
Submitted:
25 December 2023
Posted:
28 December 2023
You are already at the latest version
Abstract
Richard Peto’s Paradox, first described in 1975 from an epidemiological perspective, established an inverse correlation between the probability of developing cancer in multicellular organisms and the number of cells. Larger animals exhibit fewer tumors compared to smaller ones, though exceptions exist. Mice are more susceptible to cancer than humans, while elephants and whales demonstrate significantly lower cancer prevalence rates than humans. How nature and evolution have addressed the issue of cancer in the animal kingdom remains largely unexplored.
In the field of medicine, much attention has been devoted to cancer predisposing genes, as they offer avenues for intervention, including blocking, downregulating, early diagnosis, and targeted treatment. Predisposing genes also tend to manifest clinically earlier and more aggressively, making them easier to identify. However, despite significant strides in modern medicine, the role of protective genes lags behind.
Identifying genes with a mild predisposing effect poses a significant challenge. Consequently, comprehending the protective function conferred by genes becomes even more elusive, and their very existence is subject to questioning. While the role of variable expressivity and penetrance defects of the same variant in a family is well-documented for many hereditary cancer syndromes, attempts to delineate the function of protective/modifier alleles have been restricted to a few instances.
In this review, we endeavor to elucidate the role of protective genes observed in the animal kingdom and within certain genetic syndromes that appear to act as cancer-resistant/repressor alleles. The ultimate goal is to discern why individuals, like Winston Churchill, managed to live up to 91 years of age, despite engaging in minimal physical activity, consuming large quantities of alcohol daily, and not abstaining from smoking.
Keywords:
cancer protective genes
; Down syndrome
; Laron syndrome
Introduction
In 1992, a famous best-selling book titled "Sharks Don't Get Cancer" caused a sensation among the general public by claiming that sharks are immune to cancer due to the properties of cartilage or its extract[1]. This pseudoscientific claim created significant controversy, particularly within the scientific community. The controversy reached its peak when a phase III clinical trial utilizing shark cartilage extract failed to demonstrate any significant benefits for patients in the treatment of cancer[2].
The notion of using miraculous nutraceuticals for cancer treatment goes back to the origins of medicine itself. In modern times, this pseudoscience often relied on specific biological mechanisms purported to mediate the claimed anti-cancer effects. The book "Sharks Don't Get Cancer" was notable for initiating a false claim based on a different approach: the observation, albeit somewhat valid, that a particular species appeared somehow resistant to cancer development. This concept was not entirely new, as epidemiologist Richard Peto had observed in 1970 that larger animals, contrary to common belief, experienced fewer instances of cancer than smaller animals[3,4]. Until then, cancer had been largely viewed as a linear consequence of having many cells, with one of them eventually accumulating a critical number of mutations, leading to transformation into a cancerous cell. Peto's paradox, as it came to be known, presented a puzzle that defied simple explanation. Various attempts were made to elucidate this phenomenon in biological terms, exploring factors such as the role of the immune system and different regulatory pathways. However, any explanation had to account for the fact that specific alleles or genes in larger animals could counteract the environmental factors influencing cancer cell proliferation. Evolution likely addressed this problem in diverse ways across different species.
The sequencing of the first human genome in 2000 ushered in a new era, allowing for the direct identification of genes or gene variants associated with specific phenotypes, first in humans, then in mice, and eventually in other living organisms. Initially, the genomic revolution primarily focused on identifying disease determinants, as most genes predisposing to cancer tended to manifest in more severe phenotypes, typically in younger individuals. These predisposing genes were relatively easy to discover, especially in cases where the phenotype ran in families, affecting younger individuals and resulting in multiple tumors within the same individual[5,6,7]. This led to the identification of many genes predisposing to cancer, which paved the way for the development of numerous targeted treatments now available[8,9,10]. Conversely, while one of the predisposing alleles was considered the disease allele, the other could be considered the healthy allele. However, studies concentrating on the genetic underpinnings of health lagged behind, partly due to the challenges in identifying "healthy" subjects and defining health in a quantifiable manner.
In a seminal paper, Topol described alleles in genes with a protective effect as those that, through a classical loss-of-function effect variant, could significantly influence the development of disease[11,12]. This rigorous definition proved instrumental in overcoming many of the challenges associated with discovering genetic determinants of health. Moreover, once the gene-allele combination was identified, it became possible to target the same molecule in an attempt to replicate the spontaneous phenotype observed in the healthy population. One of the most compelling examples was the discovery of loss-of-function mutations in PCSK9, which resulted in low levels of LDL cholesterol[13]. This discovery promptly led to the production of monoclonal antibodies against PCSK9, heralding a completely new form of treatment for hypercholesterolemia[14].
The widespread availability of sequencing analysis in families with a history of severe genetic diseases unveiled a new cohort of individuals referred to as "genetic superheroes" or “human knock-outs”[15,16]. These individuals carry dominant or recessive alleles for severe genetic conditions yet remain unaffected likely due to the presence of alleles in different genes, possibly in the same or different pathways, that counterbalance the phenotypic effects of the disease-causing allele. Thus far, alleles with a major effect explaining the “genetic superhero” phenotype have yet to be discovered.
According to the most recent data from the World Health Organization, the estimated global lifetime risk of cancer from birth to death was approximately 20% in 2020 [17]. It is estimated that only 20% of tumors are associated with a mutation in a cancer predisposition gene, while about 75%-80% of cancers are sporadic and result from a combination of multiple factors (environmental, lifestyle, or medical), with a significant role also attributed to genetic background [18].
Identifying alleles that confer protection against cancer is a much more complex endeavor. It is a common observation that many individuals, despite engaging in unhealthy lifestyles for a significant portion of their lives, somehow remain protected from the most severe consequences of cancer. Winston Churchill, known for his remarkable leadership during World War II, serves as a prominent example. Despite a documented lifestyle characterized by alcohol and cigar smoking, coupled with a lack of significant physical activity, Churchill lived to the age of 91, approximately 10 years longer than the average lifespan in the Western world nowadays[19].
While creating or retrospectively studying a cohort of individuals with characteristics similar to Churchill's would be challenging and ethically problematic, the best approach to studying the “cancer resistance or cancer protection” phenomenon often arises from extreme examples, as previously mentioned. In this review, we will outline the various approaches taken by researchers in the cancer field to investigate the determinants of health against cancer in well-known genetic syndromes such as Down syndrome, Laron syndrome and triplet diseases. Additionally, we will explore how evolution may have resolved Peto's paradox in animals, devising strategies to counteract large cell populations.
REDUCED CANCER RISK IN GENETIC SYNDROMIC CONDITIONS
Patients with syndromic conditions have always been a population described in numerous studies relating to the co-occurrence of other morbidities. Among these studies, attempts were made to establish whether there was an increased risk of cancer in this patient population. Over time, this higher risk has been established for numerous syndromic conditions with a known genetic basis, such as overgrowth syndromes [20], RASophaties [21], phacomatosis [22] and some microdeletions syndromes among which velocardiofacial syndrome [23].
Although the increased risk of tumors is a known and often quantified aspect of some genetic conditions and with a defined oncological surveillance, there is not as much data on the association between specific syndromic conditions and a lower risk of malignancies. However, this information would be very useful for understanding the possible protective effect of certain mutant alleles towards the development of cancer. Many genetics syndromes could be considered as a spontaneous genetic model where the genetic cause besides being the cause of the specific condition could have, as a secondary effect, a role in cancer protection and the causative gene/genes could have a protective role against cancer. The three main occurrences present in the literature are Down syndrome, Laron syndrome and the large chapter of dynamic mutations causing brain diseases.
Down syndrome
Down syndrome (DS) has been extensively studied in relation to the reduced incidence of solid tumors. From a superficial analysis, DS individuals have the same incidence of cancer as the rest of the normal population. However, a comprehensive study involving a large cohort of individuals with DS revealed a decreased risk of all major groups of malignant solid tumors, except for testicular cancer, while leukemia is more frequent especially during the pediatric stage[24]. Particularly noteworthy was the significantly lower occurrence of lung, skin, cervical, and female breast cancers[25].
This phenomenon is remarkable considering that individuals with DS possess several major risk factors that predispose them to cancer. These factors include hypotonia leading to reduced physical activity and obesity, accelerated organ aging, immunodeficiency, dysfunction in DNA repair systems resulting in increased DNA damage, mitotic chromosomal instability, mitochondrial alterations leading to high levels of reactive oxygen species (ROS), and elevated expression of multiple oncogenes located on chromosome 21[26].
Various hypotheses have been proposed to explain this lower risk of solid tumors, encompassing genetic dosage effects, overexpression of tumor suppressor/repressor genes, disrupted metabolism, impaired neurogenesis and angiogenesis, increased apoptosis, dysregulation of the immune system, and epigenetic abnormalities.
The ETS2 (V-Ets Avian Erythroblastosis Virus E26 Oncogene Homolog 2) gene, located on chromosome 21q22.3, regulates cell survival by controlling multiple targets such as TP53, P21, CYCLIND1, PRESENILIN1, and ICAM1[27]. Initially categorized as a proto-oncogene linked to acute megakaryoblastic leukemia when involved in somatic balanced translocations[26], a pivotal study utilizing mouse models of DS revealed that overexpression of ETS2 in APCmin mice prevented the development of intestinal tumors[27,28,29]. Despite its never being found mutated in tumor predisposing conditions, ETS2 appears to act more precisely as a tumor repressor rather than a suppressor gene. Notably, in the same study, different dosages of ETS2 alleles in mice corresponded closely to the incidence of intestinal tumors in the APCmin background[29].
Another gene, SOD1, located in 21q22.11, contributes to disrupted metabolism by overexpressing superoxide dismutase 1, leading to heightened ROS levels in neurons, lymphocytes, and fibroblasts. The imbalance between the cytosolic isoform of SOD1 (elevated) and glutathione peroxidase (normal) induces intracellular ROS accumulation, consequently causing oxidative stress, cell damage, and apoptosis[30,31].
Some studies suggest that the overall impact on tumors may relate to disrupted angiogenesis, as individuals with DS often exhibit frequent benign or indolent neoplasms, but significantly fewer aggressive tumors[32]. Among the potentially "protective genes" overexpressed in DS individuals interfering with angiogenesis, the prominent one is the COL18A1 gene.
The COL18A1 (Collagen Type XVIII Alpha 1 Chain) gene encodes the alpha chain of collagen XVIII, which, upon proteolysis, transforms into endostatin, a potent inhibitor of angiogenesis by inhibiting the pro-angiogenic factor VEGFA (vascular endothelial growth factor A). Endostatin levels are increased in individuals with DS[33]. Reduced angiogenesis could play a significant role in halting tumor progression, albeit of lesser importance in preventing its occurrence.
