
Submitted:
19 December 2023
Posted:
20 December 2023
You are already at the latest version
Abstract
: Anti-MDA5 antibody bearing (anti-MDA5+)-dermatomyositis (DM) or polymyositis (PM) is notorious for causing rapidly progressive interstitial lung disease (RPILD) &/or cancers with high mortality rate. However, anti-MDA5 antibodies (Abs) are also found in other connective tissue diseases and their link with RPILD especially with regards to the mortality rate are unknown. We retrospectively recruited 71 patients bearing anti-MDA5-Abs in serum, stratified them in terms of a presence or absence of RPILD, and evaluated their clinical features, laboratory findings, associated myositis antibodies, concurrent connective tissue disease (CTD) as well as newly developed malignancies. Thirty-nine (55%) patients presented with DM/PM but 32 (45%) didn’t. Twenty-two of the former and 11 of the latter developed RPILD eventually, accounting for a total of 46% of all MDA5 bearing patients. On the other hand, 15 of all 71 (21.1%) patients had cancers. Among 32 patients who didn’t have DM/PM, 27 (38.0% of all 71) had other CTDs, indicating that only 5 (7.0% of 71) patients did not have CTDs. Senility (odds ratio [OR]=1.816, P=0.032), presence of anti-Ro-52 antibody (OR=1.676, P=0.018), elevated C-reactive protein (CRP, OR= 4.354, P<0.001) and carcinoembryonic antigen (CEA, OR=2.625, P=0.005) posed risks for RPILD. High lactose dehydrogenase (LDH, p=0.009), CRP (p=0.001), CEA (p=0.001), ferritin (p ≤ 0.001) and low albumin (p ≤ 0.001) were significantly associated with mortality. Anti-SAE antibodies were negatively correlated with RPILD as analyzed by univariate (OR=0.245, P=0.017) and multivariate (OR= 0.058, P=0.036) regressions, indicating that they may be a protective factor from RPILD (OR= 0.543, P=0.008) or fatality (OR= 0.707, P=0.012), which was also demonstrated in subgroup analyses. In contrast to various risk factors for RPILD or mortality, anti-SAE antibodies might be conversely a protective factor in anti-MDA5+ patients.
Keywords:
anti-MDA5 antibodies
; dermatomyositis (DM)
; anti-SAE antibodies
; rapidly progressive interstitial lung disease (RPILD)
1. Introduction
Amyopathic dermatomyositis (ADM) is defined as a disorder with typical cutaneous manifestations of dermatomyositis (DM) but without evidence of muscle involvement [1]. A subset of ADM with anti-melanoma differentiation-associated gene 5 antibodies (anti-MDA5 Abs) has been especially linked with rapidly progressive interstitial lung disease (RPILD) that poses very poor prognosis in eastern Asian patients [2,3,4,5]. The prevalence of RPILD in anti-MDA5+-DM patients is ranged from 38% to 70% [6,7,8]. Six-month survival rate of RPILD-ADM patients can be as low as 41% albeit aggressive treatments [9].
Variant poor prognostic factors in MDA5+-DM with ILD have been identified, including older age at disease onset, skin involvement, higher levels of lactose dehydrogenase (LDH), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), ferritin, interleukin (IL)-6, and serum tumor markers, …etc. [10,11]. However, the etiologies of anti-MDA5-associated RPILD have not been fully characterized. Only sporadic studies have pointed out the link between viral infection and anti-MDA5+-DM associated RPILD [12,13,14].
On the other hand, not only RPILD, connective tissue disease associated interstitial lung disease (CTD-ILD) including those associated with myositis will also cause progressive fibrosing ILD (PF-ILD). A diagnosis of PF-ILD must depend on the development of at least two of the three features within the previous one year without explainable reasons. These 3 features are worsening of the respiratory symptoms, physiological evidence of disease progression, and radiological evidence of disease progression [15]. Despite cumulating evidence in favor of the efficacy of anti-fibrotic drugs such as nintedanib on PF-ILD [16], there is still a lack of trials exploring the effect of such drugs on RPILD.
DM patients with anti-small ubiquitin-like modifier activating enzyme (anti-SAE) Abs tend to develop severe skin diseases without overt muscle involvement [17]. Anti-Ro52 Abs have been linked to higher prevalence of RPILD with a poorer prognosis in the anti-MDA5+DM cohort [18].
Up to now, there has been no specific criteria raised for ADM. Both 2017 EULAR/ACR and Bohan/Peter criteria did not incorporate the presence of ani-MDA5 Abs as a criterion. Thus, approximately 30% of ADM patients may have been neglected by these two criteria [19]. Previous studies have emphasized on the risk factors for anti-MDA5+-DM with RPILD. However, other anti-MDA5 antibody-associated diseases, such as subsets not fulfilling either criteria, who may or may not develop RPILD subsequently, have not been investigated. Therefore, we designed the present study to clarify different baseline conditions, clinical features, and laboratory manifestations in anti-MDA5+ patients with or without RPILD.
2. Materials and Methods
2.1. Patients and study design
We included all anti-MDA5+ patients and stratified them according to 2017 ACR/EULAR, Sontheimer’s or 1975 Bohan/Peter criteria into those with DM/RPILD and those without DM but with or without RPILD in Taipei Veterans General Hospital (TVGH) from 2018 to 2022 (Supplement Figure 1) [20,21,22]. The anti-MDA5 Abs or other myositis specific Abs were measured by the kits commercially available (EUROIMMUN [South East Asia] Pte. Ltd., Taipei, Taiwan) in routine outpatient or inpatient practice. All patients’ medical records were retrospectively reviewed. A total of 73 patients were found anti-MDA5+. Two of them were excluded because they only visited the outpatient clinic once without any pertinent data. Among the 71 included patients, 39 (55%) were classified as DM. The baseline data, clinical features, laboratory data, lung imaging, concurrent myositis Abs, concomitant malignancies, and a presence or absence of other CTDs (rheumatoid arthritis [RA], systemic lupus erythematosus [SLE], Sjögren syndrome, autoimmune hepatitis [AIH], mixed connective tissue disease [MCTD], systemic sclerosis [SSc], adult onset Still’s disease [AOSD], ankylosing spondylitis [AS], or immunoglobulin G4-related disease [IgG4-RD]) were compared between anti-MDA5+ patients with and without RPILD. Patients who were documented to have concurrent malignancies or other CTD must have been ILD-free before anti-MDA5 Abs were detected. All patients with CTD must have been regularly followed up in this hospital for at least 3 months.
ILD was identified through plain radiography and/or high-resolution computerized tomography (HRCT) of the chest. Those who were initially suspected to have ILD in chest X ray would undergo subsequent HRCT scan to confirm the diagnosis as our standard procedures in routine clinical practice. The HRCT images were independently and blindly reassessed by two radiologists after inclusion into the study protocol, ensuring inter-observer agreement. Individuals who developed progressive dyspnea, hypoxemia, and interstitial lesions as demonstrated on the imaging studies within 3 months from the onset of respiratory symptoms were defined as having RPILD [23]. A presence of interstitial pneumonia with autoimmune features (IPAF) must meet all a priori requirments and have at least one feature retrieved from at least two of the clinical, serological and morphological domains [24]. The investigation has been approved by the Institutional Review Board of the TVGH (IRB-No: 2021–06-021BC).
2.2. Statistical analyses
The features of anti-MDA5+ patients with and without RPILD were compared by Student’s t-test. Fisher’s exact test was used to evaluate the differences in frequencies for elevated serum aspartate aminotransferase (AST, normal 10-36 U/L), lactate dehydrogenase (LDH, normal 140-280 U/L in adults), creatine kinase (CK, nomal 30-170 U/L), myoglobulin (normal 5-70 μg/L), C-reactive protein (CRP, normal < 0.5 mg/dL), erythrocyte sedimentation rate (ESR, normal < 20 mm/hr), albumin (Alb, normal 3.7-5.4 gm/dL), carcinoembryonic antigen (CEA, normal < 5 μg/L), cancer antigen 15-3 (CA-153, normal ≤ 30 U/mL), IgE (normal < 180 IU/ml) and ferritin (normal 24-336 ng/mL) levels. P < 0.05 was considered statistically significant by two-tailed tests. Univariate and multivariate logistic regression analyses were used to calculate the odds ratio (OR) as well as 95% confidential interval (CI) for RPILD and death in anti-MDA5+ related diseases. Statistical Package for Social Science (SPSS) software V.25 (IBM Corp., Armonk, NY, USA) was used for the statistical descriptions and analyses.
