
Submitted:
19 December 2023
Posted:
20 December 2023
You are already at the latest version
Abstract
We investigated and quantified bacterial accumulation in facemasks used by the general population, using 16S rRNA (Sanger Sequencing), culture and biochemical analysis along with Rose Bengal staining. Additionally, a systematic overview of the literature on face mask contamination was undertaken. We found an average bacterial load of 4.24 × 104 CFU recovered/mask, with a maximum load of 2.85 × 105 CFU. This maximum is 310 times higher than the limit value for contamination of ventilation system outlet surfaces specified by the German standard VDI 6022. Biochemical and molecular identification predominantly found Staphylococcus species (80%), including Staphylococcus aureus, along with endospore-forming Bacillus spp. Literature reports also indicate contamination of masks by bacterial and fungal opportunists of the genera Acinetobacter, Aspergillus, Alternaria, Bacillus, Cadosporium, Candida, Escherichia, Enterobacter, Enterococcus, Klebsiella (including K. pneumoniae), Micrococcus, Microsporum, Mucor, Pseudomonas, Staphylococcus and Streptococcus. Bacterial counts increase linearly with wearing duration, and prolonged use may affect the skin and respiratory microbiomes, promoting consequential eye, skin, oral and airway conditions. These aspects underscore the urgent need for further research and a risk-benefit analysis in respect of mask use, particularly given their unproven efficacy in disrupting the transmission of respiratory viruses and their adverse social consequences.
Keywords:
16S rRNA gene amplicon sequencing
; adverse effects
; bacterial contamination
; fluorescent staining
; masks
; N95
; personal protective equipment
; risk
; surgical mask
1. Introduction
Facemasks covering the entrances to the airways were widely mandated during the recent SARS-CoV-2 pandemic, not only for healthcare workers but also for the general population [1]. Professions with frequent human contact were obligated to wear them for long periods as were schoolchildren [1,2,3,4,5,6].
This raises reasonable concerns: first, because use by the general population is associated with a higher risk of improper handling of the mask [7,8,9,10,11]; secondly because their efficacy against respiratory viral infections is unproven by high quality trials, which indicate little or no effect [12,13,14] and thirdly, because masks are assumed only to have positive effects [15,16,17]. In reality there is strong evidence that masks pose various risks, especially for pregnant women, children and adolescents, as well as older adults and the unwell [15,17,18,19,20]. They have several demonstrably adverse effects, affecting physiology [15,17,20,21,22,23,24], psychology [17,25] and, most obviously, social interactions [26,27,28,29,30,31,32,33,34,35,36]. Effects on childhood development are a particular concern. These adverse effects have been recently summarised as the so-called mask-induced exhaustion syndrome MIES [15,17,20]. Interestingly, Spira [37] and Fögen [38] found significantly higher SARS-CoV-2 infection and mortality rates in the mask-wearing cohorts: explanations are uncertain, but viral trapping and recycling are plausible.
A further concern, not encompassed within MIES, relates to the potential adverse microbiological consequences of wearing face masks. Owing to the creation of a warm, moist micro-environment [39,40,41,42], bacteria, fungi and even viruses may accumulate on both sides of the worn masks [43,44,45,46,47]. So far, these aspects have not been evaluated in depth. Accordingly, we undertook a microbiological exploration of face masks as used by members of the general population, together with a systematic rapid literature review.
2. Materials and methods
Rose Bengal staining and visualisation of contamination
Microbiological mask study design
Surgical face masks were collected in March 2022 from 15 random willing volunteers (employees of the Gdansk University Department), who had worn them for periods from 15 min to 12 h. Wearer details were not further recorded. Each mask was stored in a separate plastic bag until examination. The masks, excluding the ear loops, were then aseptically cut in several pieces using sterile scissors in a laminar flow cabinet. These pieces were transferred to tubes containing 15 ml of sterile phosphate-buffered saline (PBS), equilibrated for 1 min at room temperature, then vortexed for 30 s. Three unused, clean, surgical masks (Shandong KaiBo Medicinal Packaging Co., Ltd, China) were processed identically as negative controls.
To determine bacterial counts, the suspensions were diluted 10- and 100-fold, then 100-µl volumes were spread on Columbia Agar containing 5% sheep blood (Graso Biotech, Owidz, Poland). Plates were incubated aerobically overnight at 37°C, then colonies were counted. The bacterial load was determined as colony forming units per ml (CFU/ml) of suspension, then rebased as CFU/mask [39]. Ten colonies per worn mask were re-plated, grown on Tryptic Soy Broth (Graso Biotech, Owidz, Poland), then stored in 15% glycerol stock solutions (v/v) at –70 °C pending molecular identification.
Identification of isolates by Sanger Sequencing of the 16S rRNA gene
Forty isolates were identified by PCR and Sanger sequencing of the 16S rRNA gene. Briefly, bacterial colonies were suspended in 30 µl of sterile water and lysed in 95°C, followed by centrifugation at 13 000 × g for 2 min. The supernates were used for PCR. Primers were: forward F27 5’-AGAGTTTGATCMTGGCTCAG-3’ and reverse R1492 5’- TACGGYTACCTTGTTACGACTT-3’. The reaction mixture (25 µl) contained: 0.1 µM of each primer, 1 µl of bacterial supernatant, 0.6 U of Taq polymerase (EURx, Gdansk, Poland), 0.2 mM dNTPs and Taq Polymerase buffer (EURx), containing 15 mM MgCl2. Cycling conditions involved 94°C for 5 min; 30 cycles of 94°C for 1 min, 50°C for 1 min, 72°C for 1.5 min and a final step at 72°C for 5 min. Sanger sequencing was performed at Macrogen Europe (Amsterdam, The Netherlands) on a 3730xl DNA Analyzer (Thermofisher Scientific, Waltham, MA, USA). PCR amplification was as described by Monciardini et al. [48]. The sequencing data were analysed by FinchTV 1.4 (Geospiza, Inc.; Seattle, WA, USA; http://www.geospiza.com), the ends of sequenced reads were trimmed, and the resulting assemblies were blasted in the NCBI database. Sequencing data are available in Figshare at https://doi.org/10.6084/m9.figshare.23614797 (accessed on 2 July 2023).
Biochemical characterisation of isolates
All sequenced isolates were re-plated on Columbia Blood Agar with 5% sheep blood for evaluation of haemolysis, and on Mannitol Salt Agar (Graso Biotech, Owidz, Poland) for the preliminary identification of Staphylococcus spp. Staphylococci were further tested using the STAPH LATEX KIT (ProlexTM, Pro-Lab Diagnostics, Bromborough, UK) to distinguish S. aureus from other species.
Systematic literature search
We systematically searched for peer-reviewed, scientific studies, up until June 2023, that quantitatively analysed colonisation or contamination of cloth, surgical, N95 and similar masks by bacteria and fungi. The search was performed using PubMed and MEDLINE and included both qualitative and quantitative evaluations. Search terms were “(face mask) OR (facemask) OR (surgical mask) OR (FFP1) OR (FFP2) OR (FFP3) OR (N95) OR (KF94) OR (KN95)) AND ((microbial contamination) OR (bacteria) OR (fungi))“. Two independent researchers identified and screened eligible studies. Qualitative inclusion criteria were: valid reproducible presentation of the microbial contamination, comprehensible collection of evaluated masks, credibility of the results and clear focus. Quantitative inclusion criteria were: appropriate and precise methods, valid measurement of outcomes, representative selection of evaluated masks and reproducible detection/analytical methods. Selected papers were checked by at least three of the present authors for potential eligibility. Study design, methodology, analytical and experimental methods and outcomes were evaluated. Exclusions and reasons were documented. For included studies, the following data were extracted into tables: author and year, method and type of study, sample size and mask type(s), mask wearing duration(s), outcomes/examined microorganisms, content and main species. Simple mathematical calculations and graphics were performed with Libre-Office Calc, a free and open-source office package from the The Document Foundation [49].
3. Results
Abundance and types of bacteria on worn masks
Contamination of worn masks was visible, macroscopically, after staining with Rose Bengal (Figure 2). This dye binds to bacteria, fungi and tissue cells along with debris with the colour intensity suggested to reflect the degree of contamination [50,51,52,53,54].
Based upon culture, the average bacterial load of clean, never-used surgical face mask was 0.1 × 103 CFU recovered/mask whereas the arithmetic mean load on used masks was 4.24 × 104 CFU recovered/mask (geometric mean 1.3. × 104). Bacteria were most abundant on worn masks 5 and 6, with 1.03 × 105 and 2.85 × 105 CFU recovered/mask, respectively (Table 1). Biochemical and molecular identification revealed staphylococcal species on both these latter masks, including S. aureus, S. warneri and S. epidermidis (Supplementary Table 2). Although colony morphology differed between masks, the dominant phenotypes, in almost all cases including the unused masks, were the small white colonies typical of S. epidermidis and other coagulase-negative staphylococci (Supplementary Figure 1).
Identification of isolates by Sanger Sequencing of 16S rRNA gene
Out of 52 colonies subjected to PCR we chose the 40 with the most efficient product amplification for sequencing. Detailed BLAST results are presented in Supplementary Table 1.
The great majority (32, 80%) of these 40 belonged to the genus Staphylococcus confirming phenotypic identifications. We identified four coagulase-negative species: S. epidermidis (the most abundant), S. warneri, S. pasteuri and S. hominis, all of which belong to the normal human skin and nasal microbiota (Supplementary Table 2) [55]. On mask 5 we confirmed coagulase-positive Staphylococcus (Supplementary Table 2) along with S. aureus and S. argenteus.
A further four sequenced colonies comprised endospore-forming Bacillus species, namely B. cereus, B. thuringiensis, B. altitudinis, B. megaterium and others (Supplementary Table 1 and 2), which are soil bacteria [56]. Among the four remaining identified colonies (´Others´ in Figure 3) we found Sporosarcina newyorkensis, another endospore-forming Gram-positive rod, occasionally recovered from human bacteraemias and cow’s milk [57]. The sole Gram-negative species found was the pseudomonad Psychrobacter faecalis (Supplementary Table 2), a psychrophilic species associated with pigeon faeces [58] and reported also from human samples [59]. We did not isolate streptococci, although these are a major component of the human oral microbiota. Perhaps, their survival rates on the masks is low, or their recovery requires CO2-enriched incubation, not air incubation as used here.
Biochemical identification of isolates
The same 40 colonies were subjected to biochemical identification, yielding results consistent with the sequencing. Haemolysis was detected for almost all these bacteria (Supplementary Table 2) though its intensity was very variable (Supplementary Table 2, Supplementary Figure 1). Most of the bacteria showed halotolerance but only five fermented mannitol: these latter were tested for coagulase and protein A and three, all from mask 5, proved positive for both characters, confirming identification as S. aureus (Supplementary Table 2); all had morphology typical of the species (Supplementary Figure 1, Mask 5).
Systematic literature search
The literature search initially yielded 1310 results. This was narrowed (see PRISMA diagram, Figure 4) to 14 studies evaluating bacterial and fungal contamination of cloth, surgical and N95 masks, worn for periods ranging from 5 min to 3 days. Eleven studies considered bacteria, five fungi, and three both (Table 2). Four studies were for the general population whereas 10 were for healthcare workers (HCWs) [39,42,43,45,47,60,61,62,63,64,65,66,67,68]. Six were for surgical units (one specifically performing orthopaedic surgery) and five for dental practices [45,61,62,63,64]. Only two provided exact quantification and bacterial identification by 16S rRNA; these both investigated the general population [39,60]. Results of the literature search are summarised in the extraction table (Table 2).
4. Discussion
We found heavy bacterial contamination of surgical masks worn by the general population, with up to 2.85×105 CFU/mask (average 4.24×104).
Unfortunately, there are no microbiological standards for worn masks against which to review these findings; in the EU the only relevant bioburden requirement is EN 14683 for new masks, requiring ≤ 30 CFU/g. Nevertheless, since masks amount to a filtering system upstream of the respiratory tract, the limit values for ventilation systems are pertinent, notably the German standard for surfaces of ventilation and air-conditioning, VDI 6022, part 4 [69]. This specifies counts of 25 to 100 CFU/25 cm2 as ‘borderline’, whilst surfaces with counts > 100 CFU/25 cm2 require immediate action or replacement.
A disposable surgical mask has a one-side surface area of ca. 230 cm2 [70], meaning that in our worst case (2.85×105 CFU/mask = 3.09×104 CFU/25 cm2), the upper limit of VDI 6022 was exceeded by ca. 310-fold (average 46-fold) (Table 1). Values from a comparable study show 166-fold exceedance with cotton masks [39]; another study, for healthcare workers with surgical masks worn for an unspecified period, indicated >2000-fold exceedance (Table 2) [45]. It should be added that the bacterial burden of a mask lies directly in front of the respiratory tract whereas the vent of an air-conditioning system typically lies several meters away.
The EN 14683 requirements for new masks also were widely exceeded for worn items (Table 2), based upon weights of ca. 3g for a surgical mask and 4g for N95/FFP2 masks [71]; exceedance of this requirement was evident even for the unworn masks (Table 1).
The heavy general contamination of worn masks was further demonstrable by Rose Bengal staining (Figure 2).
Bacteria detected: potential clinical implications
Microbiological investigation of used mask predominantly revealed coagulase-negative skin staphylococci and endospore-forming soil bacteria (Bacillus spp.) on used (Figure 3). This predominance of staphylococci is in line with other studies on contaminated face masks in the general populace and healthcare workers [43,45,61,62,63,65]. One mask (no. 5) was contaminated with S. aureus, a well-known and versatile pathogen (Figure 3, Table 1) [72,73,74,75]. Up to 30% of the population carry nasal S. aureus without symptoms [76] though with an increased risk for autoinfection [72]. Contingent contamination of masks may facilitate dissemination of S. aureus and, plausibly skin infection [72]. An association between nasal carriage and surgical as well as KN95 mask contamination was shown previously for S. aureus and even for the non-carriers, the organism was frequently detected on KN95 masks (p=0.04, Fisher’s exact test) implying exogenous sources of contamination (hands, environment and external droplet containing air streams etc.) [72]. In support of this, some authors note S. aureus contaminates on the external as well as internal surfaces of masks [72].
