Submitted:
28 December 2023
Posted:
29 December 2023
You are already at the latest version
Abstract
Background: Pediatric Rapid Response Teams (RRTs) are expected to significantly lower pediatric mortality in healthcare settings. This study evaluates RRTs' effectiveness in decreasing cardiac arrests and unexpected Pediatric Intensive Care Unit (PICU) admissions.
Methods: A quasi-experimental study (2014-2017) at King Abdulaziz University Hospital, Jeddah, Saudi Arabia, involved 3,261 pediatric inpatients, split into pre-intervention (1,604) and post-intervention (1,657) groups. The intervention entailed pediatric specialists collaboratively managing acute decompensations following set protocols.
Results: RRT was activated 471 times, primarily for respiratory distress (29.30%), sepsis (22.30%), clinical anxiety (13.80%), and hematological abnormalities (6.7%). Family concerns triggered 0.1% of activations. Post-RRT implementation, unplanned PICU admissions significantly reduced (RR = 0.552, 95% CI 0.485-0.628, P < 0.0001), and non-ICU cardiac arrests were eliminated (RR = 0). Patient care improvement was notable, with a -9.61 coefficient for PICU admissions (95% CI: -12.65 to -6.57, P < 0.001) and a -1.641 coefficient for non-ICU cardiac arrests (95% CI: -2.22 to -1.06, P < 0.001). Sensitivity analysis showed mixed results for PICU admissions, while zero-inflation Poisson analysis confirmed a reduction in non-ICU arrests.
Conclusions: The deployment of pediatric RRTs is associated with fewer unexpected PICU admissions and non-ICU cardiopulmonary arrests, indicating improved PICU management. Further research using robust scientific methods is necessary to conclusively determine RRTs' clinical benefits.
Keywords:
pediatric rapid response team
; pediatric intensive care units
; interrupted time series analysis
; cardiopulmonary arrest in children
; quasi-experimental study
1. Introduction
Background: Indeed, due to recent advancements in pediatric care and medical technology, the proportion of children who now survive once-fatal disorders that were once deadly has grown dramatically, changing the epidemiology of pediatric [1,2] ailments that affect between 0.4% and 0.7% of all children and account for 42% of pediatric inpatients and up to 53% of PICU admissions at any given time [3]. Similar situations can be found in wealthier countries. [4] As a result, hospitalized pediatric patients frequently experience medical emergencies [5,6]. These include unplanned ICU admission, cardiac arrest while hospitalized, and death. To begin, cardiorespiratory arrest in children is a rare but tragic complication of severe sickness in hospitals. [7] P. Suominen (2000), for example, observed 0.7% cardiopulmonary arrest among hospitalized children, [8] Amelia G. Reis (2002) 3%, [9] J. Zeng (2013) 0.18%), [10] A. Latif (2014) 3%, [11] and V. Rathore (2016) 0.7-3%. [12] Additionally, the Pediatric Data Quality System Collaborative Measure Workgroup [13] selected the unplanned PICU admission rate as one of the quality metrics to be used in a systematic evaluation to identify quality improvement activities. [3] It raises the expense of living, morbidity, and mortality. Unfortunately, this is a common occurrence. For example, Kathryn O. Mansell (2018) reported 105/450 (23.3%) unscheduled PICU transfers, [14] da Silva (2013) 28/116 (24.1%) [15] It could range from 30% to 57%. [16] Ward patients admitted to the PICU had a higher death rate (odds ratio 1.65, 95% confidence interval 1.08-2.51) and lasted nearly four days longer than emergency department patients. [17] According to El Halal, Michel Georges Dos Santos (2012), and other contributors, morality doubles. [18] Similar findings were found in other publications (2.78% versus 1.95%; P-value 0.001), the hazard ratio was 1.71 (95% CI: 1.5 to 1.9), and the PICU stay was longer (4.9 versus 3.6 days; P.001).[19]
To Err Is Human contending that the problem in health care is not bad individuals; rather, decent people operate in unsafe systems that must be improved. Since the publication of "To Err Is Human: Creating a Healthier System." [20], two new papers recognize improvements while arguing that we still have a long way to go to ensure that care is as safe as it should be for all patients. [21] According to Children's Health Coalition of America (CHCA) statistics, between 2003 and 2006, 19 participating institutions reported 16% of all occurrences involving a "failed escalation of care”. [22] As a result, healthcare institutions have pledged to invest in patient safety programs. [11,23,24,25] One such initiative was the establishment of a Pediatric quick response team, a critical domain of emergency patient management in the accreditation process of the healthcare business. [26]
Pediatric Early Warning Scores (PEWS) [27,28,29] are clinical evaluation tools used by nurses to identify children who are at risk of clinical deterioration. They calculate PEWS by analyzing vital signs, patient symptoms, and signs. Using a PEWS system, which uses an escalation algorithm to warn clinicians of high-risk patients requiring a bedside evaluation and assessment. Studies have shown that pediatric intensive care units (PICUs), in-hospital cardiac arrests, and overall mortality can all be reduced. PEWS, when used in conjunction with a pediatric rapid response team treatment strategy, has been shown to reduce in-hospital mortality, cardiac arrests, hospital stays, ICU stays, and monetary expenses. [30,31,32] King Abdulaziz University Hospital in Jeddah, Saudi Arabia, a tertiary-level academic hospital, initiated a pediatric rapid team-based quality improvement effort to improve patient safety and the standard of care. To the best of our knowledge, this is the first study to apply the Bayesian structural time series model to examine the pediatric rapid response team's causal involvement in reducing non-ICU cardiorespiratory arrest and unexpected pediatric ICU admission. As well as mortality.
2. Methods
Study Design and Setting: We executed a rigorous quasi-experimental cohort investigation employing a before-and-after methodology at the renowned King Abdulaziz University Hospital situated in Jeddah, Saudi Arabia. The pediatric facility of the hospital is equipped with 50 dedicated general pediatric beds and annually accommodates approximately 1,000 pediatric admissions. Our research encompassed a timeframe from January 1, 2014, through to July 30, 2017, assimilating an aggregate of 3,261 pediatric inpatients. This cohort was bifurcated into 1,604 patients from the pre-intervention epoch (spanning January 1, 2014, to August 30, 2015) and 1,677 patients from the subsequent post-intervention phase (from September 1, 2015, to July 30, 2017).
Participants and Inclusion Criteria: Our investigative purview concentrated on pediatric inpatients within the age bracket of one month to fourteen years who registered a minimum of one nocturnal stay in a medical ward during the stipulated duration. A meticulous selection criterion was adhered to, deliberately excluding neonates and patients ascribed a "no code" designation. To ensure methodological precision, our study's locus was stringently confined to the general pediatric ward. Therefore, auxiliary domains such as the Pediatric ICU, the emergency department, the post-operative unit, and the operation theatre were consciously omitted from the investigation.
Ethical Considerations: This research endeavor received endorsement from the Institutional Review Board, King Abdullah International Research Center, Riyadh, documented under reference number [23,79]. Owing to the inherently retrospective nature of the study, the imperative for informed consent was judiciously dispensed with.
Composition of the Pediatric Rapid Response Team (RRT): Our institution's RRT is spearheaded by a physician and encompasses a multidisciplinary ensemble, including a Pediatric Intensive Care Unit (PICU) attending physician, a specialized physician, and depending on the shift, either a day-time fellow/resident or an overnight PICU fellow/resident with the support of an attending. This team is augmented by the expertise of a critical care nurse and a respiratory therapist. Notably, the nursing care is singularly allocated to the RRTs, devoid of any other concurrent patient care commitments, ensuring undivided attention round the clock. However, during nocturnal hours, the physicians, and other affiliates, while primarily dedicated to the RRT, also cater to the needs of the PICU.
