Submitted:
26 December 2023
Posted:
28 December 2023
You are already at the latest version
Abstract
Acute pancreatitis (AP) is a leading gastrointestinal disease that cause hospitalization. Initial management in the first 72 h after the diagnosis of AP is pivotal, which can influence the clinical outcomes of the disease. Initial management, including fluid resuscitation, pain control, nutritional support, antibiotic use, and endoscopic retrograde cholangiopancreatography (ERCP) in gallstone pancreatitis, plays a fundamental role in AP treatment. Recent updates for fluid resuscitation, including treatment goals, the type, rate, volume, and duration, have triggered a paradigm shift from aggressive hydration with normal saline to goal-directed and non-aggressive hydration with lactated Ringer’s solution. Evidence of the clinical benefit of early enteral feeding is becoming definitive. Routine use of prophylactic antibiotics is generally limited, and the procalcitonin based algorithm of antibiotic use has recently been investigated to distinguish between inflammation and infection in patients with AP. Although urgent ERCP (within 24 h) should be performed for patients with gallstone pancreatitis and cholangitis, urgent ERCP is not indicated in patients without cholangitis. Furthermore, convalescent treatment, including cholecystectomy in gallstone pancreatitis and alcohol intervention in alcoholic pancreatitis, is also important for improving the prognosis and prevent recurrence in patients with AP. This review focuses on recent updates on the initial and convalescent management strategies for AP.
Keywords:
acute pancreatitis
; fluid resuscitation
; initial management
1. Introduction
Acute pancreatitis (AP) is an acute inflammation of the pancreas, a vital organ responsible for the production of digestive enzymes and hormones that regulate blood sugar levels. This disease is characterized by premature activation of digestive enzymes within the pancreas, leading to autodigestion and inflammation. AP is a leading gastrointestinal disease that cause hospitalization worldwide, and its incidence is increasing in many countries [1,2]. Among patients who admitted with AP, around 80% have a mild clinical course; however, the other develop severe disease, with a mortality rate of approximately 20% [2].
Initial management in the first 72 h after diagnosis is pivotal, which can influence the clinical course and outcome of the disease. Early identification and appropriate intervention can prevent complications and improve patient outcome. Although there is no specific pharmacological therapy available for AP, initial management, including fluid resuscitation, pain control, nutritional support, antibiotic use, and endoscopic retro-grade cholangiopancreatography (ERCP) in gallstone pancreatitis, plays a fundamental role in AP treatment. Furthermore, convalescent treatment is important for improving prognosis and prevent recurrence in patients with AP [3]. This review focuses on recent updates on the initial and convalescent management strategies for AP.
2. Initial Management during the First 72 Hours
2.1. Fluid Resuscitation
Traditionally, intravenous fluid resuscitation stands out as a cornerstone in AP management of any severity [4]. In patients with AP, increased vascular permeability and decreased osmotic pressure cause extracellular fluid leakages around the pancreas and into the retroperitoneal, abdominal, and thoracic cavities, resulting in a significant loss of circulating plasma volume. This can lead to hypovolemia and hypoperfusion, even resulting in other organ failures in severe AP. Therefore, early and adequate fluid resuscitation is important to stabilize cardiovascular distress and increase pancreatic microcirculation. Several previous studies have demonstrated that initial aggressive fluid resuscitation can improve survival by minimizing pancreatic necrosis [5,6,7,8]. However, over-aggressive fluid therapy can be associated with poor clinical outcomes in patients with severe AP, including sepsis, respiratory complications, and abdominal compartment syndrome [9,10]. At present, there are no clearly defined details regarding the goal of fluid resuscitation, fluid type, rate, volume, and duration [11].
2.1.1. Goal-Directed Therapy (GDT)
In patients with AP, several current guidelines suggest using GDT for fluid resuscitation [12,13,14]. GDT refers to titration of intravenous fluids to specific clinical and biochemical targets of perfusion, such as the heart rate (HR), mean arterial pressure (MAP), central venous pressure (CVP), urine output (UO), central venous oxygen saturation (ScvO2), blood urea nitrogen (BUN) concentration, hematocrit, and lactate levels [12]. Although GDT did not result in significantly improved mortality or a decrease in the rate of persistent multiple organ failure [11], it has been considered as a structured approach in which fluid administration is guided by specific physiological targets rather than empirical estimates, especially in patients with severe AP. These "goals" are determined by various hemodynamic and biochemical parameters that reflect the patient's volume status and perfusion (Table 1).
In patients with severe AP with organ failures requiring ICU admission, a more tailored and individualized approach to fluid resuscitation is required to avoid under- or over-treatment. Because a single clinical parameter alone is unlikely to reflect the overall volume status, simultaneous assessment of multiple parameters according to each phase of early AP is more reasonable [19]. These patients should be frequently assessed ideally every 2-3 h to adjust fluid therapy based on changes in these parameters. A recent pilot study showed that fluid therapy protocols based on dynamic parameters and tests (stroke volume changes after mini-fluid challenge (250 ml normal saline within 10 minutes) and passive leg raising test) were more reliable in predicting fluid responsiveness in patients with predicted severe AP [20].
2.1.2. Fluid Type
The fluid type for resuscitation in AP is an isotonic crystalloid solution, which contains normal saline (NS) and balanced/buffered crystalloids (such as lactated Ringer’s (RL), Plasma-Lyte, or Hartmann’s solution). Although NS has traditionally been used for fluid resuscitation in AP, concerns has been raised regarding the adverse effects of NS, such as hyperchloremic non-anion gap acidosis and acute kidney injury. Regarding clinical evidence of fluid resuscitation using RL vs. NS, a meta-analysis demonstrated that the LR group was less likely than NS group to progress to moderately severe or severe AP, requiring ICU admission or developing local complications [21]. The results of two large RCTs published in 2018 suggested that balanced crystalloids (LR or Plasma-Lyte) were favored over NS. The SMART study found that the use of balanced crystalloids can reduce the composite outcomes of in-hospital mortality, new renal replacement therapy, and persistent renal dysfunction in critically ill patients [22]. Another SALT-ED trial of non-critically ill patients in the emergency department revealed that balanced crystalloids resulted in a significant decrease in major adverse kidney events within 30 days, without a difference in hospital-free days [23]. Additionally, the use of LR could be associated with an anti-inflammatory effect, as shown by the decrease in C-reactive protein levels and incidence of SIRS [24]. Although in the AGA guidelines the panel disagreed with the superiority of RL over NS due to the low quality of evidence for major clinical outcomes [12], the clinical benefits of using RL are believed to outweigh the risks. Further detailed prospective comparative studies are warranted.
