
Submitted:
19 December 2023
Posted:
20 December 2023
You are already at the latest version
Abstract
Although lymphoma is the most frequent malignancy in common variable immunodeficiency (CVID), solid tumors, especially under influence of oncogenic viruses, are not considered. Furthermore, in vitro genetic studies and cell cultures are not adequate for immune system and HBV interaction.
We adopted previously introduced clinical model of host-virus interaction (i.e. infectious process in immunodeficiency) for analysis of B cells and specific IgG role (observational study of a CVID patient who received intravenous immunoglobulin (IVIG))
Suddenly, the patient deteriorated with positive result of HBs, HBV-DNA (369x106copies). In spite of lamivudine therapy and IVIG escalation (from 0.3 to 0.4g/kg), CT showed 11cm intrahepatic tumor (hepatocellular carcinoma). Anti-HBs had been positive in time-lapse analysis (range 111-220 IU/ml). Replacement therapy intensification was complicated by immune complex disease with renal failure.
The fulminant HCC in CVID and the development of the tumor as the first sign is interesting. Unfortunately, treatment with hepatitis B immune globulins (HBIG) plays a major role in posttransplant maintenance therapy. Anti-HBs substitution has not been proven to be effective, oncoprotective nor safe. Therefore, immunosuppression in HBV-infected recipients should be carefully minimized, patient selection more precise with the exclusion of HBV-positive donors. Our clinical model show HCC pathway with important humoral host factors, contrary to epidemiological/cohort studies highlighting risk factors only (e.g. chronic hepatitis). Lack of cell cooperation, B cell deficiency observed in CVID plays a crucial role in high HBV replication, especially in carcinogenesis.

Keywords:
IgG
; protective level
; vaccination
; B cell
; large granular lymphocytes (LGLs)
; common variable immunodeficiency (CVID)
; replacement therapy
; hepatitis B immune globulins (HBIG)
; serum sickness
; Hepatitis B virus (HBV)
; oncogenesis
; hepatocellular carcinoma
1. Introduction
Infections in humoral immunodeficiencies, including oncogenic viruses such as Hepatitis B virus (HBV), have a different clinical course. Much of the literature is devoted to the vaccination and coexistence of viral hepatitis and acquired immunodeficiency syndrome (AIDS) [[1]]. Little is known about HBV in posttransplant and primary immunodeficiency, especially common variable immunodeficiency (CVID). Although the last cohort shows abnormal liver function and thrombocytopenia in most of the CVID patients, there is no standardized monitoring strategy for these patients. Evidence of liver disease was considered in CVID patients with abnormal liver function tests that should be requested every 2-4 months, but there was no consensus on the frequency of abdominal ultrasound ([2]). The tumor markers are not considered. The serology profile is difficult for interpretation without HBV-DNA analysis ([3]). For example, sometimes immune and liver abnormalities are observed, as described in Walter’s et al report ([4]). Total bilirubin increase was observed, but screening test for HBV and HCV was negative. Although mortality associated with liver disease was observed in 63% and 7% patients (3/38) had HBV, the HBV patient’s history and therapeutic regimen are not analysed. The cohort within comorbidities requiring immunomodulation did not describe solid tumors and cancer complications, exclusively leukemia/lymphoma (2). Notably, severe immunosuppressive therapy was used, for example with rituximab (B-cell depletion) and anthracycline or alkylating agents, that have been associated with a potential risk secondary malignancies (2). Unfortunately, a most of hepatocellular carcinoma (HCC) cases is still diagnosed in an advanced stage, and this generally restricts the observational analysis of HBV-induced oncogenesis and efficacy of therapies and previous vaccination. Most studies on HCC-immunosurveillance are focused on T lymphocytes and microenvironment in advanced cancer ([5]). These studies show potential therapeutic targets, but have important limitation. Such studies and methods (clinical models) do not determine the cause, i.e. the initial stage of development of HCC, but indicate the immune factors responsible for the progression (not oncogenesis). (5).
Furthermore, it is a paradigm that to provide sustained immunodefense against virus replication, protective IgG must remain above a certain threshold level. Unfortunately, for most viral diseases, the protective titer is unknown ([6]). For HBV, it is mainly derived from epidemiological studies based on vaccinated (immunocompetent) populations and public health. It is not surprising that there is no uniform agreement about protective level of IgG against HBV surface antigen antibodies (anti-HBs).Following CDC, the patient is considered to be sensitive if the result is negative, i.e., <5 mIU/mL, >5.00 and <12.0 mIU/mL. - indeterminate and ≥12.0 mIU/mL - "positive" for anti-HBs and the patient is immunized ([7]). On the other hand, another CDC publication and the recommendations published previously by MMWR Recommendations and Reports indicate a much lower protection level - greater than or equal to 10mIU/ml ([8]). It was a long-held view in science and translational medicine that, although immunogenicity is lower among immunocompromised persons, those who achieve and maintain a protective antibody response before exposure to HBV have a high level of protection from infection ([9],[10]). Even when anti-HBs concentrations decline to <10 mIU/mL, nearly all vaccinated persons remain protected against HBV infection (7) through selective expansion of clones of antigen-specific B and T lymphocytes ([11]). Such a common belief has been accompanying doctors in transplantology for years (e.g. after recipient vaccination after HSCT), especially in the case of liver transplants in severe organ dysfunction, also due to HBV, regardless of the serostatus of the donor and the recipient’s therapy ([12]). Furthermore, hepatitis B immune globulin (HBIG) is considered sufficient defense against HBV, as it provides passive anti-HBs and temporary (i.e., 3–6 months) protection (7). Obviously, this cannot be a representation for immunodeficient patients and infants, who usually do not develop properly an immune response with long IgG half-life, and B cell memory, for example in β2-Microglobulin deficiency ([13]).The key issue is whether active or passive immunization is a sufficient protection against the genetic effects of HBV, and therefore HCC.
