
Submitted:
28 December 2023
Posted:
29 December 2023
You are already at the latest version
Abstract
Immune disorders, characterized by dysregulation at cellular and inflammatory levels, result from a complex interplay of genetics and environmental factors that lead to an abnormal immune response against autoantigens, triggering tissue damage. Recent research highlights reactive antibodies as key players in autoimmune diseases and graft rejection, but the complexity of their determination limits their use in clinic. Hence, we studied the specific binding profile of serological antibodies against a panel of cellular membranes in order to determine whether this antigenic panel could be used to diagnose specific immune disorders in humans. For this purpose, cell membrane microarrays of spleen, liver, and kidney tissues of monkey, rat, and human were developed, and human sera were analyzed, including healthy controls, patients with autoimmune disorders, and kidney transplant patients. A significant increase in antibody reactivity against specific monkey kidney and spleen membranes was observed in the serum of patients with lupus nephritis, while kidney transplant patients showed a significant enhancement against human tissues and Human embryonic kidney 293 cells. These results show the potential importance for clinical and basic research purposes of studying the presence of specific IgG against membrane antigens in the serum of patients as potential biomarkers of immune disorders.
Keywords:
inflammation
; autoimmune disorders
; reactive antibodies
; microarray
1. Introduction
Inflammation constitutes a crucial element among the defense mechanisms of human body, being the process by which the immune system detects and eliminates foreign and harmful stimuli [1,2]. Inflammation can manifest as either an acute or a chronic response. On the one hand, acute inflammation is a response of the innate immune system mainly due to external agents such as microorganisms, injuries, trauma, or toxic agents, and constitutes one of the first mechanisms of defense. It is composed of cellular components like macrophages, neutrophils, dendritic cells, and natural killer cells [3,4], many of which migrate to the areas where the antigen or injury is found and initiate the innate immune response [5]. Additionally, inflammation includes blood proteins such as complement and blood coagulation systems to help in the development of the process and in the destruction of the external agent. In contrast, chronic inflammation is not only a consequence of the innate response, but it is also largely mediated by the adaptive immune response that occurs due to the presence of both foreign and self-antigens [1,6,7]. The adaptive immune system is mainly composed of lymphocytes, which circulate in the blood and accumulate in secondary lymphoid organs, like lymph nodes and spleen, among others [8,9]. Chronic inflammation is the primary cause of most chronic diseases, including autoimmune disorders or inflammatory disorders, and poses a substantial threat to both health and longevity [1,10].
Autoimmune disorders are complex diseases characterized by deregulation at both the cellular and inflammatory mediator levels [11]. Certain genetic and environmental factors play a critical role in their development. In these conditions, the immune system mistakenly targets healthy cells due to dysfunction in the adaptive immune system [12,13]. In this context, self-reactive antibodies emerge as potential key indicators of autoimmune disorders, encompassing both autoantibodies and antibodies directed against external antigens [14]. The former primarily results from a genetic predisposition, and are produced by B cells that possess the capability to identify and assail the internal components of the body [15]. Conversely, the latter arises due to the impact of environmental factors, like exposure to toxins, viruses, bacteria, and other infectious agents [15,16]. Conditions within this category include lupus nephritis (LN), systemic lupus erythematosus (SLE), ulcerative colitis (UC), Sjögren's syndrome (SjS), rheumatoid arthritis (RA), and graft rejection as in kidney transplant (KT) patients, among others. These disorders share common characteristics such as an elevated degree of incapacitation of individuals, heightened immune activation, and persistent inflammation—either systemic or localized in specific organs—resulting in the impact on diverse tissues throughout the body [4,17].
The identification of self-reactive antibodies has proven to be valuable for both diagnosis and monitoring, as it facilitates the differentiation of autoimmune disorders, predicts disease progression, and anticipates potential complications. This latter significance is underscored by the fact that the appearance of these antibodies in the serum of patients occurs long before these complications manifest [3,18]. Despite the constant need for more research in this field, the use of detection tools for these antibodies greatly improves the management of these disorders [14]. Enzyme-linked immunosorbent assays (ELISA) and antigen microarrays are generally used for their detection. However, the purification of these antigens can modify their structure and thus, their capacity to be detected by certain self-reactive antibodies, limiting their diagnostic potential. To overcame this limitation, the use of whole cells or membrane fractions can be a potential alternative, as membrane antigens are presented together with the other characteristic compounds of those membranes such as lipids. The printing of whole cells or membrane fractions on glass slides has been used to study membrane proteins and lipids by radioligand binding studies, enzymatic analyses or immunoassays [19,20,21], which have demonstrated that not only the structure and functionality of membrane proteins, but also their antigenic profile seem to be preserved in these cell membrane microarrays (CMMAs). Thus, this research focused first on the development of a methodology for the identification of reactive antibodies in the serum of patients with autoimmune disorders, using CMMAs containing kidney, spleen and liver tissues from rats, monkeys, and humans. On the other hand, a second objective was defined focusing only on sera from kidney transplant patients, due to the importance of reactive antibodies in the rejection of this type of graft. In both cases, a optimization process was performed to define the panel of samples included in the microarrays and the immunological protocol used. A significant binding of Immunoglobulin G (IgG) to the immobilized samples on the microarrays was achieved, demonstrating the effectiveness of the test to detect these reactive antibodies.
These studies demonstrate the potential of the technology, although further specific developments and expansion of the serum collection would be necessary to achieve a diagnostic device that would help clinicians in the early detection and monitoring of patients with these types of autoimmune conditions.
2. Results
2.1. Detection of self-reactive antibodies in sera from patients with autoimmune disorders
A total of 28 sera were examined in the first part of the study. Of the total of sera, 12 came from healthy individuals used as a control group, 5 from patients who underwent kidney transplantation, and the remaining samples from individuals with the following autoimmune conditions: lupus nephritis, systemic lupus erythematosus, ulcerative colitis, Sjögren's syndrome, rheumatoid arthritis and chronic kidney disease (CKD). In the group of Inflammatory disorders, samples from patients who underwent kidney transplantation were included, with the aim of observing whether there was an immune response that could indicate a potential rejection of the graft. The normality of the samples was assessed using the Shapiro-Wilk test; setting significance at α = 0.05. The results indicated that the groups deviated from a Gaussian distribution. The binding of IgGs from the different serum groups to tissues immobilized on the CMMA was compared using a two-way ANOVA with Sídác's post-hoc multiple comparison test. Significant differences (p < 0.05) were observed between the control group and the group of patients with autoimmune disorders in monkey kidney and spleen tissues, as well as some human kidney tissue. Additionally, a t test for unpaired samples was conducted to compare the serum groups, specifically in the tissues where significant differences were obtained with previously made two-way ANOVA, which revealed distinctions between both groups (Figure 1).
2.2. Reactivity of sera to the panel of samples immobilized in CMMAs
To evaluate the reactivity of the 16 sera from patients with autoimmune disorders in each tissue, a two-way ANOVA with Bonferroni's post-hoc multiple comparison test was carried out. Significant differences compared to control group (p < 0.05) were observed mainly in the sera of LN, SjS, and CKD to specific samples immobilized in CMMAs. A heat map was generated using the p-values derived from the two-way ANOVA (Figure 2).
In addition, the patient’s sera were examined by categorizing them according to the pathology. Then the reactivity of these sera was analyzed and compared with the control group, specifically in the tissues with the highest binding of reactive antibodies. The normality of the samples was assessed using the Shapiro-Wilk test, with significance set at α = 0.05. A one-way ANOVA was conducted with Dunnett's and Holm-Sidák post-hoc multiple comparison test for sera that exhibited a normal distribution, while a Kruskal-Wallis test with Dunn's post-hoc multiple comparison test was employed for those that did not conform to a normal distribution. The results obtained show significant differences for LN compared to the control group (Figure 3).
2.3. Evaluation of the test performance in the detection of reactive antibodies
Finally, an assessment of the test performance for reactive antibody detection in LN and other autoimmune disorders was conducted through a receiver operating characteristic (ROC) curve analysis [22,23]. The analysis revealed an area under the curve (AUC) of 0.98 specifically for LN compared to the control group, revealing notable sensitivity and specificity. However, the same high level of sensitivity and specificity was not achieved for the remaining studied autoimmune disorders (Figure 4).
2.4. Detection of self-reactive antibodies in sera from patients with KT
A second part of the study was developed to evaluate the reactivity of sera from patients who received kidney transplant against a specific antigenic panel. This last one was conformed of several human and rat spleen, liver, and kidney tissues, as well as monkey kidney tissue. In addition, HEK 293 cells were included. For the analysis, the sera were separates in two groups. The first group comprised all healthy patients, serving as control (n=6). The second group consisted of patients with kidney transplant (n=10). Each serum was analysed in triplicate under identical conditions to validate the obtained results. The results obtained deviated from a Gaussian distribution according to the Shapiro-Wilk test; setting significance at α = 0.05. The binding of IgGs from the different serum groups to tissues immobilized on the CMMA was compared using a two-way ANOVA with Sídác's post-hoc multiple comparison test. Significant differences (p < 0.05) were observed between the control group and the group of patients with KT in human kidney tissue and HEK 293 cells (Figure 5).
2.5. Reactivity of renal transplant patients´ sera to the CMMAs antigenic panel
To convey the reactivity of each serum in comparison to the control group against the antigenic panel sensor, a two-way ANOVA with Bonferroni's post-hoc multiple comparison test was carried out. The serum of patients 76 and 81 displayed the greatest reactivity against the panel of antigens included in the CMMAs. Sera 75, 77, 78, 79, 80, 82, and 83 also exhibited some reactivity as well but only in specific samples. In this context, HEK 293 cells and human kidney tissue showed the highest binding of reactive IgG from the sera anaylised. A heat map was generated using the p-values derived from the two-way ANOVA (Figure 6).
2.6. Principal components analysis (PCA)
To assess the distinctions among all the tissues immobilized on the CMMAs in detecting reactive sera, a principal component analysis (PCA) was conducted based on the p-values obtained from the two-way ANOVA analysis. The analysis focused on the fourth and the seventh components of all tissues.
On the left side of the analysis, all sera were depicted, including both control or negative sera in grey and transplanted or positive sera in orange. The graph illustrates the test's ability to differentiate between different groups, identifying transplant sera and control sera as belonging to their respective groups. On the right side, the graph represents the ability of each human tissue to discriminate between positive and negative sera (Figure 7).
2.7. Evaluation of the test performance. Receiver Operating Characteristic curve
Using the acquired results, a ROC curve was conducted to assess the accuracy sensitivity and specificity of the test [22,23]. The analysis revealed an area under the curve of 0.82, highlighting notable sensitivity and specificity of the test to detect reactive antibodies in sera from patients with kidney transplant (Figure 8).
3. Discussion
Despite recent advances in science in general and immunology in particular, diagnosing and managing autoimmune disorders remains a major challenge. This is attributed to the necessity for multiple tests to arrive at a diagnosis [24]. Additionally, the process can become quite sluggish due to the symptoms and damage not commonly manifesting at the onset of the disease; they may gradually appear over time or occur intermittently [25]. In this context, a tool like CMMAs to identify reactive antibodies in the serum of patients with autoimmune disorder during the initial phases of the disease could pave the way for improved monitoring and control of such patients even in asymptomatic periods [21]. This could involve early intervention with immunosuppressants or alternative therapies, preventing potential long-term damage to other tissues or organs before it manifests. Additionally, CMMAs open avenues for personalized diagnosis and therapy. Though these possibilities are currently distant, they have the potential to offer the most accurate solutions for patients and clinicians. ThusPrincipio del formularioThus, , the first part of the study aimed to assess the presence of self-reactive antibodies in the serum of patients with LN and other autoimmune disorders, comparing them with sera from healthy individuals. CMMAs with a panel of membrane samples immobilized were used as antigenic panel to test diverse sera. The results obtained underscore the efficacy of this test in detecting LN, thereby validating microarray immunodetection technology as a valuable diagnostic and monitoring tool for autoimmune disorders patients.