The use of colloids, including ‘semi-synthetic’ colloids (hydroxyethyl starch (HES), gelatin and dextran solutions) and ‘natural’ colloid (human albumin solution) is not recommended because of potential adverse effects without a demonstrable survival benefit [6,25,26]. The CHEST trial, a blinded, randomized, controlled trial comparing crystalloid and HES showed that acute kidney injury and adverse events (pruritis, skin rash) were more common in the HES group than in the NS group [25]. In addition, intravenous albumin infusion did not improve the clinical prognosis of patients with AP [27].
2.1.3. Fluid Rate and Volume
Early aggressive hydration has been widely recommended for the initial management of acute pancreatitis [12,13,14,28]. However, there are controversies regarding optimal fluid volume and infusion rate. Several RCTs subsequently compared aggressive and non-aggressive fluid resuscitation (Table 2). The results from the first two RCTs conducted in China for patients with severe AP demonstrated worse clinical outcomes with aggressive fluid therapy [29,30]. Wu et al. did not observe any differences between GDT and standard fluid therapy [31]. Although Buxbaum et al. demonstrated that aggressive fluid hydration appeared to be effective in mild AP [8], a recent large RCT of 249 patients with mild AP (WATERFALL study) was terminated early because of safety issues regarding whether aggressive fluid resuscitation was associated with an increased incidence of fluid overload (20.5% vs. 6.3%) without improvement in clinical outcomes [7].
Based on the available evidence from RCT results and several guidelines, we recommend a moderate fluid resuscitation strategy, starting with 1.5 ml/kg/hr of LR infusion rate, preceded by bolus of 10 – 20ml/kg over 2 h if patients have moderately severe to severe AP, signs of hypovolemia, acute kidney injury, or poor predictive indicators, such as hematocrit ≥ 44% or BUN > 25mg/dL. The following fluid volumes are generally considered appropriate for the initial management of AP: 3 L at 24h and 4-6 L at 48 h for mild AP; 3-4 L at 24 h and 6-8 L at 48 h based on clinical/laboratory parameters for moderate or severe AP [32].
2.1.4. Fluid Therapy Duration
In most patients with mild AP, oral feeding can be initiated 12 h after AP onset if abdominal pain is low, and fluid resuscitation can be stopped once the patient tolerates oral feeding. When patients are suspected to experience volume overload, the fluid should be decreased or stopped. The duration of fluid therapy might be longer in moderate to severe AP patients, and is guided by the patient's clinical status, including factors such as hemodynamic stability, organ function, and resolution of symptoms. Continuous monitoring with GDT is essential for adjusting fluid therapy, as needed.
2.2. Pain Control
The primary symptom of AP is abdominal pain, often severe and persistent, which requires effective management. Pain control is a pivotal element in the multidisciplinary management of AP; however, no single analgesic strategy has been universally accepted as superior in terms of efficacy and safety.
2.2.1. Opioids
Historically, there has been hesitation to use opioids for AP patients due to concerns about inducing sphincter of Oddi spasm. However, recent evidence suggests that opioids can be safely used in AP without increasing the risk of adverse events related to the sphincter of Oddi [33]. Opioids provide potent analgesia and are particularly effective in managing severe pain associated with AP. Their rapid onset of action and efficacy in reducing visceral pain makes them a preferred choice in many clinical scenarios. Although opioids are effective, they are associated with a risk of respiratory depression, constipation, and potential for dependence. However, in the context of AP, short-term use is generally considered safe [34]. Recently, a comparative RCT evaluated the efficacy and safety of intravenous buprenorphine (a more potent opioid than morphine with less respiratory depression and abuse potential) vs. IV diclofenac (a non-steroidal anti-inflammatory drugs (NSAID)) for analgesia in AP patients demonstrated that buprenorphine appears to be more effective and equally safe, even in the subgroup of patients with moderately severe or severe pancreatitis [36].

Table 2.
Summary of recent RCTs comparing the protocol of fluid resuscitation in AP.
| Reference | Participants (N) | Aggressive Resuscitation | Non-Aggressive Resuscitation | Effect of Aggressive Resuscitation |
|---|---|---|---|---|
| Mato et al. [29], 2009 | Severe AP lesser than 72 hr onset (76) | 10 – 15 ml/kg/hr | 5 – 10 ml/kg/hr | Harmful, more sepsis, mortality, mechanical ventilation, and ACS. |
| Mato et al. [30], 2010 | Severe AP lesser than 24 hr onset (115) | Rapid hemodilution with goal hematocrit < 35% at 48 hr | Slow hemodilution with goal hematocrit > 35% at 48 hr | Harmful, more sepsis, and mortality |
| Wu et al. [31], 2011 | Any severity AP (40) | GDT with 20ml/kg bolus →1.5 or 3ml/kg/hr of LR or NS |
LR or NS adjusted by physician | Similar in SIRS and CRP at 24 hr |
| Buxbaum et al. [8], 2017 | Predicted mild AP (60) | 20ml/kg bolus over 2 hr → 3ml/kg/hr infusion of LR |
10ml/kg bolus over 2hr → 1.5ml/kg/hr infusion of LR |
Beneficial, more clinical improvement, and less persistent SIRS and hemoconcentration |
| At timepoint (12, 24, 36 hours) If hematocrit, BUN, or creatinine increased, 20ml/kg bolus → 3ml/kg/hr infusion If labs were decreased and pain relived, 1.5ml/kg/hr infusion and start diet | ||||
| Cuéllar-Monterrubio et al. [35], 2020 | Any severity AP, more than 24hr onset (88) | 20ml/kg bolus → 3ml/kg/hr (first 24 hr) → 30ml/hr (next 24 hr) of HS |
20ml/kg bolus (only if hypovolemia) → 1.5ml/kg/hr (first 24 hr) → 30ml/hr (next 24 hr) of HS |
No benefit, no difference in persistent SIRS, pancreatic necrosis, respiratory complications, AKI and LOS |
| De-Madaria et al. [7], 2022 | Mild AP, lesser than 24hr onset (249) | 20ml/kg bolus → 3ml/kg/hr infusion of LR |
10ml/kg bolus (only if hypovolemia) → 1.5ml/kg/hr infusion of LR |
Harmful, mor fluid overload |
| At timepoint (3,12, 24, 48, 72 hours) If hypovolemia → 20ml/kg bolus → 3ml/kg/hr If normovolemia → 1.5ml/kg/hr If fluid overload → decrease or stop |
At timepoint (3,12, 24, 48, 72 hours) If hypovolemia → 10ml/kg bolus → 1.5 ml/kg/hr If normovolemia → 1.5ml/kg/hr If fluid overload → decrease or stop |
|||
AP, acute pancreatitis; ACS, abdominal compartment syndrome; LR, lactated Ringer’s; NS, normal saline; SIRS, systemic inflammatory response syndrome; CRP, C-reactive protein; BUN, blood urea nitrogen; HS, Hartmann’s solution; AKI, acute kidney injury; LOS. Length of stay.