This time-lapse analysis of fast HBV infection and fulminant carcinogenesis in CVID, in spite of routine vaccination, and passive immunization with very high “protective” anti-HBs level. The observational study shed light on the crucial role of humoral compartment (beyond immunoglobulins) in HBV infection as well as low effectiveness and safety of specific IgG substitution in clinical immunology. The work expands the previous model of antibody deficiency (described for CMV) in assessing their role in anti-HBV adoptive immunity (6).
2. Results
2.1. Initial Diagnosis
The CVID diagnosis was confirmed according to ESID criteria. Initial immunoparameters were presented in Table 1.
2.2. Results of Time-Lapse Analysis
Antibody against HBV core antigen (anti-HBc total) was positive after IVIG therapy (3)(Table 1). Before subsequent substitutions, the level of IgG ranged 505-1055 mg/dl, anti-HBS 111-220 IU/ml, depending on different preparations and series of IVIG and patient compliance (3). The baseline IgG level stabilized under the influence of substitution every four weeks and the patient functioned well (stable period, Table 1 and Figure 1). During this period, systematic diagnostic imaging and biochemical tests were without deviations.
Suddenly and unexpectedly, the patient developed the following symptoms: muscle and joint pain, general weakness, lack of appetite, nausea and vomiting, and stomach pain. No jaundice was observed, and ALAT and bilirubin were normal. The family doctor recognized intestinal infection. The patient received symptomatic treatment and diet. Microbiological tests were negative, but pruritus occurred. At the follow-up visit prior to subsequent IVIG substitution, the patient reported discolored stool, pain in the right hypochondrium (Figure 1, September). HBs antigen before substitution was positive, but the liver function test results were all normal (ALT=33U/L, AST=30 U/L). The pre-emptive lamivudine therapy ([14]), time-lapse analysis of anti-HBs, HBsAg, complement C3 and C4 was introduced (Figure 1). He received 300 mg/d of lamivudine in divided doses. The HBV-DNA by polymerase chain reaction (PCR) were also examined. Real time PCR showed extreme level of viral load (61500000 IU/ml i.e. 369x106copies). Opportunistic viruses (e.g. cytomegalovirus, Epstein-Barr virus) were negative and HCV and HIV RNA were not detected. Due to a significant decrease in the IgG level before the next substitution, the dose of IVIG was escalated, although anti-HBs was still high (Figure 1). In spite of lamivudine therapy as well as lack of jaundice, rapid changes in mental status or unexplained bleeding, the ultrasound image showed heterogenous nodules (1.2-3cm see Figure 2a i.e. January).
The patient had progressive resistant thrombocytopenia (till 30-40x10^3/μl) and a coagulopathy (see below ). At this stage (February) the patient was not qualified for the surgery. Due to B cells <1%, there was no target for rituximab. IVIG dose was increased for the treatment of thrombocytopenia in CVID (2) (Figure 1). Further on, computer tomography showed a 11-cm, large intrahepatic tumor; afterwards, hepatocellular carcinoma and hepatic cirrhosis were confirmed by core needle biopsy. The first biopsy (January) was non-diagnostic and showed no significant abnormalities, the second (April) (in stage IIIA-IVB HCC) was representative.
In blood analysis, positive AFP, HBsAg with significant increase was observed (HbsAg fluctuation corresponded with further IVIG escalation)(Figure 1). Interestingly, total and specific IgG level decrease was observed. Subsequently the patient developed vasculitis (Gianotti-crosti vasculitis), intensified with further IVIG dose escalation, that corresponded with C4 decrease (Figure 1), mixed coagulopathy,severe serum sickness and acute renal failure (ARF). Therefore, the tomography was not performed. Complement C3 level was normal (data not shown).
2.3. Clinical Course of HCC and Outcome
Weight loss and significant deterioration (Eastern Cooperative Oncology Group (ECOG) status 4) were observed. Because of the patient’s condition, which included the risk of severe complications and immunodeficiency, he was disqualified from oncological therapy (e.g. immunotherapy with atezolizumab) by the Tumor Board ([15]). Finally, metastases and hepatic encephalopathy were observed with fatal outcome within one month after HCC confirmation and fast tumor progression observed in ultrasonography (Figure 2b).
