
Submitted:
27 December 2023
Posted:
29 December 2023
You are already at the latest version
Abstract
Polycystic Ovary Syndrome (PCOS) is a highly prevalent endocrine-metabolic disorder in women of reproductive age. Diagnosis of this syndrome relies on criteria established by the Rotterdam Consensus, with PCOS phenotypes being crucial for distinguishing potential complications, treatment approaches, and timing. The aim of this study is to characterize the biodemographic, clinical, metabolic, and reproductive variables and their association with PCOS phenotypes in a population from the Ecuadorian Andes. Methodology: A cross-sectional study was conducted with a non-random consecutive sample of 92 women attending the gynecology and endocrinology outpatient clinic at the Technical University of Loja Hospital (UTPL)-Santa Inés, Loja, Ecuador, between January 2022 and July 2023.Results: The average age was 22±3.4 years, predominantly mestizo, urban, single, with higher education and a medium-high socioeconomic status. Oligo-amenorrhea and acne appear strongly associated with phenotypes A and B, while hirsutism and polycystic ovaries on ultrasound show a weaker association with these phenotypes. Alopecia is more prevalent in phenotypes C and D. Triglyceride levels and BMI have a strong association with phenotypes A and B. Total testosterone levels, 17 OH progesterone, LH, and free androgen index show a moderate association with phenotypes A and B, while other reproductive variables exhibit weak associations. Conclusions: Classical phenotypes A and B of PCOS are most common in Andean Ecuadorian women, carrying higher risks of insulin resistance, anovulation, metabolic disorders, and elevated triglycerides compared to phenotypes C and D. Ethnic diversity and sociocultural habits influence the prevalence and clinical manifestations of phenotypes.

Keywords:
Polycystic Ovary Syndrome
; Phenotype
; Oligomenorrhea
; Hirsutism
; Clinical Diagnosis
; Infertility
1. Introduction
The Polycystic Ovary Syndrome (PCOS) stands as the most prevalent endocrine metabolic disorder in women of reproductive age [1]. It affects an estimated 4-21% of women globally, constituting a leading cause of menstrual cycle disorders (MCD), female infertility (FI), and hyperandrogenism (HA) [2]. Its etiopathogenesis is intricate, multifactorial, and heterogeneous, involving genetic, epigenetic, and environmental factors, underscoring the critical importance of accurate diagnosis and treatment [3]. Diagnostic criteria vary internationally, with the Rotterdam 2003 criteria recommended for epidemiological and phenotypic studies. Diagnosis requires the fulfillment of two out of three criteria: ovulatory dysfunction, hyperandrogenism, and polycystic ovary morphology (PCOM) [4]. Severity prediction aligns with phenotypes, and the Rotterdam consensus identifies four distinct phenotypes: A (ovulatory dysfunction + hyperandrogenism + PCOM), B (ovulatory dysfunction + hyperandrogenism), C (hyperandrogenism + PCOM), and D (ovulatory dysfunction + PCOM) [5], with phenotypes A and B being more complex [6], higher-risk, requiring prolonged treatments [7,8,9]. However, challenges persist in defining PCOS, and certain aspects of its pathophysiology remain unclear, necessitating ongoing research [10,11].
Latin America and the Andean region of Ecuador exhibit significant variability in genetic, environmental, dietary, and ethnic patterns, with limited studies characterizing PCOS phenotypes. Given diverse genetic origins, a reasonable assumption is that this genetic diversity influences PCOS phenotypic heterogeneity. Prior studies have highlighted data limitations associated with PCOS phenotypes, particularly in ethnic populations [12]. A systematic review indicates that the prevalence of phenotypes A and B ranges from 65.8% to 87.5%. Studies in Argentina, Brazil, and Chile also identified additional complications, such as metabolic syndrome in 33.3-44% of phenotype A, 15-58% of phenotype B, 11.9-36% of phenotype C, and 14.2-66% of phenotype D, suggesting unfavorable anthropometric and metabolic profiles in Latin American women with PCOS [13]. Importantly, overweight or obese PCOS-diagnosed patients exhibit a higher prevalence of hirsutism and menstrual disorders, negatively impacting reproductive and metabolic health [14,15]. This association makes it a primary trigger for anovulatory infertility and a risk factor, increasing the likelihood of developing type 2 diabetes, insulin resistance, and cardiovascular diseases by tenfold in young women—a significant public health concern and an opportunity for early intervention [16]. The study’s objective was to characterize biodemographic, clinical, metabolic, and reproductive variables and their association with PCOS phenotypes in an Ecuadorian Andean population, establishing a foundation for identifying the unique characteristics of these patients in future research.
2. Materials and Methods
2.1. Study Design
A cross-sectional study was developed, following the guidelines of the STROBE statement, for observational studies in epidemiology [17].
2.2. Data Collection and Participants
The sample selection was performed through a non-random consecutive sampling considering patients with a diagnosis of PCOS attending the gynecology and endocrinology office of the Hospital Universidad Técnica Particular de Loja (UTPL)- Santa Inés in the city of Loja (Ecuador), during the period from January 2022 to July 2023. The city of Loja is located in a region of the Andes in southern Ecuador, with an average altitude of 2,200 meters above sea level, with a mix of ethnic backgrounds including mestizo, indigenous and Afro-Ecuadorian. Participants who agreed to enter the study underwent a complete medical history by health professionals, including family and personal history and socioeconomic survey validated by the National Institute of Statistics and Census (INEC). The women included in the study were between 18 and 40 years of age, most of the participants studied at a university center, but there are also teachers, administrative staff, service personnel and private individuals who come to this health care center.