Special consideration must be given to the DYRK1A (Dual-specificity tYrosine-phosphorylation Regulated Kinase 1A) gene, which is expressed ubiquitously and encodes a protein kinase involved in various aspects of the DS phenotype. DYRK1A participates in the proliferation and differentiation of neuronal progenitor cells[34]. It also plays a dual role in tumorigenesis, being overexpressed in numerous cancers. DYRK1A promotes tumorigenesis[35] by phosphorylating the NFAT transcription factors[36], sustaining proliferation through upregulation of the RAS/MAPK signaling pathway, resisting apoptosis via caspase 9 phosphorylation, and enhancing angiogenesis through sustained accumulation of the VEGFR2 receptor[37]. However, its pro-cancer ability is counteracted by tumor repressor properties mediated by phosphorylation of TP53 serine 15[38], inducing cell cycle arrest in G0/G1, transcriptional suppression via the DREAM complex, and playing a central role in the double-strand break repair mechanism through RNF169 phosphorylation[39].
The seemingly contradictory aspects of the DS phenotype are mirrored by the dual role of DYRK1A. While mouse models exist that either overexpress[40] or lack Dyrk1a[41], most studies using these mice focus on the neurological aspects of DS. It would be intriguing to explore in various cancer models how Dyrk1a dosage affects cancer development and progression.
In terms of the immune system, individuals with DS exhibit increased susceptibility to respiratory infections. Some propose that DS represents a primary immunodeficiency due to global thymic hypofunction and lymphopenia of T and B cells. Paradoxically, despite this immune dysfunction predicting an increased cancer incidence, this does not occur. Some authors suggest this could be due to an increased proportion of γδT cells responsible for tumor immunosurveillance, favoring the early elimination of cancer cells[42]. However, the gene or genes responsible for this phenotype remain unidentified.
Regarding epigenetic alterations, individuals with DS display an aberrant pattern of methylation across the entire genome, with areas of both hypermethylation and hypomethylation[42]. Recurrent and reproducible epigenetic changes on chromosome 21 are observed in various tissues and cell subtypes.
Chromosome 21 contains up to 30 miRNAs, with five of them being overexpressed and linked to the DS phenotype: let-7c, miR-99a, miR-125b2, miR-155, and miR-802[43]. Their overexpression leads to reduced expression of proteins encoded by the targeted mRNAs. If some of these proteins were oncogenic, this would protect individuals with DS from developing tumors. The overexpression of these miRNAs may, to some extent, explain the genome-wide impact of the extra chromosome 21.
Concerning the genetic dosage effect, the overexpression of certain genes has been examined. The S100B (S100 Calcium Binding Protein Beta) gene encodes a calcium-binding protein secreted by glial cells that induces neural cell differentiation. Its overexpression in DS promotes neurodegeneration[44] but also exhibits a protective effect against neuroblastoma [35,36,37], correlating with the absence of neuroblastoma in children with DS.
Additionally, individuals with DS manifest a premature aging phenotype across various tissues, experiencing increased genotoxic stress and oxidative DNA damage. This effect could be attributed to the overexpression of DYRK1A and ETS2, which activate the DNA damage response in multiple cells, including stem cells, leading to a stem-cell exhaustion phenotype. Mitotic instability related to the extra chromosome 21 contributes to further somatic aneuploidy and somatic mosaicism. Normally, these events would lead to increased tumor growth. However, unlike other constitutional aneuploidies such as Klinefelter and Turner syndromes, DS individuals seems to exhibit rare segmental chromosomal instability and somatic chromosomal translocations, translating into a lower susceptibility to solid tumors in both pediatric and adult populations[45] While there is debate regarding whether patients with Down syndrome exhibit a higher or lower rate of chromosomal instability compared to those without the condition, it is established that individuals with DS have a significantly lower incidence of prostate cancer. In cases where translocations involving the ERG-TMPRSS251 genes are common in the early phases of prostate cancer, it's noteworthy that such occurrences are less frequent among individuals with Down syndrome. Both of these genes are located on chromosome 21[46].
Most studies concerning the protective effects of genes on chromosome 21 in DS have emphasized the concept that likely no single gene alone can exert a significant impact. This perspective takes into account that chromosome 21 also harbors a few genes known to have an oncogenic role or to stimulate cancer cell proliferation, growth, and metastasis[26].
Among the various genes described, DYRK1A plays a significant role, seemingly implicated in all major phenotypic aspects of DS. For this reason, numerous biological approaches have been initiated to modulate the kinase activity of this protein. Interestingly, this approach will help to elucidate the multifaceted roles of this protein in the various aspects of cancer biology discovered thus far (Figure 1).
Inhibition of tumor growth-promoting mechanisms: angiogenesis is suppressed due to heightened expression of COL18A1. Increased immune cell expression: The increased circulation of γδT cells, responsible for recognizing and suppressing tumor cells, plays a role in the lower tumor incidence. Additionally, the S100B protein, while contributing to the neurodegenerative process in DS patients, exhibits a contrasting effect in both human and murine neuroblastoma cell lines blocking tumor progression.
Laron Syndrome
Laron syndrome (LS) is an autosomal recessive disorder caused by dysfunction in the growth hormone receptor. It is characterized by marked short stature, typical facial features, delayed sexual development, and obesity resulting from the inability to synthesize insulin-like growth factor I (IGF1) in response to growth hormone (GH)[47,48]. In a study conducted by Laron et al., involving a cohort of 222 patients (comprising more than half of all known patients) with congenital IGF1 deficiency (169 of which had LS), none of these individuals had a history of cancer[49]. In contrast, 9–24% of their family members had a malignancy history. This near-complete protection against cancer was observed in individuals who underwent GH treatment for a certain period, suggesting that the protective role started early during prenatal life and persisted into adulthood. Heterozygous carriers did not exhibit any dosage effect of this protective mechanism. The relationship between elevated levels of IGF1 and cancer is well established, elucidating higher cancer rates in obese individuals[50,51]. Despite being obese, Laron patients remain free from cancer. Several studies on lymphoblastoid cell lines of LS revealed significant downregulation of genes including CYCLINA1, AKT3, SP1, SERPINB2, VESICAN, NPNT, and OR5H2, while a few genes such as UGT2B15, UGT2B17, and TXNIP, involved in xenobiotics detoxification and mitochondrial redox regulation, were upregulated[52].
In vitro studies on lymphoblastoid cells from LS patients indicated reduced proliferation, altered cell-cycle dynamics, decreased motility, increased apoptosis, resistance to oxidative stress challenges, and elevated expression of tumor suppressor genes. Notably, significantly reduced total and phosphorylated levels of IGF1R, a gene commonly overexpressed in various cancer types, were found in LS cells[52]. This reduction correlated with parallel decreases in the phosphorylation of downstream signaling molecules AKT and ERK, which are typical mediators in the IGF1 and insulin pathways. The reduction in expression and activation of components within the IGF1R signaling axis might underlie the decrease in the mitogenic potential of LS cells.
Moreover, the distinct representation of IGF-binding proteins (IGFBPs) in LS-derived lymphoblasts could elucidate the lower tumor incidence in these patients. Specifically, mRNA levels of IGFBP2, IGFBP5, and IGFBP6 were decreased in LS lymphoblastoids compared to healthy controls, while IGFBP3 mRNA levels were increased in LS cells. IGFBP3 has been recognized as an anti-oncogene in various tumors, consistent with its increased levels in LS. IGFBP2 is typically associated with promoting tumorigenesis and T-cell proliferation, while IGFBP5 and IGFBP6 promote T-cell migration and act as a chemotactic agent for T-cells. Therefore, the reductions observed in these IGFBPs align with the protective role against cancer[53].
The protective effect against cancer associated with a non-functioning insulin/IGF1 pathway was confirmed in C. elegans. Mutations in the insulin/IGF-I like signaling pathway primarily increase lifespan. When this allele was combined with a null allele for a tumor suppressor gene causing germline tumors, a complete absence of tumor development was observed, suggesting that the lack of IGF1 effectively conferred resistance to tumors [54]. Studies on mice treated with growth hormone receptor antagonists have demonstrated a lower incidence of carcinogenesis[55].
An animal model of LS, the 'Laron' mouse, was created by disrupting the Gh receptor gene (Ghr1). Similar to humans with LS, Laron mice exhibit low Igf1 and elevated Gh levels. Homozygous Ghr1 knockout mice displayed the severe phenotype typical of Laron syndrome. However, heterozygous mice for the Ghr1 axis showed minimal growth impairment, but presented an intermediate biochemical phenotype, with decreased Ghr and Gh binding protein expression and slightly reduced Igf1 levels[56]. Transgenic mice expressing human GH and/or an agonist of the Igf1 receptor showed an increased incidence of breast tumor development[57]. Conversely, mice carrying a transgene causing basal breast cancer in mice, when crossed with a tamoxifen-inducible conditional KO allele for the Gh1r receptor, demonstrated that the ablation of the Gh1r axis, after tumors reached a large size, completely inhibited the growth of breast cancer cells. These findings support the idea that growth hormone receptor antagonists may reduce the growth of cancer cells[58].
Further investigations on the Igf1r conditional KO mice aimed to elucidate the influential effects on cancer metastatic growth. Metastatic spread is a crucial aspect of cancer mortality. In one study, cells from the Lewis Lung Carcinoma cells (LLC) were transplanted into mice with a Igf1r KO background, meaning that the Igf1r axis was intact in cancer cells, but it was disrupted in the tumor microenvironment. The LLC, when transplanted into wild-type mice, led to multiple pulmonary metastases, while Igf1r KO mice showed a reduced tumor burden. The same effect was replicated with a subcutaneous injection of a B16 melanoma cell line[59]. These experiments in mice effectively demonstrated the potent inhibition of the Gh1r/Igf1 pathway, whether in cancer cells or in the supporting microenvironmental cells, leading to the inhibition of cancer cell growth, reduced inflammatory infiltration, enhanced apoptosis, reduced proliferation, and metastatic arrest. Ongoing trials with Gh1r/Igf1r antagonists will reveal their potential in this therapeutic approach, initiated from the clinical observation that LS patients do not develop cancer (Figure 2).
REDUCED CANCER RISK IN SYNDROMES WITH DYNAMIC MUTATIONS
Fragile X syndrome (FXS) is caused by the absence in brain of fragile X mental retardation protein (FMRP). This protein is ubiquitously expressed suggesting that, in addition to its effects in brain, it may have fundamental roles in other organs[60].