3. Discussion
3.1. Efficacy: Anti-HBs is Not Protective per se
After the introduction of modern anti-HCV therapy, HBV-induced fulminant hepatitis and HCC are currently the most common causes of liver transplantation (LT). Patients with chronic HBV usually develop cirrhosis after several years of treatment-induced virological remission. Although the chronicity of HBV infection is attributed to inappropriate functioning of cell-mediated immunity, the humoral counterpart has not been analysed. Our recent study indicates (using the example of CMV, common cause viral hepatitis in immunodeficient patients) that transient hipogammaglobulinemia in infancy as well as secondary (posttransplant) humoral immunodeficiencies may be a good model for clinical trials, i.e., patient-centered vaccination and monitored therapy (5). Contrary to large-scale and statistically based studies based on a potential infection and statistically estimated risk, such two models show real protection against an existing infection (i.e. CMV). The absence of signs of infection in even a very large group of immunized subjects (as in clinical trials of vaccines) does not per se mean protection, because the actual exposure to the pathogen is unknown, only its certain probability. Accordingly, clinical and cohort studies on the effectiveness of specific hyperimmune immunoglobulins (HBIG) were conducted for a long time, their main shortcomings were short duration and the general assumption of a protective titer >100IU([16]). Unfortunately, the systematic metanalysis of 2162 HBV-positive patients treated with HBIG and nucleos(t)ide analogues (i.e. lamivudine and/or adefovir), showed recurrence in 6.6% of cases and HBIG protocol had no impact on HBV recurrence in patients receiving HBIG and ADV ([17]). A single study of the long-term effects of HBIG assessed time to first recurrence of hepatitis B virus (HBV)-hepatocellular carcinoma (HBV-HCC) in 14 patients (14/147, 9.5%) transplanted for HCC and who had HBV-HCC recurrence ([18]). However, from the initial group, as many as 39 patients with HCC did not survive to the end of the study due to HCC, and two due to an HBV-related complication. Furthermore, 27.5% of the donors were anti-HBs-positive, 20.1% were anti-HBc-positive, and, what is noteworthy, 1.4% were HBsAg-positive. Therefore, about 7.4% of donors were potentially HBV infectious. It corresponds with our current and previous observations of anti-HBc positive immunoglobulins that are received from extensive pool of blood donors (3). Unfortunately, in transplant practice from many years the HBV-positive (anti-HBs and anti-HBc total) donors are not disqualified. In spite of high anti-HBs levels among the 16 recipients receiving HBIG, one patient with residual anti-HBs titers below 50 UI/ml became HBsAg positive ([19]), as in the presented case (Figure 1). Expression of IgG receptors (e.g. CD16) and complement concentration (classical cascade such as C4) significantly influence the IgG efficacy(see section 3.2 and 3.3 below)
Unfortunately, in the literature, the incidence of de novo HCC in the cohort of HBV-positive transplant patients has not been studied so far (“reccurence” only). In fact, we do not know how many patients with HCC “recurrence” relapsed from extrahepatic foci and how many developed HCC de novo under the influence of HBV-mediated oncogenesis and post-transplant immunosuppression (see below). Our case with sudden-onset of oncogenesis (with fast tumor growth) and fulminant course indicates the latter scenario. It is the first signal for crucial B-cell role in HCC. Our observation is the first signal showing the role of mature B cells (in our patient in deep deficit –Table 1) in protection against HBV-induced oncogenesis, independently of the antibodies. Unlike CMV, as we showed previously (6), the presence of HBV-specific antibodies in high titers do not ensure remission nor viral clearance: HBV, unlike CMV, does not form a virome. HBV latency (presence of HBV in hepatocyte without typical cycle) is beyond IgG and may be harmful.
3.2. Specific IgG Substitution and Safety
Liver transplantation (LT) in HBV-positive recipient and especially in HBV-induced defect is the most controversial aspect of humoral protection and HBIG. The detectable HBV surface antigen level in spite of a concomitant increase of anti-HBs substitution indicates an overexpression of the HBV gene with very intensive HBs synthesis. It corresponded with immune-complex disease and significant classical complement cascade (Figure 1). Such a systemic reaction of antigen and antibodies, observed throughout the body, especially inside the vessels during substitution, was one of the elements of the deterioration of the patient's condition (serum sickness). On the other hand, the reaction of HBs with specific antibodies resulted in the limitation of further mechanisms of response to the active virus in the infectious focus: classical complement cascade. ARF following prophylactic intravenous administration of HBIG was observed in a patient who had undergone a liver transplant. Such a reaction was described almost exclusively as an adverse effect of preparations containing saccharose ([20]). What is noteworthy, immune-mediated mechanism was not analysed. On the contrary, intensive antigen-antibody reaction (Figure 1), liver and lymphatic system damage with impaired elimination of immune complexes seem to be an underestimated phenomenon, especially in patients after splenectomy or liver transplantation.The liver contains the majority of C4 transcripts throughout the body ([21]). Therefore, in hepatitis B and HBIG therapy, C4 seems to be a better and more universal signal of pathology than C3 and ALT level, which are normal in our case.
A more relevant model, especially for clinical immunology and transplantation, is maternal-fetal transmission, with or without a HBV-passive mother and combined child prophylaxis ([22]). In one study among 158 women, 143 (90.5%) received Hepatitis B immune globulin during pregnancy, and 86.0% of their children were given Hepatitis B immune globulin and Hepatitis B vaccine ([23]). Contrary to epidemiologic data, active or passive immunization was not effective. The intrauterine infection rate of newborns was 6.7%, five cases were HBsAg-positive by Umbilical Cord Blood detection and the chronic HBV rate of children was 4.0%. Interestingly, the relatively few intrauterine infections were identified in this sample, but many infants did not appear to seroconvert after vaccination. Moreover, in the original understanding, HBV pathology was associated with an immune reaction and not a cytopathic effect. And when immunity is distorted (as in our case), carcinogenesis begins to dominate.