2.3. Inclusion and Exclusion Criteria
Women with a diagnosis of PCOS less than one year old were included, with two of the three criteria described below, according to the latest consensus of the American (ASRM) and European Societies for Reproductive Medicine (ESHRE) 2010 - Rotterdam 2003:
- 1.
- Oligo/amenorrhea (menstrual cycle disturbances between less than 21 days and more than 35 to 90 days);
- 2.
- Clinical (with the presence of hirsutism, acne, androgenic alopecia) or biochemical hyperandrogenism (with elevated levels of total testosterone, SHBG (sex hormone-binding globulin), and free androgen index;
- 3.
- Ultrasound with polycystic ovarian morphology (12 or more follicles of 2 to 9 mm, with volume >10cc).
Patients in gestation, puerperium, with chronic degenerative diseases (non-classical congenital adrenal hyperplasia, androgen-producing tumor, hyperprolactinemia, thyroid dysfunction, Cushing’s syndrome, drugs with androgenic activity); women with non-ovarian hyperandrogenism; ovarian cysts were excluded. None of the women had received hormonal treatment at least three months prior to inclusion in the study.
Ninety-two patients participated in the study, 85% of whom were diagnosed with PCOS in the gynecology office and 15% were referred by the dermatology or endocrinology service. The mean age of the patients was 22 ± 3.4 years (Figure 1).
2.4. Variables
A questionnaire was applied to all participants including the following variables: phenotypes, sociodemographic, clinical, metabolic and reproductive.
- Phenotypes: As reported in the literature and the characteristics used in the diagnostic criteria, phenotype A is referred to as “complete” and both phenotypes A and B are referred to as “classic”. Women with classic PCOS appear to be more hirsute and obese, have a more irregular menstrual pattern and are more likely to have insulin resistance, dyslipidemia, hepatic steatosis and a higher risk of metabolic syndrome compared to non-hyperandrogenic phenotypes. The so-called “ovulatory” C phenotype shares characteristics with the classic PCOS and D phenotype and scores for hirsutism, androgen levels, lipids, intermediate metabolic syndrome risk. The “non-hyperandrognenic” D phenotype has a mild degree of endocrine disruption. Due to the effects of the small sample size and the similarity of clinical characteristics, it was decided to join phenotypes A+B and phenotypes C+D to establish the different associations resulting in the following.
- Sociodemographic: Age (years of age); ethnic origin (indigenous, Afro-Ecuadorian/Afro-descendant/black/mulatto/montubio/mestizo/white/other); marital status (single, married, widowed, divorced, free union); origin (urban/rural); educational level (none/early education/general basic education/high school/high school/higher education); and socioeconomic level evaluated by means of the INEC survey.
- Clinical: Oligo-amenorrhea, acne, alopecia, acanthosis nigricans (presence/absence); the physical examination to determine hirsutism used the modified Ferriman-Gallwey scale (taking as normal values those above 8), which were described by the patients, confirmed and evaluated by health personnel [4,9].
- Metabolic: Laboratory tests were considered extracted by a blood sample from each participant collected in vacutainer vacuum tubes without anticoagulant after fasting for 12 hours taken from the antecubital vein, analyzed the same day in the hospital’s ISO 9001-certified laboratory: total cholesterol (mg/dl) ≥ 200 abnormal; triglycerides (mg/dl) ≥ 150 abnormal; HDL (mg/dl) ≥ 60 abnormal; LDL (mg/dl) ≥ 160 abnormal (based on Adult Treatment Panel III guidelines); ALT (IU/l) ≥ 33 abnormal; AST (IU/l) ≥ 32 abnormal; total bilirubin (mg/dl) ≥ 1.3 abnormal; direct bilirubin (mg/dl) ≥ 0.30 abnormal; indirect (mg/dl) ≥ 0.80 abnormal; uric acid (mg/dl) ≥ 5.8 abnormal; glucose (mg/dl) ≥ 126 abnormal; HOMA- IR homeostasis assessment model ≥ 2.8 abnormal; glycosylated hemoglobin HbA1C ≥ 6.5 % abnormal; insulin (mg/dl) ≥ 25.1 abnormal [18].
The determination of weight and height was evaluated with a Health Meter (Professional) scale with a measuring rod. To determine height, the patient was asked to remove her shoes and any adornment she might be wearing on her head, to stand upright, to place her heels together and to look straight ahead at a fixed point. With the weight and height data, the body mass index (BMI) was calculated, which corresponds to the ratio between the weight expressed in kilograms and the square of the height, expressed in meters. Abdominal circumference was measured with a tape measure calibrated in millimeters and centimeters. The measurement was taken in the narrowest part of the abdomen or in the region between the last rib and the navel; a value > 85 cm indicates an elevated metabolic risk in the case of women. Hip circumference: Hip size was measured at the widest part of the buttocks measured in (cm). The Waist/Hip Index (cm) results from dividing a person’s waist circumference by his or her hip circumference, both values in centimeters (cm). A value > 0.86 was considered altered [8]. The waist/height index (cm) was considered abnormal > 0.49 to evaluate the distribution of body mass.