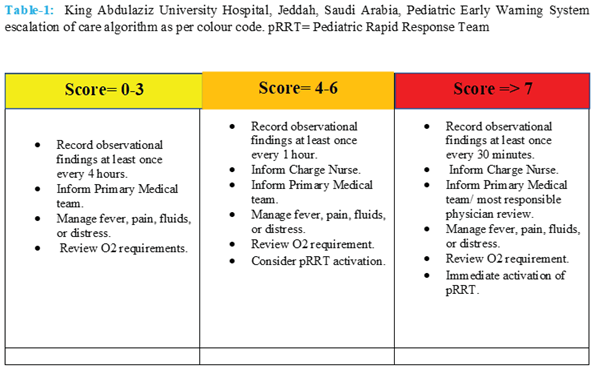
Activation and Scoring Mechanism: The RRT is promptly mobilized by invoking a dedicated pager system available for any ward patient in need. The evaluative framework for the RRT intervention employs the "Modified Pediatric Early Warning Score" or the "COAT score" (acronym for CHILDREN’s OBSERVATION AND ALERT TOOL). This tool is an adaptation from the esteemed NHS Institute for Innovation and Improvement's PEWS scoring matrix. It is pertinent to emphasize that the COAT tool is conceived as an adjunct to, and not a surrogate for, seasoned clinical discernment and comprehensive patient assessment. This evaluative mechanism probes nine salient clinical parameters as an integral component of the child’s periodic clinical surveillance, culminating in a COAT score that span between 0-26. To facilitate quick interpretation, these scores are delineated with distinct color codifications tailored for varied age brackets. It is observed that escalating COAT scores often correspond to deteriorating pediatric health. A granular action plan is orchestrated in alignment with the COAT score gradient: any score surpassing 3 is earmarked as a deviation from the norm, a score bracket of 4-6 serves as a heightened alert, urging contemplation for RRT deployment, while a score of 7 or beyond mandates the immediate summoning of the rapid response team. (Table 1)

 |
Data Acquisition: Data was collected prospectively for the intervention period and retrospectively for the pre-intervention period using electronic medical records. To assess the severity of cases before and after the intervention, a pediatric early warning signs baseline score was obtained. In addition, monthly data on pediatric ward admissions, age, gender, patient transfers to the PICU, cardiorespiratory arrest, PICU admission, and mortality were collected.
Outcome measures: The primary outcome indicators were the number of pediatric ward patients shifted to the PICU and non-ICU cardiorespiratory arrests per month. Outside of the ICU, a code was defined as any general ward patient who required tracheal intubation, chest compressions, or both respiratory and cardiopulmonary arrest. The secondary outcome for patients transported to the PICU after the quick response system is activated is mortality.
Statistical Analysis: Data preparation involved streamlining the dataset's baseline characteristics using the R package tableone. An interrupted time series (ITS) analysis was used to systematically examine the effectiveness of the Pediatric RRT in lowering the incidence of unexpected pediatric intensive care unit (PICU) admissions and non-ICU cardiac arrests. The robustness of this analytical approach in measuring the longitudinal impacts of interventions in quasi-experimental contexts was chosen. The ITS analysis was carried out in two stages: pre-intervention (from January 1, 2014, to August 30, 2015) and post-intervention (from September 1, 2015, to July 30, 2017). The trial enrolled 3,261 pediatric inpatients, with 1,604 and 1,677 patients participating in the pre- and post-intervention phases, respectively. The frequency of unplanned PICU admissions and non-ICU cardiac arrests were among the key factors examined. To assess the degree and importance of the intervention's effect, we calculated the coefficients for the time periods before and after the intervention, as well as the standard errors, t-values, and 95% confidence intervals. The statistical significance of the observed changes was tested using P-values. A statistically significant difference was defined as a P-value less than 0.05.
Finally, we used a comprehensive approach to sensitivity analysis, combining advanced statistical approaches with an interrupted time series (ITS) architecture. Bootstrapping was initially utilized to determine how stable the ITS model estimates for unscheduled PICU admissions were. This was accomplished by repeatedly resampling and recalculating the model's coefficients to determine how the size and direction of the effect varied over time. Moreover, segmented regression analysis was done to double check the results of bootstrapping. A Zero-Inflation Poisson (ZIP) model was also employed for sensitivity test to appropriately examine the post-intervention data, which revealed an excessive number of zeros in non-ICU cardiopulmonary arrests.
3. Results
Between January 1, 2014, and July 30, 2017, pediatric inpatients who spent at least one day in a medical ward were included in this study. The study comprised 3281 pediatric ward patients from the pre-intervention (1604) and post-intervention (1677) periods. Preintervention occurred between January 1, 2014, and August 30, 2015, and postintervention occurred between September 1, 2015, and July 30, 2017.The median PWES score for both groups are 6 (IQR 5-7), with a p-value of 0. 217. Gender, female 725(45.2%) versus 780 (46.5%) with p value 0.45. Preintervention median age 6(IQR 2-12), post intervention 7(IQR 3-24) months, p value 0.31. The median monthly pediatric ward to PICU admission fell from 21.5 [20.25-25.75] to 13 [10-18] with a p-value of 0.009, while the median non-ICU code fell from 2 [0.25-3] to zero with a p-value of 0.001 in a bivariate analysis. (Table 2) 471 pediatric rapid response teams have been activated in total: Respiratory distress (138/471, 29.30%), Sepsis (105/471, 22.30 %), Physician concern (65/471, 13.80 %), Hematology (32/471, 6.80 %), Cardiovascular (31/471,6.58%), Neurology (23/471, 4.88%), postoperative (9/471,1.91%) and family concern (3/471,0.1%) were the most common causes of activation. 487 individuals were admitted to the PICU prior to intervention: 487/1604 (30.5%) against 281/1677 (16.8%). Hence, unadjusted relative risk of unplan PICU admission 0.55 (0.48-0.63), p value 0.0001(Table 3). Similarly, prior to exposure to the program, cardiorespiratory arrest 24, having unexposed total 1604 ward patients, post intervention out of 1674, there are 0 events in the post-intervention group, the RR would be 0. This indicates a complete reduction in the event rate (Non-ICU Cardiopulmonary Arrest) post-intervention (Table 4). On the other hand, benefit from the activation of pediatric rapid response
A significant reduction in both unplanned pediatric intensive care unit (PICU) admissions (Figure 1) and non-intensive care unit (non-ICU) cardiopulmonary arrests (Code Blue) were observed in the interrupted time series (ITS) analysis examining the impact of the Pediatric Rapid Response Team intervention.(Figure 2) The intervention was significantly linked with a decrease in unplanned PICU admissions, as evidenced by the coefficient of -9.61 (95% CI: -12.65 to -6.57, p value 0.001) (Table 5). This means that the pediatric RRT activity resulted in 9.61 fewer unplanned PICU admissions per unit time. In parallel, the RRT intervention was associated with a significant reduction in non-ICU cardiac arrests, with a coefficient of -1.641 (95% CI: -2.22 to -1.06, p value 0.001), implying 1.64 fewer incidents per unit of time. (Table 5) These findings provide strong evidence for the RRTs intervention's effectiveness in improving crucial pediatric healthcare outcomes.
Sensitivity Test: Pre- and Post-Intervention Bootstrapped Coefficient Distribution for Unplanned Pediatric Intensive Care Unit (PICU) Admissions. This graph depicts the range of coefficients discovered using bootstrapping technique (N = 1000 resamples) to determine how a healthcare intervention affects persons who find up in the PICU unexpectedly. The original effect is depicted by a red dashed line with a mean difference of -9.61 in unplanned PICU admissions, demonstrating a decrease post-intervention. The green dashed lines represent the 95% confidence interval, which ranges from -3.65 to 4.04 and represents the variability in the estimated intervention impact. (Figure 3) This interval's broad range includes both negative and positive values, indicating significant variation across resampled datasets. This variation emphasizes how difficult it is to determine the precise impact of the intervention because it implies that, while there is an association with fewer PICU admissions, the strength and stability of this effect are variable and may depend on factors such as data noise, sample size, and the specifics of the intervention. Segmented Regression Analysis revealed a similar finding. (Figure 4) The impact of the Pediatric Rapid Response Team intervention is revealed by the Zero-Inflated Poisson (ZIP) model analysis for sensitivity testing for non-ICU cardiac arrest data. The intervention had a substantial beneficial effect on the zero-inflation component, which estimates the chance of zero occurrences (estimate = 5.081, p 0.001). This significant finding suggests that the intervention significantly increased the probability of having no post-intervention non-ICU cardiac arrests, thereby lowering their overall occurrence.
