebo (Control Group). Delayed graft function was defined as the need for at least one dialysis session within one week after transplantation [10,11]. Primary kidney nonfunction was defined as the complete lack of functionality, so that recipient never discontinued dialysis sessions after transplantation.
This study was approved by the Local Ethic Committee of the Azienda Policlinico San Marco of the University of Catania, and the patients provided written informed consent to undergo renal transplantation and participate in this protocol. Marginal donors were identified based on one or more of the following characteristics: age>60 years, history of long – standing (> 10 years) diabetes and/or hypertension, terminal serum creatinine > 2 mg/dl [22]. All kidneys > 70 years have been histologically evaluated through a tissue sample obtained from the superior pole of each donor’s kidney. Kidneys from which a biopsy specimen was obtained were selected and allocated based on severity of chronic changes, which was quantified by a predefined histologic score [3]. In brief, all changes in each evaluated component of the kidney tissue (vessels, glomeruli, tubules, and connective tissue) received a score ranging from 0 to 3. Each received a score of 0 if no changes were observed and a score of up to three if marked changes were present. Kidney with a global score ranging from 0 to 3 were considered for use as a single transplant and those with a score from 4 to 6 for use as a dual transplant; those with a score of 7 or greater were discarded [3]. Kidney transplantations were performed by the same surgical team with a standardised surgical procedure, as previously described [23]. A total of 476 consecutive patients, who underwent a kidney transplantation from deceased donor between January 2000 and December 2012, met the inclusion criteria and were prospectively randomized on 1:1 basis at the time of transplantation. A central venous line was placed in all patients at the time of surgery and was removed on the seventh postoperative day. Anaesthesiological protocol was standardized for all patients: anaesthesia was induced with propofol 2 mg*kg-1, fentanil 1.5 mcg*kg-1 and cisatracurium 2 mg*kg-1; after tracheal intubation anaesthesia was maintained with cisatracurium and fentanil on demand and sevoflurane 1-1.5 MAC; all patients received the same amount and type of infused fluids (emagel 500 ml followed by saline 1000 ml and 5% glucose up to monorenal phase), calculated as 10 ml*kg-1*h-1 starting immediately after the central venous line placement [24]. Patients in the treatment group received intravenously iloprost at 0.27 microg/min through an elastomeric pump, as previously described [25], beginning from oro-tracheal intubation of the patients, while patients in the control group received saline solution. The infusion of iloprost was continued for 72 hours in patients without DGF, while in patients with DGF it was maintained until the restoration of renal function, defined as the discontinuation of dialysis treatment. Acute kidney injury in the kidney donor was defined as ≥50% increase in the last serum creatinine level from the level of the day of admission [26,27]. Recipient hypotension was defined as the presence of a systolic arterial pressure < 100 mmHg at the time of admission for the kidney transplantation. Rephractory hypotension was treated with extra colloids and dobutamine infusion titrated to effect, as previously reported [24]. Both patients in treatment group and control group received 100 mg of furosemide at the time of reperfusion. In the immunosuppression protocol, all patients received a dose of 750 mg of prednisolone (STER) at the time of transplant and then at a dose of 1 mg/Kg per day, which was slowly tapered to a maintenance dose of 5 mg/day by the end of the sixth month. Mycophenolate mofetil (MMF) was given at a dose of 1 to 2 g/day. For patients receiving tacrolimus-based immunosuppression, tacrolimus (TAC) was initiated at 0.1 mg/Kg/die and doses were adjusted to keep levels between 10 and 12 ng/mL in the first month post-transplant and then between 8 and 10 ng/mL. For recipients receiving cyclosporine-based immunosuppression, cyclosporine (CyA) was started 2 days after operation at 5 mg/kg/die and doses were adjusted to keep levels at 200-220 ng/mL for the first three months after the transplant, then at 150 to 200 ng/mL between 3 and 6 months after the transplant, and more than 140 ng/mL thereafter. Sirolimus (SIR) was initiated at 5-6 mg beginning within day 5 post-transplant and doses were adjusted to keep levels between 8 and 12 ng/ml. Everolimus (EVE) was initiated at 1.5 mg beginning from the 3rd day after transplantation and doses were adjusted to keep levels between 5 and 7 ng/mL.
In all patients in whom an acute rejection was suspected on the basis of graft sonography appearance of worsening of graft function, a graft biopsy was obtained, and the rejection scored according to the Banff classification [28]. Rejection therapy consisted in steroid pulses of 500 mg of methylprednisolone for three days.