2.2.2. NSAIDs
NSAIDs, especially intravenous formulations, such as paracetamol, dexketoprofen, and diclofenac, offer an alternative to opioids. They can be particularly useful in patients whom opioid use might be contraindicated, or in those at risk of opioid-related side effects. Studies have indicated that NSAIDs, particularly paracetamol, can provide analgesia comparable to that of opioids in AP. Their anti-inflammatory properties may offer additional benefits in the context of pancreatitis [33]. NSAIDs are generally well-tolerated. However, they should be used with caution in patients with renal impairment, gastric ulcers, or those at a risk of bleeding.
2.2.3. Epidural Analgesia
Epidural analgesia, particularly thoracic epidural analgesia, has been explored for pain management in patients with AP admitted to the ICU. It has been associated with decreased mortality in a multicenter retrospective propensity analysis. In an EPIPAN multicenter RCT, thoracic epidural analgesia was investigated in ICU patients with AP. The trial suggested potential benefits, including improved pancreatic perfusion and decreased AP severity with no significant difference in adverse events attributable to epidural analgesia in ICU patients with severe AP [37].
2.3. Nutritional Support
Traditionally, the “pancreatic rest” concept has been suggested as the initial management of AP to avoid pain and pancreatitis aggravation. However, recent research has also shown that early oral or enteral feeding results in shorter hospital stays, fewer complications, and lower mortality rates in patients with AP [38,39,40]. One study comparing parenteral and enteral nutrition revealed that oral feeding can reduce sepsis and AP severity. These clinical benefits may result from preventing atrophy of the gastrointestinal mucosa and maintaining the function of the gut-mucosal barrier, thereby reducing bacterial translocation and minimizing the risk of infected peripancreatic necrosis [41].
2.3.1. When to Start Oral Feeding
A pooled analysis of the results of 11 RCTs that addressed the role of early vs. delayed feeding demonstrated that when started within 48 h of admission, enteral nutrition resulted in a significant reduction in the risks of multiple organ failure, pancreatic infectious complications, and mortality, compared with parenteral nutrition [40]. Therefore, most guidelines recommend early (within 24-48 hours) oral feeding rather than keeping the patient nil per os (NPO), especially if patients are pain-free and their laboratory parameters have improved [12,13,14,28].
The PYTHON trial, a multicenter, randomized, controlled superiority trial, aimed to compare the outcomes of early naso-enteric tube feeding (within 24 hours of randomization; early group) to an oral diet that starts at 72 hours after presentation (tube feeding provided if the oral diet was not tolerated; on-demand group) in patients diagnosed with AP. This study did not show a significant difference in clinical outcomes (major infection or death) between the early and on-demand groups [42]. The recent PADI trial focused on determining the optimal time to start oral refeeding in patients with mild and moderate AP to reduce hospital length-of-stay (LOS) and its complications. This trial compared immediate oral refeeding (low-fat-solid diet initiated immediately after hospital admission) with conventional oral refeeding (fasting for the first 24 to 48 h and resuming oral diet when clinical and laboratory parameters improved), highlighting the benefits of immediate oral refeeding in reducing hospital stay and cost savings with fewer complications. The authors therefore asserted to start an oral diet without waiting for improvement of clinical symptoms and laboratory findings in patients with mild or moderate AP [43].
2.3.2. Route of Tube Feeding
The current meta-analysis and guidelines strongly favor enteral over parenteral nutrition [12,40]. However, some patients who are intolerant of oral feeding within 72 hours, due to pain, vomiting and ileus, may require the placement of an enteral tube for nutritional support. The studies including three RCTs, which specifically addressed the issue of nasogastric vs. nasoenteral (either nasoduodenal or nasojejunal) feeding, did not demonstrate a clinical benefit related to the route for tube feeding, either in mild or severe AP [44]. A nasogastric tube is relatively easy to insert compared to a nasoenteral tube. Both feeding routes can be selected depending on the patient’s condition. Parenteral nutrition is indicated only when the enteral route is impossible or unable to meet the minimum calorie requirements.
2.4. Prophylactic Antibiotic Use
The pathophysiology of necrotizing pancreatitis is marked by pancreatic necrosis, which is vulnerable to microbial colonization of non-viable pancreatic tissue, resulting in infected necrosis. Infected necrosis is highly associated with mortality in late phase of AP (approximately 30 %), and mortality doubles when infected necrosis coexist with organ failure [28,45]. To mitigate the risk of infected necrosis, morbidity, and mortality in patients with predicted severe AP or diagnosed with necrotizing pancreatitis, a series of RCTs evaluated prophylactic antibiotic use before documented infection. While earlier trials and meta-analyses often showed improvement of clinical outcomes by prophylactic antibiotic use, more recent studies and subsequent meta-analyses consistently failed to demonstrate consistent evidence of benefit from antibiotic prophylaxis. [46,47] Consequently, the use of prophylactic antibiotics to reduce the frequency of infection-related complications or mortality in acute pancreatitis, including severe and necrotizing pancreatitis, remains underpowered, and further large randomized controlled trials are warranted.
2.4.1. Procalcitonin-Guided Antibiotic Use
The decision-making process regarding antibiotic use is challenging, especially in the setting of an AP patient presenting with systemic symptoms such as fever, leukocytosis, and elevated C-reactive protein levels. None of these features distinguish between inflammation and infection, leading to global overuse of antibiotic during AP hospitalization [48,49]. The PROCAP trial, the largest randomized trial to date, investigated the use of a procalcitonin algorithm (Figure 1) to guide antibiotic use in patients with AP. The study showed that procalcitonin-guided care significantly decreased the probability of being prescribed an antibiotic, without increasing the risk of infection or harm to AP patients [50].