From the most comprehensive cumulative report of tumors in FXS obtained from 1988 to 2013 the rate of the most common malignancy in men, prostate, lung and colorectal were 6.8% and 4.5% and 2.3% respectively. That is significantly less than expected estimated cancer incidence by site in normal population (21%.14% and 8%) respectively. The male to female ratio was 1.58 to 1% and female incidence of the three most common cancer breast, lung, colorectal were 6.8%, 4.5%, 2.3% respectively in comparison with normal population (29%.13% and 8%)[61,62].
There is evidence that FMRP expression can be linked to cancer. FMRP as well as FMR1 mRNA levels correlate with prognostic indicators of aggressive breast cancer and lung metastasis[63]. In particular, FMRP overexpression in murine breast primary tumors enhances lung metastasis while its reduction has the opposite effect regulating cell spreading and invasion. FMRP binds mRNAs involved in epithelial mesenchymal transition (EMT) often a prerequisite for metastases formation and invasion including E-cadherin and Vimentin mRNAs, hallmarks of EMT and cancer progression [63].
There is a statistically significant downregulation of the WNT7A gene in FXS patients compared to healthy subjects for this reason the role of the WNT7A protein has also been extensively studied. Real-time PCR in FXS patients showed a real reduction in signal intensity in FXS males compared to healthy males[64]. The reduced expression of the WNT7A gene and its consequent downregulation of the β-catenin pathway may be related to a potential protection of FXS patients from cancer. Some of the target genes of this pathway, including MYC, JUN, CYCLIND, and PPARδ genes, showed moderately reduced expression in FXS patients compared to normal subjects [64].
Huntington’s disease (HD) is a progressive brain disorder caused by the pathological CAG expansion sequence in the HTT gene. Patients with Huntington’s disease exhibit a significantly lower cancer incidence, up to 80 percent less than the general population [65]. The analysis of data from 6540 subjects in the European Huntington’s disease network REGISTRY revealed a notably reduced age-standardized incidence rate, particularly evident in prostate and colorectal cancers, which exhibited the lowest rates[65]. Several potential factors may account for these lower cancer rates. Factors such as lower life expectancy might contribute, and there could be instances where cancer is underdiagnosed among individuals with HD, especially in later stages of the illness. This could occur as relevant signs or symptoms may be overlooked or overshadowed by HD symptoms, such as cachexia.
Turner et al.[66] conducted a study examining hospital admission records in England, revealing an increased rate of cancer diagnoses within the first year after admission for HD. Interestingly, they observed an overall decrease in the rate of cancers among HD patients, particularly pronounced when excluding the first year. This suggests that under-diagnosis might be less probable in this population, contrary to what might be expected. McNulty et al. also indicated a similar effect, reinforcing this perspective.
Notably, lung cancer was the only cancer found to occur as frequently in the HD population as in the general population, as reported by Turner et al. [66]. They attributed this finding to the higher rate of smoking among individuals with HD, a trend observed in various other psychotic conditions as well[67].
While the incidence of cancer is lower in HD patients than in age-matched controls, HD-causing CAG expansions of HTT accelerate the progression of breast tumors and the development of metastases in mouse models of breast cancer. In particular Thion et al[68], showed that the length of HTT CAG correlates with lower incidence of ovarian cancer in carriers of the BRCA2 mutation and that CAG repeat length in the long HTT allele can be a factor in metastasis in sporadic breast cancer (HER+ subtype) [68]. One of the possible mechanisms linking HD and cancer protection may be RNA toxicity. Murmann A.E. and colleagues constructed small interfering RNAs based on HTT CAG repeats; these siRNAs induce cell death in vitro in all tested cancer cell lines and slow down tumor growth in a preclinical mouse model of ovarian cancer with no signs of toxicity to the mice[69]. To indirectly confirm the role of RNA toxicity, in other neurodegenerative conditions with polyglutamine expansions it was also observed a lower cancer incidence (Figure 3).
In patients with HD, however, one of the molecular causes supposed at the basis of the lower incidence of tumors is the increased level of RNAs which have a toxic action not only towards neuronal cells, causing the typical clinical signs of the disease, but also toxicity to tumor cells.
HEREDITARY CANCER SYNDROMES
A hereditary cancer syndrome is a genetic predisposition to certain types of cancer, often with onset at an early age, caused by inherited pathogenic variants in one or more genes. The most common hereditary cancer syndromes include hereditary breast and ovarian cancer syndrome, Lynch syndrome, Li–Fraumeni syndrome, Cowden syndrome, Peutz–Jeghers syndrome, and hereditary diffuse gastric cancer. The genetic causes of most hereditary cancer syndromes have already been identified and well known [70].
However, determining the precise impact of factors designated as risk factors on increasing tumorigenesis risk, particularly in individuals with hereditary forms of cancer, is often challenging. While certain factors like age, weight, tobacco smoking, and chronic inflammation are well-known and measurable, others remain less understood, such as exposure to environmental toxic substances or dietary components. Pinpointing the exact influence of these risk factors is difficult, and identifying protective factors poses an even greater challenge. Nevertheless, the widespread use of comprehensive genetic tests has been instrumental in identifying genetic variables that can potentially alter tumor progression and confer a protective role.
Below are some studies that have tried to understand whether in a population at increased risk of cancer there are factors capable of modifying the clinical prognosis.
Hereditary Breast and Ovarian Cancer Syndrome
Hereditary Breast and Ovarian Cancer syndrome is a genetic condition that significantly increases the likelihood of developing breast, ovarian, and other cancers. Studies have indicated the involvement of β-adrenoceptors in tumor progression by regulating the immune system. Specifically, the gene ADRB2, encoding β2-AR, a member of the G protein-coupled receptor superfamily, has been identified as a potential protective gene in BRCA patients[71]. It appears to play a crucial role in modulating immune responses. The expression level of ADRB2 showed a positive correlation with immune cell infiltration in BRCA cancers. Notably, its specific expression in T cell subtypes and lower expression of ADRB2 often resulted in a poorer prognosis among BRCA patients[71].
The human DNA repair protein RAD52 (hRAD52) plays a critical role in various aspects of genome maintenance. One of its well-defined roles is as a key mediator of DNA double-strand break (DSB) repair through single-strand annealing (SSA).
The RAD52 p.Ser346Ter allele has been associated with a reduced risk of developing breast cancer in BRCA2 carriers, and to a lesser extent in BRCA1 carriers. Intriguingly, the expression of RAD52 p.Ser346Ter also diminished the stimulation of SSA observed upon BRCA2 depletion. This demonstrates the reciprocal roles of RAD52 and BRCA2 in regulating DSB repair via SSA. Immunofluorescence analysis revealed limited nuclear localization of the mutant protein compared to the wild-type, indicating that the reduced nuclear levels of RAD52 p.Ser346Ter might account for the impaired DSB repair through SSA. These findings suggest that deficiencies in RAD52-dependent DSB repair are associated with a decreased risk of tumors in BRCA2-mutation carriers[72,73].
Numerous GWAS studies have presented contradictory results regarding the protective role of SNPs in prevalent cancer types and cancer predisposition syndromes. The identification of major SNPs predisposing to certain effects is influenced by confounding factors, which likely impact the identification of protective alleles as well. Additionally, only a limited number of well-defined loss-of-function variants, as outlined by Topol, appear to mediate a comparable effect.
REDUCED CANCER RISK THROUGHOUT THE ANIMAL KINGDOM
Apart from various animal models the investigation in the cancer protective effect mediated by genes have been explored in the animal kingdom starting from the observation that some very large animals, such as elephants and whales with a very long lifespan present a very low rate of cancer. Another interesting species in this respect is represented by naked mole-rat, in spite being a rodent of the size of a mouse has an extremely long lifespan up to 30-40 years and it is extremely cancer resistant. These studies aim to determine whether different species, particularly those with longer lifespans than humans, can provide valuable insights into the functioning of the major pathways involved in tumorigenesis and how evolution solved the Peto’s paradox in those species.
Among the extensively studied animal models, elephants have garnered significant attention. This species exhibits an estimated cancer mortality of 4.81%, which is nearly half the observed mortality rate in humans, ranging from 11% to 25%[74]. This disparity has been associated with elephants possessing 20 copies of the Tp53 gene, which differ in length and sequence content[75]. Notably, in the Loxodonta Africana species, recent research has demonstrated that the 20 isoforms of the Tp53 gene feature distinct BOX-I Mdm2-binding motifs[76].
MDM2, an oncoprotein, primarily interacts with TP53, facilitating its degradation. This process ensures TP53 activation only when necessary or in response to cellular damage. The proposed mechanism behind the lower incidence of tumors in elephants revolves around the existence of diverse binding epitopes that interact with Mdm2. These distinct pools of Tp53 proteins result in an enhanced apoptotic response to DNA damage[76]. The variations in BOX-I sequences of Mdm2 hinder the interaction between Tp53 and Mdm2, thereby preventing Mdm2-mediated degradation of Tp53. As a result, Tp53 continues to fulfill its role as the guardian of the genome. Having multiple finely tuned copies of Tp53 prevents cells from attempting to repair irreparable DNA damage, thereby shifting the balance towards apoptosis. This multiple-copy configuration serves as an evolutionary fail-safe mechanism against the loss of a single gene copy, as can occur in humans.
Another species extensively scrutinized for low tumor incidence is the Greenland whale (Balaena mysticetus). This species boasts a remarkable lifespan exceeding 200 years and displays a lower tumor incidence despite its size, which entails a larger number of cells and significantly greater replication and repair mechanisms compared to humans.
In this long-lived species, heightened expression of certain proteins involved in oncogenesis, such as Ercc1 and Pcna, has been observed, suggesting a potential protective role against tumors. Ercc1, an endonuclease involved in DNA damage repair, specifically addresses cross-links and mediates nucleotide excision repair[77]. Activating mutations in the Ercc1 gene have been identified in Balaena mysticetus[78], while in mice, inactivating mutations in this gene are associated with a higher incidence of tumors[79].
Furthermore, an elevated expression of the Pcna gene has been observed in Greenland whales[78]. This gene encodes a protein that plays a crucial role in supporting polymerase activity during DNA replication and repair processes[79].
The Pcna protein holds significant importance in maintaining the polymerase's attachment to DNA, thus playing a fundamental role in DNA replication. In instances of DNA damage, this protein undergoes ubiquitination, triggering two DNA repair pathways: homologous recombination and nucleotide excision repair. The suggested mechanism behind the greater resistance to DNA damage and the subsequent lower incidence of tumors in Greenland whales involves the overexpression of the PCNA gene and, consequently, an increased production of the protein.