3. Results
3.1. Clinical and laboratory features of anti-MDA5+-patients
A total of 71 anti-MDA5+-patients were included from January 2018 to August 2022. The basic characteristics of these patients were summarized in Table 1A. Twenty-five (35.2%) were male and 46 (64.8%) were female. The mean age at inclusion was 63-year-old. As shown in Supplement Figure 1, 39 (55%) were recognized to have DM, according to 2017 EULAR/ACR, 1975 Bohan-Peter or Sontheimer’s criteria, among whom 22 (31.0%) developed RPILD eventually. On the other hand, among the rest of 32 patients that didn’t have DM, 11 (15.5%) developed RPILD also. Among these 33 (46.5%) patients with RPILD, 20 (28.1%) were categorized as nonspecific interstitial pneumonia (NSIP) and 13 (18.3%) were categorized as usual interstitial pneumonia (UIP). Uniquely, 4 (5.6%) of those without DM were also classified as having interstitial pneumonia with autoimmune feature (IPAF). Twenty-seven (38.0%) were recognized to have other CTDs (overlapped with or existing without DM, as listed in supplement Table 1) and 15 (21.1%) were co-morbid with malignancy (Supplement Table 2). The CT pattern and pulmonary function data of 33 RPILD patients were summarized in supplement Table 3.
Although being insignificantly different, the anti-MDA5+ RPILD group tended to be older with a presence of higher serum AST, LDH, CRP, ESR, CA-153, CEA, IgE, and/or ferritin but lower albumin, myoglobin, and CK level than the non-RPILD counterparts.
3.2. Basic laboratory data, anti-SAE antibodies, anti-Ro52 antibodies and the mortality
Compared with those in average in the parent cohort (N=71), patients with higher LDH (508.4 ± 237.5 U/L, p=0.009), CRP (8.78 ± 8.97 mg/dl, p=0.001), CEA (15.2 ± 8.6 ng/ml, p=0.001), ferritin (3178.2 ± 2147.4 ng/ml, p ≤ 0.001) but lower albumin (2.58 ± 0.43 g/dl, p ≤ 0.001) were significantly associated with mortality.
Anti-SAE Abs were present in 32 (45.1%) patients, and anti-Ro52 Abs were present in 30 (42.3%) patients. Anti-SAE Abs occurred more frequently in anti-MDA5+ -non-RPILD patients (71.9% vs. 28.1%). Furthermore, compared with those in average in the parent cohort, the LDH (360.8 ± 127.3 U/L, p=0.043) and albumin level (3.57±0.84 g/dl, p=0.037) were significantly associated with mortality, whereas the LDH level (411.8±179.7 U/L) was significantly lower and the albumin level (3.32±0.79 g/dl) was significantly higher in anti-MDA5+ and anti-SAE+ double positive patients. The AST, myoglobulin, ESR, CA-153, CEA, and ferritin levels were lower in anti-SAE+ cohort than in the parent cohort. On the contrary, except albumin, CRP and IgE levels, other laboratory results were higher in anti-MDA5+ and anti-Ro52+ double positive cohort than in the parent cohort (data not shown).
There were 3 anti-SAE+ patients who succumbed during the study period. They were male, aged 74, 79, and 59 years respectively. All of them developed RPILD with UIP pattern. The first patient died of pneumonia with acute respiratory failure. Notably, this patient also experienced pneumothorax during the hospitalization. The second one passed away due to aspiration pneumonia. The third succumbed ultimately to aspiration pneumonia with secondary respiratory failure despite previous tracheostomy. Additionally, he also experienced pneumothorax during the last hospitalization.
3.3. Subgroup analysis: Stratification by the positivity of anti-SAE antibodies
To further clarify the role of anti-SAE in RPILD and mortality, we stratified the patients into positive or negative anti-SAE antibody group. As shown in Table 1B, the risk factor to develop RPILD in negative anti-SAE group was elevated CRP (OR=17.111, p=0.04), CEA (OR=35, p= 0.026), ferritin (OR=19, p=0.032). In contrast, none of these odd’s ratio were seen in anti-SAE positive group.

Table 1.
B. Subgroup analysis of RP-ILD in anti-SAE antibody positive and negative groups.
| Anti-SAE positive (N=32) | Anti-SAE negative(N=39) | |||||||
| RP-ILD(N=9, 28.1%) | Non-RP-ILD (N=23, 71.9%) |
p-value | OR*** (C.I.#) |
RP-ILD(N=23, 59%) | Non-RP-ILD(N=16, 41%) | p-value | OR***(C.I.#) | |
| LDH (SD**) U/L | 376.22(112.3) | 353.9((135.6) | 0.670 | 0.441(p=0.442,0.057-3.421) | 456.43(230.4) | 439.94(165.1) | 0.807 | 3.385(p=0.55, 0.279-41.087) |
| CRP (S.D.**) mg/dl | 8.23(8.9) | 2.547(3.7) | 0.018* | 2.667(p=0.427, 0.521-13.655) |
5.40(8.04) | 2.26(5.9) | 0.192 | 17.111((p=0.04,1.832-159.802*) |
| Albumin (S.D.**), g/dl | 3.31(1.1) | 3.67(0.75) | 0.358 | 1.905(p=0.659, 0.321-11.312) |
3.05(0.8) | 3.33(0.5) | 0.352 | 1.583(p=0.634, 0.23-10.904) |
| CEA (S.D.**), ng/ml | 11.45(9.6) | 5.15(4.7) | 0.116 | 3(p=0.505, 0.14-64.262) |
13.02((8.4) | 2.67(1.6) | 0.012* |
35(p=0.026, 1.743-702.993*) |
| Ferritin (S.D.**) ng/ml | 2581.25(2103.6) | 557.32(343.2) | 0.004* | 0.597(p=1.00, 0.773-1.087) |
2423.49(2215.2) | 851.15(1137.4) | 0.186 |
19(p=0.032, 1.146-314.971*) |
| CK (SD**), U/L | 157.29(99.6) | 1068.7(3395.8) | 0.49 | 0.489(p=0.662, 0.76-3.145) |
620.86(972.5) | 1492.6(2436.2) | 0.144 | 0.791( p=0.749, 0.211-2.972) |
| AST (SD**) U/L | 48.38(38.1) | 65.86(103.1) | 0.647 | 1.067(p=0.647, 0.161-7.056) |
118.43(143.2) | 58.19(38.8) | 0.111 | 2.411(p=0.209, 0.652-8.92) |
| Myoglobulin (SD**), ng/ml | 92.5(130.8) | 183.68(123.4) | 0.423 | 0.25(p=0.524, 0.07-8.56) |
6(66.7%) | 3(33.3%) | 0.439 | 0.667(p=0.646, 0.047-9.472) |
| ESR (S.D.**) mm/hr | 48.14((29.8) | 47.3(37.8) | 0.958 | 1.333(p=0.546, 0.235-7.556) |
58.25(39.8) | 42.38(30.4) | 0.231 | 1.333(p=0.465, 0.235-7.556) |
| IgE (S.D.**) KU/L | 468.96(567.1) | 155.72(117.2) | 0.215 | 0.75(p=0.652, 0.064-8.834) |
212.1(179.7) | 252.91(215.8) | 0.756 | 0.75(p=0.721, 0.064-8.834) |
| anti-Ro52 antibodies (+) | 2(22.2%) | 7(77.8%) | - | 0.653(p=0.501, 0.107-3.971) |
2(22.2%) | 7(77.8%) | - | 0.653(p=0.179, 0.107-3.971) |
| Smoking | 2(22.2%) | 7(77.8%) | - | 0.653(p=0.501, 0.107-3.971) |
2(22.2%) | 7(77.8%) | - | 0.653(p=0.415, 0.107-3.971) |
As regard to mortality (Table 1C), the mortality rate in patients with positive anti-SAE and RPILD was 33.3% (3/32), and the mortality rate in those without anti-SAE but with RPILD was 60.9% (14/39). Patients with RPILD was a major risk factor in both groups, however, the likelihood ratio (LR) being much lower in anti-SAE (+) cohort (8.455, p=0.004) than in negative counterparts (20.131, p<0.001). In addition, more risk factors were identified in antibody negative group, including elevated CRP (LR=8.238, p=0.04), CEA (LR=7.664, p= 0.06), ferritin (LR=5.868, p=0.015), AST (LR=8.289, p=0.004) and lower albumin (LR=8.388, p=0.004) levels. In anti-SAE (+) group, not only fewer risk factors were identified (only elevated CRP [LR=4.439, p=0.034] and lower albumin [LR=5.194. p=0.023]), but the LR was also lower than in anti-SAE (-) counterparts. Respiratory failure less likely occurred in anti-SAE (+) group, with only 29.1% of them developing RPILD.