4.2. Statistical analysis
This study included all recipients of deceased donor kidneys recruited over a 12-year period. Characteristics at the time of transplant of the entire cohort were compared with the use of Fisher’s exact test, the chi-square test and Student t test. The primary analysis was a comparison of incidence of delayed graft function between recipients treated with an intravenously infusion of iloprost and a group of recipients as control group. Primary end-point (delayed graft function) and secondary end points were evaluated with the use of a Cox regression model that included donor’s age, terminal serum donor’s creatinine, donor’s hemodynamic parameters (stay in ICU, presence of hypotension, presence of acute kidney injury (AKI)), donor-recipient arterial pressure match, recipient age, and rate of acute rejection. Data are expressed as mean ± standard deviation (SD). To compare parametric variables, the Pearson chi-square test or Fisher’s exact test was used. To compare nonparametric variables, the Student’s t-test or Mann–Whitney U test was used. The difference between the two means was calculated using the Wilson test. Odds ratios (OR) were reported with a 95% confidence interval (95% CI) and P-values. The level of statistical significance was determined at p < 0.05. Predictive factors of DGF with a p-value < 0.5 in univariate analysis were considered for the multivariate model using a downward stepwise binary logistic regression analysis. Rates of graft survival, censored for death, were plotted with the Kaplan Meier method. Statistical analyses were performed with SAS software, and Microsoft Excel 2021.
Author Contributions
Conceptualization, M.V, P.V, and M.S.; methodology, P.V, M.S and M.V.; formal analysis, F.S., G.R., A.G., M.G., G.R., D.Z, and M.V.; investigation, F.S., P.V., R.G.,M.S. and M.V.; data curation, F.S., G.R., D.Z; writing—original draft preparation, P.V and M.V.; writing—review and editing, M.V. All authors have read and agreed to the published version of the manuscript.
Funding
The acknowledged funders/supporters played no role in the study design, collection, analysis, interpretation of data, manuscript writing, or decision to submit the report for publication. This study was funded by the School of General Surgery of the University of Catania.
Institutional Review Board Statement
The study was conducted in accordance with the principles of the 1975 Declaration of Helsinki and the Ethical Committee of the University Hospital of Catania ruled approved this study (CT 115-2011).
Informed Consent Statement
All patients signed an informed consent detailing all the proce-dures.
Data Availability Statement
De-identified data can be made available upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Meier-Kriesche, H.U.; Schold, J.D.; Srinivas, T.R.; Kaplan B. Lack of improvement in renal allograft survival despite a marked decrease in acute rejection rates over the most recent era. Am J Transplant 2004; 4(3),378-83. [CrossRef]
- Stratta, R.J.; Rohr, M.S.; Sundberg, A.K.; Armstrong, G.; Hairston, G.; Hartmenn, E.; Farney, A.C.; Roskopf, J.; Iskandar, S.S.; Adams, P.L. Increased kidney transplantation utilizing expanded criteria deceased organ donors with results comparable to standard criteria donor transplant. Ann Surg, 2004; 239, 688-695. [CrossRef]