Differences between the control group (healthy subjects) and the different autoimmune disorders group were scrutinized in animal tissues as well as human tissue. Animal tissues were incorporated into the study to assess whether comparable outcomes could be achieved in both human and animal tissues. This was prompted by the considerable complexity and cost associated with obtaining human tissue compared to animal tissue. The challenge of acquiring human samples, coupled with the high cost, makes it more convenient to procure a substantial quantity of animal tissues, thereby enhancing the reproducibility of the results. The results obtained revealed that the IgG binding levels of sera from patients with LN to the spleen and kidney tissues of monkeys were comparable to those obtained with the corresponding human tissues.
Although this study assessed various autoimmune disorders, it was in the sera of LN patients where a higher reactivity was observed against the antigenic panel. These results may stem from the pronounced heterogeneity of LN compared to other autoimmune disorders under scrutiny that primarily target specific tissues or glands, such as ulcerative colitis [26,27,28]. LN is characterized by a high production of autoantibodies, which lead to the formation of immune complexes that are subsequently deposited in the glomerulus, initiating an inflammatory reaction and causing kidney damage over time [29,30,31,32,33]. Sera from individuals with SLE were also included in the study, a disease known for its high heterogeneity as well [34]. However, as the sera were studied in kidney, spleen, and liver tissues, and considering that LN involves antibodies specifically targeting the kidney, heightened reactivity in these tissues was consequently noted in these sera [35,36,37,38]. In the case of SjS, despite being deemed a systemic autoimmune disorder, where complications in the kidneys have also been documented, this is not very common. Only 5% of the total reported cases have renal complications, and no significant differences were identified in the conducted study [39,40]. Similar patterns are observed in RA, where kidney complications are more prevalent than SjS; however, no significant differences were identified in this regard in the study [41]. It is essential to highlight that these findings should be strengthened by expanding the number of individuals under evaluation.
The tissues that exhibited a higher antigenic recognition by the sera were the kidney and spleen tissues from both monkeys and humans. This may be, as above mentioned, principally attributed that the LN specifically target antigens in the kidneys. Regarding the spleen, the explanation may lie in the fact that the spleen, being a secondary lymphoid organ where the blood is filtered from pathogens and abnormal cells, could enhance the interaction between antigen-presenting cells and lymphocytes in response to the antigens in the sera [42]. The results revealed similarity in both animal and human tissues.
Afterward, a ROC curve analysis was conducted to assess the validity of the CMMAs test [22,23]. The approach employed to identify the optimal threshold involved calculating the distance of each cut-off point from the coordinates (0, 1) in the upper-left corner of the ROC space. At this juncture, the sensitivity was 100%, and specificity of 1 was 0%; hence, within our dataset, the threshold value on the ROC curve closest to this point was deemed the most optimal [22,23]. Based on the findings, CMMAs containing an antigenic panel of both monkey and human kidney and spleen tissues could potentially be employed as a tool for detecting reactive antibodies in sera from patients with LN. It is important to note that these results need to be reinforced with a larger number of samples. Principio del formulario
The outcomes align with the findings reported in the literature [43,44,45,46], which indicates that sera from patients with autoimmune disorders exhibit higher reactivity compared to sera from healthy individuals [47,48]. Consequently, these reactive antibodies can serve as markers for identifying out breaks of such pathologies and adjust the medication, even though it is acknowledged that there may be the presence of reactive antibodies on healthy patients [25].
Because of the significance of reactive antibodies in kidney transplant rejection [3] a second part of the study was carried out. Sera from immunosuppressed patients were employed to analyze whether the activation of the immune system, associated with transplant rejection, could be detected through CMMA technology. The aim was to observe an increased IgG binding, which should not be evident due to their immunosuppressive treatment. Additionally, since these patients did not exhibit rejection symptoms at the time of sample extraction, the early detection of elevated IgG binding to CMMAs could serve as a potential predictor for transplant rejection.
Therefore, this second study was focused on assessing the immunological reactivity of sera from kidney transplant patients against an antigenic panel consisting of both animal and human tissues. Additionally, HEK 293 cells were included as part of the antigenic sensor. The inclusion of these cells was based on studies reported in the literature validating their use in various areas of experimentation [49]. These areas encompass studies on protein expression and interaction, viral packaging, and even antibody detection [49,50]. Moreover, since these cell lines are more readily available from commercial suppliers compared to tissues from both humans and animals, their incorporation into the study would enhance result reproducibility and save costs. The study aimed to determine whether optimizing both the microarray and the immunological protocol used would result in increased binding signal of the IgG to the tissues immobilized on the microarray.
Differences between the control group and the KT group were scrutinized in the antigenic panel of tissues immobilized on the CMMAs. The results demonstrated a significant binding of IgG from the sera of KT patients to HEK cells and certain human kidney tissues. Although, HEK 293 cell lines is used as kidney epithelial cell lines [50], they also express some proteins specific from immature neurons, e.g. neurofilament proteins or alpha-internexin [51]. Hence, it is still unclear whether they should be considered a model of kidney cells or whether they should be considered instead as immature neurons [49,51,52,53]. Given this information, the significant rise in IgG binding to this cell line could be attributed to both its expression of inflammatory biomarkers (neurofilament proteins [54]) and its representation of human kidney epithelium. Anyhow, it is suggested that HEK 293 cells could be a great tool to be utilized during the monitorization of KT patients, enhancing the prediction capability of clinicians to detect possible kidney transplant rejection.
The sensitivity and specificity of the test to detect reactive antibodies in the tissue panels studied was determined. For that a PCA and a ROC curve were carried out, validating the functionality of the CMMAs. Therefore, demonstrating that the presence of specific IgG against membrane antigens in the serum of patients can be used as possible biomarkers of immune disorders.
The results obtained align with what is reported in the literature [55,56,57,58]. It is well known that reactive antibodies play a crucial role in graft survival in KT. This is due to its direct relationship with rejection and therefore decreased long-term graft survival. For these reasons, it is vital to maintain monitoring of the recipient's immune response to the graft [59].
Monitoring the immune response in transplant patients is a common practice during post-transplant treatment. The assessment includes the evaluation of transplant stability, renal function, and the recipient's immune system sensitization to the new organ [60,61]. Additionally, managing immunosuppressive treatment is a crucial aspect to monitor due to its role in long-term graft survival. While reducing it could decrease toxicity and risks of opportunistic infections, it might elevate the risk of immunological rejection [3,62]. Therefore, achieving an appropriate balance is crucial. Currently, various methods exist for monitoring these patients, ranging from biopsies, serum creatinine levels, immunoassays to even predictions based on artificial intelligence [61].
Biopsies, despite being the gold-standard technique for monitoring transplant survival, are highly invasive. On the other hand, monitoring of serum creatinine levels lacks sensitivity and specificity, although they are less invasive than biopsies. Additionally, once these levels of creatinine manifest, the damage to the graft may already be irreversible [61]. Hence, the detection of reactive antibodies against the graft through immunoassays is highly promising. ELISA-type techniques are the preferred ones, renowned for their high precision and sensitivity [24,63]. Nevertheless, their performance is overshadowed by the fact that their analysis times are lengthy, requiring qualified and experienced personnel as well as specialized laboratory equipment. Furthermore, they require higher volume of reagents and sample, making it less cost-effective techniques than CMMA [24]. Consequently, having tools that overcome these drawbacks like the CMMAs technology, would enhance the prognosis for these patients and streamline the management of the disease and its treatment [21,64]. CMMAs are cost-effective approach which also opens the possibility of creating useful POCT tools, since they require less sample, less processing times and they are less complex to carry out, with the possibility of multiplexing. Anyway, further studies will be required to explore how far the potential of CMMAs in monitoring inflammatory disorders reaches.
4. Materials and Methods
4.1. Serum samples
A total of 39 human serum samples were used in this study. Of them, the 21 samples of patients with autoimmune disorders or kidney transplantation were supplied by the BioIVT (Frankfurt, Germany), 6 control sera from the BioIVT (Frankfurt, Germany), and 12 control sera from the Biobank of Aragon Health System (Zaragoza, Spain). This latter acquisition was evaluated by the relevant ethical committees, obtaining their approval (approval ID: C.I. PI23/291). The samples were stored at -80ᵒC until analysis. The characteristics of these sera are shown in the following tables. It should be noted that KT patients were under immunosuppression treatment.

Table 1.
Information of the different human control serum samples and human serum samples from patients with autoimmune conditions used for the development of the assay.
Table 1.
Information of the different human control serum samples and human serum samples from patients with autoimmune conditions used for the development of the assay.
| ID | Age At Excision | Sex | Primary Diagnosis | Supplier |
|---|---|---|---|---|
| 248900A8 | 45 | Female | Lupus nephritis | BioIVT |
| 286224A5 | 51 | Female | Systemic lupus erythematosus | BioIVT |
| HMN645046 | 36 | Female | Lupus nephritis | BioIVT |
| HUMANSRM-875072 | 55 | Female | Systemic lupus erythematosus | BioIVT |
| HMN773201 | 54 | Female | Sjogren syndrome | BioIVT |
| HMN700845 | 55 | Female | Sjogren syndrome | BioIVT |
| HMN711044 | 54 | Female | Chronic kidney disease | BioIVT |
| HMN776494 | 54 | Female | Chronic kidney disease | BioIVT |
| HUMANSRM-838031 | 60 | Male | Ulcerative colitis | BioIVT |
| HMN1073049 | 32 | Female | Lupus nephritis | BioIVT |
| HMN869646 | 72 | Male | Rheumatoid Arthritis | BioIVT |
| HMN410375 | 68 | Male | Kidney transplant | BioIVT |
| HMN410376 | 49 | Male | Kidney transplant | BioIVT |
| HMN410377 | 64 | Female | Kidney transplant | BioIVT |
| HMN410378 | 54 | Female | Kidney transplant | BioIVT |
| HMN410379 | 25 | Male | Kidney transplant | BioIVT |
| HMN410380 | 66 | Male | Kidney transplant | BioIVT |
| HMN410381 | 60 | Female | Kidney transplant | BioIVT |
| HMN410382 | 68 | Male | Kidney transplant | BioIVT |
| HMN410383 | 70 | Male | Kidney transplant | BioIVT |
| HMN410384 | 58 | Male | Kidney transplant | BioIVT |
| HMN410388 | 83 | Female | Control | BioIVT |
| HMN410389 | 25 | Male | Control | BioIVT |
| HMN410390 | 60 | Female | Control | BioIVT |
| HMN410391 | 19 | Male | Control | BioIVT |
| HMN410392 | 29 | Female | Control | BioIVT |
| HMN410393 | 30 | Female | Control | BioIVT |
| AAA8816702 | 45 | Male | Control | Biobank of Aragon Health System |
| AAA8825493 | 46 | Male | Control | Biobank of Aragon Health System |
| AAA8825485 | 45 | Male | Control | Biobank of Aragon Health System |
| AAA7371433 | 36 | Female | Control | Biobank of Aragon Health System |
| AAA8825480 | 59 | Female | Control | Biobank of Aragon Health System |
| AAA8825474 | 49 | Male | Control | Biobank of Aragon Health System |
| AAA8825470 | 42 | Male | Control | Biobank of Aragon Health System |
| AAA8825467 | 67 | Male | Control | Biobank of Aragon Health System |
| AAA8825462 | 20 | Female | Control | Biobank of Aragon Health System |
| AAA8825459 | 54 | Male | Control | Biobank of Aragon Health System |
| AAA8825453 | 20 | Female | Control | Biobank of Aragon Health System |
| AAA8825408 | 48 | Male | Control | Biobank of Aragon Health System |
4.2. Tissue samples
Tissues from human kidney, spleen and liver biopsies were supplied by the AMSBIO (Abingdon, Oxfordshire, UK) tissue bank according to its ethical protocols (Table 3). Likewise, kidney, liver, and spleen tissue samples from male monkeys of the species Macaca fascicularis, approximately 4 years old, from the CIMA (Applied Medical Research Center of the University of Navarra) (Navarra, Spain) were included in the study. In addition, tissues of kidney, spleen and liver of rat were included as a control. They were supplied by the University of the Basque Country (Leioa, Spain). Lastly, HEK 293 cells that were used in the last part of the study were obtained from Sigma-Aldrich (Darmstadt, Germany).