2.5. ERCP Role in Gallstone Pancreatitis
Gallstones are the most common cause of AP, which is clinically initiated by the impaction of gallstone stones or sludges in the common bile duct or ampulla [51,52]. Patients with gallstone pancreatitis may develop cholangitis, organ failure, and other life-threatening complications. ERCP quickly addresses the gallstone and provides rapid biliary decompression, thereby alleviating the severity of pancreatitis. Urgent ERCP (within 24 h of admission) should be performed in patients with gallstone pancreatitis and concomitant cholangitis [53,54].
Urgent ERCP is not indicated in patients with gallstone pancreatitis and persistent obstruction without cholangitis. In a systemic review of eight RCTs, early ERCP in patients without cholangitis did not reduce the risk of overall pancreatic complications, organ failure or death [44]. Especially among patients with predicted severe acute biliary pancreatitis but without cholangitis, the results of the APEC and APEC-2 trials revealed that urgent ERCP, even when guided by endoscopic ultrasound, could not significantly reduce major complications or mortality compared with conservative treatment [55,56]. Recently, there has been a growing inclination towards a more conservative strategy, reserving ERCP for cases where there is a clear indication, such as the presence of cholangitis or persistent biliary obstruction. This shift reflects a broader trend in practice towards more personalized care, where treatments are increasingly tailored to the specific needs and circumstances of individual patients with gallstone pancreatitis.
2.6. Other therapeutic interventions
2.6.1. Low Molecular Weight Heparin (LMWH)
LMWHs such as enoxaparin are anticoagulants that prevent the formation of blood clots. Their role in acute pancreatitis is based on the premise that microvascular thrombosis plays a role in the disease progression. A recent randomized, single-bind, phase 3 control trial emphasized the potential benefits of LMWH in acute pancreatitis. The study found that LMWH can reduce necrosis of the pancreas, especially in the early phase of moderate and severe acute pancreatitis [57].
2.6.2. Protease Inhibitors
Protease inhibitors are used to treat acute pancreatitis, their effectiveness is a topic of debate. These inhibitors prevent the activation of enzymes that can damage the pancreas. A meta-analysis aimed to determine the effectiveness of protease inhibitors in reducing mortality or morbidity associated with acute pancreatitis. Overall, treatment with protease inhibitors did not significantly reduce the mortality rate associated with AP [58,59].
3. Convalescent Treatment
3.1. Cholecystectomy in Gallstone AP
3.1.1. Timing of Cholecystectomy
Prophylactic cholecystectomy is commonly recommended during initial hospital admission for patients with acute biliary pancreatitis rather than after discharge [60]. This strategy aims to prevent recurrent episodes of pancreatitis, and same-admission cholecystectomy (within seven days) is proven to be more effective than interval cholecystectomy for the prevention of recurrent gallstone-related complications with cost-effectiveness in mild gallstone pancreatitis [61,62,63]. A recent study investigated the optimal timing and safety of cholecystectomy in patients with necrotizing biliary pancreatitis, with the aim of balancing recurrent biliary events with the risk of surgical complications. In conclusion, cholecystectomy in the absence of peripancreatic collections is thought to be preferably performed within 8 weeks after discharge [64].
3.2. Alcohol Intervention in Alcoholic AP
Abstinence from alcohol can protect against recurrent AP [65]. In addition, the implementation of brief alcohol interventions during hospital admission, combined with repeated interventions, can improve the effectiveness of preventing AP recurrence [66]. However, there is still a lack of RCTs confirming the effectiveness of alcohol intervention only in patients with alcoholic AP. Further studies are needed to determine whether alcohol abstinence reduces recurrence and improves the prognosis of AP.
4. Conclusions
Initial and convalescent treatments for AP are currently evolving, based on recent clinical evidence. GDT with nonaggressive fluid resuscitation of buffered crystalloids has become the main strategy for AP treatment. Adequate pain control and early enteral feeding play important roles in the initial management of AP. Algorithm-based antibiotic use, rather than routine use for prophylaxis, makes it possible to tailor approaches to AP with clinical improvement. Except the definitive role of urgent ERCP in acute biliary pancreatitis with cholangitis, a more conservative approach becomes widely valued. New pharmacological treatments, optimal timing of cholecystectomy in necrotizing biliary pancreatitis, and the efficacy of alcohol intervention need to be investigated in the future.
Author Contributions
Conceptualization, Y.K.S. and S.H.L.; methodology, S.H.L.; investigation, Y.K.S.; writing—original draft preparation, Y.K.S.; writing—review and editing, S.H.L.; supervision, S.H.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Mederos, M.A.; Reber, H.A.; Girgis, M.D. Acute pancreatitis: A review. JAMA 2021, 325, 382–390. [CrossRef]