Similar patterns have been observed in other animal species where the expression levels of Pcna in specific organs show a close correlation with cell proliferation. For instance, in the livers of rats, lower levels of the Pcna protein have been linked to decreased levels of cell regeneration[80].
The naked mole-rat serves as a fascinating example for several reasons[81]. Firstly, it is a very small animal with an extraordinarily long lifespan for its size. Secondly, its longevity likely derives also from an incredible resistance to cancer mediated by a unique mechanism. While elephants and whales exploit some well-known genes for their cancer-resistant traits, Tp53 and Ercc1, both directly involved in DNA repair, apoptosis, and essential cell-cycle decisions, the scientific perspective shifts significantly when examining the naked mole-rat.
The molecule responsible for this unique resistance is a high molecular weight hyaluronan, a glycosaminoglycan (the primary non-protein molecule in the extracellular matrix), secreted by fibroblasts and produced abundantly by hyaluronan synthase 2 (Has2) during postnatal life[82]. The Has2 protein found in the naked mole-rat differs from the mouse and human sequences due to the substitution of two highly conserved asparagines with two serines. These alterations occur within the catalytic region, resulting in the enzyme from the naked mole-rat being highly processive and producing very high molecular weight hyaluronan.
Fibroblasts from naked mole-rats exhibit early contact inhibition, halting their growth at significantly lower densities. This mechanism is likely mediated by hyaluronan within the extracellular matrix, which directly interacts with Cd44 on the cell surface. This interaction induces early contact inhibition through p16INK4a, resulting in reduced cell proliferation, reduce hyperplasia and metastatic potential, and, on a systemic level, reduced inflammation. Additionally, it acts as an antioxidant, decreasing damage from reactive oxygen species to DNA and proteins, and makes cells more prone to apoptosis following the loss of tumor-suppressor genes[83,84].
The final confirmation that hyaluronan mediated these effects was achieved by increasing the lifespan of mice and enhancing their cancer resistance beyond that of control mice after expressing the naked mole-rat version of Hsa2. Increased expression of hyaluronan not only extended lifespan but also ensured a healthier one in mice[85](Figure 4).
Conclusions
Protective mechanisms against cancer mediated by genes are consistently found throughout the animal kingdom while the impact of environmental factors such as diet on this process is generally minimal across species, except for humans.
While many studies investigating the role of oncogenes and tumor suppressor genes have utilized the genetic tools available in mice, mice, due to their small size and shorter lifespans, are highly susceptible to cancer. In optimal laboratory conditions, most mice succumb to a lymphoproliferative disorder. It's widely acknowledged that mouse fibroblasts do not undergo replicative senescence; they require two mutations (Tp53 or Rb1 and activating Hras) to transform into cancerous cells, compared to human cells requiring at least five hits[86]. Additionally, mouse telomerase remains active in most somatic tissues. Their short lifespan and predisposition to cancer mean that any genetic intervention demonstrating the protective role of genes during tumorigenesis only showcases a proof-of-concept phenotype.
Consequently, the primary insight into the role of cancer protective genes has emerged from analyzing specific cases of human genetic syndromes. For instance, individuals with DS display resistance to the most common epithelial cancers. However, among the about 230 human genes, pinpointing the singular gene responsible or understanding if several genes collectively contribute to this protection poses a challenge. This complexity becomes clearer in monogenic conditions like LS, FXS or HD, where a particular protein or mechanism is actively involved.
Future studies that harness these mechanisms in a therapeutic context will confirm the validity of these assumptions. Furthermore, examining the role of evolution in safeguarding animals of various sizes from cancer, while also prolonging their lifespans, offers novel insights. However, replicating this intricate process in humans proves considerably more challenging. Nevertheless, understanding these evolutionary adaptations could provide new avenues for combating one of the leading causes of death and suffering in humans, offering potential breakthroughs in the field of cancer research.
References
- Lane, I.W.; Comac, L. Sharks Don’t Get Cancer, 1st edition.; Avery Pub Group: Garden City Park, N.Y, 1992; ISBN 978-0-89529-520-0. [Google Scholar]
- Loprinzi, C.L.; Levitt, R.; Barton, D.L.; Sloan, J.A.; Atherton, P.J.; Smith, D.J.; Dakhil, S.R.; Moore, D.F.; Krook, J.E.; Rowland, K.M.; et al. Evaluation of Shark Cartilage in Patients with Advanced Cancer: A North Central Cancer Treatment Group Trial. Cancer 2005, 104, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Peto, R.; Roe, F.J.; Lee, P.N.; Levy, L.; Clack, J. Cancer and Ageing in Mice and Men. Br J Cancer 1975, 32, 411–426. [Google Scholar] [CrossRef] [PubMed]
- Tollis, M.; Boddy, A.M.; Maley, C.C. Peto’s Paradox: How Has Evolution Solved the Problem of Cancer Prevention? BMC Biology 2017, 15, 60. [Google Scholar] [CrossRef] [PubMed]
- Futreal, P.A.; Liu, Q.; Shattuck-Eidens, D.; Cochran, C.; Harshman, K.; Tavtigian, S.; Bennett, L.M.; Haugen-Strano, A.; Swensen, J.; Miki, Y. BRCA1 Mutations in Primary Breast and Ovarian Carcinomas. Science 1994, 266, 120–122. [Google Scholar] [CrossRef] [PubMed]
- Miki, Y.; Swensen, J.; Shattuck-Eidens, D.; Futreal, P.A.; Harshman, K.; Tavtigian, S.; Liu, Q.; Cochran, C.; Bennett, L.M.; Ding, W. A Strong Candidate for the Breast and Ovarian Cancer Susceptibility Gene BRCA1. Science 1994, 266, 66–71. [Google Scholar] [CrossRef]
- Narod, S.A.; Foulkes, W.D. BRCA1 and BRCA2: 1994 and Beyond. Nat Rev Cancer 2004, 4, 665–676. [Google Scholar] [CrossRef] [PubMed]
- Fong, P.C.; Boss, D.S.; Yap, T.A.; Tutt, A.; Wu, P.; Mergui-Roelvink, M.; Mortimer, P.; Swaisland, H.; Lau, A.; O’Connor, M.J.; et al. Inhibition of Poly(ADP-Ribose) Polymerase in Tumors from BRCA Mutation Carriers. N Engl J Med 2009, 361, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Golan, T.; Hammel, P.; Reni, M.; Van Cutsem, E.; Macarulla, T.; Hall, M.J.; Park, J.-O.; Hochhauser, D.; Arnold, D.; Oh, D.-Y.; et al. Maintenance Olaparib for Germline BRCA-Mutated Metastatic Pancreatic Cancer. N Engl J Med 2019, 381, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Litton, J.K.; Rugo, H.S.; Ettl, J.; Hurvitz, S.A.; Gonçalves, A.; Lee, K.-H.; Fehrenbacher, L.; Yerushalmi, R.; Mina, L.A.; Martin, M.; et al. Talazoparib in Patients with Advanced Breast Cancer and a Germline BRCA Mutation. N Engl J Med 2018, 379, 753–763. [Google Scholar] [CrossRef]
- Harper, A.R.; Nayee, S.; Topol, E.J. Protective Alleles and Modifier Variants in Human Health and Disease. Nature Reviews Genetics 2015, 16, 689–701. [Google Scholar] [CrossRef]
- Nadeau, J.H.; Topol, E.J. The Genetics of Health. Nature Genetics 2006, 38, 1095–1098. [Google Scholar] [CrossRef]
- Raal, F.J.; Kallend, D.; Ray, K.K.; Turner, T.; Koenig, W.; Wright, R.S.; Wijngaard, P.L.J.; Curcio, D.; Jaros, M.J.; Leiter, L.A.; et al. Inclisiran for the Treatment of Heterozygous Familial Hypercholesterolemia. N Engl J Med 2020, 382, 1520–1530. [Google Scholar] [CrossRef]
- Giugliano, R.P.; Pedersen, T.R.; Park, J.-G.; De Ferrari, G.M.; Gaciong, Z.A.; Ceska, R.; Toth, K.; Gouni-Berthold, I.; Lopez-Miranda, J.; Schiele, F.; et al. Clinical Efficacy and Safety of Achieving Very Low LDL-Cholesterol Concentrations with the PCSK9 Inhibitor Evolocumab: A Prespecified Secondary Analysis of the FOURIER Trial. Lancet 2017, 390, 1962–1971. [Google Scholar] [CrossRef]
- Narasimhan, V.M.; Hunt, K.A.; Mason, D.; Baker, C.L.; Karczewski, K.J.; Barnes, M.R.; Barnett, A.H.; Bates, C.; Bellary, S.; Bockett, N.A.; et al. Health and Population Effects of Rare Gene Knockouts in Adult Humans with Related Parents. Science 2016, 352, 474–477. [Google Scholar] [CrossRef] [PubMed]
- Saleheen, D.; Natarajan, P.; Armean, I.M.; Zhao, W.; Rasheed, A.; Khetarpal, S.A.; Won, H.-H.; Karczewski, K.J.; O’Donnell-Luria, A.H.; Samocha, K.E.; et al. Human Knockouts and Phenotypic Analysis in a Cohort with a High Rate of Consanguinity. Nature 2017, 544, 235–239. [Google Scholar] [CrossRef]
- Zheng, R.; Wang, S.; Zhang, S.; Zeng, H.; Chen, R.; Sun, K.; Li, L.; Bray, F.; Wei, W. Global, Regional, and National Lifetime Probabilities of Developing Cancer in 2020. Sci Bull (Beijing), 2095; S2095-9273(23)00676-X. [Google Scholar] [CrossRef]
- Lu, Y.; Ek, W.E.; Whiteman, D.; Vaughan, T.L.; Spurdle, A.B.; Easton, D.F.; Pharoah, P.D.; Thompson, D.J.; Dunning, A.M.; Hayward, N.K.; et al. Most Common “sporadic” Cancers Have a Significant Germline Genetic Component. Hum Mol Genet 2014, 23, 6112–6118. [Google Scholar] [CrossRef] [PubMed]
- Launer, J. Winston Churchill and His Illnesses. Postgraduate Medical Journal 2021, 97, 135–136. [Google Scholar] [CrossRef] [PubMed]
- Manor, J.; Lalani, S.R. Overgrowth Syndromes-Evaluation, Diagnosis, and Management. Front Pediatr 2020, 8, 574857. [Google Scholar] [CrossRef]
- Recommendations for Cancer Surveillance in Individuals with RASopathies and Other Rare Genetic Conditions with Increased Cancer Risk | Clinical Cancer Research | American Association for Cancer Research. Available online: https://aacrjournals.org/clincancerres/article/23/12/e83/80230/Recommendations-for-Cancer-Surveillance-in (accessed on 30 October 2023).