3.3. Crucial Role of Lymphocyte Cooperation In Viral and Cancer Immunosurveillance
In immunocompetent patients, chronic inflammation precedes HBV-mediated oncogenesis. Recent studies have implicated T cells, especially Tc cells, but only in the HBV chronic process ([24]). Tc cell activation and IFNα2 secretion may be crucial in acute inflammation ([25]). However, since IFN-α2 was positively related to the frequency of CD8+ T lymphocytes in acute inflammation, the low level of these cells in our patient affected the innate immune response. On the contrary, viral clearance classically is monitored by serological conversion in patients infected with HBV (i.e. humoral and B-cell compartment). Viral clearance was difficult in our patient because it was associated with the HBV-specific adoptive immunity, damaged in CVID. The only indirect sign of a significant influence of B cells and humoral mechanisms on the fulminant course of HBV infection is the data from rituximab treatment, i.e. B-cell depletion therapy (14, [26]), which is overused in mild complications of CVID (2). Interestingly, using the EUROclass system ([27]), our patient was classified into the group with nearly absent B cells (less than 1%). Although coagulation disorder was present in 79% of patients with CVID-liver disease cohort, the immunosuppressive (B cell ablation therapy, cytostatics) was used for therapeutic regimen (2). Vaccination and a high level of anti-HBs do not protect such patients from fulminant disease, because the lymphatic system is overloaded with immune complexes, lymphoma (treated with rituximab) and the B-cells are eliminated for long time. Rituximab eliminates B cells (also B cell compartment in spleen and lymphatic system), causes antibody-dependent cell-mediated cytotoxicity (ADCC) with C4 complement consumption and prompt a fulminant process, also without lymphoma ([28]). From the perspective of our patient and CVID, cooperation of B cells in the follicles seems crucial, since HBV replication and HBsAg secretion proceeded extremely dynamically (Figure 1), despite the passively maintained anti-HBs (in "protective titer"). Last communication shows genetic and epigenetic mechanism and abnormal immunity, selected dysregulated interactions between B cells and the other immune cell compartments in the CVID ([29]). A similar danger is posed by LT associated with deep immunosuppression, with anti-thymocyte globulin or anti-IL-2 receptor antibody as well as calcineurin inhibitors, used in transplant procedure in 2.4%, 9.7 and 93.8% patients respectively (18).Lack of specific immunoglobulin, immune response under the influence of antigen stimulation and B cell in our patient is very suggestive (Table 1). Interestingly, also the FcγRIII (CD16) is underexpressed on lymphocytes (i.e. 5.2% -Table 1), particularly on large granular lymphocytes (LGLs) of both NK- and CD8-positive T-cell (i.e. 50.4 and about 17 cells/μl, respectively). Furthermore, this low expression may be a mechanism exacerbating HBV-related state of CD8CD103-positive lymphocyte exhaustion in HCC (5), therefore cause of fulminant course. As ADCC activation with IgG/FcγRIII activation in LGL was damaged, one of the crucial mechanisms of passive immunization and antiviral immunity in our patient was significantly low. As in the T cells, NK cells induce IFNγ and TNFα gene transcription and cytokine mRNA. Interestingly, in NK cells the signal is calcium-dependent and mediated by a cyclosporin A (CsA)-sensitive NFATp (the nuclear factor of activated T cells) ([30]). The reduction of CD16 under the influence of CsA in transplant practice may cause a similar defect as in our patient with CVID. Adequate cellular compartment with positive delayed-type hypersensitivity in Mantoux test, normal CD4 level was not compensatory for the humoral and LGL defect. This is one of the problems with immunotherapy, which is high risk for CVID patients with unknown benefits (abnormal immune response). The lack of cause eradication (viral clearance and HBV-oncogenesis) is significant in our case. Therefore, incorporation of HBV-DNA into the host's genome may initiate malignant transformation, even in the absence of chronic hepatitis or abnormal ALT. The viral genome incorporation and oncogenesis is beyond the action of IgG. Although the level of CD8 T cells was reduced by about half to normal (i.e. 128 cells/μl), LGL T cells were significantly deficient among these cells, i.e., 17 cells/μl (data not shown). Thus, the observed changes in CVID gave a specific niche for the abundant multiplication of the virus and fulminant oncogenesis. HBx oncoprotein in complex humoral disorders, the lymphatic system overload with immune complexes, caused HCC in many mechanisms in an uncontrolled manner with fast growth (Figure 1) ([31]). Both the proliferation associated with cyclins, MAPK, JAK/STAT3.5, PI3K/NFkB signaling pathways and the disruption of apoptosis (p53), regardless of the increase in viral infectivity, are intermediate are associated with intensive oncogenesis and death without cirrhosis in the observed case ([32]).
Cellular (hepatocyte) transplantation may be a much safer option than non-selective harvest donors ([33]). So far, despite the wealth of literature, oncological research has been focused on genetic issues or T cell compartment estimation in immunotherapy. The role of B cell immunosurveillance against oncogenic viruses is underestimated, especially against HBV in CVID(2,5). What is noteworthy is that the TNF gene family (e.g. transmembrane activator and calcium modulator and cyclophilin ligand interactor (TACI) is a crucial regulator of B cell receptor activation and such mutation is frequently identified in CVID patients ([34]). However, the earliest effect of TNF discovered was to inhibit tumor growth. Interestingly, lymphoma is most frequently diagnosed in CVID, but solid tumors, especially under influence of oncogenic viruses, are not considered, patients usually receive B-cell depletion therapy (2,35). Although CVID patients with liver disease most frequently presented with abnormal liver function test and abnormal abdominal ultrasound (68%) (2), in the initial stage of HCC, nodular changes are similar to nodular regenerative hyperplasia (Figure 2a), treated with rituximab (2). Lymphoproliferative disease development in patients with primary immunodeficiency requires a different investigative approach to immunotherapy ([35]). Our observation showing other humoral elements, including ADCC, LGL and the complement cascade, is a good introduction to further observations and change of existing immunotransplantation practice. Humoral immunity and complex of B cell interaction cannot be replaced by passive immunization and the administration of specific immunoglobulins ([36]). Normal aminotransferase levels as a satisfied results together with lack of agreement on frequent imaging and HBV testing as well as tumor markers overlooking constitute a significant gap in the oncosurveillance against HCC in immunodeficiency (2). Our case demonstrates the need for fast surgical interventions and targeted biopsies.
4. Materials and Methods
4.1. Material: Case Presentation
A 28-year-old, HBV-negative patient with common variable immunodeficiency (B-type) was qualified for intravenous IgG (IVIG) replacement therapy according to ESID criteria (2). The patient was not treated surgically and had not received any cosmetic procedures (including tattoos). He had no history of blood transfusion, alcohol consumption, nor injectable drug use. He used dental treatment only. In addition, he was vaccinated against HBV at birth and received a booster dose every 5 years. Initial immunoparameters are presented (Table 1). During the initial screening, the patient was anti-HBs, HBc total, HBsAg, HBV-DNA, HCV and HIV-negative. Liver function tests, basic tumor markers (i.e. CEA, AFP, beta2-microglobulin) were normal. Checkup CT before IVIG starting (chest and abdominal) showed no abnormalities in the liver. No nodular lesions were observed in either the lungs or liver, i.e., sign of granulomatous-lymphocytic interstitial lung disease and nodular regenerative hyperplasia. The patient gave written informed consent for this publication.