- Krishna, S.G.; Kamboj, A.K.; Hart, P.A.; Hinton, A.; Conwell, D.L. The changing epidemiology of acute pancreatitis hospitalizations: A decade of trends and the impact of chronic pancreatitis. Pancreas 2017, 46, 482–488. [CrossRef]
- de-Madaria, E.; Buxbaum, J.L. Advances in the management of acute pancreatitis. Nat Rev Gastroenterol Hepatol 2023, 20, 691–692. [CrossRef]
- Lee, P.J.; Papachristou, G.I. New insights into acute pancreatitis. 2019, 16, 479–496. [CrossRef]
- Lee, A.; Ko, C.; Buitrago, C.; Hiramoto, B.; Hilson, L.; et al. Lactated ringers vs normal saline resuscitation for mild acute pancreatitis: A randomized trial. 2021, 160, 955–957.e954. [CrossRef]
- Myburgh, J.A.; Finfer, S.; Bellomo, R.; Billot, L.; Cass, A.; Gattas, D.; Glass, P.; Lipman, J.; Liu, B.; McArthur, C. et al. Hydroxyethyl starch or saline for fluid resuscitation in intensive care. N Engl J Med 2012, 367, 1901–1911. [CrossRef]
- de-Madaria, E.; Buxbaum, J.L.; Maisonneuve, P.; Garcia Garcia de Paredes, A.; Zapater, P.; Guilabert, L.; Vaillo-Rocamora, A.; Rodriguez-Gandia, M.A.; Donate-Ortega, J.; Lozada-Hernandez, E.E. et al. Aggressive or moderate fluid resuscitation in acute pancreatitis. N Engl J Med 2022, 387, 989–1000. [CrossRef]
- Buxbaum, J.L.; Quezada, M.; Da, B.; Jani, N.; Lane, C.; Mwengela, D.; Kelly, T.; Jhun, P.; Dhanireddy, K.; Laine, L. Early aggressive hydration hastens clinical improvement in mild acute pancreatitis. Am J Gastroenterol 2017, 112, 797–803. [CrossRef]
- de-Madaria, E.; Soler-Sala, G.; Sanchez-Paya, J.; Lopez-Font, I.; Martinez, J.; Gomez-Escolar, L.; Sempere, L.; Sanchez-Fortun, C.; Perez-Mateo, M. Influence of fluid therapy on the prognosis of acute pancreatitis: A prospective cohort study. Am J Gastroenterol 2011, 106, 1843–1850. [CrossRef]
- De Waele, J.J.; Leppaniemi, A.K. Intra-abdominal hypertension in acute pancreatitis. World J Surg 2009, 33, 1128–1133. [CrossRef]
- Wilms, H.; Mittal, A.; Haydock, M.D.; van den Heever, M.; Devaud, M.; Windsor, J.A. A systematic review of goal directed fluid therapy: Rating of evidence for goals and monitoring methods. J Crit Care 2014, 29, 204–209. [CrossRef]
- Crockett, S.D.; Wani, S.; Gardner, T.B.; Falck-Ytter, Y.; Barkun, A.N.; American Gastroenterological Association Institute Clinical Guidelines, C. American gastroenterological association institute guideline on initial management of acute pancreatitis. Gastroenterology 2018, 154, 1096–1101. [CrossRef]
- Lee, S.H.; Choe, J.W.; Cheon, Y.K.; Choi, M.; Jung, M.K.; Jang, D.K.; Jo, J.H.; Lee, J.M.; Kim, E.J.; Han, S.Y. et al. Revised clinical practice guidelines of the korean pancreatobiliary association for acute pancreatitis. Gut Liver 2023, 17, 34–48. [CrossRef]
- Yokoe, M.; Takada, T.; Mayumi, T.; Yoshida, M.; Isaji, S.; Wada, K.; Itoi, T.; Sata, N.; Gabata, T.; Igarashi, H. et al. Japanese guidelines for the management of acute pancreatitis: Japanese guidelines 2015. J Hepatobiliary Pancreat Sci 2015, 22, 405–432. [CrossRef]
- Wu, B.U.; Bakker, O.J.; Papachristou, G.I.; Besselink, M.G.; Repas, K.; van Santvoort, H.C.; Muddana, V.; Singh, V.K.; Whitcomb, D.C.; Gooszen, H.G. et al. Blood urea nitrogen in the early assessment of acute pancreatitis: An international validation study. Arch Intern Med 2011, 171, 669–676. [CrossRef]
- Wu, B.U.; Johannes, R.S.; Sun, X.; Conwell, D.L.; Banks, P.A. Early changes in blood urea nitrogen predict mortality in acute pancreatitis. Gastroenterology 2009, 137, 129–135. [CrossRef]
- Brown, A.; Baillargeon, J.D.; Hughes, M.D.; Banks, P.A. Can fluid resuscitation prevent pancreatic necrosis in severe acute pancreatitis? Pancreatology 2002, 2, 104–107. [CrossRef]
- Jin, T.; Li, L.; Deng, L.; Wen, S.; Zhang, R.; Shi, N.; Zhu, P.; Lan, L.; Lin, Z.; Jiang, K. et al. Hemoconcentration is associated with early faster fluid rate and increased risk of persistent organ failure in acute pancreatitis patients. JGH Open 2020, 4, 684–691. [CrossRef]
- Crosignani, A.; Spina, S.; Marrazzo, F.; Cimbanassi, S.; Malbrain, M.; Van Regenmortel, N.; Fumagalli, R.; Langer, T. Intravenous fluid therapy in patients with severe acute pancreatitis admitted to the intensive care unit: A narrative review. Ann Intensive Care 2022, 12, 98. [CrossRef]
- Jin, T.; Li, L.; Zhu, P.; Deng, L.; Zhang, X.; Hu, C.; Shi, N.; Zhang, R.; Tan, Q.; Chen, C. et al. Optimising fluid requirements after initial resuscitation: A pilot study evaluating mini-fluid challenge and passive leg raising test in patients with predicted severe acute pancreatitis. Pancreatology 2022, 22, 894–901. [CrossRef]
- Zhou, S.; Buitrago, C.; Foong, A.; Lee, V.; Dawit, L.; Hiramoto, B.; Chang, P.; Schilperoort, H.; Lee, A.; de-Madaria, E. et al. Comprehensive meta-analysis of randomized controlled trials of lactated ringer's versus normal saline for acute pancreatitis. Pancreatology 2021, 21, 1405–1410. [CrossRef]
- Semler, M.W.; Self, W.H.; Wanderer, J.P.; Ehrenfeld, J.M.; Wang, L.; Byrne, D.W.; Stollings, J.L.; Kumar, A.B.; Hughes, C.G.; Hernandez, A. et al. Balanced crystalloids versus saline in critically ill adults. N Engl J Med 2018, 378, 829–839. [CrossRef]
- Self, W.H.; Semler, M.W.; Wanderer, J.P.; Wang, L.; Byrne, D.W.; Collins, S.P.; Slovis, C.M.; Lindsell, C.J.; Ehrenfeld, J.M.; Siew, E.D. et al. Balanced crystalloids versus saline in noncritically ill adults. N Engl J Med 2018, 378, 819–828. [CrossRef]
