Submitted:
18 December 2023
Posted:
19 December 2023
You are already at the latest version
Abstract
Radiation therapy is employed in treating various cancer types. However, depending on the type and stage of cancer, its benefits can be limited, and it may cause serious side effects that detrimentally affect the quality of life (QOL) for the patient. Preventing the side effects of radiation therapy can enhance the response to cancer treatment and improve the patient’s QOL. Independently, vitamin C and hydrogen have demonstrated potential in reducing the side effects of anticancer drugs and radiation therapy. Furthermore, both have been postulated to possess direct anticancer properties. However, the effects of their combined therapy remain underexplored. This study investigates the hypothesis that combining vitamin C and hydrogen efficiently prevents radiation-induced injuries.
Survival rates were investigated in cancer cell lines (MDA-MB231 and GL261) and normal cells (HUVEC) treated with hydrogen, vitamin C and irradiation. Apoptosis was assessed using the FLICA test, and EMT gene expression was elucidated via the qPCR technique.
In the normal cell line, the introduction of vitamin C and hydrogen to the culture medium boosted survival rates, exhibiting a radioprotective effect upon irradiation. In contrast, cancer cells showed a decreased survival rate with the introduction of vitamin C and hydrogen, which was further diminished with irradiation. Treated cancer cells showed signs of apoptosis. Caspase activity in viable cells was reduced by the combination treatment with vitamin C and hydrogen. Additionally, glioblastoma cells treated with this combination showed reduced EMT gene expression.
This study reveals that a combined therapy of hydrogen and vitamin C offers radioprotective effects on normal cells and exerts direct anticancer effects on cancer cells, while also amplifying the anticancer effects of radiation. Importantly, this combined therapy attenuated the radiation-induced EMT signature in the GL261 murine glioma cell line, suggesting potential in diminishing treatment resistance and tumor invasion.
Keywords:
Hydrogen
; vitamin C
; cancer treatment
; radioprotection
; HUVEC
; MDA-MB-231
; GL261
; apoptosis
; FLICA
; EMT gene expression
1. Introduction
Each year, millions of patients receive radiotherapy for cancer treatment. Many of these patients suffer from severe side effects such as mucositis, dermatitis, xerostomia, gastrointestinal disorders, bone marrow failure, and Radiation pneumonitis among others. Preventing these side effects can dramatically improve the quality of life (QOL) of patients receiving radiotherapy and decrease medical expenses associated with treatment. However, few radioprotective strategies are currently in use in clinical practice, and the treatment of radiation injury remains problematic. Moreover, radiation exposure from medical procedures is an issue of concern in many countries. In the United States, the use of computed tomography (CT) increased to 70 million scans annually in 2007 [1], and the radiation-related cancer risk is concerning.
Most of the ionizing radiation-induced damage is caused by reactive oxygen species (ROS), especially hydroxyl radicals (·OH) produced by radiolysis of H2O. Antioxidants are believed to be effective for removing ROS [2,3]. The use of antioxidants in the treatment of radiation injury has been studied extensively [2,3,4,5]. The common approach is to deliver the antioxidants concurrently; however, tumor protection is a major concern [6]. Antioxidants may facilitate tumor progression and metastasis through supporting the viability and the invasive capacity of cancer cells [7]. Randomized clinical trials demonstrated that the use of antioxidants such as alpha tocopherol and beta carotene as adjuvant therapy might compromise radiation efficacy and is associated with poor tumor control and may increase mortality [8,9,10].
Amifostine [11,12], the first radioprotective agent approved by the Federal Drug Administration, is associated with toxicities that limit its use and efficacy [13].
Both vitamin C and hydrogen protect from radiation-induced damage [14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29] and function by removing ROS from the human body. They also reduce inflammation in tissues. The two therapies are easy to perform, relatively inexpensive, and most importantly, safe [30,31,32,33,34,35,36]. They do not attenuate but sometimes enhance the effect of radiation in cancer treatment [37,38,39]. Ascorbic acid increases radiation-induced apoptosis in HL60 Human Leukemia Cell lines by activating caspases-3, 8, and 9 [38]. It has also been reported that pharmacological concentrations of ascorbate radiosensitize pancreatic tumor and glioblastoma cells [40,41,42,43].
Hydrogen and vitamin C are said to have anticancer effects [40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61]. Schoenfeld et al. recently reported a new mechanism underlying the effect of vitamin C. non-small-cell lung cancer (NSCLC) and glioblastoma (GBM) cells are selectively sensitive to vitamin C because of an altered redox-active iron metabolism [51].
Carosio et al. reported that Sodium ascorbate induces apoptosis of neuroblastoma cell lines by inhibiting iron uptake [52].
Hydrogen also has direct and indirect antitumor effects, which could be useful for the treatment of cancer patients. Hydrogen therapy improves overall survival, quality of life, blood parameters, and tumor reduction. In addition, hydrogen attenuates the risk of carcinogenesis induced by radiation.
Therefore, vitamin C and hydrogen may have additional therapeutic effects against cancer. Although the effect of each therapy on various diseases has been studied, the efficacy of combination therapy with vitamin C and hydrogen has not been evaluated to date. The combination of these two therapies could be effective for preventing side effects and improving the QOL of patients receiving radiotherapy.
1.1. Background of the idea of hydrogen vitamin C combination therapy
High-dose intravenous vitamin C infusion is used in many clinics for cancer treatment throughout the world [62,63], but its effectiveness varies from person to person. The recommended dose of vitamin C per infusion is 25 g to 100 g. In the author’s clinic (Shimokitazawa Nishiguchi Clinic, Tokyo Japan), there had been cases in which no anti-cancer effect at all was observed with high-dose vitamin C alone.
In many cases, the theory that the anticancer effect of vitamin C increases as the blood concentration rises with increasing dose, does not hold true. Therefore, the author came up with the idea of hydrogen as an adjuvant therapy, to support and enhance the effects of vitamin C. It was the origin of the hydrogen and vitamin C combination therapy, and Miyakawa M has been supporting many cancer patients in her clinic.
1.2. Hydrogen and Vitamin C Combination Therapy Method
Patients begin hydrogen inhalation 10 minutes prior to vitamin C injection. Patients are treated with high-dose vitamin C injection while inhaling simultaneous hydrogen (99.99% hydrogen gas, 250 ml/min, H2JI1, Doctor’s Man, Inc.) with nasal cannula.
To reduce the side effects of radiotherapy, daily infusions are administered after radiotherapy.
When combination therapy was used as supportive care for cancer treatment, the frequency of treatment varied from person to person, from every day, twice a week to once a month, depending on the individual’s medical condition and budget.
All patients received standard treatment at the hospital, followed by the hydrogen and vitamin C combination therapy at the clinic.
In addition, patients also performed the hydrogen and vitamin C combination therapy at home on their own as much as possible.
1.3. Home therapy
Not only treated in the clinic, but also patients treated themselves with hydrogen and vitamin C at home. Hydrogen gas inhalers, hydrogen bath generators, and hydrogen water generators were installed in patients’ homes, and patients inhale for as long as possible, take hydrogen baths, and drink hydrogen water to literally live a hydrogen-soaked life. In addition, they took hydrogen supplements when they go out or are hospitalized. Hydrogen supplements are those that produce a large amount of hydrogen gas in the intestines. Some patients were only able to incorporate a portion of these hydrogen treatments for financial reasons, so there are individual differences in the way hydrogen is incorporated at home.
For home vitamin C treatment, patients took lipo-capsule vitamin C(Lypo-C). Lypo-C is an ascorbic acid supplement in liposome capsules, which is said to increase blood levels of ascorbic acid to a higher level than regular ascorbic acid supplements. Differences were also observed in the amount of Lipo-C intake per day. These treatments were not covered by insurance, so all were done at their own expense.
1.4. Anti-cancer effects of hydrogen and vitamin C combination therapy
Although individual differences in efficacy were observed, favorable results were obtained in many patients to reduce side effects of not only radiation treatment, but also chemotherapy. It also seemed to have anti-cancer effects. The types of cancers for which efficacy was observed include lung, pancreatic, liver, colorectal, prostate, uterine, breast, and parotid cancers. However, these were all at the level of individual case reports and had not been scientifically proven. Additional studies are necessary before the combination therapy can be routinely applied for radioprotection in the clinic.
1.5. Radioprotection Case
Especially in patients with radiation induced dermatitis, we can visibly confirm the efficacy of this combination therapy. Two patients provided their consent for the publication of their information and photographs.
Case1: 85-year-old male
Malignant parotid carcinoma treated with hydrogen inhalation and vitamin C IV-injection at clinic, and home therapy (hydrogen inhalation and Lypo-C).
The patient received combination therapy at the clinic every day after radiation therapy. The skin redness begins to decrease at 30–40 minutes after the start of treatment (20–30 minutes from the start of vitamin C injection), and patient also reported decreased pain.
Figure 1, Figure 2 and Figure 3 shows the progress of the patient’s treatment. After surgery for high-grade parotid carcinoma (pathology is conduit carcinoma), stage 4, the patient underwent chemotherapy and radiation therapy at a total dose of 60 Gy for 2 months. After daily irradiation, the patient received hydrogen and vitamin C combination therapy.
Figure 1 shows the patient before the start of treatment; the skin at the irradiated site is red, swollen, and inflamed. Figure 2 shows the skin 20 minutes after the start of combination therapy, and the redness has decreased to about half of its original size. Figure 3 shows the end of combination therapy, and the redness has almost disappeared.
Remarkably, the patient was able to comfortably complete the two months of radiotherapy without suffering from mouth ulcers, dermatitis, etc., which usually appear as side effects of the treatment.
Case 2: 47-year-old female
Nasopharyngeal cancer treated with home therapy with Lipo-C, hydrogen inhalation, and hydrogen mist
This is a case of nasopharyngeal cancer treated with radiotherapy for 2 months, a total dose of 70Gy, for 35 times, and anticancer drug therapy. The patient underwent radiation therapy as an outpatient, and daily treatment at home with hydrogen inhalation, and hydrogen mist to the affected area. She also took Lypo-C every day. The skin did not sore at all, and She could complete the radiotherapy with only a little darkening and peeling. His doctor was surprised that under normal circumstances, the skin would have turned red and sore and become inflamed. Figure 4, Figure 5 and Figure 6 show the slightly darkened skin just before the end of the radiation therapy, and Figure 7 shows the skin that had already cleared up one month after the radiation therapy.
Based on these clinical experiences, we hypothesized that the combination therapy of hydrogen and vitamin C would have prevented the radiation induced injury and conducted experiments on the effects of hydrogen and vitamin C on cells.
1.6. The hypothesis
Hydrogen and vitamin C combination therapy is effective to prevent radiation injury.
2. Material and method
2.1. Cell Lines
HUVEC cells were maintained in Endothelial Cell Growth Medium 2 (PromoCell, Cat. C-22011) supplemented with Growth Medium 2 SupplementMix (PromoCell, Cat. C-39216). MDA-MB-231 was maintained in Dulbecco’s modified Eagle’s medium (Gibco, Cat. 41965) supplemented with 10% fetal bovine serum (Invitrogen, Cat. 25149-079) together with Antibiotic-Antimycotic (Gibco, Cat. 15240062). The murine glioma model GL261, provided by (NCI-Frederick), was defrosted and expanded in sphere condition (serum-free) containing DMEM/F12-GlutaMAX medium (MilliporeSigma), basic fibroblast growth factor 10 ng/ml, epidermal growth factor 20 ng/ml (Peperotech), B27-supplement 1:50 (Stem cell technology). The cells were kept in culture at 37°C in a humidified 5% CO2 atmosphere.
