
Submitted:
17 December 2023
Posted:
19 December 2023
You are already at the latest version
Abstract
Although the connection of implant abutments to implant analogs and implant bodies has been evaluated separately, comparative evaluation of connections to implant analogs and implant bodies has not been evaluated. The objective of this study was to identify whether torque applied during laboratory manufacturing and during restoration cementation affects the compatibility between the implant body-abutment and the implant analog-abutment, as well as to spot any structural differences. Three different implant system with internal conical connection (Bioinfinity, Dant, and Dentist) were used. For each group, straight abutments (n=20) were tightened to implant analogs (n=10) and implant bodies (n=10) with hand tightening and using torque wrench device. The fitting of componenets were evaluated for each group using linear and volumetric micro-CT analysis. For linear analysis, when the mean differences (difference between measurements of the linear distance of abutments during hand tightening and applying torque) values between implant analog and implant body were compared within groups, There was no statistically significant difference observed in all groups (p> 0.05). Throughout the fabrication and clinical phases, it is recommended to tighten the abutments on the analogs with a torque wrench instrument to minimize the risk of prosthetic incompatibility.
Keywords:
implant dentistry
; biomechanics
; dental prosthesis
1. Introduction
The topic of dental implant failure is extensively researched and documented in the field of dentistry. Conducting clinical investigations to assess the failure of dental implants is both expensive and time-consuming. Therefore, it is necessary to examine dental implants in a methodical way. The failure of an implant may be influenced by two main categories of factors: biological and mechanical [1]. According to Lang et al. [2], the main biological cause of peri-implantitis is the impact it has on the soft and hard tissues surrounding dental implants. On the other hand, mechanical reasons mostly concern the implant-prosthetic components as a whole. Mechanical issues associated with implants include implant fracture, abutment fracture, screw loosening and loss, and over-structure fracture [3]. The presence of an implant-abutment mismatch is recognized to elevate mechanical stress on connecting structures. Various crucial aspects influence the stability of a screw joint. The critical factors include optimal pre-load, precise fitting of implant pieces, and the stability of the implant-to-abutment contact [4]. Applying the appropriate torque to an implant screw results in a pre-load that securely keeps the components in place [5]. When comparing methods of hand tightening the abutment screw versus using a torque wrench device there is a compromise for using a mechanical torque restricting instrument [6,7]. Yang et al. [8] and Hu et al. [9] have observed that tightening procedures for the implant and abutment connection are conducted in two stages in relevant studies. During the application of prescribed torque levels, the starting torque is applied initially. Following a duration of 10 minutes, the application of the second torque takes place. The goal of conducting this procedure twice is to account for the decrease in torque values following the initial tightening, while also preventing any potential plastic deformations that may arise from excessive tightening of the screw. The literature has documented two groups of methodologies used to analyze the interaction between implants and abutments: direct approaches and indirect methods. Methods for directly collecting linear or volumetric pictures of the gap include synchrotron radiography, micro-computed tomography (micro-CT), and scanning electron microscopy (SEM) [10,11,12]. Indirect approaches entail analyzing the concentration of markers present in the fluid around the implant, such as bacteria or dye, in order to ascertain the size of the micro-gap [13,14]. The utilization of micro-tomography technology allows for the three-dimensional study of a sample without the need for cutting, coating, or subjecting the item to any specific chemical treatment, as demonstrated by Yip et al. [15]. X-ray micro-tomography offers several advantages that make it comparable to ideal 3D microscopy. It allows for the investigation of objects in their natural state without any need for preparation or alteration. Additionally, it is non-invasive and non-destructive, providing a sufficiently magnified 3D reconstruction. Furthermore, it enables the reliable measurement of numeric data pertaining to the internal structure, including morphology, structure, and ultra-structure [15]. Micro-CT is commonly employed in dental implant research due to its numerous benefits. The studies conducted by Schicho et al. [16], Narra et al. [17], and Erpaçal et al. [18]. Implant analogs are utilized in the production of implant-supported prostheses, enabling the relocation of abutments to the patient's mouth and the replication of implants in the plaster model. Studies utilizing impression methods have assessed the accuracy of analogs and their compatibility with the implant body in the literature [19]. The process of manufacturing an implant-supported prosthesis does not involve torqueing the abutments to the model. However, the difference between this manufacturing process and the delivery of the restoration in the patient's mouth after torqueing the implant body has not been adequately studied. The objective of the study was to determine if the compatibility between the implant body-abutment and the implant analog-abutment is affected by torque exerted during manufacture in the laboratory and when the restoration is cemented in place, as well as to identify any structural variations. The study's null hypothesis posited that varying tightening applications of abutments would have no impact on the fitting of both the implant body and implant analog.