Discussion: This single-center, before-and-after quasi-experimental cohort research at King Abdulaziz University Hospital in Jeddah, Saudi Arabia, reported the establishment of a PICU physician-led fast response team. This study aimed to determine the causal link between the establishment of a pediatric rapid response team and primary outcomes such as unexpected PICU admission and non-ICU cardiorespiratory arrest. In addition, to investigate if the death rate of pediatric ward patients transferred to the PICU falls when the pediatric rapid response system was implemented. In our study, the median PWES score for both groups are 6 (IQR 5-6.75) and 6(IQR 5-7) with a p-value of 0. 217 respectively. Gender, female 725(45.2%) versus 780(46.5%) with p value 0.45. Preintervention median age 6(IQR 2-12), post intervention 7(IQR 3-24) months, p value 0.31. (Table 2) Hence, the disease severity score, age, and gender are matched in both groups. During our study period, 471 pediatric rapid response systems were activated throughout a 21-month period, corresponding to 281 rapid response team activations per 1000 pediatric admissions. In our analysis, we found that respiratory distress was the leading cause of pediatric rapid response team activation. (138/471, 29.30%), whereas previously published data ranged from 36.3% to 55.9%.[33,34,35,36,37] Furthermore, sepsis (105/471, 22.30%) is the second most prevalent cause, with a higher incidence reported by White K, Scott IA, and others co-workers (2016) at 29.5%, %, [38] a lower rate than ours at 16.1%, [33] and a higher incidence reported by Lockwood JM, Ziniel SI, and Bonafide CP (2021) at 44%. [39] The pediatric rapid response team is an excellent tool for initiating early goal-directed therapy for sepsis and lowering sepsis-related mortality.[40]
Crossing the Quality Chasm, a 2001 publication, encourages healthcare professionals and policymakers to implement new system methodologies and ideas to accomplish change. One of these ideas was for hospitals to form a rapid response team that family members could call if they were worried about their children. [41,42] In our research, family participation in the pediatric rapid response system was extremely poor (3/471, 0.64%). They are unmotivated to share responsibility for their sick offspring. Family involvement is currently critical to patient safety, especially in pediatric rapid response systems. [43] We know that parents are more likely than experienced physicians and nurses to notice significant changes in their child's temperament and behavior. Transfer to the ICU is less common when family members activate the fast response team (25% vs. 59%, p-value 0.001). [44,45] and reduce mortality [46] In a survey in USA, 69% of families urged to involve in pediatric rapid response team activation. [47] As a result, the National Patient Safety Organization and the Josie King Foundation have joined forces to support the family led activation of rapid response team. [48] In contrast, Albutt et al., (2016) cited that currently there is insufficient evidence demonstrating a family activated escalation service is the most effective way to prevent patient deterioration.[49] Other noteworthy causes of emergency system activation besides respiratory and sepsis were physician concern (65/471, 13.80%), hematology (32/471, 6.80%), cardiovascular (31/471, 6.58%), neurology (23/471, 4.88%), and postoperative complications (9/471, 1.91%).
To the best of our knowledge, this is the first study that examines the causal inference concerning the pediatric rapid response team influence on the reduction of unplanned PICU admissions and pediatric non-ICU cardiorespiratory arrest using the interrupted time series model. [50] The findings of the "100,000 Lives Campaign" prompted the Institute for Healthcare Improvement to propose using rapid response teams to improve patient safety outcomes. [51] Besides, the Joint Commission mandated that United States hospitals should establish rapid response system (RRSs) as part of the 2008 National Patient Safety Goals[52]There was some disagreement; Bradford, DD., and colleagues claimed that there is weak evidence that rapid response systems are associated with a reduction in hospital mortality and cardiac arrest rates based on a systemic review, but they acknowledged that the presence of heterogeneity limited their ability to make such an assumption. [53] Similarly, Hillman and Ken (2005) identified no statistically significant difference in cardiac arrest rates (1.64 vs. 1.31, p = 0.736) or unplanned ICU hospitalizations (4.68 vs. 4.19, p = 0.599). [54]
Unplanned pediatric critical care unit admissions are a major issue in the healthcare industry. According to the Pediatric Intensive Care Audit Network, unexpected hospitalizations in critical care units in the United Kingdom (UK) were caused by sudden clinical deterioration in at least 85% of cases in 2017. [55] According to Kause, Smith, Prytherch, and Parr (2004), the UK had 47.3% verses New Zealand had 24.2%.[56] Increased ventilation time [15], a longer PICU length of stay, higher mortality [17,18,19,57] , higher acuity, and increased expense are all outcomes of unplanned PICU admission.[16] Unplanned transfers, according to Christopher P. Bonafide and colleagues (2014), are associated with a 4.97-fold increased chance of death (95% CI, 3.33-7.40; P.001). [58] It is a low-quality metric. (3) The literature indicates that the adoption of pediatric rapid response teams reduced unplanned cardiac ICU transfers from 16.8 to 7.1 per 1000 patients per day, with a p value of 0.015. [59] Panesar et al. (2014) as well reported identical finding. [60] The duration of stay in the PICU was reduced (19.0%), and mortality was reduced (22%). After rapid response team implementation, the relative risk of death following unplanned admission to the PICU was 0.685. [61] Notably, 59.66% of our rapid response calls resulted in PICU admissions in our research, which is higher than the published data range of 30% to 57% [16,62,63,64] and a similar 59.6%. [57] However, prior to the rapid response team initiative, 63% of unplanned PICU admissions from the ward occurred, whereas this decreased to 33.57% when a modified PWES score-based pediatric rapid response team intervention was implemented. Furthermore, before and after intervention, PICU admissions from the general pediatric ward were 30.5% (487/1604) versus 16.8% (281/1677). Hence, unadjusted relative risk of unplan PICU admission 0.55 (0.48-0.63), p value 0.0001(Table 3). We were able to cut unexpected PICU admissions by 45%, a statistically meaningful reduction. Moreover, we observed in the interrupted time series (ITS) analysis examining the impact of the Pediatric Rapid Response Team intervention. (Figure 2) The intervention was significantly linked with a decrease in unplanned PICU admissions, as evidenced by the coefficient of -9.61 (95% CI: -12.65 to -6.57, p value 0.001) (Table 5). This means that the RRTs activity resulted in 9.61 fewer unplanned PICU admissions per unit time.
Cardiac arrest outside of the ICU is a severe, clinically significant, and frequently fatal event. [65,66] An event like this is frequently preceded by indications that a person's health is deteriorating. This implies that it is not always a sudden or unexpected occurrence. [67,68] When a patient exhibits clinical instability, prompt intervention may reduce the number of cardiac arrests and fatalities. [32] According to Berens (2011), 2-6% of pediatric patients suffer an in-hospital cardiac arrest. Children who have a cardiopulmonary arrest in the hospital have a poor survival rate (25-38%).[69] In our pediatric rapid response team intervention associated with a significant reduction in non-ICU cardiac arrests, with a coefficient of -1.641 (95% CI: -2.22 to -1.06, p value 0.001), implying 1.64 fewer incidents per unit of time. (Table 5) These findings provide strong evidence for the RRTs intervention's effectiveness in improving crucial pediatric healthcare outcomes. On this account, such an impact has been documented by many authors. Brilli RJ, Gibson R, and other colleagues (2007) pointed out RR 0.41; 95% confidence interval, 0–0.86; p-value 0.02).[70] Subsequently, Winters, Bradford D. (2013), RR 0.62 (CI 0.45 to 084) [71] Cardiorespiratory arrest RR = 0.64, 95% CI 0.55-0.74" in the pediatric group, according to Maharaj R (2015) [72], and Trubey R and co-workers (2019), RR = 0.27, 95% CI 0.07 to 0.95. [73] Paul J. Sharek and colleagues found that the intervention had a significant effect on non-ICU cardiorespiratory arrest; the estimated rate per 1000 admissions for the postintervention group was 0.29 times that of the preintervention group (95% CI, 0.10-0.65; P = 0.008). [74] Moreover, Chong SL and Goh MSL (2022) discovered identical results [75].Additionally, Saad Al-Qahtani, (2013) proclaimed that non-ICU cardiopulmonary arrests decreased from 1.4 to 0.9 per 1,000 hospital admissions (relative risk, 0.68; 95% confidence interval, 0.53–0.86; p = 0.001) [76] Joffe et al. discovered no difference (2011) [77], and Tibballs J (2009) reported that unexpected cardiac arrests did not change from 0.19 per 1000 to 0.17 per 1000 (risk ratio 0.91, 95% CI (0.50-1.64, p value 0.75). [78] Finally we can conclude that a systemic review and meta-analysis on this regards, cardiorespiratory arrest outside of ICU, RR 0.62 CI (0.46-0.84), I210.2, p=0.35).[79] We found that out of 1674 patients treated following the intervention, not even one had a code blue, but there were 24 cardiorespiratory arrests before the program was introduced. Consequently, the Pediatric Rapid Response Team intervention dropped the cardiac arrest from 24 to 0 incidents when compared to non-ICU cardiopulmonary arrests before and after the intervention. The intervention was successful in enhancing patient safety because there was no residual risk (RR = 0). (Table 4)
In our study, the mortality contrast between the pre- and post-exposure periods is striking. Of the 1,604 infants admitted during the pre-exposure epoch, 36 succumbed post-transfer to the PICU. This is juxtaposed against the subsequent phase, where merely three out of 1,677 patients met a similar fate. This translates to a mortality rate of 22.5 per 1,000 admissions in both the antecedent and subsequent periods to the initiative's introduction. The derived unadjusted risk ratio stands at 0.08, underpinned by a confidence interval of (0.02-0.25) and a highly significant p-value of 0.0001. Our findings resonate with the broader academic discourse. Sharek PJ (2007) observed a congruent trend, wherein the mean monthly mortality rate registered an 18% descent, moving from 1.01 to 0.83 deaths per 100 discharges, demarcated by a 95% CI of (5%-30%) and a p-value of 0.007 [33]. E. J. Sandhu et al. (2015) presented mortality figures reflecting a RR of 0.79, enclosed within a 95% confidence interval of 0.63-0.98 [83]. Maharaj R. (2015) echoed these findings, tabulating a mortality RR of 0.82, with a 95% CI bracketed between 0.76-0.89 [72]. In a later study, Santhanam S. (2018) documented an overarching hospital mortality rate with an RR of 0.79, emphasizing a CI spanning 0.63 to 0.98 [71]. Gong XY (2020) further enriched the literature with evidence accentuating a significant dip in hospital mortality (P = 0.025) [84]. Bolstering these narratives, a meticulous systematic review and meta-analysis inferred that the institution of a pediatric rapid response team is invariably tethered to a substantial decrement in hospital mortality, characterized by an RR of 0.88 and a 95% CI of (0.83-0.93) [85]. Notably, a departure from this prevailing consensus was registered only by Joffe AR and Anton NR (2011), who reported a neutral impact on hospital mortality [77]. Drawing from these rigorous empirical engagements and our findings, the critical role of Pediatric Rapid Response Team interventions in mitigating pediatric mortality emerges unequivocally.