- Tamura, R. Current Understanding of Neurofibromatosis Type 1, 2, and Schwannomatosis. Int J Mol Sci 2021, 22, 5850. [Google Scholar] [CrossRef]
- Campbell, I.M.; Sheppard, S.E.; Crowley, T.B.; McGinn, D.E.; Bailey, A.; McGinn, M.J.; Unolt, M.; Homans, J.F.; Chen, E.Y.; Salmons, H.I.; et al. What Is New with 22q? An Update from the 22q and You Center at the Children’s Hospital of Philadelphia. American Journal of Medical Genetics Part A 2018, 176, 2058–2069. [Google Scholar] [CrossRef]
- Hasle, H.; Friedman, J.M.; Olsen, J.H.; Rasmussen, S.A. Low Risk of Solid Tumors in Persons with Down Syndrome. Genetics in Medicine 2016, 18, 1151–1157. [Google Scholar] [CrossRef] [PubMed]
- Dey, N.; Krie, A.; Klein, J.; Williams, K.; McMillan, A.; Elsey, R.; Sun, Y.; Williams, C.; De, P.; Leyland-Jones, B. Down’s Syndrome and Triple Negative Breast Cancer: A Rare Occurrence of Distinctive Clinical Relationship. Int J Mol Sci 2017, 18, 1218. [Google Scholar] [CrossRef] [PubMed]
- Nižetić, D.; Groet, J. Tumorigenesis in Down’s Syndrome: Big Lessons from a Small Chromosome. Nat Rev Cancer 2012, 12, 721–732. [Google Scholar] [CrossRef] [PubMed]
- Wolvetang, E.J.; Bradfield, O.M.; Hatzistavrou, T.; Crack, P.J.; Busciglio, J.; Kola, I.; Hertzog, P.J. Overexpression of the Chromosome 21 Transcription Factor Ets2 Induces Neuronal Apoptosis. Neurobiol Dis 2003, 14, 349–356. [Google Scholar] [CrossRef] [PubMed]
- C, M.-B.; C, C.; C, T.; J, J.; C, M. [Trisomy 21 and Breast Cancer: A Genetic Abnormality Which Protects against Breast Cancer?]. Gynecologie, obstetrique & fertilite 2016, 44. [Google Scholar] [CrossRef]
- Sussan, T.E.; Yang, A.; Li, F.; Ostrowski, M.C.; Reeves, R.H. Trisomy Represses Apc(Min)-Mediated Tumours in Mouse Models of Down’s Syndrome. Nature 2008, 451, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Pagano, G.; Castello, G. Oxidative Stress and Mitochondrial Dysfunction in Down Syndrome. Adv Exp Med Biol 2012, 724, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Sinha, S. Anti-Oxidant Gene Expression Imbalance, Aging and Down Syndrome. Life Sci 2005, 76, 1407–1426. [Google Scholar] [CrossRef]
- Ryeom, S.; Baek, K.-H.; Zaslavsky, A. Down’s Syndrome: Protection against Cancer and the Therapeutic Potential of DSCR1. Future Oncol 2009, 5, 1185–1188. [Google Scholar] [CrossRef]
- High Serum Endostatin Levels in Down Syndrome: Implications for Improved Treatment and Prevention of Solid Tumours - PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/11781696/ (accessed on 21 December 2023).
- Hämmerle, B.; Elizalde, C.; Galceran, J.; Becker, W.; Tejedor, F.J. The MNB/DYRK1A Protein Kinase: Neurobiological Functions and Down Syndrome Implications. J Neural Transm Suppl 2003, 129–137. [Google Scholar] [CrossRef]
- Malinge, S.; Bliss-Moreau, M.; Kirsammer, G.; Diebold, L.; Chlon, T.; Gurbuxani, S.; Crispino, J.D. Increased Dosage of the Chromosome 21 Ortholog Dyrk1a Promotes Megakaryoblastic Leukemia in a Murine Model of Down Syndrome. J Clin Invest 2012, 122, 948–962. [Google Scholar] [CrossRef] [PubMed]
- Arron, J.R.; Winslow, M.M.; Polleri, A.; Chang, C.-P.; Wu, H.; Gao, X.; Neilson, J.R.; Chen, L.; Heit, J.J.; Kim, S.K.; et al. NFAT Dysregulation by Increased Dosage of DSCR1 and DYRK1A on Chromosome 21. Nature 2006, 441, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Rozen, E.J.; Roewenstrunk, J.; Barallobre, M.J.; Di Vona, C.; Jung, C.; Figueiredo, A.F.; Luna, J.; Fillat, C.; Arbonés, M.L.; Graupera, M.; et al. DYRK1A Kinase Positively Regulates Angiogenic Responses in Endothelial Cells. Cell Rep 2018, 23, 1867–1878. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Oh, Y.; Yoo, L.; Jung, M.-S.; Song, W.-J.; Lee, S.-H.; Seo, H.; Chung, K.C. Dyrk1A Phosphorylates P53 and Inhibits Proliferation of Embryonic Neuronal Cells. J Biol Chem 2010, 285, 31895–31906. [Google Scholar] [CrossRef] [PubMed]
- Litovchick, L.; Florens, L.A.; Swanson, S.K.; Washburn, M.P.; DeCaprio, J.A. DYRK1A Protein Kinase Promotes Quiescence and Senescence through DREAM Complex Assembly. Genes Dev 2011, 25, 801–813. [Google Scholar] [CrossRef] [PubMed]
- Martinez de Lagran, M.; Benavides-Piccione, R.; Ballesteros-Yañez, I.; Calvo, M.; Morales, M.; Fillat, C.; Defelipe, J.; Ramakers, G.J.A.; Dierssen, M. Dyrk1A Influences Neuronal Morphogenesis through Regulation of Cytoskeletal Dynamics in Mammalian Cortical Neurons. Cereb Cortex 2012, 22, 2867–2877. [Google Scholar] [CrossRef] [PubMed]
- Fotaki, V.; Dierssen, M.; Alcántara, S.; Martínez, S.; Martí, E.; Casas, C.; Visa, J.; Soriano, E.; Estivill, X.; Arbonés, M.L. Dyrk1A Haploinsufficiency Affects Viability and Causes Developmental Delay and Abnormal Brain Morphology in Mice. Mol Cell Biol 2002, 22, 6636–6647. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.E.; Xing, Z.; Do, C.; Pao, A.; Lee, E.J.; Krinsky-McHale, S.; Silverman, W.; Schupf, N.; Tycko, B. Genetic and Epigenetic Pathways in Down Syndrome: Insights to the Brain and Immune System from Humans and Mouse Models. Prog Brain Res 2020, 251, 1–28. [Google Scholar] [CrossRef]
- Brás, A.; Rodrigues, A.S.; Gomes, B.; Rueff, J. Down Syndrome and microRNAs. Biomed Rep 2018, 8, 11–16. [Google Scholar] [CrossRef]
- Shapiro, L.A.; Bialowas-McGoey, L.A.; Whitaker-Azmitia, P.M. Effects of S100B on Serotonergic Plasticity and Neuroinflammation in the Hippocampus in Down Syndrome and Alzheimer’s Disease: Studies in an S100B Overexpressing Mouse Model. Cardiovasc Psychiatry Neurol 2010, 2010, 153657. [Google Scholar] [CrossRef]
- Rethoré, M.-O.; Rouëssé, J.; Satgé, D. Cancer Screening in Adults with down Syndrome, a Proposal. European Journal of Medical Genetics 2020, 63, 103783. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.P.; Cooper, C.S. ETS Gene Fusions in Prostate Cancer. Nat Rev Urol 2009, 6, 429–439. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z. Syndrome of Familial Dwarfism and High Plasma Immunoreactive Growth Hormone. Isr J Med Sci 1974, 10, 1247–1253. [Google Scholar] [PubMed]
- Amselem, S.; Duquesnoy, P.; Attree, O.; Novelli, G.; Bousnina, S.; Postel-Vinay, M.C.; Goossens, M. Laron Dwarfism and Mutations of the Growth Hormone-Receptor Gene. N Engl J Med 1989, 321, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Shevah, O.; Laron, Z. Patients with Congenital Deficiency of IGF-I Seem Protected from the Development of Malignancies: A Preliminary Report. Growth Horm IGF Res 2007, 17, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Clayton, P.E.; Banerjee, I.; Murray, P.G.; Renehan, A.G. Growth Hormone, the Insulin-like Growth Factor Axis, Insulin and Cancer Risk. Nat Rev Endocrinol 2011, 7, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Guevara-Aguirre, J.; Balasubramanian, P.; Guevara-Aguirre, M.; Wei, M.; Madia, F.; Cheng, C.-W.; Hwang, D.; Martin-Montalvo, A.; Saavedra, J.; Ingles, S.; et al. Growth Hormone Receptor Deficiency Is Associated with a Major Reduction in Pro-Aging Signaling, Cancer, and Diabetes in Humans. Sci Transl Med 2011, 3, 70ra13. [Google Scholar] [CrossRef] [PubMed]
- Werner, H.; Lapkina-Gendler, L.; Achlaug, L.; Nagaraj, K.; Somri, L.; Yaron-Saminsky, D.; Pasmanik-Chor, M.; Sarfstein, R.; Laron, Z.; Yakar, S. Genome-Wide Profiling of Laron Syndrome Patients Identifies Novel Cancer Protection Pathways. Cells 2019, 8, 596. [Google Scholar] [CrossRef] [PubMed]
- Somri, L.; Sarfstein, R.; Lapkina-Gendler, L.; Nagaraj, K.; Laron, Z.; Bach, L.A.; Werner, H. Differential Expression of IGFBPs in Laron Syndrome-Derived Lymphoblastoid Cell Lines: Potential Correlation with Reduced Cancer Incidence. Growth Horm IGF Res 2018, 39, 6–12. [Google Scholar] [CrossRef]
- Pinkston, J.M.; Garigan, D.; Hansen, M.; Kenyon, C. Mutations That Increase the Life Span of C. Elegans Inhibit Tumor Growth. Science 2006, 313, 971–975. [Google Scholar] [CrossRef]
- Grimberg, A. Mechanisms by Which IGF-I May Promote Cancer. Cancer Biol Ther 2003, 2, 630–635. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Xu, B.C.; Maheshwari, H.G.; He, L.; Reed, M.; Lozykowski, M.; Okada, S.; Cataldo, L.; Coschigamo, K.; Wagner, T.E.; et al. A Mammalian Model for Laron Syndrome Produced by Targeted Disruption of the Mouse Growth Hormone Receptor/Binding Protein Gene (the Laron Mouse). Proc Natl Acad Sci U S A 1997, 94, 13215–13220. [Google Scholar] [CrossRef] [PubMed]