2. Materials and Methods
The study included 30 dental implants with conical internal connections, along with 30 implant analogs and 60 straight abutments from three different commercial systems: BioInfinity (Turkey) (Group 1), Dant (Israel) (Group 2), and Dentis Co. (Daegu, Korea) (Group 3). A solitary researcher conducted the experiment by securely fastening each implant body and implant mimic onto a solid platform (Figure 1a, 1b).
Abutments were positioned on both the analog and implant body of each system. The initial scanning procedure commenced after the researcher manually secured the abutment to each implant body or implant analog. Subsequently, the abutments were secured using a torque wrench device to the recommended torque levels (25 Ncm for group 1, 30 Ncm for group 2, and 30 Ncm for group 3). Following a 10-minute pause, a second round of tightening was performed, and the second scanning operation commenced.
Scanning and Analysis
The samples were scanned using a high-resolution microCT machine (Skyscan 1275, Aartselaar, Belgium). The connections between the implant and abutment, as well as the analog, were specifically scanned in both the torqued and handle tightened states. The NRecon program was utilized for image reconstruction after the scanning process (NRecon Version: 1.6.9.4, Bruker MicroCT, Kontich, Belgium). During the reconstruction process, beam hardening correction, ring artifact reduction, smoothing, and frame averaging were individually changed to find the best values for each sample. The adjustment was done to optimize the quality of the reconstructed images. The reconstructed images were transmitted to the DataViewer software (Version: 1.5.6.2, Bruker MicroCT, Kontich, Belgium), and a three-dimensional reimagining was conducted. Thus, sagittal pictures were acquired for every individual sample. Following the completion of the scanning and reconstruction methods, each picture underwent examination in the sagittal plane, with further measurements taken for both linear and volumetric aspects. The linear measurements were obtained by measuring the length of the perpendicular line extending from the highest point of the abutment to the platform of the implant body or analog (Figure 2a, 2b, 2c). Volumetric measurements were obtained by determining the apical space of the implant body or analog using a horizontal line drawn from the tip of the abutment screw (Figure 3a, 3b, 3c).
Statistical Analysis
The statistical analyses were conducted using IBM's SPSS version 26.0 software. The Shapiro-Wilk test was employed to assess whether the groups followed a parametric or nonparametric distribution, and the findings indicated a parametric distribution. A one-way analysis of variance (ANOVA) was employed to ascertain any significant disparities between groups, while an independent t-test was utilized to detect differences within each group. All tests evaluated a p-value of less than 0.05 as statistically significant.
3. Results
The results provide descriptive statistics for the linear measurements of abutments placed on the implant bodies and analogs for all groups. The measurements were taken with torque applied and hand-tightened. The specific data can be seen in Table 1. A comparison was made between the torqued and hand-tightened placements of the abutments on implant analogs. A statistically significant difference was observed for the group 2 and the group 1 (p<0.05). However, no significant difference was found for the group 3 (p > 0.05). A significant statistical difference was seen when comparing the torqued and hand-tightened placements of abutments on the implant bodies in all groups (p<0.05). The placement of abutments to the implant body and implant analogs was compared within groups using hand tightening. Measurements of group 1, group 2 and group 3 did not show any statistically significant difference (p > 0.05). Comparing the positioning of abutments to the implant body and implant analog by torque, there was a statistically significant difference in group 1 (p<0.05), whereas no statistically significant difference was seen in group 2 and group 3 (p>0.05).
Table 2 presents the descriptive statistics for the volumetric measurements of all the groups, when abutments are placed on implant bodies and analogs and hand tightened or with torque. The torque and hand tightening of the abutments on implant analogs were compared. A statistically significant difference was seen for the group 2 and the group 3 (p<0.05), however no statistically significant difference was found for the group 1 (p>0.05). A significant statistical difference was for group 1 and group 2 (p<0.05) when comparing the torque and hand-tightened placements of the abutments on the implant body. However, no significant statistical difference was found for the group 3 (p>0.05). Comparison was made between the hand tightening of abutments to the implant body and the implant analogs for each group. A statistically significant difference was seen in the group 1 and the group 3 (p<0.05). However, no significant difference was found in the group 2 (p>0.05). Comparing the placement of abutments to the implant body and implant analog by torque, there was a significant statistical difference in the group 1 and the group 3 (p<0.05). However, there was no significant statistical difference seen in the group 2 (p>0.05).