2.2. Vitamin C and hydrogen treatment
The methods of administering vitamin C and hydrogen were determined based on previous cell experiment studies [47,48] and preliminary experiments. In preliminary experiments, vitamin C was administered at various concentrations in cell culture medium with reference to previous studies. As MDA-MB231 cells were almost killed at a vitamin C concentration of 2 mM, two concentrations, 0.2 mmol and 1 mM, were selected. At these concentrations, survival was increased after 24 hours for normal cells. In the experiment on EMT gene expression in glioblastoma, the vitamin C concentrations were increased to 5 mM and 10 mM based on the results of previous experiments. For hydrogen, a Pure Hydrogen Gas Generator Model HB-H10 was used for generation of hydrogen gas. The culture medium was placed in a spits (30 ml) and bubbled with 99.99% hydrogen gas at 250 ml per minute for more than 60 minutes to ensure a concentration of more than 1000 ppb when the cells were put into petri dishes.
2.3. Radiation treatment
The irradiation dose was 4 Gy and was performed using Xstrahl (LIFE SCIENCES).
Cells (HEVEC, MDA-MB231, GL261) were added to the culture medium under five condition treatments: 0.2 mmol vitamin C alone, 1 mmol vitamin C alone, hydrogen alone, 0.2 mmol vitamin C + hydrogen, 1 mmol vitamin C + hydrogen. Viability rates were compared to the control (culture medium without addition of vitamin C and hydrogen) as 1. The treatment timing of each cell line was performed at several time point:1) treatment without irradiation, 2) treatment started before irradiation, 3) treatment started after irradiation, and 4) treatment started before and added again after irradiation, and each of the five conditions were applied to all cell lines. The viability rate was observed 24 hours after irradiation (24 hours after addition without irradiation).
Viability rates were measured, using an Invitrogen Countess Automated Cell Counter (Life Technologies), three times each for HUVEC and MDA-MB231 and four times for GL261, and the average value was presented.
2.4. Fluorescent detection of ROS
For determining total ROS (superoxide and hydrogen peroxide) in HUVEC cells that underwent different treatment condition, single cell suspension was prepared from all treatment condition where treatment started either after RT and lasted for 24h, or before and after RT (24h before RT and lasted for 24h after RT). Dihydroethidium (DHE) staining (Invetrogen) was done on viable cells (1mM) for 30min at 37ºC, followed by washing with FACS buffer (PBS+4%FBS). Samples were acquired on a LSR II flow cytometer (Becton Dickinson), then data analyzed using FlowJo 10 (Becton Dickinson)
2.5. Confirmation of apoptosis
FAM-FLICA® (Fluorescent-Labeled Inhibitor of Caspases Assays) test was used to confirm the extent to which apoptosis actually occurred in MDA-MB231 cells when vitamin C and hydrogen were added and irradiated. The FLICA™ kit can easily measure active caspases from the amount of fluorescence in living cells and distinguishes between apoptosis and necrosis. Instead of using antibodies as in ELISA, the kit utilizes an inhibitor (C-terminally labeled with a red or green fluorescent probe) that is shared by each active caspase. Apoptotic cells fluoresce in red or green. This test was performed for the treatment condition that achieved the highest antitumoral in vitro efficacy depending on viability rate after treatment (hydrogen and vitamin C administered twice before and after irradiation) because the test was performed to confirm what was happening to the cells when the survival rate decreased. It was done with 4 conditions, 1. control (culture medium only), 2. 1 mM vitamin C treatment, 3. Hydrogen treatment, and 4. 1 mM vitamin C and hydrogen combination treatment. For conditions 2, 3, and 4, hydrogen and/or vitamin C were administered before and after irradiation. Photographs were taken of the same specimens at four different locations.
2.6. EMT gene expression
RNA isolation and quantitative real-time PCR.Around 1-1,5x106 cultured cells were incubated in 0.7 ml Qiazol (Qiagen) for 5 min at RT. Thereafter, 0.14 ml Chloroform was added and vigorously aspirated and centrifuged at 12000 g for 10 min at 4°C. The aqueous phase was collected and transferred to a new tube, 0.5 ml of 100% Ethanol was added and the mixture was pipetted onto an RNeasy Mini column and centrifuged (12000 g, 15 sec, RT) after which the flow-through was discarded. Then 0.5 ml RPE buffer was added to the column and centrifuged (12000 g, 15 sec, RT). This step was repeated again for 2 min. 20-30 ul of RNase-free water was used to elute the RNA. The RNA concentration was determined using a Nanodrop spectrophotometer and 1μg total RNA was used for cDNA synthesis using the iScriptTM cDNA Synthesis kit, according to manufacturer`s instructions (BioRad). Gene expression analysis was performed using quantitative real-time polymerase chain reaction (qPCR) on a QuantStudio 7 Flex Real-Time PCR System (Thermo Fisher Scientific, USA). The thermoprofile was 95ºC for 15 minutes and 40 cycles of 94ºC for 15 seconds, 55ºC for 20 seconds and 72ºC for 2 minutes. The total PCR volume of 20 microliters consisted of 10 μl 2x QuantiTectTM SYBR® Green PCR master mix (Qiagen), 2 μl 10x QuantiTect Primer Assay (Qiagen) and 20 ng cDNA (2 ng were used for actin) in 96-well optical plates. Extracted DNA samples were analysed in triplicates. The pre-validated QuantiTect Primer Assays were obtained from Qiagen. The gene expression was determined by the method of direct comparison of C T values (C T > 35 was rejected) and relative quantities calculated by the ΔΔCT equation or transformed into linear form. Transcripts were normalized to the quantity of Actin and GAPDH for each condition.

Table 1.
primers used in qPCR.
| Gene name | Accession number |
| SNAI1 | Hs_SNAI1_1_SG |
| SNAI2 | Hs_SNAI2_1_SG |
| CDH1 | Hs_CDH1_1_SG |
| TWIST1 | Hs_TWIST1_1_SG |
| TGFB1 | Hs_TGFB1_1_SG |
| STAT3 | Hs_STAT3_1_SG |
| VIM | Hs_VIM_1_SG |
| CD248 | Hs_CD248_1_SG |
| GAPDH | Hs_GAPDH_1_SG |
| ACTB | Hs_ACTB_1_SG |
2.7. Statistical Analysis
T-tests and analysis of variance were used to compare survival rates. Statistical analysis was performed using Microsoft Excel for Mac V16.77 or GraohPad Prism V8/9 software (GraphPad Software, San Diego, CA, USA) software.
3. Results
3.1. Comparative experiments of cell viability
In normal cells, viability after 24 hours of hydrogen and vitamin C treatment increased compared to controls in all five conditions, with or without irradiation. In contrast, the viability rate of cancer cells decreased in all five conditions compared to the control, except one column (Table 2 MDA-MB-231, before irradiation, with 0.2mM vitamin C).
Table 2 shows that in the absence of irradiation, the 24-hour viability rates of normal cells tended to increase with the addition of vitamin C or hydrogen alone. In the case of irradiation, the highest viability rate at 24 hours was observed when 1 mM of vitamin C and hydrogen were added to the culture medium (statistically significant only treated before and after irradiation). However, vitamin C tended to increase viability considerably even when used alone. The viability rate tended to be higher when both vitamin C and hydrogen were added at two time points, before and after irradiation. Table 3 shows that in MDA-MB231, both vitamin C and hydrogen tended to suppress the viability rate even when used as sperate treatment. The addition of vitamin C and hydrogen along with irradiation decreased the viability rate in all five conditions, but the addition of 1 mM of vitamin C and hydrogen to the culture medium significantly suppressed the viability rate 24 hours after irradiation.
Table 4 shows that in GL261, the addition of vitamin C and hydrogen to the culture medium suppressed viability after 24 hours.
Under the condition of 1 mM vitamin C plus hydrogen therapy, statistically significant results were obtained in all but the before and after irradiation periods. The lowest viability rate was observed in without irradiation, which can be interpreted as the fact that in highly malignant glioblastomas, half-way anticancer drugs or irradiation may activate surviving cancer cells and increase their proliferation rate.
These results suggest that in normal cells, the combination of 1 mM vitamin C and hydrogen is the most effective radioprotective agent.
Similarly, in cancer cells, the combination of 1 mM vitamin C and hydrogen is likely to enhance the anticancer effect of radiation.
The antioxidant effect of combination therapy in normal cells that underwent radiation therapy (Figure 8).
Normal cells (HUVEC) were used to evaluate the antioxidant effect of combination therapy in response to radiation treatment (4Gys) by measuring ROS production in normal cells. In vitro treatment started, either after radiation treatment, or before and after radiation. Vitamin C was tested at different concentrations: 0,2mM, 1mM, 5mM, 10mM alone or in combination with hydrogen. The combination therapy reduced ROS in normal cells when treatment started after RT directly with best efficacy achieved at H+10mM Vitamin C as shown in Figure 8.
3.2. Confirmation of apoptosis (Figure 9, Figure 10, Figure 11 and Figure 12)
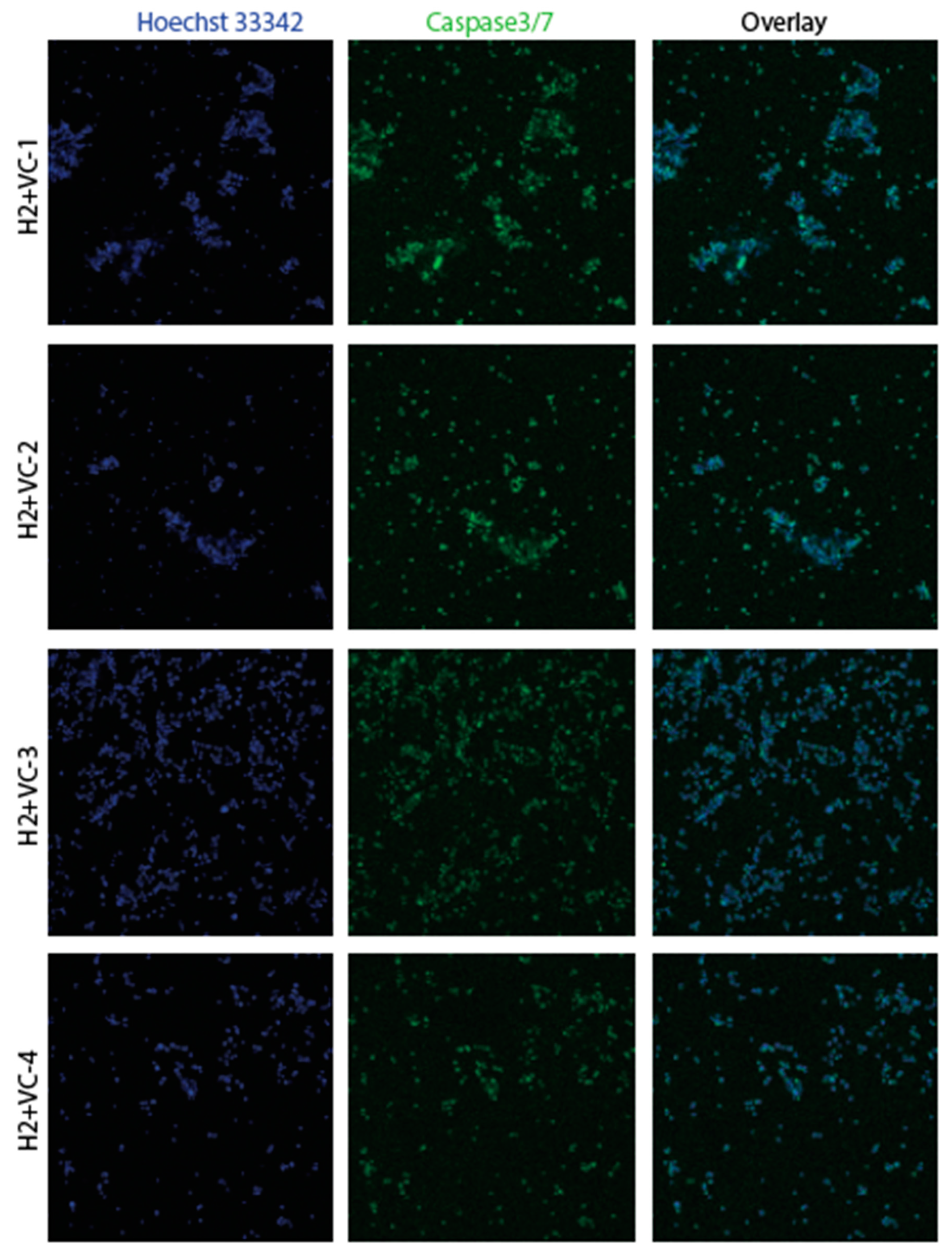
In MDA-MB231, the FLICA test was used to confirm the extent to which apoptosis actually occurred in the cells when vitamin C and hydrogen were added and irradiated. This test was performed only under the condition of the lowest survival rate (hydrogen and vitamin C administered twice before and after irradiation) because the test was performed to confirm what was happening to the cells when the viability rate decreased. Photographs were taken of the same specimens at four different locations. The four conditions were: 1. control (culture medium only), 2. 1mM vitamin C, 3. hydrogen, and 4. 1mM vitamin C and hydrogen. For conditions 2, 3, and 4, the cells were treated before and after irradiation. Figure 9 shows that little apoptosis occurred in control with only culture medium. Figure 10 shows that administration of vitamin C alone with radiation caused apoptosis at a low rate. Figure 11 shows that overall apoptosis occurred with hydrogen treatment with radiation. Figure 12 shows vitamin C treatment in combination with hydrogen with radiation exposure, apoptosis occurred overall at a much higher rate. The changes in the cells were confirmed by FLICA assay, and apoptosis was observed in cancer cells treated with hydrogen and vitamin C. The results showed that the caspase activity in viable cells was reduced by hydrogen and vitamin C treatment, and that apoptosis occurred in cancer cells treated with hydrogen and vitamin C.