4.3. Cell Membrane Microarray Fabrication
CMMAs were composed of a collection of cell membrane homogenates isolated from different tissues, including kidney, liver, and spleen of rat, monkey, and human. Additionaly, HEK cells were immobilized along with previous tissues for the second study. Briefly, samples were homogenized using either a disperser (Ultra-Turrax® T10 basic, IKA, Staufen, Germany) or a Teflon-glass grinder (Heidolph RZR 2020, Schwabach, Germany) in 20 volumes of homogenization buffer (1 mM EGTA, 3 mM MgCl2, and 50 mM Tris-HCl, pH 7.4) supplemented with 250 mM sucrose. The crude homogenate underwent a 3857 g centrifugation (AllegraTM X 22R centrifuge, Beckman Coulter, Brea, CA, USA) for 5 min at 4 ◦C. The collected supernatant was centrifuged at 18,000 g (Microfuge® 22R centrifuge, Beckman Coulter, Brea, CA, USA) for 15 min at 4 ◦C. The pellet was washed in 20 volumes of homogenized buffer and subjected to a second centrifugation under the same conditions. Subsequently, the supernatants were finally discarded, and the pellets were frozen at −80 ◦C until the fabrication of CMMAs, except for one aliquot, which was reserved for determining the protein concentration. Protein concentration was determined by the Bradford method [65] and adjusted to the final concentration.
Membrane homogenates were resuspended in printing buffer and printed onto glass slides using a noncontact microarrayer (Nanoplotter NP 2.1), depositing two replicates of each sample (30 nL/spot) onto pre-activated glass microscope slides. Membrane homogenates of each tissue were obtained from different individuals. The printing process was carried out under controlled humidity (relative humidity 60%) at a controlled temperature of 4 ◦C. CMMAs were stored at −20 ◦C until usage [64]. Prior to usage, CMMAs underwent validation through various methods [66,67]. Finally, the array contains different concentrations of rat brain cortex, which we use to calculate the amount of protein, and different concentrations of human IgGs, which we use to calculate the amount of reactive IgG in each spot, in addition to a spot of Anti-Human IgG that will indicate the total amount of IgGs contained in each serum.
4.4. Immunoassay Procedure
To detect reactive antibodies in the sera from patients with autoimmune disorders, the following protocol was implemented during the first part of the study. First, the slides were defrosted and dried for 30 minutes at room temperature in a drying chamber. Subsequently, fixation was performed with 70% methanol (Thermo Fisher Scientific, Waltham, MA, USA) at -20ºC for 10 minutes. Then, the slides were washed twice for 5 minutes with phosphate-buffered saline (sodium dihydrogen phosphate dehydrated 77 mM, sodium hydrogen phosphate monohydrated 24.2 mM, sodium chloride 1.4 M, pH 7.4) with 0.25% Triton (v/v) (0.25% PBS-T) on a slide envelope with shaking. The microarrays were then incubated with blocking solution (5% normal goat serum (NGS) (Vector Laboratories, New Ark, CA, USA), in 0.25% PBS-T) for 30 min at room temperature, followed by one-hour incubation with AffiniPure Fab Fragment Goat Anti-Human IgG (H+L) (Jackson ImmunoResearch, West Grove, PA, USA). Microarrays were incubated overnight at 4°C in a slide humidity chamber with the sample diluted 1:200 in blocking solution. After incubation, the slides were washed three times with 0.25% PBS-T for 5 minutes each in a slide envelope with shaking. The slides were then dried with a fan for 10 minutes and incubated for 1 h with goat anti-human IgG Alexa fluor 633 secondary antibody (Life Technologies Corporation, Carlsbad, CA, USA) at 2mg/ml in 2.5% NGS and 0.25% PBS-T, at room temperature in a dark humidity slide chamber. With this incubation, we guarantee that only the IgG of the sera bound to the immobilized tissue will be detected. After incubation, the slides were washed twice with 0.25% PBS-T and twice with 1X PBS for 5 minutes each in a slide envelope with shaking. Finally, dipping was carried out in distilled water. The slides were dried with a fan, and the fluorescent signal was revealed using a ChemiDoc: Universal Hood 3 imaging system (BioRad, Hercules, CA, USA) with Green EPI laser illumination and a 605/650 nm filter. The subsequent figure illustrates the sequence of steps that were undertaken (Figure 9).
For the second part of the study, several optimizations were made based on the main protocol or previous protocol. First, the slides were defrosted and dried for 30 minutes at room temperature in a drying chamber. Subsequently, fixation was performed with 70% methanol at -20ºC for 10 minutes. Then, the slides were washed three times for 10 minutes with 0.25% PBS-T on a slide envelope with shaking. The microarrays were then incubated with blocking solution for one hour at room temperature, followed by one-hour incubation with AffiniPure Fab Fragment Goat Anti-Human IgG (H+L). The slides were washed three times for 10 minutes with 0.25% PBS-T on a slide envelope with shaking. Microarrays were incubated for two hours in a slide humidity chamber with the sample diluted 1:30 in blocking solution. After incubation, the slides were washed three times with 0.25% PBS-T for 10 minutes each in a slide envelope with shaking. The slides were then dried with a fan for 10 minutes and incubated for 1 h with goat anti-human IgG Alexa fluor 633 secondary antibody at 2mg/ml in 2.5% NGS and 0.25% PBS-T, at room temperature in a dark humidity slide chamber. After incubation, the slides were washed three times with 0.25% PBS-T and twice with 1X PBS for 5 minutes each in a slide envelope with shaking. Finally, dipping was carried out in dis-tilled water. The slides were dried with a fan, and the fluorescent signal was revealed using a ChemiDoc: Universal Hood 3 imaging system with Green EPI laser illumination and a 605/650 nm filter.
4.5. Data processing and Normalization
The signal was quantified using ImageScanner software (IMG Pharma Biotech S.L., Derio, Spain). Data handling and analysis were carried out using Excel (Microsoft Corporation, Albuquerque, NM, USA) and GraphPad software version 9.2.0 (GraphPad Software, Dotmatics Inc, San Diego, CA, USA). For the microarrays, the analysis data obtained were normalized to the amount of total protein and were expressed as means of independent data points ± S.E.M. (standard error of the mean). The normality of the data was tested using Shapiro–Wilk statistical test with α = 0.05. For Gaussian distributed data, a statistical analysis was performed by two-way ANOVA with Bonferroni’s post-hoc multiple comparison test. To analyze non-parametric data, the Kruskal–Wallis test with Dunn’s multiple comparison test was performed. Statistical differences were indicated by p-values < 0.05.
5. Conclusions
CMMAs test has been designed to identify reactive antibodies associated with conditions like nephritic lupus, kidney transplant and various autoimmune disorders. The results obtained affirm the test's reliability in detecting LN when compared to healthy individuals, as demonstrated by the sensitivity and specificity values obtained in the ROC curve. At the same time the efficacy of the test to detect self-reactive antibodies in serum of patients with KT was demonstrated by the sensitivity and precision values obtained in the PCA and the ROC curve. The integration of technologies capable of early detection of reactive antibodies in autoimmune disorders, preceding acute outbreaks or complications in various organs or tissues, has the potential to significantly augment physicians' efficacy. Consequently, this advancement is poised to enhance disease management practices and contribute to superior overall health outcomes for patients.
Author Contributions
Conceptualization, G.B.-G.; Data curation, L.H.-S; Formal analysis, L.H.-S., E.D.-M., J.E.-O., A.E., R.F.; and G.B.-G.; Funding acquisition, E.A., A.R.-G and G.B.-G.; Investigation, L.H.-S. and A.E.; Methodology, L.H.-S. and A.E.; Project administration, G.B.-G.; Resources, E.A. and G.B.-G.; Supervision, A.R.-G and G.B.-G.; Writing—original draft, L.H.-S.; Writing—review and editing, L.H.-S., E.D.-M., C.M., A.R.-G and G.B.-G. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Basque Government Department of Economic development, Sustainability and Environment Bikaintek program, grant number 004-B2/2022, 005-B2/2021 and 006-B2/2021, and University of the Basque Country, UPV/EHU, grant number PIFIND21/02 and PIFIND21/04. In addition, this research was funded by Basque Government: Grants for Consolidated Research Groups (IT1657-22).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of the Biobank of Aragon Health System.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors would like to thank everyone on our teams who were willing to help.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Pahwa, R.; Goyal, A.; Jialal, I. Chronic Inflammation. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2023.
