
Submitted:
15 December 2023
Posted:
19 December 2023
You are already at the latest version
Abstract
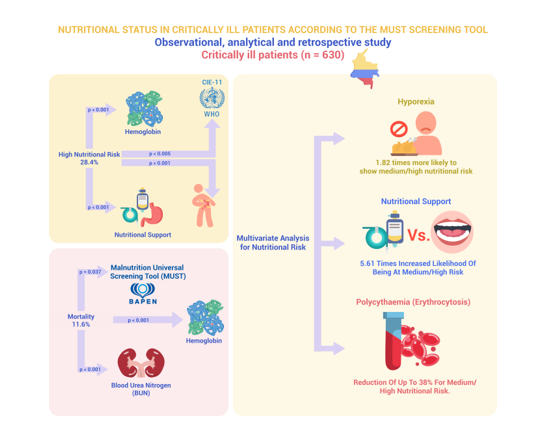
Purpose: To identify factors linked with nutritional risk via the Malnutrition Universal Screening Tool scale assessment among critically ill patients from a hospital in Cali (Colombia). Materials and methods: A retrospective, analytical observational study was conducted with patients admitted to an intensive care unit (ICU). Sociodemographic, clinical, hematological, and biochemical parameters were analyzed, as well as their association with nutritional risk and patient mortality. Binary logistic regression was applied to outline nutritional risk. Results: Overall, 28.4% prevalence of elevated nutritional risk was observed. An association was found between nutritional risk and hemoglobin and hematocrit values, primary diseases accounting for ICU admission, gastrointestinal symptoms, and nutritional support route (p < 0.05). Mortality was 11.6% and it was correlated with nutritional risk, hemoglobin, and blood urea nitrogen. Conclusions: Gastrointestinal symptoms and the type of nutritional support received during hospitalization may increase nutritional risk, whereas polycythemia was a protective factor. We found an associative model to determine nutritional risk with high specificity and an adequate diagnostic validity index.
Keywords:
Nutritional Status
; Nutritional Assessment
; Critical Patients
; Nutritional Risk
; Mortality
1. Introduction
Malnutrition, characterized by deficiencies in energy, proteins, and essential nutrients [1], profoundly affects bodily functions [2]. This concern is widespread in hospital settings globally, spanning continents such as Europe [3], Australia [4,5], Asia [6], North America [7], and Latin America [8].
Additionally, it remains an underdiagnosed condition [9] leading to inadequate treatment, often associated with healthcare professionals’ insufficient knowledge and inadequate clinical approaches and practices [10]. Clinical behaviors contributing to this issue encompass food intake interruption for diagnostic or therapeutic purposes, time constraints impeding nutrition-focused care, and absence of intervention in cases of inadequate patient food intake [11,12].
Malnutrition remarkably compromises clinical outcomes [1], impacting tissue metabolism, muscular strength, wound healing, and immune function [2]. It is associated with a higher risk of adverse events, encompassing both infectious and noninfectious complications, prolonged need for mechanical ventilation, and longer rehabilitation process [13,14,15]. Consequently, this results in extended hospital stay and heightened mortality risk [16], thereby increasing healthcare expenses, compromising patients’ quality of life, and imposing additional financial burdens on healthcare institutions [6,17].
Thus, routine nutritional assessments and monitoring play a crucial role in patient care by enabling the identification of deficiencies via screening, evaluating, and diagnosing the nutritional status [8]. This practice aids in predicting positive or negative health outcomes [18].
The prevalence of malnutrition among hospitalized adults of all ages varies widely, ranging from 20% to 69%, exacerbating during hospitalization, notably in acute inflammatory conditions [11,12]. In intensive care units (ICUs), malnutrition is prevalent, ranging from 33% to 78% [14,19,20,21,22]. However, conducting nutritional evaluations in ICUs poses challenges due to limited clinical records on nutritional parameters amidst critical patient conditions necessitating resuscitative measures and substantial fluid administration [23]. Therefore, assessing isolated weight changes may lack nutritional significance owing to confounding factors related to patients’ hydration status [9].
Currently, multiple nutritional assessment scales are available; however, none hold the status of being the definitive “gold standard” for critically ill patients [23]. Consequently, each institution opts for the one that best aligns with the characteristics of its patient population [24]. Among these methodologies, the Malnutrition Universal Screening Tool (MUST) emerges as a straightforward assessment tool designed to identify malnourished patients requiring subsequent monitoring and nutritional intervention. A prevalence range of malnutrition risk has been reported using this scale, spanning between 19% and 60% in hospitalized patients and 30% in outpatients. Notably, the MUST scale exhibits a strong level of agreement with other assessment tools such as the MEREC Bulletin, Nutrition Risk Screening (NRS), and Subjective Global Assessment tools, demonstrating substantial concordance (Kappa = 0.775–0.893) [25].
Considering these factors, the primary objective of this study is to identify the factors associated with nutritional risk by employing the MUST scale in a cohort of critically ill patients from a hospital in Cali (Colombia).
2. Materials and Methods
2.1. Design, Population, and Sample
An observational, analytical, and retrospective study was conducted with adult patients hospitalized in the ICU of a level IV clinic located in the city of Cali (Colombia). The study spanned from January 1, 2021, to April 30, 2022.
The population encompassed a total of 3988 admitted patients during this period, 2142 of which were considered potential candidates for inclusion in the study (Figure 1).
For sample size estimation, considering the risk of malnutrition ranging from 40% to 60% in hospitalized Latin American patients [26], and aiming for a 95% confidence level with an estimation precision of 4%, a minimum sample size of 454 patients was calculated. Ultimately, a study sample of 630 individuals was randomly chosen and formed the study sample.
2.2. Eligibility Criteria
The study included adult patients admitted to the ICU during the investigation period, who underwent nutritional risk assessment using the MUST scale.
Patients diagnosed with COVID-19 were excluded due to the distinct impact on nutritional status attributed to gastrointestinal and immune system disruptions, escalated metabolic activity due to the infectious process, presence of fever, and reduced oral food intake [27]. Furthermore, individuals lacking medical diagnosis data upon admission to the ICU or those with duplicate records generated within the hospital’s system due to patient transfers within the institution’s services, be it for diagnostic or surgical procedures, were excluded (Figure 1).
2.3. Variables and Measurement
2.3.1. Explanatory Variables
Sociodemographic variables—such as sex, age, and admission disease according to ICD-11—hematological variables and biochemical variables were taken into account (Table 1).
Furthermore, the presence of gastrointestinal symptoms (hyporexia, abdominal distension, diarrhea, swallowing difficulties, emesis, and abdominal pain) and the type of nutritional support received (oral, enteral, and parenteral) were included.
2.3.2. Outcome Variable
As outcome variable, nutritional risk assessed using the MUST scale—categorized into low, medium, or high risk—and vital status at discharge (alive or deceased) were considered.