Vital signs were taken by the outpatient nursing staff (after verifying that the patient had rested for 5 minutes and in case of finding altered blood pressure levels, two controls were performed at 15 and 30 min), the material for taking blood pressure was a Dash 3000 LG sphygmomanometer, considering the following as abnormal: systolic blood pressure SBP (mm/Hg) ≥ 120 abnormal; diastolic blood pressure DBP (mm/hg) ≥ 80 abnormal.
Other metabolic variables considered: vitamin D (ng/dl) value ≤20 abnormal; ionic calcium (mmol/L) ≤1.1 abnormal.
- Reproductive: Dehydroepiandrosterone DHEAS (ug/dl) ≥ 430 abnormal; total testosterone (ng/ml) ≥ 0.482 abnormal; free testosterone %, 17- OH progesterone(ng/ml) ≥ 1.4 abnormal; Androstenedione A4 (ng/ml) ≥ 3.9 abnormal; Free androgen index was calculated using the formula: Testosterone (nmol)/SHBG (nmol) x 100, considering ≥ 10 abnormal (13); Antimullerian hormone≥ 2.5 abnormal; Sex cell-binding globulin SHBG (nmol/L) ≥114.1 abnormal; Luteinizing hormone LH (mIU/L) ≥11.7 abnormal; Follicle stimulating hormone FSH (mIU/L) ≥12.5 abnormal, and gynecologic ultrasound to determine the presence of polycystic ovaries (>12 follicles, each follicle measuring between 2 and 9 mm and ovarian volume >10cc), in one or both ovaries. Laboratory tests had to be at the follicular stage (3rd to 5th) day of menstruation, in patients with amenorrhea at any period of the menstrual cycle and ultrasound after menstruation.
- Ultrasound: The ultrasound was performed by a Radiologist of the Hospital UTPL- Santa Inés, between the second and third days of the menstrual cycle to determine the number of antral follicles and volume. To be considered with Polycystic Ovarian Morphology (positive), she had to have ≥ 12 follicles in one or both ovaries, measuring between 2 and 9 mm and a total ovarian volume ≥ 10 cc. If a simple cyst, complex cyst, dominant follicle >10 mm or corpus luteum was detected, the ultrasound should be repeated in the next cycle.
2.5. Statistical Analysis
The data obtained were entered in an Excel spreadsheet; they were analyzed with the SPSS program (IMB-SPSS, version 19.0 for Mac); descriptive statistics were used with calculation of frequencies, means, medians, inferential statistics, parametric and nonparametric tests according to each variable. For the sociodemographic variables, a nonparametric test was used to compare the means of two groups because the variable does not approach normal distribution. To establish relationships between dichotomous variables, a logistic regression was performed, calculating OR values with their respective 95% CI. Values of p≤ 0.05 were considered statistically significant.
2.6. Ethical Aspects
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the University of Cuenca: Code 2022-002EO-IE.
Each of the participants was assigned a code so that anonymity and confidentiality would be preserved throughout the process. The patients who decided to participate voluntarily in the study signed an informed consent form describing the subject of the study, objectives, description of the procedures, risks and benefits, rights of the participants, among others.
3. Results
Of the total of the 92 women included in this study 61% (n=56) patients correspond to phenotype A; 13% (n=12) patients are phenotype B; 14% (n=13) patients are phenotype C and 12% (n=11) patients are phenotype D.
3.1. Sociodemographic Characteristics of the Participants
The majority of the participants were under 25 years of age (%), of mixed ethnicity (97.8%), single (94.6%), high educational level (95.7%) and medium-high socioeconomic level (75.4%) (Table 1).
3.2. Clinical Features Associated with the Different PCOS Phenotypes
In women with phenotypes A and B, 97.1% experience oligo-amenorrhea, which is a striking contrast to those with phenotypes C and D. The probability of experiencing oligo-amenorrhea is 30.3 times higher in the former group, as evidenced by a statistically significant p-value, though this is noted with a wide confidence interval. The variables of acne, acanthosis nigricans, hirsutism is more frequent in phenotypes A and B, compared to phenotypes C and D, but gave no association, nor statistically significant values (Table 2).
3.3. Metabolic Profile of the Participants
In the case of women with phenotypes A and B, 38.1% have a BMI greater than or equal to 25. This proportion is 2.1 times higher compared to women with phenotypes C and D. However, it’s important to note that this difference is not statistically significant (Table 3). In women with phenotypes A and B, 36.4% exhibit elevated triglyceride levels of 150 mg/dl or higher. This is 9.1 times more likely when compared to women with phenotypes C and D, and this difference is backed by a statistically significant p-value.
3.4. Reproductive Profile of the Participants
In women with phenotypes A and B, 54.4% have elevated levels of total testosterone. Compared to those with phenotypes C and D, they are 2.4 times more likely to exhibit elevated total testosterone levels, though this difference is not statistically significant. Additionally, 16.7% of women with phenotypes A and B have an elevated free androgen index. When compared to women with phenotypes C and D, the likelihood is 3.6 times higher, but again, this finding is not statistically significant (Table 4). The variables 17 OH progesterone, LH, AMH were also found to be higher in phenotypes A and B, but did not give statistically significant values.