The sensitivity analysis highlights the diversity in the impact of the Pediatric Rapid Response Team's (RRTs) intervention on unscheduled PICU admissions. Despite a mean admission decrease of -9.61 in the initial effect, there is significant variation suggested by the broad 95% confidence interval (-3.65 to 4.04) suggesting that the RRTs effect is inconsistent and could be impacted by factors like data noise and sample size.(Figure 3) This diversity is corroborated by the segmented regression analysis, which further emphasizes how difficult it is to measure the intervention's efficacy in decreasing unplanned PICU admissions.(Figure 4) On the other side, there is a clear positive effect when looking at non-ICU cardiac arrest data using the zero-inflated poisson (ZIP) model. The intervention's ability to minimize non-ICU cardiac arrests is shown by the significant increase in the likelihood of zero arrests post-intervention (estimate = 5.081, p 0.001). These results show how difficult it is to evaluate healthcare treatments. Further research with larger datasets or proper research technique is needed to clarify the influence of the pediatric RRTs on unplanned PICU admissions, as it shows promise in lowering non-ICU cardiac arrests.
This study's brief duration is one of its limitations. A thorough grasp of the long-term effects of the pediatric rapid response team on unanticipated PICU admissions and non-ICU cardiorespiratory arrests may not be possible given the short duration of the research. The fact that the study is based on observational studies, which are prone to bias and confounding and might not accurately reflect the true impact of the pediatric rapid response team, is a second limitation of the research. Thirdly, the generalizability of the study results outside the hospital where it was performed was constrained using single-center data. The results could be influenced by the pediatric patients' demographic, organizational, and clinical traits. Fourth, the impact of the pediatric rapid response team for reduction of hospital-wide mortality may not be accurately measured by the relative risk that was calculated without accounting for confounding factors. There are many significant missing variables in the research, such as the pediatric rapid response team's median response time, the patient outcomes following the activation of the rapid response team, the number of patients who remain in the ward, and their outcomes. The inability to compute the PRISM score for transferring patients from the ward restricted the ability to manage the impact of confounding variables. Another limitation of the research is the compliance rate of the pediatric rapid response team activation data lacking, based on modified early warning signs. It might have affected the study's results and prevented them from being extrapolated to other contexts where compliance rates might vary. Finally, the sensitivity test did not support the validity of our study finding particularly impact on reduction of unplanned PICU admission.
Our research is unique because of the novel methodology we used to validate our findings; we used ITS and then a sensitivity test. This method, in conjunction with the detailed depiction of the several charts, our study provides valuable insights into intervention efficacies and sets a high-level precedent for future efforts in evidence-based pediatric care research through the integration of these advanced statistical tools.
4. Conclusion
We must consider whether the significant benefit seen in this research because of the pediatric rapid response team's actions is a cause. More study needs to be done on this issue to attempt to demonstrate clear clinical benefits using strict scientific methods and standards.
Supplementary Materials
No supplementary file.
Author Contributions
The entire research process, from ideation to data collecting to analysis, was independently executed by Dr. Samah Al Harbi, MD, who is the only author of this work. She ensured the study was conducted in accordance with scientific standards and was responsible for writing the report and analyzing the data. Additionally, Dr. Al Harbi oversaw the project's ethical and logistical considerations and dealt with any correspondence pertaining to the publication of the manuscript. She takes full responsibility for the work and has given her final approval to the manuscript.
Funding
Not applicable.
Institutional Review Board Statement
This research endeavor received endorsement from the Institutional Review Board, King Abdullah Inter-national Research Center, Riyadh, documented under reference number 79-23. Owing to the inherently retrospective nature of the study, the imperative for informed consent was judiciously dispensed with.
Informed Consent Statement
Considering the nature of the study, consent from individual participants is not necessary. The data used in this study was anonymized beforehand.
Data Availability Statement
Data will be supplied on valid reason on request by the author.
Acknowledgments
I am grateful to Dr. Mohammed Shahab Uddin of the Pediatric Department at the Saudi Arabian Ministry of National Guard in Dammam. Crucial to the preparation of this study work has been his priceless support with modeling, statistical analysis, interpretation, and graphic display. Additionally, the entire pediatric intensive care unit and general pediatric department of King Abdulaziz University Hospital in Jeddah, Saudi Arabia, have our deepest gratitude. The success of the Pediatric Rapid Response Team's implementation may be attributed to the staff's unwavering commitment, extensive knowledge, and ability to work together. Their combined contributions have substantially enhanced the breadth and depth of my study.
Conflicts of Interest
Author has no conflicts of interest to declare.
References
- Cohen E, Kuo DZ, Agrawal R, Berry JG, Bhagat SKM, Simon TD, et al. Children with medical complexity: An emerging population for clinical and research initiatives. Pediatrics. 2011;127(3):529–38. [CrossRef]
- Elizabeth S. Barnert,Bergen B. Nelson LRT. Experts’ Perspectives toward a Population Health Approach for Children with Medical Complexity. Acad Pediatr. 2017;17(6):672–7. [CrossRef]
- Prutsky GJ, Padhya D, Ahmed AT, Almasri J, Farah WH, Prokop LJ, et al. Is unplanned PICU readmission a proper quality indicator? a systematic review and meta-Analysis. Hosp Pediatr. 2021;11(2):167–74. [CrossRef]
- Dewan T, Cohen E. Children with medical complexity in Canada. Paediatrics and Child Health (Canada). 2013;18(10):518–22. [CrossRef]
- Hillman KM, Bristow PJ, Chey T, Daffurn K, Jacques T, Norman SL, et al. Duration of life-threatening antecedents prior to intensive care admission. Intensive Care Med. 2002;28(11):1629–34. [CrossRef]
- Kause J, Smith G, Prytherch D, Parr M, Flabouris A, Hillman K. A comparison of Antecedents to Cardiac Arrests, Deaths and EMergency Intensive care Admissions in Australia and New Zealand, and the United Kingdom - The ACADEMIA study. Resuscitation. 2004;62(3):275–82. [CrossRef]
- Sandquist M, Tegtmeyer K. No more pediatric code blues on the floor: Evolution of pediatric rapid response teams and situational awareness plans. Transl Pediatr. 2018;7(4):291–8. [CrossRef]
- Suominen P, Olkkola KT, Voipio V, Korpela R, Palo R, Räsänen J. Utstein style reporting of in-hospital paediatric cardiopulmonary resuscitation. Resuscitation. 2000;45(1):17–25. [CrossRef]
- Song W, Chen S, Liu YS, He NN, Mo DF, Lan BQ, et al. A prospective investigation into the epidemiology of in-hospital cardiopulmonary resuscitation using the international Utstein reporting style. Hong Kong Journal of Emergency Medicine. 2011;18(6):391–6. [CrossRef]
- Zeng J, Qian S, Zheng M, Wang Y, Zhou G, Wang H. The epidemiology and resuscitation effects of cardiopulmonary arrest among hospitalized children and adolescents in Beijing: An observational study. Resuscitation. 2013;84(12):1685–90. [CrossRef]
- Latif A, Holzmueller CG, Pronovost PJ. Evaluating Safety Initiatives in Healthcare. Curr Anesthesiol Rep. 2014;4(2):100–6. [CrossRef]
- Rathore V, Bansal A, Singhi SC, Singhi P, Muralidharan J. Survival and neurological outcome following in-hospital paediatric cardiopulmonary resuscitation in North India. Paediatr Int Child Health. 2016;36(2):141–7. [CrossRef]
- Tang et al. 2005. 基因的改变NIH Public Access. Bone. 2008;23(1):1–7.