2.4. Measurement Instruments
The MUST scale was employed to assess the risk of malnutrition. This tool demonstrates a sensitivity of 80.2% and exhibits a high discriminative capability (area under the ROC curve of 0.868) in determining nutritional risk. This evaluation was compared against a comprehensive nutritional assessment that includes participants’ medical history, dietary-nutritional history, pharmacological treatment, physical examination, anthropometric measurements and laboratory data [28].
The MUST scale takes into account the analysis of three scores: a) body mass index (BMI) calculated as kg/m2, which is scored ≥20 kg/m2 = 0; 18.5–20 kg/m2 = 1; and ≤18.5 kg/m2 = 2; b) unintentional weight loss (WL) during the last 3–6 months, calculated as a percentage and coded as follows: WL ≤5% = 0; WL 5%–10% = 1; and WL ≥10% = 2; c) the effect of acute diseases, in which 2 points are assigned when there has been or is likely to be no nutritional intake for >5 days.
2.5. Ethical Considerations
This research adhered to the ethical guidelines of Council for International Organizations of Medical Sciences and the Declaration of Helsinki regarding the participation of human beings, including the signing of an informed consent prior to the collection of information, either by the patient or the responsible family member. The Research Ethics Committee of the Faculty of Health of the Universidad Santiago de Cali, Colombia, and the Scientific Technical Committee of the participating Clinic (Record IYECDO – 1358) approved the study.
2.6. Statistical Analysis
Statistical analyses were conducted using SPSS software version 28.0. Quantitative variables were represented using arithmetic mean and standard deviation values. The Kolmogorov–Smirnov test with Lilliefors correction was used to analyze the goodness of fit of the data at a normal distribution. Mean variation was calculated through the application of ANOVA for one factor, considering a value of p <0.05 as significant. For the comparison of nominal variables, Pearson’s Chi-square test was used with Fisher’s exact test when required.
Moreover, binary logistic regression was performed to analyze nutritional risk, categorized into low and medium/high. An initial crude analysis was performed to identify the associated variables and subsequently the adjusted estimation was performed, estimating OR values for the determination of risk and evaluating the goodness of fit of the model through the determination of Cox and Snell’s R2, Nagelkerke’s R2, and Hosmer and Lemeshow’s test. Finally, the validity index, the correct percentage of patient classification, the area under the curve (ROC) and the diagnostic accuracy of the variables proposed in the model for the determination of nutritional risk were determined, and comparisons were made with the results of the MUST scale as gold standard. This was done by calculating the sensitivity, specificity, and the positive and negative predictive value (PPV and NPV) of the model, as well as the Youden index.
3. Results
3.1. Characterization of the Study Participants
The study comprised a total of 630 patients, with 341 being male (54.1%). The overall mean age of the sample was 64.75 (SD =16.21) with a 95% CI (63.49–66.02).
A high prevalence of circulatory and respiratory diseases (50%) was observed as a cause of admission to the ICU, with significantly higher occurrence among male patients (61%).
Male patients exhibited a higher average weight, recorded at 70.08 kg (± 13.68). The MUST scale identified a nutritional risk of 28.4%, identifying a higher proportion of male patients categorized under low nutritional risk. Finally, the mortality rate among the study sample was 11.6% (Table 2).
3.2. Hematological and Biochemical Parameters Associated with Nutritional Risk
Regarding the laboratory tests conducted on the participants, an association between nutritional risk and hematological parameters (such as hemoglobin and hematocrit values) was identified, observing a lower average value (10.84 g/dL, 33.49% respectively) in patients with high nutritional risk. In the analysis of the white series, an average leukocyte counts in patients of 10.68 × 103/uL (SD= 17.22) 95% CI (9.33–12.03) was observed and, as in the biochemical tests such as renal function and electrolyte levels in blood plasma, no significant associations were identified according to nutritional risk (Table 3).
3.3. Morbidity, Gastrointestinal Symptoms, and Route of Nutritional Support Associated with Nutritional Risk
Table 4 shows other factors related to nutritional risk, including the diseases causing admission to the ICU, the presence of gastrointestinal symptoms and the route of nutritional support received. The percentage of patients at low risk was higher, and diseases of the circulatory and respiratory system (67%) and those of the nervous system, musculoskeletal system and/or trauma (65.1%) stood out. The patients with the highest prevalence of high nutritional risk were those with infectious or parasitic diseases (42.4%). In the case of gastrointestinal symptoms, we found an association between high nutritional risk of malnutrition and the presence of hyporexia, bloating, or abdominal pain, diarrhea, and swallowing difficulties or emesis, obtaining prevalence values in patients between 36.1% and 47.8%. The route of nutritional support with the greatest effect on the increase in nutritional risk was the parenteral one, with 77.3% of patients at high risk.
3.4. Factors Related to Mortality in the ICU
Patients with low nutritional risk exhibited a greater survival rate (62.1%). For hematological and biochemical parameters, an evident correlation emerged between hemoglobin and blood urea nitrogen (BUN) levels and vital status at discharge, showing lower hemoglobin values, with a mean of 10.39 g/dL (SD= 20.06) in deceased patients. Elevated BUN levels were also found in these patients, with a mean of 35.45 mg/dL (SD= 25.33) (Table 5).
3.5. Multivariate Analysis for Nutritional Risk
Variables associated with the nutritional risk of patients hospitalized in the ICU were identified and included in the adjusted binary logistic regression model to determine low and medium/high risk. This adjusted model exhibited a validity index of 65.40%, a specificity of 81.98%, a PPV of 58.68% and a NPVof 67.82%. Notably, patients experiencing hyporexia were 1.82 times more likely to face medium/high nutritional risk. Additionally, the use of the parenteral route for nutritional support showed a 5.61-fold increased likelihood of encountering this risk category compared to patients with oral feeding. In contrast, patients with polycythemia demonstrated a safeguarding effect against medium/high nutritional risk (Table 6).
4. Discussion
Our study assessed the nutritional risk of 630 critically ill patients hospitalized in a health institution in Cali, Colombia, during 2021 and 2022 and its association with clinical variables (hematological and biochemical parameters, gastrointestinal symptoms, and type of nutritional support required in the ICU).
4.1. Diseases and Nutritional Risk by Sex
The average age varied between men and women across different studies. For instance, research on an ICU in Korea revealed a higher mean age among women at 67.8 years (SD = 15.8), compared to an average of 62.4 years (SD = 14.6) in male patients (31). A similar trend was observed in a study conducted in New South Wales, Australia, with a mean age of 63.7 years in females compared to 61.8 years in males (p < 0.001) [32].
Regarding reasons for ICU admission, circulatory and respiratory diseases prevailed, consistent with a study conducted in the United States with a predominance of patients with respiratory failure (42%). However, the second most frequent cause was related to nonrespiratory sepsis (17%) [33] unlike the results of our study, in which the second most frequent disease was neoplasms.
Sociodemographic characterization in health research involves analyzing the behavior of events and categorizing them based on these variables. For example, one study found lower rates of heart disease in the female population, with 8% compared to 16% in men [32]. These results coincide with our population in Cali, Colombia, with rates of circulatory and respiratory diseases being 20% lower in women.