- ter Braak, B.; Siezen, C.; Speksnijder, E.N.; Koedoot, E.; van Steeg, H.; Salvatori, D.C.F.; van de Water, B.; van der Laan, J.W. Mammary Gland Tumor Promotion by Chronic Administration of IGF1 and the Insulin Analogue AspB10 in the p53R270H/+WAPCre Mouse Model. Breast Cancer Res 2015, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Unterberger, C.J.; McGregor, S.M.; Kopchick, J.J.; Swanson, S.M.; Marker, P.C. Mammary Tumor Growth and Proliferation Are Dependent on Growth Hormone in Female SV40 C3(1) T-Antigen Mice. Endocrinology 2022, 164, bqac174. [Google Scholar] [CrossRef] [PubMed]
- Alfaro-Arnedo, E.; López, I.P.; Piñeiro-Hermida, S.; Canalejo, M.; Gotera, C.; Sola, J.J.; Roncero, A.; Peces-Barba, G.; Ruíz-Martínez, C.; Pichel, J.G. IGF1R Acts as a Cancer-Promoting Factor in the Tumor Microenvironment Facilitating Lung Metastasis Implantation and Progression. Oncogene 2022, 41, 3625–3639. [Google Scholar] [CrossRef]
- Nobile, V.; Pucci, C.; Chiurazzi, P.; Neri, G.; Tabolacci, E. DNA Methylation, Mechanisms of FMR1 Inactivation and Therapeutic Perspectives for Fragile X Syndrome. Biomolecules 2021, 11, 296. [Google Scholar] [CrossRef]
- Schultz-Pedersen, S.; Hasle, H.; Olsen, J.H.; Friedrich, U. Evidence of Decreased Risk of Cancer in Individuals with Fragile X. Am J Med Genet 2001, 103, 226–230. [Google Scholar] [CrossRef]
- Sund, R.; Pukkala, E.; Patja, K. Cancer Incidence among Persons with Fragile X Syndrome in Finland: A Population-Based Study. J Intellect Disabil Res 2009, 53, 85–90. [Google Scholar] [CrossRef]
- Lucá, R.; Averna, M.; Zalfa, F.; Vecchi, M.; Bianchi, F.; La Fata, G.; Del Nonno, F.; Nardacci, R.; Bianchi, M.; Nuciforo, P.; et al. The Fragile X Protein Binds mRNAs Involved in Cancer Progression and Modulates Metastasis Formation. EMBO Mol Med 2013, 5, 1523–1536. [Google Scholar] [CrossRef]
- Gene Expression Profiling Identifies WNT7A as a Possible Candidate Gene for Decreased Cancer Risk in Fragile X Syndrome Patients - PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/20470940/ (accessed on 30 October 2023).
- McNulty, P.; Pilcher, R.; Ramesh, R.; Necuiniate, R.; Hughes, A.; Farewell, D.; Holmans, P.; Jones, L. ; REGISTRY Investigators of the European Huntington’s Disease Network Reduced Cancer Incidence in Huntington’s Disease: Analysis in the Registry Study. J Huntingtons Dis 2018, 7, 209–222. [Google Scholar] [CrossRef]
- Turner, M.R.; Goldacre, R.; Goldacre, M.J. Reduced Cancer Incidence in Huntington’s Disease: Record Linkage Study Clue to an Evolutionary Trade-Off? Clin Genet 2013, 83, 588–590. [Google Scholar] [CrossRef] [PubMed]
- Ehret, J.C.; Day, P.S.; Wiegand, R.; Wojcieszek, J.; Chambers, R.A. Huntington Disease as a Dual Diagnosis Disorder: Data from the National Research Roster for Huntington Disease Patients and Families. Drug Alcohol Depend 2007, 86, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Thion, M.S.; Tézenas du Montcel, S.; Golmard, J.-L.; Vacher, S.; Barjhoux, L.; Sornin, V.; Cazeneuve, C.; Bièche, I.; Sinilnikova, O.; Stoppa-Lyonnet, D.; et al. CAG Repeat Size in Huntingtin Alleles Is Associated with Cancer Prognosis. Eur J Hum Genet 2016, 24, 1310–1315. [Google Scholar] [CrossRef] [PubMed]
- Murmann, A.E.; Gao, Q.Q.; Putzbach, W.E.; Patel, M.; Bartom, E.T.; Law, C.Y.; Bridgeman, B.; Chen, S.; McMahon, K.M.; Thaxton, C.S.; et al. Small Interfering RNAs Based on Huntingtin Trinucleotide Repeats Are Highly Toxic to Cancer Cells. EMBO Rep 2018, 19, e45336. [Google Scholar] [CrossRef] [PubMed]
- Garutti, M.; Foffano, L.; Mazzeo, R.; Michelotti, A.; Da Ros, L.; Viel, A.; Miolo, G.; Zambelli, A.; Puglisi, F. Hereditary Cancer Syndromes: A Comprehensive Review with a Visual Tool. Genes (Basel) 2023, 14, 1025. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Chen, L.; Yang, A.; Lv, Z.; Xiong, M.; Shan, C. ADRB2 Is a Potential Protective Gene in Breast Cancer by Regulating Tumor Immune Microenvironment. Transl Cancer Res 2021, 10, 5280–5294. [Google Scholar] [CrossRef]
- Adamson, A.W.; Ding, Y.C.; Mendez-Dorantes, C.; Bailis, A.M.; Stark, J.M.; Neuhausen, S.L. The RAD52 S346X Variant Reduces Risk of Developing Breast Cancer in Carriers of Pathogenic Germline BRCA2 Mutations. Mol Oncol 2020, 14, 1124–1133. [Google Scholar] [CrossRef] [PubMed]
- Biswas, K.; Sharan, S.K. RAD52 S346X Variant Reduces Breast Cancer Risk in BRCA2 Mutation Carriers. Mol Oncol 2020, 14, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Abegglen, L.M.; Caulin, A.F.; Chan, A.; Lee, K.; Robinson, R.; Campbell, M.S.; Kiso, W.K.; Schmitt, D.L.; Waddell, P.J.; Bhaskara, S.; et al. Potential Mechanisms for Cancer Resistance in Elephants and Comparative Cellular Response to DNA Damage in Humans. JAMA 2015, 314, 1850. [Google Scholar] [CrossRef]
- Vazquez, J.M.; Sulak, M.; Chigurupati, S.; Lynch, V.J. A Zombie LIF Gene in Elephants Is Upregulated by TP53 to Induce Apoptosis in Response to DNA Damage. Cell Rep 2018, 24, 1765–1776. [Google Scholar] [CrossRef]
- Padariya, M.; Jooste, M.-L.; Hupp, T.; Fåhraeus, R.; Vojtesek, B.; Vollrath, F.; Kalathiya, U.; Karakostis, K. The Elephant Evolved P53 Isoforms That Escape MDM2-Mediated Repression and Cancer. Mol Biol Evol 2022, 39, msac149. [Google Scholar] [CrossRef] [PubMed]
- Formica, V.; Doldo, E.; Antonetti, F.R.; Nardecchia, A.; Ferroni, P.; Riondino, S.; Morelli, C.; Arkenau, H.T.; Guadagni, F.; Orlandi, A.; et al. Biological and Predictive Role of ERCC1 Polymorphisms in Cancer. Critical Reviews in Oncology/Hematology 2017, 111, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Keane, M.; Semeiks, J.; Webb, A.E.; Li, Y.I.; Quesada, V.; Craig, T.; Madsen, L.B.; van Dam, S.; Brawand, D.; Marques, P.I.; et al. Insights into the Evolution of Longevity from the Bowhead Whale Genome. Cell Rep 2015, 10, 112–122. [Google Scholar] [CrossRef] [PubMed]
- Hoege, C.; Pfander, B.; Moldovan, G.-L.; Pyrowolakis, G.; Jentsch, S. RAD6-Dependent DNA Repair Is Linked to Modification of PCNA by Ubiquitin and SUMO. Nature 2002, 419, 135–141. [Google Scholar] [CrossRef]
- Tanno, M.; Ogihara, M.; Taguchi, T. Age-Related Changes in Proliferating Cell Nuclear Antigen Levels. Mech Ageing Dev 1996, 92, 53–66. [Google Scholar] [CrossRef] [PubMed]
- Gorbunova, V.; Bozzella, M.J.; Seluanov, A. Rodents for Comparative Aging Studies: From Mice to Beavers. Age (Dordr) 2008, 30, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Azpurua, J.; Hine, C.; Vaidya, A.; Myakishev-Rempel, M.; Ablaeva, J.; Mao, Z.; Nevo, E.; Gorbunova, V.; Seluanov, A. High-Molecular-Mass Hyaluronan Mediates the Cancer Resistance of the Naked Mole Rat. Nature 2013, 499, 346–349. [Google Scholar] [CrossRef] [PubMed]
- Takasugi, M.; Ohtani, N.; Takemura, K.; Emmrich, S.; Zakusilo, F.T.; Yoshida, Y.; Kutsukake, N.; Mariani, J.N.; Windrem, M.S.; Chandler-Militello, D.; et al. CD44 Correlates with Longevity and Enhances Basal ATF6 Activity and ER Stress Resistance. Cell Rep 2023, 42, 113130. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Azpurua, J.; Ke, Z.; Augereau, A.; Zhang, Z.D.; Vijg, J.; Gladyshev, V.N.; Gorbunova, V.; Seluanov, A. INK4 Locus of the Tumor-Resistant Rodent, the Naked Mole Rat, Expresses a Functional P15/P16 Hybrid Isoform. Proc Natl Acad Sci U S A 2015, 112, 1053–1058. [Google Scholar] [CrossRef]
- Zhang, Z.; Tian, X.; Lu, J.Y.; Boit, K.; Ablaeva, J.; Zakusilo, F.T.; Emmrich, S.; Firsanov, D.; Rydkina, E.; Biashad, S.A.; et al. Increased Hyaluronan by Naked Mole-Rat Has2 Improves Healthspan in Mice. Nature 2023, 621, 196–205. [Google Scholar] [CrossRef]
- Rangarajan, A.; Hong, S.J.; Gifford, A.; Weinberg, R.A. Species- and Cell Type-Specific Requirements for Cellular Transformation. Cancer Cell 2004, 6, 171–183. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The pathways involved in protecting individuals with DS against tumors. Several mechanisms contributing to the lower incidence of tumors in these patients have been proposed. Increased TP53 apoptotic response: This is mediated by heightened expression of genes located on chromosome 21. These genes boost the transcription of TP53, ETS2, SOD1, and DYRK1A. Enhanced activation of DNA damage repair mechanisms leads to an increase in the repair of double strand breaks, facilitated by elevated DYRK1A expression. The overexpression of the DYRK1A gene in DS patients leads to increased activation of the DREAM complex. This complex modulates the expression of genes involved in regulating the cell cycle, thereby reducing cell proliferation.