- Mansel KO, Chen SW, Mathews AA, Gothard MD, Bigham MT. Here and Gone: Rapid Transfer From the General Care Floor to the PICU. Hosp Pediatr. 2018;8(9):524–9. [CrossRef]
- Da Silva PSL, De Aguiar VE, Machado Fonseca MC. Risk factors and outcomes of unplanned PICU postoperative admissions: A nested case-control study. Pediatric Critical Care Medicine. 2013;14(4):420–8. [CrossRef]
- Krmpotic K, Lobos AT. Clinical Profile of Children Requiring Early Unplanned Admission to the PICU. Hosp Pediatr. 2013;3(3):212–8. [CrossRef]
- Odetola FO, Rosenberg AL, Davis MM, Clark SJ, Dechert RE, Shanley TP. Do outcomes vary according to the source of admission to the pediatric intensive care unit? Pediatric Critical Care Medicine. 2008;9(1):20–5. [CrossRef]
- El Halal MGDS, Barbieri E, Filho R, Trotta E, Carvalho P. Admission source and mortality in a pediatric intensive care unit. Indian Journal of Critical Care Medicine. 2012;16(2):81–6. [CrossRef]
- Tripathi S, Kim M. Outcome Differences Between Direct Admissions to the PICU From ED and Escalations From Floor. Hosp Pediatr. 2021;11(11):1237–49. [CrossRef]
- Palatnik AM. To err IS human. Vol. 11, Nursing Critical Care. 2016. 4 p.
- Bates DW, Singh H. Two decades since to err is human: An assessment of progress and emerging priorities in patient safety. Health Aff. 2018;37(11):1736–43. [CrossRef]
- Hayes LW, Dobyns EL, DiGiovine B, Brown AM, Jacobson S, Randall KH, et al. A multicenter collaborative approach to reducing pediatric codes outside the ICU. Pediatrics. 2012;129(3):1–7. [CrossRef]
- NHS England and NHS Improvement. Implementing the NHS patient safety strategy: Safer culture, safer systems, safer patients. NHS England [Internet]. 2019;(July):1–82. Available from: https://www.england.nhs.uk/wp-content/uploads/2020/08/190708_Patient_Safety_Strategy_for_website_v4.pdf.
- Jha AK, Larizgoitia I, Audera-Lopez C, Prasopa-Plaizier N, Waters H, Bates DW. The global burden of unsafe medical care: Analytic modelling of observational studies. BMJ Qual Saf. 2013;22(10):809–15. [CrossRef]
- Thomas K, Force MV, Rasmussen D, Dodd D, Whildin S. Rapid Response Team. Crit Care Nurse. 2007;27(1):20–7.
- Accreditation Canada. Required Organizational Practices. 2020;(January):33–4. Available from: https://www.rqhealth.ca/rqhr-service-lines-files/accreditation-canada-antimicrobial-stewardship-rop.
- Cho KJ, Kwon O, Kwon JM, Lee Y, Park H, Jeon KH, et al. Detecting patient deterioration using artificial intelligence in a rapid response system. Crit Care Med. 2020;(March 2019):E285–9. [CrossRef]
- Parshuram CS, Dryden-Palmer K, Farrell C, Gottesman R, Gray M, Hutchison JS, et al. Effect of a pediatric early warning system on all-cause mortality in Hospitalized pediatric patients: The epoch randomized clinical trial. JAMA - Journal of the American Medical Association. 2018;319(10):1002–12. [CrossRef]
- Mills D, Schmid A, Najajreh M, Al Nasser A, Awwad Y, Qattush K, et al. Implementation of a pediatric early warning score tool in a pediatric oncology Ward in Palestine. BMC Health Serv Res. 2021;21(1):1–8. [CrossRef]
- Tibballs J, Kinney S, Bellomo R. A prospective before-and-after trial of a medical emergency team (multiple letters) [3]. Medical Journal of Australia. 2004;180(6):308–10. [CrossRef]
- Bellomo R, Goldsmith D, Uchino S, Buckmaster J, Hart G, Opdam H, et al. Prospective controlled trial of effect of medical emergency team on postoperative morbidity and mortality rates. Crit Care Med. 2004;32(4):916–21. [CrossRef]
- Buist MD, Moore GE, Bernard SA, Waxman BP, Anderson JN, Nguyen T V. Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: Preliminary study. Br Med J. 2002;324(7334):387–90. [CrossRef]
- Sharek PJ, Parast LM, Leong K, Coombs J, Earnest K, Sullivan J, et al. Effect of a rapid response team on hospital-wide mortality and code rates outside the ICU in a Children’s Hospital. JAMA. 2007;298(19):2267–74. [CrossRef]
- Kukreti V, Gaiteiro R, Mohseni-Bod H. Implementation of a pediatric rapid response team: Experience of the Hospital for Sick Children in Toronto. Indian Pediatr. 2014;51(1):11–5. [CrossRef]
- McKeta AS, Hlavacek AM, Chowdhury SM, Scheurer M, Graham EM, Zyblewski SC, et al. Improved outcomes after implementation of a specialized pediatric cardiac rapid response team. Cardiol Young. 2021;31(10):1582–8. [CrossRef]
- Meulmester KM, Coss-bu JA, Meskill SD, Wakefield BM, Moore RH, Vachani JG. Characteristics and Outcomes of Pediatric Rapid Response With a Respiratory Trigger. Hosp Pediatr. 11(8):806–7. [CrossRef]
- Meulmester KM, Coss-Bu JA, Meskill SD, Wakefield BM, Moore RH, Vachani JG, et al. Characteristics and Outcomes of Pediatric Rapid Response With a Respiratory Trigger. Hosp Pediatr. 2021;11(8):806–7. [CrossRef]
- White K, Scott IA, Bernard A, McCulloch K, Vaux A, Joyce C, et al. Patient characteristics, interventions and outcomes of 1151 rapid response team activations in a tertiary hospital: a prospective study. Intern Med J. 2016;46(12):1398–406. [CrossRef]
- Lockwood JM, Ziniel SI, Bonafide CP, Brady PW, O’Leary ST, Reese J, et al. Characteristics of Pediatric Rapid Response Systems: Results From a Survey of PRIS Hospitals. Hosp Pediatr. 2021;11(2):144–52. [CrossRef]
- Jung B, Daurat A, De Jong A, Chanques G, Mahul M, Monnin M, et al. Rapid response team and hospital mortality in hospitalized patients. Intensive Care Med. 2016;42(4):494–504. [CrossRef]
- Rn FJG, Certificate PN, Rn GDL, Cert IC, Grad P, Clinnurs D, et al. Australian Critical Care Family initiated escalation of care for the deteriorating patient in hospital : Family centred care or just “ box ticking ”. Australian Critical Care. 2016;29(4):195–200. [CrossRef]
- Likosky DS. Clinical Microsystems : A Critical Framework for Crossing the Quality Chasm. 2014;33–7.
- Care P centred. IMPROVING QUALITY AND SAFETY BY FOCUSING CARE ON PATIENTS AND CONSUMERS Discussion paper Draft for public consultation. 2010;(September).
