
Submitted:
18 December 2023
Posted:
19 December 2023
You are already at the latest version
Abstract
Electrical storm (ES) is defined as the presence of at least three episodes of sustained ventricular tachycardia or ventricular fibrillation within 24 hours. This patient had a previously known arterial hypertension, type II diabetes mellitus, and chronic kidney disease and has presented to the Emergency Department (ED) with symptoms of retrosternal chest pain lasting for several hours prior. The initial 12-lead electrocardiogram revealed ST segment elevation in the anterior leads (V1-V6). Emergent coronary angiography revealed an acute occlusion of the proximal left anterior descending artery (pLAD) and percutaneous coronary intervention was performed with successful implantation of one drug-eluting stent in the pLAD. On the day 8 of hospitalization, patient developed a refractory ES for which he received 50 DC shocks and did not respond to multiple lines of antiarrhythmic medications. Due to a failure of medical therapy, we decided to implant a temporary pacemaker and initiate ventricular overdrive pacing (VOP) that was successful in terminating ES. Following electrical stabilization, the patient underwent a successful ICD implantation. This case demonstrates that VOP can contribute to hemodynamic and electrical stabilization of a patient that suffers from refractory ES and this treatment modality might serve as a temporary bridge to ICD implantation.
Keywords:
acute coronary syndrome
; electrical storm
; case report
; antiarrhythmic therapy
; ventricular overdrive pacing
; VOP
; ICD
; myocardial infarction
; bridge-to-ICD
; medical management
1. Introduction
Electrical storm (ES) indicates a state of life-threatening cardiac electrical instability. It is defined as the presence of at least 3 distinct episodes of sustained ventricular tachycardia or VF in the last 24 hours [1]. We present a case of a 63- year old male who presented with acute anterior myocardial infarction (AMI) and ES refractory to multiple anti-arrhythmic therapy including propranolol, amiodarone, and lidocaine. Eventually, after temporary ventricular overdrive pacing (VOP) was initiated, the electrical storm was successfully terminated.
2. Case Report
A 63-year-old male with previously known arterial hypertension, diabetes mellitus type II, and chronic kidney disease presented to the Emergency Department (ED) with symptoms of retrosternal chest pain and diaphoresis lasting for several hours before admission. The initial electrocardiogram at the ED revealed elevation of the ST segment in the V1-V4 leads confirming the diagnosis of acute anterior myocardial infarction (Figure 1). In physical examination, bilateral crackles in the basal portions of the lungs with mild pretibial edema were determined. Laboratory investigations revealed a normal complete blood count with increased troponin I (200 ng/L) and creatinine (130 micromoles/L) levels. Soon after admission into the Intensive Coronary Care Unit, the patient became tahydyspnoic with the development of acute respiratory insufficiency.
We decided to perform endotracheal intubation and invasive mechanical ventilation was started. Emergent coronary angiography showed acute occlusion of the proximal left anterior descending artery (Figure 2A). After multiple balloon dilatations with semi-compliant balloons (2.0x20 mm and 3.0x30 mm), a one 3.5x38 mm drug-eluting stent (DES) was successfully deployed with the optimal angiographic result and TIMI 3 flow (Figure 2B).
After the procedure, the patient was hypotensive and intravenous dobutamine was started at an infusion rate of 5 mcg/kg/min with intravenous noradrenaline at an infusion rate of 6.6 mcg/min. Echocardiography showed severely reduced left ventricular ejection fraction (LVEF) with an estimated LVEF of 30 % with the Simpson Biplane method with signs of initial apical aneurysmal formation. Due to refractory oliguria, we started with renal replacement therapy (RRT) through the dialysis catheter placed in the right internal jugular vein. On day 7, the patient was successfully extubated, and previously applied inotropic and vasoactive therapy was deescalated.
On day 8 of hospitalization, he developed a refractory electrical storm for which he received more than 50 DC shocks. An example of one of numerous VT runs, as captured by ICCU telemetry, is shown below in Figure 3.
A comprehensive anti-arrhythmic therapy including metoprolol 5 mg intravenous every 5 minutes up to 3 doses, an amiodarone bolus dose of 150 mg over 10 minutes followed by continuous infusion of 1200 mg in 24 hours, and lidocaine bolus dose of 1mg/kg, repeat bolus dose of 0.5mg/kg followed by continuous infusion of 20 mcg/kg/min during 24 hours was initiated (Table 1). A bolus infusion of 2 g intravenous magnesium-sulfate was also applied. We introduced sedation with a propofol bolus dose of 50 mg intravenous followed by continuous infusion of 100 mcg/kg/min and decided to start again with the mechanical ventilation in order to suppress increased catecholaminergic drive.