- Remuzzi, G.; Cravedi, P.; Perna, A.; Dimitrov, B.; Turturro, M.; Locatelli, G.; Rigotti, P.; Baldan, N.; Betaini, M.; Valente, U.; Scalamogna, M.; Ruggenenti P. Long-term outcome of renal transplantation from older donors. N Engl J Med 2006; 354, 343-52. [CrossRef]
- Veroux, P.; Veroux, M.; Puliatti, C.; Valastro, M.; Di Mare, M.; Gagliano, M.; Macarone, M.; Cappello, D.; Spataro, M.; Giuffrida G. Kidney transplantation from cadaveric donors unsuitable for other centers and older than 60 years of age. Transplant Proc. 2005, 37:2451-2453. [CrossRef]
- Mesnard, B.; Territo, A.; Campi, R.; Hevia, V.; Andras, I.; Piana, A.; Pecoraro, A.; Boissier, R.; Prudhomme, T.; EAU-Young Academic Urologist (YAU) group of Kidney Transplantation. Kidney transplantation from elderly donors (> 70 years): a systematic review. World J Urol. 2023, 41(3),695-707. [CrossRef]
- Corona, D.; Ekser, B.; Gioco, R.; Caruso, M.; Schipa, C.; Veroux, P.; Giaquinta, A.; Granata, A.; Veroux M. Heme-Oxygenase and Kidney Transplantation: A Potential for Target Therapy? Biomolecules. 2020, 10(6):840. [CrossRef]
- Cooper, M.; Wiseman, A.C.; Doshi, M.D.; Hall, I.E.; Parsons, R.F.; Pastan, S.; Reddy, K.S.; Schold, J.D.; Mohan, S.; Hippen, B.E. Understanding Delayed Graft Function to Improve Organ Utilization and Patient Outcomes: Report of a Scientific Workshop Sponsored by the National Kidney Foundation. Am J KidneyDis. 2023 S0272-6386(23)00860-0. [CrossRef]
- Schrezenmeier, E.; Müller, M.; Friedersdorff, F.; Khadzhynov, D.; Halleck, F.; Staeck, O.; Dürr, M.; Zhang, K.; Eckardt, K.U.; Budde, K.; Lehner, L.J. Evaluation of severity of delayed graft function in kidney transplant recipients. Nephrol Dial Transplant. 2022 , 37(5):973-981. [CrossRef]
- Lapointe, I.; Lachance, J.G.; Noël, R.; Côté, I.; Caumartin, Y.; Agharazii, M.; Houde, I.; Rousseau-Gagnon, M.; Kim, S.J.; De Serres, S.A. Impact of donor age on long-term outcomes after delayed graft function: 10-year follow-up. Transpl Int. 2013, 26(2):162-9. [CrossRef]
- Li, M.T.; Ramakrishnan, A.; Yu, M.; Daniel, E.; Sandra, V.; Sanichar, N.; King, K.L.; Stevens, J.S.; Husain, S.A.; Mohan, S. Effects of Delayed Graft Function on Transplant Outcomes: A Meta-analysis. Transplant Direct. 2023, 9(2):e1433. [CrossRef]
- Swanson, K.J.; Bhattarai, M.; Parajuli, S. Delayed graft function: current status and future directions. Curr Opin Organ Transplant. 2023,28(1):1-7. [CrossRef]
- Feldman, H.I.; Gayner, R.; Berlin, J.A.; Roth, D.A.; Silibovsky, R.; Kushner, S.; Brayman, K.L.; Burns, J.E.; Kobrin, S.M.; Friedman, A.L.; Grossman, R.A.. Delayed graft function reduces renal allograft survival independent of acute rejection. Nephrol Dial Transplant 1996; 11: 1306-1313. [CrossRef]
- Heylen, L.; Pirenne, J.; Naesens, M.; Sprangers, B.; Jochmans, I. "Time is tissue"-A minireview on the importance of donor nephrectomy, donor hepatectomy, and implantation times in kidney and liver transplantation. Am J Transplant. 2021, 21(8):2653-2661. [CrossRef]
- Quiroga, I.; Mcshane, P.; Koo, D.D.; Gray, D.; Friend, P.J.; Fuggle, S.; Darby, C. Major effects of delayed graft function and cold ischemia time on renal allograft survival. Nephrol Dial Transplant 2006; 21: 1689-96.