Table 3 displays the mean difference between measurements of the linear distance of abutments during hand tightening and applying torque on the implant body and implant analog. The mean differences values between implant analog and implant body were compared within groups. There was no statistically significant difference observed in group 1, group 2, and group 3.
Table 4 displays the mean difference in volumetric measurements between hand tightening and the application of torque on the implant body and implant analog. The mean differences values between implant analog and implant body were compared within groups. The implant analog values of the group 2 were statistically higher than the implant body values of the group 2, and there was no significant difference in group 1 and group 3.
4. Discussion
This study aimed to assess the linear and volumetric differences in the connection of abutments from three different implant systems with internal hexagonal conical connections. The abutments were tightened using a torque wrench device and hand tightening to the implant body and implant analog. The disparities were assessed using a rigorous approach that involved comparing within the same system and across other systems. This was done by analyzing distances and calculating the mean differences. The disparities observed between linear analyses and volumetric analyses are attributed to variations in the intrinsic structures of the systems, which subsequently impact volumetric evaluations. When analyzing prosthodontic research, it is more clinically significant to interpret results using linear metrics [20,21]. To eliminate structural differences, the mean difference was calculated by comparing the placement of abutments using hand tightening and torque application with a wrench device on both the implant analog and the implant body. When examining data using both linear and volumetric analysis, it is evident that there are variations between the methods of hand tightening and torque application. Therefore, the study's null hypothesis has been partially refuted. In the study conducted by Singh et al. [6], a total of 120 implant analogs were evenly distributed, and the abutments were placed using both hand tightening and a torque wrench device. The fitting of the abutments to the implant analogs was assessed by employing light body impression material and a stereomicroscope. A total of 60 distinct clinicians squeezed one sample from each group. It was reported that the results obtained using hand tightened abutments were inconsistent, indicating the need for a torque wrench equipment. Upon analyzing the data from present study, it was discovered that there are variations in the tightening technique for some groups, both in terms of linear and volumetric measurements, when comparing the data acquired with the abutment connection to the implant analog using hand tightening and torque wrench device. In their study, Alikhasi et al. [22] conducted a comparison of torque values among physicians with varying degrees of expertise. They also examined models representing different regions of the mouth and utilized screwdrivers of varying sizes and forms. Therefore, it was shown that torque levels might vary depending on the kind of screwdriver, with larger values being found in the anterior region compared to the posterior region. Upon examining the literature on tightening the abutment screw in the implant abutment connection, it is evident that the implant analog, as described by Saber et al. [23], or the implant body, as described by Velez et al. [5], are the predominant choices. Saber et al. [23] said that, due to the exorbitant expense of implant components, they opted to utilize implant analogs, instead of implant bodies (fixtures) in their study. However, more investigations are required to be conducted using implant bodies. The present study investigated the attachment of abutments to both implant bodies and implant analogs using torque application and hand tightening. As a standard procedure in the clinic, the abutment attached to the