- de-Madaria, E.; Herrera-Marante, I.; Gonzalez-Camacho, V.; Bonjoch, L.; Quesada-Vazquez, N.; Almenta-Saavedra, I.; Miralles-Macia, C.; Acevedo-Piedra, N.G.; Roger-Ibanez, M.; Sanchez-Marin, C. et al. Fluid resuscitation with lactated ringer's solution vs normal saline in acute pancreatitis: A triple-blind, randomized, controlled trial. United European Gastroenterol J 2018, 6, 63–72. [CrossRef]
- Zhao, G.; Zhang, J.G.; Wu, H.S.; Tao, J.; Qin, Q.; Deng, S.C.; Liu, Y.; Liu, L.; Wang, B.; Tian, K. et al. Effects of different resuscitation fluid on severe acute pancreatitis. World J Gastroenterol 2013, 19, 2044–2052. [CrossRef]
- Du, X.J.; Hu, W.M.; Xia, Q.; Huang, Z.W.; Chen, G.Y.; Jin, X.D.; Xue, P.; Lu, H.M.; Ke, N.W.; Zhang, Z.D. et al. Hydroxyethyl starch resuscitation reduces the risk of intra-abdominal hypertension in severe acute pancreatitis. Pancreas 2011, 40, 1220–1225. [CrossRef]
- Ma, Y.; Yan, T.; Xu, F.; Ding, J.; Yang, B.; Ma, Q.; Wu, Z.; Lyu, J.; Wang, Z. Infusion of human albumin on acute pancreatitis therapy: New tricks for old dog? Front Pharmacol 2022, 13, 842108. [CrossRef]
- Working Group, I.A.P.A.P.A.A.P.G. Iap/apa evidence-based guidelines for the management of acute pancreatitis. Pancreatology 2013, 13, e1–e15. [CrossRef]
- Mao, E.Q.; Tang, Y.Q.; Fei, J.; Qin, S.; Wu, J.; Li, L.; Min, D.; Zhang, S.D. Fluid therapy for severe acute pancreatitis in acute response stage. Chin Med J (Engl) 2009, 122, 169–173. [CrossRef]
- Mao, E.Q.; Fei, J.; Peng, Y.B.; Huang, J.; Tang, Y.Q.; Zhang, S.D. Rapid hemodilution is associated with increased sepsis and mortality among patients with severe acute pancreatitis. Chin Med J (Engl) 2010, 123, 1639–1644. [CrossRef]
- Wu, B.U.; Hwang, J.Q.; Gardner, T.H.; Repas, K.; Delee, R.; Yu, S.; Smith, B.; Banks, P.A.; Conwell, D.L. Lactated ringer's solution reduces systemic inflammation compared with saline in patients with acute pancreatitis. Clin Gastroenterol Hepatol 2011, 9, 710–717 e711. [CrossRef]
- Yaowmaneerat, T.; Sirinawasatien, A. Update on the strategy for intravenous fluid treatment in acute pancreatitis. World J Gastrointest Pharmacol Ther 2023, 14, 22–32. [CrossRef]
- Gülen, B.; Dur, A.; Serinken, M.; Karcioğlu, Ö.; Sönmez, E. Pain treatment in patients with acute pancreatitis: A randomized controlled trial. 2016, 27, 192–196. [CrossRef]
- Basurto Ona, X.; Rigau Comas, D.; Urrútia, G. Opioids for acute pancreatitis pain. 2013, 2013. [CrossRef]
- Cuellar-Monterrubio, J.E.; Monreal-Robles, R.; Gonzalez-Moreno, E.I.; Borjas-Almaguer, O.D.; Herrera-Elizondo, J.L.; Garcia-Compean, D.; Maldonado-Garza, H.J.; Gonzalez-Gonzalez, J.A. Nonaggressive versus aggressive intravenous fluid therapy in acute pancreatitis with more than 24 hours from disease onset: A randomized controlled trial. Pancreas 2020, 49, 579–583. [CrossRef]
- Saini, M.; Samanta, J.; Kumar, A.; Choudhury, A.; Dhar, J.; Jafra, A.; Chauhan, R.; Muktesh, G.; Gupta, P.; Gupta, V. et al. Buprenorphine versus diclofenac for pain relief in acute pancreatitis: A double-blinded randomized controlled trial. Clin Gastroenterol Hepatol 2023. [CrossRef]
- Jabaudon, M.; Genevrier, A.; Jaber, S.; Windisch, O.; Bulyez, S.; et al. Thoracic epidural analgesia in intensive care unit patients with acute pancreatitis: The epipan multicenter randomized controlled trial. 2023, 27. [CrossRef]
- Louie, B.E.; Noseworthy, T.; Hailey, D.; Gramlich, L.M.; Jacobs, P.; Warnock, G.L. 2004 maclean-mueller prize enteral or parenteral nutrition for severe pancreatitis: A randomized controlled trial and health technology assessment. Can J Surg 2005, 48, 298–306.
- Al-Omran, M.; Albalawi, Z.H.; Tashkandi, M.F.; Al-Ansary, L.A. Enteral versus parenteral nutrition for acute pancreatitis. Cochrane Database Syst Rev 2010, 2010, CD002837. [CrossRef]
- Petrov, M.S.; Pylypchuk, R.D.; Uchugina, A.F. A systematic review on the timing of artificial nutrition in acute pancreatitis. Br J Nutr 2009, 101, 787–793. [CrossRef]
- Windsor, A.C.; Kanwar, S.; Li, A.G.; Barnes, E.; Guthrie, J.A.; Spark, J.I.; Welsh, F.; Guillou, P.J.; Reynolds, J.V. Compared with parenteral nutrition, enteral feeding attenuates the acute phase response and improves disease severity in acute pancreatitis. Gut 1998, 42, 431–435. [CrossRef]
- Bakker, O.J.; van Brunschot, S.; van Santvoort, H.C.; Besselink, M.G.; Bollen, T.L.; Boermeester, M.A.; Dejong, C.H.; van Goor, H.; Bosscha, K.; Ahmed Ali, U. et al. Early versus on-demand nasoenteric tube feeding in acute pancreatitis. N Engl J Med 2014, 371, 1983–1993. [CrossRef]
- Ramírez-Maldonado, E.; López Gordo, S.; Pueyo, E.M.; Sánchez-García, A.; Mayol, S.; et al. Immediate oral refeeding in patients with mild and moderate acute pancreatitis: A multicenter, randomized controlled trial (padi trial). 2021, 274, 255–263. [CrossRef]
- Vege, S.S.; DiMagno, M.J.; Forsmark, C.E.; Martel, M.; Barkun, A.N. Initial medical treatment of acute pancreatitis: American gastroenterological association institute technical review. Gastroenterology 2018, 154, 1103–1139. [CrossRef]
- Werge, M.; Novovic, S.; Schmidt, P.N.; Gluud, L.L. Infection increases mortality in necrotizing pancreatitis: A systematic review and meta-analysis. Pancreatology 2016, 16, 698–707. [CrossRef]