Despite these therapeutic efforts, the patient still had episodes of polymorphic ventricular tachycardia. In order to suppress refractory ventricular arrhythmia, it was decided to perform temporary VOP. This was accomplished by using a temporary pacemaker, programmed at 90 bpm, with an active fixation lead placed in the right ventricle, by the right transfemoral approach. After the placement of the temporary pacemaker, acute hemodynamic and electrical stability was achieved.
In order to exclude possible acute stent thrombosis we repeated invasive coronary angiography which revealed no signs of stent thrombosis with normal flow through the previously implanted DES. The electrolytes were within normal range and there were no metabolic disturbances observed in the laboratory workup. The measured QTc interval was within the reference range. After initial stabilization, metoprolol was replaced by propranolol peroral in a dose of 40 mg twice a day. After five days of VOP, we decided to implant the subcutaneous temporary pacing via the right subclavian vein, programmed at 85 bpm.Finally, following electrical stabilization, seven days after implantation of subcutaneous temporary pacing, the patient underwent an ICD implantation (Figure 2C) with the pacing rate programmed at 60 bpm, and two zones of tachycardia detection and corresponding therapies (VT zone: at 170 bpm; VF zone: at >210 bpm).
On the 25-day of hospitalization, he developed acute respiratory insufficiency which required non-invasive mechanical ventilation (NIV). Chest X-ray showed diffuse bilateral consolidations and his nasal swab for Sars-CoV-2 infection was found to be positive. First day of illness the remdesivir in a dose of 200 mg intravenous and the next two days in a dose of 100 mg intravenous was applied. After five days he was successfully weaned from the NIV with no signs of respiratory insufficiency. After 40 days of hospitalization, he was discharged from the hospital with optimal medical therapy including aspirin (100 mg per day), ticagrelor (90 mg twice per day), amiodarone (200 mg twice per day), metoprolol (50 mg twice per day), eplerenone (25 mg once a day), empagliflozin (10 mg once a day) and furosemide (20 mg twice a day).
3. Discussion
The incidence of sustained ventricular arrhythmias (VA) in acute coronary syndromes (ACS) is 5-10%. In the context of ischemia, VPC, VT, and VF can be secondary to an automatic or reentrant mechanism [2,3]. Studies have shown that in only 10-25% of patients with the electrical storm, clear precipitating causes were identified [4]. Electrolyte imbalance, acute ischemia, exacerbation of heart failure, adjustment of or non-compliance to anti-arrhythmic medications, and recent introduction to biventricular pacing have been identified as potential triggers [5]. According to the most recent European Society of Cardiology guidelines for the management of ventricular arrhythmias and sudden cardiac death, overdrive pacing with a slightly higher rate than the baseline rhythm can be useful to temporarily suppress slow recurrent/incessant VTs [6].
To our knowledge, temporary use of VOP has been previously described by Magdi et. al in a patient that underwent PCI and had a large anterolateral AMI for the purpose of control of the resistant arrhythmia [7]. Temporary (atrial) overdrive pacing may help to interrupt an incessant or re-occurring VA, especially in conditions such as Brugada syndrome and early repolarisation syndrome by preventing PVCs from occurring and reducing early after depolarisation [8,9]. Antiarrhythmic medications are the cornerstone of electrical storm management and their administration is required as a part of initial resuscitative measures as we summarize in Table 2 [10,11].
Current guidelines also recommend deep sedation as a therapeutic option in electrical storm refractory to antiarrhythmic drugs to reduce sympathetic overactivity involved in ES initiation and maintenance [12]. Due to the implicated role of sympathetic nervous system hyperactivity in a refractory ventricular storm, a stellate ganglion blockade might be an efficacious invasive and non-pharmacological treatment option for the management of electrical storm as it significantly reduces ventricular arrhythmia burden and a number of external and ICD shocks. Furthermore, this treatment modality has been supported by the ESC guidelines class of recommendation IIb, level of evidence C [13].