Table 1.
C. Subgroup analysis of mortality in anti-SAE antibody positive and negative groups.
| Anti-SAE positive | Anti-SAE negative | |||||||
| Mortality(N=3,9.4%) | Non-Mortality (N=29,90.6%) |
p-value | LR (C.I.) |
Mortality(N=14,35.9%) | Non-Mortality (N=25,64.1%) |
p-value | LR (C.I.) |
|
| RPILD | 3(33.3%) | 6(66.7%) | - |
8.455(p=0.004* 0.101-0.422) |
14(60.9%) | 9(39.1%) | - |
20.131(p<0.001, 0.213-0.607*) |
| LDH (S.D. **) U/L | 392.67(183.8) | 19(86.4%) | 0.656 | 1.311(p=0.252 0.645-0.972) |
402.92(245.9) | 402.92(163.4) | 0.054 | 2.906(p=0.088 0.752-1.018) |
| CRP (S.D.**) mg/dl | 11.68(7.4) | 3.42(5.6) | 0.025* |
4.493(p=0.034* 0.292-0.678) |
8.16(9.4) | 1.84(4.7) | 0.008* |
8.236(p=0.04 0.52-0.89*) |
| Albumin (S.D.**) g/dl | 2.4(0.529) | 3.73(0.8) | 0.007* |
5.194(p=0.023* 0.221-0.657) |
2.62(0.4) | 3.54(0.6) | 0.000* |
8.388(p=0.004* 0.455-0.919) |
| CEA (S.D.**) ng/ml | 11.95(12.4) | 6.12(5.8) | 0.272 | 1.827(p=0.177 0.351-345.1) |
16.5(8.2) | 4.19(4) | 0.002* |
7.664(p=0.06* 0.132-0.84) |
| Ferritin (S.D.**) ng/ml | 3038.33(2320.3) | 607.53(375.1) | 0.001* | 0.43(p=0.512 0.789-1.08) |
3208.14(2200.4) | 696.04(789) | 0.002* |
5.868(p=0.015* 0.467-0.905) |
| CK (SD**) U/L | 91.33(45.8) | 925.04(3104) | 0.651 | 3.394(p=0.065 0.375-1.783) |
754((1175.3) | 1129.9(2054.4) | 0.549 | 1.463(p=0.226, 0.586-9.291)) |
| AST (SD**, U/L | 53.67(64.6) | 61.88(92.9) | 0.884 | 0.145(p=0.704 0.128-21.732) |
119.5(83.5) | 79.28(129.8) | 0.304 |
8.289(p=0.004* 1.648-49.137) |
| Myoglobulin (SD**), ng/ml | 124.3(120.3) | 183.9(110.4) | 0.184 | 2.969(p=0.085 0.028-1.997) |
512.34(723.1) | 1133.4(1219.3) | 0.279 | 0.034(p=0.853 0.118-13.24) |
| ESR (S.D.**) mm/hr | 86.5(3.5) | 44.4(34.9) | 0.106 | 2.776(p=0.096 0.319-1.722) |
57.08(35.6) | 49.1(37.9) | 0.556 | 0.075(p=0.784, 0.278-5.454) |
| IgE (S.D.**) KU/L | 1053.5(369.8) | 130.24(106.6) | 0.000* | 2.055(p=0.152 0.15-0.455) |
127.36(149.8) | 303.12(172.6) | 0.108 | 2.284(p=0.131, 0.008-2.181) |
| anti-Ro52 antibodies (+) | 0(0%) | 9(100%) | - | 2.1(p=0.147 0.54-3.88) |
0(0%) | 9(100%) | - | 2.076(p=0.15, 0.642-12.926) |
| Smoking (+) | 1(11.1%) | 8(88.9%) | - | 0.043(p=0.836 0.104-16.55) |
1(11.1%) | 8(88.9%) | - | 1.949(p=0.163, 0.026-2.269) |
3.4. Subgroup analysis: Stratification by the diagonosis of DM or not
As shown in Table 2, the mean age in non-DM with anti-MDA5 positive group tended to be older than that in DM with anti-MDA5 group (64.7 years old vs. 62.4 years, p = 0.480) although not significantly different. On the other hand, the LDH and ferritin levels were significantly lower in non-DM with MDA5 group (LDH: 344.16 vs. 468.43, p=0.04, ferritin: 959.89 vs. 2179.56, p=0.033). The positive rate of anti-Ro52 or anti-SAE Abs were also different between two group, with anti-Ro52 being more prevalent in DM group (73.3% vs. 26.7%, p=0.009) and anti-SAE Abs being more prevalent in non-DM group (75% vs. 25%, p<0.001). Furthermore, the mortality rate was higher in DM group (OR=5.413, p=0.012), who also tended to have less anti-SAE and more anti-Ro52 Abs.
Table 2.
Subgroup analysis on the non-DM patients vs. DM patients both with anti-MDA5 Abs.
| Non-DM with anti-MDA5 | DM with anti-MDA5 | p-value | |
| Age, y/o | 64.7 (13.9) | 62.4 (13.9) | 0.480 |
| AST (S.D.) U/L | 63.83 (89.1) | 91.64 (116.6) | 0.287 |
| LDH (S.D.) U/L | 344.16 (133.9)) | 468.43 (194.7) | 0.04* |
| Myoglobulin (S.D.), ng/ml | 212.67 (163.4) | 729.59 (981.5) | 0.223 |
| CRP (S.D.) mg/dl | 4.19 (6.9) | 4.15 (6.8) | 0.981 |
| ESR (S.D.) mm/hr | 51.12 (37.6) | 49.1 (35.0) | 0.833 |
| Ferritin (S.D.) ng/ml | 959.89 (1427.2) | 2179.56 (2054.8) | 0.033* |
| CA-153 (S.D.), U/ml | 21.4 (26.3) | 19.08 (12.9) | 0.826 |
| CEA (S.D.) ng/ml | 7.75 (6.47) | 7.78 (8.1) | 0.99 |
| IgE (S.D.) KU/L | 296.5 (369.7) | 208.9 (192.2) | 0.524 |
| Alb (S.D.) g/dl | 3.46 (0.82) | 3.22 (0.76) | 0.278 |
| CK (S.D.) U/L | 755.8 (2839) | 1039.2 (1772.1) | 0.657 |
| Anti-RO52 antibody | 8 (26.7%) | 22 (73.3%) | 0.009* |
| Anti-SAE antibody | 24 (75%) | 8 (25%) | <0.001* |
| RPILD | 11 (33.3%) | 22 (66.7%) | 0.094 |
| Mortality# | 3 (17.6%) | 14(82.4%) | 0.012* |
3.5. Kaplan-Meier survival analysis of total anti-MDA5 cohort, anti-SAE+ and anti-Ro52+ groups
As shown in Figure 1 and Figure 2, the entire cohort of anti-MDA5 positive patients had a median survival time of 40.5 months. Regarding the effect of anti-SAE on the survival, the median survival time in the anti-SAE (+) group was significantly longer than that in antibody negative counterparts (47. 7 vs. 42.4 months, p=0.018). Conversely, patients with anti-Ro52 Abs had a shorter median survival time than anti-Ro negative patients (42.4 months vs. 38.7 months, p=0.021).
3.6. Univariate and multivariate logistic regression analyses for risk factors of RPILD in anti-MDA5+ patients
Univariate and multivariate analyses were performed to calculate the risk factors for RPILD in anti-MDA5+ patients (Table 3). As analyzed by univariate regression, anti-Ro52 Abs were an independent risk factor (OR=3.331 CI=1.25-8.91, P=0.017), whereas anti-SAE Abs were conversely a significant protective factor (OR=0.245 CI=1.25-8.91, P=0.017) for RPILD. Furthermore, according to multivariate regression, anti-SAE Abs still served as a protective factor from RPILD (OR= 0.058, CI=0.004-0.829, P=0.036).
Table 3.
Univariate and multivariate logistic regression analysis for the risk factors with RPILD in anti-MDA5+ patients.
Table 3.
Univariate and multivariate logistic regression analysis for the risk factors with RPILD in anti-MDA5+ patients.
| Variable | Univariate | Multivariate | ||||||
| OR | 95% CI of OR | P value | OR | 95% CI of OR | P value | |||
| Female | 1.500 | 0.559-4.025 | 0.421 | 0.494 | 0.057-4.311 | 0.523 | ||
| High AST* | 2.267 | 0.850-6.045 | 0.102 | 3.858 | 0.493-3-.172 | 0.198 | ||
| High LDH** | 1.609 | 0.351-7.377 | 0.54 | 0.254 | 0.01-6.357 | 0.404 | ||
| High Ferritin*** | 5.308 | 0.5-56.391 | 0.166 | 10.713 | 0368-312.028 | 0.168 | ||
| Ro52 | 3.331 | 1.245-8.91 | 0.017§ | 2.198 | 0.116-41.489 | 0.599 | ||
| SAE | 0.245 | 0.9-0.668 | 0.006§ | 0.058 | 0.004-0.829 | 0.036§ | ||
OR = odds ratio; CI = confidence interval. * >36 U/L; **>280 U/L; ***> 336 ng/mL; § statistically significant.