- Information A. FAMILY ACTIVATED RAPID RESPONSE TEAM WHAT WE KNOW FIVE YEARS LATER. 2012; [CrossRef]
- Bavare AC, Thomas JK, Elliott EP, Morgan AC, Graf JM. Family-Initiated Pediatric Rapid Response : Characteristics , Impetus , and Outcomes. 2018;40(2):2018. [CrossRef]
- Gill FJ, Leslie GD, Marshall AP. The Impact of Implementation of Family-Initiated Escalation of Care for the Deteriorating Patient in Hospital : A Systematic Review. 2016;13(January 2005):10–1. [CrossRef]
- Chen JG, Kemper AR, Odetola F, Cheifetz IM, Turner DA. Prevalence, Characteristics, and Opinions of Pediatric Rapid Response Teams in the United States. Hosp Pediatr. 2012;2(3):133–40. [CrossRef]
- Brady PW, Zix J, Brilli R, Wheeler DS, Griffith K, Giaccone MJ, et al. Developing and evaluating the success of a family activated medical emergency team : a quality improvement report. 2015;203–11. [CrossRef]
- Is there a role for patients and their relatives in escalating clinical deterioration in hospital ? A. 2017;20(5):2017. [CrossRef]
- Penfold RB, Zhang F. Use of interrupted time series analysis in evaluating health care quality improvements. Acad Pediatr. 2013;13(6): S38-S44. [CrossRef]
- Berwick DM, President F. Overview of the 100 , 000 Lives Campaign. 2014;(June 2006):0–1.
- Shantanam S, MUELLER. 乳鼠心肌提取 HHS Public Access. Physiol Behav. 2018;176(1):139–48.
- Bradford D, Cuong J, Elizabeth A, Peter J. Rapid response systems : A systematic review *. Crit Care Med. 2007;35(5):1238–43. [CrossRef]
- Hillman K, Chen J, Cretikos M, Bellomo R, Brown D, Finfer S, et al. Introduction of the medical emergency team ( MET ) system : a cluster-randomised controlled trial. Lancet. 366(9492):1164. [CrossRef]
- Taylor N, Hendron E, Manning JC. Paediatric family activated rapid response interventions ; qualitative systematic review. 2023;75(April). [CrossRef]
- Kause J, Smith G, Prytherch D, Parr M. A comparison of Antecedents to Cardiac Arrests , Deaths and EMergency Intensive care Admissions in Australia and New Zealand , and the United Kingdom — the ACADEMIA study for the Intensive Care Society ( UK ) & Australian and New Zealand Intensive. 2004;62:275–82. [CrossRef]
- Humphreys S, Humphreys S. Rapid Response Team Calls and Unplanned Transfers to the Pediatric Intensive Care Unit in a Pediatric Hospital. 25(2016). [CrossRef]
- Bonafide CP, Localio AR, Roberts KE, Nadkarni VM, Weirich CM, Keren R. Impact of rapid response system implementation on critical deterioration events in children. JAMA Pediatr. 2014;168(1):25–33. [CrossRef]
- Mcketa AS, Hlavacek AM, Chowdhury SM, Scheurer M, Eric M, Zyblewski SC, et al. Improved outcomes after implementation of a specialized pediatric cardiac rapid response team. 2022;31(10):1582–8. [CrossRef]
- Panesar R, Polikoff LA, Harris D, Mills B, Messina C, Parker MM. Characteristics and outcomes of pediatric rapid response teams before and after mandatory triggering by an elevated Pediatric Early Warning System (PEWS) score. Hosp Pediatr. 2014;4(3):135–40. [CrossRef]
- Kolovos NS, Gill J, Michelson PH, Doctor A, Hartman ME. Reduction in mortality following pediatric rapid response team implementation. Pediatric Critical Care Medicine. 2018;19(5):477–82. [CrossRef]
- Kinney S, Tibballs J, Johnston L, Duke T. Clinical profile of hospitalized children provided with urgent assistance from a medical emergency team. Pediatrics. 2008;121(6):1577–84. [CrossRef]
- Tibballs J, Kinney S. Reduction of hospital mortality and of preventable cardiac arrest and death on introduction of a pediatric medical emergency team. Pediatric Critical Care Medicine. 2009;10(3). [CrossRef]
- Berrens ZJ, Gosdin CH, Brady PW. Response in a Satellite Facility. 2020;20(2):172–7. [CrossRef]
- Survival after cardiac arrest in hospital. 1977;1(8024):92435. [CrossRef]
- Survival after Cardiopulmonary Resuscitation in the Hospital. 1983;1983. [CrossRef]
- Schein RMH, Hazday N, Pena M, Ruben BH, Sprung CL, Metrics P, et al. Clinical Antecedents to In-Hospital Cardiopulmonary Arrest. 1990;98(6). [CrossRef]
- Franklin C, Mathew J. Developing strategies to prevent inhospital cardiac arrest : analyzing responses of physicians and nurses in the hours before the event. 1994;22(2):7–8.
- McLellan MC, Gauvreau K, Connor JA. Validation of the Children’s Hospital Early Warning System for Critical Deterioration Recognition. J Pediatr Nurs [Internet]. 2017;32:52–8. [CrossRef]
- Brilli RJ, Gibson R, Luria JW, Wheeler TA, Shaw J, Linam M, et al. Implementation of a medical emergency team in a large pediatric teaching hospital prevents respiratory and cardiopulmonary arrests outside the intensive care unit. Pediatric Critical Care Medicine. 2007;8(3):236–46. [CrossRef]
- Shantanam S, MUELLER. Rapid-Response Systems as a Patient Safety Strategy. Physiol Behav. 2018;176(1):139–48.
- Maharaj R, Raffaele I, Wendon J. Rapid response systems: A systematic review and meta-analysis. Crit Care [Internet]. 2015;19(1):1–15. [CrossRef]
- Trubey R, Huang C, Lugg-widger F V, Hood K, Allen D, Edwards D, et al. Validity and effectiveness of paediatric early warning systems and track and trigger tools for identifying and reducing clinical deterioration in hospitalised children : a systematic review. 2019;1–22. [CrossRef]
- Sharek PJ, Parast LM, Leong K, Coombs J, Earnest K, Sullivan J, et al. Effect of a rapid response team on hospital-wide mortality and code rates outside the ICU in a Children’s Hospital. JAMA. 2007;298(19):2267–74. [CrossRef]
- Chong SL, Goh MSL, Ong GYK, Acworth J, Sultana R, Yao SHW, et al. Do paediatric early warning systems reduce mortality and critical deterioration events among children? A systematic review and meta-analysis. Resusc Plus [Internet]. 2022;11(May):100262. [CrossRef]
- Al-Qahtani S, Al-Dorzi HM, Tamim HM, Hussain S, Fong L, Taher S, et al. Impact of an intensivist-led multidisciplinary extended rapid response team on hospital-wide cardiopulmonary arrests and mortality. Crit Care Med. 2013;41(2):506–17. [CrossRef]
- Joffe AR, Anton NR, Burkholder SC. Reduction in hospital mortality over time in a hospital without a pediatric medical emergency team: Limitations of before-and-after study designs. Arch Pediatr Adolesc Med. 2011;165(5):419–23. [CrossRef]
- Tibballs J, Kinney S. Reduction of hospital mortality and of preventable cardiac arrest and death on introduction of a pediatric medical emergency team. Pediatric Critical Care Medicine. 2009;10(3). [CrossRef]
- Sandhu EJ. Rapid response teams. American Journal of Nursing. 2015;115(6):13. [CrossRef]
- Uddin MS, Abdulrahman K. Impact of Covid-19 Measures on Children Infection Related Hospitalization . Estimation of Causal Inference from observational Data , Using the Google Causal Impact , A Bayesian Structural Time-series Model. 2021;4(1):118–23. [CrossRef]
- Id JL, Id DJS, Id GIA, Id RH, Id RA, Id AZ, et al. PLOS COMPUTATIONAL BIOLOGY Bayesian structural time series for biomedical sensor data : A flexible modeling framework for evaluating interventions. 2021;1–21. [CrossRef]
- Liu J, Spakowicz D, Hoyd R, Ash G, Lou S, Lee D, et al. Bayesian Structural Time Series for Mobile Health and Sensor Data: A Flexible Modeling Framework for Evaluating Interventions. bioRxiv [Internet]. 2020 Mar 4 [cited 2020 Oct 21];2020.03.02.973677. [CrossRef]
- Sandhu EJ. Rapid response teams. American Journal of Nursing. 2015;115(6):13. [CrossRef]
- Gong XY, Wang YG, Shao HY, Lan P, Yan RS, Pan KH, et al. A rapid response team is associated with reduced overall hospital mortality in a Chinese tertiary hospital: a 9-year cohort study. Ann Transl Med. 2020;8(6):317–317. [CrossRef]
- Solomon RS, Corwin GS, Barclay DC, Quddusi SF, Dannenberg MD. Effectiveness of rapid response teams on rates of in-hospital cardiopulmonary arrest and mortality: A systematic review and meta-analysis. J Hosp Med. 2016;11(6):438–45. [CrossRef]
Figure 1.