In some cases, electrical storm patients might experience episodes of monomorphic VT based on re-entry. Therefore catheter ablation, targeting the substrate in which re-entry has formed, is an important treatment option for the electrical storm in this subset of patients [14]. Catheter ablation should also be considered in patients with recurrent symptomatic episodes of PVT or VF triggered by a similar PVC. Ablation of the focal Purkinje-related triggers frequently arising from the scar border zone at the left ventricular septum appears to be associated with short and long-term freedom from recurrent VF storm [15].
Compared to medical therapy, catheter ablation reduces the number of subsequent VT episodes especially when VT ablation is performed within one month of an electrical storm [16]. Stereotactic arrhythmia radioablation (STAR) as a noninvasive, effective, and well-tolerated treatment, may be a suitable alternative method for patients with cardiac arrhythmia who are resistant or intolerant to catheter ablation [17]. Eventually, if all these therapeutic measures failed in the acute termination of ES, mechanical circulatory support, urgent catheter ablation, or neuraxial modulation are potential options in these situations to achieve hemodynamic and electrical stabilization [18,19,20].
5. Conclusions
A temporary ventricular overdrive pacing can serve as a feasible and effective therapeutic modality in patients presented with electrical storm following acute myocardial infarction refractory to multiple anti-arrhythmic drugs. In these circumstances, ventricular overdrive pacing can play a key role in acute hemodynamic and electrical stabilization and serve as a bridge to successful ICD implantation.
Author Contributions
Conceptualization: M.M. and J.A.B.; Data curation: M.M. and J.A.B.; Writing-original draft preparation: M.M. and J.A.B.; Writing-reviewing and editing: M.M. and J.A.B.; Visualization: M.M. and J.A.B.; Supervision: J.A.B.; Funding acquisition: J.A.B.; Project administration: J.A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