analog in the model is not torqued, while the abutment put on the implant body in the patient's mouth is torqued. An assessment of this circumstance should be conducted with regards to the model's capacity to accurately replicate the characteristics of the patient's oral cavity. The current study found a statistically significant difference in linear measurements between the group 1 and group 2 when comparing hand tightening of the abutment placed on the implant analog and tightening by applying torque to the abutment on the implant body. However, there was no difference observed for the group 3. Within the context of volumetric measurements, the identical scenario was analyzed, revealing a statistically significant difference in all groups. This study included securing the samples on a reliable platform, which was identified as one of the study's limitations. In a prior investigation, Singh et al. [6] employed implant bodies, or analogs that were affixed within a solid block of acrylic material to inhibit any form of motion. The present study utilized a solid platform to securely attach the implant analogs and implant bodies. In line with prior research conducted by Schicho et al. [16], Erpaçal et al. [18], and Yiting H et al. [10], this study employed micro-CT to assess the implant body, implant analog, and abutment measures. Micro-CT is a very efficient and extensively utilized technique for examining implant components. It ensures the acquisition of high-resolution photos, so preventing any damage or destruction [25]. This technique, which enables both linear and volumetric measurements, may also be employed for conducting novel and repeated studies. Additionally, there have been studies in the literature that utilized scanning electron microscopy (SEM) [5,26]. The methodological approach of SAM analysis closely resembles that of 2D linear analyses conducted in micro-CT. These findings enhance the dependability of linear analysis. It is hypothesized in this study that the variations in linear and volumetric analyses might be attributed to structural disparities in the implant systems. To address these disparities, we compared the variation (mean difference) in data received from hand tightening and applying torque to the implant analog in each group with the variation in data obtained from hand tightening and applying torque to the implant body. Although the linear measures did not show any statistically significant difference within the three groups, only the group 2 exhibited a statistically significant difference in terms of volumetric measurements. Nevertheless, when comparisons were conducted among the groups, no statistically significant difference was seen. This greatly standardizes the outcomes of the investigation. Yang et al. [8], assessed the reverse torque measurements of abutment screws by using a torque wrench device to tighten the implants. They then allowed a 10-minute interval before tightening them once again. In a similar manner, Hu et al. [9] investigated the reverse torque values in angled abutments and performed the torque procedure twice with a 10-minute interval. In this study, the second tightening occurred 10 minutes after the initial tightening. The objective of this approach was to mitigate the settling affect [24]. In current study, implant systems with a conical internal connection were examined. In their study, Kim et al. [27] conducted a comparison of implant systems including internal connections and those using external connections. The study's findings indicate that systems with internal connections exhibit better settling compared to those with external connections. In contrast, Gehrke et al. [28] conducted a research using a single implant system that included an internal connection and they assessed the fitting of the abutments using scanning electron microscopy (SEM) at various levels of tightness. The current study aimed to assess three different implant systems with conical connections in order to establish standards. Additional investigation may be conducted to assess the compatibility of implant systems with various connections.