3.7. Subgroup analysis: Odds ratio for RPILD and mortality
The OR of various factors for RPILD are shown in Figure 3. The age ≥ 65 years was a risk factor (OR=1.816, CI=1.051-3.136, P=0.032). Other risk factors for RPILD included anti-Ro-52+ Abs (OR=1.676, CI=1.072-2.617, P=0.018), elevated CRP (OR= 4.354, CI= 1.652-11.477, P<0.001) and CEA (OR=2.625, CI=20.800-94.236, P=0.005) levels as well as an absence of anti-SAE- Abs (OR= 2.219, CI= 1.202-4.099, P=0.008). On the other hand, anti-SAE Abs served as a protective factor for RPILD (OR= 0.543, CI=0.348-0.848, P=0.008). Additional protective factors included an absence of anti-Ro52-Abs (OR= 0.502, CI=0.282-0.896, P=0.018), age below 65 years (OR= 0.592, CI= 0.373-0.940, P= 0.032), normal CRP (OR= 0.537, CI= 0.372-0.776, P<0.001) and CEA (OR= 0.188, CI= 0.48-0.728, P= 0.005) levels.
Figure 4 shows the risk factors for mortality. Although not significantly, older patients tended to have higher mortality rate than younger patients. Anti-SAE+ antibodies not only served as a protective factor from RPILD, but also from mortality (OR= 0.707, CI= 0.545, P=0.012). A presence of anti-SAE Abs and absence of anti-Ro-52-Abs were prone to exclusion of DM. Normal AST and CEA in anti-MDA5+ patients comorbid with other CTDs posed a protective factor from mortality.
4. Discussion
Anti-MDA5 Abs are notorious for causing RPILD and high mortality rate in DM patients [25]. Various therapeutic regimens have been tried to lower the high death rate [26,27,28,29], but there still lack randomized controlled trials or large prospective studies to provide evidence-based treatments. Because of a limited treatment and a poor prognosis, high index of suspicion with earlier & adequate interventions are important to prevent further morbidity and mortality. Moreover, identifying the coexisting parameters influencing MDA5 antibody’s favoring of the development of RPILD are essential as well.
Numerous studies dealing with the risk factors for RPILD in DM patients have revealed that old age, elevated LDH, ferritin, CEA, CA-153, & CRP, a presence of anti-Ro52 antibodies, high titer of anti-MDA5 antibodies as well as a short disease duration of less than 3 months are the key risk factors [30,31,32]. Furthermore, prediction model based on LDH, age and white cell count (FLAW model) has also been proposed to stratify the risks [33]. In the present study, senility, anti-Ro52 antibodies, high CRP and CEA levels were found associated with the development of RPILD, which was compatible with previous researches. With regards to the mortality, our findings were in accordance with other studies, i.e., high CRP, ferritin, AST, & CEA level as well as existing RPILD might contribute to mortality. Moreover, definite DM might also increase the mortality. Conversely, anti-MDA5+ diseases other than DM might otherwise decrease the mortality. Compared with these non-DM anti-MDA5+ individuals, most DM patients with anti-MDA5 Abs (73%) occurred with more anti-Ro52 and less anti-SAE antibodies.
To the best of our knowledge, there has been no study dealing with the relationship between anti-SAE Abs and RPILD. Encouragingly, the present study demonstrated that anti-SAE Abs were not only a protective factor from anti-MDA5+ RPILD but also a favorable parameter for getting rid of mortality. Anti-SAE+- patients has been featured with cutaneous lesions such as Göttron’s papules, violaceus rash, or the absence of overt muscle involvement [17,18,34]. Other manifestations including dysphagia, arthritis, constitutional symptoms as well as ILD were heterogenous as reported in different studies [35,36].
Except for anti-Ro52 Abs, it is unclear whether two myositis specific antibodies (MSAs) will interact with each other when coexisting. Anti-Ro52 antibodies were strongly correlated with anti-synthetase+-ILD and anti-MDA5+-ILD [37]. On the other hand, Ge et al. have found that one-third of the anti-SAE+-patients can simultaneously carry other MSAs uneventfully. Furthermore, the incidence of ILD in DM associated with the Abs was higher in Asian than in European cohort [18].
The average age of our patients (63.4 years) was older than that was reported in most of the other DM studies. This was consistent with previous concept that DM onset age in the anti-SAE+-group is significantly older than that in the antibody-negative group [18]. It also suggests that anti-SAE do have some protective effect to delay the onset of autoimmune lung injury although its mechanism is still not well clarified. On the other hand, almost half of our anti-MDA5+ patients (45.2%) concurred with anti-SAE Abs, the prevalence rate being higher than that showed in the previous Asian report.
According to our results, anti-SAE Abs might be regarded as a protective factor from both RPILD and mortality when they coexist with anti-MDA5 Abs. A previous study conducted by Ge et al has shown that anti-SAE+-DM patients have a disease activity lower than their anti-SAE- -counterparts. Since anti-SAE Abs tend to have this protective effect, anti-MDA5+ RPILD may also be guarded by anti-SAE Abs, regardless of definite presence of DM or not. Besides, anti-SAE+ -patients mainly present with typical cutaneous lesions of DM, which may alert the caregivers to investigate and intervene patients earlier, preventing possible ILD progression or mortality.
Of note, our study has also revealed the heterogeneous spectrum of anti-MDA5 antibody-associated diseases. Distinctively from non-Asian study conducted by Cavagna L et.al. [38], 24 (33.8%) of our patients were accompanied by other autoimmune diseases. Despite not being associated with RPILD, concurrent CTDs were protective factors from mortality, which might have been resulted from the prompt immunosuppressants for these CTDs. Although only 4 of our patients were diagnosed with anti-MDA5+-IPAF, none of the patients had concomitant anti-SAE Abs.
Despite pertinent findings demonstrated in this study, there were several limitations in it. Firstly, our autoantibody detections were totally dependent on EUROLINE test kit; hence, the false positive and negative rates can’t be ignored. In addition, because it is a retrospective research, some medical records are inevitably incomplete. These may include especially patients’ physical examination (PE) records including Göttron’s sign, heliotrope sign or mechanic’s hands, and because of this we were unable to analyze the correlation between PE and RPILD or mortality. Nevertheless, with so many missing data, high CEA level was still significantly associated with RPILD and mortality. This has reinforced the hypothesis that CEA activates macrophage or Kupffer cells to cause further pulmonary inflammation [31]. In addition, anti-SAE Abs might serve as a protective factor from RPILD or mortality in anti-MDA5+ RPILD patients, which needs more functional assays to verify and to explore for the underlying mechanism. Finally, this is an Asian based study. Whether its results can apply to different ethnicities is questionable, leaving a large space to fill in.
In conclusion, the present investigation has not only confirmed previous risk factors in anti-MDA5+-DM associated RPILD such as old age, ferritin, CRP, AST, CEA and anti-Ro52 Abs, but also identified anti-SAE Abs as a protective factor in Asian anti-MDA5 Abs associated diseases, especially in those concurring with RPILD of high mortality rate.
Funding
The study was partly supported by the grants from Taipei Veterans General Hospital (111-DHA0100085) and Fu Jen Catholic Hospital (FJUH111220).