The results of the FLICA test corroborated the experimental results for viability, suggesting that hydrogen and vitamin C combination therapy with radiation had anticancer effects, and hydrogen may have a greater anticancer effect than vitamin C in MDA-MB231.
Apoptosis occurred at the highest rate in the combination of vitamin C and hydrogen with radiation, suggesting that the anti-cancer effect of the combination treatment is high.
Figure 9.
Apoptosis confirmed by FLICA: control apoptosis rarely occurred in control with only culture medium.
Figure 9.
Apoptosis confirmed by FLICA: control apoptosis rarely occurred in control with only culture medium.
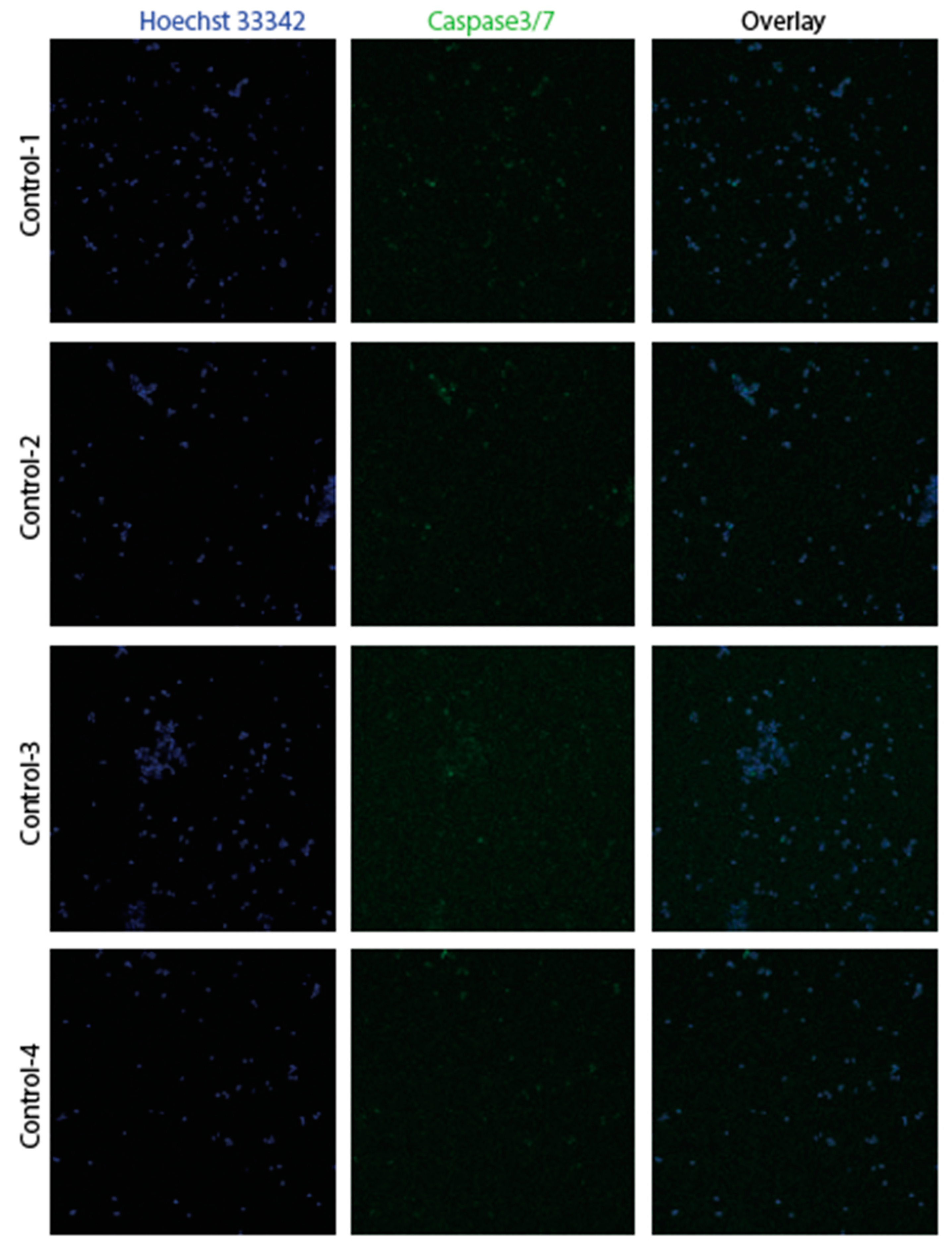
Figure 10.
Apoptosis confirmed by FLICA :vitamin C Apoptosis occurred at a low rate.
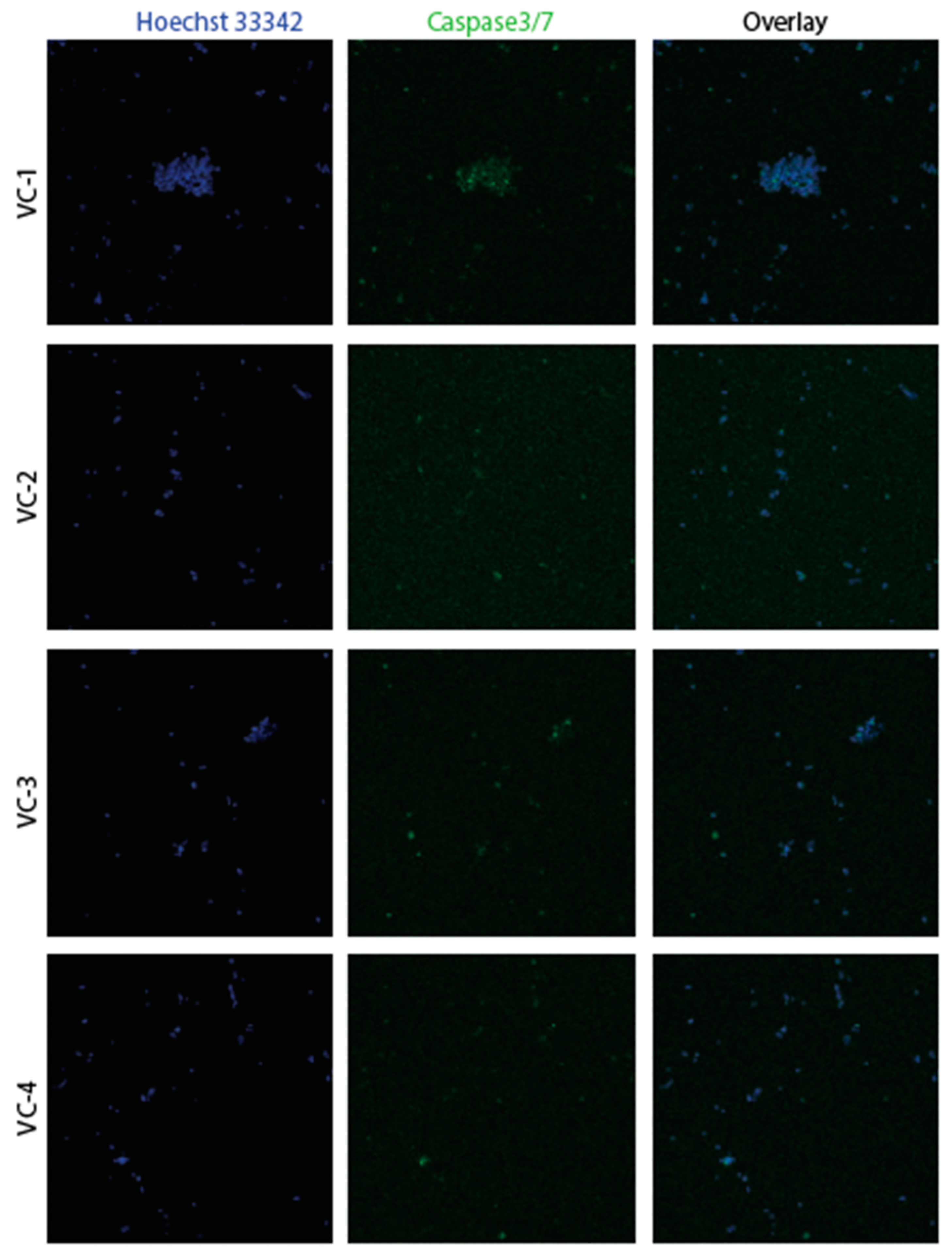
Figure 11.
Apoptosis confirmed by FLICA :hydrogen overall apoptosis occurred.