Endocrine and digestive diseases were more prevalent in female patients (59.6%), results that differ from those found in Korean ICUs, where there was a higher prevalence of liver disease in men [31]. In terms of infectious diseases, there was no significant difference between the number of male and female patients. This finding was also identified in the analysis of data collected in Australia, with patients admitted for sepsis to the ICU [32].
When analyzing nutritional status by BMI, an Australian study evidenced significant differences in terms of a higher proportion of healthy BMI (>18.5 ≤25 kg/m2) in women (39.3%) than in men (29.0%) [32]. This was not observed in the results of our study and coincides with another research conducted in the USA [34]. Regarding patient mortality, the literature has reported 19.7% in the African population hospitalized in the ICU without a diagnosis of COVID-19 [35] and 19.1% in the population admitted to the medical and surgical ICU at Brigham and Women’s Hospital in Boston, Massachusetts [14]. These figures are lower than those reported in our results (11.6%).
4.2. Hemoglobin and Electrolyte Values Associated with Nutritional Risk
Hemoglobin levels serve as indicative biomarkers reflecting both nutritional status and the physiological stress associated to patients’ disease [36]. Consequently, constant monitoring of this parameter remains pivotal [37], especially in critically ill patients due to the high incidence of anemia [38], which is associated with adverse outcomes in those with congestive heart failure [39], acute myocardial infarction [40], chronic kidney disease [41], and chronic obstructive pulmonary disease [42]. This situation is associated with failures in the withdrawal of mechanical ventilation of critically ill patients [43], increased risk of mortality [44] and the respective increase in the use of health care resources [45].
The presence of anemia in critical ill patients is the result of a shorter circulatory life of red blood cells and the decrease in their new production fundamentally related to nutritional deficiencies [45]. In addition, an increase in the hemoglobin levels of patients has been demonstrated after a higher intake of calories and proteins during hospitalization [46]. In this regard, our findings suggest that the lowest average hemoglobin level was present in patients at high nutritional risk (according to MUST), probably related to WL and low nutritional intake.
Conversely, the lymphocyte count has been included as a marker of immune competence and an indicator of the nutritional status of patients [47]. This fact has been reflected in the results of the study performed with a population of cardiac surgery patients, who were classified according to the Geriatric Nutritional Risk Index. Our study found lower lymphocyte counts, decreased sodium levels and, in turn, higher serum potassium levels in the group of patients with higher nutritional risk [48]. However, our study did not establish statistically significant associations between the analyzed electrolytes and nutritional risk. These divergences between the studies could be attributed to variations in sample sizes and data collection from single institutions. Conducting a multicenter study would likely validate and enhance the reliability of these outcomes.
4.3. Morbidity, Gastrointestinal Symptoms, and Nutritional Support Route Associated with Nutritional Risk
In 2021, the British Association for Parenteral and Enteral Nutrition reported that 40% of hospitalized adult patients were at risk of malnutrition according to the MUST tool. Notably, the prevalence was notably high among patients with gastrointestinal diseases (55%), respiratory diseases (48%) and cancer (47%) [49]. These results coincide with our research, where the highest percentages of medium/high nutritional risk were found in patients with neoplastic (46.7%) and gastrointestinal (53.3%) diseases. In the case of cancer patients, malnutrition is increased by factors related to systemic inflammatory processes, metabolic disorders such as proteolysis and lipolysis and factors associated with the disease or side effects of treatment, which generate decreased nutritional intake, lack of appetite and abdominal distension [50]. These symptoms are also very frequent in patients with gastrointestinal diseases and are responsible for a greater deterioration of nutritional status among hospitalized patients [51].
Regarding the association between gastrointestinal symptoms and nutritional risk, prior studies in elderly patients residing in rural areas of Bangladesh noted an increase in malnutrition rates (57.9%) due to the influence of severe loss of appetite caused by masticatory, digestive or inflammatory problems [52]. These is consistent with the results of our study, in which it was found that the presence of hyporexia, bloating, abdominal pain, diarrhea, swallowing difficulties and emesis increased nutritional risk.
Since these gastrointestinal symptoms reduce nutritional intake, generate malabsorption of food, and affect nutritional status, they have recently been introduced in the Global Leadership Initiative on Malnutrition (GLIM) etiological criteria for the analysis of the nutritional status of patients [53]. These criteria establish a two-step approach to diagnose malnutrition in health care settings, proposing a first step with nutritional risk screening through a valid instrument and subsequent investigation of phenotypic criteria such as WL, BMI, reduced body mass, and etiological criteria such as reduced food intake, nutrient absorption, and presence of inflammation [54].
While parenteral nutrition is reserved for patients unable to receive nutrition orally or through enteral means, being a less frequent supplementary route [55], only 3.5% of the patients in our study received this type of nutritional support. It was also observed that the type of intervention was associated with the MUST risk identified, which may explain why 48.1% of the high-risk patients in our sample received enteral support. This intervention was also documented in the United Kingdom population, where the higher the nutritional risk, the greater the use of enteral support [49].
According to the guidelines of the European Society for Clinical Nutrition and Metabolism (ESPEN), this type of intervention should be performed early in critically ill patients without oral intake [56] with the aim of preventing further nutritional deterioration associated with the disease or treatment [49], thereby lowering mortality risks. As evidenced in the population of Cali, Colombia, patients with higher nutritional risk presented higher mortality at discharge. Therefore, and according to the complexity involved in defining the feeding route, a formal evaluation of risks and benefits with the patient and family seems necessary, where the perspectives of a multidisciplinary team allow the design of a nutritional care plan adapted to the identified needs [57].
4.4. Nutritional Risk and Hematological and Biochemical Parameters Associated with Mortality in the ICU
Patients with malnutrition exhibit an increased likelihood of experiencing adverse outcomes, including increased mortality risk during hospitalization and up to 6 months after discharge [19,53]. This was evident in the finding of the Modified Nutrition Risk In the Critically Ill score in patients admitted to the ICU of Gangman Severance Hospital in Seoul, South Korea. This work showed that the nutritional risk scores were significantly higher in the nonsurvivors group. In addition, they had elevated BUN levels, with an average of 34.6 mg/dL (SD = 24.3), compared to 19.3 mg/dL (SD = 19.1) in the survivors [47]. In this same study, statistically significant differences were also found in lymphocyte levels, with a value of 1322.2/μL (SD= 974.0) in survivors versus 1084.4/μL (SD = 1105.4) in nonsurvivors [47].
All these data is consistent with the findings of our study, affirming that those patients with lower nutritional risk had a higher percentage of survival, while deceased patients showed significantly higher values of BUN in blood plasma and a lower lymphocyte counts.
4.5. MUST Nutritional Risk Associative Model
A study conducted by Lima et al. (2022) in five hospitals in Brazil compared the use of the MUST scale, Malnutrition Screening Tool, Nutritional Risk in Emergency - 2017 (NRE-2017), NRS-2002, and Short Nutritional Assessment Questionnaire applied in the first 48 hours of hospital admission in adult patients, calculating their sensitivity, specificity, PPVs, NPVs, and clinical agreement to detect malnourished patients according to GLIM criteria. The authors obtained specificity values ranging from 85.3% to 96.6%, and sensitivity values were less than 80%; the highest percentage was obtained when performing the assessment through the MUST scale, with 73.6% [54].