4. Discussion
The purpose of this study was to investigate biodemographic, clinical, metabolic and reproductive variables and their relationship with polycystic ovary syndrome phenotypes in a population of the Ecuadorian Andes. According to the last population census conducted by the Ecuadorian Institute of Statistics and Census (INEC) [19] in the province of Loja, the majority of the population is considered mestizo with 90.2%, the average number of years of schooling for people over 24 years of age is 11.8 years and 6.5 years in the rural population. The illiteracy rate is the lowest in Ecuador with 3.2% [20].
The results found in this research allow us to identify that the classical PCOS phenotypes, composed of types A and B, are the most frequent, followed by type C “ovulatory” and the less frequent type D “non-hyperandrogenic”. This finding is consistent with studies from South America [9,21,22,23] and differs from European and Asian populations, where slightly different phenotypic patterns are observed [14,24,25].
Phenotyping of PCOS has allowed a detailed assessment of the clinical and metabolic spectrum of this condition. Phenotypes A and B, considered classic, include a higher prevalence of oligo-amenorrhea and clinical signs of hyperandrogenism such as acne, consistent with previous literature [26]. In studies conducted in Latin American countries, the most prevalent phenotypes in samples with a mean age similar to our study are A and B [26], presenting overweight and hypertriglyceridemia, in agreement with the findings of our research.
The association between oligo-amenorrhea and phenotypes A and B is particularly notable, reinforcing the concept that menstrual disturbance is a significant marker of classical PCOS and may be an early predictor of other metabolic and cardiovascular comorbidities [27]. Despite the homogeneity of participants’ sociodemographic characteristics, clinical and metabolic associations vary between phenotypes, suggesting that the underlying mechanisms leading to these manifestations may be distinct, and thus potentially require differentiated therapeutic approaches. This study, however, does not examine etiological mechanisms, which is a limitation that will need to be addressed in future research [23].
The importance of ethnicity in the assessment of symptoms such as acne and hirsutism was highlighted in research carried out in Brazil and El Salvador where the Ferriman-Walley scale was applied [28]. It is important to emphasize the need to seek standardisation in the Ferriman-Walley scale modified for each of the study populations (ethnicities) for the evaluation of hirsutism [16], as sometimes the values of European populations are taken as references, which differ from those of Latin American ethnicities. It is reasonable to assume that different genetic backgrounds may influence phenotypic heterogeneity but evidence suggests that Latin American countries are similar in terms of metabolic traits [13].
Some studies also group Phenotypes A, B and C (hyperandrogenic) and compare them with type D (non-hyperandrogenic), finding that hyperandrogenic PCOS have significantly higher frequency of overweight/obesity, hyperglycemia, insulin resistance, hypertension, more altered lipid profiles and metabolic syndrome, also associated with a higher prevalence of cardiometabolic disorders [22]. It is also reported that variation between nationalities, cultures and ethnicities may influence elevated BMI (obesity). The visceral adiposity that is common in obese and non-obese women with PCOS worsens all metabolic and reproductive outcomes; increasing insulin resistance, compensatory hyperinsulinemia, as well as adipogenesis and decreased lipolysis. Obesity sensitizes theca cells that are important in LH stimulation and amplifies functional ovarian hyperandrogenism by positively regulating ovarian androgen production [29].
Previous studies have evaluated the metabolic profile of different PCOS phenotypes in Chilean and Argentinean populations showing evidence of the impact that ethnic diversity and socio-cultural habits of different countries may have. Hyperandrogenism may be strongly related to the development of metabolic alterations, with phenotypes A and B being those with the highest cardiovascular risk compared to phenotype D. This research reinforces the observation that phenotypes A and B have a higher risk of insulin resistance and metabolic disorders such as dyslipidemia and hepatic steatosis, with high prevalence of BMI and abnormal triglyceride levels [13], although high triglyceride levels have not always been identified in Latin American samples [9].
In our study we observed that especially phenotypes A and B have an elevated body mass index and waist circumference compared to phenotypes C and D. Overweight and obesity in polycystic ovary syndrome also predispose to the development of metabolic syndrome, which is not the case in lean women, with geographic differences being observed with higher risks in America compared to Europe and Asia. These differences were explained by BMI in the Americas and Asia, but not in Europe, suggesting that other factors such as genetic variation may be involved [30]. The metabolic profile of the participants highlights the relevance of BMI and triglyceride levels in the pathogenesis of the classical phenotypes suggesting that strategies aimed at lifestyle modification are needed to improve these parameters.
Phenotype A has been found to increase the likelihood of developing metabolic syndrome sixfold relative to phenotype C [22], increasing its prevalence [18]. Given the age of the sample participants, below 25 years, it is difficult to determine the prevalence of metabolic syndrome in our sample, which is usually high in Latin American women with PCOS [13,23]. On the other hand, phenotypes C and D exhibit a milder clinical profile with a lower frequency of signs of hyperandrogenism and significant metabolic alterations as noted in other similar studies [23]. This implies management strategies and follow-up of patients after individualized assessment based on phenotypes.
As reported in a case-control study, lipid profiles are also elevated in patients with PCOS, mainly triglycerides, total cholesterol, low-density lipoprotein (LDL) and cardiovascular risk (TG/HDL). Women with PCOS type D had lower insulin levels than phenotype A [31]. In our study the triglyceride level was higher in the A phenotype. This is consistent with the results of other studies, in which elevated triglyceride level is more at risk in phenotypes A and B, as well as values such as HOMA, insulin, blood pressure levels are found to be higher in the “classical” A and B phenotypes, but the latter were not significant in our sample.