Several authors have associated the use of face masks skin eruptions, some involving S. aureus [77] including new occurrence or exacerbation of acne, rosacea, and seborrhoeic dermatitis [78]. Other authors note enrichment of the normal eye microbiota with S. aureus from exhaled breath and droplets while wearing a mask contributing to the development of eyelid inflammation (chalazion) [79,80] and infections of the cornea [81], also deeper eye infections in the context of treatments (endophthalmitis following vitrectomy) [82]. There is also some evidence that S. aureus can increase replication of the SARS-CoV-2 virus by 10- to 15-fold [83], though this seems more pertinent in the upper nose than on a mask, where the virus is unlikely to be replicating.
Among other staphylococci, we predominantly found S. epidermidis (Figure 3). On one hand this is a normal and harmless component of the skin microbiota; on the other, it may be a hazard for vulnerable immunosuppressed individuals [84,85,86]. Even in healthy individuals, coagulase-negative staphylococci, at high abundance, may contribute to inflammatory skin conditions such as atopic dermatitis and acne vulgaris [55,87,88,89] with evidence that wearing a mask significantly increased the incidence of acne in particular [90,91,92,93,94,95,96,97,98].
We also found Bacillus spp. in the masks, including species that produce enterotoxins [56]. Although bacterial growth in masks may be possible (see below) we saw no evidence that growth attained the levels – typically >106/g – associated with toxins in food [99]. Moreover, wearers (except maybe children) are unlikely to chew on their masks, meaning that these organisms can be dismissed as a risk.
Literature review on mask contamination
Our literature review showed that all relevant mask types (surgical, N95, cloth) become increasingly contaminated with microorganisms during wear (Table 2, Figure 5) [39,41,42,47,62,64,68].
The literature reports contamination by bacteria of the genera Acinetobacter, Bacillus, Escherichia (specifically, E. coli, a faecal organism), Enterobacter, Enterococcus (another faecal organism), Klebsiella (including K. pneumoniae), Micrococcus, Pseudomonas, Staphylococcus (including S. aureus) and Streptococcus and by fungi of the genera Aspergillus, Alternaria, Candida, Cadosporium, Microsporum and Mucor (Table 2). These organisms are nourished by human saliva, nebulised oral biofilm and exhaled breath condensate, creating an underestimated biosafety concern.
In the general population, internal mask contamination typically exceeds external for bacteria – and perhaps, although this varies with the study – also for fungi (Table 2) [60,67]. For the healthcare workers using surgical masks, on the other hand, external contamination exceeds internal contamination both for bacteria and fungi (p<0.001) [43,45,61] and correlates with microbiological air quality in the areas where these staff were working [43]. For N95 masks, however, internal bacterial contamination appears higher than external even in healthcare settings [65]. Moreover, the total bacterial contamination of worn N95 masks exceeded that of similarly worn surgical masks [65].
Fungal contamination is seen up to 70-88% of used masks [67,68], and can be also higher inside than outside the mask [67]. This is surprising, given that fungi must come from outside the mask [60].
A comparison of maximal bacterial face mask counts for healthcare workers and the general population, based on Table 2 data and wearing/using times between 5 min and 3 days, showed a high variance in data due to the variance in wearing times and users and environmental factors. There is a tendency for higher bacterial loads in the general population (Table 2). These findings may reflect wider inappropriate and extended usage in the general population [7,8]. Due to the small number of similar studies, a meta-analytical statistical evaluation was not carried out.
Face mask contamination – contributing factors
Masks are a good matrix for microbial accumulation and potentially, growth, retaining an above-ambient temperature [100,101,102,103,104], moisture, and nutrient-rich debris [39,40,41,42,46,105]. Besides substances sucked in from the outside, nutrients comprise exhaled proteins and other debris, exfoliated and dead epithelial cells. Condensing droplets in the exhaled breath contain non-volatile metabolites, salts, lipids and proteins along with intact and degraded bacteria and viruses [106]. This organic richness was visualised in our Bengal Rose staining. Growth, rather than mere survival [39,40,42,46,105,107] of bacterial and fungal colonies is revealed by scanning electron microscopy of face masks (FFP2) worn for several hours [41].
The dead-space of rigid N95 masks provide a particularly warm, wet environment [100] with a relative humidity 1.5 to 2.6 times higher than externally [42] rising to 100% after 60 min of use [41]. This may create a particularly attractive breeding ground for bacteria [42] explaining the findings (above) that the N95 masks become more heavily contaminated than surgical masks and that, in healthcare settings, internal contamination exceeded external, reversing the pattern seen for surgical masks [65].
Microorganisms trapped and incubated in the mask may be distributed to the wearer, the environment and to others [17,108]. If leakage, owing to defect or poor fit, affects 1% of the mask area, the filtration efficiency is reduced by 50%; if the gap is 2% of the mask area, efficiency is reduced by 75% [109]. Moreover, the exhalation filtration efficiency is significantly lower than the theoretical filtration efficiency – by 12.4% and 46.3% for surgical and N95 masks, respectively [110]. In operating theatres, the recommended wearing duration is limited to few hours [111] as surgical masks lose effectiveness over time [112]. Whereas a fresh mask almost completely prevented bacterial contamination of an agar plate held 10-12 cm from the mouth, this effectiveness was measurably reduced within 30 min and negligible after 2h [113]. This brief period of filtration efficiency was further reduced if the mask was poorly fitted [109,114] or wetted [114].
Penetration of microorganisms between mask layers is possible, through capillary action depending on humidity and the specific organisms among other factors [115]. This in turn, may facilitate the formation of tiny organism-laden droplets. These then may be projected or inhaled with every breath [17,108,109,110,116,117,118]. In this context, we underscore the predominantly oral breathing while wearing a mask [17,119], in contrast to normal unimpeded breathing, which is largely via the nose, with greater filtration. Oral breathing increases the hazard of directly inhaling microorganisms from the mask into the deeper airways [120]. In a human study with a radiolabelled aerosol and average particle diameters of 4.4 µm (range 3.8-5.1 µm) scientists found a large increase in deposition in the lungs (+37%) when breathing orally compared with via the nose (75% vs. 38%) [121]. Additionally, masks – and especially the N95 type – impair natural mucociliary clearance of the upper airways, further enhancing inhalation and distribution of bacteria [122].
Face mask contamination – potential clinical implications
In a pre-COVID cross-sectional study on 710 individuals, the wearing (for religious reasons) of cloth facial coverings by Saudi women, drawn from the general population, was associated with statistically increased incidences of ‘common cold’ and asthma [18]. Elsewhere, pathophysiological skin changes [129] were associated with mask wearing in the general population and healthcare workers [130,131]. Several authors found changes in skin metabolomics, with an increased risk of barrier disruption and inflammation, putatively owing to dysbioses of the skin microbiome [129,132,133] leading to – or promoting development of – atopic dermatitis and acne vulgaris [132]. In context N95 respirators caused a more significant disorder than surgical masks [132].
Eye conditions also have been associated with mask use [79,80,81,82,116,134,135,136,137,138], whilst Islam et al. found indirect evidence of changes in the oral microbiome [139]. Sukul et al. changes in the gut microbiome (metabolic alterations) [20] whilst Xiang et al. found change of the nasal microbial communities after prolonged mask wearing [107]. Lastly, face masks are mentioned as possible factors behind an increase in mucormycosis cases during the COVID-19 pandemic particularly in immunocompromised or otherwise vulnerable individuals [67,68,140].
Findings in context
Long before the pandemic, face masks became widely used in medicine (notably surgery) healthcare and some manufacturing industries [17,141,142,143], aiming to prevent or minimise infection or contamination [8,15,70,143,144,145,146,147,148,149,150,151]. Nevertheless, their effectiveness in healthcare settings was debatable long before 2020 [152] and their role in the operating theatre remains controversial [153]. Given this history, there has been surprisingly little research on the effects of long-term usage by professional groups. Although masks filter larger debris and aerosol droplets from the air, they carry the microbiological risks outlined here along with toxicological, physiological, psychological and sociological harms [15,17,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,124,154].
The risks and benefits of requiring mask use by populations must be weighed from ethical and medical standpoints [14,15,17,155,156]. For masks to be demanded, the side effects and risks must be lower than the risk of not wearing a mask. A gold-standard Cochrane evaluation, based on clinical trials [13] found no substantive evidence of efficacy in preventing viral respiratory infections and one recent study, albeit with several possible confounders, even found mask-wearing to be associated with an increased risk of COVID-19 infection [157]. On the other hand, the potential harms are numerous [2,3,5,15,16,17,20,21,22,23,24,37,38,158,159,160,161,162,163,164]. They include MIES [17], harmful blood-gas alterations [15,20] and the potential microbiological hazards outlined here. Masks should not be mandated for the general population given this balance of evidence against their use. These points have been raised by many scientists [15,17,18,37,38,124,158,165,166] including leading breathing experts [167].
5. Limitations and strengths
The strengths of our paper are the use a precise method – 16S rRNA sequencing – to identify the bacteria found. In addition, we undertook a systematic literature overview and discuss the results from holistic microbiological and clinical perspectives. The masks collected in our study were provided by random individuals during daily life, representing a realistic general population sample. Rose Bengal staining strikingly visualised extensive contamination. Our rapid literature review should be seen only as a pilot assessment, with further analysis needed. Due to the small numbers of studies of same design, a meta-analysis was not carried out. Rather the strength of this review is qualitative, cataloguing the extensive scientific literature published by many scientists worldwide over several decades, demonstrating experimental evidence of face mask contamination and its risks.
6. Conclusions
Both our experimental study and the published literature show that face masks accumulate microorganisms, including pathobionts (Table 1 and Table 2) [39,42,43,45,47,60,61,62,63,64,65,66,67,68], with a microbial load up to several hundred times higher than the German standard VDI 6022 limit for ventilation systems surfaces [69] and the EN 14683 requirements for unused masks. Contamination increases with extended wearing time (Figure 5) [39,42,47,62,63,64,67,68] and is greater for N95 than surgical masks [65]. Most contamination was with staphylococci, occasionally including the pathogen S. aureus.
Put simply: (i) the mask act as a filter trap with bacteria accumulating on its external and internal surfaces; (ii) the mask then acts as a “microbiological incubator” at the entrance of the airways; (iii) microorganisms may grow within the mask, nourished by skin debris, mucus and “exhaled breath condensate” [17,39,40,42,46,105,106,107]. These trapped organisms/pathogens then may be inhaled, promoting infection of the respiratory tract [18,38] or, when distributed via air streams [108,109,110,117,135,136,168,169] the eye [79,80,81,82,116,135]. In addition, the skin microbiome is disrupted, potentially leading to or promoting other infections and allergic conditions [39,74,107,133,170].
Lastly, accumulated microorganisms may be distributed via leakage [108,109,110], amplified by the atomiser effect of the mask [15,17,117,171,172].
A Cochrane analysis, based solely on the highest grade of evidence, found no evidence that masks reduced the spread of respiratory viral infections in the general population [13]. On the other hand, their detriments, over and above those investigated here, are clear. They impede communication [33,34,35,91,173,174,175,176,177]. They impede learning, especially for children [2,3,5,15,27,36,154,163,166,178]. They are associated with transient hypoxaemia (decreased blood O2), transient hypercarbia (increased blood CO2) [15,17,20,22,23,24,163,164]. They deny the wearer of the most basic individuality — of showing their face [27,28,31,32,33,34,35,154,178]. Their long-term imposition is especially harmful for vulnerable members of the population [15,17,20]. Recent scientific papers indicate toxicological issues via inhalation of plastic particles and cancerogenic organic compounds originating from the mask material [15,19,124].
In short, the adverse effects of masks are clear [2,3,5,15,17,19,20,24,37,124,158,159,160,161,162,163,164,179], whereas the protective antiviral effect in real life scenarios remains doubtful [13,14,15,16,157,180,181,182,183,184,185,186,187,188,189,190,191,192,193,194,195,196,197,198]. Given this, together with the microbiological contamination issues highlighted, masking laws and requirements do not meet the basic medical ethic of ‘Do no harm’. Laws and mandates requiring mask use accordingly have no valid place in respiratory pandemic management.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
KK, BW, DL, AZ, and AJK: conceptualization and methodology. KK and AJK: software. KK, BW, DL, AZ, and AJK: formal analysis and writing—review and editing. KK, BW, DL, AZ, and AJK: investigation. KK and DL: clinical interpretations. KK, BW, DL and AJK: writing—original draft preparation. All authors have read and agreed to the published version of the manuscript.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Acknowledgements
We wish to thank Mrs Jadwiga Gronczewska from the Department of Evolutionary Genetics and Biosystematics, University of Gdańsk, Poland, for her valuable technical support on this project. We also thank Dr. Bernpohl, hygienist and microbiologist, and the ophthalmologist and physicist MPhys Dr. Mengedoht (both Gütersloh, Germany), who have inspired parts of the manuscript.
Research Ethics Statement
This study did not include human subjects. We analysed used face masks (objects) for bacterial colonization. No human material was examined. The used face masks (after they had been worn) were provided to us by anonymous voluntary donors.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Face covering policies during the COVID-19 pandemic, Our World in Data. (2023). Available online: https://ourworldindata.org/grapher/face-covering-policies-covid (accessed on 29 December 2022).