- Perico, N.; Cattaneo, D.; Sayegh, M.H.; Remuzzi, G. Delayed graft function in kidney transplantation. Lancet 2004; 364:1814-27. [CrossRef]
- Ponticelli, C.; Reggiani, F.; Moroni, G. Delayed Graft Function in Kidney Transplant: Risk Factors, Consequences and Prevention Strategies. J Pers Med. 2022, 12(10):1557. [CrossRef]
- Salguero, J.; Chamorro, L.; Gómez-Gómez, E.; de Benito, P.; Robles, J.E.; Campos, J.P. Kidney Survival Impact of Delayed Graft Function Depends on Kidney Donor Risk Index: A Single-Center Cohort Study. J Clin Med. 2023 12(19):6397. [CrossRef]
- Dahmane, D.; Audard, V.; Hiesse, C.; Pessione, F.; Bentaarit, B.; Barrou, B.; Rondeau, E.; Cohen, S.; Lang, P.; Grimbert, P. Retrospective follow-up of transplantation of kidney from marginal donors. Kidney Int 2006; 69: 546-532. [CrossRef]
- Carter, J.T.; Chan, S.; Roberts, J.P.; Feng, S. Expanded criteria donor kidney allocation: marked decrease in cold ischemia and delayed graft function at a single center. Am J Transplant 2005; 5, 2745-53. [CrossRef]
- Vacher-Coponat, H.; Purgus, R.; Indreis, M.; Moal, V.; Luciani, H.; Lechevallier, E.; Delaporte, V.; Luccioni, A.; Julian, H.; Reviron, D.; Dussol, B.; Berland, Y. Cold ischemia time in renal transplantation is reduced by a timesheet in a French transplant center. Transplantation 2007, 83, 561-55. [CrossRef]
- Hollenbeck, M.; Dinter, K.; Torsello, G.; Kock, M.; Willers, R.; Sandmann, W.; Grabensee, B. Prostaglandin E1 reduces the risk of delayed graft function after cadaveric renal transplantation. Nephrol Dial Transplant 1999, 14(suppl.4), 32-33. [CrossRef]
- Port, F.K.; Bragg-Gresham, J.L.; Metzger, R.A.; Dykstra, D.M.; Gillespie, B.W.; Young, E.W.; Delmonico, F.L.; Wynn, J.J.; Merion, R.M.; Wolfe, R.A.; Held, P.J. Donor characteristics associated with reduced graft survival: an approach to expanding the pool of kidney donors. Transplantation. 2002 74(9), 1281-1286. [CrossRef]
- Veroux, M.; Zerbo, D.; Basile, G.; Gozzo, C.; Sinagra, N.; Giaquinta, A.; Sanfiorenzo, A.; Veroux, P. Simultaneous Native Nephrectomy and Kidney Transplantation in Patients With Autosomal Dominant Polycystic Kidney Disease. PLoS One. 2016 11(6):e0155481. [CrossRef]
- Cavaleri, M.; Veroux, M.; Palermo, F.; Vasile, F.; Mineri, M.; Palumbo, J.; Salemi, L.; Astuto, M.; Murabito, P. Perioperative Goal-Directed Therapy during Kidney Transplantation: An Impact Evaluation on the Major Postoperative Complications. J Clin Med. 2019, 8(1), 80. [CrossRef]
- Veroux, P.; Veroux, M.; Macarone, M.; Bonanno, M.G.; Tumminelli, M.G. Efficacy of a novel method of intravenous infusion of the prostaglandin analogue iloprost for the treatment of lower-limb critical ischemia:an open-label, nonrandomized study in two cohorts. Curr Ther Res 2004, 65, 255-265. [CrossRef]
- Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012;120(4),c179-84. [CrossRef]
- Nita, G.E.; Gopal, J.P.; Khambalia, H.A.; Moinuddin, Z.; van Dellen, D. Kidney Transplantation From Donors With Acute Kidney Injury: Are the Concerns Justified? A Systematic Review and Meta-Analysis. Transpl Int. 2023, 36:11232. [CrossRef]
- Haas, M.;Loupy, A.; Lefaucheur C.; Roufosse, C.; Glotz, D.; Seron, D.; Nankivell, B.J.; Halloran, P.F.; Colvin, R.B.; Akalin, E.; Alachkar, N.; Bagnasco, S.; Bouatou, Y.; Becker, J.U.; Cornell, L.D.; Duong van Huyen, J.P.; Gibson, I.W.; Kraus, E.S.; Mannon, R.B.; Naesens, M.; Nickeleit, V.; Nickerson, P.; Segev, D.L.; Singh, H.K.; Stegall, M.; Randhawa, P.; Racusen, L.; Solez, K.; Mengel, M. The Banff 2017 Kidney Meeting Report: revised diagnostic criteria for chronic active T cell-mediated rejection, antibody-mediated rejection, and prospects for integrative end points for next-generation clinical trials. Am J Transplant 2018,18, 293–307. [CrossRef]
- Fernández, A.R.; Sánchez-Tarjuelo, R.; Cravedi, P.; Ochando, J.; López-Hoyos, M. Review: Ischemia Reperfusion Injury-A Translational Perspective in Organ Transplantation. Int J Mol Sci. 2020 21(22),8549. [CrossRef]
- Browne, B.J.; Holt, C.O.; Emovon, O.E. Delayed graft function may not adversely affect short-term renal allograft outcome. Clin Transplant 2003; 17 suppl 9: 35-8. [CrossRef]
- Hauet, T.; Goujon, J.M.; Vandewalle, A.; Baumert, H.; Lacoste, L.; Tillement, J.P.; Eugene, M.; Carretier, M. Trimetazidine reduces renal dysfunction by limiting the cold ischemia/reperfusion injury in autotransplanted pig kidneys. J Am Soc Nephrol. 2000, 11(1), 138-148. [CrossRef]
- Emrecan, B.; Tulukoglu, E.; Bozok, S.; Kestelli, M.; Onem, G.; Küpelioglu, A.; Yagdi, S.; Gürbüz, A. Effects of iloprost and pentoxifylline in renal ischemia reperfusion in rabbit model. Eur J Med Res 2006, 11, 295-299.