On the other hand, reproductive markers that are observed to be altered may have consequences for fertility and reproductive management [32]. Although the anti-mullerian hormone (AMH) value did not show significant differences, its tendency to be elevated in classical phenotypes requires attention due to its potential role in the assessment of ovarian reserve and reproductive prognosis [33].
Limitations include the small sample size; however, we consider that the results found allow us to obtain valuable information on the phenotypic characteristics of Ecuadorian Andean women in the absence of previous published studies. We also recognize that it was not possible to carry out a control group, due to economic reasons since each study per patient has a cost of 437 dollars and private or public health insurance does not cover the costs as long as there is no evident pathology. On the other hand, it is admitted that the study is cross-sectional and does not allow the results to be extrapolated to other populations. In addition, this study does not examine the etiological mechanisms, which is a limitation that should be addressed in future research.
5. Conclusions
Classical PCOS phenotypes A and B are the most common in Ecuadorian Andean women, with associated increased risks of insulin resistance and metabolic disorders. Ethnic diversity and socio-cultural habits influence the prevalence and clinical manifestations of the phenotypes. Phenotypes A and B have a higher risk of presenting with anovulation disorders and elevated triglycerides compared to phenotypes C and D. Hormonal (reproductive) variables do not differ in the phenotyping of these patients.
Author Contributions
MEE contributed to the conception, design, data acquisition, writing of the article. RS and CM contributed to the conception, design of the study, critical analysis of the data.TO contributed to the design and review and analysis of statistical data. FL and IC, contributed to the critical analysis of the data, results and writing of the article. EB, contributed to the review, critical analysis of data.SA, contributed to data entry in excel table and collecting information from patients and medical records. All authors gave their final approval of the version to be published.
Funding
The laboratory examinations were 80% covered by the patients’ private insurance and 20% by each participant.
Institutional Review Board Statement
The study was approved by the CEISH Ethics Committee of the University of Cuenca: Code 2022-002EO-IE.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
To the Hospital UTPL- Santa Inés, staff of the radiology service Dr. Nathalie Gonzalez, to all the staff of the Laboratory of the Hospital Santa Inés, Dr. Carlos Ruilova (Endocrinologist of the Hospital Santa Inés), and to ANID - MILENIO - NCS2021_013.
Conflicts of Interest
There was no conflict of interest in the conduct of the research and reporting.
References
- Charifson, M.A.; Trumble, B.C. Evolutionary Origins of Polycystic Ovary Syndrome: An Environmental Mismatch Disorder. Evol. Med. Public Heal. 2019, 2019, 50–63. [Google Scholar] [CrossRef] [PubMed]
- Robin, G.; Peigne, M.; Dumont, A.; Plouvier, P.; Rolland, A.-L.; Catteau-Jonard, S.; Dewailly, D. Síndrome de Ovarios Poliquísticos. EMC - Ginecol. 2020, 56, 1–18. [Google Scholar] [CrossRef]
- Ortiz-Flores, A.E.; Luque-Ramírez, M.; Escobar-Morreale, H.F. Polycystic Ovary Syndrome in Adult Women. Med. Clin. (Barc). 2019, 152, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Azziz, R.; Kintziger, K.; Li, R.; Laven, J.; Morin-Papunen, L.; Merkin, S.S.; Teede, H.; Yildiz, B.O. Recommendations for Epidemiologic and Phenotypic Research in Polycystic Ovary Syndrome: An Androgen Excess and PCOS Society Resource. Hum. Reprod. 2019, 34, 2254–2265. [Google Scholar] [CrossRef] [PubMed]
- Dietz de Loos, A.L.P.; Jiskoot, G.; Timman, R.; Beerthuizen, A.; Busschbach, J.J.V.; Laven, J.S.E. Improvements in PCOS Characteristics and Phenotype Severity during a Randomized Controlled Lifestyle Intervention. Reprod. Biomed. Online 2021, 43, 298–309. [Google Scholar] [CrossRef] [PubMed]
- Dapas, M.; Dunaif, A. The Contribution of Rare Genetic Variants to the Pathogenesis of Polycystic Ovary Syndrome. Curr. Opin. Endocr. Metab. Res. 2020, 12, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Vanhauwaert, P.S. Síndrome de Ovario Poliquístico e Infertilidad Polycystic Ovary Syndrome and Infertility. Rev. Clínica Las Condes 2021, 32, 166–172. [Google Scholar] [CrossRef]
- Bajares, D.M.; Pizzi, R. Tratamiento Basado En El Fenotipo. 2016, 76, 93–96. [Google Scholar]
- Rodrigo Carvajal, G.; Cristian Herrera, G.; Arnaldo Porcile, J. Espectro Fenotípico Del Síndrome de Ovario Poliquístico. Rev. Chil. Obstet. Ginecol. 2010, 75, 124–132. [Google Scholar] [CrossRef]
- Goodarzi, M.O.; Carmina, E.; Azziz, R. DHEA, DHEAS and PCOS. J. Steroid Biochem. Mol. Biol. 2015, 145, 213–225. [Google Scholar] [CrossRef]