- Wittau, M.; Mayer, B.; Scheele, J.; Henne-Bruns, D.; Dellinger, E.P.; et al. Systematic review and meta-analysis of antibiotic prophylaxis in severe acute pancreatitis. 2011, 46, 261–270. [CrossRef]
- Baltatzis, M.; Mason, J.M.; Chandrabalan, V.; Stathakis, P.; McIntyre, B.; et al. Antibiotic use in acute pancreatitis: An audit of current practice in a tertiary centre. 2016, 16, 946–951. [CrossRef]
- Baltatzis, M.; Mason, J.M.; Chandrabalan, V.; Stathakis, P.; McIntyre, B.; Jegatheeswaran, S.; Jamdar, S.; O'Reilly, D.A.; Siriwardena, A.K. Antibiotic use in acute pancreatitis: An audit of current practice in a tertiary centre. Pancreatology 2016, 16, 946–951. [CrossRef]
- Parniczky, A.; Lantos, T.; Toth, E.M.; Szakacs, Z.; Godi, S.; Hagendorn, R.; Illes, D.; Koncz, B.; Marta, K.; Miko, A. et al. Antibiotic therapy in acute pancreatitis: From global overuse to evidence based recommendations. Pancreatology 2019, 19, 488–499. [CrossRef]
- Siriwardena, A.K.; Jegatheeswaran, S.; Mason, J.M.; Baltatzis, M.; Sheen, A.J. et al. A procalcitonin-based algorithm to guide antibiotic use in patients with acute pancreatitis (procap): A single-centre, patient-blinded, randomised controlled trial. 2022, 7, 913–921. [CrossRef]
- Yadav, D.; Lowenfels, A.B. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology 2013, 144, 1252–1261. [CrossRef]
- Lerch, M.M.; Saluja, A.K.; Runzi, M.; Dawra, R.; Saluja, M.; Steer, M.L. Pancreatic duct obstruction triggers acute necrotizing pancreatitis in the opossum. Gastroenterology 1993, 104, 853–861. [CrossRef]
- Fan, S.T.; Lai, E.C.; Mok, F.P.; Lo, C.M.; Zheng, S.S.; Wong, J. Early treatment of acute biliary pancreatitis by endoscopic papillotomy. N Engl J Med 1993, 328, 228–232. [CrossRef]
- van Santvoort, H.C.; Besselink, M.G.; de Vries, A.C.; Boermeester, M.A.; Fischer, K.; Bollen, T.L.; Cirkel, G.A.; Schaapherder, A.F.; Nieuwenhuijs, V.B.; van Goor, H. et al. Early endoscopic retrograde cholangiopancreatography in predicted severe acute biliary pancreatitis: A prospective multicenter study. Ann Surg 2009, 250, 68–75. [CrossRef]
- Hallensleben, N.D.; Stassen, P.M.C.; Schepers, N.J.; Besselink, M.G.; Anten, M.P.G.F.; et al. Patient selection for urgent endoscopic retrograde cholangio-pancreatography by endoscopic ultrasound in predicted severe acute biliary pancreatitis (apec-2): A multicentre prospective study. 2023, 72, 1534–1542. [CrossRef]
- Schepers, N.J.; L Hallensleben, N.D.; Besselink, M.G.; F Anten, M.-P.G.; Bollen, T.L.; et al. Urgent endoscopic retrograde cholangiopancreatography with sphincterotomy versus conservative treatment in predicted severe acute gallstone pancreatitis (apec): A multicentre randomised controlled trial. 2020, 396, 167. [CrossRef]
- Patil, B.; Meena, L.N.; Sharma, D.C.; Agarwal, G.; Dadhich, Y.; et al. Impact of low-molecular-weight heparin in the treatment of moderately severe and severe acute pancreatitis; a randomized, single blind, phase 3 control trial. 2022, 101. [CrossRef]
- Seta, T.; Noguchi, Y.; Shimada, T.; Shikata, S.; Fukui, T. Treatment of acute pancreatitis with protease inhibitors: A meta-analysis correspondence and requests for reprints to. 2004, 16, 1287–1293. [CrossRef]
- Wang, G.; Liu, Y.; Zhou, S.-F.; Qiu, P.; Xu, L.; et al. Effect of somatostatin, ulinastatin and gabexate on the treatment of severe acute pancreatitis. 2016. [CrossRef]
- Crockett, S.D.; Wani, S.; Gardner, T.B.; Falck-Ytter, Y.; Barkun, A.N.; et al. American gastroenterological association institute guideline on initial management of acute pancreatitis. 2018, 154, 1096–1101. [CrossRef]
- Boerma, D.; Rauws, E.A.; Keulemans, Y.C.; Janssen, I.M.; Bolwerk, C.J.; Timmer, R.; Boerma, E.J.; Obertop, H.; Huibregtse, K.; Gouma, D.J. Wait-and-see policy or laparoscopic cholecystectomy after endoscopic sphincterotomy for bile-duct stones: A randomised trial. Lancet 2002, 360, 761–765. [CrossRef]
- da Costa, D.W.; Bouwense, S.A.; Schepers, N.J.; Besselink, M.G.; van Santvoort, H.C.; van Brunschot, S.; Bakker, O.J.; Bollen, T.L.; Dejong, C.H.; van Goor, H. et al. Same-admission versus interval cholecystectomy for mild gallstone pancreatitis (poncho): A multicentre randomised controlled trial. Lancet 2015, 386, 1261–1268. [CrossRef]
- da Costa, D.W.; Dijksman, L.M.; Bouwense, S.A.; Schepers, N.J.; Besselink, M.G.; van Santvoort, H.C.; Boerma, D.; Gooszen, H.G.; Dijkgraaf, M.G.; Dutch Pancreatitis Study, G. Cost-effectiveness of same-admission versus interval cholecystectomy after mild gallstone pancreatitis in the poncho trial. Br J Surg 2016, 103, 1695–1703. [CrossRef]
- Hallensleben, N.D.; Timmerhuis, H.C.; Hollemans, R.A.; Pocornie, S.; Van Grinsven, J.; et al. Optimal timing of cholecystectomy after necrotising biliary pancreatitis. 2022, 71, 974–982. [CrossRef]
- Pelli, H.; Lappalainen-Lehto, R.; Piironen, A.; Sand, J.; Nordback, I. Risk factors for recurrent acute alcohol-associated pancreatitis: A prospective analysis. Scand J Gastroenterol 2008, 43, 614–621. [CrossRef]
- Nordback, I.; Pelli, H.; Lappalainen-Lehto, R.; Jarvinen, S.; Raty, S.; Sand, J. The recurrence of acute alcohol-associated pancreatitis can be reduced: A randomized controlled trial. Gastroenterology 2009, 136, 848–855. [CrossRef]
Figure 1.