The patient gave consent for the use of images and de-identified information for public scientific dissemination.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hohnloser SH, Al-Khalidi HR, Pratt CM, Brum JM, Tatla DS, Tchou P, Dorian P; SHock Inhibition Evaluation with AzimiLiDe (SHIELD) Investigators. Electrical storm in patients with an implantable defibrillator: incidence, features, and preventive therapy: insights from a randomized trial. Eur Heart J. 2006 Dec;27(24):3027-32. [CrossRef]
- Piccini JP, Berger JS, Brown DL. Early sustained ventricular arrhythmias complicating acute myocardial infarction. Am J Med. 2008 Sep;121(9):797-804. [CrossRef]
- Gorenek B, Blomström Lundqvist C, Brugada Terradellas J, Camm AJ, Hindricks G, Huber K, Kirchhof P, Kuck KH, Kudaiberdieva G, Lin T, Raviele A, Santini M, Tilz RR, Valgimigli M, Vos MA, Vrints C, Zeymer U, Lip GY, Potpara T, Fauchier L, Sticherling C, Roffi M, Widimsky P, Mehilli J, Lettino M, Schiele F, Sinnaeve P, Boriani G, Lane D, Savelieva I. Cardiac arrhythmias in acute coronary syndromes: position paper from the joint EHRA, ACCA, and EAPCI task force. Europace. 2014 Nov;16(11):1655-73. [CrossRef]
- Pedersen CT, Kay GN, Kalman J, Borggrefe M, Della-Bella P, Dickfeld T, Dorian P, Huikuri H, Kim YH, Knight B, Marchlinski F, Ross D, Sacher F, Sapp J, Shivkumar K, Soejima K, Tada H, Alexander ME, Triedman JK, Yamada T, Kirchhof P, Lip GY, Kuck KH, Mont L, Haines D, Indik J, Dimarco J, Exner D, Iesaka Y, Savelieva I. EHRA/HRS/APHRS expert consensus on ventricular arrhythmias. Europace. 2014 Sep;16(9):1257-83. [CrossRef]
- Greene M, Newman D, Geist M, Paquette M, Heng D, Dorian P. Is electrical storm in ICD patients the sign of a dying heart? Outcome of patients with clusters of ventricular tachyarrhythmias. Europace. 2000 Jul;2(3):263-9. [CrossRef]
- Zeppenfeld K, Tfelt-Hansen J, de Riva M, Winkel BG, Behr ER, Blom NA, Charron P, Corrado D, Dagres N, de Chillou C, Eckardt L, Friede T, Haugaa KH, Hocini M, Lambiase PD, Marijon E, Merino JL, Peichl P, Priori SG, Reichlin T, Schulz-Menger J, Sticherling C, Tzeis S, Verstrael A, Volterrani M; ESC Scientific Document Group. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. 2022 Oct 21;43(40):3997-4126. [CrossRef]