4.2. Methods
Regular (every 4 weeks) IgG replacement therapy was carried out with intravenous preparations at a dose of 0.3g IVIG per kilogram of weight. The kinetics of real saturation was tested: serum IgG levels were determined (turbidimetry, Olympus) immediately prior to each infusion. Median IgG level was presented (Figure 1). Serum IgG and anti-HBs level significantly increased after immunoglobulin supplementation. Anti-HBs titer increased and was always over 100 IU/L (range 111-220 IU/ml) with median level 210 IU/l as presented in stable disease period (Figure 1). Routinely, he had a chest X-ray and abdominal ultrasound performed every 3-6 months and a chest CT every 12 months. Serum alanine aminotransferase (ALT) and bilirubine were tested every 3 substitutions.
5. Conclusions
Our case report is the first clinical signal for the low efficacy of IVIG/HBIG and the lack of “protection” with high anti-HBs level, with the key question of safety. Serum sickness, too rarely diagnosed in the clinical background, is a key complication of IVIG/HBIG overuse, and a clear decrease of C4 (consumption or liver production) with AFP indicates a greater usefulness of these parameters than ALT. HBV-DNA (CVID patients receive frequent immunoglobulin injections), tumor markers and regular imaging (at short intervals) should be a daily practice in clinical immunology, especially in patients on B cell depletion therapy or with hepatic involvement. Our observation indicates one more key aspect. Even properly performed vaccination does not provide protection against HBV (e.g. by cellular mechanisms postulated in the publications mentioned above (11)), if the patient has a deficiency of B cells (e.g. in TNF mutation), which are the primary antigen-presenting cells. HBV infection, as one of the strongest carcinogens, is one of the greatest challenges in immunological practice, in both primary and secondary (after rituximab) B-cell deficiencies. Apart from B cell deficiency, abnormal lymphocyte cooperation in CVID, and the low CD8 level observed in this study, expression of CD16 on LGL and ADCC are the second reason for atypical presentation with fulminant HBV-induced carcinogenesis. HBV-induced HCC in primary immunodeficiency is a very interesting and promising model for further research, but cancer development in such patients requires a different clinical and investigative approach to immunotherapy (36).
Author Contributions
PZ was responsible for the clinical diagnosis and patient management. PZ and AG analyzed the data. AG contributed reagents/materials/analysis tools. PZ wrote the manuscript. AG reviewed manuscript and editing. All authors read and approved the final manuscript.
Funding
This work was supported by private funds of the first author, from the statutory activity of Hirszfeld Institute.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
All data generated or analyzed during this study are included in this article.
Acknowledgments
We would like to express our gratitude to MSc Edyta Kocwin and Dorota Dlubek Ph.D. for the laboratory and cytometric analysis. Many thanks to J. Grycewicz for help in proofreading.
Conflicts of Interest
The authors declare no competing interests (i.e. research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest).
References
- onseca MO, Pang LW, de Paula Cavalheiro N, Barone AA, Heloisa Lopes M. Randomized trial of recombinant hepatitis B vaccine in HIV-infected adult patients comparing a standard dose to a double dose. Vaccine 2005, 23, 2902–2908. [CrossRef]
- Daza-Cajigal, V.; Segura-Guerrero, M.; López-Cueto, M.; Robles-Marhuenda. ; Camara, C.; Gerra-Galán, T.; Gómez-De-La-Torre, R.; Avendaño-Monje, C.L.; Sánchez-Ramón, S.; Bosque-Lopez, M.J.; et al. Clinical manifestations and approach to the management of patients with common variable immunodeficiency and liver disease. Front. Immunol. 2023, 14, 1197361. [Google Scholar] [CrossRef] [PubMed]
- Zdziarski, P.; Gamian, A.; Majda, J.; Korzeniowska-Kowal, A. Passive blood anaphylaxis: subcutaneous immunoglobulins are a cause of ongoing passive anaphylactic reaction. Allergy, Asthma Clin. Immunol. 2017, 13, 41. [Google Scholar] [CrossRef] [PubMed]
- Walter, J.E.; Armanios, M.; Shah, U.; Friedmann, A.M.; Spitzer, T.; Sharatz, S.M.; Hagen, C. Case 41-2015. New Engl. J. Med. 2015, 373, 2664–2676. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, G.E.M.; Cabibbo, G.; Craxì, A. Hepatitis B Virus-Associated Hepatocellular Carcinoma. Viruses 2022, 14, 986. [Google Scholar] [CrossRef] [PubMed]
- Zdziarski, P. CMV-Specific Immune Response—New Patients, New Insight: Central Role of Specific IgG during Infancy and Long-Lasting Immune Deficiency after Allogenic Stem Cell Transplantation. Int. J. Mol. Sci. 2019, 20, 271. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control And Prevention (CDC). Updated Healthcare Infection Prevention and Control Recommendations in Response to COVID-19 Vaccination. 2021. Available online: http://www.cdc.gov (accessed on).
- ast EE, Weinbaum CM, Fiore AE, Alter MJ, Bell BP, Finelli L, Rodewald LE, Douglas JM Jr, Janssen RS, Ward JW; Advisory Committee on Immunization Practices (ACIP) Centers for Disease Control and Prevention (CDC). A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP) Part II: immunization of adults. MMWR Recomm Rep. 2006 Dec 8;55(RR-16):1-33; https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5516a1. 2023.
- tevens CE, Toy PT, Taylor PE, Lee T, Yip HY. Prospects for control of hepatitis B virus infection: implications of childhood vaccination and long-term protection. Pediatrics 1992;90(1 Pt 2):170–3.