- Michels da Silva, D.; Langer, H.; Graf, T. Inflammatory and Molecular Pathways in Heart Failure-Ischemia, HFpEF and Transthyretin Cardiac Amyloidosis. Int J Mol Sci 2019, 20, 2322. [CrossRef]
- Etxebarria, A.; Díez-Martín, E.; Astigarraga, E.; Barreda-Gómez, G. Role of the Immune System in Renal Transplantation, Types of Response, Technical Approaches and Current Challenges. Immuno 2022, 2, 548–570. [CrossRef]
- Domínguez-Fernández, C.; Egiguren-Ortiz, J.; Razquin, J.; Gómez-Galán, M.; De Las Heras-García, L.; Paredes-Rodríguez, E.; Astigarraga, E.; Miguélez, C.; Barreda-Gómez, G. Review of Technological Challenges in Personalised Medicine and Early Diagnosis of Neurodegenerative Disorders. Int J Mol Sci 2023, 24, 3321. [CrossRef]
- Pontrelli, P.; Grandaliano, G.; Van Kooten, C. Editorial: Kidney Transplantation and Innate Immunity. Front Immunol 2020, 11, 603982. [CrossRef]
- Varela, M.L.; Mogildea, M.; Moreno, I.; Lopes, A. Acute Inflammation and Metabolism. Inflammation 2018, 41, 1115–1127. [CrossRef]
- Nicholson, L.B. The Immune System. Essays Biochem 2016, 60, 275–301. [CrossRef]
- Ferrero-Miliani, L.; Nielsen, O.H.; Andersen, P.S.; Girardin, S.E. Chronic Inflammation: Importance of NOD2 and NALP3 in Interleukin-1beta Generation. Clin Exp Immunol 2007, 147, 227–235. [CrossRef]
- Siu, J.H.Y.; Surendrakumar, V.; Richards, J.A.; Pettigrew, G.J. T Cell Allorecognition Pathways in Solid Organ Transplantation. Front Immunol 2018, 9, 2548. [CrossRef]
- Tsai, D.-H.; Riediker, M.; Berchet, A.; Paccaud, F.; Waeber, G.; Vollenweider, P.; Bochud, M. Effects of Short- and Long-Term Exposures to Particulate Matter on Inflammatory Marker Levels in the General Population. Environ Sci Pollut Res Int 2019, 26, 19697–19704. [CrossRef]
- Siebert, S.; Tsoukas, A.; Robertson, J.; McInnes, I. Cytokines as Therapeutic Targets in Rheumatoid Arthritis and Other Inflammatory Diseases. Pharmacol Rev 2015, 67, 280–309. [CrossRef]
- Richard-Eaglin, A.; Smallheer, B.A. Immunosuppressive/Autoimmune Disorders. Nurs Clin North Am 2018, 53, 319–334. [CrossRef]
- Ilchmann-Diounou, H.; Menard, S. Psychological Stress, Intestinal Barrier Dysfunctions, and Autoimmune Disorders: An Overview. Front Immunol 2020, 11, 1823. [CrossRef]
- Prideaux, L.; De Cruz, P.; Ng, S.C.; Kamm, M.A. Serological Antibodies in Inflammatory Bowel Disease: A Systematic Review. Inflamm Bowel Dis 2012, 18, 1340–1355. [CrossRef]
- Xiao, Z.X.; Miller, J.S.; Zheng, S.G. An Updated Advance of Autoantibodies in Autoimmune Diseases. Autoimmun Rev 2021, 20, 102743. [CrossRef]
- Cusick, M.F.; Libbey, J.E.; Fujinami, R.S. Molecular Mimicry as a Mechanism of Autoimmune Disease. Clin Rev Allergy Immunol 2012, 42, 102–111. [CrossRef]
- Gao, Z.; Feng, Y.; Xu, J.; Liang, J. T-Cell Exhaustion in Immune-Mediated Inflammatory Diseases: New Implications for Immunotherapy. Front Immunol 2022, 13, 977394. [CrossRef]
- Ho, J.; Wiebe, C.; Gibson, I.W.; Rush, D.N.; Nickerson, P.W. Immune Monitoring of Kidney Allografts. Am J Kidney Dis 2012, 60, 629–640. [CrossRef]
- Rienda, B.; Elexpe, A.; Tolentino-Cortez, T.; Gulak, M.; Bruzos-Cidón, C.; Torrecilla, M.; Astigarraga, E.; Barreda-Gómez, G. Analysis of Acetylcholinesterase Activity in Cell Membrane Microarrays of Brain Areas as a Screening Tool to Identify Tissue Specific Inhibitors. Analytica 2021, 2, 25–36. [CrossRef]
- Fernández, R.; Garate, J.; Tolentino-Cortez, T.; Herraiz, A.; Lombardero, L.; Ducrocq, F.; Rodríguez-Puertas, R.; Trifilieff, P.; Astigarraga, E.; Barreda-Gómez, G.; et al. Microarray and Mass Spectrometry-Based Methodology for Lipid Profiling of Tissues and Cell Cultures. Anal Chem 2019, 91, 15967–15973. [CrossRef]
- de la Fuente, M.; Rodríguez-Agirretxe, I.; Vecino, E.; Astigarraga, E.; Acera, A.; Barreda-Gómez, G. Elevation of Tear MMP-9 Concentration as a Biomarker of Inflammation in Ocular Pathology by Antibody Microarray Immunodetection Assays. Int J Mol Sci 2022, 23, 5639. [CrossRef]
- Fawcett, T. An Introduction to ROC Analysis. Pattern Recognition Letters 2006, 27, 861–874. [CrossRef]
- Hajian-Tilaki, K. Receiver Operating Characteristic (ROC) Curve Analysis for Medical Diagnostic Test Evaluation. Caspian J Intern Med 2013, 4, 627–635.
- Castro, C.; Gourley, M. Diagnostic Testing and Interpretation of Tests for Autoimmunity. J Allergy Clin Immunol 2010, 125, S238–S247. [CrossRef]
- Pisetsky, D.S. Pathogenesis of Autoimmune Disease. Nat Rev Nephrol 2023, 19, 509–524. [CrossRef]
- Rahman, A.; Manson, J.J.; Isenberg, D.A. Autoantibodies and Lupus Nephritis. In Lupus Nephritis; Lewis, E.J., Schwartz, M.M., Korbet, S.M., Chan, D.T.M., Eds.; Oxford University Press, 2010; p. 0 ISBN 978-0-19-956805-5.
- Ungaro, R.; Colombel, J.-F.; Lissoos, T.; Peyrin-Biroulet, L. A Treat-to-Target Update in Ulcerative Colitis: A Systematic Review. Am J Gastroenterol 2019, 114, 874–883. [CrossRef]
- Mitsuyama, K.; Niwa, M.; Takedatsu, H.; Yamasaki, H.; Kuwaki, K.; Yoshioka, S.; Yamauchi, R.; Fukunaga, S.; Torimura, T. Antibody Markers in the Diagnosis of Inflammatory Bowel Disease. World J Gastroenterol 2016, 22, 1304–1310. [CrossRef]
- Anders, H.-J.; Saxena, R.; Zhao, M.; Parodis, I.; Salmon, J.E.; Mohan, C. Lupus Nephritis. Nat Rev Dis Primers 2020, 6, 1–25. [CrossRef]
- Schaub, J.A.; Kretzler, M. Chapter 33 - Systems Biology in Diagnosis and Treatment of Kidney Disease. In Regenerative Nephrology (Second Edition); Goligorsky, M.S., Ed.; Academic Press, 2022; pp. 465–479 ISBN 978-0-12-823318-4.
- Borchers, A.T.; Leibushor, N.; Naguwa, S.M.; Cheema, G.S.; Shoenfeld, Y.; Gershwin, M.E. Lupus Nephritis: A Critical Review. Autoimmunity Reviews 2012, 12, 174–194. [CrossRef]
- Mejia-Vilet, J.M.; Rovin, B.H. 59 - Epidemiology and Management of Lupus Nephritis. In Dubois’ Lupus Erythematosus and Related Syndromes (Ninth Edition); Wallace, D.J., Hahn, B.H., Eds.; Elsevier: London, 2019; pp. 727–744 ISBN 978-0-323-47927-1.
- Musa, R.; Brent, L.H.; Qurie, A. Lupus Nephritis. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2023.
- Alarcón-Riquelme, M.E. The heterogeneity of systemic lupus erythematosus: Looking for a molecular answer. Rev Colomb Reumatol 2021, 28, 31–38. [CrossRef]
- Stinton, L.; Barr, S.; Tibbles, L.A.; Yilmaz, S.; Sar, A.; Benediktsson, H.; Fritzler, M. Autoantibodies in Lupus Nephritis Patients Requiring Renal Transplantation. Lupus 2007, 16, 394–400. [CrossRef]
- Elsayed, S.A.; Mohafez, O.M.M. Autoantibodies Spectrum in Lupus Nephritis in a Cohort of Egyptian Patients: Relation to Disease Activity and Prognostic Value. Egyptian Rheumatology and Rehabilitation 2020, 47, 39. [CrossRef]
- Chen, M.; Wang, Y.-Y.; Zhao, M.-H.; Zhang, Y.-K.; Wang, H.-Y. Autoantibodies against Glomerular Mesangial Cells and Their Target Antigens in Lupus Nephritis. Ren Fail 2005, 27, 507–513. [CrossRef]
- Lewis, E.J.; Schwartz, M.M. Pathology of Lupus Nephritis. Lupus 2005, 14, 31–38. [CrossRef]
- Carsons, S.E.; Patel, B.C. Sjogren Syndrome. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2023.
- Aiyegbusi, O.; McGregor, L.; McGeoch, L.; Kipgen, D.; Geddes, C.C.; Stevens, K.I. Renal Disease in Primary Sjögren’s Syndrome. Rheumatol Ther 2021, 8, 63–80. [CrossRef]
- Icardi, A.; Araghi, P.; Ciabattoni, M.; Romano, U.; Lazzarini, P.; Bianchi, G. [Kidney involvement in rheumatoid arthritis]. Reumatismo 2003, 55, 76–85. [CrossRef]
- Lewis, S.M.; Williams, A.; Eisenbarth, S.C. Structure-Function of the Immune System in the Spleen. Sci Immunol 2019, 4, eaau6085. [CrossRef]
- Tipton, C.M.; Fucile, C.F.; Darce, J.; Chida, A.; Ichikawa, T.; Gregoretti, I.; Schieferl, S.; Hom, J.; Jenks, S.; Feldman, R.J.; et al. Diversity, Cellular Origin and Autoreactivity of Antibody-Secreting Cell Expansions in Acute Systemic Lupus Erythematosus. Nat Immunol 2015, 16, 755–765. [CrossRef]
- Ehrenstein, M.R.; Katz, D.R.; Griffiths, M.H.; Papadaki, L.; Winkler, T.H.; Kalden, J.R.; Isenberg, D.A. Human IgG Anti-DNA Antibodies Deposit in Kidneys and Induce Proteinuria in SCID Mice. Kidney Int 1995, 48, 705–711. [CrossRef]
- Leadbetter, E.A.; Rifkin, I.R.; Hohlbaum, A.M.; Beaudette, B.C.; Shlomchik, M.J.; Marshak-Rothstein, A. Chromatin-IgG Complexes Activate B Cells by Dual Engagement of IgM and Toll-like Receptors. Nature 2002, 416, 603–607. [CrossRef]
- Hakkim, A.; Fürnrohr, B.G.; Amann, K.; Laube, B.; Abed, U.A.; Brinkmann, V.; Herrmann, M.; Voll, R.E.; Zychlinsky, A. Impairment of Neutrophil Extracellular Trap Degradation Is Associated with Lupus Nephritis. Proc Natl Acad Sci U S A 2010, 107, 9813–9818. [CrossRef]
- Santambrogio, L.; Marrack, P. The Broad Spectrum of Pathogenic Autoreactivity. Nat Rev Immunol 2023, 23, 69–70. [CrossRef]
- Trier, N.H.; Houen, G. Antibody Cross-Reactivity in Auto-Immune Diseases. International Journal of Molecular Sciences 2023, 24, 13609. [CrossRef]
- Lin, Y.-C.; Boone, M.; Meuris, L.; Lemmens, I.; Van Roy, N.; Soete, A.; Reumers, J.; Moisse, M.; Plaisance, S.; Drmanac, R.; et al. Genome Dynamics of the Human Embryonic Kidney 293 Lineage in Response to Cell Biology Manipulations. Nat Commun 2014, 5, 4767. [CrossRef]
- Jeon, J.-H.; Baek, I.-C.; Hong, C.-H.; Park, K.H.; Lee, H.; Oh, E.-J.; Kim, T.-G. Establishment of HLA Class I and MICA/B Null HEK-293T Panel Expressing Single MICA Alleles to Detect Anti-MICA Antibodies. Sci Rep 2021, 11, 15716. [CrossRef]
- Shaw, G.; Morse, S.; Ararat, M.; Graham, F.L. Preferential Transformation of Human Neuronal Cells by Human Adenoviruses and the Origin of HEK 293 Cells. FASEB J 2002, 16, 869–871. [CrossRef]
- Oka, Y.; Nakajima, K.; Nagao, K.; Miura, K.; Ishii, N.; Kobayashi, H. 293FT Cells Transduced with Four Transcription Factors (OCT4, SOX2, NANOG, and LIN28) Generate Aberrant ES-like Cells. J Stem Cells Regen Med 2010, 6, 149–156. [CrossRef]
- Chae, S.W.; Cho, E.-Y.; Park, M.S.; Lee, K.-B.; Kim, H.; Kim, U. Polycystin-1 Expression in Fetal, Adult and Autosomal Dominant Polycystic Kidney. J Korean Med Sci 2006, 21, 425–429. [CrossRef]
- Larrea, A.; Elexpe, A.; Díez-Martín, E.; Torrecilla, M.; Astigarraga, E.; Barreda-Gómez, G. Neuroinflammation in the Evolution of Motor Function in Stroke and Trauma Patients: Treatment and Potential Biomarkers. Current Issues in Molecular Biology 2023, 45, 8552–8585. [CrossRef]
- Mishra, M.N.; Baliga, K.V. Significance of Panel Reactive Antibodies in Patients Requiring Kidney Transplantation. Saudi J Kidney Dis Transpl 2013, 24, 495–499. [CrossRef]
- Friedewald, J.J.; Kurian, S.M.; Heilman, R.L.; Whisenant, T.C.; Poggio, E.D.; Marsh, C.; Baliga, P.; Odim, J.; Brown, M.M.; Ikle, D.N.; et al. Development and Clinical Validity of a Novel Blood-Based Molecular Biomarker for Subclinical Acute Rejection Following Kidney Transplant. Am J Transplant 2019, 19, 98–109. [CrossRef]
- Naesens, M.; Khatri, P.; Li, L.; Sigdel, T.K.; Vitalone, M.J.; Chen, R.; Butte, A.J.; Salvatierra, O.; Sarwal, M.M. Progressive Histological Damage in Renal Allografts Is Associated with Expression of Innate and Adaptive Immunity Genes. Kidney Int 2011, 80, 1364–1376. [CrossRef]
- Gibney, E.M.; Cagle, L.R.; Freed, B.; Warnell, S.E.; Chan, L.; Wiseman, A.C. Detection of Donor-Specific Antibodies Using HLA-Coated Microspheres: Another Tool for Kidney Transplant Risk Stratification **Portions of This Study Were Delivered as an Oral Presentation at the American Transplant Congress, Seattle, WA, 20–25 May 2005. Nephrology Dialysis Transplantation 2006, 21, 2625–2629. [CrossRef]
- Zhang, Q.; Reed, E.F. The Importance of Non-HLA Antibodies in Transplantation. Nat Rev Nephrol 2016, 12, 484–495. [CrossRef]
- Josephson, M.A. Monitoring and Managing Graft Health in the Kidney Transplant Recipient. Clin J Am Soc Nephrol 2011, 6, 1774–1780. [CrossRef]
- Han, H.S.; Lubetzky, M.L. Immune Monitoring of Allograft Status in Kidney Transplant Recipients. Frontiers in Nephrology 2023, 3.