- Magdi M, Mubasher M, Alzaeem H, Hamid T. Resistant Ventricular Arrhythmia and the Role of Overdrive Pacing in the Suppression of the Electrical Storm. Case Rep Cardiol. 2019 May 22;2019:6592927. [CrossRef]
- European Heart Rhythm Association; Heart Rhythm Society; Zipes DP, Camm AJ, Borggrefe M, Buxton AE, Chaitman B, Fromer M, Gregoratos G, Klein G, Moss AJ, Myerburg RJ, Priori SG, Quinones MA, Roden DM, Silka MJ, Tracy C, Smith SC Jr, Jacobs AK, Adams CD, Antman EM, Anderson JL, Hunt SA, Halperin JL, Nishimura R, Ornato JP, Page RL, Riegel B, Priori SG, Blanc JJ, Budaj A, Camm AJ, Dean V, Deckers JW, Despres C, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J, Osterspey A, Tamargo JL, Zamorano JL; American College of Cardiology; American Heart Association Task Force; European Society of Cardiology Committee for Practice Guidelines. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death). J Am Coll Cardiol. 2006 Sep 5;48(5):e247-346. [CrossRef]
- Priori SG, Wilde AA, Horie M, Cho Y, Behr ER, Berul C, Blom N, Brugada J, Chiang CE, Huikuri H, Kannankeril P, Krahn A, Leenhardt A, Moss A, Schwartz PJ, Shimizu W, Tomaselli G, Tracy C; Document Reviewers; Ackerman M, Belhassen B, Estes NA 3rd, Fatkin D, Kalman J, Kaufman E, Kirchhof P, Schulze-Bahr E, Wolpert C, Vohra J, Refaat M, Etheridge SP, Campbell RM, Martin ET, Quek SC; Heart Rhythm Society; European Heart Rhythm Association; Asia Pacific Heart Rhythm Society. Executive summary: HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes. Europace. 2013 Oct;15(10):1389-406. [CrossRef]
- Al-Khatib SM, Stevenson WG, Ackerman MJ, Bryant WJ, Callans DJ, Curtis AB, Deal BJ, Dickfeld T, Field ME, Fonarow GC, Gillis AM, Granger CB, Hammill SC, Hlatky MA, Joglar JA, Kay GN, Matlock DD, Myerburg RJ, Page RL. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2018 Sep 25;138(13):e210-e271. [CrossRef]
- Kowlgi GN, Cha YM. Management of ventricular electrical storm: a contemporary appraisal. Europace. 2020 Dec 23;22(12):1768-1780. [CrossRef]