When comparing these findings with our associative model, which includes the presence of hyporexia, the interpretation of hemoglobin values and the route of nutritional support used in the patient, we can also observe that sensitivity values (39.68%) are lower than specificity values (81.98%). This is an associative model that could be useful to identify hospitalized population with low nutritional risk.
These diagnostic accuracy measures and their low sensitivity values might be associated with the exclusion of data on BMI or involuntary WL in patients. This is because these were not considered as independent variables in the model since both are included in the outcome variable of the MUST scale, which would statistically imply collinearity between these variables. However, the five scales mentioned above and the GLIM criteria for the diagnosis of patients with malnutrition had implicit data related to BMI or WL, either in kg or in percentage and, in turn, the GLIM criteria include these variables within its phenotypic criteria [54]. Consequently, it seems evident that the inclusion of these variables increases the predictive capacity and complementarity between each scale and the criteria.
4.6. Study Limitations
One limitation of our study involved the impact of the COVID-19 pandemic, which posed challenges in sample collection due to the distinct pathophysiological features outlined in the selection criteria.
Moreover, the associative model of nutritional risk was established and assessed in a population with very specific sociodemographic and clinical characteristics, so it is necessary to validate the model in other populations to corroborate its diagnostic accuracy. In addition, it seems evident that there is a need to identify a variable that could increase the sensitivity of this model, which would improve its discriminant capacity and diagnostic validity in the identification of patients with medium/high nutritional risk.
5. Conclusions
Our study evidenced that the presence of a gastrointestinal symptom, such as hyporexia, has a direct effect on the increase of nutritional risk, as does the use of enteral or parenteral nutritional support as a substitute for oral intake. Conversely, polycythemia emerged as a protective factor, reducing the likelihood of medium/high nutritional risk by 38%.
Within this ICU patient sample, an associative model was found to determine nutritional risk based on the presence of hyporexia, the interpretation of hemoglobin levels and the route of nutritional support used. This model has obtained a high specificity and an adequate index of diagnostic validity for the classification of patients with nutritional risk.
Funding
This research did not receive any specific grants from funding agencies in the public, commercial, or nonprofit sectors.
Acknowledgments
This research has been funded by the General Research Directorate of Universidad Santiago de Cali under call No. 02-2023.
Conflicts of Interest
The authors declare that there is no conflict of interest.
References
- Robinson MK, Mogensen KM, Casey JD, McKane CK, Moromizato T, Rawn JD, Christopher KB. The relationship among obesity, nutritional status, and mortality in the critically ill. Critical Care Medicine. 1;43.1 (2015):87-100. [CrossRef]
- Ferrie S. What is nutritional assessment? A quick guide for critical care clinicians. Australian Critical Care. 33.3 (2020): 295-299. [CrossRef]
- Leij-Halfwerk S, Verwijs M.H, van Houdt S, Borkent J.W, Guaitoli P.R, Pelgrim T., ... & Manuel Consortium. Prevalence of protein-energy malnutrition risk in European older adults in community, residential and hospital settings, according to 22 malnutrition screening tools validated for use in adults≥ 65 years: a systematic review and meta-analysis. Maturitas, 126 (2019): 80-89. [CrossRef]
- Agarwal E, Ferguson M, Banks M, Batterham M, Bauer J, Capra S. & Isenring E. Malnutrition and poor food intake are associated with prolonged hospital stay, frequent readmissions, and greater in-hospital mortality: results from the Nutrition Care Day Survey 2010. Clinical nutrition, 32. 5 (2013): 737-745. [CrossRef]
- Barker L.A, Gout B.S., & Crowe T.C. Hospital malnutrition: prevalence, identification and impact on patients and the healthcare system. International journal of environmental research and public health, 8.2 (2011): 514-527. [CrossRef]
- Lam N.V, Sulo S, Nguyen H.A, Nguyen T.N, Brunton C, Duy N.N & Nguyen H.B. High prevalence and burden of adult malnutrition at a tertiary hospital: An opportunity to use nutrition-focused care to improve outcomes. Clinical Nutrition Open Science, 40 (2021): 79-88. [CrossRef]
- Allard J.P, Keller H, Jeejeebhoy K.N, Laporte M, Duerksenm D.R, Gramlich L, & Lou, W. Malnutrition at hospital admission—contributors and effect on length of stay: a prospective cohort study from the Canadian Malnutrition Task Force. Journal of Parenteral and Enteral Nutrition, 40.4 (2016): 487-497. DOI: . [CrossRef]
- Correia M.I.T, Perman M.I & Waitzberg D.L. Hospital malnutrition in Latin America: A systematic review. Clinical nutrition, 36.4 (2017): 958-967. [CrossRef]
- Correia, M.I.T.D. Nutrition screening vs nutrition assessment: what’s the difference?. Nutrition in Clinical Practice. 33.1 (2018): 62-72. [CrossRef]
- Guzman, M.A., & Calamba, P.G.S. Level Of Knowledge, Attitudes And Practices On Adult Patient’s Hospital Malnutrition Among Resident Physicians In A Tertiary Government Hospital. Clinical Nutrition ESPEN, 54 (2023) 525. Available online: https://clinicalnutritionespen.com/article/S2405-4577(22)00698-2/pdf (accessed on 8 september 2023).