Authors’ Contributions
C.-Y.T. and H.-T.L. were responsible for conceptualization, original draft preparation and study methodology. H.-C.T. and W.-S.C. wrote the draft together. Y.-S.S, C.-T.C. performed statistical analysis and data curation. C.-C.L., W.-S.C., W.-R.C., H.-T.L, Y.-Y.Y., and C.-Y.T were involved in validation, reviewing and editing. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Tang, K.; Zhang, H.; Jin, H. Clinical characteristics and management of patients with clinical amyopathic dermatomyositis: a retrospective study of 64 patients at a tertiary dermatology department. Front. Med. (Lausanne) 2021, 8, 783416. [Google Scholar] [CrossRef] [PubMed]
- Cao, H.; Pan, M.; Kang, Y.; Xia, Q.; Li, X.; Zhao, X.; Shi, R.; Lou, J.; Zhou, M.; Kuwana, M.; et al. Clinical manifestations of dermatomyositis and clinically amyopathic dermatomyositis patients with positive expression of anti-melanoma differentiation-associated gene 5 antibody. Arthritis Care Res. (Hoboken) 2012, 64, 1602–1610. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Cao, M.; Plana, M.N.; Liang, J.; Cai, H.; Kuwana, M.; Sun, L. Utility of anti-melanoma differentiation-associated gene 5 antibody measurement in identifying patients with dermatomyositis and a high risk for developing rapidly progressive interstitial lung disease: a review of the literature and a meta-analysis. Arthritis Care Res. (Hoboken) 2013, 65, 1316–1324. [Google Scholar] [CrossRef]
- Koga, T.; Fujikawa, K.; Horai, Y.; Okada, A.; Kawashiri, S.-Y.; Iwamoto, N.; Suzuki, T.; Nakashima, Y.; Tamai, M.; Arima, K.; et al. The diagnostic utility of anti-melanoma differentiation-associated gene 5 antibody testing for predicting the prognosis of Japanese patients with DM. Rheumatology (Oxford) 2012, 51, 1278–1284. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Kuwana, M. Clinically amyopathic dermatomyositis. Curr. Opin. Rheumatol. 2010, 22, 639–643. [Google Scholar] [CrossRef]
- Moghadam-Kia, S.; Oddis, C.V.; Sato, S.; Kuwana, M.; Aggarwal, R. Antimelanoma differentiation-associated gene 5 antibody: expanding the clinical spectrum in north American patients with dermatomyositis. J. Rheumatol. 2017, 44, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Vinik, O.; Shojania, K.; Yeung, J.; Shupak, R.; Nimmo, M.; Avina-Zubieta, J.A. Clinical spectrum and therapeutics in Canadian patients with anti-melanoma differentiation-associated gene 5 (MDA5)-positive dermatomyositis: a case-based review. Rheumatol. Int. 2019, 39, 1971–1981. [Google Scholar] [CrossRef] [PubMed]
- He, C.; Li, W.; Xie, Q.; Yin, G. Rituximab in the treatment of interstitial lung diseases related to anti-melanoma differentiation-associated gene 5 dermatomyositis: a systematic review. Front. Immunol. 2022, 12, 820163. [Google Scholar] [CrossRef] [PubMed]
- Ye, S.; Chen, X.-x.; Lu, X.-y; Wu, M.-f.; Deng, Y.; Huang, W.-q.; Guo, Q.; Yang, C.-d.; Gu, Y.-y.; Bao, C.-d.; et al. Adult clinically amyopathic dermatomyositis with rapid progressive interstitial lung disease: a retrospective cohort study. Clin. Rheumatol. 2007, 26, 1647–1654. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Gao, X.; Li, Y.; Jia, X.; Zhang, X.; Xu, Y.; Gan, Y.; Li, S.; Chen, R.; He, J.; et al. Predictors and mortality of rapidly progressive interstitial lung disease in patients with idiopathic inflammatory myopathy: a series of 474 patients. Front. Med. (Lausanne) 2020, 7, 363. [Google Scholar] [CrossRef]
- Shirakashi, M.; Nakashima, R.; Tsuji, H.; Tanizawa, K.; Handa, T.; Hosono, Y.; Akizuki, S.; Murakami, K.; Hashimoto, M.; Yoshifuji, H.; et al. Efficacy of plasma exchange in anti-MDA5-positive dermatomyositis with interstitial lung disease under combined immunosuppressive treatment. Rheumatology (Oxford) 2020, 59, 3284–3292. [Google Scholar] [CrossRef]
- Kato, H.; Takeuchi, O.; Sato, S.; Yoneyama, M.; Yamamoto, M.; Matsui, K.; Uematsu, S.; Jung, A.; Kawai, T.; Ishii, K.J.; et al. Differential roles of MDA5 and RIG-I helicases in the recognition of RNA viruses. Nature 2006, 441, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Miner, J.J.; Diamond, M.S. MDA5 and autoimmune disease. Nat. Genet. 2014, 46, 418–419. [Google Scholar] [CrossRef]
- Nishina, N.; Sato, S.; Masui, K.; Gono, T.; Kuwana, M. Seasonal and residential clustering at disease onset of anti-MDA5-associated interstitial lung disease. R.M.D. Open. 2020, 6, e001202. [Google Scholar] [CrossRef] [PubMed]
- Raghu, G.; Remy-Jardin, M.; Richeldi, L.; Thomson, C.C.; Inoue, Y.; Johkoh, T.; Kreuter, M.; Lynch, D.A.; Maher, T.M.; Martinez, F.J.; et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults: an official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respi.r Crit. Care Med. 2022, 205, e18–e47. [Google Scholar] [CrossRef]
- Tzilas, V.; Tzouvelekis, A.; Ryu, J.H.; Bouros, D. 2022 update on clinical practice guidelines for idiopathic pulmonary fibrosis and progressive pulmonary fibrosis. Lancet Respir. Med. 2022, 10, 729–731. [Google Scholar] [CrossRef] [PubMed]
- Tarricone, E.; Ghirardello, A.; Rampudda, M.; Bassi, N.; Punzi, L.; Doria, A. Anti-SAE antibodies in autoimmune myositis: identification by unlabelled protein immunoprecipitation in an Italian patient cohort. J. Immunol. Methods. 2012, 384, 128–134. [Google Scholar] [CrossRef]
- Ge, Y.; Lu, X.; Shu, X.; Peng, Q.; Wang, G. Clinical characteristics of anti-SAE antibodies in Chinese patients with dermatomyositis in comparison with different patient cohorts. Sci. Rep. 2017, 7, 188. [Google Scholar] [CrossRef]