This figure illustrates the results of the Interrupted Time Series (ITS) analysis focusing on the impact of the Pediatric Rapid Response Team intervention on unplanned Pediatric Intensive Care Unit (PICU) admissions. The plot displays the observed unplanned PICU admission rates over time alongside the fitted values predicted by the ITS model. A vertical grey dashed line indicates the intervention's implementation in September 2015, demarcating the pre- and post-intervention phases. The trend lines provide a visual representation of unplanned PICU admissions, demonstrating a notable decrease following the introduction of the RRTs intervention.
Figure 1.
This figure illustrates the results of the Interrupted Time Series (ITS) analysis focusing on the impact of the Pediatric Rapid Response Team intervention on unplanned Pediatric Intensive Care Unit (PICU) admissions. The plot displays the observed unplanned PICU admission rates over time alongside the fitted values predicted by the ITS model. A vertical grey dashed line indicates the intervention's implementation in September 2015, demarcating the pre- and post-intervention phases. The trend lines provide a visual representation of unplanned PICU admissions, demonstrating a notable decrease following the introduction of the RRTs intervention.
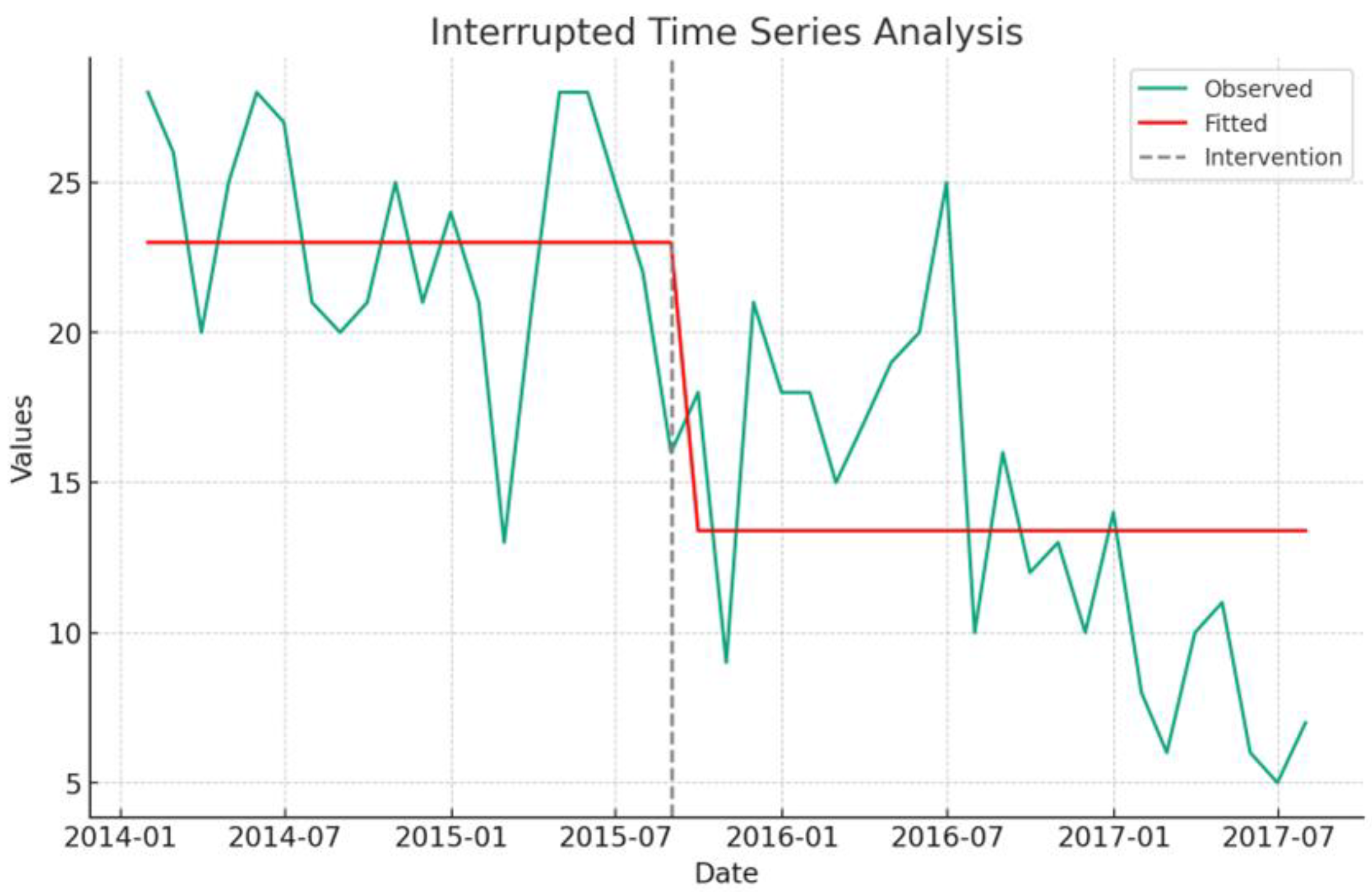
Figure 2.
An Interrupted Time Series (ITS) analysis displays the monthly counts of non-ICU cardiorespiratory arrests in pediatric patients from January 2014 to July 2017, with observed data and fitted model values illustrated in distinct line styles. The implementation of the Pediatric Rapid Response Team in September 2015 is denoted by a grey dashed line, serving as a demarcation for comparing trends and assessing the intervention's impact in the pre- and post-intervention periods.
Figure 2.
An Interrupted Time Series (ITS) analysis displays the monthly counts of non-ICU cardiorespiratory arrests in pediatric patients from January 2014 to July 2017, with observed data and fitted model values illustrated in distinct line styles. The implementation of the Pediatric Rapid Response Team in September 2015 is denoted by a grey dashed line, serving as a demarcation for comparing trends and assessing the intervention's impact in the pre- and post-intervention periods.
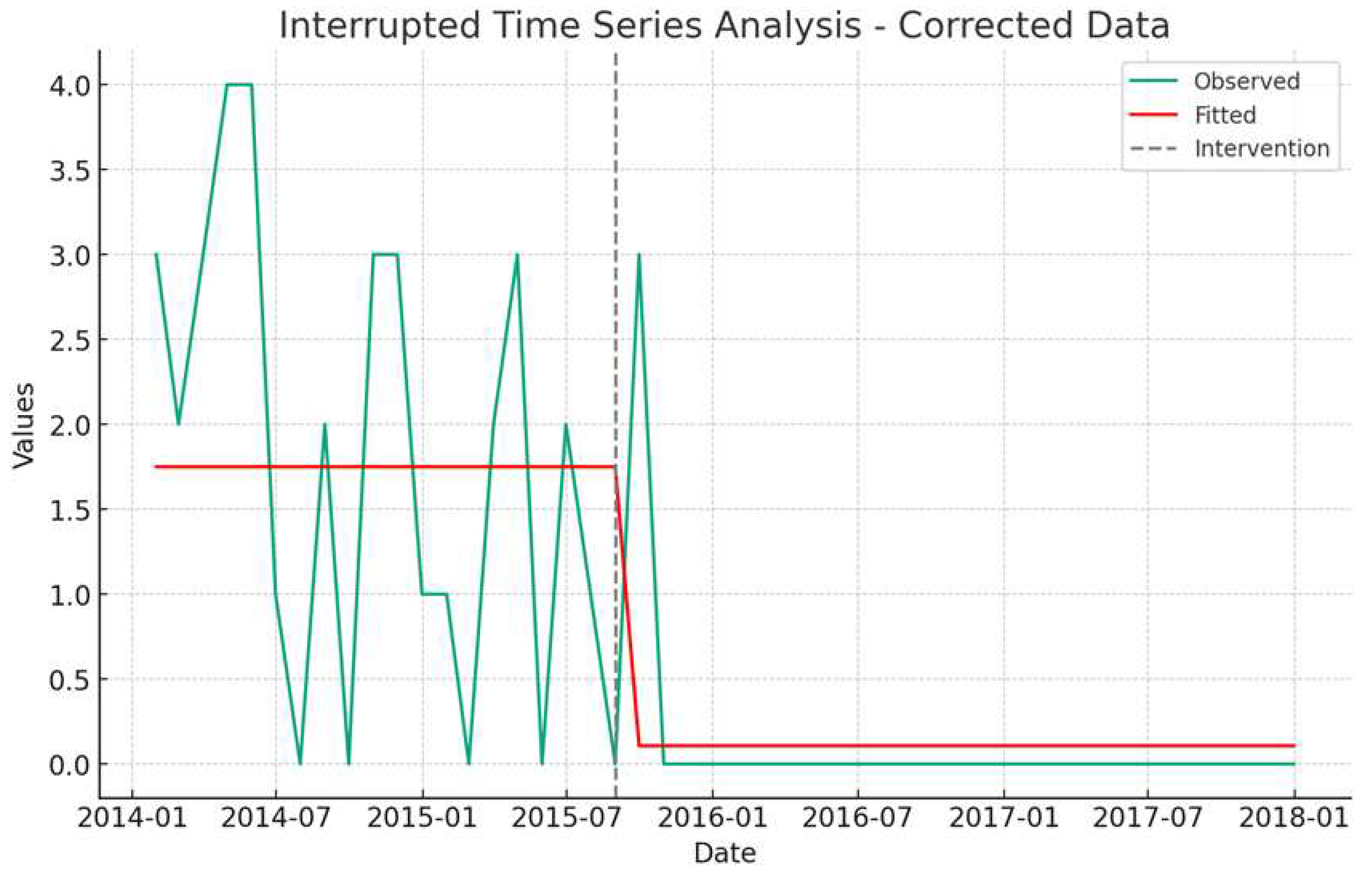
Figure 3.