- Aytacoglu, B.N.; Sucu, N.; Tamer, L.; Polat, A.; Gul, A.; Degirmenci, U.; Mavioglu, I.; Dikmengil, M. Iloprost for the attenuation of ischaemia/reperfusion injury in a distant organ. Cell Biochem Funct 2006, 24, 341-346. [CrossRef]
- Neumayer, H.H.; Schreiber, M.; Wagner, K. Prevention of delayed graft function in cadaveric kidney transplants by the calcium antagonist diltiazem and the prostacyclin-analogue iloprost. Outcome of a prospective randomized clinical trial. Prog Clin Biol Res 1989, 301, 289-295.
- Kassis, H.M.; Minsinger, K.D.; McCullough, P.A.; Block, C.A.; Sidhu, M.S.; Brown, J.R. A Review of the Use of Iloprost, A Synthetic Prostacyclin, in the Prevention of Radiocontrast Nephropathy in Patients Undergoing Coronary Angiography and Intervention. Clin Cardiol. 2015, 38(8), 492-8. [CrossRef]
- Hansen, J.M.; Christensen, N.J.; Fogh-Andersen, N.; Strandgaard, S. Effects of the prostacyclin analogue iloprost on cyclosporine-induced renal hypoperfusion in stable renal transplant recipients. Nephrol Dial Transplant 1996, 11, 340-346. [CrossRef]
- Grosso, G.; Corona, D.; Mistretta, A.; Zerbo, D.; Sinagra, N.; Giaquinta, A.; Cimino, S.; Ekser, B.; Giuffrida, G.; Leonardi, A.; Gula, R.; Veroux, P.; Veroux, M. Delayed graft function and long-term outcome in kidney transplantation. Transplant Proc. 2012, 44(7), 1879-83. [CrossRef]
Figure 1.
Kaplan-Meier analysis demonstrated a worse graft survival in patients with delayed graft function compared to patients with immediate graft function.
Figure 1.
Kaplan-Meier analysis demonstrated a worse graft survival in patients with delayed graft function compared to patients with immediate graft function.
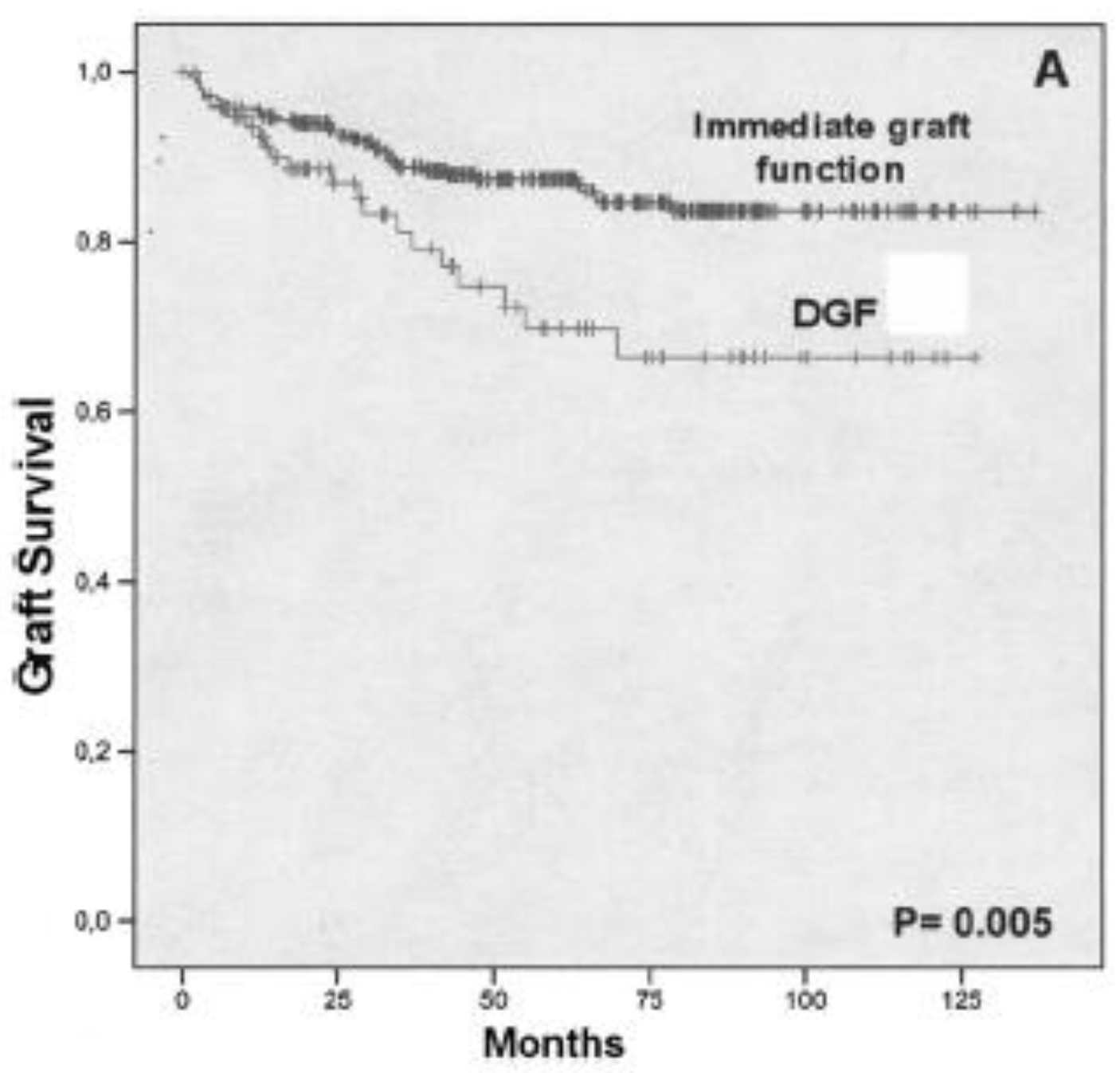