- S.N. Ladhani, Face masking for children - time to reconsider, Journal of Infection. 85 (2022) 623–624. [CrossRef]
- S. Thomson, Mask mandates for children during the COVID-19 pandemic: an international human rights perspective, Scand J Public Health. 50 (2022) 683–685. [CrossRef]
- World Health Organization, U.N.C. Fund (UNICEF), WHO - Advice on the use of masks for children in the community in the context of COVID-19: annex to the advice on the use of masks in the context of COVID-19, 21 August 2020, (2020). Available online: https://apps.who.int/iris/handle/10665/333919 (accessed on 7 November 2020).
- S. Schwarz, E. Jenetzky, H. Krafft, T. Maurer, D. Martin, Corona child studies “Co-Ki”: first results of a Germany-wide register on mouth and nose covering (mask) in children., Monatsschr Kinderheilkd. 169 (2021) 353–365. [CrossRef]
- World Health Organization, WHO - Advice on the use of masks in the context of COVID-19: interim guidance, 5 June 2020, (2020). Available online: https://apps.who.int/iris/handle/10665/332293 (accessed on 7 November 2020).
- K.J. Cummings, J. Cox-Ganser, M.A. Riggs, N. Edwards, K. Kreiss, Respirator Donning in Post-Hurricane New Orleans - Volume 13, Number 5—May 2007 - Emerging Infectious Diseases journal - CDC, (2007). [CrossRef]
- J. Gralton, M.-L. McLaws, Protecting healthcare workers from pandemic influenza: N95 or surgical masks?, Crit Care Med. 38 (2010) 657–667. [CrossRef]
- I. Kappstein, Mund-Nasen-Schutz in der Öffentlichkeit: Keine Hinweise für eine Wirksamkeit, Krankenhaushygiene up2date. 15 (2020) 279–295. [CrossRef]
- R. Roberge, Facemask use by children during infectious disease outbreaks, Biosecur Bioterror. 9 (2011) 225–231. [CrossRef]
- A.P.S. Munro, R.C. Hughes, Face coverings have little utility for young school-aged children, Archives of Disease in Childhood. 108 (2023) 77–78. [CrossRef]
- T. Jefferson, M. Jones, L.A.A. Ansari, G. Bawazeer, E. Beller, J. Clark, J. Conly, C.D. Mar, E. Dooley, E. Ferroni, P. Glasziou, T. Hoffman, S. Thorning, M.V. Driel, Physical interventions to interrupt or reduce the spread of respiratory viruses. Part 1 - Face masks, eye protection and person distancing: systematic review and meta-analysis, medRxiv. (2020) 2020.03.30.20047217. [CrossRef]
- T. Jefferson, L. Dooley, E. Ferroni, L.A. Al-Ansary, M.L. van Driel, G.A. Bawazeer, M.A. Jones, T.C. Hoffmann, J. Clark, E.M. Beller, P.P. Glasziou, J.M. Conly, Physical interventions to interrupt or reduce the spread of respiratory viruses, Cochrane Database of Systematic Reviews. (2023). [CrossRef]
- J. Sandlund, R. Duriseti, S.N. Ladhani, K. Stuart, J. Noble, T.B. Høeg, Child mask mandates for COVID-19: a systematic review, Archives of Disease in Childhood. (2023). [CrossRef]
- K. Kisielinski, S. Wagner, O. Hirsch, B. Klosterhalfen, A. Prescher, Possible toxicity of chronic carbon dioxide exposure associated with face mask use, particularly in pregnant women, children and adolescents – A scoping review, Heliyon. 0 (2023). [CrossRef]
- E. Coma, M. Català, L. Méndez-Boo, S. Alonso, E. Hermosilla, E. Alvarez-Lacalle, D. Pino, M. Medina, L. Asso, A. Gatell, Q. Bassat, A. Mas, A. Soriano-Arandes, F.F. Avilés, C. Prats, Unravelling the role of the mandatory use of face covering masks for the control of SARS-CoV-2 in schools: a quasi-experimental study nested in a population-based cohort in Catalonia (Spain), Archives of Disease in Childhood. (2022). [CrossRef]
- K. Kisielinski, P. Giboni, A. Prescher, B. Klosterhalfen, D. Graessel, S. Funken, O. Kempski, O. Hirsch, Is a Mask That Covers the Mouth and Nose Free from Undesirable Side Effects in Everyday Use and Free of Potential Hazards?, International Journal of Environmental Research and Public Health. 18 (2021) 4344. [CrossRef]
- E.F.E.M. Ahmad, M. Mohammed, A.A. Al Rayes, A. Al Qahtani, A.G. Elzubier, F.A.E. Suliman, The Effect of Wearing the Veil by Saudi Ladies on the Occurrence of Respiratory Diseases, Journal of Asthma. 38 (2001) 423–426. [CrossRef]
- H. Ryu, Y.-H. Kim, Measuring the quantity of harmful volatile organic compounds inhaled through masks, Ecotoxicology and Environmental Safety. 256 (2023) 114915. [CrossRef]
- P. Sukul, J. Bartels, P. Fuchs, P. Trefz, R. Remy, L. Rührmund, S. Kamysek, J.K. Schubert, W. Miekisch, Effects of COVID-19 protective face masks and wearing durations on respiratory haemodynamic physiology and exhaled breath constituents, European Respiratory Journal. 60 (2022). [CrossRef]
- R. G. M. Al-Allaff, S. M. Y. Al-Taee, S. T. D. Baker, Some Immunological Impacts of Face Mask Usage During the COVID-19 Pandemic, Pakistan Journal of Biological Sciences. 24 (2021) 920–927. [CrossRef]
- R.J. Vakharia, I. Jani, S. Yadav, T. Kurian, To Study Acute Changes in Brain Oxygenation on MRI in Healthcare Workers Using N95 Mask and PPE Kits for Six Hours a Day, Indian J Radiol Imaging. 31 (2021) 893–900. [CrossRef]
- C.S.W. Law, P.S. Lan, G.H. Glover, Effect of wearing a face mask on fMRI BOLD contrast, NeuroImage. 229 (2021) 117752. [CrossRef]
- S. Patel, E. Mohapatra, A.K. Suganthy, S. Shah, J. Abraham, R. Nanda, A.K. Behera, A. Gupta, A pilot study to evaluate the changes in venous blood gas parameters and hypoxia biomarkers in health care workers using different kinds of masks, Lung India. 40 (2023) 134–142. [CrossRef]
- D. Prousa, Studie zu psychischen und psychovegetativen Beschwerden mit den aktuellen Mund-Nasenschutz-Verordnungen, (2020). [CrossRef]
- M.A. Pavlova, C.-C. Carbon, Y. Coello, A.A. Sokolov, A.M. Proverbio, Editorial: Impact of face covering on social cognition and interaction, Front Neurosci. 17 (2023) 1150604. [CrossRef]
- C.-C. Carbon, M.J. Held, A. Schütz, Reading Emotions in Faces With and Without Masks Is Relatively Independent of Extended Exposure and Individual Difference Variables, Frontiers in Psychology. 13 (2022). Available online: https://www.frontiersin.org/articles/10.3389/fpsyg.2022.856971 (accessed on 1 February 2023).
- F. Schönweitz, J. Eichinger, J. Kuiper, F. Ongolly, W. Spahl, B. Prainsack, B. Zimmermann, The social meanings of artefacts: Face masks in the COVID-19 pandemic, Frontiers in Public Health. 10 (2022). Available online: https://www.frontiersin.org/articles/10.3389/fpubh.2022.829904 (accessed on 14 October 2023).
- C. Villani, S. D’Ascenzo, E. Scerrati, P. Ricciardelli, R. Nicoletti, L. Lugli, Wearing the face mask affects our social attention over space, Frontiers in Psychology. 13 (2022). Available online: https://www.frontiersin.org/articles/10.3389/fpsyg.2022.923558 (accessed on 14 October 2023).
- A.M. Proverbio, A. Cerri, The Recognition of Facial Expressions Under Surgical Masks: The Primacy of Anger, Frontiers in Neuroscience. 16 (2022). Available online: https://www.frontiersin.org/articles/10.3389/fnins.2022.864490 (accessed on 14 October 2023).
- F. Grundmann, K. Epstude, S. Scheibe, Face masks reduce emotion-recognition accuracy and perceived closeness, PLOS ONE. 16 (2021) e0249792. [CrossRef]
- L. Mathis, The Effects of Face Masks on Emotion Interpretation in Socially Anxious Individuals, Graduate Student Journal of Psychology. 20 (2023). [CrossRef]
- T.L. Truong, S.D. Beck, A. Weber, The impact of face masks on the recall of spoken sentences, J Acoust Soc Am. 149 (2021) 142–144. [CrossRef]
- R. Sönnichsen, G. Llorach Tó, S. Hochmuth, V. Hohmann, A. Radeloff, How Face Masks Interfere With Speech Understanding of Normal-Hearing Individuals: Vision Makes the Difference, Otol Neurotol. 43 (2022) 282–288. [CrossRef]
- V.S. McKenna, C.L. Kendall, T.H. Patel, R.J. Howell, R.L. Gustin, Impact of Face Masks on Speech Acoustics and Vocal Effort in Healthcare Professionals, The Laryngoscope. 132 (2022) 391–397. [CrossRef]
- Education recovery in early years providers: spring 2022, GOV.UK. (2022). Available online: https://www.gov.uk/government/publications/education-recovery-in-early-years-providers-spring-2022/education-recovery-in-early-years-providers-spring-2022 (accessed on 1 February 2023).
- B. Spira, Correlation Between Mask Compliance and COVID-19 Outcomes in Europe, Cureus. 14 (2022) e24268. [CrossRef]
- Z. Fögen, The Foegen effect: A mechanism by which facemasks contribute to the COVID-19 case fatality rate, Medicine (Baltimore). 101 (2022) e28924. [CrossRef]
- L. Delanghe, E. Cauwenberghs, I. Spacova, I. De Boeck, W. Van Beeck, K. Pepermans, I. Claes, D. Vandenheuvel, V. Verhoeven, S. Lebeer, Cotton and Surgical Face Masks in Community Settings: Bacterial Contamination and Face Mask Hygiene, Front Med (Lausanne). 8 (2021) 732047. [CrossRef]
- J. Szostak-Kotowa, Biodeterioration of textiles, International Biodeterioration & Biodegradation. 53 (2004) 165–170. [CrossRef]
- A. Buzzin, G. Domènech-Gil, E. Fraschetti, E. Giovine, D. Puglisi, D. Caputo, Assessing the consequences of prolonged usage of disposable face masks, Sci Rep. 12 (2022) 16796. [CrossRef]
- Q. Yang, H. Li, S. Shen, G. Zhang, R. Huang, Y. Feng, J. Yang, S. Ma, Study of the micro-climate and bacterial distribution in the deadspace of N95 filtering face respirators, Sci Rep. 8 (2018) 17382. [CrossRef]
- P. Luksamijarulkul, N. Aiempradit, P. Vatanasomboon, Microbial Contamination on Used Surgical Masks among Hospital Personnel and Microbial Air Quality in their Working Wards: A Hospital in Bangkok, Oman Med J. 29 (2014) 346–350. [CrossRef]
- A.A. Chughtai, S. Stelzer-Braid, W. Rawlinson, G. Pontivivo, Q. Wang, Y. Pan, D. Zhang, Y. Zhang, L. Li, C.R. MacIntyre, Contamination by respiratory viruses on outer surface of medical masks used by hospital healthcare workers, BMC Infect Dis. 19 (2019) 491. [CrossRef]
- D. Monalisa, Microbial Contamination of the Mouth Masks Used By Post- Graduate Students in a Private Dental Institution: An In-Vitro Study, (2017) 7.
- K. Kisielinski, B. Wojtasik, Suitability of Rose Bengal sodium salt staining for visualisation of face mask contamination by living organisms, AIMSES. 9 (2022) 218–231. [CrossRef]
- Z. Liu, Y. Chang, W. Chu, M. Yan, Y. Mao, Z. Zhu, H. Wu, Z. Jie, K. Dai, H. Li, F. Liu, Z. Zhai, Surgical masks as source of bacterial contamination during operative procedures, Journal of Orthopaedic Translation. 14 (2018) 57–62. [CrossRef]
- P. Monciardini, M. Sosio, L. Cavaletti, C. Chiocchini, S. Donadio, New PCR primers for the selective amplification of 16S rDNA from different groups of actinomycetes1, FEMS Microbiology Ecology. 42 (2002) 419–429. [CrossRef]
- Calc | LibreOffice - Free Office Suite - Based on OpenOffice - Compatible with Microsoft, (2023). Available online: https://www.libreoffice.org/discover/calc (accessed on 17 March 2023).
- R.P.G. Feenstra, S.C.G. Tseng, What Is Actually Stained by Rose Bengal?, Archives of Ophthalmology. 110 (1992) 984–993. [CrossRef]
- H.J. Conn, Rose Bengal as a General Bacterial Stain, J Bacteriol. 6 (1921) 253–254.