- Guerra, G.; Srinivas, T.R.; Meier-Kriesche, H.-U. Calcineurin Inhibitor-Free Immunosuppression in Kidney Transplantation. Transplant International 2007, 20, 813–827. [CrossRef]
- Sakamoto, S.; Putalun, W.; Vimolmangkang, S.; Phoolcharoen, W.; Shoyama, Y.; Tanaka, H.; Morimoto, S. Enzyme-Linked Immunosorbent Assay for the Quantitative/Qualitative Analysis of Plant Secondary Metabolites. J Nat Med 2018, 72, 32–42. [CrossRef]
- Elexpe, A.; Nieto, N.; Fernández-Cuétara, C.; Domínguez-Fernández, C.; Morera-Herreras, T.; Torrecilla, M.; Miguélez, C.; Laso, A.; Ochoa, E.; Bailen, M.; et al. Study of Tissue-Specific Reactive Oxygen Species Formation by Cell Membrane Microarrays for the Characterization of Bioactive Compounds. Membranes (Basel) 2021, 11, 943. [CrossRef]
- Bradford, M.M. A Rapid and Sensitive Method for the Quantitation of Microgram Quantities of Protein Utilizing the Principle of Protein-Dye Binding. Anal Biochem 1976, 72, 248–254. [CrossRef]
- Hebert-Chatelain, E.; Desprez, T.; Serrat, R.; Bellocchio, L.; Soria-Gomez, E.; Busquets-Garcia, A.; Pagano Zottola, A.C.; Delamarre, A.; Cannich, A.; Vincent, P.; et al. A Cannabinoid Link between Mitochondria and Memory. Nature 2016, 539, 555–559. [CrossRef]
- Manuel, I.; Barreda-Gómez, G.; González de San Román, E.; Veloso, A.; Fernández, J.A.; Giralt, M.T.; Rodríguez-Puertas, R. Neurotransmitter Receptor Localization: From Autoradiography to Imaging Mass Spectrometry. ACS Chem Neurosci 2015, 6, 362–373. [CrossRef]
Figure 1.
Binding of human IgG from both healthy individuals and patients with autoimmune diseases to various tissues (ng/prot). A) Differences between healthy patients and patients with autoimmune disorders in all tissues; B) in monkey kidney; C) in monkey spleen; and D) in human kidney. Rat (R), monkey (M), human (Hm). p < 0.05 (*); p < 0.01 (**); p < 0.001 (***); and p < 0.0001 (****).
Figure 1.
Binding of human IgG from both healthy individuals and patients with autoimmune diseases to various tissues (ng/prot). A) Differences between healthy patients and patients with autoimmune disorders in all tissues; B) in monkey kidney; C) in monkey spleen; and D) in human kidney. Rat (R), monkey (M), human (Hm). p < 0.05 (*); p < 0.01 (**); p < 0.001 (***); and p < 0.0001 (****).
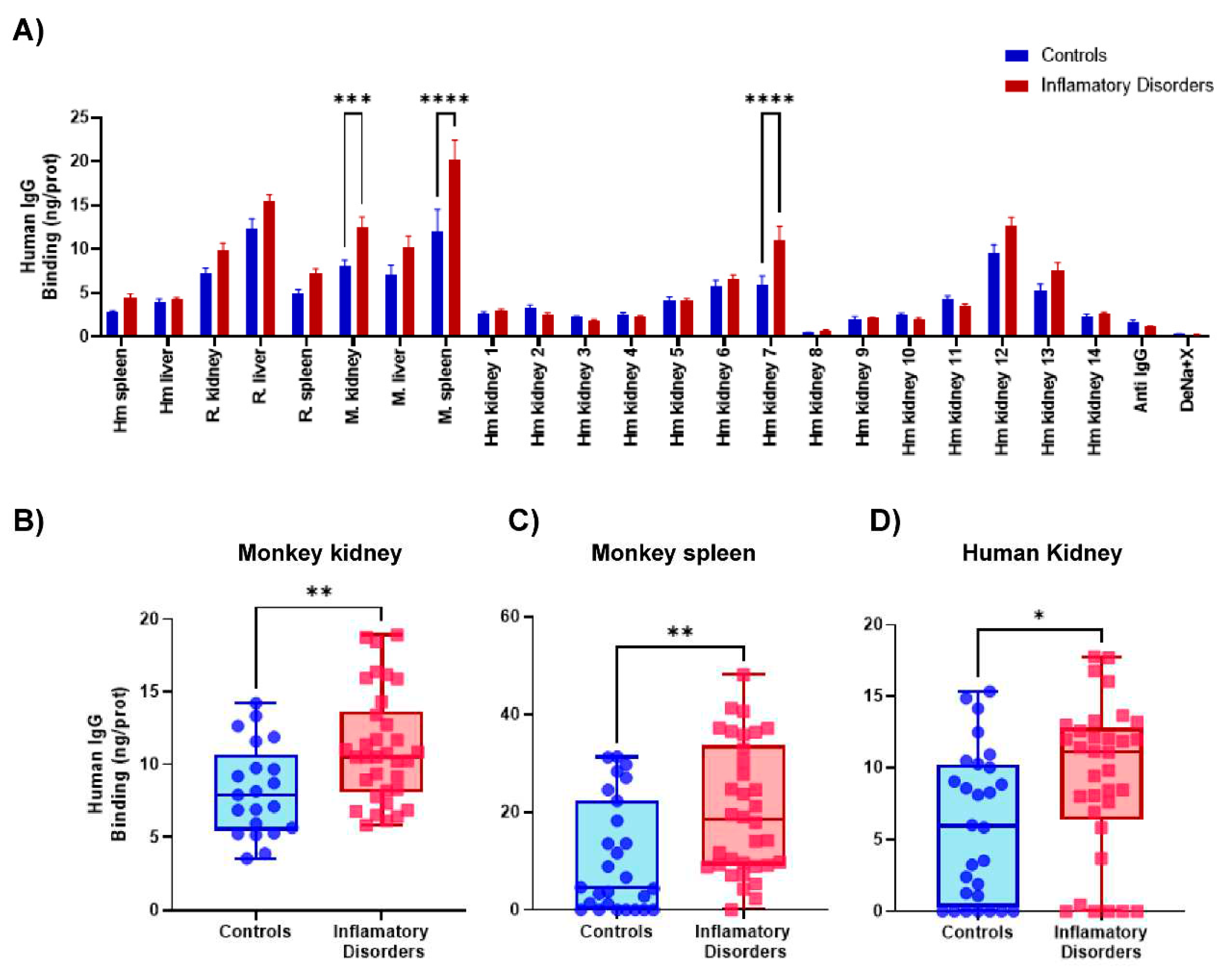
Figure 2.
Heat map obtained from ordinary two-way ANOVA with Bonferroni’s multiple comparison test. SLE: systemic lupus erythematosus; LN: lupus nephritis; SjS: Sjögren's syndrome; CKD: chronic kidney disease; UC: ulcerative colitis; RA: rheumatoid arthritis; R: rat; M: monkey; H: human. P valor of this test is represented on the heat map: p < 0.05 (*); p < 0.01 (**); p < 0.001 (**); and p < 0.0001 (****).
Figure 2.
Heat map obtained from ordinary two-way ANOVA with Bonferroni’s multiple comparison test. SLE: systemic lupus erythematosus; LN: lupus nephritis; SjS: Sjögren's syndrome; CKD: chronic kidney disease; UC: ulcerative colitis; RA: rheumatoid arthritis; R: rat; M: monkey; H: human. P valor of this test is represented on the heat map: p < 0.05 (*); p < 0.01 (**); p < 0.001 (**); and p < 0.0001 (****).