- Lizneva, D.; Suturina, L.; Walker, W.; Brakta, S.; Gavrilova-Jordan, L.; Azziz, R. Criteria, Prevalence, and Phenotypes of Polycystic Ovary Syndrome. Fertil. Steril. 2016, 106, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Pehlivanov, B.; Orbetzova, M. Characteristics of Different Phenotypes of Polycystic Ovary Syndrome in a Bulgarian Population. Gynecol. Endocrinol. 2007, 23, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Marchesan, L.B.; Ramos, R.B.; Spritzer, P.M. Metabolic Features of Women with Polycystic Ovary Syndrome in Latin America: A Systematic Review. Front. Endocrinol. (Lausanne). 2021, 12, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dapas, M.; Lin, F.T.J.; Nadkarni, G.N.; Sisk, R.; Legro, R.S.; Urbanek, M.; Geoffrey Hayes, M.; Dunaif, A. Distinct Subtypes of Polycystic Ovary Syndrome with Novel Genetic Associations: An Unsupervised, Phenotypic Clustering Analysis. PLoS Med. 2020, 17, 1–28. [Google Scholar] [CrossRef]
- Puttabyatappa, M.; Cardoso, R.C.; Padmanabhan, V. Effect of Maternal PCOS and PCOS-like Phenotype on the Offspring’s Health. Mol. Cell. Endocrinol. 2016, 435, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, M.; Iturrieta, V.; Aguilera, G.; Cárcamo, G.; Galvez, L.; Valdés, P. Características Clínicas y Metabólicas de Síndrome de Ovario Poliquístico En La Ciudad de Temuco. Rev. chil. endocrinol. diabetes 2014, 7, 85–88. [Google Scholar]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 2. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes—2023. Diabetes Care 2023, 46, S19–S40. [Google Scholar] [CrossRef] [PubMed]
- Instituto Ecuatoriano de Estadísticas y Censos del Ecuador Encuesta de Estratificación Del Nivel Socioeconómico NSE 2011. 2011 2011, 1–4.
- INEC Censo Población y Vivienda 2010. Fasciculo Provincial Loja. Ecuador en cifras 2010, 1, 1–8. [Google Scholar]
- Carmona-Ruiz, I.O.; Saucedo-de la Llata, E.; Moraga-Sánchez, M.R.; Romeu-Sarrió, A. Síndrome de Ovario Poliquístico: ¿Ha Aumentado Su Prevalencia? Ginecol. Obstet. Mex. 2015, 83, 750–759. [Google Scholar]
- Tavares, A.; Rêgo Barros, R.C. The Prevalence of Metabolic Syndrome in the Different Phenotypes of Polycystic Ovarian Syndrome. Rev. Bras. Ginecol. e Obstet. 2019, 41, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Ladrón De Guevara, A.; Fux-Otta, C.; Crisosto, N.; Szafryk De Mereshian, P.; Echiburú, B.; Iraci, G.; Perez-Bravo, F.; Sir-Petermann, T. Metabolic Profile of the Different Phenotypes of Polycystic Ovary Syndrome in Two Latin American Populations. Fertil. Steril. 2014, 101. [Google Scholar] [CrossRef]
- Daan, N.M.P.; Louwers, Y.V.; Koster, M.P.H.; Eijkemans, M.J.C.; De Rijke, Y.B.; Lentjes, E.W.G.; Fauser, B.C.J.M.; Laven, J.S.E. Cardiovascular and Metabolic Profiles amongst Different Polycystic Ovary Syndrome Phenotypes: Who Is Really at Risk? Fertil. Steril. 2014, 102, 1444–1451.e3. [Google Scholar] [CrossRef]
- Yang, R.; Li, Q.; Zhou, Z.; Qian, W.; Zhang, J.; Wu, Z.; Jin, L.; Wu, X.; Zhang, C.; Zheng, B.; et al. Changes in the Prevalence of Polycystic Ovary Syndrome in China over the Past Decade. Lancet Reg. Heal. - West. Pacific 2022, 25, 1–10. [Google Scholar] [CrossRef]
- Singh, P.; Barbieri, J.S.; James, W.D.; Thiboutot, D. Letter to the Editor from Singh et Al: “Female Adult Acne and Androgen Excess: A Report from the Multidisciplinary Androgen Excess and PCOS Committee. ” J. Endocr. Soc. 2022, 6, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.Y.; Knochenhauer, E.S.; Bartolucci, A.A.; Azziz, R. Phenotypic Spectrum of Polycystic Ovary Syndrome: Clinical and Biochemical Characterization of the Three Major Clinical Subgroups. Fertil. Steril. 2005, 83, 1717–1723. [Google Scholar] [CrossRef]
- Gabrielli, L.; Aquino, E.M.L. Polycystic Ovary Syndrome in Salvador, Brazil: A Prevalence Study in Primary Healthcare. Reprod. Biol. Endocrinol. 2012, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Glueck, C.J.; Goldenberg, N. Characteristics of Obesity in Polycystic Ovary Syndrome: Etiology, Treatment, and Genetics. Metabolism. 2019, 92, 108–120. [Google Scholar] [CrossRef]
- Lim, S.S.; Kakoly, N.S.; Tan, J.W.J.; Fitzgerald, G.; Bahri Khomami, M.; Joham, A.E.; Cooray, S.D.; Misso, M.L.; Norman, R.J.; Harrison, C.L.; et al. Metabolic Syndrome in Polycystic Ovary Syndrome: A Systematic Review, Meta-Analysis and Meta-Regression. Obes. Rev. 2019, 20, 339–352. [Google Scholar] [CrossRef]
- Jamil, A.S.; Alalaf, S.K.; Al-Tawil, N.G.; Al-Shawaf, T. A Case-Control Observational Study of Insulin Resistance and Metabolic Syndrome among the Four Phenotypes of Polycystic Ovary Syndrome Based on Rotterdam Criteria Female Fertility. Reprod. Health 2015, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Teede, H.J.; Tay, C.T.; Laven, J.; Dokras, A.; Moran, L.J.; Piltonen, T.T.; Costello, M.F.; Boivin, J.; M. Redman, L.; A. Boyle, J.; et al. Recommendations from the 2023 International Evidence-Based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. Fertil. Steril. 2023, 120, 767–793. [Google Scholar] [CrossRef] [PubMed]
- Panidis, D.; Tziomalos, K.; Misichronis, G.; Papadakis, E.; Betsas, G.; Katsikis, I.; Macut, D. Insulin Resistance and Endocrine Characteristics of the Different Phenotypes of Polycystic Ovary Syndrome: A Prospective Study. Hum. Reprod. 2012, 27, 541–549. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram of the participants included in the study.
