
Submitted:
22 December 2023
Posted:
26 December 2023
You are already at the latest version
Abstract
Presenting a rare case of adult-onset mature cystic teratoma of the spinal cord in the thoracolumbar spinal cord in a 54-year-old male whose chief complaint was lower back pain radiating to both legs while other findings were normal. X-ray images of the thoracolumbar spine showed early degenerative changes and unfused posterior elements noted in lower sacral vertebral levels. Magnetic resonance images of the lumbar spine showed a well-defined non-enhancing intramedullary altered intensity lesion noted at the level of conus at the L1-L2 vertebral level. The resected tumour was histopathologically diagnosed as a mature cystic teratoma. The patient's symptoms improved following the surgery.
Keywords:
Spinal cord
; Mature teratoma
; MRI
; Intramedullary
; Spinal tumours
Introduction
Teratomas are tumours derived from multipotential cells that originate during regular organ development, resulting in tissues that encompass a combination of ectodermal, endodermal, mesodermal germ layers and reproductive tissues.[1] Originating congenitally, these tumours exhibit a spectrum of differentiation, categorized as mature, immature, or malignant.[2] They manifest as unilocular or multilocular cystic growths, lined by squamous epithelium housing skin appendages like hair follicles, sweat glands, and sebaceous glands.[3]
Teratomas in the spinal region are exceptionally uncommon, representing only 0.15–0.18% of the total spinal tumour cases. Their occurrence is more prevalent in pediatric patients, comprising 5–10% of spinal tumours, as opposed to their infrequent manifestation in adults.[4,5,6,7,8] Among spinal teratomas, 40% reside within the spinal cord (intramedullary), while 60% are situated outside the spinal cord (extramedullary).[9]
Case Presentation
A 54-year-old male presented with persistent lower back pain for the past 25 days, accompanied by radiating discomfort to both thighs, with a predominant effect on the right side. The patient, however, denied any history of falls, trauma, sudden spine jerks, or heavy weight lifting. Clinical examination revealed the presence of paraspinal muscle spasm and tenderness specifically localized to the L3-L4 vertebral level. Notably, neurological examination results were within normal limits. Despite the absence of apparent external factors, the patient's symptoms, including back pain and difficulty walking, prompted medical attention and evaluation at the hospital.
X-ray showed early degenerative changes and the presence of unfused posterior elements was identified in the lower sacral vertebral levels.[Figure 1(A) and (B)] Moreover, a well-defined, non-enhancing intramedullary lesion with altered intensity was discovered at the conus level, specifically at the L1-L2 vertebral level. This lesion exhibited a complex pattern on various imaging sequences. On T1-weighted images, it presented as hyperintense with an internal hypointense solid component, indicative of an internal fat component, which was further confirmed by its suppression on fat-suppressed images. Conversely, on T2-weighted images, the lesion displayed heterogeneity, ranging from isointense to hyperintense, with an internal isointense solid component.
Importantly, T1, T2, and STIR (Short Tau Inversion Recovery) (Figure 2 and Figure 3) weighted sequences collectively suggested a mixed solid-cystic nature of the lesion. Notably, T1-weighted fat-suppressed images specifically highlighted the fatty component of the lesion, further emphasizing the presence of internal fat. Post-contrast imaging revealed an absence of enhancement in the lesion, indicating a lack of response to contrast administration.