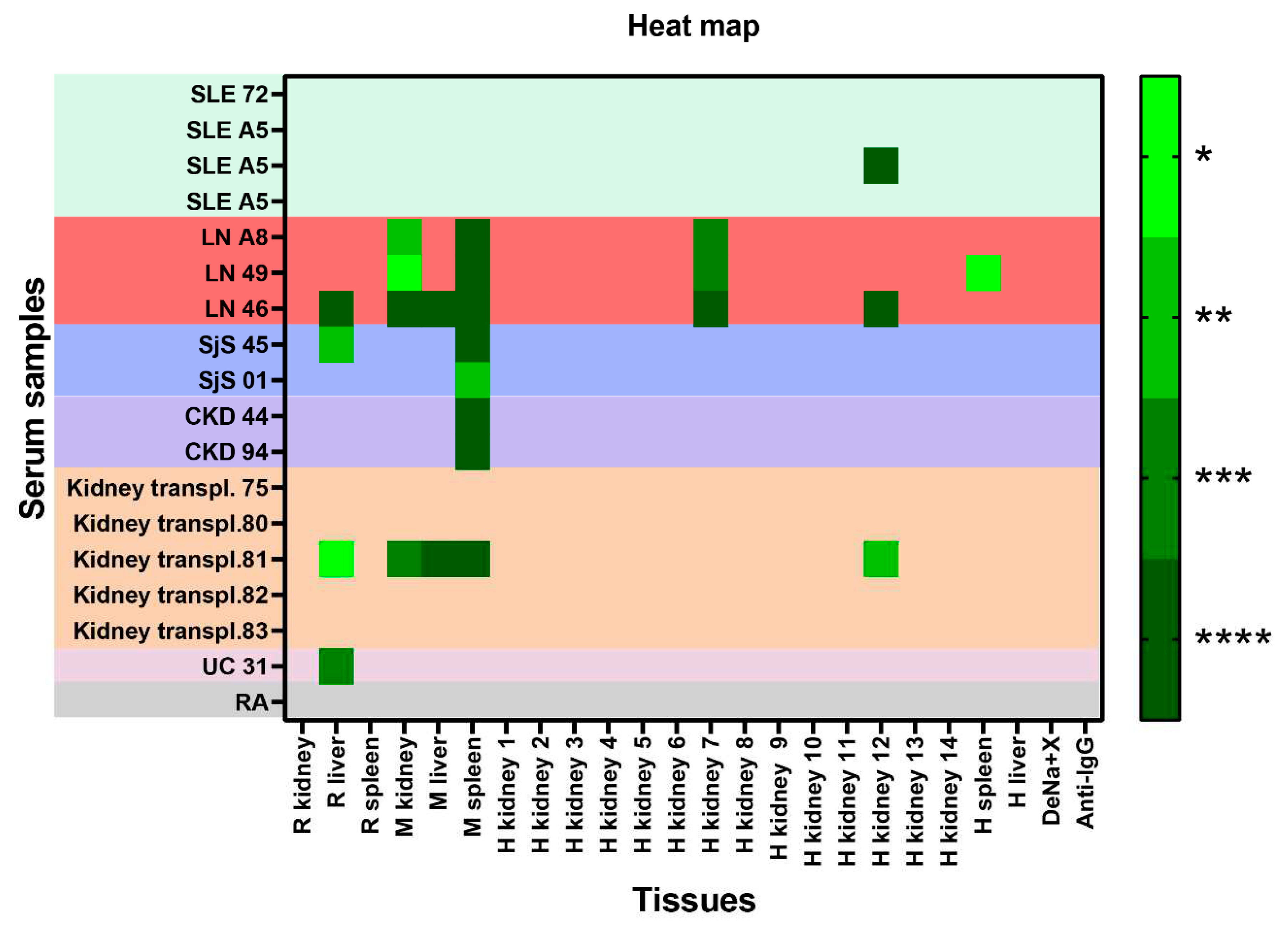
Figure 3.
Binding of human IgG from both healthy individuals and patients with autoimmune disorders to various tissues (ng/prot). A) Differences between healthy patients and patients with autoimmune disorders in human spleen, (ordinary one-way ANOVA with Holm-Sidák multiple comparison test); B) in human kidney (ordinary one-way ANOVA with Dunnett’s multiple comparisons test); C) in monkey spleen (Kruskal-Wallis test with Dunn’s multiple comparison test); and D) in monkey kidney (ordinary one-way ANOVA with Dunnett’s multiple comparison test). p < 0.05 (*); p < 0.01 (***); and p<0.001 (***).
Figure 3.
Binding of human IgG from both healthy individuals and patients with autoimmune disorders to various tissues (ng/prot). A) Differences between healthy patients and patients with autoimmune disorders in human spleen, (ordinary one-way ANOVA with Holm-Sidák multiple comparison test); B) in human kidney (ordinary one-way ANOVA with Dunnett’s multiple comparisons test); C) in monkey spleen (Kruskal-Wallis test with Dunn’s multiple comparison test); and D) in monkey kidney (ordinary one-way ANOVA with Dunnett’s multiple comparison test). p < 0.05 (*); p < 0.01 (***); and p<0.001 (***).
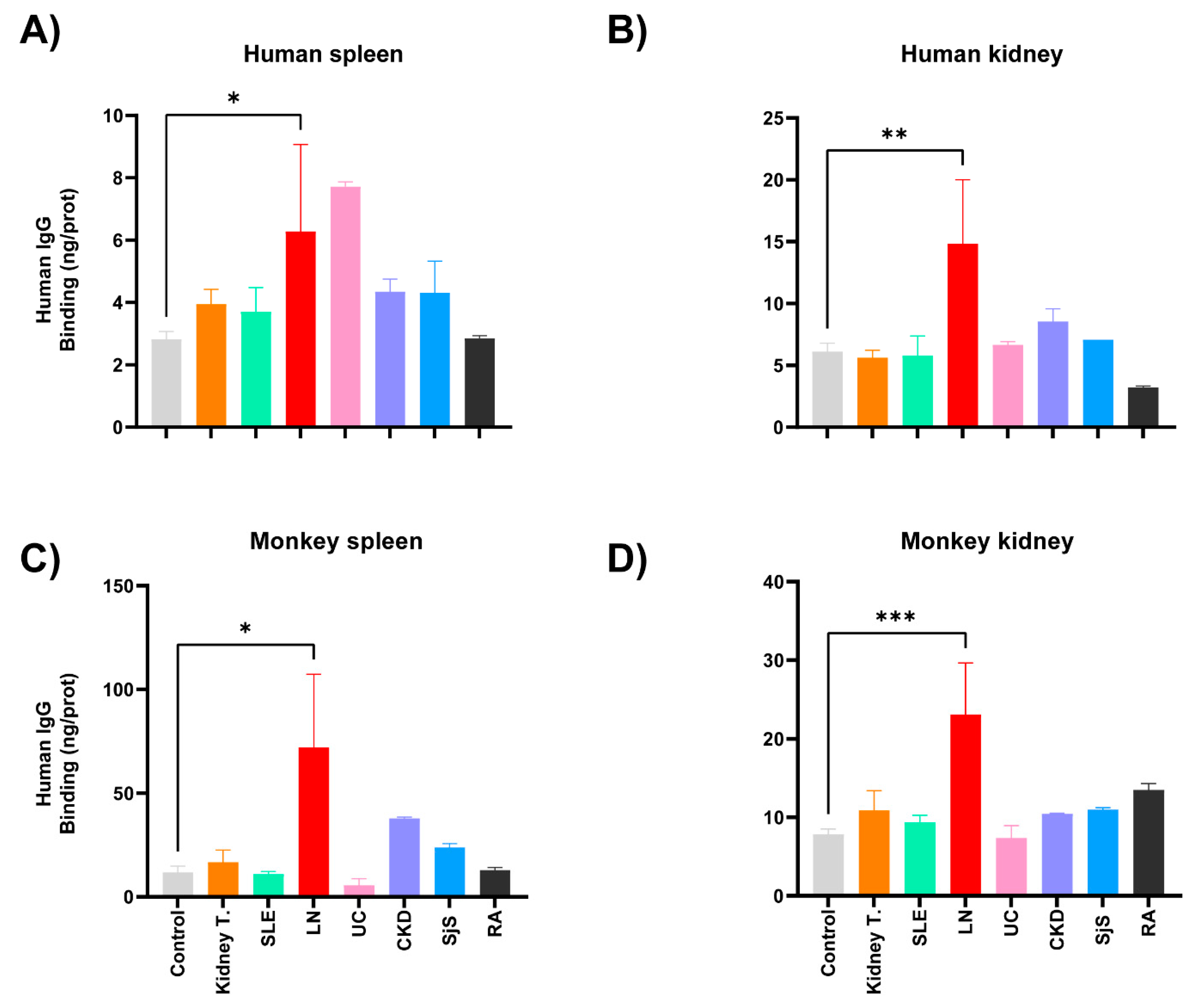
Figure 4.
ROC analysis: (A) for autoimmune disorders (SjS, AUC = 0.5309; UC, AUC = 0.6543; and KT, AUC = 0.6667), and (B) for lupus nephritic (LN, AUC =0.98) and for other autoimmune disorders (SLE, AUC= 0.5926; CDK, AUC= 0,7284; and RA, AUC = 0.6667).
Figure 4.
ROC analysis: (A) for autoimmune disorders (SjS, AUC = 0.5309; UC, AUC = 0.6543; and KT, AUC = 0.6667), and (B) for lupus nephritic (LN, AUC =0.98) and for other autoimmune disorders (SLE, AUC= 0.5926; CDK, AUC= 0,7284; and RA, AUC = 0.6667).
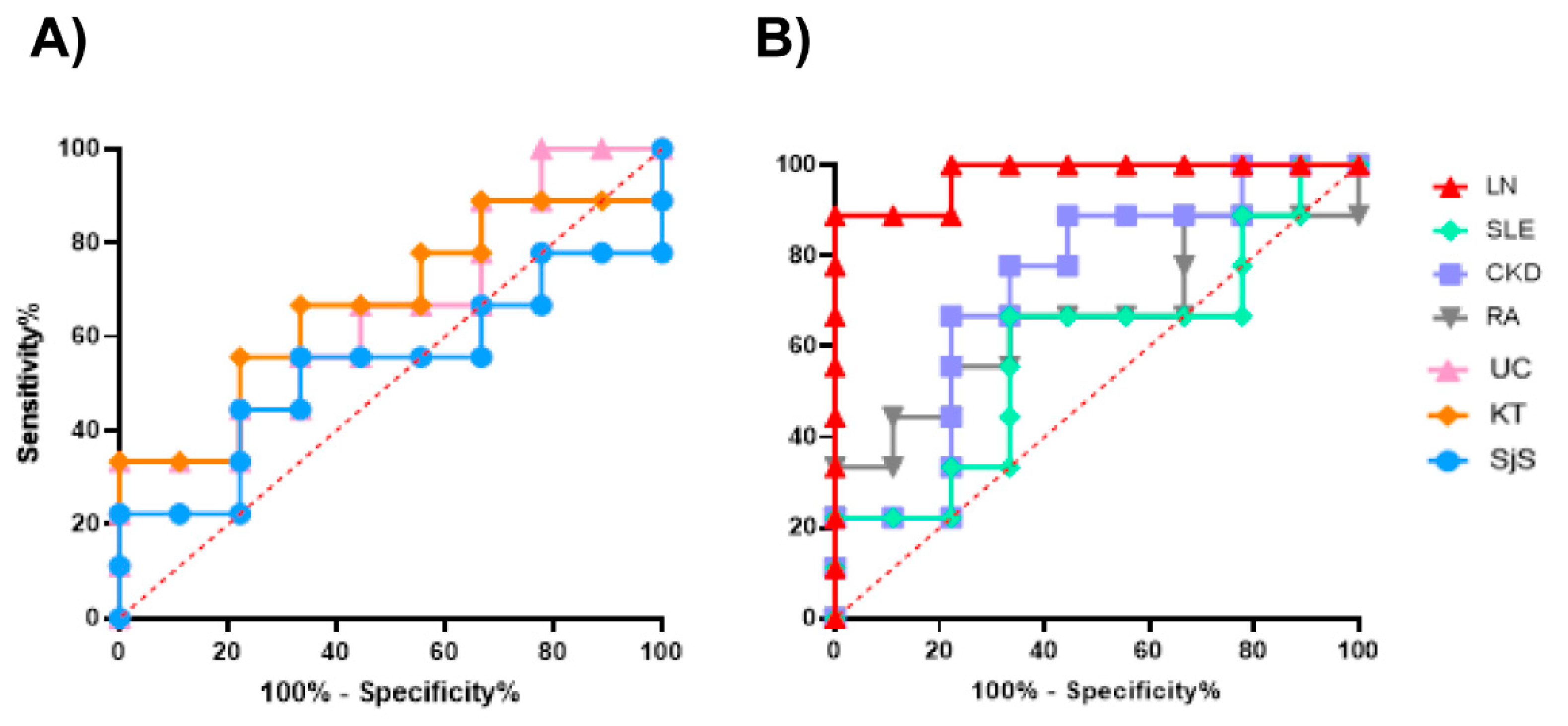
Figure 5.