- Kirkland LL, Shaughnessy E. Recognition and prevention of nosocomial malnutrition: a review and a call to action. Am J Med; 130.12 (2017):1345e50. [CrossRef]
- Marshall AP, Takefala T, Williams LT, Spencer A, Grealish L, Roberts S. Health practitioner practices and their influence on nutritional intake of hospitalised patients. Int J Nurs Sci. 6.2 (2019):162e8. [CrossRef]
- Weijs PJ, Looijaard WG, Dekker IM, Stapel SN, Girbes AR, Oudemans-van Straaten HM, et al. Low skeletal muscle area is a risk factor for mortality in mechanically ventilated critically ill patients. Crit Care. 18 (2014):R12. [CrossRef]
- Mogensen KM, Robinson MK, Casey JD, Gunasekera NS, Moromizato T, Rawn JD, Christopher KB. Nutritional Status and Mortality in the Critically Ill. Crit Care Med. 43.12 (2015):2605-15. [CrossRef]
- Jensen GL, Cederholm T, Correia ITD, Gonzalez MC, Fukushima R, Higashiguchi T. GLIM criteria for the diagnosis of malnutrition: a consensus report from the global clinical nutrition community. JPEN (J Parenter Enteral Nutr) 43.1 (2019): 32e40. [CrossRef]
- Inciong, J.F.B., Chaudhary, A., Hsu, H. S., Joshi, R., Seo, J. M., Trung, L. V., ... & Usman, N. Hospital malnutrition in northeast and southeast Asia: A systematic literature review. Clinical nutrition ESPEN, 39 (2020): 30-45. [CrossRef]
- Inciong JFB, Chaudhary A, Hsu HS, Joshi R, Seo JM, Trung LV, Ungpinitpong W, Usman N, Pradelli L, Omaralsaleh AJ. Economic burden of hospital malnutrition: A cost-of-illness model. Clin Nutr ESPEN. 48 (2022): 342-350. [CrossRef]
- Cederholm T, Bosaeus I, Barazzoni R, Bauer J, Van Gossum A, Klek S, Muscaritoli M, Nyulasi I, Ockenga J, Schneider SM, de van der Schueren MA, Singer P. Diagnostic criteria for malnutrition - An ESPEN Consensus Statement. Clin Nutr. 34.3 (2015):335-40. [CrossRef]
- Ceniccola G.D,.C. Relevance of AND-ASPEN criteria of malnutrition to predict hospital mortality in Holanda T.P, Pequeno R.S.F, Mendonça V.S, Oliveira A.B.M, Carvalho L.S.F., & Araujo W.M critically ill patients: A prospective study. Journal of critical care, 44 (2018): 398-403. [CrossRef]
- Fontes D, Generoso Sde V, Toulson Davisson Correia MI. Subjective global assessment: a reliable nutritional assessment tool to predict outcomes in critically ill patients. Clin Nutr. 33.2 (2014):291-5. [CrossRef]
- Atalay BG, Yagmur C, Nursal TZ, Atalay H, Noyan T. Use of subjective global assessment and clinical outcomes in critically ill geriatric patients receiving nutrition support. JPEN J Parenter Enteral Nutr. 32.4 (2008):454-9. [CrossRef]
- Lew CCH, Yandell R, Fraser RJL, Chua AP, Chong MFF, Miller M. Association Between Malnutrition and Clinical Outcomes in the Intensive Care Unit: A Systematic Review [Formula: see text]. JPEN J Parenter Enteral Nutr. 41.5 (2017):744-758. [CrossRef]
- Díaz G, T D Correia MI, Gonzalez MC, Reyes M. The global leadership initiative on malnutrition criteria for the diagnosis of malnutrition in patients admitted to the intensive care unit: A systematic review and meta-analysis. Clin Nutr. 42.2 (2023):182-189. [CrossRef]
- Theilla, M., Rattanachaiwong, S., Kagan, I., Rigler, M., Bendavid, I., & Singer, P. (2021). Validation of GLIM malnutrition criteria for diagnosis of malnutrition in ICU patients: An observational study. Clinical Nutrition. 40.5 (2021): 3578-3584. [CrossRef]
- Stratton RJ, Hackston A, Longmore D, Dixon R, Price S, Stroud M, et al. Malnutrition in hospital outpatients and inpatients: prevalence, concurrent validity and ease of use of the ‘malnutrition universal screening tool’ (‘MUST’) for adults. British Journal of Nutrition. Cambridge University Press; 92.5 (2004): 799–808. [CrossRef]
- Papapietro K, Méndez C, Matos AA, et al. Current clinical nutrition practices in critically ill patients in Latin America: a multinational observational study. Crit Care. 21 (2017): 227. [CrossRef]
- Abate, Semagn Mekonnen, et al. Prevalence and outcomes of Malnutrition among hospitalized COVID-19 patients: A systematic review and meta-analysis. Clinical Nutrition ESPEN 43 (2021): 174-183. [CrossRef]
- Castro-Vega I, Veses-Martín S, Cantero-Llorca J, Salom-Vendrell C, Bañuls C, Hernández-Mijares A. Validación del cribado nutricional Malnutrition Screening Tool comparado con la valoración nutricional completa y otros cribados en distintos ámbitos sociosanitarios. Nutr. Hosp. 2018 [Internet]; 35(2):351-358. Available online: https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0212-16112018000200351 (accessed on 26 jun 2023).
- British Association of Parenteral and Enteral Nutrition – BAPEN. Malnutrition Universal Screening Tool (Instrumento universal para el cribado de la malnutrición) [Internet]. 2003 Available online: https://www.bapen.org.uk/images/pdfs/must/spanish/must-toolkit.pdf (accessed on 25 august 2023).
- Savin, Z., Kupershmidt, A., Phollan, D., Lazarovich, A., Rosenzweig, B., Shashar, R., ... & Mano, R. The role of malnutrition universal screening tool in predicting outcomes after radical cystectomy. Surgical Oncology. 49 (2023): 101962. [CrossRef]
- Park J, Jeon K, Chung C.R, Yang J.H, Cho Y.H, Cho J., Et al. nationwide analysis of intensive care unit admissions, 2009–2014–The Korean ICU National Data (KIND) study. Journal of Critical Care, 44 (2018): 24-30. [CrossRef]
- Thompson K, Finfer S, Woodward M, Leong R, Liu B. Sex differences in sepsis hospitalisations and outcomes in older women and men: a prospective cohort study. Journal of Infection 84.6 (2022): 770-776. [CrossRef]
- Jaitovich A, Khan M, Itty R, Chieng H, Dumas C, Nadendla P., Et al. ICU admission muscle and fat mass, survival, and disability at discharge: a prospective cohort study. Chest, 155.2 (2019): 322-330. [CrossRef]
- Kumar SI, Doo K, Sottilo-Brammeier J, Lane C, Liebler JM. Super Obesity in the Medical Intensive Care Unit. J Intensive Care Med. 35.5 (2020):478-484. [CrossRef]
- Anesi G, Savarimuthu S, Invernizzi J, Hyman R, Ramkillawan A, Eddey C., Et al. ICU Mortality Across Prepandemic and Pandemic Cohorts in a Resource-Limited Setting: A Critical Care Resiliency Analysis From South Africa. CHEST Critical Care, 1.1 (2023):100005. [CrossRef]
- Parent B, Seaton M, and O’Keefe G.E. "Biochemical markers of nutrition support in critically ill trauma victims." Journal of Parenteral and Enteral Nutrition 42.2 (2018): 335-342. [CrossRef]
- Drews R. Critical issues in hematology: anemia, thrombocytopenia, coagulopathy, and blood product transfusions in critically ill patients. Clinics in chest medicine 24.4 (2003): 607-622. [CrossRef]
- Vincent J, Baron J.F, Reinhart K, Gattinoni L, Thijs L, Webb A., Et al. Anemia and blood transfusion in critically ill patients. Jama, 288. 12 (2002): 1499-1507. [CrossRef]
- Go AS, Yang J, Ackerson LM, Lepper K, Robbins S, Massie BM, Shlipak MG. Hemoglobin level, chronic kidney disease, and the risks of death and hospitalization in adults with chronic heart failure: the Anemia in Chronic Heart Failure: Outcomes and Resource Utilization (ANCHOR) Study. Circulation. 13;113. 23 (2006): 2713-23. [CrossRef]
- Salisbury AC, Alexander KP, Reid KJ, Masoudi FA, Rathore SS, Wang TY, Bach RG, Marso SP, Spertus JA, Kosiborod M. Incidence, correlates, and outcomes of acute, hospital-acquired anemia in patients with acute myocardial infarction. Circ Cardiovasc Qual Outcomes. 3(4) (2010):337-46. [CrossRef]
- Mehdi U, Toto RD. Anemia, diabetes, and chronic kidney disease. Diabetes Care. 2009 Jul; 32.7 (2009):1320-6. DOI: https://doi.org/10.2337%2Fdc08-0779.