- Al-Khatib SM, Stevenson WG, Ackerman MJ, Bryant WJ, Callans DJ, Curtis AB, Deal BJ, Dickfeld T, Field ME, Fonarow GC, Gillis AM, Granger CB, Hammill SC, Hlatky MA, Joglar JA, Kay GN, Matlock DD, Myerburg RJ, Page RL. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: Executive summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm. 2018 Oct;15(10):e190-e252. [CrossRef]
- Meng L, Tseng CH, Shivkumar K, Ajijola O. Efficacy of Stellate Ganglion Blockade in Managing Electrical Storm: A Systematic Review. JACC Clin Electrophysiol. 2017 Sep;3(9):942-949. [CrossRef]
- Nayyar S, Ganesan AN, Brooks AG, Sullivan T, Roberts-Thomson KC, Sanders P. Venturing into ventricular arrhythmia storm: a systematic review and meta-analysis. Eur Heart J. 2013 Feb;34(8):560-71. [CrossRef]
- Komatsu Y, Hocini M, Nogami A, Maury P, Peichl P, Iwasaki Y, et al. Catheter ablation of refractory ventricular fibrillation storm after myocardial infarction: a multicenter study. Circulation 2019;139:2315–2325. [CrossRef]
- Dinov B, Arya A, Bertagnolli L, Schirripa V, Schoene K, Sommer P, Bollmann A, Rolf S, Hindricks G. Early referral for ablation of scar-related ventricular tachycardia is associated with improved acute and long-term outcomes: results from the Heart Center of Leipzig ventricular tachycardia registry. Circ Arrhythm Electrophysiol. 2014 Dec;7(6):1144-51. [CrossRef]
- Wang S, Luo H, Mao T, Xiang C, Hu H, Zhao J, Wang X, Wang J, Liu H, Yu L, Jiang H. Stereotactic arrhythmia radioablation: A novel therapy for cardiac arrhythmia. Heart Rhythm. 2023 Sep;20(9):1327-1336. [CrossRef]
- Le Pennec-Prigent S, Flecher E, Auffret V, Leurent G, Daubert JC, Leclercq C, Mabo P, Verhoye JP, Martins RP. Effectiveness of Extracorporeal Life Support for Patients With Cardiogenic Shock Due To Intractable Arrhythmic Storm. Crit Care Med. 2017 Mar;45(3):e281-e289. [CrossRef]
- Vergara P, Tung R, Vaseghi M, Brombin C, Frankel DS, Di Biase L, Nagashima K, Tedrow U, Tzou WS, Sauer WH, Mathuria N, Nakahara S, Vakil K, Tholakanahalli V, Bunch TJ, Weiss JP, Dickfeld T, Vunnam R, Lakireddy D, Burkhardt JD, Correra A, Santangeli P, Callans D, Natale A, Marchlinski F, Stevenson WG, Shivkumar K, Della Bella P. Successful ventricular tachycardia ablation in patients with electrical storm reduces recurrences and improves survival. Heart Rhythm. 2018 Jan;15(1):48-55. [CrossRef]