Binding of human IgG from both healthy individuals and patients with KT to kidney, liver, or spleen samples from rat (R), monkey (M) and human (H) (ng/prot). p < 0.05 (*); p < 0.01 (**); p < 0.001 (***); and p < 0.0001 (****).
Figure 5.
Binding of human IgG from both healthy individuals and patients with KT to kidney, liver, or spleen samples from rat (R), monkey (M) and human (H) (ng/prot). p < 0.05 (*); p < 0.01 (**); p < 0.001 (***); and p < 0.0001 (****).
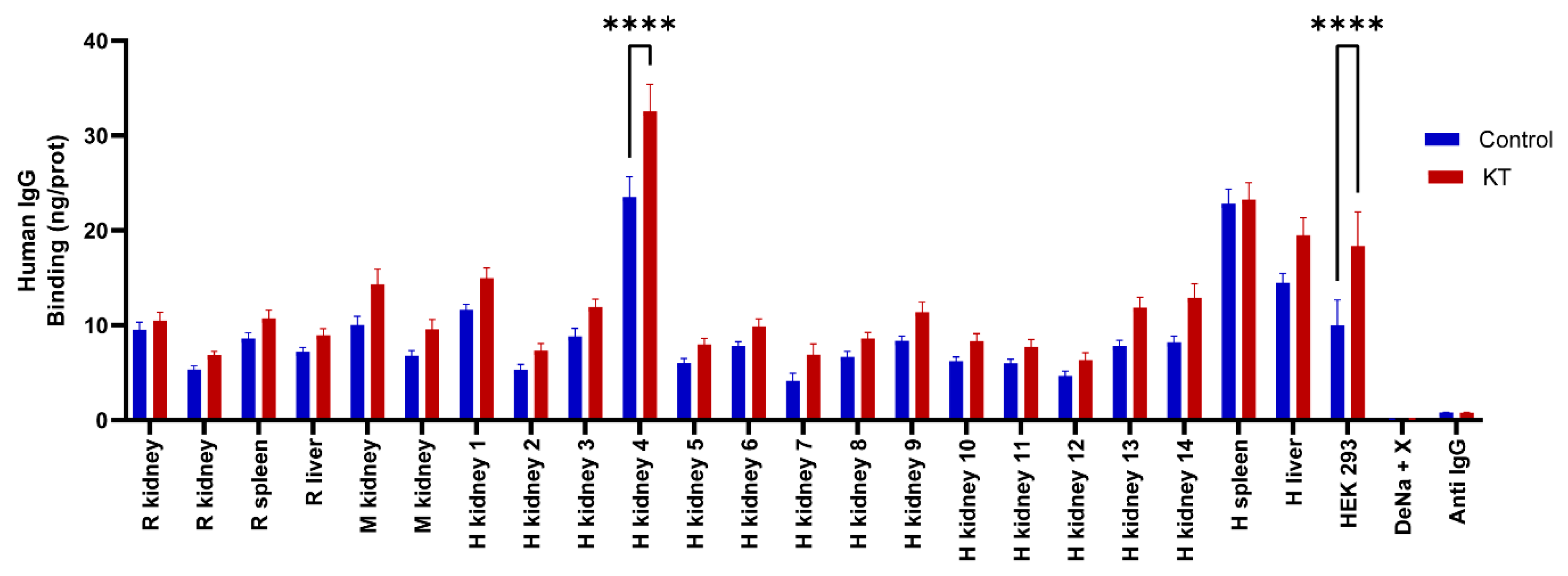
Figure 6.
Heat map obtained from ordinary two-way ANOVA with Bonferroni’s multiple comparison test. P valor of this test is represented on the heat map. p < 0.05 (*); p < 0.01 (**); p < 0.001 (**); and p < 0.0001 (****).
Figure 6.
Heat map obtained from ordinary two-way ANOVA with Bonferroni’s multiple comparison test. P valor of this test is represented on the heat map. p < 0.05 (*); p < 0.01 (**); p < 0.001 (**); and p < 0.0001 (****).
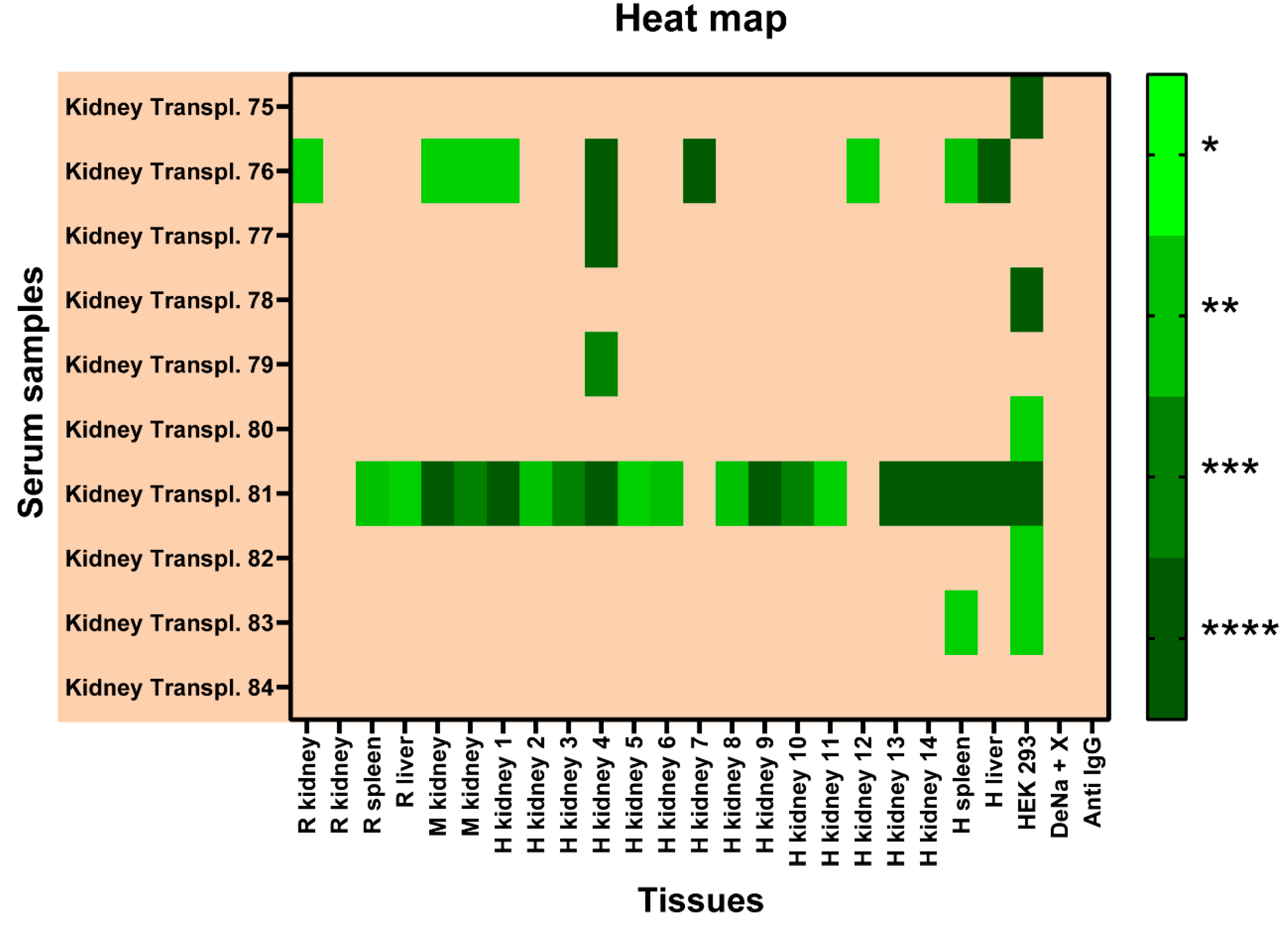
Figure 7.
Principal component analysis (PCA) to examine the fourth and the seven principal component (PC4, PC7) of the tissues. Left, representing sera. Right, representing tissues.
Figure 7.
Principal component analysis (PCA) to examine the fourth and the seven principal component (PC4, PC7) of the tissues. Left, representing sera. Right, representing tissues.
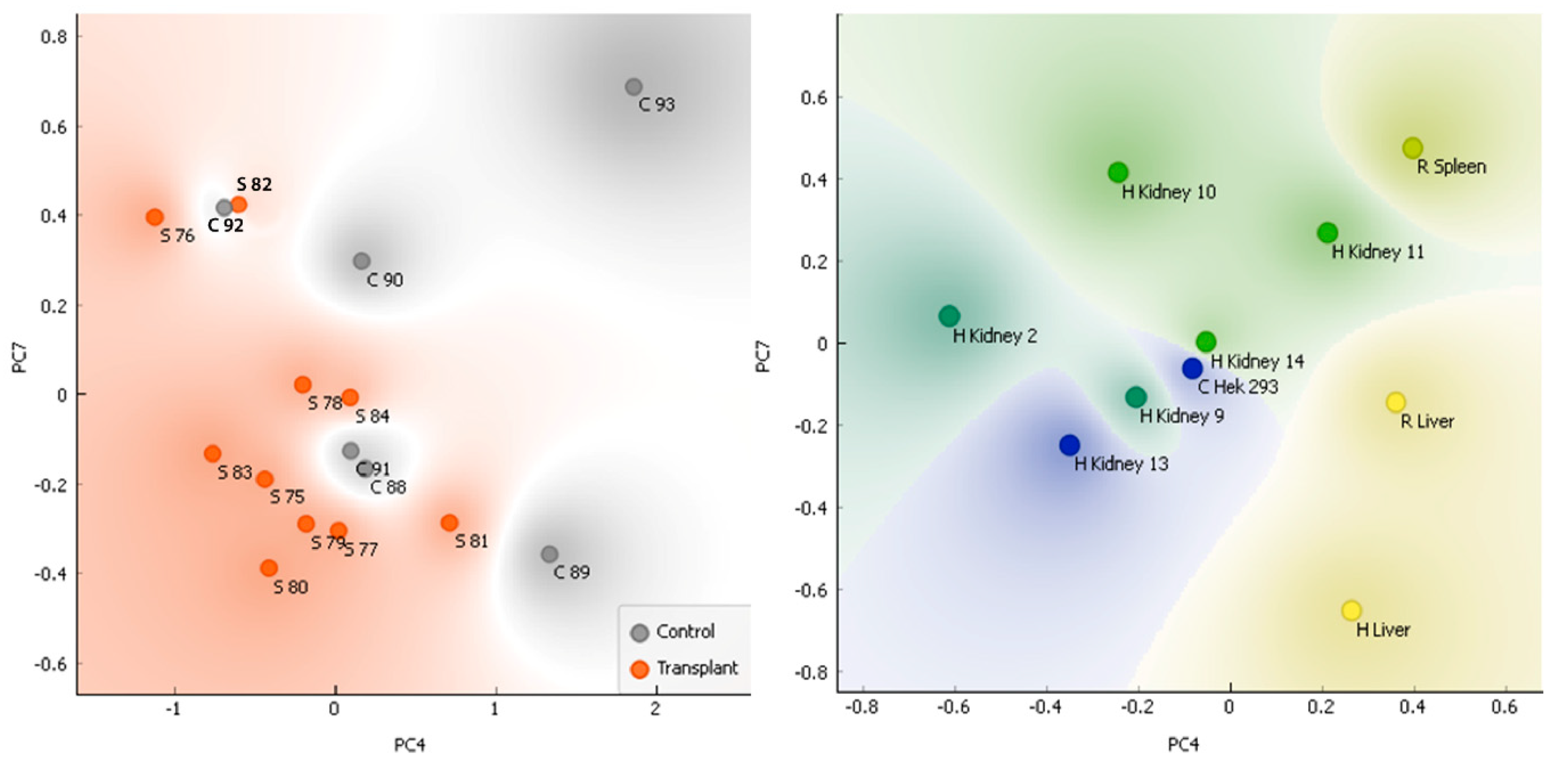
Figure 8.