- W.E. Maneval, Staining Bacteria and Yeasts with Acid Dyes, Stain Technology. 16 (1941) 13–19. [CrossRef]
- D.C. Saha, A Rapid Staining Method for Detection of Endophytic Fungi in Turf and Forage Grasses, Phytopathology. 78 (1988) 237. [CrossRef]
- B. Wojtasik, M. Zbawicka, L. Grabarczyk, W. Juzwa, Flow cytometric approach to evaluate the impact of hydro-technical concrete compounds’ release to the freshwater microbiome, Environ Monit Assess. 193 (2021) 698. [CrossRef]
- A.L. Byrd, Y. Belkaid, J.A. Segre, The human skin microbiome, Nat Rev Microbiol. 16 (2018) 143–155. [CrossRef]
- N.A. Logan, Bacillus and relatives in foodborne illness, J Appl Microbiol. 112 (2012) 417–429. [CrossRef]
- W.J. Wolfgang, A. Coorevits, J.A. Cole, P. De Vos, M.C. Dickinson, G.E. Hannett, R. Jose, E.J. Nazarian, P. Schumann, A. Van Landschoot, S.E. Wirth, K.A. Musser, Sporosarcina newyorkensis sp. nov. from clinical specimens and raw cow’s milk, International Journal of Systematic and Evolutionary Microbiology. 62 (2012) 322–329. [CrossRef]
- P. Kämpfer, A. Albrecht, S. Buczolits, H.-J. Busse, Psychrobacter faecalis sp. nov., a new species from a bioaerosol originating from pigeon faeces, Syst Appl Microbiol. 25 (2002) 31–36. [CrossRef]
- P. Deschaght, M. Janssens, M. Vaneechoutte, G. Wauters, Psychrobacter isolates of human origin, other than Psychrobacter phenylpyruvicus, are predominantly Psychrobacter faecalis and Psychrobacter pulmonis, with emended description of P. faecalis, International Journal of Systematic and Evolutionary Microbiology. 62 (2012) 671–674. [CrossRef]
- A.-M. Park, S. Khadka, F. Sato, S. Omura, M. Fujita, K. Hashiwaki, I. Tsunoda, Bacterial and fungal isolation from face masks under the COVID-19 pandemic, Sci Rep. 12 (2022) 11361. [CrossRef]
- R. Sachdev, K. Garg, G. Singh, V. Mehrotra, Is safeguard compromised? Surgical mouth mask harboring hazardous microorganisms in dental practice, J Family Med Prim Care. 9 (2020) 759–763. [CrossRef]
- M.P. Gund, G. Boros, M. Hannig, S. Thieme-Ruffing, B. Gärtner, T.R. Rohrer, A. Simon, S. Rupf, Bacterial contamination of forehead skin and surgical mask in aerosol-producing dental treatment, J Oral Microbiol. 13 (2021) 1978731. [CrossRef]
- M.P. Gund, J. Naim, M. Hannig, A. Halfmann, B. Gärtner, G. Boros, S. Rupf, CHX and a Face Shield Cannot Prevent Contamination of Surgical Masks, Front Med (Lausanne). 9 (2022) 896308. [CrossRef]
- V. Checchi, M. Montevecchi, L. Valeriani, L. Checchi, Bioburden Variation of Filtering Face Piece Respirators over Time: A Preliminary Study, Materials. 15 (2022) 8790. [CrossRef]
- M. Yousefimashouf, R. Yousefimashouf, M.S. Alikhani, H. Hashemi, P. Karami, Z. Rahimi, S.M. Hosseini, Evaluation of the bacterial contamination of face masks worn by personnel in a center of COVID 19 hospitalized patients: A cross-sectional study, New Microbes New Infect. 52 (2023) 101090. [CrossRef]
- M. Nightingale, M. Mody, A.H. Rickard, M. Cassone, Bacterial contamination on used face masks among nursing home healthcare personnel, Antimicrob Steward Healthc Epidemiol. 3 (2023) e54. [CrossRef]
- V.C. Keri, A. Kumar, G. Singh, A. Mandal, H. Ali, P. Ranjan, N. Wig, Pilot study on burden of fungal contamination in face masks: need for better mask hygiene in the COVID-19 era, Infez Med. 29 (2021) 557–561. [CrossRef]
- Y. Merad, Z. Belmokhtar, O. Hadjazi, M. Belkacemi, D. Matmour, Z. Merad, A. Bassaid, O. Megherbi, Fungal contamination of medical masks among forensic healthcare workers in the COVID19 era, New Microbes and New Infections. 53 (2023) 101134. [CrossRef]
- VDI 6022, VDI. (2023). Available online: https://www.vdi.de/richtlinien/unsere-richtlinien-highlights/vdi-6022 (accessed on 14 October 2023).
- S. Rengasamy, A. Miller, B.C. Eimer, R.E. Shaffer, Filtration Performance of FDA-Cleared Surgical Masks, J Int Soc Respir Prot. 26 (2009) 54–70.
- J. Fernández-Arribas, T. Moreno, R. Bartrolí, E. Eljarrat, COVID-19 face masks: A new source of human and environmental exposure to organophosphate esters, Environment International. 154 (2021) 106654. [CrossRef]
- P. Ostrowski, H. Masiuk, P. Kulig, A. Skoryk, A. Wcisłek, J. Jursa-Kulesza, A. Sarna, M. Sławiński, M. Kotowski, K. Tejchman, K. Kotfis, J. Sieńko, Medical Face Masks Do Not Affect Acid–Base Balance Yet Might Facilitate the Transmission of Staphylococcus aureus in Hospital Settings during the COVID-19 Pandemic, International Journal of Environmental Research and Public Health. 20 (2023) 2474. [CrossRef]
- A. Sakr, F. Brégeon, J.-L. Mège, J.-M. Rolain, O. Blin, Staphylococcus aureus Nasal Colonization: An Update on Mechanisms, Epidemiology, Risk Factors, and Subsequent Infections, Frontiers in Microbiology. 9 (2018). Available online: https://www.frontiersin.org/articles/10.3389/fmicb.2018.02419 (accessed on 14 October 2023).
- R.R. Dietert, J.M. Dietert, The Human Superorganism: Using Microbes for Freedom vs. Fear, Applied Microbiology. 3 (2023) 883–905. [CrossRef]
- D. Nowicka, E. Grywalska, Staphylococcus aureus and Host Immunity in Recurrent Furunculosis, Dermatology. 235 (2019) 295–305. [CrossRef]
- L. Akhtar Danesh, Z. Saiedi Nejad, H. Sarmadian, S. Fooladvand, A. van Belkum, E. Ghaznavi-Rad, Elimination of Staphylococcus aureus nasal carriage in intensive care patients lowers infection rates, Eur J Clin Microbiol Infect Dis. 39 (2020) 333–338. [CrossRef]
- C. Han, J. Shi, Y. Chen, Z. Zhang, Increased flare of acne caused by long-time mask wearing during COVID-19 pandemic among general population, Dermatologic Therapy. 33 (2020) e13704. [CrossRef]
- P. Bortoluzzi, V. Boneschi, S. Veraldi, “Mask” Tinea: An Increasing Infection during COVID-19 Pandemic, Mycopathologia. 187 (2022) 141–142. [CrossRef]
- R.Z. Silkiss, M.K. Paap, S. Ugradar, Increased incidence of chalazion associated with face mask wear during the COVID-19 pandemic, Am J Ophthalmol Case Rep. 22 (2021) 101032. [CrossRef]
- W. Akioud, S. Sebbata, Y. Mozarie, A. Oubaaz, Chalazion and Face Mask Wear during COVID-19 Pandemic: Is There A Link?, European Journal of Medical and Health Sciences. 5 (2023) 17–19. [CrossRef]
- M. Molero-Senosiain, S. Tiew, A. Patel, I. Houben, N. Dhillon, Impact of face mask wear on bacterial keratitis, Journal Français d’Ophtalmologie. 46 (2023) e37–e39. [CrossRef]
- T. Sakamoto, H. Terasaki, T. Yamashita, H. Shiihara, R. Funatsu, A. Uemura, Increased incidence of endophthalmitis after vitrectomy relative to face mask wearing during COVID-19 pandemic, British Journal of Ophthalmology. 107 (2023) 1472–1477. [CrossRef]
- M.I. Goncheva, R.M. Gibson, A.C. Shouldice, J.D. Dikeakos, D.E. Heinrichs, The Staphylococcus aureus protein IsdA increases SARS CoV-2 replication by modulating JAK-STAT signaling, iScience. 26 (2023). [CrossRef]
- M. Otto, Staphylococcus epidermidis – the “accidental” pathogen, Nat Rev Microbiol. 7 (2009) 555–567. [CrossRef]
- S.M.K. Schoenfelder, C. Lange, M. Eckart, S. Hennig, S. Kozytska, W. Ziebuhr, Success through diversity – How Staphylococcus epidermidis establishes as a nosocomial pathogen, International Journal of Medical Microbiology. 300 (2010) 380–386. [CrossRef]
- C. Heilmann, W. Ziebuhr, K. Becker, Are coagulase-negative staphylococci virulent?, Clin Microbiol Infect. 25 (2019) 1071–1080. [CrossRef]
- F. Khorvash, F. Abdi, H.H. Kashani, F.F. Naeini, T. Narimani, Staphylococcus aureus in Acne Pathogenesis: A Case-Control Study, N Am J Med Sci. 4 (2012) 573–576. [CrossRef]
- K. Findley, E.A. Grice, The Skin Microbiome: A Focus on Pathogens and Their Association with Skin Disease, PLOS Pathogens. 10 (2014) e1004436. [CrossRef]
- R.D. Bjerre, J. Bandier, L. Skov, L. Engstrand, J.D. Johansen, The role of the skin microbiome in atopic dermatitis: a systematic review, Br J Dermatol. 177 (2017) 1272–1278. [CrossRef]
- C.C.I. Foo, A.T.J. Goon, Y. Leow, C. Goh, Adverse skin reactions to personal protective equipment against severe acute respiratory syndrome – a descriptive study in Singapore, Contact Dermatitis. 55 (2006) 291–294. [CrossRef]
- E. Rosner, Adverse Effects of Prolonged Mask Use among Healthcare Professionals during COVID-19, J Infect Dis Epidemiol. 6:130 (2020). [CrossRef]
- L. Techasatian, S. Lebsing, R. Uppala, W. Thaowandee, J. Chaiyarit, C. Supakunpinyo, S. Panombualert, D. Mairiang, S. Saengnipanthkul, K. Wichajarn, P. Kiatchoosakun, P. Kosalaraksa, The Effects of the Face Mask on the Skin Underneath: A Prospective Survey During the COVID-19 Pandemic, J Prim Care Community Health. 11 (2020) 2150132720966167. [CrossRef]
- M. Abduljabbar, D.E. Kalthoum, M. Bakarman, I. Wahby Salem, Z. Alsulaimani, W. Alharbi, S. Shawish, R. Alsobhi, The Correlation Between Wearing Face Masks and Skin Damage in Adults During the COVID-19 Pandemic: A Cross-Sectional Study in Jeddah, Saudi Arabia, Cureus. 14 (2022) e31521. [CrossRef]
- A. Villani, G. Fabbrocini, M.C. Annunziata, L. Potestio, Maskne prevalence and risk factors during the COVID-19 pandemic, J Eur Acad Dermatol Venereol. (2022) 10.1111/jdv.18248. [CrossRef]
- R. a Bakhsh, S.Y. Saddeeg, K.M. Basaqr, B.M. Alshammrani, B.S. Zimmo, Prevalence and Associated Factors of Mask-Induced Acne (Maskne) in the General Population of Jeddah During the COVID-19 Pandemic, Cureus. 14 (n.d.) e26394. [CrossRef]
- A. Dani, A. Eseonu, K. Bibee, Risk factors for the development of acne in healthcare workers during the COVID-19 pandemic, Arch Dermatol Res. 315 (2023) 1067–1070. [CrossRef]
- O. Falodun, N. Medugu, L. Sabir, I. Jibril, N. Oyakhire, A. Adekeye, An epidemiological study on face masks and acne in a Nigerian population, PLOS ONE. 17 (2022) e0268224. [CrossRef]
- Y.-F. Cheng, H. Zhao, J. Li, K.E. Lipa, H.-F. Xie, B. Wang, Y.-X. Huang, Factors aggravating acne vulgaris during the COVID-19 pandemic in China: a web-based cross-sectional survey, Eur Rev Med Pharmacol Sci. 26 (2022) 7305–7312. [CrossRef]
- Sandra M. Tallent, Ann Knolhoff, E. Jeffery Rhodehamel, Stanley M. Harmon, Reginald W. Bennett, Bacteriological Analytical Manual (BAM); Chapter 14: Bacillus cereus., FDA, 1996. Available online: https://www.fda.gov/food/laboratory-methods-food/bam-chapter-14-bacillus-cereus (accessed on 15 October 2023).
- R. Roberge, S. Benson, J.-H. Kim, Thermal burden of N95 filtering facepiece respirators, Ann Occup Hyg. 56 (2012) 808–814. [CrossRef]
- R.J. Roberge, J.-H. Kim, S.M. Benson, Absence of consequential changes in physiological, thermal and subjective responses from wearing a surgical mask, Respiratory Physiology & Neurobiology. 181 (2012) 29–35. [CrossRef]
- J.-H. Kim, S.M. Benson, R.J. Roberge, Pulmonary and heart rate responses to wearing N95 filtering facepiece respirators, Am J Infect Control. 41 (2013) 24–27. [CrossRef]
- A. Scarano, F. Inchingolo, F. Lorusso, Facial Skin Temperature and Discomfort When Wearing Protective Face Masks: Thermal Infrared Imaging Evaluation and Hands Moving the Mask, Int J Environ Res Public Health. 17 (2020). [CrossRef]
- S.-R. Park, J. Han, Y.M. Yeon, N.Y. Kang, E. Kim, Effect of face mask on skin characteristics changes during the COVID-19 pandemic, Skin Res Technol. 27 (2021) 554–559. [CrossRef]
- Y.-H. Lee, H. Kim, D.W. Heo, I.-S. Ahn, H.-K. Park, Oral microbiome of the inner surface of face masks and whole saliva during the COVID-19 pandemic, Frontiers in Oral Health. 4 (2023). Available online: https://www.frontiersin.org/articles/10.3389/froh.2023.1178020 (accessed on 28 October 2023).
- S. Szunerits, H. Dӧrfler, Q. Pagneux, J. Daniel, S. Wadekar, E. Woitrain, D. Ladage, D. Montaigne, R. Boukherroub, Exhaled breath condensate as bioanalyte: from collection considerations to biomarker sensing, Anal Bioanal Chem. 415 (2023) 27–34. [CrossRef]
- G. Xiang, K. Xu, Y. Jian, L. He, Z. Shen, M. Li, Q. Liu, Prolonged mask wearing changed nasal microbial characterization of young adults during the COVID-19 pandemic in Shanghai, China, Frontiers in Immunology. 14 (2023). Available online: https://www.frontiersin.org/articles/10.3389/fimmu.2023.1266941 (accessed on 28 October 2023).