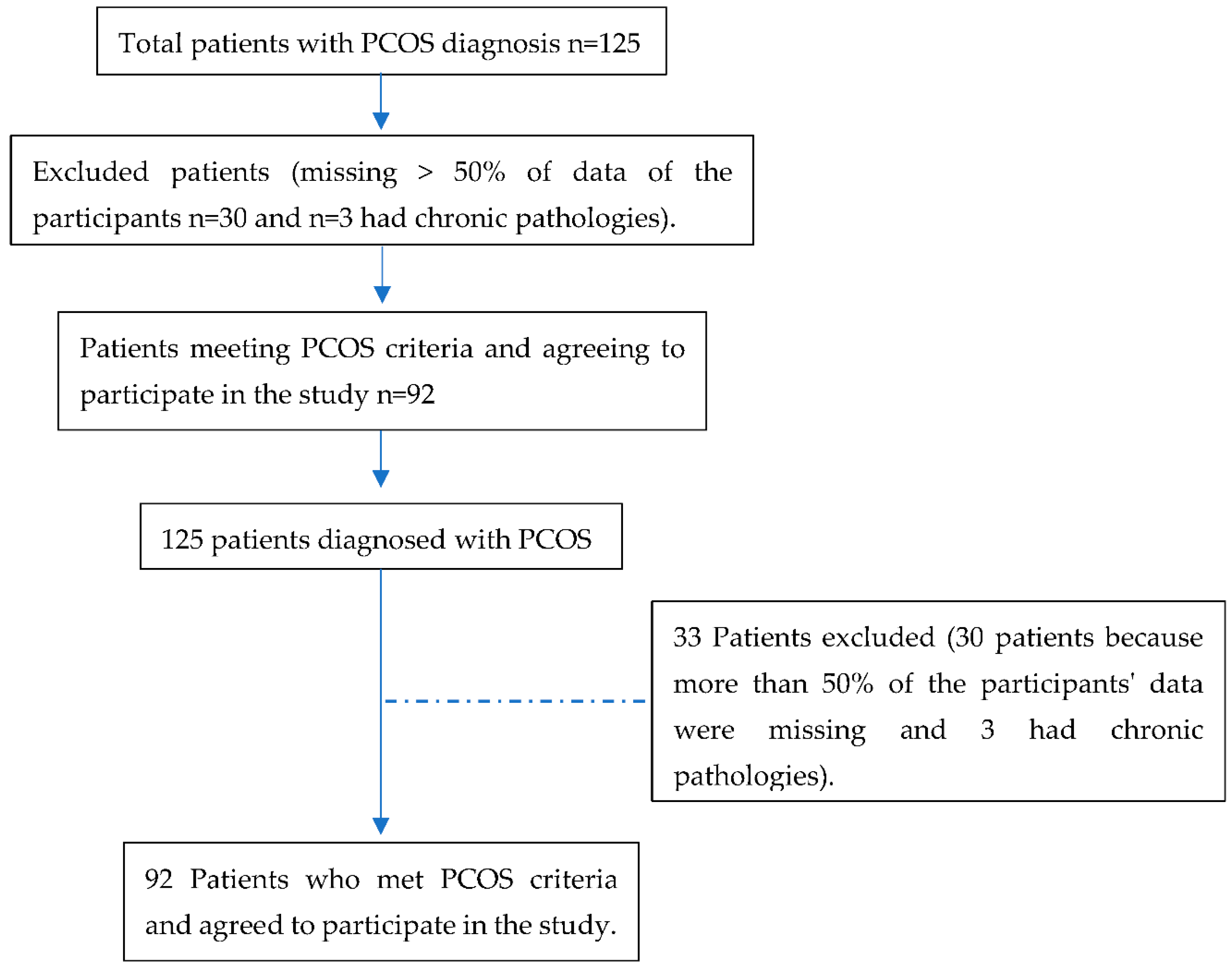

Table 1.
Sociodemographic characteristics and phenotypes of PCOS.
| Biodemographic variables | Totaln (%) |
Phenotypes A y B n(%) |
Phenotypes C y D n(%) |
|---|---|---|---|
| Sample | 92(100) | 69(75.3) | 23(24.7) |
| Age (years ± SD) | 22±3.4 | 22.6±3.8 | 23.6±5.4 |
| Ethnic origin | |||
| Mestiza | 90(97.8) | 67(98.5) | 23(95.8) |
| Origin | |||
| Urban | 88(95.7) | 67(98.5) | 21(87.5) |
| Marital status | |||
| Single | 87(94.6) | 64(94.1) | 23(95.8) |
| Educational level | |||
| Higher | 88(95.7) | 65(95.6) | 23(95.8) |
| Socioeconomic level | |||
| Upper middle | 52(75.4) | 40(76.9) | 12(70.6) |
Table 2.