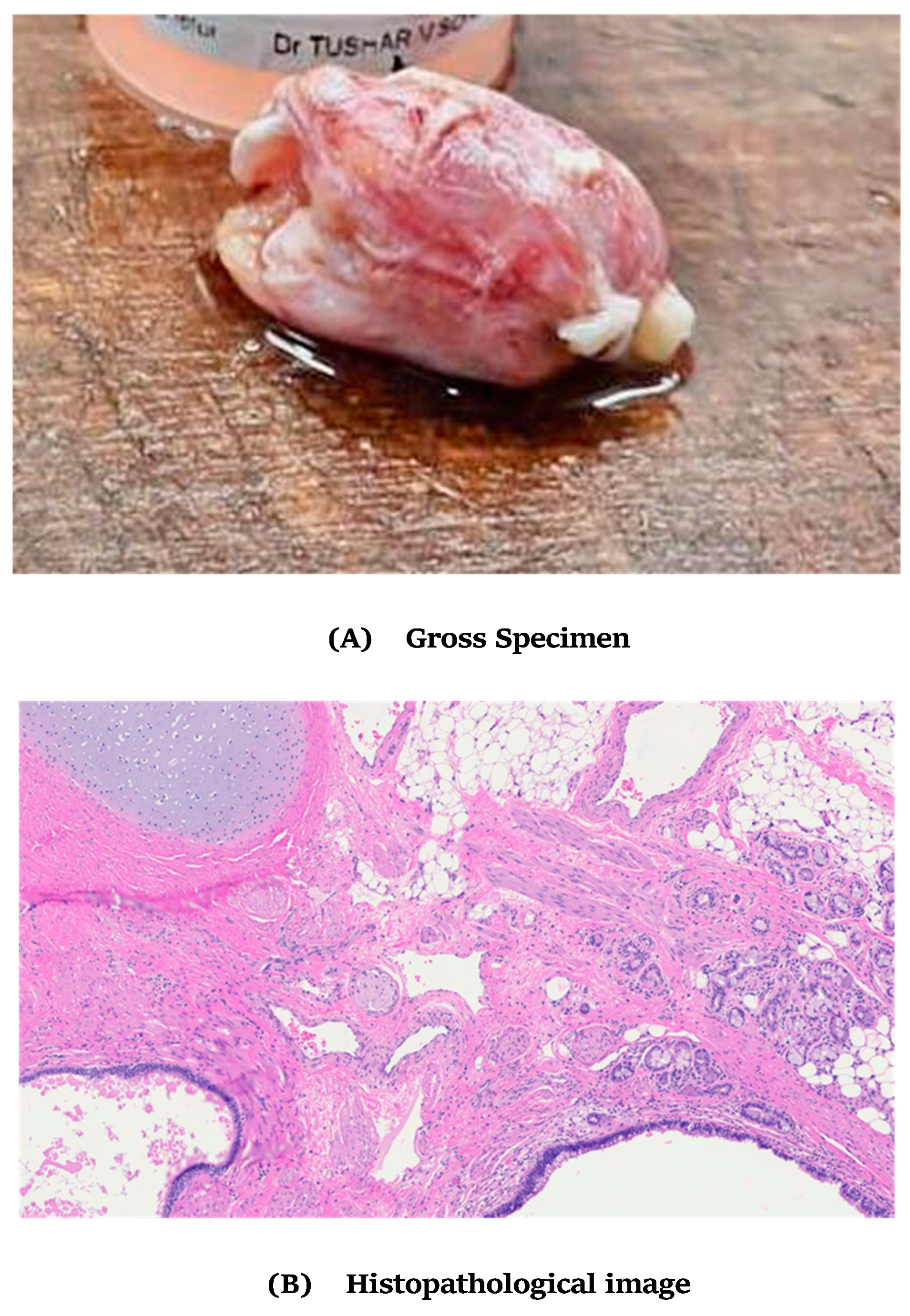
Subsequently, the patient underwent a surgical procedure at the neurosurgery department, during which the lesion was excised. The excised tissue was then forwarded for histopathological examination. The histological sections (Figure 4) reveal the presence of stratified squamous epithelium and transitional epithelium, along with adnexal structures such as sebaceous glands and sweat glands. Notably, mature adipose tissue, muscle tissue, glial tissue, respiratory-type mucosal glands, and blood vessels are observed. Additionally, keratin flakes are evident in the findings. These observations collectively suggest the diagnosis of a Mature Cystic Teratoma.