- So, H.; So, J.; Lam, T.T.-O.; Wong, V.T.-L.; Ho, R.; Li, W.L.; Mok, C.C.; Lau, C.S.; Tam, L.-S. Performance of the 2017 European Alliance of Associations for Rheumatology/American College of Rheumatology classification criteria in patients with idiopathic inflammatory myopathy and anti–melanoma differentiation–associated protein 5 positivity. Arthritis Rheumatol. 2022, 74, 1588–1592. [Google Scholar] [CrossRef]
- Bohan, A.; Peter, J.B. Polymyositis and dermatomyositis (first of two parts). N. Engl. J. Med. 1975, 292, 344–347. [Google Scholar] [CrossRef]
- Bohan, A.; Peter, J.B. Polymyositis and dermatomyositis (second of two parts). N Engl J Med 1975, 292, 403–407. [Google Scholar] [CrossRef]
- Lundberg, I.E.; Tjärnlund, A.; Bottai, M.; Werth, V.P.; Pilkington, C.; de Visser, M.; Alfredsson, L.; Amato, A.A.; Barohn, R.J.; Liang, M.H.; et al. 2017 European League Against Rheumatism/American College of Rheumatology classification criteria for adult and jvenile idiopathic inflammatory myopathies and their major subgroups. Ann. Rheum. Dis. 2017, 76, 1955–1964. [Google Scholar] [CrossRef]
- Kobayashi, N.; Takezaki, S.; Kobayashi, I.; Iwata, N.; Mori, M.; Nagai, K.; Nakano, N.; Miyoshi, M.; Kinjo, N.; Murata, T.; et al. Clinical and laboratory features of fatal rapidly progressive interstitial lung disease associated with juvenile dermatomyositis. Rheumatology (Oxford) 2015, 54, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Graney, B.A.; Fischer, A. Interstitial pneumonia with autoimmune features. Ann. Am. Thorac. Soc. 2019, 16, 525–533. [Google Scholar] [CrossRef]
- Wu, W.; Guo, L.; Fu, Y.; Wang, K.; Zhang, D.; Xu, W.; Chen, Z.; Ye, S. Interstitial lung disease in anti-MDA5 positive dermatomyositis. Clin. Rev. Allergy Immunol. 2021, 60, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, H.; Nakashima, R.; Hosono, Y.; Imura, Y.; Yagita, M.; Yoshifuji, H.; Hirata, S.; Nojima, T.; Sugiyama, E.; Hatta, K.; et al. Multicenter prospective study of the efficacy and safety of combined immunosuppressive therapy with high-dose glucocorticoid, tacrolimus, and cyclophosphamide in interstitial lung diseases accompanied by anti-melanoma differentiation-associated gene 5-positive dermatomyositis. Arthritis Rheumatol. 2020, 72, 488–498. [Google Scholar]
- So, H.; Wong, V.T.L.; Lao, V.W.N.; Pang, H.T.; Yip, R.M.L. Rituximab for refractory rapidly progressive interstitial lung disease related to anti-MDA5 antibody-positive amyopathic dermatomyositis. Clin. Rheumatol. 2018, 37, 1983–1989. [Google Scholar] [CrossRef]
- Kurasawa, K.; Arai, S.; Namiki, Y.; Tanaka, A.; Takamura, Y.; Owada, T.; Arima, M.; Maezawa, R. Tofacitinib for refractory interstitial lung diseases in anti-melanoma differentiation-associated 5 gene antibody-positive dermatomyositis. Rheumatology (Oxford) 2018, 57, 2114–2119. [Google Scholar] [CrossRef] [PubMed]
- McPherson, M.; Economidou, S.; Liampas, A.; Zis, P.; Parperis, K. Management of MDA-5 antibody positive clinically amyo9athic dermatomyositis associated interstitial lung disease: a systematic review. Semin. Arthritis Rheum. 2022, 53, 151959. [Google Scholar] [CrossRef]
- 30 You, H.; Wang, L.; Wang, J.; Lv, C.; Xu, L.; Yuan, F.; Li, J.; Wu, M.; Zhou, S.; Da, Z.; et al. Time-dependent changes in RPILD and mortality risk in anti-MDA5+ DM patients: a cohort study of 272 cases in China. Rheumatology (Oxford) 2023, 62, 1216–1226. [Google Scholar] [CrossRef]
- Zhu, D.; Qiao, J.; Tang, S.; Pan, Y.; Li, S.; Yang, C.; Fang, H. Elevated carcinoembryonic antigen predicts rapidly progressive interstitial lung disease in clinically amyopathic dermatomyositis. Rheumatology (Oxford) 2021, 60, 3896–3903. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Y.; Ye, L.; Chen, F.; Shen, Y.; Lu, X.; Wang, G.; Shu, X. Different multivariable risk factors for rapid progressive interstitial lung disease in anti-MDA5 positive dermatomyositis and anti-synthetase syndrome. Front. Immunol. 2022, 13, 845988. [Google Scholar] [CrossRef] [PubMed]
- So, J.; So, H.; Wong, V.T.-L.; Ho, R.; Wu, T.Y.; Wong, P.C.-H.; Tam, L.H.-P.; Ho, C.; Lam, T.T.-O.; Chung, Y.K.; et al. Predictors of rapidly progressive interstitial lung disease and mortality in patients with autoantibodies against melanoma differentiation-associated protein 5 dermatomyositis. Rheumatology (Oxford), 4444. [Google Scholar]
- Peterson, L.K.; Jaskowski, T.D.; La’Ulu, S.L.; Tebo, A.E. Antibodies to small ubiquitin-like modifier activating enzyme are associated with a diagnosis of dermatomyositis: results from an unselected cohort. Immunol. Res. 2018, 66, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Bodoki, L.; Nagy-Vincze, M.; Griger, Z.; Betteridge, Z.; Szöllősi, L.; Dankó, K. Four dermatomyositis-specific autoantibodies-anti-TIF1γ, anti-NXP2, anti-SAE and anti-MDA5-in adult and juvenile patients with idiopathic inflammatory myopathies in a Hungarian cohort. Autoimmun. Rev. 2014, 13, 1211–1219. [Google Scholar] [CrossRef] [PubMed]
- Muro, Y.; Sugiura, K.; Akiyama, M. Low prevalence of anti-small ubiquitin-like modifier activating enzyme antibodies in dermatomyositis patients. Autoimmunity 2013, 46, 279–284. [Google Scholar] [CrossRef]
- Shao, C.; Sun, Y.; Huang, H.; Zhang, Z.; Pan, R.; Xu, K.; Zhang, X.; Zhang, Y.; Xu, Z. Myositis specific antibodies are associated with isolated anti-Ro-52 associated interstitial lung disease. Rheumatology (Oxford) 2022, 61, 1083–1091. [Google Scholar] [CrossRef]
- Cavagna, L.; Meloni, F.; Meyer, A.; Sambataro, G.; Belliato, M.; de Langhe, E.; Cavazzana, I.; Pipitone, N.; Triantafyllias, K.L.; Mosca, M.; et al. Clinical spectrum time course in non-Asian patients positive for anti-MDA5 antibodies. Clin. Exp. Rheumatol.
Figure 1.
Kaplan-Meier survival curve of anti-SAE Abs positive and negative patients.
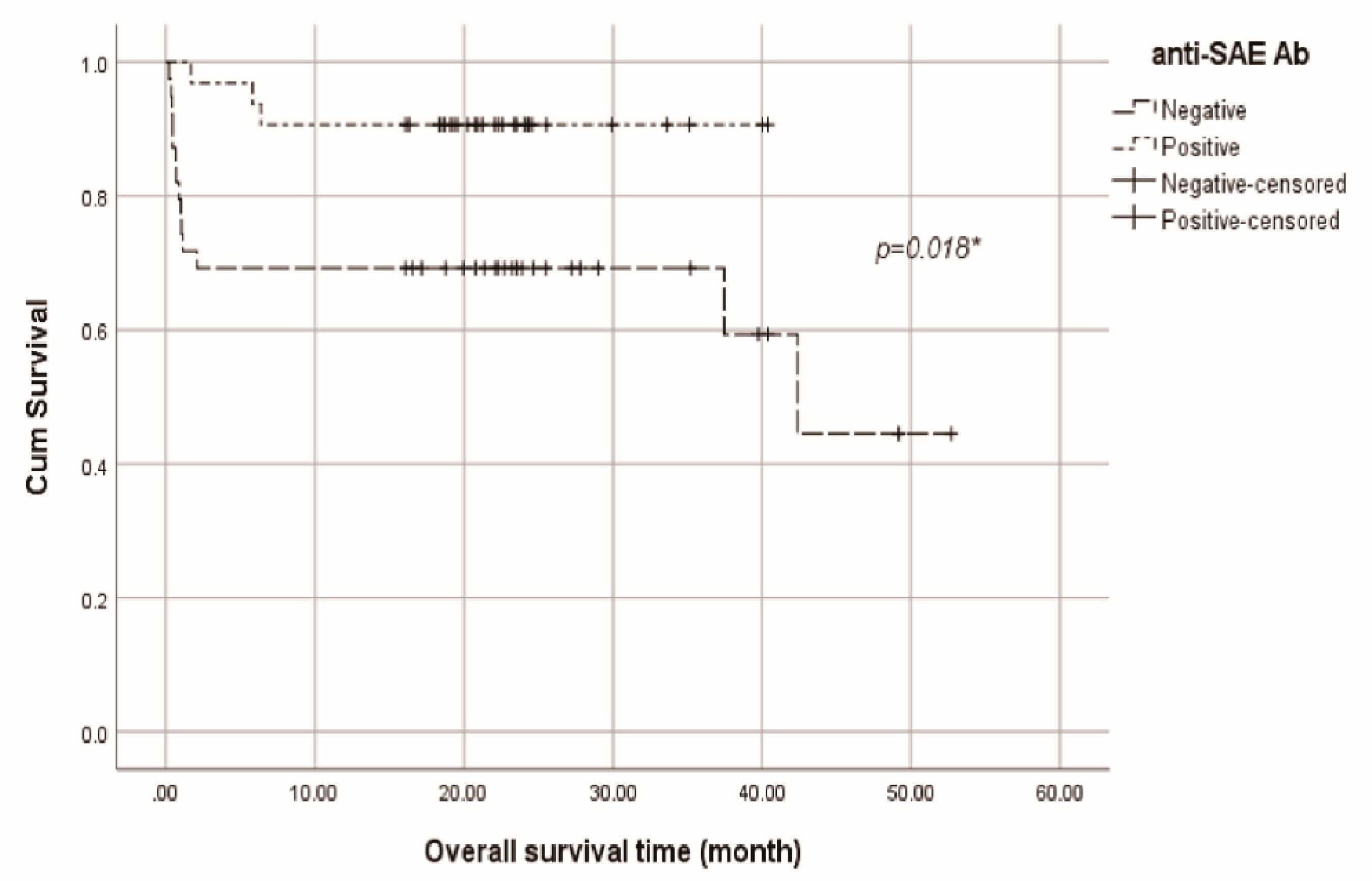
Figure 2.
Kaplan-Meier survival curve of anti-Ro52 Abs positive and negative patients.