Figure 1.
The pathways involved in protecting individuals with DS against tumors. Several mechanisms contributing to the lower incidence of tumors in these patients have been proposed. Increased TP53 apoptotic response: This is mediated by heightened expression of genes located on chromosome 21. These genes boost the transcription of TP53, ETS2, SOD1, and DYRK1A. Enhanced activation of DNA damage repair mechanisms leads to an increase in the repair of double strand breaks, facilitated by elevated DYRK1A expression. The overexpression of the DYRK1A gene in DS patients leads to increased activation of the DREAM complex. This complex modulates the expression of genes involved in regulating the cell cycle, thereby reducing cell proliferation.
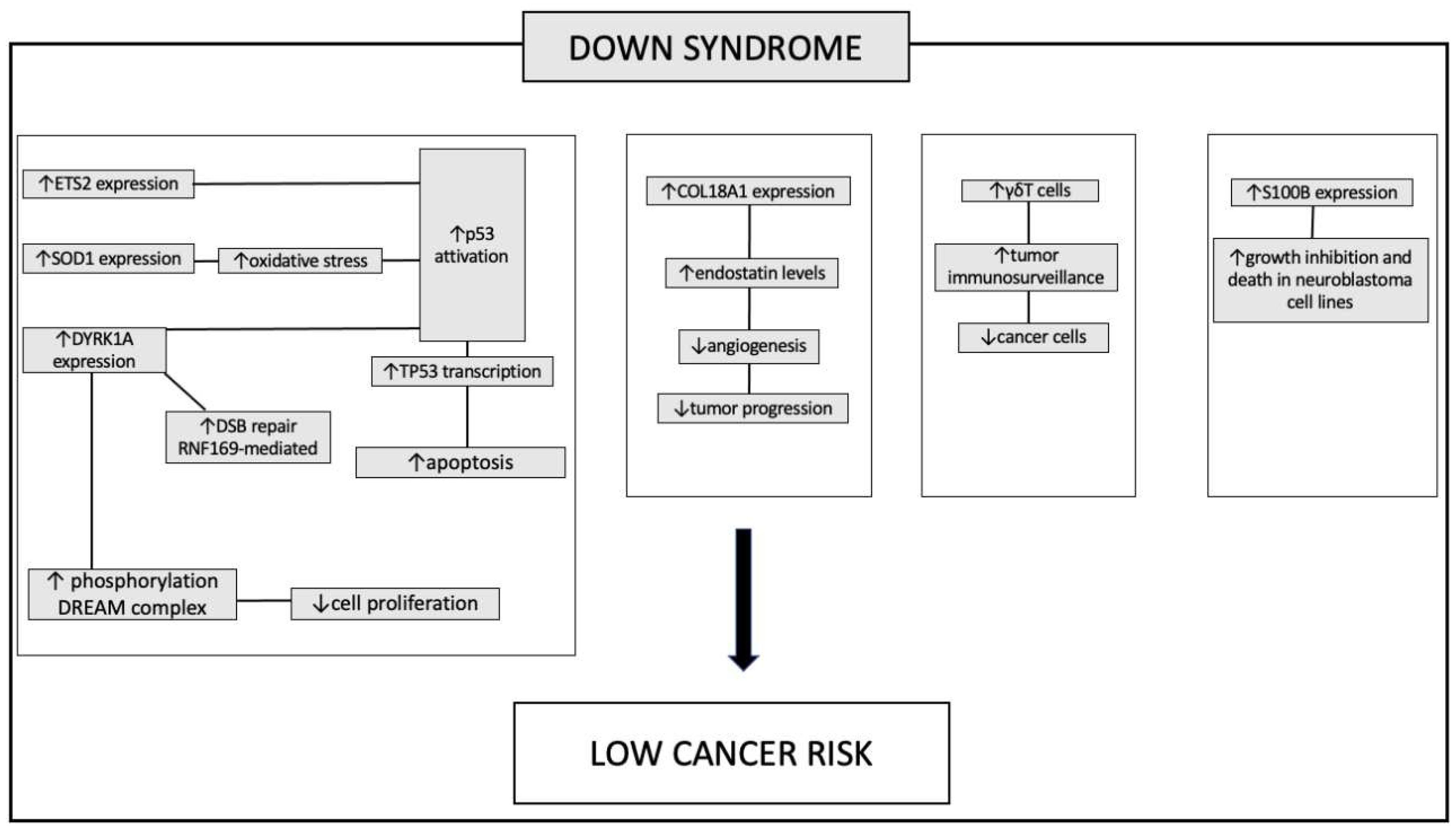
Figure 2.
The pathway involved in protection against tumor in patients with Laron syndrome. During normal development growth hormone (GH) is typically secreted by the pituitary gland and exerts its effects through the growth hormone receptor (GHR) presents in various organs and cell types. Insulin-like growth factor 1 (IGF1) is released into the bloodstream, reaching different target organs and tissues. IGF1 negatively regulates GH secretion. However, in Laron syndrome, mutations in the GHR lead to increased GH levels while IGF1 levels remain very low. This particular combination mediates a protective effect against cancer despite these patients being obese. In cancer cases, a coordinated disruption of this axis at various levels results in markedly elevated IGF1 levels, thereby increasing downstream signaling.
Figure 2.
The pathway involved in protection against tumor in patients with Laron syndrome. During normal development growth hormone (GH) is typically secreted by the pituitary gland and exerts its effects through the growth hormone receptor (GHR) presents in various organs and cell types. Insulin-like growth factor 1 (IGF1) is released into the bloodstream, reaching different target organs and tissues. IGF1 negatively regulates GH secretion. However, in Laron syndrome, mutations in the GHR lead to increased GH levels while IGF1 levels remain very low. This particular combination mediates a protective effect against cancer despite these patients being obese. In cancer cases, a coordinated disruption of this axis at various levels results in markedly elevated IGF1 levels, thereby increasing downstream signaling.
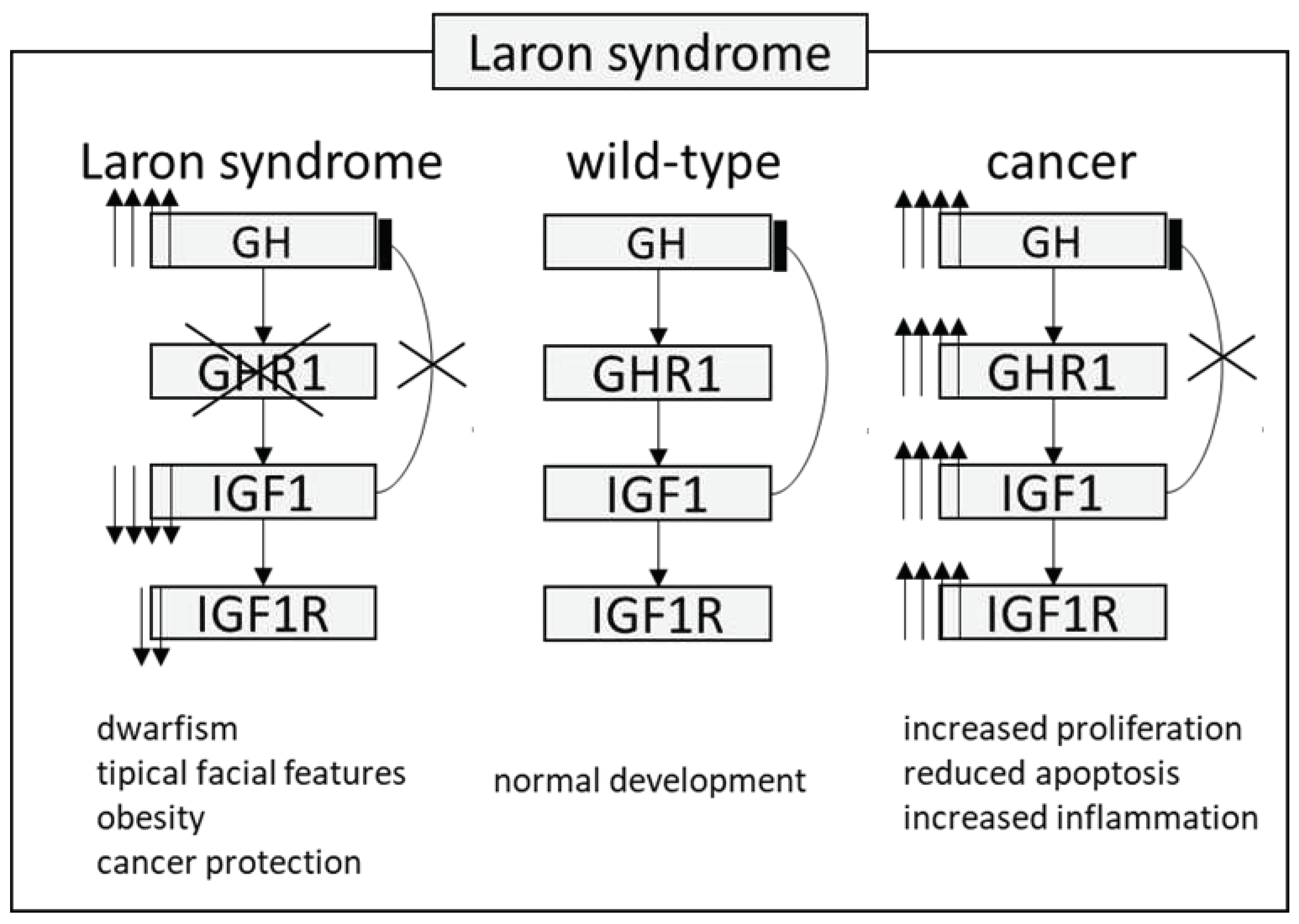
Figure 3.