- adler SC, Coleman PJ, O'Malley P, Judson FN, Altman N. Evaluation of long-term protection by hepatitis B vaccine for seven to nine years in homosexual men. In: Hollinger FB, Lemon SM, Margolis H, eds. Viral hepatitis and liver disease: proceedings of the 1990 International Symposium on Viral Hepatitis and Liver Disease. Baltimore, MD: Williams & Wilkins; 1991:776–8.
- anatvala JE, Van Damme P. Hepatitis B vaccine–-do we need boosters? J Viral Hepat 2003;10:1–6.
- Hwang, S.; Moon, D.-B.; Lee, S.-G.; Park, K.-M.; Kim, K.-H.; Ahn, C.-S.; Lee, Y.-J.; Chu, C.-W.; Yang, H.-S.; Cho, S.-H.; et al. Safety of anti-hepatitis B core antibody-positive donors for living-donor liver transplantation. Transplantation 2003, 75, S45–S48. [Google Scholar] [CrossRef]
- Ardeniz. ; Unger, S.; Onay, H.; Ammann, S.; Keck, C.; Cianga, C.; Gerçeker, B.; Martin, B.; Fuchs, I.; Salzer, U.; et al. β2-Microglobulin deficiency causes a complex immunodeficiency of the innate and adaptive immune system. J. Allergy Clin. Immunol. 2015, 136, 392–401. [Google Scholar] [CrossRef]
- Giordano, C.; Picardi, M.; Pugliese, N.; Vincenzi, A.; Abagnale, D.P.; De Fazio, L.; Giannattasio, M.L.; Fatigati, C.; Ciriello, M.; Salemme, A.; et al. Lamivudine 24-month-long prophylaxis is a safe and efficient choice for the prevention of hepatitis B virus reactivation in HBsAg-negative/HBcAb-positive patients with advanced DLBCL undergoing upfront R-CHOP-21. Front. Oncol. 2023, 13, 1130899. [Google Scholar] [CrossRef]
- dziarski, P. Importance of the Tumor Boards' decisions for the patientcentered care - case studies in the COVID-19 era. Pol Merkur Lekarski. 2022 Apr 19;50(296):78-85.
- Mas, A.; Castells, L.; Abradelo, M.; Bernardos. ; Páez, A.; Woodward, M.; Sousa, J. Evaluation of Anti-HBs Serum Levels and Pharmacokinetic Profile After Intravenous Administration of Niuliva, a New Hepatitis B Immunoglobulin, Following Liver Transplantation. Transplant. Proc. 2009, 41, 4253–4258. [Google Scholar] [CrossRef]
- Cholongitas, E.; Goulis, J.; Akriviadis, E.; Papatheodoridis, G.V. Hepatitis B immunoglobulin and/or nucleos(t)ide analogues for prophylaxis against hepatitis b virus recurrence after liver transplantation: A systematic review. Liver Transplant. 2011, 17, 1176–1190. [Google Scholar] [CrossRef] [PubMed]
- Beckebaum, S.; Herzer, K.; Bauhofer, A.; Gelson, W.; De Simone, P.; de Man, R.; Engelmann, C.; Müllhaupt, B.; Vionnet, J.; Salizzoni, M.; et al. Recurrence of Hepatitis B Infection in Liver Transplant Patients Receiving Long-Term Hepatitis B Immunoglobulin Prophylaxis. Ann. Transplant. 2018, 23, 789–801. [Google Scholar] [CrossRef] [PubMed]
- Roque-Afonso, A.M.; Feray, C.; Samuel, D.; Simoneau, D.; Roche, B.; Emile, J.-F.; Gigou, M.; Shouval, D.; Dussaix, E. Antibodies to hepatitis B surface antigen prevent viral reactivation in recipients of liver grafts from anti-HBC positive donors. Gut 2002, 50, 95–99. [Google Scholar] [CrossRef] [PubMed]
- onataccio M, Dalle Ore G, Donataccio D. Acute renal failure following intravenous administration of hepatitis B im-munoglobulin in liver transplantation. Minerva Gastroenterol Dietol. 5: 2009 Dec;55(4), 2009.
- A Blanchong, C.; Chung, E.K.; Rupert, K.L.; Yang, Y.; Yang, Z.; Zhou, B.; Moulds, J.M.; Yu, C. Genetic, structural and functional diversities of human complement components C4A and C4B and their mouse homologues, Slp and C4. Int. Immunopharmacol. 2001, 1, 365–392. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Song, A.; Lin, X.; Lu, J.; Zheng, S.; Ma, L.; Ren, S.; Zheng, Y.; Chen, X. Clinical characteristics of hepatitis flares during pregnancy and postpartum in Chinese chronic hepatitis B virus carriers—a prospective cohort study of 417 cases. Front. Immunol. 2022, 13, 1031291. [Google Scholar] [CrossRef] [PubMed]
- uo Y, Liu J, Meng L, Meina H, Du Y. Survey of HBsAg-positive pregnant women and their infants regarding measures to prevent maternal-infantile transmission.BMC Infect Dis. 2010 Feb 15;10:26.