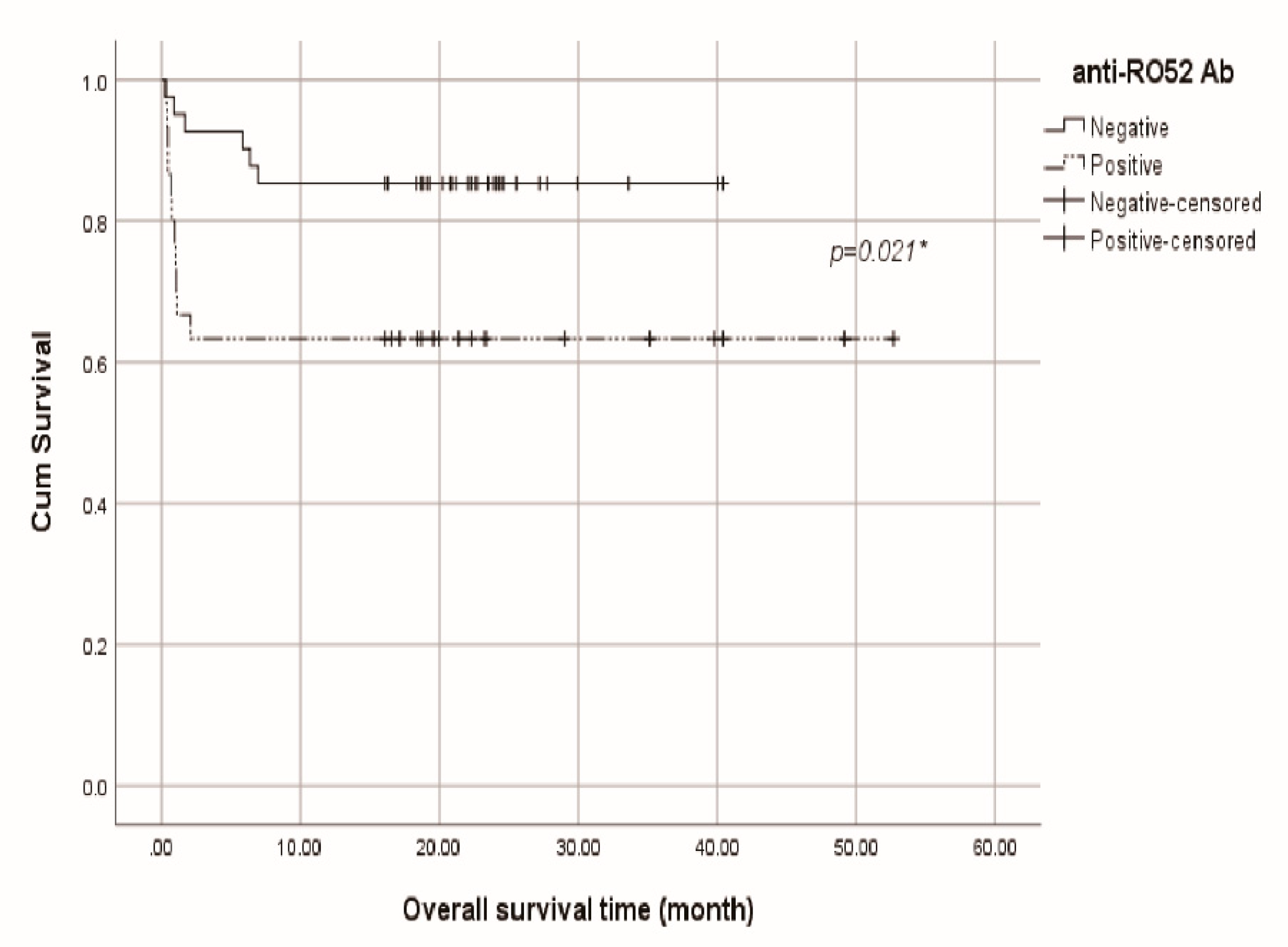
Figure 3.
Forest plot to show odds ratios for RPILD or non-RPILD.
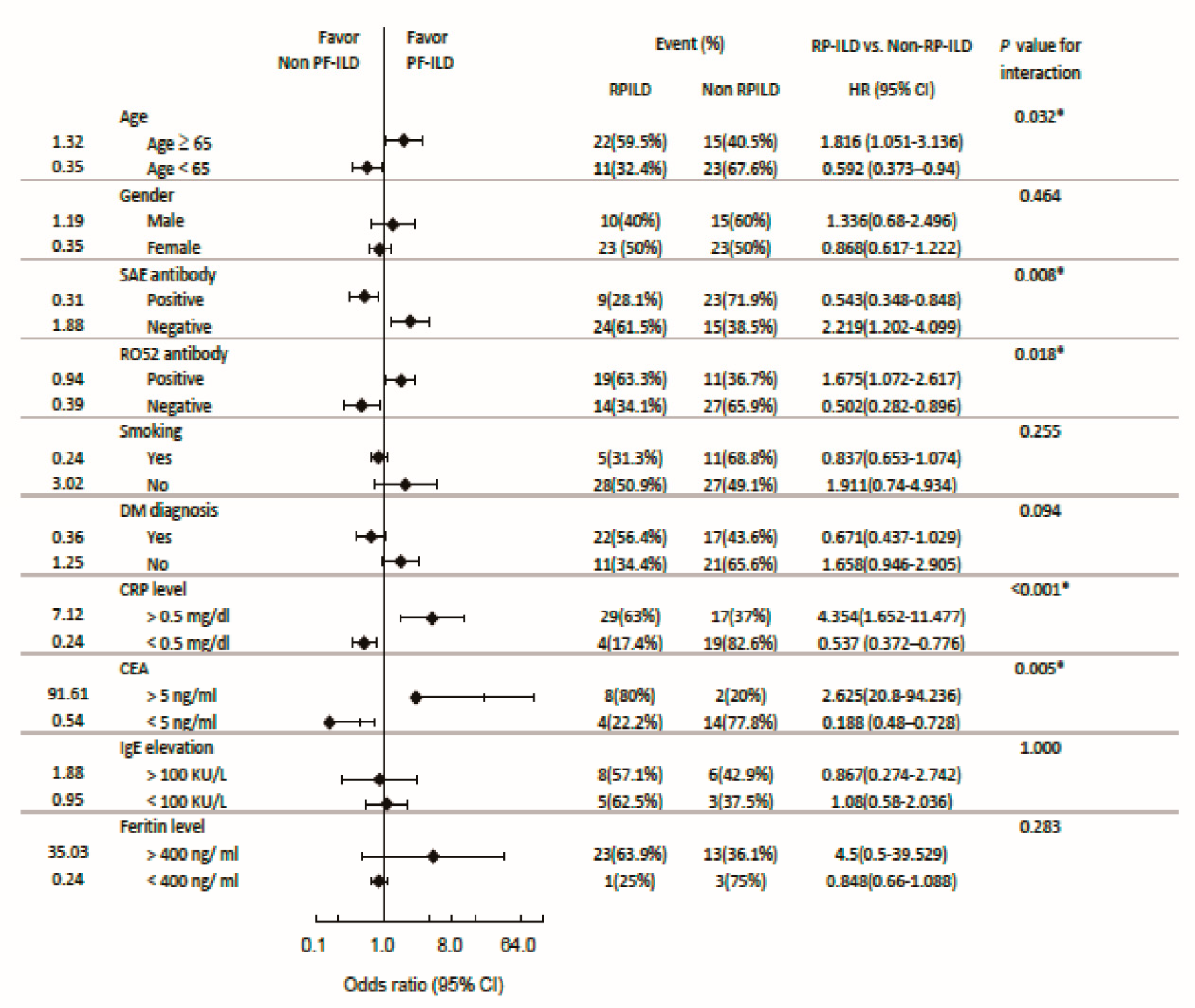
Figure 4.
Forest plot to show odds ratios for mortality in RPILD patients.