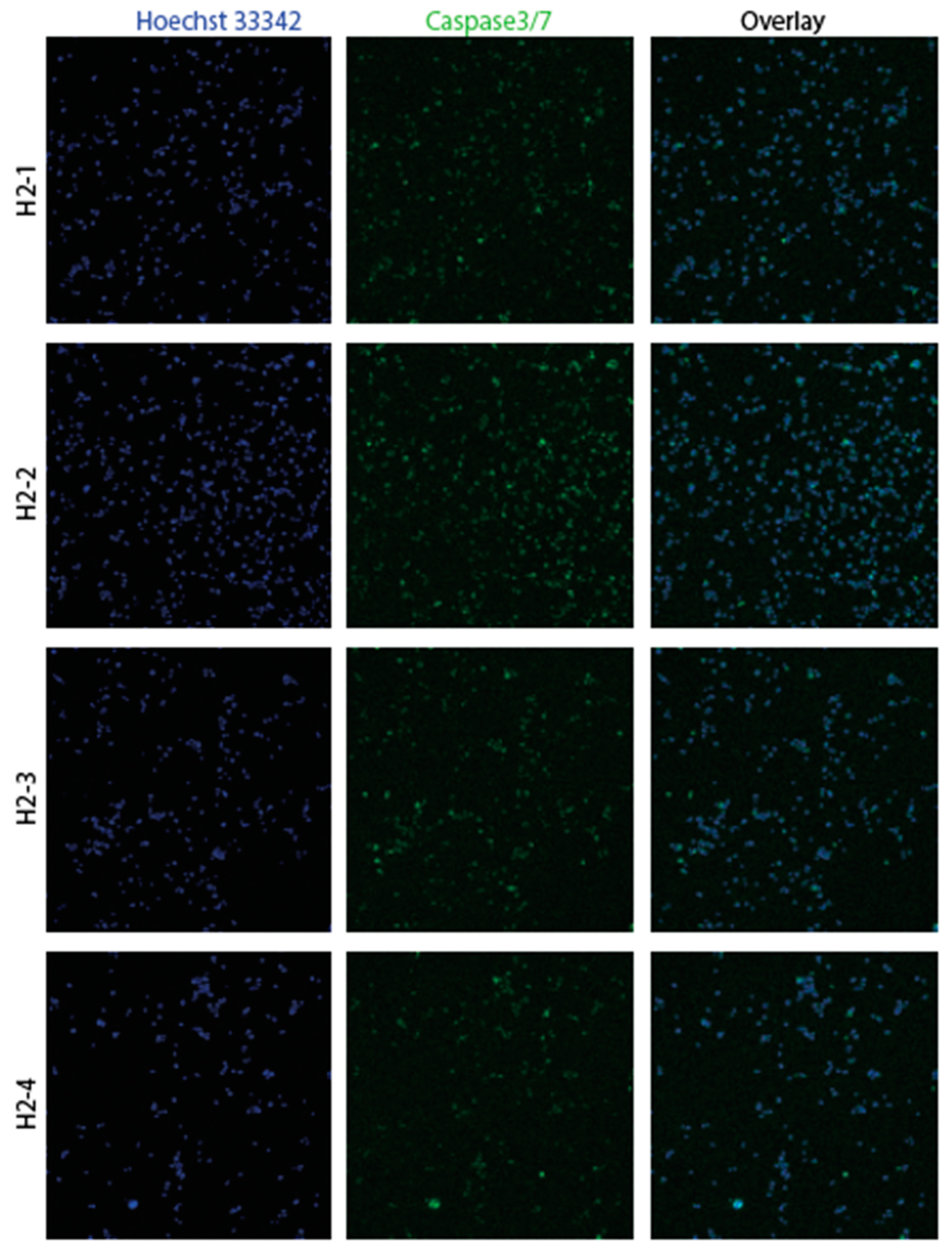
Figure 12.
Apoptosis confirmed by FLICA :hydrogen and vitamin C apoptosis occurred overall at a much higher rate.
Figure 12.
Apoptosis confirmed by FLICA :hydrogen and vitamin C apoptosis occurred overall at a much higher rate.
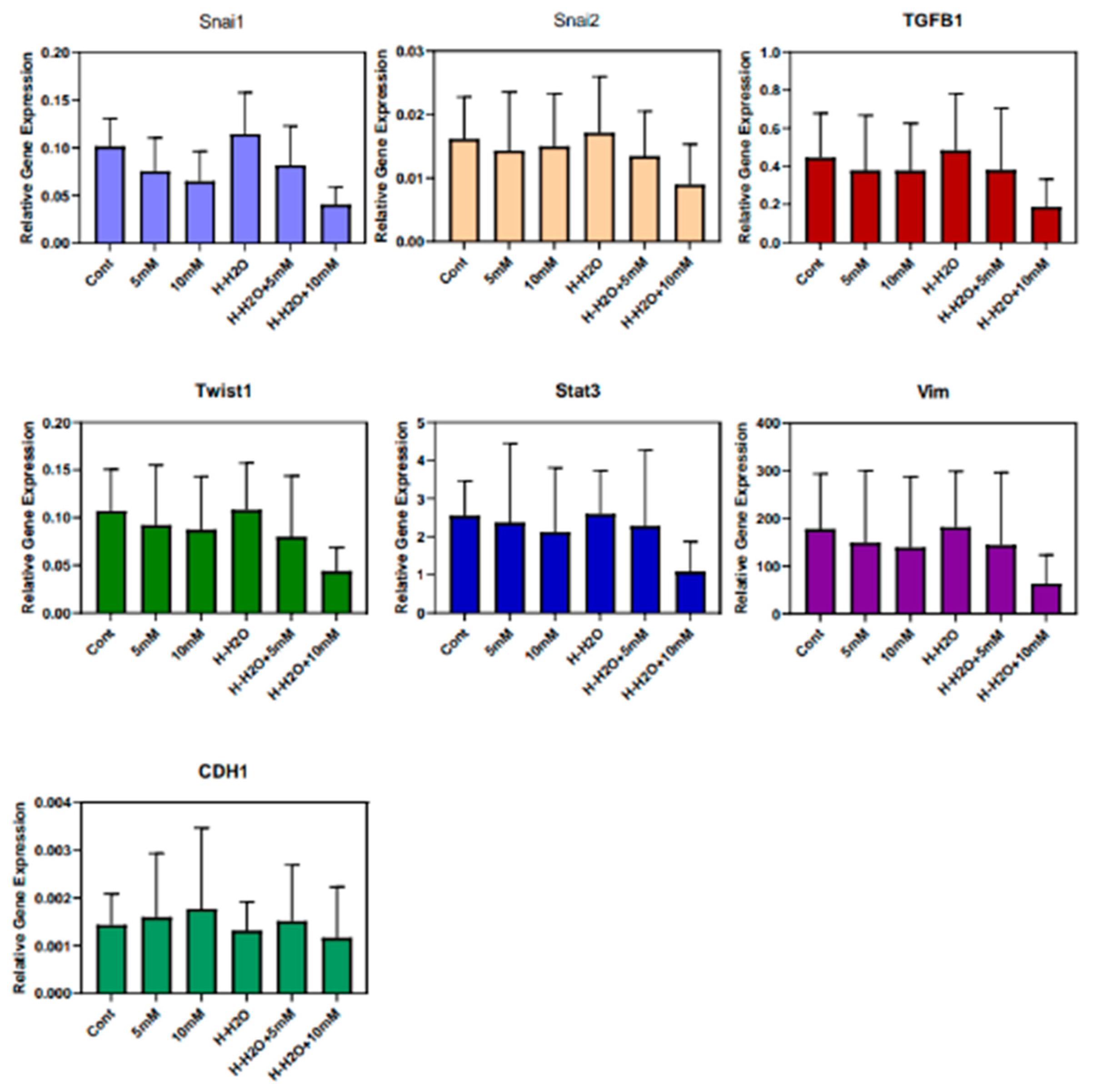
3.3. The EMT signature in GBM
In high grade glioma, EMT gene signature is associated with therapy resistance [64]. In our work, we treated GL261 glioma cells with Vitamin C and hydrogen. The combination of Vitamin C treatment with hydrogen reduced the gene expression of most EMT gene set (Snai1, Snai2, Twist1, Stat3, TGFB1, Vim) almost by 50%. The expression of cadherin (CDH1) seemed to be less affected (Figure 12). The result suggests that hydrogen and vitamin C combination therapy has anti-cancer-effects through reducing EMT signature that usually mediate therapy resistance and tumor invasion.
Figure 13.
In vitro treatment of GL261 glioma cell line with hydrogen and vitamin C showing the combination therapy reduce EMT gene signature up to 50%, while cadherin (CDH1) expression seemed to be less affected. Gene expression was quantified by qPCR. EMT gee set included Snai1, Snai2, Twist1, Stat3, TGFB1, Vim, CDH1.
Figure 13.
In vitro treatment of GL261 glioma cell line with hydrogen and vitamin C showing the combination therapy reduce EMT gene signature up to 50%, while cadherin (CDH1) expression seemed to be less affected. Gene expression was quantified by qPCR. EMT gee set included Snai1, Snai2, Twist1, Stat3, TGFB1, Vim, CDH1.
Upon radiation treatment, the combination therapy with high concentration of vitamin C achieved the best consistent EMT inhibitory effect (Figure 14). Thus we see that the combination of high dose Vitamin C (10mM) with hydrogen has inhibitory effect on the intrinsic EMT expression in GL261, and RT-induced EMT, suggesting antitumoral effect.
4. Discussion
4.1. Effects of vitamin C and Hydrogen Peroxide(H2O2)
The effectiveness of vitamin C in cancer treatment was reported by Pauling as early as in 1976 [65]. Over the past 50 years, the effectiveness of vitamin C in cancer treatment has been recognized to some extent. Vitamin C is shown to not only decreases radiation-associated complications but has also the potential to kill cancer cells directly. Although, there is no clear evidence based on human randomized controlled studies, animal studies and clinical case reports show the preventive effects on radiation-induced injuries [14,15,16]. This may be attributed to the effect of vitamin C as an antioxidant and the fact that vitamin C has an anti-inflammatory effect and may reduce inflammation in cancer patients [47]. This property could be helpful for preventing radiation injury. Moreover, vitamin C may enhance the efficacy of radiation in the treatment of cancer, as it is suggested to function as a radiosensitizer [40,41,42,43]. Importantly, vitamin C is harmless to normal cells, and selectively targets cancer cells [44]. Vitamin C acts as a pro-drug for H2O2 formation and, through this mechanism, kills cancer cells [45]. When vitamin C is sufficiently concentrated in the blood, it is transported outside blood vessels, generating large quantities of hydrogen peroxide (H2O2). Normal, healthy cells are unaffected by H2O2, generating by vitamin C at higher concentrations, as they possess enzymes such as catalase that can neutralize it. Since the cancer cells lack these enzymes, the cellular function is dramatically altered when they take in reactive oxygen and as a consequence of this, cancer cells enter into apoptosis process [66]. Previously, it has been shown by in vitro experiments that increasing vitamin C concentration to the maximum level, up to 20 mM, will kill almost all cancer cells [48]. However, even when intravenous infusions temporarily increased the concentration of vitamin C in the blood, the anticancer effect was often not sufficient. This was thought to be due to some other factors that prevented vitamin C from becoming the standard of care in cancer treatment so far. To overcome this obstacle, the authors considered combining vitamin C with hydrogen. Although hydrogen and vitamin C combination therapy is still not sufficient in terms of anticancer activity, the results of this study suggest that it may be quite effective in terms of radioprotection. Further in vivo experiments are required to confirm the antitumoral efficacy of combining vitamin C and hydrogen.
4.2. The effects of hydrogen
Hydrogen is originally produced by intestinal bacteria in the gut and is naturally present in the body [67]. Previously, it was shown that hydrogen acts as a therapeutic and preventive antioxidant in cultured cells and has cytoprotective effects against oxidative stress [68]. The mechanisms for the effects of hydrogen are also becoming clearer [69]. Hydrogen can rapidly pass through biological membranes and diffuse into the cytosol because of its small size. In addition, hydrogen is soluble in both water and lipids, which contributes to its diffusibility. Hydrogen reaches the cell nucleus and mitochondria, protecting nuclear DNA and mitochondria. In addition, it passes through the blood brain barrier. Hydrogen selectively removes highly active oxidants such as hydroxyl radicals (•OH) induced by radiation and does not react with ROS, which have low reactivity, such as superoxide, H2O2, and CO. ROS with low reactivity play important roles in signal transduction and the immune system [70]. Other antioxidant supplements such as vitamin E also remove all these ROS, which is necessary, and have possibility to increase mortality [8,9,10]. It means that the fear that antioxidants support tumor cells.