5. Conclusions
The results of this study identified significant differences between hand tightening and torque applied values of abutments connected to the analogs. The discrepancy in values between hand tightening and torque applied to analogs is comparable to those associated with the implant body. To reduce the likelihood of prosthetic incompatibility, it is advisable to use a torque wrench instrument to tighten the abutments on the analogs throughout both the fabrication process and clinical phases. This study will provide foundation for future investigations that will assess implant systems with various types of connections.
Author Contributions
Conceptualization, B.A. and K.O.; methodology B.A. and M.O.; software, B.B. and M.O.; validation, M.K. and S.S.; formal analysis, A.Ş. and M.O.; investigation, B.A. and A.Ş.; resources, F.G and M.K.; data curation, K.O. and F.G.; writing – orijinal draft preparation, B.A., M.O and B.B., writing – review and editing, K.O., A.Ş. and S.S.; visualization, A.Ş..; supervision, K.O and S.S.; Project administratiton, B.A. and M.K.; funding acqusition, B.A.
Funding
This research received no external funding.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Acknowledgments
The authors would like to thank to BioInfiniyt Implant CO. Turkey, Dant Implant CO. Israel and Dentis Implant CO. Korea for providing implant components.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Stavropoulos, A, Bertl, K, Eren, S, Gotfredsen, K. Mechanical and biological complications after implantoplasty—A systematic review. Clin Oral Impl Res. 2019; 30: 833–848. [CrossRef]
- Lang, N.P., Wilson, T.G. and Corbet, E.F. Biological complications with dental implants: their prevention, diagnosis and treatment Note. Clinical Oral Implants Research: Chapter 9, 2000, 11: 146-155. [CrossRef]
- Schwarz, Melvyn S. Mechanical complications of dental implants. Clinical Oral Implants Research: Chapter 10, 2000, 11: 156-158. [CrossRef]
- Georgios Siamos, Sheldon Winkler, Kenneth G. Boberick; The Relationship Between Implant Preload and Screw Loosening on Implant-supported Prostheses. J Oral Implantol 1 April 2002; 28 (2): 67–73. [CrossRef]
- Vélez, J.; Peláez, J.; López-Suárez, C.; Agustín-Panadero, R.; Tobar, C.; Suárez, M.J. Influence of Implant Connection, Abutment Design and Screw Insertion Torque on Implant-Abutment Misfit. J. Clin. Med. 2020, 9, 2365. [CrossRef]
- Singh, Himani, et al. Implant abutment using hand drivers versus torque wrench. Bioinformation, 2023, 19.2: 221-225. [CrossRef]
- Sameera Y, Rai R. Tightening torque of implant abutment using hand drivers against torque wrench and its effect on the internal surface of implant. The Journal of the Indian Prosthodontic Society, 2020, 20.2: 180. [CrossRef]
- Yang S., Qin Y., Guo X., Li Y. An In Vitro Study of Fluid Contaminations Influences on Reverse Torque Values of Implant-Abutment Connections. BioMed Research International, 2022, 2022. [CrossRef]
- Hu, E., Petrich, A., Imamura, G. and Hamlin, C.Effect of screw channel angulation on reverse torque values of dental implant abutment screws. Journal of Prosthodontics, 2019, 28.9: 969-972.. [CrossRef]
- He Y, Fok A, Aparicio C, Teng W. Contact analysis of gap formation at dental implant-abutment interface under oblique loading: A numerical-experimental study. Clin Implant Dent Relat Res. 2019; 21: 741–752. [CrossRef]
- Zipprich H, Weigl P, Ratka C, Lange B, Lauer H-C. The micromechanical behavior of implant-abutment connections under a dynamic load protocol. Clin Implant Dent Relat Res. 2018; 20: 814–823. [CrossRef]
- Vinhas, A.S.; Aroso, C.; Salazar, F.; López-Jarana, P.; Ríos-Santos, J.V.; Herrero-Climent, M. Review of the Mechanical Behavior of Different Implant–Abutment Connections. Int. J. Environ. Res. Public Health 2020, 17, 8685. [CrossRef]
- Aloise, J.P., Curcio, R., Laporta, M.Z., Rossi, L., Da Silva, A.M.Á. and Rapoport, A. Microbial leakage through the implant–abutment interface of Morse taper implants in vitro. Clinical oral implants research, 2010, 21.3: 328-335. [CrossRef]