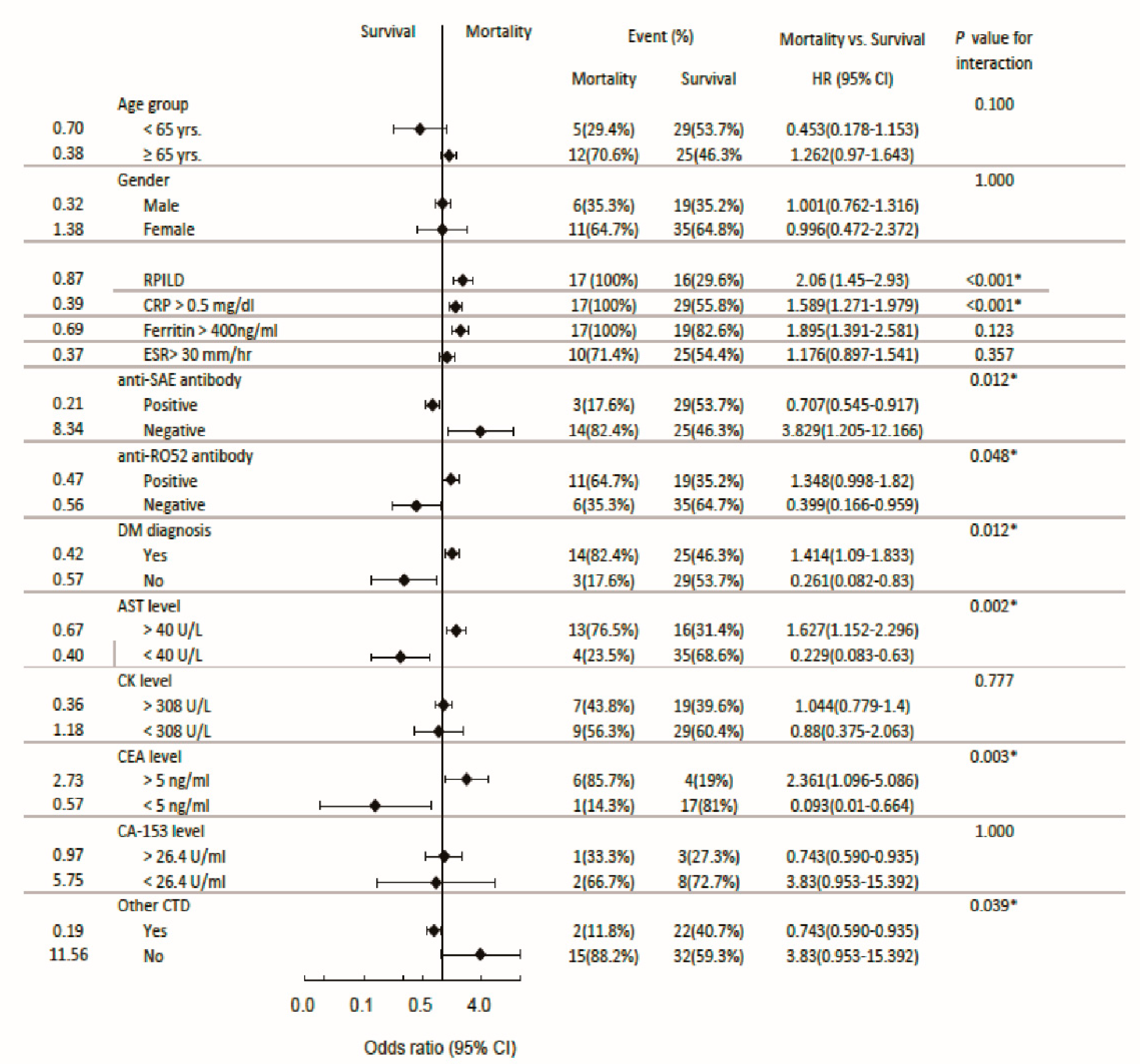
Table 1.
A. Baseline characteristics of 71 patients with anti-MDA5 antibodies.
| Total Patients (n=71) |
RPILD* (n=33) |
Non RPILD (n=38) |
Concurrent anti-SAE Abs (n=32) |
Concurrent anti-Ro52 Abs (n=30) |
Mortality (n=17) |
|
|---|---|---|---|---|---|---|
| Male (%) | 25 (35.2%) | 10 (30.3%) | 15(39.5%) | 14(43.8%) | 6(20%) | 6(35.3%) |
| Female (%) | 46 (64.8%) | 23 (69.7%) | 23(60.5%) | 18(56.3%) | 24(80%) | 11(64.7%) |
| Mean age (SD**) | 63.4 (13.9) | 65.5 (11.1) (p=0.239) |
61.6 (15.8) (p=0.238) |
64.5 (14.2) (p=0.546) |
60.9 (13.5) (p=0.192) |
67.1 (9.4) (p=0.21) |
| DM/PM (%) | 39 (55%) | 22 (56.4%) | 17 (43.6%) | 8 (25%) | 22 (73.3%) | 14 (82.4%) |
| AST (SD**) U/L |
79.8 (105.9) | 97.9 (126.5) | 63.6 (82.0) | 61.0 (89.5) (p=0.194) |
106.1 (132.5) (p=0.086) |
107.9 (82.8) (p=0.209) |
| LDH (SD**) U/L | 411.8 (179.7) | 427.5 (205.7) | 397.0 (152.9) | 360.8 (127.3) (p=0.043) |
448.1 (218.7) (p=0.139) |
508.3 (237.5)(p=0.009) |
| CK (SD**), U/L | 928.1 (2318.8) | 504.2 (847.4) | 1279.3 (3015.2) | 832.4 (2931.7) (P=0.926) |
959.3 (1732.9) (P=0.059) |
629.8 (1084.8)(P=0.234) |
| Myoglobulin (SD**), ng/ml | 574.5 (851.6) | 548.1 (819.1) | 606.8 (938. 9) | 157.6 (122.4) (p=0.11) |
582.4 (854.6) (p=0.968) |
448.3 (693.6) (p=0.602) |
| CRP (S.D.**) mg/dl | 4.17 (6.80) | 6.03 (8.18) | 2.46 (4.74) | 4.25 (6.18) (p=0.937) |
3.36 (6.56) (p=0.405) |
8.78 (8.97) (p=0.001) |
| ESR (S.D.**) mm/hr |
50.0 (35.9) | 56.2 (36.6) | 44.5 (34.9) | 47.5 (35.3) (p=0.634) |
50.4 (32.8) (p=0.94) |
61.3 (34.4)(p=0.18) |
| Albumin (S.D.**), g/dl | 3.32 (0.79) | 3.11 (0.82) | 3.56 (0.69) | 3.57 (0.84) (p=0.037) |
3.10 (0.74) (p=0.098) |
2.58 (0.43) (p=<0.001) |
| CA-153(S.D.**), U/ml |
19.9 (17.8) | 32.9 (18.8) | 10.1 (9.2) | 10.5 (10.5) (p=0.087) |
26.1 (7.8)(p=0.517) | 29.0 (12.8) (p=0.339) |
| CEA (S.D.**), ng/ml | 7.8 (7.4) | 12.5 (8.4) | 4.2 (3.9) | 6.9 (6.7) (p=0.569) |
11.0 (9.8) (p=0.239) |
15.2 (8.6) (p=0.001) |
| IgE (S.D.**), KU/L |
260.7 (306.8) | 310.9 (378.1) | 188.1 (150.3) | 298.1 (402.8) (p=0.58) |
155.1 (215.9) (p=0.335) |
392.0 (491.9) (p=0.176) |
| Ferritin (S.D.**) ng/ml | 1722.2 (1920.2) | 2449.8 (2152.8) | 630.8 (602.0) | 1063.3 (1338.1) (p=0.076) |
2245.4 (1982.7) (p=0.120) |
3178.2 (2147.4)(p<0.001) |
| Smoking (%) | 16 (22.5%) | 5 (15.2%) | 11 (28.9%) | 9 (56.3%) | 4 (25%) | 2 (11.8%) |
| Malignancy (%) | 15 (21.1%) | 11 (73.3%) | 4 (26.7%) | 5 (33.3%) | 2 (13.3%) | 6 (35.3%) |
| Other CTD*** (%) | 27 (38%) | 10 (41.7%) | 14 (58.3%) | 13 (54.2%) | 13 (54.2%) | 2 (11.8%) |
| Anti-SAE antibody (%) | 32 (45.1%) | 9 (28.1%) | 23 (71.9%) | 5 (15.6%) | 3 (17.6%) | |
| Anti-Ro52 antibody (%) | 30 (42.3%) | 19 (63.3%) | 11 (36.7%) | 5 (15.6%) | 11 (64.7%) | |
| Mortality (%) | 17 (23.9%) | 17 (100%) | 0 (0) | 3 (17.6%) | 11 (64.7%) |
The presence of Abs was detected by Euroimmun kit, SAE & Ro52 Abs being found to have the strongest negative or positive correlations with ILD. Abs other than anti-SAE or Ro52 were rarely encountered and so, were not shown in this table. All comparisons were made between the individual subgroups and the total patients (mother cohort, N=71) with p values < 0.05 as significant.*Rapidly Progressive interstitial lung disease. **S.D., standard deviation. ***CTD, connective tissue disease: RA, SLE, Sjögren, AIH, MCTD, SSc, AOSD, AS, IgG4-RD. Missing data: AST, LDH, myoglobulin, CRP, ESR, albumin, CA-153, CEA, IgE, Ferritin.. Normal ranges of albumin, ESR, CRP, AST, LDH, CA-153, CEA, IgE, myoglobulin and ferritin are listed in Methods.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