- Mukherjee, R.M.; level, R.b.s.H.; Reddy, P.B.; Arava, J.; Rao, P.; Mitnala, S.; Gupta, R.; Reddy, D. Relationship between serum HBsAg level, HBV DNA level, and peripheral immune cells in patients with chronic hepatitis B virus infection. Hepatic Med. Évid. Res. 2010, 2, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.; Yang, L.; Bi, X.; Deng, W.; Jiang, T.; Lin, Y.; Wang, S.; Zhang, L.; Liu, R.; Chang, M.; et al. Cytokine profiles and CD8+ T cells in the occurrence of acute and chronic hepatitis B. Front. Immunol. 2022, 13. [Google Scholar] [CrossRef]
- Guo, X.; Ji, T.; Xin, S.; Xu, J.; Yu, Y. A case report of hepatitis B virus reactivation 19 months after cessation of chemotherapy with rituximab. Front. Immunol. 2022, 13, 1083862. [Google Scholar] [CrossRef] [PubMed]
- Wehr, C.; Kivioja, T.; Schmitt, C.; Ferry, B.; Witte, T.; Eren, E.; Vlkova, M.; Hernandez, M.; Detkova, D.; Bos, P.R.; et al. The EUROclass trial: defining subgroups in common variable immunodeficiency. Blood 2008, 111, 77–85. [Google Scholar] [CrossRef]
- Buonomo, A.R.; Viceconte, G.; Scotto, R.; De Angelis, M.; Tozza, S.; Manganelli, F.; Lanza, A.G.; Di Costanzo, G.G.; Gentile, I. Seronegative occult HBV reactivation complicated with fulminant acute liver failure after rituximab for chronic inflammatory demyelinating polyneuropathy. Infect. Dis. 2019, 52, 216–218. [Google Scholar] [CrossRef]
- Rodríguez-Ubreva, J.; Arutyunyan, A.; Bonder, M.J.; Del Pino-Molina, L.; Clark, S.J.; de la Calle-Fabregat, C.; Garcia-Alonso, L.; Handfield, L.-F.; Ciudad, L.; Andrés-León, E.; et al. Single-cell Atlas of common variable immunodeficiency shows germinal center-associated epigenetic dysregulation in B-cell responses. Nat. Commun. 2022, 13, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Aramburu, J.; Azzoni, L.; Rao, A.; Perussia, B. Activation and expression of the nuclear factors of activated T cells, NFATp and NFATc, in human natural killer cells: regulation upon CD16 ligand binding. J. Exp. Med. 1995, 182, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Lupberger, J.; Hildt, E. Hepatitis B virus-induced oncogenesis. World J. Gastroenterol. 2007, 13, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Levrero, M.; Zucman-Rossi, J. Mechanisms of HBV-induced hepatocellular carcinoma. J. Hepatol. 2016, 64, S84–S101. [Google Scholar] [CrossRef] [PubMed]
- dziarski, P. Cellular transplantation–orthotopic liver transplantation alternative. Pol Merkur Lekarski. 2007 Oct;23(136):297-301.
- Roosens, W.; Staels, F.; Van Loo, S.; Humblet-Baron, S.; Meyts, I.; De Samblanx, H.; Verslype, C.; van Malenstein, H.; van der Merwe, S.; Laleman, W.; et al. Rituximab and improved nodular regenerative hyperplasia-associated non-cirrhotic liver disease in common variable immunodeficiency: a case report and literature study. Front. Immunol. 2023, 14, 1264482. [Google Scholar] [CrossRef]
- Zdziarski, P.; Gamian, A. Lymphoid Interstitial Pneumonia in Common Variable Immune Deficiency – Case Report With Disease Monitoring in Various Therapeutic Options: Pleiotropic Effects of Rituximab Regimens. Front. Pharmacol. 2019, 9, 1559. [Google Scholar] [CrossRef]
- Matson, E.M.; Abyazi, M.L.; Bell, K.A.; Hayes, K.M.; Maglione, P.J. B Cell Dysregulation in Common Variable Immunodeficiency Interstitial Lung Disease. Front. Immunol. 2021, 11. [Google Scholar] [CrossRef]
Figure 1.
Severe and fatal HBV infectious process in CVID patient with IVIG therapy. Time-line shows HBV-induced hepatocellular carcinoma, serum sickness (with vasculitis and renal failure) development in spite of “protective” anti-HBS level (yellow line). Very fast tumor growth corresponded with alfa fetoprotein (AFP) level. This indicates that the cancer process began around November (extrapolation based on available ultrasound data -dashed red line). The point corresponded with start of significant decrease of specific anti-HBs (to 185 mg/dl) within the period (September –November). The fall in the pound exacerbated in spite of IVIG dose escalation.
Figure 1.
Severe and fatal HBV infectious process in CVID patient with IVIG therapy. Time-line shows HBV-induced hepatocellular carcinoma, serum sickness (with vasculitis and renal failure) development in spite of “protective” anti-HBS level (yellow line). Very fast tumor growth corresponded with alfa fetoprotein (AFP) level. This indicates that the cancer process began around November (extrapolation based on available ultrasound data -dashed red line). The point corresponded with start of significant decrease of specific anti-HBs (to 185 mg/dl) within the period (September –November). The fall in the pound exacerbated in spite of IVIG dose escalation.