ROC curve analysis for the sera of KT patients vs healthy controls (AUC = 0.82).
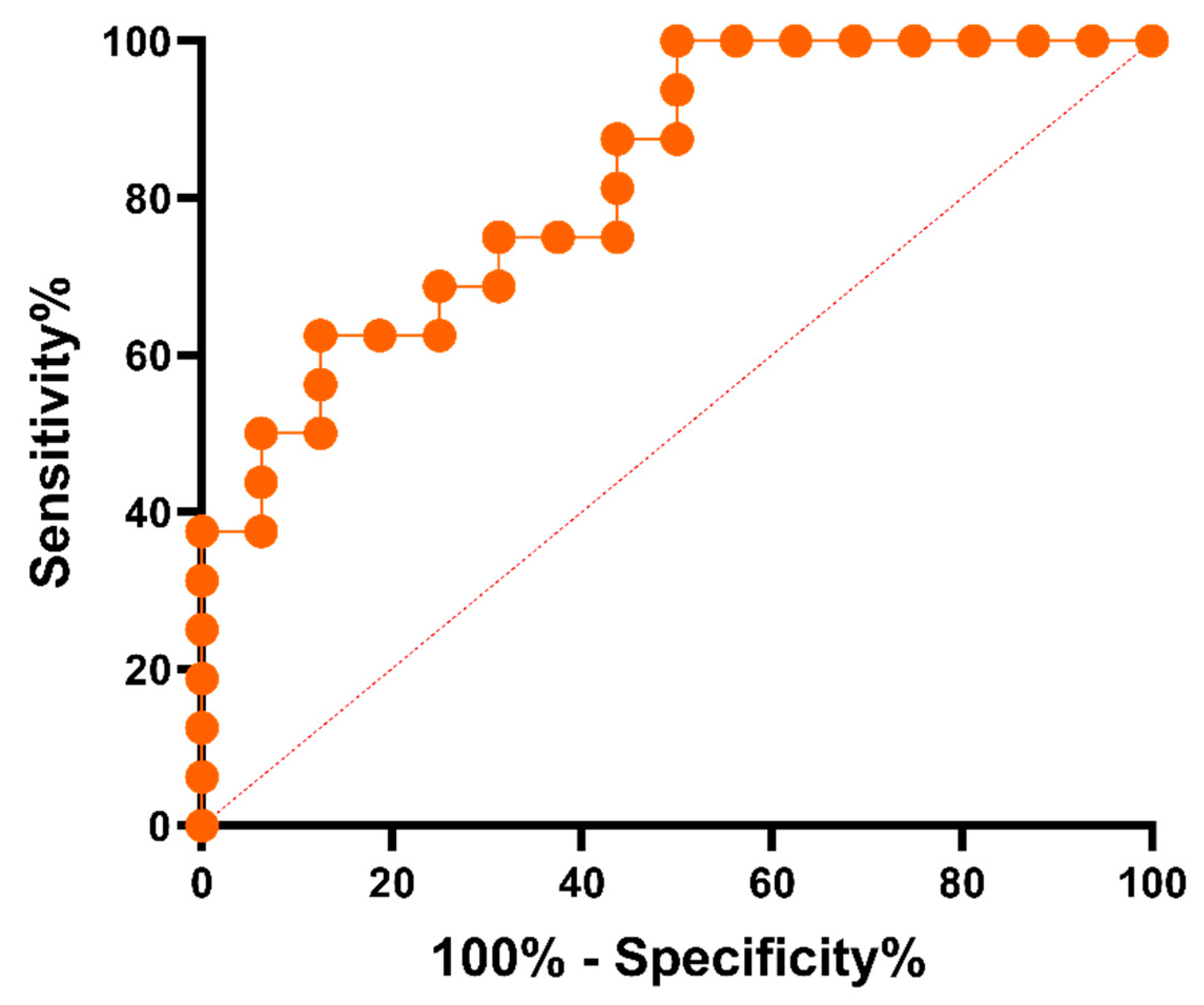
Figure 9.
Immunoassay procedure. Information of the CMMA and the samples used.
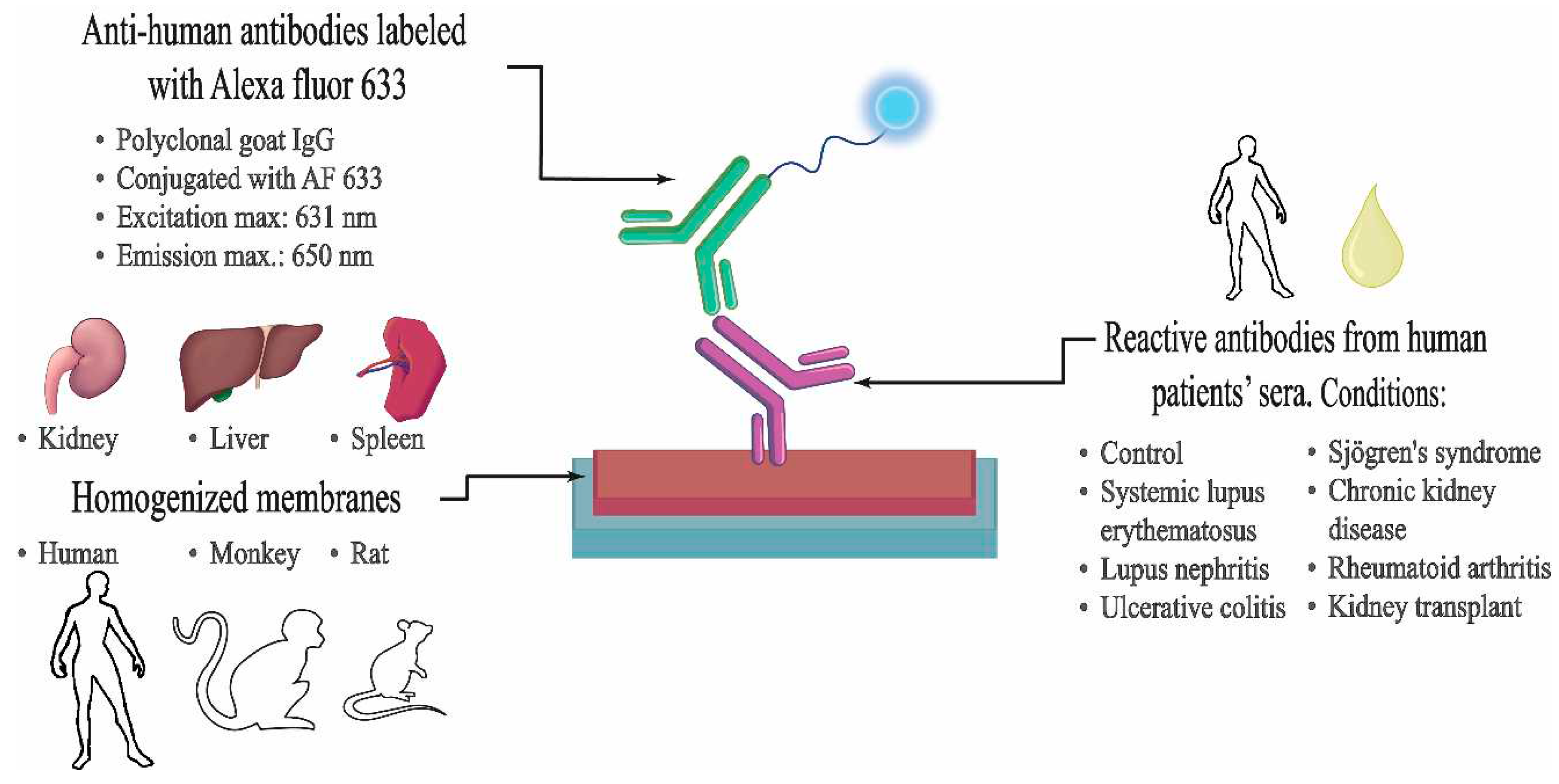
Table 3.
Information of the different human tissue samples used for CMMAs development.
| ID | Category | Anatomical Site | Sex | Age | Race | Procurement Type | Procurement Date |
|---|---|---|---|---|---|---|---|
| S6-32 Liver | Normal tissues | Liver | Male | 46 | Caucasian (White) | Autopsy | 18/03/2011 |
| S13-41 Spleen | Normal tissues | Spleen | Male | 48 | Caucasian (White) | Autopsy | 27/02/2012 |
| 90-M-13-28 Kidney, Cortex | Normal tissues | Kidney, Cortex and Medulla | Male | 44 | Caucasian (White) | Autopsy | 12/01/2015 |
| 4650955 Kidney CM | Normal tissues | Kidney, Cortex and Medulla | Female | 69 | Caucasian (White) | Autopsy | 02/05/2017 |
| 4641480 Kidney CM | Normal tissues | Kidney, Cortex and Medulla | Female | 70 | Caucasian (White) | Autopsy | 28/04/2017 |
| 4647875 Kidney CM | Normal tissues | Kidney, Cortex and Medulla | Female | 68 | Caucasian (White) | Autopsy | 27/04/2017 |
| 4638771 Kidney CM | Normal tissues | Kidney, Cortex and Medulla | Male | 60 | Caucasian (White) | Autopsy | 19/04/2017 |
| 4698698 Kidney CM | Normal tissues | Kidney, Cortex and Medulla | Female | 52 | Caucasian (White) | Autopsy | 17/08/2017 |
| 4645480 Kidney CM | Normal tissues | Kidney, Cortex and Medulla | Male | 48 | Caucasian (White) | Autopsy | 18/04/2017 |
| 113-AFJF Kidney CM | Normal tissues | Kidney, Cortex and Medulla | Male | 60 | Caucasian (White) | Organ recovery | 08/10/2018 |
| A27 Kidney Medulla | Normal tissues | Kidney, Medulla | Male | 50 | Caucasian (White) | Autopsy | 14/04/2007 |
| S1-32 Kidney Medulla | Normal tissues | Kidney, Medulla | Male | 38 | Caucasian (White) | Autopsy | 18/02/2015 |
| S2-32 Kidney Medulla | Normal tissues | Kidney, Medulla | Female | 52 | Caucasian (White) | Autopsy | 24/02/2015 |
| 113-AGET292 Kidney Cortex | Normal tissues | Kidney, Cortex | Male | 41 | Caucasian (White) | Organ recovery | 24/05/2019 |
| 113-AHAM474 Kidney Cortex | Normal tissues | Kidney, Cortex | Male | 64 | Caucasian (White) | Organ recovery | 13/01/2020 |
| 4616286 Kidney CM | Normal tissues | Kidney, Cortex | Female | 46 | Caucasian (White) | Organ recovery | 24/02/2016 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