Clinical variables and association with PCOS phenotypes.
| Clinical variables | Total (%) | Phenotypes A y B n (%) |
Phenotypes C y D n (%) |
OR | IC 95% |
|---|---|---|---|---|---|
| Oligomenorrhea* | 78(85.7) | 66(97.1) | 12(52.2) | 30.3 | 5.9; 153.9 |
| Hirsutism | 61(78.2) | 45(78.9) | 16(76.2) | 1.2 | 0.4; 3.8 |
| Acne | 74(87.1) | 56(88.9) | 18(81.8) | 1.8 | 0.4; 6.8 |
| Alopecía | 22(25.3) | 14(21.2) | 8(38.1) | 0.4 | 0.2; 1.3 |
| Acanthosis nigricans | 40(48.2) | 31(50.0) | 9(42.9) | 1.3 | 0.5; 3.6 |
| Polycystic ovaries ultrasound volume ≥ 10 cc | 65(86.7) | 44(83.0) | 21(95.5) | 0.2 | 0.1; 1.9 |
* Oligomenorrhoea (cycles > 35 days) or amenorrhea (no menstruation in the last 3 months).
Table 3.
Metabolic variables and association with PCOS phenotypes.
| Metabolic variables | Total (%) | Phenotypes A y B n (%) |
Phenotypes C y D n (%) |
OR | IC 95% |
|---|---|---|---|---|---|
| BMI ≥ 25.0 | 29(34.1) | 24(38.1) | 5(22.7) | 2.1 | 0.7; 6.4 |
| Waist to height/ratio ≥0.49 | 45( 60.0) | 36(63.2) | 9(50.0) | 1.7 | 0.6; 4.9 |
| Waist hip/radio ≥ 0.86 | 30(40.5) | 22(40.0) | 8(42.1) | 0.9 | 0.3; 2.6 |
| Total Colesterol ≥ 200 mg/dl | 25(34.2) | 19(33.9) | 6(35.3) | 0.9 | 0.3; 2.9 |
| Triglycerides ≥ 150 mg/dl * | 21(29.2) | 20(36.4) | 1(5.9) | 9.1 | 1.1; 74.2 |
| LDL≥ 160.1mg/dl | 21( 30.0) | 16(29.6) | 5(31.3) | 0.9 | 0.3; 3.1 |
| ALT≥33 U/l | 17(24.3) | 14(25.9) | 3(18.8) | 1.4 | 0.3; 5.6 |
| AST≥ 32 U/l | 11(15.7) | 8(14.8) | 3(18.8) | 0.8 | 0.2; 3.3 |
| Direct Bilirrubin ≥ 0.30 mg/dl | 6(9.7) | 4(8.2) | 2(15.4) | 0.5 | 0.1; 3.0 |
| Uric Acid≥ 5.8 mg/dl | 8(10.3) | 6(10.9) | 2(8.7) | 1.3 | 0.2; 6.7 |
| HOMA-IR ≥ 2.8 | 49(59.0) | 37(59.7) | 12(57.1) | 1.1 | 0.4; 3.0 |
| Insulin≥ 25.1 uUI/ml | 13(15.5) | 12(19.0) | 1(4.8) | 4.7 | 0.6-38.6 |
| Blood pressure>120/80 mm/Hg | 42(50.0) | 32(51.6) | 10(45.5) | 1.3 | 0.5-3.4 |
| Vitamin D | 31(43.7) | 25(43.9) | 6(42.9) | 1.1 | 0.3-3.4 |
* p<0.001.
Table 4.
Reproductive variables and association with PCOS phenotypes.
| Reproductive variables | Total (%) |
Phenotypes A y B (%) |
Phenotypes C y D (%) |
OR | IC 95% |
|---|---|---|---|---|---|
| DHEAS≥ 430 ug/dl | 6(7.7) | 5(8.3) | 1(5.6) | 1.5 | 0.2; 14.2 |
| Total Testosterona ≥ 0.482 ng/ml | 45(48.9) | 37(54.4) | 8(33.3) | 2.4 | 0.9; 6.3 |
| 17-OH Progesterone ≥ 1.4 ng/ml | 37(51.4) | 32(57.1) | 5(31.3) | 2.9 | 0.9; 9.6 |
| Androstenedione≥ 3.9 ng/ml | 22(29.3) | 17(29.3) | 5(29.4) | 1.0 | 0.3; 3.2 |
| LH ( Folicular phase) ≥11.7 mUI/ml | 30(40.0) | 25(44.6) | 5(26.3) | 2.3 | 0.7; 7.1 |
| SHBG≥114.1 nmol/l | 14(16.3) | 11(17.2) | 3(13.6) | 0.8 | 0.2; 3.0 |
| Free androgen index(FAI) | 11(13.9) | 10(16.7) | 1(5.3) | 3.6 | 0.4; 30.1 |
| AMH> 2.5 (ng/mL) | 51(91.1) | 41(93.2) | 10(83.3) | 3.4 | 0.2; 65.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