Discussion
Teratomas affecting the spinal cord are extremely rare, primarily identified in the sacrococcygeal and thoracolumbar regions.[10,11] Their classification hinges on the tumour's location, categorised as either extradural or intradural teratomas. Intradural teratomas, further classified as extramedullary or intramedullary based on their positioning, pose a diagnostic challenge with controversial pathogenesis. [9]
Two predominant theories, namely the dysembryonic theory and the misplaced germ cell theory, are central to discussions on the origin of intradural spinal teratomas. [12,13] The dysembryonic theory posits that these teratomas arise from pluripotent cells, and in the presence of a locally disrupted developmental environment, these cells undergo disordered differentiation. Specifically, when developmental irregularities occur within a primitive streak or a caudal cell mass, it leads to the development of spinal teratomas.[14] Conversely, the misplaced germ cell theory proposes that pluripotent primordial germ cells originating from the neural tube undergo mislocation during their migration from the yolk sac to the gonad, ultimately resulting in the formation of spinal teratomas.[12]
The differentiation of intramedullary teratomas into mature and immature forms depends on the extent of cell differentiation. A mature teratoma, characterized by well-differentiated cells, typically exhibits features associated with benign tumours. [11] Conversely, immature teratomas, housing primitive, immature, and undifferentiated cell characteristics, often manifest malignant tumour attributes.[3]
Imaging studies play a pivotal role in the diagnostic process. X-rays and CT scans are instrumental in revealing structural changes in the spinal bones induced by tumours, such as spinal canal widening, congenital nonunion, incomplete segmentation, and spina bifida.[15] However, MRI emerges as the most informative imaging modality for cervical intramedullary teratomas, offering insights into the tumour's location and size, hence, serves as a gold standard test. [11]
On MRI, these lesions present as lobular masses with homogeneous intermediate signal intensity arising from within the spinal cord, exhibiting indistinct enhancement with contrast medium. Some lesions may feature cystic cavities, prominently visible in MRI scans. [16]
Histopathological analysis of the resected tissue is imperative for establishing a definitive diagnosis and differentiating between mature and immature lesions. [3,6,9,10,17] A mature teratoma showcases a blend of well-differentiated tissues from the three germ layers: endoderm, mesoderm, and ectoderm.[3,11] In contrast, immature teratomas comprise poorly differentiated cells and tissues, potentially displaying primitive structures. The distinction of intramedullary teratomas from other lesions—such as astrocytomas, ependymomas, hemangioblastomas, schwannomas, neurofibromas, and enterogenous cysts—presents a diagnostic challenge due to structural similarities, necessitating a meticulous approach.[3,11]
Long-term prognosis, notably the likelihood of recurrence, is a key indicator closely tied to the tumour's nature—whether it is a mature or immature teratoma. Also, the potential for recurrence may be influenced by the ongoing debate within the medical community regarding the impact of subtotal resection.[6,15]
The intricacies of managing spinal teratomas underscore the importance of a multidisciplinary approach, integrating clinical, imaging, and histopathological findings to ensure accurate diagnosis, appropriate treatment, and informed prognostication.
Conclusion
When faced with adults presenting symptoms of lower back pain and bilateral radiculopathy, it becomes imperative to explore uncommon diagnostic considerations, including the potential presence of spinal cord tumours like mature teratoma. In such clinical scenarios, the utilization of MRI imaging proves indispensable for achieving an early and precise diagnosis. This imaging modality stands out as superior in effectively localizing spinal cord tumours, offering valuable insights into whether they are situated extramedullary or intramedullary. Moreover, MRI plays a pivotal role in discriminating against the nature of the tumour, facilitating the crucial differentiation between benign and malignant characteristics. In the comprehensive evaluation of lower back pain and bilateral radiculopathy in adults, the application of MRI becomes an indispensable tool, enabling a thorough assessment and informed decision-making concerning appropriate therapeutic interventions. This diagnostic approach significantly enhances the capacity to promptly identify and address potential spinal cord tumours, thereby ensuring a more efficient and targeted management strategy.
Funding
"None of the authors have a financial interest in any of the products, devices, or drugs mentioned in this manuscript.".
Conflicts of Interest
The authors of this report declare that they have no conflicts of interest to disclose.
Patient Consent
The patient in the study was provided with detailed information about the purpose, procedures, and confidentiality measures associated with the research. The patient was given ample time to review the informed consent, ask questions, and make an informed decision regarding their participation. Written informed consent was obtained from the patient prior to their involvement in the study. .