In the past ten years, several studies reported the preventive and therapeutic effects of hydrogen. These studies cover various biological effects against oxidative stress in almost all organs [71,72,73]. Studies on the treatment of diseases with hydrogen have reported that no side effects at all occur. It became clear that the biological and medical roles of hydrogen are broad, including anti-inflammatory, antiapoptotic, and antiallergic effects. In addition to its efficacy in animal models, many studies examined and reported the efficacy of hydrogen in clinical practice. Furthermore, hydrogen may act as a radioprotector by neutralizing •OH radicals in irradiated tissues. Cyuai et al. showed that the effects of hydrogen are similar to those of Amifostine without side effects, thereby, it can be an ideal radioprotective agent [29]. Yang et al. showed that hydrogen induces apoptosis in endometrial cancer cells via the TNF and NF-κB pathways [56,57]. They also showed that irradiation of HEC1A cells in hydrogen-treated cultures significantly increased the rate of apoptosis compared to normal cultures, indicating that hydrogen is an effective enhancer of radiotherapy. Another study by Liu et al. showed that hydrogen is a potential antitumor agent in GBM therapy [58].
4.3. Expected benefits of hydrogen and vitamin C combination therapy
Under certain conditions, vitamin C plays a role as a pro-oxidant and may induce oxidative stress [74,75]. When vitamin C leads to the production of excess H2O2, the generation of •OH increases and may damage normal cells. In such circumstance, hydrogen can selectively remove •OH and compensate for the effect of vitamin C. Inflammation is associated with cancer metastasis [76,77]. Our data suggests that the combination therapy of Vitamin C with hydrogen reduced ROS level in normal cells supporting the antioxidant role of this treatment.
Our results showed that vitamin C and hydrogen each had anticancer effects on tumor cells and protective effects on normal cells. These effects were further increased when vitamin C and hydrogen were combined. Furthermore, when irradiation was added, the anticancer effect of radiation was enhanced and the radioprotective effect on normal cells was demonstrated. These effects were greater during combination treatment in contrast to treatment with vitamin C and hydrogen alone. Moreover, a higher concentration of vitamin C at 1 mM was more effective than at 0.2 mM. The strongest effects were obtained when hydrogen and vitamin C were added to the cells twice, before and after irradiation. Previously, experiments using mice have shown that using vitamin C before and after irradiation suppresses radiation-induced gastrointestinal damage [14]. Interestingly, our experiments also showed that the addition of hydrogen and vitamin C before and after irradiation was the most effective strategy. However, the viability rate of glioblastoma cells increased after irradiation compared to that without irradiation. This may be due to the fact that irradiation activates the cells and increases the proliferation rate as it is the case of this very malignant tumors in patients. Experiments showed that the hydrogen and vitamin C combination therapy protects normal cells from radiation and impairs cancer cells. It was confirmed that apoptosis occurred in cancer cells after hydrogen and vitamin C combination therapy and irradiation. Furthermore, in glioblastoma, the EMT signature in GBM was reduced in response to combination therapy, which suggests that hydrogen and vitamin C combination therapy has anti-cancer-effects through reducing EMT pathway that play essential role in therapy resistance and tumor invasion.
4.4. Hydrogen and vitamin C combination therapy in health and disease
We aim to routinely administer vitamin C injection and hydrogen inhalation to all patients undergoing radiation therapy. Hydrogen inhalation and high-dose vitamin C injection should be administered before radiation and additional treatment after radiation will boost the effect. The hydrogen and vitamin C combination therapy may also be effective for preventing the complications of brachytherapy in various cancers including prostate cancer, as well as in patients receiving radioiodine therapy for thyroid cancer. In addition, the combination therapy has capacity to reduce the risk of secondary cancer induced by radiation. In addition to cancer patients, individuals exposed to radiation, such as those undergoing upper gastrointestinal tests, CT scans, and those traveling by airplane or space flight, may benefit from vitamin C treatment (orally or via injection according to the situation) and hydrogen (gas inhalation, hydrogen saturated water, hydrogen bath, or hydrogen tablet, according to the situation) before and after the exposure. Regarding medical exposure, the combination therapy will reduce potential radiation-related cancer risks. The proposed combination therapy may also be effective against the risk of continuous radiation exposure in cases such as; individuals living in radiation polluted regions such as Chernobyl and Fukushima in Japan, individuals receiving internal exposure through radiation polluted foods, and individuals working as radiologists or radiation technicians. In summary, the combination therapy is recommended for all people to improve health and prevent diseases by reducing active oxygen.
4.5. Limitations and issues to be solved
This study is an in vitro experiment based on a hypothesis derived from a case. Future clinical studies are needed to confirm the hypothesis. The amount of vitamin C covered by medical insurance is small and far from a sufficient dose in many countries. In addition, there are not so many clinics that offer vitamin C injection, and the procedure is expensive for patients although, oral vitamin C intake via supplements is an alternative. Patients can take vitamin C supplement by themselves to compensate for the needs. Moreover, hydrogen therapy is not covered by insurance. Since hydrogen gas generators are relatively expensive and sometimes difficult to purchase for individuals, hydrogen-rich water and hydrogen supplements may play an important role. Both these alternatives, vitamin C and hydrogen supplement are easy to obtain by patients. In addition, the price of high-dose vitamin C injection and hydrogen inhalation may decrease as the demand increases. The widespread use of this therapy should benefit patients, and it would be desirable for health insurance to cover the cost of combination therapy. Unfortunately, most radiology specialists are unaware of the effects of the two therapies. When they consult with their doctors about incorporating hydrogen or vitamin C treatment, they are often saddened to hear that they should not use treatments for which there is little evidence, or that they will not be treated in the hospital if they do so on their own judgment. Doctors are often surprised when patients who receive the combination therapy show only mild complications, but they question the effectiveness of the combination therapy in reducing side effects of radiation. Therefore, reporting the results of combination therapy to a wider audience, especially for radiology specialists, should be raised. Since there is no evidence from randomized controlled trials, it is hoped that trials will be conducted in the future.
5. Conclusion
Combination therapy consisting of high-dose vitamin C injection and hydrogen inhalation may reduce the side effects of radiotherapy by decreasing •OH associated with the reaction of radiation with H2O. Hydrogen facilitates vitamin C absorption and have ability to prevent its excessive oxidative effects. Both therapies are safe and may improve the QOL of patients, as well as decrease medical expenses associated with the treatment of the side effects of radiotherapy. The anti-inflammatory effects of the combination therapy may attenuate radiation injuries and prevent cancer metastasis. The antitumor effects of the combination therapy could also improve survival in cancer patients. Although further studies are needed to confirm the effects of the combination therapy, we believe that the therapy has potential significance for preventing and treating radiation-induced damage in cancer patients. This combination therapy seems to be effective against many conditions, not only in radioprotection, but also in many diseases such as herpes simplex infection, shingles, cystitis, hearing loss, glaucoma, cataracts, renal failure, liver dysfunction, stroke, angina pectoris pain from rheumatoid arthritis, stomatitis, asthma, atopic dermatitis, non-tuberculous mycobacteria, psoriasis, the common cold, pneumonia, lower back pain, stiff shoulder, sunburn, insomnia, and acne, among others. All these diseases are caused by reactive oxygen species and inflammation. The combination of hydrogen and vitamin C is expected to be a savior for many diseases and for health promotion for all people.
6. Patents
A patent for the hydrogen and vitamin C combination therapy is pending from Hosei University, to which M.M. belongs.
Author Contributions
M.M. conceived the study, conducted clinical and cellular experiments, and wrote the paper. S.Z. executed cellular experiments and statistical analyses. J.B. contributed to glioblastoma cell experiments, extracted glioblastoma mRNA, performed radiation experiments on cells, and contributed to writing relevant sections of the paper. CM and KI performed ROS staining and data analysis P.I. handled qPCR and its subsequent data analysis. A.M. provided clinical conceptual guidance and supervised the experiments. A.M. and P.U. oversaw the research.