Table 1.
Univariate analysis for the risk factor for delayed graft function in the entire cohort.
| DGF (n=172) |
No DGF (n=304) |
P value | |
|---|---|---|---|
| Mean Donor’s age (yr) | 57.2±15.8 | 47.1±18.8 | <.001 |
| Donor’s age | |||
| <55 years | 76 (44.1) | 191 (62.8) | .032 |
| 66-70 years | 49 (28.4) | 77 (25.3) | .543 |
| > 70 years | 47 (27.3) | 36 (11.8) | <.001 |
| Donors with AKI | 41 (23.8) | 38 (12.5) | .001 |
| Female Donor | 75 (43.6) | 155 (50.9) | .121 |
| Use of vasopressors | 165(95.9) | 285 (93.7) | .744 |
| Stay in ICU | 5.4±4.0 | 4.9±3.9 | .251 |
| Mean Cold Ischemia time (min) | 1070±450 | 882±331 | <.001 |
| Cold ischemia time | |||
| < 24 hours | 132 (76.7) | 270 (88.9) | .635 |
| > 24 hours | 40 (23.3) | 34 (11.1) | < .001 |
| Recipient’s age | 52.9±11.4 | 46.0±11.9 | < .001 |
| Male recipients (%) | 110(63.9) | 193(63.4) | .884 |
| Recipient’s Hypotension | 30 (17.4) | 12 (3.9) | <.001 |
| Waiting list (months) | 24.4±21.2 | 16.5±14.4 | .001 |
| Time on dialysis (months) | 65.0±50.8 | 39.9±32.7 | < .001 |
Table 2.
Multivariate analysis for the incidence of delayed graft function.
| Characteristics | OR | 95% CI | P value |
|---|---|---|---|
| Donor age | |||
| Donor age < 70 years | reference | ||
| Donors age > 70 years | 2.50 | 1.40-3.05 | <.001 |
| Cold ischemia time | |||
| < 24 h | reference | ||
| >24 h | 2.60 | 1.50-4.51 | < .001 |
| Donors with AKI | 2.71 | 1.61-4.52 | .021 |
| Time on dialysis | |||
| < 12 months | reference | ||
| 12-24 months | 1.01 | 0.66-1.56 | .908 |
| >24 months | 2.87 | 1.91-4.33 | < .001 |
| Recipient age > 60 ys | 3.39 | 2.14-5.38 | < .001 |
| Recipient’s hypotension | 5.06 | 2.52 – 10.1 | < .001 |
Table 3.