- Larrucea Verdugo C, Jaramillo Núñez G, Acevedo Avila A, Larrucea San Martín C. Microleakage of the prosthetic abutment/implant interface with internal and external connection. In vitro study. Clin. Oral Impl. Res. 25, 2014, 1078–1083. [CrossRef]
- Yip, G., Schneider, P., Roberts, E. W. Micro-computed tomography: high resolution imaging of bone and implants in three dimensions. In: Seminars in Orthodontics. WB Saunders, 2004. p. 174-187. [CrossRef]
- Schicho, K., Kastner, J., Klingesberger, R., Seemann, R., Enislidis, G., Undt, G., Wanschitz, F., Figl, M., Wagner, A. and Ewers, R. Surface area analysis of dental implants using micro-computed tomography. Clinical oral implants research, 2007, 18.4: 459-464. [CrossRef]
- Narra, N., Antalainen, A. K., Zipprich, H., Sandor, G. K., Wolff, J. Microcomputed tomography-based assessment of retrieved dental implants. International Journal of Oral & Maxillofacial Implants, 2015, 30.2. [CrossRef]
- Erpaçal B, Adıgüzel Ö, Cangül S. The use of micro-computed tomography in dental applications. Int Dent Res 2019;9(2):78-91. [CrossRef]
- Maria, R., Tan, M.Y., Wong, K.M., Lee, B.C.H., Chia, V.A.P., Tan, K.B.C. Accuracy of implant analogs in 3D printed resin models. Journal of Prosthodontics, 2021, 30.1: 57-64. [CrossRef]
- Akat B, Şentürk A, Ocak M, Kiliçarslan MA, Özcan M. Does cad software affect the marginal and internal fit of milled full ceramic crowns?. Braz oral res. 2022;36:e042. [CrossRef]
- Bayrak A, Akat B, Ocak M, Kιlιçarslan MA, Özcan M. Micro-Computed Tomography Analysis of Fit of Ceramic Inlays Produced with Different CAD Software Programs. Eur J Prosthodont Restor Dent. 2021 Aug 31;29(3). PMID: 33393742. [CrossRef]
- Alikhasi, M., Kazemi, M., Jalali, H., Hashemzadeh, S., Dodangeh, H., Yilmaz, B. Clinician-generated torque on abutment screws using different hand screwdrivers. The Journal of Prosthetic Dentistry, 2017, 118.4: 488-492. [CrossRef]
- Saleh Saber F, Abolfazli N, Jannatii Ataei S, Taghizade Motlagh M, Gharekhani V. The effect of repeated torque tightening on total lengths of implant abutments in different internal implant‒abutment connections. J Dent Res Dent Clin Dent Prospects. 2017 Spring;11(2):110-116. Epub 2017 Jun 21. PMID: 28748052; PMCID: PMC5519991. [CrossRef]
- Bulaqi, H. A., Mashhadi, M. M., Safari, H., Samandari, M. M., Geramipanah, F. Dynamic nature of abutment screw retightening: finite element study of the effect of retightening on the settling effect. The Journal of prosthetic dentistry, 2015, 113.5: 412-419. [CrossRef]
- Min, C. K., and Kim, K. A. A. Quantitative analysis of metal artefacts of dental implant in CBCT image by correlation analysis to micro-CT: A microstructural study. Dentomaxillofacial Radiology, 2021, 50.3: 20200365. [CrossRef]
- Butkevica, A., Nathanson, D., Pober, R., Strating, H. Measurements of repeated tightening and loosening torque of seven different implant/abutment connection designs and their modifications: An in vitro study. Journal of Prosthodontics, 2018, 27.2: 153-161. [CrossRef]
- Kim, K.-S., Lim, Y.-J., Kim, M.-J., Kwon, H.-B., Yang, J.-H., Lee, J.-B., Yim, S.-H. Variation in the total lengths of abutment/implant assemblies generated with a function of applied tightening torque in external and internal implant–abutment connection. Clinical oral implants research, 2011, 22.8: 834-839. [CrossRef]
- Gehrke, S. A., Shibli, J. A., Aramburu Junior, J. S., Sánchez de Val, J. E. M., Calvo-Girardo, J. L., Dedavid, B. A. Effects of different torque levels on the implant-abutment interface in a conical internal connection. Brazilian oral research, 2016, 30. [CrossRef]
Figure 1.
a) Hand tightening (left) and b) using a torque wrench device (right) on a solid platform.
Figure 1.
a) Hand tightening (left) and b) using a torque wrench device (right) on a solid platform.

Figure 2.
Linear measurement of a) group 1 (left) and b) group 2 (central) c) group 3 (right).
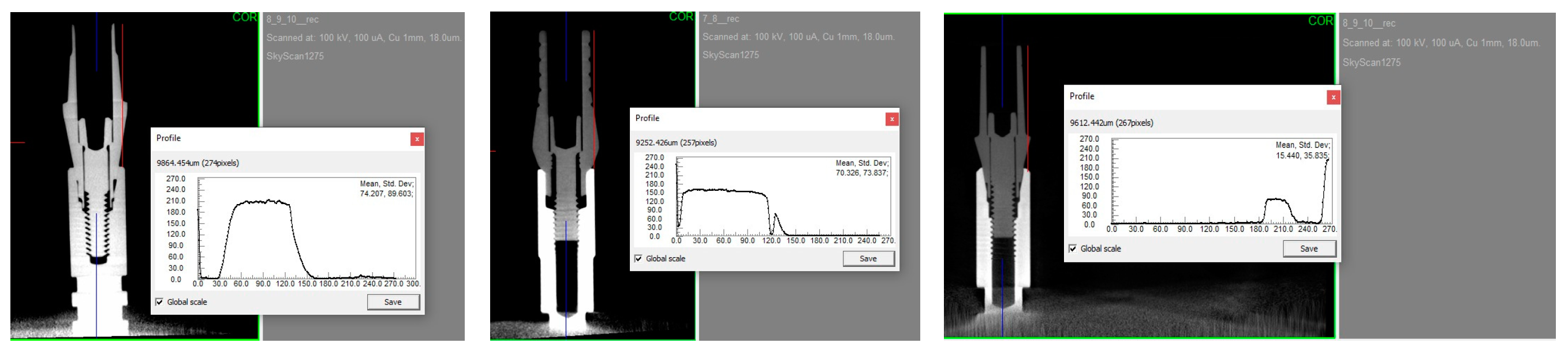
Figure 3.
Volumetric measurement of a) group 1 (left) and b) group 2 (central) c) group 3 (right).