Funding
This research received no funding. Part of the publication cost of the paper was supported by The Hosei Society of Sustainability Studies.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest statement
The authors declare no conflicts of interest.
References
- Berrington de González A, Mahesh M, Kim KP, Bhargavan M, Lewis R, Mettler F, Land C. Projected cancer risks from computed tomographic scans performed in the United States in 2007. Arch Intern Med. 2009 Dec 14;169(22):2071-7. [CrossRef]
- Fischer N, Seo EJ, Efferth T. Prevention from radiation damage by natural products. Phytomedicine. 2018; Aug 1;47:192-200. [CrossRef]
- Yahyapour R, Shabeeb D, Cheki M, Musa AE, Farhood B, Rezaeyan A, Amini P, Fallah H, Najafi M. Radiation Protection and Mitigation by Natural Antioxidants and Flavonoids: Implications to Radiotherapy and Radiation Disasters. Curr Mol Pharmacol. 2018;11(4):285-304. [CrossRef] [PubMed]
- Saif-Elnasr M, Abdel-Aziz N, Ibrahim EL-Batal A. Ameliorative effect of selenium nanoparticles and fish oil on cisplatin and gamma irradiation-induced nephrotoxicity in male albino rats. Drug Chem Toxicol. 2018; Sep 11:1-10. [CrossRef]
- Nukala U, Thakkar S, Krager KJ, Breen PJ, Compadre CM. Aykin-Burns N. Antioxidant Tocols as Radiation Countermeasures (Challenges to be Addressed to Use Tocols as Radiation Countermeasures in Humans). Antioxidants (Basel). 2018 Feb 23;7(2). pii: E33. [CrossRef]
- Camphausen K, Citrin D, Krishna MC, Mitchell JB. Implications for tumor control during protection of normal tissues with antioxidants. J Clin Oncol. 2005 Aug 20;23(24):5455-7. [CrossRef] [PubMed]
- Hawk MA, McCallister C, Schafer ZT. Antioxidant Activity during Tumor Progression: A Necessity for the Survival of Cancer Cells? Cancers. 2016 Oct; 8(10): 92. [CrossRef]
- Bairati I, Meyer F, Gélinas M, Fortin A, Nabid A, Brochet F, Mercier JP, Têtu B, Harel F, Abdous B, Vigneault E, Vass S, Del Vecchio P, Roy J. Randomized trial of antioxidant vitamins to prevent acute adverse effects of radiation therapy in head and neck cancer patients. J Clin Oncol. 2005 Aug 20;23(24):5805-13. [CrossRef] [PubMed]
- Meyer F, Bairati I, Fortin A, Gélinas M, Nabid A, Brochet F, Têtu B. Interaction between antioxidant vitamin supplementation and cigarette smoking during radiation therapy in relation to long-term effects on recurrence and mortality: a randomized trial among head and neck cancer patients. Int J Cancer. 2008 Apr 1;122(7):1679-83. [CrossRef] [PubMed]
- Bjelakovic G, Nikolova D, Gluud C. Meta-regression analyses, meta-analyses, and trial sequential analyses of the effects of supplementation with beta-carotene, vitamin A, and vitamin E singly or in different combinations on all-cause mortality: do we have evidence for lack of harm? PLoS One. 2013 Sep 6;8(9):e74558. [CrossRef]
- Orditura M, De Vita F, Roscigno A, Infusino S, Auriemma A, Iodice P, Ciaramella F, Abbate G, Catalano G. Amifostine: A selective cytoprotective agent of normal tissues from chemo-radiotherapy induced toxicity (Review). Oncol Rep. 1999 Nov-Dec;6(6):1357-62. [CrossRef] [PubMed]
- Koukourakis, MI. Radiation damage and radioprotectants: new concepts in the era of molecular medicine. Br J Radiol. 2012 Apr;85(1012):313-30. [CrossRef]
- Ferraiolo DM, Veits-keenan A. Insufficient evidence for interventions to prevent dry mouth and salivary gland dysfunction post head and neck radiotherapy. Evid Based Dent. 2018 Mar 23;19(1):30-31. [CrossRef]
- Ito Y, Kinoshita M, Yamamoto T, Sato T, Obara T, Saitoh D, Seki S, Takahashi Y. A combination of pre- and post-exposure ascorbic acid rescues mice from radiation-induced lethal gastrointestinal damage. Int J Mol Sci. 2013 Sep 27;14(10):19618-35. [CrossRef]
- Jafari E, Alavi M, Zal F. The evaluation of protective and mitigating effects of vitamin C against side effects induced by radioiodine therapy. Radiat Environ Biophys. 2018 Aug;57(36):233-240. [CrossRef]
- Velauthapillai N, Barfett J, Jaffer H, Mikulis D, Murphy K. Antioxiants taken orally prior to diagnostic radiation exposure can prevent DNA injury. J Vasc Interv Radiol. 2017 Mar;28(3):406-411. [CrossRef]
- Kennedy M, Bruninga K, Mutlu EA, Losurdo J, Choudhary S, Keshavarzian A. Successful and sustained treatment of chronic radiation proctitis with antioxidant vitamins E and C. Am J Gastroenterol. 2001 Apr;96(4):1080-4. [CrossRef] [PubMed]
- Sato T, Kinoshita M, Yamamoto T, Ito M, Nishida T, Takeuchi M, Saitoh D, Seki S, Mukai Y. Treatment of irradiated mice with high-dose ascorbic acid reduced lethality. PLoS One. 2015 Feb 4;10(2):e0117020. [CrossRef]
- Saga R, Uchida T, Takino Y, Kondo Y, Kobayashi H, Kinoshita M, Saitoh D, Ishigami A, Makishima M. Radiation-induced gastrointestinal syndrome is exacerbated in vitamin C-insufficient SMP30/GNL knockout mice. Nutrition. 2021 Jan;81:110931. [CrossRef] [PubMed]
- Liu C, Cui J, Sun Q, Cai J. Hydrogen therapy may be an effective and specific novel treatment for acute radiation syndrome. Med Hypotheses. 2010 Jan;74(1):145-6. [CrossRef]
- Schoenfeld MP, Ansari RR, Zakrajsek JF, Billiar TR, Toyoda Y, Wink DA, Nakao A. Hydrogen therapy may reduce the risks related to radiation-induced oxidative stress in space flight. Med Hypotheses. 2011 Jan;76(1):117-8. [CrossRef]
- Qian L, Shen J, Chuai Y, Cai J. Hydrogen as a New Class of Radioprotective Agent. Int J Biol Sci. 2013 Sep 14;9(9):887-94. [CrossRef]
- Terasaki Y, Ohsawa I, Terasaki M, Takahashi M, Kunugi S, Dedong K, Urushiyama H, Amenomori S, Kaneko-Togashi M, Kuwahara N, Ishikawa A, Kamimura N, Ohta S, Fukuda Y. Hydrogen therapy attenuates irradiation-induced lung damage by reducing oxidative stress. Am J Physiol Lung Cell Mol Physiol. 2011 Oct;301(4):L415-26. [CrossRef] [PubMed]
- Slezák J, Kura B, Frimmel K, Zálešák M, Ravingerová T, Viczenczová C, Okruhlicová Ľ, Tribulová N. Preventive and therapeutic application of molecular hydrogen in situations with excessive production of free radicals. Physiol Res. 2016 Sep 19;65 Suppl 1:S11-28. [CrossRef] [PubMed]
- Hu Q, Zhou Y, Wu S, Wu W, Deng Y, Shao A. Molecular hydrogen: A potential radioprotective agent. Biomed Pharmacother. 2020 Oct;130:110589. [CrossRef] [PubMed]
- Abou-Hamdan M, Gardette B, Cadet J, Gharib B, De Reggi M, Douki T, Triantaphylides C. Molecular hydrogen attenuates radiation-induced nucleobase damage to DNA in aerated aqueous solutions. Int J Radiat Biol. 2016 Sep;92(9):536-41. [CrossRef] [PubMed]
- Kang KM, Kang YN, Choi IB, et al. Effects of drinking hydrogen-rich water on the quality of life of patients treated with radiotherapy for liver tumors. Med Gas Res. 2011 Jun 7;1(1):11. [CrossRef]
- Chuai Y, Gao F, Li B, Zhao L, Qian L, Cao F, Wang L, Sun X, Cui J, Cai J. Hydrogen-rich saline attenuates radiation-induced male germ cell loss in mice through reducing hydroxyl radicals. Biochem J. 2012 Feb 15;442(1):49-56. [CrossRef] [PubMed]
- Zhao L, Zhou C, Zhang J, Gao F, Li B, Chuai Y, Liu C, Cai J. Hydrogen protects mice from radiation induced thymic lymphoma in BALB/c mice. Int J Biol Sci. 2011 Mar 25;7(3):297-300. [CrossRef]
- Chen P, Reed G, Jiang J, Wang Y, Sunega J, Dong R, Ma Y, Esparham A, Ferrell R, Levine M, Drisko J, Chen Q. Pharmacokinetic Evaluation of Intravenous Vitamin C: A Classic Pharmacokinetic Study. Clin Pharmacokinet. 2022 Sep;61(9):1237-1249. [CrossRef]
- Stephenson CM, Levin RD, Spector T, Lis CG. Phase I clinical trial to evaluate the safety, tolerability, and pharmacokinetics of high-dose intravenous ascorbic acid in patients with advanced cancer. Cancer Chemother Pharmacol. 2013 Jul;72(1):139-46. [CrossRef]
- Hoffer LJ, Levine M, Assouline S, Melnychuk D, Padayatty SJ, Rosadiuk K, Rousseau C, Robitaille L, Miller WH Jr. Phase I clinical trial of i.v. ascorbic acid in advanced malignancy. Ann Oncol. 2008 Nov;19(11):1969-74. Erratum in: Ann Oncol. 2008 Dec;19(12):2095. [CrossRef] [PubMed]
- Welsh JL, Wagner BA, van’t Erve TJ, Zehr PS, Berg DJ, Halfdanarson TR, Yee NS, Bodeker KL, Du J, Roberts LJ 2nd, Drisko J, Levine M, Buettner GR, Cullen JJ. Pharmacological ascorbate with gemcitabine for the control of metastatic and node-positive pancreatic cancer (PACMAN): results from a phase I clinical trial. Cancer Chemother Pharmacol. 2013 Mar;71(3):765-75. [CrossRef]
- Böttger F, Vallés-Martí A, Cahn L, Jimenez CR. High-dose intravenous vitamin C, a promising multi-targeting agent in the treatment of cancer. J Exp Clin Cancer Res. 2021 Oct 30;40(1):343. [CrossRef]
- Tamura T, Hayashida K, Sano M, Suzuki M, Shibusawa T, Yoshizawa J, Kobayashi Y, Suzuki T, Ohta S, Morisaki H, Fukuda K, Hori S. Feasibility and Safety of Hydrogen Gas Inhalation for Post-Cardiac Arrest Syndrome - First-in-Human Pilot Study. Circ J. 2016 Jul 25;80(8):1870-3. [CrossRef] [PubMed]
- Cole AR, Sperotto F, DiNardo JA, Carlisle S, Rivkin MJ, Sleeper LA, Kheir JN. Safety of Prolonged Inhalation of Hydrogen Gas in Air in Healthy Adults. Crit Care Explor. 2021 Oct 8;3(10):e543. [CrossRef]
- Vollbracht C, Schneider B, Leendert V, Weiss G, Auerbach L, Beuth J. Intravenous vitamin C administration improves quality of life in breast cancer patients during chemo-/radiotherapy and aftercare: results of a retrospective, multicentre, epidemiological cohort study in Germany. In Vivo. 2011 Nov-Dec;25(6):983-90. [PubMed]