- I.M. Viola, B. Peterson, G. Pisetta, G. Pavar, H. Akhtar, F. Menoloascina, E. Mangano, K.E. Dunn, R. Gabl, A. Nila, E. Molinari, C. Cummins, G. Thompson, T.-Y.M. Lo, F.C. Denison, P. Digard, O. Malik, M.J.G. Dunn, C.M. McDougall, F.V. Mehendale, Face Coverings, Aerosol Dispersion and Mitigation of Virus Transmission Risk, IEEE Open J Eng Med Biol. 2 (2021) 26–35. [CrossRef]
- F. Drewnick, J. Pikmann, F. Fachinger, L. Moormann, F. Sprang, S. Borrmann, Aerosol filtration efficiency of household materials for homemade face masks: Influence of material properties, particle size, particle electrical charge, face velocity, and leaks, Aerosol Science and Technology. 55 (2021) 63–79. [CrossRef]
- Y. Shah, J.W. Kurelek, S.D. Peterson, S. Yarusevych, Experimental investigation of indoor aerosol dispersion and accumulation in the context of COVID-19: Effects of masks and ventilation, Physics of Fluids. 33 (2021) 073315. [CrossRef]
- R. Datta, Use of Surgical Facemasks in the Operation Theatre: Effective or Habit?, Medical Journal Armed Forces India. 66 (2010) 163–165. [CrossRef]
- M.H. Barbosa, K.U. Graziano, Influence of wearing time on efficacy of disposable surgical masks as microbial barrier, Braz. J. Microbiol. 37 (2006) 216–217. [CrossRef]
- U.S. Kelkar, B. Gogate, S. Kurpad, P. Gogate, M. Deshpande, How effective are face masks in operation theatre? A time frame analysis and recommendations., International Journal of Infection Control. 9 (2013).
- A. Tcharkhtchi, N. Abbasnezhad, M. Zarbini Seydani, N. Zirak, S. Farzaneh, M. Shirinbayan, An overview of filtration efficiency through the masks: Mechanisms of the aerosols penetration, Bioactive Materials. 6 (2021) 106–122. [CrossRef]
- N.V. McCullough, L.M. Brosseau, D. Vesley, Collection of three bacterial aerosols by respirator and surgical mask filters under varying conditions of flow and relative humidity, The Annals of Occupational Hygiene. 41 (1997) 677–690. [CrossRef]
- A. Hadayer, A. Zahavi, E. Livny, O. Gal-Or, A. Gershoni, K. Mimouni, R. Ehrlich, PATIENTS WEARING FACE MASKS DURING INTRAVITREAL INJECTIONS MAY BE AT A HIGHER RISK OF ENDOPHTHALMITIS, Retina. 40 (2020) 1651–1656. [CrossRef]
- C. Huber, Masks, false safety and real dangers, Part 4: Proposed mechanisms by which masks increase risk of COVID-19, Primary Doctor Medical Journal. (2020) 1–9.
- Boris Borovoy, Colleen Huber, Maria Crisler, Masks, false safety and real dangers, Part 2: Microbial challenges from masks, PDMJ. (2020) 1–19.
- M. Wyszyńska, A. Czelakowska, P. Rosak, E. Białożyt-Bujak, O. Gruca, J. Rosak-Szyrocka, J. Kasperski, M. Skucha-Nowak, Changes in the Oral Cavity Mucosal Surface under the Influence of Wearing Protective Face Masks—Nitric Oxide Concentration Analysis—Preliminary Report, Coatings. 12 (2022) 1164. [CrossRef]
- ICRP: Human respiratory tract model for radiological protection. A report of a Task Group of the International Commission on Radiological Protection, Ann ICRP. 24 (1994) 1–482.
- M.L. Everard, J.G. Hardy, A.D. Milner, Comparison of nebulised aerosol deposition in the lungs of healthy adults following oral and nasal inhalation, Thorax. 48 (1993) 1045–1046. [CrossRef]
- C. Cengiz, İ.H. Can, The effect of N95 and surgical masks on mucociliary clearance function and sinonasal complaints, Eur Arch Otorhinolaryngol. 279 (2022) 759–764. [CrossRef]
- S. Sangkham, O. Faikhaw, N. Munkong, P. Sakunkoo, C. Arunlertaree, M. Chavali, M. Mousazadeh, A. Tiwari, A review on microplastics and nanoplastics in the environment: Their occurrence, exposure routes, toxic studies, and potential effects on human health, Marine Pollution Bulletin. 181 (2022) 113832. [CrossRef]
- K. Kisielinski, S. Hockertz, O. Hirsch, S. Korupp, B. Klosterhalfen, A. Schnepf, G. Dyker, Wearing Face Masks as a Potential Source for Inhalation and Oral Uptake of Inanimate Toxins: a Scoping Review, (2023). [CrossRef]
- A. Khan, Z. Jia, Recent insights into uptake, toxicity, and molecular targets of microplastics and nanoplastics relevant to human health impacts, iScience. 26 (2023). [CrossRef]
- H. Liang, Y. Ji, W. Ge, J. Wu, N. Song, Z. Yin, C. Chai, Release kinetics of microplastics from disposable face masks into the aqueous environment, Science of The Total Environment. 816 (2022) 151650. [CrossRef]
- J. Ma, F. Chen, H. Xu, H. Jiang, J. Liu, P. Li, C.C. Chen, K. Pan, Face masks as a source of nanoplastics and microplastics in the environment: Quantification, characterization, and potential for bioaccumulation, Environmental Pollution. 288 (2021) 117748. [CrossRef]
- S. Wieland, A. Balmes, J. Bender, J. Kitzinger, F. Meyer, A.F. Ramsperger, F. Roeder, C. Tengelmann, B.H. Wimmer, C. Laforsch, H. Kress, From properties to toxicity: Comparing microplastics to other airborne microparticles, Journal of Hazardous Materials. 428 (2022) 128151. [CrossRef]
- W.-L. Teo, The “Maskne” microbiome – pathophysiology and therapeutics, International Journal of Dermatology. 60 (2021) 799–809. [CrossRef]
- Y. Sawada, Occupational Skin Dermatitis among Healthcare Workers Associated with the COVID-19 Pandemic: A Review of the Literature, International Journal of Molecular Sciences. 24 (2023) 2989. [CrossRef]
- 131. A. Tunçer Vural, The development of acne vulgaris due to face masks during the pandemic, risk awareness and attitudes of a group of university students, Journal of Cosmetic Dermatology. 21 (2022) 5306–5313. [CrossRef]
- Y. Liu, H. Zhao, H. Chen, X. Li, C. Ran, H. Sun, L. Wang, Does mask wearing affect skin health? An untargeted skin metabolomics study, Environ Int. 178 (2023) 108073. [CrossRef]
- J.K. Brooks, A.S. Sultan, M.A. Jabra-Rizk, Prolonged facial mask wear is a concern for the development of dysbiotic microbiome, Respiratory Medicine and Research. 81 (2022) 100877. [CrossRef]
- V.A. Koshevarova, Z.K. Westenhaver, M. Schmitz-Brown, B.J. McKinnon, K.H. Merkley, P.K. Gupta, Blepharoconjunctivitis and Otolaryngological Disease Trends in the Context of Mask Wearing during the COVID-19 Pandemic, Clinics and Practice. 12 (2022) 619–627. [CrossRef]
- W.G. Schultheis, J.E. Sharpe, Q. Zhang, S.N. Patel, A.E. Kuriyan, A. Chiang, S.J. Garg, J. Hsu, Effect of Taping Face Masks on Quantitative Particle Counts Near the Eye: Implications for Intravitreal Injections in the COVID-19 Era, American Journal of Ophthalmology. 225 (2021) 166–171. [CrossRef]
- B. Burgos-Blasco, P. Arriola-Villalobos, J.I. Fernandez-Vigo, C. Oribio-Quinto, M. Ariño-Gutierrez, D. Diaz-Valle, J.M. Benitez-del-Castillo, Face mask use and effects on the ocular surface health: A comprehensive review, The Ocular Surface. 27 (2023) 56–66. [CrossRef]
- M. Moshirfar, W.B. West, D.P. Marx, Face Mask-Associated Ocular Irritation and Dryness, Ophthalmol Ther. 9 (2020) 397–400. [CrossRef]
- L. Boccardo, Self-reported symptoms of mask-associated dry eye: A survey study of 3,605 people, Contact Lens and Anterior Eye. 45 (2022). [CrossRef]
- S.R. Islam, D. Prusty, S. Maiti, R. Dutta, P. Chattopadhyay, S.K.K. Manna, Effect of short-term use of FFP2 (N95) mask on salivary metabolome of young healthy volunteers: A pilot study., Mol. Omics. (2023). [CrossRef]
- U. Arora, M. Priyadarshi, V. Katiyar, M. Soneja, P. Garg, I. Gupta, V. Bharadiya, P. Berry, T. Ghosh, L. Patel, R. Sarda, S. Garg, S. Agarwal, V. Arora, A. Ramprasad, A. Kumar, R.K. Garg, P. Kodan, N. Nischal, G. Singh, P. Jorwal, A. Kumar, U. Baitha, V.P. Meena, A. Ray, P. Sethi, I. Xess, N. Vikram, S. Sinha, A. Biswas, A. Thakar, S. Bhatnagar, A. Trikha, N. Wig, Risk factors for Coronavirus disease-associated mucormycosis, J Infect. 84 (2022) 383–390. [CrossRef]
- N.L. Belkin, The evolution of the surgical mask: filtering efficiency versus effectiveness, Infect Control Hosp Epidemiol. 18 (1997) 49–57. [CrossRef]
- C. Matuschek, F. Moll, H. Fangerau, J.C. Fischer, K. Zänker, M. van Griensven, M. Schneider, D. Kindgen-Milles, W.T. Knoefel, A. Lichtenberg, B. Tamaskovics, F.J. Djiepmo-Njanang, W. Budach, S. Corradini, D. Häussinger, T. Feldt, B. Jensen, R. Pelka, K. Orth, M. Peiper, O. Grebe, K. Maas, E. Bölke, J. Haussmann, The history and value of face masks, European Journal of Medical Research. 25 (2020) 23. [CrossRef]
- S.-A. Lee, S.A. Grinshpun, T. Reponen, Respiratory Performance Offered by N95 Respirators and Surgical Masks: Human Subject Evaluation with NaCl Aerosol Representing Bacterial and Viral Particle Size Range, Ann Occup Hyg. 52 (2008) 177–185. [CrossRef]
- M.G.L. Ntlailane, J. Wichmann, Effectiveness of N95 respirators for nanoparticle exposure control (2000–2016): a systematic review and meta-analysis, J Nanopart Res. 21 (2019) 170. [CrossRef]
- L.P. Samaranayake, K.S. Fakhruddin, H.C. Ngo, J.W.W. Chang, C. Panduwawala, The effectiveness and efficacy of respiratory protective equipment (RPE) in dentistry and other health care settings: a systematic review, Acta Odontologica Scandinavica. 78 (2020) 626–639. [CrossRef]
- K. Willeke, Y. Qian, J. Donnelly, S. Grinshpun, V. Ulevicius, Penetration of Airborne Microorganisms Through a Surgical Mask and a Dust/Mist Respirator, American Industrial Hygiene Association Journal. 57 (1996) 348–355. [CrossRef]
- T.K. Hodous, C.C. Coffey, The role of respiratory protective devices in the control of tuberculosis, Occup Med. 9 (1994) 631–657.
- Y. Qian, K. Willeke, S.A. Grinshpun, J. Donnelly, C.C. Coffey, Performance of N95 Respirators: Filtration Efficiency for Airborne Microbial and Inert Particles, American Industrial Hygiene Association Journal. 59 (1998) 128–132. [CrossRef]
- M. Loeb, N. Dafoe, J. Mahony, M. John, A. Sarabia, V. Glavin, R. Webby, M. Smieja, D.J.D. Earn, S. Chong, A. Webb, S.D. Walter, Surgical Mask vs N95 Respirator for Preventing Influenza Among Health Care Workers: A Randomized Trial, JAMA. 302 (2009) 1865. [CrossRef]
- J.D. Smith, C.C. MacDougall, J. Johnstone, R.A. Copes, B. Schwartz, G.E. Garber, Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: a systematic review and meta-analysis, CMAJ. 188 (2016) 567–574. [CrossRef]
- I. Liu, V. Prasad, J. Darrow, Evidence for Community Face Masking to Limit the Spread of SARS-CoV-2: A Critical Review, Health Matrix: The Journal of Law-Medicine. 33 (2023) 1.
- M. Vincent, P. Edwards, Disposable surgical face masks for preventing surgical wound infection in clean surgery, Cochrane Database Syst Rev. 4 (2016) CD002929. [CrossRef]
- H.N. Burdick, H. Maibach, Clinical relevance of masks in the operating room? A systematic review, Clinical Infection in Practice. 12 (2021) 100087. [CrossRef]
- C.-C. Carbon, Wearing Face Masks Strongly Confuses Counterparts in Reading Emotions, Frontiers in Psychology. 11 (2020). Available online: https://www.frontiersin.org/articles/10.3389/fpsyg.2020.566886 (accessed on 14 October 2023).
- World Medical Association, WMA - The World Medical Association-Declaration of Helsinki, (2013). Available online: https://www.wma.net/what-we-do/medical-ethics/declaration-of-helsinki/ (accessed on 8 November 2021).
- WHO, World Medical Association (WMA): Declaration of Helsinki. Ethical principles for medical research involving human subjects., Bulletin of the World Health Organization. 79 (2001) 373–374.