References
- Li Y, Yang B, Song L, Yan D. Mature teratoma of the spinal cord in adults: An unusual case. Oncol Lett. 2013, 6, 942–946. [Google Scholar] [CrossRef] [PubMed]
- Willis RA (Ed.) Atlas of Tumour Pathology, 1st edition; Armed Forces Institute of Pathology; Washington, District of Columbia, 1951; Teratomas; pp. 9–58. [Google Scholar]
- Ak H, Ulu MO, Sar M, Albayram S, Aydin S, Uzan M. Adult intramedullary mature teratoma of the spinal cord: a review of the literature illustrated with an unusual example. Acta Neurochir (Wien). 2006, 148, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen TB, Kernohan JW, Adson AW. PATHOLOGIC CLASSIFICATION, WITH SURGICAL CONSIDERATION, OF INTRASPINAL TUMORS. Ann Surg. 1940, 111, 513–530. [Google Scholar] [CrossRef] [PubMed]
- Baysefer A, Akay KM, Izci Y, Kayali H, Timurkaynak E. The clinical and surgical aspects of spinal tumours in children. Pediatr Neurol. 2004, 31, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Nonomura Y, Miyamoto K, Wada E, et al. Intramedullary teratoma of the spine: report of two adult cases. Spinal Cord. 2002, 40, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Sharma MC, Aggarwal M, Ralte AM, et al. Clinicopathological study of spinal teratomas. A series of 10 cases. J Neurosurg Sci. 2003, 47, 95–100. [Google Scholar]
- Krishna KK, Agarwal PA, Agarwal SI, Jain MM. Dermoid of the conus medullaris. J Clin Neurosci. 2004, 11, 796–797. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Cornejo VJ, Martínez-Pérez M, Polo-García LA, Martínez-Lage JF, Poza M. Cystic mature teratoma of the filum terminale in an adult. Case report and review of the literature. Neurocirugia (Astur). 2004, 15, 290–293. [Google Scholar] [CrossRef]
- Poeze M, Herpers MJ, Tjandra B, Freling G, Beuls EA. Intramedullary spinal teratoma presenting with urinary retention: case report and review of the literature. Neurosurgery. 1999, 45, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Sung KS, Sung SK, Choi HJ, Song YJ. Spinal intradural extramedullary mature cystic teratoma in an adult. J Korean Neurosurg Soc. 2008, 44, 334–337. [Google Scholar] [CrossRef] [PubMed]
- 12. REWCASTLE NB, FRANCOEUR J. TERATOMATOUS CYSTS OF THE SPINAL CANAL; WITH "SEX CHROMATIN" STUDIES. Arch Neurol 1964, 11, 91–99. [CrossRef]
- al-Sarraj ST, Parmar D, Dean AF, Phookun G, Bridges LR. Clinicopathological study of seven cases of spinal cord teratoma: a possible germ cell origin. Histopathology. 1998, 32, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Reddy CR, Rao KV, Jagabhandhu N. Intraspinal teratoma associated with diastematomyelia. Indian J Pathol Bacteriol. 1968, 11, 77–81. [Google Scholar]
- Makary R, Wolfson D, Dasilva V, Mohammadi A, Shuja S. Intramedullary mature teratoma of the cervical spinal cord at C1-2 associated with occult spinal dysraphism in an adult. Case report and review of the literature. J Neurosurg Spine. 2007, 6, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Hejazi N, Witzmann A. Spinal intramedullary teratoma with exophytic components: report of two cases and review of the literature. Neurosurg Rev. 2003, 26, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Cavazzani P, Ruelle A, Michelozzi G, Andrioli G. Spinal dermoid cysts originating intracranial fat drops causing obstructive hydrocephalus: case reports. Surg Neurol. 1995, 43, 466–470. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Early degenerative changes and unfused posterior elements were noted in lower sacral vertebral levels.
Figure 1.
Early degenerative changes and unfused posterior elements were noted in lower sacral vertebral levels.


Figure 2.
MRI Examination.


Figure 3.