- Shinozaki K, Hosokawa Y, Hazawa M, Kashiwakura I, Okumura K, Kaku T, Nakayama E. Ascorbic acid enhances radiation-induced apoptosis in an HL60 human leukemia cell line. J Radiat Res. 2011;52(2):229-37. [CrossRef] [PubMed]
- Runtuwene J, Amitani H, Amitani M, Asakawa A, Cheng KC, Inui A. Hydrogen-water enhances 5-fluorouracil-induced inhibition of colon cancer. Peer J. 2015 Apr 7;3:e859. [CrossRef]
- Du J, Cieslak JA 3rd, Welsh JL, Sibenaller ZA, Allen BG, Wagner BA, Kalen AL, Doskey CM, Strother RK, Button AM, Mott SL, Smith B, Tsai S, Mezhir J, Goswami PC, Spitz DR, Buettner GR, Cullen JJ. Pharmacological Ascorbate Radiosensitizes Pancreatic Cancer. Cancer Res. 2015 Aug 15;75(16):3314-26. [CrossRef]
- Alexander MS, Wilkes JG, Schroeder SR. Pharmacological ascorbate reduces radiation-induced normal tissue toxicity and enhances tumor radiosensitization in pancreatic cancer. Cancer Res. 2018 Dec 15;78(24):6838-6851. [CrossRef]
- Herst PM, Broadley KW, Harper JL, McConnell MJ. Pharmacological concentrations of ascorbate radiosensitize glioblastoma multiforme primary cells by increasing oxidative DNA damage and inhibiting G2/M arrest. Free Radic Biol Med. 2012 Apr 15;52(8):1486-93. [CrossRef] [PubMed]
- Castro ML, McConnell MJ, Herst PM. Radiosensitisation by pharmacological ascorbate in glioblastoma multiforme cells, human glial cells, and HUVECs depends on their antioxidant and DNA repair capabilities and is not cancer specific. Free Radic Biol Med. 2014 Sep;74:200-9. [CrossRef] [PubMed]
- Cvissers MCM, Das AB. Potential Mechanisms of Action for Vitamin C in Cancer: Reviewing the Evidence. Front Physiol. 2018 Jul 3;9:809. [CrossRef]
- Mastrangelo D, Pelosi E, Castelli G, Lo-Coco F, Testa U. Mechanisms of anti-cancer effects of ascorbate: Cytotoxic activity and epigenetic modulation. Blood Cells Mol Dis. 2018 Mar;69:57-64. [CrossRef] [PubMed]
- Agathocleous M, Meacham CE, Burgess RJ, Piskounova E, Zhao Z, Crane GM, Cowin BL, Bruner E, Murphy MM, Chen W, Spangrude GJ, Hu Z, DeBerardinis RJ, Morrison SJ. Ascorbate regulates haematopoietic stem cell function and leukaemogenesis. Nature. 2017 Sep 28;549(7673):476-481. [CrossRef]
- Mikirova N, Casciari J, Rogers A, Taylor P. Effect of high-dose intravenous vitamin C on inflammation in cancer patients. J Transi Med. 2012 Sep 11;10:189. [CrossRef]
- Chen Q, Espey MG, Krishna MC, Mitchell JB, Corpe CP, Buettner GR, Shacter E, Levine M. Pharmacologic ascorbic acid concentrations selectively kill cancer cells: action as a pro-drug to deliver hydrogen peroxide to tissues. Proc Natl Acad Sci U S A. 2005 Sep 20;102(38):13604-9. [CrossRef]
- Yun J, Mullarky E, Lu C, Bosch KN, Kavalier A, Rivera K, Roper J, Chio II, Giannopoulou EG, Rago C, Muley A, Asara JM, Paik J, Elemento O, Chen Z, Pappin DJ, Dow LE, Papadopoulos N, Gross SS, Cantley LC. Vitamin C selectively kills KRAS and BRAF mutant colorectal cancer cells by targeting GAPDH. Science. 2015 Dec 11;350(6266):1391-6. [CrossRef]
- Cimmino L, Dolgalev I, Wang Y, Yoshimi A, Martin GH, Wang J, Ng V, Xia B, Witkowski MT, Mitchell-Flack M, Grillo I, Bakogianni S, Ndiaye-Lobry D, Martín MT, Guillamot M, Banh RS, Xu M, Figueroa ME, Dickins RA, Abdel-Wahab O, Park CY, Tsirigos A, Neel BG, Aifantis I. Restoration of TET2 Function Blocks Aberrant Self-Renewal and Leukemia Progression. Cell. 2017 Sep 7;170(6):1079-1095.e20. [CrossRef]
- Schoenfeld JD, Sibenaller ZA, Mapuskar KA, Wagner BA, Cramer-Morales KL, Furqan M, Sandhu S, Carlisle TL, Smith MC, Abu Hejleh T, Berg DJ, Zhang J, Keech J, Parekh KR, Bhatia S, Monga V, Bodeker KL, Ahmann L, Vollstedt S, Brown H, Shanahan Kauffman EP, Schall ME, Hohl RJ, Clamon GH, Greenlee JD, Howard MA, Schultz MK, Smith BJ, Riley DP, Domann FE, Cullen JJ, Buettner GR, Buatti JM, Spitz DR, Allen BG. O2⋅- and H2O2-Mediated Disruption of Fe Metabolism Causes the Differential Susceptibility of NSCLC and GBM Cancer Cells to Pharmacological Ascorbate. Cancer Cell. 2017 Apr 10;31(4):487-500.e8. Erratum in: Cancer Cell. 2017 Aug 14;32(2):268. [CrossRef]
- Carosio R, Zuccari G, Orienti I, Mangraviti S, Montaldo PG. Sodium ascorbate induces apoptosis in neuroblastoma cell lines by interfering with iron uptake. Mol Cancer. 2007 Aug 30;6:55. [CrossRef]
- Saitoh Y, Okayasu H, Xiao L, Harata Y, Miwa N. Neutral pH hydrogen-enriched electrolyzed water achieves tumor-preferential clonal growth inhibition over normal cells and tumor invasion inhibition concurrently with intracellular oxidant repression. Oncol Res. 2008;17(6):247-55. [CrossRef] [PubMed]
- Saitoh Y, Yoshimura Y, Nakano K, Miwa N. Platinum nanocolloid-supplemented hydrogendissolved water inhibits growth of human tongue carcinoma cells preferentially over normal cells. Exp Oncol. 2009 Sep;31(3):156-62. [PubMed]
- Runtuwene J, Amitani H, Amitani M, Asakawa A, Cheng KC, Inui A. Hydrogen-water enhances 5-fluorouracil-induced inhibition of colon cancer. PeerJ. 2015 Apr 7;3:e859. [CrossRef]
- Yang Y, Liu YP, Bao W, Chen JS, Xi XW. RNA sequencing analysis reveals apoptosis induction by hydrogen treatment in endometrial cancer via TNF and NF-κB pathways. Transl Cancer Res. 2020 May;9(5):3468-3482. [CrossRef]
- Yang Y, Liu PY, Bao W, Chen SJ, Wu FS, Zhu PY. Hydrogen inhibits endometrial cancer growth via a ROS/NLRP3/caspase-1/GSDMD-mediated pyroptotic pathway. BMC Cancer. 2020 Jan 10;20(1):28. [CrossRef]
- Liu MY, Xie F, Zhang Y, Wang TT, Ma SN, Zhao PX, Zhang X, Lebaron TW, Yan XL, Ma XM. Molecular hydrogen suppresses glioblastoma growth via inducing the glioma stem-like cell differentiation. Stem Cell Res Ther. 2019 ;10(1):145. 21 May. [CrossRef]
- Akagi J, Baba H. Hydrogen gas restores exhausted CD8+ T cells in patients with advanced colorectal cancer to improve prognosis. Oncol Rep. 2019 Jan;41(1):301-311. [CrossRef] [PubMed]
- Chen JB, Kong XF, Mu F, Lu TY, Lu YY, Xu KC. Hydrogen therapy can be used to control tumor progression and alleviate the adverse events of medications in patients with advanced non-small cell lung cancer. Med Gas Res. 2020 Apr-Jun;10(2):75-80. [CrossRef]
- Mohd Noor MNZ, Alauddin AS, Wong YH, Looi CY, Wong EH, Madhavan P, Yeong CH. A Systematic Review of Molecular Hydrogen Therapy in Cancer Management. Asian Pac J Cancer Prev. 2023 Jan 1;24(1):37-47. [CrossRef]
- https://riordanclinic.org/what-we-do/high-dose-iv-vitamin-c/ Last accessed on October 28, 2023.
- Ngo B, Van Riper JM, Cantley LC, Yun J. Targeting cancer vulnerabilities with high-dose vitamin C. Nat Rev Cancer. 2019 May;19(5):271-282. [CrossRef]
- Mahabir R, Tanino M, Elmansuri A, Wang L, Kimura T, Itoh T, Ohba Y, Nishihara H, Shirato H, Tsuda M, Tanaka S. Sustained elevation of Snail promotes glial-mesenchymal transition after irradiation in malignant glioma. Neuro Oncol. 2014;16:671–685. [CrossRef]
- E Cameron, L Pauling Supplemental ascorbate in the supportive treatment of cancer: Prolongation of survival times in terminal human cancer. Proc Natl Acad Sci 1976 Oct;73(10):3685-9. [CrossRef]
- Ahmad IM, Aykin-Burns N, Sim JE, Walsh SA, Higashikubo R, Buettner GR, Venkataraman S, Mackey MA, Flanagan SW, Oberley LW, Spitz DR. Mitochondrial O2*- and H2O2 mediate glucose deprivation-induced stress in human cancer cells. J Biol Chem. 2005 Feb 11;280(6):4254-63. [CrossRef] [PubMed]
- Michael, D. Levitt Production and Excretion of Hydrogen Gas in Man. N Engl J Med 1969; 281:122-127. [CrossRef]
- Ohsawa I, Ishikawa M, Takahashi K, Watanabe M, Nishimaki K, Yamagata K, Katsura K, Katayama Y, Asoh S, Ohta S. Hydrogen acts as a therapeutic antioxidant by selectively reducing cytotoxic oxygen radicals. Nat Med. 2007 Jun;13(6):688-94. [CrossRef] [PubMed]
- Radyuk, SN. Mechanisms Underlying the Biological Effects of Molecular Hydrogen. Curr Pharm Des. 2021;27(5):626-735. [CrossRef] [PubMed]
- Li Z, Xu X, Leng X. Roles of reactive oxygen species in cell signaling pathways and immune responses to viral infections. Arch Virol. 2016 Mar;162(3):603-610. [CrossRef]
- Ichihara M, Sobue S, Ito M, Ito M, Hirayama M, Ohno K. Beneficial biological effects and the underlying mechanisms of molecular hydrogen - comprehensive review of 321 original articles. Med Gas Res. 2015 Oct 19;5:12. [CrossRef]
- Zhang L, Yu H, Tu Q, He Q, Huang N. New Approaches for Hydrogen Therapy of Various Diseases. Curr Pharm Des. 2021;27(5):636-649. [CrossRef] [PubMed]
- Ohta, S. Molecular hydrogen as a preventive and therapeutic medical gas: initiation, development and potential of hydrogen medicine. Pharmacol Ther. 2014 Oct;144(1):1-11. [CrossRef]
- Podmore ID, Griffiths HR, Herbert KE, Mistry N, Mistry P, Lunec J. Vitamin C exhibits pro-oxidant properties. Nature. 1998 Apr 9;392(6676):559. [CrossRef] [PubMed]
- Lee SH, Oe T, Blair IA. Vitamin C-induced decomposition of lipid hydroperoxides to endogenous genotoxins. Science. 2001 Jun 15;292(5524):2083-6. [CrossRef] [PubMed]
- Duarte TL, Lunec J. Review: When is an antioxidant not an antioxidant? A review of novel actions and reactions of vitamin C. Free Radic Res. 2005 Jul;39(7):671-86. [CrossRef] [PubMed]
- Wu Y, Zhow BP. Inflammation is a driving force of cancer metastasis. Cell Cycle. 2009 Oct 15;8(20):3267-73.
- Coussens LM, Werb Z. Inflammation and cancer. Nature. 2002 Dec 19;420(6917):860-7.
Figure 1.
Before combination therapy.

Figure 2.
20 min after the start of combination therapy.

Figure 3.
After combination therapy.

Figure 4.
days before end of radiation therapy.

Figure 5.
days before end of radiation therapy.

Figure 6.
the last day of radiation therapy.
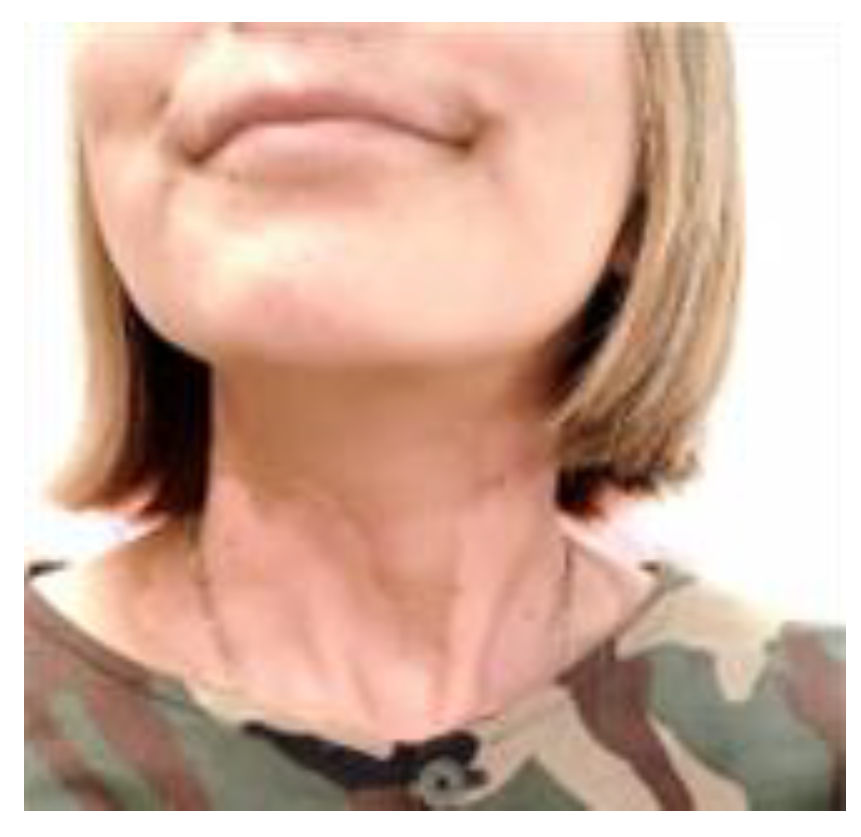
Figure 7.
one months after radiation therapy.
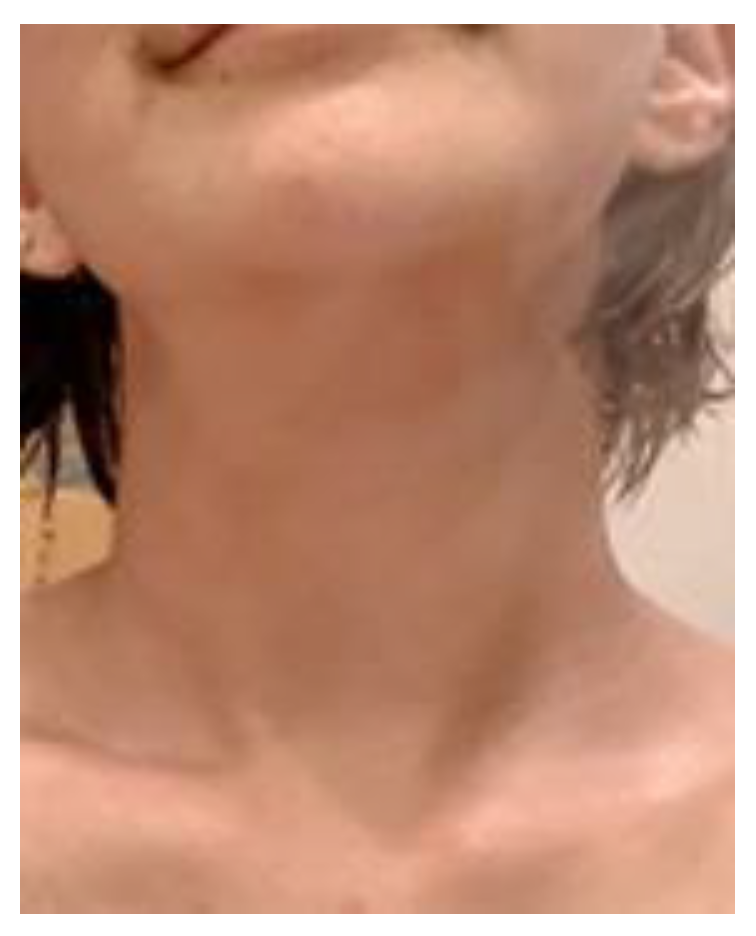
Figure 14.