- I.H. Elgersma, A. Fretheim, P. Elstrøm, P. Aavitsland, Association between face mask use and risk of SARS-CoV-2 infection: Cross-sectional study, Epidemiol Infect. 151 (2023) e194. [CrossRef]
- A. Boretti, Efficacy of Generalized Face Masking Mandates, Health Services Research and Managerial Epidemiology. 8 (2021) 23333928211058023. [CrossRef]
- P. Galanis, I. Vraka, D. Fragkou, A. Bilali, D. Kaitelidou, Impact of personal protective equipment use on health care workers’ physical health during the COVID-19 pandemic: A systematic review and meta-analysis, American Journal of Infection Control. 49 (2021) 1305–1315. [CrossRef]
- T. Unoki, H. Sakuramoto, R. Sato, A. Ouchi, T. Kuribara, T. Furumaya, J. Tatsuno, Y. Wakabayashi, A. Tado, N. Hashimoto, N. Inagaki, Y. Sasaki, Adverse Effects of Personal Protective Equipment Among Intensive Care Unit Healthcare Professionals During the COVID-19 Pandemic: A Scoping Review, SAGE Open Nursing. 7 (2021) 23779608211026164. [CrossRef]
- H. Dirol, E. Alkan, M. Sindel, T. Ozdemir, D. Erbas, The physiological and disturbing effects of surgical face masks in the COVID-19 era, BLL. 122 (2021) 821–825. [CrossRef]
- R.P. Gaikwad, A.B. Banodkar, V.P. Nandgaonkar, Respiratory Consequences of N95 Mask during Covid-19 Pandemic- An Observational Study, International Journal of Health Sciences and Research. 11 (2021) 55.
- H. Walach, H. Traindl, J. Prentice, R. Weikl, A. Diemer, A. Kappes, S. Hockertz, Carbon dioxide rises beyond acceptable safety levels in children under nose and mouth covering: Results of an experimental measurement study in healthy children, Environmental Research. 212 (2022) 113564. [CrossRef]
- C. Acuti Martellucci, M.E. Flacco, M. Martellucci, F.S. Violante, L. Manzoli, Inhaled CO2 Concentration While Wearing Face Masks: A Pilot Study Using Capnography, Environ Health Insights. 16 (2022) 11786302221123573. [CrossRef]
- M.D.F. Ahmad, S. Wahab, F. Ali Ahmad, M. Intakhab Alam, H. Ather, A. Siddiqua, S. Amir Ashraf, M. Abu Shaphe, M. Idreesh Khan, R. Ali Beg, A novel perspective approach to explore pros and cons of face mask in prevention the spread of SARS-CoV-2 and other pathogens, Saudi Pharmaceutical Journal. 29 (2021) 121–133. [CrossRef]
- N. Shobako, Lessons from the health policies for children during the pandemic in Japan, Frontiers in Public Health. 10 (2022). Available online: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1015955 (accessed on 25 September 2023).
- J.D. Beauchamp, C.A. Mayhew, Revisiting the rationale of mandatory masking, J. Breath Res. 17 (2023) 042001. [CrossRef]
- L. Mastropasqua, M. Lanzini, L. Brescia, R. D’Aloisio, M. Nubile, M. Ciancaglini, C. D’Amario, L. Agnifili, R. Mastropasqua, Face Mask-Related Ocular Surface Modifications During COVID-19 Pandemic: A Clinical, In Vivo Confocal Microscopy, and Immune-Cytology Study, Translational Vision Science & Technology. 10 (2021) 22. [CrossRef]
- S. D’Souza, T. Vaidya, A.P. Nair, R. Shetty, N.R. Kumar, A. Bisht, T. Panigrahi, T.S. J, P. Khamar, M.M. Dickman, R. Agrawal, S. Mahajan, S. Sengupta, R.M.M.A. Nuijts, S. Sethu, A. Ghosh, Altered Ocular Surface Health Status and Tear Film Immune Profile Due to Prolonged Daily Mask Wear in Health Care Workers, Biomedicines. 10 (2022) 1160. [CrossRef]
- S. Jin, D. Wetzel, M. Schirmer, Deciphering mechanisms and implications of bacterial translocation in human health and disease, Current Opinion in Microbiology. 67 (2022) 102147. [CrossRef]
- S. Asadi, C.D. Cappa, S. Barreda, A.S. Wexler, N.M. Bouvier, W.D. Ristenpart, Efficacy of masks and face coverings in controlling outward aerosol particle emission from expiratory activities, Scientific Reports. 10 (2020) 15665. [CrossRef]
- S. Bagchi, S. Basu, S. Chaudhuri, A. Saha, Penetration and secondary atomization of droplets impacted on wet facemasks, Phys. Rev. Fluids. 6 (2021) 110510. [CrossRef]
- T. Rebmann, R. Carrico, J. Wang, Physiologic and other effects and compliance with long-term respirator use among medical intensive care unit nurses, Am J Infect Control. 41 (2013) 1218–1223. [CrossRef]
- Ł. Matusiak, M. Szepietowska, P. Krajewski, R. Białynicki-Birula, J.C. Szepietowski, Inconveniences due to the use of face masks during the COVID-19 pandemic: A survey study of 876 young people, Dermatologic Therapy. 33 (2020) e13567. [CrossRef]
- Naylor, L.A. Burke, J.A. Holman, Covid-19 Lockdown Affects Hearing Disability and Handicap in Diverse Ways: A Rapid Online Survey Study, Ear Hear. 41 (2020) 1442–1449. [CrossRef]
- F. Thomas, C. Allen, W. Butts, C. Rhoades, C. Brandon, D.L. Handrahan, Does wearing a surgical facemask or N95-respirator impair radio communication?, Air Med J. 30 (2011) 97–102. [CrossRef]
- C.A. Heider, M.L. Álvarez, E. Fuentes-López, C.A. González, N.I. León, D.C. Verástegui, P.I. Badía, C.A. Napolitano, Prevalence of Voice Disorders in Healthcare Workers in the Universal Masking COVID-19 Era, The Laryngoscope. n/a (2020). [CrossRef]
- H. Sezer, D. Çınar, N. Kılıç Akça, The effect of prolonged use of surgical masks during face-to-face teaching on cognitive and physiological parameters of nursing students: A cross-sectional and descriptive study, Nurse Education in Practice. 72 (2023) 103779. [CrossRef]
- C. Elbl, J.X. Brunner, D. Schier, A. Junge, H. Junge, Protective face masks add significant dead space, European Respiratory Journal. 58 (2021). [CrossRef]
- A. Chandra, T.B. Høeg, Lack of correlation between school mask mandates and paediatric COVID-19 cases in a large cohort, Journal of Infection. 85 (2022) 671–675. [CrossRef]
- J. Xiao, E.Y.C. Shiu, H. Gao, J.Y. Wong, M.W. Fong, S. Ryu, B.J. Cowling, Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings—Personal Protective and Environmental Measures - Volume 26, Number 5—May 2020 - Emerging Infectious Diseases journal - CDC, (2020). [CrossRef]
- M.X. Wang, S.X.W. Gwee, P.E.Y. Chua, J. Pang, Effectiveness of Surgical Face Masks in Reducing Acute Respiratory Infections in Non-Healthcare Settings: A Systematic Review and Meta-Analysis, Frontiers in Medicine. 7 (2020). Available online: https://www.frontiersin.org/articles/10.3389/fmed.2020.564280 (accessed on 26 November 2022).
- M.S. Fønhus, T.K. Dalsbø, K.G. Brurberg, Facemasks to prevent transmission of respiratory illness, such as COVID-19, Norwegian Institute of Public Health, 2021. Available online: https://fhi.brage.unit.no/fhi-xmlui/handle/11250/2756758 (accessed on 7 November 2021).
- A.E. Aiello, V. Perez, R.M. Coulborn, B.M. Davis, M. Uddin, A.S. Monto, Facemasks, hand hygiene, and influenza among young adults: a randomized intervention trial, PLoS One. 7 (2012) e29744. [CrossRef]
- E. Zain Alabdeen, A. Choudhry, D. Al-Naji, Effect of use of Face mask on Hajj related Acute Respiratory Infection among Hajjis from Riyadh -A Health Promotion Intervention study, FETP Saudi Epidemiology Bulletin. 12 (2005) 27–28.
- M. Alfelali, E.A. Haworth, O. Barasheed, A.-M. Badahdah, H. Bokhary, M. Tashani, M.I. Azeem, J. Kok, J. Taylor, E.H. Barnes, H. El Bashir, G. Khandaker, E.C. Holmes, D.E. Dwyer, L.G. Heron, G.J. Wilson, R. Booy, H. Rashid, Hajj Research Team, Facemask against viral respiratory infections among Hajj pilgrims: A challenging cluster-randomized trial, PLoS One. 15 (2020) e0240287. [CrossRef]
- L. Canini, L. Andréoletti, P. Ferrari, R. D’Angelo, T. Blanchon, M. Lemaitre, L. Filleul, J.-P. Ferry, M. Desmaizieres, S. Smadja, A.-J. Valleron, F. Carrat, Surgical mask to prevent influenza transmission in households: a cluster randomized trial, PLoS One. 5 (2010) e13998. [CrossRef]
- C.R. MacIntyre, S. Cauchemez, D.E. Dwyer, H. Seale, P. Cheung, G. Browne, M. Fasher, J. Wood, Z. Gao, R. Booy, N. Ferguson, Face mask use and control of respiratory virus transmission in households, Emerg Infect Dis. 15 (2009) 233–241. [CrossRef]
- C.R. MacIntyre, H. Seale, T.C. Dung, N.T. Hien, P.T. Nga, A.A. Chughtai, B. Rahman, D.E. Dwyer, Q. Wang, A cluster randomised trial of cloth masks compared with medical masks in healthcare workers, BMJ Open. 5 (2015) e006577. [CrossRef]
- J.M. Simmerman, P. Suntarattiwong, J. Levy, R.G. Jarman, S. Kaewchana, R.V. Gibbons, B.J. Cowling, W. Sanasuttipun, S.A. Maloney, T.M. Uyeki, L. Kamimoto, T. Chotipitayasunondh, Findings from a household randomized controlled trial of hand washing and face masks to reduce influenza transmission in Bangkok, Thailand, Influenza Other Respir Viruses. 5 (2011) 256–267. [CrossRef]
- B.J. Cowling, R.O.P. Fung, C.K.Y. Cheng, V.J. Fang, K.H. Chan, W.H. Seto, R. Yung, B. Chiu, P. Lee, T.M. Uyeki, P.M. Houck, J.S.M. Peiris, G.M. Leung, Preliminary Findings of a Randomized Trial of Non-Pharmaceutical Interventions to Prevent Influenza Transmission in Households, PLoS One. 3 (2008). [CrossRef]
- B.J. Cowling, K.-H. Chan, V.J. Fang, C.K.Y. Cheng, R.O.P. Fung, W. Wai, J. Sin, W.H. Seto, R. Yung, D.W.S. Chu, B.C.F. Chiu, P.W.Y. Lee, M.C. Chiu, H.C. Lee, T.M. Uyeki, P.M. Houck, J.S.M. Peiris, G.M. Leung, Facemasks and hand hygiene to prevent influenza transmission in households: a cluster randomized trial, Ann Intern Med. 151 (2009) 437–446. [CrossRef]
- T. Suess, C. Remschmidt, S.B. Schink, B. Schweiger, A. Nitsche, K. Schroeder, J. Doellinger, J. Milde, W. Haas, I. Koehler, G. Krause, U. Buchholz, The role of facemasks and hand hygiene in the prevention of influenza transmission in households: results from a cluster randomised trial; Berlin, Germany, 2009-2011, BMC Infect Dis. 12 (2012) 26. [CrossRef]
- E.L. Larson, Y. Ferng, J. Wong-McLoughlin, S. Wang, M. Haber, S.S. Morse, Impact of Non-Pharmaceutical Interventions on URIs and Influenza in Crowded, Urban Households, Public Health Rep. 125 (2010) 178–191.
- J.L. Jacobs, S. Ohde, O. Takahashi, Y. Tokuda, F. Omata, T. Fukui, Use of surgical face masks to reduce the incidence of the common cold among health care workers in Japan: a randomized controlled trial, Am J Infect Control. 37 (2009) 417–419. [CrossRef]
- H. Bundgaard, J.S. Bundgaard, D.E.T. Raaschou-Pedersen, C. von Buchwald, T. Todsen, J.B. Norsk, M.M. Pries-Heje, C.R. Vissing, P.B. Nielsen, U.C. Winsløw, K. Fogh, R. Hasselbalch, J.H. Kristensen, A. Ringgaard, M. Porsborg Andersen, N.B. Goecke, R. Trebbien, K. Skovgaard, T. Benfield, H. Ullum, C. Torp-Pedersen, K. Iversen, Effectiveness of Adding a Mask Recommendation to Other Public Health Measures to Prevent SARS-CoV-2 Infection in Danish Mask Wearers, Ann Intern Med. (2020). [CrossRef]
- A. Juutinen, E. Sarvikivi, P. Laukkanen-Nevala, O. Helve, Face mask recommendations in schools did not impact COVID-19 incidence among 10–12-year-olds in Finland – joinpoint regression analysis, BMC Public Health. 23 (2023) 730. [CrossRef]
- S.A. Gómez-Ochoa, T. Muka, Meta-analysis on facemask use in community settings to prevent respiratory infection transmission shows no effect, International Journal of Infectious Diseases. 103 (2021) 257–259. [CrossRef]
Figure 1.
Rose Bengal staining of worn face masks. The area analysed is marked by the red frame. The mask dimensions indicated by the manufactures (175 × 95 mm) exclude folds, which enlarge the surface area.
Figure 1.
Rose Bengal staining of worn face masks. The area analysed is marked by the red frame. The mask dimensions indicated by the manufactures (175 × 95 mm) exclude folds, which enlarge the surface area.