- Similowski T, Agustí A, MacNee W, Schönhofer B. The potential impact of anaemia of chronic disease in COPD. Eur Respir J ;27 (2006):390–396. DOI: . [CrossRef]
- Khamiees M, Raju P, DeGirolamo A, AmoatengAdjepong Y, Manthous CA. Predictors of extubation outcome in patients who have successfully completed a spontaneous breathing trial. Chest. 120 (2001):1262–1270. [CrossRef]
- Rasmussen L, Christensen S, Lenler-Petersen P, Johnsen SP. Anemia and 90-day mortality in COPD patients requiring invasive mechanical ventilation. Clin Epidemiol. 17;3 (2010):1-5. [CrossRef]
- Hayden SJ, Albert TJ, Watkins TR, Swenson ER. Anemia in critical illness: insights into etiology, consequences, and management. Am J Respir Crit Care Med. 15;185(10) (2012):1049-57. [CrossRef]
- Zaher S. "Observational study to assess the relationship between enteral nutrition delivery and nutritional biomarkers among mechanically ventilated critically ill patients." Saudi Journal of Biological Sciences 29.12 (2022): 103466. DOI: . [CrossRef]
- Son D.H, Kim K.S, Lee H.S, Lee JW., & Shin C.S. Derivation and validation of a new nutritional index for predicting 90 days mortality after ICU admission in a Korean population. Journal of the Formosan Medical Association, 119.8 (2020): 1283-1291. [CrossRef]
- Wu L, Yan Q, Mai H, Song J, Ye L, Che X, & Wang L. Does the Geriatric Nutritional Risk Index Play a Predictive Role in Postoperative Atrial Fibrillation and Outcomes in Cardiac Surgery?. Journal of Cardiothoracic and Vascular Anesthesia, 37.1 (2023): 58-64. [CrossRef]
- Stratton R, Beggs E, Holmes E, Burden S, & Cawood A. National survey of malnutrition and nutritional care in adults. (2021): [Internet]. Available online: https://www.bapen.org.uk/pdfs/reports/mag/national-survey-of-malnutrition-and-nutritional-care-2020.pdf (accesed on 10 july 2023).
- Morton M, Patterson J, Sciuva J, Perni, J, Backes F, Nagel C y Chambers LM. Malnutrition, sarcopenia, and cancer cachexia in gynecologic cancer. Gynecologic Oncology 175 (2023): 142-155. [CrossRef]
- Allen B. y Saunders J. Malnutrition and undernutrition: causes, consequences, assessment and management, Medicine. 51 (2023): 461 - 468. [CrossRef]
- Razon A.H, Haque M.I, Ahmed M.F., & Ahmad T. Assessment of dietary habits, nutritional status and common health complications of older people living in rural areas of Bangladesh. Heliyon, 8(2) (2022). [CrossRef]
- Rosato E, Gigante A, Pellicano C, Colalillo A, Alunni-Fegatelli D., & Muscaritoli M. Phase angle, nutritional status, and mortality in systemic sclerosis: An exploratory pilot study. Nutrition 107 (2023): 111946. [CrossRef]
- Lima J, Dias A.J.B, Burgel C.F, Bernardes S, Gonzalez M.C., & Silva F.M. Complementarity of nutritional screening tools to GLIM criteria on malnutrition diagnosis in hospitalised patients: A secondary analysis of a longitudinal study. Clinical Nutrition, 41.10 (2022): 2325-2332. [CrossRef]
- Pearcy J, Agarwal E, Isenring E, Somani A, Wright C., & Shankar B. Ward-based nutrition care practices and a snapshot of patient care: Results from nutritionDay in the ICU. Clinical nutrition ESPEN 41 (2021): 340-345. [CrossRef]
- McClave S.A, Taylor B.E, Martindale R.G, Warren M.M, Johnson D.R, Braunschweig C & Compher C. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (ASPEN). JPEN. Journal of parenteral and enteral nutrition, 40(2) (2016): 159-211. [CrossRef]
- Burch N. Artificial nutrition support. Medicine, 51(7) (2023): 474-479. [CrossRef]
Figure 1.
Sample selection flow diagram.
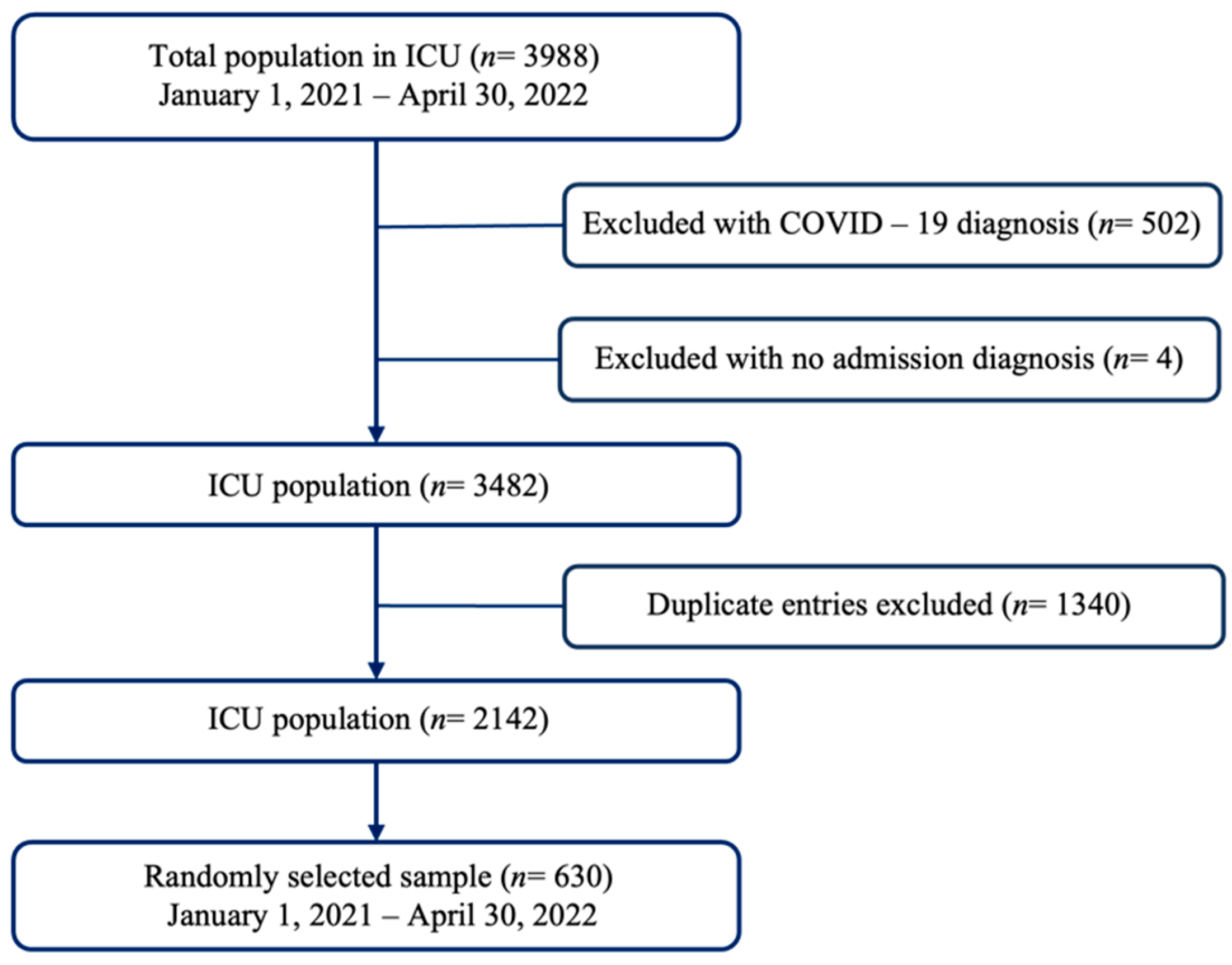

Table 1.