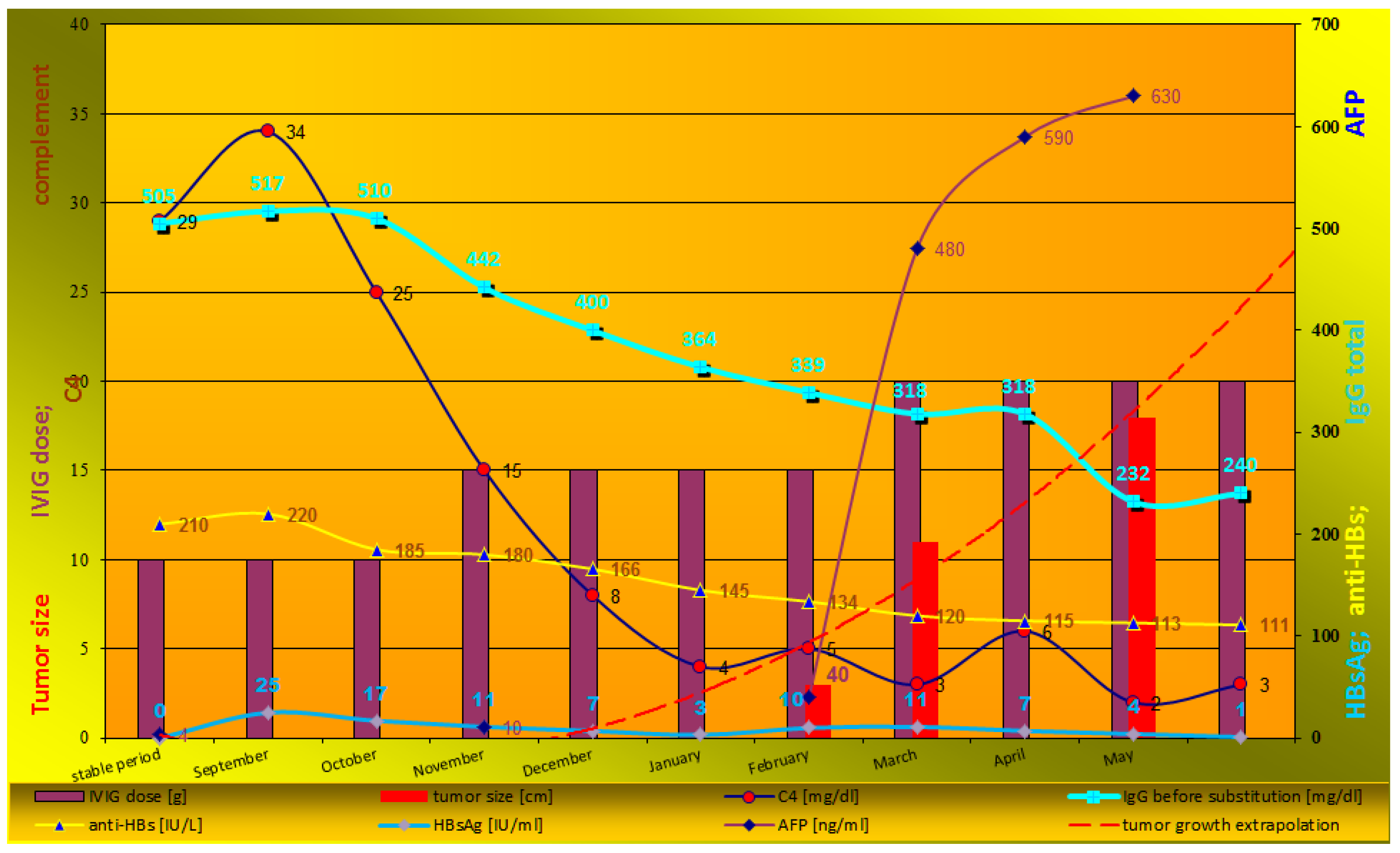
Figure 2.
Fulminant hepatocellular carcinoma HCC progression in patient with immunodeficiency. Regularly (every 3 months) performed ultrasound examinations did not show any changes in October, but ultrasound image showed heterogenous nodules (January, 2a) that resemble nodular regenerative hyperplasia, typical for CVID (2). First blind liver biopsy (January) was non-diagnostic. Afterwards, a 110-mm tumor developed and HCC was confirmed by second biopsy (April). Finally, fulminant growth till 180mm was observed despite lamivudine therapy, vaccination, normal ALT, and high anti-HBs level (2b).
Figure 2.
Fulminant hepatocellular carcinoma HCC progression in patient with immunodeficiency. Regularly (every 3 months) performed ultrasound examinations did not show any changes in October, but ultrasound image showed heterogenous nodules (January, 2a) that resemble nodular regenerative hyperplasia, typical for CVID (2). First blind liver biopsy (January) was non-diagnostic. Afterwards, a 110-mm tumor developed and HCC was confirmed by second biopsy (April). Finally, fulminant growth till 180mm was observed despite lamivudine therapy, vaccination, normal ALT, and high anti-HBs level (2b).


Table 1.
Basic immunoparameters and peripheral lymphocyte profile.
| %lymphocytes | Cells/μl | Normal Range | |
|---|---|---|---|
| CD3 | 54.4 | 706.6 | 700-2100 |
| CD4 | 42.7 | 555.5 | 300-1400 |
| CD8 | 9.9 | 128.7 | 200-900 |
| CD27+CD8+ | 7.9 | 102.2 | |
| CD27+CD4+ | 40.2 | 522.1 | |
| CD27+CD8+CD45 RO+ | 2.2 | 29.0 | |
| CD27+CD8+CD45 RO- | 5.6 | 73.2 | |
| CD27+CD4+CD45 RO+ | 14.2 | 184.7 | |
| CD27+CD4+CD45 RO- | 26.0 | 337.4 | |
| CD16 | 5.2 | 67.5 | |
| CD56+CD3+ | 1.0 | 12.5 | 250-320 |
| CD56+CD16+ | 3.9 | 50.4 | 90-600 |
| CD19 | 0.9 | 11.2 | 100-500 |
| CD27+CD19+ | 0.7 | 9.1 | |
| IVIG replacement therapy | initial phase | stable period | Normal Range |
| IgG [mg/dl] | 80 | 505-1055 | 700-1600 |
| IgA [mg/dl] | <5 | NT | 70-150 |
| IgM [mg/dl] | < 10 | NT | 40-230 |
| Anti-HBs | <5* | 111-220 | NA |
| Anti HBc total | Negative | Positive** | Negative |
| β2m (mg/L) | 0.98 | 0.9-1.7 | 0.8-2.2 |
| C4 [mg/dl] | 38 | 29 | 10-40 |
* anti-HBs as well as other vaccine-induced IgG are not observed. Memory B cell and plasma cells in bone marrow were not detected. ** False positive, under influence of passive transfer from IVIG (3).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