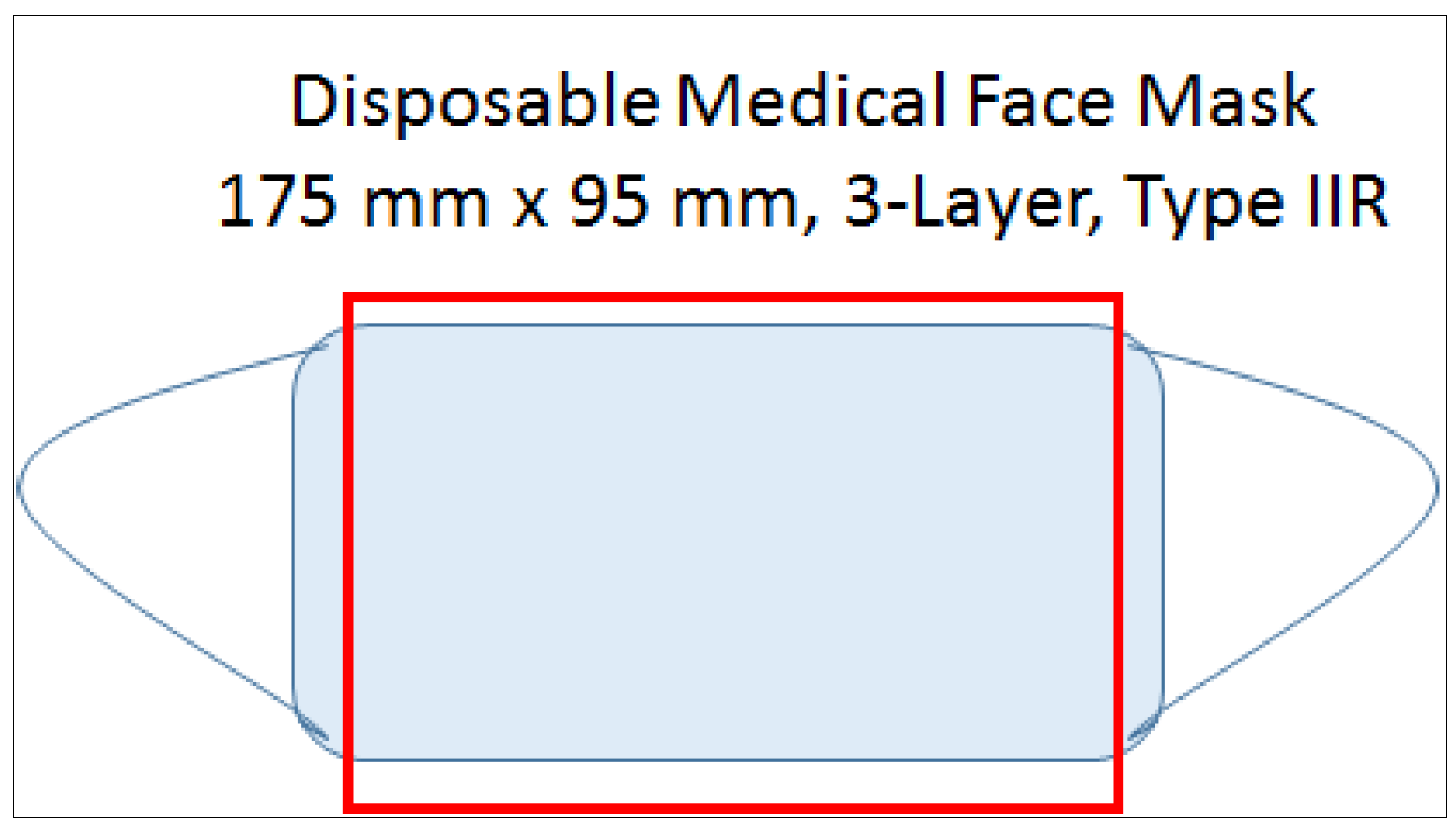
Figure 2.
Example masks staining with Bengal Rose, binding to tissue cells, debris and bacteria.
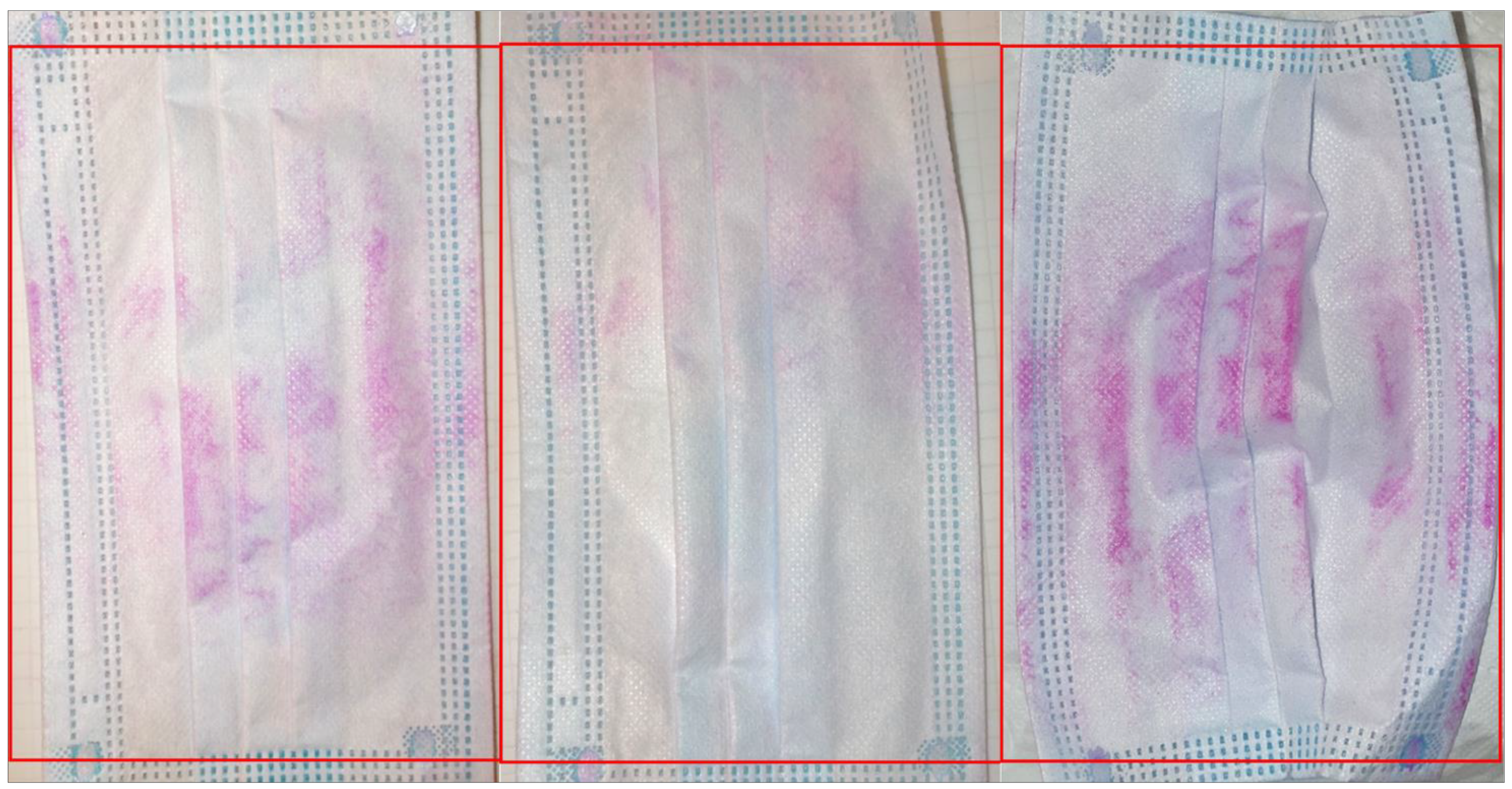
Figure 3.
The relative abundance of different bacterial species recovered from masks.
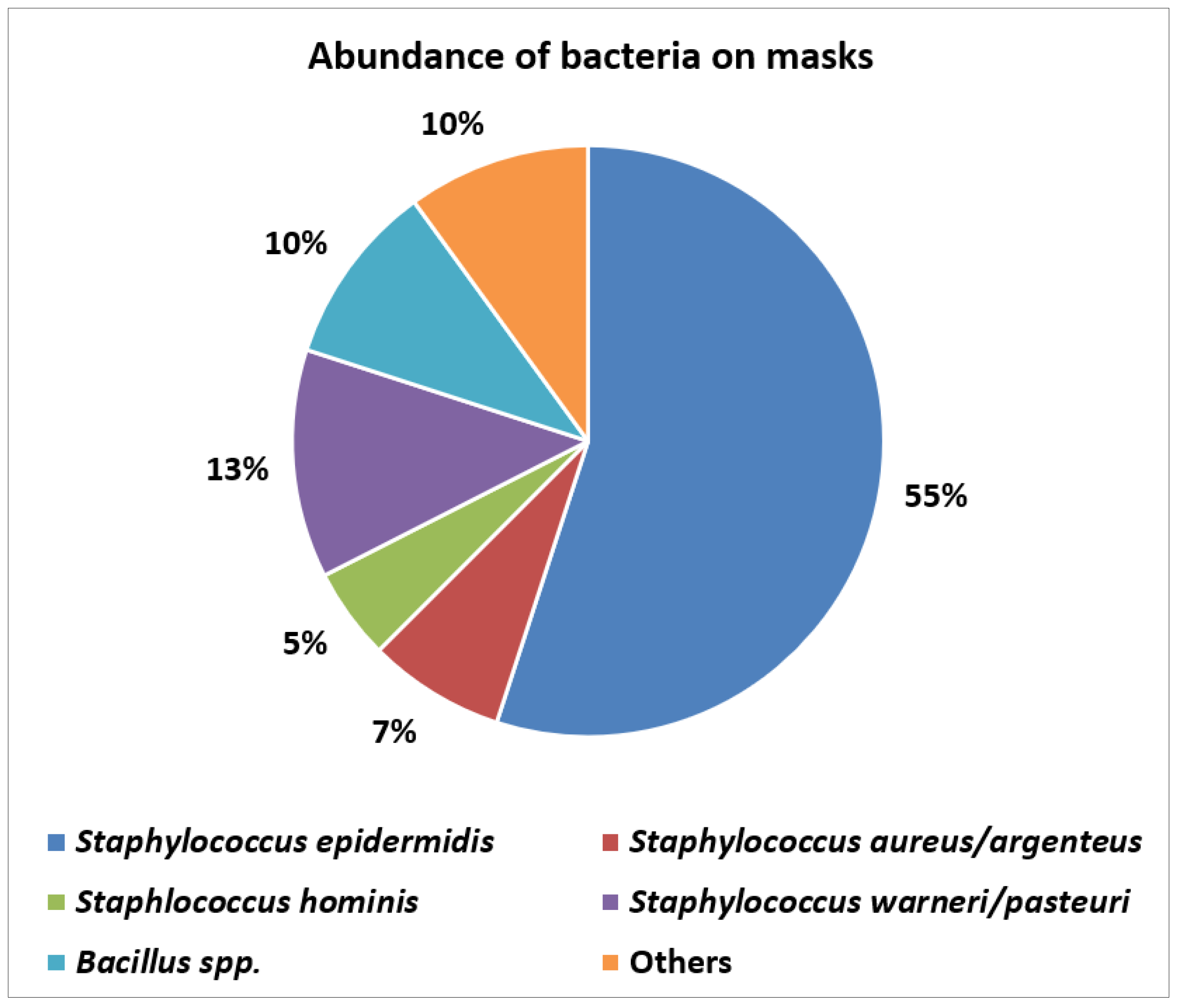
Figure 4.
PRISMA flow chart for the literature search.
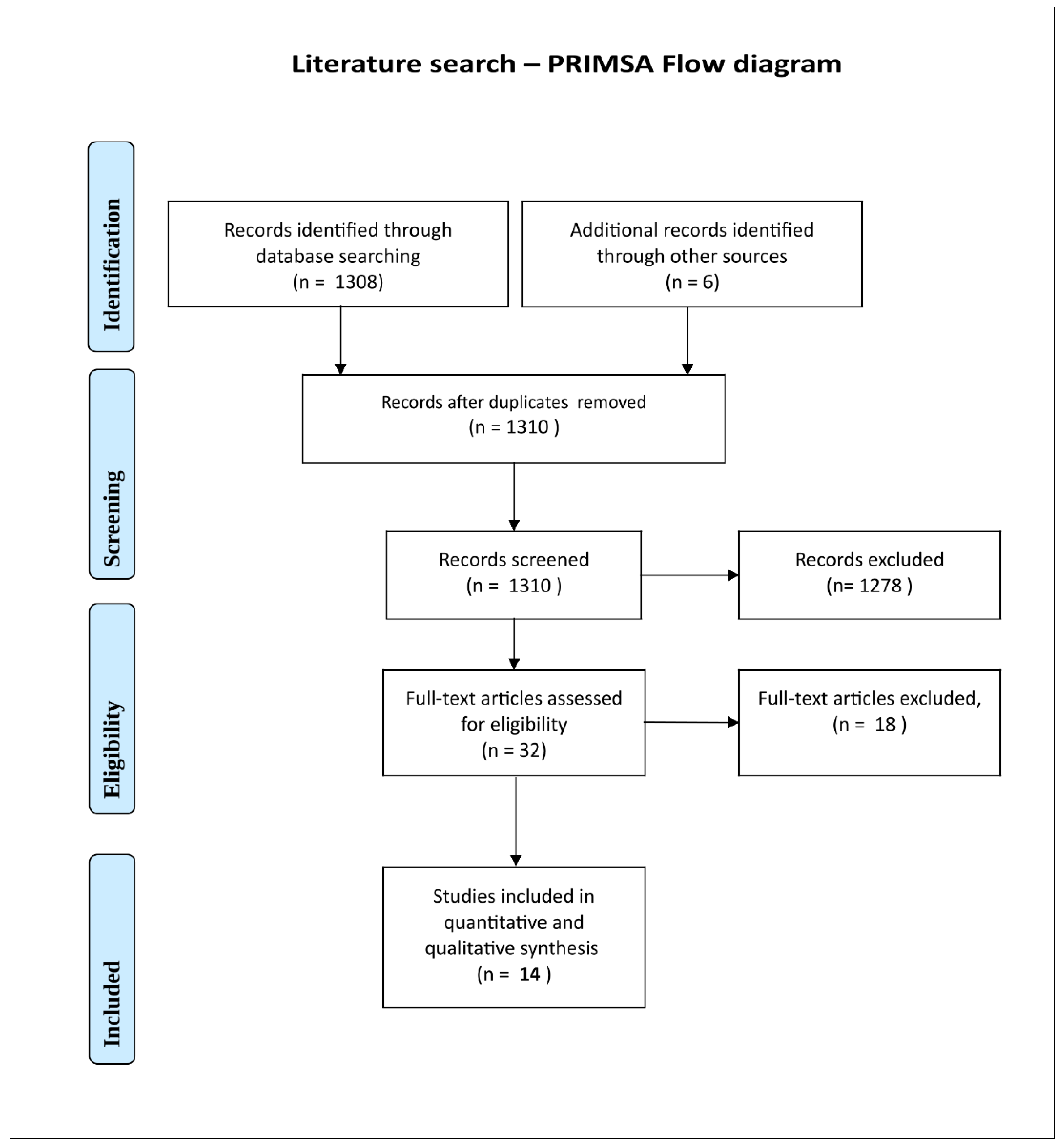
Figure 5.