In vitro treatment of GL261 glioma cell line with hydrogen and vitamin C after radiation treatment (After RT) or before and after (Before + After RT) compared to non-radiation treatment (NO-RT). Gene expression was quantified by qPCR relatively to UBC gene expression and calculated using 2^-D ct. EMT gee set included Snai1, Snai2, Twist1, Stat3, TGFB1, Vim, CDH1.
Figure 14.
In vitro treatment of GL261 glioma cell line with hydrogen and vitamin C after radiation treatment (After RT) or before and after (Before + After RT) compared to non-radiation treatment (NO-RT). Gene expression was quantified by qPCR relatively to UBC gene expression and calculated using 2^-D ct. EMT gee set included Snai1, Snai2, Twist1, Stat3, TGFB1, Vim, CDH1.
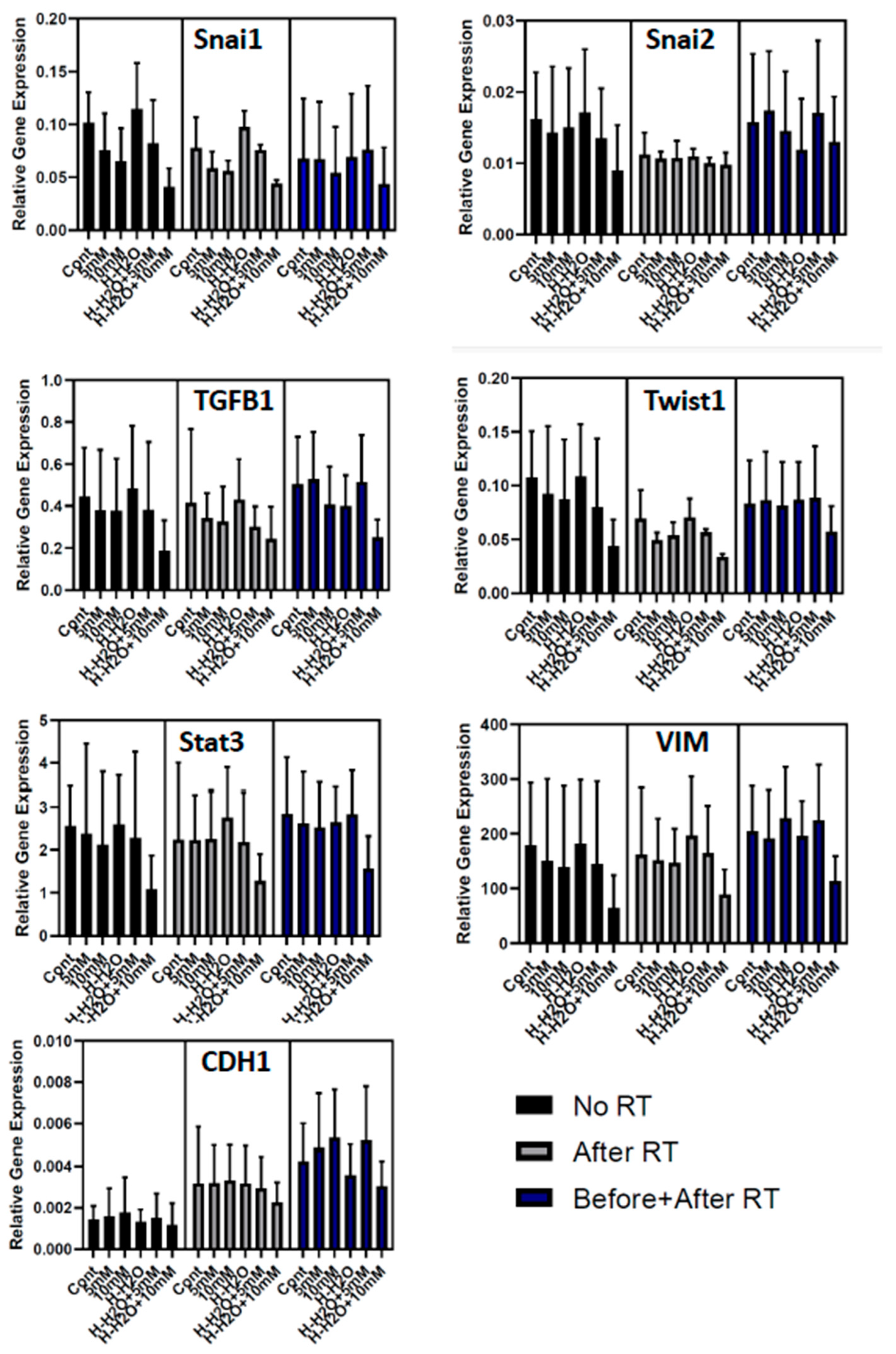
Figure 8.
Quantification of ROS production in normal cells (HUVEC) using Dihydroethidium (DHE) fluorescent staining. ROS is reduced in response to combination therapy and to higher extent when treatment started after RT than before and after RT, with highest efficacy seen in high dose 10mM+ H.
Figure 8.
Quantification of ROS production in normal cells (HUVEC) using Dihydroethidium (DHE) fluorescent staining. ROS is reduced in response to combination therapy and to higher extent when treatment started after RT than before and after RT, with highest efficacy seen in high dose 10mM+ H.
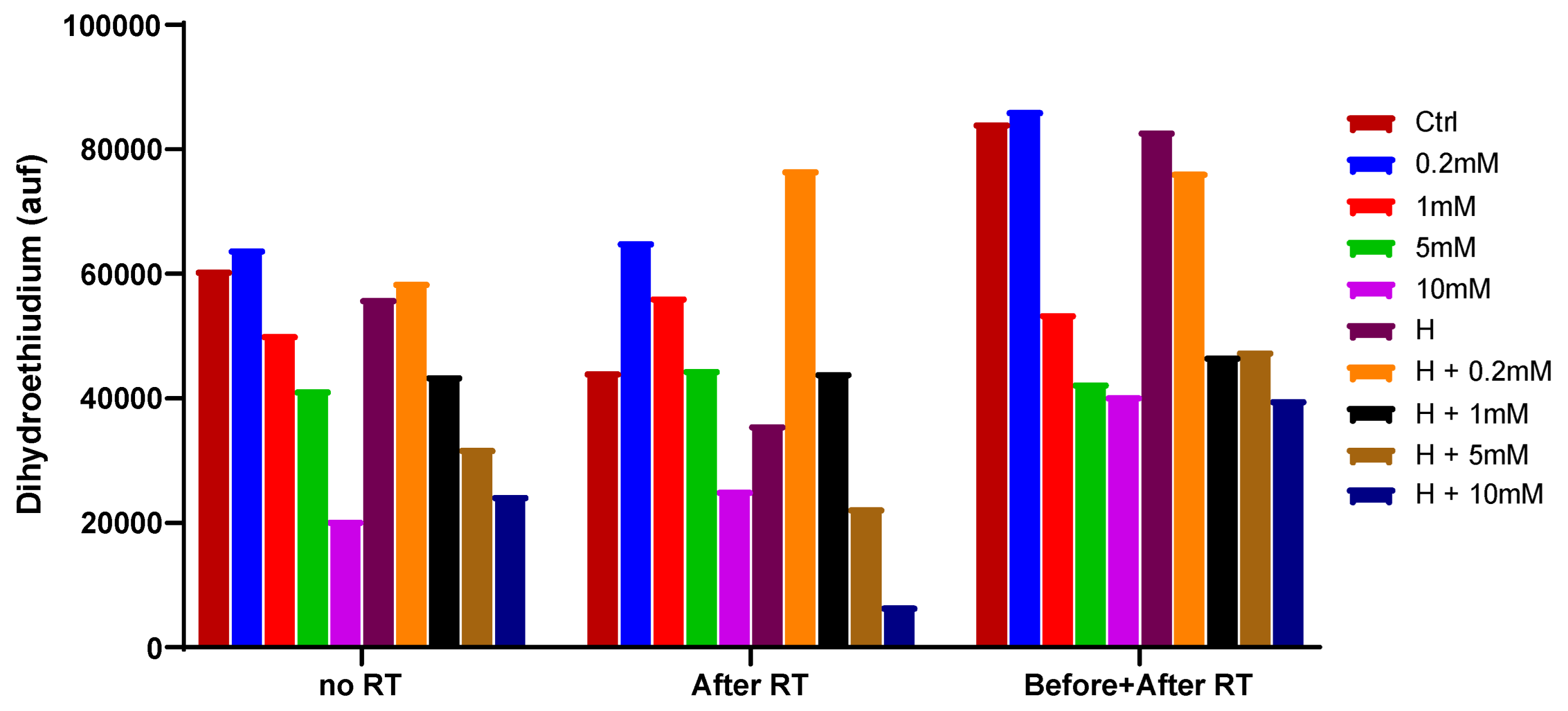
Table 2.
Normal cells (HUVEC) .
| control | VC0.2mM | VC1mM | H2 | H2+VC0.2mM | H2+VC1mM | |
| Without RD | 1 | 1.31 | 1.35 | 1.21 | 1.03 | 1.14 |
| Before RD | 1 | 1.37 | 1.34 | 1.27 | 1.31 | 1.56 |
| After RD | 1 | 1.47 | 1.47 | 1.14 | 1.37 | 1.52 |
| Before and After RD | 1 | 1.52 | 1.58 | 1.09 | 1.61 | 1.8* |
Table 3.
Brest cancer cells (MDA-MB-231).
| control | VC0.2mM | VC1mM | H2 | H2+VC0.2mM | H2+VC1mM | |
| Without RD | 1 | 0.94 | 0.81 | 0.84 | 0.87 | 0.85 |
| Before RD | 1 | 1.09 | 0.75 | 0.83 | 0.71 | 0.63* |
| After RD | 1 | 0.74 | 0.62* | 0.81 | 0.65* | 0.44** |
| Before and After RD | 1 | 0.72* | 0.62** | 0.76 | 0.76 | 0.44 *** |
Table 4.
Glioblastoma (GL261).
| control | VC0.2mM | VC1mM | H2 | H2+VC0.2mM | H2+VC1mM | |
| Without RD | 1 | 0.85 | 0.72 | 0.93 | 0.84 | 0.54* |
| Before RD | 1 | 0.89 | 0.77 | 0.89 | 0.8 | 0.73* |
| After RD | 1 | 0.86 | 0.61* | 0.83 | 0.71* | 0.71* |
| Before and After RD | 1 | 0.9 | 0.77 | 0.92 | 0.88 | 0.76 |
Survival rate of control group standardized to 1 . Analysis of variance showed a statistically significant difference compared to the control group(*:p<0.05 **:p<0.01, ***:p<0.001) .
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