Hematological and biochemical variables and their measurement.
| Hematological parameter | ||
| Hemoglobin | Normal range | 12.3–15.3 g/dL |
| Anemia | <12.3 g/dL | |
| Polycythemia | >15.3 g/dL | |
| Leukocyte levels | Normal range | 4.5–11 × 103/uL |
| Leukocytosis | >11 × 103/uL | |
| Leukopenia | <4.5 × 103/uL | |
| Lymphocyte levels | Normal range | 1.0– 4.8 × 103/uL |
| Lymphocytosis | >4.8 × 103/uL | |
| Lymphopenia | <1.0 × 103/uL | |
| Biochemical parameters | ||
| Urea nitrogen levels | Normal range | 7–20 mg/dL |
| Increased | >20 mg/dL | |
| Decreased | <7 mg/dL | |
| Creatinine levels | Normal range | 0.7–1.4 mg/dl |
| Increased | >1.4 mg/dl | |
| Decreased | <0.7 mg/dl | |
| Chlorine levels | Normal range | 96 – 106 mEq/L |
| Hyperchloremia | >106 mEq/L | |
| Hypochloremia | <96 mEq/L | |
| Potassium levels | Normal kalemia | 3.5 – 5.0 mEq/L |
| Hyperkalemia | >5 mEq/L | |
| Hypokalemia | <3.5 mEq/L | |
| Sodium levels | Normal range | 135 – 145 mEq/L |
| Hypernatremia | >145 mEq/L | |
| Hyponatremia | <135 mEq/L | |
Abbreviations: g, gram; dL, deciliter; uL, units per liter; mg, milligrams; mEq, milliequivalent; L, liter.
Table 2.
Characterization of patients admitted to the ICU.
| Variables | Total x̄ (±SD) n (%) | Female x̄ (±SD) 289 (45.87%) | Male x̄ (±SD) 341 (54.13%) | p |
|---|---|---|---|---|
| Age | 64.75 (± 16.21) | 63.32 (± 18.08) | 65.97 (± 14.35) | 0.041 |
| Cause of admission ICD-11 | ||||
| Circulatory and respiratory diseases | 315 (50) | 123 (39) | 192 (61) | 0.011 |
| Neoplasms | 107 (17) | 50 (46.7) | 57 (53.3) | |
| Nervous and musculoskeletal diseases and trauma | 83 (13.1) | 45 (54.2) | 38 (45.8) | |
| Endocrine and digestive diseases | 47 (7.5) | 28 (59.6) | 19 (40.4) | |
| Infectious or parasitic diseases | 33 (5.2) | 17 (51.5) | 16 (48.5) | |
| Other diseases | 45 (7.1) | 26 (57.8) | 19 (42.2) | |
| Days of hospitalization | 6.06 (8.49) | 6.25 (10.24) | 5.90 (6.69) | 0.612 |
| Deaths | 73 (11.6) | 35 (48) | 38 (52.) | 0.706 |
| Weight | 66.35 (± 13.78) | 61.95 (± 12.55) | 70.08 (± 13.68) | <0.001 |
| BMI | 24.76 (± 4.75) | 24.83 (± 4.98) | 24.70 (± 4.57) | 0.746 |
| Nutritional risk | ||||
| Low risk | 383 (60.8) | 161 (42) | 222 (58) | 0.054 |
| Medium risk | 68 (10.8) | 36 (52.9) | 32 (47.1) | |
| High risk | 179 (28.4) | 92 (51.4) | 87 (48.6) | |
x̄: Average; ±SD: Standard deviation.
Table 3.
Hematological and biochemical parameters associated with nutritional risk.
| Laboratory tests | x̄ (±SD) | MUST scale | |||
|---|---|---|---|---|---|
| Low risk | Medium risk | High risk | p | ||
| Hemoglobin (g/dL) | 11.46 (2.60) | 11.79 (2.67) | 11.21 (2.55) | 10.84 (2.32) | <0.001 |
| Hematocrit (%) | 35.37 (7.68) | 36.35 (7.80) | 34.76 (7.91) | 33.49 (6.98) | <0.001 |
| Leukocytes (x103/uL) | 10.68 (17.22) | 10.21 (11.05) | 9.14 (5.82) | 12.27 (27.73) | 0.308 |
| Lymphocytes (x103/uL) | 2.01 (9.77) | 2.08 (10.86) | 1.43 (0.70) | 2.04 (8.89) | 0.876 |
| BUN (mg/dL) | 25.63 (18.41) | 25.40 (18.49) | 23.72 (16.68) | 26.83 (18.88) | 0.460 |
| Creatinine (mg/dL) | 1.61 (2.08) | 1.65 (2.08) | 1.67 (2.25) | 1.50 (1.99) | 0.716 |
| Chlorine (mEq/L) | 104.09 (7.89) | 104.45 (5.99) | 104.89 (4.27) | 103.02 (11.51) | 0.091 |
| Potassium (mEq/L) | 4.15 (0.64) | 4.15 (0.59) | 4.14 (0.61) | 4.14 (0.75) | 0.971 |
| Sodium (mEq/L) | 139.13 (5.03) | 139.28 (5.42) | 139.61 (3.15) | 138.62 (4.68) | 0.251 |
x̄: Average; SD: Standard deviation.
Table 4.