Time dependency of face mask contamination during wear, based upon literature data (Table 2). The diagrams indicate the association between CFU/mask and wearing duration, based on mean values from three publications [42,47,64]. If included in the primary studies, the standard deviations are also shown. Yang et al. investigated the inner surfaces of masks worn by the general population, whereas both Liu et al. and Checchi et al. examined the outer layers of masks worn by HCW.
Figure 5.
Time dependency of face mask contamination during wear, based upon literature data (Table 2). The diagrams indicate the association between CFU/mask and wearing duration, based on mean values from three publications [42,47,64]. If included in the primary studies, the standard deviations are also shown. Yang et al. investigated the inner surfaces of masks worn by the general population, whereas both Liu et al. and Checchi et al. examined the outer layers of masks worn by HCW.
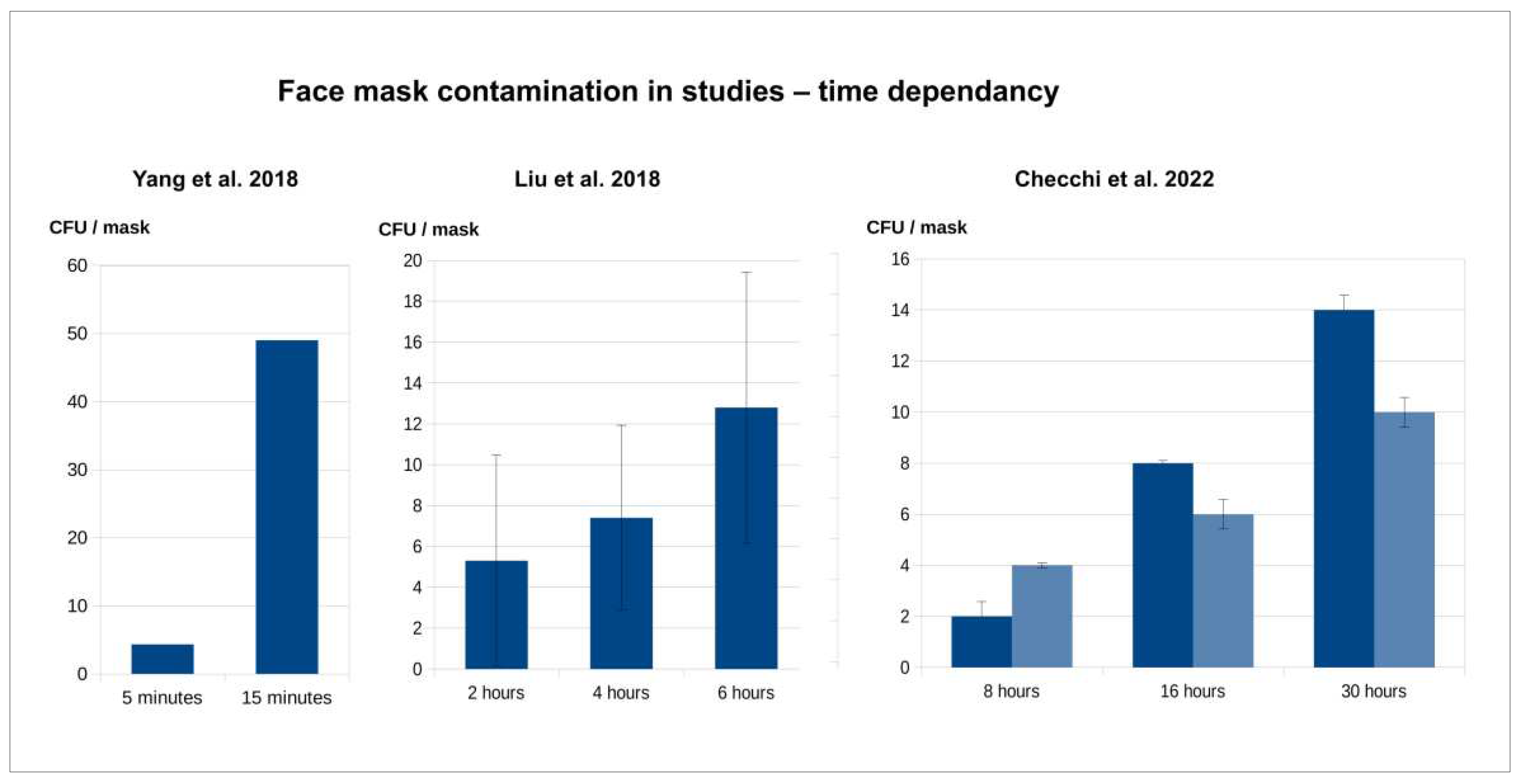

Table 1.
The abundance of bacteria in masks.
| Mask number | Average CFU* recovered/mask and standard deviation** |
|---|---|
| 3 clean masks | 0.1 ± 0.09 × 103 |
| 1 | 4.8 ± 0.3 × 103 |
| 2 | 9.29 ± 0.17 × 104 |
| 3 | 1.35 ± 0.15 × 103 |
| 4 | 9.3 ± 0.3 × 103 |
| 5 | 1.03 ± 0.03 × 105 |
| 6 | 2.85 ± 0.05 × 105 |
| 7 | 1.79 ± 0.14 × 104 |
| 8 | 9.15 ± 0.15 × 103 |
| 9 | 0.45 ± 0 × 103 |
| 10 | 5.55 ± 0.45 × 103 |
| 11 | 3.47 ± 0.29 × 104 |
| 12 | 1.76 ± 0.05 × 104 |
| 13 | 3.45 ± 1.05 × 103 |
| 14 | 1.55 ± 0.05 × 104 |
| 15 | 3.53 ± 0.08 × 104 |
*CFU – colony forming units, ** Standard deviation of three replicates.
Table 2.
Microbiological findings of the literature search (mask contamination with bacteria and fungi).
Table 2.
Microbiological findings of the literature search (mask contamination with bacteria and fungi).
| Author and year | Mask types (population) |
Duration of wear | n | Contamination | Method | Maximum level of contamination* | Principal microorganisms detected |
|---|---|---|---|---|---|---|---|
| Present study 2023 | surgical, disposable (general population) |
5 min- 12 h |
15 | bacterial (nearly whole mask) |
PBS, agar plates 16S rRNA |
2.85 ×105 / mask |
Staphylococcus aureus, Staphylococcus warneri, Staphylococcus epidermidis, B. cereus, B. thuringiensis, B. altitudinis, B. megaterium |
| Checchi 2022 [64] | N95 (HCW, dental practice) |
30 h | 6 | bacterial (outer surface samples) |
agar plates, eye sighting and counting |
101-141 / outer mask area sample | not specified |
| Delanghe 2021 [39] | cotton, surgical (general population) |
4 h | 21 | bacterial (half mask) |
PBS, agar plates 16S rRNA |
1.53×105 ± 1.96×105 / cotton mask 1.79×104 ± 1.63×104 / surgical mask |
Staphylococcus spp., Bacillus spp., Acinetobacter spp. |
| Gund 2021 [62] | surgical (HCW, dental practice) |
45-60 min |
32 | bacterial, (external surface samples) |
agar plates, MALDI-TOF MS, colony counter | <102 / contact sample external surface |
S. epidermidis, S. capitis, S. saprophyticus, B. cereus |
|
Gund 2022 [63] |
surgical over N95 (HCW, dental practice) |
60-90 min | 102 | bacterial, (external surface samples) |
agar plates, MALDI-TOF MS, colony counter |
80 ± 130 / imprint external surface |
Streptococcus, Staphylococcus spp., Micrococcus spp., Bacillus spp. |
| Keri 2021 [67] | cloth, surgical, N95 (general population) |
4-72 h | 50 | fungi, (inner and outer surface samples) |
agar plates, microscopy, lactophenol cotton blue |
fungi: 64% outside (32 in 50 masks) 67% inside (14 in 21 masks) |
Aspergillus niger, Rhizopus arrhizus, Syncephalastrum spp., Mucor spp. |
| Liu 2018 [47] | Surgical (HCW, orthopaedic surgery) |
2-6 h | 40 | bacterial, (first outer layer, second outer layer samples) |
agar plates, eye sighting and counting |
bacteria: 5.3 (0-2h) / layer samples 7.4 (2-4h) /layer samples 12.8 (4-6h) / layer samples |
not specified |
| Lukasmijarkul 2014 [43] | surgical (HCW) |
not given (working day) |
203 | bacterial, fungal, (outer side and inner side) |
agar plates, Gram´s stain, lactophenol cotton blue. microscopic morphology |
bacteria: 47 ± 56 / inside area sample 166 ± 199 / outside area sample fungi: 15 ± 9 / inside area sample 34 ± 18 / outside area sample |
Staphylococcus spp., Pseudomonas spp. Aspergillus spp., Penicillium spp. |
| Merad 2023 [68] | surgical, N95 (HCW) |
1-7 h | 52 | fungal, inner side samples | agar plates, macroscopic and microscopic features of growing colonies |
fungi: 88% surgical 8% KN95 |
Alternaria spp. (32%), Penicillium spp. (20%), Aspergillus spp. (16%) |
| Monalisa 2017 [45] | surgical (HCW, dental practice) |
not given (working day) |
36 | bacterial, fungal, (outer side and face-side samples) |
agar plates, colony counter, biochemical tests | bacteria: 31.7×102 / outer sample 22.8 ×105 / internal sample |
E. coli (54%), S. aureus (25%), Klebsiella spp. (5%), Enterococcus spp. (4%), Pseudomonas spp.(3%), Enterobacter spp. (2%), Candida (6%), Aspergillus spp., Cladosporium spp., Alternaria spp. |
| Nightingale 2023 [66] | surgical (HCW) |
4-8 h | 69 | bacterial (whole mask) |
selective plates, catalase and coagulase tests |
bacterial: 44.9% |
Enterococcus spp. (44.9%) S. aureus (15.9%), Klebsiella pneumoniae (14.5%) |
| Park 2022 [60] | non-woven, gauze, polyurethane (general population) |
1 day (3-6 h) up to 3 days |
109 | bacterial, fungal, (outer side and face-side samples) |
agar plates, 16S rRNA sampling, Gram staining |
bacteria: 168.6 ± 24.7 / face-side 36.0 ± 7.0 / outer side fungi: 4.6 ± 1.9 / face-side 6.1 ± 1.9 / outer side |
S. epidermidis, S. aureus, B. cereus, S. saprophyticus Aspergillus, Microsporum, Cladosporium |
| Sachdev 2020 [61] | surgical (HCW, dental practice) |
30 min | 240 | bacterial, fungal, (outside and inside samples) |
agar plates, Gram´s stain, lactophenol cotton blue, microscopic morphology |
bacteria: 48±26 / inside mask 180±110 / outside mask fungi: 14±6 / inside mask 32±13 / outside mask |
Staphylococcus spp. (26.35%), Pseudomonas spp. (17.82%), Streptococcus spp. (15.50%), Aspergillus (6.97%) |
| Yang 2018 [42] | N95 (general population) |
5+15 min | 2 | bacterial, (inner surface samples) |
agar plates, eye sighting and counting |
bacteria: 4.33 (5 min sample) 49 (15 min sample) |
not specified |
| Yousefimashouf 2023 [65] | surgical, N95 (HCW) |
≤2-8 h | 175 | bacterial, (inner and outer surface samples) |
immersion physiological serum, agar plates, analytical profile index kit |
Bacteria distribution on 471 positive isolates: 52.2 % (N95) 47.8 % (surgical) counts N95, inner vs outer: 128:118 counts surgical, inner vs. outer: 106:119 |
Coagulase-negative Staphylococcus (28%) Acinetobacter baumannii (20.8%), Pseudomonas aeruginosa (13.8%), E. coli (10.8%), S. aureus (10.1%), ß-Haemolytic Streptococcus (5.9%), Enterobacter (5.4%), Klebsiella (3.8%), Enterococcus (1.3%) |
Legend: Grey background = studies in healthcare settings; white background = studies on general population, n – the number of masks tested. *CFU (Colony Forming Units) per mask, resp. CFU/area, or alternatively percentage of positive tested masks (any contamination found, regardless of level). Abbreviations: HCW: Health care workers; MALDI-TOF MS: matrix-assisted laser desorption/ionization time of flight mass spectrometry; PBS: phosphate-buffered saline.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