Procalcitonin based algorithm in RPOCAP trail [49].
Figure 1.
Procalcitonin based algorithm in RPOCAP trail [49].
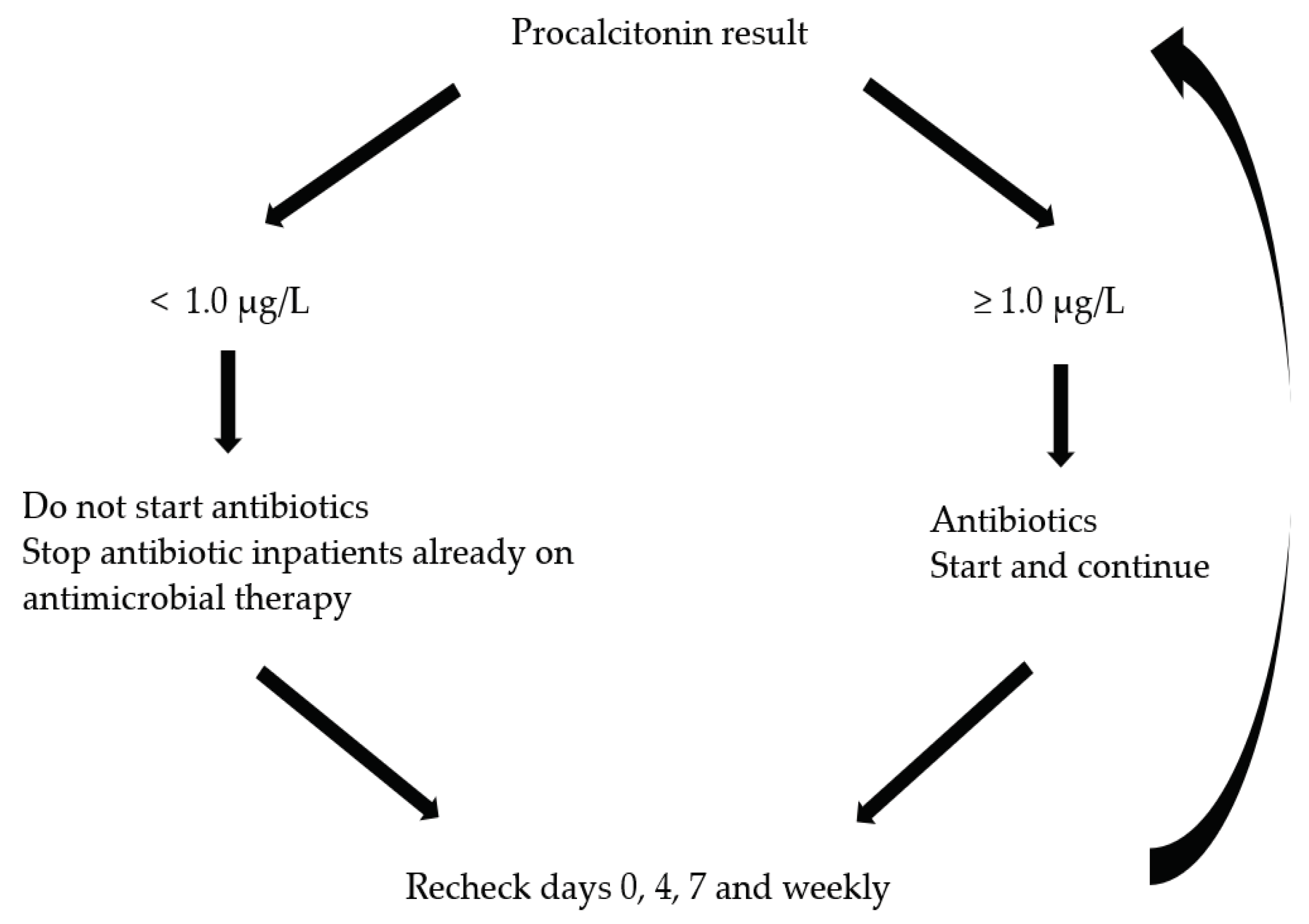
Table 1.
Physiological parameters and its significance in GDT.
| Parameters and Target | Significance in GDT |
|---|---|
| HR < 120 /min | An elevated heart rate can indicate an imbalance between oxygen supply and demand, guiding therapeutic interventions in GDT. Persistent tachycardia might suggest inadequate resuscitation or ongoing inflammation. |
| MAP 65-90 mmHg | A consistent MAP is crucial for ensuring adequate blood flow to vital organs. In GDT, adjustments in fluid volume and vasopressor medications might be considered to maintain or achieve a target MAP, ensuring optimal organ perfusion. |
| CVP 8 – 12 cmH2O | It indicates the volume and filling status of the right atrium. In GDT, CVP is used to assess the patient's volume status and right-sided cardiac preload, guiding fluid management. |
| UO ≥ 0.5 ml/kg/hr | A decrease in UO is an early and sensitive indicator of reduced kidney perfusion. Maintaining adequate urine output is crucial in GDT as it provides valuable information on general tissue perfusion. |
| ScvO2 ≥ 70% | An indicator in assessing the adequacy of tissue oxygenation. A decrease in ScvO2 can suggest that tissue oxygen demand is exceeding supply. This could be due to decreased oxygen delivery (e.g., due to low cardiac output or hemoglobulin) or increased oxygen consumption (e.g., due to increased metabolic demand). |
| BUN < 25mg/dL | An elevated BUN has been useful prognostic biomarker of severe AP, reflecting acute renal injury in AP caused by decrease in circulatory volume and direct injury mechanisms, which is facilitated by the autodigestion and inflammatory cytokines [15,16]. Whereas a declining or normalized BUN level reflects recovery of renal perfusion and adequate resuscitation. |
| Hematocrit < 44% | Hemoconcentration (high hematocrit values) is linked with high fluid sequestration and increased viscosity which might contribute to impaired pancreatic microcirculation. Therefore, hematocrit has long been identified as a marker associated with the development of pancreatic necrosis and persistent organ failure [17,18]. Fluid rate adjustment can be guided by the biochemical targets of hematocrit of 35 – 44% at 12 and 24 hours after AP onset. |
| Lactate | Lactate level increases when aerobic cellular respiration is impaired with switch to anaerobic metabolism. Elevated lactate level has been considered as a well-recognized biomarker of tissue hypoxia/hypoperfusion in the critically ill patients. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