- Do DH, Bradfield J, Ajijola OA, Vaseghi M, Le J, Rahman S, Mahajan A, Nogami A, Boyle NG, Shivkumar K. Thoracic Epidural Anesthesia Can Be Effective for the Short-Term Management of Ventricular Tachycardia Storm. J Am Heart Assoc. 2017 Oct 27;6(11):e007080. [CrossRef]
Figure 1.
Electrocardiogram (ECG) during admission at the Emergency Department revealed elevation of the ST segment in the V1-V6 leads consistent with acute anterior myocardial infarction.
Figure 1.
Electrocardiogram (ECG) during admission at the Emergency Department revealed elevation of the ST segment in the V1-V6 leads consistent with acute anterior myocardial infarction.
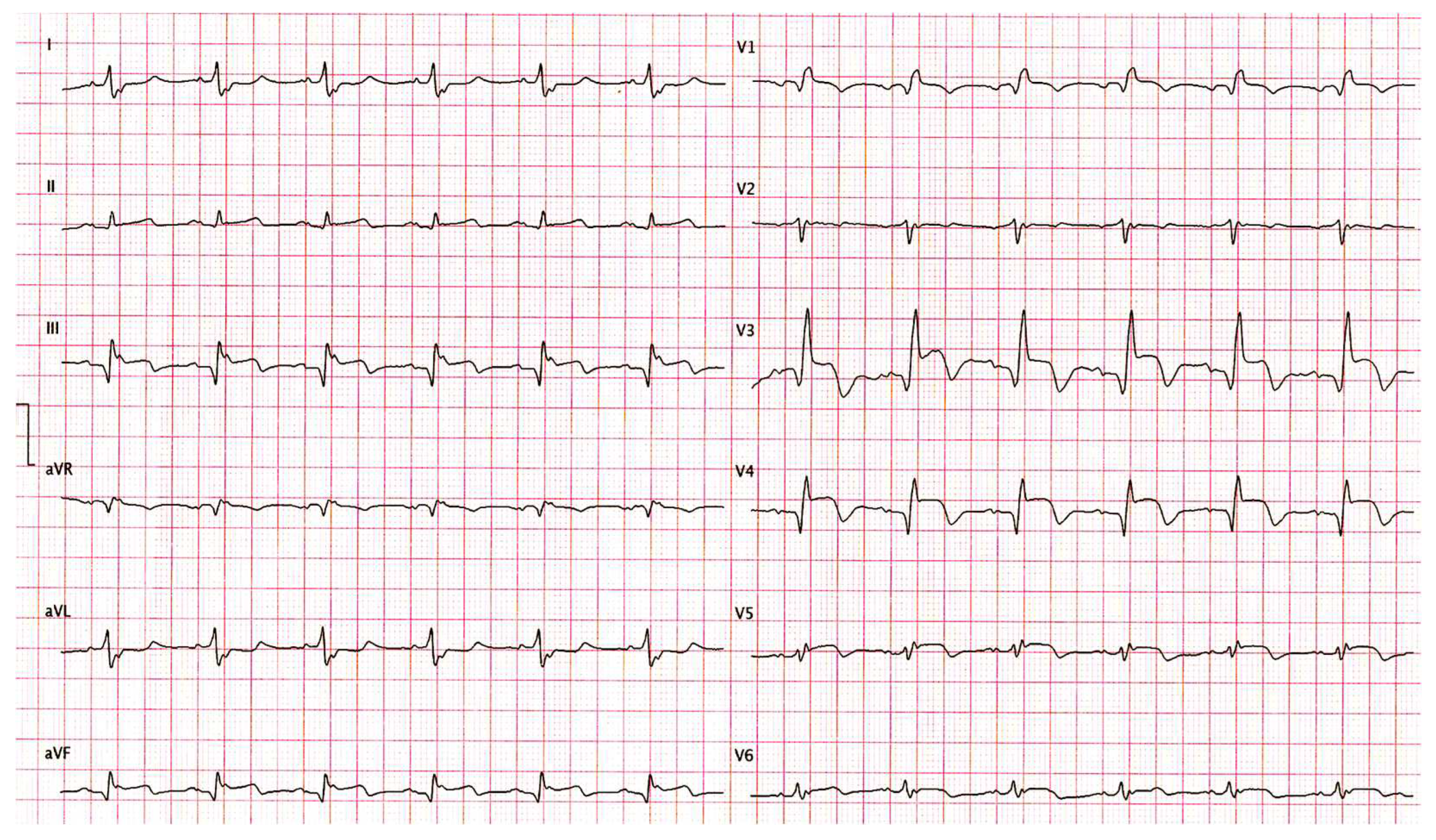
Figure 2.
A) Coronary angiography showing acute occlusion of the proximal left anterior descending artery (LAD); B) Coronary angiography showing established TIMI 3 flow through previously occluded LAD, following percutaneous coronary intervention and drug-eluting stent implantation; C) Antero-posterior chest X-ray showing the implanted ICD.
Figure 2.
A) Coronary angiography showing acute occlusion of the proximal left anterior descending artery (LAD); B) Coronary angiography showing established TIMI 3 flow through previously occluded LAD, following percutaneous coronary intervention and drug-eluting stent implantation; C) Antero-posterior chest X-ray showing the implanted ICD.
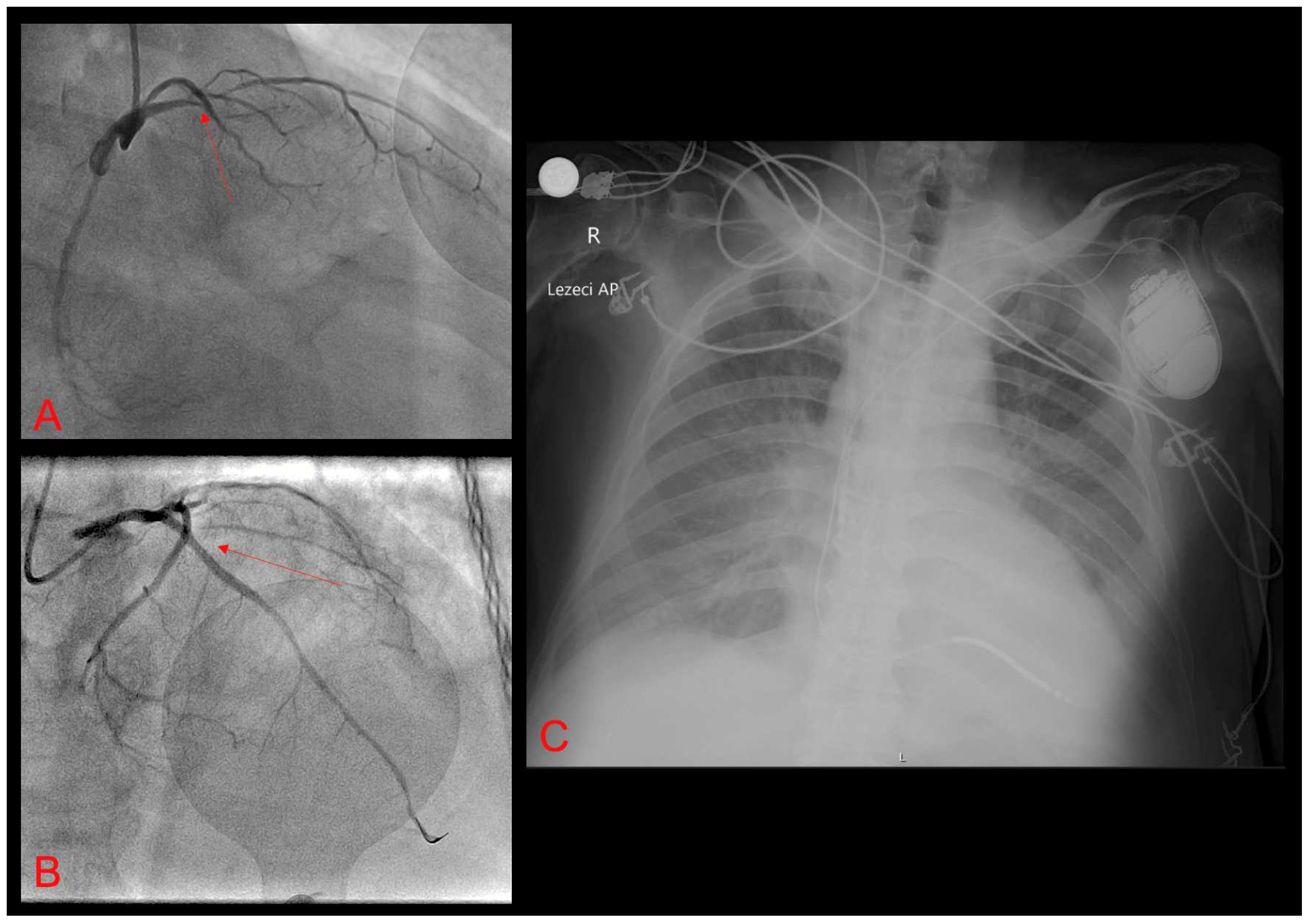
Figure 3.
Electrocardiogram (ECG) from the telemetry system in the Coronary Care Unit (CCU) showing one of the many episodes of refractory electrical storm (polymorphic VT/VF) despite optimal antiarrhythmic therapy.
Figure 3.
Electrocardiogram (ECG) from the telemetry system in the Coronary Care Unit (CCU) showing one of the many episodes of refractory electrical storm (polymorphic VT/VF) despite optimal antiarrhythmic therapy.
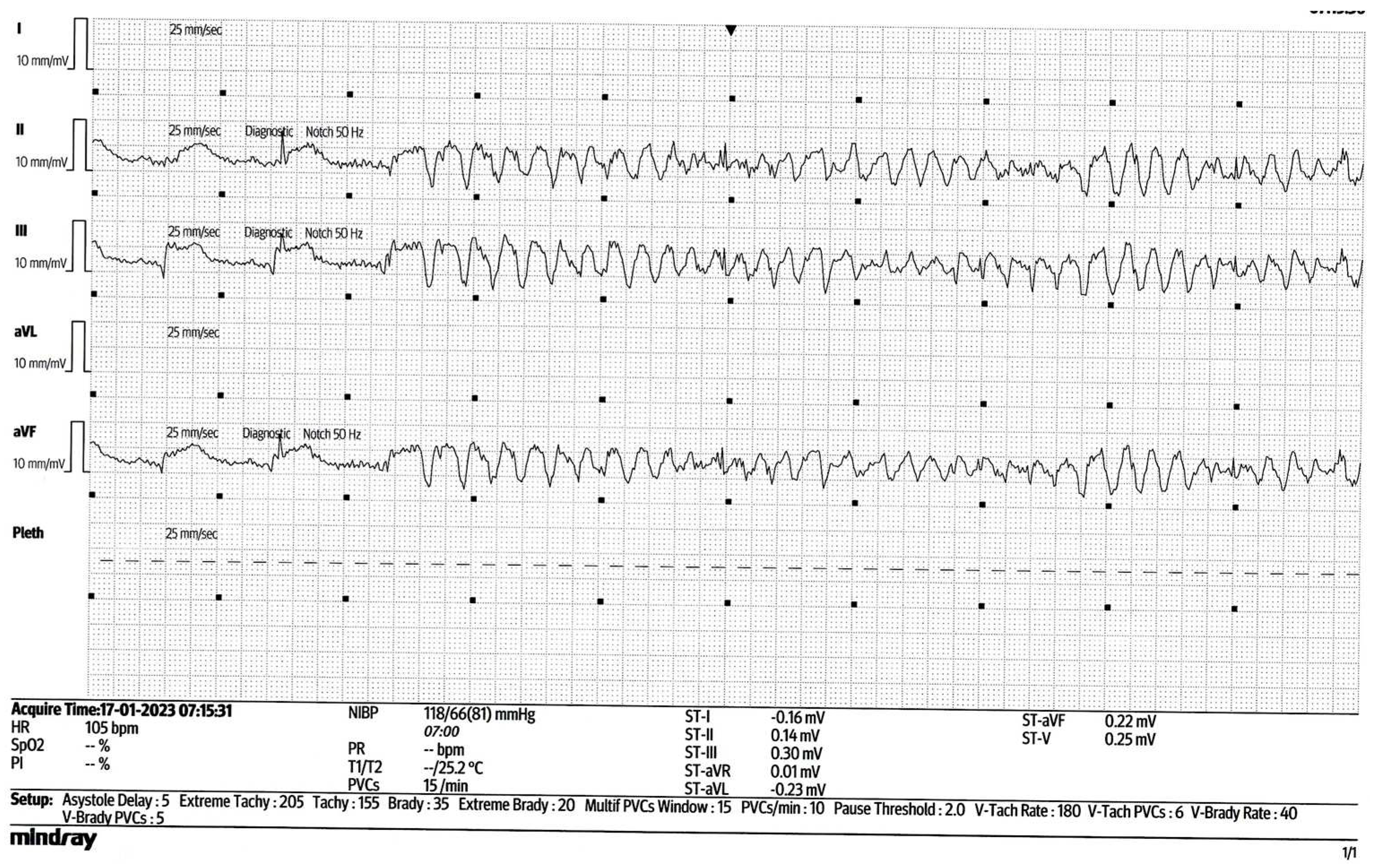

Table 1.