Factors related to the results of the MUST scale.
| MUST scale nutritional risk | High risk n (%) |
Medium risk n (%) |
Low risk n (%) |
Total | p |
|---|---|---|---|---|---|
| 179 (28.41) | 68 (10.8) | 383 (60.8) | 630 | ||
| Cause of admission ICD -11 | |||||
| Circulatory and respiratory diseases | 68 (21.6) | 36 (11.4) | 211 (67) | 315 (50) | 0.005 |
| Neoplasms | 41 (38.3) | 9 (8.4) | 57 (53.3) | 107 (17) | |
| Nervous and musculoskeletal diseases and trauma | 20 (24.1) | 9 (10.8) | 54 (65.1) | 83 (13.2) | |
| Endocrine and digestive diseases | 18 (38.3) | 7 (15) | 22 (46.8) | 47 (7.5) | |
| Infectious or parasitic diseases | 14 (42.4) | 1 (3) | 18 (54.6) | 33 (5.2) | |
| Other diseases | 18 (40) | 6 (13.3) | 21 (46.7) | 45 (7.1) | |
| Gastrointestinal symptoms | |||||
| Presence of hyporexia | 65 (47.8) | 8 (5.9) | 63 (46.3) | 136 (21.6) | <0.001 |
| Absence of hyporexia | 114 (23.1) | 60 (12.2) | 320 (64.8) | 494 (78.4) | |
| Presence of abdominal distension | 73 (36.1) | 21 (10.4) | 108 (53.5) | 202 (32.1) | 0.012 |
| Absence of abdominal distension | 106 (24.8) | 47 (11) | 275 (64.3) | 428 (67.9) | |
| Presence of diarrhea | 59 (43.7) | 10 (7.4) | 66 (48.9) | 135 (21.4) | <0.001 |
| Absence of diarrhea | 120 (24.2) | 58 (11.7) | 317 (64) | 495 (78.6) | |
| Presence of abdominal pain | 89 (37.6) | 20 (8.4) | 128 (54) | 237 (37.6) | <0.001 |
| Absence of abdominal pain | 90 (22.9) | 48 (12.2) | 255 (64.9) | 393 (62.4) | |
| Presence of swallowing difficulties | 70 (45.7) | 5 (3.3) | 78 (51) | 153 (24.3) | <0.001 |
| Absence of swallowing difficulties | 109 (22.9) | 63 (13.2) | 305 (63.9) | 477 (75.7) | |
| Presence of emesis | 86 (39.5) | 16 (7.3) | 116 (53.2) | 218 (34.6) | <0.001 |
| Absence of emesis | 93 (22.6) | 52 (12.6) | 267 (64.8) | 412 (65.4) | |
| Nutritional support route | |||||
| Oral route | 125 (23.5) | 64 (12.1) | 342 (64.4) | 531 (84.3) | <0.001 |
| Enteral route | 37 (48.1) | 4 (5.2) | 36 (46.8) | 77 (12.2) | |
| Parenteral route | 17 (77.3) | 0 | 5 (22.7) | 22 (3.5) | |
Table 5.
Factors related to mortality in the ICU.
| Variables | Alive x̄ (±SD) n (%) |
Dead x̄ (±SD) n (%) |
p |
|---|---|---|---|
| Nutritional risk according to MUST | |||
| High risk | 149 (26.8) | 30 (41.1) | 0.037 |
| Medium risk | 62 (11.1) | 6 (8.2) | |
| Low risk | 346 (62.1) | 37 (50.7) | |
| Hematological parameters | |||
| Hemoglobin (g/dL) | 11.60 (2.63) | 10.39 (20.06) | < 0.001 |
| Leukocytes (x103/uL) | 10.52 (17.92) | 11.85 (10.52) | 0.533 |
| Lymphocytes (x103/uL) | 2.12 (10.39) | 1.10 (0.56) | 0.396 |
| Biochemical parameters | |||
| BUN (mg/dL) | 24.32 (16.89) | 35.45 (25.33) | < 0.001 |
| Creatinine (mg/dL) | 1.55 (2.06) | 2.02 (2.08) | 0.068 |
| Chlorine (mEq/L) | 104.15 (6.78) | 103.61 (13.21) | 0.728 |
| Potassium (mEq/L) | 4.13 (0.62) | 4.23 (0.77) | 0.318 |
| Sodium (mEq/L) | 139.17 (4.73) | 138.78 (6.86) | 0.631 |
x̄: Average; ±SD: Standard deviation.
Table 6.
Multivariate logistic regression model of nutritional risk association.
| Raw estimate (unadjusted) | Adjusted estimate | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | Low Nutritional Risk | Medium / High Nutritional Risk | OR | 95% CI | p | OR | 95% CI | p |
| Hyporexia | ||||||||
| No | 320 (64.78) | 174 (35.22) | 1 (Ref.) | - | - | 1 (Ref.) | - | - |
| Yes | 63 (46.32) | 73 (53.68) | 0.47 | 0.32 - 0.69 | 0.000 | 1.82 | 1.22 - 2.71 | 0.003 |
| Interpretation of hemoglobin levels | ||||||||
| Normal range | 122 (65.95) | 63 (34.05) | 1 (Ref.) | - | - | 1 (Ref.) | - | - |
| Polycythemia | 45 (83.33) | 9 (16.67) | 0.39 | 0.18 - 0.84 | 0.017 | 0.38 | 0.17 - 0.84 | 0.017 |
| Anemia | 216 (55.24) | 175 (44.76) | 1.57 | 1.09 - 2.26 | 0.015 | 1.31 | 0.89 - 1.91 | 0.168 |
| Nutritional support route | ||||||||
| Oral support | 342 (64.41) | 189 (35.59) | 1 (Ref.) | - | - | 1 (Ref.) | - | - |
| Enteral support | 36 (46.75) | 41 (53.25) | 2.06 | 1.27 - 3.34 | 0.003 | 1.85 | 1.13 - 3.04 | 0.015 |
| Parenteral support | 5 (22.73) | 17 (77.27) | 6.15 | 2.23 - 16.94 | 0.000 | 5.61 | 2.00 - 15.74 | 0.001 |
| Evaluation of the associative model for nutritional risk | ||||||||
| Reference test | ||||||||
| Diagnostic test | Sick | Healthy | Total | |||||
| Positive | 98 | 69 | 167 | |||||
| Negative | 149 | 314 | 463 | |||||
| Total | 247 | 383 | 630 | |||||
| Value | CI (95%) | |||||||
| Sensitivity (%) | 39.68 | 33.37 | 45.98 | |||||
| Specificity (%) | 81.98 | 78.00 | 85.96 | |||||
| Validity index (%) | 65.40 | 61.60 | 69.19 | |||||
| Predictive value + | 58.68 | 50.92 | 66.45 | |||||
| Predictive value − | 67.82 | 63.46 | 72.18 | |||||
| Prevalence (%) | 39.21 | 35.31 | 43.10 | |||||
| Youden index | 0.22 | 0.14 | 0.29 | |||||
| Likelihood ratio + | 2.20 | 1.69 | 2.87 | |||||
| Likelihood ratio − | 0.74 | 0.66 | 0.82 | |||||
OR: Odds Ratio; CI: Confidence Interval; Qualitative variables: absolute frequency (relative frequency). Cox and Snell’s R2: 0.073. Nagelkerke’s R2: 0.099. Hosmer and Lemeshow: 0.621. Area under the curve - ROC: 0.644.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