Sensitivity Test by Bootstrapped Coefficient Distribution for Unplanned PICU Admissions. This histogram depicts the distribution from 1000 bootstrapped samples analyzing the impact of a healthcare intervention on unplanned PICU admissions. The original mean difference of -9.61 (red dashed line) suggests a reduction in admissions post-intervention. The 95% confidence interval, ranging from -3.65 to 4.04 (green dashed lines), indicates substantial variability in the intervention's effect.
Figure 3.
Sensitivity Test by Bootstrapped Coefficient Distribution for Unplanned PICU Admissions. This histogram depicts the distribution from 1000 bootstrapped samples analyzing the impact of a healthcare intervention on unplanned PICU admissions. The original mean difference of -9.61 (red dashed line) suggests a reduction in admissions post-intervention. The 95% confidence interval, ranging from -3.65 to 4.04 (green dashed lines), indicates substantial variability in the intervention's effect.

Table 2.
Comparative Outcomes Pre- and Post-Intervention. Both cohorts exhibited a consistent PEWS median score of 6 (p=0.217). Demographic variables, including median age and gender, showed no significant disparities (p=0.31 and p=0.45, respectively). However, metrics like Ward to PICU admission (WdToPICUAd), inPtcode events (Pediatric code outside of ICU), PICU mortality, and MortalityWAd (Mortality of PICU patients with unplanned transfer from Ward) were notably significant (p<0.05 for each).
Table 2.
Comparative Outcomes Pre- and Post-Intervention. Both cohorts exhibited a consistent PEWS median score of 6 (p=0.217). Demographic variables, including median age and gender, showed no significant disparities (p=0.31 and p=0.45, respectively). However, metrics like Ward to PICU admission (WdToPICUAd), inPtcode events (Pediatric code outside of ICU), PICU mortality, and MortalityWAd (Mortality of PICU patients with unplanned transfer from Ward) were notably significant (p<0.05 for each).
| Variable | Pre-intervention | Post-intervention | p-value |
| Date range | January 1, 2014, to August 30, 2015, | 1st September 2015, to July 30, 2017. | x |
| Total number of months | 22 | 21 | x |
| PEWS score (median [IQR]) | 6.00 [5.00, 6.75] | 6.00 [5.00, 7.00] | 0.217 |
| Age, median (IQR) | 6(IQR 2-12), | 7(IQR 3-24) | 0.31 |
| Gender, Female (%) | 725(45.2%) | 780(46.5%) | 0.45 |
| Ward admission (median [IQR]) | 72.50 [67.25, 79.75] | 80.00 [78.00, 82.00] | 0.009 |
| WdToPICUAd (median [IQR]) | 21.50 [20.25, 25.75] | 13.00 [10.00, 18.00] | <0.001 |
| inPtcode (median [IQR]) | 2.00 [0.25, 3.00] | 0.00 [0.00, 0.00] | <0.001 |
| PICU Mortality (median [IQR]) | 3.00 [2.00, 3.00] | 1.00 [1.00, 2.00] | 0.001 |
| MortalityWAd (median [IQR]) | 2.00 [0.25, 2.00] | 0.00 [0.00, 0.00] | <0.001 |
Table 3.
Shows a two-by-two contingency table evaluating the impact of a Pediatric Rapid Response Team on unplanned PICU admissions. Comparing pre- and post-intervention periods, the data reveals a notable reduction in admissions, with an estimated relative risk of 0.552 and a 95% confidence interval of 0.485 to 0.628, demonstrating a significant decrease (P-value < 0.0001). This highlights the RRTs effectiveness in enhancing patient safety and quality of care in high-impact healthcare settings.
Table 3.
Shows a two-by-two contingency table evaluating the impact of a Pediatric Rapid Response Team on unplanned PICU admissions. Comparing pre- and post-intervention periods, the data reveals a notable reduction in admissions, with an estimated relative risk of 0.552 and a 95% confidence interval of 0.485 to 0.628, demonstrating a significant decrease (P-value < 0.0001). This highlights the RRTs effectiveness in enhancing patient safety and quality of care in high-impact healthcare settings.
| PICU Admission | Non PICU Admission | Total | |
| Exposed (Post Intervention) | 281 | 1396 | 1677 |
| Un-Exposed (Pre-Intervention) | 487 | 1117 | 1604 |
| Total | 768 | 2513 | 3281 |
| Results: Estimate 0.552, 95% CI 0.485-0.628), P-value 0.0001 | |||
Table 4.
Compares non-ICU cardiopulmonary arrests before and after the Pediatric Rapid Response Team intervention, showing a reduction from 24 to 0 cases. This complete elimination post-intervention (RR=0) highlights the intervention's effectiveness in improving patient safety.
Table 4.
Compares non-ICU cardiopulmonary arrests before and after the Pediatric Rapid Response Team intervention, showing a reduction from 24 to 0 cases. This complete elimination post-intervention (RR=0) highlights the intervention's effectiveness in improving patient safety.
| College | Cardiopulmonary Arrest | No Cardiopulmonary Arrest | Total |
| Pre-Intervention | 24 | 1580 | 1604 |
| Post- Intervention | 0 | 1674 | 1674 |
| Total | 24 | 3254 | 3278 |
| Results: Since there are 0 events in the post-intervention group, the RR would be 0. This indicates a complete reduction in the event rate (Non-ICU Cardiopulmonary Arrest) post-intervention. | |||
team, unadjusted relative risk of mortality 0.08(0.03-0.26), p-value 0.0001. Interestingly, pre versus post period PICU sources of admission from ward 487/779 (62.5%), 281/837(33.6%) respectively. PICU observed crude mortality 7.7 % versus 3.0%.
Table 5.
Interrupted Time Series analysis results, evaluating Pediatric Rapid Response Team effects on Unplanned PICU Admissions and Non-ICU Cardiopulmonary Arrests. Coefficients indicate change in outcomes post-intervention; negative values denote reductions. Standard errors assess estimate precision, t-values test the effect significance, and 95% Confidence Intervals indicate probable coefficient range. P-values (<0.001) demonstrate strong evidence against the null hypothesis. Results suggest significant reductions in both unplanned PICU admissions and Non-ICU Cardiopulmonary Arrests post-RRTs implementation.
Table 5.
Interrupted Time Series analysis results, evaluating Pediatric Rapid Response Team effects on Unplanned PICU Admissions and Non-ICU Cardiopulmonary Arrests. Coefficients indicate change in outcomes post-intervention; negative values denote reductions. Standard errors assess estimate precision, t-values test the effect significance, and 95% Confidence Intervals indicate probable coefficient range. P-values (<0.001) demonstrate strong evidence against the null hypothesis. Results suggest significant reductions in both unplanned PICU admissions and Non-ICU Cardiopulmonary Arrests post-RRTs implementation.
| Variable | Coefficient | Std Error | t- value | 95% CI | P-value |
| Unplanned PICU Admission | |||||
| Intercept | 23.00 | 1.100 | 20.97 | 20.78-25.22 | <0.001 |
| RRTs action | -9.61 | 1.504 | -6.391 | -12.65 to -6.57 | <0.001 |
| Non-ICU Cardiopulmonary Arrest (Code Blue) | |||||
| Intercept | 1.750 | 0.220 | 7.963 | 1.31-2.19 | <0.001 |
| RRTs action | -1.641 | 0.288 | -5.71 | -2.22 to -1.06 | <-0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