Pathways involved in protection against tumor in patient with dynamic mutations: Fragile X syndrome (FXS) and Huntington disease (HD). In patients with FXS, increased levels of the FMRP (fragile X mental retardation 1 protein) appear to alter the expression of proteins that promote tumor progression. In particular, the typical invasiveness of tumor cells is inhibited through the decreased expression of the vimentin protein and cell adhesion is instead promoted thanks to the increased expression of E-cadherin. Another mechanism underlying the lower incidence of cancer in patients with FXS is the decreased expression of the WNT7A (WNT family member 7A) gene which, through downregulation of the beta-catenin pathway, prevents the invasiveness of tumor cells.
Figure 3.
Pathways involved in protection against tumor in patient with dynamic mutations: Fragile X syndrome (FXS) and Huntington disease (HD). In patients with FXS, increased levels of the FMRP (fragile X mental retardation 1 protein) appear to alter the expression of proteins that promote tumor progression. In particular, the typical invasiveness of tumor cells is inhibited through the decreased expression of the vimentin protein and cell adhesion is instead promoted thanks to the increased expression of E-cadherin. Another mechanism underlying the lower incidence of cancer in patients with FXS is the decreased expression of the WNT7A (WNT family member 7A) gene which, through downregulation of the beta-catenin pathway, prevents the invasiveness of tumor cells.
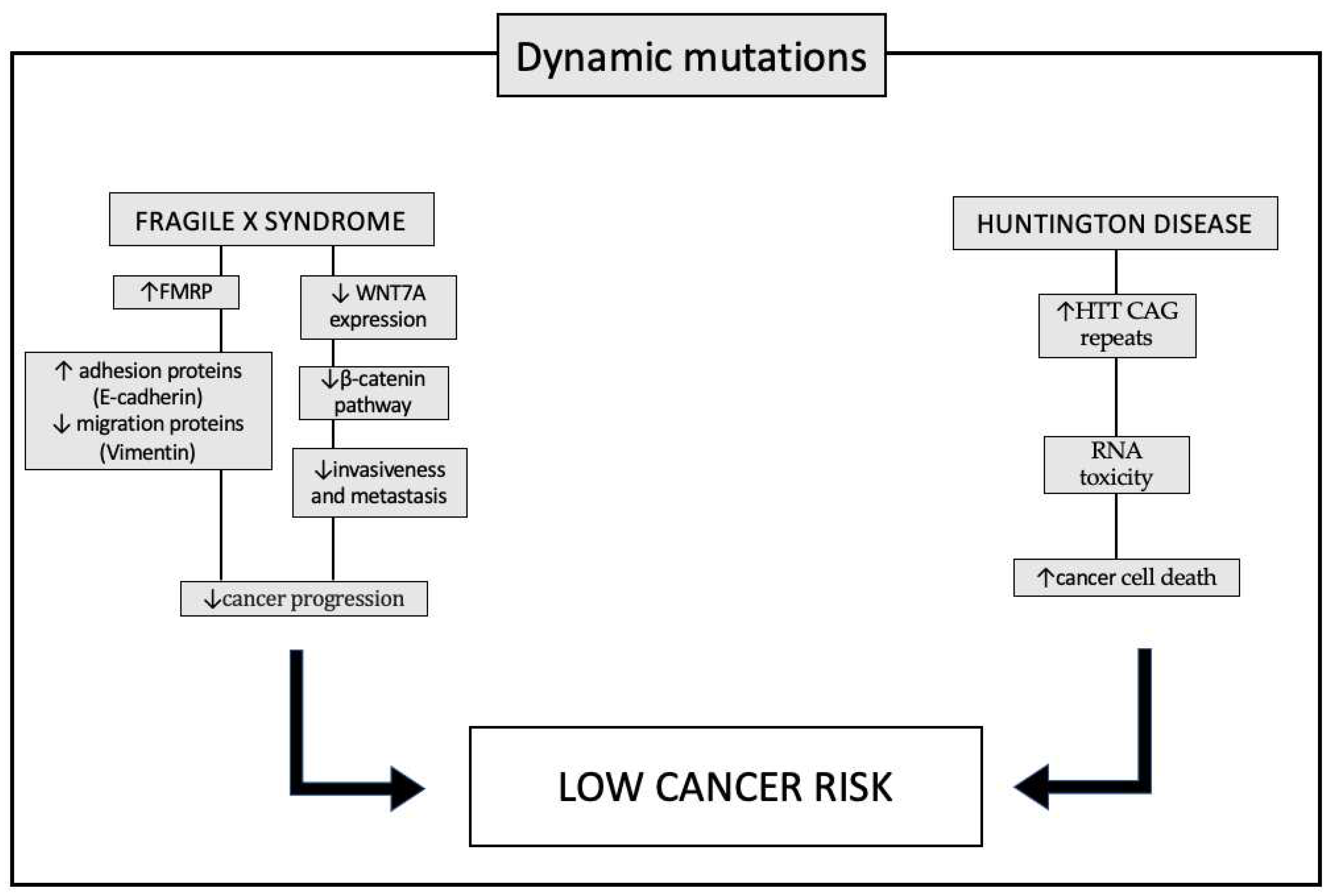
Figure 4.
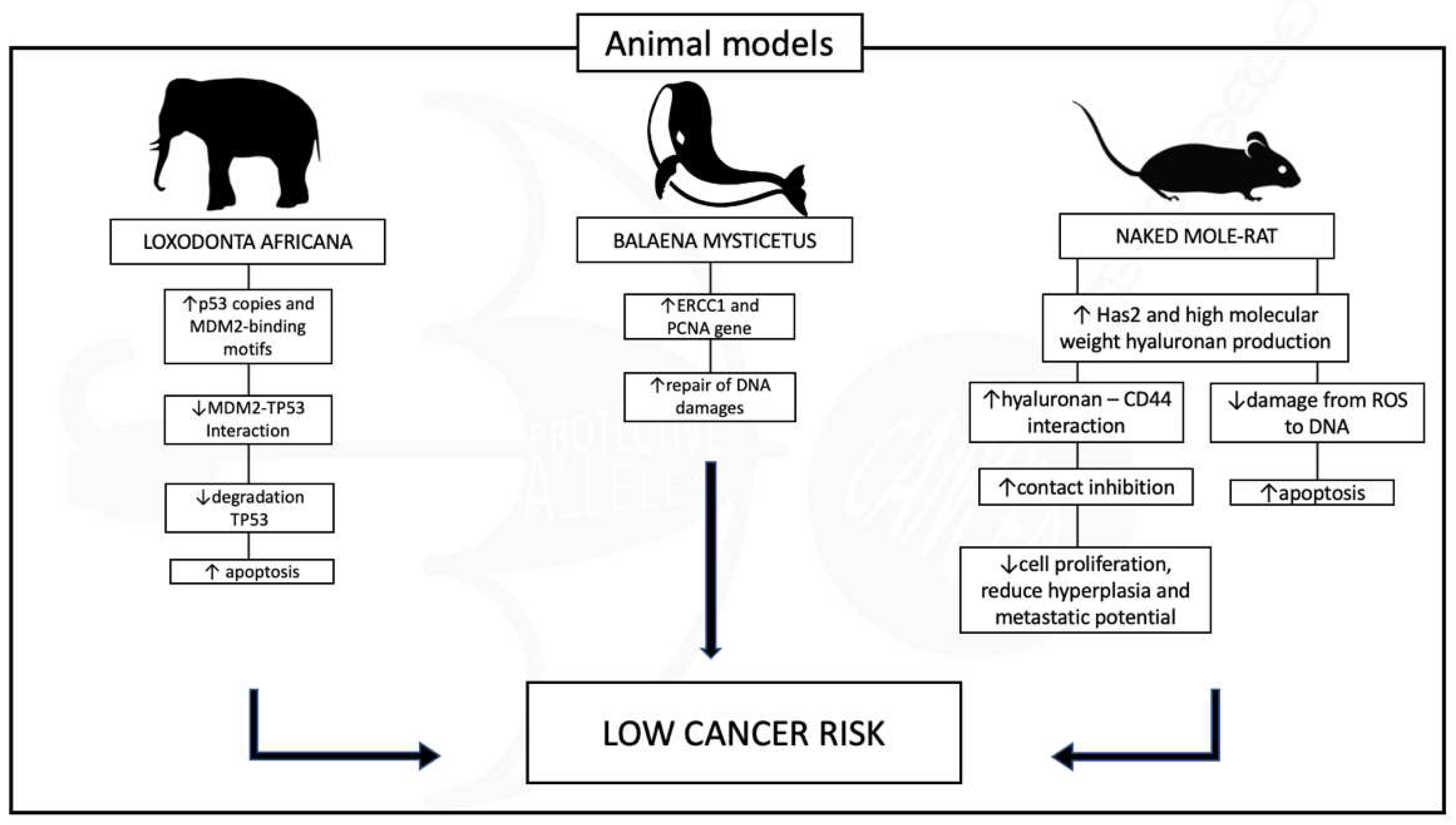
Different pathways play a role in protecting animals against tumors. In elephants, the gene Tp53 undergoes amplification, increasing up to 20 copies. The finely regulated multiple copies of this gene activated by DNA damage, prevent the transformation of cells with significant DNA damage into cancerous cells by inducing apoptosis. Similarly, in whales, a comparable effect is achieved through the overexpression of the ERCC1 protein. This overexpression enhances the whales' capability to repair DNA, contributing to a heightened defense against cancer. Conversely, the naked mole-rat utilizes a completely distinct mechanism for tumor protection. These rodents synthesize an exceptionally large hyaluronan molecule, which induces early contact inhibition in fibroblasts. This process leads to reduced cell proliferation, diminished hyperplasia, decreased inflammation, and a lowered potential for metastasis.
Figure 4.
Different pathways play a role in protecting animals against tumors. In elephants, the gene Tp53 undergoes amplification, increasing up to 20 copies. The finely regulated multiple copies of this gene activated by DNA damage, prevent the transformation of cells with significant DNA damage into cancerous cells by inducing apoptosis. Similarly, in whales, a comparable effect is achieved through the overexpression of the ERCC1 protein. This overexpression enhances the whales' capability to repair DNA, contributing to a heightened defense against cancer. Conversely, the naked mole-rat utilizes a completely distinct mechanism for tumor protection. These rodents synthesize an exceptionally large hyaluronan molecule, which induces early contact inhibition in fibroblasts. This process leads to reduced cell proliferation, diminished hyperplasia, decreased inflammation, and a lowered potential for metastasis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