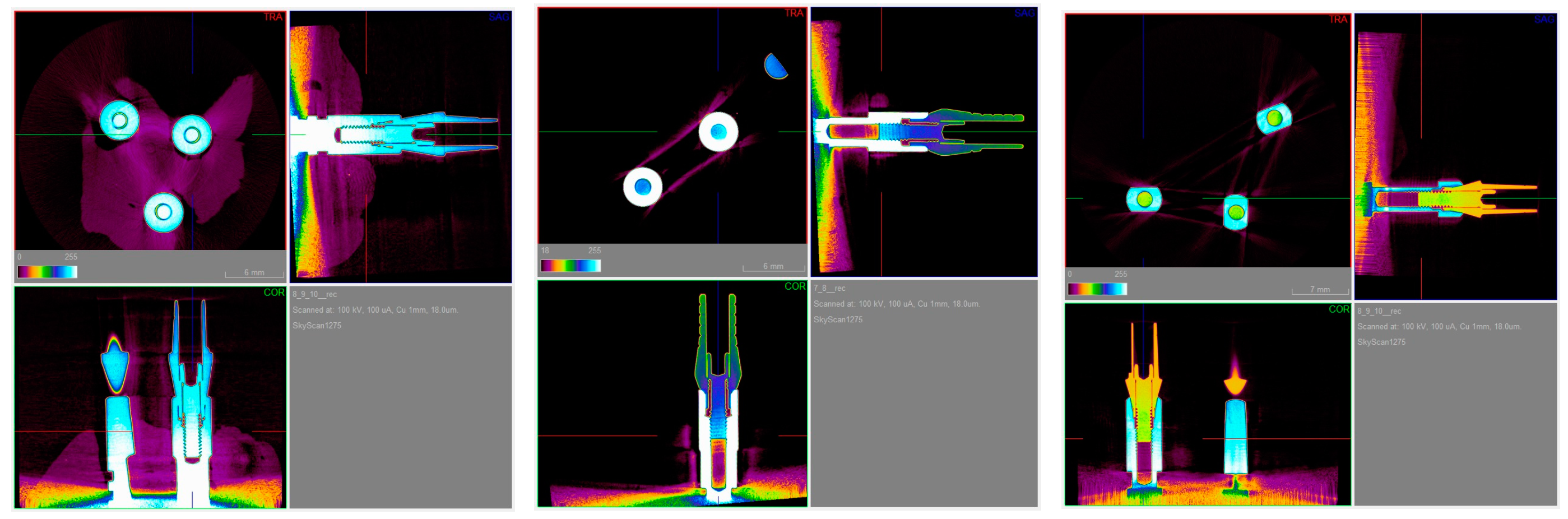

Table 1.
Descriptive statistical analysis of linear analysis.
| Group | Connection |
Tightening | Mean | Standart deviation | Standart error | Min. | Max. | % 95 Lower bond |
95% Upper bound | p |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Implant Analog | Torqued | 9753,80 | 230,896 | 73,016 | 9348 | 9990 | 9588,63 | 9918,97 | A,a |
| Hand tightened | 9973,30 | 93,597 | 29,598 | 9760 | 10044 | 9906,34 | 10040,26 | A,b | ||
| Implant Body | Torqued | 9462,80 | 217,302 | 68,717 | 9094 | 9740 | 9307,35 | 9618,25 | A,c | |
| Hand tightened | 9770,00 | 110,623 | 34,982 | 9560 | 9972 | 9690,86 | 9849,14 | A,ab | ||
| 2 | Implant Analog | Torqued | 9202,40 | 81,998 | 25,930 | 9072 | 9311 | 9143,74 | 9261,06 | B,ac |
| Hand tightened | 9429,50 | 235,224 | 74,384 | 8905 | 9792 | 9261,23 | 9597,77 | B,b | ||
| Implant Body | Torqued | 9067,90 | 180,939 | 57,218 | 8730 | 9326 | 8938,46 | 9197,34 | B,c | |
| Hand tightened | 9313,20 | 90,785 | 28,709 | 9126 | 9444 | 9248,26 | 9378,14 | B,ab | ||
| 3 | Implant Analog | Torqued | 9138,30 | 86,271 | 27,281 | 8985 | 9288 | 9076,59 | 9200,01 | B,a |
| Hand tightened | 9331,70 | 141,769 | 44,831 | 9133 | 9612 | 9230,28 | 9433,12 | B,ab | ||
| Implant Body | Torqued | 9164,60 | 238,558 | 75,439 | 8910 | 9558 | 8993,95 | 9335,25 | B,a | |
| Hand tightened | 9466,70 | 250,168 | 79,110 | 9126 | 9927 | 9287,74 | 9645,66 | B,b |
The mean difference is significant at the 0.05 level. Identical letters show a lack of significance. Capital letters indicate comparison among all groups. Lowercase letters indicate within-group comparisons.
Table 2.