Drugs with dose and type of administration that are indicated and were used for the management of our patient with the intention to terminate the electrical storm.
Table 1.
Drugs with dose and type of administration that are indicated and were used for the management of our patient with the intention to terminate the electrical storm.
| Drug | Dose | Administration |
|---|---|---|
| Amiodarone | 150 mg bolus + 1200 mg continuous infusion during 24 hours | intravenous |
| Lidocaine | Bolus dose of 1mg/kg, with repeat bolus dose of 0.5mg/kg, followed by the continuous infusion of 20 mcg/kg/min. during 24 hours | intravenous |
| Metoprolol | 5 mg intravenous every 5 minutes; up to 3 doses | intravenous |
| Magnesium-sulphate | 2 g bolus dose | intravenous |
| Propofol | 50 mg bolus dose + continuous infusion of 100 mcg/kg/min. | intravenous |
| Propranolol | 40 mg twice a day after acute stabilization | oral |
Table 2.
Summary of the antiarrhythmic drugs that have an indicated use for the electrical storm –reproduced and modified based on the work of Kowlgi et al. [11].
Table 2.
Summary of the antiarrhythmic drugs that have an indicated use for the electrical storm –reproduced and modified based on the work of Kowlgi et al. [11].
| Drug | Dose |
|---|---|
| Amiodarone | IV: bolus 150 mg for stable VT; maintenance: 1 mg/min × 6 h, then 0.5 mg/min × 18 h; PO: 400 mg × q 8–12 h for 7–14 days, then 200–400 mg daily |
| Lidocaine | IV: bolus 1–1.5 mg/kg, can repeat up to total of 3 mg/kg, maintenance: 1–4 mg/min |
| Propranolol | IV: 1–3 mg q5 min to a maximum of 5 mg; PO: 10–40 mg q6 h immediate release; 60–160 mg q12 h extended release |
| Mexiletin | 150–300 mg PO q8–12 h |
| Procainamide | IV: bolus 10 mg/kg over 20 min, maintenance 2–3 g/24 h; oral: 500–1250 mg q6 h |
| Quinidine | Quinidine sulfate: 200–600 mg PO q6–12 h; quinidine gluconate 324–648 mg PO q8 h; IV loading dose 800 mg/50 mL, maintenance 50 mg/min |
| Sotalol | IV: 7 5 mg q12 h; PO: 80–160 mg q12 h |
| Metoprolol | IV: 5 mg q5 min up to 3 doses; PO: metoprolol tartarate 25–100 mg q12 h |
| Esmolol | IV: bolus: 0.5 mg/kg, maintenance: 0.05 mg/kg/min |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