T1, T2 and STIR weighted sequences show mixed solid cystic nature of the lesion.
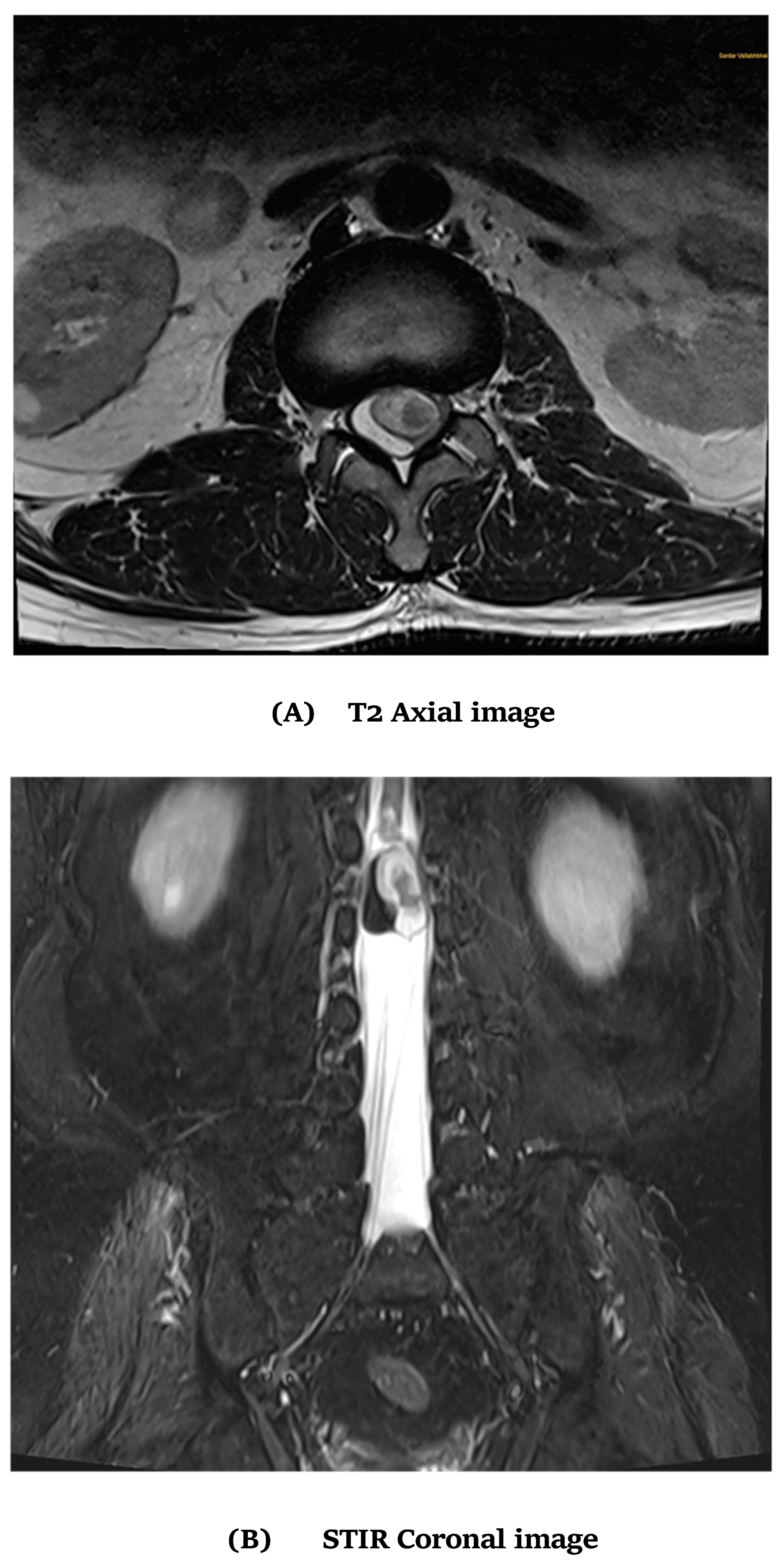
Figure 4.
Histological examination.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