Descriptive statistical analysis of volumetric analysis.
| Group | Connection | Tightening | Mean | Standart deviation | Standart error | Min. | Max. | % 95 Lower bond | 95% Upper bound | p |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Implant Analog | Torqued | ,793 | ,084 | ,026 | ,696 | ,973 | ,733 | ,853 | A,a |
| Hand tightened | ,910 | ,131 | ,041 | ,717 | 1,137 | ,816 | 1,004 | B,a | ||
| Implant Body | Torqued | 1,289 | ,300 | ,095 | ,982 | 1,965 | 1,074 | 1,503 | C,b | |
| Hand tightened | 1,877 | ,096 | ,030 | 1,700 | 1,982 | 1,808 | 1,946 | D,c | ||
| 2 | Implant Analog | Torqued | 6,234 | ,774 | ,245 | 5,174 | 7,716 | 5,680 | 6,788 | E,ac |
| Hand tightened | 7,163 | ,698 | ,221 | 5,857 | 8,200 | 6,664 | 7,662 | F,b | ||
| Implant Body | Torqued | 3,339 | ,280 | ,088 | 3,010 | 3,744 | 3,139 | 3,539 | G,c | |
| Hand tightened | 3,597 | ,320 | ,101 | 3,183 | 4,181 | 3,368 | 3,826 | H,ab | ||
| 3 | Implant Analog | Torqued | 13,153 | ,455 | ,144 | 12,469 | 13,859 | 12,827 | 13,478 | I,a |
| Hand tightened | 13,705 | ,823 | ,260 | 12,737 | 15,285 | 13,116 | 14,293 | J,b | ||
| Implant Body | Torqued | 5,024 | ,223 | ,070 | 4,507 | 5,272 | 4,864 | 5,183 | K,c | |
| Hand tightened | 5,790 | ,413 | ,131 | 5,225 | 6,481 | 5,494 | 6,085 | L,c |
The mean difference is significant at the 0.05 level. Identical letters show a lack of significance. Capital letters indicate comparison among all groups. Lowercase letters indicate within-group comparisons.
Table 3.
Comparison of mean difference of tightening methods in linear measurements.
| Group | Connection | Mean | Standart deviation | Standart error | Min. | Max. | 95% Lower Bound | 95% Upper Bound | p |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Implant Analog | 219,5000 | 232,76705 | 73,60740 | 20,00 | 660,00 | 52,9885 | 386,012 | A,a |
| Implant Body | 307,2000 | 252,56190 | 79,86708 | 40,00 | 734,00 | 126,5281 | 487,8719 | A,a | |
| 2 | Implant Analog | 227,1000 | 272,69945 | 86,23514 | -371,00 | 576,00 | 32,0226 | 422,1774 | A,a |
| Implant Body | 245,3000 | 185,90502 | 58,78833 | 20,00 | 558,00 | 112,3116 | 378,2884 | A,a | |
| 3 | Implant Analog | 193,4000 | 145,95981 | 46,15655 | 12,00 | 468,00 | 88,9866 | 297,8134 | A,a |
| Implant Body | 302,1000 | 248,30557 | 78,52112 | 36,00 | 766,00 | 124,4729 | 479,7271 | A,a |
The mean difference is significant at the 0.05 level. Identical letters show a lack of significance. Capital letters indicate comparison among all groups. Lowercase letters indicate within-group comparisons.
Table 4.
Comparison of mean difference of tightening methods in volumetric measurements.
| Group | Connection | Mean | Standart deviation | Standart error | Min. | Max. | 95% Lower Bound | 95% Upper Bound | p |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Implant Analog | 219,5000 | 232,76705 | 73,60740 | 20,00 | 660,00 | 52,9885 | 386,012 | A,a |
| Implant Body | 307,2000 | 252,56190 | 79,86708 | 40,00 | 734,00 | 126,5281 | 487,8719 | A,a | |
| 2 | Implant Analog | 227,1000 | 272,69945 | 86,23514 | -371,00 | 576,00 | 32,0226 | 422,1774 | A,a |
| Implant Body | 245,3000 | 185,90502 | 58,78833 | 20,00 | 558,00 | 112,3116 | 378,2884 | A,a | |
| 3 | Implant Analog | 193,4000 | 145,95981 | 46,15655 | 12,00 | 468,00 | 88,9866 | 297,8134 | A,a |
| Implant Body | 302,1000 | 248,30557 | 78,52112 | 36,00 | 766,00 | 124,4729 | 479,7271 | A,a |
The mean difference is significant at the 0.05 level. Identical letters show a lack of significance. Capital letters indicate comparison among all groups. Lowercase letters indicate within-group comparisons.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