Clinical characteristics and comparison between the recipients who received iloprost (n=238) and the control group (n=238).
Table 3.
Clinical characteristics and comparison between the recipients who received iloprost (n=238) and the control group (n=238).
| Group and characteristics | Treatment group (N=238) | Control Group (N=238) | P value |
|---|---|---|---|
| Donor | |||
| Age (yr) | 50.9 ± 20.4 | 50.7± 19.8 | .845 |
| Male Sex (%) | 91 (38.2) | 69 (28.9) | .032 |
| Terminal Serum Creatinine (mg/dl) | 1.13 ± 0.3 | 1.11 ± 0.3 | .532 |
| Use of vasoactive amines (%) | 200 (84%) | 203 (85.2) | .624 |
| Diabetes (%) | 18 (7.5) | 13 (5.4) | .223 |
| Arterial Hypertension > 10 ys (%) | 95 (39.9) | 92 (38.6) | .498 |
| Cold Ischemia Time (hr) | 17.3±7.4 | 13.8±6.2 | <.001 |
| Cerebral haemorrhage/ischemia brain death (%) | 141 (59.2) | 158 (66.3) | .147 |
| Non traumatic brain death (%) | 93 (39) | 78 (32.7) | .122 |
| Other cause of brain death | 4 (1.6) | 2 (0.8) | .554 |
| Use of vasoamine drugs | 225 (94.5) | 228 (95.7) | .922 |
| Stay in ICU | 4.9±3.8 | 5.3±4.2 | .279 |
| Recipient | |||
| Age (yr) | 49±11.1 | 47.9±12 | .324 |
| Male sex (%) | 159 (66.8) | 142 (59.6) | .424 |
| Time on Dialysis (mo) | 50±23.4 | 47.1±26.2 | .113 |
| Time on waiting list (mo) | 23.9±33 | 15±16 | < .001 |
| Peritoneal dialysis (%) | 5 (2.1) | 9 (3.7) | .433 |
| Dual transplant (%) | 17 (7.1) | 11 (4.6) | .115 |
| HCV seropositivity | 36 (15.1) | 11(4.6) | <.05 |
| Delayed graft function (%) | 51 (21.4) | 121 (50.9) | < .001 |
| Discontinuation of dialysis (dy) | 10.5±8.3 | 13.4±6.7 | .016 |
| Primary Non Function (%) | 6 (2.5%) | 6(2.5%) | 1 |
| Acute rejection | 16 (6.7) | 25 (10.5) | .141 |
| Immunosuppression | |||
| Induction (basiliximab) | 68 (28.5) | 55 (23.1) | .753 |
| Induction (thymoglobuline) | 22 (9.2) | 24 (10) | .883 |
| Tacrolimus | 150 (63) | 164 (68.9) | .214 |
| MMF | 205 (86.1) | 185 (77.7) | .301 |
| Sirolimus | 36 (15.1) | 26 (10.9) | .112 |
| Cyclosporine | 29 (12.1) | 55 (23.1) | .108 |
| Everolimus | 14 (5.8) | 19 (7.9) | .323 |
| Hospital stay | 10.5±4.4 | 13.3±6.4 | <.05 |
| 30-day acute rejection | 22 (9.2) | 25 (10.5) | .212 |
| Postoperative Death (30-day) | 3 (1.2) | 4 (0.8) | .823 |
| 1-y Serum Creatinine (mg/dL) | 1.41±0.61 | 1.60±0.65 | .008 |
| 5-y Serum Creatinine (mg/dL) | 1.50±0.62 | 1.66±0.81 | .045 |
| 10-y Serum Creatinine (mg/dL) | 1.54±0.76 | 1.64±0.55 | .525 |
| 1-y Graft Survival | 93.3% | 92% | < .05 |
| 5-y Graft Survival | 83% | 83.7% | < .05 |
| 10-y Graft Survival | 75% | 74% | .183 |
| 1-y Patient Survival | 96.7% | 92.1% | .185 |
| 5-y Patient Survival | 96.3% | 93.7% | .211 |
| 10-y patient Survival | 80% | 77% | .172 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



